Embed Size (px)
Citation preview
O C T O B E R 2 0 0 7
State Perspectives onEmerging MedicaidLong-Term CarePolicies and Practices
National Association of State Medicaid Directors
An Affiliate of the American Public Human Services Association
361185_Lot1_Cover_1 11/7/07 2:38 PM Page 1
State Perspectives on Emerging Medicaid
Long-Term Care Policies and Practices
361185_Lot1_Text_i 11/7/07 5:39 PM Page i
© 2007 National Association of State Medicaid Directors. All rights reserved.an affiliate of the American Public Human Services Association
361185_Lot1_Text_ii 11/7/07 5:39 PM Page ii
iii
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
Acknowledgements ............................................................................................................v
Executive Summary ..........................................................................................................vii
Introduction: The Deficit Reduction Act and Medicaid Long-Term Care Services ..........1
Finding 1: Eligibility for Medicaid was Tightened Under the DRA and States Responded ................................................................................3
Finding 2: Most States Have not used the Family Opportunity Act to Extend Medicaid Coverage to Children with Disabilities in Families with Higher Incomes..............................................................11
Finding 3: States Use Their Money Follows the Person Grant Dollars in Several Ways ............................................................................11
Finding 4: To Date, Most States are not Opting to Switch to theNew HCBS State Plan Amendment (SPA) Option ..................................13
Finding 5: States are Initiating Efforts to Transition Individuals Out of Institutions ..................................................................................14
Finding 6: States are Using Managed Care for Individuals with Disabilities ..............14
Finding 7: Fewer than 10 States Plan to Submit a SPA for Personal Care Services (Cash and Counseling) Programs ......................................15
Finding 8: Special Needs Plans are in Place in at Least 20 States, but States Have Concerns about Coordination between Medicare and Medicaid ............................................................................18
Finding 9: Long-Term Care Reform in the States Continues to Encourage Home- and Community-Based Living................................21
Finding 10: States are Using Care Coordination to Improve and Integrate Care ........22
Finding 11: More States Using Disease Management to Help Manage Chronic Conditions ....................................................................24
Finding 12: Many States are Using the New Option on Long-Term Care Partnership Programs ..............................................................................26
Finding 13: Benchmark Benefit Packages are not Widely Used for Long-Term Care Services ..................................................................28
Conclusion: Policy and Practice Outlook ....................................................................31
Glossary ............................................................................................................................33
Table of Contents
361185_Lot1_Text_iii 11/7/07 5:39 PM Page iii

iv
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Tables and Figures
Figure 1: State Changes to Apply Partial Months of Ineligibility for IndividualsApplying for Medical Assistance for their LTC Costs..................................4
Figure 2: State Changes to Accumulate Multiple Transfers in More than One Month and Impose a Single Period of Ineligibility into One Period ..........5
Figure 3: State Changes Regarding the Purchase of Promissory Notes, Loans, and Mortgages................................................................................6
Figure 4: State Changes Regarding the Purchase of Life Estates Requiring that the Individual Purchasing the Life Estate in Another’s Home to Reside there for at Least One Year ........................................................7
Figure 5: State Home Equity Limits..........................................................................9
Figure 6: State Personal Care Services and the Option to Hire/Fire Consumer Directed Aides ................................................................16
Figure 7: States Offering Consumer Directed Services within 1916(c) Waivers for the MR/DD Population ....................................................................17
Figure 8: States with Special Needs Plans Enrolling Dual Eligibles ..........................20
Figure 9: States with a Care Coordination Model ..................................................23
Figure 10: States with a Disease Management Program ............................................25
Figure 11: State Long-Term Care Partnership Program Progress ..............................27
Appendices
Appendix A: State Citations on DRA Implementation..................................................39
Appendix B: Section 6086: Home- and Community-Based Services ............................45
Appendix C: Section 6087: Self-Directed Personal Assistance Services (PAS) and “Cash and Counseling” ....................................................................49
361185_Lot1_Text_iv 11/7/07 5:39 PM Page iv
v
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
T his survey represents an addition to a series ofprojects by the National Association of StateMedicaid Directors (NASMD). This Long-
Term Care survey, the second in our collection, pro-vides us with a better understanding of Long-TermCare initiatives at the state and federal levels.
We would like to thank the more than 50 stateofficials who completed this comprehensive surveyand responded to our follow-up questions. We recog-nize that this survey required a great deal of coordi-nation among state Medicaid agencies and we appre-ciate all of the effort. We are extremely grateful to themembers of the NASMD and Centers for Medicareand Medicaid Services Eligibility and Long-TermCare Technical Advisory Groups (TAG) for assistingus in the development of the survey instrument andin gathering the results. Chronic Care and EligibilityTAG member guidance was invaluable in the devel-opment of the publication.
Chronic Care TAG Eligibility TAGAnn Kohler Marybeth McCafffreyCarol Stekel Kathy HenryDoug Porter Stan RosensteinDeanna Hartwig Linda SkinnerTonya Keller Jacky StokesEllie Shea-Delaney Karen GibsonCynthia Bowling Jones Barbara BarnesPam Parker Elena JosephickCharles Wilhelm Jim JonesSam Waldrep Gretel FeltonJason Wolcott Joanne Terlizzi
The NASMD Executive Committee provided essen-tial leadership on this important project. Ilana Cohenserved as the senior staff member on this project andwas ably assisted by Lynn Scully with the support ofRobyn Bockweg, and Jacqueline Richardson. LarryGoolsby provided his editorial insights. NASMDplans to update this survey annually.
With appreciation,
Martha A. RohertyDirectorNational Association of State Medicaid Directorsan affiliate of the American Public Human Services Association
Acknowledgements
361185_Lot1_Text_v 11/7/07 5:39 PM Page v

361185_Lot1_Text_vi 11/7/07 5:39 PM Page vi
vii
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
O ver the last decade, there has been a signifi-cant shift in distributing Medicaid Long-Term Care (LTC) funding towards home-
and community-based services (HCBS) and awayfrom institutional settings. During this time, stateshave increased their support for Long-Term Careservices in individuals’ homes and in other communi-ty-based settings such as adult day care and assistedliving facilities as an alternative to nursing homes andother institutions. For many vulnerable elderly andnonelderly individuals with physical, developmental,or cognitive disabilities, these alternative settings andservices are seen as preferable to institutional care.The process for realigning policies to facilitate reformin the Long-Term Care systems and to foster the fullintegration of individuals with disabilities into societyis complex and far-reaching. Since the elderly andpersons with disabilities have significant health needs,they are among the most costly of Medicaid benefici-aries. Many government agencies and programs willneed to enter into extensive assessments and interac-tive policy initiatives to remove the existing barrierswoven through the fabric of federal and state policies.
The Deficit Reduction Act of 2005 (DRA) madesignificant changes in the Medicaid program, includ-ing changes in the states’ flexibility to design benefit
packages, prescription drug payment policies, premi-um and cost-sharing rules, and Long-Term Carereforms. The purpose of this survey analysis is to pro-vide the states with an overview of the implementa-tion of these DRA changes across the country. Thispaper specifically reviews the DRA changes in Long-Term Care services and the steps the states have takenwith respect to the changes. The following states andterritories participated in the survey: Alabama, Alaska,Arizona, Arkansas, California, Colorado, Connecti-cut, Delaware, Florida, Georgia, Guam, Idaho,Illinois, Indiana, Kentucky, Louisiana, Maine,Maryland, Massachusetts, Michigan, Minnesota,Mississippi, Missouri, Montana, Nebraska, Nevada,New Hampshire, New Jersey, New Mexico, NorthCarolina, North Dakota, Oregon, Ohio, PuertoRico, Rhode Island, South Carolina, South Dakota,Tennessee, Texas, Utah, Vermont, Virginia, Wash-ington, West Virginia, Wisconsin, and Wyoming.Please note that Guam and Puerto Rico have uniqueprograms and therefore may not have answered someof the questions. In addition, the information on theLong-Term Care Partnership Programs (LTCPP)was taken from earlier work that was done in collab-oration with George Mason University and theCenter for Health Care Strategies.
Executive Summary
361185_Lot1_Text_vii 11/7/07 5:39 PM Page vii

The key findings of the survey include:
Finding 1 Eligibility for Medicaid was Tightened Under the DRA andStates Responded
Finding 2 Most States Have not Used the Family Opportunity Act toExtend Medicaid Coverage to Children with Disabilities inFamilies with Higher Incomes
Finding 3 States use Their Money Follows the Person Grant Dollars inSeveral Ways
Finding 4 To Date, Most States are not Opting to Switch to the NewHCBS State Plan Amendment (SPA) Option
Finding 5 States are Initiating Efforts to Transition Individuals Out ofInstitutions
Finding 6 States are Using Managed Care for Individuals with Disabilities
Finding 7 Fewer than 10 States Plan to Submit a SPA for Personal CareServices (Cash and Counseling) Programs
Finding 8 Special Needs Plans are in Place in at Least 20 States, but StatesHave Concerns About Coordination Between Medicare andMedicaid
Finding 9 Long-Term Care Reform in the States Continues to EncourageHome- and Community-Based Living
Finding 10 States are Using Care Coordination to Improve and IntegrateCare
Finding 11 More States Using Disease Management to Help ManageChronic Conditions
Finding 12 Many States are Using the New Option on Long-Term CarePartnership Programs
Finding 13 Benchmark Benefit Packages are not Widely used for Long-TermCare Services
viii
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
361185_Lot1_Text_viii 11/7/07 5:39 PM Page viii
1
T he Deficit Reduction Act made several majorchanges to how states can provide Long-TermCare services and who is eligible for those
services. Specific changes included:
Eligibility
� Lengthens the look-back period on asset transfers.
� Changes the penalty period.
� Requires annuities to be disclosed and statesnamed remainder beneficiary.
� Requires states to use the income-first rule.
� Excludes coverage for individuals with higherhome equity.
Long-Term Care Partnership Programs
� Allows states to expand the Long-Term CarePartnership Programs.
Family Opportunity Act
� Creates a new option for states to extendMedicaid “buy-in” coverage to children with disabilities whose family income is up to 300 percent of poverty.
Money Follows the PersonDemonstration Program
� Awards competitive grants to states to increasethe use of HCBS.
State Option to Provide HCBS Services
� Allows states to provide a comprehensive packageof community-based services under theirMedicaid state plans that previously could onlybe provided by a waiver.
Personal Care Services “Cash andCounseling” Option
� Allows states to provide for self-direction of services without requesting a waiver.
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
The Deficit Reduction Act and Medicaid Long-Term
Care Services
361185_Lot1_Text_1 11/7/07 5:39 PM Page 1
Medicaid DemographicsThere are approximately 58 million Medicaid benefi-ciaries which constitutes approximately 20 percent ofthe total population of the U.S. The demographicbreakdown of the Medicaid population is as follows:
� 52 percent are children age 17 and under.
� 23 percent are adults between the ages of 18 and 64.
� 15 percent are blind or disabled individuals under age 64.
� 10 percent are over the age of 65.
Medicaid Spending on Long-Term Care
� Medicaid accounts for at least 40 percent of allLong-Term Care services, making it the nation’slargest single payer of Long-Term Care services.1
� Total Medicaid Long-Term Care expenditures inFY 2006 equaled $99.3 billion, an increase of 3.4percent over FY 2005.2
� Medicaid nursing home expenditures in FY 2006were $47.7 billion.3
� Over 400,000 children and over 1 million adultsunder 65 use Long-Term Care services, and 75percent of the children who use Long-Term Careservices qualify for Medicaid.4
Medicaid Spending on Long-Term Careby Services
� 44 percent of Long-Term Care spending was onnursing facilities.
� 41 percent of Long-Term Care spending washome health and personal care services.
� 11 percent of Long-Term Care spending was onIntermediate Care Facility for Persons withMental Retardation (ICF/MR) services.
� 4 percent of Long-Term Care spending was onmental health facilities.5
Medicaid and Home- and Community-Based Services
� Individuals under 65 are more likely then thoseover 65 to use HCBS.6
� Expenditures for community-based Long-TermCare services continue to increase more rapidlythan institutional expenditures.
� Total HCBS increased by 8.1 percent to $39.1 bil-lion. HCBS waiver expenditures increased 10.6percent to $25.6 billion and now account forabout 65 percent of all Medicaid community-based Long-Term Care spending.7
� Spending for community-based Long-Term Careservices rose to 39 percent of all Medicaid Long-Term Care costs, while 61 percent wasspent on institutional services.8
2
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
1 Kaiser Family Foundation: Medicaid/SCHIP: Medicaid’sLong-Term Care Beneficiaries: An Analysis of SpendingPatterns, 2006 http://www.kff.org/medicaid/7576.cfm
2 Burwell, B., Sredl, K. and Eiken, S: Medicaid Long-TermCare Expenditures in FY 2006. Thomson Healthcare,August 10, 2007
3 Ibid.4 Kaiser Family Foundation: Medicaid/SCHIP: Medicaid’s
Long-Term Care Beneficiaries: An Analysis of SpendingPatterns, 2006 http://www.kff.org/medicaid/7576.cfm
5 Ibid.6 Kaiser Family Foundation: Medicaid/SCHIP: Medicaid’s
Long-Term Care Beneficiaries: An Analysis of SpendingPatterns, 2006 http://www.kff.org/medicaid/7576.cfm
7 Burwell, B., Sredl, K. and Eiken, S: Medicaid Long-TermCare Expenditures in FY 2006. Thomson Healthcare,August 10, 2007.
8 Ibid.
Snapshot of the Medicaid ProgramLong-Term Care Benefits
361185_Lot1_Text_2 11/7/07 5:39 PM Page 2
3
T he Deficit Reduction Act of 2005 (P.L. 109-171) created new Medicaid transfer-of-assetrules. On July 27, 2006, the Centers for
Medicare and Medicaid Services (CMS) sent guid-ance to the states on how to implement the newrequirements.9 To comply with tightening of eligibil-ity under the DRA, the majority of states had tochange their state laws. This section of the reportdeals with the specific provisions contained inSections 6011 and 6016 of the Deficit Reduction Actand how states have responded.
Changing the Look-Back Period Section 6011 of the DRA lengthened the look-backperiod for Medicaid eligibility from three to five yearsfor all asset transfers, and 33 states have already madethe necessary changes to comply with this newrequirement. Of those states that have not yet madethe changes, two states expect to make the changes in2007, one state expects to make changes in 2010,two states are waiting for approval of a proposed rule,one state will be phasing the look-back period in, andone state does not need to make changes to complyat this time.
Changing the Start Date of the Penalty PeriodSection 6011 also requires states to change the startdate of the penalty period, and 34 states have alreadydone so. Prior to the change in the law, the penaltyperiod began either in the month of the transfer or inthe month following the transfer. Some state and fed-eral officials believed that some individuals wereavoiding the penalty period by not applying forMedicaid services until the expiration of the penaltyperiod, and therefore pressed for the statutory fix.
For those states that have already made thechanges, the penalty period will begin in the monthduring which assets were transferred; in six states itwill begin in the month after which assets were trans-ferred and in 15 states it will begin on the first day ofthe month following advance notice.
For the states that have not yet implemented, twostates are waiting for approval of a proposed rule, onestate will implement in 2007, one state will imple-ment by 2010, and one state will implement withinthree months after their state changes are enacted.
Changing the Requirements on PartialMonths of IneligibilityPrior to the DRA, states had the option to imposepenalty periods for asset transfers in a month thatwere less than the state’s average monthly cost to aprivate patient of nursing home care in the state.Under the change in statute, states are now requiredto impose penalty periods even in the case of smallerasset transfers where the period of ineligibility wouldbe less than a full month. If the calculation of thepenalty period produces a fractional amount, thepenalty must include a partial month disqualification.
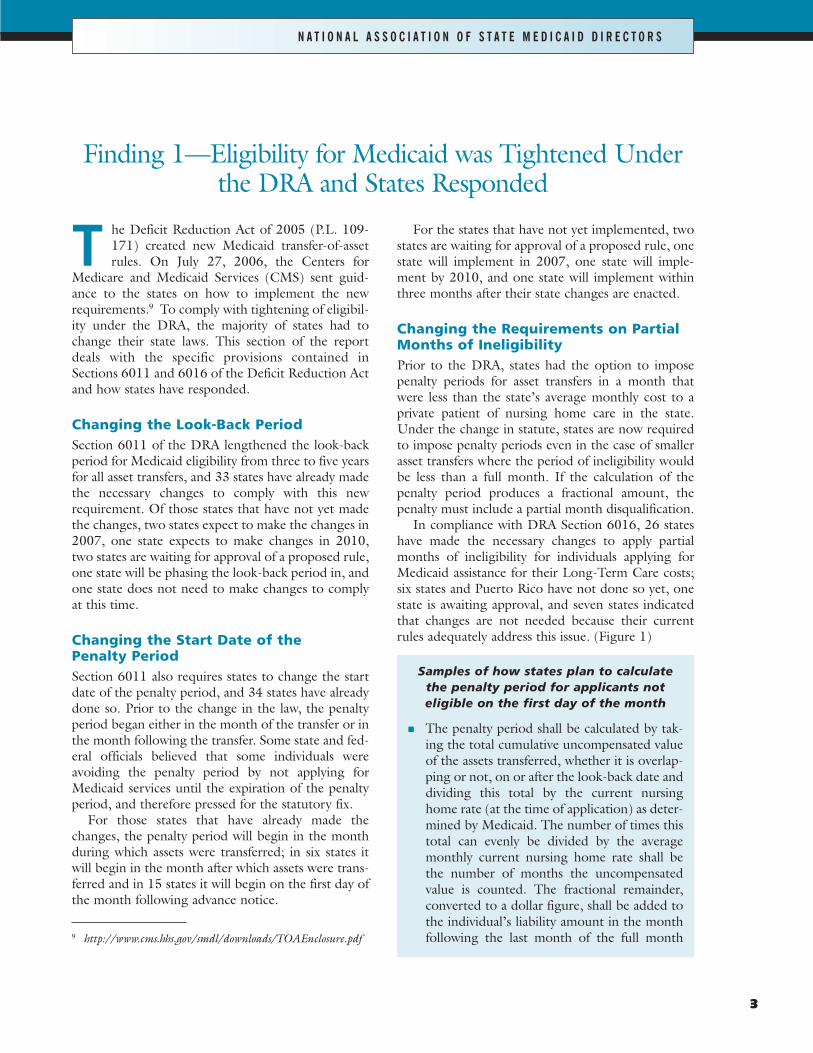
In compliance with DRA Section 6016, 26 stateshave made the necessary changes to apply partialmonths of ineligibility for individuals applying forMedicaid assistance for their Long-Term Care costs;six states and Puerto Rico have not done so yet, onestate is awaiting approval, and seven states indicatedthat changes are not needed because their currentrules adequately address this issue. (Figure 1)
Samples of how states plan to calculate the penalty period for applicants not eligible on the first day of the month
� The penalty period shall be calculated by tak-ing the total cumulative uncompensated valueof the assets transferred, whether it is overlap-ping or not, on or after the look-back date anddividing this total by the current nursinghome rate (at the time of application) as deter-mined by Medicaid. The number of times thistotal can evenly be divided by the averagemonthly current nursing home rate shall bethe number of months the uncompensatedvalue is counted. The fractional remainder,converted to a dollar figure, shall be added tothe individual’s liability amount in the monthfollowing the last month of the full month
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
9 http://www.cms.hhs.gov/smdl/downloads/TOAEnclosure.pdf
Finding 1—Eligibility for Medicaid was Tightened Underthe DRA and States Responded
361185_Lot1_Text_3 11/7/07 5:39 PM Page 3
penalty period. (A penalty period will never bestarted in a month in which an applicant isineligible.)
� The penalty period will begin with the date oftransfer or the application month, whichever isthe later date.
� If there is a penalty period, the individual willbe eligible for restricted services.
� Divide the uncompensated value of the trans-ferred asset by the average monthly nursinghome cost. The result is a percentage (e.g., 50percent). Determine the number of days thereare in the month the penalty ends. The num-ber of days’ penalty in that month is based onthe percentage. For example, if the penaltyends in June, which has 30 days, and the per-centage is 50 percent, then there are 15 daysof penalty.
4
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
L E G E N D :
States that have made changes
States that have not yet made the changes*
States that do not need to make changes because their legislation complies
States that are waiting on approval of a proposed ruling
*Note: Puerto Rico has not made the changes to their legislation. Data is unavailable for Guam.
State Changes to Apply Partial Months of Ineligibility for Individuals Applying for MedicalAssistance for their LTC CostsF I G U R E 1
361185_Lot1_Text_4 11/7/07 5:39 PM Page 4
5
� The penalty period is calculated on a dailybasis. For those who do not meet the level ofcare until a day other than the first, an ineligi-bility period will be calculated in days, and theyserve that period.
� The penalty period calculation is the sameregardless of whether the applicant is eligibleor not eligible on the first day of the month.The calculation establishes the length of thepenalty period. The state has the flexibility tobegin the period and end the period any dayof the month.
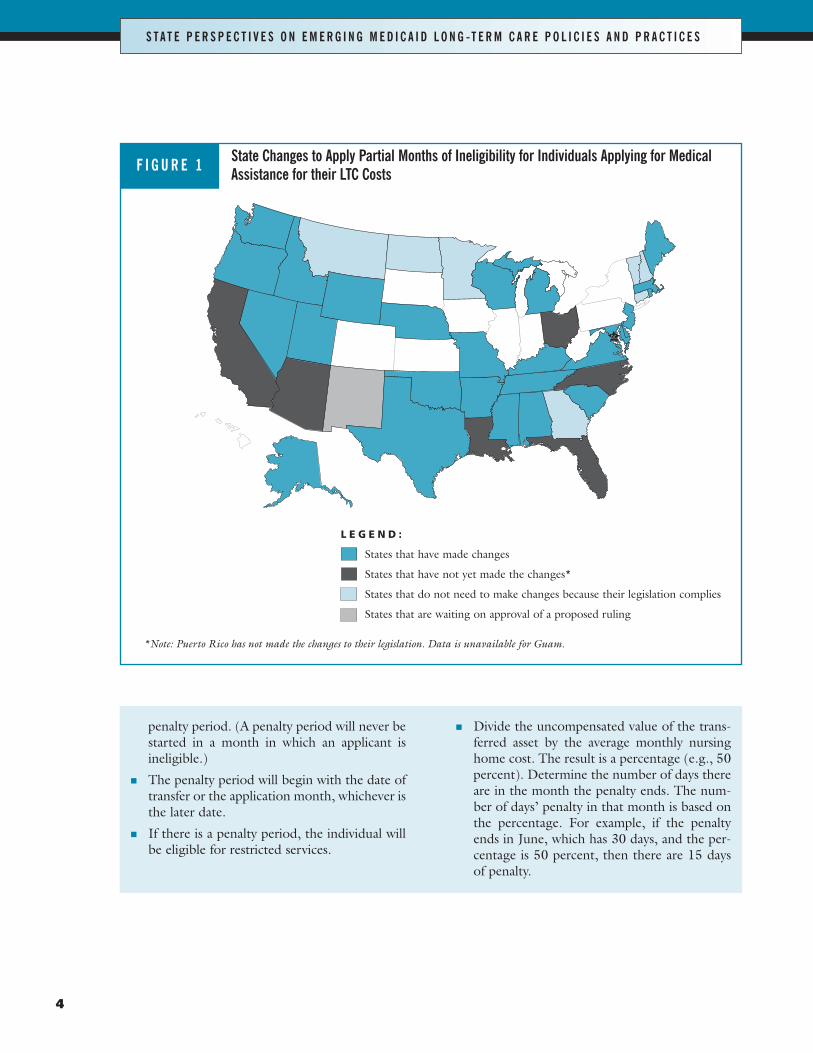
Changes to Accumulate MultipleTransfers in One MonthBy the summer of 2007, at least 30 states will havemade the changes to accumulate multiple transfers inmore than one month and impose a single period ofineligibility into one penalty period in order to con-form with DRA Section 6016. Four states and PuertoRico have not done so yet, or are in the process ofgetting approval and six states do not need to do sobecause their current rules comply. Four states plan toimplement in the summer of 2007, one state plans toimplement by 2010, and two states are waiting forapproval of a proposed rule. (Figure 2)
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
* Note: Puerto Rico has not made the changes to their legislation. California plans to make the changes by 2010. Virginia plans to make the changes by late 2008. Data is unavailable for Guam.
L E G E N D :
States that will have made the changes as of the summer of 2007
States that have not yet made the changes*
States that do not need to make changes because their legislation complies
States that are waiting on approval of legislation/rule
State Changes to Accumulate Multiple Transfers in More than One Month and Impose a Single Period of Ineligibility into One PeriodF I G U R E 2
361185_Lot1_Text_5 11/7/07 5:39 PM Page 5
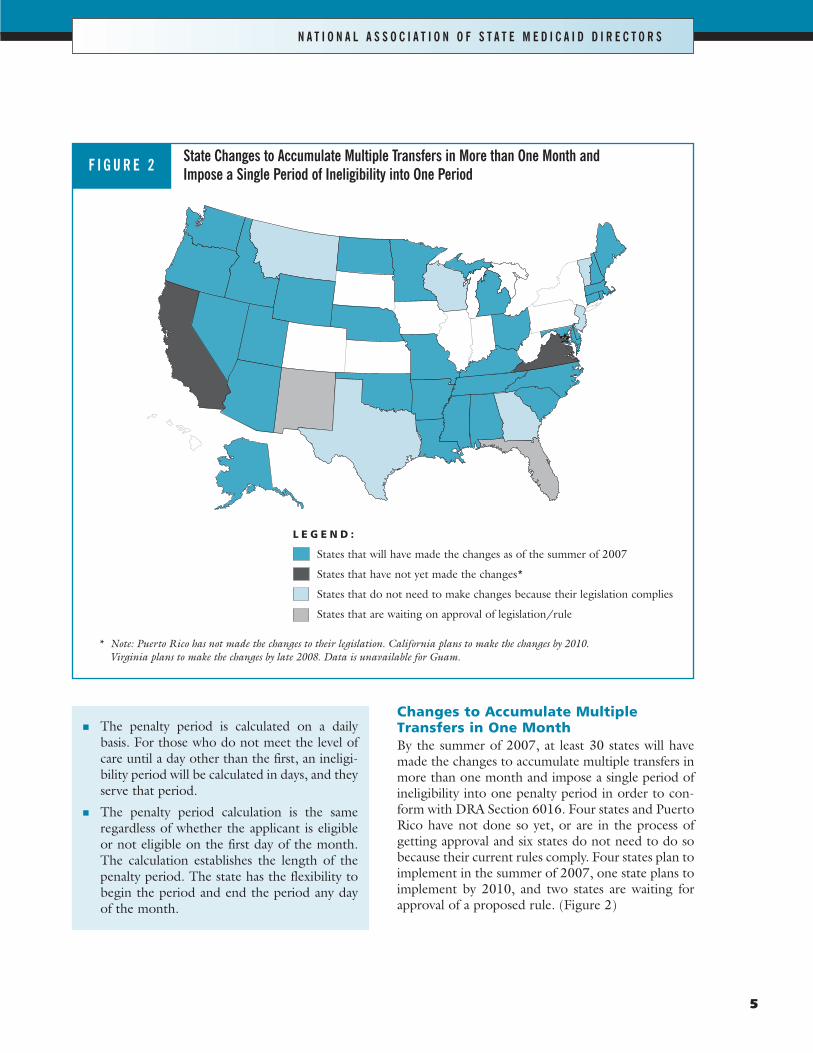
Changes Regarding Purchase ofPromissory Notes, Loans, andMortgagesBy the fall of 2007 at least 35 states will have madethe changes or do not need to make changes regard-ing purchase of promissory notes, loans, and mort-gages that were outlined in Section 6016. (Figure 3)
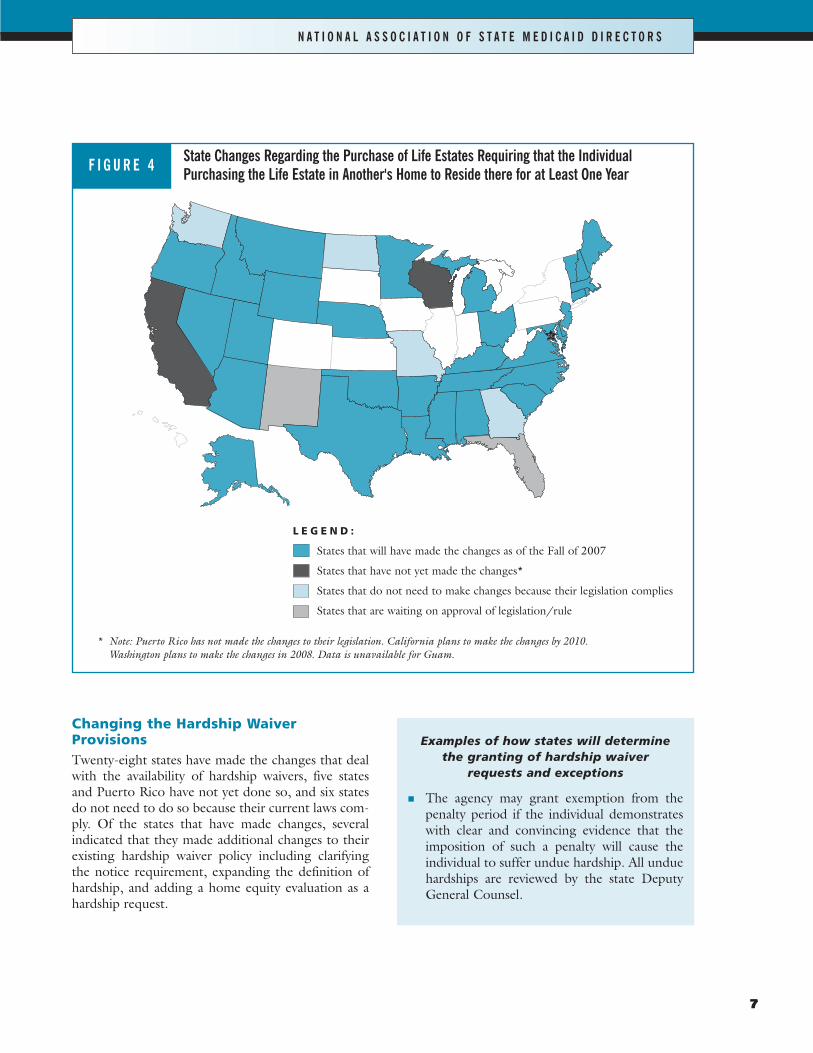
Changing Requirements Regarding thePurchase of Life EstatesAt least 32 states have made changes pertaining toSection 6016 regarding the purchase of life estatesthat require the individual purchasing the life estate inanother’s home to reside there for a period of at leastone year after the date of purchase. Four states andPuerto Rico have not implemented this yet. Of thosestates, one state will do so in 2010 and two states arewaiting for approval of a proposed rule. Four statessaid that changes to their laws are not needed to com-ply. (Figure 4)
6
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
* Note: Puerto Rico has not made the changes to their legislation. California plans to make the changes by 2010. Data is unavailablefor Guam.
L E G E N D :
States that have made the changes as of the Fall of 2007
States that have not yet made the changes*
States that do not need to make changes because their legislation complies
States that are waiting on approval of legislation/rule
State Changes Regarding the Purchase of Promissory Notes, Loans, and MortgagesF I G U R E 3
361185_Lot1_Text_6 11/7/07 5:39 PM Page 6
7
Changing the Hardship WaiverProvisionsTwenty-eight states have made the changes that dealwith the availability of hardship waivers, five statesand Puerto Rico have not yet done so, and six statesdo not need to do so because their current laws com-ply. Of the states that have made changes, severalindicated that they made additional changes to theirexisting hardship waiver policy including clarifyingthe notice requirement, expanding the definition ofhardship, and adding a home equity evaluation as ahardship request.
Examples of how states will determine the granting of hardship waiver
requests and exceptions
� The agency may grant exemption from thepenalty period if the individual demonstrateswith clear and convincing evidence that theimposition of such a penalty will cause theindividual to suffer undue hardship. All unduehardships are reviewed by the state DeputyGeneral Counsel.
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
* Note: Puerto Rico has not made the changes to their legislation. California plans to make the changes by 2010. Washington plans to make the changes in 2008. Data is unavailable for Guam.
L E G E N D :
States that will have made the changes as of the Fall of 2007
States that have not yet made the changes*
States that do not need to make changes because their legislation complies
States that are waiting on approval of legislation/rule
State Changes Regarding the Purchase of Life Estates Requiring that the IndividualPurchasing the Life Estate in Another's Home to Reside there for at Least One YearF I G U R E 4
361185_Lot1_Text_7 11/7/07 5:39 PM Page 7

� In cases where there has been financialexploitation by a family member or other thirdparty and there is no evidence that the recipientparticipated in the transfers and the transferredassets cannot be returned, then a hardshipwaiver will be granted.
� The person receives an eviction notice fromthe nursing home and has tried all legal meansto stop the eviction.
� The individual is exploited as determined bythe Adult Protective Unit, if the individual canprove all of the following: (1) neither the indi-vidual nor the spouse (taking into considera-tion all exempt and non-exempt income andassets) have the means to pay; (2) the recipientof the transferred asset is unable or unwillingto give the asset or any part of the asset back;(3) the individual has made all reasonableefforts to recover the transferred asset andcooperated with the department to recoverthe asset; (4) the individual must agree in writ-ing that if the transferred asset or its equivalentis recovered, the individual will reimburse thestate for funds expended as a result of theapproved claim of undue hardship; and (5)that to prove it would be undue hardship.
� The eligibility worker must obtain verificationthat a denial of benefits would result in a life-threatening situation, and it must be demon-strated that all other possible exceptions to theimposition of the transfer penalty have beenexplored.
� Any of the following exist: (1) location of thereceiver of the asset is unknown to the client orother family members or other interested par-ties, and the client has no place to return in thecommunity and/or receive the care requiredto meet the client’s needs; ( 2) client can showthat physical harm may come as a result of pur-suing the return of the asset, and the client hasno place to return in the community and/orreceive the care required to meet the client’sneeds; or (3) receiver of the asset is unwillingto cooperate (such as an Adult ProtectiveServices exploitation or potential fraud case)with the client, and the client has no place toreturn to in the community and/or receive thecare required to meet the client’s needs.
� Any of the following: (1) a Power of Attorney(POA) or guardian transferred the asset andwas not acting in the person’s best interestswhen the transfer was made; (2) the personwas deprived of the asset(s) by fraud or mis-representation; or (3) the person cannotrecover the asset(s) due to loss, destruction,theft, or other similar circumstances.
� The person to whom the asset(s) was trans-ferred has no reasonable way to make arrange-ments for the person seeking care up to thevalue of the transfer; and the person seekingcare has made reasonable efforts to obtainreturn of the asset(s); and the person seekingcare can demonstrate that efforts to obtain theasset(s) or adequate value for them probablywould not succeed.
� The client is unable to access home equity in ex-cess of $500,000 due to a lien or legal impedi-ment, and without these services the client willbe endangered.
8
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
361185_Lot1_Text_8 11/7/07 5:39 PM Page 8
9
Changes in Annuities Relating to theDisclosure of Interests and RemainderBeneficiaryThirty-one states have made the changes as a result ofDRA Section 6012 that deal with the changes inannuities requiring the applicant to disclose his/herinterest or his/her spouse’s interest in an annuity andname the state as remainder beneficiary.
Income-First Rule ChangesThirteen states have made changes with regard to theincome-first rule, three states and Puerto Rico havenot made changes, and 24 states do not need to makechanges because their current rules comply with thisrequirement. One state is waiting for approval of aproposed rule before implementing, one state willimplement shortly, and one state is still unsure aboutwhen they will be able to implement.
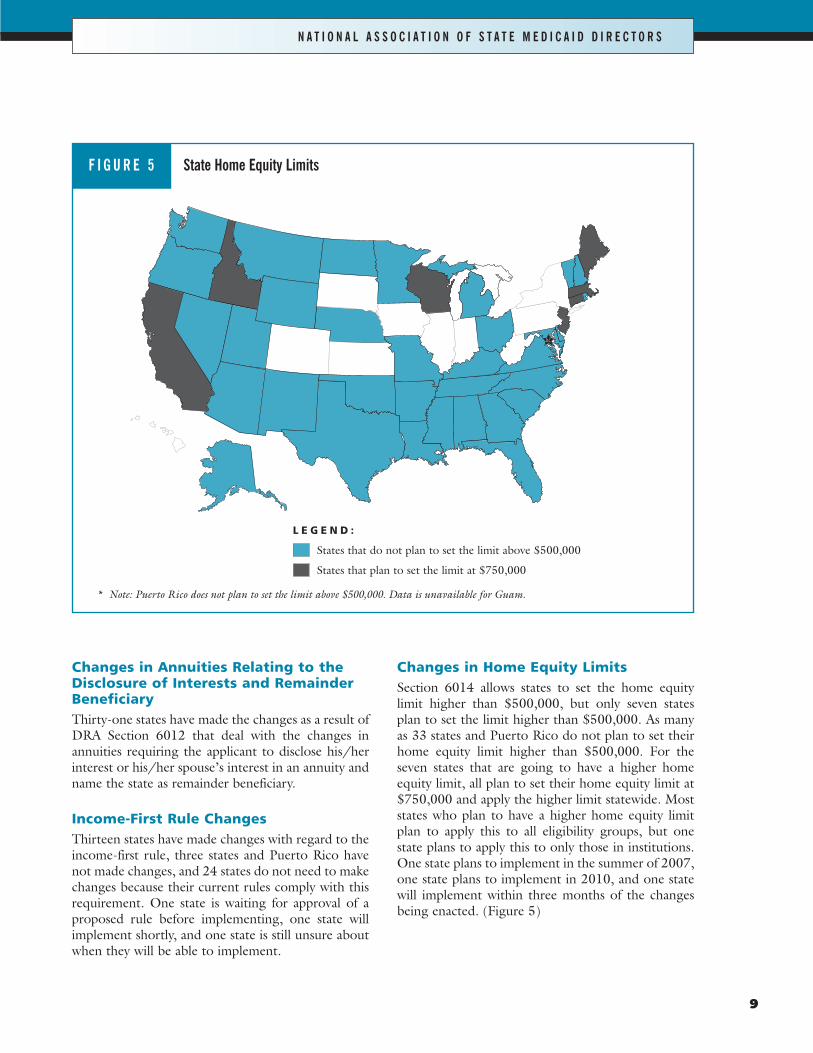
Changes in Home Equity LimitsSection 6014 allows states to set the home equitylimit higher than $500,000, but only seven statesplan to set the limit higher than $500,000. As manyas 33 states and Puerto Rico do not plan to set theirhome equity limit higher than $500,000. For theseven states that are going to have a higher homeequity limit, all plan to set their home equity limit at$750,000 and apply the higher limit statewide. Moststates who plan to have a higher home equity limitplan to apply this to all eligibility groups, but onestate plans to apply this to only those in institutions.One state plans to implement in the summer of 2007,one state plans to implement in 2010, and one statewill implement within three months of the changesbeing enacted. (Figure 5)
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
* Note: Puerto Rico does not plan to set the limit above $500,000. Data is unavailable for Guam.
L E G E N D :
States that do not plan to set the limit above $500,000
States that plan to set the limit at $750,000
State Home Equity LimitsF I G U R E 5
361185_Lot1_Text_9 11/7/07 5:39 PM Page 9

10
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Recalculating the Penalty PeriodTwenty-eight states plan to recalculate the penaltyperiod when a portion of the transferred resources arereturned to the Long-Term Care recipient, and fivestates will require all of the transferred resources to bereturned in order for the divestment penalty period tobe eliminated. Connecticut, Florida, and Ohio willrecalculate the penalty period when a portion isreturned and eliminate the penalty period if all assetsare returned. Two states have made changes to theirpolicy dealing with the “intent” to divest in order toqualify for Medicaid.
Examples of how and when states will consider transfers to be divestments
� A divestment has occurred when a recipienttakes action to make an asset unavailable; forexample, adding another person’s name to anasset and the asset cannot be made availablewithout that other person’s permission.
� The transfer is for less than fair market value;the transferor was not in good health at thetime; and the transferor applied for Long-Term Care benefits under the Medicaid pro-gram within the look-back period.
� Whenever an individual sells, gives away, orreduces the individual’s ownership interest ina resource within the look-back period andfails to receive fair compensation.
� When it is made for inadequate consideration.
� The agency considers any transfer during theappropriate look-back period by the nursing-facility resident or spouse of a resource, orinterest in a resource, owned by or available tothe nursing-facility resident or the spouse(including the home or former home of thenursing-facility resident or the spouse) for lessthan fair-market value a disqualifying transferunless listed as permissible in state laws. Theagency may consider as a disqualifying transferany action taken to avoid receiving a resourceto which the nursing-facility resident orspouse is or would be entitled if such actionhad not been taken. Action taken to avoidreceiving a resource may include, but is notlimited to, waiving the right to receive aresource, not accepting a resource, agreeing tothe diversion of a resource, or failure to takelegal action to obtain a resource. In determin-ing whether or not failure to take legal actionto receive a resource is reasonably considereda transfer by the individual, the agency willconsider the specific circumstances involved. Adisqualifying transfer may include any actiontaken that would result in making a formerlyavailable asset no longer available.
� Unless the person can establish that the trans-fer was solely for another purpose, or had asudden onset of illness after the transfer, thetransfer is considered to be for Medicaid pur-poses.
� Transfers are not considered a divestment ifthe transfer was solely for a purpose other thanto qualify for Medicaid.
361185_Lot1_Text_10 11/7/07 5:39 PM Page 10
11
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
T he Deficit Reduction Act Section 6062 creat-ed a new option for states to extend Medicaidcoverage to children with disabilities. The new
Medicaid coverage would create a “buy-in” opportu-nity for parents of children with disabilities with fam-ily incomes up to 300 percent of the federal povertylevel (FPL). Under the DRA, coverage would bephased in starting in 2007 for children up to age 6and coverage for children up to age 19 by 2009.Under the new section, states are allowed to chargepremiums and require parents to participate inemployer-sponsored insurance if the employer paysfor at least 50 percent of the premium.
According to the results of the survey, three statesplan to make this option available to such families and28 states, Puerto Rico, and Guam do not plan tomake this available. However, four states are still con-sidering this option and three other states cover theseindividuals in another manner. One state plans tomake this available in 2008 and another state isunsure when the Family Opportunity Act will beavailable. One state plans to set the income level upto 300 percent, another state up to 200 percent, andanother state between 200 and 300 percent.
Finding 2—Most States Have not Used the FamilyOpportunity Act to Extend Medicaid Coverage to Children
with Disabilities in Families with Higher Incomes
T he Money Follows the Person DemonstrationProgram authorizes the secretary of U.S.Health and Human Services to award compet-
itive grants to increase the use of HCBS rather thanthe traditional institutional services. The demonstra-tion program goal is to create an incentive for statesto “rebalance” their long-term services programs byproviding grant funding for two years. States whoreceive the grant awards will receive an enhancedmatch for each eligible individual that transitionsfrom an institution to the community. States must,however, continue to support the individuals whohave moved into the community setting after thetwo-year grant cycle ends. States are allowed to setcriteria for eligibility but eligible individuals musthave been institutionalized for at least six months andup to a max of two years. The total funding availablefor this demonstration program is $1.8 billion.
To date, 31 states have successfully competed for$1.4 billion in funding. Several states that receivedgrant funds for Money Follows the Person havedescribed how they plan to use these funds to assistnearly 38,000 individuals in their transition from insti-tutional care to home- and community-based care.
Several states have targeted the populationsinclude individuals with physical disabilities, the agingpopulation, and individuals with traumatic braininjuries.
Oregon Money Follows the Person Initiative
Oregon plans to demonstrate that long-term institu-tionalized populations of people with complex med-ical and Long-Term Care needs can be served in theircommunities with wrap-around packages of supportsand services. Specific populations that Oregon pro-poses to serve include:
� 40 children with developmental disabilities inpediatric nursing facilities
� 300 seniors with end-stage dementia in nursingfacilities
� 300 adults with physical disabilities in nursingfacilities; and
� 140 adults with developmental disabilities innursing and intermediate care facilities.
Finding 3—States Use Their Money Follows the Person Grant Dollars in Several Ways
361185_Lot1_Text_11 11/7/07 5:40 PM Page 11

12
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
These 780 individuals account for 16.5 percent ofOregon’s institutionalized Medicaid population. Staffin Oregon believe that the successful transition ofthese individuals to the community will begin build-ing the next national model to provide HCBS to peo-ple not typically able to use these services.
Texas Money Follows the Person Initiative
Texas proposes to build on its current practice ofassisting individuals to transition out of institutionsinto community-based programs and to focus newefforts on persons with complex support needs, par-ticularly those with behavioral health conditions. Thisgrant will provide Texas with the opportunity to con-duct rebalancing efforts that would have been diffi-cult without the additional federal funding. Texas isproposing a new strategy for transitioning individualswith intellectual and developmental disabilities out ofcommunity-operated nine-plus-bed IntermediateCare Facilities for Persons with Mental Retardation(ICFs/MR) into the community with new demon-stration services for persons with behavioral healthconditions.
For individuals in nursing facilities, Texas will (1)build upon its current Money Follows the PersonInitiative and use the enhanced match to financecommunity-based services and improve outreachefforts; (2) target for transition, individuals with com-plex support needs in general and (3) through a newpilot focused on individuals with co-occurring behav-ioral health conditions; and (4) provide post-transi-tional services to assist in a successful transition.
For individuals in institutions serving persons withintellectual and developmental disabilities, Texas will(1) continue its current Promoting IndependencePriority Populations Initiative and use the enhancedmatch to transition individuals out of 14-plus-bedcommunity-operated ICFs/MR and State MentalRetardation Facilities; and (2) implement a new ini-tiative to close nine-plus-bed community-operatedICFs/MR and transition residents to other settings oftheir choice, including home- and community-basedwaiver programs.
Washington State Roads to Community Living Project
Washington’s Roads to Community Living will assist660 citizens in Washington State who want to movefrom institutional settings to their own communities.Target groups for this project include older adults,individuals with developmental disabilities, individu-als with physical disabilities, and individuals withmental illness who need extra services and support tomove home. The project will provide intensive tran-sition support and one-time goods and services need-ed to set up and maintain community living. Theproject includes strong partnerships with theHousing Trust Fund, local Housing Authorities,Vocational Rehabilitation, the Department of MentalHealth, the Division of Developmental Disabilities,Tribal Nations, Area Agencies on Aging, theAssociations of Centers for Independent Living, andother consumer advocacy groups in project designand implementation.
361185_Lot1_Text_12 11/7/07 5:40 PM Page 12

13
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
T he Deficit Reduction Act amends Section1915 of the Social Security Act to allow forstates to provide a comprehensive package of
home- and community-based waiver services undertheir Medicaid state plan. Prior to the change in theDRA, states were only allowed to provide HCBSunder a waiver.
There are a number of significant differences forstates in using the new state plan option versus theHCBS waiver. Differences include limited services,awaiting federal guidance, and lack of flexibility towaiver comparability among populations, increasedstate costs, functional eligibility that is too restrictive,financial eligibility barriers, and financial constraints.(For a complete list of the differences between thenew state plan option and the HCBS waiver, seeAppendix B.)
At least two states plan to submit SPAs to provideHCBS, while 16 states and Guam are still unsureabout whether they will submit an SPA for these serv-ices. As of the release of the survey, only Iowa hasreceived approval for its new state plan amendmentfor HCBS.
Populations States May Cover if HCBS SPA Option is Elected
� Developmentally disabled
� Physically disabled
� Elderly
� Persons needing Assertive Community Treatment(ACT) services.
� Medicaid recipients utilizing Adult Day Health
� Medicaid recipients utilizing HCBS Home-BasedHabilitation
� Medicaid recipients utilizing HCBS PartialHospitalization
� Medicaid recipients utilizing HCBS PsychosocialRehabilitation Services specifically for individualswith Chronic Mental Illness
Select Services States May Provide under a HCBS SPA
� Adult day health care
� Attendant care
� Companion care
� Emergency alert system
� Habilitation (day treatment and training, andsupported employment)
� Home-delivered meals
� Home health services/home health aide
� Home health services/RN continuous and RNintermittent
� Home health services/LPN intermittent andLPN continuous
� Home modification
� Respite (short-term and continuous in-home andgroup respite)
� Assertive Community Treatment (ACT) services
� HCBS Partial Hospitalization
� HCBS Psychosocial Rehabilitation Services forindividuals with Chronic Mental Illness
This list represents information only for states thatresponded to the survey.
Eligibility for HCBS ServicesThe DRA allows states to set eligibility for the newSPA HCBS up to 150 percent of the FPL. For thestates considering the new state plan amendment forthese services, one state plans to set the income levelat 150 percent of FPL, one state is still unsure, andone state plans to set it at three times SSI eligibilitylimit.
Finding 4—To Date, Most States are not Opting to Switchto the New HCBS State Plan Amendment (SPA) Option
361185_Lot1_Text_13 11/7/07 5:40 PM Page 13
14
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
A significant finding was that states are actingaggressively to move beneficiaries, when pos-sible, from institutional settings to communi-
ty settings. States are taking the following steps tomove beneficiaries from institutions to communitysettings.
State Innovations to Transition Individuals Out of Institutions
� Establishing one-stop resource centers to providea coordinated system of information and access forany person seeking Long-Term Care services andsupports
� Developing web sites to provide up-to-date infor-mation on home- and community-based Long-Term Care services and supports
� Completing comprehensive studies to improve thestate’s understanding of the financial and structur-al barriers to increasing access to HCBS
� Expanding funding to increase the number of frailand elder clients served by the programs currentlyoffered
� Adding a relocation case management service tothe Medicaid State Plan to assist people in movingout of institutions to community settings. Thisenabled the state to serve a broader group thanindividuals transitioning to home- and communi-ty-based waivers
� Creating a new Long-Term Care pre-admissionscreening tool
� Providing for transitional needs under a “HomeAgain” waiver
� Providing counseling and transition assistance toMedicaid beneficiaries residing in nursing homeswho wish to return to the community
� Reviewing all Nursing Facility admissions at 45days post admission; sending brochures with op-tions and contacts to new admissions; institutingcommunity transitional services into 1915(c)waivers; cooperating with centers for independentliving
� Providing for “establishment” funds (e.g., furni-ture, lights, water, etc.)
� Establishing a portability program in which eligi-ble individuals who have resided in a nursinghome for 90 days or more may be transferred intothe Waiver for Individuals with Physical Disa-bilities and having their funding follow them
� Approving spouses as paid caregivers and adding24-hour in-home care in certain instances
� Collaborating with the nursing home ombudsmanprogram to assist in transitioning individuals
Finding 5—States are Initiating Efforts to TransitionIndividuals Out of Institutions
O f the states that responded to the survey,13 and Puerto Rico indicated that theyhave a managed care program for individu-
als with disabilities on their Medicaid program.
Five states’ managed care programs are within anHCBS waiver while eight states and Puerto Ricohave a managed care program within their StatePlan.
Finding 6—States are Using Managed Care for Individuals with Disabilities
361185_Lot1_Text_14 11/7/07 5:40 PM Page 14
15
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
I n the late 1990s with the assistance and supportof the Robert Wood Johnson Foundation,Arkansas, Florida, and New Jersey were given
special waiver authority to test the use of self-directedpersonal care services. Under the waiver program,these three states allowed beneficiaries to managetheir personal assistance and other Long-Term Careservices by “cashing out” the funds that they wouldhave received from the states. The success of the threeearly implementer states led to the IndependencePlus initiative, which encouraged all states to provideMedicaid beneficiaries with self-directed services.Independence Plus allows states to develop programsusing either the 1115 or 1915(c) waiver authority.
The Deficit Reduction Act created anotherauthority for states to provide self-directed personalcare services under 1915 (j), but this time under astate plan amendment option. There are many differ-ences between the waiver and SPA authorities,including the ability to waive statewideness and theability to limit the program to certain populations.(For a complete comparison of the new SPA author-ity, Independence Plus waiver option, and the 1115waiver, see Appendix C.)
At the time of the survey, only five states plan tosubmit a SPA for self-directed personal care servic-es, that is, cash and counseling. States who chosethis option believe the program will be helpfulbecause it will give participants more flexibility andauthority in the hiring and selection of their Long-Term Care providers. States also believe that pro-viding participants with choices will lead them tomake better decisions.
States moving toward the 1915(j) option includetwo states that are transitioning from a traditional1115 waiver.
Benefits of Self-Directed Services Using the 1915(j) Option
� Allows clients on two existing HCBS waivers the opportunity to self-direct personal care,homemaker, and companion services
� Allows participants more flexibility andauthority in the hiring, training, and selectionof Long-Term Care providers
� Provides the participants with choices andallows them to share responsibility, whichleads to better decision making
� Allows target populations ultimate flexibilitysecuring non-medical services and promotesmore independence
� Changes will increase service options for peo-ple with disabilities
Information as reported by states considering usingthe 1915 (j) option
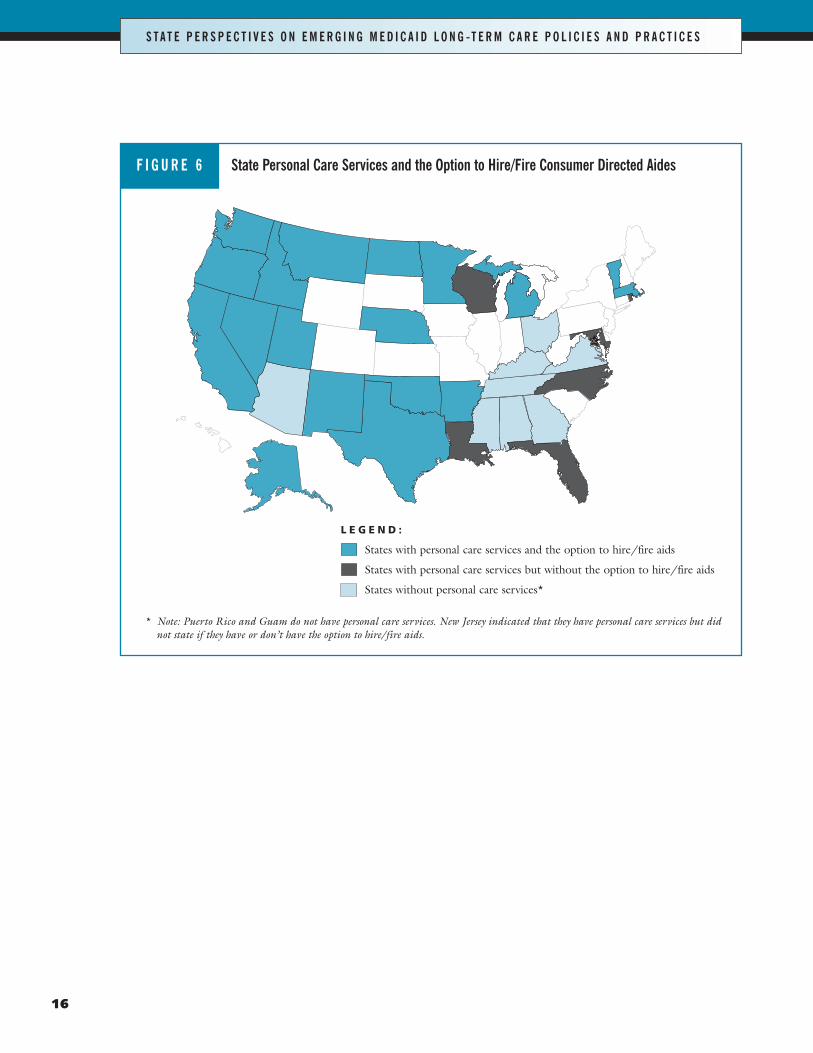
Twenty-five states currently offer personal care serv-ices and 8 states, Puerto Rico, and Guam do not. Ofthe 25 states, 18 states provide consumers with theoption to hire/fire individual consumer-directedaides, and in 16 of these states this option is widelyavailable. (Figure 6)
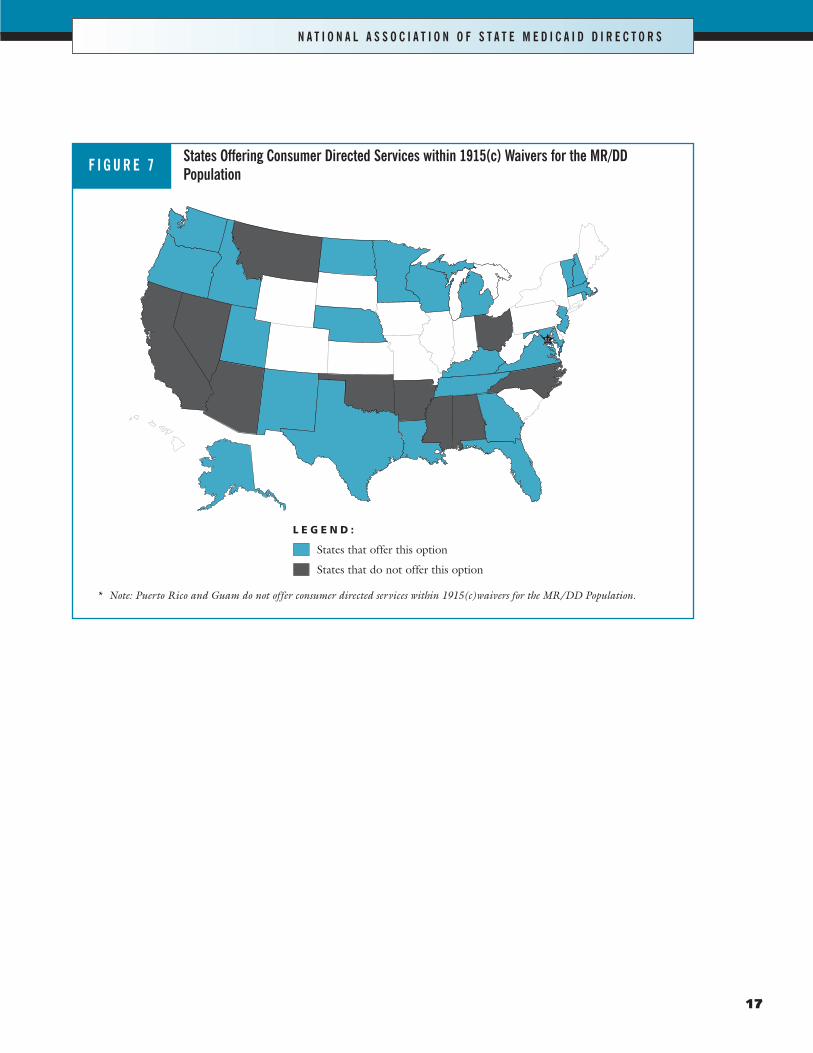
Eight states are considering a 1915(j) SPA to givethose eligible for state personal care services theopportunity to direct an individual budget. Currently26 states offer consumer-directed services within1915(c) waivers for their elderly and/or disabledpopulations. Twenty-four states offer consumer-directed services within 1915(c) waivers for theMentally Retarded/Developmentally Delayed popu-lation (MR/DD). (Figure 7)
Finding 7—Fewer than 10 States Plan to Submit a SPA for Self-Directed Personal Care Services
(Cash and Counseling) Programs10
10 The data for this was collected prior to the release of theState Medicaid Director letter providing states with moreinformation on the SPA for self-directed personal care serv-ices as well as a pre-print. NASMD will be investigatingwhether or not additional states will now take the option.
361185_Lot1_Text_15 11/7/07 5:40 PM Page 15
16
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
* Note: Puerto Rico and Guam do not have personal care services. New Jersey indicated that they have personal care services but didnot state if they have or don’t have the option to hire/fire aids.
L E G E N D :
States with personal care services and the option to hire/fire aids
States with personal care services but without the option to hire/fire aids
States without personal care services*
State Personal Care Services and the Option to Hire/Fire Consumer Directed AidesF I G U R E 6
361185_Lot1_Text_16 11/7/07 5:40 PM Page 16
17
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
States Offering Consumer Directed Services within 1915(c) Waivers for the MR/DDPopulationF I G U R E 7
* Note: Puerto Rico and Guam do not offer consumer directed services within 1915(c)waivers for the MR/DD Population.
L E G E N D :
States that offer this option
States that do not offer this option
361185_Lot1_Text_17 11/7/07 5:40 PM Page 17

18
S pecial Needs Plans (SNPs) are enrolling dualeligibles in 20 states and Puerto Rico. PuertoRico and eleven of these states are contracting
with SNPs for Medicaid services for dual eligibles.The states vary with regard to the populationsenrolled in SNPs: two states cover duals over 21, onestate covers those over 65, one state covers disabledpersons between 18 and 64 and those over 65, onestate covers all duals except those residing in institu-tions, one state covers aged/blind/disabled, onestate covers both seniors and persons with disabili-ties, and one state covers the frail elderly who arephysically disabled and are in nursing homes. Statesare working with nonprofit health plans, privatehealth plans, their CMS regional offices, MedicareAdvantage, managed care organizations, and otherunits of their state government to develop SpecialNeeds Plans.
Sample Special Needs Plans Activities
Florida’s Nursing Home Diversion Waiver (1915(c))offers acute and Long-Term Care services to duallyeligible elders at risk for nursing home placement.Program providers are responsible for coordinatingall the enrollee’s care needs regardless of fundingsource. Some Nursing Home Diversion plans havebeen certified as SNPs by Medicare. Florida’s
Medicaid program is developing a program to servedually eligible elders at risk for nursing home place-ment. This program will allow recipients to enrollsimultaneously with the same Medicaid and MedicareAdvantage managed care contractor. The new pro-gram will allow integration at the plan level. The newprogram’s contractors will contract with SNPs.
There are 12 dual-eligible SNPs currently operat-ing in Minnesota and are sponsored by nine healthplans, all of which also participate in Medicaid man-aged care. The state holds contracts with 10 of theseSNPs. Nine of the SNPs serve over 35,000 dually eli-gible seniors under a fully integrated Medicare-Medicaid primary, acute, and Long-Term Care pro-gram called Minnesota Senior Health Options(MSHO). One SNP serves 800 people with disabili-ties age 18 to 64 enrolled in Minnesota DisabilityHealth Options (MnDHO), also a fully integratedMedicare-Medicaid, primary, acute, and Long-TermCare program. The two other SNPs do not yet havecontracts with the state, but one of them has enrolledover 600 dually eligible people with disabilities. Thestate currently has a solicitation pending for addition-al contracts with SNPs for a new primary and acutecare program for people with disabilities age 18 to 64called Special Needs BasicCare (SNBC), effectiveJanuary 1, 2008.
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Finding 8—Special Needs Plans are in Place in at Least 20 States, but States Have Concerns About Coordination
Between Medicaid and Medicare
361185_Lot1_Text_18 11/7/07 5:40 PM Page 18
19
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
Additional State Concerns with Special Needs Plans
� The SNP may not improve the coordinationof care for Medicaid members since mostMedicaid members are required to be enrolledin a Medicaid managed care organization.
� In states with a large managed care popula-tion, the SNP would not provide significantimprovement with coordination of care.
� Service providers lack experience with De-velopmentally Delayed clients/Mental Healthclients under 65, specifically as it pertains totargeted services coordination.
� Medicare-only SNPs that don’t have corre-sponding Medicaid contracts will cost-shift toMedicaid’s Long-Term Care systems.
� Failure to integrate Medicare and Medicaidpayments and services results in fragmentedcare and poor clinical outcomes for frail dualeligibles.
� CMS has not provided enough specificityabout coordination of care.
� The lack of provider network standards resultin a wide variation among SNPs.
� SNPs are not available statewide, especiallynot in rural areas.
� The enrollment/disenrollment activities donot always coordinate from Medicare toMedicaid, causing gaps in coverage for clients.
� There need to be additional consumer protec-tions regarding marketing to potentialenrollees.
*As reported by States in the NASMD Survey onLong-Term Care
361185_Lot1_Text_19 11/7/07 5:40 PM Page 19
20
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
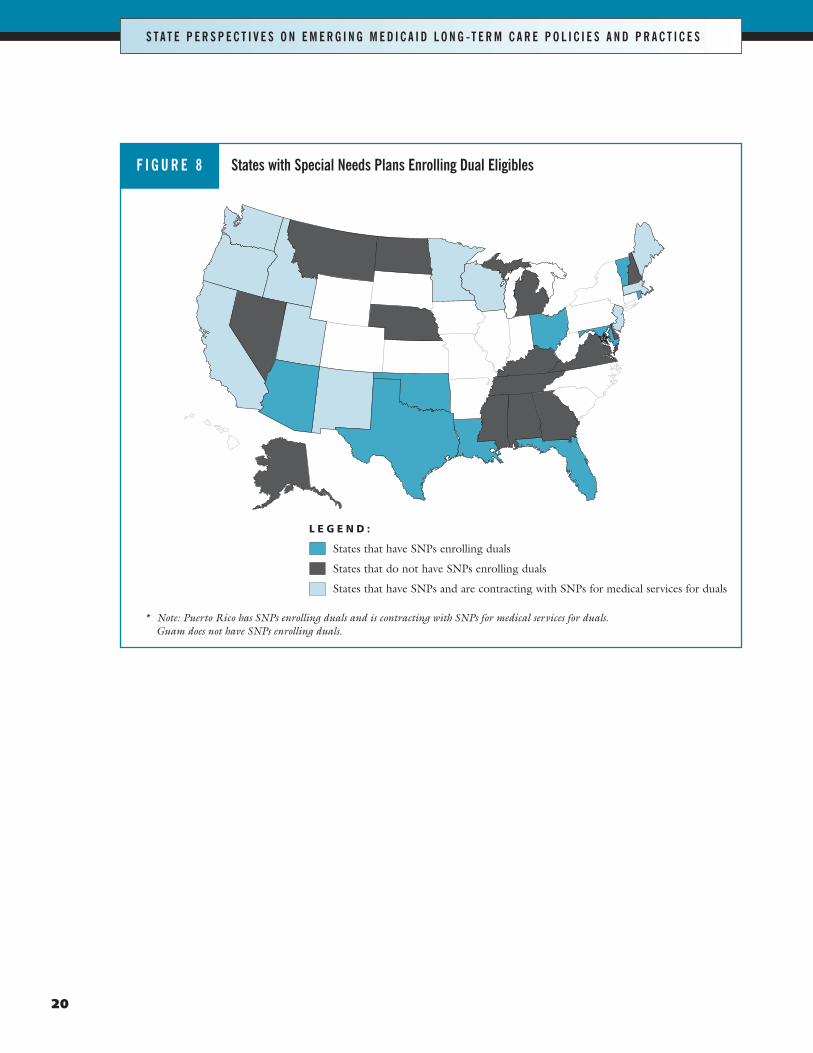
* Note: Puerto Rico has SNPs enrolling duals and is contracting with SNPs for medical services for duals.Guam does not have SNPs enrolling duals.
L E G E N D :
States that have SNPs enrolling duals
States that do not have SNPs enrolling duals
States that have SNPs and are contracting with SNPs for medical services for duals
States with Special Needs Plans Enrolling Dual EligiblesF I G U R E 8
361185_Lot1_Text_20 11/7/07 5:40 PM Page 20
21
S tates reported a wide range of Long-TermCare reform activities being implemented inthe last year. Several states worked to ease the
eligibility process by providing useful screening toolsto potential beneficiaries. Several states indicated thatthey were engaged in Long-Term Care planningmedia awareness campaigns to encourage citizens toplan for their future health needs. One state indicat-ed that it had undergone a major nursing homereform effort in the last year. The majority of statesindicated that they were engaged in efforts to consol-idate, coordinate, and improve home- and communi-ty-based services.
Sample State Long-Term Care Reform Initiatives
New Jersey—Governor Jon Corzine (D) signedthe Independence, Dignity and Choice in Long-Term Care Act into law on June 21, 2006. The actcalls for the reallocation of Medicaid Long-TermCare expenditures and the creation of a moreappropriate balance between funding for nursinghomes and community-based services. The pro-gram, known as Global Options for Long-TermCare (GO for LTC), is continuing the restructur-ing of New Jersey’s Long-Term Care system. Theact also directs the Department of Health andSenior Services (DHSS) to implement a system ofstatewide Long-Term Care service coordinationand management, identify home- and communi-ty-based Long-Term Care models that are effi-cient and cost-effective alternatives to nursinghome care. DHSS will also develop and imple-ment a consumer assessment instrument that isdesigned to expedite the process to authorize theprovision of HCBS through fast-track eligibilityprior to formal financial eligibility determination.In addition, DHSS is authorized to develop aquality assurance system, make information avail-able to the general public, and create a MedicaidLong-Term Care Funding Advisory Council.
Vermont—Under Vermont’s 1115 waiver(Choices for Care), spouses may now be paid toprovide care. Also, an option has been developedfor 24-hour, in-home care, using a home provideror shared living arrangement. Vermont Medicaidcarefully monitored several patients with mentalhealth and Long-Term Care needs who left thestate mental hospital for independent living envi-ronments to ensure that provisions for 24-hourcare are realistic.
Over the next year, the states report that theyhave a series of Long-Term Care initiativesplanned. Several states indicated that they wereconsidering new initiatives on managed care forthe elderly and disabled population. Some statesindicated an interest in pursuing The Program ofAll-Inclusive Care for the Elderly (PACE). Thereis also significant interest in the states in pursuingadditional self-directed options for beneficiaries.
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
Finding 9—Long-Term Care Reform in the StatesContinues to Encourage Home- and
Community-Based Living
361185_Lot1_Text_21 11/7/07 5:40 PM Page 21
C are coordination is a process that includesassessing the needs of a client and effectivelyplanning, arranging, coordinating and fol-
lowing-up on services that most appropriately meetthe identified needs of the client. States have usedcare coordination (for Medicaid recipients) to im-prove the quality of care that they receive.
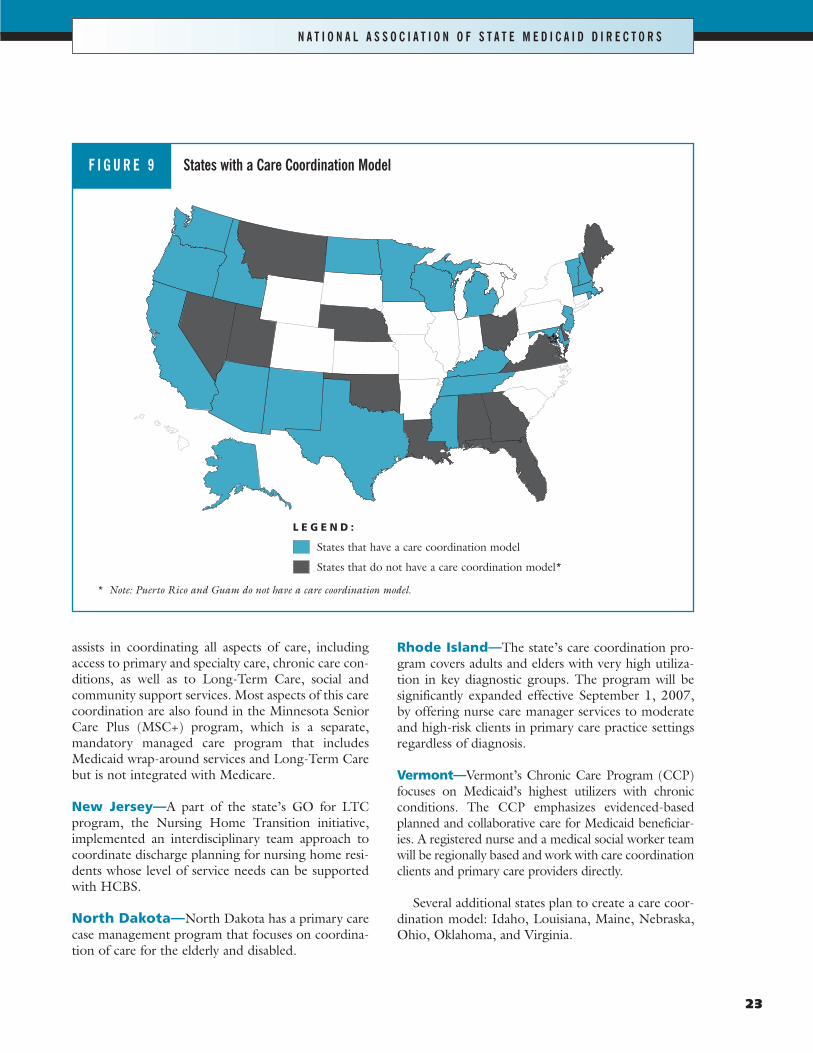
One of the strongest trends identified in this sur-vey was the use of care coordination to assist in theimprovement and integration of care. At this time, atleast 21 states have created some form of a care coor-dination model. The goal of these models is toimprove and integrate care and each state has adopt-ed unique features to cater to states individual needs.(Figure 9)
Examples of Care Coordination
Arizona—The Arizona model serves people whoare developmentally disabled, physically disabled,and/or elderly and who are at risk of an institutionallevel of care. All members are assigned a case manag-er to assist with the coordination of care. Memberscan move between HCBS and institutional settings asneeded. The only restriction on HCBS is that the costof care must be no more than the Medicaid cost ofinstitutional care.
California—California will provide care coordina-tion for individuals with chronic conditions who areseriously ill. The goal of the state’s new program is toenhance the coordination of care, improve healthoutcomes, and decrease the long-term costs of chron-ically ill populations by using a holistic approach.Interventions will include intensive case managementand Disease Management strategies including: refer-rals to improve mobility and provide needed financialand social support, disease self-management educa-tion, development of individualized care plans usingevidence-based practice guidelines, and promotion ofthe use of disease/patient registries to share data.
Idaho—The 2006 Idaho legislature directed theDepartment of Health and Welfare to increase itscoordination with Medicare as part of the overallstrategy for improving Medicaid efficiency and saving
Medicaid funds. The Idaho benefit package coordi-nates and integrates benefits for individuals eligiblefor both Medicare and Medicaid. It is one of thethree benefit packages that comprise Idaho’sMedicaid Modernization plan. Individuals who optinto the Medicare/Medicaid Coordinated Plan willreceive an integrated benefits program offered by aparticipating Medicare Advantage Organization(MAO). Medicaid will pay the premium for the inte-grated Medicare Advantage Plan offered by a partici-pating MAO. The integrated Medicare AdvantagePlan will cover some services usually covered byMedicaid, such as primary care case management,prescribed drugs not covered by Medicare Part D,and dentures.
Kentucky—Kentucky’s plan focuses on combiningthe efforts of the private sector, universities, pro-viders, and others to support the overall care coordi-nation and utilization of supplies and services. Pilot,disease-specific programs have been established in theareas of Pediatric Asthma, Pediatric Obesity, PediatricDiabetes, Diabetes, COPD/Asthma, Adult Obesity,and Health at Heart initiatives. Currently these arestrictly Disease Management with plans to expandinto a care coordination model.
Maryland—Maryland contracts for care coordina-tion services for individuals in the Rare andExpensive Case Management Program. Care coor-dinators help develop plans of care and ensure thatindividuals receive a wider spectrum of Medicaidcovered services if necessary.
Massachusetts—Massachusetts has a special carecoordination plan for pediatric patients. Under theMassachusetts model, all Medicaid cases for childrenwith complex care are managed by a care coordinator.
Minnesota—The state has a comprehensive carecoordination model for seniors and people with dis-abilities that applies to enrollees in all settings (nurs-ing home, waiver, and other community settingsregardless of level of need). All enrollees are screenedwithin 30 days of enrollment and are assigned a carecoordinator or health service coordinator. The staff
22
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Finding 10—States are Using Care Coordination to Improve and Integrate Care
361185_Lot1_Text_22 11/7/07 5:40 PM Page 22
23
assists in coordinating all aspects of care, includingaccess to primary and specialty care, chronic care con-ditions, as well as to Long-Term Care, social andcommunity support services. Most aspects of this carecoordination are also found in the Minnesota SeniorCare Plus (MSC+) program, which is a separate,mandatory managed care program that includesMedicaid wrap-around services and Long-Term Carebut is not integrated with Medicare.
New Jersey—A part of the state’s GO for LTCprogram, the Nursing Home Transition initiative,implemented an interdisciplinary team approach tocoordinate discharge planning for nursing home resi-dents whose level of service needs can be supportedwith HCBS.
North Dakota—North Dakota has a primary carecase management program that focuses on coordina-tion of care for the elderly and disabled.
Rhode Island—The state’s care coordination pro-gram covers adults and elders with very high utiliza-tion in key diagnostic groups. The program will besignificantly expanded effective September 1, 2007,by offering nurse care manager services to moderateand high-risk clients in primary care practice settingsregardless of diagnosis.
Vermont—Vermont’s Chronic Care Program (CCP)focuses on Medicaid’s highest utilizers with chronicconditions. The CCP emphasizes evidenced-basedplanned and collaborative care for Medicaid beneficiar-ies. A registered nurse and a medical social worker teamwill be regionally based and work with care coordinationclients and primary care providers directly.
Several additional states plan to create a care coor-dination model: Idaho, Louisiana, Maine, Nebraska,Ohio, Oklahoma, and Virginia.
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
* Note: Puerto Rico and Guam do not have a care coordination model.
L E G E N D :
States that have a care coordination model
States that do not have a care coordination model*
States with a Care Coordination ModelF I G U R E 9
361185_Lot1_Text_23 11/7/07 5:40 PM Page 23

24
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
D isease Management (DM) is defined as a sys-tem of coordinated health care interventionsand communications for populations with
conditions in which patient self-care efforts are signif-icant. Chronic diseases such as diabetes, obesity, con-gestive heart failure, and untreated or under-treatedasthma can lead to unnecessary hospitalizationsand/or necessitate the need for Long-Term Care ser-vices. States have begun aggressive campaigns to mon-itor and prevent complications through care thatincludes helping patients to adhere to medication reg-imens to develop healthy lifestyle choices, and to seekregular professional monitoring of their symptoms.
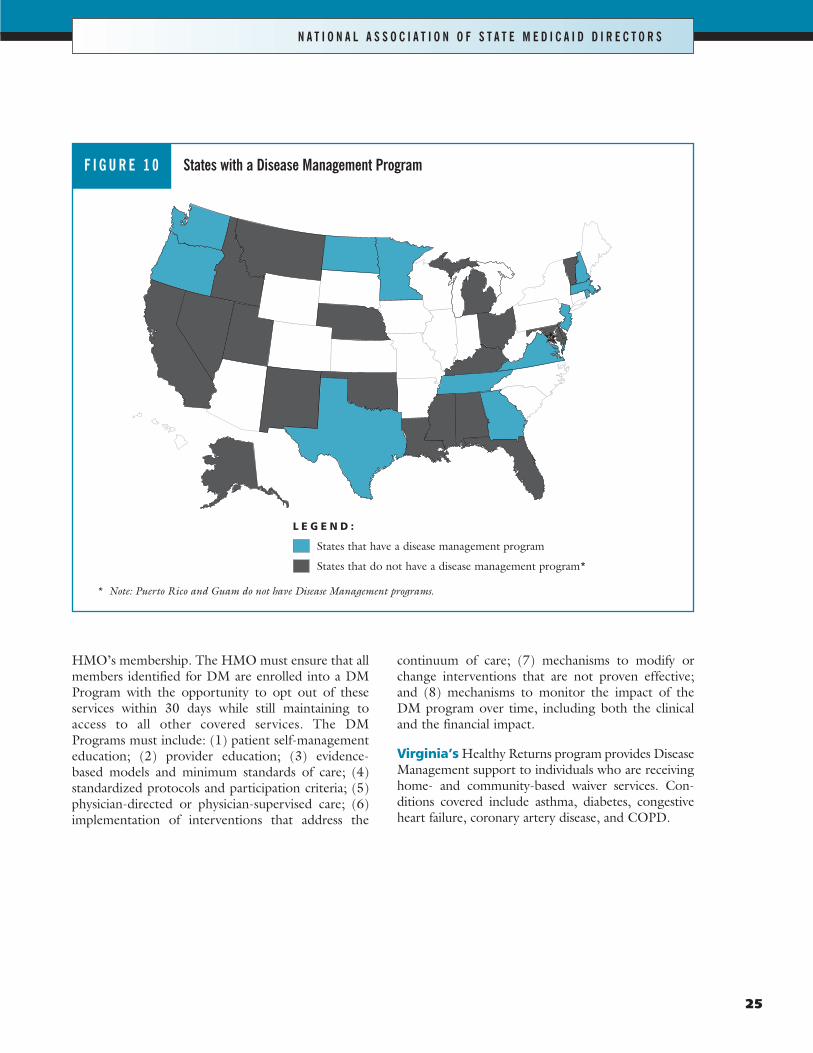
At this time, at least 12 states have DiseaseManagement programs that apply to their Long-Term Care settings, and numerous other states indi-cated that they are developing programs. Some of thestates report limiting their DM progam to partici-pants with certain chronic conditions or certain plans.Several additional states indicated that it was arequirement that the Managed Care plans that theycontract with have Disease Management compo-nents. (Figure 10)
Selected State Disease Management Programs
Idaho’s current Disease Management program tar-gets specific diseases of all participants. Long-TermCare participants receive their Disease Managementservices from their acute care provider even if theyreside in a Long-Term Care setting.
Minnesota’s managed care contracts requireDisease Management Programs for all enrollees. Thestate currently requires Disease Management Pro-grams for diabetes and heart disease.
New Jersey’s Department of Health and SeniorServices was awarded a three-year federal grant(Empowering Older People to Take More Control oftheir Health through Evidence-Based PreventionPrograms). New Jersey was among 16 states selectedto implement low-cost, community-based disease anddisability prevention programs that have proven toreduce the risk of disease and disability among olderadult participants. New Jersey is establishing theChronic Disease Self-Management (CDSM) Pro-gram and Healthy IDEAS (Identifying Depression,Empowering Activities for Seniors) program.
North Dakota will be implementing Disease Man-agement for all Medicaid recipients that have asthma,diabetes, Chronic Obstructive Pulmonary Disease(COPD), and Chronic Heart Failure (CHF).
Tennessee’s Disease Management is applied acrossthe board to its entire Medicaid population, includingthose who receive Long-Term Care services.
Texas HMOs must provide, or arrange to have pro-vided to members, comprehensive Disease Manage-ment services consistent with state statutes and regu-lations. Such Disease Management services must bepart of a person-based approach to DM and holisti-cally address the needs of persons with multiplechronic conditions. HMOs must develop and main-tain screening and evaluation procedures for the earlydetection, prevention, treatment, or referral of partic-ipants at risk for or diagnosed with chronic conditionssuch as asthma, diabetes, chronic obstructive pul-monary disease, congestive heart failure, coronaryartery disease, or other chronic diseases based uponan evaluation of the prevalence of a disease within the
Finding 11—More States Using Disease Management toHelp Manage Chronic Conditions
361185_Lot1_Text_24 11/7/07 5:40 PM Page 24
25
HMO’s membership. The HMO must ensure that allmembers identified for DM are enrolled into a DMProgram with the opportunity to opt out of theseservices within 30 days while still maintaining toaccess to all other covered services. The DMPrograms must include: (1) patient self-managementeducation; (2) provider education; (3) evidence-based models and minimum standards of care; (4)standardized protocols and participation criteria; (5)physician-directed or physician-supervised care; (6)implementation of interventions that address the
continuum of care; (7) mechanisms to modify orchange interventions that are not proven effective;and (8) mechanisms to monitor the impact of theDM program over time, including both the clinicaland the financial impact.
Virginia’s Healthy Returns program provides DiseaseManagement support to individuals who are receivinghome- and community-based waiver services. Con-ditions covered include asthma, diabetes, congestiveheart failure, coronary artery disease, and COPD.
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
* Note: Puerto Rico and Guam do not have Disease Management programs.
L E G E N D :
States that have a disease management program
States that do not have a disease management program*
States with a Disease Management ProgramF I G U R E 1 0
361185_Lot1_Text_25 11/7/07 5:40 PM Page 25
26
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
I n the 1980s, the Robert Wood Johnson Found-ation (RWJF) provided grants to states to sup-port the development of a unique insurance
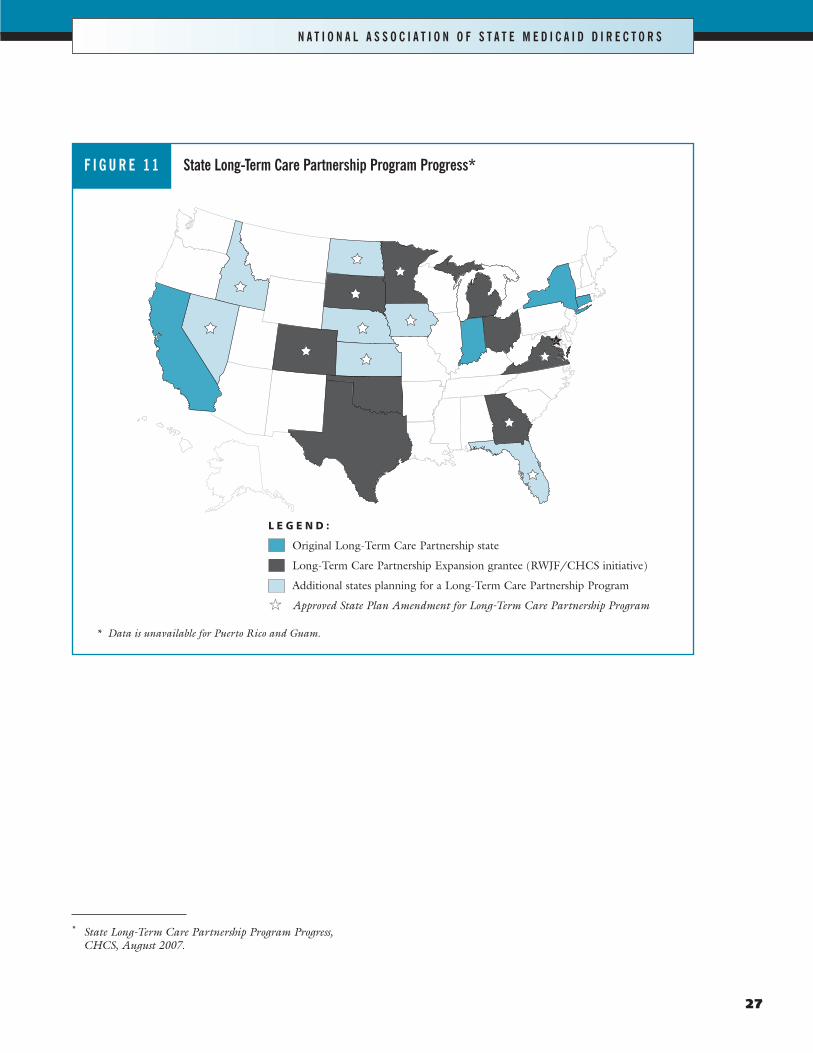
model that encourages consumers to purchase Long-Term Care insurance. The program allows states topromote the purchase of LTC insurance by offeringaccess to Medicaid under special eligibility rulesshould additional LTC coverage (beyond the terms inthe LTC insurance contract) be needed. The originaldemonstration model has been underway since 1992in California, Connecticut, Indiana, and New York.The Deficit Reduction Act lifted the technical barri-ers Congress had imposed on such programs, allow-ing for the expansion of the LTCPP to other states.11
The DRA requires programs to include certainconsumer protections and requires that policiesinclude inflation protection when purchased by a per-son under age 76.
The LTCPP was designed to attract consumerswho might not otherwise purchase LTC insurance.States offer the guarantee that if benefits under aLTCPP policy do not sufficiently cover the cost ofcare, the consumer may qualify for Medicaid underspecial eligibility rules while retaining a pre-specifiedamount of assets. Consumers are protected from hav-ing to become impoverished to qualify for Medicaid,and states avoid the burden of Long-Term Care.
According to the Center for Health Care Stra-tegies, 17 states are currently making efforts towardPartnership program implementation. Of the 17states, 12 states already have approved state planamendments.12 (Figure 11)
Finding 12—Many States are Using the New Option onLong-Term Care Partnership Programs
11 Long-Term Care Partnership Expansion: A NewOpportunity for States, CHCS, NASMD, and GeorgeMason University, May 2007
12 http://www.rwjf.org/programareas/resources/product.jsp?id=18647&pid=1144
361185_Lot1_Text_26 11/7/07 5:40 PM Page 26
27
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
* State Long-Term Care Partnership Program Progress,CHCS, August 2007.
L E G E N D :
Original Long-Term Care Partnership state
Long-Term Care Partnership Expansion grantee (RWJF/CHCS initiative)
Additional states planning for a Long-Term Care Partnership Program
�� Approved State Plan Amendment for Long-Term Care Partnership Program
* Data is unavailable for Puerto Rico and Guam.
State Long-Term Care Partnership Program Progress*F I G U R E 1 1
361185_Lot1_Text_27 11/8/07 9:03 PM Page 27

A t this time four states have adopted a DRAbenchmark benefit package for Long-TermCare services. Idaho and Kentucky provided
comprehensive Long-Term Care reform benefit pack-ages while Virginia and Washington provided DiseaseManagement.
Alternative Benefit Packages under theDeficit Reduction Act
Section 6044 of the Deficit Reduction Act providesstates with the flexibility to change their Medicaidbenefit packages without regard to traditionalrequirements such as statewideness, comparability,freedom of choice, or certain other traditional Med-icaid requirements. Certain groups are protectedfrom changes under the benchmark benefit packages.States may use these packages for alternative benefits,such as providing Disease Management Services orother services to members on a voluntary basis.13
Some of the reasons states cited for not consider-ing using the DRA benchmark benefit packagesinclude other Long-Term Care priorities; the needfor legislative approval before making such a change;the limited availability for populations; and in certainjurisdictions Long-Term Care is not covered and thefunds are not available to add it. In addition, there isa limited understanding of how to use the newbenchmark flexibilities under the DRA.
Idaho’s Medicaid reform initiative used the DRAbenchmark benefit flexibilities and divided the stateprogram into three programs, including one for chil-dren and working age adults, one for individuals withdisabilities, and one for individuals on both Medicaidand Medicare. Idaho’s reform initiative sought toencourage preventive treatment but also providingadditional tailored benefits to individuals with disabil-ities and the elderly. The programs for the disabledand elderly included enhanced services such as pri-mary care case management, dental, vision, trans-portation, extensive mental health services, services
for individuals with developmental disabilities, andtargeted case management.
Kentucky’s current KYHealth Choices includesfour benchmark programs to cover all populationsand existing services within the state of Kentucky.
� Global Choices covers the general Medicaid pop-ulation;
� Family Choices covers most children, includingthe Kentucky Children’s Health InsuranceProgram (KCHIP) population;
� Optimum Choices covers Intermediate Care Fa-cility for the Mentally Retarded (ICF/MR) levelof care individuals with mental retardation anddevelopment disabilities, including those in theSupports for Community Living (SCL) waiver;
� Comprehensive Choices covers nursing facilitylevel of care individuals who are disabled, includ-ing those in the Acquired Brain Injury, Home-and Community-Based, and Model II (VentilatorDependent) waivers.
Optimum Choices and Comprehensive Choicesunder the new Kentucky plan cover Long-Term Careservices. The entire Kentucky Medicaid redesign wasstructured to ensure a continuum of care that maxi-mizes the use of services provided at home.14
Virginia and Washington have SPAs under the newDRA benchmark benefit package design to tailorDisease Management Programs. Washington submit-ted a request to offer regular Medicaid services plusDisease Management Services to adult Medicaidrecipients with complex medical needs who are diag-nosed with certain chronic medical conditions,including diabetes, heart failure, coronary artery dis-ease, cerebrovascular disease, renal failure, and chron-ic pain associated with musculoskeletal conditionsand other chronic illness. According to theWashington SPA approval notification, the bench-mark services will benefit Medicaid recipients in thefollowing ways:
28
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Finding 13—Benchmark Benefit Packages are not Widely Used for Long-Term Care services
13 For additional information, see www.cms.hhs.gov. 14 For additional information on the KYHealth Choices, seehttp://chfs.ky.gov/NR/rdonlyres/70AC8C04-BDEF-4A64-AB06-45FEE8285A04/0/1115waiver.pdf.
361185_Lot1_Text_28 11/7/07 5:40 PM Page 28

29
� Assist individuals in locating a medical home pri-mary care provider (PCP) and learning to use thePCP appropriately;
� Increase the ability of individuals to follow theirprovider’s prescribed plan of care and to play amore proactive role in their own health carethrough education about their chronic conditions,and helping them to become more efficient con-sumers of the health care system;
� Support primary care providers by providing theirpatients with chronic conditions access to nursehelp lines and referrals for needed services; and
� Provide feedback from patients about their healthactivities to the primary care providers to helpfacilitate changes to a patient’s plan of care.
Beneficiaries in the Washington plan will receive thefollowing additional benefits: education about their
specific condition; access to a nurse call line; regular-ly scheduled telephone calls providing health caremanagement and support; and care coordination,including feedback to the primary care physician.
Virginia’s Healthy Returns Benchmark BenefitSPA was approved in March 2007 and providesMedicaid recipients with asthma, congestive heartfailure, coronary artery disease, and/or diabetes anadditional set of services. All Medicaid enrollees areeligible to participate in the Healthy Returns initiativeexcept those who are enrolled in managed care, aredual eligibles, live in institutional settings, or whohave third party insurance. The program will providerecipients with condition-specific education, access toa 24-hour nurse call line, regularly scheduled tele-phone calls with health support, and care coordina-tion to the primary care physician. Virginia is hopingto enroll 25,000 participants in the program.
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
361185_Lot1_Text_29 11/7/07 5:40 PM Page 29

361185_Lot1_Text_30 11/7/07 5:40 PM Page 30
31
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
T his report provides a detailed snapshot of stateactions in Medicaid Long-Term Care duringthe late summer of 2007. As states gain expe-
rience using the Deficit Reduction Act (DRA, P.L.109-171) provisions, this document will help policy-makers and Medicaid stakeholders assess the impactof this landmark legislation on state Long-Term Carepolicies and practices.
The Deficit Reduction Act made several majorchanges to Long-Term Care services in both howstates can provide the services and who is eligible forthose services. States were required to tighten theireligibility rules to the Medicaid program by changingthe penalties, changing the methodologies for count-ing assets, and excluding individuals with higherhome equities from coverage. By tightening the eligi-bility rules, both states and the federal governmenthope to ensure that those individuals who are eligibleare enrolled and cared for under the Medicaid pro-gram. However, the states and federal governmentalso have an interest in ensuring that those who havedivested their assets in the past in order to qualify forthe program are no longer able to do so.
The DRA also created a series of opportunities forstates to encourage more home- and community-based opportunities for individuals with disabilitiesand illness. Through the Money Follows the PersonDemonstration programs and the cash and counsel-ing state plan option, states will continue to expandtheir efforts to move individuals out of institutions.As the federal grant dollars disappear over the nextyear or two, one policy question already being debat-ed is, will the states have the funding and infrastruc-ture necessary to keep individuals who desire toremain in their communities after the federal demon-stration funding is no longer available.
The DRA also offered states the opportunity topromote the purchase of LTC insurance by offeringaccess to Medicaid under special eligibility rulesshould additional LTC coverage (beyond the terms inthe LTC insurance contract) be needed. Many statesalready have taken up the opportunity to offer thisprogram, with still more states planning to do so in2008. Whether or not this program can keep individ-uals off of the Medicaid program for longer, howev-er, remains in question.
Another significant finding of the report was thenumber of states working on preventing the need forLTC services through the use of aggressive care coor-dination programs and Disease Management strate-gies. The outcome of these efforts will not be knownfor years, but early indications are that they canimprove outcomes for patients while also saving theprograms money.
It is too soon to assess the impact that the DRAhad on Long-Term Care reforms and the Medicaidprograms. Many states are still interpreting the guid-ance from CMS and trying to determine what itmeans for their individual state and what initiativesthey will take. A tightening of some of the states’budgets may also stall efforts to develop comprehen-sive Long-Term Care strategy.
Finally, as Congressional leaders signal their will-ingness to reform additional areas of Long-TermCare in the Medicaid programs, Medicaid directorsand state policymakers will be interested in the direc-tion that Congressional leaders take. The Presidentialrace also will likely enter into the debate as many ofthe candidates have indicated that health care reformwill top their agendas.
Policy and Practice Outlook
361185_Lot1_Text_31 11/7/07 5:40 PM Page 31

361185_Lot1_Text_32 11/7/07 5:40 PM Page 32

33
Activities of Daily Living (ADLs)Basic personal activities, which include bathing,dressing, transferring from bed to chair, toilet assis-tance, mobility, and eating. ADLs are used to meas-ure how dependent a person may be on requiringassistance in performing any or all of these activities.15
Asset Transfers RequirementRequires states to lengthen the look-back period forasset transfers to establish Medicaid eligibility fornursing home coverage from three to five years andchanges the start of the penalty from the date of thetransfer to the date of Medicaid eligibility; requiresannuities to be disclosed and states to be named abeneficiary for cost of Medicaid assistance; requiresstate to use the income-first rule; and excludes cover-age for individuals with home equity in excess of$500,000 (or up to $750,000 at state option), withan exception when a spouse or child with a disabilityis residing in the home.16
Care CoordinationThe goal of care coordination is to improve and inte-grate the care while reducing the unnecessary con-sumption of services. Some models focus more on themedical care and are often created for certain popula-tions while other models combine both the medicaland Long-Term Care needs; others focus on screen-ing and care planning.
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
15 (Clearinghouse for the Community Living ExchangeCollaborative glossary, http://www.hcbs.org/glossary.php)
16 (Kaiser Family Foundation: Medicaid/SCHIP: Long TermCare Medicaid Long-Term Services Reforms in the DeficitReduction Act, 2006, http://www.kff.org/medicaid/7486.cfm)
Cash and CounselingA program that gives elderly and disabled Medicaidconsumers who receive personal assistance servicesthe option of directing their own care. These servicesinclude help with everyday needs like bathing, dress-ing, grooming, cooking, and housekeeping.Traditionally, state Medicaid programs have contract-ed with home care agencies to provide these services.Although consumers may choose from among avail-able agencies, they often have little say in who willprovide these very personal services. By redirectingpersonal assistance funds from agencies to consumersthemselves, Cash and Counseling allows people tohire whomever they want to provide their care anddecide for themselves if they would rather purchase amicrowave oven to heat up their meals or hire an aideto cook for them.17
Cash and Counseling does not increase states’Medicaid costs if people receive the care to whichthey are entitled under the traditional system. Thisconclusion is based on the findings of the evaluationof the original Cash and Counseling Demonstrationand Evaluation programs in Arkansas, Florida, andNew Jersey. Cash and Counseling intends to increaseconsumer satisfaction, quality, and efficiency in theprovision of personal assistance services.
Consumer ChoiceThis is provided when there is a range of serviceoptions to meet the diverse needs of consumers. Thedegree to which consumers have choice must gobeyond the range of service choices and includeopportunities for consumers to decide when andwhere services will be provided, and how and bywhom tasks will be performed.18
17 (C&C FAQs available at http://www.cashandcounseling.org/about/FAQ)
18 (Clearinghouse for the Community Living ExchangeCollaborative glossary, http://www.hcbs.org/glossary.php)
Glossary
361185_Lot1_Text_33 11/7/07 5:41 PM Page 33

34
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Consumer-Directed ProgramsConsumers can decide which services to use, whichworkers to hire, and what time of day they will come.They can decide whether to hire family members andwhether to spend the available funds on things otherthan services (like appliances or home modifications).In some consumer-directed programs, consumers paytheir workers themselves; in others, consumerschoose to have an “intermediary service organiza-tion” handle payments.19
DRA Annuity RequirementsApplicants must disclose to the state any interest theapplicant or spouse has in the annuity; the state mustbe named as remainder beneficiary if the applicant orspouse is the annuitant; new provisions for the treat-ment of the purchase of certain annuities as a transferfor less than fair market value.20
Disability“With respect to an individual, (A) a physical or men-tal impairment that substantially limits one or more ofthe major life activities of such individual; (B) arecord of such impairment; or (C) being regarded ashaving an impairment.” (ADA, 42 USC 12102)“The phrase physical impairment includes but is notlimited to … orthopedic, visual, speech, and hearingimpairments, cerebral palsy, epilepsy, muscular dys-trophy, multiple sclerosis, cancer, heart disease, dia-betes, mental retardation, emotional illness, specificlearning disabilities, HIV disease (whether sympto-matic or asymptomatic), tuberculosis, drug addiction,and alcoholism… The phrase ‘major life activities’means functions such as caring for one’s self, per-forming manual tasks, walking, seeing, hearing,speaking, breathing, learning, and working” (ADAHandbook, pp. II-16 through II-19).21
19 (Clearinghouse for the Community Living ExchangeCollaborative glossary, http://www.hcbs.org/glossary.php)
20 (CMS State Medicaid Director Letter, July 27, 2006:Transfer of Assets,http://www.cms.hhs.gov/SMDL/SMD/itemdetail.asp?filterType=dual,%20date&filterValue=2|yyyy&filterByDID=1&sortByDID=1&sortOrder=ascending&itemID=CMS1184961&intNumPerPage=10)
21 (Clearinghouse for the Community Living ExchangeCollaborative glossary, http://www.hcbs.org/glossary.php)
Disease ManagementDisease Management is defined as a system of coordi-nated health care interventions and communicationsfor populations with conditions in which patient self-care efforts are significant.
Dual EligiblesIndividuals with certain combinations of needs whoenroll in both the state-administered Medicaid pro-gram and the federally administered Medicare pro-gram are referred to as dual eligibles. Currently, dualeligibles (sometimes referred to as “duals”) receiveprescription drugs and most Long-Term Care bene-fits from Medicaid, while they are covered byMedicare for acute benefits such as doctor’s visits andinpatient hospital care.22
Family Opportunity ActCreates a new option for states to extend Medicaid“buy-in” coverage to children with disabilities withfamily income up to 300 percent of poverty.23
FFPFederal Financial Participation.24
Fiscal IntermediariesOrganizations that provide third-party and fourth-party financial services between recipient and pro-viders of a benefit.25
FMAPFederal Medical Assistance Percentage.26
22 (Clearinghouse for the Community Living ExchangeCollaborative glossary, http://www.hcbs.org/glossary.php)
23 (Kaiser Family Foundation, Medicaid/SCHIP: Long-TermCare Medicaid Long-Term Services Reforms in the DeficitReduction Act, 2006, http://www.kff.org/medicaid/7486.cfm)
24 (Clearinghouse for the Community Living ExchangeCollaborative glossary, http://www.hcbs.org/glossary.php)
25 ibid26 ibid
361185_Lot1_Text_34 11/7/07 5:41 PM Page 34
35
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
HCBSHome- and Community-Based Services are servicesor other supports to help people with disabilities of allages to live in the community. Each state has a mix ofprograms and funding sources. The Medicaid pro-gram pays for many of these services in all states.27
Home- and Community-Based WaiversSection 2176 of the Omnibus Reconciliation Act of1987 permits states to offer, under a waiver, a widearray of home- and community-based services that anindividual may need to avoid institutionalization.Regulations to implement the act list the followingservices as home- and community-based services thatmay be offered under the waiver program: case man-agement, homemaker, home health aide, personalcare, adult day health care, habilitation, respite care,and other services.28
Home Equity ProvisionThe DRA imposes a limit of $500,000 on the valueof an individual’s home equity. States may increasethis up to $750,000.29
Income First RuleAs required by the DRA, this is the amount of theinstitutionalized spouse’s income that would be madeavailable to the community spouse before computingthe amount of additional resources that would berequired to bring the community spouse’s income upto the standard.30
27 ibid28 ibid29 (CMS State Medicaid Director Letter, July 27, 2006:
Transfer of Assets, http://www.cms.hhs.gov/SMDL/SMD/itemdetail.asp?filterType=dual,%20date&filterValue=2|yyyy&filterByDID=1&sortByDID=1&sortOrder=ascending&itemID=CMS1184961&intNumPerPage=10)
30 (CMS State Medicaid Director Letter, July 27, 2006:Transfer of Assets, http://www.cms.hhs.gov/SMDL/SMD/itemdetail.asp?filterType=dual,%20date&filterValue=2|yyyy&filterByDID=1&sortByDID=1&sortOrder=ascending&itemID=CMS1184961&intNumPerPage=10)
Level of Care (LOC)Amount of assistance required by consumers, whichmay determine their eligibility for programs and serv-ices. Levels include protective, intermediate, andskilled.31
Long-Term Care (LTC)Range of medical and/or social services designed tohelp people who have disabilities or chronic careneeds. Services may be short- or long-term and maybe provided in a person’s home, in the community, orin residential facilities (e.g., nursing homes or assistedliving facilities).32
Look-Back PeriodThis was lengthened from 36 months to 60 monthsas a result of the DRA.33
Money Follows the PersonDemonstrationAuthorizes the secretary of U.S. HHS to grantcompetitive awards to states to increase the use ofcommunity versus institutional services, and pro-vides for an enhanced federal medical assistancepercentage (FMAP) for 12 months for each persontransitioned from an institution to the communityduring the demonstration period. Eligible partici-pants must have resided in an institution for a peri-od from 6 months to 2 years, as determined by thestate, and states must continue to provide commu-nity services after the demonstration period for aslong as the individual remains on Medicaid and inneed of community services.34
31 (Clearinghouse for the Community Living ExchangeCollaborative glossary, http://www.hcbs.org/glossary.php)
32 ibid33 (CMS State Medicaid Director Letter, July 27, 2006:
Transfer of Assets, http://www.cms.hhs.gov/SMDL/SMD/itemdetail.asp?filterType=dual,%20date&filterValue=2|yyyy&filterByDID=1&sortByDID=1&sortOrder=ascending&itemID=CMS1184961&intNumPerPage=10)
34 (Kaiser Family Foundation, Medicaid/SCHIP: Long-TermCare Medicaid Long-Term Services Reforms in the DeficitReduction Act, 2006, http://www.kff.org/medicaid/7486.cfm)
361185_Lot1_Text_35 11/7/07 5:41 PM Page 35

36
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
The federal government will pay for 75 to 90 per-cent of the costs of transitioning individuals out ofnursing homes and into the community. The follow-ing states received grants for this demonstration pro-gram: Arkansas, California, Connecticut, Delaware,District of Columbia, Georgia, Hawaii, Illinois,Indiana, Iowa, Kansas, Kentucky, Louisiana, Mary-land, Michigan, Missouri, Nebraska, New Hamp-shire, New Jersey, New York, North Carolina, NorthDakota, Ohio, Oklahoma, Oregon, Pennsylvania,South Carolina, Texas, Virginia, Washington, andWisconsin.35
Partial Month PenaltiesAs a result of the DRA, states must impose partialmonth penalties for transfers that are less than theaverage cost of care for one month.36
Penalty PeriodAs a result of the DRA, the penalty period nowbegins on whichever occurs later of the date of trans-fer or the date the individual would otherwise be eli-gible for Medicaid coverage of Long-Term Care.37
Personal Assistance Services (PAS)Personal Assistance Servics include many differentkinds of assistance to people with disabilities whoneed help with Activities of Daily Living (ADLs) orInstrumental Activities of Daily Living (IADLs).38
35 (CMS, http://www.cms.hhs.gov/DeficitReductionAct/Downloads/MFP_FactSheet.pdf)
36 (CMS State Medicaid Director Letter, July 27, 2006:Transfer of Assets, http://www.cms.hhs.gov/SMDL/SMD/itemdetail.asp?filterType=dual,%20date&filterValue=2|yyyy&filterByDID=1&sortByDID=1&sortOrder=ascending&itemID=CMS1184961&intNumPerPage=10)
37 (CMS State Medicaid Director Letter, July 27, 2006:Transfer of Assets, http://www.cms.hhs.gov/SMDL/SMD/itemdetail.asp?filterType=dual,%20date&filterValue=2|yyyy&filterByDID=1&sortByDID=1&sortOrder=ascending&itemID=CMS1184961&intNumPerPage=10)
38 (Clearinghouse for the Community Living ExchangeCollaborative glossary, http://www.hcbs.org/glossary.php)
Personal CarePersonal care is defined as assistance with activities ofdaily living as well as with self-administration of med-ications and preparation of special diets (also calledcustodial care).39
Service CoordinatorsThese assist consumers to assess their need for servic-es, arrange and coordinate the services, and monitorthe services. Different programs use different terms,including “case managers,” “care managers,” and“service brokers.” Case manager is the term for“service coordinator” used by the Medicaid Programand some state HCBS programs.40
Special Needs Plans (SNPs)SNPs provide an opportunity to integrate care and pro-vide benefits to certain populations that have beenidentified as institutionalized beneficiaries; beneficiarieswho are dually eligible for Medicare and Medicaid; andbeneficiaries with severe or disabling chronic condi-tions. Plans can limit enrollment to one of the specialneeds populations and tailor the benefits and providernetworks to meet the needs of specific groups.
39 (Clearinghouse for the Community Living ExchangeCollaborative glossary, http://www.hcbs.org/glossary.php)
40 ibid
361185_Lot1_Text_36 11/7/07 5:41 PM Page 36

37
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
State Option to Provide HCBS ServicesDRA Section 6086, also known as SSA Section 1915(i),allows states the opportunity to submit a State PlanAmendment (SPA) to provide home- and community-based services for elderly and disabled individuals. Thiscreates a new state option for states to provide all HCBSwaiver services without needing to get a waiver for sen-iors and people with disabilities up to 150 percent ofpoverty; there is no requirement that eligible beneficiar-ies require an institutional level of care. It also requiresstates to establish more stringent eligibility criteria forinstitutional services and permits states to cap enroll-ment, maintain waiting lists, and offer the option with-out providing services statewide.41
Undue HardshipThe DRA requires states to have undue hardship pro-visions that allow the state to waive a penalty periodwhen an individual would be deprived of medical caresuch that his/her life or health would be endangeredor that the individual would be deprived of food,clothing, shelter, or other necessities of life.42
41 (Kaiser Family Foundation, Medicaid/SCHIP: Long-TermCare Medicaid Long-Term Services Reforms in the DeficitReduction Act, 2006, http://www.kff.org/medicaid/7486.cfm)
42 (CMS State Medicaid Director Letter, July 27, 2006:Transfer of Assets, http://www.cms.hhs.gov/SMDL/SMD/itemdetail.asp?filterType=dual,%20date&filterValue=2|yyyy&filterByDID=1&sortByDID=1&sortOrder=ascending&itemID=CMS1184961&intNumPerPage=10)
1915 (c) waiverThe 1915(c) waiver for Medicaid home- and commu-nity-based services waivers that allow states to requestwaivers of certain federal requirements to allow devel-opment of HCBS treatment alternatives to institu-tional care so long as these alternatives cost no morethan it would to provide the same care in an institu-tional setting.43
43 (Clearinghouse for the Community Living ExchangeCollaborative glossary, http://www.hcbs.org/glossary.php)
361185_Lot1_Text_37 11/7/07 5:41 PM Page 37

361185_Lot1_Text_38 11/7/07 5:41 PM Page 38
39
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
References to state laws, regulations,and/or policies regarding implementa-tion of the DRA §6011 (look-back period):AK: 7 AAC 100.510(c)
AR: Supplement 9(b) to attachment 2.6A pages 1 – 7 of the Arkansas State Plan
CT: UPM 3029; five year look back to be phased in
ID: http://adm.idaho.gov/adminrules/rules/idapa16/0305.pdf (IDAPA 16.03.05.833)
KY: 907 KAR 1:650
MA: Regulations revised at 130 CMR 520.019 (B).
MN: Minn. Stat. §256B.0595
NE: 469 NAC 2-009.10B3a
OK: OHCA Policy – http://www.okhca.org/provider/policy/pdflib/chapter35.pdf OAC 317:35-19-20
OR: Oregon Administrative Rule(OAR)461-140-0210
RI: Medicaid Policy 384
TX: TAC Title 1 Part 15 Chapter 358 Subchapter DRule §358.431(B)(i) http://info.sos.state.tx.us/pls/pub/readtac$ext.TacPage?sl=R&app=9&p_dir=&p_rloc=&p_tloc=&p_ploc=&pg=1&p_tac=&ti=1&pt=15&ch=358&rl=431
VT: Rule M440.3(a)
VA: 12VAC30-40-300
WA: Washington Administrative Code 388-513-1363
References to state laws, regulations,and/or policies regarding implementa-tion of DRA §6011 (penalty period):AK: 7 AAC 100.510(g)
AR: Supplement 9(b) to attachment 2.6A pages 1 – 7 of Arkansas State Plan
ID: http://adm.idaho.gov/adminrules/rules/idapa16/0305.pdf (16.03.05.835)
KY: 907 KAR 1:650
MA: Revised regulations revised at 130 CMR520.019 I(3).
MN: Minn. Stat. §256B.0595
NE: 469 NAC 2-009.10B3b
OH: Ohio Administrative Code 5101:1-39-07Medicaid: Transfer of Resources
OK: OHCA Policy – http://www.okhca.org/provider/policy/pdflib/chapter35.pdf OAC 317:35-19-20
OR: OAR 461-140-0296
RI: Medicaid Policy 384
TX: TAC Title 1 Part 15 Chapter 358 Subchapter DRule §358.431(D)(i) http://info.sos.state.tx.us/pls/pub/readtac$ext.TacPage?sl=R&app=9&p_dir=&p_rloc=&p_tloc=&p_ploc=&pg=1&p_tac=&ti=1&pt=15&ch=358&rl=431
VT: Rule M440.41
VA: 12VAC30-40-300
WA: Washington Administrative Code 388-513-1363
APPENDIX A : State Citations on DRA Implementation
361185_Lot1_Text_39 11/7/07 5:41 PM Page 39
References to state laws, regulations,and/or policies regarding implementa-tion of DRA §6016 (partial months ofineligibility):AK: 7 AAC 100.510(e)(3)
AR: Supplement 9 (b) to attachment 2.6A pages 1 – 7 of Arkansas State Plan
CT: UPM 3028; 3029
ID: http://adm.idaho.gov/adminrules/rules/idapa16/0305.pdf (16.03.05.834)
MA: Revised regulations at 130 CMR 520.019 ©(d).
MT: Administrative Rules of Montana 37.82.101
NE: 469 NAC 2-009.10B3b
ND: N.D.A.C. 75-02-02.1-33.1
OH: Ohio Administrative Code 5101:1-39-07Medicaid: Transfer of Resources
OK: OHCA Policy – http://www.okhca.org/provider/policy/pdflib/chapter35.pdf OAC 317:35-19-20
OR: OAR 461-140-0296
RI: Medicaid Policy 384
TX: TAC Title 1 Part 15 Chapter 358 Subchapter DRule §358.431 http://info.sos.state.tx.us/pls/pub/readtac$ext.TacPage?sl=R&app=9&p_dir=&p_rloc=&p_tloc=&p_ploc=&pg=1&p_tac=&ti=1&pt=15&ch=358&rl=431
VA: 12VAC30-40-300
WA: WA Administrative Code 388-513-1364.
References to state laws, regulations,and/or policies regarding implementa-tion of DRA §6016 (accumulating multiple transfers):AK: 7AAC 100.510 (f)
AR: Supplement 9(b) to Attachment 2.6A, pages 1 – 7 of Arkansas State Plan
CT: UPM 3029
DE: DSSM 20350.4
ID: http://adm.idaho.gov/adminrules/rules/idapa16/0305.pdf (16.03.05.835)
MA: Revised regulations at 130 CMR 520.019(G)(2)(i).
MN: Minn. Stat. §256B.0595
MT: ARM 37.82.101 already opted in State Plan
NE: 469 NAC 2-009.10B3b
OH: Ohio Administrative Code 5101:1-39-07Medicaid: Transfer of Resources
OK: OHCA Policy – http://www.okhca.org/provider/policy/pdflib/chapter35.pdf OAC 317:35-19-20
OR: OAR 461-140-0296
RI: Medicaid Policy 384
TX: TAC Title 1 Part 15 Chapter 358 Subchapter DRule §358.431 (I) http://info.sos.state.tx.us/pls/pub/readtac$ext.TacPage?sl=R&app=9&p_dir=&p_rloc=&p_tloc=&p_ploc=&pg=1&p_tac=&ti=1&pt=15&ch=358&rl=431
WA: Washington Administrative Code 388-513-1363
40
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
361185_Lot1_Text_40 11/7/07 5:41 PM Page 40
41
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
References to state laws, regulations,and/or policies regarding implementa-tion of DRA §6016 (purchasing of promissory notes, mortgages, loans):AK: 7 AAC 100.510(k)(10)
AZ: ARS 36-2934.02
AR: Medical Services Policy MS 06-09 dated 10-1-06
CT: Uniform Policy Manual 3029.14
DE: DSSM 20330.3
ID: http://adm.idaho.gov/adminrules/rules/idapa16/0305.pdf (16.03.05.831)
KY: 907 KAR 1:650
MA: Revised regulations at 130 CMR 515.001 (J).
MN: Minn. Stat. §256B.0595
NE: 469 NAC 2-009.07B10
OK: OHCA Policy – http://www.okhca.org/provider/policy/pdflib/chapter35.pdf OAC 317:35-5-45
OR: OAR 461-0145-0330
RI: Medicaid Policy 384
TX: TAC Title 1 Part 15 Chapter 358 Subchapter DRule §358.431 (H) http://info.sos.state.tx.us/pls/pub/readtac$ext.TacPage?sl=R&app=9&p_dir=&p_rloc=&p_tloc=&p_ploc=&pg=1&p_tac=&ti=1&pt=15&ch=358&rl=431
VT: Rule M440.36
VA: 12VAC30-40-300
References to state laws, regulations,and/or policies regarding implementa-tion of DRA §6016 (purchasing of lifeestates):AK: 7 AAC 100.512(c)
AR: Medical Services Policy 06-09 dated 10-1-06
CT: UPM 3029.13
DE: DSSM 20320.2.2
ID: http://adm.idaho.gov/adminrules/rules/idapa16/0305.pdf (16.03.05.247)
KY: 907 KAR 1:585
MA: Revised regulations at 130 CMR 520.019 (I).
MN: Minn. Stat. §256B.0595
NE: 469 NAC 2-009.07B8
OH: Ohio Administrative Code 5101:1-39-32Medicaid: life estates and life leases.
OK: OHCA Policy – http://www.okhca.org/provider/policy/pdflib/chapter35.pdf OAC 317:35-5-41
OR: OAR 461-145-0310
RI: Medicaid Policy 384
TX: TAC Title 1 Part 15 Chapter 358 Subchapter DRule §358.431 (I) http://info.sos.state.tx.us/pls/pub/readtac$ext.TacPage?sl=R&app=9&p_dir=&p_rloc=&p_tloc=&p_ploc=&pg=1&p_tac=&ti=1&pt=15&ch=358&rl=431
VT: Rule M440.32
VA: 12VAC30-40-290
WA: Washington State will be strengthening our regulations, but current regulations allow us todeny these transfers as invalid.
361185_Lot1_Text_41 11/7/07 5:41 PM Page 41
References to state laws, regulations,and/or policies regarding implementa-tion of DRA §6011 (Hardship Waivers):AK: 7 AAC 100.512(c)
AR: Medical Services Policy 06-09 dated 10-1-06
CT: UPM 3029.13
DE: DSSM 20320.2.2
ID: http://adm.idaho.gov/adminrules/rules/idapa16/0305.pdf (16.03.05.247)
KY: 907 KAR 1:585
MA: Revised regulations at 130 CMR 520.019 (I).
MN: Minn. Stat. §256B.0595
NE: 469 NAC 2-009.07B8
OH: Ohio Administrative Code 5101:1-39-32Medicaid: life estates and life leases.
OK: OHCA Policy – http://www.okhca.org/provider/policy/pdflib/chapter35.pdf OAC 317:35-5-41
OR: OAR 461-145-0310
TX: TAC Title 1 Part 15 Chapter 358 Subchapter DRule §358.431 (I) http://info.sos.state.tx.us/pls/pub/readtac$ext.TacPage?sl=R&app=9&p_dir=&p_rloc=&p_tloc=&p_ploc=&pg=1&p_tac=&ti=1&pt=15&ch=358&rl=431
VT: Rule M440.32
VA: 12VAC30-40-290
WA: Washington State will be strengthening our regulations, but current regulations allow us todeny these transfers as invalid.
References to state laws, regulations,and/or policies regarding implementa-tion of DRA §6012 (annuities):AK: 7 AAC100.514(7)
AR: Supplement 9(b)-Attachment 2.6A pages 1 – 7
CT: UPM 3029
DE: DSSM 20330.4.1
ID: http://adm.idaho.gov/adminrules/rules/idapa16/0305.pdf (16.03.05.838)
KY: 907 KAR 1:650
MA: Revised regulations at 130 CMR 515.001(J)(2)(a)(i).
MN: Minn. Stat. §§256B.056 and 256B.0594
NE: 469 NAC 2-009.07A5c(2)
OH: Ohio Administrative code 5101:1-39-22.8
OK: OHCA Policy – http://www.okhca.org/provider/policy/pdflib/chapter35.pdf OAC 317:35-5-41
OR: OAR 461-145-0022
RI: Medicaid Policy 384
TN: Department of Human Services Rules filed asPublic Necessity effective June 1, 2007
TX: TAC Title 1 Part 15 Chapter 358 Subchapter DRule §358.431
VT: Rule M440.34
VA: 12VAC30-40-10
WA: Washington Administrative Code 388-561-200.
42
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
361185_Lot1_Text_42 11/7/07 5:41 PM Page 42
43
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
References to state laws, regulations,and/or policies regarding implementa-tion of DRA §6013 (income first rules):AK: 7 AAC 100.560
CT: UPM 1570.25
ID: http://adm.idaho.gov/adminrules/rules/idapa16/0305.pdf (16.03.05.744)
MA: Regulations at 130 CMR 520.017 (C).
NE: 469 NAC 2-010.01D
OH: 12/01/06 Ohio Administrative Code 5101:1-39-24
OR: OAR 461-160-0580
RI: Medicaid Policy 380
TX: TAC Title 1 Part 15 Chapter 358 Subchapter DRule §358.503 http://info.sos.state.tx.us/pls/pub/readtac$ext.TacPage?sl=R&app=9&p_dir=&p_rloc=&p_tloc=&p_ploc=&pg=1&p_tac=&ti=1&pt=15&ch=358&rl=503
VA: 12VAC30-110-960
WA: Washington Administrative Code 388-513-1325(see also 1315 and 1330) Washington Statealready uses the income first method.
References to state laws, regulations,and/or policies regarding implementa-tion of DRA §6014 (home equity):CT: UPM 4030.20
ID: http://adm.idaho.gov/adminrules/rules/idapa16/0305.pdf (16.03.05.238)
MA: Revised regulations at 130 CMR 515.001 (G) (3).
MT: ARM 37.82.101
NE: 469 NAC 2-009.07B1c
OH: Ohio Administrative Code 5101:39-31
OR: OAR 461-145-0220
RI: Medicaid Policy 384
VT: Rule M233.26
WA: Home Equity in RCW 74.04.005; WashingtonAdministrative Code 388-513-1350
361185_Lot1_Text_43 11/7/07 5:41 PM Page 43
361185_Lot1_Text_44 11/7/07 5:41 PM Page 44
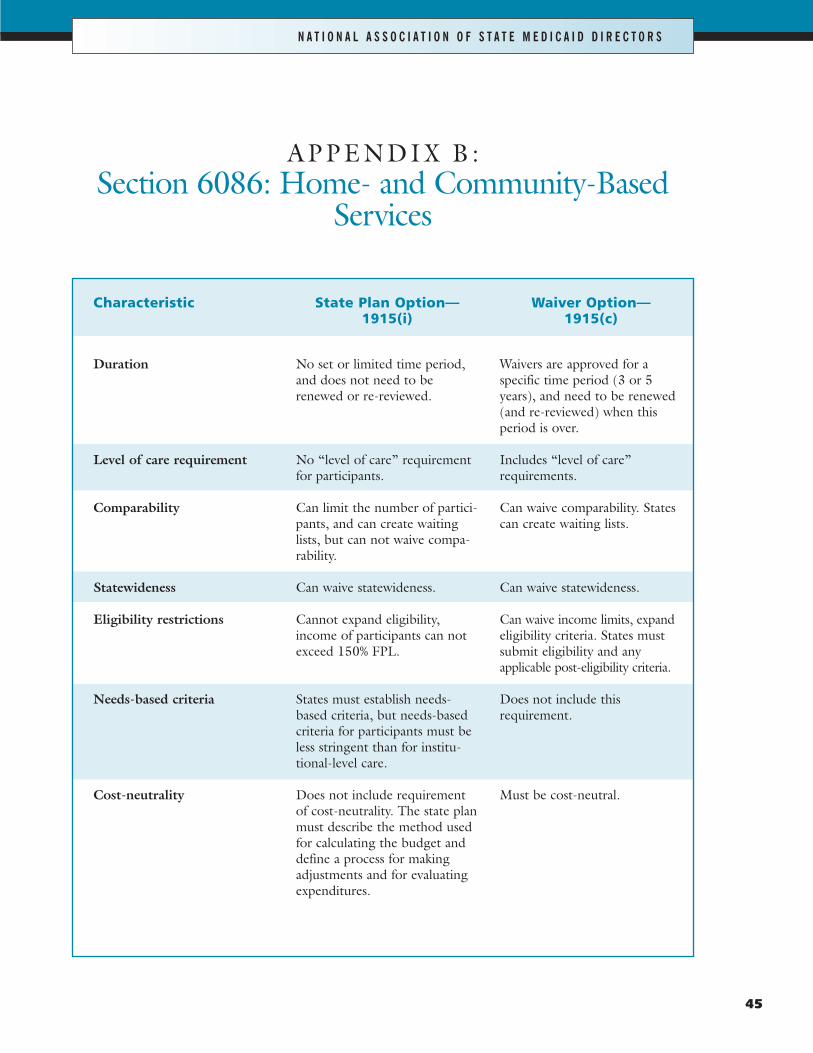
45
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
APPENDIX B : Section 6086: Home- and Community-Based
Services
Characteristic
Duration
Level of care requirement
Comparability
Statewideness
Eligibility restrictions
Needs-based criteria
Cost-neutrality
State Plan Option—1915(i)
No set or limited time period,and does not need to berenewed or re-reviewed.
No “level of care” requirementfor participants.
Can limit the number of partici-pants, and can create waitinglists, but can not waive compa-rability.
Can waive statewideness.
Cannot expand eligibility,income of participants can notexceed 150% FPL.
States must establish needs-based criteria, but needs-basedcriteria for participants must beless stringent than for institu-tional-level care.
Does not include requirementof cost-neutrality. The state planmust describe the method usedfor calculating the budget anddefine a process for makingadjustments and for evaluatingexpenditures.
Waiver Option—1915(c)
Waivers are approved for a specific time period (3 or 5years), and need to be renewed(and re-reviewed) when thisperiod is over.
Includes “level of care” requirements.
Can waive comparability. Statescan create waiting lists.
Can waive statewideness.
Can waive income limits, expandeligibility criteria. States mustsubmit eligibility and any applicable post-eligibility criteria.
Does not include this requirement.
Must be cost-neutral.
361185_Lot1_Text_45 11/7/07 5:41 PM Page 45
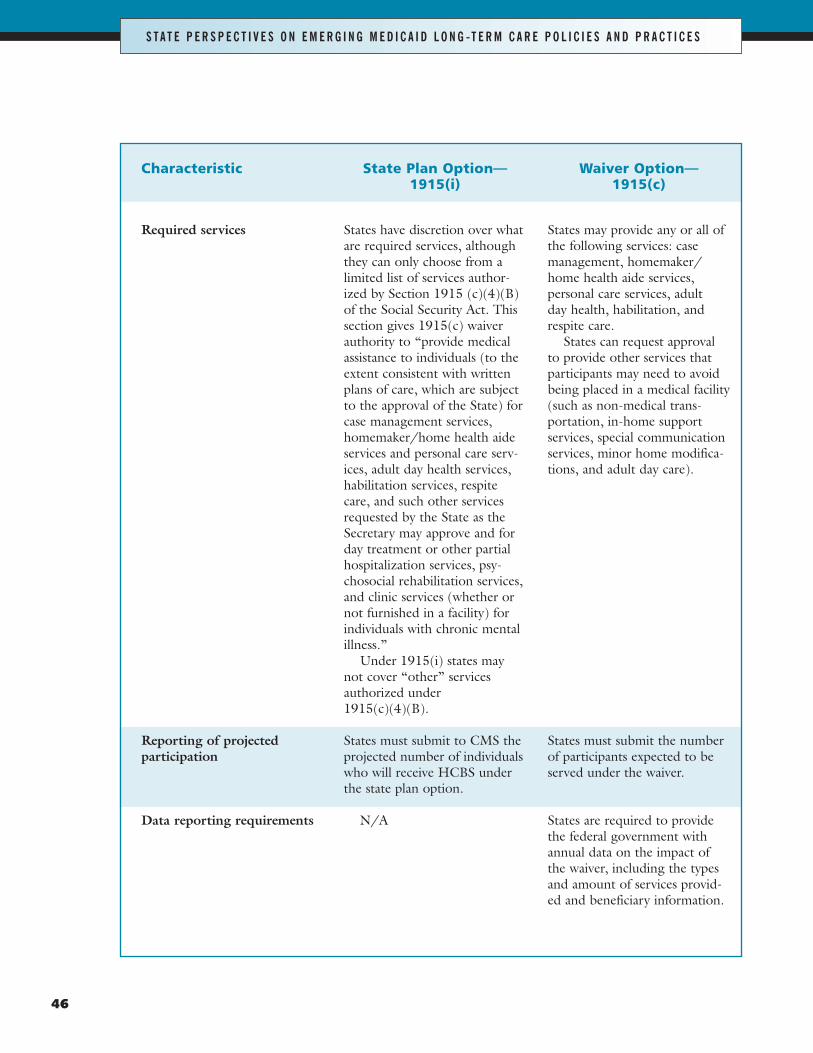
46
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Characteristic
Required services
Reporting of projected participation
Data reporting requirements
State Plan Option—1915(i)
States have discretion over whatare required services, althoughthey can only choose from alimited list of services author-ized by Section 1915 (c)(4)(B)of the Social Security Act. Thissection gives 1915(c) waiverauthority to “provide medicalassistance to individuals (to theextent consistent with writtenplans of care, which are subjectto the approval of the State) forcase management services,homemaker/home health aideservices and personal care serv-ices, adult day health services,habilitation services, respitecare, and such other servicesrequested by the State as theSecretary may approve and forday treatment or other partialhospitalization services, psy-chosocial rehabilitation services,and clinic services (whether ornot furnished in a facility) forindividuals with chronic mentalillness.”
Under 1915(i) states maynot cover “other” servicesauthorized under1915(c)(4)(B).
States must submit to CMS theprojected number of individualswho will receive HCBS underthe state plan option.
N/A
Waiver Option—1915(c)
States may provide any or all ofthe following services: casemanagement, homemaker/home health aide services, personal care services, adult day health, habilitation, andrespite care.
States can request approvalto provide other services thatparticipants may need to avoidbeing placed in a medical facility(such as non-medical trans-portation, in-home supportservices, special communicationservices, minor home modifica-tions, and adult day care).
States must submit the numberof participants expected to beserved under the waiver.
States are required to providethe federal government withannual data on the impact ofthe waiver, including the typesand amount of services provid-ed and beneficiary information.
361185_Lot1_Text_46 11/7/07 5:41 PM Page 46
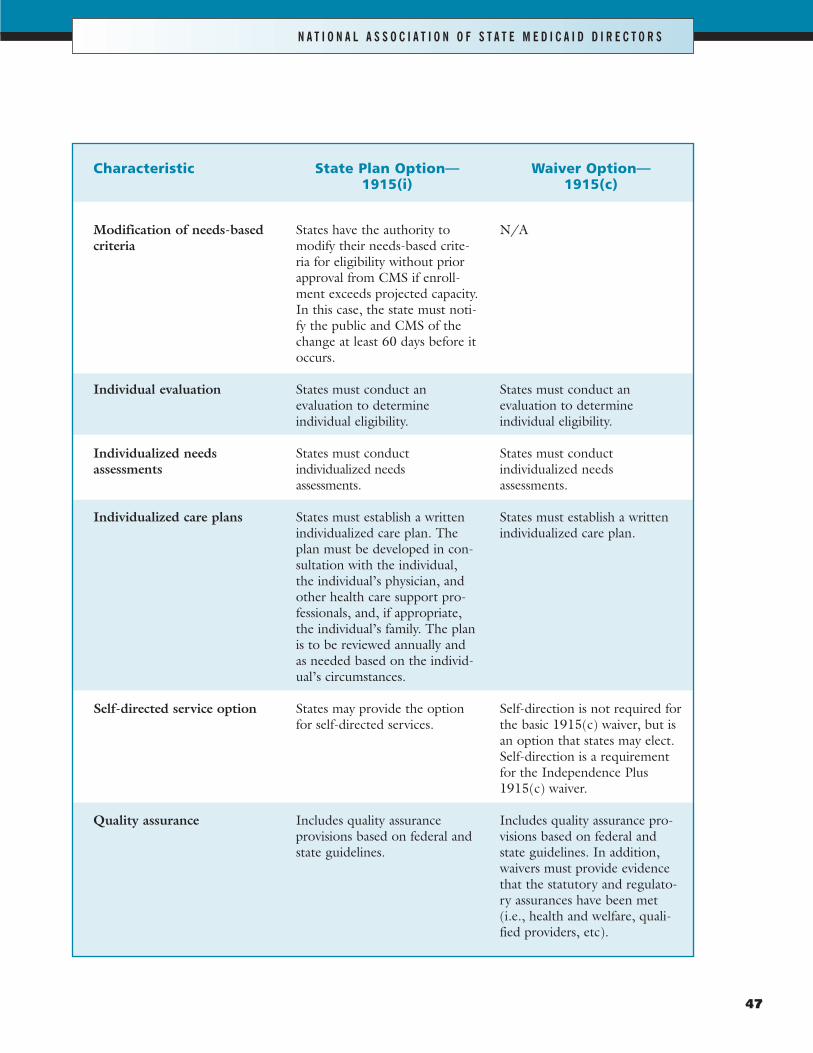
47
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
Characteristic
Modification of needs-based criteria
Individual evaluation
Individualized needsassessments
Individualized care plans
Self-directed service option
Quality assurance
State Plan Option—1915(i)
States have the authority tomodify their needs-based crite-ria for eligibility without priorapproval from CMS if enroll-ment exceeds projected capacity.In this case, the state must noti-fy the public and CMS of thechange at least 60 days before itoccurs.
States must conduct an evaluation to determine individual eligibility.
States must conduct individualized needs assessments.
States must establish a writtenindividualized care plan. Theplan must be developed in con-sultation with the individual,the individual’s physician, andother health care support pro-fessionals, and, if appropriate,the individual’s family. The planis to be reviewed annually andas needed based on the individ-ual’s circumstances.
States may provide the optionfor self-directed services.
Includes quality assurance provisions based on federal andstate guidelines.
Waiver Option—1915(c)
N/A
States must conduct an evaluation to determine individual eligibility.
States must conduct individualized needs assessments.
States must establish a writtenindividualized care plan.
Self-direction is not required forthe basic 1915(c) waiver, but isan option that states may elect.Self-direction is a requirementfor the Independence Plus1915(c) waiver.
Includes quality assurance pro-visions based on federal andstate guidelines. In addition,waivers must provide evidencethat the statutory and regulato-ry assurances have been met(i.e., health and welfare, quali-fied providers, etc).
361185_Lot1_Text_47 11/7/07 5:41 PM Page 47
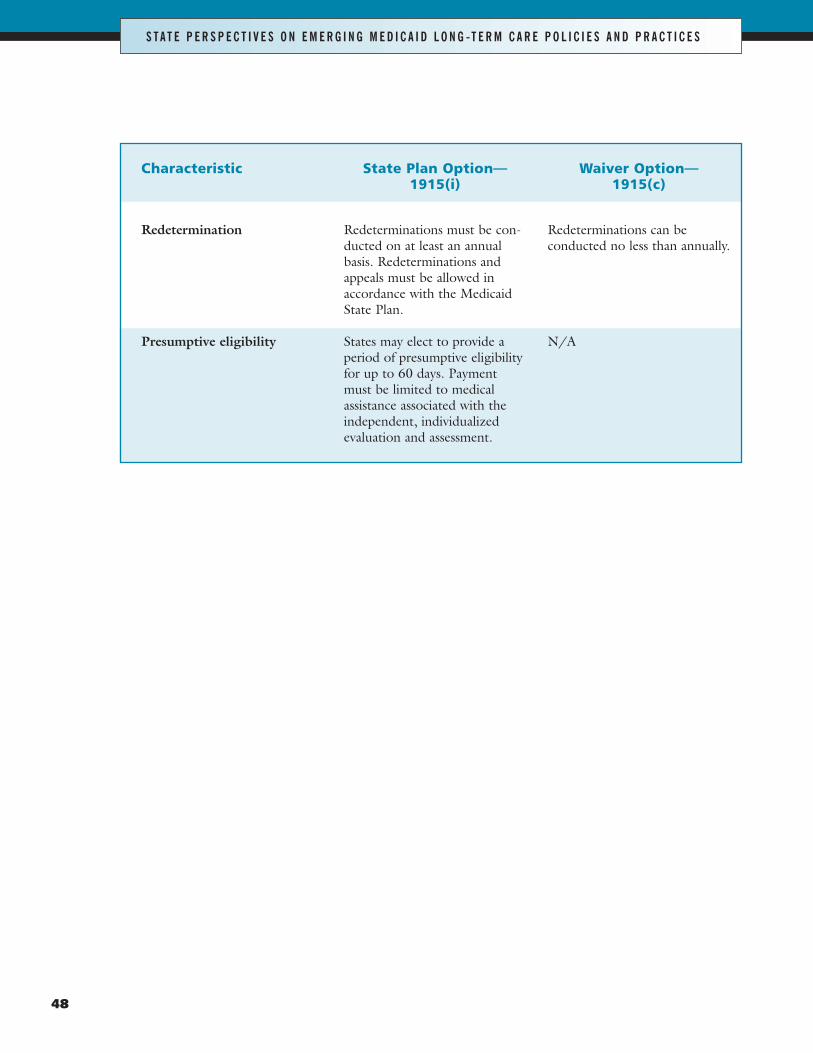
48
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Characteristic
Redetermination
Presumptive eligibility
State Plan Option—1915(i)
Redeterminations must be con-ducted on at least an annualbasis. Redeterminations andappeals must be allowed inaccordance with the MedicaidState Plan.
States may elect to provide aperiod of presumptive eligibilityfor up to 60 days. Paymentmust be limited to medicalassistance associated with theindependent, individualizedevaluation and assessment.
Waiver Option—1915(c)
Redeterminations can be conducted no less than annually.
N/A
361185_Lot1_Text_48 11/7/07 5:41 PM Page 48
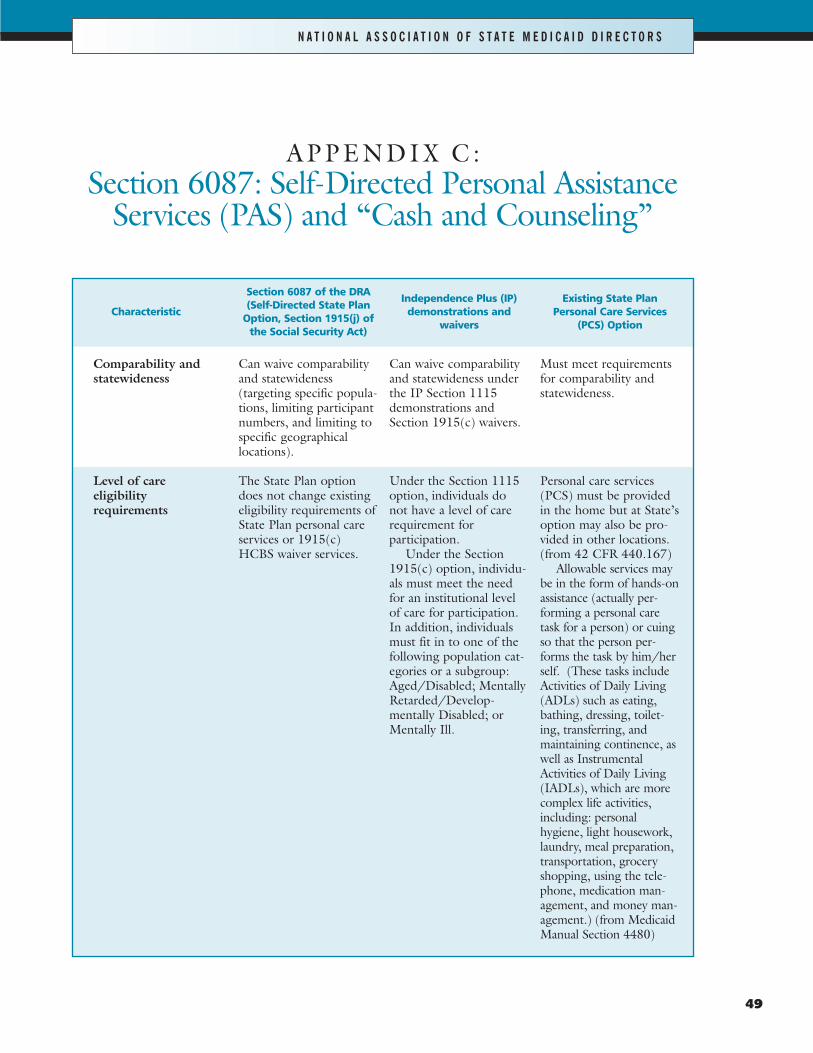
49
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
APPENDIX C: Section 6087: Self-Directed Personal Assistance
Services (PAS) and “Cash and Counseling”
Characteristic
Comparability andstatewideness
Level of care eligibility requirements
Section 6087 of the DRA(Self-Directed State Plan
Option, Section 1915(j) ofthe Social Security Act)
Can waive comparabilityand statewideness (targeting specific popula-tions, limiting participantnumbers, and limiting tospecific geographical locations).
The State Plan optiondoes not change existingeligibility requirements ofState Plan personal careservices or 1915(c)HCBS waiver services.
Independence Plus (IP)demonstrations and
waivers
Can waive comparabilityand statewideness underthe IP Section 1115demonstrations andSection 1915(c) waivers.
Under the Section 1115option, individuals do not have a level of carerequirement for participation.
Under the Section1915(c) option, individu-als must meet the needfor an institutional levelof care for participation.In addition, individualsmust fit in to one of thefollowing population cat-egories or a subgroup:Aged/Disabled; MentallyRetarded/Develop-mentally Disabled; orMentally Ill.
Existing State PlanPersonal Care Services
(PCS) Option
Must meet requirementsfor comparability andstatewideness.
Personal care services(PCS) must be providedin the home but at State’soption may also be pro-vided in other locations.(from 42 CFR 440.167)
Allowable services maybe in the form of hands-onassistance (actually per-forming a personal caretask for a person) or cuingso that the person per-forms the task by him/herself. (These tasks includeActivities of Daily Living(ADLs) such as eating,bathing, dressing, toilet-ing, transferring, andmaintaining continence, aswell as InstrumentalActivities of Daily Living(IADLs), which are morecomplex life activities,including: personalhygiene, light housework,laundry, meal preparation,transportation, groceryshopping, using the tele-phone, medication man-agement, and money man-agement.) (from MedicaidManual Section 4480)
361185_Lot1_Text_49 11/7/07 5:41 PM Page 49
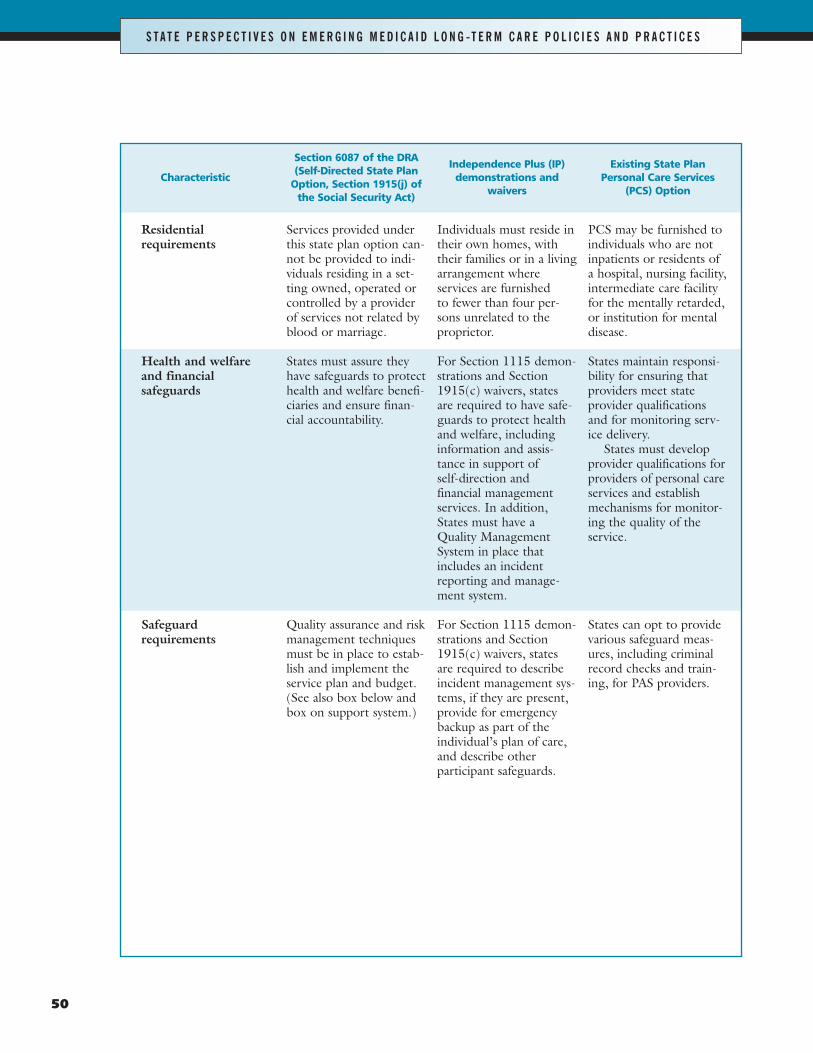
50
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Characteristic
Residential requirements
Health and welfareand financial safeguards
Safeguard requirements
Section 6087 of the DRA(Self-Directed State Plan
Option, Section 1915(j) ofthe Social Security Act)
Services provided underthis state plan option can-not be provided to indi-viduals residing in a set-ting owned, operated orcontrolled by a providerof services not related byblood or marriage.
States must assure theyhave safeguards to protecthealth and welfare benefi-ciaries and ensure finan-cial accountability.
Quality assurance and riskmanagement techniquesmust be in place to estab-lish and implement theservice plan and budget.(See also box below andbox on support system.)
Independence Plus (IP)demonstrations and
waivers
Individuals must reside intheir own homes, withtheir families or in a livingarrangement where services are furnished to fewer than four per-sons unrelated to the proprietor.
For Section 1115 demon-strations and Section1915(c) waivers, statesare required to have safe-guards to protect healthand welfare, includinginformation and assis-tance in support of self-direction and financial managementservices. In addition,States must have aQuality ManagementSystem in place thatincludes an incidentreporting and manage-ment system.
For Section 1115 demon-strations and Section1915(c) waivers, statesare required to describeincident management sys-tems, if they are present,provide for emergencybackup as part of theindividual’s plan of care,and describe other participant safeguards.
Existing State PlanPersonal Care Services
(PCS) Option
PCS may be furnished toindividuals who are notinpatients or residents ofa hospital, nursing facility,intermediate care facilityfor the mentally retarded,or institution for mentaldisease.
States maintain responsi-bility for ensuring thatproviders meet stateprovider qualificationsand for monitoring serv-ice delivery.
States must developprovider qualifications forproviders of personal careservices and establishmechanisms for monitor-ing the quality of theservice.
States can opt to providevarious safeguard meas-ures, including criminalrecord checks and train-ing, for PAS providers.
361185_Lot1_Text_50 11/7/07 5:41 PM Page 50
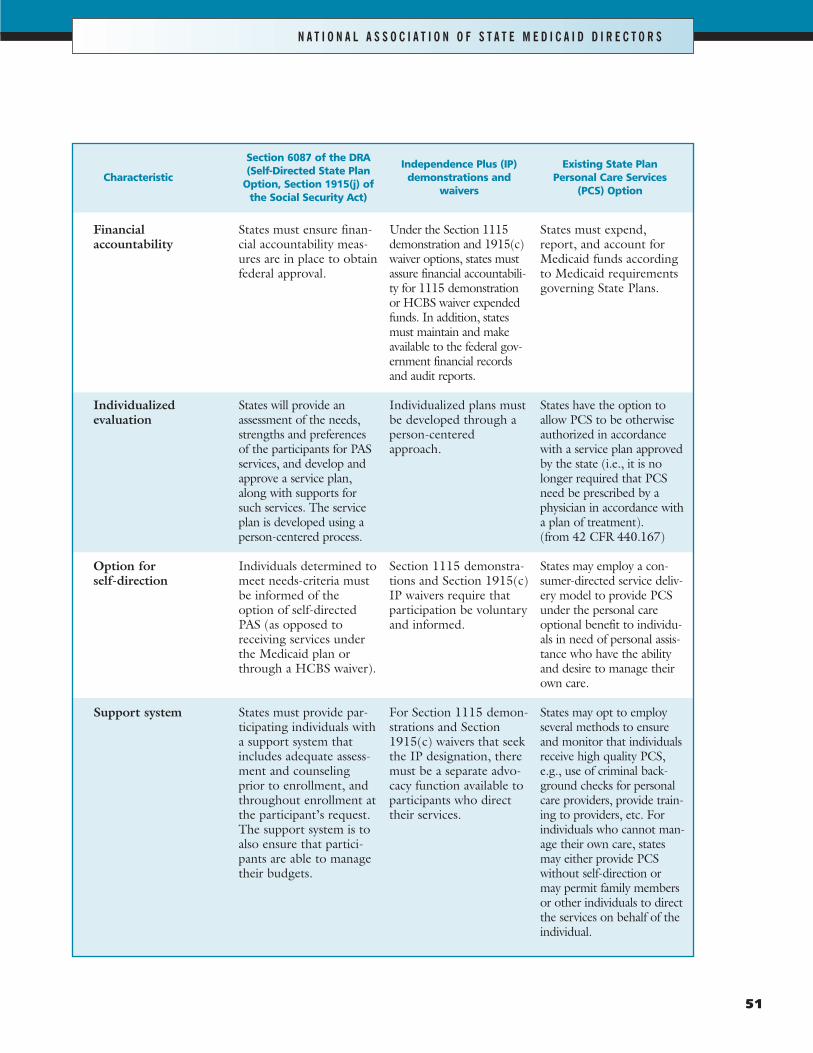
51
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
Characteristic
Financial accountability
Individualized evaluation
Option for self-direction
Support system
Section 6087 of the DRA(Self-Directed State Plan
Option, Section 1915(j) ofthe Social Security Act)
States must ensure finan-cial accountability meas-ures are in place to obtainfederal approval.
States will provide anassessment of the needs,strengths and preferencesof the participants for PASservices, and develop andapprove a service plan,along with supports forsuch services. The serviceplan is developed using aperson-centered process.
Individuals determined tomeet needs-criteria mustbe informed of theoption of self-directedPAS (as opposed toreceiving services underthe Medicaid plan orthrough a HCBS waiver).
States must provide par-ticipating individuals witha support system thatincludes adequate assess-ment and counselingprior to enrollment, andthroughout enrollment atthe participant’s request.The support system is toalso ensure that partici-pants are able to managetheir budgets.
Independence Plus (IP)demonstrations and
waivers
Under the Section 1115demonstration and 1915(c)waiver options, states mustassure financial accountabili-ty for 1115 demonstrationor HCBS waiver expendedfunds. In addition, statesmust maintain and makeavailable to the federal gov-ernment financial recordsand audit reports.
Individualized plans mustbe developed through aperson-centeredapproach.
Section 1115 demonstra-tions and Section 1915(c)IP waivers require thatparticipation be voluntaryand informed.
For Section 1115 demon-strations and Section1915(c) waivers that seekthe IP designation, theremust be a separate advo-cacy function available toparticipants who directtheir services.
Existing State PlanPersonal Care Services
(PCS) Option
States must expend,report, and account forMedicaid funds accordingto Medicaid requirementsgoverning State Plans.
States have the option toallow PCS to be otherwiseauthorized in accordancewith a service plan approvedby the state (i.e., it is nolonger required that PCSneed be prescribed by aphysician in accordance witha plan of treatment). (from 42 CFR 440.167)
States may employ a con-sumer-directed service deliv-ery model to provide PCSunder the personal careoptional benefit to individu-als in need of personal assis-tance who have the abilityand desire to manage theirown care.
States may opt to employseveral methods to ensureand monitor that individualsreceive high quality PCS,e.g., use of criminal back-ground checks for personalcare providers, provide train-ing to providers, etc. Forindividuals who cannot man-age their own care, statesmay either provide PCSwithout self-direction ormay permit family membersor other individuals to directthe services on behalf of theindividual.
361185_Lot1_Text_51 11/7/07 5:41 PM Page 51
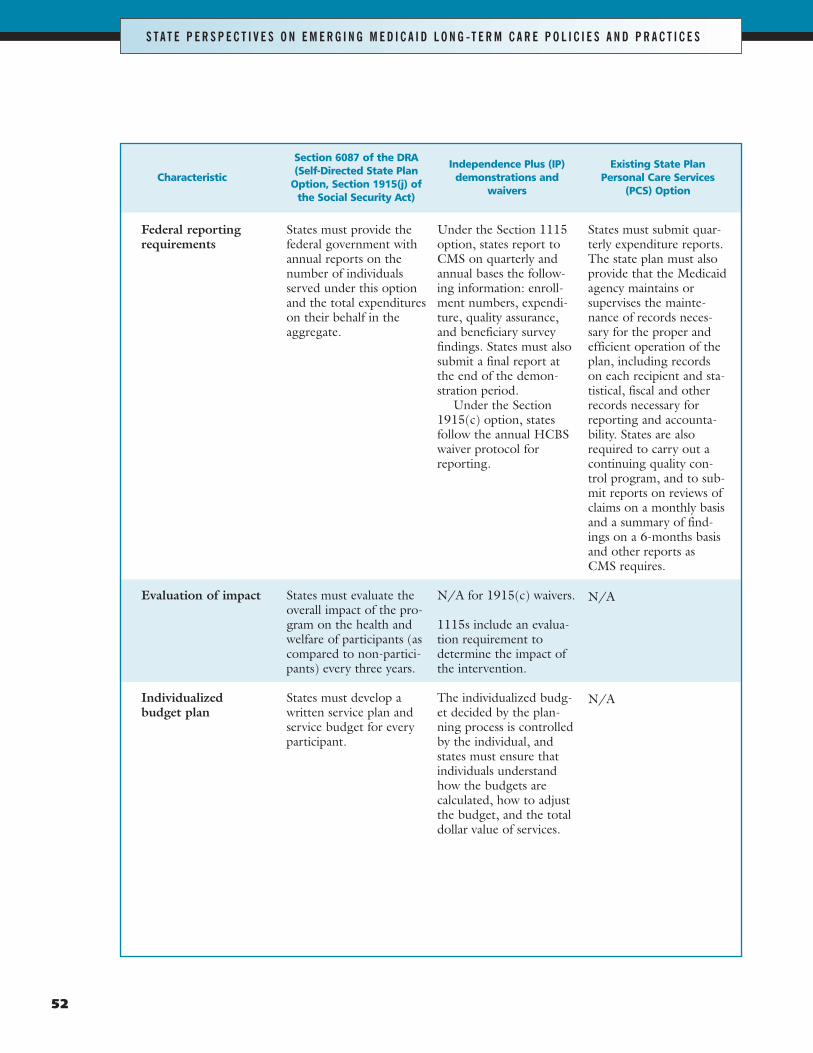
52
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Characteristic
Federal reportingrequirements
Evaluation of impact
Individualized budget plan
Section 6087 of the DRA(Self-Directed State Plan
Option, Section 1915(j) ofthe Social Security Act)
States must provide thefederal government withannual reports on thenumber of individualsserved under this optionand the total expenditureson their behalf in theaggregate.
States must evaluate theoverall impact of the pro-gram on the health andwelfare of participants (ascompared to non-partici-pants) every three years.
States must develop awritten service plan andservice budget for everyparticipant.
Independence Plus (IP)demonstrations and
waivers
Under the Section 1115option, states report toCMS on quarterly andannual bases the follow-ing information: enroll-ment numbers, expendi-ture, quality assurance,and beneficiary surveyfindings. States must alsosubmit a final report atthe end of the demon-stration period.
Under the Section1915(c) option, statesfollow the annual HCBSwaiver protocol forreporting.
N/A for 1915(c) waivers.
1115s include an evalua-tion requirement todetermine the impact ofthe intervention.
The individualized budg-et decided by the plan-ning process is controlledby the individual, andstates must ensure thatindividuals understandhow the budgets are calculated, how to adjustthe budget, and the totaldollar value of services.
Existing State PlanPersonal Care Services
(PCS) Option
States must submit quar-terly expenditure reports.The state plan must alsoprovide that the Medicaidagency maintains orsupervises the mainte-nance of records neces-sary for the proper andefficient operation of theplan, including recordson each recipient and sta-tistical, fiscal and otherrecords necessary forreporting and accounta-bility. States are alsorequired to carry out acontinuing quality con-trol program, and to sub-mit reports on reviews ofclaims on a monthly basisand a summary of find-ings on a 6-months basisand other reports as CMS requires.
N/A
N/A
361185_Lot1_Text_52 11/7/07 5:41 PM Page 52
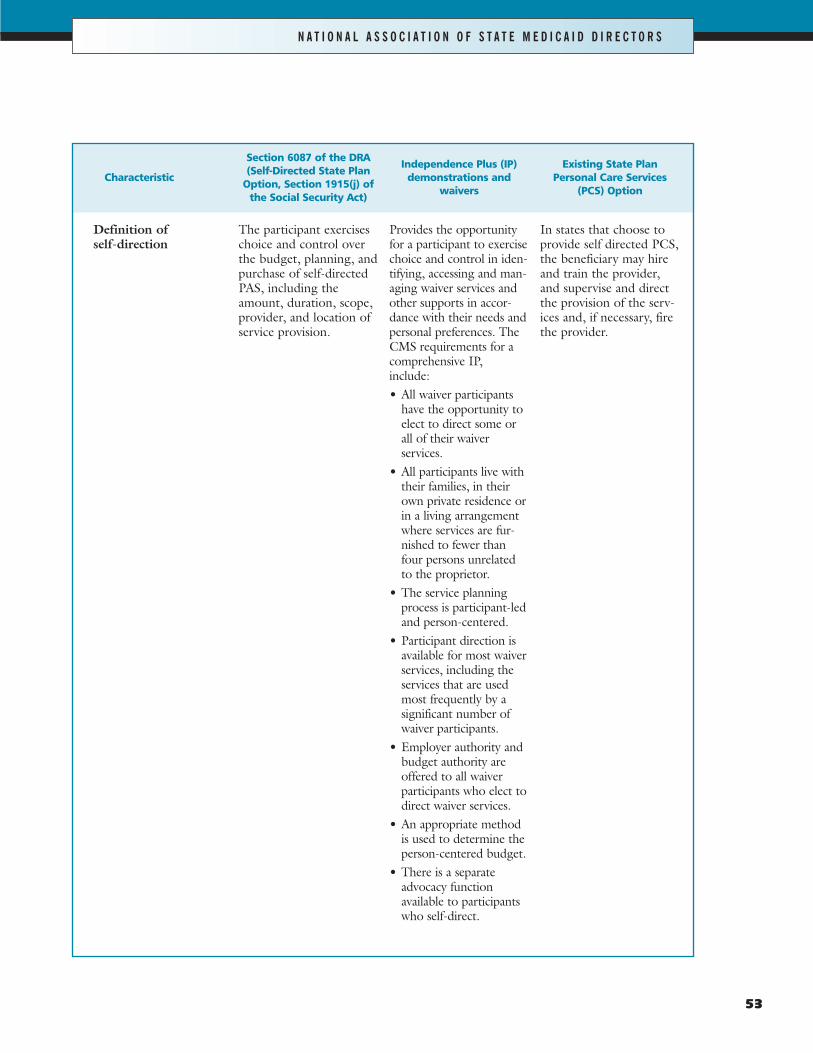
53
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
Characteristic
Definition of self-direction
Section 6087 of the DRA(Self-Directed State Plan
Option, Section 1915(j) ofthe Social Security Act)
The participant exerciseschoice and control overthe budget, planning, andpurchase of self-directedPAS, including theamount, duration, scope,provider, and location ofservice provision.
Independence Plus (IP)demonstrations and
waivers
Provides the opportunityfor a participant to exercisechoice and control in iden-tifying, accessing and man-aging waiver services andother supports in accor-dance with their needs andpersonal preferences. TheCMS requirements for acomprehensive IP,include:• All waiver participants
have the opportunity toelect to direct some orall of their waiver services.
• All participants live withtheir families, in theirown private residence orin a living arrangementwhere services are fur-nished to fewer thanfour persons unrelatedto the proprietor.
• The service planningprocess is participant-ledand person-centered.
• Participant direction isavailable for most waiverservices, including theservices that are usedmost frequently by a significant number ofwaiver participants.
• Employer authority andbudget authority areoffered to all waiver participants who elect todirect waiver services.
• An appropriate methodis used to determine theperson-centered budget.
• There is a separate advocacy function available to participantswho self-direct.
Existing State PlanPersonal Care Services
(PCS) Option
In states that choose toprovide self directed PCS,the beneficiary may hireand train the provider,and supervise and directthe provision of the serv-ices and, if necessary, firethe provider.
361185_Lot1_Text_53 11/7/07 5:41 PM Page 53
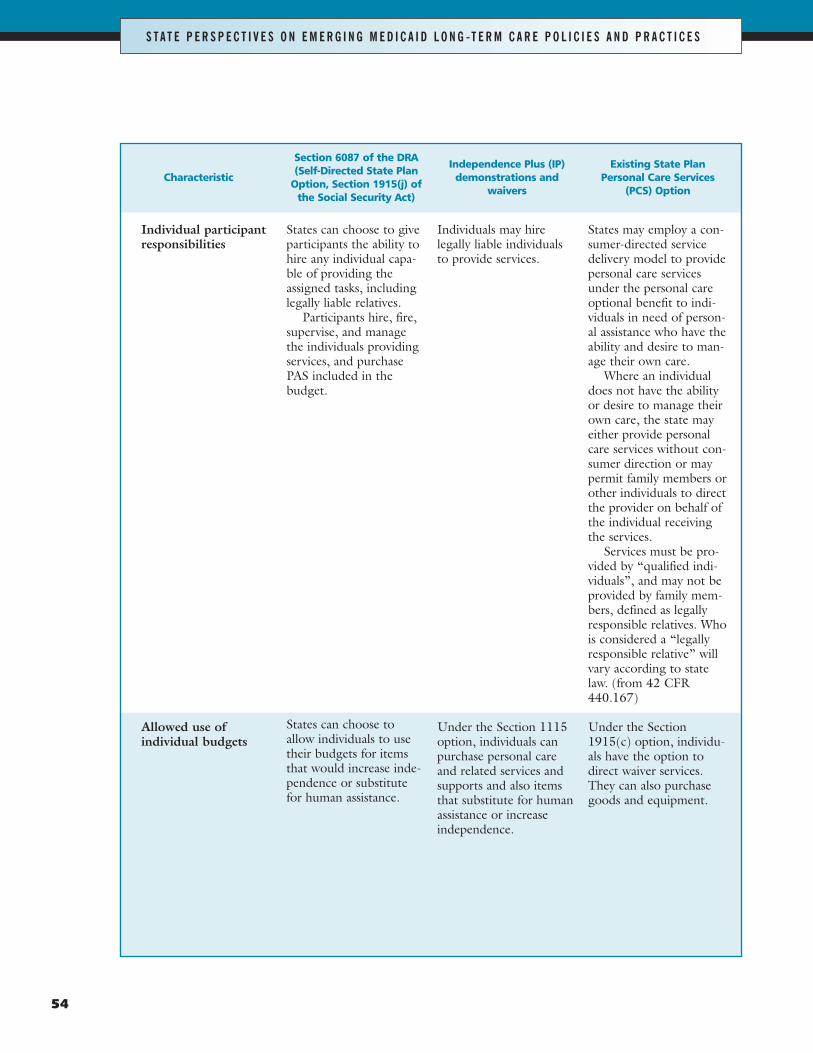
54
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Characteristic
Individual participantresponsibilities
Allowed use of individual budgets
Section 6087 of the DRA(Self-Directed State Plan
Option, Section 1915(j) ofthe Social Security Act)
States can choose to giveparticipants the ability tohire any individual capa-ble of providing theassigned tasks, includinglegally liable relatives.
Participants hire, fire,supervise, and managethe individuals providingservices, and purchasePAS included in thebudget.
States can choose toallow individuals to usetheir budgets for itemsthat would increase inde-pendence or substitutefor human assistance.
Independence Plus (IP)demonstrations and
waivers
Individuals may hirelegally liable individualsto provide services.
Under the Section 1115option, individuals canpurchase personal careand related services andsupports and also itemsthat substitute for humanassistance or increaseindependence.
Existing State PlanPersonal Care Services
(PCS) Option
States may employ a con-sumer-directed servicedelivery model to providepersonal care servicesunder the personal careoptional benefit to indi-viduals in need of person-al assistance who have theability and desire to man-age their own care.
Where an individualdoes not have the abilityor desire to manage theirown care, the state mayeither provide personalcare services without con-sumer direction or maypermit family members orother individuals to directthe provider on behalf ofthe individual receivingthe services.
Services must be pro-vided by “qualified indi-viduals”, and may not beprovided by family mem-bers, defined as legallyresponsible relatives. Whois considered a “legallyresponsible relative” willvary according to statelaw. (from 42 CFR440.167)
Under the Section1915(c) option, individu-als have the option todirect waiver services.They can also purchasegoods and equipment.
361185_Lot1_Text_54 11/7/07 5:41 PM Page 54
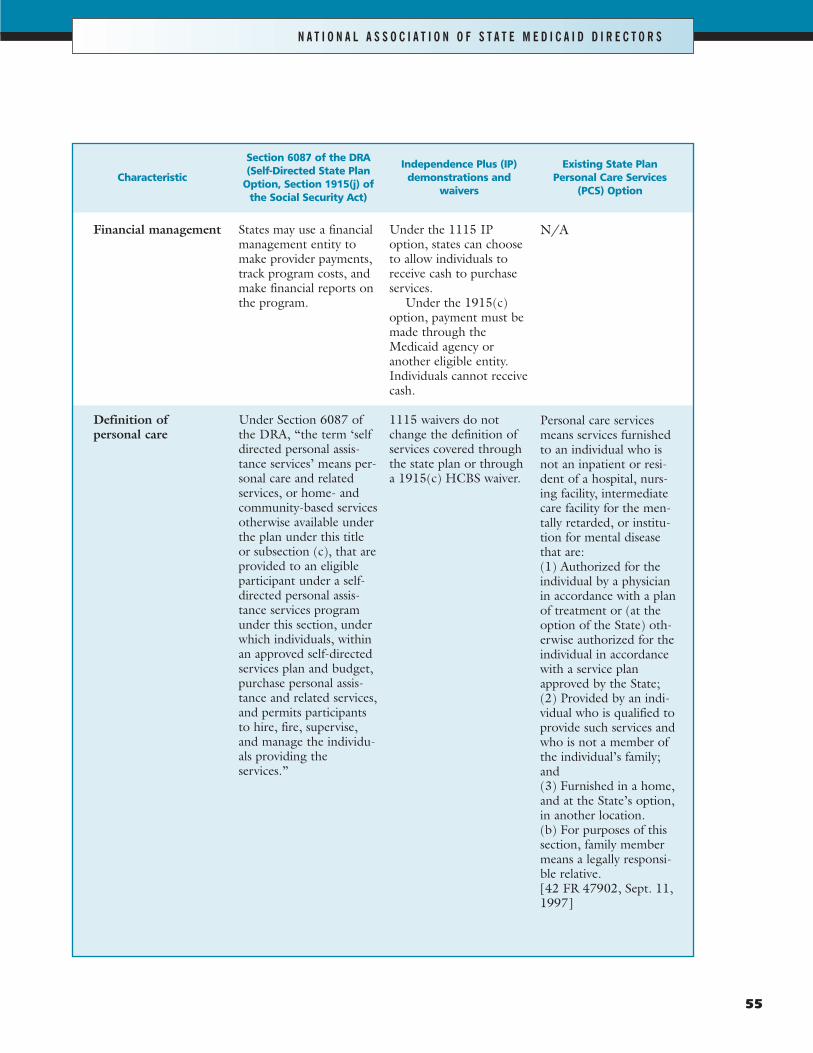
55
N A T I O N A L A S S O C I A T I O N O F S T A T E M E D I C A I D D I R E C T O R S
Characteristic
Financial management
Definition of personal care
Section 6087 of the DRA(Self-Directed State Plan
Option, Section 1915(j) ofthe Social Security Act)
States may use a financialmanagement entity tomake provider payments,track program costs, andmake financial reports onthe program.
Under Section 6087 ofthe DRA, “the term ‘selfdirected personal assis-tance services’ means per-sonal care and relatedservices, or home- andcommunity-based servicesotherwise available underthe plan under this titleor subsection (c), that areprovided to an eligibleparticipant under a self-directed personal assis-tance services programunder this section, underwhich individuals, withinan approved self-directedservices plan and budget,purchase personal assis-tance and related services,and permits participantsto hire, fire, supervise,and manage the individu-als providing the services.”
Independence Plus (IP)demonstrations and
waivers
Under the 1115 IPoption, states can chooseto allow individuals toreceive cash to purchaseservices.
Under the 1915(c)option, payment must bemade through theMedicaid agency oranother eligible entity.Individuals cannot receivecash.
1115 waivers do notchange the definition ofservices covered throughthe state plan or througha 1915(c) HCBS waiver.
Existing State PlanPersonal Care Services
(PCS) Option
N/A
Personal care servicesmeans services furnishedto an individual who isnot an inpatient or resi-dent of a hospital, nurs-ing facility, intermediatecare facility for the men-tally retarded, or institu-tion for mental diseasethat are:(1) Authorized for theindividual by a physicianin accordance with a planof treatment or (at theoption of the State) oth-erwise authorized for theindividual in accordancewith a service planapproved by the State;(2) Provided by an indi-vidual who is qualified toprovide such services andwho is not a member ofthe individual’s family;and(3) Furnished in a home,and at the State’s option,in another location.(b) For purposes of thissection, family membermeans a legally responsi-ble relative. [42 FR 47902, Sept. 11,1997]
361185_Lot1_Text_55 11/7/07 5:42 PM Page 55
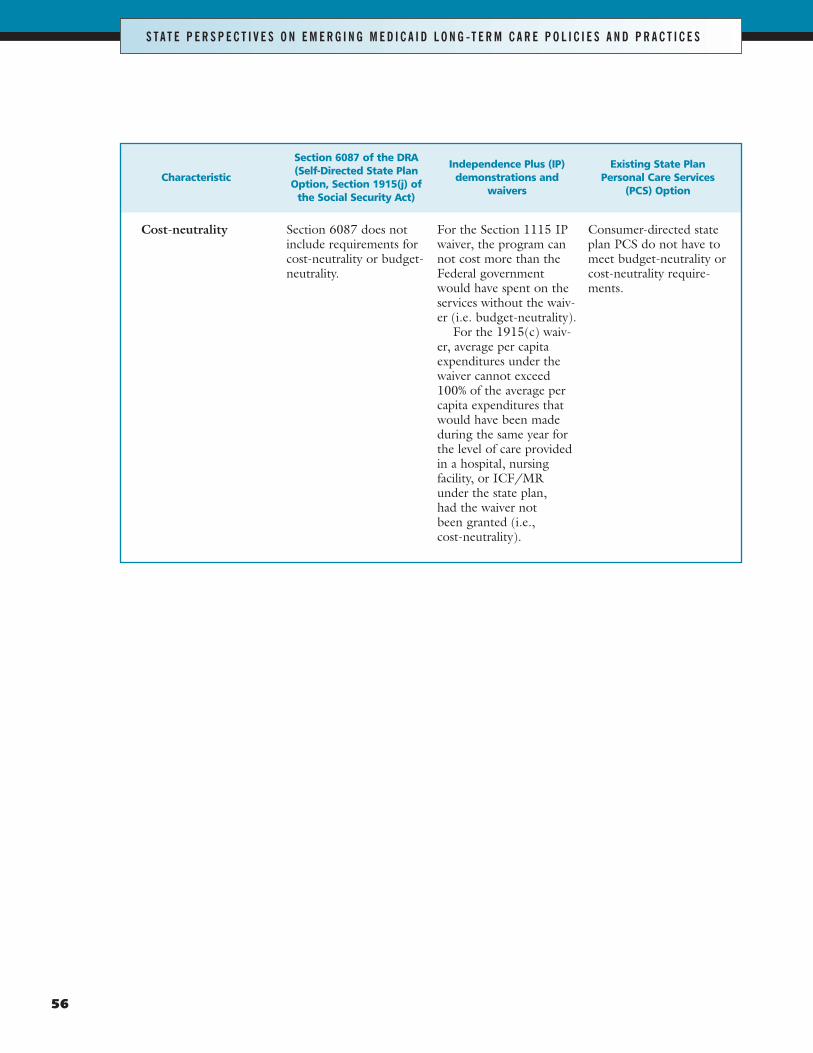
56
S T A T E P E R S P E C T I V E S O N E M E R G I N G M E D I C A I D L O N G -T E R M C A R E P O L I C I E S A N D P R A C T I C E S
Characteristic
Cost-neutrality
Section 6087 of the DRA(Self-Directed State Plan
Option, Section 1915(j) ofthe Social Security Act)
Section 6087 does notinclude requirements forcost-neutrality or budget-neutrality.
Independence Plus (IP)demonstrations and
waivers
For the Section 1115 IPwaiver, the program cannot cost more than theFederal governmentwould have spent on theservices without the waiv-er (i.e. budget-neutrality).
For the 1915(c) waiv-er, average per capitaexpenditures under thewaiver cannot exceed100% of the average percapita expenditures thatwould have been madeduring the same year forthe level of care providedin a hospital, nursingfacility, or ICF/MRunder the state plan, had the waiver not been granted (i.e., cost-neutrality).
Existing State PlanPersonal Care Services
(PCS) Option
Consumer-directed stateplan PCS do not have tomeet budget-neutrality orcost-neutrality require-ments.
361185_Lot1_Text_56 11/7/07 5:42 PM Page 56
810 First Street, NE | Suite 500 | Washington, DC 20002 | (202) 682-0100 | www.aphsa.org
361185_Lot1_Cover 11/7/07 7:34 PM Page 2





























