Embed Size (px)
Citation preview

HYGIENE PROMOTION FOR DIARRHOEAL DISEASES PREVENTION THROUGH THE
GOVRNMENT OF MALAWI’S PERINATAL CARE SYSTEM & COMMUNITY BASED CHILD CARE
CENTRES (CBCCCS)
STATUS OF NATIONAL HWTS POLICIES, GOVERNMENT EFFORTS
AND ENABLING ENVIRONMENTBY
H. D. MASUKUDEPUTY DIRECTOR OF PREVENTIVE HEALTH SERVICES - MOH
VIP HOTELMAPUTO, MOZAMBIQUE
20TH JUNE 2012

OUTLINE OF PRESENTATION
Introduction Background Information Overall Objectives Expected Results/Outcomes Activities of the Project Successes Observed Challenges Government efforts, enabling environment &
policies

INTRODUCTION Govt of Malawi Ministry of Health in collaboration
with UNICEF & PSI/MW piloted hygiene promotion through targeting mothers who attend ANC (May 2007 – Mar 2008)
The initiative focused on the following key hygiene improvement interventions:– safe storage and treatment of water at the household level (point-
of-use)– Hand washing with soap at critical times– Access to and effective use of sanitation facilities e. g. pit latrines
In 2009 the initiative extended to CBCCs in the same impact areas
INTRODUCTION (Cont..) The initiative was implemented as part of GOMs
ACSD programme. Project was funded by USAID through UNICEF Implemented by MOH and PSI/MW Project piloted in two districts: Blantyre and
Salima– 15 health facilities were involved (8 in Blantyre & 7 in
Salima) US CDC did baseline survey & follow-up (final)
evaluation of the project.

BACKGROUND INFORMATION(PROJECT CONTEXT)
Malawi population: almost 12 m Women make up 51% of total pop.
– 42% of these are WCB age (15 -49 years old) An estimated 550,000 women are pregnant
each year 93% of preg. Women attend ANC from
skilled providers

BACKGROUND INFORMATION/ PROJECT CONTEXT(Cont..)
While use of ANC services was high, about 57% of preg. women delivered at a health facility Very few mothers (7%) reported back for
postnatal checks MMR remain very high (984/100,000 LB) –
(now 675/100,000 LB – 2010 MDHS) Under five and child mortality remain high

BACKGROUND INFORMATION (Cont..)
Main causes of child deaths: malaria, diarrhoeal diseases and ARI (DHS 2004)
HIV & AIDS also contribute to the morbidity &mortality
In recent National surveys (2004 MDHS), about 20% of Children U/5 suffered an episode of diarrhoea 2 wks preceding data collection
Contaminated drinking water & poor hygiene are some of the factors contributing to poor indicators
BACKGROUND INFORMATION (Cont..)
Access to improved sanitation was about 46% Surveys by different institutions had shown
that hygiene behaviour were poor– 2005 evaluation of IMCI prog.(2000-2004)– PSI data collected in 2005e.g. proper hand washing: ranged between 35 -
50% after using the latrine, <10% before feeding or cooking (UNICEF & GoM 2005; PSI, 2006)

STRATEGIC OBJECTIVES/PURPOSE
To explore and document a new programming approach for influencing hygiene behaviour among mothers through promotion of three key hygiene practices:– Correct methods and frequency of handwashing– Proper use of latrines incl disposal of children’s faeces– Proper treatment and storage of drinking water at point
of use (household)

STRATEGIC OBJECTIVES/PURPOSE (Cont..) To use a pregnancy period as a motivating
period for adoption of good water handling practices and hygiene behaviours

OVERALL OBJECTIVES
To reduce morbidity and mortality from diarrhoeal diseases among children under five. To establish the antenatal care system as a
viable platform for the promotion of key hygiene promotion products and education messages for diarrhoeal disease reduction

EXPECTED RESULTS Increased access to hygiene improvement
products by 15,000 women around 15 HF in SA & BT districts
Increased competencies of 345 health workers to educate and demonstrate 3 key hygiene behaviours during antenatal visits
A systematic monitoring & assessment available on the project process, impact of hygiene kit provision & usage, and prevalence of diarrhoeal diseases in target districts

ACTIVITIES OF THE PROJECT Baseline survey Training of health workers Distribution of hygiene kits & refills to ANC mothers
– Kit comprised of: Water storage bucket with tap A bottle of Water guard, ORS, & hand-soap
Hygiene promotion campaigns Follow up of mothers to monitor use of the supplies Water quality testing Evaluation survey (s)

Activities of the project

SUCCESSES OBSERVED

Water Storage and Treatment (For Program Participants)
CharacteristicBaseline (N=389)
Follow-up (N=330)
Stores drinking water 99% 100%Container with lid± 93% 97%Removes by tap or pouring* 3% 52%“Protects” drinking water* 86% 99%
WaterGuard* 44% 91%Boil* 34% 16%Chlorine stock solution 13% 12%
±p<0.02 ,*p<0.0001

WaterGuard Knowledge and Use(For Program Participants)
CharacteristicBaseline (N=389)
Follow-up (N=330)
Heard of WaterGuard* 87% >99%
Knows correct procedure for WaterGuard use (No. caps, wait time)*
29% 62%
Ever used WaterGuard* 60% 100%
*p<0.0001

Observed WaterGuard Use(For Program Participants)
CharacteristicBaseline (N=231)
Follow-up (N=182)
Observed WG use*(WG bottle + residual chlorine)
2% 61%
Observed WG use AND purchase WG(WG bottle + residual chlorine +
purchase)
(est. 2%) 33%
*p<0.0001

Diffusion to Community (Friends/ relatives of program participants)
CharacteristicBaseline (N=230)
Follow-up (N=164)
WATER TREATMENTFriend in program shared information ---- 62%Observed WG use* 2% 29%Observed WG use AND purchase WG*
(est. 2%) 26%
HANDWASHING STEPS 1. Uses soap to wash hands* 23% 66%2. Lathers hands completely* 18% 61%3. Air dries or uses clean towel 44% 41%
*p<0.0001
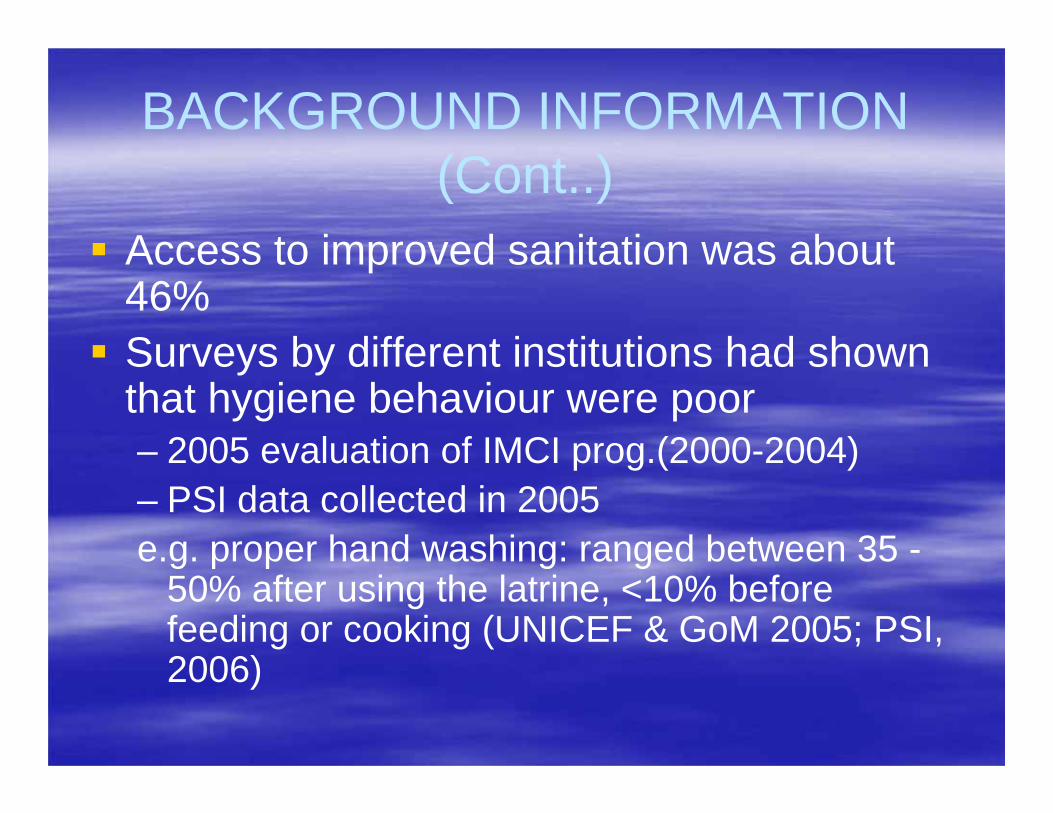
Pregnancy Outcomes
Characteristic
Percent of Participants
Blantyre (N*=182)
Percent of Participants
Salima (N*=148)
3 or more antenatal visits 73 72Delivery at health facility 89 59Postnatal check 71 41Baby alive 93 95Baby seen by health care provider 89 94
*N may vary by small numbers

DIARRHOEAL DISEASES CONTROL THROUGH CBCCCs

Activities done
Baseline survey Briefing extension workers Training care givers on key hygiene
practices Distribution of kits and refills Hygiene promotion campaigns Follow up of children in homes Evaluation was supposed to be
conducted after six months but delayed.

Introduction
This is an extension to diarrhoeal control through perinatal care It started in October 2009 Funded by UNICEF Targeting 3400 beneficiaries in both
districts (2400 children and 1000 pregnant women in 1st trimester)

Activities done
Program evaluation data was collected in 2011 and partially analyzed by district statisticians without guidance
At the dissemination meeting in February 2012, it was recommended that the data needed to be cleaned and
the credibility of the data was also questioned since it was collected by extension workers who were implementing the project.

Machinga District:Safe Water and Hygiene Program

Program Partners
Ministry of Health Malawi Clinton Health Access Initiative (CHAI) PATH Population Services International (PSI) Centers for Disease Control and
Prevention (CDC)

Program Implementation-2009
Training of clinic staff in SWS and handwashing Water and Hygiene Kits distributed in 15 health
facilities throughout Machinga District Provided 4 refills of WaterGuard and soap at ANC
and postnatal care visits to promote clinic attendance
Partner of pregnant woman must be present at ANC visit in order to receive Water Hygiene Kit
Health Surveillance Assistant (HSA) home visits provided ongoing education and monitoring


Results: Observed WaterGuard Use(For Program Participants)
Baseline (n=106)
Follow-up (n=97)
Observed WG use (WG bottle + residual chlorine) * 0% 69%
Observed WG use AND purchase of WG * 0% 36%
* p < 0.0001

Observed WG bottle in home Residual chlorine in stored water
+
Observed WaterGuardUse

Confirmed WaterGuard Use by HSA visits
Percent of Program
Participantswith
ConfirmedWG use
Number of HSA Visits
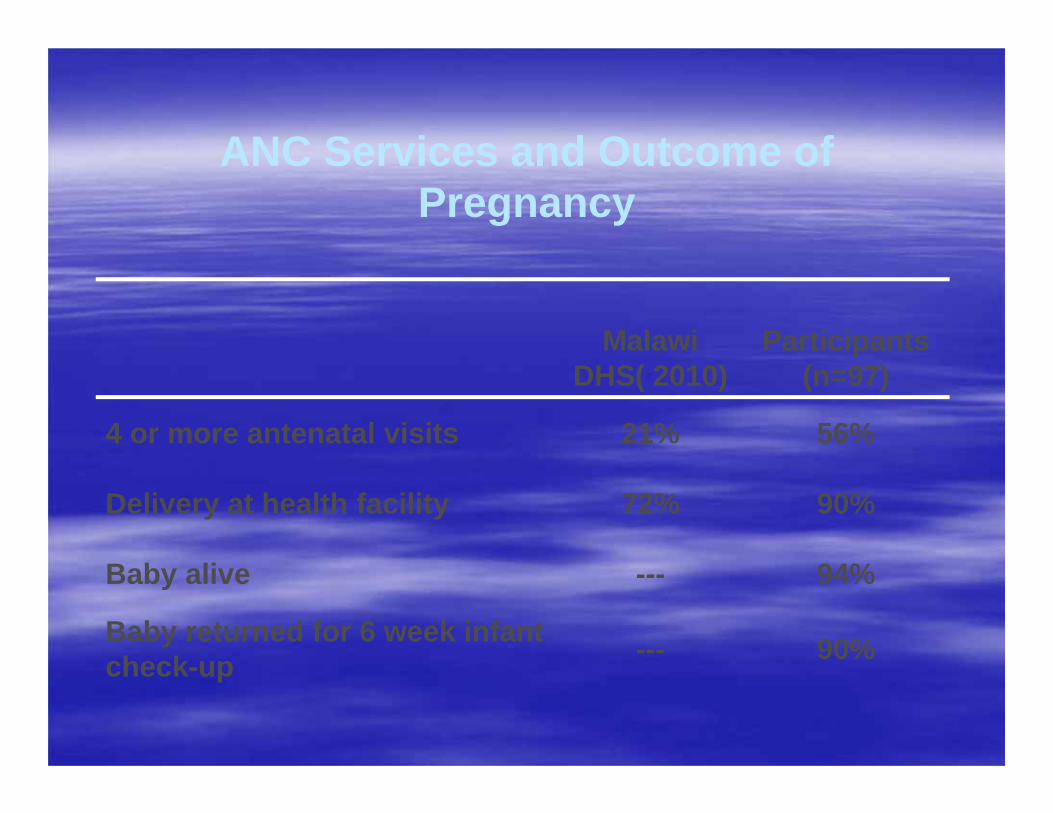
ANC Services and Outcome of Pregnancy
Malawi DHS( 2010)
Participants (n=97)
4 or more antenatal visits 21% 56%
Delivery at health facility 72% 90%
Baby alive --- 94%
Baby returned for 6 week infant check-up --- 90%
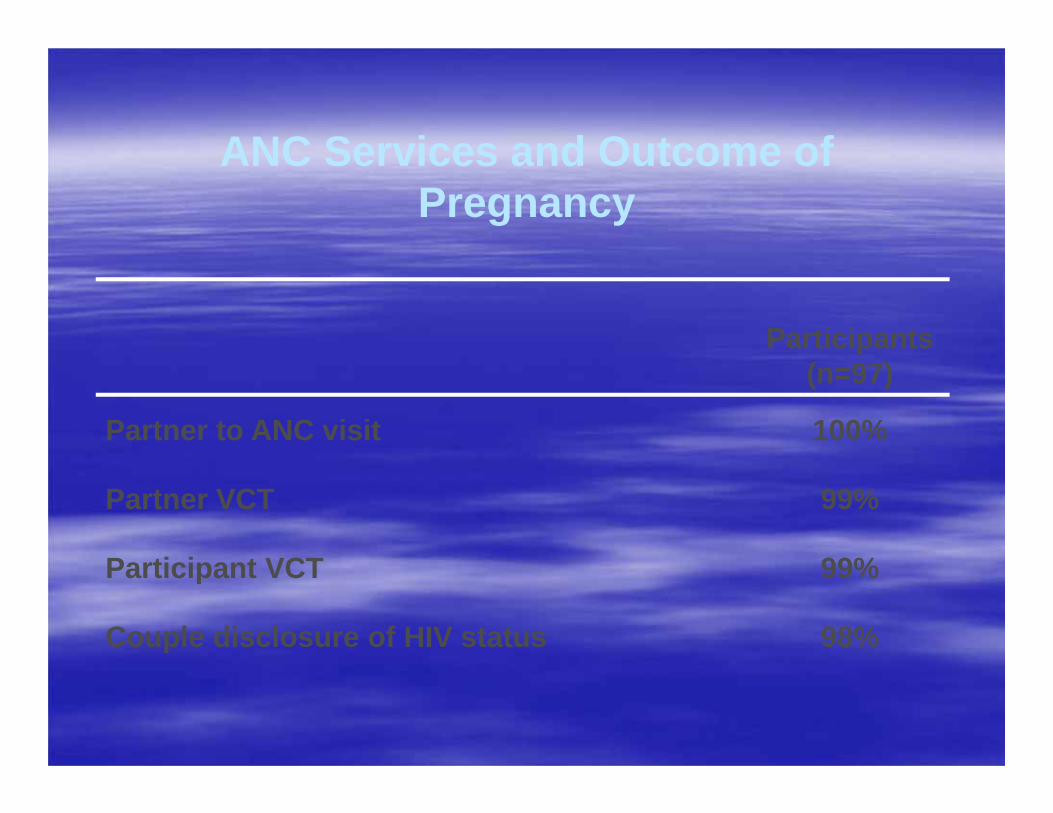
ANC Services and Outcome of Pregnancy
Participants (n=97)
Partner to ANC visit 100%
Partner VCT 99%
Participant VCT 99%
Couple disclosure of HIV status 98%
CHALLENGES
Work overload on part of nurses Misuse of the kits (buckets and soap) Movement of mothers/families from one
village or district to the other The type of taps of the buckets were
imported (not be made locally), made it difficult to replace broken ones. Shrinking resources to allow for scaling up
of the interventions

Government Efforts, Enabling nvironment & Status of HWTS PoliciesGoM through the MOH facilitated the dissemination of the pilot results to a wide range of stakeholdersGoM sees the use the antenatal care system as a viable platform for the ntegration & promotion of HWTS and education messages for diarrhoeal disease reduction– Therefore, pilot facilities in the three districts
Government Efforts, Enabling Environment & Status of HWTS
Policies (cont…)Availability of Health Surveillance Assistance (HSAs) allow for proper follow up of interventions at household levelStrengthened partnerships with other stakeholders to expand the interventionsSocial marketing by the private sector and partners
overnment Efforts, Enabling Environment & Status of HWTS Policies (cont…)
Existing policies provides for the treatment of water at household level during emergencies.However, there is need to elaborate clear policies on HWTS and the environment under which the intervention will be mplemented
Conclusion
Evidence from the pilot in Malawi has shown that promotion of HWTS & other hygiene practices can be integrated into existing service delivery systems such as ANC.Based on the perceived and real benefits, the hygiene behaviours can also diffuse into the communities.There is need to elaborate policy on ntegration HWTS & consider scaling up