Embed Size (px)
Citation preview

STATE OF THE ART IN THE
TREATMENT OF PATIENTS
WITH ACUTE HEART FAILURE
MARKO TURINA University Hospital
Zurich
Switzerland


LVAD with atomic drive, built by the US Atomic
Energy Commission (1971)

Steam Engine (!) for LVAD
AEC, cca 1971

Implanted Atomic LVAF
AEC, 1971

First Clinical Application of LVAD
DeBakey 1966

Zurich paracorporeal assist system, 1976

Zürcher Kreislaufassistenz System im klinischen Einsatz, 1976

First total artificial heart implantation (DeVries & Jarvik, 1982)


MECHANICAL CIRCULATORY ASSISTANCE:
MAIN APPLICATIONS
• Short term (<2 weeks) postoperative or post
interventional support: IABP, Abiomed 5000
• Bridge to transplant or bridge to recovery:
Thoratec, Heartmate II, Micromed, Jarvik 7,
CorAid, Berlin Heart, etc.
• Permanent Implantation (“Destination
Therapy”): Abiomed, CardioWest, Lionheart

ECMO (Extracorporeal membrane oxygenation): obvious
first step in postoperative low output and urgent assist

Diastolic Augmentation
Coronary Perfusion
Assisted Aortic End-
Diastolic Pressure
MVO2 Demand
Assisted
Systole
Unassisted
Systole
Balloon
Inflation
Unassisted Aortic
End-Diastolic
Pressure
140
120
100
80
60
mm
Hg
IABP: FIRST STEP IN
PREOPERATIVE STABILIZATION
OF ACUTE CORONARY
SYNDROMS, URGENT CABG, AND
POSTOP. LOS


Fast Archimedic pumps (e.g.
Impella): very efficient for a
short period (24 hours?),
multiple contraindications
(aortoiliac disease, aortic
prosthesis or AI, more difficult
in right assist)

Tandem Heart for
percutaneous
transseptal use

Left-heart bypass with
Carlens-Dennis cannula
(1960/61)

Abiomed BVS-5000: pneumatic pumping
and filling chamber (artificial atrium)

MECHANICAL
CIRCULATORY ASSISTANCE Abiomed BVS-5000: drive console

ORTHOTOPIC ARTIFICIAL HEARTS
FROM THE SEVENTIES

ORTHOTOPIC ARTIFICIAL HEART
”Most promising” development of the eighties

Present clinical experience
Orthotopic total artificial heart
• Still excessive complication rate:
Thromboembolism und complex anticoagulation
infections und mechanical defects.
• Minimal support from the industry (e.g. Elimination
of Lionheart by Arrow).
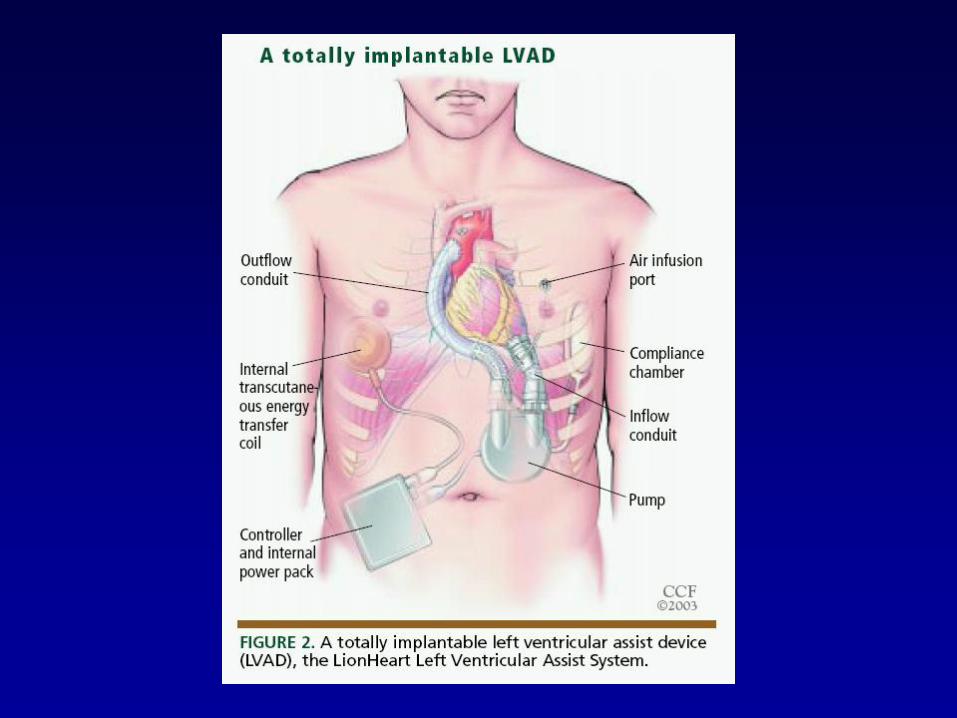
• Totally implantable systems still have major
problems: transcutaneous energy transfer, volume
compensation chamber, auto regulation
• Presently TAH can be used only in major,
specialized centers


“Lionheart”, First totally implantable LV assist
system with compliance chamber

Compliance Chamber is essential in totally
implantable systems
Implantiertes Atomherz (AEC, 1971)


In the field of mechanical circulatory assistance,
companies frequently change names, owners
and direction of development.
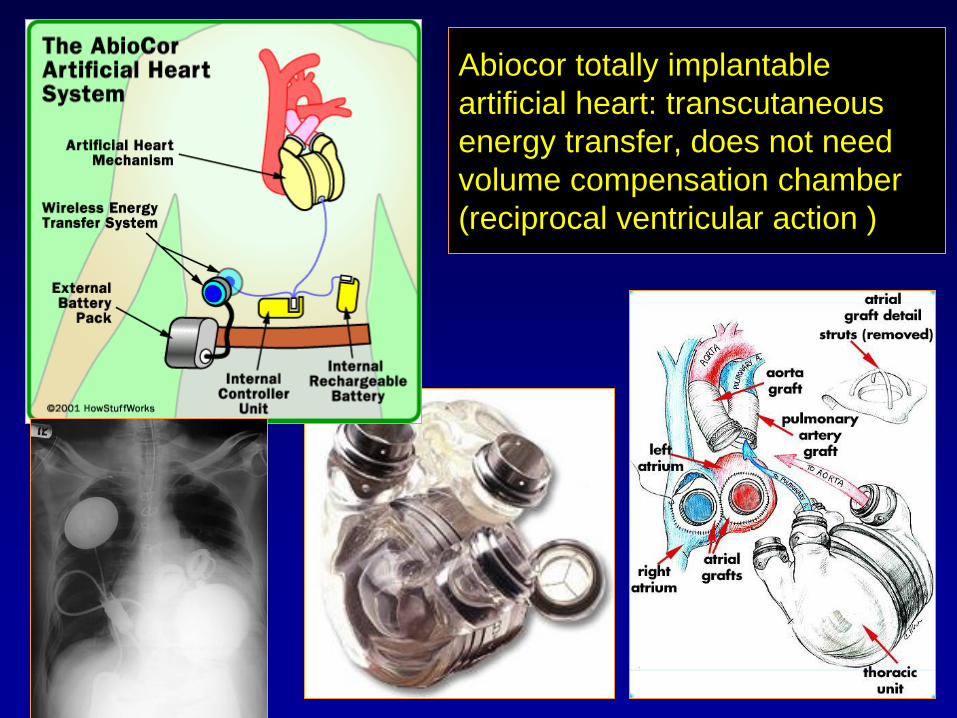
Abiocor totally implantable
artificial heart: transcutaneous
energy transfer, does not need
volume compensation chamber
(reciprocal ventricular action )

Volume compensation chamber is not necessary
in pumps with reciprocal ventricular action
(Abiocor)


Syncardia
Cardiowest
Kunstherz
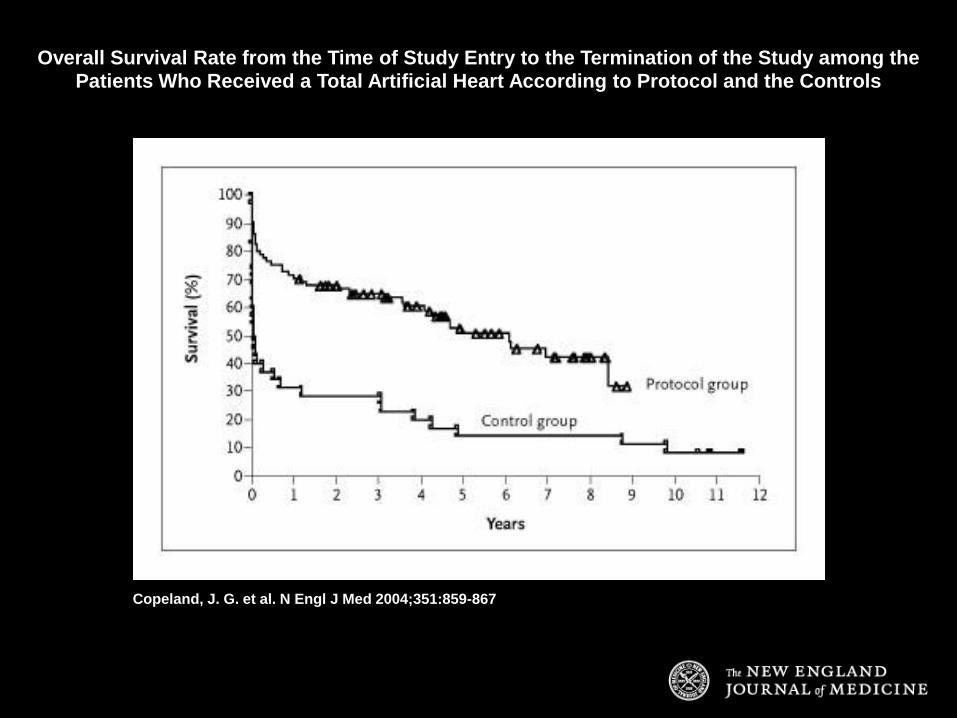
Copeland, J. G. et al. N Engl J Med 2004;351:859-867
Overall Survival Rate from the Time of Study Entry to the Termination of the Study among the Patients Who Received a Total Artificial Heart According to Protocol and the Controls
What did we learn in recent years?
Long-term circulatory assistance
Totally implantable biventricular artificial heart is
rarely used: difficult anticoagulation, mechanical
defects, infection, embolization, limited mobility
There is a widespread use of LVADs (Left Ventricular
Assist Device), as „Bridge to Transplant“, and
emerging as permanent solution (“Destination
Therapy”)

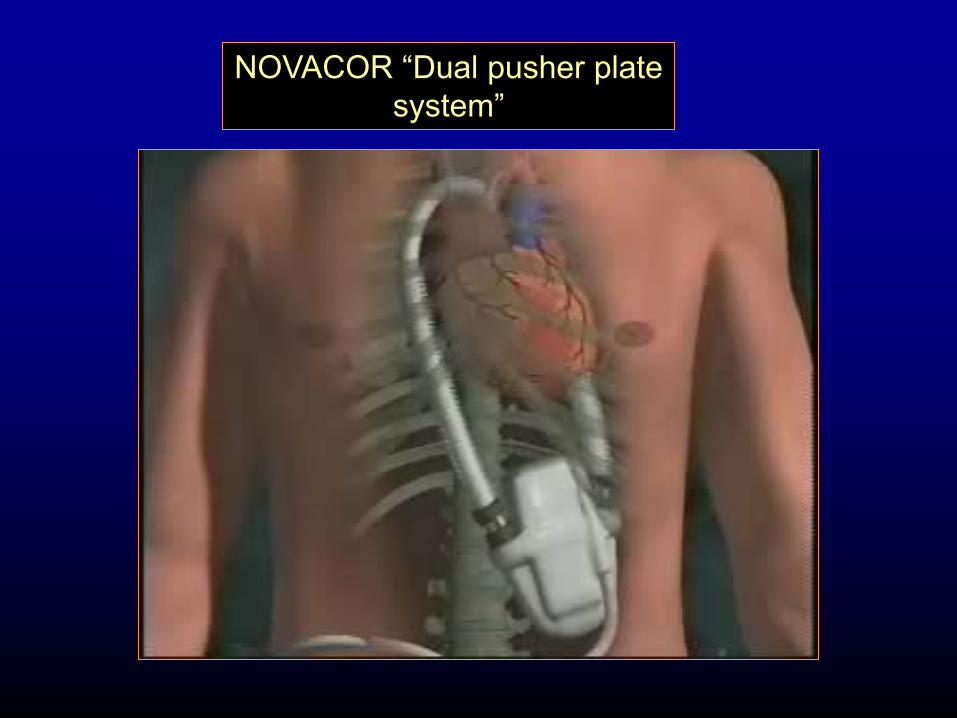
NOVACOR “Dual pusher plate
system”

NOVACOR “Dual pusher plate
system”
NOVACOR “Dual pusher plate
system”

Heart Mate XVE Device
Components

Heart Mate Device

HEARTMATE II AXIAL FLOW PUMP


THE NASA DE BAKEY LVADTM
OUTFLOW
GRAFT
LVAD

MICROMED LVAD ACTION

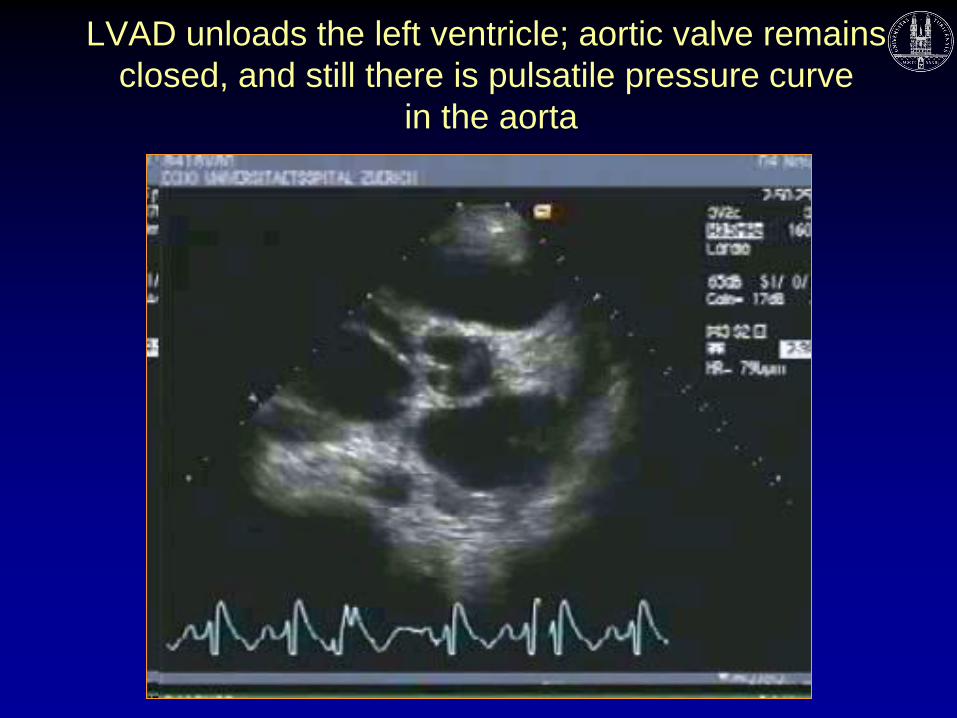
LVAD unloads the left ventricle; aortic valve remains
closed, and still there is pulsatile pressure curve
in the aorta

LVADs are not created equal: Micromed DeBakey is a
minimal pump, and a LionHeart is much bigger device!
Axial flow
pump
Transit-time
flowmeter
Aortic graft

19 year old patient with
muscular dystrophy and
cardiomyopathy, LVAD
implant in profound
cardiogenic shock; fully
recovered and mobile 2
weeks after surgery.
Successful heart
transplant 4 months
later.

Special devices for pediatric use: Berlin Heart

Trend towards smaller pumps: Coraid
Device
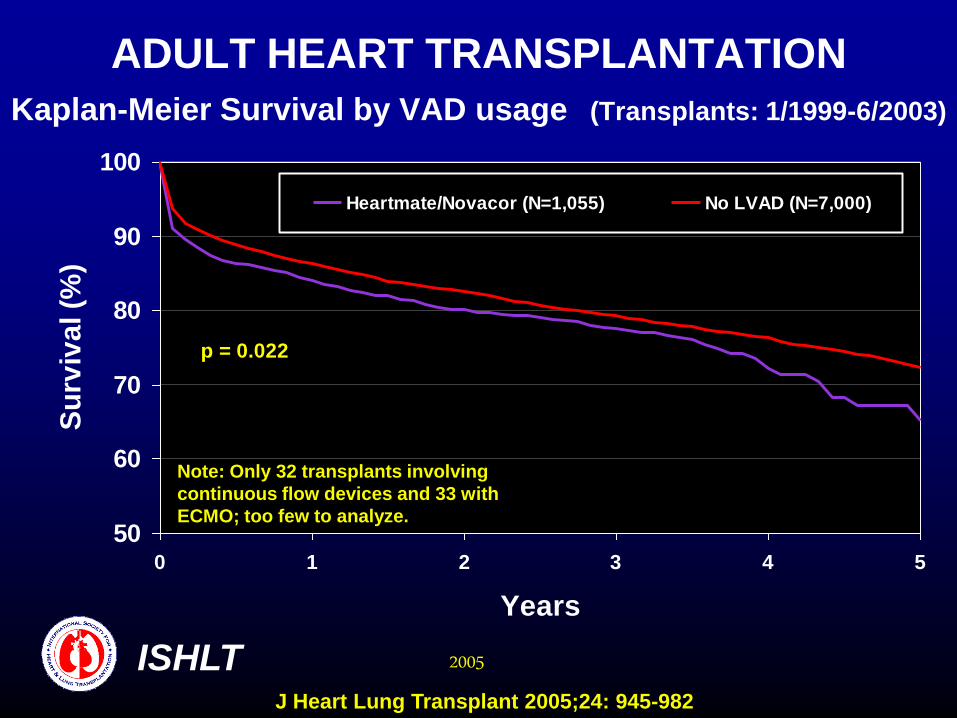
ADULT HEART TRANSPLANTATION Kaplan-Meier Survival by VAD usage (Transplants: 1/1999-6/2003)
50
60
70
80
90
100
0 1 2 3 4 5
Years
Su
rviv
al (%
)
Heartmate/Novacor (N=1,055) No LVAD (N=7,000)
p = 0.022
ISHLT 2005
Note: Only 32 transplants involving
continuous flow devices and 33 with
ECMO; too few to analyze.
J Heart Lung Transplant 2005;24: 945-982

Physical exercise in patients with
DeBakey LVAD (Zurich Experience)
• No pump manipulation necessary
• Flow increase up to 50% above
resting values regularly observed
during exercise.
• Prior to TX all patients reached
normal level of activity (NYHA I - II)
• Ambulatory treatment possible:
patients can leave the hospital

NEW GENERATION OF AXIAL-
FLOW PUMPS Recent insights
• It is not necessary to replace the whole
heart: most patients recover with an efficient
left heart bypass device alone.
• High PVR normalizes with prolonged
pumping
• Small size of the device is essential.
• High-speed (8’000-10’000 RPM) axial-flow
pumps are not necessarily hemolytic.
• Early ambulation and full mobility greatly
accelerate patient’s recovery.




Copyright ©2004 The Society of Thoracic Surgeons
Dembitsky, W. P. et al.; Ann Thorac Surg 2004;78:2123-2130
Freedom from left ventricular assist device (LVAD) failure

Clinical requirements for a widely
usable LVAD
• Reliability (safe operation ~ 2 years)
• Small size
• Needs only a low-degree anticoagulation (INR 2.0 –
2.5)
• Transcutaneous energy transfer (no wires exiting
the body)
• Several sizes of the device (children, small females,
etc.)
• Self-regulation (exercise, sleep)
• Quiet operation
• Affordable price (50 – 100 K€)
Presently, such a device does not exist!

Time between overhaul (TBO) in some well known objects
Robinson helicopter: 2’200
hours (92 days)
Piston aeroplane engine:
1’600 hours (67 days)
Jet engine: 5’000 – 8’000
hours (208 - 333 days); but
time between engine
maintenance 80-100 hours
(3-4 days)


Present state of the art in the field of
assisted circulation Summary
• LVADs belong to clinical routine in a well equipped
center.
• Best results are obtained as the bridge to transplant.
• Total orthotopic artifical heart still has too many
complications and cannot be recommended for
everyday use.
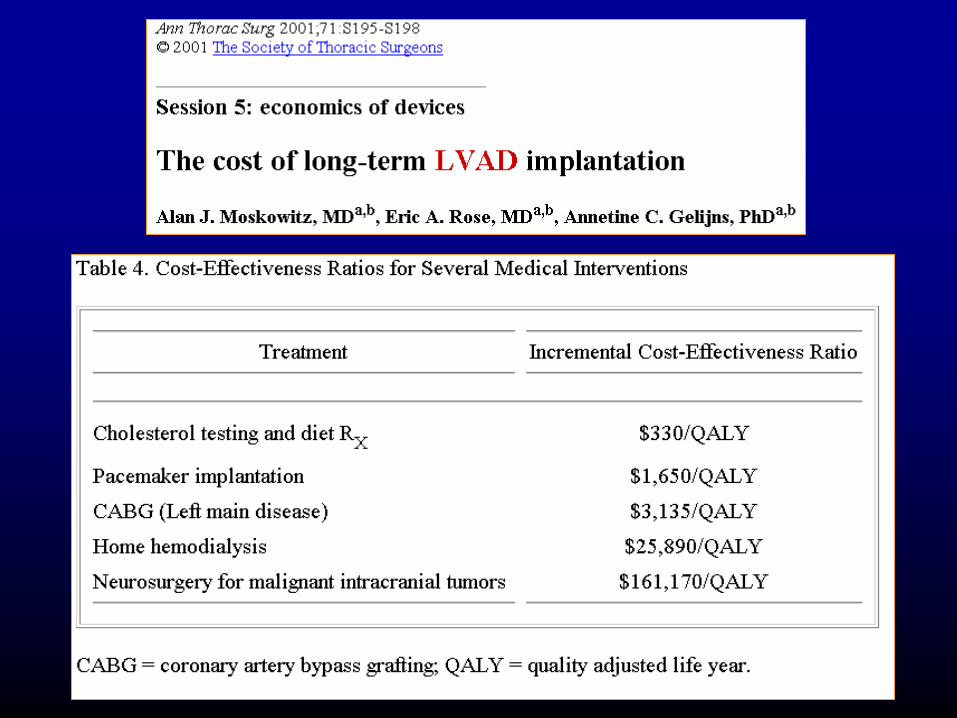
• Mechanical circulatory assistance is a cost- and
resources-intensive treatment.
• Such therapy remains reserved for a few
specialized, supraregional centers.


![Prevention of Worsening Heart Failure by Serelaxin in ... Failure/RELAX-AHF (2)].pdf · Prevention of Worsening Heart Failure by Serelaxin in Patients Admitted for Acute Heart Failure:](https://img.pdfslide.us/doc/110x75/5cce5b0088c9934c718cf98b/prevention-of-worsening-heart-failure-by-serelaxin-in-failurerelax-ahf-2pdf.jpg)


























