-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
1/57 WWW.AMERICANPROGRESS.O
State Options to Control Health Care
Costs and Improve QualityBy Zeke Emanuel, Joshua Sharfstein,
Topher Spiro, and Meghan O’Toole April 2016
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
2/57
State Options to ControlHealth Care Costs andImprove Quality
By Zeke Emanuel, Joshua Sharfstein, Topher Spiro, and Meghan
O’Toole
April 2016
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
3/57
1 Introduction and summary
4 Establish a cost growth goal
7 Publish a health and cost outcomes scorecard
9 Adopt payment and delivery system reform goals
11 Implement bundled payments for all payers
13 Institute global budgets for hospitals
15 Launch all-payer claims databases
18 Expand evidence-based home visiting services
21 Improve price transparency
23 Integrate behavioral health and primary care
27 Combat addiction to prescription drugs and heroin
33 Improve the delivery of long-term care
36 Align scope of practice with community needs
38 Institute reference pricing in the state employee
plan
40 Expand the use of telehealth
42 Decrease unnecessary emergency room use
44 Conclusion
47 Endnotes
Contents
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
4/57
1 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Introduction and summary
Te recen debae on healh care reorm has occurred mosly a he
naional level.
Te Affordable Care Ac, or ACA, was a momenous change or he U.S.
healh
care sysem. So ar, 20 million people have gained healh insurance
coverage
due o he ACAa hisoric reducion in he number o uninsured people
in he
Unied Saes.1
Te ACA also conained several ools designed o conrol healh care
coss. I
creaed he Cener or Medicare & Medicaid Innovaion, or CMMI,
which isauhorized o es new paymen and delivery mehods in order o
lower coss and
improve qualiy or individuals who receive benefis rom Medicare;
Medicaid;
or he Children’s Healh Insurance Program, or CHIP.2 CMMI is
currenly esing
and evaluaing many differen models, including accounable care
organizaions,
bundled paymens or hip and knee replacemens, and primary
care medical
homes. Te ACA also reduced Medicare paymens o Medicare Advanage
plans;
o hospials wih poor qualiy measures; and o medical providers,
which has had
a spillover effec on privae insurance.3
Parly due o he ACA, healh care cos spending growh has slowed in
recen
years. Beore 2014, here were five years o hisorically low
growh, and 2011
was he firs ime in a decade ha spending on healh care grew
slower han he
U.S. economy.4 Healh care coss are sill projeced o grow
aser han he overall
economy, however, and healh care spending already pus remendous
pressure on
sae and ederal budges and limis spending on oher imporan
services.5 More
needs o be done o susain his slowdown in growh.
Te curren poliical environmen makes i unlikely ha reorms o
conrol sys-
emwide healh care coss will be achieved a he ederal level in he
near uure.Saes, however, are well-posiioned o ake he lead on
implemening cos conrol
and qualiy improvemen reorms. Indeed, many saes are already
innovaing and
seeing posiive resuls.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
5/57
2 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Tere are several advanages o implemening reorms a he sae level.
Sae-level
reorms can be ailored o work bes or each sae, depending on he
srucure o
is insurance markes, he size o he sae, and is demographics. Saes
also have
considerable auhoriy over he regulaion o healh insurance and he
provision o
healh care wihin heir borders. Saes conrol heir own insurance
markes: Tey
run heir Medicaid and CHIP programs and sae employee plans, and
cerainsaes run he exchanges or individual healh insurance. Saes
also conrol he
rae review process, scope-o-pracice regulaions, physician
licensing, anirus
laws, and provider and insurer regulaions. Lasly, saes and
governors have con-
siderable convening power o bring ogeher diverse sakeholders,
making reorm
effors more poliically easible.
Te innovaions ha some saes are implemening o reduce coss while
main-
aining or improving qualiy can and should be replicaed by oher
saes. Tis
repor lays ou a comprehensive summary o opions, as oulined in he
ollow-
ing able, ha saes can choose rom o improve he qualiy and
susainabiliy oheir healh care sysems. Generally, hese opions relae
o implemening new
paymen models, increasing accounabiliy and ransparency,
collecing more
daa, increasing he use o high-value services and pracices, and
removing barri-
ers o effecive pracices.
We have included examples rom some o he mos pioneering
saes and oher
examples where saes are insiuing similar reorms, as well as
deails rom hese
saes’ experiences and heir sraegies o make he reorms successul.
Tese
examples are no an exhausive lis o all he saes ha may be
underaking hese
reorms. Oher ideas and sraegies have no been used beore.
Imporanly, hese
reorms are no muually exclusive; in ac, saes should adop as many
as possible.
All o hese reorm opions would help saes slow he growh o
healh care coss,
improve he qualiy o heir healh care sysems, and proec heir
residens.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
6/57
3 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Policy options and selected state examples
Establish a cost growth goal.
• Examples from Massachusetts, Maryland, and Rhode Island
Publish a health and cost outcomes scorecard.
• Examples from Maryland and Oregon
Adopt payment and delivery system reform goals.
• Examples from Massachusetts, Maryland, Rhode Island, and
California
Implement bundled payments for all payers.
• Examples from Arkansas, Tennessee, Ohio, and Delaware
Institute global budgets for hospitals.
• Example from Maryland
Launch all-payer claims databases.
• Examples from Maine, Colorado, New Hampshire, and
Washington
Expand evidence-based home visiting services.
• Examples from Minnesota and South Carolina
Improve price transparency.
• Examples from New Hampshire and Massachusetts
Integrate behavioral health and primary care.
• Examples from Oregon, Washington, and Colorado
Combat addiction to prescription drugs and heroin.
• Examples from Maryland, Florida, New York, and Rhode
Island
Improve the delivery of long-term care.
• Examples from California, Maryland, Montana, Oregon, Texas
and Missouri
Align scope of practice with community needs.
Institute reference pricing in the state employee plan.
• Example from California
Expand the use of telehealth.
• Examples from Maryland, New York, Virginia, the District
of
Columbia, and Pennsylvania
Decrease unnecessary emergency room use.
• Examples from Georgia, New Mexico, Indiana, Minnesota,
Washington, and Wisconsin
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
7/57
4 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Establish a cost growth goal
A cos growh goal conrols healh care coss by seting a cap
on he growh o a
sae’s per capia healh care spending. ypically, his cap is
deermined by per
capia growh in he sae economy, as measured by he gross sae
produc, or
GSP. Tese goals represen a public commimen o hold healh care
coss below
a se arge, increasing accounabiliy or all sakeholders. Even i a
goal does no
have sancioning power or fines i i is exceeded, i has a powerul
impac. Because
saes rack heir goal and repor on progress, seting goals
increases ransparency
and improves daa collecion.
In 2012, Massachusets became he firs sae o esablish a cos growh
goal. I
enaced legislaion ha limis he annual percenage growh in oal
healh care
spending o growh in he sae economy, adjused o remove flucuaions
due o
business cycles. Massachusets calculaes oal healh care
expendiures using hree
componens: all medical expenses paid o providers by all public
and privae pay-
ers; all paien cos-sharing amouns; and he ne cos o privae
insurance, such as
adminisraive expenses. Te sae hen compares ha oal o he poenial
GSP
o he commonwealh.6 Tis reorm coninued he effors o he sae’s
2006 healh
care legislaion, which ocused on coverage expansion, and 2008
legislaion ha
auhorized he collecion o deailed inormaion rom healh care
organizaions.7
Massachusets’ 2012 legislaion creaed he Healh Policy Commission,
or HPC,
o esablish and monior he cos growh arge, as well as he Cener or
Healh
Inormaion and Analysis o collec healh care daa.8 Each year,
he HPC ses he
sae’s healh care cos growh benchmark and moniors he perormance o
all
hospials, physician groups, accounable care organizaions, and
payers. Te HPC
noifies hose eniies i hey have exceeded he cos growh goal and
can require
hem o implemen perormance improvemen plans.9
Te HPC also conducsreviews o mergers and acquisiions and
issues annual repors and cos reviews o
inorm he public.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
8/57
5 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Massachusets was able o build consensus or a cos growh goal and
greaer
ransparency in healh care coss largely because providers
preerred hose
reorms o he sronger regulaory sysem ha he sae had iniially
proposed.10
Alhough Massachusets did no mee is cos growh arge or 2015,
he moni-
oring and daa collecion enabled i o ideniy ha i had ailed he
arge, and
no meeing he arge is galvanizing effors or addiional and sronger
reorms oconrol coss.11
In January 2014, Maryland also se a cos growh goal in agreemen
wih he
Ceners or Medicare & Medicaid Services, or
CMS.12 Maryland’s goal builds
upon he sae’s unique all-payer rae seting sysem or
hospialsmeaning ha
all payers pay he raes ha are se or each hospialha he Maryland
legislaure
esablished in he early 1970s.13 Te goal limis all-payer
annual per capia hospi-
al growh, including inpaien and oupaien care, o 3.58 percenhe
10-year
compound annual growh rae in per capia GSP.14 Maryland will
also limi annual
Medicare per capia hospial cos growh o a rae lower han he
naional annualper capia growh rae or he years 2015 hrough 2018. Te
sae has pledged o
achieve hese goals by ransiioning o new paymen models, as well
as by imple-
mening several oher iniiaives o lower coss and improve qualiy.
For example,
he sae commited o reducing is Medicare readmission rae and is
rae o
hospial-acquired condiions.15
Recenly, Rhode Island’s Working Group or Healhcare
Innovaioncharged
wih proposing soluions o improve healh, enhance paien
experience, and
reduce per capia cossincluded a flexible spending arge as one o
is our
primary recommendaions or conrolling healh care
spending.16 Tis would
be a nonbinding, annual arge or growh in medical
expendiures se a no
greaer han Rhode Island’s long-erm economic growh rae. Te
working group
endorsed a flexible arge over a hard cap on healh care spending
growh, which
also had been considered bu was deermined o be unnecessary
unless healh care
cos growh remains oo high. Te group also recommended ha Rhode
Island
regularly calculae and publicize oal medical expenses or he sae,
hold hearings
o undersand healh care cos growh, and reques perormance
improvemen
plans rom payers or providers i heir coss are increasing
unsusainably.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
9/57
6 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Options for implementation
Oher saes should se similar cos growh arges and monior and
enorce he
goals hrough eiher exising resourcessuch as sae healh
commissionsor by
orming a new eniy. Tis reorm would send a srong signal ha
governors and
saes are commited o aking acion o reduce healh care coss; i also
would norequire a large amoun o unding and could be esablished
quickly. For a governor
looking or a simple bu effecive reorm, seting a cos growh goal
would be a
good choice.
Sae governmens have muliple opions or implemening and phasing in
a cos
growh goal. Firs, a sae could ollow Massachusets’ and Maryland’s
example
bu provide more cushion in he firs ew years. Te arge or
per capia healh
care cos growh, or example, could be se a growh in he per capia
GSP plus
an addiional 0.5 percen over he firs hree years, hen rache down
o mach
he growh in per capia GSP in subsequen years. Second, saes have
choices orhe ype o healh care coss included in heir goals. Tey
could begin by seting
he arge or he cos o hospial care or hree years and hen expand he
goal o
cover he oal cos o care in laer years.
A sae also could negoiae an agreemen wih he ederal
governmen o share
he significan ederal savings ha meeing he goal would bringan
idea ha he
Cener or American Progress has previously proposed.17 I
saes mee a arge or
growh in oal healh care spending per capia, he ederal governmen
also would
realize savings in Medicare, Medicaid, Affordable Care Ac
subsidies, and oher
ederal healh care programs. Tereore, a sae could negoiae an
agreemen wih
he ederal governmen, under a waiver wih CMS, o share 50 percen o
he ed-
eral savings ha would occur i he sae mees he cos arge while also
meeing
qualiy measures. Tis increased savings o he sae could help ge
buy-in rom
he legislaure and oher sakeholders or he cos growh goal.
I esablishing a cos arge wih enorcemen auhoriy hrough legislaion
is no
possible, a governor could esablish a nonbinding cos growh goal
o pu pres-
sure on hospials and providers o hold down cosslike Rhode Island
did. In
his way, he governor would use convening auhoriy and he power o
he bullypulpi o shine a public spoligh on excessive providers and
encourage volunary
compliance wih he arge.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
10/57
7 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Publish a health and cost
outcomes scorecard
Publishing a sae scorecard on healh and cos oucomes is anoher
simple bu
imporan iniiaive ha all saes should insiue. Tis reorm would
require only
limied unding and could be accomplished absen new legislaion bu
would
emphasize ha he sae is ocused on addressing healh and cos
issues. A score-
card would enable sae sakeholders o undersand he curren sae o he
sysem
and le he sae publicly rack progress oward goals, increasing he
accounabiliy
o providers, payers, and oher sakeholders. Saes also could use
he scorecard as a
managemen dashboard or heir highes prioriies. Addiionally, saes
would havehe opion o build on he saewide scorecard by publishing
similar, more specific
scorecards wih relevan measures or individual hospials and
physician groups.
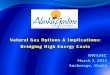
A poenial lis o measures or a sae scorecard is shown
below; oher liss
which overlap somewhahave been recommended recenly by he
Insiue o
Medicine and implemened in Maryland and Oregon.18 Such
measures would pro-
vide an excellen assessmen o he healh o he sae’s populaion
as well as he
qualiy and affordabiliy o care delivered o residens. Addiional
measures could
be added and exising measures could be updaed over ime o
reflec he sae’s
prioriies. In general, measures should be undersandable, measure
broad sysem
impac, and be validaed and readily available.
o he exen possible, measures should show rends over he previous
five years
and should be broken down by couny, race and ehniciy, and
socio-economic
saus. For each measure, saes should adop boh absolue
argesperormance
compared wih he naional median or 75h percenileand improvemen
ar-
ges, in erms o percenage change.
A public commen period can help wih public engagemen and
accepance o hemeasures. When Maryland esablished a scorecard in
2011, more han 350 public
commens were received. Te sae now makes daa on is measures
available on
an ineracive websie, wih daa broken down by couny and by race
and ehniciy
where possible.19
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
11/57
8 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Health measures
• Life expectancy
• Rate of infant mortality
• Rate of age-adjusted mortality fromheart disease
• Rate of age-adjusted mortality
from cancer
• Rate of diabetes
• Rate of clinical depression
• Rate of children and adults who are
overweight and obese
• Rate of births with low weight
• Rate of preterm birth
• Self-reported well-being
System quality measures
• Rate of immunization for children
• Rate of influenza immunization
• Rate of hospital-acquired infections• Rate of avoidable
hospitalizations (for
diabetes, chronic obstructive pulmo-
nary disease, congestive heart failure,
and asthma)
• Rate of hospital readmission
• Rate of tobacco use and alcohol and
drug misuse or poisoning deaths
• Screening for clinical depression
• Elective delivery before 39 weeks
• Rate of developmental screening up
to age 3
• Emergency department utilization
• Percentage of all-payer provider rev-
enue that is not fee for service
• Surveys on access to care and satisfac-
tion with care
• Adoption of electronic health records
Community measures
• Rate of child poverty
• Rate of teen pregnancy
• Air quality and drinking waterquality index
Cost and affordability meas
• Family spending burden: me
individual health care spending—
premiums and out-of-pocket co
as a share of median individual i
• Population spending burden
health care spending in the stat
share of gross state product
• State spending burden: healt
spending by the state as a share
state budget
Example health care scorecard
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
12/57
9 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Adopt payment and delivery
system reform goals
Seting goals o change paymen and delivery sysems o reward
high-value care
is anoher way or saes o increase ransparency and signal a
commimen o
sysem ransormaion.
Value-based payment goals
Alernaive paymen models are a ransiion away rom
volume-based care where providers are paid based on he quaniy
o services providedo value-
based care, where paymens o providers are based on he
healh and well-being
o heir paiens as well as heir oal cos o care. Secreary o healh
and human
services Sylvia Burwell recenly announced a naional arge o
making 50 percen
o Medicare paymens hrough alernaive paymen models and linking 90
percen
o paymens o value or qualiy by 2018.20 Saes should adop
similar arges or
heir Medicaid programs and all payers and should ideniy and
annually repor
he percenage o paymen in he sae ha is value based. Saes could se
hese
arges hrough legislaion or a publicly saed goal. Massachusets’
2012 cos con-
rol legislaion, or example, creaed a requiremen or 80 percen o
is Medicaid
beneficiaries o be in alernaive paymen conracs by July
2015 and or com-
mercial plans o implemen alernaive paymen models as much as
possible.21 Te
Massachusets Healh Policy Commission repors annually on he
percenage o
alernaive paymen models by payer ype.
In Maryland’s agreemen wih he Ceners or Medicare & Medicaid
Services,
he sae agreed o ransiion a leas 80 percen o hospial revenue in
he sae o
populaion-based paymen mehods.22 Similarly, Rhode Island’s
Working Group
or Healhcare Innovaion recommended ha all o he sae’s payers move
awayrom ee-or-service paymen oward alernaive paymen models and ha
hey
align around he ederal goals.23
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
13/57
10 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
DSRIP waivers
Delivery Sysem Reorm Incenive Paymen, or DSRIP, waivers offer
anoher way
or saes o access significan ederal unding and ake concree acions
o sup-
por paymen and delivery sysem reorm, ye only a ew saes so ar
have aken
advanage o hese waivers. DSRIP waivers are par o Medicaid’s
broader Secion1115 waiver program, which gives saes flexibiliy in
esing paymen and delivery
sysem reorms and offering a broader se o services in heir
Medicaid program.24
Te waivers provide unding o suppor healh care providers in
changing he pay-
men and delivery sysem or Medicaid beneficiaries.25
DSRIP waivers provide millions o dollars o healh care providers
ha mee
perormance merics in our general areas esablished by
CMS.26 Over he firs
hree years, hese merics ocus on processsysem redesign and
inrasrucure
developmen. In he laer years, he merics are based on
oucomesclinical ou-
come improvemens and populaion healh. Te specific merics or each
o heour areas vary by sae. Under Caliornia’s DSRIP waiver, or
example, is public
hospials are implemening 15 care-delivery reorm projecs, and he
hospials
have seen posiive progress in decreasing wai imes, reducing
hospial-associaed
inecions, and improving paien ineracions.27
While DSRIP waivers mus be budge neural o he ederal
governmen, hey
allow saes o ronload ederal unding given ha early invesmens are
needed
o realize savings in laer years.28 Tese waivers also can be
used in effec o repur-
pose saey ne paymens o hospials or delivery sysem reorm and o
smooh a
financial glide pah or providers, increasing provider
paricipaion in and accep-
ance o reorm.
Te unds available under DSRIP waivers are subsanial and vary by
he size o
he projecssaes such as New York and exas have received more han
$6
billion and $11 billion, respecively, over a five-year
period, while New Jersey
received $167 million or a smaller iniiaive.29
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
14/57
11 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Implement bundled payments
for all payers
Under he predominan ee-or-service paymen sysem, healh care
providers
are paid separaely or each individual service. In conras, a
bundled paymen
compensaes all o a paien’s healh care providers wih a single,
fixed, compre-
hensive paymen ha covers all o he clinically recommended
services relaed o a
paien’s episode o care, or all reamen and services provided o
rea a paricular
condiion over a defined period o ime. Tese paymens can be
adjused based on
he paien’s healh saus. Bundles can enable care coordinaion,
reduce variaion
in spending and clinical reamens, provide greaer ransparency and
accounabil-iy on price and qualiy, and allow providers o ransiion o
wider-scale paymen
reorms.30 Tey are also associaed wih qualiy measures o
assure ha he qualiy
o care ha paiens receive is preserved or enhanced.
Te ederal governmen is currenly esing several new approaches or
bundled
paymen models, bu saes also have a grea opporuniy o implemen
bundled
paymens. Several saes are adoping bundled paymen models o shif
he ocus
o carerom providing more services o improving qualiy and
reducing he
cos o care. Arkansas iniiaed his effor, and ennessee, Ohio, and
Delaware are
among oher saes ha have since adoped bundled paymens. Te mos
common
approach is o use he bundles as widely as possible across
providers and payers
wihin he sae. Tus, here is an effor o require he bundles
in boh Medicaid
and privae insurance, or a leas wih hose insurers on he exchange
and provid-
ing coverage o sae workers.
Te Arkansas Healh Care Paymen Improvemen Iniiaive is he only
saewide
paymen reorm ha involves all major public and privae payers. Te
iniiaive
aligns bundled paymens across Medicare; Medicaid; privae
insurers; and some
sel-insured employers, including Wal-Mar. Arkansas’ iniiaive
also ocuses onexpanding access o medical homes.31 Te sae
projecs ha he iniiaive will save
$1.1 billion over hree years and $8.9 billion by 2020.32
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
15/57
12 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Arkansas iniially launched five mulipayer episodes: upper
respiraory inecion;
oal hip and knee replacemen; congesive hear ailure; atenion
defici hyper-
aciviy disorder; and perinaal care. Currenly, he sae has
launched or sared
work on 16 episodes o care,33 and i has se a goal o
applying bundled paymens
o 50 percen o 70 percen o oal healh care spending in he sae over
he nex
ew years.34
In he Arkansas iniiaive, providers are sill paid on a
ee-or-service basis. Payers
designae a principal accounable provider, or PAP, who is he main
decision-
maker or mos care and coordinaes wih oher providers during an
episode.
Payers rack qualiy and coss across all episodes during a ime
period. I a PAP
keeps he average cos below a hreshold and mees qualiy sandards,
hen i can
keep a share o he savings. Bu i he average cos is above he
hreshold, hen he
PAP mus pay back a share o he excess coss. Since perormance is
measured
based on he average cos across all episodes, raher han he
cos o an individual
episode, providers have less incenive o sin on care in any given
case. Oherproecions include paien risk or severiy adjusmens o he
hresholds; paien
oulier exclusions; and sop-loss adjusmens, or maximum downside
risk.
Options for implementation
Given bundled paymens’ poenial o save money or saes while
improving he
qualiy o care, all saes should ac o implemen bundled paymens
saewide,
ideally wih he paricipaion o all payers. However, saes also
could iniially sar
wih bundled paymens in heir Medicaid program, require
Medicaid managed
care companies o include bundles in heir conracs, or use bundles
in he sae
employee plan.
o sreamline work and allow rapid deploymen o he bundles, saes
should
uilize bundles ha have already been developed in oher saes or or
Medicare.
Tese bundles include: hip replacemens; knee replacemens; prenaal
care and
delivery; ashma hospializaions; coronary arery bypass graf
surgery; sen
placemen; coronary caheerizaion; and breas cancer adjuvan
herapy.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
16/57
13 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Institute global budgets
for hospitals
Global budges are a ool o conrol healh care coss and encourage
hospials o
ocus on he healh o heir communiy raher han only he provision o
healh
care services. Insead o separae payers reimbursing hospials or
each individual
service or procedure, under a global budgeing sysem, a sae
agency ses a fixed
budge or each hospial each year based on acors including
pas expendiures,
pas clinical perormance, and projeced changes in levels o
services, wages, and
populaion growh.
Global budges conrol coss by eliminaing he incenives or hospials
o increase
heir volume o services because he amoun o revenue hey receive
each year is
fixed and predicable and does no depend on he number o paiens
served or
services perormed. Wihin prese limis, a he end o he year,
hospials keep
money lef over. I hey overspend heir budge, he hospials are
responsible or
hese exra coss and do no receive addiional revenue.
Maryland is he only sae ha has esablished global budges. In
2010, 10 rural
hospials in Maryland signed ono he sae’s global budge pilo
because hey
waned o ransorm heir care delivery sysems and improve he
healh o heir
communiies, bu hey required a sable revenue base while doing so.
Ten, in
2014, Maryland esablished global budges or all o is hospials as
par o an agree-
men wih he Ceners or Medicare & Medicaid
Services.35 Alhough he saewide
effor was volunary, all 46 hospials in he sae had signed on
wihin six monhs. 36
Hospials in Maryland suppored he ransiion o global
budges.37 Payers also
suppored global budges because hey help conain healh care coss
by reducing
volume and avoidable hospial use. Imporanly, he sae
undersood ha i would
be criical o build consumer suppor or his reorm, which i
accomplished inpar hrough a consumer engagemen ask
orce.38
Te Maryland Healh Services Cos Review Commission, or HSCRC, has
he
auhoriy o se each hospial’s oal annual revenue a he beginning o
each fiscal
year. Annual revenue is deermined rom a hisorical base
period ha is adjused
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
17/57
14 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
o reflec a number o acors, including inflaion, populaion change,
inrasruc-
ure requiremens, changes in levels o uncompensaed care coss, and
qualiy.
Annual revenue also may be modified or changes in service
levels, marke share
shifs, or shifs o services o unregulaed setings.39 Te HSCRC
also collecs and
disribues paien-cenered daa o hospials monhly on poenially
avoidable
uilizaion and on high-uilizaion paiens.
Since he inroducion o saewide global budges in Maryland, oucomes
have
improved across he board. Poenially avoidable hospial uilizaion,
Medicare
readmission raes, and inpaien admissions have all
declined.40 Furhermore, in
2014, all-payer hospial spending growh per capia grew jus 1.47
percen, which
is lower han he 3.58 percen limi se by he sae’s cos growh goal.
Tereore,
he sae saved Medicare more han $100 million in jus he firs
year.41
Maryland’s unique all-payer rae seting sysem helped aciliae he
sae’s ransi-
ion o global budges. Bu global budgeing is possible wihou
cenralized raeseting, and oher saes are invesigaing his model.
Options for implementation
Addiional saes should consider seting global budges or
hospials. An iniial
sep would be o convene a group o hospials, payers, physicians,
and consum-
ers o assess global budge seting wihin he sae and deermine wha
would be
needed or effecive implemenaion.
A second sep would be o pilo global budges or hospials in
a ew regions o
build suppor or a saewide iniiaive, as Maryland did. A sae
could use is
convening auhoriy o encourage payers and a ew hospials o
implemen global
budges volunarily. Hospials sruggling o mainain volumes o
paiens and rev-
enue levels, such as rural hospials, are good candidaes or
global budges; reed
rom ee-or-service incenives, hese hospials can ocus on reducing
avoidable
admissions and improving oucomes.
o move orward, he sae would need a mechanism o se a arge budge
or eachhospial, develop an approach o enorce i, and promoe payer
paricipaion. A
waiver rom CMS would be necessary or Medicare paricipaion.
A sae also could
incenivize paricipaion and help prepare hospials or he ransiion
o global
budges by providing grans or inrasrucure and new saffing
needed or global
budges. Maryland provided such grans when i inroduced
global budges.42
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
18/57
15 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Launch all-payer claims databases
All-payer claims daabases, or APCDs, are large-scale
daabases ha sysemaically
collec medical claims, pharmacy claims, denal claims, and
eligibiliy and pro-
vider files rom privae and public payers in a
sae.43 Te daa include he acual
prices ha healh plans have negoiaed wih providers. Currenly, 18
saes have
enaced laws o creae APCDs.44
APCDs are usually creaed by a sae mandae, which requires
all payers in a sae
o submi heir daa. Tere are also a ew volunary APCDs ha are
esablished wihou legislaion; wih hese, he sae canno compel all
payers o submi heir
daa, and he sae has no auhoriy o assess penalies or
nonreporing.45
All saes should have an APCD, as hey are insrumenal in
enabling cos conrol
and qualiy improvemen effors. APCDs can help saes undersand cos,
uiliza-
ion, and qualiy baselines rom which o evaluae he impac o reorms.
Tey
enable saes o undersand he healh o heir ciizens and he healh
care ha is
being provided o hem. Saes can ideniy variaion beween
high- and low-cos
providers and differences in coss or reamen opions or a given
condiion; hey
also can deec dispariies in access o services in differen pars o
a sae.
Daa provided by APCDs can help consumers choose high-qualiy care
and make
inormed decisions.46 Insurers can use APCD daa o negoiae
appropriae raes
and seer heir consumers oward high-value care.47 Finally,
APCDs are used in
premium rae-review processes o allow saes o veriy i proposed rae
increases
are in line wih increases in claims or changes in he risk
pool.
Te efficien use o APCD daa can lead o significan cos savings.
For example,
a sudy based on daa rom Maine’s APCD ound ha i poenially
avoidablehospial admissions and he use o oher hospial services ha
are high cos and
have wide variaion in cosas idenified hrough he APCDwere reduced
by
50 percen, medical spending by commercial payers could be
reduced by 11.5
percen, and Medicaid spending could be reduced by 5.7
percen.48
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
19/57
16 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Anoher example rom Colorado shows how saes can ideniy
rends hrough
APCD daa, calculae poenial savings, and arge inervenions.
Te Cener
or Improving Value in Healh Carea nonprofi ha adminisers
Colorado’s
APCDanalyzed daa on he prevalence o cesarean deliveries,
which can pose
healh risks and also are more expensive han vaginal deliveries.
Te Unied Saes
has pledged o decrease he rae o cesarean deliveries in low-risk
women by 10percen by 2020.49 Tey ound ha he rae o cesarean
deliveries was increasing
in Colorado, as well as ha people wih commercial insurance were
significanly
more likely o have cesarean deliveries han Medicaid enrollees.
Alhough he daa
could no reveal why he raes o cesarean deliveries differed by
ype o coverage,
hey showed areas ha policymakers could arge o reverse he rend o
increas-
ing cesareanshereore prevening unnecessary healh risks o mohers
and
children. Te analysis also ound ha reducing he rae o cesarean
deliveries only
10 percen would save he sae $6.5 million per year.
Te coss o develop and operae an APCD vary depending on he size o
hesae, he scope o he daa colleced, and oher acors. In he saes ha
already
have APCDs, he average cos o develop and implemen hem was $1.1
million,
and annual ongoing coss average $600,000.50 Saes use a
variey o sources o
und he developmen and operaion o heir APCDs, ypically unding par
o
heir APCDs hrough general appropriaions or ees assessed on healh
plans or
providers.51 Many saes also receive gran unding o suppor
APCD develop-
men.52 Some saes have included APCD developmen and
improvemen as
a componen o ederal rae review grans, while ohers have used he
ederal
Beacon Communiy Programwhich suppors communiies in adoping
elec-
ronic healh records and healh inormaion exchangeso obain unds.
New
Hampshire has leveraged Medicaid unding or is APCD. Finally,
saes can und
heir APCDs in par hrough selling daa o researchers and oher
sakeholders.
Tere are many resources o help saes esablish an APCD, and he bes
pracices
rom oher saes can be applied o address sakeholders’ concerns.
For example,
healh care providers may be concerned abou daa proecions in an
APCD
such as making public he discoun arrangemens ha providers have
wih pay-
ers.53 I is imporan o include payers and providers in he
APCD creaion process
and gain heir inpu on he bes way o srucure daa collecion and
release inorder o build buy-in. Te APCD Councila nonprofi ha helps
saes wih
APCD developmenhas creaed model legislaion or APCD
developmen, as
well as a model or saes o ollow when seting up an APCD,
and i can provide
guidance on daa collecion and daa release rules.54
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
20/57
17 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Options for implementation
An APCD is an imporan ool or all saes. Te 2016 U.S.
Supreme Cour
decision Gobeille vs. Liberty Mutual Insurance
Company ruled ha he Employee
Reiremen Income Securiy Ac o 1974 exemps sel-unded insurers
rom
reporing daa o APCDs.55
Tereore, saewide mandaory APCDs may no lon-ger be
possible, unless he U.S. Deparmen o Labor issues new rules o
require
sel-unded plans o submi daa, bu saes can sill esablish saewide
APCDs
wih required reporing excep or sel-unded insurers. Saes
hen could ask sel-
unded insurers o submi daa o he APCD volunarily.
I a saewide APCD is no possible immediaely, a sae also could
recrui one
large healh sysem o agree o work wih he sae in esablishing an
APCD; his
would creae more pressure or oher healh sysems o similarly
sign ono an
APCD. Saes also could hink abou saring wih a volunary APCD
and ransi-
ioning laer o a required APCD. Washingon ook his approach in
2004 and isnow implemening an APCD wih mandaory
reporing.56 Saes ha are iner-
esed in creaing an APCD should use exising resources and
organizaions in heir
saes, such as academic or oher healh care insiuions, wih
experise in healh
care daa o help wih he creaion or running o he APCD.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
21/57
18 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Expand evidence-based
home visiting services
Home visiing programs connec parens wih nurses, social workers,
or oher
proessionals who provide coaching and guidance on healhy child
developmen
and link amilies wih oher imporan services. Tese programs are
among he
mos effecive governmen programs ever sudied in erms o consisenly
produc-
ing boh posiive oucomes and cos savings, and hey are an imporan
ool o
reduce rising income inequaliy.57 Randomized conrolled
rials esing he impac
o home visiing services have ound ha he mos effecive models
reduce he risk
o inan deah; reduce he need or paymens rom he Supplemenal
Nuriion Assisance Program, or SNAP, and emporary Assisance or
Needy Families,
or ANF; lower criminal offenses and subsance abuse; preven child
abuse and
malreamen; increase breaseeding and immunizaion; and increase
amily
economic securiy.58
In addiion o improving he lives o he amilies ha paricipae,
evidence-based
home visiing services acually pay or hemselves. A CAP analysis o
exensive
research on he reurn on invesmen o he Nurse-Family Parnership,
or NFP
one o he mos widespread and sudied home visiing programsound
ha,
even accouning or he coss o providing he program, a sae can
expec average
savings o more han $7,400 rom each birh enrolled in NFP by he
ime a child is
18 years old.59
However, evidence-based home visiing programs serve only a small
porion o
he eligible amilies, largely due o unding challenges. In 2015,
he larges ederal
unding source or home visiing programshe Maernal, Inan, and
Early
Childhood Home Visiing Program, or MIECHVwas only able o serve
abou
115,000 parens and children, a small racion o he children and
amilies who
live in povery in he Unied Saes.60
Saes mus piece ogeher muliple undingsources, which is
adminisraively complicaed and ime-consuming, inhibiing
saes rom providing hese imporan services o all eligible amilies.
Home visi-
ing also requires invesmens in he firs ew years o a child’s lie
ha are paid off
laer in savingsa challenge or saes because hey are required o
balance heir
budges on an annual or a biannual basis.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
22/57
19 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Despie hese challenges, saes should ac quickly o expand home
visiing pro-
grams and provide coverage o all eligible amilies, raher han
spending money
in he uure on cosly services. Combining curren unding sources
and using
innovaive financing mehods can provide he invesmen needed now o
realize
significan savings and improved oucomes or amilies in he uure. I
saes were
o offer home visiing services consisenly o eligible residens, he
savings romproviding hese services would more han cover he coss
afer he firs ew years.61
Options for implementation
Saes have several opions o expand he reach o heir home visiing
programs.
Firs, saes can work o increase Medicaid unding or heir home
visiing pro-
grams. Greaer Medicaid reimbursemen would require ha saes employ
home
visiing adminisraors wih experise in Medicaid benefis and
reimbursemen
bu would provide a sable unding source. Saes would also
save more han heirshare o he coss o unding increased home visiing
hrough Medicaid. Home
visiing aciviies ha saes have ound o be eligible or
Medicaid coverage and
paymen include: assessmens; developing care plans and monioring
progress;
reerrals; amily planning aciviies; and providing menal healh
services.62 Recen
guidance rom he Ceners or Medicare & Medicaid Services and
he Healh
Resources and Services Adminisraion oulines he Medicaid
financing mecha-
nisms available o saes or home visiing programs.63 However,
Medicaid unding
is insufficien o und he enire range and duraion o home visiing
programs, so
saes would need o supplemen Medicaid wih oher unding
sources.
Second, saes could encourage or require Medicaid managed care
organizaions
o offer home visiing services as a benefi o all eligible
Medicaid beneficiaries.
All Medicaid managed care organizaions in Minnesoa, or
insance, volunarily
offer home visiing programs because hey recognize he cos
effeciveness o
hese programs.64
Tird, saes could negoiae a Medicaid waiver wih CMS o provide
ederal
maching unding and ronload unding or home visiing. Medicaid
Secion
1115 waiverswhich give saes flexibiliy o es innovaions and offer
servicesno usually covered by Medicaidwould allow saes o und he ull
range o
home visiing services compleely hrough Medicaid and offer hese
imporan
services o every eligible amily. Secion 1915(b) waiverswhich
allow saes o
implemen services ha are no oherwise available hrough managed
care orga-
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
23/57
20 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
nizaions, arge specific populaions, and resric he choice o
providersare
anoher opion. Souh Carolina recenly received approval or a
1915(b) waiver
rom CMS ha he sae will use o launch a pilo program or NFP.65
Lasly, saes could use innovaive Pay or Success models o und home
visiing,
as several saes are in he process o doing.66
In hese models, also known as socialimpac bonds, local
banks, communiy oundaions, naional oundaions, and
invesmen banks pu up capial o scale home visiing programs, and
he govern-
men pays hese invesors back only i resuls are achieved and
savings maerialize.
In Souh Carolina, Gov. Nikki Haley (R) is pioneering such a
social impac bond
modelin conjuncion wih he 1915(b) waivero und home visiing
and
expand hese imporan services o more mohers and
children.67 Tis ype o pay-
men model can solve he iming issue inheren o home visiing
services: Capial
is needed upron, bu savings accrue over a longer ime period.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
24/57
21 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Improve price transparency
Te U.S. healh care sysem, especially healh care prices, is
characerized by a lack
o ransparency. Tis impedes marke compeiion and prevens paiens
and heir
providers rom making inormed healh care decisions. Consumers do
no know
how much a procedure, medicaion, or hospial say will cos. Prices
or he same
service can vary significanly by provider, and providers charge
differen payers
differen amouns or he same service.
However, here is no consisen evidence ha higher prices are
correlaed wihhigher-qualiy healh care services.68 Even when
prices are lised, hose are ofen
no he prices ha paiens acually will be charged. Prices may
differ, or example,
because o he paiens’ insurance coverage or because o he
coss o oher provid-
ers who may be involved in he paiens’ care. Docors make reerrals
wihou
knowing he prices charged by oher providers and prescribe
medicaion and
medical devices wihou knowing heir prices. Widespread price
variaion, which
is enabled by he lack o price ransparency, adds abou $36 billion
o he expenses
o people wih employer-sponsored healh insurance.69
Price ransparency provides consumers wih accurae and imely
inormaion
ha hey can use o make inormed healh care
choices.70 ransparency also
can expose marke condiions and make markes more compeiive,
resuling in
prices ha reflec he cos and value o he healh care services ha
are provided.71
Despie he challenges o achieving price ransparencyincluding he
variey o
insurance benefi designs and legal barriers o disclosing
pricesall saes should
expand price ransparency effors by offering consumer-riendly
esimaes o com-
mon healh care services and qualiy inormaion.
New Hampshire is a pioneer in price ransparency and is he only
sae o havereceived an “A” grade or sae ransparency rom Caalys or
Paymen Reorm,
a nonprofi working o promoe higher-value healh care in he Unied
Saes.72
New Hampshire uses is all-payer claims daabase o publish he
acual coss ha
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
25/57
22 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
consumers can expec o pay or healh care services.73 Te sae
recenly added
addiional procedures, qualiy daa, and a consumer-riendly inerace
o encour-
age consumers o shop around or he bes-value services.
Massachusets also has been a leader in price ransparency. Since
2014,
Massachusets has required insurers and healh plan adminisraors o
offerconsumers provider-specific esimaes o heir ou-o-pocke coss or
specific
hospial says or procedures.74 Tese prices include coss or
boh docors and
healh care aciliies insead o discree services. Tese esimaes are
binding,
unless he paien receives addiional services ha were no anicipaed
o be par
o he reamen.75 Te Massachusets law also requires providers
o give paiens
inormaion ha heir insurer migh need o calculae heir ou-o-pocke
coss.
In addiion o hese consumer-ocused requiremens, healh care
providers in
Massachusets also mus disclose heir esimaed charges. Te sae has
insiued
iniiaives aimed a sudying prices and increasing access o qualiy
and cosdaahe Healh Policy Commission sudies price variaion, and all
healh care
organizaions mus submi annual cos and qualiy daa o he
commission. A
public websie liss daa abou he relaive coss o differen
providers, increasing
consumers’ access o crucial inormaion.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
26/57
23 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Integrate behavioral health
and primary care
Behavioral healh issues are associaed wih poor physical healh
oucomes.
Paiens wih boh ype 2 diabees and menal illness, or example, have
a higher
moraliy rae han hose wih jus diabees or jus menal
illness.76 Individuals
wih severe menal illness, depression, demenia, and
subsance use disorders have
reduced chances o survival afer a cancer diagnosis, independen o
he cancer
sage a diagnosis.77 People wih menal disorders have a lower
age o deah by an
average o 8.2 years.78
Tose wih comorbid behavioral and medical healh issues do no only
have worse
healh oucomeshey also produce subsanial coss o he healh care
sysem.
Milliman, an acuarial and consuling firm, conduced an analysis
ha ound ha
hose wih chronic medical and comorbid menal healh condiions or
subsance
use disorders can incur coss ha are 2 imes o 3 imes he coss o
hose wih-
ou comorbid menal healh condiions or subsance use
disorders.79 Because
Medicaid is he larges payer or behavioral healh reamen, saes
shoulder
significan coss rom behavioral healh issues.80
Behavioral healh services are ofen provided compleely separaely
rom he
physical healh sysem. Addiionally, many paiens preer o seek care
or behav-
ioral healh issues rom heir primary care docors, who are ofen
ill-equipped o
deliver appropriae care.81 However, he effecive inegraion o
behavioral and
medical services can help improve healh oucomes and lower coss.
For example,
he Milliman analysis ound ha he effecive inegraion o care could
save abou
9 percen o 16 percen o he addiional spending on hose wih
comorbid menal
healh condiions or subsance use disorders.82
Tere is a coninuum o approaches o inegrae physical and
behavioral healhcare.83 In an inegraed care pracicehe mos
inegraed on he coninuuma
eam o primary care and behavioral healh providers work ogeher o
address
behavioral healh issues ha presen in primary
care.84 Oher less ully inegraed
bu sill helpul approaches include coordinaed caresuch as
universal screening
or behavioral healh disorders in primary care, or
co-locaionwhere physical
and behavioral healh care services are provided a he same
locaion.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
27/57
24 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
One example o an inegraed care inervenion is he Improving
Mood-
Promoing Access o Collaboraive reamen, or IMPAC, care
managemen
program developed a he Universiy o Washingon ha is designed o
rea lae-
lie depression in primary care. Tis model is also known as
Collaboraive Care.
Depression is a common and expensive condiion in older adulsone
ha ofen
occurs wih oher healh problems.85
However, ew older aduls receive effecivereamen, ofen
because hey are no diagnosed. Addiionally, more han 90 per-
cen o older aduls wih depression preer o receive care rom heir
primary care
provider raher han a menal healh specialis, even hough primary
care docors
do no have he same experise in menal healh.86
Wih he IMPAC inervenion, paiens have a depression care
manager,
supervised by a psychiaris, who works direcly wih he paien’s
primary care
provider. Tis eam sysemaically racks he paien’s oucomes and
adjuss he
reamen i he paien is no improving.87 Te paien also receives
educaion,
an anidepressan medicaion when recommended, and individual
counselingsessions. In conras, usual care or paiens diagnosed wih
depression in primary
care consiss o jus a prescripion or an anidepressan or a reerral
o a menal
healh provider.88
A randomized conrolled rial o he IMPAC inervenionacross 18
diverse
primary care clinics in five saesshowed ha i more han doubled he
effec-
iveness o depression reamen or hese older aduls in primary care
setings,
increased paien saisacion, improved physical uncioning, and
saved abou
10 percen o oal healh care coss or he inervenion
paiens.89 Te IMPAC
program has since been expanded o include adolescens and
nonelderly aduls,
as well o oher behavioral healh condiions, including anxiey and
subsance
abuse.90 Tis model o care has now been implemened in
hundreds o organiza-
ions across he counry.91
Several saes are implemening new paymen models or innovaive
models o care
o promoe he effecive inegraion o behavioral and physical
healh.
Oregon is piloing an Alernaive Paymen Mehodology a hree
communiy
healh ceners, which is allowing or beter inegraion o behavioral
healh and pri-mary care.92 Te Alernaive Paymen Mehodology pilo
is designed o promoe
comprehensive care or a populaion by paying he communiy healh
ceners a
per-member-per-monh, or PMPM, ee insead o on a ee-or-service
basis. Te
pracices are able o look broadly a how hey rea heir paiens and
have he
flexibiliy o use some o he PMPM paymen on behavioral healh
services. For
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
28/57
25 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
example, some o he pracices are embedding behavioral healh
docors in pri-
mary care eams, so ha he primary care physicians can immediaely
reer paiens
o he behavioral healh providers in person a he end o a primary
care visi.
In several saes, Medicaid managed care organizaions are
implemening pro-
grams o coordinae care or paiens wih comorbid behavioral and
physicalhealh condiions.93 For example, Communiy Healh Plan o
Washingon,
which is a nonprofi plan serving he Medicaid populaion,
has implemened
he IMPAC model. Te Washingon healh plan suppors he creaion o
he
reamen eams ha are required as par o IMPAC and invess in
addiional
raining or he providers o implemen he model. Afer he healh plan
expanded
he model rom wo pilo sies o saewide, i achieved savings o abou
$11 per
member per monh in jus he firs 14 monhs.
Colorado is using a Sae Innovaion Models gran rom he Ceners or
Medicare
& Medicaid Services o implemen a saewide behavioral healh
iniiaive. Teiniiaive aims or 80 percen o Colorado residens o have
access o inegraed
care or behavioral healh and primary care in primary care
setings by 2019, and
projecs ha his will save $330 million over five years.94 As
par o his effor, he
sae will implemen inegraed care in Medicaid and he sae healh
employee
plan o spur broader adopion o inegraed care across he sae, and i
will pro-
vide pracice ransormaion suppor o 400 primary care
pracices o enable hem
o inegrae behavioral and physical healh services.95
Privae insurers also have insiued programs o help coordinae
behavioral and
physical healh care. Aena, or example, developed a Depression in
Primary
Care Program o suppor primary care physicians in diagnosing and
monioring
paiens wih depression.96 Tis program provides primary care
physicians wih a
diagnosic ool and reimburses hem or heir ime spen screening or
depression
and ollow-up monioring.
Options for implementation
Tese examples show how saes can ake a lead role in inegraing
behavioralhealh and primary care. Firs, a sae could enac legislaion
o require primary
care providers o screen all paiens or menal healh issues and hen
reer hem
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
29/57
26 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
or appropriae care. Tis approach would no inegrae care ully, bu
i would
require he sae o assess paiens’ access o menal healh providers
and ake
seps o improve access as needed.
Second, saes could aciliae and operaionalize he inegraion o
behavioral
and physical healh by removing paymen barriers ha hinder he
inegraion ocare. For example, some saes do no allow healh ceners o
bill or he coss o
muliple servicessuch as boh a physical healh and a behavioral
healh ser-
viceo he same person in he same day, which discourages he
co-locaion o
hese services.97 In some saes, Medicaid will no reimburse
or healh behavior
and assessmen inervenion codes a Federally Qualified Healh
Ceners.98 Some
saes do no uilize billing codes ha were esablished or Medicaid
paymen or
Screening, Brie Inervenion, and Reerral o reamen, or SBIRa mehod
o
screening or subsance use disorders. Anoher issue is ha in some
saes, mos
payers do no reimburse or communiy healh workers o suppor care
manage-
men o behavioral and physical healh issues.99 And he
ee-or-service paymensysem does no allow or reimbursemen o he ype o
care coordinaion ha
Oregon is promoing wih is Alernaive Paymen Mehodology pilo.
Tird, saes could implemen, wih a pilo or wih a saewide
expansion, an
effecive inegraed care model, such as he IMPAC inervenion
described
above. Healh Homes, which is a reamen model ha was esablished by
he
Affordable Care Ac o coordinae care or Medicaid
beneficiaries wih more han
one chronic condiion, can be used o implemen collaboraive care
programs
such as IMPAC.100
Fourh, saes could reduce barriers o he sharing o inormaion
beween
primary care and behavioral healh providers. Confidenialiy laws
or behavioral
healh are ofen more resricive han hose or physical healhor
example, i
a paien’s consen is required o share daa on menal healh reamen
across
providers.101 Saes wih resricive confidenialiy laws should
amend hese laws
o permi greaer sharing o inormaion while sill proecing paien
privacy.
Saes can, or example, permi he sharing o daa on behavioral healh
or rea-
men purposes. However, saes do no have he auhoriy o overcome
resric-
ive ederal law around he sharing o daa relaed o addicion reamen,
houghhe U.S. Deparmen o Healh and Human Services is proposing o
modiy
hese regulaions.102
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
30/57
27 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Combat addiction to prescription
drugs and heroin
Drug overdose deahs, addicion, and emergency deparmen visis
relaed o
subsance use disorders have surged in recen years, and he Ceners
or Disease
Conrol and Prevenion has labeled i an epidemic.103 Addicion
o prescripion
opioids and heroin, which is ound across all demographic and
income groups,
is driving his epidemic. From 2002 o 2013, here was a 286 percen
increase in
he number o heroin-relaed overdose deahs.104 Ofen, people
become addiced
o prescripion opioid painkillers, obained boh legally and
illegally, and hen
become addiced o heroin, which is much cheaper.105 Te
coss associaed wihdrug overdose and addicion are large and growing,
and Medicaid bears a large
percenage o hese coss.106
Te ederal governmen has aken seps o implemen policies o reduce
drug addic-
ion and overdose, such as providing greaer raining on opioid
prescribing or ed-
eral healh care proessionals.107 Bu saes have he abiliy o
effec greaer change
because hey regulae he pracice o medicine wihin heir
saes.108 However, saes
mus overcome several barriers o reducing prescripion drug and
heroin use.
Sigma and misconcepions surrounding addicion are common and
presen a
serious barrier o effecive reamen. Addicion is a chronic
diseasea ac ha
is commonly misundersood and ha conribues o sigma. Sigma, in
urn, can
preven access o effecive reamen. For example, he use o
medicaion-assised
reamen,* or MA, has been shown o produce subsanial cos savings
as well as
reduce drug use, disease raes, and criminal aciviy among addiced
people, and
i is more effecive han shor-erm managed wihdrawal reamen, or
deoxifica-
ion.109 Te Insiue or Clinical and Economic Review has ound
ha or every
addiional dollar spen on MA, $1.80 in savings are
realized.110 Ye a judge or
parole officer may order an offender o end MA because he or she
believes heperson is no ruly in recovery.
* With MAT, medications are used in conjunction with behavioral
therapy to reduce the symptoms of substance use withdrawal. Three
medi-
cations are approved by the Food and Drug Administration to
treat opioid use disorders: methadone; buprenorphine; and
naltrexone. SeeCindy Mann and others, “Medication Assisted
Treatment for Substance Use Disorders” (Baltimore: Centers for
Medicare & Medicaid Services,
2014), available at
http://www.medicaid.gov/federal-policy-guidance/downloads/cib-07-11-2014.pdf.
http://www.medicaid.gov/federal-policy-guidance/downloads/cib-07-11-2014.pdfhttp://www.medicaid.gov/federal-policy-guidance/downloads/cib-07-11-2014.pdf
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
31/57
28 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Second, access o effecive reamen is limied. Only 10 percen o
Americans
wih addicions and subsance use disorders receive any care
each year.111 An esi-
maed 65 percen o people in prison have a drug or alcohol
addicion, ye only 11
percen receive proessional reamen while incarceraed. Shorages o
clinicians
who care or individuals wih subsance use disorders and
limied spos available
or reamen resric he number o people who can access reamen.
People whoare uninsured also have rouble affording reamen.
Even hose who are able o access reamen find i hard o access
effecive rea-
men. As o 2014, only 13 saes included all approved addicion
medicaions on
heir Medicaid preerred drug liss, many insurers impose onerous
requiremens
on addicion reamensuch as quaniy or lieime limisand many
privae
insurers do no cover mehadone reamen.112 For example, in
order o prescribe
buprenorphinean effecive medicaion approved o rea opioid
addicion
docors mus ake an eigh-hour course and apply or a special
license, which
limis he number o docors permited o prescribe his addicion
medicaion.113 Tese resricions mean ha only 2.2 percen o docors
me he requiremens o
prescribe buprenorphine in 2012.114 Since addicion is a
chronic disease, limis on
how long an individual can receive reamen misundersand drug
addicion, are
counerproducive, and can resul in higher long-erm coss.
Tird, many saes lack access o imely and comprehensive daa. Many
saes rack
overdose deahs bu wih significan lag ime and wihou deailed
inormaion.
Addiional daa on overdose deahs and on nonaal overdoses
can help saes,
local jurisdicions, police deparmens, and healh proessionals
pinpoin rouble
areas and where o launch inervenions sraegically.
State strategies for combating addiction and overdose deaths
Examples rom our saes illusrae how saes are using some o he
available
ools o couner drug addicion and overdose deahs.
In 2014, ormer Gov. Marin O’Malley (D) o Maryland signed an
execuive order
o esablish an Overdose Prevenion Council o reduce he number o
overdose-relaed deahs in he sae. Te sae also creaed a saewide plan
and anoher
plan or correcional insiuions. Gov. Larry Hogan (R) coninued his
work by
esablishing he Heroin and Opioid Emergency ask Force and an
Iner-Agency
Coordinaing Council in 2015.115 Oher acions he sae has aken
include:
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
32/57
29 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
• Adding a requiremen or educaion on opioid prescribing or
all docors as a
condiion o licensure.116
• Making naloxone, which reverses a heroin overdose, available
wihou
prior auhorizaion.117
• Auhorizing via sae legislaion amily members and ohers o
carry naloxone.118
• Launching a major campaign o link people o reamen and o educae
on
overdose and addicion. Te sae also is working wih he Sae
Deparmen o
Educaion o include educaion on he consequences o prescripion
painkillers
and heroin in school curricula.119
• Promoing evidence-based reamen and increasing capaciy a
reamen ceners.120
• Working wih hospials on a volunary reporing sysem or
nonaal overdoses
so ha he sae can offer reamen o preven aal overdoses.121
• Releasing deailed annual and quarerly repors, which include
daa on deahs
by ypes o drug- and alcohol-relaed inoxicaion
deahs.122
Maryland heavily ocuses on daa and underook a projec o link daa
across
muliple sae agencies o make policy improvemens.123 Te
Overdose Prevenion
Council was able o coordinae aciviies among differen sae
agencies, break
down silos, overcome legal barriers o sharing daa, and develop a
comprehensive
daa se o individuals who died o an overdose. Tese seps helped he
sae and
local jurisdicions ideniy paterns o overdose aciviy and arge
heir public
healh responses and planned inervenions. For example, he sae was
able o
ideniy ha individuals released rom correcions aciliies were a
much higher
risk o overdose deah ollowing release. As a resul, he sae
correcions agency
ook on a greaer role in educaing inmaes on overdose prevenion
and reamen,
and he Deparmen o Public Saey and Correcional Services made
recommen-
daions o improve access o reamen.
In recen years, Florida was home o a large number o “pill
mills,” or pain man-
agemen clinics ha were improperly prescribing and dispensing
prescripion
drugs. In 2010, 93 o he op 100 oxycodone dispensing docors were
in Florida;
he number o people dying rom oxycodone overdoses in he sae was
skyrock-
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
33/57
30 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
eing. People across he counry were flooding ino Florida o obain
prescrip-
ions.124 Beginning in 2010, sae officials, wih assisance
rom he ederal Drug
Enorcemen Adminisraion, aced o sop hese abuses. Te sae:
• Required pain managemen clinics o regiser wih he sae and be
owned
by docors125
• Required physicians o regiser in prescripion drug monioring
programs,
or PDMPs126
• Disallowed physicians rom dispensing prescripion painkillers
rom
heir offices127
• Increased penalies or docors who overprescribed drugs128
Tese iniiaives have been successul: Te number o oxycodone pills
in Floridaand he number o pain clinics have been halved, and he
number o oxycodone
deahs in 2012 was less han hal he number in 2010.129
In 2012, New York passed legislaion o make changes o is PDMP in
order o
increase is effeciveness and uilizaion. PDMPs are saewide
elecronic daa-
bases ha collec daa on conrolled prescripion drugs
dispensed in he sae.
New York made he sysem more user riendly, included greaer deail
in repors
o encourage docors o use hem, allowed docors o designae saff o
access he
sysem o run repors or hem, and allowed access or licensed
pharmaciss.130
New York also now requires physicians o consul he PDMP beore
prescribing
cerain conrolled subsances.131 Addiionally, beginning in
2016, here is manda-
ory elecronic prescribing or all prescripions in he saemaking
New York he
firs sae o require his.132 Elecronic prescribing connecs
docors and pharma-
ciss elecronically and allows or easier communicaion and deecion
o raud.133
Rhode Island has insiued deailed reporing o boh aal and nonaal
drug over-
doses; he level o deail and imeliness o he daa are
rare.134 For every opioid-
relaed overdose, a hospial is required o noiy he sae healh
deparmen and
provide demographic inormaion on he paien, as well as sae wheher
naloxone was adminisered and a wha dose, where he overdose
occurred, and wheher he
person died. Te sae also quickly publicizes he number o drug
overdoses and
wha drugs were involved in he overdose, such as by heroin
mixed wih he pow-
erul painkiller enanyl. Tis inormaion helps he sae ideniy risk
acors or
overdoses, inorms is policies, and draws greaer public atenion o
he problem.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
34/57
31 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Options for implementation
Alhough none are a silver bulle, key componens o effecive
sraegies or saes
o comba addicion o prescripion drugs and heroin include he
ollowing acions.
Improving data collection and utilization
• Improve he daa collecion and analysis o measures relaed o
addicion and
overdose. Real-ime daa help healh proessionals undersand where
overdoses
are occurring and allow hem o pinpoin where o deploy resources.
Daa also
help overcome parisan differences and sigma around addicion by
allowing
people o undersand he exen o he problem and wha is happening in
heir
own communiies.
• Esablish an effecive PDMP. PDMPs can be used o analyze
prescribingpracices by physicians and pharmacies and ideniy he
uilizaion o high-risk
paiens. Mos saes currenly have PDMPs, bu hey differ in heir
unding,
use, and capabiliies, and PDMP paricipaion by providers is very
low in mos
saes.135 For insance, only 16 saes currenly require docors
o use PDMPs.136
In a sample o saes where docors can choose wheher o consul heir
sae’s
PDMP beore prescribing an opioid, hey did so only 14 percen o he
ime in
2015.137 Funding is available rom he U.S. Deparmen o Jusice
o plan, imple-
men, and enhance PDMPs.138
• Collaborae and link daa wih oher saes. For example, Maryland
recenly
announced ha is PDMP will now link o Virginia’s, and evenually o
oher
saes, o ideniy wheher paiens are filling prescripions ouside
Maryland.139
Increasing access to evidence-based treatment
• Reimburse or Screening, Brie Inervenion, and Reerral o
reamenan
evidence-based pracice used o ideniy, reduce, and preven abuse o
and
dependence on alcohol and illici drugs.140
Saes could obain ederal granunding or SBIR hrough he
Subsance Abuse and Menal Healh Services
Adminisraion, or SAMHSA, and also draw down Medicaid
maching unds.
• Increase access o reamen by expanding Medicaid. Te Affordable
Care
Ac requires coverage or subsance abuse reamen or all
insurers, including
Medicaid, bu many aduls in he 19 nonexpansion saes sill lack
access o
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
35/57
32 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
insurance and, hereore, subsance abuse reamen.141 A recen
repor rom
he Deparmen o Healh and Human Services ound ha abou 1.9
million
uninsured people wih a menal illness or subsance use disorder
live in saes
ha have no ye expanded Medicaid.142
•Increase Medicaid reimbursemen raes or oupaien reamen and
provideaddiional unding o reamen ceners o help increase ceners’
capaciy.
• Leverage available ederal unding o increase he accessibiliy o
naloxone
and increase access o MA.143 In March 2016, he Obama
adminisraion
announced ha SAMHSA is releasing new unding opporuniies or saes
o
expand heir MA services and or saes o purchase and disribue
naloxone.144
Training and education
• Develop policies o improve he prescribing o opiaes, involving
physicians,
paiens, insurers, pharmacies, and licensing boards. Licensing
boards could,
or example, require educaion o docors or conrolled subsances
licensure.
Insurers and pharmacies could esablish lock-in programs ha limi
cerain
paiens’ access o prescripions a paricular pharmacies and allow
providers o
monior paiens’ medicaion uilizaion.
• Creae public awareness and educaion campaigns o encourage he
respon-
sible use o opioid medicaions, preven addicions, and reduce
sigma. Lack o
public awareness is a major driver o opioid addicion; almos hal
o users o
opioid painkillers do no know ha hey are as addicive as
heroin.145 And hose
addiced o opioid painkillers are 40 imes more likely o become
addiced o
heroin han hose who are no dependen on opioid
painkillers.146 For example,
he Rhode Island Deparmen o Healh recenly launched a media
campaign
called “Addicion is a Disease. Recovery is Possible” ha
highlighs eigh resi-
dens’ sories o addicion and recovery.147
• Require ha medical schools in he sae include insrucion on
addicion and
subsance abuse. Currenly, he Hospial o he Universiy o
Pennsylvania is heonly medical school in he counry o require his,
bu more han 60 medical
schools have pledged ha hey will require heir sudens o ake some
orm o
prescriber educaion beginning in all 2016.148
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
36/57
33 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Improve the delivery of
long-term care
Long-erm care is a range o services and suppors o mee a person’s
daily
personal care and healh needs over an exended period o
ime.149 oday, more
han 12 million elderly or disabled Americans rely on long-erm
care, and he
demographics o many saes creae significan challenges or heir
long-erm care
sysems.150 In paricular, he number o elderly Americans is
increasingand
projeced o coninue o increasea a aser rae han he nonelderly
populaion.
Given hese rends, he need or long-erm care is projeced o double
over he
nex ew decades.151 Because Medicaid is he larges financer o
long-erm care,sae budges will bear a significan amoun o he coss rom
his increased need
or long-erm care.152
Reorms o saes’ curren long-erm care delivery sysems can no only
improve
access and qualiy bu also lower coss. Policymakers have recenly
ocused
increased atenion on hese challenges. Some saes ook advanage o
he
Balancing Incenive Program in he Affordable Care Ac o increase
access o
home and communiy-based services and o rebalance he sysem oward
nonin-
siuional setings.153 However, his unding expired in
Sepember 2015.
Options for improving long-term care
Saes can choose rom several opions o increase he susainabiliy o
heir long-
erm care sysems.
Rebalancing toward home- and community-based services
Policymakers should iniiae or build on curren effors o rebalance
heir saes’
long-erm suppors and services oward home- and communiy-based
services.
Services provided in communiy setings are ar less expensive han
services
provided in nursing homes.154 Tis ocus is paricularly
imporan as saes increas-
ingly move oward managed care delivery or hese services.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
37/57
34 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Te Communiy Firs Choice Opion or Medicaid programs, esablished
by he
ACA, offers enhanced ederal maching unds or providing
home- and commu-
niy-based atendan services and suppors.155 In order o
qualiy or he enhanced
6 percen maching rae, hese services mus be offered hroughou he
sae and
wihou a wailis. Tis enhanced maching rae can generae a
significan amoun
o new unding or a sae.156
Five saesCaliornia, Maryland, Monana, Oregon, and exascurrenly
have
approved sae plan amendmens or his opion.157 All saes
should modiy heir
Medicaid programs o include he Communiy Choice Firs Opion, which
would
make permanen he ypes o incenives ha were available on a
emporary basis
under he Balancing Incenive Program or under waivers rom he
Ceners or
Medicare & Medicaid Services, which allow saes o adop
Medicaid policies ha
differ rom sandard Medicaid requiremens.
Offering Health Homes to patients with multiple chronic
conditions
Sae Medicaid programs also should offer Healh Homes, which are
an opional
Medicaid sae plan benefi ha les saes coordinae care or Medicaid
beneficia-
ries wih chronic condiions, such as people who suffer rom
serious menal healh
condiions, subsance use disorders, ashma, diabees, hear disease,
or obesiy.158
Healh Homes can help inegrae and coordinae acue, primary, menal
healh,
and long-erm care or hese high-risk paricipans.159 Tis
inensive care coordina-
ion aims o reduce emergency room use, hospial admissions and
readmissions,
and reliance on long-erm care aciliies. In Missouri, Healh Homes
have reduced
blood pressure and choleserol, reduced hospializaions, and
saved $15.7 million
in he firs wo years.160
Healh Homes have designaed healh care providers working wih a
healh care
eam, which could include a nurse coordinaor, a menal healh
proessional, and a
pharmacis. Tey receive a ee or providing he ollowing
services:161
• Care managemen
• Prevenion and screening o menal illness and subsance use
disorders
• ransiional care rom inpaien o oher setings, such as discharge
planning
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
38/57
35 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
• Reerral o communiy and social services
• Use o healh inormaion echnology
• Reporing daa on paien oucomes
Te ACA offers significan unding or saes ha wish o implemen his
program
or heir Medicaid enrollees. For he firs wo years o he program,
he ederal gov-
ernmen will pay or 90 percen o he coss.162 Saes reain
flexibiliy in designing
paymen mehodologies and choosing eligible Healh Home providers.
Currenly,
19 saes have approved Healh Home sae plan amendmens wih
CMS.163
Saes wih managed long-erm care should require insurers o offer
similar Healh
Homes o Medicaid-eligible individuals wih chronic condiions.
Encouraging the purchase of private long-term care insurance
Mos Americans are no able o pay or heir long-erm care and
incorrecly
assume ha Medicare, privae healh insurance, or reiremen plans
will cover he
coss.164 Saes should encourage he purchase o privae
long-erm care insur-
ance by offering reundable ax credis o people who purchase
minimum levels
o privae long-erm insurance. Tese ax credis would be an upron
invesmen
ha would over ime help lower coss in he Medicaid program because
individu-
als may have oherwise relied enirely on Medicaid o und heir
long-erm care.
Compared wih he curren, limied ederal ax deducion, a reundable,
sliding-
scale sae ax credi exclusively or he purchase o long-erm care
insurance
would offer ar greaer assisance or hose who wish o buy
hese producs.
Individuals would qualiy or a credi i hey bough a qualified
long-erm care
insurance policy. o proec consumers, hese policies would be
guaraneed issue
and would include a minimum level o benefis ha could no vary
based on age or
healh saus and have proecion agains inflaion. o proec agains
adverse selec-
ionpeople waiing o buy long-erm care insurance unil hey begin o
need
ihere also would be a five-year waiing period. Te new ax credi
would beavailable o hose who firs purchase a policy when hey are
ages 60 and under; his
would urher reduce adverse selecion and keep premium
amouns affordable.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
39/57
36 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Align scope of practice with
community needs
Scope o pracice reers o he services ha a healh care proessional
is legally
allowed o provide or a paien in a paricular seting.165 In
paricular, scope-o-
pracice laws regulae he role o nurse praciioners and physician
assisans.
Nurses make up he larges segmen o he healh care workorce in he
Unied
Saes, ye many o hem ace barriers o uilizing heir raining o he
ulles exen
possible.166 Removing hese barriers would improve he
produciviy o he healh
care sysem. In addiion, sysemaic reviews o randomized conrolled
rials have
ound ha nurse praciioners and physicians provide similar qualiy
care and hapaiens are saisfied wih he care provided by a nurse
praciioner.167
Inappropriae or overbearing scope-o-pracice regulaions can
preven rained
healh care proessionals rom uilizing heir ull se o skills, limi
paiens’ access
o care and choice o providers, and increase healh care
coss.168 Allowing nurse
praciioners and physician assisans o pracice wih more
independence would
increase marke compeiion and increase he supply o primary care
providers,
hereby improving paiens’ access o providers.169 In 2014,
more han 58 million
Americans lived in areas wih primary care physician
shorages.170 Saes wih large
rural populaions ace paricular challenges: One-fifh o all
Americans live in rural
areas, bu only one-enh o physicians pracice in hese
communiies.171
As a 2010 repor rom he Insiue o Medicine on he uure o
nursing saed,
“Te asks nurse praciioners are allowed o perorm are deermined no
by heir
educaion and raining bu by he unique sae laws under which hey
work.”172
Mos saes, or example, require a physician’s supervision or nurse
praciioners
o see paiens.173 In many saes, nurse praciioners are limied
or prohibied rom
prescribing medicaions, admiting paiens o a hospial, assessing
paien condi-
ions, and ordering and evaluaing ess. Nurse praciioners also ace
paymenissues. In some saes, nurse praciioners are cerified insead o
licensed, which
creaes billing obsacles wih insurance companies and prevens
nurse praciio-
ners rom esablishing heir own pracices.174
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
40/57
37 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
A 2013 sudy o he scope-o-pracice laws ha govern nurse
praciioners working
in reail clinics, which provide quick diagnosis or reamen or
common condi-
ions in reail setings such as grocery sores, ound ha eliminaing
resricions on
scope o pracice could resul in large cos savings.175 Te
sudy ound ha he cos
per episode reaed in a reail clinic was lower in saes where
nurse praciioners
were allowed o pracice and prescribe independenly. I also
ound ha care pro- vided by nurse praciioners was o similar
qualiy o care provided by physicians.
Saes also have conduced analyses ha show poenial cos savings
rom
expanding he scope o pracice or nurse praciioners and physician
assisans
in primary care. For example, Florida’s Office o Program Policy
Analysis and
Governmen Accounabiliy ound ha he sae’s healh care sysem could
annu-
ally save $44 million in Medicaid and $2.2 million in he sae
employee healh
insurance plan by expanding scope o pracice.176
Options for implementation
Progress is being made: By he end o 2015, 21 saes had changed
heir laws o
give nurse praciioners ull pracice and prescripive auhoriy, and
anoher six
saes had expanded heir scope-o-pracice laws.177 However,
more progress is
possible, especially in he mid-Alanic and Souhern saes, where
scope-o-prac-
ice regulaions end o be more resricive. Oher saes should amend
heir sae
laws o remove burdensome barriers or nurse praciioners. For
example, saes
should require payers o direcly reimburse nurse praciioners who
are pracicing
wihin heir scope o pracice as deermined by sae law.178
Apar rom modiying scope o pracice hrough legislaion, sae
officials can ake
addiional acions. Saes can review curren scope-o-pracice
regulaions and
recommend modificaions. Saes also can se up independen
commissions o
review evidence and make deerminaions or recommendaions o he
legislaure
and governor on scope-o-pracice issues.
-
8/18/2019 State Options to Control Health Care Costs and Improve
Quality
41/57
38 Center for American Progress | State Options to Control
Health Care Costs and Improve Quality
Institute reference pricing in the
state employee plan
Healh care benefis or sae employees and reirees accoun or a
majoriy o he
growh in sae and local governmen healh care spending. Spending
on hese
benefis grew 61 percen in jus he pas six
years.179
Wih reerence pricing, insurers or employers se a maximum
price or wha hey
will pay or a paricular procedure, and paiens are
encouraged o shop around o
choose a high-value provider.180 I paiens choose a provider
wih a higher price
han he reerence price, hey mus pay he difference. Reerence
pricing also canhelp consumers make inormed decisions on heir