Embed Size (px)
Citation preview

STATE OF INDIANA
Family and Social Services Administration,
Office of Medicaid Policy and Planning
State Medicaid Health Information Technology Plan (SMHP)
Annual Update
August 2016

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 2 of 81
SMHP ANNUAL UPDATE – 2016
Version Number
Date Revision History Author(s)
1.0 December 2010 Indiana HIT SMHP first draft submitted to OMPP for review Fox Systems 1.06 January 2011 Indiana HIT SMHP submitted to CMS Jared Linder 1.09 March 2011 Indiana HIT SMHP resubmitted to CMS based on feedback Jared Linder 1.10 April 2011 Indiana HIT SMHP resubmitted to CMS with required changes
in accordance with CMS’ April 4, 2011 Letter and Enclosures A, B, and C sent to Pat Casanova, Indiana Medicaid Director. Pat Casanova received CMS’ approval of the IN HIT SMHP V1.10 by Rick Freidman via email dated April 26, 2011.
Jared Linder, Pat Casanova
1.11 March 2012 Indiana HIT SMHP developed as an annual update to be submitted to CMS; applied the State Medicaid HIT Plan (SMHP) Template to the Indiana 2012 Annual Update of the SMHP; and Applied the FSSA HIT Coordinator and HIT Project Manager changes to reflect document as the final version.
Amie Redmon, Jared Linder, Pat Casanova
2.0 March 2013 and May 2013 Numerous minor updates across the entire document.
Areas which changed most significantly include: - Update on Medicaid-related HIT activities (see section
1.2) - Update on “as-is” HIT landscape including adoption of e-
prescribing and electronic transmission of continuity of care information (see sections 1.3; 2.1; 2.4)
- Update on status of statewide HIE initiatives/activities
(see section 2.6; 2.7; 2.9; 6.3) - Update on status of related initiatives such as the projects
funded by Beacon grant awards and developments in statewide broadband-class communications deployment (see sections 2.5.3; 2.5.4)
- Reaffirmation of Indiana’s to-be vision and roadmap for
HIT and HIE in support of its medical assistance programs (Indiana Health Care Programs) (see sections 3.2; 6)
- Update on other Medicaid IT and IT-related initiatives
such as MMIS, enterprise data warehouse and PBM with enhanced IT capabilities (see sections 2.1.3; 4.4; 6.4)
- Update on EHR incentive program’s administrative
structure, system capabilities (the latter focused on MAPIR) and ongoing provider communication and outreach efforts (see sections 1.1; 4.6; 4.12..2;
4.13.2.1; 4.14) - Update on the EHR incentive program’s Audit Strategy
(also refer to the Audit Plan submitted to CMS) - Per feedback from CMS received in May 2013: added to
sections 4.8, 4.12 and 4.13 and provided a completed
Health Management Associates, Carenza Love

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 3 of 81
SMHP ANNUAL UPDATE – 2016
Version Number
Date Revision History Author(s)
2013 State Medicaid Changes Checklist as an addendum Indiana HIT SMHP Final update submitted to CMS
3.0 May 2014 Numerous minor updates across the entire document. Areas which changed most significantly include: - Update on summary of activities conducted during Year
3, and key program statistics update (see section 1.2) - Update on transition of state level designated entity
HIT/HIE leadership from IHIT to FSSA (see sections 2.1) - Update on electronic information exchange statistics
(see section 2.4) - Removed entire section on IHIT governance (formerly
section 3.1.1) - Update on executive leadership description (see
section 3.1.2) - Update on timeline of key state Medicaid HIE/HIT
initiatives (see sections 3.2 and 6.1) - Update on requirements for pre-payment review of
attestation verification (see 4.12) - Removed section on coordination with IHIT (formerly
section 4.20) - Updates on the State’s Audit Strategy (see sections 5.0,
5.4, 5.5) Indiana HIT SMHP Final update submitted to CMS
Carenza Love
4.0 June 2014 Numerous minor updates across the entire document. Areas which changed most significantly include: - Update most SMHP-U and APD-U submission and
approval dates (see section 1.1) - Summary of HIT activities conducted during Year 4 and
key program statistics update (see section 1.2) MITA self- assessment completion update (see section 2.12)
Carenza Love
4.1 April 2016 Addendum for Modifications to Meaningful Use in 2015-2017 Final Rule - Table for changes to Eligible Professional (EP) Meaningful
Use objectives and reporting periods - Table for changes to Eligible Hospital (EH) Meaningful Use
objectives and reporting periods
Myers and Stauffer, LC
5.0 August 2016 Full rewrite and/or update to all sections and subsections Myers and Stauffer, LC

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 4 of 81
SMHP ANNUAL UPDATE – 2016
Version Number
Date Revision History Author(s)
Section 6: The State’s HIT Roadmap added as required by CMS in 2015

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 5 of 81
SMHP ANNUAL UPDATE – 2016
Table of Contents A. Introduction and Overview ...................................................................................................................... 10
A.1 EHR Incentive Program Overview ..................................................................................................................... 11
A.2 Summary of HIT Activities to date in Year 5 ...................................................................................................... 12
A.3 Summary of Indiana’s HIT Future ...................................................................................................................... 13
B. Indiana’s “As Is” HIT Landscape ................................................................................................................ 15
B.1 Current HIT Environment – Overview ............................................................................................................... 15
B.2 HIT Activities Supporting Medicaid ................................................................................................................... 16
B.3 OMPP Quality Monitoring and Improvement ................................................................................................... 17
B.4 Electronic Information Exchange ...................................................................................................................... 18
B.5 Electronic Public Health Reporting .................................................................................................................... 23
B.6 Statewide HIE Networks .................................................................................................................................... 24
B.7 Core Interoperability Projects ........................................................................................................................... 28
B.8 Current HIE Architecture/Structure .................................................................................................................. 28
B.9 Governance for State Health Information Exchange ........................................................................................ 29
B.10 Veterans Administration and Indian Health Services Providers ..................................................................... 30
B.11 Medicaid Information Technology Architecture (MITA) ................................................................................. 30
B.12 MMIS HIT/HIE Environment ............................................................................................................................ 30
B.13 Summary of Medicaid Environmental “As Is” E-scan ...................................................................................... 31
C. Indiana’s “To Be” HIT Landscape .................................................................................................................. 35
C.1 Public-Private Stakeholder Cooperation ........................................................................................................... 35
C.2 Vision for HIT Environment ............................................................................................................................... 36
C.3 Public Health – Health Information Technology Strategy ................................................................................. 40
D. Activities Necessary to Administer and Oversee the EHR Incentive Program ................................................. 42
D.1 Concept of Operation and Administration ........................................................................................................ 42
D.2 Audit Work Group ............................................................................................................................................. 42
D.3 Technology Work Group ................................................................................................................................... 43
D.4 Clinical Quality Work Group .............................................................................................................................. 43
D.5 Provider Communications ................................................................................................................................. 43
D.6 Recent Changes in State Laws and Regulations ................................................................................................ 44
D.7 Policy Changes ................................................................................................................................................... 45
D.8 HIE/HIT Activities across State Borders............................................................................................................. 50

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 6 of 81
SMHP ANNUAL UPDATE – 2016
D.9 Privacy Regulatory Changes .............................................................................................................................. 50
D.10 Provider Contract Changes ............................................................................................................................. 50
D.11 Provider Eligibility Determination ................................................................................................................... 50
D.12 Processing Payments to Providers .................................................................................................................. 56
D.13 Provider National Provider Identifier (NPI) ..................................................................................................... 59
D.14 Role of Contractors in Indiana EHR Incentive Program Implementation ....................................................... 60
D.15 Reporting Requirements ................................................................................................................................. 60
D.16 Coordination with Medicare to Prevent Duplicate Payments ........................................................................ 61
D.17 Incentive Payment Recoupment ..................................................................................................................... 61
D.18 Fraud and Abuse Prevention ........................................................................................................................... 62
D.19 Provider Appeals ............................................................................................................................................. 64
D.20 Federal Financial Participation (FFP) ............................................................................................................... 64
D.21 Meaningful Use and Patient Volume Criteria ................................................................................................. 65
D.22 Dependence upon Federal Initiatives ............................................................................................................. 68
E. The State’s Audit Strategy ........................................................................................................................... 70
E.1 Category 1 – Incentive Payment Audits ............................................................................................................ 70
E.2 Category 2 – Administrative Expense Audits ..................................................................................................... 71
E.3 Audit Settings..................................................................................................................................................... 71
E.4 Audit Methodologies, Standards, Processes, and Procedures .......................................................................... 72
E.5 Audit Planning ................................................................................................................................................... 74
F. The State’s HIT Roadmap ............................................................................................................................. 78
F.1 Moving from “As Is” to “To Be” HIT Landscape ................................................................................................. 78
F.2 Tactics to Support the Strategy for the HIT Roadmap ....................................................................................... 78
F.3 MMIS-Related Activities .................................................................................................................................... 81
F.4 HIT Objectives for Meaningful Use of Clinical Data ........................................................................................... 81

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 7 of 81
SMHP ANNUAL UPDATE – 2016
List of Key Terms and Acronyms The following acronyms are used throughout the document:
Acronym Definition ACA Affordable Care Act ADT Admit, Discharge, Transfer
AHRQ Agency for Healthcare Research and Quality AIU Adopt, Implement or Upgrade CAH Critical Access Hospital CCD Continuity of Care Document CCN CMS Certification Number
CEHRT Certified Electronic Health Record Technology CHC Community Health Center CHIP Children's Health Insurance Program
CHIRP Children and Hoosier Immunization Registry Program CHPL ONC Certified EHR Health IT Product List CIO Chief Information Officer
CMO Care Management Organization CMS Centers for Medicare & Medicaid Services CPOE Computerized Physician Order Entry CQM Clinical Quality Measure D4D DOCS4DOCS® DA Division of Aging
DDRS Division of Disability and Rehabilitative Services DFR Division of Family Resources
DMHA Division of Mental Health and Addiction DUA Data Use Agreement ED Emergency Department
EDW Enterprise Data Warehouse EH Eligible Hospital
EHR Electronic Health Record ELR Electronic Laboratory Reporting EP Eligible Professional
ESB Enterprise Service Bus ESSENCE Electronic Surveillance System for the Early Notification of Community-based Epidemics
FA Fiscal Authority FCC Federal Communications Commission FFP Federal Financial Participation FFS Fee-for-Service FFY Federal Fiscal Year
FQHC Federally Qualified Health Center FSSA Indiana Family and Social Services Administration

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 8 of 81
SMHP ANNUAL UPDATE – 2016
Acronym Definition GUI Graphic User Interfaces
HEDIS Healthcare Effectiveness Data and Information Set HHS Health and Human Services HIE Health Information Exchange HIO Health Information Organization HIP Healthy Indiana Plan
HIPAA Health Insurance Portability and Accountability Act HISP Health Information Service Provider HIT Health Information Technology
HITECH Health Information Technology for Economic and Clinical Health Act HP Hewlett Packard IAC Indiana Administrative Code
IAPD Implementation Advance Planning Document IAPD-U Implementation Advance Planning Document Update
IHA Indiana Hospital Association IHCP Indiana Health Care Programs IHIC Indiana Health Informatics Corporation IHIE Indiana Health Information Exchange IHIT Indiana Health Information Technology, Inc. IHS Indian Health Services IIS Immunization Information System
INPC™ Indiana Network for Patient Care™ IPHCA Indiana Primary Health Care Association
IRS Internal Revenue Service ISDH Indiana State Department of Health ITN Indiana Telehealth Network LEIE List of Excluded Individuals Entities
MAPIR Medical Assistance Provider Incentive Repository MCO Managed Care Organization MED Medicare Exclusion Database MHIN Michiana Health Information Network MITA Medicaid Information Technology Architecture MMIS Medicaid Management Information System MOU Memorandum of Understanding MSLC Myers and Stauffer LC MTF Camp Atterbury Medical Treatment Facility MU Meaningful Use NCD Notifiable Conditions Detector
NCQA National Committee for Quality Assurance NPI National Provider Identifier
NPPES National Plan and Provider Enumeration System

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 9 of 81
SMHP ANNUAL UPDATE – 2016
Acronym Definition OMPP Office of Medicaid Policy and Planning ONC The Office of the National Coordinator PAPD Planning Advance Planning Document PCCM Primary Care Case Management PECOS Provider Enrollment, Chain and Ownership System
PHA Purdue Healthcare Advisors PHA Public Health Authority
PHESS Public Health Emergency Surveillance System PTN Practice Transformation Network PY Program Year
R&A Medicare & Medicaid EHR Incentive Program Registration & Attestation System REC Regional Extension Center RHC Rural Health Center SDE State Designated Entity
SHIECAP Health Information Exchange Strategic and Operational Plan SMHP State Medicaid Health Information Technology Plan SOA Service Oriented Architecture SSA Social Security Administration SUR Surveillance Utilization and Review TA Technical Assistance
TCPI Transforming Clinical Practice Initiative TIN Taxpayer Identification Number
VLER Virtual Lifetime Electronic Record VXU Unsolicited Vaccination Record Update

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 10 of 81
SMHP ANNUAL UPDATE – 2016
A. Introduction and Overview The Indiana Family and Social Services Administration (FSSA) in conjunction with The Office of Medicaid Policy and Planning (OMPP) is the State entity responsible for administering the Indiana Medicaid program with approximately 1.46 million enrollees1. FSSA is committed to improving the quality of care for Medicaid beneficiaries in the State and the health status of this population and strongly believes that health information technology (HIT) can have a significant impact on health care quality, outcomes, and health status. Thus, FSSA is committed to continuing to work with health care providers to better serve their patients through data sharing of electronic health information and meaningful use of HIT.
The implementation of the Medicaid Electronic Health Record (EHR) Incentive Payment Program initiative (hereafter referred to as the “EHR Incentive Program” or “Program”) is a major cornerstone towards improving provider access to, and use of, electronic health information that should lead to improved health outcomes and status for Medicaid members. Since May 2, 2011, the State of Indiana has been operating its EHR Incentive Program per 42 CFR Parts 412, 413, 422, 495, et al. Funding for the Program is provided at a 90% match by the Centers for Medicare & Medicaid Services (CMS), while the State of Indiana provides the additional 10% matching funds for program administration activities.
In order to participate in the EHR Incentive Program, a State Medicaid Health Information Technology Plan (SMHP) must be submitted and approved by CMS. Moreover, a Medicaid HIT Implementation Advance Planning Document (I-APD) must be submitted by the State and approved by CMS before federal funding can be accessed for program administration and incentive payments to eligible professionals (EPs), eligible hospitals (EHs) and Critical Access Hospitals (CAHs). The State’s first SMHP and Medicaid HIT I-APD was approved by CMS in April 2011 and an update (IAPD-U) was submitted in November 2014 and approved in March 2015. The State submitted and CMS approved an SMHP addendum for the Modifications to Meaningful Use (MU) in 2015-2017 final rule in March 2016.
Indiana developed the requirements needed to build the operations and IT infrastructure for operating the Program and while the IT infrastructure is substantially in place, the operations infrastructure continues to evolve particularly in response to the requirements in the Modifications to Meaningful Use in 2015-2017 final rule published in October 2015.
In 2010, the Governor of Indiana established Indiana Health Information Technology, Inc. (IHIT) as the state designated entity (SDE) to build on the established work of the four successful private sector health information organizations (HIOs) and named a HIT Coordinator to lead this effort. The four HIOs include: HealthBridge, HealthLINC, Indiana Health Information Exchange (IHIE) partnered with the Regenstrief Institute, and Michiana Health Information Network (MHIN). Since health information exchange (HIE) is a critical enabler of EHR meaningful use, the State incorporated many elements of the HIE Strategic and Operational Plan (SHIECAP) into its original SMHP. The original SHIECAP was approved by the Office of the National Coordinator of Health Information Technology (ONC) on January 21, 2011. The ONC-funded grant funding for IHIT expired in March 2014, and the State transitioned the oversight role to FSSA for all statewide HIT/HIE related initiatives and continued coordination of the HIT infrastructure. This SMHP update reflects the ongoing effort to ensure that the SMHP and SHIECAP remain aligned.
1 Based on information in statehealthfacts.org (a publication of the Kaiser Family Foundation)

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 11 of 81
SMHP ANNUAL UPDATE – 2016
During the latter part of 2011, Indiana determined a number of critical projects that had to be implemented for the EHR Incentive Program initiatives for Year 2. An IAPD-U was submitted on December 29, 2011 and approved by CMS on January 18, 2012. The State submitted the most recent IAPD-U in November 2014, with a supplemental submission on January 8, 2015, and received CMS approval on March 3, 2015, in the continued support of the following key activities:
• Development and implementation of verification processes of EPs, EHs, and CAHs regarding their efforts to adopt, implement, or upgrade (AIU) Certified Electronic Health Record Technology (CEHRT) and the meaningful use of said technology as a condition of receiving incentive payments;
• Implementation and ongoing support of the Medical Assistance Provider Incentive Repository (MAPIR) System, a multi-state collaborative effort that funded an EHR Incentive Program administration system that interfaces with Indiana’s Medicaid Management Information System (MMIS);
• Development and implementation of program integrity procedures and related system changes;
• Development and implementation of the EHR Incentive Program Audit Plan; and
• Provider outreach, training and education on EHR Incentive Program rules and the meaningful use of CEHRT.
A.1 EHR Incentive Program Overview Implementation and meaningful use of CEHRT will improve access to health information for Indiana Medicaid members and providers. Certified EHRs facilitate easier coordination of care for the many providers who may be treating a Medicaid patient and provide patients with more readily accessible information needed to make important decisions about their health care. Indiana Medicaid will have access to clinical and administrative information for children, pregnant women, disabled, and adult populations and will use this information to improve coordination of care and health outcomes for those Hoosiers served.
The State of Indiana has adopted the national goals for the EHR Incentive Programs; these include:
1) Enhance care coordination and patient safety;
2) Reduce paperwork and improve efficiencies;
3) Facilitate electronic information sharing across providers, payers, and state lines; and
4) Enable data sharing using state HIEs and the Sequoia Project eHealth Exchange (eHealth Exchange).
Achieving these goals will improve health outcomes, facilitate access, simplify care, and reduce costs of healthcare nationwide. In accordance with provisions within the American Recovery and Reinvestment Act (ARRA), OMPP implemented the Indiana Medicaid EHR Incentive Program to provide incentive payments to eligible EPs, EHs, and CAHs. Additionally, OMPP has worked closely with federal and state partners to ensure the Medicaid EHR Incentive Program aligns with the SHIECAP, thereby advancing state-level and national goals for HIE.
The incentive payments directed to EPs, EHs, or CAHs are not reimbursement for services rendered by these providers; they are issued to incentivize the adoption, implementation or upgrade of CEHRT and the subsequent meaningful use of CEHRT as defined by CMS.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 12 of 81
SMHP ANNUAL UPDATE – 2016
OMPP elected to leverage business processes throughout the agency and, where feasible, integrate the Indiana EHR Incentive Program into the standard Medicaid Information Technology Architecture (MITA) business processes and OMPP’s day-to-day operations. During the Implementation Phase, OMPP developed state-specific business processes where a MITA business or organizational process was not identified. Examples of these processes include Indiana EHR Incentive Program eligibility, Indiana Health Care Programs (IHCP) member volume, attestation receipt and validation, and provider registration and query to the Medicare & Medicaid EHR Incentive Program Registration & Attestation System (R&A).
During 2013 and into 2014, OMPP transitioned the driver for incentive payments in accordance with the MU Stage 2 rule and will transition to the modified Stage 2 ruling in 2015 and 2016. As part of the MAPIR multi-state collaborative, all regulation changes for modified MU Stage 2 have been completed by Hewlett Packard and the implementation of the upgrade to MAPIR has commenced. Indiana’s most recent MAPIR upgrades include a combination of version 5.6 and 5.7, which was implemented in July 2016. Any future regulation changes that affect provider attestations will be handled in the same manner.
A.2 Summary of HIT Activities to date in Year 5 Major Program achievements in Year 5 included, but were not limited to:
• Opening of Program Year (PY) 2015 for EPs, EHs, and CAHs: o PY 2015 opened briefly in 2015 to allow AIU and MU attestations to the Indiana R&A before it was
closed due to the Modification to Meaningful Use in 2015-2017 final rule. o PY 2015 re-opened on July 11, 2016, for additional AIU and MU attestations incorporating the
changes in the Modification final rule published in October 2015. • Continuation of audit program per the Audit Plan submitted to CMS:
o In 2015, the State resumed AIU audits from PY 2014 recipients. o The State has also completed EP MU audits from PY 2013 recipients.
• From an information systems perspective, the State continued to participate in the MAPIR collaborative. MAPIR continues to supports the Program’s administrative requirements for meaningful use-based incentive payments.
o Version 5.6 and 5.7 of MAPIR went live in July 2016.
The following table (next page) shows incentive payment statistics for EPs, EHs and CAHs as of April 20162.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 13 of 81
SMHP ANNUAL UPDATE – 2016
Figure 1: Key EHR Incentive Program Statistics
Type Amounts/Totals Eligible Professionals
Unique EP Count 2,887 # AIU Payments 2,772 AIU Payment Total $58,451,688.00 # MU Payments 2,124 MU Payments Total $19,065,530.00
Total EP Payments to Date $77,517,218.00 Eligible Hospitals
Unique EH/CAH Count 125 # AIU Payments 100 AIU Payment Total $62,346,576.83 # MU Payments 199 MU Payments Total $68,093,291.42
Total EH/CAH Payments to Date $130,439,868.25 GRAND TOTAL $207,957,086.25
2 Based on information from the CMS Combined Medicare and Medicaid Payments by State and Unique Count of Providers by State reports from CMS.gov.
In the first three (3) Federal Fiscal Years (FFYs) of the EHR Incentive Payment Program, OMPP estimated that approximately 3,225 EPs and 76 EHs in the state of Indiana would receive $148 million in EHR Incentive Payments covered at 100% federal financial participation (FFP) under ARRA. The EH estimation was exceeded including attestations and payments in early 2015 while outreach efforts continue to include potential EPs in PY 2015 and PY 2016, the last year to attest to AIU and/or join the Medicaid EHR Incentive Program.
A.3 Summary of Indiana’s HIT Future OMPP recognizes that the Medicaid Program will play a significant role in transforming health care in Indiana and has developed its vision for HIT to address many of the challenges of integration with the HIO networks.
Replacement of the MMIS is a priority project for OMPP. The new MMIS, currently planned to be fully in production by the end of 2016, will provide improved functionality including Service Oriented Architecture (SOA), Enterprise Service Bus (ESB), a rules engine, and automated workflow functions that will support HIT/HIE efforts. The focus aimed at obtaining new technology and then leveraging this technology is an integral part of the statewide HIT solution.
Implementation of EHRs will improve access to health information for Indiana Medicaid members and providers. EHRs facilitate easier and quicker coordination of care for the many providers who may be treating a Medicaid patient and provide patients with more readily accessible information needed to make important decisions about their health care. Indiana Medicaid will have access to clinical and administrative information for children, pregnant women, disabled, and adult populations and will use this information to improve coordination of care and health outcomes for those Hoosiers served.
The State has data use agreements (DUA) in place with two state HIOs including a DUA with IHIE through June 2017

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 14 of 81
SMHP ANNUAL UPDATE – 2016
and a DUA with MHIN through February 2017. In addition, the State has a Memorandum of Understanding (MOU) with the Indiana State Department of Health (ISDH) through June 2017.
OMPP began making incentive payments for MU in 2013 and continued 2014 and 2015. Activities surrounding Modified MU Stage 2 and gathering Clinical Quality Measures (CQMs) are defined in later sections of this SMHP.
To support the implementation of the EHR Incentive Program, OMPP instituted three work groups:
1. Audit Work Group 2. Technology Work Group 3. Quality Work Group
These work groups were designed to advise the core OMPP team managing the EHR Incentive Program. The scope of their advisory function included but was not limited to:
• Developing and reviewing existing policies (e.g. Audit, Program Integrity, Clinical Quality Review, and Quality Improvement Measures, etc.);
• Building EHR Incentive Program-specific policies, procedures, and checklists; • Ensuring that desk audits and field audits are conducted in a manner that has a defined criteria for
selection; • Results presentation and reportable opportunities for improvement; and • Management of regulatory or financial infractions.
Having completed four (4) successful years for the EHR Incentive Program, OMPP informally dissolved the above mentioned work groups; however, OMPP and FSSA staff meet regularly to discuss audits and works closely with Indiana’s third-party auditor, Myers & Stauffer LC. Indiana continues to participate in the HP MAPIR multi-state collaborative and works closely with the MMIS and MITA implementation and management teams.
As Indiana’s EHR Incentive Program is further refined and improved upon within, and further defined by CMS with tools refined by the ONC, the State will update any changes necessary in regulations, policy, program, and/or processes. In addition to the updated SMHP, the necessary IAPD(s) will also be developed, updated, and submitted to CMS.
Advancing Indiana’s MITA maturity within each of the current MITA Business Areas will also continue. Following are just some of the initiatives designed to further the State’s MITA capability maturity:
• The new MMIS; • A new Enterprise Data Warehouse (EDW); • A new Pharmacy Benefits Management (PBM) solution; • A series of HIE initiatives including support of ePrescribing, exchange of prior authorization data and
clinical data exchange; and • Design and deployment of an Integrated Eligibility Determination solution for the State’s health care
programs.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 15 of 81
SMHP ANNUAL UPDATE – 2016
B. Indiana’s “As Is” HIT Landscape Indiana completed an initial environmental scan (e-scan) in 2010 as part of its initial SMHP plan to establish a baseline for assessing levels of provider EHR adoption and HIE connectivity. The e-scan revealed widespread adoption of industry leading EHR products among providers primarily in urban areas, and interest from rural provider practices and clinics in how the EHR Incentive Program might help them to acquire EHR capacity. At the time of the scan, Indiana was home to four (4) well-established Regional Health Information Organizations (HIOs). The Governor also established the Indiana Health Information Technology, Inc. (IHIT) in 2010 as the state’s designated entity for HIE to lead statewide HIE planning and coordination as part of the State HIE Cooperative Agreement Program (SHIECAP).
A second e-scan was performed for this current update to the SMHP in May and June 2016 to reassess the overall adoption of CEHRT in Indiana as well as the transition of the SDE to the state. This e-scan expanded from the original e-scan in 2010 and incorporated surveys and interviews with statewide stakeholders not previously surveyed including mental and behavioral health centers, home health providers, long-term care and rehabilitation facilities, and ambulance services. An overview of the 2016 e-scan is included below in Section B.13.
B.1 Current HIT Environment – Overview Indiana’s HIT environment is active with multi-faceted efforts to support provider HIT capacity and foster the sharing of clinical and administrative data to improve health care and support system improvements. The State has taken an active role through its state health agencies and Medicaid program to promote HIT adoption and HIE development, building upon its private health care marketplace. Indiana continues to be home to four well-established HIOs, each functioning in different capacities for community partners. In addition to the HIO efforts with their providers, the State continues to work with one of the original Regional Extension Centers (REC). IHIT’s former role as the SDE has now transitioned to FSSA under its Healthcare Strategies and Technologies division and actively participates in the Indiana Hospital Association’s (IHA) Council on Information Management and Health Information Exchange Task Force. The State’s range of activities will include workgroups, educational forums, targeted activities related to the EHR Incentive Program, and convening activities to foster targeted strategic and tactical plans for expanding HIT and HIE capacity.
With leadership from the HIT Coordinator, FSSA is supporting coordination and collaboration among the HIOs and OMPP to foster data sharing among Medicaid providers to promote heath care quality and efficiency. OMPP is contracting with IHIE to aggregate Medicaid claims with medical and pharmacy data in its repository to create a Continuity of Care (CCD) record that can be shared between Medicaid providers. OMPP is also in the planning phase of a similar initiative with the Michiana HIE.
E-prescribing is increasing, as evidenced by dramatic increases in the numbers of pharmacies connected to the Allscripts network and e-prescribing rates among providers that have risen exponentially year after year since 2010. In line with the State’s SHIECAP targets at the end of the first quarter of 2013, the HIOs implemented standardized CCDs via Connect gateways to increase hospital’s ability to access clinical care summaries. A consumer engagement strategy is being implemented to expand use of PHR portal and access to immunization records.
For Medicaid providers in particular as of early 2016, statistics from Indiana’s EHR Incentive Program show that more

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 16 of 81
SMHP ANNUAL UPDATE – 2016
than 2,800 EPs and 125 EHs and CAHs have received at least one incentive payment for the adoption and meaningful use of an EHR.
B.2 HIT Activities Supporting Medicaid Within Indiana’s executive branch, two agencies administer Medicaid and other health care programs. The Indiana Family and Social Services Administration (FSSA) and its Office of Medicaid Policy and Planning (OMPP) are responsible for the Medicaid program as the designated state agency under the federal Medicaid statute. The Indiana State Department of Health (ISDH) is the public health agency for the state and oversees the local health departments. ISDH is responsible for most of Indiana’s health programs. The Executive Board of ISDH, the agency’s ultimate authority, and the State Health Commissioner are appointed by the governor. The State Health commissioner is the secretary of the Executive Board and the chief executive of ISDH. By law, the commissioner must be licensed to practice medicine in Indiana.
The Secretary of FSSA and the Commissioner of ISDH are required by statute to coordinate related programs, including the Medicaid program. The Secretary of FSSA is accountable for formulating overall policy for family, health, and social services in Indiana, including the resolution of administrative, jurisdictional, or policy conflicts between a division of FSSA and ISDH. By statute, FSSA must advise the Commissioner of ISDH of proposed rules affecting common areas of interest, including Medicaid, and obtain comments from ISDH on the proposed rule. Indiana has multiple health services programs with overlapping constituencies in both FSSA and ISDH. Other divisions in FSSA with Medicaid responsibilities include the Division of Aging (DA), Division of Disability and Rehabilitative Services (DDRS), which administers Medicaid waivers for home-based, long term care for the elderly, disabled and other special populations, and the Division of Family Resources (DFR) which has eligibility determination responsibilities in programs for children, pregnant women and low income families, and the Division of Mental Health and Addiction (DMHA).
The Children’s Health Policy Board, comprised of the Secretary of FSSA, the State Health Commissioner, the Insurance Commissioner, the State Personnel Director, the Budget Director, the State Superintendent of Public Instruction, and the Director of the Division of Mental Health, directs policy coordination for Indiana’s children's health programs, including Children’s Health Insurance Program (CHIP).
Under the auspices of OMPP, the Hoosier Healthwise Program provides health care services to Indiana’s children, low-income families and pregnant women. Individuals who enroll in Hoosier Healthwise are eligible for either Medicaid benefits or benefits through the Children’s Health Insurance Program (CHIP).
The State contracts with Managed Care Organizations (MCO) to provide services to Hoosier Healthwise enrollees through a medical home and a committed provider network throughout the State. Hoosier Care Connect is an enhanced Primary Care Case Management (PCCM) Program provided through OMPP, which contracts with three Care Management Organizations (CMOs).
Medicaid HIT related activities are overseen by both FSSA - through the Healthcare Strategies and Technologies Division and ISDH. The HIT Coordinator plays a coordination role between the agencies and with the range of external entities who participate in aspects of the Medicaid program that rely upon sharing electronic health data.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 17 of 81
SMHP ANNUAL UPDATE – 2016
B.3 OMPP Quality Monitoring and Improvement The overarching mission of the Indiana Office of Medicaid Planning and Policy (OMPP) is to improve the health and quality of Hoosier lives through planning and initiatives concentrating on timely access to health care, cost management, and quality. The Indiana OMPP works to achieve this mission through a strategy that involves data driven decision making, implementation of evidence-based practices, fiscal responsibility, and active engagement with providers, members, health plans, and state and local governments.
OMPP supports a multi-faceted program of value-based contracting to serve Indiana’s Medicaid and CHIP population, including a strategy for ongoing quality improvement relying upon HIT supported quality reporting and analysis. OMPP began collecting quarterly reports from the MCOs on a variety of quality indicators for preventive health, for children and adolescents, and for pregnant women, and newborns. This increased access to data allowed the OMPP to track and monitor performance on key quality indicators and steer the focus toward improvement activities.
Effective January 1, 2008, the Healthy Indiana Plan (HIP) benefits became available through private insurers. The State contracts with three insurance carriers for the HIP program, Anthem, MDWise and Coordinated Care Corporation, to ensure comprehensive and committed health networks across the State are offering a choice of plans to Medicaid enrollees. HIP insurance carriers are required to submit claims/encounter-based, outcomes measures to assess the provision of various screening and prevention measures, as well as immunizations.
OMPP also administers the Primary Care Case Management, which contracts with three CMOs, to assist with care coordination, provider relations and member services. Hoosier Care Connect care management services for special populations with disabilities and chronic illnesses. The Hoosier Care Connect contracts include incentive and reporting requirements for addressing conditions amenable to care management, reflecting the unique needs of the disabled and wards/fosters population. OMPP has been able to incrementally raise performance benchmarks, such as well child visits for children 0 to 15 months of age where the percentage of members with six or more visits during the first 15 months of life were measures based on the Healthcare Effectiveness Data and Information Set (HEDIS) W15 using hybrid data. All three MCOs improved year over year from 2011 – 2013.
Over time, OMPP has gathered and evaluated clinical quality measures based on paid claims/encounters stored in the MMIS to monitor Medicaid utilization and quality variables. Within the State government, electronic data sharing was instituted between the OMPP and DMHA as well as ISDH, including county level data, to monitor and improve the quality of care for pregnant women, children, and those with serious mental illness. Standardized assessments of persons receiving care at the State’s Community Mental Health Centers are received by DMHA and linked to Medicaid claims data in order to better understand total utilization of mental health services.
OMPP created the Quality Strategy Committee and holds quarterly meetings where performance data is shared. The Committee’s role is to assist in the development and monitoring of the identified goals and objectives and to advise and make recommendation to OMPP. The members of the Quality Strategy Committee include: OMPP, FSSA, DMHA, ISDH, providers, health plan quality managers, advocacy groups, consumers, and members of academia.
Having accomplished operational implementation of the EHR Incentive Program, OMPP is in the process of re-aligning its internal and external quality oversight and improvement processes to integrate reporting of CQMs and other measures of health care provider performance, update quality improvement strategies with its partner HIOs,

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 18 of 81
SMHP ANNUAL UPDATE – 2016
and identify the most productive way in which OMPP staff can utilize these measures and capabilities.
B.4 Electronic Information Exchange Indiana has robust exchange of health information across the public and private stakeholders. OMPP administers the Medicaid program in Indiana and is the largest payer in the State and supports electronic information exchange for claims and measurement data. Information exchange is expanding across clinical care delivery providers, payers, and public data resources. Multiple data sources and data receivers are working collaboratively to provide technical services to facilitate the exchange of health information to improve data interoperability to improve secure and appropriate use of health data to inform treatment, payment, and population health. Indiana leveraged multiple funding Health Information Technology for Economic and Clinical Health Act (HITECH) grant opportunities advancing EHR technology adoption, connecting data sources, improving interoperability of health information, improving outcomes and measurement, and coordinating state and federal health IT initiatives. Indiana’s Health IT and Exchange progress is noted below.
B.4.1 Electronic Clinical Laboratory Ordering and Results Delivery Across Indiana, laboratories and providers are primarily using Directed Exchange to support electronic clinical laboratory results delivery. Historically, providers have used the electronic order entry hosted by laboratory providers outside of HIO web portals or EMR interfaces. However, the state’s major HIOs are evolving with their architectures to begin to serve as hubs for lab ordering and results delivery; integration has been completed to enable results sharing between sub-state HIOs, and increased capacity to support ELR with public health. IHIT offered incentive payments for rural hospitals and clinics to connect to HIE infrastructure, either through sub-state HIOs or via direct messaging, to send and receive lab results. As a result of these incentives, over 92% of providers at Federally Qualified Health Centers (FQHC), Community Health Centers (CHC), and Rural Health Centers (RHC) were connected to an HIO at the end of 2013.
DOCS4DOCS® (D4D) is an electronic results delivery service provided by the Indiana Health Information Exchange (IHIE). It offers a single source for clinical information such as lab results, radiology reports, transcriptions, pathology and hospital admissions reports, discharge and transfer reports from all participating Indiana hospitals, physician practices, labs and radiology centers. Results can be viewed through a web-based portal or delivered directly into an electronic medical record system. IHIE’s D4D Service is used by as clinical messaging application in which more than 25,000 providers in over 6,000 locations throughout Indiana receive clinical results as the ordering physician.
IHIT worked to assist independent labs in establishing connectivity with the state’s HIE infrastructure, including public health ELR.
B.4.2 Exchange of Continuity of Care Information Efforts are currently underway to drive interoperability between the sub-state HIOs and expand the ability to deliver results and messages to any provider connected to one of the sub-state HIOs. All four of the HIOs accomplished this by launching shared provider directories and Direct-compliant transport by implementing Health Information Service Provider (HISP) protocols. As part of statewide interoperability initiatives, the sub-state HIOs

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 19 of 81
SMHP ANNUAL UPDATE – 2016
are leveraging Direct messaging as well as certified participants of the Sequoia Project eHealth Exchange (formerly known as NwHIN) Connect software standards to actively exchange consolidated care summaries using a continuity of care document (CCD) format. Using eHealth Exchange gateways, they are able to query other data sources to identify if additional information exists on a patient. Patient information is merged into a single document by the HIO initiating the query then delivered to the point of care via Direct messaging. Currently, approximately 38 of Indiana’s hospitals are electronically sharing care summaries with unaffiliated hospitals and providers. To date, more than 9.7 million Admit-discharge-transfer (ADTs) and 650,000 CCDs were shared in 2016 alone.
B.4.3 Broadband Internet Access and Telehealth Indiana received $16 million from the Federal Communications Commission's (FCC's) Rural Health Care Pilot Program, and as a result, created the Indiana Telehealth Network (ITN). Since 2010, ITN and the Indiana Broadband Mapping Project have received approximately $3.2M in federal grants. ITN formed an FCC Rural Health Care Steering Committee, which was made up of representatives from healthcare providers, telecommunication companies, representatives from the Indiana Office of Community & Rural Affairs, and representatives from the Indiana Rural Health Association, the lead entity for the ITN.
The five year project was divided into three phases and the work successfully concluded in 2015. The table below presents a summary of the project phases.
Table 2. Broadband Network Five-Year Summary
Phase 1 Phase II Phase III
Reduced bandwidth costs Reduced Primary Rate Interface
(PRI) costs Doubled the speed of
existing broadband connections
85% funding for construction of fiber to their hospitals
Completed ability to transmit images Improved economic opportunities
Expanded ability to conduct Telehealth encounters over a dedicated health care network
Disaster Recovery E-Learning Internet Access Videoconferencing
Seamless interfaces with the Indiana Health Information Organizations (HIOs)
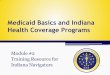
Overall, access to a wired connection of at least 10mbps has improved from 86.6% to 90.7% in Indiana. Meaningful Use objectives with an exclusion for broadband access require a connection of at least 4mbps for 50% of inhabitants within a 50 mile radius. In addition, 100% of Indiana residents have access to mobile broadband services and 78.6% have access to fixed wireless services. Approximately 2% of Indiana residents do not have any wired internet providers available where they live. Figure 1 below (next page) shows overall coverage for Indiana.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 20 of 81
SMHP ANNUAL UPDATE – 2016
Figure 2: Indiana Broadband Coverage by County
B.4.4 Regional Extension Centers (REC) Indiana had two (2) RECs that contracted with ONC:
• HealthBridge, currently part of the Health Collaborative, operated the Tri-State HIT Regional Extension Center (REC)
• Purdue Healthcare Advisors (PHA, formerly known as I-HITEC), operated by Purdue University.
Through an additional 90-10 funding match and a $250 per provider fee, PHA is guiding EPs through the EHR incentive program while helping them adjust to using their CEHRTs in a meaningful way. Since the additional work began in October 2014, PHA has worked and is currently working with 125 unique organizations representing approximately 1,020 EPs, many of those organizations enrolling in the assistance program for multiple EHR Incentive Program years. With the approval of the 2016 IAPD-U, PHA will secure a contract with FSSA to continue the work through September 2018. The scope of PHA includes statewide educational sessions including webinars and in-person sessions when requested. PHA monitors a dedicated email and a call center open for participating EPs and providers with questions about eligibility and meaningful use. The dedicated email and call center assist providers with varying types of issues as illustrated by Figure 2 below (next page).

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 21 of 81
SMHP ANNUAL UPDATE – 2016
Figure 2. Purdue Health Authority EP Help Desk Utilization
As the work with EPs has evolved with the release of the Modifications to Meaningful Use in 2015-2017 and Stage 3 Meaningful Use final rules, PHA has expanded their services to include security risk assessments and have made external vulnerability scans and technology wellness checks.
PHA also provides direct assistance to FSSA in the administration and oversight of the Indiana Medicaid EHR Incentive Program. PHA works directly with the HIT Coordinator. PHA will administer web-based program satisfaction surveys on an annual basis. Results from the 2015 program satisfaction survey will be included in Section 4.
Because PY 2016 will be the last year that EPs and EHs, including CAHs, can join the Medicaid EHR Incentive Program, PHA will continue outreach through newsletters, webinars, direct one-on-one conversations that come in via the call center and reminders at conferences and other stakeholder meetings. The 2016 e-scan provider survey results will be shared with PHA for use in further outreach.
B.4.5 Beacon Community Grant In May 2010, Indiana received $16 million in grant funding for the Beacon Communities Cooperative Agreement Program administered by U.S. Department of Health and Human Services (HHS) and Office of the National Coordinator for Health Information Technology (ONC). Specific goals for the Central Indiana Beacon Community included3:
• Improve health outcomes for patients with diabetes by helping providers manage patient performance on measures of blood sugar and cholesterol;
• Improve health outcomes by increasing appropriate use of preventive services, such as immunizations and screening for cancers of the colon and cervix;
• Reduce hospital admissions and emergency room visits for patients with conditions that could have been treated in an outpatient setting; and

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 22 of 81
SMHP ANNUAL UPDATE – 2016
• Strengthen health IT infrastructure and extending exchange capabilities to help physicians achieve measurable and sustainable improvements for patients.
3 Based on the Central Indiana Beacon Community fact sheet from healthit.gov.
At the grant conclusion, more than 2.7 million patients were touched by a Beacon intervention administered by one or more of the 1,600 providers or 57 hospitals participating in grant activities. Colorectal cancer screenings increased by 8.5% to 66.02%, exceeding the goal of 60.42% and cervical cancer screenings have increased 3.24% to 81.38%. Diabetic patients with acceptable ranges of blood glucose levels (HbA1C) have improved by 3.5% and the number of diabetic patients with cholesterol levels in acceptable ranges increased by 1.5%.
B.4.6 EvidenceNOW – Advancing Heart Health in Primary Care The state of Indiana is currently participating in EvidenceNOW, an Agency for Healthcare Research and Quality (AHRQ) grant initiative launched in May 2015 and continuing through May 2018. This initiative assists small- and medium-sized primary care practices in using the latest evidence to improve heart health and contribute to the national effort of preventing 1 million heart attacks and strokes by 2017. Purdue Health Authority (PHA) is leading the recruiting and improvement efforts led by Northwestern University’s School of Medicine. PHA is assisting nearly 50 small practices around the state in improving their Million Hearts cardiovascular measures around aspirin therapy, blood pressure control, cholesterol management, and smoking cessation.
EvidenceNOW consists of two main goals: improving the delivery of heart health care across the country and understanding what type of supports help primary care practices achieve these improved health outcomes. Additionally, the initiative has an aspirational goal that each involved practice will meet the national target of having 70 percent of all patients adopting the ABCS of cardiovascular health. Indiana, Illinois, and Wisconsin make up the Midwest cooperative. The Midwest cooperative has a target of recruiting 250 – 300 small- and medium-sized, independent primary care practices. Additionally, the AHRQ has awarded a grant to the Oregon Health and Science University to conduct an independent national evaluation of the overall EvidenceNOW initiative.
B.4.7 Transforming Clinical Practice Initiative One of the largest federal investments designed to support clinician practices through nationwide, collaborative, and peer-based learning networks is the Transforming Clinical Practice Initiative (TCPI). These peer-based learning networks known as Practice Transformation Networks (PTN) are designed to coach, mentor, and assist clinicians in developing core competencies specific to practice transformation. This will allow clinician practices to become actively engaged in transformation and collaboration within a broad community. This initiative was aided by the Affordable Care Act (ACA) to strengthen the quality of patient care and spend health care dollars more wisely while aligning with the criteria for innovative models set forth in the ACA.
The University was awarded $46.4M by the U.S. Department of Health and Human Services and is working with the Regional Extension Center, seven additional universities, three state Health Departments and Indiana’s four HIOs. Purdue Health Authority is leading Indiana’s efforts for the Great Lakes PTN, led by the Indiana University School of Medicine. In this role, PHA coordinates and serves as a key delivery member for much of the value-based care transformational assistance for over 3,400 providers throughout Indiana.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 23 of 81
SMHP ANNUAL UPDATE – 2016
B.5 Electronic Public Health Reporting The Indiana State Department of Health (ISDH), in conjunction with FSSA/OMPP, has been actively planning for the changes to Meaningful Use and advancing health information exchange through specialized registries such as the immunization registry and the cancer registry. ISDH is working with FSSA to submit an Implementation Advanced Planning Document (IAPD) to enhance and evolve the immunization system to better support Indiana providers and citizens while advancing health IT in Indiana.
B.5.1 Emergency Surveillance System Indiana’s Public Health Emergency Surveillance System (PHESS) was established over a decade ago by the Indiana State Department of Health (ISDH) in partnership with the Regenstrief Institute. It electronically links Indiana’s hospital emergency departments to the ISDH to create a statewide, standards-based public health surveillance system. A component of PHESS, the Electronic Surveillance System for the Early Notification of Community-based Epidemics (ESSENCE), is used by healthcare providers for reporting specific cases of communicable diagnosis to health departments.
Support for the PHESS system is ending in June 2016 since current guidance doesn’t require syndromic event types. The PHESS system will be maintained and access available; however further evolution of the PHESS system is no longer supported.
B.5.2 Immunization Registry The Children and Hoosier Immunization Registry Program (CHIRP) was established in 2002 under Indiana Codes IC16-38-5 as a web-based electronic database to collect immunization records for individuals of all ages in Indiana. By centralizing immunization records, individuals in the state now have access to their records through private providers, local health departments, and schools at no cost to the consumer, including Indiana providers.
CHIRP is able to communicate bi-directionally; however, it not yet able to communicate in real time. All received messages are stored and batched nightly, causing a moderate delay. ISDH is currently working with FSSA on an Implementation Advanced Planning Document (IAPD) for a real-time bi-directional interface with a target completion date of late 2017.
CHIRP has become a valuable resource to the more than 9,000 active users, including providers and citizens of Indiana by reducing staff time spent on searching for immunization records, tracking vaccine inventory and providing a more complete immunization history. The registry provides a suggested immunization schedule and, through My VaxIndiana, a secure consumer portal implemented in 2012 by OMPP in collaboration with ISDH, citizens can print and save their immunization records. This initiative links My VaxIndiana to HIO-sponsored Personal Health Records (PHR) via Direct Messaging.
ISDH serves as the Public Health Authority (PHA) for the State of Indiana and as such, provides assistance to EPs, EHs and CAHs participating in the EHR Incentive Program. CHIRP can currently accept, validate and document provider attestations for Meaningful Use, including the 2015-2017 Modification to Meaningful Use final rule. There are currently 141 hospitals linked to CHIRP both via direct data entry or HL7; 117 are connected using HL7 messaging and 109 have successfully attested to Meaningful Use. In additional, there are over 700 providers in production. All but

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 24 of 81
SMHP ANNUAL UPDATE – 2016
one of Indiana’s 92 counties have access to CHIRP including all of the Indiana Local Health Departments. As of June 2016, CHIRP receives an average 16,000 HL7 Unsolicited Vaccination Record Update (VXU) messages, approximately 100,000 per week.
B.5.3 Electronic Laboratory Reporting and Syndromic Surveillance Electronic Laboratory Reporting (ELR) and Syndromic Surveillance have been very successful objectives for Indiana hospitals. Approximately 91% of ISDH’s reportable conditions are transmitted via ELR using an HL7 message with 83% of these meeting Meaningful Use Stage 2 requirements. More than 180 hospitals are linked and ISDH is currently planning to update their 410 IAC (Indiana Administrative Code) rule to achieve 100% electronic submission of ELR.
All hospitals with emergency departments are currently reporting syndromic surveillance. Recently, two urgent care facilities linked with a larger hospital system have begun reporting syndromic surveillance. EPs participating in the Medicaid EHR Incentive Program are exempt from the syndromic surveillance reporting requirement; however, FSSA and ISDH have recognized that there is a large potential for expanding beyond hospitals and including more urgent care facilities and ambulatory providers.
B.5.4 Cancer Registry With the changes to the public health reporting objective in the 2015-2017 Modifications to Meaningful Use final rule, there has been an increased interest in the Indiana State Cancer Registry. Between June 2015 and June 2016, 55 EPs have indicated their intent to send files for MU Cancer Reporting, 16 EPs have sent files to the Cancer Registry, and 406 files have passed validation.
B.5.5 HIE Network Support Indiana HIE’s and hospitals participate in the Public Health Emergency Surveillance System (PHESS) network, the statewide infrastructure to analyze “primary complaint” data from Indiana emergency departments for the early detection of acts of bioterrorism and other public health emergencies. Currently, 120 Indiana emergency departments (ED) are connected.
Additionally, the HIE networks support Communicable Disease Reporting by leveraging the developed Notifiable Conditions Detector (NCD), an ONC-certified technology for electronic lab reporting, to identify list of communicable diseases with positive results and flagged to be sent to ISDH.
Indiana HIEs can also document immunization information at point of care, and immunization administration information is reported to CHIRP.
B.6 Statewide HIE Networks There are four established health information exchange networks operated by Health Information Organizations (HIOs) that currently serve Indiana and, in some cases, border-states and regional partners. These HIE networks were developed initially with a majority of hospital participation, although they continue to expand their provider outreach efforts especially in the context of the EHR Incentive Program. Each network has distinct characteristics in terms of their geographic region, participants, and business model.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 25 of 81
SMHP ANNUAL UPDATE – 2016
Networks currently in existence in Indiana are listed in Table 3, below:
Table 3. Major Indiana Regional Health Information Organizations/Networks
Regional Network Providers Covered Status
HealthBridge Greater Cincinnati tristate area physicians Operational
HealthLINC Physicians in Lawrence, Monroe, Orange, and Owen counties
Operational
Indiana Health Information Exchange (IHIE)
Represents hospitals, healthcare providers, researchers, public health organizations and economic development groups
Operational
Michiana Health Information Network (MHIN)
Over 3,000 physicians in northern Indiana and southwestern Michigan
Operational
B.6.1 HealthBridge HealthBridge has offered operational health information exchange since 1998. Its mission is to build a collaborative network of organizations and technology to improve the quality and efficiency of health care delivery. Recently, HealthBridge became part of a team of organizations called the Health Collaborative, working together with the Greater Cincinnati Health Council to advance health care transformation and the Three Part Aim of better care, better health, and lower costs. HealthBridge serves a primary service area in the Greater Cincinnati tristate area that includes four Indiana counties. HealthBridge has more than 7,500 physicians in its provider directory and 3.0 million patient records, with approximately 3-5 million electronic messages per month, including clinical lab tests, radiology reports, and discharge summaries.
B.6.2 HealthLINC HealthLINC is a community-based organization that has offered operational health information exchange since 2007 to healthcare stakeholders in Lawrence, Monroe, Orange and Owen counties. Recently, HealthLINC became a community partner with The Health Collaborative, sending greater than 110,000 secure clinical results per month. HealthLINC is a true community collaboration that includes 85% of community physicians representing more than 400,000 patients’ records in its community patient index. HealthLINC continues to make special efforts to improve care coordination for under-served populations including the uninsured and patients with chronic mental illness. HealthLINC also analyzes statistics including total results per month per practice, results per month at the community level and the number of practices with clinical messaging. HealthLINC has created a health service directory that includes more than 285 physicians, 4 regional hospitals, 4 long term care facilities, a surgery center, and a clinic-based regional laboratory setting the stage for care coordination improvements using HIT and EHRs.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 26 of 81
SMHP ANNUAL UPDATE – 2016
B.6.3 Indiana Health Information Exchange (IHIE) IHIE is a tax-exempt, nonprofit corporation founded in 2004 with 111 Indiana hospitals, approximately 33,500 healthcare providers, researchers, public health organizations, and economic development groups representing over 18 million unique patients. IHIE is a leading provider of scalable health information exchange services with demonstrated and sustainable technologies and processes.
IHIE hosts one of the nation’s largest inter-organizational clinical data repository, a patient-centric community health record for millions of Indiana citizens. This resource is an aggregated clinical data for a patient or a population and includes provider, payer, and public health data from real-time interfaces from providers providing labs, radiology, CCDs, transcriptions, cardiology information, and ADTs. This information is utilized heavily in hospital emergency departments, but also in a growing number of clinical and population health management settings, including medical research. Figure 3 below demonstrates IHIE’s geographic coverage area in Indiana.
Figure 3. IHIE Geographic Coverage Area
B.6.3.1 Multi-stakeholder Private Governance Each participating provider signs a Participant Agreement and participates in the committee discussing and determining the functioning rules of the sharing information across the Indiana Network for Patient Care™ (INPC™). This group determines the approved use cases for sharing, accessing, and using information across IHIE participating organizations. This private HIE governance body is only for IHIE participants, and FSSA has a seat on the Management Committee of the INPC™.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 27 of 81
SMHP ANNUAL UPDATE – 2016
B.6.3.2. Current IHIE Services of the Indiana Health Information Exchange • Sequoia Project eHealth Exchange - IHIE has expanded use of the eHealth Exchange for automated Social
Security Administration (SSA) disability determination via electronic request and record retrieval of INPC data through the eHealth Exchange. IHIE fulfills about 100 SSA applicant requests per day; previously, manual record gathering took 4 months to 3 years. Additionally, Indiana health providers can share veteran’s clinical data via the eHealth Exchange as part of the VLER program. IHIE supplies about 90% of the clinical data that the VA receives from eHealth Exchange trading partner; and IHIE data has been accessed in all 50 states. IHIE supports eligible professional and hospitals’ Meaningful Use Stage 2 Transitions of Care requirements as directed by Meaningful Use Stage 2 guidelines by being an “officially on-boarded” eHealth Exchange participant enables us to offer customers Transitions of Care, taking advantage of existing HIE infrastructure. Participating Indiana HIEs support the eHealth Exchange use cases:
o SSA Disability Determination - IHIE has expanded use of the eHealth Exchange for automated SSA disability determination via electronic request and record retrieval of INPC data through the eHealth Exchange. IHIE fulfills about 100 SSA applicant requests per day; previously, manual record gathering took 4 months to 3 years.
o Veteran’s Affairs Data Exchange with VLER - Indiana health providers can share veteran’s clinical data via the eHealth Exchange as part of the VLER program. IHIE supplies about 90% of the clinical data that the VA receives from eHealth Exchange trading partner; and IHIE data has been accessed in all 50 states.
o Meaningful Use Stage 2 Transition of Care Requirements - IHIE supports eligible professional and hospitals’ Meaningful Use Stage 2 Transitions of Care requirements as directed by Meaningful Use Stage 2 guidelines by being an “officially on-boarded” eHealth Exchange participant enables us to offer customers Transitions of Care, taking advantage of existing HIE infrastructure.
• ACO & Population Health Services - In addition to eHealth Exchange, IHIE’s ACO & Population Health Services, ADT registration alerts are available in any care setting. These ADT alerts support event notification for multiple use cases including emergency room admission, hospital discharge, or ambulatory encounter event. Event notifications are available from HIE participants and can be sent for a specific patient list to managed care organizations, care coordinators, and care teams for follow up care coordination. IHIE also provides a Clinical Data Report including 36 approved data elements. The Clinical Data Report is accessible by clinical care team members. INPC has approved access to Care Managers to include expanded care team members and to assist care coordination work using IHIE data. Reports delivered daily with information on when patient presented for care and diagnosis as well as approved lab value information.
B.6.4 Michiana Health Information Network (MHIN) MHIN was formally established in 1998 with the mission to provide single source, secure access and delivery of medical information leading to the care and quality of a person. MHIN serves over 13,000 physicians, representing 356 participating organizations/clinics including hospitals, clinics, skilled nursing facilities, ACOs, laboratories, alcohol and drug treatment centers, and behavioral health clinics. These participating organizations represent over 1.8

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 28 of 81
SMHP ANNUAL UPDATE – 2016
million patients across northern Indiana and southwestern Michigan. To date, MHINs network has had approximately 420,000 CCD exchanges.
B.6.4.1 MHIN 2016 – 2018 Population Health Strategic Plan MHIN’s 2016 – 2018 population health strategic plan includes an ambitious research agenda that considers future changes around shifting community priorities, emergent unforeseen health needs of the community, and funding opportunities. The plan’s purpose lies in improving the health of local communities by outlining priority areas of population health focus and accommodating the significant shifts seen in the health landscape within the U.S. in the last several years.
MHIN has created the MHIN Data Set of Social Determinants of Health which was derived from traditional medical information collected in EHRs. MHIN plans to implement this population health strategy over the next three years, concentrating on using the Data Set of Social Determinants to inform and enhance its Bio-Surveillance efforts, Remote Monitoring, and selected Regional Health priorities. Throughout this plan, MHIN will be working with academic researchers, industry experts, utilizing bleeding-edge technology, and evidence-based methodologies to identify, acquire, and operationalize the MHIN-specific Data Set of Social Determinants of Health with the goal of integrating it into the regional exchange and analysis of health data, to improve the capacity of our provider and public health system.
B.7 Core Interoperability Projects IHIT created five projects with each HIE and project plans for each category of development. In addition to these first five projects, OMPP worked with funds made available through the Challenge Grant program to fund three additional projects that play a part of the roadmap. Many of these projects have ongoing work and will be highlighted in the State HIT Roadmap section.
• Project 1: HIE to HIE Connectivity – Messaging • Project 2: HIE to HIE Connectivity – Bi-direction Summary Record Exchange • Project 3: Public Health Connectivity and Exchange • Project 4: Standards and Normalization • Project 5: HIE Longitudinal Patient Record Incentive
B.8 Current HIE Architecture/Structure The current “As Is” HIE architecture is depicted below and identifies the four HIOs participating in statewide HIE and data sharing within the State of Indiana.
The depiction below also represents the complex relationships between the data users and HIE service entities. The foundation (blue ellipses) of the HIE model is the data service users. There are three types of users represented: physicians/clinics, hospitals and payers. The “mezzanine” is supported by four exchange network’s infrastructure. HealthBridge and HealthLINC are illustrated as one support because HealthBridge provides the infrastructure and connectivity for HealthLINC. CMS and the SDE are represented outside of the structure illustrating their regulatory and standard-setting functions.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 29 of 81
SMHP ANNUAL UPDATE – 2016
Figure 4. Indiana HIE Network Structure
B.9 Governance for State Health Information Exchange In carrying out its former leadership and coordinating role for the state, as designated by the Governor, IHIT developed a governance model and instituted a formal governance structure that leverages private sector HIE development while ensuring strong state direction and multi-stakeholder collaboration. Indiana’s current statewide HIE governance leveraged the state-led HIE governance structure and processes and built well-established governance models continued by its four major private sector HIOs, an infrastructure that is already continue to oversee stakeholder involvement and the provision of many of the required HIE services. IHIT focused and directed the efforts of the HIE stakeholders - Indiana HIOs, state agencies, HIT vendors, providers and consumers - in four strategic areas: Connecting Data Sources, Interoperability, Improving Outcomes, and Federal/State Initiatives.
Through IHIT’s formal structures, processes, and policies, Indiana’s Health IT stakeholders continue to expand on these foundations and to strengthen information exchange across Indiana. Most significantly, the blended strong public and private sector representation and “distributed” approach to governance that built on the well-established HIE governance structures and processes of Indiana’s four HIOs.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 30 of 81
SMHP ANNUAL UPDATE – 2016
As an active stakeholder in the distributed governance structure, FSSA currently participates with Health Information Exchange Task Force convened by the Indiana Hospital Association. This group contains 25 hospital representatives who work with data and information needs within their organizations. This includes CEOs, CIOs, market analysts, quality directors, and other interested parties. FSSA also holds a seat on IHIE’s management committee facilitating expanding HIE use cases in line with Indiana’s key Health IT strategic areas.
B.10 Veterans Administration and Indian Health Services Providers There are two federal health care delivery systems in Indiana. The Richard L. Roudebush VA Medical Center in Indianapolis, Indiana, is a part of the Veterans in Partnership integrated healthcare network delivery system providing primary care, specialty care, extended care, and related services to veterans. The Camp Atterbury Medical Treatment Facility (MTF), a user of VISTA EHR technology, is located near Edinburgh, Indiana. Under a pilot project between IHIE and the US Department of Veteran Affairs, the eHealth Exchange gateway was used to share information electronically to support health care services provided both at Roudebush and by private health care providers in Central Indiana who signed up on a voluntary basis for the HIE service. Subsequently, the four Indiana HIOs also established connections via the eHealthExchange using the Connect Gateway.
Indiana has no enrolled Indian Health Services (IHS) providers at this time.
B.11 Medicaid Information Technology Architecture (MITA) During 2014-2015, the State conducted a MITA self-assessment that included the HIT business unit, as per the finalization of the MITA 3.0 business process model and related self-assistance guidance.
The current MMIS project demonstrates the State of Indiana’s commitment to move its Medicaid enterprise systems up the MITA “capability maturity ladder” and line up the State’s Medicaid enterprise systems more closely with the Seven Standards and Conditions for IT development (modularity, industry standards, reuse/leverage, business results, etc.) promoted by CMS. Moreover, the State’s commitment to leveraging IT capabilities across programs and even states is illustrated by the adoption of MAPIR.
B.12 MMIS HIT/HIE Environment Indiana’s current MMIS is built on a nearly twenty-year old platform known as IndianaAIM. The current system uses batch processing and flat-file data transfers for interoperability, and does not perform real-time transactions.
The current system is in the process of being replaced with new technology capable of enhanced automation and more efficient/economical processing capabilities in the future. Technical capabilities anticipated to be provided by the system will include: enhanced workflow, web services, a rules engine, and an enterprise service bus. The new system will have an inherent EHR capability to enhance and/or streamline many functions currently performed including care management and prior authorizations. OMPP’s timeline is to have the replacement MMIS in production by the end of 2016.
OMPP will share services in a standard format when the data is used to promote care coordination for Hoosier members and/or transmitted to achieve EP, EH or CAH Meaningful Use requirements. Maintenance of the Health

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 31 of 81
SMHP ANNUAL UPDATE – 2016
Insurance Portability and Accountability Act (HIPAA) and the ARRA security standards for receipt and transmission of the health information is a priority for OMPP, IHIE, and stakeholders participating in the statewide HIE network. Data will be exchanged for purposes of treatment, payment and program operations in accordance with HIPAA requirements.
B.13 Summary of Medicaid Environmental “As Is” E-scan In early spring 2016, FSSA contracted the services of Myers and Stauffer LC (MSLC) to conduct an e-scan to inform on the state of HIT and EHR adoption in the State of Indiana. Outreach for the e-scan included:
• Online survey to EPs, EHs and CAHs;
• One-on-one interviews with statewide stakeholders;
• Interviews with statewide partners including HIOs and Purdue Healthcare Advisors; and
• Interviews with coordinating state agencies.
B.13.1 Survey Strategy Two surveys were developed to communicate with specific provider groups: one for EPs (both participating and non-participating providers in the EHR Incentive Program) and one for EHs (both participating and non-participating hospitals in the EHR Incentive Program). MSLC used the previous survey as a guide, using the Survey Monkey tool because of its ease of use and consulted with its Health IT, Meaningful Use and Incentive Program subject matter experts to compose the EP and EH surveys.
Working with oversight from FSSA and the HIT Coordinator, MSLC partnered with Purdue Health Authority to disseminate the survey as widely as possible. In addition to promoting the survey in newsletters and webinars, PHA reached out to numerous organizations and associations to aid in the dissemination of the survey link. Some of these entities include: Indiana chapters of the American Academy of Pediatrics, American College of Cardiology, American College of Physicians and the American College of Surgeons. The American Congress of Obstetricians and Gynecologists (District V), the Fort Wayne Medical Society, the Indiana Academy of Family Physicians, the Indiana Association of Healthcare Quality, the Indiana Health Information Management Association, Indiana Hospital Association, Indiana Primary Health Care Association, Indiana Rural Health Association, Indianapolis Medical Society, Indiana Neurological Society, and the Indiana HIOs were also notified of the survey and asked to aid in the dissemination.
B.13.2 Survey Limitations The sample size is greater than the original e-scan from 2010/2011; however, it does not represent the entire provider population of Indiana. In order to round out the picture of EHR adoption and HIT/HIE in Indiana, FSSA and MSLC conducted numerous one-on-one interviews with stakeholders including the Indiana Health Care Association, Indiana Hospital Association, Indiana Health Information Exchange, the Division of Mental Health and Addiction, Indiana State Department of Health, Indiana Association for Rehabilitation Facilities, Indiana Council of Community Mental Health Centers, Purdue Health Authority, and the Indiana Rural Health Association.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 32 of 81
SMHP ANNUAL UPDATE – 2016
B.13.3 “As Is” Eligible Professional E-scan The EP survey did not limit the recipients of the survey link to only those providers eligible for the Medicaid EHR Incentive Program resulting in a large variety of provider type responses. Because there were no limitations, 173 responses were received representing over 1,300 health care providers in the state of Indiana. The five categories of Provider Type provided in the survey were Medical Care – General Practice (GP, FP, Internal Medicine, Pediatrics, PA, NP, RN), Medical Care – Specialist (GI, ENT, Cardiology, Oncology, OB/GYN, Ophthalmology, Etc.), Behavioral Health – Psychiatrist, Psychologist, Psychoanalyst, Social Worker, Dental – Dentist, Family Dentist, Dental Surgeon, and Other.
Table 4 - Indiana Provider SMHP Survey Provider Type Responses
Provider Type Category Percent of Responses
Medical Care - General Practice (GP, FP, Internal Medicine, Pediatrics, PA, NP, RN)
33.92%
Medical Care – Specialist (GI, ENT, Cardiology, Oncology, OB/GYN, Ophthalmology, Etc.)
11.11%
Behavioral Health – Psychiatrist, Psychologist, Psychoanalyst, Social Worker
12.87%
Dental – Dentist, Family Dentist, Dental Surgeon 13.45% Other 28.65%
If a survey responder chose “Other,” the survey prompted for a specification in the provider type. Asking for a specific type when “Other” was chosen allowed for a broader view into the provider landscape, EHR adoption and HIE adoption. Provider type specifications when “Other” was chosen included home health providers, physical, occupational and speech therapists, long term care providers, chiropractors, EMT and ambulance services, hospice, and optometrists.
A little over 97% of the practices that responded to the survey serve Medicaid patients with 38% percent of those practices indicating that more than 50% of their patients are enrolled in Medicaid. Unlike the EH respondents to the survey which will be summarized in the following section, the majority of practices still maintain some form of a paper chart. Seventy-five percent (75%) of responding practices use an EHR with 84% of those practices using a Certified EHR. Approximately 46% of practices that responded do not maintain paper charts and 16% of practices that responded primarily use paper charts but do record some clinical data electronically. The higher number of practices that maintain paper charts at various levels may be due to the larger number of non-eligible professionals that responded to the survey and may be seen as an opportunity to expand EHR adoption outside of the primary care arena.
The EP survey asked respondents to share the three most significant ways that the EHR has hindered the care provided to patients along with the three most significant ways that EHRs have improved the care of their patients. As we have seen since the inception of the EHR Incentive Program through the technical assistance provided through the RECs, the three largest complaints center around lack of training, workflow changes and the time spent entering data while attending to the patient. Although there are still some challenges adapting to EHRs,

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 33 of 81
SMHP ANNUAL UPDATE – 2016
62% of respondents agreed that the use of their EHR facilitates access to and use of the patient health data among members of the health care team while 44% noted that the use of the EHR reduces errors and 41% said that they believe the EHR improves the quality of patient care.
Since the original survey performed in the previous e-scan, Meaningful Use efforts have helped interoperability progress as well as patient engagement to allow more patients to access their health information through a patient portal as well as other time-saving tasks leading to a higher level of patient portal usage. Of the practices that indicated they provide patient portal access, 70% of them report that the patient portal is accessed mostly for lab results while 60% of practices noted that the patient portal is used secondarily for prescription refills and appointment scheduling.
Lastly, the EP survey asked respondents to answer a few questions about HIEs and participation in one or more of Indiana’s four HIOs. One hundred and one survey respondents shared whether or not they have joined an HIE with 61% of the EP practices indicated that they have not primarily because the larger HIEs in Indiana do not currently provide EHR integration with many ambulatory EHRs and that the primary focus has been on hospital participation. Of the 33 respondents that shared which functions would enhance their return on investment for their chosen HIE, 70% said that bi-directional exchange with other ambulatory providers would be the best enhancement. Clinical quality measure collection and reporting was a priority for 52% of the respondents while 45% suggested integration with claims data.
B.13.4 “As Is” Hospital E-scan Like the EP survey, the EH survey was not limited to hospitals eligible for one or both of the EHR Incentive Programs and received 37 responses. Of the responses, there were 23 community hospitals, 4 CAHs, 4 behavioral health/mental health hospitals, and 3 public hospitals. EHR adoption is high among the survey respondents with 34 of the hospitals having a certified EHR in use, one hospital in the process of implementing a certified EHR and only one hospital with no plans to adopt due to the lack of specialized software for their patient population.
Much like the EP survey, EHs reported the workflow design is their greatest barrier along with increased difficulty in Meaningful Use objectives and the implementation and use of the patient portal (a Meaningful Use Stage 2 requirement). The majority of the EHs eligible for the Medicaid EHR Incentive Program have already received three payments and is no longer eligible for additional payments. Even though the EHs said that the patient portal was a barrier for them, 92% of respondents indicated that they do offer a functioning patient portal and it is used primarily for accessing lab results (96%) with downloading discharge instructions at 57% and billing information at 44%.
EHs, like EPs, were asked to share the three most significant ways that the EHR has hindered the care provided to patients along with the three most significant ways that EHRs have improved the care of their patients. EHs indicated that the time to train and time to convert old records are two of the greatest hindrances. Fifty-four percent (54%) of hospital respondents also noted that system incompatibility and interoperability are also challenges. EHs did note that EHRs reduce errors (88%), facilitate access to and use of patient health data among members of the health care team (79%), and that information from the EHR enables better decision making in patient care (50%).
Lastly, the EH survey asked about HIE participation by hospitals in Indiana. HIE participation amongst hospitals is

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 34 of 81
SMHP ANNUAL UPDATE – 2016
very high with 83% of the respondents indicating they’ve joined an HIE. Three hospitals said that they haven’t joined because of vendor readiness, not enough participation with coordinating providers and cost. The EH survey asked which HIE each EH participates in and 94% of the EHs indicated that they subscribe to IHIE. EHs were asked which functions would enhance their return on investment for their chosen HIE and 75% of the respondents said bi-directional exchange with ambulatory providers would be the greatest enhancement with 63% responding that integration with claims data would be another valuable enhancement. Figure 5 from the IHIE website below demonstrates HIE connectivity for Indiana hospitals.
Figure 5. Indiana Hospitals with HIE Connectivity

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 35 of 81
SMHP ANNUAL UPDATE – 2016
C. Indiana’s “To Be” HIT Landscape Indiana continues its vision for electronic health records (EHR) adoption and implementation and widespread, robust exchange of health information to improve health and health care for Indiana. The vision was crafted based on an appreciation for the Indiana culture of marketplace innovations. The early direction for Indiana’s HIT development was shaped by the private sector, forged by the successful efforts of the nation’s leading HIOs, IHIE and HealthBridge. The HITECH Act and the State Health Information Exchange Cooperative Agreement Program (SHIECAP) provided the impetus to coalesce Indiana’s vision into a strategic plan and operational pathway toward the future “To Be” HIT landscape, building on a foundation of HIE business acumen, and policy leadership provided by FSSA. The designation of Indiana Health Information Technology, Inc. (IHIT) as the leading governance entity for Indiana’s HIT and HIE efforts provided a formal bridge between sectors, and a venue for collaborative, negotiated HIT and HIE solutions that has now transitioned to FSSA leadership. Public and private stakeholders continue as integral partners in the governance, development and operations of Indiana’s developing statewide health information system.
The Indiana Strategic and Operational Plans submitted to ONC under SHIECAP identified HIT and HIE capacity development to goals for improving health care, including for those served by Medicaid and other public programs. The SHIECAP remains the key state strategy coordinating public and private Health Information Technology and Exchange strategies. Additionally, Indiana’s MMIS implementation with estimated late 2016 completion supports the State’s management of its public programs in conjunction with the HIT and HIE assets developing across the broad landscape.
As mentioned earlier, ISDH, in conjunction with FSSA/OMPP, has been actively planning for health information exchange through specialized registries such as the immunization registry and the cancer registry. ISDH is working with FSSA to submit an Implementation Advanced Planning Document (IAPD) to enhance and evolve the immunization system to better support Indiana providers and citizens while advancing health IT in Indiana.
The “To Be” HIT Landscape will build on efforts outlined in the Strategic and Operational Plans, MMIS implementation and capabilities, the planned HIE IAPD, and the EHR Incentive Program operations. Continued provider adoption of certified electronic health record technology will improve point of care access to health information for Indiana Medicaid members and providers. Expanded HIE technical services providing timely access to health information across organizations continue to facilitate coordination of care. Additionally, as more providers’ health data systems are connected to the developing health information network, clinical data aggregation will support advanced data sets for advanced population health measurement. This will help improve the quality and cost-effectiveness of health care provided for individuals and families and of the Indiana health care system as a whole.
C.1 Public-Private Stakeholder Cooperation Public and private stakeholder cooperation is essential for executing Indiana’s vision for HIT. This cooperation includes a flexible, inclusive, and effective governance structure engaging diverse stakeholders across sectors and network aligned to common objectives. Indiana Health Information Technology, Inc. (IHIT) previously played this critical role to ensure that all stakeholders participate and are served by HIT and HIE services. As a non-profit, state-

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 36 of 81
SMHP ANNUAL UPDATE – 2016
level governance and coordinating entity, IHIT built on the experiences of previous HIT stakeholder collaborations including: the Indiana Health Informatics Corporation (IHIC), a public instrumentality created in 2007 under statute by the State of Indiana to guide and promote health information exchange within the State; the State HIE Collaboration began in 2008; and the Exhibit Indiana initiative coordinated by BioCrossroads, to establish a convening and coordination structure and governance processes for generating multi-stakeholder buy-in and the trust necessary for effective public-private collaboration.
IHIT captured lessons learned from these efforts as its formal structures and processes were crafted. Most significantly, IHIT provided a venue that blended strong public and private sector representation, and used a “distributed” approach to governance that built on the well-established HIE governance structures and processes of Indiana’s four HIOs.
The cooperative HIT and HIE governance structure will continue to leverage the well-established HIE governance structures and processes. FSSA continues to be a key stakeholder and attends privately convened stakeholder groups, including the Indiana Network for Patient Care™ (INPC™) and the Indiana Hospital Association’s HIT advisory Council on Information Management and Health Information Task Force. As objectives develop, additional stakeholders will be identified to join the existing convening groups to facilitate new or extended technical services. FSSA will also support internal OMPP EHR Incentive program workgroups and other Medicaid IT system coordination connecting the internal Medicaid enterprise planning to the external, private stakeholders as needed to support a broadening Indiana health information network. Additional state agencies, such as ISDH will engage FSSA and the external HIT community to coordinate advancing Health IT and Exchange strategies.
C.1.1 HIT Coordinator The HIT Coordinator is located within FSSA and reports to the Chief Information Officer (CIO) and oversees all HIT related initiatives for the state of Indiana. This role embodies a collaborative multi-sector approach. The HIT Coordinator brings sectors and interests together to consider policy goals for improving health care including for Medicaid and CHIP, and continuously focusing and facilitating the efforts of the four Indiana HIOs, providers, vendors, agencies and stakeholders at large on the four “strategic pillars” of Indiana’s Strategic and Operational Plans: connecting data sources, fostering interoperability, improving outcomes, and leveraging Federal/State Initiatives. Additionally, the HIT Coordinator provides staff guidance on Medicaid’s role within the HIE, and provides vision and direction for the EHR Incentive program with regards to (a) meaningful use realization and acceleration and (b) the role of HIE in achieving this goal. This role provides vision and guidance to Medicaid on leveraging HIT program goals with existing programs, and assists with work plans and resource management, program metrics/operations and performance management. The HIT Coordinator makes operational recommendations for HIT initiatives, and serves as the primary contact with CMS and ONC for HIT and HIE efforts as mentioned above.
C.2 Vision for HIT Environment In its Strategic and Operational Plans, Indiana lays out four (4) “strategic pillars” that serve as the vision and pathway for the state’s HIT environment: connecting data sources, fostering interoperability, improving outcomes, and leveraging Federal/State Initiatives.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 37 of 81
SMHP ANNUAL UPDATE – 2016
As national standards further develop and through the various targeted projects underway, the state will continue from IHIT’s efforts to work with the HIOs to foster increased interoperability, data standardization and security. Building from efforts being driven by private market trading partner agreements, IHIT and its partners leveraged additional open source tools and specifications (e.g. Direct and the Connect Gateway) developed as part of the Sequoia Project eHealth Exchange.
The strategies formerly pursued by IHIT and its partners, and the continuation of these activities by FSSA, EPs and EHs (including CAHs) will continue to gain and expand connectivity and the ability to exchange health information within and outside their HIO for the purposes of treatment, payment, and health plan operations (TPO). A comprehensive strategy for expanding interoperability through the HIOs is designed to ensure that the adoption of certified EHR technology will target eligible professionals and hospitals but encompass other health care providers and the industry at-large.
Interoperability for individual providers outside of an HIO ecosystem will be accelerated by providing secure HIE messaging for clinical information between health care providers, enable the capture of core information to facilitate care coordination and point of care decision making, and will foster more timely access to care for Hoosiers without delays while reducing the administrative burden of paper-based exchanges.
As the majority of providers are gaining active status as participants in the EHR incentive program, demonstrating meaningful use and the reporting of Clinical Quality Measurements (CQM) will continue to be the prevailing priorities as Stage 2 and Stage 3 requirements are instituted. Organizing an integrated quality reporting strategy is an important ongoing focus, seeking to build upon developing cross-HIO querying of repositories and other strategies currently in play to expand and enhance interoperability of clinical data.
The public health opportunities associated with building the capacity of the statewide HIE network are immense. The State Immunization registry and public health surveillance reporting database are two examples of databases that can be populated with information that is gathered through the HIOs. Many providers are already required to submit multiple files for secondary uses by public health officials for monitoring and reporting purposes. FSSA is actively working with ISDH on a public health HIE expansion leveraging the EHR Meaningful Use Incentive Program. ISDH has identified the following improvements to public health and public health data systems:
• More complete and accurate information (data quality) • Improved coordination of care • Improved responsiveness to communicable disease outbreaks. • Healthier patient populations and communities • Standards for quicker implementation and transmission of MU data. • Funds to support facilities move to electronic and upgrade their feeds. • Ability to transfer health information easily between Local Health Departments, other states, and
federal partners. • Exponential growth in storage costs.
Medicaid has confirmed a contractor to replace the existing MMIS system to be in production by 2016. The new MMIS will contain an enterprise service bus, a rules engine, and workflow management components. Provider and member portal capabilities will continue and provide stakeholders with a mechanism for managing their

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 38 of 81
SMHP ANNUAL UPDATE – 2016
demographic information and the capability to obtain access to Medicaid policy rules and submit claims/encounters.
Both Indiana Health Information Exchange (IHIE) and HealthBridge currently have connections to the eHealth Exchange. In the future Indiana will need to maintain the sustainability of the HIO structure that has occurred over the past 15 years. Integration of the HIOs will be driven by the private sector needs and desire of Indiana health care providers for data sharing relationships to facilitate exchange of ePHI for TPO and to monitor health care outcomes.
FSSA recognizes that the agency will play a significant role in transforming health care in Indiana and has developed its vision for HIT to address many of the challenges of integration with the HIOs. Obtaining and leveraging new technology is a key component. Implementation of a new MMIS is a major priority for providing improved functionality that will support OMPP and statewide HIT/HIE efforts.
Indiana’s vision for HIT also relies heavily on utilizing meaningful use of clinical information obtained through adoption, implementation and upgrade of certified EHR systems by providers and facilities and leveraging HIO technologies currently in place in Indiana. Through the use of EHR systems, HIE and other technologies described in the following sections, OMPP is positioned well over the next three to five years to significantly impact the following shared goals, initially established in IHIT’s Strategic Plan:
• Connect data sources;
• Interoperability;
• Improve outcomes;
• Establish secure statewide and interstate HIE; and
• Focus on prevention.
Realizing these broad goals for IHIT and its stakeholders includes the following eight components and related strategies:
Table 5– Components of Indiana’s Strategic Plans Shared Goals
Components Projects
1. Simplified access to Health Care Information and Services for Beneficiaries
Enhance secure web-based Beneficiary information, communication, outreach, and tracking
Provide enhanced provider online search capabilities
Improve service delivery through Interactive Voice Response (IVR) and VOIP (Voice Over Internet Protocol) technologies where possible
Design and implement online capabilities to enhance quality consumer directed access to care
Development of strong Medical Home delivery system

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 39 of 81
SMHP ANNUAL UPDATE – 2016
Components Projects
Increase collaboration between all state payer and providers
Streamline Point of Service functions (e.g., Smart Cards)
Fully develop e-Prescribing functionality
2. Simplified interaction with the Health Care infrastructure for providers
Credentialing
Web-based Access
Enhanced Technology Supports
3. Improved Health Care Outcomes – measured by increased usage of performance criteria
Create clear outcomes and expectations for providers to address pay for performance and quality of care
Incentivize providers to use quality preventative care
Utilizing HIE/HIT to improve health care Quality and Safety.
Develop and expand innovative approaches to prevention.
Develop a comprehensive statistical profile for delivery and utilization patterns
4. Evolving use of modern information technology to improve the delivery of health care and outcomes, identify administrative efficiencies, coordination, and optimization of care
Administrative Efficiencies-
Coordination of Care
5. Integrated medical service delivery model that includes high quality Medicaid providers
Encourage and promote retention of quality Medicaid providers
Explore health care literacy program to reduce Emergency Room use by Medicaid population
Implement Statewide HIE to improve episode of care management
Improve eligibility coordination and knowledge sharing between agencies and business partners
6. Move from “client” focus to “family” or “community” based health care
Development of strong Medical Home model delivery system

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 40 of 81
SMHP ANNUAL UPDATE – 2016
Components Projects
7. Public Health Centralized ISDH Meaningful Use (MU) Hub
MU Website
MU Data Portal
Real-time Bidirectional Interface for CHIRP
Data Encryption Implementation and Security Scan
8. Technical Assistance (TA) for Providers through REC-like services
90/10 funding for Purdue Health Authority to continue technical assistance (TA) and outreach for providers interested in EHR adoption, Meaningful Use, Interoperability and HIE participation
C.3 Public Health – Health Information Technology Strategy ISDH plans to leverage Meaningful Use EPs and EHs as the primary groups for improving the quality, safety, and health of citizens of Indiana. To meet the objectives, ISDH and FSSA have identified the following list of projects to streamline and improve data collection and quality to support population health:
• Centralized ISDH Meaningful Use Hub (MU Data Hub) – design, develop, and implement a supporting end user support and system/data interaction
o MU User Support Website: public health meaningful use registration, training, and guidance for public health reporting measures
o ISDH MU Data Portal (DP): electronic system providing quality assurance testing for accurate MU data to IDSH registries (Cancer, ELR, Syndromic Surveillance, and Immunization [MyVax])
o ISDH MU Data Portal (DP) Automated Feedback Tools: alert system to assess quality of data message for planning, data feed and quality discrepancies, and support ticket generation for ongoing tracking and monitoring of issues.
• State Immunization Information System (CHIRP) Bidirectional Interfaces (Real-time Bidirectional Immunization Interfaces) – improve bidirectional connections for data submission and retrieval from EPs, EHs and CAHs and timeliness of immunization data flow
o Bidirectional Immunization Data Submission and Retrieval by EPs, EHs, and CAHs: continue to connect and bi-directionally submit and receive immunization forecasts and histories to/from the Immunization Information System (IIS) and to/from EPs, EHs, and CAHs
o Real-time Bidirectional Immunization Data Flow: improve timeliness of querying IIS for stored immunization messages, moving from batch processes via nightly deduplication process taking 12-36 hours to near real-time
• ISDH MU Data Encryption Audit and Security Scan (Security Scan) – review and conduct a series of internal and external security scan and identify count measures for any security gaps for data transmission and storage
• Meaningful Use Training and Outreach (MU Training) – provide Public Health reporting Meaningful use attestation support for providers and facilities in cooperation with other MU technical assistant partners.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 41 of 81
SMHP ANNUAL UPDATE – 2016
o Outreach Plan: Develop outreach and support plan for ISDH Cancer Registry data submissions o Cancer Registry Guidelines: Increase Cancer Registry data submissions from more facilities o Training Material: Develop Public Health MU Training material to streamline and facilitate public
health data reporting attestation requirements in cooperation with other MU TA partners
Figure 6. Outside ISDH Electronic Data Flow

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 42 of 81
SMHP ANNUAL UPDATE – 2016
D. Activities Necessary to Administer and Oversee the EHR Incentive Program This section includes a description of the business processes OMPP will employ to ensure that eligible professionals (EP) and eligible hospitals (EH) including Critical Access Hospitals (CAH) have met Federal and State statutory requirements to receive incentive payments in the EHR Incentive Program. OMPP plans to use their standard MITA business processes where feasible, and integrate the Indiana EHR Incentive Program into day-to-day operations in partnership with Hewlett Packard (HP) where appropriate. Examples of new state-specific business processes to be developed include:
• Provider registration
• Provider eligibility determination and verification
• Medicaid patient volume verification
• Provider attestation verification Adopt, Implement or Upgrade (AIU) and Meaningful Use (MU)
• Query to the Medicare and Medicaid EHR Incentive Program Registration & Attestation System (R&A)
D.1 Concept of Operation and Administration OMPP administers the Indiana Medicaid EHR Incentive Program using resources located in the HIT Unit within FSSA’s Division of Healthcare Strategies and Technologies. The HIT Coordinator is responsible for developing operational policies and procedures for the EHR Incentive Program, researching regulatory questions as they arise, and completing additional activities to plan, coordinate and update the SMHP and IAPD and oversight of the pre- and post-payment activities. The HIT Coordinator is responsible for overall coordination of program, oversight and supervision of HP for pre-payment activities and Myers and Stauffer LC for post-payment activities. The HP staff is responsible for performing provider enrollment, customer service, help desk support and maintenance of the EHR Incentive Program system. In addition, HP supports the review and approval of requests received from the Medicare & Medicaid EHR Incentive Program Registration & Attestation System (R&A), monthly payment processing and required EHR Incentive payment reporting. In its role as program administrator, the HIT Coordinator also coordinates provider outreach with Purdue Health Authority (PHA) which provides technical services to eligible professionals, hospitals, and CAHs enrolling in the Indiana Medicaid EHR Incentive Program.
The OMPP leverages existing Medicaid business processes to manage the program including provider enrollment, provider payment process, provider audits and state and federal reporting.
D.2 Audit Work Group The Indiana Health Information Technology EHR Incentive Program FSSA Audit Work Group, having successfully produced the Indiana HIT FSSA Audit Plan no longer meets on a regular basis; however, the HIT Coordinator meets with the FSSA audit staff on a regular basis in between active audit periods. In addition, during active audit periods, the HIT Coordinator meets with the FSSA audit team once a week to discuss any issues. The FSSA audit staff generates weekly reports that are shared with the HIT Coordinator. Myers and Stauffer, LC is

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 43 of 81
SMHP ANNUAL UPDATE – 2016
the third-party auditor for the Indiana EHR Incentive Program and meets regularly with FSSA on past, current and future audits as well as updates to the Audit Plan required annually by CMS for the EHR Incentive Program.
D.3 Technology Work Group The Technology Work Group assisted in identification of system requirements and development and planning for the ongoing EHR Incentive Program systems updates. Having successfully procured and implemented the Indiana R&A, he Technology Work Group is no longer necessary. The HIT Coordinator regularly communicates with HP regarding the Medical Assistance Provider Incentive Repository (MAPIR) system and is responsible for the review of data standard needs and further exploration of issues like integration of the MMIS to the larger statewide HIE initiatives. The HIT Coordinator meets regularly with the FSSA staff responsible for the Medicaid Enterprise systems.
D.4 Clinical Quality Work Group Early in the program development process, OMPP Quality Staff participated in an intensive work session to consider how EHR meaningful use reporting requirements and the development of expanded clinical data capture and reporting by EP, EH and CAH using certified EHR technology would impact OMPP’s objectives for clinical quality measurement and reporting. An initial informal Clinical Quality Work Group was formed of medical, clinical, quality, and audit staff formed to discuss legislation, review data, make recommendations, and provides direction on clinical and quality assurance issues and measures related to this program.
Currently, there are no plans to formally institute a Clinical Quality Work Group, but as HIT, HIE, and interoperability continue to advance in Indiana, the HIT Coordinator will re-examine the impacts of the first phase of the Program, consider the implications of expanded capacity for clinical data reporting among Medicaid programs and the HIOs, and formulate a strategy for collecting, analyzing and making full use of Clinical Quality Measures (CQM) and other meaningful use measures.
D.5 Provider Communications The HIT Coordinator, in partnership with PHA as the REC and primary responsible entity for outreach to EPs, EHs and CAHs, communicates prior, during, and after each attestation program year. PHA performs all outreach on attestation and eligibility requirements as well as education on Meaningful Use using newsletters, webinars and direct outreach. HP, the current MMIS Fiscal Agent Vendor, has many communication requirements and touch points currently used with regards to communicating within FSSA and OMPP, as well as communicating with Providers and other external entities.
D.5.1. External Surveys External surveys, including those performed for this latest version of the SMHP (see Section B13), have been performed. In 2015, PHA performed a provider satisfaction survey.
• Survey 1: Indiana EHR Incentive Program - Medicaid Providers Satisfaction Survey: In 2015, Purdue Health Authority (PHA) conducted a provider satisfaction survey in order to assess the satisfaction of

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 44 of 81
SMHP ANNUAL UPDATE – 2016
providers participating in the Indiana Medicaid EHR Incentive Program. The survey consisted of 14 questions and was sent to 591 contacts from the MAPIR system. By the close of the survey period, the response rate was 12% with 70 organizations fully completing the survey. In summary, 74% of the respondents were either “very likely” or “likely” to continuing to attest for Meaningful Use and 77% of respondents were satisfied with the help they received when they contacted customer service either via email or phone.
• Survey 2: Indiana EHR Incentive Program – AIU-only Medicaid Providers Survey: In addition to the Medicaid Provider Satisfaction Survey, PHA conducted a survey for AIU-only providers in the Indiana EHR Incentive Program. The 7-question survey was conducted to assess the reasons providers participating in the EHR Incentive Program completed AIU but have not yet attested to Meaningful Use. The survey was sent to 201 EPs and had 35 responses for a 17% response rate. One hundred percent (100%) of respondents indicated that they were still using their EHR and 83% planned on attesting to Meaningful Use. When asked about the biggest challenge with the adoption of an EHR, several respondents indicated that poor reporting capability, incorrect data, and problems with the patient portal for their chosen EHR were their biggest barriers.
D.5.2. Publications • Bulletins, Banners, Newsletters, Letters, and Website: OMPP and HP utilize multiple media outlets such as
bulletins, banners, newsletters, letters, and the websites (e.g. www.indianamedicaid.com and www.cms.gov/EHRIncentivePrograms) to communicate HIT EHR relevant-information with the Provider Community during the life of the Indiana EHR Incentive Program project. The bulletins, banners, newsletters, and any website documentation will be referenced to the applicable website if a web posting or if a non-web posting, the communication will be posted on the OMPP HIT SharePoint site by the HIT Coordinator.
D.5.3. Program Process Audits
• Internal Audits: OMPP is required to participate in an In-Office Review Audit conducted by FSSA Audit Services Team and the Indiana State Board of Accounts and/or upon request by CMS. All audits require HIT EHR Project Team Member commitment and participation at various stages of the audit process. From the preparation work, to mock-audit activities, to documentation preparation, report creation, etc., all audit-related communications, documentation, and the work products created are critical to the success of the audit. All audit findings will be posted in a secured area on the OMPP HIT SharePoint site by the HIT Coordinator and/or the FSSA Audit Services Team members or their appointed designee(s).
D.6 Recent Changes in State Laws and Regulations At this time, no state laws or regulations have been identified that will impact the continued operation of the Program. Although the governor established the Indiana Health Information Technology, Inc. (IHIT), to provide strong oversight, the IHIT operated under a governance model that combined private sector electronic HIE with strong state direction and multi-stakeholder collaboration. To date, this process has enabled Indiana to move toward the necessary support of meaningful use through the efforts of the four exchange networks that currently operate within Indiana without the need for new state laws or regulations.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 45 of 81
SMHP ANNUAL UPDATE – 2016
At this time, no state laws or regulations have been identified that will impact the implementation of the Indiana EHR Incentive Program, and no new laws are currently anticipated as a result; however, 2016 is an election year and many senior position across the government may change which may result in a slight shift on HIT strategies.
D.7 Policy Changes Early in the initial implementation of the EHR Incentive Program in Indiana, it was determined that Indiana would need to address the issue of enrolling Physician Assistants (PA) within the MMIS program. CFR§495.306 specifies an FQHC or RHC must be PA led in order for PAs to qualify for incentive payments as an eligible professional. If an Indiana Medicaid enrolled FQHC or RHC becomes PA led, and that PA meets all program, eligibility and patient volume requirements of an eligible professional, Medicaid will assist the PA with enrollment in the EHR Incentive Program. To address this issue PAs are now enrolled within MMIS, thus ensuring capability to make appropriate incentive payments to all eligible EPs. So far, Indiana has only enrolled one PA that was confirmed as meeting the requirement for “so led.” In the future, prior to enrolling a PA in the MMIS, Medicaid will determine whether the PA leads an FQHC or RHC by checking with the Indiana Primary Health Care Association (IPHCA), the clinic’s web site and/or the Indiana State Office of Rural Health Programs.
As regulations from CMS are issued, policies are updated to reflect the changes. Examples of these changes which have been incorporated into the SMHP include changes to the final Stage 2 Meaningful Use regulations, the 2014 Flexibility rule and the Modified Stage 2 rule. As the HIT Coordinator further refines the program operations to meet the Meaningful Use requirements, policy changes may be required and will be addressed according to existing program policy maintenance procedures as needed. These policy updates, should they be required, will be reported in a subsequent iteration of the SMHP.
D.7.1 Modification to Meaningful Use in 2015-2017 SMHP Addendum On October 16, 2015, CMS published a Final Rule, Medicare and Medicaid Programs; Electronic Health Record Incentive Program – Stage 3 and Modifications to Meaningful Use in 2015 through 2017 to the Federal Register, or the 2015-2017 Modifications Rule. The changes specified in the 2015-2017 Modifications Rule were effective on December 15, 2015.
Indiana completed a comprehensive analysis of the 2015-2017 Modifications Rule and the following tables outline the changes to Meaningful Use (MU) and the EHR Incentive Program that Indiana plans to incorporate starting in Program Year 2015 for Eligible Professionals (EP) and Eligible Hospitals (EH) respectively.
This addendum was submitted to and approved by CMS in April 2016 and the approved changes are in the tables below.
Table 6. Eligible Professionals (EP) – 2015-2017 Modifications to Meaningful Use
Eligible Professionals (EP) – 2015-2017 Modifications to Meaningful Use (MU)
Change Explanation Effective Program Year
90-day reporting period for 2015
First time and returning EPs attesting to MU will choose any continuous 90-day period in calendar year 2015 for their EHR reporting period.
2015

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 46 of 81
SMHP ANNUAL UPDATE – 2016
Eligible Professionals (EP) – 2015-2017 Modifications to Meaningful Use (MU)
Change Explanation Effective Program Year
90-day reporting period for 2016
EPs attesting to MU for the first time in 2016 will choose any continuous 90-day period in calendar year 2016 for their EHR reporting period.
2016
Full year reporting period for 2016
Returning EPs attesting to MU in 2016 will use the full calendar year 2016 for their EHR reporting period. 2016
90-day reporting period for 2017
EPs attesting to MU for the first time in 2017 will choose any continuous 90-day period in calendar year 2017 for their EHR reporting period. EPs attesting to Stage 3 MU for the first time in 2017 only will choose any continuous 90-day period in calendar year 2017 for their EHR reporting period.
2017
Full year reporting period for 2017
Returning EPs attesting to Stage 2 MU in 2017 will use the full calendar year 2017 for their EHR reporting period.
2017
Remove the differentiation between MU Core and Menu objectives
Starting in 2015, all MU objectives will be required and will be considered “Core” objectives.
2015 2016 2017
Stage 1 specifications for EPs in 2015; lower thresholds and exclusions
EPs scheduled to demonstrate Stage 1 MU in 2015 will be required to report to the Stage 2 MU objectives for all consolidated objectives. EPs will report on Stage 1 MU specifications for objectives that have a lower threshold in Stage 1 MU than Stage 2 MU. Exclusions for objectives that do not have an equivalent Stage 2 MU objective are available. If an EP is scheduled to demonstrate Stage 1 MU in 2015 but can attest to the Stage 2 MU threshold on an objective, he/she may choose to do so.
2015
Modified Stage 2 MU objectives in 2016 and 2017
All EPs will attest to the modified, consolidated Stage 2 MU objectives in 2016 and 2017, regardless of stage in 2015, including Adopt, Implement or Upgrade (AIU).
2016 2017
2014 Edition Certified Electronic Health Record Technology (CEHRT)
A 2014 Edition CEHRT is required for all attestations, AIU or MU, in program years 2015 and 2016.
2015 2016
CEHRT Edition(s) in 2017 EPs may use either a 2014 Edition, 2014/2015 Edition combination, or 2015 Edition CEHRT for MU attestations in program year 2017.
2017
MU required measures for 2015-2017
The 10 modified MU measures for EPs in 2015-2017 include:
1. Protect Patient Health Information 2. Clinical Decision Support 3. Computerized Physician Order Entry (CPOE) 4. Electronic Prescribing
2015 2016 2017

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 47 of 81
SMHP ANNUAL UPDATE – 2016
Eligible Professionals (EP) – 2015-2017 Modifications to Meaningful Use (MU)
Change Explanation Effective Program Year
5. Health Information Exchange 6. Patient Specific Health Education 7. Medication Reconciliation 8. Patient Electronic Access
a. Measure 2 – remove 5% threshold for 2015 and 2016 and require that at least one (1) patient (or authorized representative) seen by the EP views, downloads, or transmits their health information to a third party.
b. Measure 2 – in 2017, the threshold returns to 5% of all unique patients (or authorized representative) seen by the EP views, downloads, or transmits their health information to a third party.
9. Secure Electronic Messaging a. In 2015, the capability for patients to send
a secure electronic message with the EP is fully enabled in the CEHRT.
b. In 2016, at least one (1) patient seen by the EP during the EHR reporting period, a secure message was sent using the electronic messaging function of the CEHRT.
c. In 2017, at least 5% of unique patients seen by the EP sent a secure message using the electronic messaging function of the CEHRT.
10. Public Health Reporting
Discontinued MU measures 2015-Forward
The MU measures discontinued starting in program year 2015 and moving forward through the program include:
1. Record Demographics 2. Record Vital Signs 3. Record Smoking Status 4. Clinical Summaries 5. Structured Lab Results 6. Patient Lists 7. Patient Reminders 8. Summary of Care
a. Measure 1 – Any method b. Measure 3 – Test
9. Electronic Notes 10. Imaging Results 11. Family Health History
2015 2016 2017

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 48 of 81
SMHP ANNUAL UPDATE – 2016
Table 7. Eligible Hospitals (EH) – 2015-2017 Modifications to Meaningful Use
Eligible Hospitals (EH) – 2015-2017 Modifications to Meaningful Use (MU)
Change Explanation Effective Program Year
90-day reporting period for 2015
First time and returning EHs attesting to MU will choose any continuous 90-day period in calendar year 2015 for their EHR reporting period.
2015
90-day reporting period for 2016
EHs attesting to MU for the first time in 2016 will choose any continuous 90-day period in calendar year 2016 for their EHR reporting period.
2016
Full year reporting period for 2016
Returning EHs attesting to MU in 2016 will use the full calendar year 2016 for their EHR reporting period. 2016
90-day reporting period for 2017
EHs attesting to MU for the first time in 2017 will choose any continuous 90-day period in calendar year 2017 for their EHR reporting period. EHs attesting to Stage 3 MU for the first time in 2017 only will choose any continuous 90-day period in calendar year 2017 for their EHR reporting period.
2017
Full year reporting period for 2017
Returning EHs attesting to Stage 2 MU in 2017 will use the full calendar year 2017 for their EHR reporting period.
2017
Remove the differentiation between MU Core and Menu objectives
Starting in 2015, all MU objectives will be required and will be considered “Core” objectives.
2015 2016 2017
Stage 1 specifications for EPs in 2015; lower thresholds and exclusions
EHs scheduled to demonstrate Stage 1 MU in 2015 will be required to report to the Stage 2 MU objectives for all consolidated objectives. EPs will report on Stage 1 MU specifications for objectives that have a lower threshold in Stage 1 MU than Stage 2 MU. Exclusions for objectives that do not have an equivalent Stage 2 MU objective are available. If an EH is scheduled to demonstrate Stage 1 MU in 2015 but can attest to the Stage 2 MU threshold on an objective, the EH may choose to do so.
2015
Modified Stage 2 MU objectives in 2016 and 2017
All EHs will attest to the modified, consolidated Stage 2 MU objectives in 2016 and 2017, regardless of stage in 2015, including Adopt, Implement or Upgrade (AIU).
2016 2017
2014 Edition Certified Electronic Health Record Technology (CEHRT)
A 2014 Edition CEHRT is required for all attestations, AIU or MU, in program years 2015 and 2016.
2015 2016
CEHRT Edition(s) in 2017 EHs may use either a 2014 Edition, 2014/2015 Edition combination, or 2015 Edition CEHRT for MU attestations in program year 2017.
2017
MU required measures for 2015-2017
The nine (9) modified MU measures for EHs in 2015-2017 include:
2015 2016

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 49 of 81
SMHP ANNUAL UPDATE – 2016
Eligible Hospitals (EH) – 2015-2017 Modifications to Meaningful Use (MU)
Change Explanation Effective Program Year
1. Protect Patient Health Information 2. Clinical Decision Support 3. Computerized Physician Order Entry (CPOE) 4. Electronic Prescribing 5. Health Information Exchange 6. Patient Specific Health Education 7. Medication Reconciliation 8. Patient Electronic Access
a. Measure 2 – remove 5% threshold for 2015 and 2016 and require that at least one (1) patient (or authorized representative) discharged from the EH’s inpatient (POS21) or emergency department (POS23) views, downloads, or transmits their health information to a third party.
b. Measure 2 – in 2017, the threshold returns to 5% of all unique patients (or authorized representative) discharged from the EH’s inpatient (POS21) or emergency department (POS23) views, downloads, or transmits their health information to a third party.
9. Public Health Reporting
2017
Discontinued MU measures 2015-Forward
The MU measures discontinued starting in program year 2015 and moving forward through the program include:
1. Record Vital Signs 2. Record Smoking Status 3. Structured Lab Results 4. Patient Lists 5. Summary of Care
a. Measure 1 – Any method b. Measure 3 – Test
6. Electronic Notes 7. Imaging Results 8. Family Health History 9. eMAR 10. Structured Labs to Ambulatory Providers 11. Advanced Directives
2015 2016 2017

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 50 of 81
SMHP ANNUAL UPDATE – 2016
D.8 HIE/HIT Activities across State Borders Currently providers from Illinois, Ohio, Michigan, and Kentucky can be enrolled as Indiana Medicaid providers and Indiana Medicaid receives data from these providers. This exchange of information allows Indiana providers who are relying on patients from one of our border state’s Medicaid programs to meet volumes for EHR Incentive Program eligibility. Additionally, the surrounding states will have access to Indiana Medicaid eligibility and patient volume information to verify corresponding data for providers relying on Indiana information for their EHR Incentive Programs. Since Indiana has HIOs that span state lines, Medicaid works through the HIOs and uses the HIOs’ relationships to foster interstate health information data exchange. OMPP will reevaluate the need for these agreements in the future should this information become available through the national HIE infrastructure.
D.9 Privacy Regulatory Changes On an ongoing basis, FSSA and OMPP ensures the State’s HIT and HIE efforts, including the EHR Incentive Program, are aligned and fostering stakeholder compliance with appropriate state and federal privacy and security provisions and industry standards.
Early in 2013 final omnibus amendments (the 2013 Amendments) to the Privacy, Security, Breach Notification and Enforcement Rules of the Health Information Portability and Accountability Act (the HIPAA rules) were issued, as directed by the HITECH Act of 2009. The 2013 Amendments include a number of sweeping changes with implications for entities that transmit and analyze health care data. Key provisions expand the definition of a business associate and establish a higher threshold for determining whether a breach occurred. OMPP is working to assess its internal operations. The HIT Coordinator and IHIT are working with the HIOs and the State’s RECs to ensure that providers, organizations and information sharing partners are aware of their added responsibilities, and that they revisit their Business Associate Agreement and overall contracting and business processes to ensure compliance with new privacy and security provisions.
D.10 Provider Contract Changes At the time of enrollment all new IHCP providers are required to execute a provider agreement with OMPP. This agreement addresses the exchange of information, including health information, between the provider and the Medicaid Agency. It also addresses the requirements for providers to comply with all federal and state statutes and regulations, to fully cooperate with federal and state officials in the conduct of inspections, reviews and audits, and to make full reimbursement of any disallowances related to payments previously made. In addition it includes providers appeal rights and responsibilities.
D.11 Provider Eligibility Determination To be eligible for the Indiana EHR Incentive Program, a professional must be enrolled in the MMIS as a traditional Medicaid provider and meet certain Medicaid patient volume requirements.
When the EP, EH, or CAH has completed registration in the Medicare & Medicaid EHR Incentive Program R&A System, the provider will be instructed on how to register and attest using Indiana’s provider incentive payment system, MAPIR, which is integrated into Indiana’s existing provider web portal. Providers will be able to log on to

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 51 of 81
SMHP ANNUAL UPDATE – 2016
the provider portal and complete registration and attest to AIU and patient volume during their first program year. Initially providers submitted via fax additional information needed to complete the attestation; MAPIR functionality has been subsequently deployed that enables providers to submit all of this information electronically.
Web InterChange is an interactive Web application that allows providers to access the IHCP computer system through the Internet. Web InterChange is fast, reliable, secure, free, and does not require providers to obtain or use special software. The product is well known to the Indiana Medicaid Providers who currently use the web site to submit claims, view claims status online, review remittance advice, request prior authorization, inquire about checks, maintain provider profile and demographics, and verify member eligibility and review provider education materials and obtain program manuals for all Indiana Health Care Programs.
The Web InterChange serves as the gateway and using their Web InterChange sign-in, providers easily link to the EHR Provider Incentive Payment system to enter EHR enrollment and attestation information. EPs and EHs log on to Indiana’s existing provider portal using their valid provider identification number (ID) to register. After entering the CMS Registration Number and receiving confirmation of Medicare & Medicaid EHR Incentive Program Registration & Attestation System (R&A) registration, within the portal the system validates eligibility of the provider’s enrolled type as well as the NPI/TIN (National Provider Identifier/Taxpayer Identification Number) combination.
The following process flowcharts (Figure 7, below and next page) show the high level process that eligible providers and hospitals go through to enroll in Indiana’s Medicaid EHR Incentive Program.
Figure 7. EP and EH Registration and Attestation Processes

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 52 of 81
SMHP ANNUAL UPDATE – 2016
When the EHR Incentive Payment system receives a transaction from the Medicare & Medicaid EHR Incentive Program R&A indicating that a provider has registered for the Indiana EHR Incentive Program, a transaction is stored in a database in the MMIS for record tracking.
Two basic validations are made: 1) validate the provider is currently enrolled as an Indiana Medicaid provider; and 2) validate the provider is an eligible professional or eligible hospital. If these conditions are not met, a “provider not eligible” status is automatically sent back to the Medicare & Medicaid EHR Incentive Program R&A.
Indiana has incorporated the following features for the Indiana EHR Incentive Program web site:
1. Instructions on the EHR Provider Enrollment Process
2. How to correct registration error with the Medicare & Medicaid EHR Incentive Program R&A
3. How to calculate patient threshold
4. How to assign payment to a third party and OMPP verifications of information provided
5. How to request an appeal for a provider enrollment or payment decision
6. Information and links to CMS EHR Incentive Program web site and Fact Sheets
7. Goals and objectives of EHR Incentive Program
The OMPP contractor verifies provider eligibility for the EHR Incentive Program and updates the EHR Incentive Payment system accordingly. This triggers a registration eligibility response transaction (B-7) update to the Medicare & Medicaid EHR Incentive Program R&A. In addition, when eligibility and all supporting documentation has been received and verified a duplicate payment inquiry is sent to the Medicare & Medicaid EHR Incentive Program R&A.
Components of the provider eligibility processing include:
• Attestation Verification: The EP must enter the numerator and denominator for patient volume (e.g.,

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 53 of 81
SMHP ANNUAL UPDATE – 2016
Medicaid or needy individuals). Based upon provider ID the EHR Incentive Payment system will query Medicaid paid claims/encounters history to determine reasonableness of the numerator entered. In instances where there is a greater variance in the MMIS generated encounters versus the provider entered encounters for the numerator, Indiana will require supporting documentation to be submitted by the provider during the pre-payment review. For subsequent years (2-6) Indiana will request that the provider generate a report of all patients seen for the period of report, using the certified EHR decision support capabilities, and attach the documentation to the attestation as an electronic file. This information is used by Hewlett Packard Enterprises to manually review the overall content of each application. To determine the reasonableness of patient volume reported for out-of-state providers, OMPP manually contacts the other state’s Medicaid Fiscal Agent or payers, request paid claims/encounters , or uses the other state’s/payer’s provider capabilities for requesting ad hoc reports. Providers are identified using the NPI and TIN numbers entered on the Medicare & Medicaid EHR Incentive Program R&A. EHs are matched against the Medicare CCN number and cost reports queried to ensure lengths of stay of 25 days or less. OMPP uses Medicaid and total discharges from the hospital’s most recent three years of cost reports to verify lengths of stay of 25 days or less and any other information entered by the hospitals. Reports are requested for the time period entered for payment in the Medicare & Medicaid EHR Incentive Program R&A.
• Adopt/Implement/Upgrade (AIU) Attestation: Indiana assumes that all EPs and EHs will attest to adopt, implement or upgrade for year one (1). A copy of the invoice, purchase order, or licensing agreement for the certified EHR technology that includes the CEHRT number within the documentation, must be available if the provider is selected for post payment audit.
• Hospital Based Professional: per §495.4 EPs who render more than 90 percent of health care services within a hospital setting are not eligible to participate in the Indiana Medicaid EHR Incentive Program. Automating validation of claims/encounter history is currently available. As a result, OMPP has developed automated standard queries and the EHR business team will manually validate claims/encounters to ensure the provider is not hospital based prior to approval of payment. OMPP intends to maximize automation to the extent possible and automate this process as quickly as possible after implementation of the program. As a result of MU Stage 2 final regulations, EPs who use CEHRT in the inpatient or emergency department of a hospital, are now eligible if they can demonstrate that the EP funds the acquisition, implementation, and maintenance of CEHRT, including supporting hardware and any interfaces necessary to meet meaningful use without reimbursement from an eligible hospital or CAH.
• Provider Licensure and Sanction: OMPP’s enrollment processes include collection of disclosure information and verification against the List of Excluded Individuals Entities (LEIE) at time of enrollment and re-enrollment. While some enrollment information is matched against the MED monthly, steps have been taken, including developing system enhancements, to include all disclosure information in the monthly Medicare Exclusion Database (MED) match. When the provider enrolls in the EHR Provider Enrollment System, the system verifies that the provider is valid based on NPI and TIN on file. OMPP manually checks for current licensure against the most recent file received from the Indiana Professional Licensing Agency. When the provider is not found on this data file, OMPP verifies information on the Indiana Professional Licensing Agency web site to determine licensure. In addition to the OIG sanction list check by the Medicare

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 54 of 81
SMHP ANNUAL UPDATE – 2016
& Medicaid EHR Incentive Program R&A, OMPP also manually verifies that the provider is not listed on the OIG sanction list or under state sanctions.
• EPs and EHs with EHR systems currently installed must go through a process to certify this technology as meeting all requirements of 45CFR Part 170. These providers may register AIU during year 1 and attest to adopt (that is acquired and installed), implement (that is trained staff, deployed tools, exchanged data) or upgrade (that is expanded functionality or interoperability). A copy of the invoice, purchase order, or licensing agreement for the certified EHR technology must be available if the provider is selected for post payment audit.
• Meaningful Use Verification: Provider Enrollment System accepts, queries and stores meaningful use measures (Core) and Clinical Quality (Menu) as reported by the eligible provider during their years 2-6. EPs are asked to attest to the numerator and denominator reported, and paid claims/encounters are validated accordingly. When Medicare verifies that meaningful use requirements have been met for EHs and CAHs, the facility is deemed eligible for the Indiana Medicaid EHR Incentive Program. Indiana Medicaid assumes the results of the pre-payment hospital verification activities will be available from the Medicare & Medicaid EHR Incentive Program R&A to the EHR Provider Enrollment System.
• Needy Individuals: Medicaid EPs practicing predominately within an FQHC or RHC must have a minimum of 30% patient volume attributable to “needy individuals” and demonstrate 30 percent of all patient encounters be attributable to needy individuals over any continuous 90 day period within the most recent calendar year prior to reporting or the preceding 12 month period from the date of attestation. The EP will enter the numerator and denominator into the EHR Provider Enrollment System for validation. The definition of “needy individuals” published in the Final Rule at Section 1903 (t)(3)(F) of the Act will be used by Indiana to determine appropriateness of inclusion in the numerator and denominator. Needy individuals mean individuals that meet one of the following:
o Received medical assistance from Medicaid or the Children’s Health Insurance Program (CHIP) or a Medicaid or CHIP demonstration project approved under section 1115 of the Act
o Were furnished uncompensated care by the provider
o Were furnished services at either no cost or reduced cost based on a sliding scale determined by the individual’s ability to pay
Medicaid EPs are considered as practicing predominately in FQHCs/RHCs when the clinical location for over 50 percent of his/her total patient encounters over a period of six months within the prior calendar year (or preceding 12 month period from the date of attestation) is an FQHC or an RHC. Verification for volume of needy individuals is through attestation by EPs, including Physicians (MD/DO), Pediatrician or Nurse Practitioner/ Advanced Practice Nurse, Certified Nurse Midwife, Dentist, or Physician Assistants practicing within an FQHC or RHC that is PA led.
When possible, OMPP verifies that the EP meets the “practices predominately” requirement for the FQHC/RHC by validating numerator provided in attestation for FQHC/RHC against paid claims /encounters from data warehouse using the same verification as for EPs.
Providers that do not meet eligibility requirements for the program are informed of the specific issues that affect

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 55 of 81
SMHP ANNUAL UPDATE – 2016
their eligibility and process for redress.
D.11.1 Eligible Providers The Providers (EPs, EHs, CAHs) eligible to participate in the Indiana Medicaid EHR Incentive Program are shown below. EHs are those with a CMS Certification Number (CCN) number within the CCN range defined by CMS. EPs are required to meet Medicaid patient volume criteria on an annual basis. To receive payment from the Indiana Medicaid EHR Incentive Program, EPs and EHs must first register with the Medicare & Medicaid EHR Incentive Program R&A and select State of Indiana within the Medicare & Medicaid EHR Incentive Program R&A registration system.
EPs and EHs qualifying for eligibility in the Indiana EHR Incentive Program are identified in Table 8 (below).
Table 8. Providers (EP, EH, and CAH) Qualifying for Indiana Medicaid EHR Incentive Program
Eligible Provider MMIS Designation Physician (MD/DO) Type 31 / Specialty 310-346 Pediatrician* (identified on Medicaid provider)
Type 31 / Specialty 345
Dentist Type 27 / Specialty 271-277 Advanced Practice Nurse** Type 09 / Specialty 090-095 Physician Assistant Type 10 / Specialty 100 Hospital – Acute Care, Critical Access, Children’s
Type 01 / Specialty 010
*Indiana Medicaid recognizes the specialty “pediatrician” as indicated by the physician on his/her provider agreement and enrollment application.
** Pursuant to 848 IAC 4-1-3 Advanced Practice Nurse (Provider Type 09) includes: Nurse Practitioner, Certified Nurse Midwife and Clinical Nurse Specialist. Advance Practice Nurses are inclusive of all types of Nurse Practitioners and all Nurse Practitioners are included under the Advance Practice Nurse designation.
Providers and hospitals that were not included in ARRA §4201 and are currently not eligible for the Indiana EHR Incentive Program include behavioral health (substance abuse and mental health) providers and facilities and long term care providers and facilities.
[Note that some provider types that are eligible for the Medicare program, such as Chiropractors, are not eligible for the Indiana Medicaid EHR Provider Incentive Payment Program. Indiana will conduct outreach activities as necessary to encourage providers who are eligible under the Medicare program only to enroll appropriately.]
D.11.2 Provider Registration Process All EPs and EHs will access the CMS web site for the Medicare & Medicaid EHR Incentive Program R&A to register for payment. Information entered into the Medicare & Medicaid EHR Incentive Program R&A will include: NPI, TIN, EHR product and EHR certification number. The CMS certified EHR number that comes from the ONC Certified EHR Health IT Product List (CHPL) website will be listed on the Medicare & Medicaid EHR Incentive Program R&A

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 56 of 81
SMHP ANNUAL UPDATE – 2016
registration by provider at the time of attestation to AIU. The provider will also report that number to Indiana. The MAPIR system completes an automated review of the CMS certified EHR number which is compared to the CHPL site.
All EHs must have a current enrollment record in Provider Enrollment, Chain and Ownership System (PECOS) and have a CCN within the range approved by CMS to participate in the EHR Provider Incentive Payment Program. EPs who are only participating in the Medicaid EHR Incentive Program are not required to have a valid PECOS enrollment record on file.
In provider year 1, verification of AIU is handled through manual review of provider-submitted documentation attached to attestation in the EHR Incentive Payment system. This documentation shall include evidence of contractual obligation to AIU certified EHR technology. Verification audits of submitted attachments are conducted prior to incentive payment being made.
In the first year of participation, providers must demonstrate meaningful use for a 90-day EHR reporting period; in subsequent years, providers will demonstrate meaningful use for a full year EHR reporting period (an entire fiscal year for hospitals or an entire calendar year for EPs). Providers who participate in the Medicaid EHR Incentive Programs are not required to demonstrate Meaningful Use in consecutive years as described in the table, but their progression through the stages of Meaningful Use must follow the same overall structure of two years meeting the criteria of each stage, with the first year of meaningful use participation consisting of a 90-day EHR reporting period.
For 2014 only, all providers regardless of their stage of meaningful use were required to demonstrate meaningful use for a 3-month EHR reporting period. CMS permitted this one-time 3-month reporting period in 2014 only so that all providers who must upgrade to 2014 Certified EHR Technology will have adequate time to implement their new Certified EHR systems.
Starting in 2015, the EHR reporting period for all providers will be based on the calendar year. For the 2015 program year only, The EHR reporting period for all providers will be any continuous 90-day period. EPs may select an EHR reporting period of any continuous 90 day period from January 1, 2015 through December 31, 2015. Eligible hospitals and CAHs may select an EHR reporting period of any continuous 90 day period from October 1, 2014 to December 31, 2015.
D.12 Processing Payments to Providers Payments are made directly to enrolled EPs, EHs, or an employer or clinic to which a provider has assigned payment. Incentive payments and 1099s are issued through the MMIS. The state uses the MMIS specialty listing for purposes of meeting the eligible provider enrollment category. The State identifies administrative costs to administer the program, as well as direct payments to eligible providers who request payment for AIU or demonstrate meaningful use. Reporting on the CMS 37 and 64 reports is available in the MMIS and the standard MITA FFP drawdown business process is used to receive and track incentive monies received from CMS.
On the front end, the EHR Incentive Payment system interfaces with the Medicare & Medicaid EHR Incentive Program R&A to access registration, record and collect, process, and store attestation and meaningful use measures. OMPP operational staff have the capability to manually review and edit information entered into the EHR Incentive Payment system. The Medicare & Medicaid EHR Incentive Program R&A is the source for provider registration and entry of NPI, TIN, EHR product and certification number. The provider is directed to correct any

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 57 of 81
SMHP ANNUAL UPDATE – 2016
errors in the Medicare & Medicaid EHR Incentive Program R&A database prior to any processing being completed in Indiana’s EHR Incentive Payment system.
Eligible and enrolled EPs may choose to reassign their incentive payments to their employer or to an entity with which they have a contractual arrangement and the incentive payment will be made to the Tax ID on file for their employer, allowing the employer to request and receive the EPs incentive payment. The EP may reassign the entire amount of the incentive payment to only one employer. The EP is required to attest that assignment of payment by the EP to the respective employer or facility is voluntary and that no more than 5 percent (5%) of such payment is retained for costs unrelated to EHR technology.
All providers are required to enroll in the Medicaid program prior to enrollment in a Medicaid MCO network. Indiana only makes incentive payments to the provider or employer tax IDs as approved by the eligible provider. No incentive payments are made through a Medicaid MCO.
It is understood that the National Plan and Provider Enumeration System (NPPES) registration system requires all providers to assign payment at the national level. The Medicare & Medicaid EHR Incentive Program R&A Registration transaction to the State includes not only the EP’s Personal TIN, but also the Payee TIN. OMPP assigns the payment at the state level, as the national level has no way to validate the payee TIN/EP TIN combination. The Indiana EHR Incentive Payment system lists the valid individual and group NPIs, names, IDs, and TINs associated with the EP who is registering at the state level. The EP has the opportunity to choose which of these valid entities to assign his/her EHR incentive payment. The MMIS then creates payments accordingly. MMIS expenditure entries are automatically created when OMPP staff verifies that all supporting documentation has been submitted by the EP/EH and that all of the requirements for payment have been satisfied. The incentive payments are considered supplemental payments. A specific funding code is applied to provider incentive payments to enable reporting and payment tracking in the MMIS.
Funds are disbursed as specified by the State Medicaid business rules. Payments are routed as specified by the “pay to” instruction from the Medicare & Medicaid EHR Incentive Program R&A most recent registration transaction, to the EFT account on the file for the Payee TIN. OMPP staff updates the Payment History Information data store, the Perform Accounting Functions, and State Financial Management business processes with transaction accounting detail.
Providers determined to be eligible for the Indiana Medicaid EHR Incentive Program payments are identified and payments made on a weekly basis as incentive payment is requested. Payments are made within 45 days of receipt of the Medicare & Medicaid EHR Incentive Program R&A registration requesting payment.
Providers determined to be ineligible for the Incentive EHR Provider Incentive Program payments are notified via mail of the decision, the reason(s) for the decision, and the OMPP process for requesting a reconsideration or appeal. OMPP now uses electronic means for notice of eligibility denial to speed the communication with the providers. Also, communication of ineligibility determination by use of electronic communications such as email is already occurring. These methods will increase the timeliness of the overall process while also assisting providers by including access or links to EHR incentive program details, thereby providing support and education to all inquiring providers.
System controls are used in the MMIS financial subsystem to ensure appropriate payments and reporting. The State

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 58 of 81
SMHP ANNUAL UPDATE – 2016
participates in the registration and payment reporting to the Medicare & Medicaid EHR Incentive Program R&A. The EHR Incentive Payment system retrieves information from the Medicare & Medicaid EHR Incentive Program R&A based on unique provider NPI and TIN prior to completing the payment process to ensure that EPs or EHs do not collect EHR incentive payments from multiple states.
D.12.1 Provider Payment Request Providers are required to attest to the year of their participation and that they have not requested eligibility for the same year in the Medicare (for EPs) or another state’s EHR Provider Incentive Payment program. Connectivity and data compared with the Medicare & Medicaid EHR Incentive Program R&A are used to validate this information prior to making the incentive payment.
Provider participation in the Indiana Medicaid EHR Incentive Program is tracked in the Indiana EHR Incentive Payment system and the MMIS. The Provider’s status relative to Program eligibility is assessed with each annual payment request. The eligibility determination includes the interrogation of the Medicare & Medicaid EHR Incentive Program R&A to assess previous payments based on unique provider NPI and TIN.
The EHR Provider Enrollment System maintains data for each participating Provider, records the year in which payments are requested, and the Indiana Medicaid EHR Incentive Program requirements relative to the year of the request. Each eligible provider is limited to a maximum of six payments. New provider requests for enrollment in Indiana Medicaid EHR Incentive Program will not be allowed after December 31, 2016.
D.12.2 Provider Payment Calculations Indiana Medicaid disburses incentive payments directly to eligible professionals and eligible hospitals (including CAHs) through the MMIS, not through the managed care organizations (MCOs) or other intermediaries.
All EPs and EHs are required to complete an annual registration and attestation process in the Medicare & Medicaid EHR Incentive Program R&A and Indiana Medicaid EHR Incentive Program administration system to request incentive payment. Eligible providers who attest to AIU in year 1 must maintain documentation on file to support AIU (e.g., license agreement, purchase order) and use of certified EHR technology during the report period. Please refer to 5. Section E: The State’s Audit Strategy for additional audit information.
D.12.2.1 Eligible Hospital (EH) Payment Calculation The Indiana EHR Incentive Program hospital aggregate incentive amount calculation will be a one-time, up-front calculation using the equation outlined in the Final Rule, as follows:
• (Overall EHR Amount) times (Medicaid Share) where Overall EHR Amount Equals {Sum over 4 year of [(Base Amount plus Discharge Related Amount Applicable for Each Year) times Transition Factor Applicable for Each Year]} times Medicaid Share Equals {(Medicaid inpatient-bed-days plus Medicaid managed care inpatient-bed-days) divided by [(total inpatient-bed days) times (estimated total charges minus charity care charges) divided by(estimated total charges)]}
Indiana pays the aggregate hospital incentive payment amount over a period of three annual payments, contingent on the hospital’s annual attestations and registrations for the annual Indiana EHR Incentive Program.
In the first year, if all conditions for payment are met, 50 percent of the aggregate amount will be paid to the EH. In

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 59 of 81
SMHP ANNUAL UPDATE – 2016
the second year, if all conditions for payment are met, 40 percent, of the aggregate amount will be paid to the EH. In the third year, if all conditions for payment are met, 10 percent of the aggregate amount will be paid to the EH. A hospital must initiate participation by no later than December 31, 2016. Since Indiana is disbursing over three years, participation after 2016 can be non-consecutive to still receive the full amount. A hospital must initiate participation by 2016, but after that they only have to participate consecutively when: 1) the state is paying out over 6 years; and 2) they want the full amount.
Consistent with the Stage 2 regulation changes, hospitals that begin participation in 2013 and later can now use the most recent continuous 12 month period for which data are available prior to the payment year. Additionally, hospitals that began receiving payment in a program year prior to 2013 will not have to adjust previous calculations (previously Medicaid eligible hospitals calculated the base year using a 12 month period ending in the Federal fiscal year before the hospital’s fiscal year that serves as the first payment year).
Also, and in accordance with Stage 2 MU regulations, Indiana understands that hospitals may switch the state from where they receive EHR incentive payments provided that, with concurrence from CMS, Indiana and the other state are able to work together to determine the remaining payments due to the hospital based on the aggregate incentive amount already paid. The hospital will then assume the second state’s payment cycle, less the money paid from the first state.
D.12.2.2 Eligible Professional (EP) Payment Calculation The EPs will receive incentive payment not to exceed $21,250 in the first year or maximum of $8,500 in years 2-6. In no case shall an EP participate for longer than six (6) years or receive payment in excess of the maximum $63,750. Per §495.310, an EP may not begin receiving payments later than calendar year 2016. EPs may receive payments on a non-consecutive, annual basis. No attestations will be accepted after program year 2021 and all payment will be made within 45 days of the attestation date. The payment calculation for EPs is automated within the Indiana EHR Incentive Payment system.
Pediatricians attesting to a patient volume between 20% - 29% receive 2/3 of the incentive payment amount. EPs enrolled in the MMIS with provider specialty 345 meet the definition of Pediatrician. Pediatricians who carry between 20 and 29 percent Medicaid patient volume have their payment reduced by one-third. The Pediatrician will not receive more than $14,167 in the first year and not more than $5,667 for subsequent years. The total incentive payments for six years will not exceed $42,500. All other requirements noted above for an EP remain the same.
D.13 Provider National Provider Identifier (NPI) OMPP currently requires that all providers submit a valid NPI as a condition of Medicaid provider enrollment. Each EP or EH will be enrolled as an IHCP provider and will therefore, without any change in process or system modification, meet the requirement and have reported an NPI. OMPP will perform a NPPES search to validate NPIs during the enrollment process.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 60 of 81
SMHP ANNUAL UPDATE – 2016
D.14 Role of Contractors in Indiana EHR Incentive Program Implementation Indiana works closely with Hewlett Packard (HP), the current MMIS contractor to operate the Indiana EHR Incentive Program. In order to implement the EHR Incentive Program during May 2011, OMPP leveraged the EHR system solution that was in place and implemented in Oklahoma. Indiana received written approval from CMS to use funds approved under the SMHP Planning Advanced Planning Document (P-APD) to fund Indiana’s portion of the EHR Incentive Payment system development effort. Indiana submitted an IAPD to transfer funds for system development from the P-APD to the implementation phase, as well as for funding other EHR Provider Incentive Payment Program implementation and operations costs. The initial SMHP IAPD was submitted and approved on April 26, 2011. The latest IAPD-U was approved in September 2015.
OMPP is now using the EHR Incentive Payment system for provider eligibility and AIU and MU attestations. The EHR Incentive Payment system is used as the interface to the Medicare & Medicaid EHR Incentive Program R&A. Indiana previously completed both connectivity and validation testing with the Medicare & Medicaid EHR Incentive Program R&A as of March 2011 with an initial implementation date of May 1, 2011.
The OMPP Fiscal Agent has provided the EHR Incentive Payment system software for use in enrolling EPs and EHs in the program (MAPIR). The EHR Incentive Payment system contains screens for providers to enter required information and attest to patient volumes, enter meaningful use measures, etc. as well as functioning as the direct interface to the Medicare & Medicaid EHR Incentive Program R&A. Since OMPP is leveraging existing MITA business processes and capabilities, the fiscal agent’s help desk, provider services and call center for enrollment, payments inquiries, and appeals is used to support the EHR Incentive Program. Incentive payments are being made directly from the MMIS to the EP or EH or as assigned by the EP.
Originally, the contracted Pharmacy Benefit Manager (PBM) for Fee-for-Service (FFS) patients did not have the capability to accept e-Prescribing transactions. However the State has secured a vendor who can facilitate the processing of these transactions. The MCO’s PBMs do have capability to accept ePrescribe transactions and the MCO formularies are available to the EPs and EHs through this ePrescribe capability. The MCOs, as a condition of participation, provide paid encounter claims that are used by OMPP to verify reasonableness of Medicaid patient volume. At this time this will be the extent of the role of the MCOs within the EHR Incentive Program. Provider incentive payments will not be made through the MCOs, but rather directly to eligible providers through the MMIS.
The state began contracting with Truven Health Analytics and MSLC to provide administrative oversite of payment recoupments and to execute the Meaningful Use audit function.
D.15 Reporting Requirements In order to ensure that no amounts higher than 100% of FFP will be claimed for reimbursement, payment to Indiana Medicaid EHR Incentive Program eligible providers are reported on separate lines on the CMS 64 (MAR 1060/1062 reports) and 37 reports. These reports are reviewed for accuracy and deficiencies prior to submission to CMS.
OMPP submits program participation data to CMS including data for the number, type, and practice location(s) of providers who qualified for an incentive payment on the basis of having adopted, implemented, or upgraded

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 61 of 81
SMHP ANNUAL UPDATE – 2016
certified EHR technology or who qualified for an incentive payment on the basis of having meaningfully used such technology as well as aggregate de-identified data.
D.16 Coordination with Medicare to Prevent Duplicate Payments OMPP relies on the Medicare & Medicaid EHR Incentive Program R&A to support the registration of Indiana providers wishing to participate in the Indiana Medicaid EHR Incentive Program. OMPP evaluates transactions from the Medicare & Medicaid EHR Incentive Program R&A to determine if providers eligible for both Medicaid and Medicare payments have already received Medicare payments.
MAPIR has an electronic bi-directional interface with the Medicare & Medicaid EHR Incentive Program R&A. Specification details for this interface are described in the MAPIR system documentation provided separately to CMS.
D.17 Incentive Payment Recoupment In the event OMPP determines monies have been paid inappropriately, the existing recoupment process is leveraged to recover the funds. An Accounts Receivable (AR) record is created associated with the appropriate provider and the payment identified as an overpayment. If payment amounts need to be collected, they are refunded to CMS via the appropriate CMS 64 adjustment. Indiana Medicaid policy allows OMPP to work out an acceptable repayment period dependent upon the provider circumstances and the amount of the AR.
Indiana considers provider incentive payment as revenue to the provider and shown on the provider’s annual 1099. When the provider is currently identified as a provider for whom payments are being offset through MMIS to recoup monies paid in error, the incentive payment is withheld, partially or in full, to satisfy monies owed to the Medicaid program.
AR can be manually established in the MMIS through the AR entry window. Or, an AR can be established in the MMIS through MAPIR. This process is described in the MAPIR Administrative User Manual. Once the AR is established, Finance staff has the ability to turn the manual recoupment indicator on or off. If the manual recoupment indicator is turned on, then the system will not recover money from any payments, and all recoupment must be applied manually through the AR Disposition window for that record. Finance staff also has the ability to choose how the system will recoup money. The system will recover either a user specified percentage of each payment, or a user specified payment rate. Finally, the user can specify a weekly maximum recoupment amount for a Provider/Service location from the Provider AR Recoupment limit window. If a recoupment limit record exists, the system will not recoup any money once the weekly recoupment limit has been recovered.
These funds are identified as Indiana EHR Incentive Program reversals and as such reduce the amount of the Quarterly Provider Incentive Payment Federal Fund draw.
OMPP has procedures to verify the eligibility for payments and disbursement of provider payments. Monies are recouped if there are overpayments or erroneous payments. A system is in place to fight fraud and abuse, ensuring that there is no duplication of payment between Medicare and Medicaid as well as no duplication with other neighboring state’s payments. Indiana uses the Medicare & Medicaid EHR Incentive Program R&A to identify and

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 62 of 81
SMHP ANNUAL UPDATE – 2016
prevent duplicate payments with Medicare and neighboring states.
In addition, processes are in place to identify when income is taxable, and if so to report it to the Internal Revenue Service (IRS) on form 1099. Reports are made to the federal government as required. ARRA reporting has been established, and a determination made of what financial information is to be reported on the CMS 64 Reports.
D.18 Fraud and Abuse Prevention At this time OMPP does not have any automated exchange of information with the Indiana Professional Licensing Agency (IPLA). All providers are manually checked for valid licensure before being enrolled in Indiana Medicaid. When the provider enrolls in the EHR Incentive Program through the EHR Incentive Payment system, the system will verify the provider is valid based on NPI and TIN on the MMIS Master Provider file. The system then checks provider type and specialty to ensure the provider is an EP or EH. OMPP manually checks for current licensure against the most recent file from the IPLA. When the provider is not found on this data file, OMPP will manually verify with IPLA by checking their web site to determine valid licensure.
The state contracts with an outside vendor to check for sanctions on all Medicaid providers. Once a month, CMS sends a data file that is run against the Master Provider file to check for any new sanctions. The monthly sanction listing is continuously used to verify eligibility of currently-enrolled providers as well as providers seeking to enroll as a new IHCP provider. CMS also sends letters when new providers to the State are sanctioned. OMPP staff use multiple local resources to identify new sanctions. All these sources are reviewed prior to completing any provider’s enrollment in the Indiana Medicaid EHR Incentive Program.
OMPP continues to ask eligible professionals to attest that they are not hospital-based and do not provide in excess of 90% of their Medicaid patient encounters within a hospital and/or emergency room setting. In addition, OMPP continues to analyze professional claims/encounters for the reporting period with the provider’s NPI in the rendering provider field, and look at the place of service for the EP’s professional and hospital claims/encounters. Since the definition of “hospital based” now includes inpatient or Emergency Room (ER) setting, OMPP plans to use only Place of Service Codes 21 – Inpatient Hospital and POS 23 – Emergency Room as a basis for “hospital-based” services. During year 1, OMPP used repeatable queries for EHR Eligibility Operations Staff to use in manually determining EP hospital-based status; OMPP is determining options to improve the timeliness and efficiency of the enrollment process after launch. OMPP generates reports monthly from its data warehouse and uses these reports to manually review eligibility of EPs prior to approval of eligibility. If the predominant place of service is reported at the inpatient hospital or emergency room, OMPP will consider the provider to be hospital-based and will deny eligibility. Predominantly hospital-based is defined as more than 90% Medicaid services rendered within a hospital or ER setting.
Providers practicing within an FQHC or RHC setting shall not be subject to pre-payment verification. Program Integrity will audit using data warehouse reporting and follow up with further review if aberrancy noted.
D.18.1 Data Sources Used for Verification All encounter data is stored in the MMIS. Indiana will be able to use this data to validate patient volumes and claims/encounter volumes.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 63 of 81
SMHP ANNUAL UPDATE – 2016
The paid claims data and paid encounter claims received from the MCOs will be used as a check against that reported for patient volume by EPs. OMPP will query paid claims/encounter data from its data warehouse to verify the reasonableness of patient volume attested to by EPs. EPs will be asked to provide separate patient volume numbers from each of the different locations associated with their NPI, allowing for easier validation of volumes.
For eligible hospitals a check is conducted with the data warehouse to verify average length of stay for patients included in the numerator is 25 days or less.
D.18.2 AIU Verification EPs and EHs are required to attest to AIU in the EHR Provider Enrollment System and to produce documented evidence of AIU for onsite audits. This documentation required for post payment audit includes:
• Documentation referring to the certified EHR technology by name and certification number; the provider must be able to identify the modules certified and verify the CMS EHR Certification ID and CHPL product information
• Documentation showing a financial and/or contractual commitment (i.e., copy of invoice, purchase order, receipt, license agreement, contract copy)
• Documentation referring to the hospital attesting the commitment was made by another entity on the hospital’s behalf and the documentation will consist of a copy of use agreement, entity/hospital ownership, etc.
For EPs practicing within an FQHC/RHC review of documentation for the FQHC/RHC is acceptable. The document date does not have to be within the preceding fiscal year, if the reported version of the EHR technology was certified after the documentation date.
D.18.3 Validating Meaningful Use Indiana elected not to capture Meaningful Use measures for EPs during year one of the Indiana Medicaid EHR Incentive Program. An initial informal Clinical Quality Work Group was formed of medical, clinical, quality, and audit staff formed to discuss legislation, review data, make recommendations and provide direction on clinical and quality assurance issues and measures related to the EHR Incentive Program.
The Indiana EHR Provider Enrollment System accepts provider entry of Meaningful Use measures and determines accuracy of the numerator and denominator reported to meet these requirements. Indiana assumes that EHs currently participating in the Medicare PQRI program and EHR Incentive Program will report these measures to Medicaid beginning year 1. OMPP relies on provider attestation of accuracy of Meaningful Use measures reported in year 1. Our automated system has been updated to accept clinical quality measures to support attestation of Modified MU Stage 2 by a series of phased enhancements, all of which were implemented in July 2016.
OMPP will rely on Medicare & Medicaid EHR Incentive Program R&A accuracy of reported EHR product and EHR certification number as its primary source to verify if a provider has certified EHR technology available. The provider will also be required to include the CEHRT CHPL number on the contractual agreement submitted for each attestation year. The provider will be able to transmit and receive protected health information to and from other health care providers through his/her respective HIO. Indiana will work with the HIOs to determine if the number

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 64 of 81
SMHP ANNUAL UPDATE – 2016
and type of records (claim/encounter, lab results, radiology reports, ePrescribe transaction) transmitted by the EPs or EHs through the HIO will be available to OMPP through standard reporting mechanisms.
Indiana relies on MAPIR to accept provider entry of MU measures and determine accuracy of the numerator and denominator reported to meet these requirements.
OMPP will rely on Medicare & Medicaid EHR Incentive Program R&A accuracy of reported EHR product and EHR certification number as its primary source to verify if a provider has certified EHR technology available.
D.19 Provider Appeals OMPP has a process in place for an eligible provider to appeal payments and provider eligibility determinations, which is used to administer EHR Incentive Program payment appeals. OMPP has established an administrative review process to speed determinations—in this case, providers must obtain review from the contractor before filing an appeal with the state. The appeal process includes provider appeal of payments, provider eligibility determination and demonstration of efforts to adopt, implement, upgrade, or meaningfully use certified EHR technology.
OMPP leverages existing processes in place to manage formal provider appeals. OMPP works to minimize the number of complaints that require a formal appeals process by working closely with providers throughout the process. Complaints are defined as problems reported by providers that have been escalated to management level for resolution.
Complaints are documented by the fiscal authority (FA). The FA reviews and approves the request or forwards the request to level 2 reviews within the EHR Provider Incentive Program Operations Staff.
OMPP’s EHR Incentive Program Operations staff contacts the provider by phone to review eligibility requirements and provider’s eligibility information. A formal letter of denial with appeals rights is generated to those providers in “provider not eligible status.” Structured protocols and documentation exist to move the communication up the complaint channel. Provider Appeal criteria are specific and noted by regulation. Requests for documents are managed manually. Confidential documents are transferred by certified mail. Verification of information is handled and documented manually.
The Provider Manual includes information on how a provider may submit an appeal for the Indiana Medicaid EHR Incentive Program.
D.20 Federal Financial Participation (FFP) OMPP authorizes each incentive payment due to the provider through the EHR Incentive Payment system and subsequently the MMIS system. EPs are offered a choice of direct or assigned payments. In the case where the provider is a member of a group and chooses to assign the incentive payment to the group, these payments will be made to a group consistent with existing MMIS capabilities.
Providers are offered the option to participate in the voluntary retention at the time they request their annual incentive payment.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 65 of 81
SMHP ANNUAL UPDATE – 2016
D.21 Meaningful Use and Patient Volume Criteria D.21.1 Meaningful Use Measures – General Statement Indiana is using the MU measures, effective for 2013, as defined in the Final Stage 2 Rule at §495.6, Meaningful Use Objectives and Measures for EPs, EHs and CAHs. Updated to these rules were issued in September 2014 (2014 Flexibility Rule) at which time they were implemented in the program. These rules were again updated in 2015 (Modifications to Meaningful Use in 2015-2017 Rule) which have been incorporated.
D.21.2 Patient Volume Criteria by Program Indiana Medicaid services are provided to beneficiaries through multiple delivery systems. For purposes of the Indiana Medicaid EHR Incentive Program, the enrolled beneficiaries in the following programs are considered toward meeting patient volume:
• Hoosier Healthwise - Hoosier Healthwise is Indiana's health care program for low income families, pregnant women, and children.
• CHIP Package A - Effective January 1, 2013, in accordance with changes made in the MU Stage 2 regulations, Indiana added CHIP Package A beneficiaries as eligible to be considered toward meeting patient volume. CHIP Package A (the Medicaid expansion portion) covers uninsured children in families with incomes slightly higher than the Hoosier Healthwise program.
• Hoosier Care Connect - Hoosier Care Connect is a health care program that is designed to serve Medicaid beneficiaries who may have special health needs or benefit from specialized attention. Care Connect serves the aged, blind, disabled, wards of the court and foster children, or children receiving adoptive services and beneficiaries must also have one of the following medical conditions: Asthma, Diabetes, Heart Failure, Congestive Heart Failure, Hypertensive Heart and Kidney Disease, Rheumatic Heart Illness, Severe Mental Illness, Serious Emotional Disturbance for Wards and Fosters, and Depression.
• Healthy Indiana Plan (HIP) - The HIP plan covers individuals who do not live with a dependent child, and parents who earn up to approximately $44,000 annually for a family of four, have been uninsured for six months and do not have access to insurance through their employer.
• Traditional Medicaid - Traditional Medicaid is a low-income healthcare program that offers medical care such as doctor visits, prescription drugs, dental and vision care, family planning, mental health care, surgeries and hospitalizations. The Traditional Medicaid program is for individuals who have both Medicaid and Medicare eligibility, have a spend down/monthly deductible, or are refugees.
D.21.3 Patient Volume Calculation To calculate patient volumes for the Indiana Medicaid EHR Incentive Program, OMPP defers to the option at 42 CFR 495.306(c), which employs the patient encounter methodology. For patient volume calculations all populations funded by Title XIX and Title XIX expansion are considered eligible, and may be used in the numerator of the patient formula ratio. Additionally, as stipulated in the final MU Stage 2 Regulations, providers may count in the numerator any service rendered on any one day to a Medicaid-enrolled individual, regardless of payment liability.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 66 of 81
SMHP ANNUAL UPDATE – 2016
This includes zero-pay claims and encounters. Also, providers may count in the numerator of the patient volume ratio of out-of-state Medicaid recipients, if properly documented and needed to meet the patient threshold. FQHCs and RHCs will be able to use Title XXI members as well to calculate the needy individual calculation.
OMPP is using unique claims/encounter claims for the calculation of patient volume rather than using panel size or more complex equations. All fee-for-service and encounter information is captured in the MMIS, making retrieval of claims/encounter data possible for all Medicaid patients. This calculation is used for both EP and EH patient volume calculations.
Even after the changes made by the MU Stage 2 Regulations, identification of CHIP Package C members remains a significant issue for Indiana. Hoosier Healthwise members who receive services paid by Title XXI are seamlessly integrated through the Medicaid expansion 1115 waiver. Due to this integration, it is difficult for EPs, EHs, or CAHs to distinguish between patients receiving medical assistance under the Title XIX or Title XIX expansion versus Title XXI. The Hoosier Healthwise membership card does not distinguish between programs nor does the remittance advice report distinguish which funding sources paid for member’s claims. Additionally, the MMIS does not habitually generate premium reports and provider rosters down to that level of fidelity necessary to how the fund code/program code used to pay a Hoosier Healthwise provider. To account for this, and to reduce provider burden, Indiana will apply a percentage methodology to account for its CHIP member population. This percentage reduction will be applied in a single calculation at a statewide level, and will be used by all providers to better calculate their Medicaid patient volume.
Currently 2.52 percent of IHCP members are CHIP Package C recipients. This figure will apply by providers to the numerator in the Medicaid patient volume and will be adjusted on an annual basis.
OMPP is adopting the encounter methodology from the Final Rule §495.306, as updated in the MU Stage 2 final rule and the Modified Stage 2 final rule, to determine patient volumes EP and EH eligibility for the EHR Incentive Program. EP/EH patient volume threshold shall be calculated as follows for 2015 only:
• The EHR reporting period for EPs, eligible hospitals, and CAHs is any continuous 90-day period within the calendar year. EPs may select an EHR reporting period for any continuous 90 days from January 1, 2015 through December 31, 2015. Eligible hospitals and CAHs may select an EHR reporting period of any continuous 90-day period from October 1, 2014 to December 31, 2015. For eligible professionals, the action may occur at any point during that time as long as it is no earlier than January 1, 2015 and no later than the date of attestation for their 2015 EHR reporting period. For eligible hospitals and CAHs, the action may occur at any point during that time so long as it is no earlier than October 1, 2014 and no later than the date of attestation for their 2015 EHR reporting period. This is intended to accommodate the shift from reporting based on the federal fiscal year to the calendar year for eligible hospitals and CAHs.
• Medicaid providers may demonstrate patient volume by having patient encounters within the 90-day period using the methodology as follows:
o [Total (Medicaid) patient encounters in any representative continuous 90-day period in the calendar year /Total patient encounters in that same 90-day period] * 100
• “…A Medicaid provider must annually meet patient volume requirements of §495.306, as these requirements are established below in this SMHP.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 67 of 81
SMHP ANNUAL UPDATE – 2016
• “…The regulation at §495.306, as updated in the MU Stage 2 Regulation, states that a Medicaid encounter will exist where the individual was Medicaid enrolled (or enrolled in a CHIP expansion, but not the CHIP Part C stand-alone option) regardless of whether Medicaid paid all or part. However, providers will be allowed to include in the patient volume calculation individuals who are part of expansion populations under section 1115(a)(2) of the Act.” Indiana members across eligibility categories and funding sources are issued a single Indiana Health Coverage Programs (IHCP) card, thereby potentially hindering providers’ ability to differentiate between CHIP Package C (stand-alone) and Medicaid and CHIP Package A members. To account for this, and to reduce provider burden, Indiana will apply a percentage methodology to account for its CHIP member population. This percentage reduction will be applied in a single calculation at a statewide level, and will be used by all providers to better calculate their Medicaid patient volume. This percentage reduction will be published and available to providers, and will be updated annually to reflect changes.
• “…all EPs and the vast majority of hospitals will need to meet certain patient volume thresholds in order to be eligible for incentive payments. (The only exception to this rule is for Children’s Hospitals, which have no patient volume threshold requirement)…”
• “…for the Hoosier Healthwise member volume, these thresholds are calculated using as the numerator the individual EPs total number of member encounters in any representative continuous 90-day period in the calendar year of attestation and the denominator is all patient encounters for the same individual professional over the same 90-day period.”
• “…for the Hoosier Healthwise member volume, these thresholds are calculated using as the numerator the individual hospital’s total number of member encounters in any representative continuous 90-day period in the calendar year of attestation and the denominator is all patient encounters for the same individual hospital over the same 90-day period.”
• “EPs practicing predominantly in an FQHC or RHC must have a minimum 30% patient volume attributable to needy individuals as defined in §495.302 and will be evaluated according to their “needy individual” patient volume. To be identified as a “needy individual” patients must meet one of the following criteria:
o Received medical assistance from Hoosier Healthwise or CHIP;
o Were furnished uncompensated care by the provider; or
o Were furnished services at either no cost or reduced cost based on a sliding scale determine by the individual’s ability to pay.
• The number of needy individual encounters are calculated using as the numerator the individual EPs total number of needy individual encounters in any representative continuous 90-day period in the calendar year of the date of attestation and the denominator is all patient encounters for the same individual professional over the same 90-day period.”
Beginning in 2016 OMPP will adopt the encounter methodology from the Final Rule §495.306, as updated in the MU Stage 2 final rule and the Modified Stage 2 final rule. The EHR reporting period for this period must be completed within January 1 and December 31 of the calendar year. EPs eligible hospitals, and CAHs that are new

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 68 of 81
SMHP ANNUAL UPDATE – 2016
participants in the program would have an EHR reporting period of any continuous 90-day period between January 1, 2016 and December 31, 2016. However, for all returning participants, the EHR reporting period would be a full calendar year from January 1, 2016 through December 31, 2016.
In 2017, the EHR reporting period will be one full calendar year for all providers except new participants and/or providers who choose to implement Stage 3. Participants and/or providers who choose to attest to Stage 3 Meaningful Use in 2017 will be allowed a 90-day reporting period. Table 9 (below) summarizes the patient volume rules for Indiana’s EHR Incentive Program.
Table 9. Patient Volumes for Indiana EHR Incentive Program
EH Type Patient Volume over 90-day Period
Acute Care Hospitals • 10%
Children’s Hospitals • No percentage required
Critical Access Hospitals • 10%
EP Type Patient Volume over 90-day Period for 2015
Physicians (MD or DO) • 30 %
Dentists
Advanced Practice Nurses*/Nurse Practitioners or Certified Nurse Midwifes
Physicians (MD or DO), Dentists, Certified Nurse-Midwives, Advanced Practice Nurses*/Nurse Practitioners, and Physician Assistants who are practicing predominantly in an FQHC or RHC
• For Medicaid EPs in FQHC or RHC – 30% Needy Individuals (including Hoosier Healthwise Title XIX and CHIP Title XXI members)
Pediatricians** (identified on Medicaid provider agreement)
• 30% - EP receives full incentive payment • Patient volume = 20 – 29% the
pediatrician may qualify for 2/3 incentive payment
* Pursuant to 848 IAC 4-1-3 Advanced Practice Nurse (Provider Type 09) includes: Nurse Practitioner, Certified Nurse Midwife and Clinical Nurse Specialist. Advance Practice Nurses are inclusive of all types of Nurse Practitioners and all Nurse Practitioners are included under the Advance Practice Nurse designation.
**Indiana Medicaid recognizes the specialty “pediatrician” as indicated by the physician on his/her provider agreement and enrollment application.
D.22 Dependence upon Federal Initiatives Recent federal HIT initiatives, such as the State HIE Cooperative Agreement, the RECs, broadband initiatives, and the EHR MU Incentive Program, were designed to accelerate and broaden changes in our health care systems by building information system capacity. Ultimately, meeting federal targets to foster the adoption of EHRs and deploy state and regional exchange networks were intended to improve health care, population health, and the cost of care. Despite the presence of Indiana’s long established and successful HIOs and HIE networks, OMPP has been dependent on the success of HITECH and other federal initiatives to advance priorities for Indiana’s essential

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 69 of 81
SMHP ANNUAL UPDATE – 2016
HIT/HIE infrastructure serving public health care programs. Specifically for Indiana, these priorities includes supporting individual providers to adopt and effectively utilize new information system capacity i.e. EHRs and HIE, and to enhance the safety, quality and overall value of health care services provided to Medicaid and CHIP enrollees. As the OMPP’s HIE partners have experienced, support from federal initiatives has “raised the bar” for what can be accomplished in building HIE capacity and redefining health care business operations.
As HITECH Act funding is phased out, Indiana is dependent upon its working relationships with ONC, CMS and other agencies to take advantage of remaining resources, leverage opportunities for technical assistance, and to share the results of HIT innovations and testing projects for lessons learned, best practices, and specific examples of how EHRs and electronic exchange can further benefit both providers and members.
Moving forward, OMPP is dependent upon CMS as a critical partner in ongoing efforts to build and sustain organizational infrastructure and operations. This includes being able to leverage federal resources to sustain coordination with the effective HIE governance and the role of the HIT coordinator to continue the successful multi-sector collaboration and coordinated efforts to leverage investments in HIT and HIE technology. As the Indiana Medicaid EHR Incentive Program continues to mature, CMS support will be critical as OMPP and Medicaid providers work through challenges to enhance their meaningful use reporting using their EHR systems and HIE connectivity.
Overall, OMPP is dependent upon federal agencies for continued support through rule making, standards development and public policy. Coordination among federal agencies and initiatives is important for its impact at the state level to streamline quality reporting efforts and find ways for the HIE marketplace to leverage effective Meaningful Use requirements and subsequent CQM measures. OMPP is dependent upon ONC to assist with moving the marketplace, such as by upgrading product certification so that Indiana Medicaid providers can adopt, implement, or upgrade to appropriate certified EHR systems.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 70 of 81
SMHP ANNUAL UPDATE – 2016
E. The State’s Audit Strategy The aforementioned Audit Work Group, in addition to approved contractor, Meyers and Stauffer, LC and Truven Health Analytics have developed the State’s Audit Strategy and Plan for the Indiana Medicaid EHR Incentive Program. The Audit Strategy update was approved by CMS on December 11, 2014. Policies and procedures from FSSA’s Audit Services, Medicaid Finance and Program Integrity units will be used during the life of the project to perform the auditing for the EHR Incentive Program. Indiana FSSA Audit Services and the Indiana HIT FSSA Audit Work Group will work collaboratively with the Indiana FSSA Medicaid Finance Team, the Indiana FSSA Program Integrity Team, the HIT FSSA Work Groups, Indiana’s MMIS Fiscal Agent (HP), and other HIT-required resources and entities to ensure needed information and data is both provided and/or received in a timely manner.
Following (Table 10, below) is a summary of audits performed in 2013 per the Regional Office (RO) Data Tool submitted in 2015:
Table 10. Audit Statistics as reported in RO Data Tool submission to CMS
Type of Audit Actual Notes
EP AIU audit 57
EP MU audit 136
EH audit 0 No AIU EH providers attested in 2013; MU will be completed by CMS
The number of Program Year 2014 and 2015 audits to be performed will be based in part on risk analysis from Program Year 2013 audits and will also represent a sample size of providers paid.
E.1 Category 1 – Incentive Payment Audits In accordance with §495.318 and §495.320, the State administers Incentive Payments to providers under the Indiana EHR Incentive Program at 100% FFP. The following auditing phases are in scope for the Indiana EHR Incentive Program and Indiana FSSA Audit Services:
• Phase 1 – Pre-payment Auditing of Eligible Professionals (EPs) and Eligible Hospitals (EHs) for Adopt, Implement, or Upgrade (AIU) attestations applicable to participation Year 1 Provider Incentive Payments;
• Phase 2 – Pre-payment procedures of EPs and Post-Payment Auditing of EPs and EHs for Adopt, Implement, and Upgrade attestations applicable to participation Year 1 Provider Incentive Payments;
• Phase 3 – Pre-payment procedures of EPs and Post-Payment Auditing of EPs for Meaningful Use (MU) Stage 1 attestations and for automated reporting of clinical quality measures (CQMs) using certified EHR technology which is interoperable with the system designated by the State to receive the data (e.g. HP’s MAPIR system and application) applicable to providers participation in Years 2 through 6 Payment Years; and

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 71 of 81
SMHP ANNUAL UPDATE – 2016
• Phase 4 – Pre-payment procedures of EPs and Post-Payment Auditing of EPs for MU Modified Stage 2 and Stage 2 attestations and, as they become available, Stage 3 attestations.
Note #1: CMS has communicated its intention to audit all EHs for meaningful use for provider participation in Years 2 through 6. The state of Indiana agrees to have CMS perform these audits; thus the State is not including EH MU audits in its audit strategy.
Note #2: Post-payment validation of MU is incorporated in the audit strategy within this category of audits.
E.2 Category 2 – Administrative Expense Audits In accordance with §495.322 and §495.324, enhanced federal funding participation (FFP) is available for the Indiana EHR Incentive Payment program. As such, there are strict guidelines in the application, approval, and retention process of the granted 90% FFP. CMS allows the 90% FFP for state expenditures of administrative activities in support of the Indiana EHR Incentive Program with prior CMS approval.
The Indiana FSSA Medicaid Finance Team will continue to conduct Category 2 – Administrative Expense Audits. The Category 2 – Administrative Expense Audits are independent of the Category 1 – Incentive Payment Audits. However, the post-auditing findings from both audit events are shared internally with the Indiana EHR Incentive Program Leadership Team and posted on the secure HIT FSSA SharePoint site.
The following budget items are included in the Administrative Expense Audit and are reflected in §495.338(g):
• The cost to implement and administer the incentive payments to eligible providers;
• Procurement or acquisition costs;
• State personnel costs;
• Contractor services costs;
• Hardware, software, and licensing expenses;
• Equipment and supplies;
• Training and outreach expenses;
• Travel costs;
• Administrative operations costs; and
• Miscellaneous expenses for the project not otherwise categorized.
E.3 Audit Settings EHR incentive payment audits are conducted within two settings:
• Desk audit – this is an audit conducted within the State of Indiana’s physical office location for AIU audits or within the physical office location of contractor, Myers and Stauffer, LC for MU audits.
• Field audit – this is an audit conducted specifically with a provider, onsite at their physical location with

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 72 of 81
SMHP ANNUAL UPDATE – 2016
advance notice of the audit and on a mutually agreed upon date.
The Indiana HIT EHR Administrative Audit is conducted within one setting:
• Desk audit – this is an audit conducted within the State of Indiana’s physical office location.
E.4 Audit Methodologies, Standards, Processes, and Procedures Indiana FSSA Audit Services, Myers and Stauffer, LC and the Indiana FSSA Medicaid Finance Team employ consistent methods, standards, processes, and procedures in order to perform the required audit tasks for the Indiana EHR Incentive Program to be in full compliance with the CMS regulations.
Indiana understands the importance of the State’s requirements of monitoring, measuring, verifying, validating, and reporting activities as it pertains to disbursing incentive payments to the providers related to the following areas:
• Adopt, Implement, or Upgrade (AIU);
• Meaningful Use (MU) of certified EHR technology; and
• Receipt of automated reporting of clinical quality measures.
A provider selection process based on proven Medicaid stratification variables and risk assessment criteria will be utilized for the Incentive Payment Audits prior to the audit(s) being performed. Indiana FSSA Audit Services and the HIT FSSA Audit Work Group is committed to utilize existing and successful Program Integrity policies, processes, and procedures, in addition to defined Fraud and Abuse Detection Audit policies, processes, and procedures where appropriate. Where required, the Indiana EHR Incentive Program FSSA Audit Work Group has developed Indiana EHR Program-specific auditing policies, processes, and/or procedures to ensure thorough and independent reviews are performed. Indiana FSSA Audit Services Reports and Findings are documented in detail, and through the examination of the audit results, any additional controls, changes, or process improvements will be recommended and considered for future implementation. Indiana also understands the importance of managing the fiduciary responsibilities of financial accountability and oversight of the administrative activities and funds related to the components of the Indiana Medicaid EHR Incentive Payment program’s budget allowing 90% FFP as outlined in Administrative Expense Audits. The Indiana FSSA Medicaid Finance Team will monitor, measure, verify, validate, and report the financial information in accordance with both state and federal regulations.
E.4.1 Audit Periods E.4.1.1 Phase 1 The Phase 1 Audit Period has been identified as Monday, May 2, 2011 through Wednesday, February 29, 2012. May 2, 2011 was the first business day which Indiana enrolled an eligible provider in the Indiana EHR Incentive Payment Program.
The Phase 1 Auditing Period data will include eligible providers (e.g., both EPs and EHs) participating in the Indiana EHR Incentive Program meeting AIU attestations and paid the participating Year 1 incentive payment. The Phase 1

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 73 of 81
SMHP ANNUAL UPDATE – 2016
Audit Period is considered the 2011 Calendar Year (Participating Year 1) plus the two (2) tail months into Calendar Year 2012 (e.g., January 1 – February 29, 2012).
E.4.1.2 Phase 2 and Beyond The FSSA has contracted with Truven Health Analytics and Myers and Stauffer LC to implement the Phase 2 and Phase 3 MU audit reviews, which are detailed below. The auditing processes and procedures for MU Modified Stage 2 and Stage 3 will be revised after the State determines the changes required to incorporate the Modified Stage 2 and Stage.
CMS released a final rule in 2015 that specifies criteria that eligible professionals (EPs), eligible hospitals, and critical access hospitals (CAHs) must meet in order to continue to participate in the Medicare and Medicaid EHR Incentive Programs. The final rule’s provisions encompass EHR Incentive Programs in 2015 through 2017 (Modified Stage 2) as well as Stage 3 in 2018 and beyond.
Starting in 2015, all providers will be required to attest to a single set of objectives and measures known as Modified Stage 2. Since this change may occur after providers have already started to work toward meaningful use in 2015, there are alternate exclusions and specifications within individual objectives for providers who were previously scheduled to be in Stage 1 of the EHR Incentive Programs.
Starting in 2015, the EHR reporting period for EPs, EHs, and CAHs will be based on the calendar year. This allows more time for hospitals and CAHs to implement certified EHR technology, and aligns the EHR Incentive Programs with reporting periods in other CMS quality reporting programs.
In 2015, all providers are required to use technology certified to the 2014 Edition. In 2016 and 2017, providers can choose to use technology certified to the 2014 Edition or the 2015 Edition.
In 2015 only, the EHR reporting period for EPs, EHs, and CAHs is any continuous 90-day period within the calendar year. EPs may select an EHR reporting period for any continuous 90 days from January 1, 2015 through December 31, 2015. Eligible hospitals and CAHs may select an EHR reporting period of any continuous 90-day period from October 1, 2014 to December 31, 2015. This is intended to accommodate the shift from reporting based on the federal fiscal year to the calendar year for eligible hospitals and CAHs. Beginning with 2016, the EHR reporting period must be completed within January 1 and December 31 of the calendar year. EPs eligible hospitals, and CAHs that are new participants in the program would have an EHR reporting period of any continuous 90-day period between January 1, 2016 and December 31, 2016. However, for all returning participants, the EHR reporting period would be a full calendar year from January 1, 2016 through December 31, 2016. In 2017, the EHR reporting period would be one full calendar year for all providers except new participants and/or providers who choose to implement Stage 3, who are allowed a 90-day reporting period.
There are several alternate exclusions and specifications for certain measures that are intended to help providers previously scheduled to be in Stage 1 that may not otherwise be able to meet the criteria in 2015 and 2016 because they require the implementation of certified EHR technology beyond the functions that were required for Stage 1.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 74 of 81
SMHP ANNUAL UPDATE – 2016
OMPP has a standard tail period of 60 days. However, OMPP maintains flexibility to address unavoidable events, such as rule changes, which may affect a significant portion of the provider population. When these events occur, OMPP may extend the tail period to provide adequate time for the providers to submit their attestations.
The Phase 2 Audit Period is for Program Year 2012, which was October 1, 2011 through September 30, 2012 for EHs and January 1, 2012 through December 31, 2012 for EPs. Phase 2 also included a 60 day attestation tail period for both EHs and EPs.
Beginning in program year 2018, Phase 3 MU Audit Periods for the payment year in which the EP is first demonstrating MU, will be any continuous 90-day period within the calendar year. For the subsequent payment years following the payment year in which the EP has first successfully demonstrates MU, the period will be the calendar year. FSSA will continue to monitor the Phase 3 rules for updates and modifications and will implement these as appropriate.
Indiana FSSA Audit Services and the Indiana HIT FSSA Work Group will reassess the results of the most recent MU provider’s auditing results, internal and external documentation, CMS audits or recommendations, and provider audit reports and audit findings to capture lessons learned in order to improve any internal audit processes, adopt new audit procedures, or identify other areas to enhance for the following audit years.
E.5 Audit Planning E.5.1 Audit Preparation FSSA Audit Services or their contractor will obtain and review the following information and data in order to prepare for Desk Audits, Target Audits, Onsite Audits, and/or Field Audits of AIU payments, including, but not limited to:
• Review summary of Eligible Professionals (EPs) and Eligible Hospitals (EHs) Indiana EHR AIU Incentive Payments paid;
• Review the detail list of EPs and EHs and their respective Indiana EHR AIU Incentive Payments paid;
• Review the federal and state acceptability criteria (e.g. AIU of CEHRT) for paying the incentive payments to providers participating in Year 1;
• Review sample(s) of an official copy(s) or access electronic attached attestation materials provided to Indiana during the provider registration process;
• Review a sample of Medicaid enrollment volume reports submitted by the providers;
• Review a sample other reports or information submitted by the providers during the Indiana HIT EHR registration and attestation process;
• Review a sample of providers who were deemed ineligible by the Fiscal Agent (e.g. providers sent a formal denial letter with appeal rights with a status of “provider not eligible status”);
• Review of the current State Medicaid Health Information Technology Plan (SMHP); and
• Identify, document, and perform detailed provider data selection criteria.
As a component of Audit Planning for AIU audits, Indiana FSSA Audit Services considers a number of risk

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 75 of 81
SMHP ANNUAL UPDATE – 2016
assessments based on the following examples, including, but not limited to:
• Current FSSA Program Integrity and Fraud and Abuse Detection audit policies, processes, procedures, and risk assessments of individual providers;
• Providers subjected to other program integrity audits;
• EHs with exceptionally large incentive payment amounts;
• Providers with licensure suspensions, OIG debar, etc.; and
• Unusual distribution pattern of claims or Meaningful Use measure reporting by Provider.
Additional information, Medicaid providers who are known within the agency for aberrant billing procedures and for which a Field Audit is scheduled, will be reviewed by the FSSA Audit team for appropriateness of EHR Incentive Program payments. There are several approaches to making a risk analysis. Regardless of the method followed, the FSSA Audit team must consider all factors relevant to the audit objective.
OMPP did not perform post-payment auditing for meaningful use during Year 1 Participation, but did focus on AIU of CEHRT. FSSA Audit Services has leveraged their documented Audit policies and procedures, OMPP’s current MITA business processes, and Program Integrity’s policies and procedures for conducting risk assessment and conducting post-payment audits.
E.5.2 Preparation for EHR Incentive Payment Audits FSSA Audit Services or their contractor will obtain and review the following information and data in order to prepare for Desk Audits, Target Audits, Onsite Audits, and/or Field Audits of Meaningful Use payments, including, but not limited to:
• Review summary of Eligible Professionals (EPs) and Eligible Hospitals (EHs) Indiana HIT EHR MU Incentive Payments paid;
• Analyze the detail list of EPs and their respective Indiana EHR MU Incentive Payments paid for purposes of creating an audit population;
• Review other reports or information submitted by the providers during the Indiana HIT EHR registration and attestation process as necessary to conduct risk assessment;
• Review of the current State Medicaid Health Information Technology Plan (SMHP); and
• Identify, document, and perform detailed provider risk assessment selection criteria for the reported Meaningful Use numerators and denominators.
A detailed description of the review process for these audits is outlined in the Audit Strategy that was updated by FSSA and submitted to CMS in 2016.
E.5.3 Additional Information Provider “pre-appeal” situations could include disputed payment amounts, Medicaid patient volume percentage, evaluation of hospital-based services for an EP, and a hospital’s qualification to participate. The pre-appeal process

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 76 of 81
SMHP ANNUAL UPDATE – 2016
may be initiated by a phone call or through written notification of the discrepancy. In the pre-appeal process, the provider will have ten (10) business days to provide the additional information that supports their request, prior to their request being denied. If that information is not provided within the given time frame or the information is insufficient, the provider will be notified either by phone or via mail that the request is being denied. At this point, the provider can choose to proceed to a formal appeal process.
OMPP has an established Program Integrity (PI) department which is responsible for preventing fraud, waste, and abuse through yearly and “as needed” audits. This department is overseen by the Program Integrity Manager and will work in collaboration with the Surveillance Utilization and Review (SUR) contractor, and FSSA Audit Services where appropriate.
OMPP ensures that a system is in place to fight fraud and abuse, ensuring that there is no duplication of payment between Medicare and Medicaid as well as no duplication with other neighboring state’s payments. Indiana shall use the Medicare & Medicaid EHR Incentive Program Registration & Attestation System (R&A) to identify and prevent duplicate payments with Medicare and neighboring states during the post-payment process.
The State’s FSSA Audit Services Team and the OMPP Program Integrity Team work in partnership where high risk providers may be identified. It is the goal of the State for the HIT EHR FSSA Audit processes to verify and validate accuracy and legitimacy of the payments made through this program.
The State is continuing to work with Truven and MSLC to develop and improve a number of processes based on knowledge gained over the past five years, as well as through their experience with the EHR program.
The State of Indiana will continue to use the past participation process as a foundation to determine potential weakness, improve or revise existing procedures, or identify opportunities for provider education or training, including, but not limited to, monitoring and analyzing trends, reviewing data reports with related health informatics, and payment and/or meaningful use measurements necessary to monitor, measure, report and improve the program.
E.5.4 Incentive Payment Recoupment In the event OMPP determines monies have been paid inappropriately, the current recoupment process will be leveraged to recover the funds. An Accounts Receivable (AR) record will be created associated with the appropriate provider and the payment identified as an overpayment. Payment amounts may need to be collected and would be refunded to CMS via the appropriate CMS 64 adjustment. Indiana Medicaid policy allows OMPP to work out an acceptable repayment period dependent upon the provider circumstances and the amount of the AR.
Indiana shall consider provider incentive payment as revenue to the provider and shown on the provider’s annual 1099. When the provider is currently identified as a provider for whom payments are being offset through MMIS to recoup monies paid in error, the incentive payment will be withheld, partially or in full, to satisfy monies owed to the Medicaid program.
AR can be manually established in the MMIS through the AR entry window. From this window, an AR record can be setup against a provider. Finance staff has the ability to turn the manual recoupment indicator on or off. If the manual recoupment indicator is turned on, then the system will not recover money from any payments, and all recoupment must be applied manually through the AR Disposition window for that record. Finance staff also has the

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 77 of 81
SMHP ANNUAL UPDATE – 2016
ability to choose how the system will recoup money. The system will recover either a user specified percentage of each payment, or a user specified payment rate. Finally, the user can specify a weekly maximum recoupment amount for a Provider/Service location from the Provider AR Recoupment limit window. If a recoupment limit record exists, the system will not recoup any money once the weekly recoupment limit has been recovered.
These funds will be identified as Indiana HIT EHR MU Incentive Payment Program reversals and as such will reduce the amount of the Quarterly Provider Incentive Payment Federal Fund draw.
During the implementation phase, OMPP established procedures to verify the eligibility for payments and disbursement of provider payments. Monies must be recouped if there are overpayments or erroneous payments. A system is in place to fight fraud and abuse, ensuring that there is no duplication of payment between Medicare and Medicaid as well as no duplication with other neighboring state’s payments. Indiana uses the Medicare & Medicaid EHR Incentive Program R&A to identify and prevent duplicate payments with Medicare and neighboring states.
In addition, processes must be in place to identify when income is taxable, and if so to report it to the Internal Revenue Service (IRS) on form 1099. Reports must be made to the federal government as required. ARRA reporting must be established, and the determination made of what financial information must be captured and made through ARRA and reported on the CMS 64 Reports.
E.5.5 Audit Tools The following tools will be used during the Indiana EHR Incentive Program and the Audit Plan:
• Audit materials
• FSSA HIT SharePoint site
• Indiana HIT Field Audit Document Request List
• Indiana HIT Desk Audit Report Template
• Indiana HIT Field Audit Report Template
• Indiana HIT Audit Findings Template
OMPP ensures that a system is in place to fight fraud and abuse, ensuring that there is no duplication of payment between Medicare and Medicaid as well as no duplication with other neighboring state’s payments. Indiana shall use the Medicare & Medicaid EHR Incentive Program Registration & Attestation System (R&A) to identify and prevent duplicate payments with Medicare and neighboring states during the post-payment process.

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 78 of 81
SMHP ANNUAL UPDATE – 2016
F. The State’s HIT Roadmap In its initial SMHP, OMPP focused on the planning and implementation tasks necessary to ensure implementation of Indiana EHR Incentive Program. It also laid out a comprehensive roadmap spanning several years to achieve incremental goals and objectives for realizing HIT and HIE capacity. This section includes an updated overview of how OMPP plans to move from the current “As Is” HIT environment to achieve the “To Be” vision for health information exchange. It reflects the progress that has been made as well as the new opportunities that have arisen. This updated view of Indiana’s HIT Roadmap incorporates the next challenges for Indiana’s EHR Incentive Program to prepare for future meaningful use requirements, and aligns with funding requests for the projects in support of goals and objectives over the next five years.
F.1 Moving from “As Is” to “To Be” HIT Landscape Table 11 (next page) captures the universe of health care IT projects, many which are currently underway, that are part of a set of incremental planning and implementation activities that impact or are impacted by the EHR Incentive Program.
OMPP is focused on its next phase of activity, including program process improvements, management and reporting tools, enhanced provider outreach, training, and education, auditing and fraud detection methods, and other system changes. OMPP is also moving forward with its plan for MMIS re-procurement and Public Health information exchange. Beyond the initiatives in Table 11, OMPP continues to take a targeted approach toward projects that promote the four “pillars” of the state’s comprehensive HIT/HIE strategy:
1. Data access
2. Interoperability
3. Improving outcomes
4. Supporting federal and state health care programmatic initiatives
Within this context, OMPP is currently focused on specific Medicaid HIT/HIE strategic priorities that are timely with the goal of advancing health information capacity to the next level. Top priorities for Medicaid include, developing quality reporting including CQMs and other reporting of clinical data, and building capacity for data analytics. Other areas of technical and policy development include expanding query-based exchange, addressing data segmentation and issues related to more granular patient consent, and responding to evolving technical standards and HIPAA rules.
F.2 Tactics to Support the Strategy for the HIT Roadmap As a result of the e-scan performed for the 2016 update to the Indiana SMHP, many new strategies were identified and existing strategies expanded. The following tactics are necessary to support the strategies outlined in the table above:
• Continued collaboration with public private stakeholder engagement and technology implementations
• Monitor Indiana’s HIT and HIE portfolio management and progress

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 79 of 81
SMHP ANNUAL UPDATE – 2016
• Transparent measurement and reporting on federal/state funded programs and insight into private HIT and HIE market progress
• Coordination with Medicaid programs providing support and solutions identifying HIT and HIE opportunities for underserved populations
• Medicaid quality measurement strategy supporting MCOs
• Support and coordination with ISDH Public Health IT Strategy improving the quality, safety, and health of citizens of Indiana through improved data collection and data quality supporting population health measurement
Table 11. OMPP IT Roadmap (Includes HIT/E and mission-critical administrative systems)
As Is To Be
MU Incentive Program
• Technical Assistance (TA) and outreach to providers that participated in REC and continue to require TA for EHR adoption and MU
• Additional support to rural providers, critical access hospitals
• Benchmarks for the Incentive Program overall targets by the end of 2016, 2021
HIE Services
Governance
• Attendance at HIT/E stakeholder convening events
• Coordination with public and private HIT/E strategic efforts and technical services
• Coordination with private HIE market to advance electronic exchange of health information
• Continued collaboration with public private stakeholder engagement
• State HIT portfolio management
• Expand Indiana health information network for complete geographic and provider coverage
Advance Health Information Exchange HIE Functionality
• Submit APD for enhanced Public Health data reporting technical infrastructure development and advanced technical assistance
• Coordination between ISDH and HIEs for coordinated public health reporting reducing needs for point to point connections.
• Identify underserved care providers such as school health clinics querying through HIE.
• Coordination with private HIE stakeholders to advance use of Standards and Normalization to improve data quality
• Future development for querying CHIRP for up to date patient immunization information is available
• Awareness of Indiana’s private HIE technology advancements and innovations
• Continued focus on strategies to reduce the obstacles to HIE adoption in rural and underserved areas across the state.
• Identify other underserved populations and provider groups needing additional assistance
• EHR Interoperability - INPC-to-EHR inter-operability jointly designed with customers and EHR vendors
• Neighboring State HIE - Statewide and Interstate data exchange that strengthens sustainability and value proposition in healthcare markets that cross state lines
• Support for Population Health - Services to provide data and

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 80 of 81
SMHP ANNUAL UPDATE – 2016
As Is To Be information to support population health management
Technical Assistance Coordination
Technology Adoption Practice Transformation Assistance
• Continue Meaningful Use provider attestation assistance (REC)
• Educate on quality improvement and workflow improvement
• Attestation walk thrus - including troubleshooting with HP/MAPIR
• Documentation/audit recommendations
• Education on value based purchasing to providers
• Providing education and simple root cause analysis/ gap analysis on metrics and trouble shoot, address and improve metrics, security risk assessment, and registration and attestations.
• Expanded Rural Health support for Critical Access EP
• Expand technical assistance to additional Medicaid providers regardless of MU eligibility, including Safety Net hospitals
• Meaningful Use help desk coordination
• Coordinate education programs across MU, HIE, TCPI, PH MU attestation, and other provider education services
• Statewide technical assistance increasing successful MU attestations
• Increased technology adoption by rural, non-eligible providers
Public Health – Meaningful Use Support and Data Portal
Public Health Meaningful Use Assistance
• Develop and submission of Advanced Planning Document (APD) supporting public health information technology and exchange for MU attestations with MU technical assistance, help desk, PH MU data portal (DDI), and security assessment
• Implement PH MU website portal
• Design, develop, and implement MU data portal as a central public health data gateway for multiple registries.
• Develop new guidelines and outreach plan for submitting to ISDH Cancer Registry
• Improved and increased public health data reporting to support MU
• Reduced MU exemptions • Improved PH data quality • Coordinated provider MU TA and
education • Bidirectional immunization
information available real-time for accurate immunization updates
• Increase data reporting to ISDH Cancer Registry
Public Health Technical Services
• CHIRP • MyVax • Electronic Lab reporting • Syndromic Surveillance
• Public Health Data Quality Assurance
• Public Health Data Gateway • ISDH MU Data Encryption
Audit and Security Scan • Cancer registry technical
guideline
• Bidirectional immunization data submission and retrieval by EPs, EHs, and CAHs:
• Real-time bidirectional immunization data flow
• ISDH MU Data Encryption Audit and Security Scan

State of Indiana Family and Social Services Administration – Office of Medicaid Policy & Planning
State Medicaid HIT Plan (SMHP) 2016 Update
Page 81 of 81
SMHP ANNUAL UPDATE – 2016
F.3 MMIS-Related Activities Replacement of the MMIS represents an enormous technical move forward for OMPP. In addition to web-based graphical user interfaces (GUIs), Medicaid operations, members and providers alike will benefit from the enhanced interoperability features of the new MMIS. The new technology (e.g., SOA and ESB) when implemented will improve data sharing with HIOs, ISDH and other stakeholders. The new MMIS solution should be fully implemented by late 2016.
In addition to MMIS replacement, a number of projects are planned to expand, leverage or replace existing systems and features, dependent upon the completion of the MMIS replacement:
• OMPP is in the process of implementing an Enterprise Data Warehouse, also by late 2016.
• A new Pharmacy Benefit Manager initiative, which will facilitate e-Prescribing among Medicaid providers and pharmacies, is also in progress.
In addition, federally-mandated MMIS projects include planning, assessment, and compliance with ICD-10 and 5010, as well as D.0.and 3.0. Planning will address provisions for replacing the eligibility and enrollment system in conjunction with the rollout of the ACA.
F.4 HIT Objectives for Meaningful Use of Clinical Data An updated strategy for capturing clinical quality measures and data from EPs and EHs is being developed as the participants in the EHR Incentive Program prepare for Stage 2 and Stage 3 reporting requirements. As the majority of providers are gaining active status as participants in the EHR incentive program, demonstrating meaningful use and the reporting of Clinical Quality Measures will continue to be the prevailing priorities as Stage 2 and Stage 3 requirements are instituted. Organizing and integrated quality reporting strategy is an important ongoing focus
Enhanced data collection will support a wide range of analyses. For instance, working collaboratively with ISDH to develop population based data analytics will be one priority. The public health opportunities associated with building the capacity of the statewide HIE network are immense. The State Immunization registry and public health surveillance reporting database are two examples of databases that can be populated with information that is gathered through the HIOs. The FSSA HIT unit is working closely with ISDH to plan and fund further expansion of the Indiana Immunization Registry capabilities described in the SHIECAP and the IAPD currently being submitted to CMS.