Embed Size (px)
Citation preview
Stated Preference Methods
Research in Health Care
Decision Making
A Critical Review of Its Use in the
European Regulatory Environment.
Kevin Marsh, Evidera
Axel Mühlbacher, Hochschule Neubrandenburg
Janine van Til, University of Twente
7 November 2017
Objectives
▪ To map which stated preference methods are being used
in the European regulatory environment
• “A more systematic consideration of preferences as part of
regulatory decisions”
• Identification, weighting and aggregation of decision criteria
▪Outline, conclusion:• Identification of gaps in the use of preference methods
• Implications of existing experience for the use of stated preference
methods
• A research agenda for the development of stated preference
methods
• Limitations with the approach adopted in this research
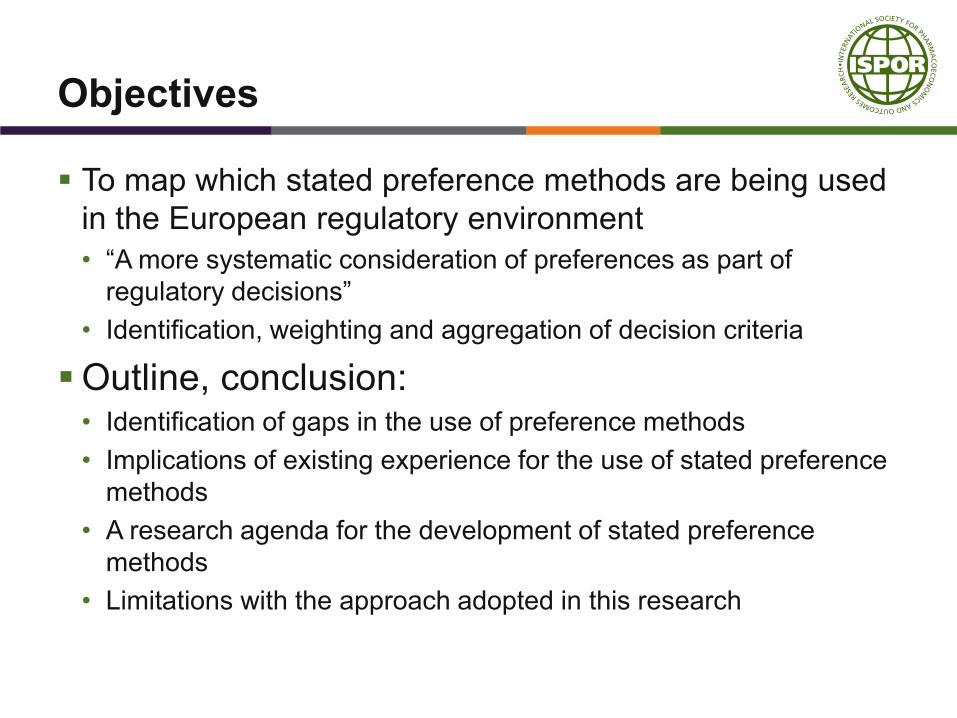
Overview of the Review
Do
ne
alr
ead
y
Cu
rren
t
tas
k
Problem: Literature and website reviews revealed little information on stated preference methods
used
Purpose of survey: Identification of stated preference methods used by the institutions involved in
HTA
INTRODUCTION
TBD
▪ SIG WG objectives
– Definition of preference methods
▪ Process / findings to date
▪ Next steps
▪ Introduce the workshop
CASE STUDY 1
CEA VS MCDA
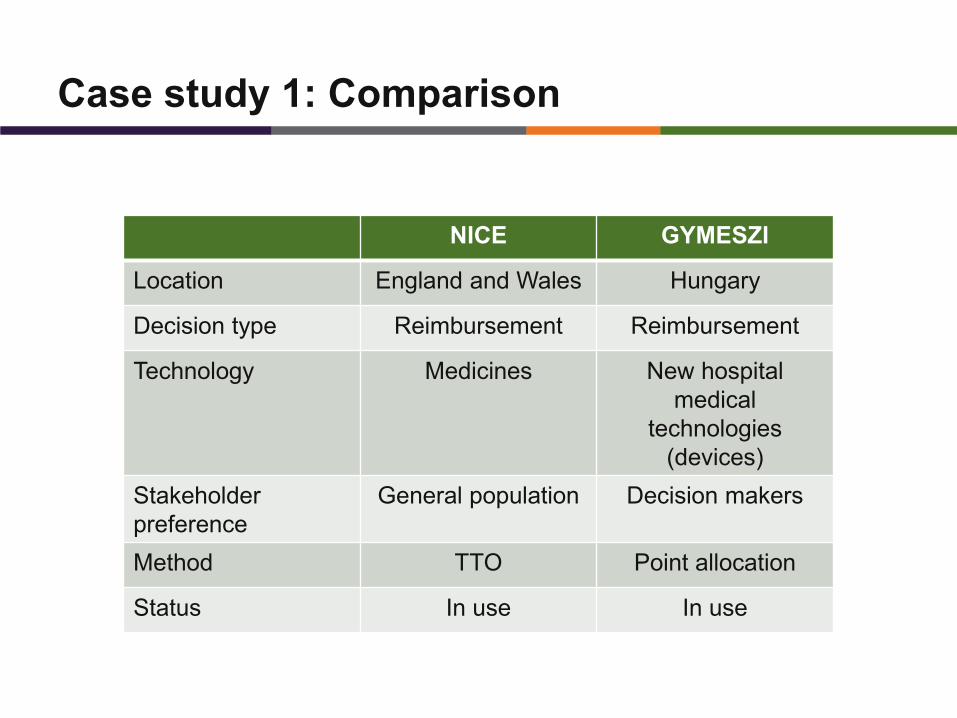
Case study 1: Comparison
NICE GYMESZI
Location England and Wales Hungary
Decision type Reimbursement Reimbursement
Technology Medicines New hospital
medical
technologies
(devices)
Stakeholder
preference
General population Decision makers
Method TTO Point allocation
Status In use In use
Case study 1: NICE
8
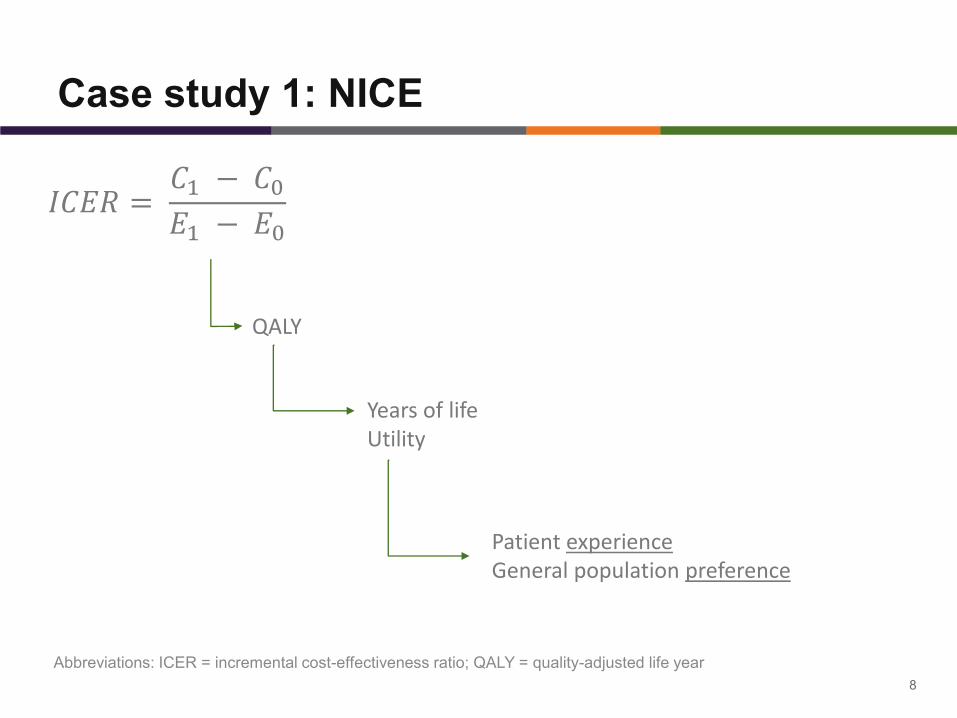
𝐼𝐶𝐸𝑅 =𝐶1 − 𝐶0𝐸1 − 𝐸0
QALY
Years of lifeUtility
Patient experienceGeneral population preference
Abbreviations: ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life year
Case study 1: NICE
9
Abbreviations: ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life year
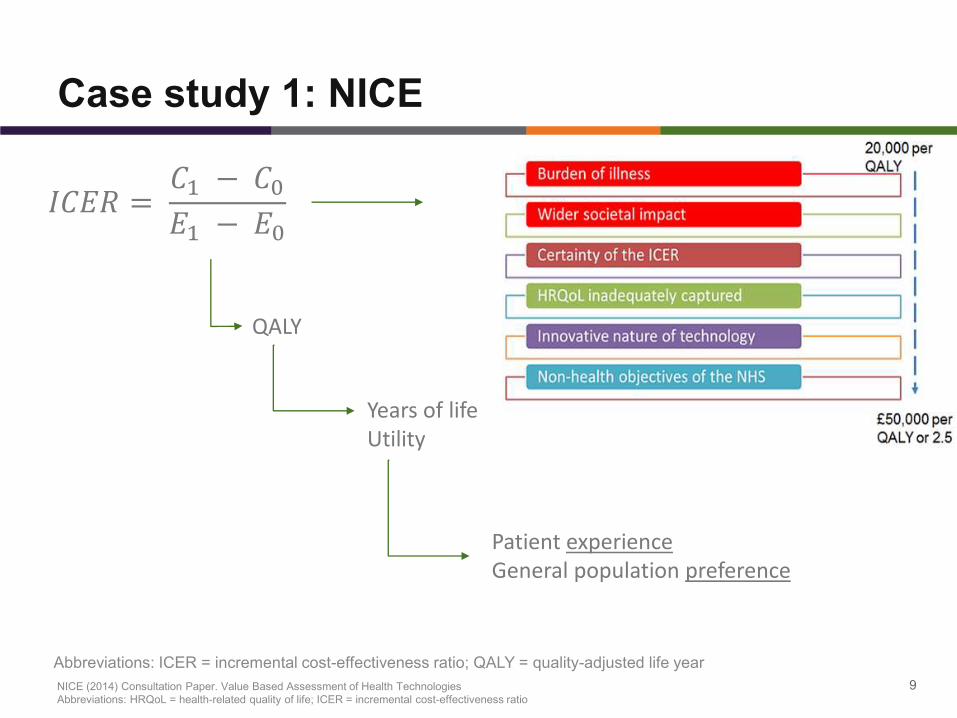
𝐼𝐶𝐸𝑅 =𝐶1 − 𝐶0𝐸1 − 𝐸0
QALY
Years of lifeUtility
Patient experienceGeneral population preference
NICE (2014) Consultation Paper. Value Based Assessment of Health Technologies
Abbreviations: HRQoL = health-related quality of life; ICER = incremental cost-effectiveness ratio
Case study 1: GYMESZI
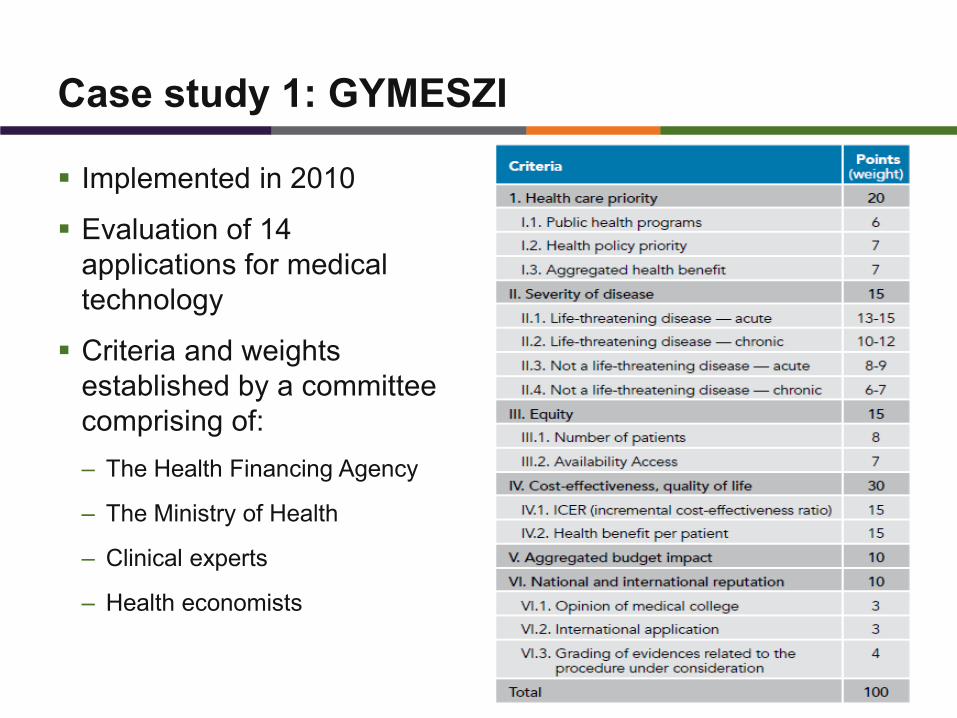
▪ Implemented in 2010
▪ Evaluation of 14
applications for medical
technology
▪ Criteria and weights
established by a committee
comprising of:
– The Health Financing Agency
– The Ministry of Health
– Clinical experts
– Health economists
10
Case study 1: Assessment
11
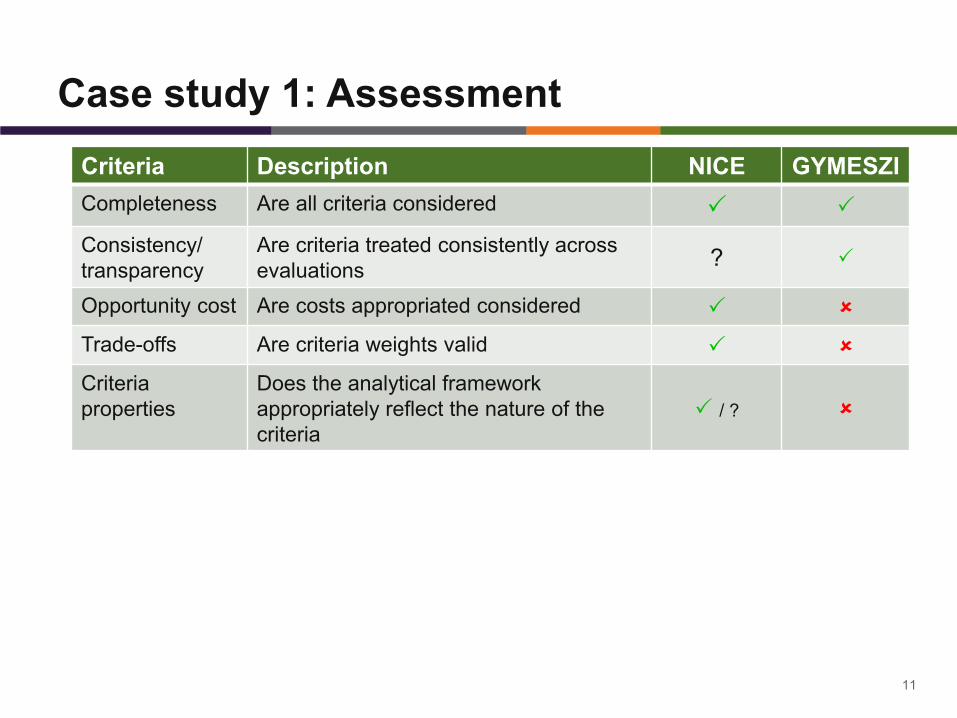
Criteria Description NICE GYMESZI
Completeness Are all criteria considered
Consistency/
transparency
Are criteria treated consistently across
evaluations?
Opportunity cost Are costs appropriated considered
Trade-offs Are criteria weights valid
Criteria
properties
Does the analytical framework
appropriately reflect the nature of the
criteria
/ ?
Case study 1: Poll
▪ Which of the two examples do you think is the appropriate way
to incorporate preferences into reimbursement decisions
– NICE
– GYMESZI
– NEITHER
12
CASE STUDY 2
IQWIG’S PILOTS: DCE VS AHP
German pilot – DCE Hepatitis C
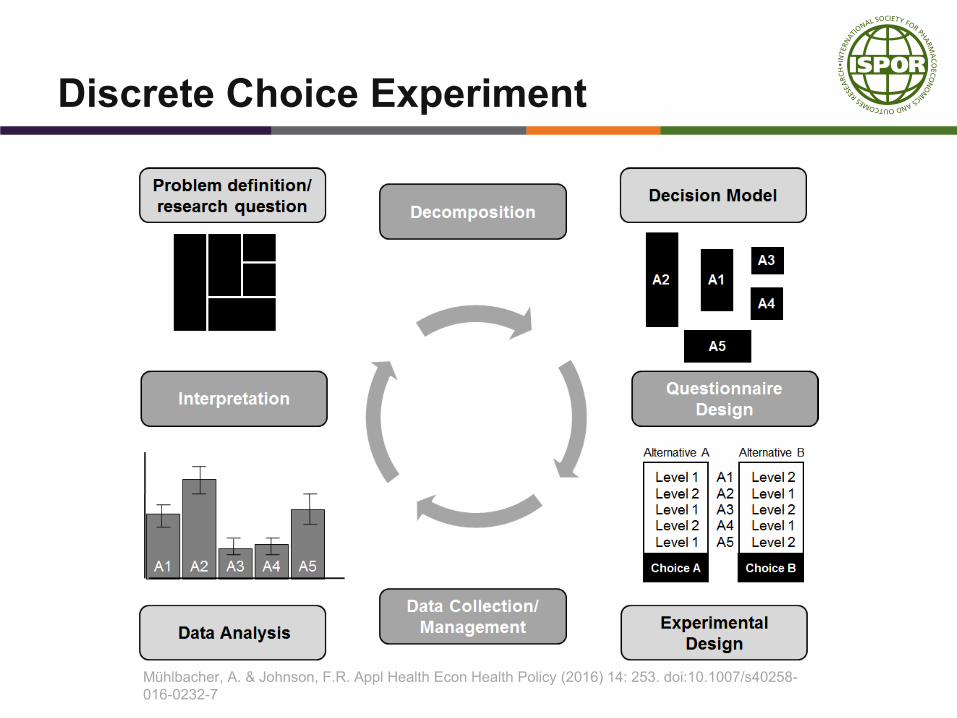
Discrete Choice Experiment
Mühlbacher, A. & Johnson, F.R. Appl Health Econ Health Policy (2016) 14: 253. doi:10.1007/s40258-
016-0232-7
German pilot – DCE Hepatitis C
▪ Objectives:• The pilot’s aim was to investigate to what extent a DCE can be
used as a method for the identification, weighting and prioritization in the case of multiple endpoints
▪ Method:• DCE including 7 attributes of antiviral treatment of hepatitis C:
• Treatment efficacy (Probability of sustained viral response 6 months after end of therapy)
• Adverse events (Duration of flu-like symptoms after injection, Probability of gastro-intestinal symptoms, Probability of psychiatric symptoms, Probability of skin symptoms and/or alopecia)
• Treatment burden (Duration of antiviral therapy, Frequency of interferon injections)
• 2 Subsamples: Patient and expert respondents
German pilot – DCE Hepatitis C
▪ Conclusion:
• For patients it was shown that it was feasible to weight patient-
relevant outcomes via a DCE
• In the comparison of patient preferences and opinions of
healthcare professionals, the sequence was the same for 4 of the 7
attributes; however, the magnitude of the weighting deviated for
further attributes.
• DCE method can be applied to other questions
German pilot – AHP Depression
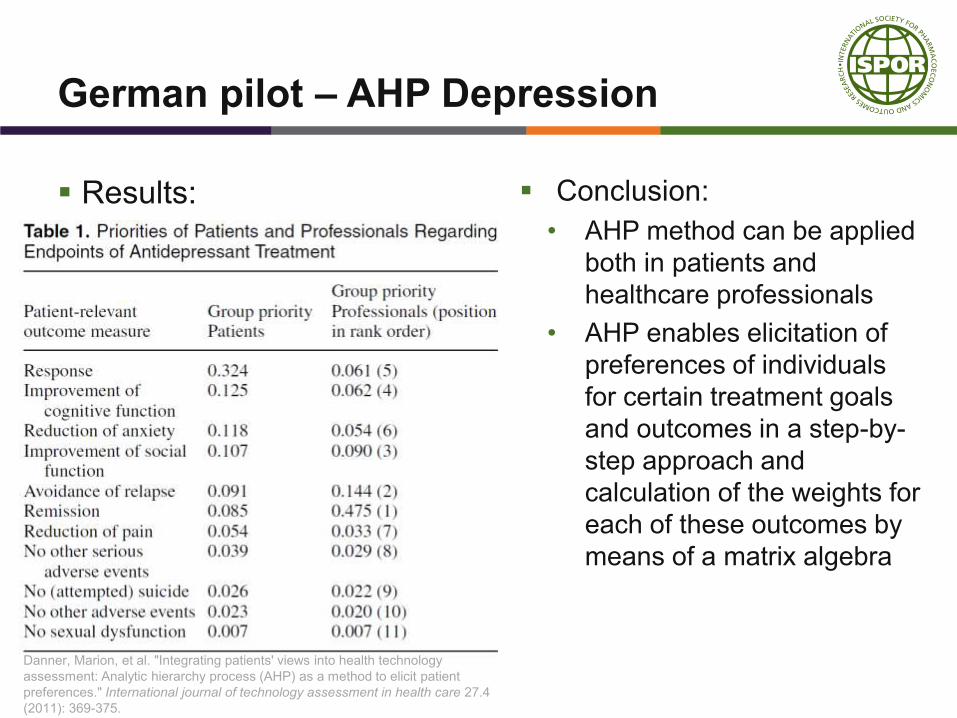
German pilot – AHP Depression
▪ Objectives:
• This pilot project’s goal was to examine to what extent the AHP
method can be applied in health economic evaluations in Germany
in the identification, weighting, and prioritization of multiple patient-
relevant outcomes.
▪ Method:
• AHP evaluating 11 endpoints of antidepressant treatment
• 2 Subsamples: Patient and expert respondents
• Response
• Remission
• Cognitive function
• Reduction of anxiety
• Social function
• Avoidance of relapse
• Reduction of pain
• Other serious adverse events
• (Attempted) Suicide
• Other adverse events
• Sexual dysfunction
German pilot – AHP Depression
▪ Results: ▪ Conclusion:
• AHP method can be applied
both in patients and
healthcare professionals
• AHP enables elicitation of
preferences of individuals
for certain treatment goals
and outcomes in a step-by-
step approach and
calculation of the weights for
each of these outcomes by
means of a matrix algebra
Danner, Marion, et al. "Integrating patients' views into health technology
assessment: Analytic hierarchy process (AHP) as a method to elicit patient
preferences." International journal of technology assessment in health care 27.4
(2011): 369-375.
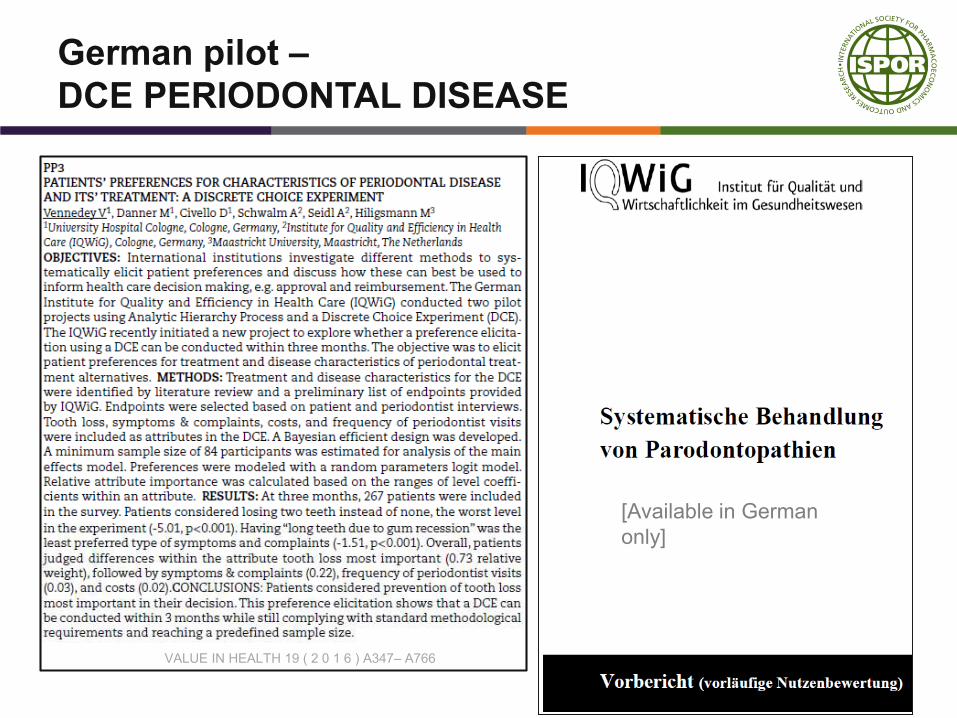
German pilot –
DCE PERIODONTAL DISEASE
VALUE IN HEALTH 19 ( 2 0 1 6 ) A347– A766
[Available in German
only]
German pilot –
DCE PERIODONTAL DISEASE
▪Objective:
• The pilot’s aim was to explore whether a preference
elicitation using a DCE can be conducted within 3
months
▪ Method:
• DCE including 4 attributes of treatment and disease characteristics
of periodontal treatment alternative
• Tooth loss
• Symptoms & complaints
• Frequency of periodontist visits
• Cost
• Patient respondents
German pilot –
DCE PERIODONTAL DISEASE
▪Results:• Relative importance of attributes
• Tooth loss (0.73 relative weight)
• Symptoms & complaints (0.22)
• Frequency of periodontist visits (0.03)
• Costs (0.02)
▪ Conclusion:
• DCE is feasible within 3 months
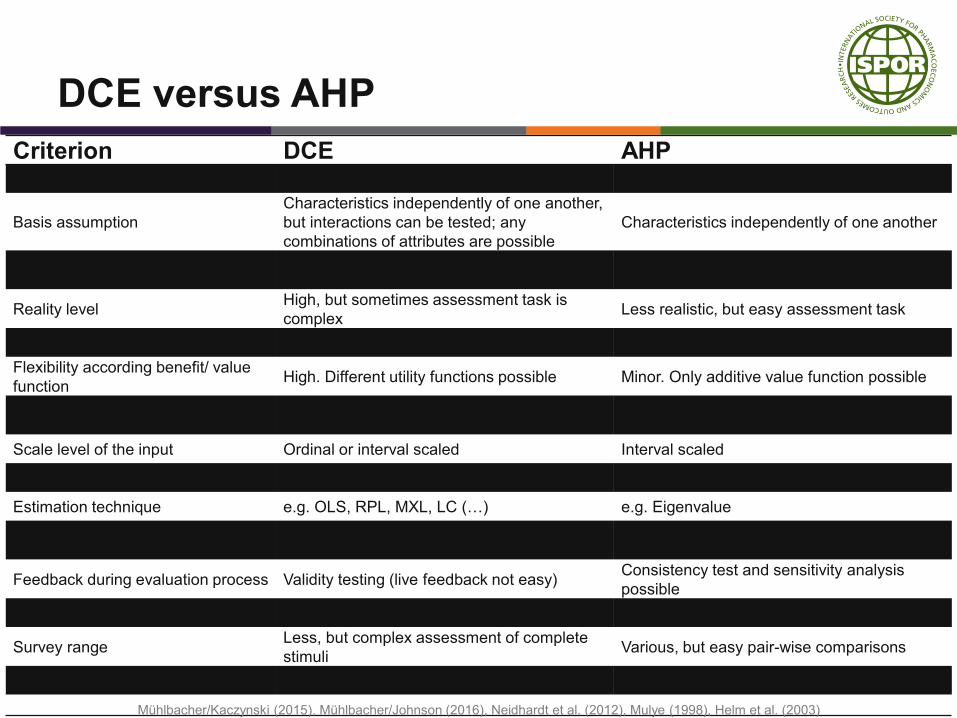
DCE versus AHP
Criterion DCE AHPMethodological approach Decompositional Compositional
Basis assumption
Characteristics independently of one another,
but interactions can be tested; any
combinations of attributes are possible
Characteristics independently of one another
Evaluation process Holistic evaluation of stimuliPair-wise comparisons of alternatives and
decision criteria
Reality levelHigh, but sometimes assessment task is
complexLess realistic, but easy assessment task
Benefit/ value model Additive part worth model Weighted additive model
Flexibility according benefit/ value
functionHigh. Different utility functions possible Minor. Only additive value function possible
Target object/ respondentsMarket segment on the basis of individual
customerSingle decision-maker or group
Scale level of the input Ordinal or interval scaled Interval scaled
Scale level of the output Interval scaled Ratio scaled
Estimation technique e.g. OLS, RPL, MXL, LC (…) e.g. Eigenvalue
Interpretation of importance weights Part worth value of attribute (utility scale)Relative importance of one criteria for target
achievement (no utility scale)
Feedback during evaluation process Validity testing (live feedback not easy)Consistency test and sensitivity analysis
possible
Cognitive stress for respondents High. Grows with the increasing of attributes Minor
Survey rangeLess, but complex assessment of complete
stimuliVarious, but easy pair-wise comparisons
Restrictions on use Up to six attributes with 2-4 levels Various attributes possible
Mühlbacher/Kaczynski (2015), Mühlbacher/Johnson (2016), Neidhardt et al. (2012), Mulye (1998), Helm et al. (2003)
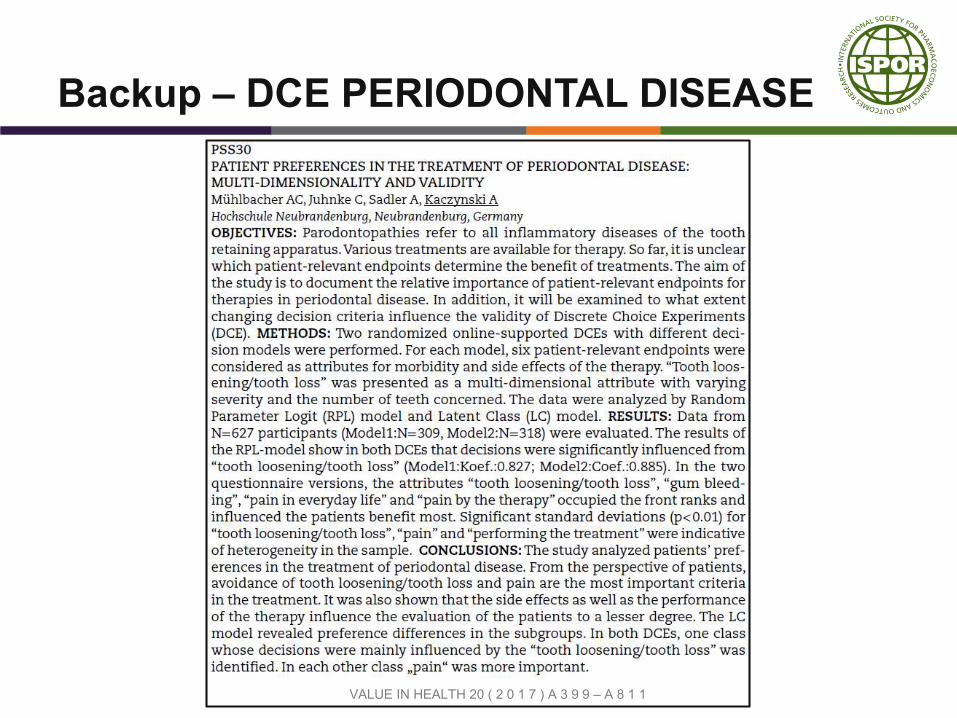
Backup – DCE PERIODONTAL DISEASE
VALUE IN HEALTH 20 ( 2 0 1 7 ) A 3 9 9 – A 8 1 1
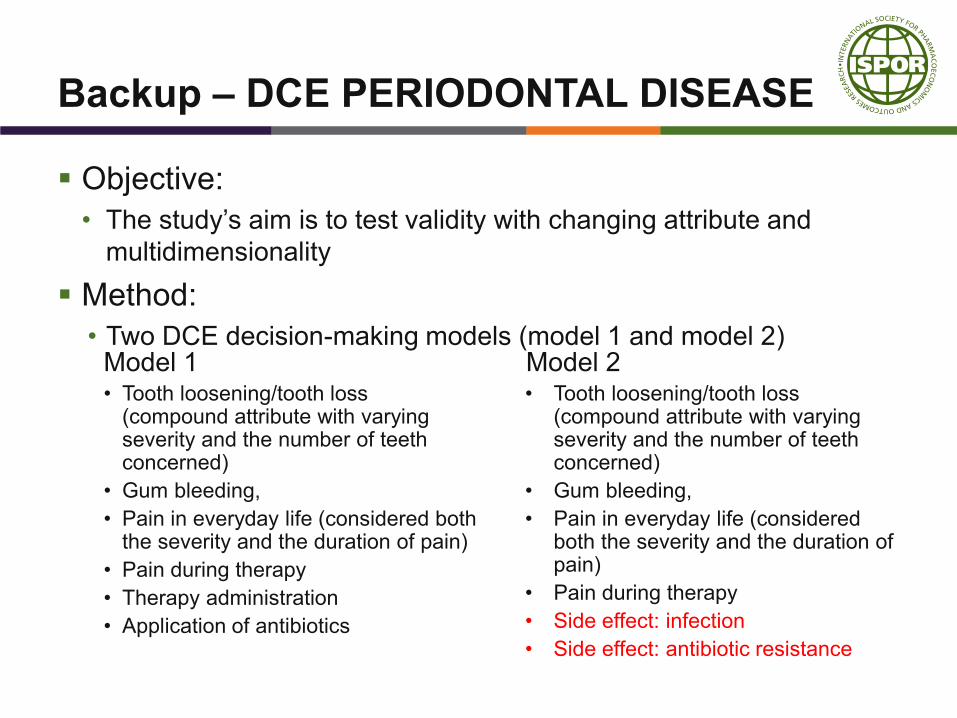
Backup – DCE PERIODONTAL DISEASE
▪ Objective:
• The study’s aim is to test validity with changing attribute and
multidimensionality
▪ Method:
• Two DCE decision-making models (model 1 and model 2)Model 1• Tooth loosening/tooth loss
(compound attribute with varying severity and the number of teeth concerned)
• Gum bleeding,
• Pain in everyday life (considered both the severity and the duration of pain)
• Pain during therapy
• Therapy administration
• Application of antibiotics
Model 2• Tooth loosening/tooth loss
(compound attribute with varying severity and the number of teeth concerned)
• Gum bleeding,
• Pain in everyday life (considered both the severity and the duration of pain)
• Pain during therapy
• Side effect: infection
• Side effect: antibiotic resistance
Backup – DCE PERIODONTAL DISEASE
▪ Results – Model 1Random parameter logit model (95% confidence interval) (model 1,
N=300)
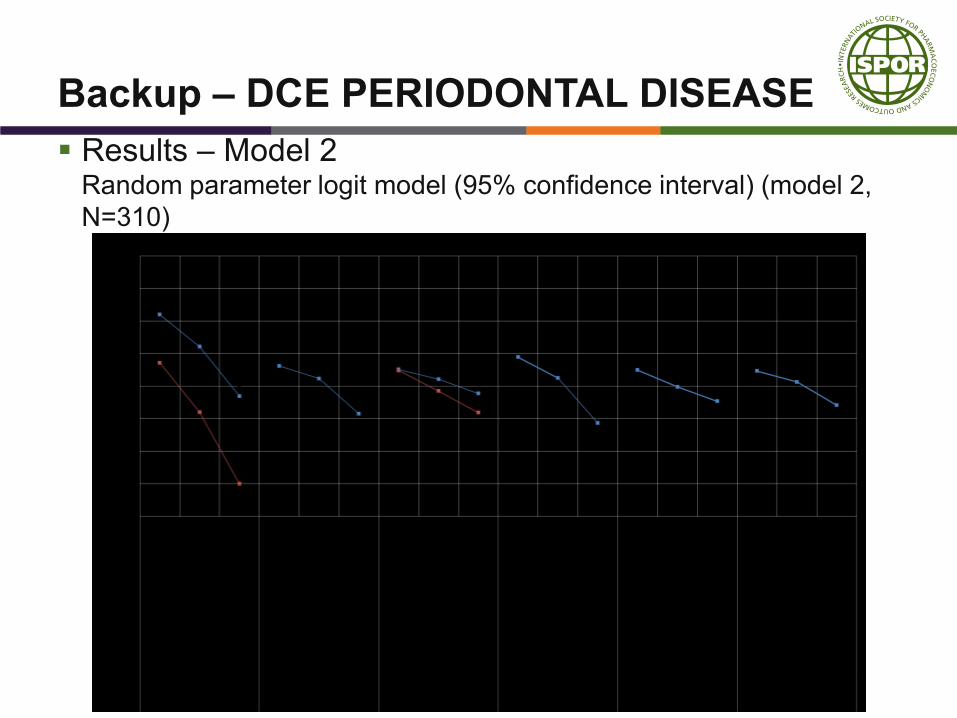
Backup – DCE PERIODONTAL DISEASE
▪ Results – Model 2Random parameter logit model (95% confidence interval) (model 2,
N=310)
CASE STUDY 3
EMA’S PILOTS: SWING
WEIGHTING WORKSHOPS VS
PATIENT SURVEYS
Articles:
▪ Incorporating Patient Preferences Into Drug Development and
Regulatory Decision Making: Results From a Quantitative Pilot
Study With Cancer Patients, Carers, and Regulators –
Postmus et al., 2017
▪ Is quantitative benefit–risk modelling of drugs desirable or
possible? – Phillips et al., 2011
Is quantitative benefit–risk modelling of drugs
desirable or possible? - Phillips et al., 2011
▪ Objective: To determine whether quantitative benefit-risk
modelling is possible
▪ Method: MCDA with the expected utility rule
▪ Case study: Weight Loss Drug
▪ Value Tree: one favourable effect and five unfavourable effects
▪ Value Functions: concave value function, provided by an
expert roleplaying an assessor
▪ Weight Elicitation: Swing Weighting
Quantitative Pilot Study With Cancer Patients,
Carers, and Regulators - Postmus et al., 2017
▪ Objectives: To explore the feasibility of a lean method for
eliciting individual patient preferences
▪ Method: MCDA
▪ Case study: Treatment of Melanoma
▪ Value Tree: one favourable effect and two unfavourable effects
▪ Value Functions: linear value function, assumption by team
▪ Weight Elicitation: Swing Weighting – Ordinal Judgements
MCDA - Swing Weighting
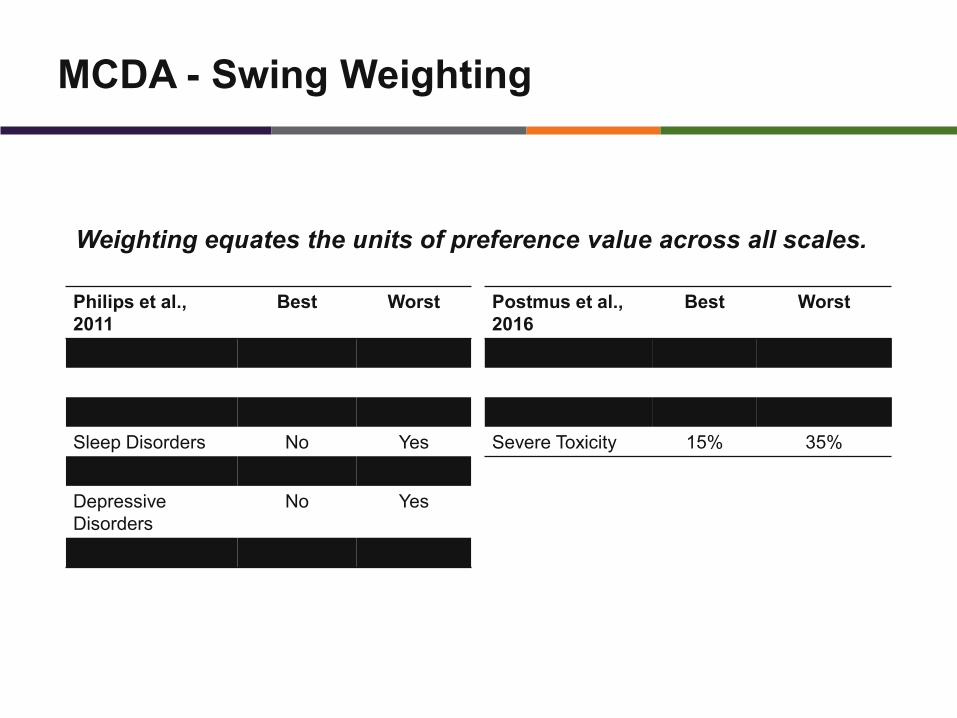
Weighting equates the units of preference value across all scales.
Philips et al.,
2011
Best Worst
Weight Loss 15% 0%
Anxiety No Yes
Sleep Disorders No Yes
Mood Alterations No Yes
Depressive
Disorders
No Yes
Irritability No Yes
Postmus et al.,
2016
Best Worst
Overall Survival 65% 45%
Moderate Toxicity 5% 20%
Severe Toxicity 15% 35%
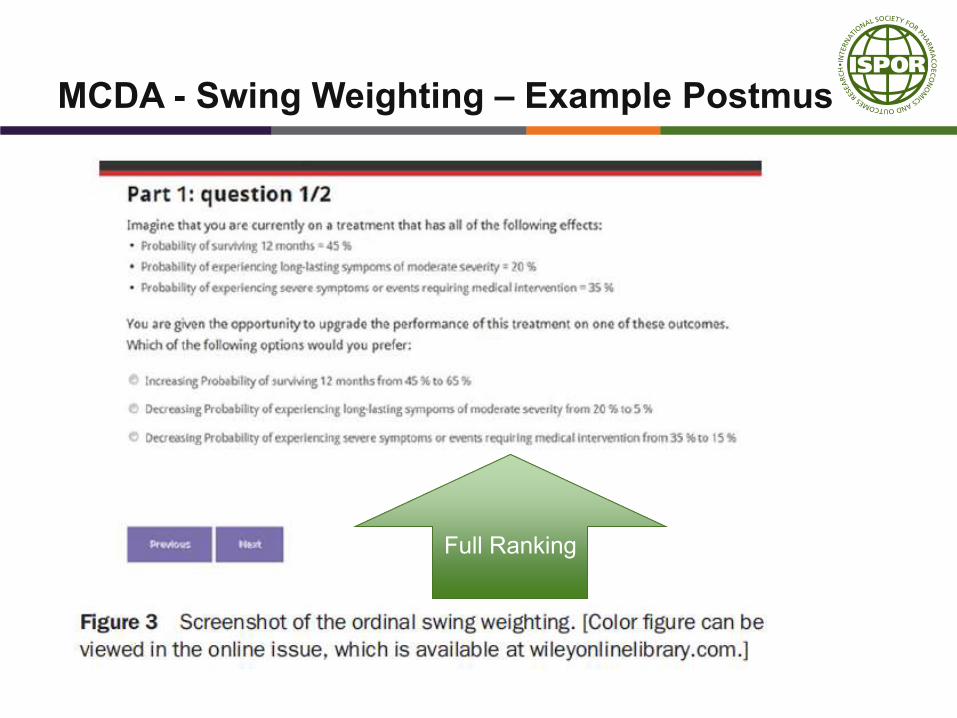
MCDA - Swing Weighting – Example Postmus
Full RankingFull Ranking
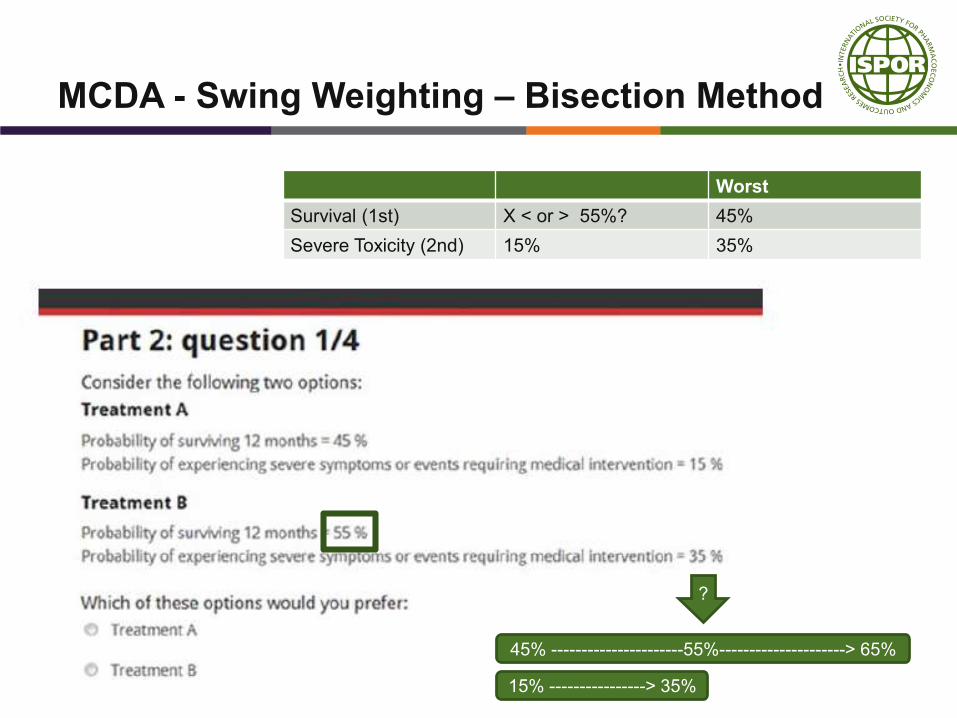
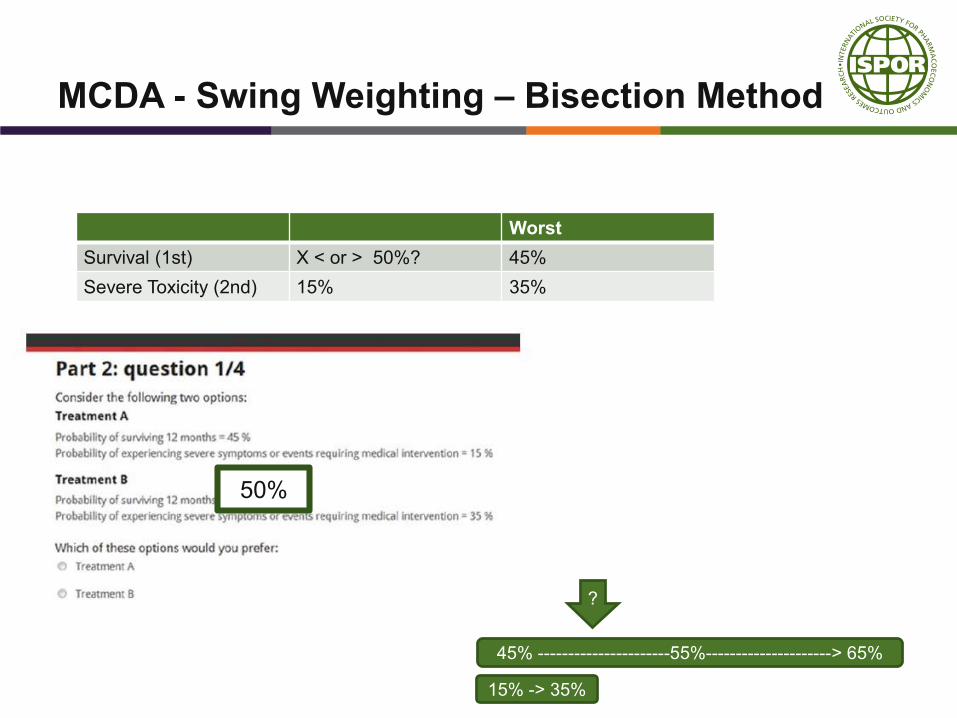
MCDA - Swing Weighting – Bisection Method
Worst
Survival (1st) X < or > 55%? 45%
Severe Toxicity (2nd) 15% 35%
45% ----------------------55%---------------------> 65%
15% ----------------> 35%
?
MCDA - Swing Weighting – Bisection Method
Worst
Survival (1st) X < or > 50%? 45%
Severe Toxicity (2nd) 15% 35%
45% ----------------------55%---------------------> 65%
15% -> 35%
?
50%
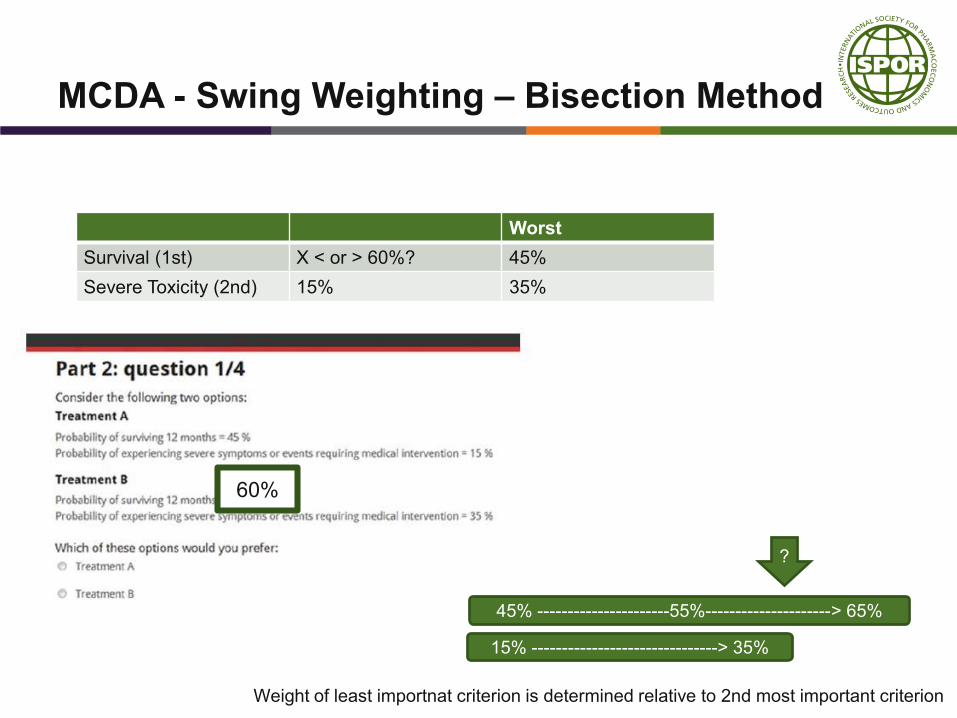
MCDA - Swing Weighting – Bisection Method
Worst
Survival (1st) X < or > 60%? 45%
Severe Toxicity (2nd) 15% 35%
45% ----------------------55%---------------------> 65%
15% -------------------------------> 35%
?
60%
Weight of least importnat criterion is determined relative to 2nd most important criterion
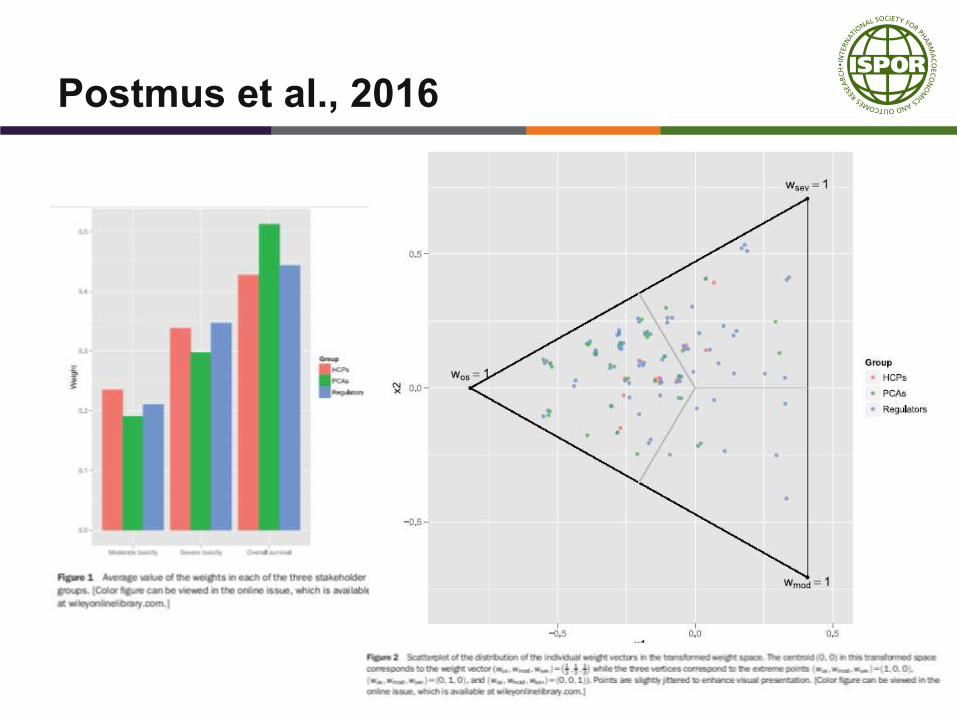
Postmus et al., 2016
Is quantitative benefit–risk modelling of drugs
desirable or possible? - Phillips et al., 2011
▪ Method: MCDA with the expected utility rule
▪ Case study: Weight Loss Drug
▪ Value Tree: one favourable effect and five unfavourable effects
▪ Value Functions: concave value function, provided by an
expert roleplaying an assessor
▪ Weight Elicitation: Swing Weighting – Relative Judgements
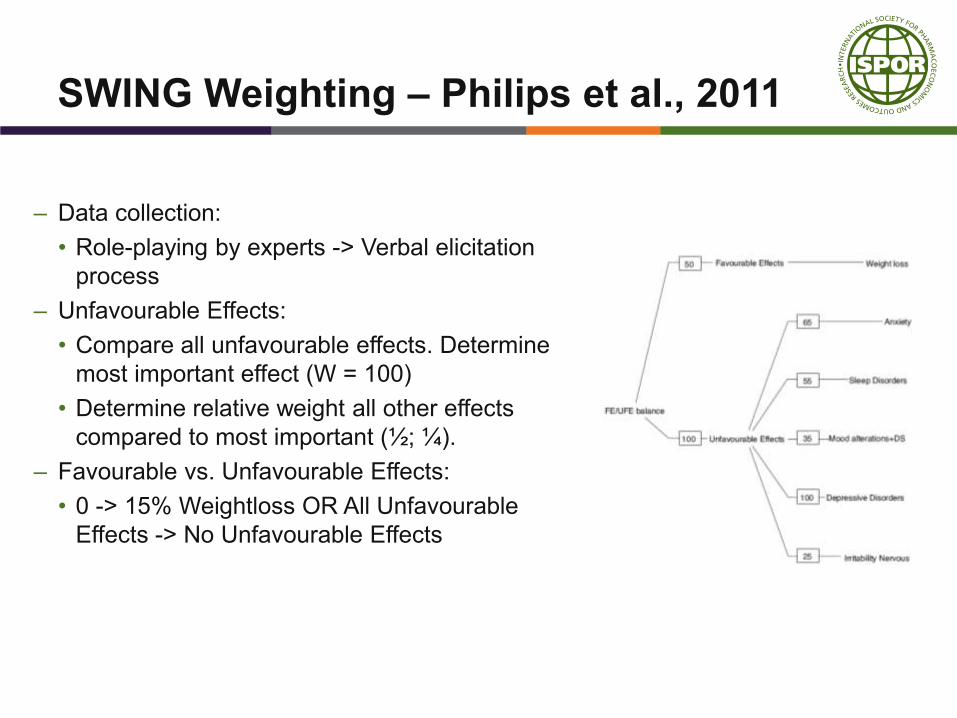
SWING Weighting – Philips et al., 2011
– Data collection:
• Role-playing by experts -> Verbal elicitation
process
– Unfavourable Effects:
• Compare all unfavourable effects. Determine
most important effect (W = 100)
• Determine relative weight all other effects
compared to most important (½; ¼).
– Favourable vs. Unfavourable Effects:
• 0 -> 15% Weightloss OR All Unfavourable
Effects -> No Unfavourable Effects
Benefits of SWING weighting - Philips
▪ Swing weighting results in explicit assessment of assessors
judgements, which could increase transparancy and
consistency
▪ Swing weighing can accommodate any kind of data
▪ Using pre-defined scales (and global estimates of weight
ranges) allows weights to be assigned to all scales even
before data about the options are considered
Benefits of SWING weighting - Postmus
▪ Bisection swing weighting was considered intuitive by patients
▪ Regulators felt that outcomes where useful to identify
subgroups of patients
▪ Recommendation to combine with face-to-face meetings with
patients to understand preference constructions and context
▪ Regulators felt that outcomes where easy to interpret, time
frame of elicitation process was feasible
49
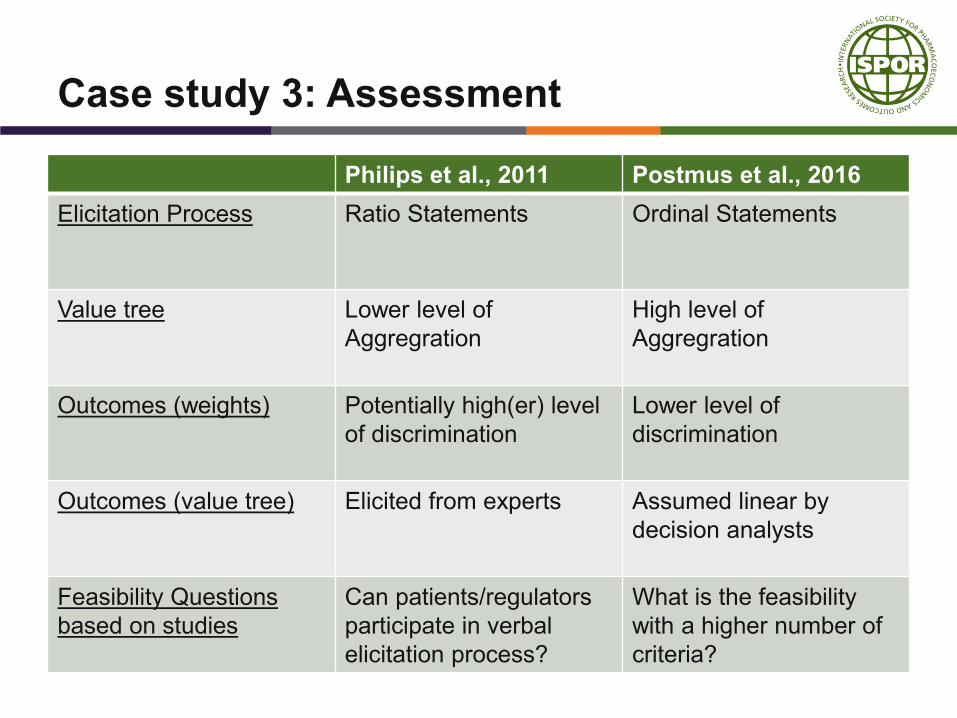
Case study 3: Assessment
Philips et al., 2011 Postmus et al., 2016
Elicitation Process Ratio Statements Ordinal Statements
Value tree Lower level of
Aggregration
High level of
Aggregration
Outcomes (weights) Potentially high(er) level
of discrimination
Lower level of
discrimination
Outcomes (value tree) Elicited from experts Assumed linear by
decision analysts
Feasibility Questions
based on studies
Can patients/regulators
participate in verbal
elicitation process?
What is the feasibility
with a higher number of
criteria?

CONCLUSION
TBD
▪ Pull together the themes emerging from the case studies