Embed Size (px)
Citation preview

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 1 of 62
STATISTICAL ANALYSIS PLAN
Study: EP0069Product: UCB0942
A double-blind, randomized, placebo-controlled study of the efficacy, safety/tolerability, and pharmacokinetic profile of UCB0942 in adult patients with highly drug-resistant focal epilepsy.
SAP/Amendment Number DateFinal SAP 03 Jul 2015Amendment 1 07 Oct 2016
Confidentiality Statement
ConfidentialThis document is the property of UCB and may not – in full or in part – be passed on, reproduced,
published, or otherwise used without the express permission of UCB.
20152015t 2t 2
COPY ts ws
This do
cumen
tThisThis
u
cann
ot nn
be us
ed to
supp
ort an
y mark
eting
01616
autho
rizati
on ap
plica
tion
e effica effich highlhigh
and a
ny ex
tensio
ns or
varia
tions
there
of.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 2 of 62
TABLE OF CONTENTSLIST OF ABBREVIATIONS.................................................................................................... 51 INTRODUCTION ............................................................................................................. 82 PROTOCOL SUMMARY................................................................................................. 82.1 Study objectives ................................................................................................................. 8
2.1.1 Primary objective................................................................................................... 82.1.2 Secondary objectives ............................................................................................. 82.1.3 Exploratory objectives ........................................................................................... 8
2.2 Study variables................................................................................................................... 92.2.1 Efficacy variables .................................................................................................. 9
2.2.1.1 Primary efficacy variable ............................................................................ 92.2.1.2 Secondary efficacy variables....................................................................... 92.2.1.3 Exploratory efficacy variables.................................................................... 9
2.2.2 Pharmacokinetic variables ................................................................................... 102.2.3 Other exploratory variables ................................................................................. 102.2.4 Safety variables.................................................................................................... 11
2.3 Study design and conduct ................................................................................................ 122.4 Determination of sample size........................................................................................... 133 DATA ANALYSIS CONSIDERATIONS ...................................................................... 133.1 General presentation of summaries and analyses ............................................................ 133.2 General study level definitions ........................................................................................ 15
3.2.1 Analysis timepoints ............................................................................................. 153.2.1.1 Relative day............................................................................................... 153.2.1.2 Study periods ............................................................................................. 15
3.3 Definition of Baseline values........................................................................................... 163.4 Protocol deviations........................................................................................................... 173.5 Analysis sets..................................................................................................................... 17
3.5.1 Enrolled Set ......................................................................................................... 173.5.2 Randomized Set ................................................................................................... 173.5.3 Safety Set ............................................................................................................. 173.5.4 Full Analysis Set.................................................................................................. 173.5.5 Per Protocol Set ................................................................................................... 173.5.6 Other analysis sets ............................................................................................... 17
3.6 Treatment assignment and treatment groups ................................................................... 183.7 Center pooling strategy .................................................................................................... 183.8 Coding dictionaries .......................................................................................................... 183.9 Changes to protocol-defined analyses.............................................................................. 193.10 Definition of study-specific derived variables ................................................................. 19
REDACTED ........ONSONS
s and as and a............
COPY ...............
This do
cumen
t3.53.33
cann
ot 4.5.5.55
beSaSaus
ed ollele
Randoandoto .
ed Sed Ssu
pport
vava...............
.......
any dsds .....
alueslue
marketi
ng .........
......................
autho
rizati
on ....
...................
analyanaly
appli
catio
n ...................
.................
and .......... an
y ...........ex
tensio
ns
.........................
..........
or......... varia
tions
... 8.. 8
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 3 of 62
3.10.1 Seizure frequency related variables ..................................................................... 193.10.2 Seizure freedom ................................................................................................... 203.10.3 Seizure-free days ................................................................................................. 203.10.4 Patient Weighted Quality of Life in Epilepsy Inventory ..................................... 203.10.5 Medications.......................................................................................................... 21
4 STATISTICAL/ANALYTICAL ISSUES ....................................................................... 224.1 Adjustments for covariates............................................................................................... 224.2 Handling of dropouts or missing data .............................................................................. 224.3 Interim analyses and data monitoring .............................................................................. 23
4.3.1 Safety Review Group........................................................................................... 234.3.2 Blinded Interim Analysis ..................................................................................... 23
4.4 Multicenter studies........................................................................................................... 244.5 Multiple comparisons/multiplicity................................................................................... 244.6 Use of an efficacy subset of subjects ............................................................................... 244.7 Active-control studies intended to show equivalence...................................................... 244.8 Examination of subgroups ............................................................................................... 244.9 End of Study Analyses..................................................................................................... 255 STUDY POPULATION CHARACTERISTICS............................................................. 255.1 Subject disposition ........................................................................................................... 255.2 Protocol deviations........................................................................................................... 266 DEMOGRAPHICS AND OTHER BASELINE CHARACTERISTICS ........................ 266.1 Demographics .................................................................................................................. 266.2 Medical history and concomitant diseases....................................................................... 26
6.2.1 History of epilepsy............................................................................................... 266.3 Prior and concomitant medications.................................................................................. 27
6.3.1 Non- Antiepileptic drugs ..................................................................................... 286.3.2 Antiepileptic drugs............................................................................................... 28
7 MEASUREMENTS OF TREATMENT COMPLIANCE............................................... 298 EFFICACY ANALYSES ................................................................................................ 308.1 Statistical analysis of the primary efficacy variable ........................................................ 308.2 Statistical analysis of the secondary efficacy variables ................................................... 308.3 Analysis of exploratory efficacy variables ...................................................................... 319 PHARMACOKINETICS................................................................................................. 339.1 Non compartmental PK analysis...................................................................................... 339.2 Population pharmacokinetics ........................................................................................... 349.3 Pharmacokinetic/pharmacodynamic analysis .................................................................. 3410 SAFETY ANALYSES..................................................................................................... 3410.1 Extent of exposure ........................................................................................................... 34
REDACTED T............
...........ER BAER BA
COPY .........
TICSICS
This do
cumen
t 99.19.1
cann
otatistitistiAnalAnaPP
beticaltical us
ed MM
CY ANY ANa
toENTENsu
pport
mpilepticilepti
eptic drptic drT
any .....
edicaedicamark
eting
A............
ant disent dis........
autho
rizati
on ............
.....................
SELSEL
appli
catio
n .
........................
...........
and .......
......an
y ............
exten
sions...........
..............................
or ...... va
riatio
ns
2222222
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 4 of 62
10.2 Adverse events ................................................................................................................. 3410.3 Clinical laboratory evaluations ........................................................................................ 3610.4 Vital signs, physical findings, and other observations related to safety .......................... 37
10.4.1 Vital signs ............................................................................................................ 3710.4.2 Electrocardiograms .............................................................................................. 3810.4.3 Doppler echocardiography................................................................................... 3810.4.4 Physical examination ........................................................................................... 3810.4.5 Columbia-Suicide Severity Rating Scale............................................................. 3810.4.6 Neurological examination.................................................................................... 3810.4.7 Psychiatric and cognition assessment and withdrawal monitoring ..................... 3810.4.8 Other safety variables .......................................................................................... 39
11 OTHER ANALYSES ...................................................................................................... 3912 REFERENCES ................................................................................................................ 4013 APPENDICES ................................................................................................................. 4213.1 Treatment groups in TFL outputs .................................................................................... 4213.2 PCST criteria.................................................................................................................... 43
13.2.1 Hematology.......................................................................................................... 4313.2.2 Blood chemistry................................................................................................... 4413.2.3 Urinalysis ............................................................................................................. 4513.2.4 Vital signs and body weight ................................................................................ 46
13.3 QOLIE-31-P total and subscale score calculations.......................................................... 4813.4 SSQ Scoring Algorithm ................................................................................................... 5113.5 SAP Amendment 1 .......................................................................................................... 53STATISTICAL ANALYSIS PLAN SIGNATURE PAGE..................................................... 62
REDACTED ............
..........score score
COPY .........
........
This do
cumen
t can
not b
e use
d to s
uppo
rt any
AA marketi
ng c
.........................
AN SIN S
autho
rizati
on ............
.....................
alcualcu
appli
catio
n .
........................
...........
and .......
......an
y ............
exten
sions...........
..............................
or ...... va
riatio
ns
388383
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 5 of 62
LIST OF ABBREVIATIONS50%RR 50% responder rate
75%RR 75% responder rate
ADaM analysis dataset model
AE adverse event
AED antiepileptic drug
ALP alkaline phosphatase
ALT alanine aminotransferase
ANCOVA analysis of covariance
AST aspartate aminotransferase
AUC area under the concentration-time curve
AUCτ area under the plasma concentration-time curve over a dosing interval
BMI body mass index
BPRS Brief Psychiatric Rating Scale
BRV brivaracetam
BUN blood urea nitrogen
CF correction factor
CI confidence interval
CIWA-B Clinical Institute Withdrawal Assessment-Benzodiazepines
Cmax maximum observed plasma drug concentration
CRF case report form
CRO contract research organization
C-SSRS Columbia Suicide Severity Rating Scale
CSR clinical study report
Ctrough measured concentration at the end of a dosing interval at study state
CV coefficient of variation
DAP data analysis plan
DBP Diastolic blood pressure
DNA Deoxyribonucleic acid
ECG electrocardiogram
ES enrolled set
EudraCT European Union Drug Regulating Authorities Clinical Trials
REDACTED
ntervanterva
COPY lele
This do
cumen
tDBPBP
DD
cann
ot P
be us
ed to
supp
ort
ontractntra
ColCo
any eport fport mark
eting
al
ute Wiute W
obsobser
autho
rizati
on ap
plica
tion e ove ovan
d overver
any e
xtens
ions o
r vari
ation
s the
reof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 6 of 62
FAS Full Analysis Set
FDA Food and Drug Administration
HBsAg hepatitis B surface antigen
HCV-Ab hepatitis C antibody
HIV-1/2Ab human immunodeficiency virus-1/2 antibody
ICF Informed Consent Form
ICH International Conference on Harmonization
ILAE International League Against Epilepsy
IMP investigational medicinal product
LDH lactate dehydrogenase
LEV levetiracetam
MedDRA Medical Dictionary for Regulatory Activities
MCH mean corpuscular hemoglobin
MCHC mean corpuscular hemoglobin concentration
MCV mean corpuscular volume
MINI Mini International Neuropsychiatric Interview
MMSE mini-mental state examination
mRNA messenger RNA
n number of observations
NCA non-compartmental analysis
OLE Open Label Extension study
PCST potentially clinical significant treatment-emergent
PK pharmacokinetic(s)
PK-PPS Pharmacokinetic Per Protocol Set
PPS Per Protocol Set
PR pulse rate
PT preferred term
QOLIE-31-P Quality of Life Inventory in Epilepsy-31-P
QTcB QT interval corrected for heart rate using Bazett’s formula
QTcF QT interval corrected for heart rate using Fridericia’s formula
RBC red blood cells
RS Randomized Set
REDACTEDeuropeurop
examexa
RNARNA
COPYn con co
e
This do
cumen
tQOLOL
cann
ot
LILI
be us
ed to
supp
ort
otentiatenti
pharpha
any LabelLabemark
eting
ervatioervat
artmenartme
autho
rizati
on
sysychiachi
minatiminat
appli
catio
n ess
centratcentra
and a
ny ex
tensio
ns or
varia
tions
there
of.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 7 of 62
SAE serious adverse event
SAP Statistical analysis plan
SBP systolic blood pressure
SD standard deviation
SFU Safety Follow-up
SI Standard International
SOC system organ class
SRG Safety Review Group
SS Safety Set
SSQ seizure severity questionnaire
t1/2 apparent terminal elimination half-life, reported in hours
TFL table listing figure
tmax time of occurrence of maximum observed plasma drug concentration
ULN upper limit of normal
VNS vagal nerve stimulation
WBC white blood cell
WHODD World Health Organization Drug Dictionary
REDACTED
rganizganiz
COPY
This do
cumen
t can
not b
e use
d to s
uppo
rt any
mark
eting
autho
rizati
on
zation ation
appli
catio
n ved plaed pl
and d ininan
y n hon h
exten
sions
or va
riatio
ns th
ereof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 8 of 62
1 INTRODUCTIONThe purpose of this statistical analysis plan (SAP) is to provide all information that is necessary to perform the required statistical analysis of data collected in EP0069. It also defines the summary tables, listings, and figures (TFLs) to be included in the final Clinical Study Report (CSR) according to the protocol.
This SAP is based upon, and assumes familiarity, with the following study documents:
Protocol Amendment 4: 05 October 2016
Unless specified below, the study will be analyzed as described in the most recent version of the protocol (EudraCT-Number: 2014-003330-12).
If a future protocol amendment necessitates a substantial change to the statistical analysis of the study data, this SAP will be amended accordingly. If, after database lock, additional analyses are required to supplement the planned analyses described in this SAP, those unplanned analyses will not be described in the amended SAP but they will be described in a separate analysis plan.However, if analysis definitions have to be modified or updated, a SAP amendment will be required. The content of this SAP is compatible with the International Conference on Harmonization (ICH)/ Food and Drug Administration (FDA) E9 Guidance documents (ICH E9, 1998).
UCB is the Sponsor and PRA is the Contract Research Organization (CRO) for this study.
2 PROTOCOL SUMMARY2.1 Study objectives2.1.1 Primary objectiveThe primary objective is to evaluate the efficacy of UCB0942 administered concomitantly with each subject’s current, stable antiepileptic drug (AED) regimen in subjects who have 4 or more focal seizures with or without secondary generalization per week and who have failed to achieve seizure control with ≥4 AED regimens of adequate dose and duration.
2.1.2 Secondary objectivesThe secondary objectives are to:
! Evaluate the safety and tolerability of UCB0942.
! Evaluate the pharmacokinetics (PK) of UCB0942 and its metabolites.
2.1.3 Exploratory objectivesThe exploratory objectives are to:
! Identify genetic polymorphisms, gene expression patterns, plasma proteins, plasma lipids or other plasma substances that predict or are associated with disease etiology, drugresponse, or tolerability.
! Use video recordings to explore the effect of UCB0942 on seizure type, seizure severity, seizure duration and duration of the postictal period.
! Evaluate the efficacy of UCB0942 using exploratory efficacy variables.
REDACTED RYY COPY earch earch
This do
cumen
t !ca
nnot
e exploexplo
be uaua us
edthe he
ate tate t
to cti
sasu
pport
aryry ooyy b
ives aves a
any coco
regimegimmark
eting
he effihe eff
pilepticpileptondaond
autho
rizati
onOrgOr ap
plica
tion ionalona
E9 GuE9 Gu
rganrgan
and n a a
AP amAP amll
anyunplunp
sepasepex
tensio
ns i
al anal anaditionditionlal
oron on ova
riatio
ns th
ereof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 9 of 62
2.2 Study variables2.2.1 Efficacy variablesThe periods for which the efficacy variables are calculated are described in Section 3.2.1.2.
2.2.1.1 Primary efficacy variableSeizure frequency will be determined using subject diary cards. The subject will be instructed as to how to complete the diary and the procedure for completing the diary will be identical during the Inpatient and Outpatient Maintenance Periods.
The primary outcome measure is the 75% responder rate (75%RR). In the active group this is defined as the proportion of subjects with a 75% or greater reduction in the focal seizure (IA1, IB, IC) frequency during the last 2 weeks of the Inpatient Period compared to the 2-week Prospective Outpatient Baseline. In the placebo group the 75%RR is defined as the proportion of subjects with a 75% or greater reduction in the focal seizure frequency during the first 2 weeks of the Inpatient Period (the 2 weeks on placebo) compared to the Prospective Outpatient BaselinePeriod.
2.2.1.2 Secondary efficacy variablesThe 2-week Inpatient Period to be considered is the last 2 weeks of the Inpatient Period for the active group, and the first 2 weeks of the Inpatient Period for the placebo group (see Section 3.2.1.2).
The secondary efficacy variables are:
! Median percent reduction in focal seizure frequency from the Baseline Period to the 2-week Inpatient Period, the Outpatient Maintenance Period and On-UCB0942 Overall.
! Seizure-free rate during the 2-week Inpatient Period, the last 4 weeks of the Outpatient Maintenance Period, and the On-UCB0942 Overall Period (Section 3.10.2 ).
! The 75%RR during the last 4 weeks of the Outpatient Maintenance Period, and On-UCB0942 Overall.
! Percentage of seizure-free days during the 2-week Inpatient Period and OutpatientMaintenance Period (Section 3.10.2).
2.2.1.3 Exploratory efficacy variablesFor all the exploratory efficacy variables, the Inpatient Period to be considered for the active group is the last 2 weeks and for the placebo group is the first 2 weeks of the Inpatient Period.
Exploratory efficacy variables are as follows:
! Median seizure frequency by focal seizure type (IA1, IB, IC) per study period: Baseline, 1st
Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week, the 2-week Inpatient Period,Outpatient Maintenance Period, and On-UCB0942 Overall.
! The 50% responder rate (50%RR) during the 2-week Inpatient Period and during the Outpatient Maintenance Period.
! Seizure Severity Questionnaire score (SSQ, Cramer et al, 2002) change from Baseline to the end of the Inpatient Period and the end of the Outpatient Maintenance Period.
REDACTED
eizure eizureMainteMainte
kk
COPYstst
PeriodPerio
This do
cumen
tMcann
ot oratoryratory
MeMe
bexp
e lase lasus
edxplpl
ploraplora
to plorlorsu
pport
re--free free
odod ((SeS
any4 w4 wmark
eting
en
k InpatInpatn-UCBUCB
weewe
autho
rizati
on
frequfrequnanceance
appli
catio
n
weekseeks od for thfor t
and
pecec anying ing
ctive tive ex
tensio
nsup thp th
eizureeizuree 22--ww
as theas theg thg th
or hishisva
riatio
ns
s s ring ng
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 10 of 62
! Changes in average seizure severity as calculated by the percentage of all seizures that are type IC for the 2-week Inpatient and Outpatient Maintenance Periods.
! Change from Baseline in Quality of Life Inventory in Epilepsy-31-P (QOLIE-31-P, Cramer et al, 2003) subscales and total score for the Outpatient Visits 10, 12, 15, 17.
2.2.2 Pharmacokinetic variablesPlasma concentrations of UCB0942, will be used to derive PK-population parameters.
The following PK variables will be calculated:
! AUCτ: area under the plasma concentration-time curve over a dosing interval.
! Cmax: maximum observed plasma drug concentration.
! tmax: time of occurrence of Cmax.
! t½: apparent terminal elimination half-life, reported in hours.
! Ctrough: measured concentration at the end of a dosing interval at study state.
2.2.3 Other exploratory variablesBlood samples for DNA, mRNA, and lipidomics/proteomics/additional blood biomarkers will be collected during the study:
! DNA: One tube for DNA isolation will be collected at the beginning of the Inpatient Period of the study. The DNA may be used to assess known variants associated with drug-resistant epilepsy or AED resistance and may be used for further genetic analyses relating to epilepsy and drug response.
! mRNA: One tube will be collected on the day before the first dose of UCB0942/placebo, and 1 tube will be collected on the last day of the Inpatient Maintenance Dose Week. The mRNA samples may be used to identify gene expression patterns that are associated with disease etiology, that predict (Baseline sample), or that are associated with (post-treatment sample) drug response.
! Lipidomics/proteomics/additional blood biomarkers: One tube will be collected on the day before the first dose of UCB0942 or placebo, and 1 tube will be collected on the last day of the Inpatient Maintenance Dose Week. These samples may be used for additional blood biomarker analysis.
All subjects will be asked to provide specific consent for these samples. Refusal to provide consent for the collection of samples for DNA, mRNA, and lipidomics/proteomics will not disqualify the subject from participating in the study.
Single archive blood samples (for potential background AED assay) will be collected at the start of titration, the end of the Inpatient Period, and at the end of the Outpatient Maintenance Period (before last dose of investigational medicinal product [IMP]). These samples will be collected just before the morning dose of IMP and stored for up to 1 year after the study ends.
During the Inpatient Period, there will be video monitoring of subjects in their rooms (and in other areas depending on the infrastructure of each site) to allow detection of nocturnal seizures
REDACTED be collbe col
o asseassayay be u be yy
COPYroteomoteo
This do
cumen
t isqsq
SinSinca
nnotjectscts
ent foent foqualual
be er r
wus
ed e ff
tient Mient Mr anaana
tofirstfirstsu
pport
aseas
eomicomicd
anyntifyntif
elineelinmark
eting
ed on ted on
last dalast fyfy gy
autho
rizati
on
lectedectedss knss kn
used fused
appli
catio
nl at stat s
mics/adics/a
and
stut
any e
xtens
ions o
r vari
ation
s o
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 11 of 62
and seizures not recorded by the subject and to assess seizure type, severity, duration and the duration of the postictal period. The video data will not be used to corroborate or supplement the diary data and shall not influence the diary seizure capture by the subject.
2.2.4 Safety variablesThe safety of participating subjects will be closely monitored. Psychiatric assessment will be performed by a staff member trained in the identification of psychiatric symptoms, and the assessments will be performed using the Brief Psychiatric Rating Scale (BPRS; Overall and Gorham, 1962), which assesses various psychiatric domains including:
! Changes in mood and symptoms of depression or mania.
! Changes in thinking and perception, and other symptoms of psychosis.
! Changes in behavior.
Other safety variables are:
! Adverse events (AEs) reported by the subject and/or caregiver or observed by the Investigator or inpatient staff.
! Serious AE (SAEs).
! Subject withdrawals or premature UCB0942 tapering due to AEs.
! Changes in clinical laboratory test parameters.
! Changes in vital sign parameters – pulse rate (PR), systolic blood pressure (SBP), diastolic blood pressure (DBP), and respiratory rate.
! Changes in 12-lead electrocardiogram (ECG) parameters.
! Changes in key cardiac structures on 2-dimensional Doppler echocardiography from Baseline to after treatment (end of dosing and 6 months after last dose).
! Changes in physical examination (including body weight) and neurological examination findings.
! Changes in memory or cognition as assessed with the mini-mental state examination (MMSE; Folstein et al, 1975).
! Changes indicative of a hypersensitivity reaction including an AE or laboratory value (as defined below) suggestive of internal organ involvement (including but not limited to hepatitis, nephritis, pneumonitis, carditis, colitis, encephalitis, pancreatitis, myositis, arthritis, or hematologic system involvement) combined with at least 1 of the following: fever, rash, lymphadenopathy, or eosinophilia.
∀ Treatment-emergent abnormal laboratory value criteria suggestive of internal organ involvement or eosinophilia:
◦ Eosinophils % ≥10%
◦ Eosinophils absolute ≥0.5G/L
◦ Neutrophils absolute <1.5G/L
REDACTED ersers
se ratese rateoryory ratratyy
ogramogram
COPYperingperin
ss
This do
cumen
t can
not titisti
hemahemlylympmpyyy
be belbel
is, nis, nus
ed
ndicatidicatielowlow
toein ein esupp
ort
ry or cy or cet aet
any inatioinatiomark
etingm (ECm (EC
s on on 22ng andng an
autho
rizati
on g
e (PR)(PR)e..
CC
appli
catio
n
due todue
and r obseobse
any e
xtens
ions o
r vari
ation
s the
reof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 12 of 62
◦ Platelets ≤100G/L
◦ Alanine aminotransferase (ALT) ≥2x upper limit of normal (ULN)
◦ Aspartate aminotransferase (AST) ≥2x ULN
! Any indication of withdrawal symptoms using the Clinical Institute Withdrawal Assessment-Benzodiazepines (CIWA-B; Busto et al, 1989).
! Changes in suicidality using the Columbia-Suicide Severity Rating Scale (C-SSRS).
2.3 Study design and conductEP0069 is a Phase 2A, double-blind, randomized, placebo-controlled, multicenter study that will test the potential efficacy, safety/tolerability, and PK profile of UCB0942 in adult subjects with highly drug-resistant focal epilepsy.
At least 46 subjects will be randomized 1:1 to receive UCB0942 400mg bid or placebo as add-on to each subject’s concomitant AED regimen. Stratified randomization will be used to ensure balance in the 2 treatment arms on the levetiracetam (LEV)-use factor (3 strata):
1. LEV prior and current use (concomitant use of LEV at study entry).
2. LEV Prior Use Only=History of prior LEV use and must have discontinued 4 weeks prior to study entry.
3. LEV Naïve=No history of prior LEV use, and no use at study entry.
All subjects will stay in the clinical unit for a total of 3 weeks and will then be discharged for an 8-week Outpatient Period. Titration to UCB0942 400mg bid will occur over the course of 1 week in the clinical unit. Subjects in the active arm will be titrated to UCB0942 400mg bid, during the first inpatient week. Subjects who initially received placebo will be titrated to UCB0942 400mg bid during the last week of the 3-week Inpatient Period. For subjects in the active arm who do not tolerate UCB0942 400mg bid, during the third week of the Inpatient Period the dose can be tapered to UCB0942 200mg bid before starting the 8-week Outpatient Period. Similarly, for subjects in the placebo group the dose can be tapered to a tolerable dose during the Outpatient Period.
For a general presentation of the study design refer to Figure 2‒1.
The total duration of the study after Screening is 20 weeks for each subject, including the Prospective Outpatient Baseline Period (2 to 3 weeks), the Inpatient Period (3 weeks), the Outpatient Period (8 weeks of treatment and 2 weeks of taper), and a Safety Follow-Up (SFU)Period (4 weeks). The total duration of exposure to UCB0942 during this study is 13 weeks.
Subjects who drop out prior to their Visit 6 may be replaced.
REDACTED nd
r a totar a totaUCB09CB0
tive arive arnitialnitial
COPY d d
d nod no
This do
cumen
t can
not4 wew
jects wects
bePeriPer
weeweeus
edn ofof
Outpatiutpatiioio
to of thof thsu
pport
p tp
ation otion
anyd bed be
the dthe dmark
etingrm
allylly recrecyyek Inpak Inp
, duringdurineforefo
autho
rizati
on
o use ause a
al of 3al of 3942 4042 4
m wim wi
appli
catio
n y entryentryy
st have t have
and
wiwor (3 sr (3
any dd oro
ll be ll be ex
tensio
nstududy ty t subjsubj
or por p
or va
riatio
ns th
ereof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 13 of 62
Figure 2‒1: Study design
Maint. = maintenance; OLE = open-label extension; Sbjs=subjects; Titrat. = titration.
An echocardiogram is planed to be performed 6 months after the last dose. If not all echocardiographs are completed by the time of the initial database locks, the database will be unlocked so that the echocardiography data will be included and cleaned. These data will be reported in an addendum.
2.4 Determination of sample sizeThis is an exploratory pilot study to obtain a first evaluation of the efficacy (estimate and variability) of UCB0942 in this specific refractory population. The planned sample size was evaluated based on placebo results obtained in similar refractory epileptic populations from brivaracetam (BRV) and lacosamide Phase 3 studies in add-on focal epilepsy and the desired effect was based on a doubling of the effect of lacosamide and BRV in patients in the current target population.
For the primary efficacy variable, the 75%RR in the placebo group from these historical studies was estimated to be less than 5%. The response on UCB0942 was expected to be 36.5% in order to provide clear differentiation from lacosamide and BRV in this patient population. Based on a two-group Fisher's exact one-sided test with a ratio active:placebo of 1:1, the required number of subjects is 23 in each arm to detect a significant difference between the two groups with a power of 80% and a false positive rate of 5%.
3 DATA ANALYSIS CONSIDERATIONS3.1 General presentation of summaries and analysesStatistical evaluation will be performed by UCB or designee and supervised by the ExploratoryStatistics Department of UCB unless otherwise indicated. Data may be summarized by study period and by timepoint, if applicable.
The analysis datasets will follow the UCB analysis dataset model (ADaM) data specifications.
REDACTEDf thef th will bwill b
ssamam
COPY cts; cts
monthmonthhehe ii
This do
cumen
t 3333
cann
otpp
ts is 2s is 20% an0% a
bee
FishFishus
edo be be ar diar di
toficacicacl
supp
ortubling ling
cy
anylts lts
samidsamidmark
eting
mpleplobtain abtain
ecific rcifics obts ob
autho
rizati
onhs afaf
nitialnitialbe ince inc
plele
appli
catrat. = tirat. =
fterfter
icatio
n aaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaannnnnnnnnnnnnnnddddddd
aaannnyyy e
xttttttttttttttttttttttttttttttttttteeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeennnnnnns
ionnnnnnnnnnnnnssssssssss o
r
ions
vaarrrrriiiiiiaaa
tiothe
reof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 14 of 62
All analysis will be performed using SAS® version 9.3, or higher (SAS Institute, Cary, NC, USA). The PK variables will be computed by non-compartmental analysis (NCA) with Phoenix WinNonlin® (version 6.2, or higher) using the actual sampling times.
A glossary of common abbreviations will be provided and will contain abbreviations not footnoted in the tables, figures, and listings.
For continuous variables, summary statistics will include number of observations (n), mean, median, quartiles, standard deviation (SD), minimum, and maximum, and may also include 95% confidence intervals (CI). Categorical endpoints will be summarized using number of subjects, frequency, and percentages. Coefficient of variation (CV), geometric mean, and 95% CI will also be presented in the descriptive statistics for PK parameters. Missing data will not be imputedapart from the exceptions as outlined in Section 4.2.
When reporting relative frequencies or other percentage values, the following rules apply:
! For values where all subjects fulfill certain criteria, the percentage value will be displayed as 100.
! For values where the absolute frequency is 0, there will be no percentage presented at all.
! All other percentage displays will use 1 decimal place.
When reporting descriptive statistics, the following rules will apply in general:
! n will be an integer.
! Mean, SD, and median will use 1 decimal place more than the original data.
! The CV will be reported as a percentage to 1 decimal place.
! Minimum and maximum will be reported using the same number of decimal places as the original value.
! If no subjects have data at a given timepoint, for example, then only n=0 will be presented. However, if n<3, present the n, minimum and maximum only. If n=3, n, mean, median, minimum and maximum will be presented only. The other descriptive statistics will be left blank.
Details of statistical summaries for safety are described in Section 9.
General statistical and reporting conventions are outlined in UCB Global Statistical Conventions; Version 1.0 dated 26 June 2013.
For PK calculations the User guide for Clinical Pharmacokinetics Modeling and Simulation; Version 8.0, dated 4 July 2012 of UCB will be considered as guideline.
REDACTED mal plmal pl
entageentage
reprep
COPYg rulesg rules
This do
cumen
t can
nocalcalc
ion 8.on 8.be
da
culcuus
edical ancal anatedated
to l susu supp
ortum wim w
ummum
any givgi
he n, he n,willi
marketi
ng
ported orted
iven ven
autho
rizati
on
lace mace m
to 1 to 1
appli
catio
no perco per
will awill
and a
ny
lue wlue wex
tensio
nsC
e impuimp
g ruleg rule
orwiwiva
riatio
ns
95% 5% ects, ects,
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 15 of 62
3.2 General study level definitions3.2.1 Analysis timepoints 3.2.1.1 Relative dayThe relative day of an event will be derived with the start date of first IMP administration as reference date, up to and including the last day of the IMP administration:
! Active group: Date of the first/last UCB0942 administration (including the tapering period, where applicable)
! Placebo group: Date of the first Placebo administration /last Placebo administration (before the first UCB0942 administration).
Relative days for an event or measurement occurring before the reference date are calculated as follows:
Relative Day=(Event Date-Reference Date)
Relative days for an event or measurement occurring on or after the reference date to the last day of IMP administration are calculated as follows:
Relative Day=(Event Date-Reference Date)+1
For events or measurements occurring after the date of last dosing (as defined above), the relative day will be calculated with the date of last IMP administration as reference. Relative day in this case will be prefixed with ‘+’ in the data listings and will be calculated as follows:
Relative Day=+(Event Date-Reference Date)
Therefore, for the active group, every relative day post the tapering period will be presented with a prefix, and for the placebo group, every day since the first UCB0942 dose (2nd Inpatient Week) be presented with a prefix.
There is no relative Day 0. Relative day is not calculated for partial dates in cases where relative day is shown in a subject data listing. In such cases, relative day should be presented as ‘--’ in the subject data listings.
3.2.1.2 Study periodsThe following periods, and their combinations will be considered in the definition of efficacy and safety variables:
! Baseline Period: Prospective Outpatient Baseline Period consisting of 2 to 3 weeks of prospective post-screening subject diary seizure counts.
! Inpatient Period: The Double-Blind Inpatient Treatment Period, with the following sub-periods.
∀ 1st Inpatient Week: Double-Blind Titration Week (active group on UCB0942 titration; placebo group on placebo)
∀ 2nd Inpatient Week: Double-Blind Maintenance-Dose Week (active group on UCB0942 maintenance; placebo group on placebo)
REDACTEDa
ata lisata li
++(Eve(Ev
ryry relarelayyvev
COPY te of lte of l
st Ist IMM
This do
cumen
tppcann
otspectpect
InpatInpat
bene Pene Peii
used
rioioiablesables
toodsodssu
pport
y perioperio
anytivetiv
listinlistinmark
eting
ativeiveeryry daydayyy
ve dave d
autho
rizati
onlas
MP adMP adstings tings
vent Dent D
ve de d
appli
catio
n e r
nce Dance D
st dost do
and
referrefean
y exte
nsion
sonn (b(
e are care c
or (be(beva
riatio
ns
odod, ,
thereo
f.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 16 of 62
∀ 3nd Inpatient Week: Transition to Outpatient Week (active group on UCB0942 maintenance; placebo group on UCB0942 titration).
∀ 2-week Inpatient Period: For the active treatment group this is the last 2 weeks of the Inpatient Treatment Period and for the placebo treatment group this is the first 2 weeks of the Inpatient Treatment Period.
! Outpatient Maintenance Period: 8 week Outpatient open-label (active group on UCB0942 maintenance; placebo group on UCB0942 maintenance).
! Last 4 weeks of Outpatient Maintenance Period.
! On-UCB0942 Overall: This is the whole period while the subjects have been taking UCB0942 (from the 1st Week of the Inpatient period for the active group and from the 3rd
week of the Inpatient period for the Placebo group, until the end of Outpatient period or Tapering).
! Tapering Period.
! SFU Period.
! Overall: Whole study duration (start of 1st inpatient week through end of SFU).
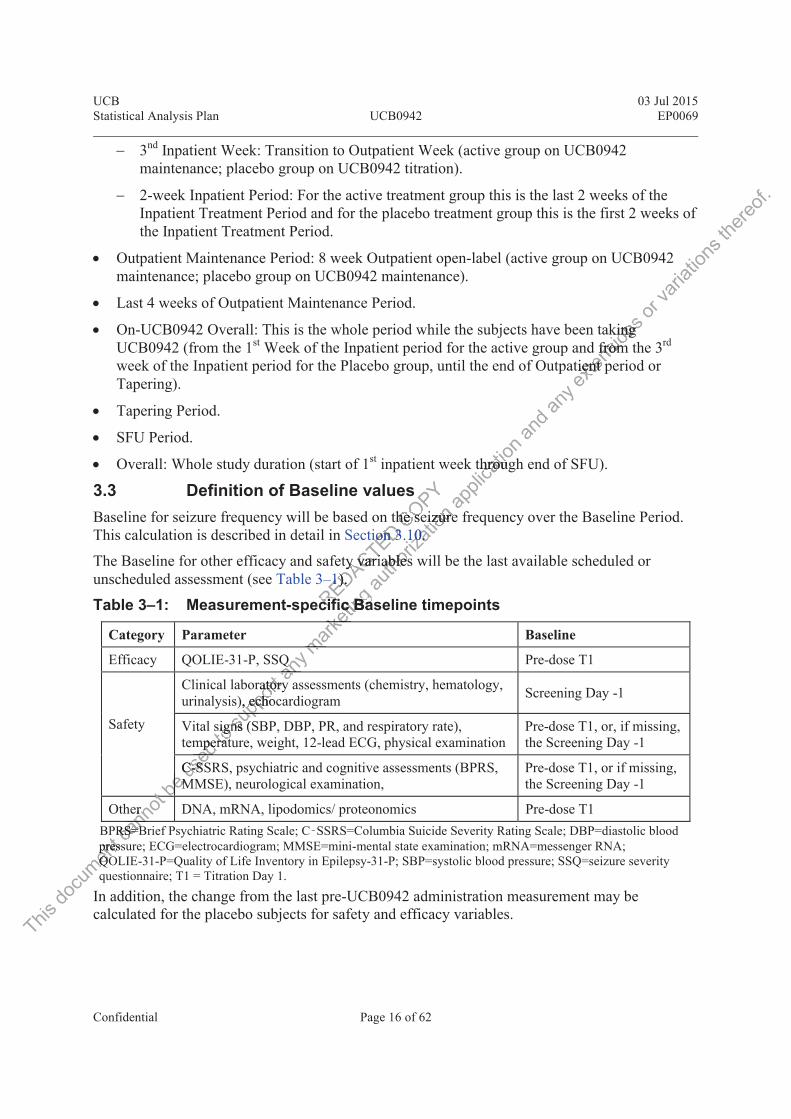
3.3 Definition of Baseline valuesBaseline for seizure frequency will be based on the seizure frequency over the Baseline Period. This calculation is described in detail in Section 3.10.
The Baseline for other efficacy and safety variables will be the last available scheduled or unscheduled assessment (see Table 3‒1).
Table 3‒1: Measurement-specific Baseline timepoints
Category Parameter Baseline
Efficacy QOLIE-31-P, SSQ Pre-dose T1
Safety
Clinical laboratory assessments (chemistry, hematology, urinalysis), echocardiogram Screening Day -1
Vital signs (SBP, DBP, PR, and respiratory rate), temperature, weight, 12-lead ECG, physical examination
Pre-dose T1, or, if missing, the Screening Day -1
C-SSRS, psychiatric and cognitive assessments (BPRS, MMSE), neurological examination,
Pre-dose T1, or if missing, the Screening Day -1
Other DNA, mRNA, lipodomics/ proteonomics Pre-dose T1BPRS=Brief Psychiatric Rating Scale; C‑SSRS=Columbia Suicide Severity Rating Scale; DBP=diastolic blood pressure; ECG=electrocardiogram; MMSE=mini-mental state examination; mRNA=messenger RNA; QOLIE-31-P=Quality of Life Inventory in Epilepsy-31-P; SBP=systolic blood pressure; SSQ=seizure severity questionnaire; T1 = Titration Day 1.
In addition, the change from the last pre-UCB0942 administration measurement may be calculated for the placebo subjects for safety and efficacy variables.
REDACTEDion ion 33
tyy varivariyy11). ).
cifcif
COPY he sehe se
This do
cumen
tpresspressQOQO
cann
ot err tanRS=BRS=B
beMMbebus
edmperper
C-C-SSSed tosignsigneraterat
supp
ortratoryatory), echocecho
gns (nsup
any QQ
y aan
marketi
ng
fic Basc Bake
m
autho
rizati
oneizureeizure100..
ablesables
appli
catio
n througthrou
and a
ny ex
tensio
ns
king king d fromfrom
tient pient p
or va
riatio
ns th
ereof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 17 of 62
3.4 Protocol deviationsImportant protocol deviations are deviations from the protocol which could potentially have a meaningful impact on the study conduct or on the primary efficacy outcome, secondary efficacy variables, PK data or key safety data for an individual subject. Important protocol deviations will be reviewed as part of the data cleaning process and all important deviations will be identified and documented to confirm exclusion from the analysis sets.
After all data have been verified/coded/entered into a database, all protocol deviations will be classified according to their impact on study objectives during the database pre-lock data evaluation meeting (DEM). The purpose of this meeting will be to check all protocol deviations, define the analysis sets, and check the quality of the data. The review will also help decide how to manage problems in the subjects’ data (e.g., missing values, withdrawals, dropouts, and protocol deviations). After the classification of all deviations, Statistical Programming will then incorporate the definition of the analysis populations into the analysis files for statistical evaluation. If necessary, appropriate actions will be implemented in the SAP before locking the database. After the pre-analysis review, resolution of all issues, and documentation of all decisions, the database will be locked.
3.5 Analysis sets3.5.1 Enrolled SetThe Enrolled Set (ES) will consist of all subjects who have signed the informed consent form (ICF).
3.5.2 Randomized SetThe Randomized Set (RS) will consist of all enrolled subjects randomized into the study.
3.5.3 Safety SetThe Safety Set (SS) will consist of all subjects in the RS who have received at least 1 dose ofIMP.
3.5.4 Full Analysis SetThe FAS will consist of all subjects in the RS who received at least 1 dose of IMP, and have at least 1 post-Baseline seizure diary.
3.5.5 Per Protocol SetThe Per-Protocol Set (PPS) will consist of subjects in the FAS Population who do not have a major protocol deviation impacting the primary efficacy variable.
3.5.6 Other analysis setsThe Pharmacokinetic Per-Protocol Set (PK-PPS) will consist of subjects in the RS who received at least 1 dose of IMP who do not have a major protocol deviation impacting the PK variables.The evaluable population for the PK analysis will consist of those subjects in the PK-PPS for whom a sufficient number of samples are available to determine at least 1 PK parameter. At the discretion of the pharmacokineticist, a subject may be excluded from this set.
REDACTED
ist of ast of a
COPY whowho
This do
cumen
tThe Phe at lat
cann
otrotooto
6P
beotoctococooco
usedPer Per P
colco
to e see s
Psu
pport
ysis is of all suf all seizueiz
any
SS
marketi
ng all ll
f all suf all s
autho
rizati
onhavehav
l enrenr
appli
catio
n anddocumocum
any foof
SAPSAP bbex
tensio
nsdev
decid decidpouts,outs,
rammammor str st
rviatviatva
riatio
ns
be e
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 18 of 62
3.6 Treatment assignment and treatment groupsIncorrectly-treated subjects will be evaluated during the DEM to assess the potential impact of such cases and any special analysis considerations. The treatment assignment for the SS, PK-PPS will be according to the actual treatment received, whereas the treatment assignment for the PPS and the FAS will be based on the randomized treatment.
Listings and summaries will be presented by the most appropriate treatment group and for the most appropriate period and all outputs will use the conventions outlined in Table 3‒2.
Table 3‒2: Table conventions
Label used in outputs Description
By
Arm
Placebo/UCB0942 Subjects randomized to Placebo; period: whole study
UCB0942/UCB0942 Subjects randomized to UCB0942; period: whole study
All UCB0942 Subjects
All subjects; period: whole study
By
Peri
od
Placebo only Subjects randomized to Placebo; period: 1st+ 2nd Inpatient week
UCB0942 TitrationSubjects randomized to UCB0942; period: 1st Inpatient weekSubjects randomized to Placebo; period: 3rd Inpatient week
UCB0942 Maintenance
Subjects randomized to UCB0942; period: 2nd Inpatient week to the end of Outpatient PeriodSubjects randomized to Placebo; period: whole Outpatient Period
UCB0942 TaperSubjects randomized to UCB0942; period: 2- week Taper Period Subjects randomized to Placebo; period: 2- week Taper Period
SFUSubjects randomized to UCB0942; period: SFUSubjects randomized to Placebo; period: SFU
On-UCB0942 Overall
Subjects randomized to UCB0942; period: 1st Inpatient week to end of the Outpatient Maintenance PeriodSubjects randomized to Placebo; period: 3rd Inpatient week to end of the Outpatient Maintenance Period
3.7 Center pooling strategySubjects with highly drug-resistant focal epilepsy will be enrolled at up to 10 clinical centers. The data from all centers will be pooled. The data summaries and statistical analyses will not be performed by center, unless otherwise is stated.
3.8 Coding dictionariesAdverse events and medical history will be coded according to the latest available version of the Medical Dictionary for Regulatory Activities (MedDRA®). Medications will be coded according to the latest available version of the World Health Organization Drug Dictionary (WHODD).
The medical procedures will not be coded.
REDACTEDomizeomizOutpatOutpat
ts rands rand
jects jects ED
COPYtoto UCUzed to Pzed to
C
This do
cumen
t ill
3.83.8ca
nnots witwit
rs. s. ThThl not not
be
ithithus
ed
edCeCe
to su
pport
2
anySSubu
aaaaamark
etingrandorando
ects rancts ra
ubjectsubjecbj
rk
autho
rizati
onPlacPlac
d to Ud to Utient Pent P
domizeomize
io
au
appli
catio
n ; periodperioio
n
B0942B0942cebceb
lic
and d an
ywhole wholeaex
tensio
ns s
studytudyen
e
or ova
riatio
ns th
ereof.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 19 of 62
3.9 Changes to protocol-defined analysesThe protocol states that all analyses will be based on the randomized treatment. However, the PK and safety analyses will be performed on the actual treatment received.
The Change in time to recovery (protocol, section 4.1.3) will not be analyzed in this study.
The efficacy endpoints will be reported and analyzed in the periods specified in the protocol, and also at additional periods if deemed appropriate.
3.10 Definition of study-specific derived variables3.10.1 Seizure frequency related variables
! Seizure frequency
Initial Processing of Diary Data
Each seizure code in the clinical database will be mapped to exactly 1 of the following codes based on the 1981 International League Against Epilepsy (ILAE) classification: I, IA, IA1, IA2, IA3, IA4, IB, IB1, IB2, IC, II, IIA, IIB, IIC, IID, IIE, IIF, or III.
With regard to cluster seizures, investigator sites are to report the number of cluster episodes rather than reporting the estimated number of individual seizures. Therefore, no imputation will be applied for the seizure counts corresponding to reports of cluster seizures.
Calculation of Total Seizure Counts by Study Period
The total number of seizures for seizure types IA1 (not IA2-4), IB (i.e. IB1 and IB2), IC (i.e. IC1, IC2, and IC3), and the total number of focal seizures (IA1, IB, IC), and the total number of seizures for all seizure types (I+II+III) will be calculated across all diary records over the study period being summarized.
Calculation of Adjusted Seizure Frequency
Weekly adjusted seizure frequency for seizure types IA1 (not IA2-4), IB (i.e. IB1 and IB2), IC (i.e. IC1, IC2, and IC3), and the total number of focal seizures (IA1, IB, IC) will be calculated for the period of interest by dividing the number of seizures for each seizure type by the number of days for which the diary was completed for each study period, and multiplying the resulting value by 7.
The 28-day adjusted seizure frequency will be calculated in a similar way as above.
Calculation of Log-Transformed Values
The above values for each study period of interest will be transformed using the function ln(x+1), where ln represents the natural logarithm function.
! Percent reduction in seizure frequencyPercent reduction from Baseline in seizure frequency to the corresponding evaluation Period will be calculated using the following formulae:ChangefromBaselineintheweeklyadjustedseizurefrequencyWeeklyadjustedseizurefrequencyduringtheBaselineperiod × 100
REDACTED eDpes pes IAIA
r of foof fI)) willwill
COPYala
eporteport
riodriodC
This do
cumen
t!!PP
cann
otove vve v+1), w1), w
beof of be
usedustedsted
f Lf L
to su
pportbyy divdiv
diaryiary wwyy
anyncyncy
he tothe toi
marqq ketin
g l b
equencquencaryy fofoyy
autho
rizati
on
1 (no1 (noocal scal s
be cabe ca
appli
catio
n the numhe nu
zures. zures.s of cluof cl
andsificsifican
ythe fothe fcatica
exten
sions
or va
riatio
ns th
ereof.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 20 of 62
The change from Baseline is calculated subtracting the weekly adjusted seizure frequency during the period of interest from the weekly adjusted seizure frequency during the Baseline period.
The following categories of percent reduction in seizure frequency from Baseline to thecorresponding Treatment Period will be computed: <-25%, -25% to <25%, 25% to <50%, 50% to <75%, 75% to <100%, and 100%.
! XX% Responder Rate in seizure frequency
A subject is defined as a responder if s/he has a reduction in seizure frequency of at least XX% from their Baseline seizure frequency. The XX%RRs that will be calculated include, but are not limited to 50%, 75%, and will be calculated as follows:CountofrespondersduringtheperiodCountofrespondersduringtheperiod + Countofnonrespondersduringtheperiod × 1003.10.2 Seizure freedom A subject is defined as seizure free over a specific time period if they meet all of the following criteria:
1. The subject completed this specific time period.
2. The subject did not have any missing diary days over the time period.
3. The subject did not report any seizure of any type over the time period. Period-specific algorithm rules will be added for the seizure freedom evaluation.
! Seizure-free rateThe seizure-free rate (%) for a specific time period will be calculated using the following formula: CountofseizurefreesubjectsduringtheperiodCountofseizurefreesubjectsduringtheperiod + Countofnonseizurefreesubjectsduringtheperiod × 1003.10.3 Seizure-free daysThe percentage of seizure-free days for a specific time period will be calculated using the following formula: CountofseizurefreedaysduringthetimeintervalCount of days of the time interval will available seizure diary data × 1003.10.4 Patient Weighted Quality of Life in Epilepsy InventoryThe Patient Weighted QOLIE-31-P is an adaptation of the original QOLIE-31 (Cramer et al, 1998). The QOLIE-31-P includes 30 items grouped into 7 multi-item subscales (seizure worry [5 items], overall quality of life [2 items], emotional well-being [5 items], energy/fatigue [4 items], cognitive functioning [6 items], medication effects [3 items], and social function [5 items]) and a health status item. The QOLIE-31-P total score, subscale scores, and health status item score are calculated according to the scoring algorithm described below, with scores ranging from 0 to 100 and higher scores indicating better functioning. In addition to these 31 items, the QOLIE-31-P includes seven items assessing the degree of “distress” associated with the topic of each subscale (ie, distress items) and 1 item asking about the relative importance of each subscale topic (ie, prioritization item).
REDACTED e free fr
c time c time
COPY ver er
ypype ove ovreedree
This do
cumen
tcogncognhehe
cann
otent ent ). TheThe
ms], oms], o
be
t Wt Wus
ed Counoun
PaPa
to ntntto supp
ortfree free
CouCan
ydaydayssd
marketi
ng rere freefreehee periperrkau
thoriz
ation
ver ter dom eom e
perioperio
appli
catio
n
e time ptime
the the
andmeemeean
y et alet a
exten
sions
erioderiodns×orarear va
riatio
ns
XX% % re nre n
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 21 of 62
Subscale Scores
As a first step to calculating the subscale scores, the individual responses for the 30 subscale items are rescaled to a 0 to 100 scale with higher scores reflects better functioning; the rescaled values for each item are defined in Section 13.3. Each subscale score is then calculated by summing the rescaled responses for that subscale and dividing by the number of items with a non-missing response. A subscale score will be calculated only if at least 50% of the items within the subscale are present.
Total Score
Total score is calculated as a weighted sum of the subscale scores based on the weighting inSection 13.3. Total score will be missing if at least 1 subscale score is missing. Total score will range from 0 to 100 with a higher score reflecting better functioning.
Health Status Item
Responses for the health status item are a multiple of 10 ranging from 0 to 100 with a higher score corresponding to a better health status. The health status item response is analyzed without rescaling.
Distress Items
Each subscale includes 1 distress item. The response for each distress item is an integer ranging from 1 to 5. The response for each distress item will be converted to a 0 to 100 scale (ie, 0, 25, 50, 75, and 100) with a higher score corresponding to greater distress.
Prioritization Item
The response for each subscale for the prioritization item is an integer ranging from 1 to 7. The prioritization ranking is analyzed without rescaling.
3.10.5 MedicationsEach medication will be classified as either an AED or a non-AED. Medications recorded on the Prior and Concomitant AED case report form (CRF) will be classified as AEDs. Medications recorded on the Prior and Concomitant Non-AED CRF can be classified as either AEDs or Non-AEDs based on the following rules and based on manual review of such medications.
Benzodiazepines taken more than once per week for non-epilepsy indications will generally be classified as AEDs. Generally, benzodiazepines taken with a frequency of QD, BID, TID, QID, 5XD, 6XD, QOD, QAM, or QPM will be classified as AEDs. With regard to PRN use, each individual intake of a benzodiazepine is to be recorded on the CRF and the classification of such benzodiazepines as an AED will generally be assessed on an individual basis. In general, all benzodiazepines will be reviewed during pre-lock meeting to ensure the appropriate classification as AEDs or non-AEDs.
Other medications which pharmacologically can be classified as an AED but which were taken for non-epilepsy indications may also be classified as AEDs. The classification of such medications will be determined during the database pre-lock meeting and prior unblinding.
There may be medications recorded on the Prior and Concomitant Medications CRF which are taken for seizure rescue. These medications will be classified as AEDs. The identification of such medications will be based on a manual evaluation of the indication and other CRF fields.
REDACTEDndinndin
e prioe priothouthou
COPYe for e forwill bewill b
g
This do
cumen
t lassas
OtOt
cann
otdiazepiazepzodiazodiasifisifi
beQ
intakintaus
edEDs. Ds. OD,OD,
toakenkenG
supp
ortConcConclowingowin
n m
any edd
case rase rmark
eting
oriut rescut resc
d as eas
autho
rizati
one cone coto greto gre
itizattiza
appli
catio
n
each dach nv
and
0 t0 tresponespon
any
to 10o 10ex
tensio
nshtingting
tal scoal scoor gg ini
varia
tions
there
of.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 22 of 62
4 STATISTICAL/ANALYTICAL ISSUES4.1 Adjustments for covariatesThe primary analysis will be conducted using adjustment for the stratification variable; the LEV-use factor (3 strata):
1. LEV prior and current use (concomitant use of LEV at study entry).
2. LEV Prior Use Only=History of prior LEV use and must have discontinued 4 weeks prior to study entry.
3. LEV Naïve=No history of prior LEV use, and no use at study entry.
4.2 Handling of dropouts or missing dataMissing data will not be imputed with the following exceptions:
Seizure diary:
Seizure frequency will be computed over non-missing diary days as described in Section 3.10; missing seizure diary days will not be considered in the calculation of seizure frequency.Generally, compliance with the daily seizure diary is expected to be high in a refractory population and, therefore, the impact of missing diary data is expected to be minimal. However, the impact of missing diary data cannot be ruled out, and missing data will be assessed as part of the database pre-lock meeting to ensure an acceptable level of compliance with the seizure diary across the study population.
For subjects who prematurely discontinue, or have missing diary days, the calculation of theseizure frequency over a specified period will be based on available seizure diary up to the lastdiary entry. This effectively imputes the unobserved seizures after discontinuation with the seizure frequency observed prior to discontinuation.
Times and Dates:
Times and partial dates may be imputed for statistical analyses for specific outcomes according to the following rules. Imputed times and dates should not be shown in the listing.
Imputation of Start Times and Partial Start Dates:
! If only the date is specified and it is the date of the first dose, then use the time of the first dose, otherwise, use 00:00.
! If only the month and year are specified and the month and year of first dose is not the same as the month and year of the start date, then use the 1st of the month and 00:00.
! If only the month and year are specified and the month and year of first dose is the same as the month and year of the start date, then use the date and time of first dose.
! If only the year is specified, and the year of first dose is not the same as the year of the start date, then use January 1st and 00:00 of the year of the start date.
! If only the year is specified, and the year of first dose is the same as the year of the start date,then use the date and time of the first dose.
REDACTED e, or h, or h
iodiod wiwis the us the
ii
COPYdad
ut, andut, andtabletable
This do
cumen
tthth!!
cann
othe me m
If onlIf onltheh
bethe mthe momo
usede
wise, wise,
m
tois sis s supp
ortputeduted
mes anes a
anye impe imp
dd tit
marketi
ngunobunobiscontiniscont
autho
rizati
one leve leve
have mhave mill be ll be bb
appli
catio
n on ofn ofto be ho be
is expes expmissimissl
anddescrdescr
f sf
any e
xtens
ions o
r vari
ation
s
or to r to
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 23 of 62
! If the start date is completely unknown and end date is unknown or not prior to first dose, then use the date and time of first dose.
! If the start date is completely unknown and end date is known to be prior to first dose, then set start date equal to end date.
Imputation of End Times and Partial End Dates:
! If only the date is specified, then use 23:59 as end time.
! If only the month and year are specified, then use the last day of the month.
! If only the year is specified, then use December 31 of that year.
! If the stop date is completely unknown, do not impute the stop date.
4.3 Interim analyses and data monitoring4.3.1 Safety Review GroupIn order to monitor the safety data, a Safety Review Group (SRG) will be established prior to the start of the study with the intention of protecting the safety, health, and wellbeing of each participating subject. The precise membership, scope, and responsibilities of the SRG are described in the SRG Charter.
The SRG will meet once the first 4 subjects have completed the Transition-to-Outpatient Period (Visit 6) or withdrawn from the study before Visit 6. Subsequent meetings will occur when the first 10 subjects, the first 16 subjects, and the first 22 subjects have completed Visit 6 or withdrawn from the study before Visit 6. Thereafter, SRG meetings will be held on an as required/ad hoc basis, in response to emerging data, and at the request of any member of the SRG.
The SRG will remain blinded through the first database lock (see Protocol; Section 12.3.3) unless emergent safety information requires unblinding of individual drug allocation for optimal assessment and response to AEs of concern. At the time of the first database lock, the Study Physician(s), clinical pharmacologist, DS representative, biostatistician, and other UCB personnel will be unblinded as to all subjects’ treatment allocation at the beginning of the Inpatient Period.
4.3.2 Blinded Interim AnalysisAn interim analysis will be performed if needed for purposes of planning and designing of future studies. If performed, this analysis will be conducted when at least 75% of patients have been randomized and completed through the Inpatient Period (completed through Visit 5).
All subjects who have completed through Visit 5 at the time of the data snapshot will be included in the interim analysis.
All statistical analyses will be described in detail in a separate interim SAP or appropriate charter document.
For the interim analysis, the primary efficacy variable (75%RR) will be analyzed using the methods described for the primary efficacy analysis. In addition, seizure-free rate, 50%RR, and percent reduction in focal seizure frequency will be analyzed as described for the secondary/exploratory analyses.
REDACTED VisitVisihe firsthe first
ThereTheremergimergi
COPY complcomp
it 6.it 6
This do
cumen
tin thn th
AA
cann
otizedzed
subjesubjee
beperfoperf used
nnallysysisi
tondendesu
pport
macoacded as ed a
d
anys of s of
cologolomark
eting
gh the fh the
on requn reqf cof
autho
rizati
on leteete
. SubsSubt 222 su2 s
eaftereafterng dang da
appli
catio
nh, anh, anponsibionsib
ted thed t
and ill be ll be
ndd
any e
xtens
ions o
r vari
ation
s the
reof.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 24 of 62
The 75%RR, Seizure-free rate, and 50%RR variables may also be analyzed using Bayesian logistic regression. If Bayesian analysis is peformed, the percent reduction in focal seizure frequency from the Baseline will be estimated using Bayesian analysis of variance (ANOVA) and/or ANCOVA. For these analyses, posterior medians, 95% credible intervals for the treatment effect, and additional posterior probabilities will be presented. Non informative and informative priors will be considered, and sensitivity to different prior settings will be assessed. Other efficacy variables may also be analyzed in the Bayesian framework.
The following safety data will also be presented:
! Treatment emergent AEs
! AEs leading to drop-out or withdrawal
! SAEs
! Laboratory assessments out of normal range
! BPRS
The study will not be terminated early for either efficacy or futility based on the results of this interim analysis and therefore, an alpha penalty may not assessed. At a maximum, an alpha penalty of 0.001 may be assessed on the primary efficacy variable.
The study is not expected to be stopped due to safety reasons during this interim analysis, since there are ongoing quarterly Safety Review Group meetings already planned for this purpose. Therefore, no criteria for evaluation of early stopping due to safety are included.
An unblinded team will be established at both the Sponsor and CRO and will include the following roles (all unblinded): Statistician, Statistical Programmer, and Project Lead. All staff involved in the conduct of the study, including staff at UCB, the CRO, participating vendors, and the participating sites will remain blinded to individual treatment identity and will not be informed of the results of the interim analysis until final unblinding.
4.4 Multicenter studiesThe data from different centers will be pooled.
4.5 Multiple comparisons/multiplicityNo adjustments for multiplicity will be made as the statistical analyses will be exploratory in nature.
4.6 Use of an efficacy subset of subjectsAll efficacy analyses will be performed for the FAS. The primary analysis will be performed for the PPS as well. No further efficacy subsets are planned.
4.7 Active-control studies intended to show equivalenceNot applicable.
4.8 Examination of subgroupsDescriptive analysis may be performed by the 3 LEV-use levels for some variables, including, but not limited to the primary efficacy variable, and the seizure-freedom.
REDACTED oup oupy stoppy stopp
at bothat bothsticiansticianincinc
COPY caca
fetyfety reryyp mep m
This do
cumen
t e e
4.74.7ca
nnot efficacfficac
PPSPPS
be us
edfor mfor mto
tipm
supp
ort
centersenter
ple cple c
any sstudtudmark
eting
n, Sn, ncludincludin
inded tndedrim anim an
autho
rizati
oneasoaso
eetingeetingping dping d
h the Sh the SStaSta
appli
catio
n tyty babayysed. Aed. A
variablariab
sons ons
and a
ny ex
tensio
ns or
varia
tions
there
of.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 25 of 62
Descriptive analysis will performed for subjects requiring dose reduction from study medication at any point during the study prior to the protocol-defined taper. The following tables will be repeated for these subjects:
! 75%, 50% Responder Rate in Focal Seizure Frequency Summary
! Incidence of TEAEs - Overview
! Incidence of TEAEs
4.9 End of Study AnalysesThe database lock and unblinding may occur in a tiered approach, as described in the protocol. Details regarding the tiered database lock will be described in the Data Management Plan (DMP).
Data analysis and production of TFLs will occur as follows:
After the final subject has completed through Visit 15 (end of Outpatient Maintenance Period) and the corresponding database lock has occurred, all TFLs will be produced and analyses of all data at time points through Visit 15 will be considered final. Note that unblinding of the placebo-controlled portion of the study (Visits 3-5) will occur prior to this analysis, as described in the protocol and DMP. TFLs will include all study visits as planned in the SAP. However, only those time points through Visit 15 will be considered final. TFLs will be annotated with a header to display which visits are considered final.
After the final subject has completed through Visit 20 (End of Taper and Safety Follow Up Period) and the corresponding database lock has occurred, all TFLs will be produced and analyses of all data at time points through Visit 20 will be considered final.
After the final subject has completed the echocardiogram required at 6 months (±1 month) after the last dose, and the corresponding database lock has occurred, the echocardiogram TFLs will be produced and considered final.
5 STUDY POPULATION CHARACTERISTICS5.1 Subject dispositionThe number of subjects screened, enrolled into the study, subjects included in each analysis set, and subjects who completed or prematurely discontinued the study, as well as the reason for discontinuation, will be presented for the RS by treatment group, and for All Subjects using frequency counts and percentages. The discontinuations due to AEs will be summarized in a separate table. Screen failure reasons will be summarized.
In addition, the following listings will be provided by treatment group:
! Subject disposition (ES)
! Study discontinuation (RS)
! Subject visit dates (RS)
! Subject analysis sets (ES)
REDACTED gh Visgh Vis
ock haock hugh Vugh V
d thd th
COPY vivsideresidere
al.al.
This do
cumen
t! SS
!!
cann
ottabtab
dditiondition
S
becounounbleble
used
cocon, wil, wil
untsnts
toec
omomppsu
pport
ddispis
cts scrts scr
any PULPULmark
eting
he echoe echo
databadatab
autho
rizati
on
sit 20 (t 20 as occas oc
Visit 2isit 2
appli
catio
nte thathaprior tprior
s as plaas pd finad fina
and
nt ntprodurodu
tt
any
MaiMaiex
tensio
ns propro
ent Plant Plaor otooto
varia
tions
there
of.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 26 of 62
5.2 Protocol deviationsA listing of all important protocol deviations identified at the database pre-lock meeting will be presented for all subjects in the FAS, and will include the deviation type and description. The number and percentage of subjects in the FAS with important protocol deviations will be summarized by period and overall if appropriate. The denominator for percentages will be the number of subjects in the FAS.
6 DEMOGRAPHICS AND OTHER BASELINE CHARACTERISTICS
6.1 DemographicsA by-subject listing of Baseline demographic characteristics will be presented by treatment group for the ES. This will include the date of birth, age (in years), sex, race, ethnicity, height (in cm), weight (in kg), and body mass index (BMI, in kg/m²).
All Baseline demographic characteristics obtained at the Screening Visit will be summarized for the FAS by treatment group, and for All Subjects (apart from the date of birth).
BMI (in kg/m²) is calculated based on the following formula:BMI �kgm�� = Weight(kg)Height(m)�Body mass index will be reported to 1 decimal place.
The following age groups will be summarized in the same table:
! 12 - <18 years ! ≤18 years! 18 - <65 years ! 19 - <65 years! 65 - <85 years ! ≥65 years! ≥ 85 years
Childbearing potential will be listed for the RS.
Lifestyle information (alcohol, tobacco, caffeinated beverage, and illicit drug use) will be listed and summarized by treatment group and for the RS.
6.2 Medical history and concomitant diseasesMedical history and ongoing medical conditions will be listed and summarized for the SS by treatment group and MedDRA® system organ class (SOC) and preferred term (PT). The start date (month and year only) and end date (or ongoing if applicable) will also be included in the listing. Epilepsy history will not be included in these tables.
Procedure history will be listed separately by the procedure reported term for the SS by treatment group. Concomitant medical procedures carried out during the study will be listed for the SS. For this listing, concomitant is defined in Section 6.3 as for concomitant medications.
6.2.1 History of epilepsyThe history of epilepsy will be listed for all subjects in the ES.
REDACTEDal plaal pl
rized ized i
!! ≤≤!
COPY ightighHeighHeigPY
ac
This do
cumen
t ProcProcgrgr
cann
ot t grg
monthmonthng. ng. EE
be toryor
grougrouus
edMededryry aa
to tr
dicicsu
pport
be be
alcohollcohoeatmeatm
any
listelis
marketi
ng ≤1
19 19 !!
autho
rizati
on htt ((
ce.e.
in the in the
18 y8 y
appli
catio
n at
kgkg))(m)(m)ppan
disit wsit wte ofe of
any
wilwi
exten
sions
byy treatreaethniethni
or va
riatio
ns th
ereof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 27 of 62
Etiology of epilepsy
The number and percentage of subjects with each type of etiology as specified in the CRF (genetic, congenital, etc) will be summarized for the FAS and listed for the RS.
Epileptic seizure profile
The number and percentage of subjects experiencing each seizure type during the last 4 weeks prior to the screening visit will be summarized for the FAS based on the ILAE Seizure Classification History CRF.
The overall number and percentage of subjects with a history of type I, II, III seizures will be summarized. In addition, the overall number and percentage of subjects with a history of type IA, IB, IC will be summarized.
Focus localization
The number and percentage of subjects with each category of focus localization (unknown, frontal, temporal, parietal, occipital) will be summarized for the FAS. Subjects may be counted in more than 1 category of focal localization.
History of epileptic seizures
History of epileptic seizures, including the number and percentage of subjects with a history of status epilepticus, the number and percentage of subjects with a history of withdrawal seizures, and quantitative summaries of epilepsy duration, age at onset of first seizure, and percent of life with epilepsy, will be summarized for the FAS and listed for the RS.
Historical seizure count
The Historical Seizure Count CRF records the number of seizures experienced by the subject during the 4 weeks prior to study entry. These data will only be provided in subject data listing for the RS and will not be summarized.
Seizure types experienced during baseline
The number and percentage of subjects experiencing each seizure type during the Baseline Period will be summarized for the FAS based on data from the subjects’ seizure diaries. The following seizure types will be summarized: I, IA, IB, IC, II, IIA through IIF, III, and clusters.
Subjects will be counted for all higher levels of seizure type categories corresponding to the seizure types or seizure sub-types reported on the CRF. For example, subjects with an IA1 seizure will be counted for types I and IA.
Baseline focal seizure frequency
Baseline weekly adjusted weight frequency will be summarized with descriptive statistics for the FAS. Additionally, baseline weekly adjusted frequency will be summarized for the FAS for seizure types IA, IB, and IC.
6.3 Prior and concomitant medicationsThe medications will be classified as AEDs or non-AEDs based on coded terms. The list of coded terms considered AEDs will be finalized prior to database lock and unblinding. Prior and concomitant non-AED medications will be listed for the SS by treatment group and by WHODD
REDACTEDn, ,
ASAS anan
ecordecordryry
COPYnd pnd ubjectubjectage age
This do
cumen
tFASFASseisei
cann
ote focfocno
eline eline
be bebe us
ed couou
or seizr seize coe co
tounteuntesu
pport
e of ofzed for ed fo
es wills will
anyg bg by
f subf su
marketi
ngds theth
y. ThesTheszed.ed.
basebas
autho
rizati
onts w
e at onat ond listed liste
he nhe
appli
catio
n
rcentagcentawith with
andSubSuban
yizatioizatiobjecbje
exten
sionsryy of ofyy
orill bill bvari
ation
s
b
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 28 of 62
Anatomical Main Group [Level 1], Therapeutic Subgroup [Level 2], PT and reported term. This listing will be repeated for all AED medications.
Any non-coded terms will report Level 1 and Level 2 as UNCODED in the listing.
Prior medications include any medications that started prior to the date of first dose of study drug. Concomitant medications are medications taken at least one day in common with the study medication dosing period. Medications may be both prior and concomitant. Past medications are a subset of prior medications, and include prior medications with a stop date before the date of first study medication administration.
6.3.1 Non- Antiepileptic drugsThe number and percentage of subjects taking prior non-AED medications will be summarized for the SS by WHODD Anatomical Main Group [Level 1], Therapeutic Subgroup [Level 2], and PT.
The number and percentage of subjects taking concomitant non-AED medications will be summarized separately for the SS by WHODD Anatomical Main Group [Level 1], Therapeutic Subgroup [Level 2], and PT, and by treatment group for the whole study period. In the same table, the number and percentage of subjects taking concomitant non-AED medications will be summarized by the following treatment periods as defined in Section 3.2.1.2: Placebo Only, UCB0942 Titration, UCB0942 Maintenance, UCB0942 Taper, and UCB0942 Overall.
6.3.2 Antiepileptic drugsPrevious AED Medications
The number and percentage of subjects taking prior or concomitant AED medications will be summarized for the SS by PT.
Number of previous AEDs
The number of AEDs taken prior to study entry will be summarized for the SS based on the following categorization: <4, 4 or 5, 6 or 7, 8-10,>10 AEDs.
Previous AEDs by reason for AED discontinuation
The number and percentage of subjects by reason for discontinuation of previous AEDs will be summarized for the SS. Percentages for each reason for discontinuation will be relative to the number of subjects taking each AED.
Since reason for discontinuation is collected as free text field, a medical review will be conducted prior to database lock and unblinding to combine like terms. The combined terms only will be presented in the summary table. Both the reported and combined terms will be listed.
Use of vagal nerve stimulation at study entry
The number and percentage of subjects with active vagal nerve stimulation (VNS), and the percentage of subjects with no VNS implant or a non-active VNS implant will be summarized for the SS.
All other VNS data (eg, use of magnet, VNS settings) will be listed but will not be summarized.
REDACTED
ects taects ta
COPYnn
defineefinCB094B094
This do
cumen
tlistedsted
UU
cann
ot asoso
ucted pcted yy willwillyyd
be
on fon fus
edthe he bjectsjects
toercenrceSS
supp
ort 4, 4, 44
on forn foup
ntant
anyior toior t
4 or4 o
marketi
ngakingkingau
thoriz
ation42 Ta42 T
ng png
appli
catio
nGrouGrohole stole s
itant ntant nd in d in SeSap
andD medmed
oupou
any gg ex
tensio
ns
l be sube sgrouprou
or va
riatio
ns
te e
thereo
f.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 29 of 62
Number of AEDs taken at study entry
The number and percentage of subjects taking 1, 2, and 3, 4, 5, >5 AEDs at the time of study entry will be summarized for the SS. The same summary will be reported separately by VNS use at study entry (no VNS or VNS not active versus currently active VNS).
Levetiracetam use at study entry
The number and percentage of subjects in each LEV-use category at study entry will be summarized for the SS:
1. LEV prior and current use (concomitant use of LEV at study entry).
2. LEV Prior Use Only=History of prior LEV use and must have discontinued 4 weeks prior to study entry.
3. LEV Naïve=No history of prior LEV use, and no use at study entry.
Concomitant AED Medications
The number and percentage of subjects taking concomitant AED medications will be summarized separately for the SS by PT, and by treatment group for the whole study period. In the same table, the number and percentage of subjects taking concomitant non-AED medications will be summarized by the following treatment periods as defined in Section 3.2.1.2: Placebo Only, UCB0942 Titration, UCB0942, UCB0942 Taper, and UCB0942 Overall.
Changes to Concomitant AEDs
All concomitant AEDs will be listed for subjects requiring a dose change to any concomitant AED during the study. A change is defined as any of the following occurring after randomization through the end of the Outpatient Maintenance period:
! Initiation of a new AED
! Termination of an existing AED
! Dose change for an existing AED (increase or decrease)
! Change in frequency of an existing AED
7 MEASUREMENTS OF TREATMENT COMPLIANCEStudy drug compliance will be assessed from the day of first IMP administration to the day of last dose during the taper period, or up to the end of the outpatient period for the subjects who will continue to the open label extension (OLE). Compliance will be calculated as 100 times the dose (tablets) taken divided by the planned dose (tablets) that should have been taken. If a subject withdraws from the study during a treatment period, their compliance will be calculated up to the time that they dropped out. After a subject has dropped out, the compliance should not be set to zero. Compliance will be listed and summarized for the SS.
Compliance will be included in the study drug administration listing. In addition, the mean compliance will be listed for each subject, for each of the following treatment periods: 1st
Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week, Outpatient Maintenance Period, Tapering Period, SFU Period, UCB0942 Overall.
REDACTED bjects bjects
ned asned aOutpaOutp
COPYs
aper, aper,
This do
cumen
tp ttbe sebe se
C
cann
obletsletsect witct wit
to tho th
beue toe ts)s)
used
plianianng theg theo t
to anceancesu
pportncycy of ofyy
SURSUR
anystingstingmark
eting
at
AEDAED
A
autho
rizati
on
s requirequis any any
tientient
appli
catio
nfor tor toncomoncom
efined finedand UCnd U
anddicatidicat
theth
any e
xtens
ions weeks weeks or
varia
tions
there
of.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 30 of 62
Compliance will be summarized by treatment group for the following treatment periods: 1st
Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week, Outpatient Maintenance Period, Tapering Period, SFU Period, and UCB0942 Overall. The compliance for the subjects randomized to placebo will be summarized separately for the Placebo and UCB0942 compliance. Additionally, the number and percentage of subjects with compliance levels <80%, 80% to 120%, and >120% will be summarized by treatment group for the overall UCB0942 treatment period.
8 EFFICACY ANALYSESAll seizure diary data will be listed for the RS. The summaries will include the statistics for continuous or categorical variables as specified in Section 3.1.
For the efficacy analyses the term “by treatment group” corresponds to the UCB0942/Placebo group, the UCB0942/UCB0942 group, and the All UCB0942 Subjects group.
8.1 Statistical analysis of the primary efficacy variableThe primary outcome measure is the 75%RR which is defined as the proportion of subjects with a 75% or greater reduction in focal seizure frequency during the 2-week Inpatient Period (as defined in Section 3.2.1.2) compared to the Baseline Period.
The 75%RR will be analyzed using a logistic regression with effects for treatment, for the 3 levels of LEV use, and the log-transformed Baseline seizure frequency as a continuous covariate.
The frequency and percentage of 75%RR will be reported with the estimated odds-ratios and two-sided Wald 95% CI for UCB0942 versus placebo.
The primary analysis will be performed for the FAS but also for the PPS.
8.2 Statistical analysis of the secondary efficacy variablesAll analyses of the secondary efficacy analyses will be done for the FAS.
Median percent reduction in weekly focal seizure frequency
The percent reduction in focal seizure (Type IA1+IB+IC) frequency from Baseline Period to the 2-week Inpatient Period will be compared between the UCB0942 and placebo arms using a Wilcoxon-Mann-Whitney test. The Hodges-Lehmann non-parametric estimator will be used to estimate the median percent reduction in seizures between groups and its corresponding 95% CI will be provided.
Percent reduction in focal seizure frequency from the Baseline Period to the Outpatient Maintenance Period and On-UCB0942 Overall will be assessed using summary tables by treatment group.
The percent reduction in focal seizure frequency from the Baseline Period to the 2-week Inpatient Period, the Outpatient Maintenance Period and the On-UCB0942 Overall period will be presented graphically with box-plots.
75%RR on percent reduction in weekly focal seizure frequency
This score will be calculated during the last 4 weeks of the Outpatient Maintenance Period, and On-UCB0942 Overall, and will be compared to the Baseline Period by treatment group using summary statistics.
REDACTEDll be rl be rsus plsus pl
ed ed for for
sissis
COPYsion sionline seine s
This do
cumenThe phe pInpInp
cann
otancancment ment
pepe
beductictiee
used
ananed. d.
ioi
ton pen pesu
pport
ocalcal sd will bwill
tneytney tyy
anyekleklyny
se
marketi
ng
s of thof thacycy anaanyy
llyy f
autho
rizati
oneizuzu
eporteeportlaceboacebo
the FAhe F
appli
catio
n2-we-we
with effwith eure fure
and e propprop
any riablriabex
tensio
ns cs
B0942B0942p.
orforforva
riatio
ns th
ereof.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 31 of 62
Seizure free rate
The seizure free rate for the 2-week Inpatient Period will be analyzed using a logistic regression with effects for treatment and log-transformed Baseline seizure frequency as a continuous covariate, if applicable. Odds-ratio of UCB0942 versus placebo groups and its 95% CIs will be estimated.
The seizure freedom will also be evaluated by treatment group for the last 4 weeks of the Outpatient Period and for the On-UCB0942 Overall period using summary statistics.
Percentage of seizure free days
The percentage of seizure free days will be assessed during the 2-week Inpatient and the Outpatient Maintenance periods using summary statistics by treatment group. 95% Hodges-Lehmann CIs for the median will be estimated.
8.3 Analysis of exploratory efficacy variablesAll analyses of the exploratory efficacy analyses will be done for the FAS.
50%RR on percent reduction in weekly focal seizure frequency
The 50%RR on percent reduction in weekly focal seizure frequency for the 2-week Inpatient Period (see Section 2.2.1.3) will be analyzed only for the FAS using a logistic regression with effects for treatment, for the 3 levels of LEV-use, and the log-transformed Baseline seizure frequency as a continuous covariate. The 50%RR at the Outpatient Maintenance Period will be summarized by treatment group.
Median seizure frequency by focal seizure type
An analysis of covariance (ANCOVA) will be performed on the log-transformed weekly seizure frequency during the 2-week Inpatient Period. Specifically, ln(1+weekly seizure frequency during the 2-week Inpatient Period) will be modeled with treatment group as factor and ln(1+weekly seizure frequency during the Baseline Period) as covariate. Contrasts will be estimated to compare UCB0942 to placebo results observed. Transformation of efficacy data could be envisaged given the data distribution. This analysis will be repeated for all the subtypes of focal seizures (Type IA1, IB, IC, and disabling [IB+ IC]).
The seizure frequency for the focal seizures (Type IA1+ IB +IC) and focal seizure subtypes (Type IA1, IB, IC, and disabling [IB+ IC]) will also be summarized by treatment group and UCB0942 Overall for the following study periods: Baseline, 1st Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week, 2-week Inpatient, Outpatient Maintenance Period, and On-UCB0942 Overall.
The mean 28-day adjusted seizure frequency by focal seizure subtype (Type IA1, IB, IC, and disabling [IB+ IC]) will be displayed graphically as stacked bar charts for the following study periods: Baseline, 1st Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week, 2-week Inpatient,Outpatient Maintenance Period, and On-UCB0942 Overall. This will also be presented by subject.
The mean percent reduction in seizure frequency from baseline to each of the following study periods will be presented as a bar chart: 1st Inpatient Week, 2nd Inpatient Week, 3rd Inpatient
REDACTED RR
re e tytypyDA
A) wiA) wintnt
COPYr ther thand thand
R at tR at t
This do
cumen
tdisabisabperiperO
cann
ot meanmeanblibl
benpatpa us
edC, a, a
erallrall ftieti
to ncycyandand
supp
orhe dhe d
IAA11, IBI
y for fory
any42 to 42 to
datadat
marketi
ngwill bell bPeriodPeriod
) will bwill buring tring
autho
rizati
on he
the Ohe O
peeuth
bebe
appli
catio
n quencyquenc
FAS usAS ue loglog
andFASASan
y SS
exten
sions
d the the % Hod% Ho
or va
riatio
ns th
ereof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 32 of 62
Week, 2-week Inpatient, Outpatient Maintenance Period, and On-UCB0942 Overall. This will also be presented by subject
Change in seizure severity
Seizure severity is calculated as the percentage of seizures that are type IC out of the total number of focal seizures during a given period. Change from Baseline in seizure severity is the seizure severity in the period of interest minus the seizure severity during the 2-week prospective baseline period. Seizure severity and its change from baseline will be listed and summarized by treatment group for the 2-week Inpatient and Outpatient Maintenance Periods. For subjects not experiencing IC seizures during the observed period, severity is considered to be 0%.
Seizure severity questionnaire
Changes in SSQ will be summarized by treatment group for the Inpatient Period (V3, 4, 5), the Outpatient Period (V10, 15) and for the Tapering and SFU periods (V15, 17, 18, 20) using summary statistics. Mean change from baseline in SSQ total and subscores will be presented graphically.
The SSQ total score (TS) is derived using the algorithm in Appendix x.
Quality of life
The observed values, and changes from Baseline for the QOLIE-31-P total score and the subscales will be listed for all subjects for visits 3, 10, 12, 15, 17. The prioritization item will be listed separately.
The QOLIE-31-P change from Baseline will be summarized by treatment group usingdescriptive statistics for visits 10, 12, 15, 17.
The QOLIE-31-P mean change from Baseline for the total score and the sub-scores will be presented in line plots with 95% Hodges-Lehmann CIs for the whole study period.
Exploratory analyses for efficacy
Median 28-day seizure frequency by focal seizure type: An analysis of covariance (ANCOVA) will be performed on the log-transformed weekly seizure frequency during the 2-week Inpatient Period. Specifically, ln(1+weekly seizure frequency during the 2-week Inpatient Period) will be modeled with treatment group as factor and ln(1+weekly seizure frequency during the Baseline Period) as covariate. Contrasts will be estimated to compare UCB0942 to placebo results observed. Transformation of efficacy data could be envisaged given the data distribution. This analysis will be repeated for all the subtypes of focal seizures (Type IA1, IB, IC, and disabling [IB+ IC]).
The seizure frequency for the focal seizures (Type IA1+ IB +IC) and focal seizure subtypes (Type IA1, IB, IC, and disabling [IB+ IC]) will also be summarized by treatment group and UCB0942 Overall for the following study periods: Baseline, 1st Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week, 2-week Inpatient, Outpatient Maintenance Period, and On-UCB0942 Overall.
Exploratory analysis will be performed on the seizure count and SSQ data collected during the tapering and SFU periods. The focal seizure frequency will be summarized by treatment groupfor the tapering and SFU periods.
REDACTED will beill be
5,5, 1717
m Bam Ba
COPYr the r the3, 10, 3, 10,
This do
cumen
tTyTyppyyUCBUCWW
cann
ot ]).).
seizuseizupepe
beill beill b us
ediate.te
nsformsforme re r
to mene. Ce C
supp
ortlogog--tratrn(1+we1+wnt grnt g
any ncyncy bbymark
etingaselineaselin
dgesges--LeL
autho
rizati
on 12, 12,
e e summsum.
appli
catio
n ndix xdix
QOLIEQOLI151
and
x
any,,
res wires wex
tensio
ns
od (Vd (V18, 18,
or va
riatio
ns
vve e byby
ts nos no
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 33 of 62
The relationship between QOLIE-31-P parameters and efficacy parameters will be evaluatedgraphically. Plots may include, but are not limited to, scatterplots of the QOLIE-31-P subscales and total score versus the focal seizure reduction at the end of the Outpatient Maintenance Period. This plot will be repeated for the 75%RR.
All video data recorded in the CRF will be listed.
9 PHARMACOKINETICS All PK analyses will be performed for the PK-PPS.
9.1 Non compartmental PK analysisPlasma concentrations of UCB0942, will bedetermined from blood samples obtained in the study, during the Titration and Maintenance Periods in order to investigate the population PK of UCB0942 and its major metabolites.
Individual concentrations of UCB0942, will be listed by treatment group for the FAS and will include the actual and nominal sampling times and the deviation between them. All deviations will be calculated relative to the IMP administration.
Individual concentrations will be summarized by treatment group, and sampling times for the PK-PPS using n, mean, median, SD, minimum, maximum, geometric mean, and geoCV and 95%CI (assuming log-normally distributed data). This table will be repeated for UCB0942,
.
The following plots will be produced for UCB0942,for the PK-PPS:
! All individual concentration time profiles will be displayed graphically on a linear and semi-logarithmic scale.
! Spaghetti plots with the individual plasma concentrations over time profiles for eachtreatment group will be displayed for all subjects (linear and semi-logarithmic scale).
! Geometric mean profiles (with and without corresponding lower and upper limit of the 95%CI) for the treatment groups will be displayed on the same plot.
The figures will include the LLOQ on the semi-logarithmic plots only.
The following PK parameters will be calculated for UCB0942 and its metabolites:
! AUCτ: area under the plasma concentration-time curve over a dosing interval, asdetermined using the linear trapezoidal rule.
! Cmax: maximum observed plasma concentration.
! tmax: time of Cmax.
! t½: apparent terminal elimination half-life, reported hours, as determined via simple linear regression (slope = -λz) of natural log (ln) concentration vs time for data points in the terminal phase of the concentration-time curve. t½ is calculated as ln(2)/λz.
! Ctrough: measured concentration at the end of a dosing interval at steady state.
REDACTED COPY mumu
table wtable w
CB094CB094
e profie prof
This do
cumen
t can
not b
e use
d to su
pport
any m
arketi
ng au
thoriz
ation
appli
catio
n and
anal samal samto the o the
oup, anup, ageomegeom
will beill be
42,42,
files wiles w
dual plaual pplayayed fed
es (with(witgroupgrou
ude thede th
K parapar
areaaremined mined
Cmaxmax::
ttmm
!!
y exten
sions
or va
riatio
ns th
ereof.
ill bell beMainteMaint
metabmetab
d any
zat
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 34 of 62
The PK parameters will be calculated via NCA methods using Phoenix WinNonlin (version 6.2 or higher) using the actual sampling times by PRA with UCB’s supervision. Actual sampling times relative to dosing rather than nominal times will be used in the calculation of all derived PK parameters.
The PK parameters of UCB0942 and its metabolites will be listed and summarized using the following descriptive statistics: n, geometric mean, lower and upper 95% CI, geometric CV, arithmetic mean, SD, median, and minimum and maximum values.
Graphical outputs over time will be produced on the trough plasma drug concentrations.
9.2 Population pharmacokineticsIf appropriate, a population PK analysis of UCB0942 and identified active metabolites, will be performed using non-linear mixed effects modeling within the population software (NONMEM) aimed at identifying relevant covariates (demographic variables, other AEDs). The population PK analysis will be performed by UCB and will be described in a separate data analysis plan (DAP), and it will be reported in a separate report.
9.3 Pharmacokinetic/pharmacodynamic analysis Exploratory population PK-PD analysis may be performed if needed to characterize the relationship between exposure to UCB0942 and the clinical and/or safety clinical outcome. A separate DAP will describe the analysis, which will be reported in a separate report.
10 SAFETY ANALYSES10.1 Extent of exposureAll study drug administration information will be listed by treatment group.
The duration of study drug will be calculated as the date of last dose of study drug minus the date of first dose of study drug plus 1 day. The duration will be listed for each subject for the following treatment periods: 1st Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week, Outpatient Maintenance Period, Tapering Period, SFU Period, UCB0942 Overall.
The duration of study drug exposure will be calculated as the date of last dose of study drug during the Period of interest minus the date of first dose of study drug plus 1 day.
The duration of study drug exposure (in days) will be summarized by treatment group. The exposure for the subjects randomized to placebo will be summarized separately for the Placebo and UCB0942 exposure. The number and percentage of subjects with the following categories of durations of study drug exposure will also be summarized: ≤1 week, >1 to ≤2 weeks, >2 to ≤4 weeks; 4 to ≤6 weeks; >6 to ≤8 weeks; >8 to ≤9 weeks; >9 to ≤11 weeks; >11 weeks.
10.2 Adverse eventsAdverse events will be recorded from the time informed consent is granted until study completion or study termination (end of the SFU period). All AEs will be coded using the latest available version of MedDRA and will be categorized by intensity (mild/moderate/severe).
Listings will be provided for all AEs, SAEs, AEs leading to tapering, AEs leading to withdrawal, and AEs leading to death by treatment group for the SS.
REDACTED
mation mation
COPYcliniclinill be rill be
This do
cumen
t 0.20.AdAd
cann
ot s ofo
s; 4 to 4 to
22
be 42 42
of stuof stuus
ed uu
he subje sub2 exex
toddy dy su
pport
ug expg ex
nterest terest
any nnp
d, Tapd, Tamark
eting
n wiwi
lculatedlculateay. Theay. Thpatiepat
autho
rizati
onreprep
will bill b
appli
catio
n nalynalysf needef need
al l and/andporteport
and
s
any
s)ste de dataat
exten
sions
bolitesolites
tware ware ).). ThT
or va
riatio
ns th
ereof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 35 of 62
A treatment-emergent adverse event (TEAE) is defined as any event not present prior to the initiation of the first dose of study treatment or any unresolved event already present before initiation of the first dose that worsens in intensity following exposure to the treatment.
The number and percentage of subjects who experience TEAEs will be summarized by SOC and PT, and by treatment group. In the same table, the number and percentage of subjects will be summarized by the following treatment periods as defined in Section 3.2.1.2: Placebo Only, UCB0942 Titration, UCB0942 Maintenance, UCB0942 Taper, and On-UCB0942 Overall.
The following tabular summaries will be presented for the SS:
! Incidence of AEs - Overview
! Incidence of TEAEs
! Incidence of Serious TEAEs
! Incidence of TEAEs by Relationship
! Incidence of SAEs by Relationship
! Incidence of Non-Serious TEAEs by Relationship
! Incidence of Fatal TEAEs by Relationship
! Incidence of TEAEs by Maximum Relationship
! Incidence of TEAEs by Maximum Intensity
! Incidence of TEAEs leading to Tapering
! Incidence of TEAEs leading to Withdrawal
! Incidence of Non-Serious TEAEs above the Threshold of 5% of Subjects
! Incidence of Non-Serious TEAEs above the Threshold of 5% of Subjects by Relationship
Where dates are missing or partially missing, AEs will be assumed to be treatment-emergent, unless there is clear evidence (through comparison of partial dates, see Section 4.2) to suggest that the AE started prior to the first dose of study treatment.
Summary tables will contain counts of subjects, percentages of subjects in parentheses and the number of events where applicable. A subject who has multiple events in the same SOC and PT will be counted only once in the subject counts but all events will be included.
In summaries including relationship to study treatment, the following relationships will be summarized: ‘Not related’, ‘Related’. Subjects who experience the same event multiple times will be included in the most related category. Events with missing relationship will be considered as ‘Related’ to the last given study product for summary purposes but recorded as missing in the listings.
In summaries including intensity, the following intensity categories will be summarized: ‘Mild’, ‘Moderate’, ‘Severe’. Subjects who experience the same event multiple times will be included in the most severe category. Events with missing intensity will be considered as ‘Severe’ events for summary purposes but recorded as missing in the listings.
REDACTED ttyy
ringing
Withdrithdr
COPY ip ip
This do
cumen
tas ‘Rs ‘Rlistilist
cann
otari
arizedrizedl be inbe inReRe
beies iies ius
eds whwh
ed onld onto
ll coll cwhewhe
supp
ort nce (tce (
r to theto th
contaon
any rtiallrtially
(thrth
marketi
ng aww
above abov
AEs abAEs a
autho
rizati
on
wal wal
appli
catio
n and
any e
xtens
ions o
r vari
ation
s the
reof.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 36 of 62
Adverse event summaries will be ordered in terms of decreasing frequency for SOC, and PT within SOC, in the UCB0942 overall column.
10.3 Clinical laboratory evaluationsAll summaries of laboratory parameters will only summarize parameters planned based on the protocol; however, both planned and unplanned laboratory parameters will be provided in subject data listings.
Observed laboratory data (chemistry, hematology, urinalysis measurements as listed in Table 8‒1), and changes from Baseline for numeric parameters will be listed and summarized for the SSby treatment group. The change from the last pre-UCB0942 administration measurement will be listed and summarized for the placebo group. Laboratory values will be grouped according to the laboratory function panel shown in Table 8‒1 and flagged as high or low based on thepossibly clinically significant treatment emergent (PCST) criteria, if applicable. The number and percentage of subjects with a PCST low or high value will be summarized by treatment group. In the same table, the number and percentage of subjects will be summarized by the following treatment periods as defined in Section 3.2.1.2: Placebo Only, UCB0942 Titration, UCB0942Maintenance, UCB0942 Taper, and UCB0942 Overall.
Possibly clinically significant treatment emergent criteria are based on FDA Division of Neuropharmacologic Drug Products guidelines with some UCB-defined additions (Section 13.2).
For the laboratory parameters that are identified in Table 8‒1, the change in category (normal range: low, normal, high) at the end of Maintenance from Baseline will be presented in shift tables.
Additional laboratory tests (including serology –only at Screening-, drugs and alcohol,pregnancy) performed will be listed, but will not be summarized. REDACTEDenanenan
seroloserol, but , but
COPYh somsom
in n TaTa
This do
cumen
t can
not b
e use
d to s
uppo
rt any
mark
etingwill will a
uthori
zatio
nbleble 88e e fromfro
ogygy ––
appli
catio
n e basedbase
e UCBUCB
and izedzed
0942 942 an
y d byby tyyd byd b
exten
sions
mententaccordccord
sed oed oble. Tle. T
t
or thth
tt wwva
riatio
ns
lee 88‒‒he She S
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 37 of 62
Table 8‒1: Clinical laboratory measurements
Category Panel Variable
Serology HBsAg, HCV Ab, HIV1 Ab, HIV2 Ab
Hematology
Red blood cell RBC count, hemoglobina, hematocrit, MCH, MCHC, MCV
White blood cell WBC counta, basophils, eosinophils, lymphocytes, monocytes, neutrophilsa
Platelet Platelet count
Clinical chemistry
Electrolytes Sodium, chloride, potassium
Minerals Calcium, magnesium
Metabolic Glucose
Liver function ALPa, ALTa, ASTa, total bilirubina, LDH
Kidney function BUN or urea
Other Creatininea
Urinalysis Dipstick Total protein, pH, glucose, WBC, RBC ALP=alkaline phosphatase, ALT=alanine aminotransferase, AST=aspartate aminotransferase, HBsAg=hepatitis B surface antigen, HCV-Ab=hepatitis C virus antibody, HIV=human immunodeficiency virus, LDH=lactate dehydrogenase; MCH=mean corpuscular hemoglobin; MCHC=mean corpuscular hemoglobin concentration; MCV=mean corpuscular volume; RBC=red blood cell; WBC=white blood cell.aShift tables will be presented for these variables.
10.4 Vital signs, physical findings, and other observations related to safety
10.4.1 Vital signsA by-subject listing of all observed vital measurements (including SBP, DBP, PR, respiratory rate, weight, oral body temperature) and changes from Baseline will be listed. This listing will include a flag for measurements identified or as being PCST as calculated by the criteria outlined in Section 13.2.
Measured values, and changes from Baseline for all vital sign measurements (excluding weightand temperature) will be summarized by treatment group and timepoint. The change from the last pre-UCB0942 administration measurement will be listed and summarized for the placebo group.
The number and percentage of subjects with a PCST value, PCST low values, and PCST high value will be summarized for SBP, DBP, PR, and body weight by treatment group. In the same table, the number and percentage of subjects will be summarized by the following treatment periods as defined in Section 3.2.1.2: Placebo Only, UCB0942 Titration, UCB0942Maintenance, UCB0942 Taper, and On-UCB0942 Overall. Percentages will be relative to the number of subjects with an assessment within each period.
Potentially clinical significant treatment-emergent criteria are based on FDA Division of Neuropharmacologic Drug Products guidelines with some UCB-defined additions.
REDACTEDMCHMCHell; WBell; WB
ical ical ff
COPY ucouc
PYAST=aAST=a=hum=humHCHC
This do
cumen
t alulutabletablpp
cann
ot numbnumb
ue we w
be B0B0 us
ed , anan
ree) wi) wi09494
tond cndsu
pport
peraerarementemen
any rvedved
raturatu
marketi
ng findin
v
autho
rizati
onas
an iman imC=m=meaea
BC=whC=wh
ndindi
appli
catio
n nWBC,WBCca
t
ppspartatpartat
and
Hd an
y y exten
sions
io
te
or ova
riatio
ns
atva
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 38 of 62
10.4.2 ElectrocardiogramsObserved ECG data (ventricular rate, PR, QT, QTcB [QT corrected for heart rate using Bazett’s formula], and QTcF [QT corrected for heart rate using Fridericia’s formula], and QRS) and changes from Baseline will be listed and summarized by treatment group and period. The change from the last pre-UCB0942 administration measurement will be listed and summarized for the placebo group. A separate listing will report the ECG findings. QTcB and QTcF will be calculated for all subjects as below:���� = ����� ��⁄ and ���� = �����/��� , where QT is the QT interval as reported in the ECG
transfer and HR is the heart rate as reported in the ECG transfer.
The number and percentage of subjects with no abnormality, an abnormal but not clinically significant finding, and a clinically significant finding will be summarized by treatment group.The number and percentage of subjects will be summarized by the following treatment periods as defined in Section 3.2.1.2: Placebo Only, UCB0942 Titration, UCB0942 Maintenance, UCB0942 Taper, and On-UCB0942 Overall. Percentages will be relative to the number of subjects with an ECG result at each timepoint. Subjects will be counted at most once within each time point based on the worst observed outcome across all abnormalities at that timepoint.
Summaries of shift from Baseline will also be provided based on the categories normal and abnormal by treatment group. In the same table, the number and percentage of subjects will be summarized by the following treatment periods as defined in Section 3.2.1.2: Placebo Only, UCB0942 Titration, UCB0942 Maintenance, UCB0942 Taper, and On-UCB0942 Overall.
10.4.3 Doppler echocardiographyDoppler echocardiography abnormalities at Baseline and subsequent visits will be listed and summarized by treatment group and period. All available echocardiography data will be reported in the CSR and its addendum.
10.4.4 Physical examinationA listing of abnormal physical examination findings at will be provided; no summaries of physical examination findings are planned.
10.4.5 Columbia-Suicide Severity Rating ScaleAll C-SSRS data obtained at Screening and subsequent visits will be listed for the FAS.
10.4.6 Neurological examinationA listing of abnormal neurological examination findings at will be provided for the FAS; no summaries of neurological examination findings are planned.
10.4.7 Psychiatric and cognition assessment and withdrawal monitoringPsychiatric and cognitive assessments (BPRS and MMSE throughout the study) as well as the changes from Baseline will be listed. The changes from Baseline will be summarized bytreatment group for the FAS.
Any symptoms of withdrawal reactions will be monitored using the CIWA-B questionnaire. TheCIWA-B scores will listed and summarized by treatment group.
REDACTEDa
, UCB, UCB
raphyaphyitiesitiespepe
COPY ed bedhe nume num
as des de
This do
cumen
t 0.40.4PsPs
cann
otg of of mariesaries
4 74 7
be
f abf abus
eda obtob
NeNe
to btabtasu
pport
calcaldings adings
mbia-mbia
any nn
l exal exmark
eting
at Bt Beriodriod. AA
natioati
autho
rizati
onmb
efinedfinedB0942B0942
yyBasBas
appli
catio
nounteuntormalitormal
sed on ed onber aner an
andative ive
tedted
any ng tg
MainMaint
exten
sions
ot clint clin
treatmtreatmtreatre
or G G va
riatio
ns
G
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 39 of 62
10.4.8 Other safety variablesTreatment-emergent abnormal laboratory value criteria suggestive of internal organ involvement or eosinophilia will be listed by the following treatment periods as defined in Section 3.2.1.2: Placebo Only, UCB0942 Titration, UCB0942 Maintenance, UCB0942 Taper, and On-UCB0942 Overall.
11 OTHER ANALYSESThe analyses for blood samples for DNA, mRNA, and lipidomics/proteomics/additional blood biomarkers, and other exploratory variables will be described in a separate DAP.
If there is a high number of missing observations (>15%), due to withdrawals or missing measurements, further post-hoc analyses may be performed, for example for the QOLIE-31-P, and other questionnaires.
REDACTED COPY
This do
cumen
t can
not b
e use
d to s
uppo
rt any
mark
eting
autho
rizati
on ap
plica
tion a
nd an
y exte
nsion
s ssing singQOLIQOLI
or va
riatio
ns
ood ood
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 40 of 62
12 REFERENCESBeyenburg S, Stavem K, Schmidt D. Placebo-corrected efficacy of modern nonenzyme-inducing AEDs for refractory focal epilepsy: systematic review and meta-analysis. Epilepsia. 2012 Mar;53(3):512-20.
Brodie MJ, Barry SJ, Bamagous GA, Norrie JD, Kwan P. Patterns of treatment response in newly diagnosed epilepsy. Neurology. 2012 May;78(20):1548-54.
Busto UE, Sykora K, Sellers EM. A clinical scale to assess benzodiazepine withdrawal. J Clin Psychopharmacol. 1989 Dec;9(6):412-6
Chung S, Ben-Menachem E, Sperling MR, Rosenfeld W, Fountain NB, Benbadis S, Hebert D, Isojärvi J, Doty P. Examining the clinical utility of lacosamide: pooled analyses of three phase II/III clinical trials. CNS Drugs. 2010 Dec;24(12):1041-54.
Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia. 1981:22:489-501.
CPMP/ICH/135/95 Note for guidance on Good Clinical Practice (EMEA) Jul 2002.
Cramer JA, Perrine K, Devinsky O, Bryant-Comstock L, Meador K, Hermann B. Development and cross-cultural translations of a 31-item quality of life in epilepsy inventory. Epilepsia. 1998:39(1):81-8.
Cramer JA, Baker GA, Jacoby A. Development of a new seizure severity questionnaire: Initial reliability and validity testing. Epil Res. 2002:48:187-97.
Cramer JA, Van Hammée G, N132 Study Group. Epilepsy Behav. 2003:4(2):118-23.
Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975 Nov;12(3):189-98.
Kwan P, Arzimanoglou A, Berg AT, Brodie MJ, Allen Hauser W, Mathern G, Moshé SL, Wiebe S, French J. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia. 2010;51(6):1069-77.
Mohanraj R, Brodie MJ. Diagnosing refractory epilepsy: response to sequential treatment schedules. Eur J Neurol. 2006 Mar;13(3):277-82.
Overall JE, Gorham DR. The brief psychiatric rating scale. Psychological Reports 1962:10:799-812
Posner K. 2007. State of the Science: Measurement of Suicidal Adverse Events and The Columbia Suicide Severity Rating Scale. NCDEU: Boca Raton, FL.
Posner K, Melvin GA, Stanley B, Oquendo MA, Gould M. 2007b. Factors in the assessment of suicidality in youth. CNS Spectr; 12:156-162.
Posner K, Oquendo M, Gould M, Stanley B, Davies M. 2007a. Columbia Classification Algorithm of Suicide Assessment (C-CASA): Classification of Suicidal Events in the FDA’s Pediatric Suicidal Risk Analysis of Antidepressants. Am J Psychiatry; 165:1035-1043.
REDACTED ment oment o
2002:42002:
StudyStudy GGyy
RR
COPYLL
of lifeof lif
This do
cumen
tPosnPosnsuisui
cann
otK. 2K. 2umbiaumbia
be us
ed
orhamrhamtoeuroeurosu
pportugug
n on Thon T
MJ. DiMJ. Dll
anyg ATg A
g resig resimark
eting
GrG
R. “MinR. “Mliniciannicia
ATAT
autho
rizati
on
of f a nea ne48:1848:18
rouproup
appli
catio
n e (EM (EM
Meador eadorin epiin ep
and n ofo an
yue Aue Aof epf ep
exten
sions, HebHeb
of threof thre
AgA
or va
riatio
ns
Clin lin
thereo
f.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 41 of 62
Schiller Y, Najjar Y. Quantifying the response to antiepileptic drugs: effect of past treatment history. Neurology. 2008 Jan 1;70(1):54-65.
Steinhoff BJ. Efficacy of perampanel: a review of pooled data. Epilepsia. 2014 Jan;55 Suppl 1:9-12.
REDACTED COPY
This do
cumen
t can
not b
e use
d to s
uppo
rt any
mark
eting
autho
rizati
on ap
plica
tion a
nd an
y exte
nsion
s or v
ariati
ons t
hereo
f.

UC
B03
Jul 2
015
Stat
istic
al A
naly
sis P
lan
UC
B09
42EP
0069
Con
fiden
tial
Page
42
of 6
2
13A
PPEN
DIC
ES
13.1
Trea
tmen
t gro
ups
in T
FL o
utpu
ts
TFL
Gro
upB
y A
rmB
y Pe
riod
Plac
ebo/
UC
B09
42U
CB
0942
/U
CB
0942
All
UC
B09
42
Subj
ects
Plac
ebo
only
UC
B09
42
Titra
tion
UC
B09
42
Mai
nten
ance
UC
B09
42
Tape
rO
n-U
CB
0942
O
vera
llSu
bjec
t di
spos
ition
XX
X
Prot
ocol
D
evia
tions
XX
X
Dem
ogra
phic
sX
XX
Epile
psy
hist
ory
XX
X
Prio
rM
edic
atio
nsX
XX
Con
com
itant
Med
icat
ions
XX
XX
XX
X
Stud
y M
edic
atio
n Ex
posu
re /
Com
plia
nce
XX
XX
XX
X
PKX
XA
EsX
XX
XX
XX
Labs
, Vita
ls,
ECG
, Oth
er
Safe
tyX
XX
PCST
In
cide
nce
XX
XX
XX
X
Effic
acy
XX
XA
E=ad
vers
e ev
ent;
ECG
=ele
ctro
card
iogr
am; P
CST
=pot
entia
lly c
linic
al si
gnifi
cant
trea
tmen
t-em
erge
nt; P
K=p
harm
acok
inet
ics.
REDACTED
XX
ED
DDDDAED
COPY OPC
This do
cumen
t can
not oot
troca
rdro
card
be eus
ed
XX
dto otsu
pport
ort
s
any
anmark
eting
kem
autho
rizati
on
izaho
au
appli
catio
n oncccca
pica
and dan
y ya
exten
sions
on
CB
094
B09
4Ta
peTa
pe xte e
or ova
riatio
ns th
ereof.

UC
B03
Jul 2
015
Stat
istic
al A
naly
sis P
lan
UC
B09
42EP
0069
Con
fiden
tial
Page
43
of 6
2
13.2
PCST
crit
eria
13.2
.1H
emat
olog
y Pa
ram
eter
Con
vent
iona
l Uni
tsSI
Uni
tsC
F
Hem
atoc
rit
For 1
m to
< 6
m: #
25%
For 1
m to
< 6
m:
#02
5%
1Fo
r 6 m
to <
2 y
: #
27%
For 6
m to
< 2
y:
#02
7%Fo
r 2 y
to <
4 y
: #
29%
For 2
y to
< 4
y:
#02
9%Fo
r 4 y
to <
12
y: #
32%
(F); #
35%
(M)
For 4
y to
< 1
2 y:
#
032%
(F); #
035%
(M)
For ∃
12 y
: #
32%
(F); #
37%
(M)
For ∃
12 y
: #
032%
(F); #
037%
(M)
Hem
oglo
bin
For %
6 m
: #
9.7
g/dL
For %
6 m
: #
97 g
/L10
For 6
m to
< 1
2 y:
#10
.0 g
/dL
For 6
m to
< 1
2 y:
#
100
g/L
For ∃
12 y
: #
9.5
g/dL
(F); #
11.5
g/d
L (M
)Fo
r ∃12
y:
#95
g/L
(F); #
115
g/L
(M)
Plat
elet
s#
75 x
109 /L
or ∃
700
x 10
9 /L#
75 x
109 /L
or ∃
700
x 10
9 /LN
/A
WB
CFo
r %17
y:
<3.
0 x
109 /L
or >
20 x
109 /L
; Fo
r %17
y:
<3.
0 x
109 /L
or >
20 x
109 /L
; N
/AFo
r ∃17
y:
<2.
8 x
109 /L
or >
16 x
109 /L
;Fo
r ∃17
y:
<2.
8 x
109 /L
or >
16 x
109 /L
;
RB
CFo
r %17
y:
<2.
5 x
106 /m
m3
For %
17 y
: <
2.5
x 10
12/L
1Fo
r ∃17
y:
<2.
0 x
106 /m
m3 (F
); <
2.5
x 10
6 /mm
3(M
)Fo
r ∃17
y:
<2.
0 x
1012
/L (F
); <
2.5
x 10
12/L
(M)
Eosi
noph
ils∃
10%
or ∃
0.7
x 10
9 /L∃
0.10
or ∃
0.7
x 10
9 /L0.
01 o
r N/A
Neu
troph
ils#
15%
or #
1.0
x 10
9 /L#
0.15
or #
1.0
x 10
9 /L0.
01 o
r N/A
Bas
ophi
ls∃
5% o
r ∃0.
4 x
109 /L
∃0.
05 o
r ∃0.
4 x
109 /L
0.01
or N
/AM
onoc
ytes
∃20
% o
r ∃1.
5 x
109 /L
∃0.
20 o
r ∃1.
5 x
109 /L
0.01
or N
/A
Lym
phoc
ytes
For 1
m to
< 6
m: #
22%
or ∃
80%
For 1
m to
< 6
m:
#0.
22 o
r ∃0.
80
0.01
#2.
1 x
109 /L
or ∃
8.5
x 10
9 /L#
2.1
x 10
9 /L o
r ∃8.
5 x
109 /L
N/A
For 6
m to
< 2
y:
#15
% o
r ∃80
%
For 6
m to
< 2
y:
#0.
15 o
r ∃0.
80
0.01
#1.
5 x
109 /L
or ∃
7.5
x 10
9 /L#
1.5
x 10
9 /L o
r ∃7.
5 x
109 /L
N/A
For 2
y to
< 1
2 y:
#
12%
or ∃
80%
Fo
r 2 y
to <
12
y: #
0.12
or ∃
0.80
0.
01#
1.0
x 10
9 /L o
r ∃7.
5 x
109 /L
#1.
0 x
109 /L
or ∃
7.5
x 10
9 /LN
/AFo
r 12
y to
%17
y: #
10%
or ∃
80%
Fo
r 12
y to
%17
y: #
0.10
or ∃
0.80
0.
01#
0.5
x 10
9 /L o
r ∃5.
5 x
109 /L
#0.
5 x
109 /L
or ∃
5.5
x 10
9 /LN
/AFo
r ∃17
y:
#10
% o
r ∃80
%
For ∃
17 y
: #
0.10
or ∃
0.80
0.
01#
0.5
x 10
9 /L o
r ∃4.
5 x
109 /L
#0.
5 x
109 /L
or ∃
4.5
x 10
9 /LN
/AREDACTED DDDDD
(M)
(M)
ACEDR
COPY
75 x
15
x Y
For
For %% OPY
FoFo
This do
cumen
t can
not tb
e 1##
0.5
0. bus
edoror5
x 10
x 10
99
0%
0%
to /L ∃∃808
supp
ort
∃7.5
x
.5 x
%
%
L
or
or ∃
any
101099 /L/m
arketi
ng
nget
ar
LL
autho
rizati
on17 y7 y
r ∃∃17
17
Fo
r Fo
r %%at
FoFo ho thhhhau
appli
catio
n
##979
2 y:
y:
##
1
/L o
r /L
orpli
y:y:ap
and
2%%03
232%%
77aan
y
%(F
);(F
)
exten
sions
on
ns
or va
riatio
ns th
ereof.

UC
B03
Jul 2
015
Stat
istic
al A
naly
sis P
lan
UC
B09
42EP
0069
Con
fiden
tial
Page
44
of 6
2
13.2
.2B
lood
che
mis
try
Para
met
erC
onve
ntio
nal U
nits
SI U
nits
CF
AST
(SG
OT)
>3
times
of
ULN
>3
times
of
ULN
N/A
ALT
(SG
PT)
>3
times
of
ULN
>3
times
of
ULN
N/A
ALP
For %
17 y
: >
2 tim
es o
f U
LN, i
f nor
mal
rang
ead
just
ed to
the
age
rang
e;
For %
17 y
: >
2 tim
es o
f U
LN, i
f nor
mal
rang
ead
just
ed to
the
age
rang
e;
N/A
For ∃
17 y
: >
3 tim
es o
f U
LNFo
r ∃17
y:>
3 tim
es o
f U
LNG
GT
>3
times
of
ULN
, if b
asel
ine
valu
e <
3 tim
es o
f U
LN>
3 tim
es o
f U
LN, i
f bas
elin
e va
lue
<3
times
of
ULN
N/A
BU
N>
30 m
g/dL
>10
.71
mm
ol/L
0.35
7U
rea
>60
mg/
dL>
10.0
2 m
mol
/L0.
167
Cre
atin
ine
For %
17 y
: >
1.5
mg/
dL;
For %
17 y
: >
132.
6 um
ol/L
; 88
.4Fo
r ∃17
y:
>2.
0 m
g/dL
For ∃
17 y
: >
176.
8 um
ol/L
Cre
atin
ine
clea
ranc
e (c
alc)
For %
12 y
: %
70 m
l/min
(Sch
war
tz)(a
)Fo
r %12
y:
%70
ml/m
in (S
chw
artz
)(a)
N/A
For ∃
12 y
: %
70 m
l/min
(Coc
krof
t)(b)
For ∃
12 y
: %
70 m
l/min
(Coc
krof
t)(b)
Tota
l bili
rubi
n>
2.0
mg/
dL>
34.2
um
ol/L
17.1
Glu
cose
#50
mg/
dL o
r ∃18
0 m
g/dL
#2.
775
mm
ol/L
or ∃
9.99
mm
ol/L
0.05
55
Tota
l Pro
tein
For ∃
1 m
to %
6 m
: #
3.6
g/dL
or ∃
7.8
g/dL
For ∃
1 m
to %
6 m
: #
36 g
/L o
r ∃78
g/L
10Fo
r ∃6
m to
%17
y:
#4.
7 g/
dL o
r ∃9.
5 g/
dLFo
r ∃6
m to
%17
y:
#47
g/L
or ∃
95 g
/LFo
r ∃17
y:
#4.
5 g/
dL o
r ∃9.
0 g/
dLFo
r ∃17
y:
#45
g/L
or ∃
90 g
/L
Alb
umin
For %
17 y
: #
2.4
g/dL
or ∃
6.5
g/dL
For %
17 y
: #
24 g
/L o
r ∃65
g/L
10Fo
r ∃17
y:
#2.
5 g/
dL o
r ∃6.
5 g/
dLFo
r ∃17
y:
#25
g/L
or ∃
65 g
/L
Glo
bulin
For %
17 y
: #
1.2
g/dL
or ∃
5.0
g/dL
For %
17 y
:#
12 g
/L o
r ∃50
g/L
10Fo
r ∃17
y:
#1.
5 g/
dL o
r ∃5.
0 g/
dLFo
r ∃17
y:
#15
g/L
or ∃
50 g
/L
Sodi
umFo
r %17
y:
#12
0 m
Eq/L
or ∃
155
mEq
/LFo
r %17
y:
#12
0 m
mol
/L o
r ∃15
5 m
mol
/L1
For ∃
17 y
: #
115
mEq
/L o
r ∃15
5 m
Eq/L
For ∃
17 y
: #
115
mm
ol/L
or ∃
155
mm
ol/L
Pota
ssiu
mFo
r %17
y:
#3.
0 m
Eq/L
or ∃
6.5
mEq
/LFo
r %17
y:
#3.
0 m
mol
/L o
r ∃6.
5 m
mol
/L1
For ∃
17 y
: #
3.0
mEq
/L o
r ∃5.
8 m
Eq/L
For ∃
17 y
: #
3.0
mm
ol/L
or ∃
5.8
mm
ol/L
Cal
cium
For %
17 y
: #
7 m
g/dL
or ∃
11.5
mg/
dLFo
r %17
y:
#1.
75 m
mol
/L o
r ∃2.
875
mm
ol/L
0.25
For ∃
17 y
: #
7 m
g/dL
or ∃
15.5
mg/
dLFo
r ∃17
y:
#1.
75 m
mol
/L o
r ∃3.
875
mm
ol/L
Uric
Aci
dFo
r < 1
2 y:
∃
8 m
g/dL
For <
12
y:
∃47
5.84
um
ol/L
59.4
8Fo
r ∃12
y:
∃8
mg/
dL (F
); ∃
9.5
mg/
dL (M
)Fo
r ∃12
y:
∃47
5.84
um
ol/L
(F); ∃
565.
06 u
mol
/L (M
)C
hole
ster
ol∃
300
mg/
dL∃
7.77
mm
ol/L
0.02
59H
DL
#25
mg/
dL#
0.65
mm
ol/L
0.02
59LD
L∃
200
mg/
dL∃
5.18
mm
ol/L
0.02
59Tr
igly
cerid
es∃
300
mg/
dL∃
3.42
mm
ol/L
0.01
14a Sc
hwar
tz e
quat
ion
(pat
ient
s <12
): C
r Cl m
l/min
= [H
eigh
t (cm
) * 0
.55]
/ se
rum
cre
atin
ine
b C
ockr
oft e
quat
ion
(pat
ient
s >12
):M
ale:
Cr C
l ml/m
in =
[(14
0-ag
e) x
bod
y w
eigh
t (kg
)] /
(72
x se
rum
cre
atin
ine)
; Fe
mal
e: C
r Cl m
l/min
= [(
140-
age)
x b
ody
wei
ght (
kg)]
/ (7
2 x
seru
m c
reat
inin
e)] x
0.8
5C
F=co
rrec
tion
fact
or.
REDACTED DDDTE
DAR
COPY
.775
m.7
75 Y
For or ∃∃P
Y
For
Fo
This do
cumen
t can
-
nnot C
r C
r2)
:):M
alM
alag
e) x
age)
beCl m
Clbe
be
used
to su
pportm
5.5
mg
5 m
g
po
(F); F); ∃∃
99
any
Eq/L
Eq/L
mg/
dLg/
dLny /d
marketi
ng
ting
LL
ar
autho
rizati
on
m
m
∃∃6
m
6 m
Fo
r Fo
r∃∃11
For
Foriz
hoFhoho ut
appli
catio
n
>
n
%%7070n
%%L
ca
mol
/L o
mol
/Lpl
to
to%ap
and
32.6
u2.
6 u d
176.
876
. aan
y ny aex
tensio
ns
norm
al
norm
al
rang
e;
ange
;
ns
<<3 3
timtim exte
e
or orva
riatio
ns
ari va
thereo
f.

UC
B03
Jul 2
015
Stat
istic
al A
naly
sis P
lan
UC
B09
42EP
0069
Con
fiden
tial
Page
45
of 6
2
13.2
.3U
rinal
ysis
Qua
litat
ive
urin
e pa
ram
eter
s are
gen
eral
ly re
porte
d by
a d
escr
iptiv
e sc
ore,
whi
ch d
iffer
s am
ong
labo
rato
ries.
For d
ata
anal
ysis
pu
rpos
e, a
four
-poi
nt sc
ale
is u
sed.
Fiv
e-po
int,
six-
poin
t, or
seve
n-po
int s
cale
s will
be
colla
psed
into
a fo
ur-p
oint
scal
e fir
st. A
val
ue is
co
nsid
ered
pos
sibl
y cl
inic
ally
sign
ifica
nt tr
eatm
ent-e
mer
gent
abn
orm
al if
an
upw
ard
shift
of a
t lea
st 2
deg
rees
from
the
base
line
occu
rs u
nder
inve
stig
atio
nal t
reat
men
t. To
col
laps
e th
e re
sults
in a
five
-poi
nt sc
ale
into
a fo
ur-p
oint
scal
e, th
e lo
wes
t 2 p
ositi
ve re
sults
w
ill b
e co
mbi
ned
(see
exa
mpl
e be
low
). Fo
r res
ults
repo
rted
with
a sc
ale
of m
ore
than
five
-poi
nt, p
leas
e co
nsul
t you
r stu
dy p
hysi
cian
fo
r how
to c
olla
pse
into
four
-poi
nt sc
ale.
Ori
gina
l Fiv
e-po
int S
cale
Four
-poi
nt S
cale
Neg
ativ
e/N
one
Neg
ativ
e/N
one
Trac
e/R
are/
Mild
/A F
ewTr
ace/
1+/R
are/
Mild
/A F
ew1+ 2+
/Mod
2+/M
od3+
/Sev
3+/S
ev
REDACTED DCOPY
This do
cumen
t can
not b
e use
d to s
uppo
rt any
mark
eting
autho
rizati
on ap
plica
tion a
nd an
y exte
nsion
s
urde
gre
degr
esc
ale
scal
epl
eas
plea
s
or--popo
varia
tions
For
For dd
thereo
f.
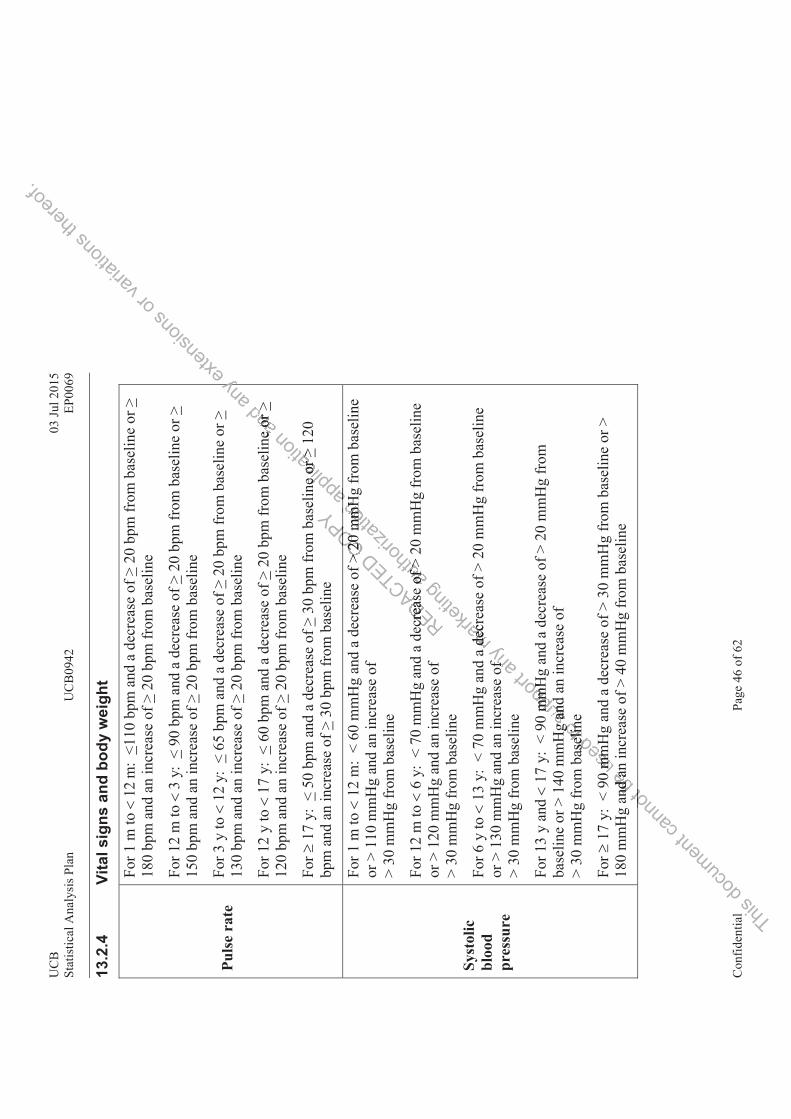
UC
B03
Jul 2
015
Stat
istic
al A
naly
sis P
lan
UC
B09
42EP
0069
Con
fiden
tial
Page
46
of 6
2
13.2
.4Vi
tal s
igns
and
bod
y w
eigh
t
Puls
e ra
te
For 1
m to
%12
m:
<110
bpm
and
a d
ecre
ase
of >
20 b
pm fr
om b
asel
ine
or >
180
bpm
and
an
incr
ease
of >
20 b
pm fr
om b
asel
ine
For 1
2 m
to %
3 y:
<90
bpm
and
a d
ecre
ase
of >
20 b
pm fr
om b
asel
ine
or >
150
bpm
and
an
incr
ease
of >
20 b
pm fr
om b
asel
ine
For 3
y to
%12
y:
<65
bpm
and
a d
ecre
ase
of >
20 b
pm fr
om b
asel
ine
or >
130
bpm
and
an
incr
ease
of >
20 b
pm fr
om b
asel
ine
For 1
2 y
to %
17 y
: <
60 b
pm a
nd a
dec
reas
e of
>20
bpm
from
bas
elin
e or
>12
0 bp
m a
nd a
n in
crea
se o
f >20
bpm
from
bas
elin
e
For ∃
17 y
: <
50 b
pm a
nd a
dec
reas
e of
>30
bpm
from
bas
elin
e or
>12
0 bp
m a
nd a
n in
crea
se o
f >30
bpm
from
bas
elin
e
Syst
olic
bl
ood
pres
sure
For 1
m to
%12
m:
< 60
mm
Hg
and
a de
crea
se o
f > 2
0 m
mH
g fr
om b
asel
ine
or >
110
mm
Hg
and
an in
crea
se o
f >
30 m
mH
g fr
om b
asel
ine
For 1
2 m
to %
6 y:
< 7
0 m
mH
g an
d a
decr
ease
of >
20
mm
Hg
from
bas
elin
e or
> 1
20 m
mH
g an
d an
incr
ease
of
> 30
mm
Hg
from
bas
elin
e
For 6
y to
%13
y:
< 70
mm
Hg
and
a de
crea
se o
f > 2
0 m
mH
g fr
om b
asel
ine
or >
130
mm
Hg
and
an in
crea
se o
f >
30 m
mH
g fr
om b
asel
ine
For 1
3 y
and %
17 y
: <
90 m
mH
g an
d a
decr
ease
of >
20
mm
Hg
from
ba
selin
e or
> 1
40 m
mH
g an
d an
incr
ease
of
> 30
mm
Hg
from
bas
elin
e
For ∃
17 y
: <
90 m
mH
g an
d a
decr
ease
of >
30
mm
Hg
from
bas
elin
e or
>
180
mm
Hg
and
an in
crea
se o
f > 4
0 m
mH
g fr
om b
asel
ine
REDACTED
ecre
ase
crea
s
COPY
> 20
m>
20 OP
This do
cumen
t can
not ot
be
nd a
nnd
a
used
asese
0 m
mm
m
toHgg
elin
elin
supp
ort
0 m
mH
mm
Hg
and
and
any
of f
marketi
ng
a de
cre
dec
autho
rizati
on
mm
Hm
mH
of >of >
appli
catio
n
ne o
r >e
or >
a
and
e or
e
or >>
any yex
tensio
ns or
varia
tions
there
of.
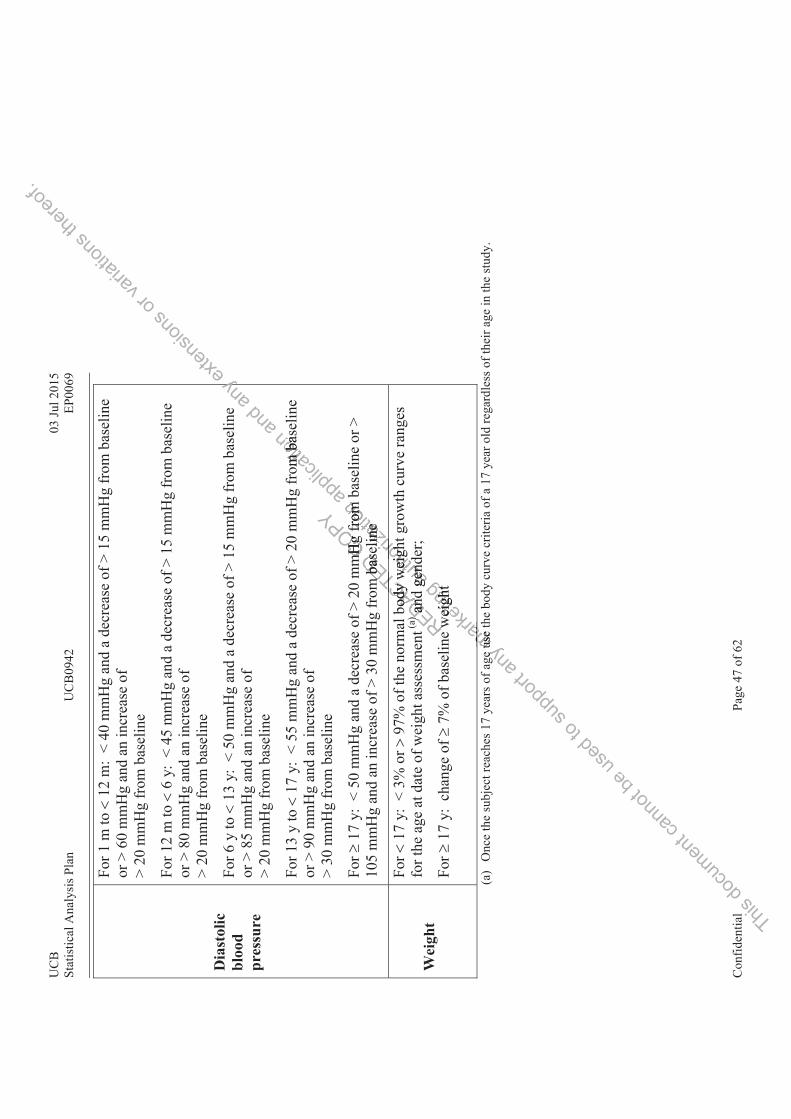
UC
B03
Jul 2
015
Stat
istic
al A
naly
sis P
lan
UC
B09
42EP
0069
Con
fiden
tial
Page
47
of 6
2
Dia
stol
ic
bloo
d pr
essu
re
For 1
m to
%12
m:
< 40
mm
Hg
and
a de
crea
se o
f > 1
5 m
mH
g fr
om b
asel
ine
or >
60
mm
Hg
and
an in
crea
se o
f >
20 m
mH
g fr
om b
asel
ine
For 1
2 m
to %
6 y:
< 4
5 m
mH
g an
d a
decr
ease
of >
15
mm
Hg
from
bas
elin
e or
> 8
0 m
mH
g an
d an
incr
ease
of
> 20
mm
Hg
from
bas
elin
e
For 6
y to
%13
y:
< 50
mm
Hg
and
a de
crea
se o
f > 1
5 m
mH
g fr
om b
asel
ine
or >
85
mm
Hg
and
an in
crea
se o
f >
20 m
mH
g fr
om b
asel
ine
For 1
3 y
to %
17 y
: <
55 m
mH
g an
d a
decr
ease
of >
20
mm
Hg
from
bas
elin
e or
> 9
0 m
mH
g an
d an
incr
ease
of
> 30
mm
Hg
from
bas
elin
e
For ∃
17 y
: <
50 m
mH
g an
d a
decr
ease
of >
20
mm
Hg
from
bas
elin
e or
>
105
mm
Hg
and
an in
crea
se o
f > 3
0 m
mH
g fr
om b
asel
ine
Wei
ght
For %
17 y
: <
3% o
r &97
% o
f the
nor
mal
bod
y w
eigh
t gro
wth
cur
ve ra
nges
fo
r the
age
at d
ate
of w
eigh
t ass
essm
ent(a
)an
d ge
nder
;
For ∃
17 y
: ch
ange
of ∃
7% o
f bas
elin
e w
eigh
t
(a)
Onc
e th
e su
bjec
t rea
ches
17
year
s of a
ge u
se th
e bo
dy c
urve
crit
eria
of a
17
year
old
rega
rdle
ss o
f the
ir ag
e in
the
stud
y.
REDACT
bodyod
yw
yy))
CTED
m b
ase
m b
as
and
and
ew
ew
CTCOPY
mH
g f
mH
g
This do
cumen
t can
not b
e use
d to s
uppo
rt any
ge e
marketi
ng
wei
ght
wei
ght
ma
use
tus
e
autho
r
wei
ghw
eighor
izatio
n
from
fr
omel
ine
elin
e
gend
gend
ori
appli
catio
n
om b
asm
ba
b
and a
ny yex
tensio
ns or
varia
tions
there
of.

UC
B03
Jul 2
015
Stat
istic
al A
naly
sis P
lan
UC
B09
42EP
0069
Con
fiden
tial
Page
48
of 6
2
13.3
QO
LIE-
31-P
tota
l and
sub
scal
e sc
ore
calc
ulat
ions
The
follo
win
g ou
tline
s the
cal
cula
tion
of th
e su
bsca
le sc
ores
for t
he Q
OLI
E 31
P. T
he re
scal
ed re
spon
ses a
re p
rovi
ded
for e
ach
item
. Th
e su
bsca
le sc
ores
are
cal
cula
ted
by su
mm
ing
the
resc
aled
resp
onse
s for
that
subs
cale
and
div
idin
g by
the
num
ber o
f ite
ms w
ith a
no
n-m
issi
ng re
spon
se. N
ote
that
the
divi
sors
show
n as
sum
e th
at a
ll ite
ms f
or e
ach
subs
cale
hav
e a
resp
onse
; the
div
isor
will
diff
er if
th
ere
are
mis
sing
resp
onse
s. A
subs
cale
scor
e w
ill b
e ca
lcul
ated
onl
y if
at le
ast 5
0% o
f the
item
s with
in th
e su
bsca
le a
re p
rese
nt.
REDACTED COPY
This do
cumen
t can
not b
e use
d to s
uppo
rt any
mark
eting
autho
rizati
on ap
plica
tion a
nd an
y exte
nsion
shepo
nse
pons
eth
in th
hin
th
or
e nunu
varia
tions
prov
prov
thereo
f.

UC
B03
Jul 2
015
Stat
istic
al A
naly
sis P
lan
UC
B09
42EP
0069
Con
fiden
tial
Page
49
of 6
2
Res
pons
eFi
nal S
core
Scal
e/It
em N
umbe
rs1
23
45
6Su
btot
al0-
100
poin
t sca
le
Seiz
ure
Wor
ry30
.0
2040
6080
100
____
_31
.0
33.3
66.7
100
––––
____
_32
.0
5010
0––
––__
___
33.
033
.366
.710
0––
––__
___
34.
100
7550
250
––__
___
TOTA
L :
____
_÷
5 =
____
_O
vera
ll Q
ualit
y of
Life
1.M
ultip
ly e
ach
resp
onse
by
10__
___
36.
100
7550
250
––__
___
TOTA
L :
____
_÷
2 =
____
_E
mot
iona
l Wel
l-Bei
ng7.
020
4060
8010
0__
___
8.0
2040
6080
100
____
_9.
100
8060
4020
0__
___
10.
020
4060
8010
0__
___
11.
100
8060
4020
0__
___
TOTA
L :
____
_÷
5 =
____
_E
nerg
y/Fa
tigue
2.10
080
6040
200
____
_3.
100
8060
4020
0__
___
4.0
2040
6080
100
____
_5.
020
4060
8010
0__
___
TOTA
L :
____
_÷
4 =
____
_ C
ogni
tive
Func
tioni
ng19
.0
2040
6080
100
____
_20
.0
33.3
66.7
100
––––
____
_21
.0
2040
6080
100
____
_22
.0
2040
6080
100
____
_23
.0
2040
6080
100
____
_24
.10
075
5025
0––
____
_
TOTA
L :
____
_÷
6 =
____
_
REDACTED
_ __
000 00
TOTO
COPY
__
___
__
This do
cumen
t can
not2020b
e
2020
used
4040 66.7
66.7
to
00
supp
ort an
y 202 8080
marketi
ng
OTATA
L :
L :
0 00
autho
rizati
on
___
_____
_____
___
appli
catio
n
÷ 2
= 2
=
and a
ny ex
tensio
ns or
varia
tions
there
of.
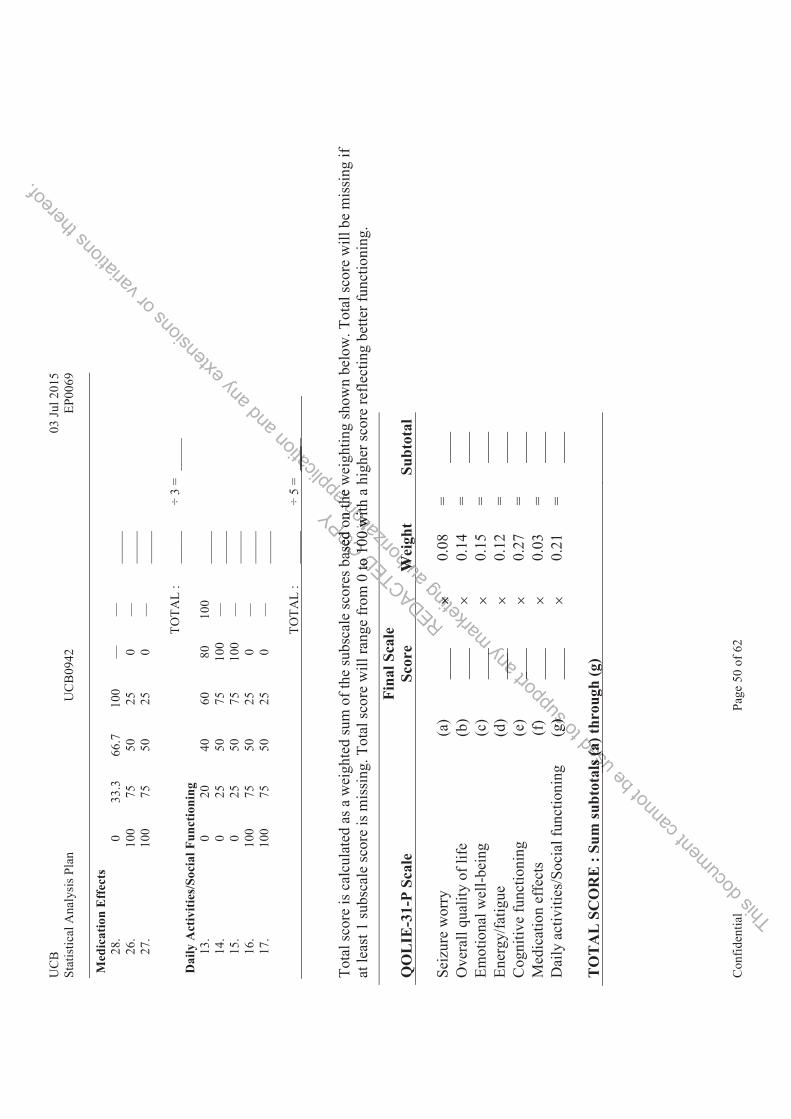
UC
B03
Jul 2
015
Stat
istic
al A
naly
sis P
lan
UC
B09
42EP
0069
Con
fiden
tial
Page
50
of 6
2
Med
icat
ion
Eff
ects
28.
033
.366
.710
0––
––__
___
26.
100
7550
250
––__
___
27.
100
7550
250
––__
___
TO
TAL
:__
___
÷ 3
= __
___
Dai
ly A
ctiv
ities
/Soc
ial F
unct
ioni
ng13
.0
2040
6080
100
____
_14
.0
2550
7510
0––
____
_15
.0
2550
7510
0––
____
_16
.10
075
5025
0––
____
_17
.10
075
5025
0––
____
_
TOTA
L :
____
_÷
5 =
____
_
Tota
l sco
re is
cal
cula
ted
as a
wei
ghte
d su
m o
f the
subs
cale
scor
es b
ased
on
the
wei
ghtin
g sh
own
belo
w. T
otal
scor
e w
ill b
e m
issin
g if
at le
ast 1
subs
cale
scor
e is
mis
sing
. Tot
al sc
ore
will
rang
e fr
om 0
to 1
00 w
ith a
hig
her s
core
refle
ctin
g be
tter f
unct
ioni
ng.
QO
LIE
-31-
P Sc
ale
Fina
l Sca
le
Scor
eW
eigh
tSu
btot
al
Seiz
ure
wor
ry(a
)__
__∋
0.08
=__
__O
vera
ll qu
ality
of l
ife(b
)__
__∋
0.14
=__
__Em
otio
nal w
ell-b
eing
(c)
____
∋0.
15=
____
Ener
gy/fa
tigue
(d)
____
∋0.
12=
____
Cog
nitiv
e fu
nctio
ning
(e)
____
∋0.
27=
____
Med
icat
ion
effe
cts
(f)
____
∋0.
03=
____
Dai
ly a
ctiv
ities
/Soc
ial f
unct
ioni
ng(g
)__
__∋
0.21
=__
__
TO
TA
L S
CO
RE
: Su
m su
btot
als (
a) th
roug
h (g
)
REDACTEDto
to
TTTE
DDDA
COPY
ased
oas
ed o
1010
This do
cumen
t can
not b
e use
d
als (
a)ls
(a)
usto (g
supp
ort ___
g))
any __
____
___
marketi
ng
∋∋
autho
rizati
on
on thn th
00 w
ith0
with
We
We
iza
aaau
appli
catio
n
____
____ at
hew
hew
and a
ny ex
tensio
ns or
varia
tions
there
of.

UC
B03
Jul 2
015
Stat
istic
al A
naly
sis P
lan
UC
B09
42EP
0069
Con
fiden
tial
Page
51
of 6
2
13.4
SSQ
Sco
ring
Alg
orith
mIt
ems
Scor
ing
Alg
orith
mL
abel
A. B
efor
e Se
izur
esA
. Bef
ore
Seiz
ures
1. W
arni
ng
Scor
e =1
a W
arni
ng sc
ore
1a. H
elpf
ul S
core
1-
7 B
. Dur
ing
Seiz
ures
B. D
urin
g Se
izur
es2.
Mov
emen
ts
Scor
e =
2a+2
b÷ 2
or 3
a (m
utua
lly e
xclu
sive
sect
ions
) M
ovem
ent d
urin
g se
izur
es sc
ore
2a. S
ever
e Sc
ore
1-7
2b. B
othe
rsom
e Sc
ore
1-7
3. A
ltere
d C
onsc
ious
ness
Sc
ore
= 2a
+2b÷
2 o
r 3a
(mut
ually
exc
lusi
ve se
ctio
ns)
Alte
red
cons
ciou
snes
s sco
re
3a. B
othe
rsom
e Sc
ore
1-7
C. A
fter
Sei
zure
s C
. Aft
er S
eizu
res
4. R
ecov
er A
fter S
eizu
res
If n
o, C
ompo
nent
C=0
; if y
es,
scor
e q.
5, 6
, 7
Rec
over
y du
ratio
n sc
ore
5. C
ogni
tive
Eff
ects
R
ecov
ery
Cog
nitiv
e= T
otal
5a,
5b
, 5c
÷ 3
Cog
nitiv
e ef
fect
s sco
re
5a. F
requ
ency
Sco
re
1-7
5b. S
ever
e Sc
ore
1-7
5c. B
othe
rsom
e Sc
ore
1-7
6. E
mot
iona
l Eff
ects
R
ecov
ery
Emot
iona
l = T
otal
6a,
6b
, 6c
÷ 3
Emot
iona
l eff
ects
scor
e
6a. F
requ
ency
Sco
re
1-7
6b. S
ever
e Sc
ore
1-7
6c. B
othe
rsom
e Sc
ore
1-7
7. P
hysi
cal E
ffec
ts
Rec
over
y Ph
ysic
al =
Tot
al 7
a,
7b, 7
c ÷
3 Ph
ysic
al e
ffec
ts sc
ore
7a. F
requ
ency
Sco
re
1-7
7b. S
ever
e Sc
ore
1-7
REDACTED D
0; if
y0;
if yT
E
ive=
iv
e= ED
COPY
AA
OPYCOO
This do
cumen
t ntca
nnot no
ca
be us
ed 11 ededededed
u
to -77 77tosu
pport
ery
ery
EmEyy
t
6b6
t
7
sup
any ny a
marketi
ngTota
Tota
kema
autho
rizati
on n
t at at ati at
es,
es,
riz
lla
appli
catio
n tio
red
coed
coica
a
and
ng g a
any
seiz
seiny
exten
sions
s
enex
or ova
riatio
ns th
ereof.
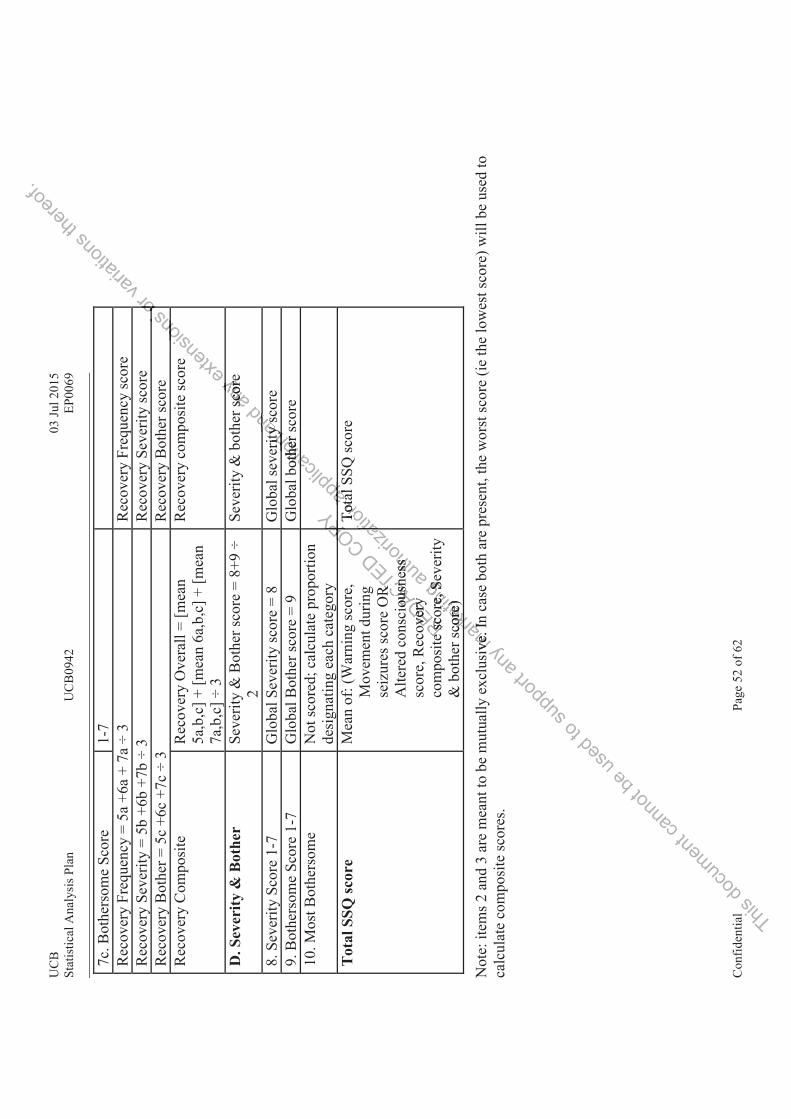
UC
B03
Jul 2
015
Stat
istic
al A
naly
sis P
lan
UC
B09
42EP
0069
Con
fiden
tial
Page
52
of 6
2
7c. B
othe
rsom
e Sc
ore
1-7
Rec
over
y Fr
eque
ncy
= 5a
+6a
+ 7
a ÷
3 R
ecov
ery
Freq
uenc
y sc
ore
Rec
over
y Se
verit
y =
5b +
6b +
7b ÷
3
Rec
over
y Se
verit
y sc
ore
Rec
over
y B
othe
r = 5
c +6
c +7
c ÷
3 R
ecov
ery
Bot
her s
core
Rec
over
y C
ompo
site
R
ecov
ery
Ove
rall
= [m
ean
5a,b
,c] +
[mea
n 6a
,b,c
] + [m
ean
7a,b
,c] ÷
3
Rec
over
y co
mpo
site
scor
e
D. S
ever
ity &
Bot
her
Seve
rity
& B
othe
r sco
re =
8+9
÷
2 Se
verit
y &
bot
her s
core
8. S
ever
ity S
core
1-7
G
loba
l Sev
erity
scor
e =
8 G
loba
l sev
erity
scor
e9.
Bot
hers
ome
Scor
e 1-
7 G
loba
l Bot
her s
core
= 9
G
loba
l bot
her s
core
10. M
ost B
othe
rsom
e N
ot sc
ored
; cal
cula
te p
ropo
rtion
de
sign
atin
g ea
ch c
ateg
ory
Tot
al S
SQ sc
ore
Mea
n of
: (W
arni
ng sc
ore,
M
ovem
ent d
urin
g se
izur
es sc
ore
OR
A
ltere
d co
nsci
ousn
ess
scor
e, R
ecov
ery
com
posi
te sc
ore,
Sev
erity
&
bot
her s
core
)
Tota
l SSQ
scor
e
Not
e: it
ems 2
and
3 a
re m
eant
to b
e m
utua
lly e
xclu
sive
. In
case
bot
h ar
e pr
esen
t, th
e w
orst
scor
e (ie
the
low
est s
core
) will
be
used
to
calc
ulat
e co
mpo
site
scor
es.
REDACTED
R
R
ious
neou
snov
ery
over
ye
sco
e sc
o
COPY OPYOPOPPOP
This do
cumen
t can
not b
e use
d to s
uppo
rt any
mark
eting
ore,
Se
ore,
Sco
re)
core
)
rk
ive.
Ive
. I
autho
rizat
ess ss
ationTo
tTo
t
atap ta
llappli
catio
n ritity
othe
r sot
hern
at
ap
and
ty sysnd
any
scor
esc
oryex
tensio
ns
on
e
or oooova
riatio
ns th
ereof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 53 of 62
13.5 SAP Amendment 1Rationale for the Amendment
The SAP was amended for consistency wit hProtocol Amendment 4 and for clarity.
Modifications and Changes
Change #1
Section 2.2.1.1. Primary Efficacy VariableThe primary outcome measure is the 75% responder rate (75%RR). In the active group this is defined as the proportion of subjects with a 75% or greater reduction in the focal seizure frequency during the last 2 weeks of the Inpatient Period compared to the 2-week Prospective Outpatient Baseline.
Has been changed to
The primary outcome measure is the 75% responder rate (75%RR). In the active group this is defined as the proportion of subjects with a 75% or greater reduction in the focal seizure (IA1, IB, IC) frequency during the last 2 weeks of the Inpatient Period compared to the 2-week Prospective Outpatient Baseline.
Change #2
Section 2.2.1.3 Exploratory Efficacy Variables, 4th bullet
! Changes in average seizure severity as calculated by the percentage of seizures that are type IC for the 2-week Inpatient and Outpatient Maintenance Periods.
Has changed to
! Changes in average seizure severity as calculated by the percentage of all seizures that are type IC for the 2-week Inpatient and Outpatient Maintenance Periods.
Change #3
Section 2.3 Study design and conduct, last paragraphAn echocardiogram is planed to be performed 6 months after the last dose. If not all echocardiographs are completed by the time of the database lock, the database will be unlocked so that the echocardiography data will be included and cleaned. These data will be reported in an addendum.
Has changed to
An echocardiogram is planed to be performed 6 months after the last dose. If not all echocardiographs are completed by the time of the initial database locks, the database will beunlocked so that the echocardiography data will be included and cleaned. These data will be reported in an addendum.
Change #4
Section 3.1 General presentation of summaries and analyses
REDACTED iablesiables
yy as caas cayyOutpaOutpa
COPY
This do
cumen
tAn eAn eechech
cann
ot m.m.
chanchan
beechoch us
ed amm
phs arhs arhocaoca
tom is m is su
pport
designdesign
anyatienatienmark
eting
atientien
verityveritt
autho
rizati
on
s, 4, 4thth bb
alculaalculantnt
appli
catio
n ). In. Inuction uction
eriod criod c
and
In tn t
any e
xtens
ions roup toup t
l seizuseizweek Pweek P
or va
riatio
ns th
ereof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 54 of 62
A glossary of common abbreviations will be provided and will contain abbreviations not footnoted in the tables, figures, and listings.
Was added.
Change #5
Section 3.2.1.2 Study periods, last bullet
! Overall: Whole study duration
Was changed to
! Overall: Whole study duration (start of 1st inpatient week through end of SFU).
Change #6
Section 4.2 Handling of dropouts or missing data
! If the start date is completely unknown, then use the date and time of first dose.
Was changed to
! If the start date is completely unknown and end date is unknown or not prior to first dose, then use the date and time of first dose.
! If the start date is completely unknown and end date is known to be prior to first dose, then set start date equal to end date.
Change #7
Section 4.3 Interim analyses and data monitoring
Was renamed as:4.3.1 Safety Review Group
Change #8
Section 4.3.1 Safety Review GroupThe SRG will remain blinded during the study unless emergent safety information requires unblinding of individual drug allocation for optimal assessment and response to AEs of concern.
Was changed to
The SRG will remain blinded through the first database lock (see Protocol; Section 12.3.3) unless emergent safety information requires unblinding of individual drug allocation for optimal assessment and response to AEs of concern. At the time of the first database lock, the Study Physician(s), clinical pharmacologist, DS representative, biostatistician, and other UCB personnel will be unblinded as to all subjects’ treatment allocation at the beginning of the Inpatient Period.
Change #9
Section 4.3.2 Blinded Interim Analysis
Was added.
Change #10
REDACTED
data mdata m
COPY d dated date
This do
cumen
tpersoersoInpInp
cay nn
ote
ment ment siciansicianonon
bell
ergenergenus
ed
remrem
to su
pport
w Gw linded inded
ual druual dr
any
GroGrmark
eting
autho
rizati
on i
monitoonito
appli
catio
n nown onown
is knos kno
and a
ny
first firstex
tensio
ns or
varia
tions
there
of.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 55 of 62
Section 4.8 Examination of Subgroups
Descriptive analysis will performed for subjects requiring dose reduction from study medication at any point during the study prior to the protocol-defined taper. The following tables will be repeated for these subjects:
! 75%, 50% Responder Rate in Focal Seizure Frequency Summary
! Incidence of TEAEs - Overview
! Incidence of TEAEs
Was added.
Change #11
Section 4.9 End of Study Analyses
Was added.
Change #12
Section 5.2 Protocol DeviationsA listing of all important protocol deviations identified at the database pre-lock meeting will be presented for all subjects in the SS, and will include the deviation type and description. Thenumber and percentage of subjects in the SS with important protocol deviations will besummarized by period and overall if appropriate. The denominator for percentages will be the number of subjects in the SS.
Was changed to
A listing of all important protocol deviations identified at the database pre-lock meeting will be presented for all subjects in the FAS, and will include the deviation type and description. The number and percentage of subjects in the FAS with important protocol deviations will be summarized by period and overall if appropriate. The denominator for percentages will be the number of subjects in the FAS.
Change #13
Section 6.1 DemographicsChildbearing potential and lifestyle will be listed in separate listingsLifestyle information (alcohol, tobacco, caffeinated beverage, and illicit drug use) will be listed and summarized by treatment group and for All Subjects.
Was changed to
Childbearing potential will be listed for the RS.
Lifestyle information (alcohol, tobacco, caffeinated beverage, and illicit drug use) will be listed and summarized by treatment group and for the RS.
Change #14
Section 6.2 Medical history and concomitant diseasesFor this listing, concomitant is defined in Section 6.3 as for concomitant medications.
REDACTEDate. Tate.
eviateviat
COPYthe dthe h impoh impo
ThTh
This do
cumen
t hil
LifeLifca
nnot changhang
ldbedbe
bearizearizeused
tentientirmatiomati
dd
to ratiaia
supp
ort
aphicphic
any all all
S..mark
etingtions ions
anand wid ws in thein thel if aif
autho
rizati
onortanrtan
he dene den
ii
appli
catio
n e datab data
deviatioeviatiant pnt p
and a
ny ex
tensio
ns or
varia
tions
there
of.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 56 of 62
Was added.
Change #15
Section 6.2.1 History of EpilepsyClassification of epileptic syndromeThe number and percentage of subjects with each epileptic syndrome will be summarized for theFAS based on the Classification of Epileptic Syndrome CRF. This summary will include thenumber and percentage of subjects within the following categories: localization-related epilepsy;idiopathic, symptomatic, and cryptogenic localization-related epilepsy; generalized epilepsy;epilepsies undetermined whether focal or generalized including the sub-categories for bothgeneralized and focal seizures and without unequivocal generalized or focal seizures; and situation-related seizures.
Was removed.
Change #16
Section 6.3 Prior and concomitant medicationsThe medications will be classified as AEDs or non-AEDs in the CRF, and will be reviewedduring the DEM. Prior and concomitant non-AED medications will be listed for the SS bytreatment group and by WHODD Anatomical Main Group [Level 1], Therapeutic Subgroup[Level 2], PT and reported term. This listing will be repeated for all AED medications.Any non-coded terms will report Level 1 and Level 2 as UNCODED in the listing.Prior medication definitionIf a subject takes a medication between the Screening date and before the date of study drugadministration, this medication will be classified as ‘prior medication’. With this definition, anymedication recorded that has been taken for at least 1 day and has been stopped before theInpatient Period will be considered as prior.Concomitant medication definitionPrior medication not stopped before the study drug administration date will be classified as‘concomitant medication’. Medication will be labeled as ‘concomitant medication’ when the startdate is between the date (including the date) of study drug administration and the final study visitor, in case of early termination, on the date of the subject’s last visit. With this definition, anymedication that has been taken for at least 1 day during the study period will be considered as
concomitant.
Was changed to
The medications will be classified as AEDs or non-AEDs based on coded terms. The list of coded terms considered AEDs will be finalized prior to database lock and unblinding. Prior and concomitant non-AED medications will be listed for the SS by treatment group and by WHODDAnatomical Main Group [Level 1], Therapeutic Subgroup [Level 2], PT and reported term. This listing will be repeated for all AED medications.
Any non-coded terms will report Level 1 and Level 2 as UNCODED in the listing.
Prior medications include any medications that started prior to the date of first dose of study drug. Concomitant medications are medications taken at least one day in common with the study medication dosing period. Medications may be both prior and concomitant. Past
REDACTEDLevLev
the Sche Sce clase clas
aken aken
COPYGrouGrobe repbe re
velvel
This do
cumen
t oncnAnaAnalili
cann
otdicaticaed termd termcomcom
beged ed
titi
used
d toto
to be su
pportincludnclud
minatioinatieen taeen ta
anyforfor
edicatdicadi
marketi
ngn for a for as prior. prior
nre thre t
autho
rizati
onpeatpeat
2 as U2 as
creeninreeninifiedfied
appli
catio
n e CRF,CRFons wilns wi
up [Lp [Leveatedted
and a
ny ex
tensio
nsr bobo
es; anes; anor
pspsyothoth
varia
tions
lepsyepsysy;y;
thereo
f.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 57 of 62
medications are a subset of prior medications, and include prior medications with a stop date before the date of first study medication administration.
Change #17
Section 6.3.2 Antiepileptic drugs
Since reason for discontinuation is collected as free text field, a medical review will be conducted prior to database lock and unblinding to combine like terms. The combined terms only will be presented in the summary table. Both the reported and combined terms will be listed.
Was added.
Change #18
Section 6.3.2 Antiepileptic drugs
Changes to Concomitant AEDs
All concomitant AEDs will be listed for subjects requiring a dose change to any concomitant AED during the study. A change is defined as any of the following occurring after randomization through the end of the Outpatient Maintenance period:
! Initiation of a new AED
! Termination of an existing AED
! Dose change for an existing AED (increase or decrease)
! Change in frequency of an existing AED
Was added.
Change #19
Section 8.3 Analysis of Exploratory Efficacy VariablesMedian seizure frequency by focal seizure typeAn analysis of covariance (ANCOVA) will be performed on the log-transformed weekly seizurefrequency during the 2-week Inpatient Period. Specifically, ln(1+weekly seizure frequencyduring the 2-week Inpatient Period) will be modeled with treatment group as factor andln(1+weekly seizure frequency during the Baseline Period) as covariate. Contrasts will beestimated to compare UCB0942 to placebo results observed. Transformation of efficacy datacould be envisaged given the data distribution. This analysis will be repeated for all the subtypesof focal seizures (Type IA1, IB, IC).The seizure frequency for the focal seizures (Type IA1+ IB +IC) and focal seizure subtypes(Type IA1, IB, IC) will also be summarized by treatment group and UCB0942 Overall for thefollowing study periods: Baseline, 1st Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week,2-week Inpatient, Outpatient Maintenance Period, and On-UCB0942 Overall.Change in seizure severityThe change in seizure severity is calculated as the change from Baseline in the percentage ofseizures that are type IC out of the total number of focal seizures. It will be listed andsummarized by treatment group for the 2-week Inpatient and Outpatient Maintenance Periods.
REDACTED (increincre
isting sting
COPY
This do
cumen
t(TyTyppyyyfolfol
cann
ot enven
al seizal seie seizuseizu
beo coconvisnvis
used
k InIeizureizureompomp
toe 2
InpaInpasu
pportbby foy f
nce (ANce (A22--weewe
anyratorato
oc
marketi
ng A au
thoriz
ation
ease oease o
AEDAED
appli
catio
nchanchawing owing o
ce perice per
and
angang
any e
xtens
ions o
r vari
ation
s
s be e
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 58 of 62
Seizure severity questionnaireChanges in SSQ will be summarized by treatment group for the Inpatient Period (V3, 4, 5), theOutpatient Period (V10, 15) and for the Tapering and SFU periods (V15, 17, 18, 20) usingsummary statistics.Quality of lifeThe observed values, and changes from Baseline for the QOLIE-31-P total score and thesubscales will be listed for all subjects for visits 3, 10, 12, 15, 17. The prioritization item will belisted separately.The QOLIE-31-P change from Baseline will be summarized by treatment group usingdescriptive statistics for visits 10, 12, 15, 17.The QOLIE-31-P mean change from Baseline for the total score and the sub-scores will bepresented in line plots with 95% CIs for the whole study period.Exploratory analyses for efficacyMedian 28-day seizure frequency by focal seizure type: An analysis of covariance (ANCOVA)will be performed on the log-transformed weekly seizure frequency during the 2-week InpatientPeriod. Specifically, ln(1+weekly seizure frequency during the 2-week Inpatient Period) will bemodeled with treatment group as factor and ln(1+weekly seizure frequency during the BaselinePeriod) as covariate. Contrasts will be estimated to compare UCB0942 to placebo resultsobserved. Transformation of efficacy data could be envisaged given the data distribution. Thisanalysis will be repeated for all the subtypes of focal seizures (Type IA1, IB, IC).The seizure frequency for the focal seizures (Type IA1+ IB +IC) and focal seizure subtypes(Type IA1, IB, IC) will also be summarized by treatment group and UCB0942 Overall for thefollowing study periods: Baseline, 1st Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week, 2-week Inpatient, Outpatient Maintenance Period, and On-UCB0942 Overall.Exploratory analysis will be performed on the seizure count and SSQ data collected during thetapering and SFU periods. The focal seizure frequency will be summarized by treatment groupfor the tapering and SFU periods.The relationship between QOLIE-31-P parameters and efficacy parameters will be evaluatedgraphically. Plots may include, but are not limited to, scatterplots of the QOLIE-31-P subscalesand total score versus the focal seizure reduction at the end of the Outpatient MaintenancePeriod. This plot will be repeated for the 75%RR.All video data recorded in the CRF will be listed.
Was changed to Median seizure frequency by focal seizure type
An analysis of covariance (ANCOVA) will be performed on the log-transformed weekly seizure frequency during the 2-week Inpatient Period. Specifically, ln(1+weekly seizure frequency during the 2-week Inpatient Period) will be modeled with treatment group as factor and ln(1+weekly seizure frequency during the Baseline Period) as covariate. Contrasts will be estimated to compare UCB0942 to placebo results observed. Transformation of efficacy data could be envisaged given the data distribution. This analysis will be repeated for all the subtypes of focal seizures (Type IA1, IB, IC, and disabling [IB+ IC]).
The seizure frequency for the focal seizures (Type IA1+ IB +IC) and focal seizure subtypes (Type IA1, IB, IC, and disabling [IB+ IC]) will also be summarized by treatment group and UCB0942 Overall for the following study periods: Baseline, 1st Inpatient Week, 2nd Inpatient
REDACTED yy tre treyyent Went W
PeriodPeriodd on td on
l seizl seiz
COPYl seizl seie IA1+e IA1
reatmeat
This do
cumen
t (1(1estimestimcoco
cann
otcyy ddng the g the
1+we+we
bes of s of durdur
usede frequfrequse
c
to su
pportepeatpeat
in thein th
any butbu
l seizl seizted
marketi
ngzure fzure f
31-1-P paP put aret ar
autho
rizati
on + II
tment ment Week, 2eek, 2
d, andd, andhe seihe seiff
appli
catio
n freqeqCB094B0942
d givend giveures (Tres (TIB +B +
andek Inpk In
quenquean
y arirng theng thpa
exten
sionswill bwill b
riancanc
or va
riatio
ns
eethe
reof.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 59 of 62
Week, 3rd Inpatient Week, 2-week Inpatient, Outpatient Maintenance Period, and On-UCB0942 Overall.
The mean 28-day adjusted seizure frequency by focal seizure subtype (Type IA1, IB, IC, and disabling [IB+ IC]) will be displayed graphically as stacked bar charts for the following study periods: Baseline, 1st Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week, 2-week Inpatient,Outpatient Maintenance Period, and On-UCB0942 Overall. This will also be presented bysubject.
The mean percent reduction in seizure frequency from baseline to each of the following study periods will be presented as a bar chart: 1st Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week, 2-week Inpatient, Outpatient Maintenance Period, and On-UCB0942 Overall. This will also be presented by subject
Change in seizure severity
Seizure severity is calculated as the percentage of seizures that are type IC out of the total number of focal seizures during a given period. Change from Baseline in seizure severity is the seizure severity in the period of interest minus the seizure severity during the 2-week prospective baseline period. Seizure severity and its change from baseline will be listed and summarized by treatment group for the 2-week Inpatient and Outpatient Maintenance Periods. For subjects not experiencing IC seizures during the observed period, severity is considered to be 0%.
Seizure severity questionnaire
Changes in SSQ will be summarized by treatment group for the Inpatient Period (V3, 4, 5), the Outpatient Period (V10, 15) and for the Tapering and SFU periods (V15, 17, 18, 20) using summary statistics. Mean change from baseline in SSQ total and subscores will be presented graphically.
The SSQ total score (TS) is derived using the algorithm in Appendix x.
Quality of life
The observed values, and changes from Baseline for the QOLIE-31-P total score and the subscales will be listed for all subjects for visits 3, 10, 12, 15, 17. The prioritization item will be listed separately.
The QOLIE-31-P change from Baseline will be summarized by treatment group usingdescriptive statistics for visits 10, 12, 15, 17.
The QOLIE-31-P mean change from Baseline for the total score and the sub-scores will be presented in line plots with 95% Hodges-Lehmann CIs for the whole study period.
Exploratory analyses for efficacy
Median 28-day seizure frequency by focal seizure type: An analysis of covariance (ANCOVA) will be performed on the log-transformed weekly seizure frequency during the 2-week Inpatient Period. Specifically, ln(1+weekly seizure frequency during the 2-week Inpatient Period) will be modeled with treatment group as factor and ln(1+weekly seizure frequency during the Baseline Period) as covariate. Contrasts will be estimated to compare UCB0942 to placebo results observed. Transformation of efficacy data could be envisaged given the data distribution. This
REDACTED atmentatment
TaperinTaperim basem base
COPY, sev, sev
This do
cumen
tMedMedwiwi
cann
oted ind in
loratooratoca
beE-3131n lin l
usedisticsstics
11 PP
tohanhansupp
orthana
or all sr all s
ge
any
nges nges mark
eting
using tusing
autho
rizati
on
t grougrouing anng an
eline iline i
appli
catio
n du
will be ill beintenanntena
eritity is y is
ande in e in
urinurinan
yCC outousei
exten
sionspa
. Th Toratientien
varia
tions
udyudy
thereo
f.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 60 of 62
analysis will be repeated for all the subtypes of focal seizures (Type IA1, IB, IC, and disabling [IB+ IC]).
The seizure frequency for the focal seizures (Type IA1+ IB +IC) and focal seizure subtypes (Type IA1, IB, IC, and disabling [IB+ IC]) will also be summarized by treatment group and UCB0942 Overall for the following study periods: Baseline, 1st Inpatient Week, 2nd Inpatient Week, 3rd Inpatient Week, 2-week Inpatient, Outpatient Maintenance Period, and On-UCB0942 Overall.
Exploratory analysis will be performed on the seizure count and SSQ data collected during the tapering and SFU periods. The focal seizure frequency will be summarized by treatment group for the tapering and SFU periods.
The relationship between QOLIE-31-P parameters and efficacy parameters will be evaluated graphically. Plots may include, but are not limited to, scatterplots of the QOLIE-31-P subscales and total score versus the focal seizure reduction at the end of the Outpatient Maintenance Period. This plot will be repeated for the 75%RR.
All video data recorded in the CRF will be listed.
Change #20
Section 10.2 Adverse EventsAdverse events will be recorded from the time informed consent is granted until studycompletion or study termination. All AEs will be coded using the latest available version of MedDRA and will be categorized by intensity (mild/moderate/severe).
Has changed to
Adverse events will be recorded from the time informed consent is granted until study completion or study termination (end of the SFU period). All AEs will be coded using the latest available version of MedDRA and will be categorized by intensity (mild/moderate/severe).
Change #21
REDACTEDl be cl be sitity (my (m
m thm th
COPY nformeforme
co
This do
cumen
t can
not b
e use
d to s
uppo
rt any
mark
etinghe timhe tim
d of theof thd will bwill
autho
rizati
oned coed coded uoded u
mild/mmild/m
appli
catio
n
on
and a
nyent Ment Mexte
nsion
s nt
be evbe evLIEIE-3-3
MM
org
grogrva
riatio
ns
g the the
thereo
f.
UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 61 of 62
Section 10.4.2 Electrocardiograms
Formulas for QTcB and QTcF have been added.
Change #22
Section 10.4.3 Dopper EchocardiographyDoppler echocardiography results at Baseline and subsequent visits, and changes from baselinewill be listed and summarized by treatment group and period. All available echocardiography
data will be reported in the CSR and its addendum.
Has changed to
Doppler echocardiography abnormalities at Baseline and subsequent visits will be listed and summarized by treatment group and period. All available echocardiography data will be reported in the CSR and its addendum.
Change #23
Appendix 13.4 SSQ Scoring Algorithm
Has been added.
REDACTED COPY
This do
cumen
t can
not b
e use
d to s
uppo
rt any
mark
eting
autho
rizati
on ap
plica
tion a
nd an
y exte
nsion
s be listee liste
data wata w
or va
riatio
ns
y
thereo
f.

UCB 03 Jul 2015 Statistical Analysis Plan UCB0942 EP0069
Confidential Page 62 of 62
STATISTICAL ANALYSIS PLAN SIGNATURE PAGEThis document has been reviewed and approved per the Review and Approval of Clinical Documents Standard Operating Procedures. Signatures indicate that the final version of the Statistical Analysis Plan (SAP) or amended SAP is released for execution.
REDACTED COPY
This do
cumen
t can
not b
e use
d to s
uppo
rt any
mark
eting
autho
rizati
on ap
plica
tion a
nd an
y exte
nsion
s or v
ariati
ons t
hereo
f.
ELECTRONIC SIGNATURES
Signed by Meaning of Signature Server Approval Date
(dd-mon-yyyy(HH:mm))
REDACTED COPY
This do
cumen
t can
not b
e use
d to s
uppo
rt any
mark
eting
autho
rizati
on ap
plica
tionnn aa
nnd
ana
yan
y erveay ex
tensio
ns or
varia
tions
there
of.





























