Embed Size (px)
Citation preview

4050 Esplanade Way
Tallahassee, Florida 32399-0950
Tel: 850.488.2786 | Fax: 850. 922.6149
Chad Poppell, Secretary Rick Scott, Governor
STATE OF FLORIDA
DEPARTMENT OF MANAGEMENT SERVICES
DIVISION OF STATE GROUP INSURANCE
INVITATION TO NEGOTIATE
INSURED HEALTH MAINTENANCE ORGANIZATION BENEFITS
and SELF-INSURED HEALTH PLAN SERVICES
ITN NO.: DMS 15/16-005
Replies DUE:
October 23, 2015
Refer ALL Inquiries to:
Maureen Livings, Procurement Officer
Departmental Purchasing
Department of Management Services
4050 Esplanade Way, Suite 335.2Y
Tallahassee, FL 32399-0950

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 2
Table of Contents
Section 1 Introduction .............................................................................................................. 5
1.1 Purpose ......................................................................................................................... 5
1.2 Overview of the Program .............................................................................................. 5
1.3 Questions Being Explored ............................................................................................. 8
1.4 Specific Goals of the ITN ............................................................................................... 8
1.5 Contact Person .............................................................................................................. 9
1.6 Anticipated Contract Term ........................................................................................... 9
1.7 Schedule of Events and Deadlines .............................................................................. 10
1.8 Notice of Intent to Submit a Reply and Non-Disclosure Agreement .......................... 11
Section 2 General Instructions to Vendors ............................................................................. 13
2.1 General Overview ....................................................................................................... 13
2.2 Contacting Department Personnel ............................................................................. 13
2.2.1 Contact Other than During the Negotiation Phase ................................................ 13
2.2.2 Violation of Contact Limitations ............................................................................. 14
2.3 Order of Precedence ................................................................................................... 14
2.4 Vendor Questions ....................................................................................................... 14
2.5 Florida Substitute Form W-9 Process ......................................................................... 15
2.6 MFMP Registration ..................................................................................................... 15
2.7 Special Accommodation ............................................................................................. 15
2.8 Receipt of Replies........................................................................................................ 15
2.8.1 Reply Deadline ........................................................................................................ 15
2.8.2 Changes to Replies after Submission Prohibited .................................................... 16
2.8.3 Receipt Statement .................................................................................................. 16
2.9 Cost of Preparation ..................................................................................................... 16
2.10 Electronic Posting of Department Decisions .............................................................. 16
2.11 Firm Reply ................................................................................................................... 16
2.12 Use of Reply Content .................................................................................................. 17

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 3
2.13 Public Records and Vendor’s Confidential Information ............................................. 17
2.13.1 Public Records ......................................................................................................... 17
2.13.2 Replies are Public Records ...................................................................................... 17
2.13.3 Replies will be Subject to Public Inspection ............................................................ 17
2.13.4 How to Claim Trade Secret or Other Exemptions ................................................... 17
2.13.5 Public Records Request ........................................................................................... 18
2.13.6 Department Not Obligated to Defend Vendor’s Claims ......................................... 18
2.14 General Instructions to Vendors PUR 1001 Form and General Contract Conditions
PUR 1000 ..................................................................................................................... 18
2.15 Section 20.055(5), Florida Statutes ............................................................................. 19
2.16 Subcontracting ............................................................................................................ 19
2.17 Protests ....................................................................................................................... 20
2.17.1 Time Limits for Filing Protests ................................................................................. 20
2.17.2 Bond Must Accompany Protest .............................................................................. 20
2.17.3 Filing a Protest ........................................................................................................ 20
2.18 Department’s Reserved Rights ................................................................................... 21
2.18.1 Waiver of Minor Irregularities ................................................................................ 21
2.18.2 Right to Inspect, Investigate and Rely on Information ........................................... 21
2.18.3 Rejection of All Replies ........................................................................................... 21
2.18.4 Withdrawal of ITN ................................................................................................... 21
2.18.5 Reserved Rights after Notice of Award ................................................................... 22
2.18.6 No Contract until Execution .................................................................................... 22
Section 3 Responding to the ITN ............................................................................................ 23
3.1 Overview ..................................................................................................................... 23
3.2 Submittal of Replies .................................................................................................... 23
3.3 Format of Reply ........................................................................................................... 23
3.4 Draft Contract ............................................................................................................. 26
Section 4 Evaluation and Negotiation Methodology.............................................................. 27
4.1 Selection Criteria ......................................................................................................... 27
4.2 Evaluation and Negotiation Process ........................................................................... 27

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 4
4.2.1 Phase One – Evaluation – General Overview ......................................................... 27
4.2.2 Phase Two – Negotiations – General Overview...................................................... 27
4.3 Evaluation Phase ......................................................................................................... 28
4.3.1 Scoring of Technical Information ............................................................................ 28
4.3.2 Scoring of Financial Replies ..................................................................................... 31
4.4 Negotiation Phase ....................................................................................................... 32
4.4.1 Determination of Vendors Advancing to Negotiations .......................................... 32
4.4.2 Goal of Negotiations ............................................................................................... 32
4.4.3 Vendor Attendance at Negotiations ....................................................................... 32
4.4.4 Revised Replies and Best and Final Offers .............................................................. 33
4.4.5 Other Department Rights during Negotiations ...................................................... 33
4.5 Negotiation Meetings Not Open to Public ................................................................. 34
4.6 Final Selection and Notice of Intent to Award Contract ............................................. 34
4.6.1 Award Selection ...................................................................................................... 34
4.6.2 Department’s Negotiation Team Recommendation .............................................. 34
4.6.3 Secretary of the Department’s Approval ................................................................ 35
4.7 Posting Notice of Intent to Award .............................................................................. 35
Section 5 Minimum Qualifications ......................................................................................... 36
Section 6 Minimum Service Requirements ............................................................................ 40
Section 7 Corporate Information ............................................................................................ 75
Section 8 Vendor and Subcontractor Information ................................................................. 78
Section 9 Technical Information ............................................................................................. 94
Section 10 Service and Program Information ........................................................................... 98
Section 11 Recommended Solutions and Alternatives .......................................................... 105
Section 12 Network Information ............................................................................................ 109
Section 13 Financial Reply ...................................................................................................... 110
Section 14 Purchasing Forms .................................................................................................. 111
Section 15 Attachments .......................................................................................................... 116

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 5
Section 1 Introduction
1.1 Purpose
The Florida Department of Management Services invites interested vendors to submit replies to
this Invitation to Negotiate (“ITN”). The purpose of this ITN is to explore the various questions
identified in this ITN and to determine, through the negotiation process, the preferred set of
solutions to achieve the goals of the ITN.
1.2 Overview of the Program
Pursuant to section 110.123, Florida Statutes, the Department’s Division of State Group
Insurance (“Division”) administers the State Group Insurance Program (“Program”). The
Program is comprised of a package of insurance benefits, including health insurance options,
flexible spending and health savings accounts, life insurance, dental insurance, and other
supplemental insurance products for State of Florida employees and retirees, COBRA
participants, and covered spouses and/or children. Each employee, retiree or COBRA
participant that is the primary insured is an “Enrollee.” Covered spouses and/or children are
“Dependents.” Each individual covered under the Program is a “Member.”
Through the Program, the Department currently offers four (4) medical benefit plan designs
option. Two (2) of these are Preferred Provider Organization (“PPO”) plans, while the other two
(2) plans are either Health Maintenance Organizations (“HMO”) or HMO-style plans.
The PPO options, available statewide, are currently self-funded, with medical benefits
administered by a single third party administrator (“TPA”). The insured HMO and self-insured
HMO-style options are currently provided by six (6) separate HMOs and TPAs, with a mix of fully
insured and self-insured funding arrangements. A single pharmacy benefits manager, currently
CVS/Caremark, administers the pharmacy benefits for all plans with the exception of Medicare
Advantage HMO Enrollees, whose pharmacy benefits are administered by their respective
HMOs.
The PPO options are as follows:
The Standard PPO Plan
The Health Investor PPO Plan (high deductible with a health savings account (“HSA”))
The HMO and HMO-style options are as follows:
The Standard HMO Plan
The Health Investor HMO Plan (high deductible with an HSA)
The benefits to be provided by the successful vendor(s) are described in Attachment H: Covered
Benefits and Services.
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 6
The “Plan Year” runs from January 1 to December 31 of each calendar year. The State provides
two (2) primary enrollment opportunities outside of qualifying status change events: 1) when a
person begins employment with the State, and 2) annually during an open enrollment period.
Open enrollment changes are effective January 1 of the following year. The State’s outsourced
human resource administrator, People First, handles all enrollment activity and its system is the
system of record for eligibility determinations.
Presently, Enrollees are eligible to enroll in any HMO or HMO-style plan with a service area that
includes their home or work address within the state of Florida. Currently a single HMO or TPA
in each county is available to Enrollees within the State, except for six (6) counties (Flagler,
Volusia, St. Lucie, Palm Beach, Broward and Miami-Dade) where two (2) are available to
Enrollees.
Health insurance premiums for active employees are funded primarily through employer
contributions and include a fixed employee payroll deduction. The Department collects
employer and employee contributions from which fully-insured premiums, self-insured claims
costs, and fees are paid. Enrollee and employer contributions are established annually through
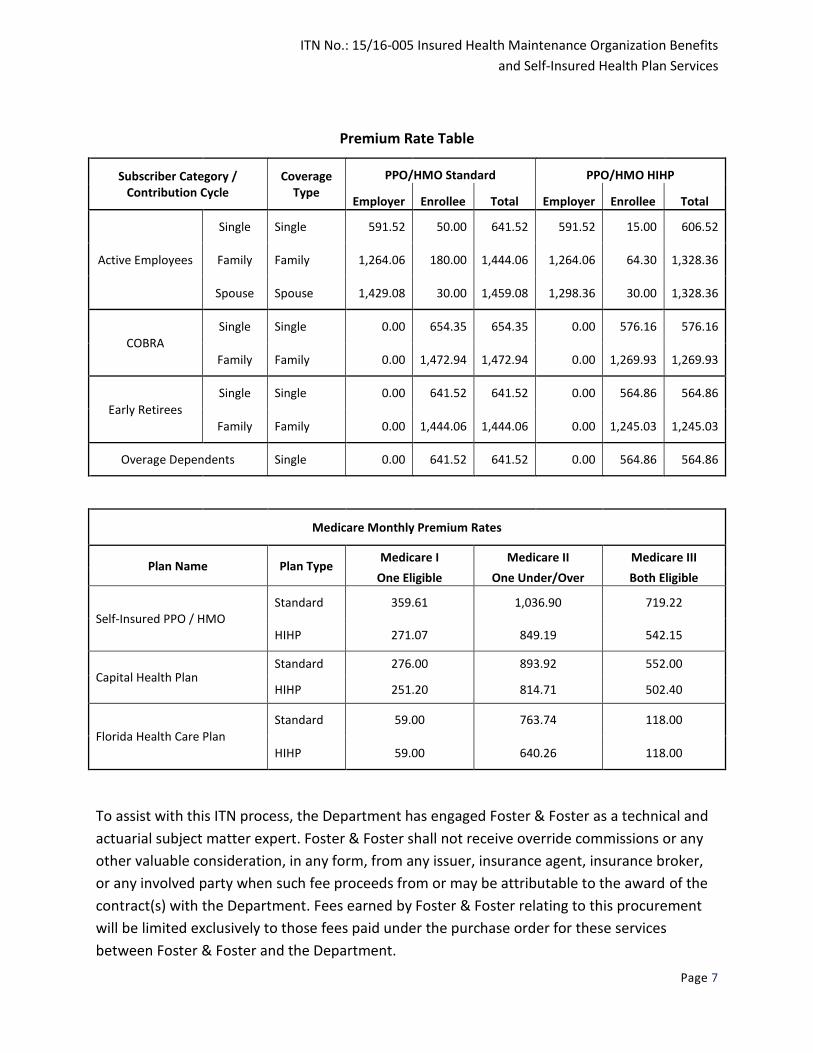
the State’s General Appropriations Act. Currently, Enrollees pay a premium based on coverage
tier (i.e., single or family) and whether they enroll in a Standard Plan or Health Investor Plan.
The employee and employer contributions are the same for all standard plan options and for all
health investor plan options regardless of vendor or plan type (i.e., PPO or HMO). Non-
Medicare eligible retirees pay the full premium; COBRA enrollees pay the full premium plus a
two percent (2%) administrative fee. Contribution amounts and premiums for 2015 are
provided on the following page.
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 7
Premium Rate Table
Subscriber Category /
Contribution Cycle Coverage
Type
PPO/HMO Standard PPO/HMO HIHP
Employer Enrollee Total Employer Enrollee Total
Active Employees
Single Single 591.52 50.00 641.52 591.52 15.00 606.52
Family Family 1,264.06 180.00 1,444.06 1,264.06 64.30 1,328.36
Spouse Spouse 1,429.08 30.00 1,459.08 1,298.36 30.00 1,328.36
COBRA
Single Single 0.00 654.35 654.35 0.00 576.16 576.16
Family Family 0.00 1,472.94 1,472.94 0.00 1,269.93 1,269.93
Early Retirees
Single Single 0.00 641.52 641.52 0.00 564.86 564.86
Family Family 0.00 1,444.06 1,444.06 0.00 1,245.03 1,245.03
Overage Dependents Single 0.00 641.52 641.52 0.00 564.86 564.86
Medicare Monthly Premium Rates
Plan Name Plan Type Medicare I Medicare II Medicare III
One Eligible One Under/Over
Both Eligible
Self-Insured PPO / HMO Standard 359.61 1,036.90 719.22
HIHP 271.07 849.19 542.15
Capital Health Plan
Standard 276.00 893.92 552.00
HIHP 251.20 814.71 502.40
Florida Health Care Plan
Standard 59.00 763.74 118.00
HIHP 59.00 640.26 118.00
To assist with this ITN process, the Department has engaged Foster & Foster as a technical and
actuarial subject matter expert. Foster & Foster shall not receive override commissions or any
other valuable consideration, in any form, from any issuer, insurance agent, insurance broker,
or any involved party when such fee proceeds from or may be attributable to the award of the
contract(s) with the Department. Fees earned by Foster & Foster relating to this procurement
will be limited exclusively to those fees paid under the purchase order for these services
between Foster & Foster and the Department.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 8
1.3 Questions Being Explored
Vendors are not to respond directly to these questions. The Department will use the
information obtained throughout this ITN process to assist it in developing opinions and
positions regarding the following questions:
a. How can the Department most efficiently provide health care benefits to Program
Members?
b. Is a fully-insured program, a self-insured program, or a combination of both in the best
interest of the State?
c. Is a single vendor or multiple vendor platform in the best interest of the State?
d. Should the Department establish a county-by-county program or are there other geographic
distributions that may be in the best interest of the State, and which approach provides the
best value?
e. What levels of network discount guarantees and risk corridor guarantees or medical loss
ratio reimbursements are available to provide the best value?
f. Can the State achieve greater value by carving out or including pharmacy benefits with the
insured HMO benefits provider?
g. Can the State achieve greater value by including an insured Medicare Advantage Plan with
prescription drug coverage with the insured HMO benefits provider?
h. How can the Department ensure pricing remains competitive throughout the entire term of
the contract?
i. How can the Department best ensure flexibility for future program changes (e.g., benefit
design, moving to a defined contribution structure, implementing employee or Member
wellness initiatives)?
j. Can greater value be attained by pricing certain programs separately on a per Member per
month utilization basis (e.g., disease management)?
k. What value propositions can vendors offer that are in the best interest of the State?
l. The remaining questions and issues being explored are provided in sections 6 – 13 .
1.4 Specific Goals of the ITN
a. To establish a contract(s) promoting the cost efficient and prudent administration of the
HMO and HMO-style benefit plans.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 9
b. To establish a flexible contract(s) that provides the ability to effectuate future policy and
program changes. Future changes may include, but are not limited to benefit design,
changing contribution structures, and implementing employee or Member wellness
initiatives.
c. To determine the combination of services, service areas, service levels, and pricing terms
preferred by the Department and that will provide the best overall value in executing
preferred solutions.
d. To ensure continued price competition throughout the initial term and any renewal years of
the contract.
e. To ensure the best value for the State.
1.5 Contact Person
All contact with the Department regarding the ITN shall be directed to the procurement officer
in writing by email only and must contain the ITN number in the subject line of the email. No
facsimiles or telephone calls will be accepted for any reason.
The exclusive point of contact for all communications regarding this ITN is:
Maureen Livings, Procurement Officer
Departmental Purchasing
Department of Management Services
4050 Esplanade Way, Suite 335.2Y
Tallahassee, FL 32399-0950
Email: [email protected]
1.6 Anticipated Contract Term
The Department anticipates that the contract will be entered into by June 1, 2016, allowing the
successful vendor(s) up to seven (7) months to provide transition services before providing
services under the contract resulting from this ITN. The anticipated length of the initial term of
the contract is three (3) years; however, negotiations may lead to a shorter or longer period in
the resulting contract. The contract may be renewed for a period not to exceed three (3) years
or for the term of the original contract, whichever period is longer. Such renewal shall be made
at the Department’s sole discretion and shall be contingent upon satisfactory performance
evaluations as determined by the Department and shall be subject to the availability of funds.
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 10
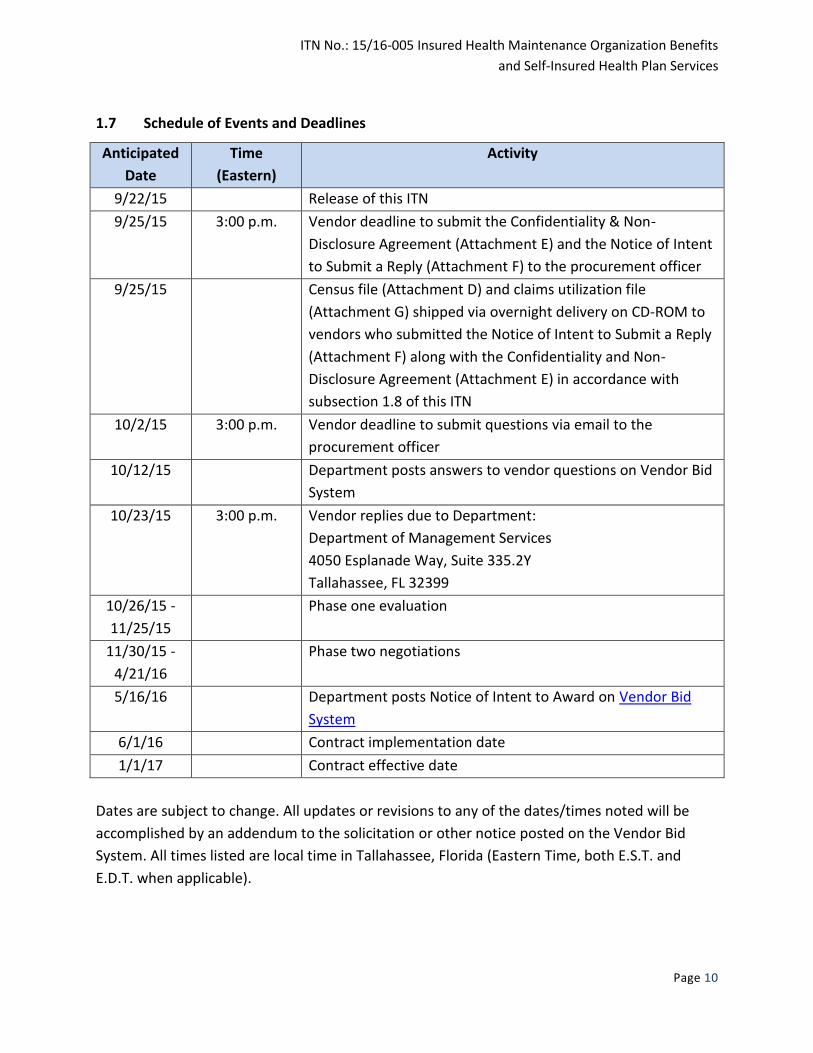
1.7 Schedule of Events and Deadlines
Anticipated
Date
Time
(Eastern)
Activity
9/22/15 Release of this ITN
9/25/15 3:00 p.m. Vendor deadline to submit the Confidentiality & Non-
Disclosure Agreement (Attachment E) and the Notice of Intent
to Submit a Reply (Attachment F) to the procurement officer
9/25/15 Census file (Attachment D) and claims utilization file
(Attachment G) shipped via overnight delivery on CD-ROM to
vendors who submitted the Notice of Intent to Submit a Reply
(Attachment F) along with the Confidentiality and Non-
Disclosure Agreement (Attachment E) in accordance with
subsection 1.8 of this ITN
10/2/15 3:00 p.m. Vendor deadline to submit questions via email to the
procurement officer
10/12/15 Department posts answers to vendor questions on Vendor Bid
System
10/23/15 3:00 p.m. Vendor replies due to Department:
Department of Management Services
4050 Esplanade Way, Suite 335.2Y
Tallahassee, FL 32399
10/26/15 -
11/25/15
Phase one evaluation
11/30/15 -
4/21/16
Phase two negotiations
5/16/16 Department posts Notice of Intent to Award on Vendor Bid
System
6/1/16 Contract implementation date
1/1/17 Contract effective date
Dates are subject to change. All updates or revisions to any of the dates/times noted will be
accomplished by an addendum to the solicitation or other notice posted on the Vendor Bid
System. All times listed are local time in Tallahassee, Florida (Eastern Time, both E.S.T. and
E.D.T. when applicable).

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 11
1.8 Notice of Intent to Submit a Reply and Non-Disclosure Agreement
To be eligible to reply to this ITN, vendors must obtain the claims utilization file (Attachment G)
and the census file (Attachment D) directly from the Department procurement officer. These
files contain certain confidential/HIPAA protected information and data.
To obtain these files and data, vendors must submit a fully completed copy of the
Confidentiality and Non-Disclosure Agreement (Attachment E) and the Notice of Intent to
Submit a Reply (Attachment F) to the procurement officer, by email at
[email protected], by the time and date indicated in subsection 1.7,
Schedule of Events and Deadlines.
Upon receipt of the forms, the Department will send the claims utilization file (Attachment G)
and the census file (Attachment D) on CD-ROM by Federal Express overnight delivery.
The census file (Attachment D) includes the following information for current HMO Enrollees:
Year of birth
Gender
Home ZIP code
Plan name (Standard or HDHP)
Plan coverage tier (Active Single, Active Family, Non-Medicare Single, Non-Medicare
Family, Medicare I, Medicare II or Medicare III)
Number of dependents
The claims utilization file (Attachment G) includes:
System-generated claim number
Patient home county
Total charge amount
DRG code
Primary diagnosis code
Diagnosis code 2
Diagnosis code 3
Diagnosis code 4
Diagnosis code 5
Procedure code
Procedure code modifier
Place of service
Provider Federal Tax ID

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 12
Provider name
Provider specialty
Provider sub-code
Medicare eligibility indicator
Vendors who submitted a Notice of Intent to Submit a Reply (Attachment F) and the
Confidentiality and Non-Disclosure Agreement and received the data included in Attachments D
and G but failed to submit a reply to the ITN shall destroy the confidential information,
including any copies, by the time replies are due and shall provide a certification and complete
access list (page 3 of Attachment E: Confidentiality and Non-Disclosure Agreement) to the
procurement officer that vendor has complied with this requirement on or before the due date
of replies.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 13
Section 2 General Instructions to Vendors
2.1 General Overview
The ITN process is divided into two (2) phases. The evaluation phase involves the Department’s
initial evaluation of replies. During the evaluation phase, all responsive replies will be evaluated
to establish a competitive range of replies reasonably susceptible of award. The Department
will then select one (1) or more vendors within the competitive range with which to commence
negotiations.
The negotiation phase involves negotiations with the vendors. During the negotiation phase,
the Department may request revised replies and/or best and final offers based on the
negotiations. After negotiations, the Department intends to post a notice of intent to award a
contract(s), identifying the responsive and responsible vendor(s) that provides the best value.
Responsive vendors who are not selected for negotiations will not be formally eliminated from
the ITN process until the posting of the notice of intent to award. Final contract terms will be
established with the selected vendor(s) during the negotiation phase.
2.2 Contacting Department Personnel
2.2.1 Contact Other than During the Negotiation Phase
Prospective vendors or persons acting on their behalf may not contact, between the release of
this ITN and the end of the seventy-two (72) hour period (Saturdays, Sundays and State
holidays excluded) following the Department's posting of the notice of intent to award a
contract, any Department personnel or consultants, or any employee or officer of the executive
or legislative branch concerning any aspect of this solicitation, except in writing to the
procurement officer in accordance with subsection 1.5 above or as otherwise provided in this
solicitation. Any such contact by an affiliate, a person with a relevant business relationship with
a prospective vendor, or an existing or prospective subcontractor to a prospective vendor is
assumed to be on behalf of a prospective vendor unless otherwise shown.
During the negotiation phase of this ITN: (i) any contact and communication between the
members of the negotiation team for the prospective vendor(s) with whom the Department is
negotiating and the negotiation team for the Department is permissible, but only "on the
record" (as required by subsection 286.0113(2), Florida Statutes) during the negotiations
meetings; and (ii) communication between the lead negotiator for the prospective vendor with
whom the Department is negotiating and the procurement officer outside of the negotiation
meetings is permissible so long as it is by email only.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 14
2.2.2 Violation of Contact Limitations
Violation of the provisions of subsection 2.2.1 of this ITN may be grounds for rejecting a reply, if
determined by the Department to be material.
2.3 Order of Precedence
In the event of conflict in terms among the foregoing during this ITN, the following order of
precedence shall apply.
Addenda to the ITN, if any
This ITN
All attachments and exhibits to this ITN
The Department’s draft contract
2.4 Vendor Questions
Vendors will submit all questions during the question and answer period in writing to the
procurement officer by email. The deadlines for submission of questions are reflected in
subsection 1.7 of this ITN.
Each vendor’s submission of questions must be clearly labeled with the title of this ITN and the
ITN number.
Questions must be submitted in the following format to be considered:
Vendor
Question
#
Vendor
Name
ITN
Section
ITN Page # Question
Responses to all written questions, and any resulting revisions to the ITN, will be posted
through the Vendor Bid System.
Questions will not constitute formal protest of the specifications or of the ITN.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 15
2.5 Florida Substitute Form W-9 Process
State of Florida vendors must register and complete an electronic Florida Substitute Form W-9.
The Internal Revenue Service (IRS) receives and validates the information vendors provide on
the Form W-9. For instructions on how to complete the Florida Substitute Form W-9, please
visit: http://www.myfloridacfo.com/Division/AA/StateAgencies/W-9Instructions022212.pdf.
The awarded vendor(s) if any must have completed this process prior to contract execution.
This form is not required to be submitted with the reply to the ITN.
2.6 MFMP Registration
The awarded vendor(s) providing self-insured health plan services shall pay the required MFMP
transaction fee(s) as specified by statute, unless an exemption has been requested and
approved prior to the award of the contract pursuant to Rule 60A-1.032 of the Florida
Administrative Code.
The awarded vendor(s), if any, must have completed this process prior to contract execution.
For additional information, please visit: https://vendor.myfloridamarketplace.com/.
2.7 Special Accommodation
Any person requiring a special accommodation because of a disability should call Departmental
Purchasing at (850) 488-1308 at least five (5) business days prior to the scheduled event.
Persons with hearing or speech impairments should call Departmental Purchasing by using the
Florida Relay Service at (800) 955-8771 (TDD).
2.8 Receipt of Replies
2.8.1 Reply Deadline
Replies must be received by the Department no later than the date and time provided in
subsection 1.7 of this ITN and addressed to the procurement officer at:
Department of Management Services
4050 Esplanade Way, Suite 335.2Y
Tallahassee, FL 32399
All methods of delivery or transmittal to the procurement officer are exclusively the
responsibility of vendors and the risk of non-receipt or delayed receipt shall be borne
exclusively by the vendors.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 16
2.8.2 Changes to Replies after Submission Prohibited
During the evaluation phase, no changes, modifications, or additions to the reply will be
allowed after the replies have been opened. However, the Department reserves the right to
seek clarifications or additional information.
2.8.3 Receipt Statement
Replies not received at the specified address by the deadline will be rejected, remain unopened
and retained for use in the event of a dispute. After the contract award, the Department will
return the originals to the vendor.
2.9 Cost of Preparation
Neither the Department nor the State is liable for any costs incurred by a vendor in responding
to this ITN.
2.10 Electronic Posting of Department Decisions
On the dates indicated on the Schedule of Events and Deadlines in subsection 1.7, as amended
or updated, the Department shall electronically post a notice of the Department’s decisions at
the following Vendor Bid System website: http://vbs.dms.state.fl.us/vbs/main_menu.
IT IS THE SOLE RESPONSIBILITY OF VENDORS TO CHECK THE VENDOR BID SYSTEM FOR
INFORMATION AND UPDATES.
2.11 Firm Reply
The Department may make an award within two-hundred-forty (240) calendar days after the
date the final replies are due. By submitting a reply, vendors acknowledge and agree that their
replies shall remain firm for (and shall not be withdrawn) for at least two-hundred-forty (240)
calendar days after the final replies have been submitted. If an award is not made within the
two-hundred-forty (240) day period, the final reply shall remain firm until either the
Department awards the contract or the Department receives from the vendor written notice
that the reply is withdrawn.
Vendors may request to withdraw replies within seventy-two (72) hours (excluding state
holidays, Saturdays and Sundays) after the due date for replies provided in the Schedule of
Events and Deadlines, subsection 1.7 of this ITN. Requests received in accordance with this
provision may be granted by the Department upon proof of the impossibility to perform based
upon an obvious error as determined solely by the Department.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 17
2.12 Use of Reply Content
All materials produced to the Department through this ITN become the exclusive property of
the Department and may not be removed by vendors. Further, all replies become the property
of the Department and will not be returned to the vendor. The Department will have the right
to use any or all ideas or adaptations of the ideas presented in the reply. Selection or rejection
of a reply of award will not affect this right.
2.13 Public Records and Vendor’s Confidential Information
2.13.1 Public Records
All electronic and written communications pertaining to this ITN, whether sent from or received
by the Department, are subject to Florida’s public records law, chapter 119, Florida Statutes.
Subsection 2.13.4 below addresses the submission of trade secret and other information
exempted from public inspection.
2.13.2 Replies are Public Records
All materials submitted in reply to this ITN will be a public record subject to the provisions of
chapter 119, Florida Statutes. Selection or rejection of a reply does not affect the public record
status of the materials.
2.13.3 Replies will be Subject to Public Inspection
Unless exempted by law, all public records are subject to public inspection and copying under
Florida’s public records law, chapter 119, Florida Statutes. A time-limited exemption from
public inspection is provided for the contents of replies pursuant to subsection 119.071(1)(b),
Florida Statutes. Once that exemption expires, all contents of replies become subject to public
inspection unless another exemption applies. Any claim of trade secret exemption for any
information contained in vendor’s reply to this solicitation will be waived upon submission of
the reply to the Department, unless the claimed trade secret information is submitted in
accordance with subsection 2.13.4. This waiver includes any information included in the
vendor’s reply outside of the separately bound document described below.
2.13.4 How to Claim Trade Secret or Other Exemptions
If a vendor considers any portion of the documents, data, or records submitted in its reply to be
trade secret or otherwise exempt from public inspection or disclosure pursuant to Florida’s
Public Records Law, the vendor must submit all such information as a separately bound,
unredacted document clearly labeled “Attachment to Invitation to Negotiate, Number
DMS 15/16-005—Exempt Material,” together with a brief written description of the grounds for

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 18
claiming exemption from the public records law, including the specific statutory citation for
such exemption.
Vendor must also simultaneously provide the Department with a separate, electronic redacted
copy of its reply. The file name of the electronic redacted copy shall contain the name of
vendor, the ITN number, and redacted copy (e.g., Vendor Name_DMS ITN 15/16-005_redacted
copy.pdf). The first page of the electronic redacted copy and each page on which information is
redacted shall prominently display the phrase “Redacted Copy.”
This submission must be made no later than the reply submittal deadline. Where such
information is part of material already required to be submitted as a separately bound or
enclosed portion of the reply, it shall be further segregated and separately bound or enclosed
and clearly labeled as set forth above in addition to any other labeling required for the material.
2.13.5 Public Records Request
If a vendor fails to mark any materials submitted to the Department as exempt and failed to
submit a redacted copy as provided in this section, the vendor waives the exemption, and the
Department will produce all of vendor’s documents, data or records to any person requesting a
copy under chapter 119, Florida Statutes. The vendor exclusively bears the burden of complying
with subsection 2.13.4 to ensure its exempt information is appropriately marked.
2.13.6 Department Not Obligated to Defend Vendor’s Claims
The Department is not obligated to agree with a vendor’s claim of exemption and, by
submitting a reply, the vendor agrees to defend its claim that each and every portion of the
redactions is exempt from inspection and copying under Florida’s Public Records Law. Further,
by submitting a reply, the vendor agrees to protect, defend, indemnify and hold harmless the
Department for any and all claims and litigation (including litigation initiated by the
Department), including attorney’s fees and costs, arising from or in any way relating to vendor’s
assertion that the redacted portions of its reply are trade secrets or otherwise exempt from
public disclosure under chapter 119, Florida Statutes.
2.14 General Instructions to Vendors PUR 1001 Form and General Contract Conditions PUR 1000
The Florida Administrative Code requires that the Department include the standard PUR 1001
Form “General Instructions to Vendors” and the PUR 1000 “General Contract Conditions” with
this solicitation. The PUR 1001 and the PUR 1000 forms can be found at:
http://www.dms.myflorida.com/business_operations/state_purchasing/documents_forms_ref
erences_resources/purchasing_forms.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 19
The Department is permitted by the Florida Administrative Code, however, to override the
provisions of both forms. Accordingly, the terms and conditions of PUR 1001 FORM do not
apply to this solicitation and are instead modified and superseded by the instructions,
specifications, and other terms contained throughout this ITN. The terms and conditions of PUR
1000 do not apply to this solicitation and are instead modified and superseded by the draft
contract included as Attachment A to this ITN.
2.15 Section 20.055(5), Florida Statutes
Vendor and any subcontractor understand and will comply with subsection 20.055(5), Florida
Statutes, which places a legal duty on the vendor and any subcontractor to cooperate with the
inspector general in any investigation, audit, inspection, review, or hearing.
2.16 Subcontracting
The successful vendor(s) is fully responsible for all work performed under the resultant contract
of this solicitation. If vendor intends to use any subcontractors to perform the work, such
subcontractors shall be identified as required by ITN section 8. If a vendor should need to
replace a subcontractor prior to the Department’s notice of intent to award, the vendor shall
provide to the procurement officer a request to substitute the subcontractor, explaining why
the vendor seeks to substitute the subcontractor. The substitution will be subject to
Department approval.
The successful vendor(s) acknowledges that it will not be released of its contractual obligation
to the Department because of any subcontract. The Department may treat vendor’s use of a
subcontractor not disclosed during the ITN process or approved by the Department as a breach
of contract.
Health care providers are not considered subcontractors. Rented networks are also not
considered subcontractors and the successful vendor(s) using rented networks will not be
excused from performance should the rented network become unavailable to the vendor at any
time.
Any processes, services, and deliverables that are subcontracted or provided by a subsidiary or
third party (e.g., via a rental network), including but not limited to, the provider network,
clinical management, customer service, disease management vendors, printing services, and so
forth, shall be managed through vendor and be seamless and transparent to both the members
and the Department.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 20
2.17 Protests
Section 120.57, Florida Statutes, applies to this solicitation, as modified by subsection
110.123(3)(d)4, Florida Statutes.
2.17.1 Time Limits for Filing Protests
Any person whose substantial interests are adversely affected by the decision or intended
decision made by the Department pursuant to this solicitation shall file with the Department a
formal written protest petition in writing within seventy-two (72) hours after the posting of
the Department’s notice of decision or intended decision in accordance with subsection
110.123(3)(d)4, Florida Statutes.
2.17.2 Bond Must Accompany Protest
When protesting a decision or intended decision (including a protest of the terms, conditions,
and specifications of the solicitation), the protestor must post a bond equal to one percent (1%)
of the Department’s estimated contract amount. The estimated contract amount for any
protest of this procurement is $310,000,000.
The estimated contract amount is not subject to protest. The bond must be conditioned upon
the payment of all costs and charges that are adjudged against the protestor in the
administrative hearing in which action is brought and in any subsequent appellate court
proceeding. In lieu of a bond, the Department will accept a cashier’s check, official bank check,
or money order. An original cashier’s check, official bank check, or money order must be posted
in the same fashion as a protest bond.
FAILURE TO POST AN ORIGINAL BOND OR OTHER SECURITY REQUIRED BY LAW AT THE TIME
OF FILING THE FORMAL WRITTEN PROTEST WILL RESULT IN A REJECTION OF THE PROTEST.
2.17.3 Filing a Protest
A formal written protest is “filed” when actually received by the procurement officer listed in
subsection 1.5 or by the Department’s agency clerk. Filing of a formal written protest may be
achieved by hand-delivery, courier, mail, facsimile, or email. Actual delivery by the deadline
shall remain the sole responsibility of the protestor, and the risk of non-receipt or delayed
receipt shall be borne exclusively by the protestor.
A protest bond must be posted together with the formal written protest. A protest bond is
“posted” when the original bond is physically tendered to the procurement officer or agency
clerk. Bonds (and cashier’s checks, official bank checks, or money orders) cannot be posted by
facsimile, email, or other transmission that does not result in the original being physically
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 21
tendered to the Department. Actual posting of a bond by the deadline shall remain the sole
responsibility of the protestor, and the risk of non-receipt or delayed receipt shall be borne
exclusively by the protestor.
FAILURE TO FILE A PROTEST WITHIN THE TIME PRESCRIBED IN SUBSECTION 120.57(3),
FLORIDA STATUTES (as altered by subsection 110.123(3)(d)4, OR FAILURE TO POST THE BOND
OR OTHER SECURITY REQUIRED BY LAW WITHIN THE TIME ALLOWED FOR FILING A BOND
SHALL CONSTITUTE A WAIVER OF PROCEEDINGS UNDER CHAPTER 120, FLORIDA STATUTES.
2.18 Department’s Reserved Rights
2.18.1 Waiver of Minor Irregularities
The Department reserves the right to waive minor irregularities when to do so would be in the
best interest of the State of Florida. A minor irregularity is a variation from the terms and
conditions of this ITN that does not affect the price of the reply or give the vendor a substantial
advantage over other vendors and thereby restrict or stifle competition and does not adversely
impact the interests of the Department. At its option, the Department may allow a vendor to
correct minor irregularities but is under no obligation to do so. In doing so, the Department
may request a vendor to provide clarifying information or additional materials to correct the
irregularity. However, the Department will not request and a vendor may not provide the
Department with additional materials that affect the price of the reply, or give the vendor an
advantage or benefit not enjoyed by other vendors.
2.18.2 Right to Inspect, Investigate and Rely on Information
The Department reserves the right to inspect vendor’s facilities and operations, to investigate
any vendor representations and to rely on information about a vendor in the Department’s
records or known to its personnel in making its best value determination.
2.18.3 Rejection of All Replies
The Department reserves the right to reject all replies at any time, including after an award is
made, when to do so would be in the best interest of the state of Florida, and by doing so the
Department will have no liability to any vendor.
2.18.4 Withdrawal of ITN
The Department reserves the right to withdraw the ITN at any time, including after an award is
made, when to do so would be in the best interest of the state of Florida, and by doing so the
Department will have no liability to any vendor.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 22
2.18.5 Reserved Rights after Notice of Award
The Department reserves the right, after posting notice thereof, to withdraw or amend its
notice of intent to award and re-open negotiations with any vendor at any time prior to
execution of a contract.
2.18.6 No Contract until Execution
A notice of intent to award under this ITN shall not constitute or form any contract between the
Department and a vendor. No contract shall be formed until such time as a vendor and the
Department formally execute a contract with requisite written signatures.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 23
Section 3 Responding to the ITN
3.1 Overview
Replies should provide a straightforward, concise description of the vendor’s ability to provide
the solution sought by the solicitation. Excessive information distracts readers from focusing on
essentials. Properly referenced replies may be in the form of informational materials and
brochures, but must be specific to the issue raised or question asked. When responding to
specific questions, vendors must reprint each question in its entirety in the reply.
The vendor’s reply may not apply any conditions or exceptions to any mandatory requirements
of the solicitation.
The reply text must be at least 11 pt Calibri, Arial or Times New Roman in legible font.
3.2 Submittal of Replies
Each vendor is responsible for ensuring that its reply is delivered at the proper time and to the
proper place. REPLIES MUST BE RECEIVED AT OR BEFORE THE TIME AND DATE reflected on the
schedule included in subsection 1.7 (“Schedule of Events and Deadlines”) of this ITN. The
Department will reject replies received after this deadline.
Each submission must be in a sealed box(es) and addressed to the attention of the
procurement officer and indicate the Departmental Purchasing address, the ITN number, and
date and time the reply is submitted. Any submitted documents claimed to be exempt from
Florida’s Public Records Law must comply with the provisions of subsection 2.13.4 (“How to
Claim Protection for Exempt Materials”) at the time of the reply submission.
The reply must be submitted in a properly marked, sealed box(es) containing the following:
a. One (1) original unredacted and 10 (ten) separate unredacted, bound paper copies;
b. Ten (10) electronic copies on ten (10) separate CD-ROMs or “thumb drives”; and
c. One (1) electronic redacted copy of entire reply on CD-ROM or “thumb drive” (if applicable,
as described in subsection 2.13.4 (“How to Claim Protection for Exempt Materials”) of this
ITN).
3.3 Format of Reply
THE VENDORS MUST SUBMIT REPLIES IN THE FOLLOWING FORMAT AND ORDER IN
ACCORDANCE WITH THE INSTRUCTIONS PROVIDED IN EACH CORRESPONDING SECTION OF
THIS ITN. EACH REPLY MUST BE TABBED AS FOLLOWS:

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 24
TAB 1: Transmittal Letter
The purpose of this letter is to transmit the reply and acknowledge the receipt of any addenda.
The transmittal letter should be brief and signed by an individual who is authorized to commit
the vendor to the services and requirements as stated in this ITN. The transmittal letter must
also include the name and contact information for the vendor’s primary contact person for this
solicitation. The transmittal letter must not exceed one (1) page.
TAB 2: Title Page and Table of Contents
The title page should bear the name and address of vendor and the name and number of this
ITN. This should be followed by a table of contents for the entire reply.
TAB 3: Exempt Information
A listing of information that is declared proprietary, trade secret or confidential and claimed to
be exempt from public disclosure is to be provided immediately following the table of contents.
This listing must identify each section of the reply that has been marked as exempt and
excluded from the redacted copy provided with the reply as described in subsection 2.13
(“Public Records and Vendor’s Confidential Information”) of this ITN.
TAB 4: Executive Summary
Vendor must condense and highlight the contents of the reply to the ITN in a separate, section
titled “Executive Summary” including a general description of how the vendor intends to offer
the services sought by this ITN.
TAB 5: Minimum Qualifications (ITN Section 5)
Vendors must provide a response to each of the minimum qualifications identified in section 5
of this ITN. A response of “No” or failure to submit a response to any of the minimum
qualifications in section 5 of this ITN will disqualify the vendor from further consideration.
TAB 6: Minimum Service Requirements (ITN Section 6)
Vendors must provide a response acknowledging the ability and agreement to provide the
minimum service requirements as required in section 6 of this ITN. A response of “No” or
failure to submit a response to section 6 of this ITN will disqualify the vendor from further
consideration.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 25
TAB 7: Corporate Information (ITN Section 7)
Vendors must provide responses to the questions and requests for information in section 7
(“Corporate Information”) of this ITN. Failure to provide a response to any item in section 7
may disqualify the vendor from further consideration.
TAB 8: Vendor and Subcontractor Information (ITN Section 8)
Vendors must provide a response to each requested item in section 8 (“Vendor and
Subcontractor Information”) of this ITN. Additional tables may be added by the vendor as
needed for the response to any item in section 8.
TAB 9: Technical Information (ITN Section 9)
Vendors must respond to each question and request for information in section 9 of this ITN.
Vendors must restate each item and provide a response to the item in at least 11 pt Calibri,
Arial or Times New Roman, blue font. Vendors must respond to all parts of each question or
request for information. Failure to submit a response to a question or request for information
may disqualify the vendor from further consideration. See subsection 4.3.1 (“Scoring of
Technical Information”) of this ITN for scoring. Tab 9 must be limited to fifty (50) singled sided
or twenty-five (25) double sided pages in font indicated above.
TAB 10: Service and Program Information (ITN Section 10)
Vendors must provide a response to each requested item in section 10 of this ITN. Failure to
provide a response to any item in section 10 may disqualify the vendor from further
consideration.
TAB 11: Recommended Solutions and Alternatives (ITN Section 11)
Vendors must provide a response to each requested item in section 11 of this ITN.
TAB 12: Network Information (ITN Section 12)
Vendors must complete and submit Attachment B: Network Information as instructed in
section 12 of this ITN. Failure to provide a GeoAccess® and disruption analysis using an intact
workbook with complete information for any item in Attachment B may disqualify the vendor
from further consideration.
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 26
TAB 13: Financial Reply (ITN Section 13)
Vendors must provide a financial reply by completing and submitting the Microsoft Excel
document labeled Attachment C: Financial Reply.
Vendors must complete the financial reply according to the instructions in Attachment C.
Vendors must submit the final electronic version (on CD-ROM or thumb drive) of the financial
reply in original file format (Excel .xls) with the Excel workbook intact (see subsection 4.3.2 for
scoring information). Vendors may not add additional tabs to the workbook or break apart the
tabs of the workbook and submit as separate attachments. Failure to provide a financial reply
using an intact workbook with complete pricing information for any item in Attachment C will
disqualify the vendor from further consideration.
TAB 14: Purchasing Forms (ITN Section 14).
Vendors must complete and submit the following forms listed below in the following order
displayed:
a. Form 1 – Vendor Certification
b. Form 2 – Notice of Conflict of Interest
c. Attachment E: Confidentiality and Non-Disclosure Agreement Page 3, “Vendor’s Employees
Who Will Be Given Access to the Confidential Information” Note: this form is required even
if there are no updates from the initial submittal.
3.4 Draft Contract
Attachment A is the Department’s draft contract. Any attempts to red-line or modify the terms
of the Department’s draft contract will be disregarded and ignored by the Department during
the evaluation phase. Therefore, vendors should not make alterations or edits to the
Department’s draft contract. (The Department may negotiate and consider red-line edits or
modification during the negotiation phase.)
The draft contract contains the following documents as attachments. These attachments do not
need to be returned with the ITN reply.
a. Affidavit of Best Pricing
b. Affidavit of Warranty of Security
c. Affidavit of No Offshoring
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 27
Section 4 Evaluation and Negotiation Methodology
The Department intends to award a contract(s) to the responsible and responsive vendor(s)
that presents the best value. The Department may award multiple contracts.
4.1 Selection Criteria
The following award selection criteria shall apply for this ITN:
Criteria
Vendor’s articulation of its approach and solution; and the ability of the
approach and solution to meet the Department’s needs, the requirements
of this ITN, and ITN sections 6 through 13.
The vendor’s approach and solution and any value enhancements at no
additional cost to the State.
Vendor references, track record implementing similar solutions to the one
specified in this ITN, and overall experience.
Vendor’s pricing, overall costs to the Department, and financial guarantees.
4.2 Evaluation and Negotiation Process
4.2.1 Phase One – Evaluation – General Overview
The Department will appoint an evaluation team for the initial evaluation and scoring of the
replies for the evaluation phase (phase one). Each evaluator will be provided a copy of each
vendor’s reply. Foster & Foster will independently review Attachment B: Network Information
and Attachment C: Financial Reply and will provide the Department with a summary of these
replies.
The Department will score replies consistent with subsection 4.3 below.
4.2.2 Phase Two – Negotiations – General Overview
The Department will establish a negotiation team to conduct the negotiations, assess the final
value proposition of each vendor, and make an award recommendation to the Department. The
negotiation team will not be bound by phase one scoring and has full authority to reassess any
of the phase one evaluation determinations and may consider any additional information that

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 28
comes to its attention during the negotiations phase. The negotiation team will not engage in
any scoring.
Vendors may be provided an opportunity to recommend enhanced value alternatives, offer
alternative solutions and deliverables, provide additional information, and other options during
the negotiation phase that would present the best value to the State. The Department reserves
the right to negotiate different terms and related price adjustments if the Department
determines that such changes would provide the best value to the State. The negotiation team
may address proposed alternative terms or deliverables during negotiations but it is under no
obligation to accept proposed alternative terms or deliverables. If the negotiation team
determines that a proposed alternative is not acceptable and the vendor fails to offer another
alternative that is acceptable to the negotiation team, the vendor may be removed from
further consideration.
4.3 Evaluation Phase
The Department’s initial evaluation of replies will determine which vendors are considered to
fall within the competitive range of vendors reasonably susceptible of award and eligible for
inclusion in the negotiation phase (phase two). All replies that meet the pass/fail requirements
in section 5: Minimum Qualifications and are determined to be otherwise responsive will be
evaluated using the following process:
The evaluation phase (phase one) begins with the scoring of technical replies based on the
methodology described in subsection 4.3.1. Technical Information will be allocated a maximum
of 350 points. Financial Replies will be allocated a maximum of 650 points.
The maximum points any vendor can achieve is 1,000 points.
4.3.1 Scoring of Technical Information
The technical information sections count as thirty-five percent (35%) of the overall score and
are comprised of the following ITN sections: section 9: Technical Information and section 12:
Network Information. The scoring analysis will be conducted for each county for which a vendor
submits a reply.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 29
Scoring of Section 9 (Technical Information)
Evaluators will score section 9: Technical Information, worth a total of eighty (80) points. Each
vendor response to the eight (8) questions will be scored and may earn a maximum of five (5)
points. After the responses have been scored on the five (5) point scale, the scores will be
multiplied by two (2) for a maximum possible score of eighty (80) points. For example:
Vendor A receives a total score of thirty-five (35) points based on the five (5) point scale.
Vendor A will earn seventy (70) points for section 9.
The five point scale that will evaluators will use is below.
SCORING SCALE
5 = Superior. The response exhaustively addresses the question and demonstrates vendor has
extraordinary experience in performing the required services related to the question. The
response indicates vendor would provide exceptionally enhanced value to the State and/or to
Members. The response demonstrates the ability of the vendor to exceed the State’s
requirement, provide outstanding quality of service levels, provide cost savings or cost
avoidance to the State, and/or implement innovative ideas.
4 = Good. The response extensively addresses the question and demonstrates exceptional
experience in performing the required services related to the question. The response indicates
vendor would provide enhanced value to the State and/or to Members.
3 = Adequate. The response adequately addresses the question and demonstrates vendor has
sufficient experience in performing the required services related to the question.
2 = Poor. The response minimally addresses the question or demonstrates vendor has nominal
experience in performing the required services related to the question.
1 = Unsatisfactory. The response inadequately addresses the question or demonstrates vendor
has very limited experience in performing the required services related to the question.
0 = Inadequate. The response is blank, does not address the question, or demonstrates vendor
has no experience in performing the required services related to the question.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 30
Scoring of Section 12 (Network Information)
The GeoAccess® reports and provider disruption reports will be scored based on responses to
Attachments B-1 through B-7.
The four (4) provider categories of the GeoAccess® reports (Attachments B-1 through B-4) will
be scored separately from the disruption reports (Attachments B-5 through B-7). Attachments
B-1 through B-4 each are eligible for thirty-three and three-quarters (33.75) points.
For the GeoAccess® reports, in each county the vendor with the highest percentage of
employees meeting the access criteria in each of the four (4) provider categories will earn the
full thirty-three and three-quarters (33.75) points for that category. All other vendors in that
county will earn points in proportion to the ratio of their percentage of employees meeting the
access criteria to the highest percentage in the county. For example, if there are two (2)
vendors for a certain county:
Vendor A’s network Adult Primary Care Physician (PCP) access score is one hundred percent
(100%) of employees.
Vendor B’s network Adult PCP access score is ninety-two percent (92%) of employees.
Vendor A will earn thirty-three and three-quarters (33.75) points for the Adult PCP category
as the highest percentage of the vendors in that county.
Vendor B will earn thirty-one and five-hundredths (31.05) points for the Adult PCP category,
based on the following formula:
Similarly, for the provider disruption reports (Attachment B-5 through B-7), the vendor with the
highest percentage of utilized providers considered in-network in each of the three (3)
categories (Attachment B-5 through B-7) will earn the full forty-five (45) points for each county.
Each vendor’s provider disruption score below the highest scoring vendor’s score will earn
proportional points. For example, if there are only two (2) vendors for a certain county:
Vendor A’s network matches one-hundred percent (100%) of facilities.
Vendor B’s network matches ninety percent (90%) of facilities.
Vendor A will earn forty-five (45) points for the facilities category as the highest percentage
of the vendors in that county.
Vendor B will earn forty and one-half (40.5) points for the facilities category, based on the
following formula:

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 31
The maximum possible points for a technical reply in each county is 350.
Scored Questions 80
GeoAccess® 135
Disruption 135
Total 350
4.3.2 Scoring of Financial Replies
The financial reply will count as sixty-five percent (65%) of the overall score and will be
evaluated based on responses for at least one of the two (2) funding scenarios in Attachments
C-5 and C-6, with a maximum score of six-hundred fifty (650) points for each county. The two
(2) funding scenarios are as follows:
a. Self-insured health plan services for medical benefits without prescription drug benefits.
b. Fully-insured medical benefits without prescription drug benefits.
For counties included in the vendor’s reply, vendors must submit a reply by county under a self-
insured funding scenario or a fully-insured funding scenario, or they may submit replies for both
scenarios.
Responses under the self-insured scenario will be evaluated based on the projected monthly
expense per Enrollee, utilizing the re-priced claims by county and the proposed monthly
administrative fee per Enrollee. If vendor provides a tiered administrative fee based on the
number of covered Enrollees, the fee used to determine the score for each county will be
determined using the number of non-PPO Enrollees in that county as of July 2015. The re-priced
medical claims will be projected to the proposed contract period utilizing trend rates of seven
percent (7%) per year for medical claims.
Responses under the fully-insured scenario will be evaluated based on the projected monthly
expense per Enrollee, utilizing the premium provided for each county.
The vendor with the lowest projected monthly expense per Enrollee for the proposed contract
period for each county, regardless of the funding scenario, will be awarded the full six-hundred
fifty (650) points for that county. The remaining vendors in that county will earn points in
proportion to the ratio of the lowest projected expense to their reply’s projected expense. For
example, if there are only two (2) vendors for a certain county:
Vendor A has a projected monthly expense per employee of $500

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 32
Vendor B has a projected monthly expense per employee of $520
Vendor A will earn six-hundred fifty (650) points for that county as the lowest monthly cost
per employee
Vendor B will earn six-hundred twenty-five (625) points, based on the following formula:
4.4 Negotiation Phase
4.4.1 Determination of Vendors Advancing to Negotiations
The Department intends to select no fewer than two (2) vendors using the Phase One scoring
specified above with whom to conduct negotiations.
Although the Department intends to negotiate with at least two (2) vendors, it reserves the
right to select more or fewer vendors with whom to negotiate.
No presumption of preference or merit in the negotiation process or for contract award shall
arise from the scores awarded during the evaluation phase and such scores shall not carry over
to the negotiation phase.
The Department will establish a negotiation team to conduct negotiations and make award
recommendations. The negotiation team will use the Selection Criteria to determine best value;
however, the negotiation team is not bound by the phase one scoring and will have full
authority to reassess any evaluation phase determinations and may consider all information
that comes to its attention during the negotiations.
The Department may negotiate sequentially or concurrently (or a combination of both) and
may at any time during the negotiation phase eliminate a vendor from further consideration.
Additionally, the Department reserves the right to conclude negotiations at any time and
proceed to contract award.
4.4.2 Goal of Negotiations
The negotiation process is intended to enable the Department to determine which vendor(s)
presents the best value and to establish the principle terms and conditions of such contract.
4.4.3 Vendor Attendance at Negotiations
The Department reserves the right to require attendance at negotiation sessions by particular
representatives of the vendor. At a minimum, the Department expects that the following
representatives will be in attendance: the account manager, the implementation manager, the

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 33
executive sponsor and any other individuals who will perform a critical role in the day-to-day
management of the contract. The vendor should limit its negotiation team to six (6) individuals.
Any written summary of presentations or demonstrations provided by vendors during negotiations
shall include a list of attendees, a copy of the agenda, and copies of any visuals or handouts, all of
which shall become part of the vendor(s) reply. Failure to provide any information requested by the
Department during the Negotiation Phase may result in termination of negotiations with the
vendor.
4.4.4 Revised Replies and Best and Final Offers
During the negotiation phase, the Department will request clarification and revisions to replies
(including best and final offers) until it is satisfied that it has achieved the best value for the
State.
4.4.5 Other Department Rights during Negotiations
The Department reserves the right at any time during the negotiation process to:
a. Schedule additional negotiating sessions with any or all vendors.
b. Require any or all vendors to provide additional, revised, or final written replies addressing
specified topics.
c. Require any or all vendors to provide written best and final offer(s).
d. Require any or all responsive vendors to address services, prices, or conditions offered by
any other vendor.
e. Pursue a contract with one (1) or more responsive vendors for the services encompassed by
this ITN, any addenda thereto, and any request for additional, revised, or final written
replies or request for best and final offers.
f. Award contracts to responsive vendors by type of service or geographic area, or both.
Geographic areas may be county-by-county, any combination of two (2) or more counties,
statewide, or as otherwise determined by the negotiation team to be in the best interests of
the State in providing best value.
g. Arrive at an agreement with any responsive vendors(s), finalize principal contract terms
with such vendor and terminate negotiations with any or all other vendors, regardless of
the status of or scheduled negotiations with such other vendors.
h. Decline to conduct further negotiations with any vendor.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 34
i. Re-open negotiations with any vendor.
j. Take any additional administrative steps deemed necessary in determining the contract
award, including additional fact-finding, evaluation, or negotiation where necessary and
consistent with the terms of this solicitation.
k. Review and rely on relevant information contained in the replies or other information
gathered by the Department regardless of source.
The Department has sole discretion in deciding whether and when to take any of the foregoing
actions, the scope and manner of such actions, the vendor(s) affected, and whether to provide
concurrent public notice of such decision.
4.5 Negotiation Meetings Not Open to Public
Negotiations between the Department and vendors are temporarily exempted from chapter
286, Florida Statutes.
Negotiation team strategy meetings are exempted by subsection 286.0113(2)(a), Florida
Statutes.
The Department will record all meetings of the negotiation team, as required by law, and such
recordings will eventually become public record pursuant to chapter 286, Florida Statutes.
During negotiations, vendors must inform the Department if any portion of the meetings
should be considered exempt because of discussions of trade secrets so that the Department
can make appropriate arrangements for the segregation of the recording.
4.6 Final Selection and Notice of Intent to Award Contract
4.6.1 Award Selection
The Department will select for award the responsive and responsible vendor(s) that provides
the best value to the State based on the Selection Criteria in subsection 4.1.
The Department reserves the right to make a single or multiple awards or to make no awards
at all.
4.6.2 Department’s Negotiation Team Recommendation
The Department’s negotiation team will develop a recommendation as to the award that will
provide the best value. In so doing, the negotiation team will not engage in scoring, but will
arrive at its recommendation by majority vote.
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 35
The scores from the evaluation phase will not carry over into the negotiation phase, and the
negotiation team will not be bound by those scores. The negotiation team will forward its
recommendation to the Secretary of the Department or his designee for review.
4.6.3 Secretary of the Department’s Approval
The Secretary of the Department or his designee will make the final decision to approve or
reject the recommendations of the negotiation team.
4.7 Posting Notice of Intent to Award
If the Department decides to award a contract(s), it will post a notice of intent to award
contract, stating its intent to enter into one or more contracts with vendor(s) identified therein,
on the Vendor Bid System website: http://vbs.dms.state.fl.us/vbs/main_menu. If the
Department decides to reject all replies, it will post its notice at the same Vendor Bid System
website.
Vendor shall destroy the confidential information, including any copies, remaining in its
possession within the later of five (5) business days of the State’s notice of intent to award in
connection with this ITN or the conclusion of any legal proceedings or protest regarding the
procurement and shall provide a certification and a final access list to the procurement officer
as defined in the ITN that it has complied with this requirement.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 36
Section 5 Minimum Qualifications
Instructions: Vendors must respond to each of the following minimum qualifications. Vendors
must meet the minimum qualifications identified below. Failure to submit a response, or
selection of the response “No” will disqualify the vendor from further consideration.
Vendors must copy and paste without modification both the statements and boxes for each
of the numbers in this section into their replies and then select either “Yes” or “No.”
1. Vendor confirms that it will be able to provide all required services to Members
beginning January 1, 2017.
☐ Yes ☐ No
2. Vendor agrees that its reply is not contingent upon being the only plan offered in a
service area and does not include any minimum participation or employee contribution
requirements.
☐ Yes ☐ No
3. Vendor is authorized and registered by the Florida Department of State to do business
in Florida.
☐ Yes ☐ No
Submit proof of such registration as Reply Attachment 5.3
4. Vendor possesses a current accreditation from Accreditation Association for Ambulatory
Health Care, National Committee for Quality Assurance, Joint Commission of the
Accreditation of Healthcare Organizations, or Utilization Review Accreditation
Commission.
☐ Yes ☐ No
Submit proof of such accreditation for the corporate entity submitting the reply as Reply
Attachment 5.4
5. Vendor confirms that it is not in receivership under the Florida Division of Rehabilitation
and Liquidation or under regulatory action per the Florida Office of Insurance
Regulation.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 37
☐ Yes ☐ No
6. Vendor is able to and agrees to administer the Plan in accordance with the plan design
as specified in Attachment H: Covered Benefits and Services.
☐ Yes ☐ No
7. Vendor is registered or certified as required by the Florida Office of Insurance
Regulation.
☐ Yes ☐ No
Submit proof of such registration/certification as Reply Attachment 5.7
For vendors submitting pricing replies for any county under the fully-insured scenario, the
vendor must also respond to each of the following pass/fail requirements. A selection of the
response “No” will disqualify the vendor from further consideration. If a vendor is not bidding
any county under the fully-insured scenario, the vendor should check “Not Applicable”
indicating it is not bidding any fully-insured scenario.
8. Vendor has at least five (5) years of experience in providing HMO services with $90
million in annual earned premium in its commercial group business.
☐ Yes ☐ No ☐Not Applicable
Describe such experience and identify the top five (5) clients as Reply Attachment 5.8.
9. Vendor has at least five (5) years of experience in providing HMO Services for more than
15,000 covered lives in the state of Florida in its commercial business.
☐ Yes ☐ No ☐Not Applicable
Describe such experience and identify the top five (5) clients by number of covered lives
as Reply Attachment 5.9.
10. Vendor has had at least one (1) government client with at least $10 million in annual
earned premium in the State of Florida in its commercial group business.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 38
☐ Yes ☐ No ☐Not Applicable
Provide the name, contact person, address, telephone number, and email address for
such client(s) as Reply Attachment 5.10.
11. Vendor is presently registered or certified as required by Florida law as a Commercial
Health Care Provider by the Agency for Health Care Administration for each county in
the vendor’s proposed service area.
☐ Yes ☐ No ☐Not Applicable
Submit proof of such registration/certification for the corporate entity submitting the
reply as Reply Attachment 5.11.
For vendors submitting pricing replies for any county under the self-insured scenario, the
vendor must also respond to each of the following pass/fail requirements. A selection of the
response “No” will disqualify the vendor from further consideration. If a vendor is not bidding
any county under the self-funded scenario, the vendor should check “Not Applicable”
indicating it is not bidding any self-funded scenario.
12. Vendor administers self-insured benefits for at least one (1) government client with at
least $10 million in annual medical claims in the State of Florida in its commercial group
business.
☐ Yes ☐ No ☐Not Applicable
Provide the name, contact person, address, telephone number, and email address for
such client(s) as Reply Attachment 5.12.
13. Vendor has at least five (5) years of experience in administering self-insured benefits
with $90 million in annual medical claims in its commercial group business.
☐ Yes ☐ No ☐Not Applicable
Provide the name, contact person, address, telephone number, and email address for
such client(s) as Reply Attachment 5.13.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 39
14. Vendor has at least five (5) years of experience in administering self-insured benefits for
more than 15,000 covered lives in the state of Florida in its commercial business.
☐ Yes ☐ No ☐Not Applicable
Provide the name, contact person, address, telephone number, and email address for
such client(s) as Reply Attachment 5.14.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 40
Section 6 Minimum Service Requirements
Instructions: Vendors must be able to provide all minimum service requirements below. Failure
to submit a response or selection of the response “No” will disqualify the vendor from further
consideration.
Vendors must copy and paste without modification both the statement and box below into
their replies.
Vendor confirms that it can and will provide, at a minimum, all minimum service requirements
as described in this ITN section 6.
☐ Yes ☐ No
1. Implementation Plan
Vendor shall submit the final implementation plan to the Department for approval not later
than ten (10) business days following execution of the contract. If the Department deems
the implementation plan to be insufficient, vendor shall work diligently to deliver an
updated, final implementation plan satisfactory to the Department, recognizing that time is
of the essence. Implementation plan shall be based on the proposed implementation plan
submitted by vendor during the procurement process.
Implementation plan shall fully detail all steps necessary to begin full performance of the
contract on January 1, 2017, 12:00:00 a.m., EST, and specifically identify due dates of all
steps with a person assigned responsibility for each. Implementation plan shall include the
following action items:
a. Establish an interactive Enrollee website with value add features (see MSR-23 below),
mobile app, dedicated toll-free phone line, interactive voice response system, and
Department approved communications at least two weeks in advance of the fall 2016
open enrollment period for the 2017 plan year.
b. Participate in fall 2016 open enrollment for the 2017 plan year benefit fairs and
meetings coordinated by the Department.
c. Schedule regular implementation status meetings and/or conference calls with contract
manager. Vendor shall appoint one of their team members to be responsible for
recording detailed meeting minutes and follow up action items on behalf of all team
members, including assignment of tasks and due dates. Minutes of decisions made and
list of action items shall be sent to contract manager within twenty-four (24) hours of
the end of the meeting/call.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 41
d. Conduct background checks in accordance with the contract’s section 3, Contract
Administration, including subcontractors.
e. Apply the provisions of Attachment H: Covered Benefits and Services and successfully
implement all necessary system edits, controls, and/or other policy/procedural
functions to ensure accurate administration and provision of Plan coverage for
Enrollees.
f. Test enrollment files, review key procedures and program process controls (i.e.
approval, design, testing, acceptance, user involvement, segregation of duties, and
documentation). Department must render functional acceptance approval prior to go-
live.
g. Submit to a pre-implementation audit of approximately 200-300 test claims and a
service delivery readiness assessment.
h. Finalize and validate billing procedures, invoice design, banking, reconciliation and other
financial processes, all subject to Department’s prior approval.
i. Design and present to the Department for approval all communication materials to be
used for Plan Enrollees. Communication materials include ID cards, brochures,
explanation of benefit statement forms, paper claim (reimbursement) forms, Summary
Plan Description (SPDs), Summaries of Benefits and Coverage (SBCs), standard letters,
system generated letters, templates, envelopes, clinical program notices and letters,
appeal denial letters, posters and, if applicable, mail order and other pharmacy forms
and flyers.
j. Ensure that ID cards and Plan education materials are mailed to Enrollees no later than
December 20, 2016 for coverage effective January 1, 2017.
k. Create an education plan for medical providers/prior authorization staff at physician’s
offices so they know the Plan benefits, including providing a regularly updated online
reference guide for doctor's office staff regarding pre-authorization processes for
medical services, supplies, prescriptions, utilization management, surgeries, and other
Plan access/pre-authorization requirements.
l. Finalize a process for tracking and responding to Member inquiries and complaints,
which includes measuring and reporting turn-around time.
m. Vendor shall be one-hundred percent (100%) operational prior to the effective date of
January 1, 2017, 12:00:00 a.m., EST. Vendor pays the liquidated damages listed in the
contract (Implementation Delays) for failure to meet this milestone.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 42
n. Vendor shall mail ID Cards (without Social Security Numbers) to all Enrollees the earliest
of December 20, 2016 or ten (10) business days after receipt of a clean and accurate
enrollment file.
2. Account Manager
a. Vendor shall assign a dedicated, but not necessarily exclusive, account manager as the
primary contact for the Department, unless the Department determines an exclusive
account manager is in the State's best interest.
b. The account manager shall participate on the implementation team and coordinate,
troubleshoot, advance and track the State’s interests and requests throughout the
organization.
c. If requested by the Department, the account manager shall be replaced. If in the State’s
best interest, replacement may be interviewed and approved by the Department.
3. Account Management Team
a. Vendor shall assign a dedicated, but not necessarily exclusive, account management
team which may include an executive sponsor, an account manager, a data/fiscal
analyst, enrollment/eligibility manager, claims manager, customer service manager,
medical director, and, if applicable, a pharmacist.
b. Vendor agrees that replacement of personnel to the account management team
assigned to this contract shall be subject to the Department's prior written approval,
should the Department request it at the time.
c. The account management team shall act on behalf of the State in advancing the
interests of the State through vendor's corporate structure.
d. The account management team shall be able to devote the time and resources needed
to successfully manage the account including being available for frequent telephonic,
email, and on-site consultations.
e. The account management team shall be thoroughly familiar with vendor's functions and
operations that relate directly or indirectly to the Department and the Plan including but
not limited to provider networks, claims and enrollment systems, systems reporting
capabilities, claims adjudication policies and procedures, standard and non-standard
banking arrangements, and relationships with third parties. Account management team
shall be on the forefront of healthcare industry trends, medical technology
developments, and best-in-class practices and share this knowledge with the State.
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 43
f. Vendor shall maintain a current account management team organizational chart.
Vendor shall promptly notify the Department of any changes and provide detailed
information regarding new personnel including name, professional background, mailing
and physical address, email address, work and cell phone numbers along with an
updated organizational chart.
g. Department may give a plan performance review to the account management team or
separately to each team member. An action plan, as determined by the Department,
must be implemented based on measurement criteria listed in the Performance
Guarantees section.
4. Background Checks
Vendor shall comply with employee and Subcontractor Security Requirements, including
performing background checks described in section 3.2.5, Background Screening, of the
contract.
5. Dedicated Teams
a. Vendor shall assign a dedicated, but not necessarily exclusive, customer service team for
the Department, unless the Department determines an exclusive team is in the State's
best interest.
b. Vendor shall assign a dedicated, but not necessarily exclusive, enrollment and eligibility
manager for the Department.
c. Vendor shall assign a dedicated, but not necessarily exclusive, billing manager for the
Department.
d. Vendor shall assign a dedicated, but not necessarily exclusive, claims supervisor for the
Department, unless the Department determines an exclusive claims supervisor is in the
best interest of the State.
e. Vendor shall assign dedicated, but not necessarily exclusive, claims processors for the
Department, unless the Department determines exclusive claims processors is in the
State's best interest.
f. Vendor shall assign a dedicated, but not necessarily exclusive, claims processing facility
for the Department.
g. The Department reserves the right to accept or decline vendor's designated claims
supervisor, claims processor(s), and/or claims facility for any reason at any time.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 44
6. Meetings/Conference Calls
a. Quarterly Meetings: vendor shall attend all quarterly meetings at the State offices in
Tallahassee, Florida, or by telephone conference call as directed by the Department.
Vendor shall not be entitled to additional compensation for meeting preparation or
attendance. Quarterly reports are due within forty-five (45) calendar days following
quarter end and meetings/calls are to be held within sixty (60) calendar days following
quarter end. The fourth quarter meeting shall include both quarterly and annual
calendar year reports and deliverables. Requirement also includes quarterly reports and
meetings as required by the Department through the sixteen (16) month period or
following termination of the contract resulting from this ITN.
i. Agenda: At the Department's request, vendor shall provide for the Department's
approval a draft agenda five (5) business days in advance of a meeting allowing
changes to the agenda and a reasonable opportunity to prepare for the meeting.
At a minimum, vendor and Department will discuss medical goals (pharmacy
goals, if applicable), set expectations and priorities, review vendor's quarterly
reports (e.g., thoroughly explain based on data the reasons for increases and
decreases in utilization and cost), and other issues such as performance
guarantees, quality assurance, operations, network status and access (including
pharmacy, if applicable), benefit and program changes or enhancements,
legislative matters, audits, cost trends, utilization patterns, program outcomes,
customer service issues, future goals and planning, and other issues reasonably
related to the contract. Vendor shall address past performance, anticipated
future performance, and compare the Plan's experience to 1) national trends, 2)
vendor's total book of business, 3) other governmental clients, and 4) vendor's
"best in class."
ii. Minutes: Within five (5) business days after any meeting, vendor shall provide the
Department detailed draft meeting minutes. Department will review and revise
the draft minutes as appropriate and return to vendor. Vendor shall provide the
Department with final minutes within three (3) business days after revised
minutes. Minutes shall include a list and description of follow up Deliverables,
with assigned person and due date.
b. Other Meetings: progress meetings, issue meetings, and emergency meetings shall be
held as necessary. Either party may call such a meeting, subject to reasonable notice.
Any meeting held in person shall be at the State's offices in Tallahassee, Florida. Vendor
shall not be entitled to additional compensation for meeting preparation or attendance.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 45
7. Benefit Fairs
a. Vendor shall participate in all locations as applicable to vendor's service area of the
annual open enrollment benefit fairs that are sponsored by the Department or its
designee. Number of fairs and locations may vary each year, but approximately twenty-
four (24) fairs statewide are held in the fall. Vendor's representatives attending the
benefit fairs shall be employees of vendor (not subcontractors or temporary personnel)
and adequately trained and knowledgeable about the Plan. Vendors shall educate
Members on Plan benefits, services and other tips to ensure a positive Member
experience.
b. Vendor shall be responsible for all costs associated with participating in benefit fairs
including travel and a proportionate share of facility fees. For illustrative purposes, in
2014 the share of fees was one-hundred-fifty dollars ($150) per vendor per fair.
c. Vendor shall not solicit State Employees at the work place or during work hours in
person, by email or other means, except during Department-sponsored benefit fairs or
meetings hosted by a State agency or university for its employees.
d. Vendor shall not discuss with Enrollees or prospective Enrollees or in any manner allude
to coverage, products, or materials other than those explicitly related to the Plan
without the permission of the Department. Such prohibition shall also apply to vendor’s
state-specific website.
8. Advertisements and Marketing Materials
a. Vendor shall submit copies of all promotional and Enrollee educational materials to the
Department for prior written approval, if distributed to or accessed by Enrollees for
marketing the Plan. All such materials shall be approved in writing by the Department
prior to use.
b. As applicable, vendor shall pay for the expenses for printing and mailing the State of
Florida Summary Plan Description, Certificate of Coverage, and any associated forms.
c. Vendor shall assist the Department (i.e., review, clarify, edit, and confirm accuracy) as
requested in developing Department communications on the Plan including but not
limited to the Summary Plan Description and the Department's benefit website:
www.mybenefits.myflorida.com.
9. Plan Materials
a. No promotional or Enrollee educational materials related to the Plan may be distributed
or otherwise communicated without the prior review and written approval of the
Department.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 46
b. Subject to the Department's customization and written approval, on a Plan Year basis,
vendor shall be responsible for the development of Plan benefit information including
but not limited to 1) open enrollment brochures and promotional pieces, and 2) other
Plan-related printed materials (e.g., Summary Plan Description, ID cards, benefit
brochures, claim forms, clinical program access tips and notices along with letters,
notices, preformatted letters, templates, system generated letters and notifications,
correspondence forms, Explanation of Benefits (EOBs), and other written materials and
forms).
c. In addition, vendor shall provide ongoing via secure website and/or annually by mail a
summary of covered health care expenses along with Member responsibility amounts
for the purpose of helping Enrollees make better informed health decisions. Therefore,
two (2) weeks prior to the first day of each annual open enrollment, vendor shall either
1) mail this health care summary to the Enrollee and each adult Member, or 2) send
Enrollees and each adult Member a notice advising them how to register themselves to
access this summary information online.
d. Vendor shall be responsible for writing, printing, distributing, and mailing all such
Department-approved information.
e. Vendor shall provide, upon request of the Member, printed materials in a medium
widely accepted for the visually impaired.
f. All printed material shall be provided in electronic format with final versions submitted
to the Department in PDF file format.
10. Provider Directory (e-version)
a. Vendor shall provide an online directory of network providers, which shall be updated
and made available to Members in real time (i.e., same day when provider notifies
vendor or, if provider suddenly stops seeing patients, when vendor learns of it through
Member calls, other providers, other means and media). Directory shall state the list will
change as needed, as well as displaying the actual date of most recent update (e.g.,
noted by “Last Update”).
b. In addition to online, vendor shall provide and support mobile applications of the online
provider directory for cell phones, tablets and other mobile devices.
c. Vendor shall mail provider directories to Members upon request.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 47
11. Membership Materials
Vendor shall mail the following materials to new Enrollees within four (4) business days
after receipt of the enrollment data file or notice from the Department or its designated
agent:
a. Flyer, letter or other mailer advising on where to locate the Summary Plan Description,
how to select a PCP, and other information applicable the plan and enrollment; and
b. Member Identification Cards.
Membership mailing may include a customized greeting and form letter to new Enrollees,
subject to the Department's prior approval. Letter may include a summary of information
already contained in the Summary Plan Description and/or highlight important information
(e.g. how to obtain a referral to a specialist or access urgent or after-hours care).
Vendor may supply new Enrollee information kits to local state agency personnel offices
throughout their respective service areas. Department must pre-approve these enrollment
kits.
12. Summary Plan Description (SPD) (distribution)
Vendor shall use and make available online and by print upon request the Department-
approved Summary Plan Description with certain edits allowed to provide contact
information, vendor-unique processes, and other limited information, all pre-approved by
the State.
Vendor shall provide the Summary Plan Description in Spanish and other language versions where mandated by law based on census demographics.
13. ID Cards
a. Vendor shall provide ID cards to new Enrollees.
b. Vendor shall mail one (1) ID card for each individual contract and at least one (1)
additional ID card for each family contract.
c. Vendor shall provide additional ID cards as requested by the Enrollee.
d. Vendor shall display on the ID cards unique Enrollee-identifying numbers (not SSNs).
Although never displayed, SSN shall be the number of record and maintained in
vendor's information system. ID cards shall be compliant with State standards. ID cards
shall display information for both medical and, if applicable, pharmacy benefits.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 48
14. Mail
Vendor shall hold returned mail for thirty (30) calendar days during which time vendor shall
search for an updated address with each subsequent file coming from People First. After
thirty (30) calendar days, vendor shall store copies on its document imaging system and
destroy the returned mail.
Special post office boxes: vendor shall maintain dedicated post office boxes (e.g., one box
each for claims, appeals, general correspondence, returned mail) which shall be used
exclusively for State-specific correspondence and Plan Enrollees.
15. Department Inquiries, Account Service, and Dispute Support
Vendor shall upon request of the Department or its attorneys and at no additional cost
assist the Department in responding to inquiries received by the Department from
Members, providers, or other persons related to any aspect of Services delivered under the
contract. Such requests shall be a) given a priority status, b) subject to a method of tracking,
c) result in the delivery of all requested information, documentation, etc., and d) handled or
overseen by a lead customer service person.
Vendor shall immediately assist the Department in preparing its reply when the Department
requires an instant reply, including providing data and documentation within the time
frames prescribed by the Department given at that time.
16. Public Records Requests and Subpoenas
Vendor shall upon request and at no additional cost provide the Department with any
necessary data, documents, and so forth, to enable the Department to respond in a timely
manner to public records requests and subpoenas related to any aspect of Services
delivered under the contract.
17. Requests for Legislative Initiatives
Vendor shall make available, at no additional cost to the Department, all necessary
resources to assist the Department in responding to bill analyses, legislative inquiries and
requests including but not limited to the account management team, analytics and
outcomes, research and development, actuarial support, and government relations
department related to any aspect of Services delivered under the contract. Vendor shall
respond within the timeframe set by the Department, which shall be determined at the
time of the inquiry depending upon the scope and complexity of the request.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 49
18. Underwriting and Actuarial Services
Vendor shall provide the Department with underwriting and/or actuarial services related to
any aspect of Services delivered under the contract at no additional cost to the Department.
For actuarial certification and required signature activities by a Fellow of the Society of
Actuaries, up to fifty (50) hours per calendar year shall be designated for these services with
unused hours rolled over to the following year.
19. Consulting Services
Vendor shall, upon request, provide consulting services at no additional cost to the
Department related to the Services (e.g. to verify improved pricing, review consolidated
claims platforms, and other situations).
20. Medicare Secondary Payer
Vendor shall coordinate benefits with Medicare's third party administrators without
involving the Member (see MSR 52 below). Vendor shall respond to all Medicare Secondary
Payer notices to avoid offsets to the State.
21. Customer Service Unit
a. Vendor shall maintain a customer service unit dedicated, but not necessarily exclusive,
to performing all aspects of Member-related customer service and shall include a state-
of-the-art call center. Calls to this unit shall be accepted and answered promptly by a
live customer service representative during the hours of 8:00 a.m. to 6:00 p.m. Eastern
Time, Monday through Friday, excluding State holidays set forth in section 110.117,
Florida Statutes.
b. Vendor shall maintain an exclusive toll-free customer service number, which will permit access anywhere in the United States. Customer service unit is subject to pertinent requirements in the Performance Guarantees section.
22. Customer Service Operations
The customer service operation shall include, at a minimum, the following:
a. Integrated member support for all plan services;
b. Plan specific training and knowledge to assist Members, prospective Enrollees,
physicians, pharmacists, etc. regarding Plan;
c. Assist Members who contact vendor's customer service unit with only their name
and/or Social Security number;

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 50
d. Maintain an enrollment file that identifies eligible Members and other pertinent
information regarding Members;
e. Processes for triaging emergency requests (i.e. out-of-network provider coordination,
early fills, if appropriate);
f. Adequate and appropriate access to the customer service system for Members with
disabilities (e.g. TTY and online access);
g. Sufficient personnel available to provide multi-lingual (Spanish, at a minimum) service
and the ability to provide service to the hearing and vision impaired;
h. Information systems capable of electronically transmitting, receiving, and updating
Enrollee profile information from People First as required in contract Attachment 3:
Enrollment File Interface Layout. Maintain a service disruption plan or procedure to
continue customer service activities when temporarily unavailable due to either
scheduled or unforeseen events (e.g., relocating offices, repairing/restoring utility or
power supply, upgrading phone systems, and other events). The Department shall be
notified as soon as possible for scheduled disruptions and other events; and
i. Provide services on a reciprocal basis throughout its authorized service areas to
Members enrolling in its plan. An eligible dependent of an Enrollee living in a different
service area is entitled to receive the same Services in that Dependent’s remote service
area if such county is part of the vendor's commercial book of business.
23. Member Website Tools
Vendor shall provide and maintain a State of Florida-specific Member website with 24/7
access for medical, general health and, if applicable, prescription drug information, if
applicable. This website shall include links to the Department's website and other state,
federal, and condition-specific websites as appropriate to make available a variety of
information to Members. Such web-and/or cloud-based access shall include the ability to, at
a minimum:
a. Access forms and brochures;
b. Order ID cards and/or otherwise display ID cards on a mobile application;
c. Access preventive educational information;
d. Access general health and chronic disease information;
e. Track medical out-of-pocket Plan limit (medical only);
f. Track federal out-of-pocket limit (medical and pharmacy combined);

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 51
g. Track Health Investor Health Plan accumulator information including separate tracking for both individual and family member out-of-pocket costs;
h. Complete online health risk assessments;
i. Communicate with a customer service representative;
j. Offer other valuable tools;
k. Locate participating network physicians and hours of operation when hours are known;
l. Locate participating network facilities and hours of operation when hours are known; and
m. For fully insured plans providing prescription drug benefits, track prescription drug history.
24. Cost Estimator
The online system shall offer a cost estimator that shows the maximum Member cost share
and the plan cost share for a specific procedure prior to rendering of the service.
25. Member Satisfaction Surveys
Vendor shall conduct an annual Member satisfaction to measure overall satisfaction subject
to contract Attachment 2: Performance Guarantees. Survey instrument, methodology,
timing, and distribution are subject to the Department’s approval. In addition to the
vendor’s annual Member survey, Department may conduct its own Member satisfaction
survey. The Department may select the survey instrument and may either conduct or have
it conducted by an independent third party. Survey results shall be used, in part, to
determine satisfactory performance of the contract. If the survey shows unsatisfactory
performance, vendor shall implement a corrective action plan approved by the Department.
26. Protected Health Information
Vendor agrees to adhere to leading industry practices in the development, implementation,
and application of administrative, physical and technical safeguards that reasonably and
appropriately protect the confidentiality, integrity, and availability of the protected health
information that vendor creates, receives, maintains, or transmits in vendor's
administration of the Plan, as required by the HIPAA security standards and all applicable
HIPAA administrative simplification rules.
27. The Department Determines Eligibility
Vendor shall permit all eligible Enrollees as determined by the Department or its designee
to obtain health insurance benefits for themselves and their eligible dependents. The

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 52
Department retains final authority in determining eligibility and this determination may
result in rare instances when the effective date goes back more than sixty (60) calendar
days.
28. Selection of a Primary Care Physician (PCP)
a. Vendor shall offer Enrollees a choice of PCPs and either require or strongly encourage
each family member to select one.
b. Vendor shall not use a State agency personnel office or the Department as an
intermediary for the PCP selection process.
c. If applicable, vendor shall make it clear to Members that the Plan requires each Member
to select a PCP. Absent that selection, vendor may assign one to each family member
with the Member’s option to change via vendor’s website or member services.
d. Vendor must encourage and make available internet or computerized telephone
response systems to facilitate PCP selection. If available, such internet or mobile
application means shall be advertised by vendor in Enrollee communications.
e. Do Not Delay Enrollment due to No PCP Selected: vendor shall not delay an Enrollee's
effective date of coverage because of failure to select and register with a PCP. Further, if
vendor requires a PCP selection, then vendor shall send member a letter within ten (10)
business days of coverage effective date asking them to choose a PCP with steps on how
to register such selection with the vendor.
29. Verification of Persons with Disabilities
Vendor agrees to maintain and verify documentation of permanent and total disability
status for eligible dependents of Enrollees. Vendor must verify permanent disability status
at least every five (5) years using a process approved by the Department.
30. Notify the Department
a. Vendor shall, within twenty-four (24) hours of announcement, notify the State if vendor
or provider network loses any accreditation, service area approval, licenses, or liability
insurance coverage.
b. Vendor shall, within twenty-four (24) hours of announcement, notify the Department
with a statement of justification in the event of a major loss of network health care
providers or disruption to the network (i.e. loss of a hospital, facility, provider group,
and so forth). The statement shall include the following:

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 53
i. Member Impact Report: a description of how the contract action impacts the
interests of the State including number of impacted Members; and
ii. Confirmation that vendor shall continue to maintain minimum access standards
through other providers.
31. Continuity of Care
Vendor shall continue coverage under certain circumstances when provider contract is
terminated.
a. Unexpected: vendor shall notify impacted Members as soon as administratively possible
but no later than five (5) business days of vendor receiving formal notice when a
provider’s contract unexpectedly terminates (e.g., death or loss/suspension of a license
to practice medicine and so forth).
For terminating PCPs, vendor shall assist Members in selecting another PCP. New
selection shall be effective the day immediately following the provider’s termination
effective date or sooner if requested. If the provider does not properly notify vendor of
intent to terminate, then vendor shall pursue disputes with the provider’s contract
without interruption of patient care.
b. Expected: vendor shall notify impacted Members at least thirty (30) calendar days prior
to the expected termination date of provider's contract when failure to renew,
unsuccessful negotiations, and so forth.
c. As provided for in subsection 110.123(3)(h)6, Florida Statutes, when vendor terminates
a provider without cause, vendor shall allow Members to continue coverage when
medically necessary the longer of: through completion of a condition for which the
Member was receiving care at the time of termination, until the Member selects
another treating provider, or until the next open enrollment period offered, but no
longer than six (6) months after the termination of the contract. Vendor shall allow
pregnant Members to continue care with a terminated treating provider until
completion of post-partum care.
d. These requirements shall not apply to treating providers who have been terminated
from the vendor for cause. Vendor shall develop and maintain policies and procedures
for the provision of continued care as prescribed above.
e. Vendor's physician and hospital contracts shall have a "continuation of care" clause
consistent with the requirements of subsection 110.123(3)(h)6, Florida Statutes.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 54
32. Nominating Providers
Vendor shall have a procedure in place to allow plan Members and/or the State to
nominate providers to be considered for inclusion in vendor’s network and/or vendor’s sub-
contracted provider’s network (e.g., Applied Behavior Analysis (ABA) therapists, mental
health providers, urgent care centers, primary care physicians, and others).
33. Annual Visits
Vendor shall perform annual visits to network physician offices, both general practitioners
and specialists, to educate the physician's or facility's business office manager on Plan
benefits, billing, and resolving claim issues.
34. Access Standards
Vendor shall establish and maintain a comprehensive network of participating physicians,
hospitals and other providers and facilities to sufficiently provide all services under the Plan.
In addition, vendor shall provide access to the doctor types and hospitals listed in the
Performance Guarantees section.
35. Balance Billing Prohibited
Vendor confirms that, for insured HMO benefits, procedures are in place for ensuring that a
network provider does not bill State of Florida Enrollees and/or the State any amount in
excess of the contracted network rate, network allowance or allowed amount in accordance
with chapter 641, Florida Statutes.
36. Onsite Clinic
a. Vendor may be required to assist the Department in examining the feasibility of
implementing, staffing, and maintaining an on-site clinic.
b. In the event the Department establishes an on-site clinic, vendor shall enter a network
contract allowing Enrollees in-network utilization of the clinic.
37. Enrollment File Transfers from the Department
a. Vendor shall maintain an information system capable of electronically receiving and
updating Enrollee information on weekly, monthly and/or ad hoc basis (e.g. eligibility,
change of address, coverage information, and so forth). Vendor shall accurately convert
and load the Department's enrollment files in a secure point-to-point connection
format.
b. Vendor shall maintain enrollment records for all Enrollees based on the Department's
weekly and monthly enrollment files.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 55
c. Vendor agrees that the Department's enrollment file shall be the official system of
record. Vendor shall not overwrite, update or in any way change the enrollment
information without the express written direction from the Department or People First.
d. Vendor shall accept the enrollment files in a format and according to the schedule
required by the Department in contract Attachment 3: Enrollment File Interface Layout
and Attachment 4: Enrollment File Transfer Schedule.
e. In addition to the file schedule above, vendor shall accept enrollment file typically
provided at the end of November following open enrollment for the purpose of
generating ID cards for distribution prior to the new Plan Year.
f. The enrollment files shall be processed as required by contract Attachment 2:
Performance Guarantees.
g. Vendor shall conduct and maintain enrollment reconciliation between vendor's system
information/files and the Department's enrollment files.
h. Enrollment file transfers and subsequent discrepancy reports between vendor and the
Department shall be exchanged using a method required by the Department.
i. Enrollment updates including manual reinstatements and terminations from People
First shall be processed as required by contract Attachment 2: Performance Guarantees
at no additional cost to the Department.
38. Paid Claims File to the Department and/or Department’s Designee
Vendor shall provide a secured file including all claim data related to the Plan in the data file
layout and timeframe specified by the Department. Data shall be provided in a secured
method to the Department and/or a third party designated by the Department and shall
include, but not be limited to, trade secret, proprietary or confidential claim related
financial information: total charged amount, allowed amount, discount amount, deductibles
and copayments, and plan payment amount provider information ,including, but not limited
to, name, location and National Provider Identifier or Tax Identification Number; and all
fields, whether received electronically or via paper, from CMS 1500 (837-P) and UB-05 (837-
I) medical claims forms including all patient demographic information (including dependent
social security number), diagnosis codes, procedure codes, surgical procedure codes,
modifiers, and all other data elements associated with each claim. All claims processed
during the reporting period, including paid, denied and adjusted claims, shall be included.
The Department reserves the right to utilize the monthly paid claims files in any manner
deemed necessary, including but not limited to, source data for audit purposes. Failure to

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 56
timely submit complete, properly formatted data shall be considered a material breach of
the contract and shall be subject to the breach requirements in the contract.
39. Use of Plan Data
a. Vendor shall not sell or share the Plan's data without the prior written authorization of
the Department.
b. Vendor agrees that the only compensation to be received by or on behalf of its
organization in connection with this Plan shall be that which is paid directly by the State.
40. System Upgrades, Enhancements and Problems
a. Vendor shall provide at least six (6) months prior notice of any significant planned
system upgrades or changes, including but not limited to claims, customer service,
enrollment, operating systems and any other changes that may materially affect the
administration of the Plan. Changes shall be subject to the Department's prior written
approval.
b. Vendor shall immediately notify the Department upon the discovery of problems or
issues impacting claims processing related to the Plan. Failure to timely notify the
Department shall be considered a material breach of contract resulting from this ITN.
c. Vendor shall not take corrective action related to systemic problems or issues impacting
claims processing related to the Plan without the written approval of the Department.
41. Out-of-Pocket Accumulators
On a daily basis or more frequently as mutually agreed vendor shall:
a. Provide the file of all Member accumulator information to the Department’s pharmacy
benefits manager and/or other required third parties. This file shall be formatted as
agreed upon by the parties and approved by the Department, subject to the
Performance Guarantees section and/or contract.
b. In addition, vendor shall be the record keeper of Member medical and drug spend
accumulator information and update applicable Member cost shares (i.e., remaining
deductible, medical out-of-pocket maximum, and global out-of-pocket maximum) using
all pertinent information as appropriate and consistent with the Plan design.
42. Paid Claims Exchange with PBM
On a monthly basis or more frequently as mutually agreed vendor shall:
a. Provide a file of all paid claim activity to the Department’s pharmacy benefits manager
and/or other required third parties.
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 57
b. Accept a paid claim file from the Department’s pharmacy benefits manager and/or
other required third parties.
This file shall be formatted as agreed upon by the parties and approved by the Department,
subject to the Performance Guarantees section and/or contract.
43. Other Data Transfers as Required
a. File transfers between vendor and Department and/or authorized third parties shall be
exchanged using a method, format and frequency required by the Department.
b. Vendor shall provide all medical and pharmacy data related to the plan to the
Department and/or to a third party designated by the Department, in the time frame
and in the format specified by the Department. Failure to timely submit complete,
properly formatted data shall be considered a material breach of the contract.
44. Records Retention
Vendor shall retain records as required by the contract, or longer, if required by state
and/or federal laws or regulations.
45. Claims Processing and Adjudication
a. Vendor shall establish and perform all aspects of claims processing, coordination of
benefits, claims reimbursement, point-of-sale transactions, adjudication, and payment
in accordance with the Summary Plan Description. Vendor shall verify benefits and
eligibility before authorizing services.
b. Vendor’s claims processing guidelines are subject to the claims standards in the
Performance Guarantees section including, but not limited to, for timeliness, financial
accuracy, payment accuracy, and overpayment recovery, and so forth.
46. Standard Claims Administration Practices
a. Vendor shall receive, process, and adjudicate claims in accordance with best industry
practices using nationally recognized standards, as determined by the Department. At
the Department’s direction, vendor shall implement best industry practices.
b. Vendor certifies its ability to administer the Plan in compliance with all State and federal
mandated benefits.
c. Vendor shall maintain a system for statistically profiling charges and allowances by
procedure code and by ZIP code. Regarding claims edits within the claims adjudication
process, vendor shall use, in accordance with the CMS National Correct Coding Initiative
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 58
(NCCI), Procedure-to-Procedure (PTP) edits, Outpatient Code Editor (OCE) and Medically
Unlikely Edits (MUE).
d. Vendor agrees that illnesses, conditions and services associated with its preferred
medical facilities and/or centers of excellence programs shall be bundled with regard to
reimbursement. Vendor also agrees that the facility shall be at risk for costs incurred in
excess of the negotiated (bundled) charge.
e. Vendor shall accept and load historical data from any carrier that severs ties with the
Department for tracking and accurate payment of benefits (i.e., service limits,
deductible accumulator, and medical and global member out-of-pocket max amounts).
47. Must Offer Standard and Health Investor Health Plan (HIHP) Plan Options
Vendor shall accommodate both a standard plan and a health savings account qualified high
deductible health plan design (e.g. HIHP), as described in the Department’s Summary Plan
Description.
48. Summary Plan Description (Strict Adherence)
The Florida Legislature, through the annual General Appropriations Act, establishes the
desired set of benefits. Vendor shall strictly adhere to the coverage provisions of the
Summary Plan Description, including but not limited to providing payment of non-network
services except in the case of verified emergencies.
49. Conversion Policy
Vendor agrees to provide a post-COBRA fully insured conversion policy to terminated
Enrollees, pursuant to sections 627.651(1), 627.6675, 641.3921 and 641.3922, Florida
Statutes.
50. Other Coverage Liability
Vendor shall conduct other coverage liability (OCL) verification annually through the most
appropriate channel, which may involve the Member.
51. Coordination of Benefits
a. Vendor shall use applicable State laws for determining order of liability for Coordination
of Benefits (COB) including but not limited to other insurance, workers’ compensation
insurance, and Medicare. In addition to order of liability, vendor shall interface with the
State’s workers’ compensation vendor, Centers for Medicare and Medicaid (CMS)
through voluntary data exchange, and other payers and methods as the Department
determines.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 59
b. Vendor shall coordinate benefits on a pay-and-pursue basis for active Enrollees and
Dependents and, conversely, a pursue-and-pay basis for all other Members.
c. As a secondary payer, vendor shall reimburse as specified in the Coordination of
Benefits section of the Summary Plan Description.
d. As secondary payer, vendor shall coordinate with Medicare and benefits shall be paid up
to the lessor of 1) the covered expenses Medicare does not pay, up to Medicare
allowance, or 2) the amount this Plan would have paid if Member had no other
coverage. Plan benefits for Members who are eligible for Medicare Parts A and B but
have not enrolled will be paid as if Medicare had paid first as the primary plan.
52. Coordination with Medicare’s Third Party Administrators
a. Vendor shall coordinate with Medicare’s third party administrators and shall ensure that
claims are processed with primary and secondary payers without involving the Enrollee.
Vendor shall be responsible for timely responding and resolving all Medicare Secondary
Payer (MSP) notices to avoid offsets to the State of Florida. Vendor shall be financially
responsible for its failure to accurately and timely resolve such MSP notices resulting in
the offset of State funds.
b. Plan benefits for Enrollees who are eligible for Medicare Parts A and B, but failed to
enroll, will be paid as if Medicare had paid first as the primary plan.
c. As secondary payer to Medicare, vendor shall allow for, and establish, automatic
crossover from Medicare.
d. Vendor shall appropriately process electronic (real time) and paper claim submissions
for Coordination of Benefits (COB) as secondary payer for Medicare Part D enrollees.
53. Subrogation
Vendor shall identify, to the extent possible, any claim payments for which the plan has, or
may have, a right of subrogation. Vendor shall make a reasonable and diligent effort to
enforce, in accordance with section 768.76, Florida Statutes, and the Summary Plan
Description, any subrogation claim belonging to the Plan. Vendor shall develop and
implement a subrogation process subject to the Department's approval for reporting
subrogation claims belonging to the Plan. Vendor shall pursue, settle and collect all
subrogation rights allowed in the Summary Plan Description. Department must approve any
recommended settlement if less than the State’s full lien amount minus any cost sharing or
reduction allowed by section 768.76, Florida Statutes. Additionally, vendor shall develop a
monthly subrogation report, subject to the Department's approval, for reporting the
identification, status, and resolution of all pertinent subrogation cases.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 60
Recovery amounts from subrogated claims shall not be reduced or otherwise offset by contingency fees or other fees charged by an auditor or other recovery service.
54. Explanation of Benefits (EOB) Statement
Monthly: Vendor shall furnish an Explanation of Benefits (EOB) Statement for all claims
processed within a month timeframe via regular mail to last known address. In lieu of hard
copy EOB, vendor may provide a per-claim electronic EOB, subject to authorization of the
Enrollee. Department must approve and may customize the design of the EOB.
The EOB shall include all claim details, including accumulation balances for each medical
and global out-of-pocket maximum amounts (i.e., medical only claims and, separately,
medical and prescription drugs, respectively). Vendor shall be the keeper of
record/accumulator of medical and prescription drug claims and shall be responsible for
accurately storing, calculating and displaying (hard copy and online) both accumulation
amounts in real-time (online).
In addition, vendor shall provide two (2) member Benefit Statements each year: one near
the start of the open enrollment period showing year-to-date claims; the other just after
the start of the new year showing previous calendar year claims. The fall Benefit Statement
provides members the value of their plan by showing how much the plan paid versus the
Member paid; annual Benefits Statement provides the same plus information that the
Member uses for tax filing purposes.
55. Inaccurate Payments
a. Upon discovery, notification, or recoveries as part of audits (i.e., vendor self-audit,
Department/contract required audit, eligibility audit, hospital audits, and/or provider
audits) or other claim review activities, the vendor shall fully rectify the inaccurate
payment, including but not limited reprocessing incorrect claims and reimbursing the
Department, whenever payment is made that is not in accordance with the terms of the
contract. The vendor shall reimburse one hundred percent (100%) of all identified
overpayments to the Department. Such overpayments shall not be reduced by
contingency fees or other fees charged by an auditor or other recovery service.
b. Vendor shall reimburse the Enrollee in the event a recovery impacts the Enrollee's cost
share. In certain situations, vendor may repay health care provider with instructions for
them to repay member. Simultaneously, vendor shall notify Enrollee of any applicable
refund.
c. Under a self-funded arrangement, vendor shall reimburse the Department first and then
pursue reimbursement from the provider. Vendor shall send payment of these

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 61
recoveries to the State via an electronic fund transfer. Daily claims funding will not be
reduced or otherwise offset by these overpayment recovery amounts.
56. Recovery Procedures
a. Vendor shall have procedures in place for recovery of capitation fee and claims
processing financial errors identified in all audits (i.e., vendor self-audit, Department or
contract required audit, eligibility audit, hospital, and provider audits). Vendor shall
recover and send payment of these recoveries to the State, not reduce the daily claims
funding amounts or otherwise offset amounts, subject to the standards in the
Performance Guarantees section.
b. Under a fully insured arrangement, recoveries shall be credited to the Plan's financial
experience.
c. The vendor shall reimburse the Department for any and all overpayments regardless of
whether the overpayment is recovered from the Plan member or provider, and
regardless of how the error was discovered. Reimbursement shall be made to the
Department via an electronic fund transfer or to the Plan member, as applicable, within
sixty (60) days of identifying the overpayment.
57. Accounting System
Vendor shall maintain an accounting system and employ accounting procedures and
practices conforming to generally accepted accounting principles and standards. Vendor’s
accounting records and procedures for medical and pharmacy, if applicable, shall be open
to inspection by the Department, or its authorized representatives, at any time during the
contract period and for so long thereafter, as Department requires. However, that any such
inspections shall be subject to confidentiality protocol requirements. All charges, costs,
expenses, etc. applicable to the contract shall be readily ascertainable from such records. As
applicable, supporting documentation for all charges, fees, guaranteed savings and rebate
payments including reimbursement invoices for prescription drug payment shall be readily
ascertainable from such records.
58. Appeal Services
a. At no additional cost to the Department, vendor shall administer appeals in accordance
with the appeals process described in the Summary Plan Description and as otherwise
required by the Department, state and federal law. Such appeals include Level I appeals,
medical review/assistance to the Department for Level II appeals, administrative
hearings and, for fully insured arrangements, external reviews by vendor's Independent
Review Organization (IRO). Department shall approve and may customize any and all
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 62
correspondence, letters, communications and so forth related to any part of the appeals
process. Vendor shall adhere to the standards in Performance Guarantees section.
Vendor shall maintain a record of all grievances/appeals from Members and shall
provide a summary of grievances/appeals to the Department quarterly, or more
frequently upon request. Upon request, vendor shall provide a narrative summary of
the reasons for the grievances/appeals, the disposition thereof, and any corrective
action plans implemented as the result of the grievance/appeal.
b. Appeal-related Documentation and Testimony: Upon Department's request or its
attorneys and within specified timeframes by the Department, vendor shall provide all
documentation related to a Plan Member's appeal/administrative hearings(s). This
documentation shall include but not be limited to clinical/medical policy guidelines, any
notes, medical review notes or statements of medical providers and/or vendor's medical
reviewers or consulting medical providers. Vendor shall make available the
documentation and testimony of vendor's employees, physicians, nurses, consultants,
associates and other personnel necessary for the Department's presentation of the
review or appeal/administrative hearings via telephone or in-person if required by the
Department, at no cost to the Department.
59. Notify Enrollee if Not Paid within 45 Days
Pursuant to subsection 110.123(5)(g), Florida Statutes, vendor shall provide written notice
to Enrollees if any payment to any provider remains unpaid forty-five (45) Calendar Days
after receipt of the Claim.
60. Medical Necessity Determination and Review
a. Prior to any denial of an appeal as not medically necessary, experimental, and/or
investigational, the claim being appealed shall be reviewed by an appropriate medical
professional. Vendor shall apply the definition of "Medically Necessary" as defined in
the Summary Plan Description and in accordance with vendor's medical policy or
coverage guidelines in effect at the time the claims is incurred. Vendor shall create,
maintain, and annually update medical guidelines, which shall be thoroughly researched
using published medical literature. Except for appeals on eligibility, the Department may
request and vendor shall provide a medical review in any other instance.
b. In accordance with the Summary Plan Description and Florida Law, the Department shall
have full and final decision making authority concerning eligibility, coverage, benefits,
claims and interpretation of the Summary Plan Description.
c. Vendor shall provide copies of medical policy guidelines upon the Department's request.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 63
61. Prescription Drug Rebates
Vendor shall provide to the State one hundred percent (100%) of all prescription drug
rebates, discounts, dispensing fees and other pharmaceutical manufacturer revenue
collected and related to claims as part of this Plan. Such rebates and other revenue shall be
separately identified and included in the quarterly report as described in Quarterly Reports
section within these Requirements.
62. Fraud and Abuse Investigations
Vendor shall develop and/or maintain protocols, procedures, and/or system edits, subject
to the Department’s approval and customization upon request, to aggressively monitor for
fraud, abuse and waste. Vendor shall provide the Department with a quarterly report of all
fraud and fraud-prevention activities and discoveries relating to this contract subject to the
accuracy and timeliness provisions in the Performance Guarantees.
Vendor shall investigate any fraudulent, suspected fraud or suspicious activity relating the
Plan which it believes to be fraudulent or abusive whenever detected or brought to
vendor's attention by the Department or other persons. Vendor shall timely notify the
Department of any fraudulent or abusive Claims or other activities relating to the Plan
which it uncovers and shall fully cooperate with and assist the Department, law
enforcement, and State agencies in their investigations or inquiries regarding any such
matters and in any related recovery efforts.
63. Audit Trail
Vendor shall establish and maintain an effective audit trail for each Claim received for
medical and, if applicable, pharmacy services.
64. Unusual Charges Review
At no additional cost to the State, vendor shall obtain the advice and consultation of
qualified experts (internal or external, as needed) to review unusual charges or Claims for
medical and, if applicable, pharmacy benefits to ensure strict adherence to all Plan
provisions.
65. Care Management and Utilization Management
Vendor shall maintain policies and procedures in its care management and utilization
review processes for the Plan:
a. Pre-certification;
b. Prior authorization;

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 64
c. Concurrent review and discharge planning for inpatient admissions;
d. Retrospective clinical review;
e. Second surgical opinions;
f. Other care management programs currently offered or implemented in the future;
g. Use of an automated system for medical and pharmacy benefits with the ability to
provide utilization statistics and savings reports, including utilization trends, care
management interventions, and clinical and financial outcomes ;
h. Use of an automated system for identification, tracking, and management of care
management activities. The system shall be fully integrated to include medical and
pharmacy claims processing, benefits and enrollment systems, if separately maintained.
Medical necessity and length of stay criteria shall be integrated within the system.
Vendor's utilization review staff shall have access to online diagnostic and procedure
codes ;
i. DRG validation;
j. Responses on all urgent and/or emergency utilization review prior authorization/pre-
certification requests for medical and, if applicable, pharmacy benefits, shall be made to
the attending physician, hospital, patient, and claim administrator within twenty-four
(24) hours of initial request;
k. Responses on all routine utilization review prior authorization/pre-certification requests
for medical and, if applicable, pharmacy benefits shall be made to the attending
physician, hospital, patient, and claim administrator within fourteen (14) Calendar Days
of initial request; and
l. The licensed care management staff shall have an average of five (5) years of clinical
experience. A licensed physician shall provide oversight to all non-clinical support staff
participating in care management activities. Only a licensed physician may issue clinical
denials.
66. Required Format and Timeliness
Vendor shall electronically deliver all reports listed in contract Attachment 5: Reporting
and Deliverables in the format, frequency, timeframe and to the intended recipient noted
in the list of reports or as otherwise required by the Department. The Department shall not
be required to produce such reports in a self-service manner by accessing vendor’s online
reporting tool.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 65
Vendor shall provide all required reports and/or deliverables to the Department and/or its
authorized third party in a format specified by the Department showing utilization, claims
reporting, and administrative services, fees and other activities, (i.e., administrative
services only, or fees for optional clinical management programs) data by both plan
options (Standard and Health Investor), benefit type (medical and, if applicable, pharmacy
and aggregated medical-pharmacy), and by subgroup. The subgroups at a minimum are:
active employee, including variable hour (hourly) employees, COBRA, retirees not eligible
for Medicare, and retirees eligible for Medicare. Administrative activities include claims
adjudication, customer service, medical management and so forth.
67. Vendor's One-Day Acknowledgement of Report Requests
Vendor shall acknowledge report requests within one (1) business day and shall provide an
expected timeline for completion and delivery date. Such reports may include Plan-specific
financial and statistical files, claims processing, Enrollee services, network adequacy, patient
management, and medical and drug utilization reports, as applicable.
68. Revenue Estimating Conference Report
Vendor shall provide the required data and forecasts in support of the Department's
Revenue Estimating Conference Report. Such data shall be provided in the timeframes and
layout specified by the Department.
69. Redacted Copies
Reports containing proprietary, trade secret and/or confidential information shall be
delivered in a redacted format at the same time as any non-redacted report, with redacted
report delivered electronically. Complete and detailed supporting documentation must be
provided with the submission of each report. Supporting documentation must identify the
source of the material.
70. Evidence Based Medicine
If the Department chooses to implement evidence based medicine or disease management
programs at any point during the contract, vendor shall cooperate fully with the
Department’s vendor, including coordination of care management activities and
transmission of data to and from the vendor in a mutually acceptable format and at no
additional cost.
71. Clinician Staffed Toll-Free Line
Vendor shall make available to all Members a 24/7/365 clinician staffed toll-free line.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 66
Clinical staff shall, at a minimum, address immediate and every day health issues and
concerns, and distribute educational materials
72. Prenatal Education and Early Intervention Program
Vendor shall make available to pregnant Members a prenatal education and early
intervention program to screen for potential risk factors and assist in development of
personalized education and monitoring program, including monitoring of high-risk
pregnancies.
73. Direct Deposit EFT
Vendor shall accept payments from the Department processed through the Department’s
standard transmittal process (i.e. EFT transfer to the vendor) and by Department
determined due dates. The vendor must complete a direct deposit authorization form
(currently form number DFS-A1-26E rev.6/2014).
The vendor shall provide any payments due to the Department through the normal
transmittal process (i.e. EFT transfer from the vendor) and by Department determined due
dates.
74. Net of Funds and/or Offset Prohibited
All payments to the Department shall be made separately by electronic funds transfer from
any payment balances due from the Department. The netting of payments related to the
Plan is prohibited.
75. Overpayments Must Reconcile
Vendor shall remit overpayments to the Department monthly by electronic funds transfer.
Such overpayments shall reconcile with monthly reports in a form required by the
Department.
76. Premium Payments – Fully Insured Arrangement
Under a fully insured arrangement, vendor shall conform to the following procedures for
the invoicing of contracted premiums.
a. After the close of the month, vendor shall accept monthly fully insured premium
payments processed on or about the twentieth (20th) day of each following month
based on the Department’s enrollment report data as calculated by the Department.
Retro adjustments for enrollment in prior months may also be included in the payment.
b. Vendor agrees that the only compensation to be received by or on behalf of its
organization for this contract shall be the premiums paid directly by the Department for
fully insured plans.
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 67
77. ASO Fee Payments – Self-Funded Arrangement
a. Vendor shall provide the Department a detailed (itemized) invoice for administrative
fees and charges no later than the tenth (10th) Calendar Day of each month following
the month services were rendered. Required detail and documentation for such invoices
shall be as specified by the Department and shall provide sufficient detail for pre and
post audit. Invoices and supporting documentation shall be provided in paper and
electronically.
b. Upon determination by the Department that the invoices are complete and accurate
and that payment is due, the Department shall process each invoice in accordance with
the provisions of section 215.422, Florida Statutes. The Department shall forward
payment through electronic funds transfer to the vendor for the invoiced amount.
c. If the Department contests the invoice charges as submitted, vendor may be required to
provide additional documentation.
d. Vendor agrees that the only compensation to be received by or on behalf of its
organization for this contract shall be administrative fees.
78. Banking Requirements
Vendor shall establish and maintain a medical claims reimbursement demand deposit
account at no cost to the Department to assign, report, and provide audit controls for
Department's claim liability for medical claims benefit payments made solely under the
contract resulting from this ITN.
a. This account shall only be used by vendor to:
i. Request funding;
ii. Provide online detailed reconciliation data, which shall be provided within 24
hours of liability assignment;
iii. Detail monthly issued/cashed reporting on medical claim payments to or on
behalf of those Members under the Plan; and
iv. Issue benefit payments using either tamper resistant drafts or secured electronic
funds transfer (EFT).
b. Vendor shall cover day one claims liability prior to invoicing the Department on day two.
Vendor shall provide daily invoice notices via email to the Department covering all
checks presented (cleared), excluding outstanding issued checks, and EFT payments
settled for the prior day and the Department will wire payment to vendor's designated
demand deposit bank account previously agreed to by the Department.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 68
c. Vendor shall provide at least ninety 90 days’ notice to the Department if vendor changes
the bank account. Vendor shall suspend issuance of drafts or electronic fund transfers in
payment of medical claims upon receipt of written notice of contract termination to the
designated representative of the vendor by the Department.
d. The Department shall only reimburse vendor's daily invoices for EFT transaction and
cleared checks that have been presented to vendor's bank account. Issued and
outstanding checks will not be included in the reimbursement.
e. The banking contract shall include but not be limited to a record of electronic funds
transfers and/or transmission of daily written drafts register by vendor to the bank for
positive confirmation procedures. The transmission must include draft number, draft
amount, payee's name and date of draft. The method of transmission shall be
determined by mutual agreement between vendor and the Department's bank with
approval by vendor's bank.
f. The Department shall identify the necessary documentation and the related reporting
requirements for the reconciliation. Vendor shall submit to the Department
recommended processes and internal controls developed by vendor to identify
payments due to overbilling and other errors that may occur as part of the payment
process. Reconciliation activities shall include but are not limited to:
i. Daily notification of amount of request
ii. Listing of daily charged claim activity report (claim charge activity by check/item
and Member)
iii. Daily detail report for transfer evaluation (all claim charge items at Enrollee
level)
iv. Monthly bank account statement
v. Monthly summary of daily bank activity for each calendar year
vi. Monthly Outstanding Report #1 (checks less than 90 days old that have not
cashed)
vii. Monthly Outstanding Report #2 (checks that are more than 90 days old that
have not been cashed)
viii. Monthly aged outstanding report with stop payment placed (details the in-house
stop payments placed on items that remain uncashed 12 months from issuance)
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 69
ix. Monthly issue/cashed reconciliation report (issued vs. cashed items in policy
month).
79. Daily Funding for Medical Claims Paid
a. Vendor shall provide the Department with an itemized invoice for reimbursement of
processed Claims on a daily basis, with Claims broken out by Enrollee subgroup (active,
including variable hour (hourly) employees), COBRA, retirees eligible for Medicare, and
retirees not eligible for Medicare).
b. Weekly invoices shall be sent to the State by 4:00 p.m. Eastern Time each Monday (next
day if State holiday) for Claims processed during the prior week. Weekly invoices shall
be specific to a given month with the last invoice possibly having less than a full seven
(7) Calendar Days to capture the period from the ending date of the previous invoice to
the end of the specific month.
c. All invoices shall set forth details specified by the Department to ensure a proper pre-
audit and post-audit. Details shall include, but not be limited to, an invoice statement
provided on vendor letterhead, an invoice number, the employer or client number, the
billing period, an invoice date, and addressed to the Department.
80. Readiness Assessment
The Department and/or its authorized third party auditor may conduct a readiness
assessment of specific claims or other areas of the vendor as determined by the
Department prior to the Effective Date. Such assessment may include, but shall not be
limited to, procedures, computer systems, claims files, customer service records, accounting
records, internal audits, and quality control assessments.
81. Quarterly Self Audits
Vendor shall perform at least quarterly internal audits on a statistically valid sampling of
claims with results reported to the Department quarterly. Results shall be used to validate
self-reported quarterly performance metrics for claims timeliness, processing accuracy,
payment accuracy and financial accuracy.
82. Audit of Host Plans/Reciprocal Agreements with Other Plans
Vendor shall provide one hundred percent (100%) transparency and audit ability for any
and all financial transactions related to claims incurred by our plan Members in or out-of-
network, and submitted by a provider, Member, or third party.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 70
83. Quality Assurance Reviews for the Auditors
On a regularly scheduled basis, vendor shall review its procedures and processes for
medical and pharmacy to assess quality performance on Claims, suspense, adjustments, as
well as customer service inquiries by phone, mail, e-mail, etc. At the time of the audit,
vendor shall advise the Department on how the following areas are handled to ensure
quality:
a. Technical
b. Claim turnaround times
c. Financials
d. Call center and customer service
e. Mailroom operations
f. Imaging/record retention
g. Claims processing
h. Invoices/invoice generation
i. Write-offs
j. Recovery of overpayments
k. Paper claims payments and reimbursements
84. SSAE 16 External Audit
The vendor shall, at its expense, undergo an annual audit in accordance with the AICPA
Statement of Auditing Standards, A.U. section 324-Reports on the Processing of
Transactions by Service Organizations, specifically reporting on the Policies and Procedures
Placed in Operation and Tests of Operating Effectiveness.
The report shall cover the twelve (12) month time period of July 1 through June 30 of each
year. Reports are due to the Department by October 1 each year following the twelve (12)
month time period of July 1 through June 30. The audit shall be performed by an
independent accounting/auditing firm. The vendor is required to provide prior timely notice
to the Department of the independent accounting/audit firm conducting the audit with the
Department being permitted to review and comment on the audit period and the
associated scope of the audit. The SSAE 16 Report shall be subject to the provisions in
Performance Guarantees.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 71
85. Audits
a. The vendor shall provide the Department and the Department's third party auditor at
least the following audit access, in addition to any other audit rights specified in the ITN,
the network information, the contract and the financial reply:
i. To audit any data necessary to ensure the vendor is complying with all contract
terms; such audit rights include but not are not limited to: 100% of claims data,
approved and denied utilization management reviews, clinical program outcomes,
appeals, and information related to the reporting and measurement of
performance guarantees.
ii. To perform ongoing post claims audits as allowed in subsection 110.12301(1),
Florida Statutes.
iii. To audit post termination;
iv. To audit more than once per year if the audits are different in scope or for
different services;
v. To perform additional audits during the year of similar scope if requested as a
follow-up to ensure significant or material errors found in an audit have been
corrected and are not recurring, or if additional information becomes available to
warrant further investigation; and
b. The vendor shall submit to ongoing real-time post-payment claims audits and an annual
audit of contractual compliance as deemed appropriate by the Department. The vendor
shall cooperate with requests for information, which includes, but is not limited to, the
timing of the audit, deliverables, data/information requests and the time to respond to
questions during and after the audit process. The vendor shall provide a response to all
audit findings within 15 days of delivery to the vendor, or at a later date if mutually
determined to be more reasonable based on the number and type of findings.
86. Audit Findings
a. Upon the discovery of any overpayment(s) that result in financial harm to the
Department, the vendor shall immediately reimburse the Department one hundred
(100%) of the total overpayment amount upon finalization of the audit. Overpayments
arising from audit findings are not to be offset from claims or administration experience
and must be paid separately.
b. If an audit finding determines that there are systematic issues affecting the adjudication
of claims related to the Plan, the vendor shall coordinate with the Department to

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 72
develop and immediately implement a corrective action plan subject to the
customization and approval of the Department.
87. Hospital Audits
a. The vendor agrees to perform hospital records audits (including clinical and billing
issues) on each hospital admission exceeding $50,000 in paid claims. In the event that
the number of claims exceeding $50,000 in paid claims represents less than 2% of all
hospital admissions, the vendor shall perform additional hospital records audits on
those claims less than $50,000 beginning with the highest paid amount and continuing
in decreasing order until at least 2% of all hospital admissions have been audited.
b. Vendor shall report such audit results and recoveries to the Department in accordance
with the Performance Guarantees section.
88. Data Remains Property of the Department
All claim records and eligibility data used by vendor relating to this contract shall remain the
property of the Department.
89. Fiduciary Responsibility
Vendor shall agree to assume Claim fiduciary responsibility, including appeals, for Claim
adjudication and defense of utilization review decisions.
90. Legal Defense
a. Vendor shall provide necessary legal defense and assistance as required in the event of
litigation for goods and services related to the performance of this ITN and/or contract.
b. Vendor shall cover all costs associated with legal defense in the event of Plan-related
litigation or any other litigation.
c. Vendor shall prepare and file all legal documents with Florida Office of Insurance
Regulation, Florida Agency for Health Care Administration, and other agencies as
necessary to implement and maintain the plan, including policies, amendments,
contracts, required state filings, and development of Summary Plan Description formats.
91. Disaster Recovery Plan
a. Vendor shall develop, implement, and maintain a disaster recovery plan and shall
submit a copy of such for review by the Department on or before the effective date of
this contract. At a minimum, the disaster recovery plan shall include daily backup of
Plan-related files/data, a contingency provision so that critical services are provided
within twenty-four (24) hours, and a fully operational provision so that all services are
provided within 48 hours of activating the disaster recovery plan at the same or better

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 73
level of service as before the disaster recovery plan was activated. Any changes to the
plan throughout the term of the contract must be sent to the Department.
b. Vendor shall conduct annual mock disaster recovery exercises to perform an annual test
of its recovery/backup systems. Vendor shall report the results of such exercises to the
Department by December 31 of each year.
92. Contract Termination
Vendor agrees that, upon contract termination or expiration, vendor pays the cost of all
work required by a new administrator to bring its data and records in unsatisfactory
condition up to date and such expenses shall be reimbursed by vendor within three (3)
months of the end of the contract term. Department shall make final determination
regarding the condition of data and vendor's obligation under this provision.
Vendor shall continue to process and adjudicate run-out claims in accordance with the
terms of this contract and perform any related necessary claim services including medical
review and adjustments, customer service activities, Department and Auditor General audit
and support services, banking activities, including the continued transmission of related
data files to the Department and its third-party vendors, and any other mutually agreed
upon activities through the end of the 16-months following the effective date of
termination of the contract.
93. Services after Contract Termination
As mutually agreed upon by the Department and the vendor, vendor shall continue to
provide the following services to ensure that the contractually required services resulting
from this ITN are maintained at the required level of proficiency for up to sixteen (16)
months following the effective date of termination of the contract.
a. Mailroom services
b. Appeals services
c. System/technical services
d. Claim entry, adjudication and adjustments based on Summary Plan Description
e. Coordination of benefits
f. Subrogation tasks
g. Customer service and call center operations
h. Medical review as necessary

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 74
i. Issue payments/checks and Explanation of Benefits Statements
j. Collection of overpayments
k. Banking activities
l. Reports
m. The Department and Plan Members shall continue to have the same current online
system access to information
n. Other tasks as required by the Department.
All claim records including all data elements of such electronic claim records and eligibility data used by relating to this contract shall remain the property of the Department and shall be provided to the Department immediately upon contract termination and at the end of the 16-month period following termination of the contract.
94. Compliance with Law
Vendor shall monitor federal and state legislation affecting the delivery of medical and
prescription drug benefits under the Plan and promptly report to the Department on those
issues prior to the effective date of any mandated Plan changes. In addition, vendor shall
provide the Department with interpretation as to the impact of such laws or regulations on
the Plan. Vendor shall absorb the cost of programming all benefit design changes.
95. Online Reporting and Management Tools
a. Vendor shall provide for unlimited users of the Department, at no additional cost, online
user access to its reporting and management services, systems, programs, current and
historical other covered liability, customer service call and correspondence notes and
logs
b. Vendor shall provide corresponding manuals and any other printed or digital material or
CIDs used in connection with the systems. This online tool shall have data accumulation,
claims specific and ad hoc reporting capabilities.
c. Vendor shall, upon request of the Department, provide Department staff with training
at the Department’s facilities for the online reporting and management tools.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 75
Section 7 Corporate Information
Instructions: Please provide a response to the following questions. The vendor’s response to
this section will not be scored. However, this section will be reviewed to determine if the
vendor’s reply conforms in all material respects to this solicitation and to determine the
vendor’s responsibility.
Vendors must copy and paste without modification both the statement and box below into
their replies. Describe vendor’s current accreditation status.
1. Provide an organizational chart identifying the names, area of expertise, functions, and
reporting relationships of key people directly responsible for implementing the State of
Florida account.
2. Provide the name of the person with primary responsibility for planning, supervising, and
implementing the program for the State.
a. What other duties, if any, will this person have during implementation? Please include
the number and size of other accounts for which this person will be responsible for
during the same time period.
b. What percentage of this person's time will be devoted to the State during the
implementation process?
4. Provide an organizational chart identifying the names, functions and reporting relationships
of key people directly responsible for account support services to the State.
5. Provide the name of the person with primary responsibility for planning, supervising, and
performing account services for the State.
a. What other duties, if any, does this person have? Please include the number and size of
other accounts for which this person is responsible.
b. What percentage of this person's time will be devoted to the State?
c. Describe the role and support by the account manager for the annual open enrollment
process (i.e. meetings, communications, implementation of plan design changes,
modification and updating of files, etc.)
6. Describe how many account executives and group services representatives will work full-
time on the State's account, and how many will work part-time on the State's account.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 76
7. Provide a copy of vendor's most recent financial ratings and complete the following table,
as applicable:
A.M. Best
Standard & Poor’s
Dunn and Bradstreet
Fitch Weiss Moody
Current Financial Rating
Date of Rating
Prior Financial Rating
Date of Rating
If such ratings are not available for the vendor, vendor must submit its two most recent audited
financial statements.
8. Provide a profile of vendor's HMO business for each of the latest three calendar years
(2012, 2013 and 2014).
Calendar Year 2012
Calendar Year 2013
Calendar Year 2014
Total premium volume
Total number of clients
Total number of Enrollees covered
Number of public sector clients
Average size of public sector clients
Number of public sector Enrollees
Number of claims handled
Number of plans terminated
Average size of terminated plans
9. Disclose all interests of key personnel, including officers, medical directors, board members
or significant shareholders who have any ownership or management interest in any
network affiliate.
10. Describe, to the best of vendor's knowledge, any acquisitions or mergers in which vendor is
expected to be involved within the next twelve (12) months.
11. Describe any and all acquisitions or mergers in which vendor was involved within the last
five (5) years.
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 77
12. For the performance of services similar to those required in this ITN, has vendor ever been
notified of or been declared in breach or default of a contract; received written notice that
it was considered to be in breach or default; or been defaulted on a contract with any other
business entity?
If so, provide the particulars, including when, where, which parties were involved, what
occurred, and the ultimate outcome.
13. Has vendor ever been issued a letter of non-compliance on a contract involving services
similar to those required in this ITN?
If so, advise when, where and the ultimate outcome of such actions.
14. Has vendor ever terminated or given notice of termination of any contract for which it
performed services similar to those required in this ITN?
If so, provide the particulars, including when, where, which parties were involved, what
occurred, and the ultimate outcome.
15. Has vendor ever received notice of termination or have had a contract terminated by the
other party for which it performed services similar to those required in this ITN?
If so, provide the particulars, including when, where, which parties were involved, what
occurred, and the ultimate outcome.
16. Has vendor ever been assessed or paid liquidated damages/performance credits or any
other type of penalty for failure to meet performance metrics regarding the performance of
services similar to those required in this ITN?
If so, advise when, where, the amount(s) paid and the outcome of such actions.
17. Describe any discipline, fines, litigation and/or government action taken, threatened or
pending against vendor or any entities of vendor during the last five (5) years regarding the
performance of services similar to those required in this ITN. This information must include
whether the vendor has had any registrations, licenses, and/or certifications suspended or
revoked in any jurisdiction within the last five years, along with an explanation of
circumstances.
18. Identify and describe all data security incidents related to unauthorized access of client or
member data or unauthorized physical access to the data center experienced within the last
five years. Explain how the organization handled such incidents.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 78
Section 8 Vendor and Subcontractor Information
The vendor’s response to this section will not be scored. However, this section will be reviewed
to determine if the vendor’s reply conforms in all material respects to this solicitation and to
determine the vendor’s responsibility.
Instructions: Provide a response to each requested item below
A. Vendor General Information
Company Information Response
Vendor’s legal name
Address
City
State
ZIP Code
Web address
Corporate tax status
Federal Employer
Identification Number
(FEIN)

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 79
B. Contact Information
Identify the primary contact person responsible for the overall development of the vendor’s
reply.
Primary Contact Response
Name
Title
Address
City
State
ZIP Code
Telephone number
Email address

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 80
C. Executive Sponsor
Provide the following information regarding the Executive Sponsor that will be assigned to
the State’s account. This individual is the highest ranking officer with direct involvement in
the State’s account. In addition, submit a resume or curriculum vitae as Reply Attachment
8C for the Executive Sponsor below.
Executive Sponsor Response
Name
Title
Address
City
State
ZIP Code
Telephone number
Email address
Years of HMO and/or TPA
industry experience
Years with the organization
Years in the current
position
Proposed percent of time
dedicated to the
Department
Number of HMO and/or
TPA clients, and size of
accounts

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 81
D. Account Manager
Provide the following information regarding the Account Manager that will be assigned to
the State’s account. This individual provides oversight of account services for the State. In
addition, submit a resume or curriculum vitae as Reply Attachment 8D for the Account
Manager below.
Account Manager Response
Name
Title
Address
City
State
ZIP Code
Telephone number
Email address
Years of HMO and/or TPA
industry experience
Years with the organization
Years in the current
position
Proposed percent of time
dedicated the Department
Number of HMO and/or
TPA clients, and size of
accounts

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 82
E. Account Management Team Members
Provide the following information regarding the account management team that will be
assigned to the State’s account (add additional tables as needed for this response). In
addition, submit a resume or curriculum vitae as Reply Attachment 8E for each account
management team member below.
Account Management
Team Member Response
Name
Title
Address
City
State
ZIP Code
Telephone number
Email address
Years of industry
experience
Years with the
organization
Years in the current
position
Proposed percent of
time dedicated to State
of Florida Plan
Number and size of
other accounts
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 83
F. Implementation Manager
Provide the following information regarding the implementation manager that will be
assigned to the State’s account. In addition, submit a resume or curriculum vitae as Reply
Attachment 8F for the implementation manager below.
Implementation Manager Response
Name
Title
Address
City
State
ZIP Code
Telephone number
Email address
Years of industry experience
Years with the organization
Years in the current position
Proposed percent of time
dedicated to the State of
Florida Plan
Number and size of other
accounts
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 84
G. Customer Service Manager
Provide the following information regarding the customer service manager that will be assigned
to the State’s account. In addition, submit a resume or curriculum vitae as Reply Attachment
8G for the customer service manager below.
Customer Service Manager Response
Name
Title
Address
City
State
ZIP Code
Telephone number
Email address
Years of industry experience
Years with the organization
Years in the current position
Proposed percent of time
dedicated to State of Florida
Plan
Number and size of other
accounts

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 85
H. Analyst
Provide the following information regarding the financial analyst that will be assigned to the
State’s account. In addition, submit a resume or curriculum vitae as Reply Attachment 8H
for the analyst below.
Analyst Response
Name
Title
Address
City
State
ZIP Code
Telephone number
Email address
Years of industry experience
Years with the organization
Years in the current position
Proposed percent of time
dedicated to State of Florida
Plan
Number and size of other
accounts
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 86
I. Medical Director
Provide the following information regarding the medical director that will be assigned to the
State’s account. In addition, submit a resume or curriculum vitae as Reply Attachment 8I
for the medical director below.
Medical Director Response
Name
Title
Address
City
State
ZIP Code
Telephone number
Email address
Years of industry experience
Years with the organization
Years in the current position
Proposed percent of time
dedicated to State of Florida
Plan
Number and size of other
accounts

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 87
J. Subcontractors
Provide responses below for each Subcontractor that the vendor proposes to perform any
of the required Services under the contract. Copy and insert additional tables as needed.
Information Subcontractor #1
Subcontractor Name
Corporate address, telephone
number and website
Office address, telephone
number and website of the
proposed Subcontractor that
will be performing any of the
required services under the
contract
Federal Employer
Identification Number
(Employer ID or Federal Tax
ID, FEID)
Occupational license number
(if applicable)
W-9 Verification
Primary contact person name,
address, email address and
telephone number
Brief summary of the history
of the Subcontractor's
company and information
about the growth of the
organization on a national
level and within the State of
Florida
Describe any significant

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 88
government action or
litigation taken or pending
against the Subcontractor's
company or any entities of
the Subcontractor's company
during the most recent five
years
List and describe the Services
the Subcontractor will be
responsible for in the
performance of the contract
Explain the process for
monitoring the performance
of the Subcontractor and
measuring the quality of its
results.
What procedures does
vendor have in place to
ensure Subcontractor
compliance with HIPAA
requirements?
Describe the process that
vendor will implement during
the contract term to ensure
that background checks (as
described in the contract) will
be completed on the
Subcontractor.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 89
K. References
Provide at least four (4 ) references as follows:
The two largest public sector clients for whom the vendor currently provides similar
services to those sought in this ITN.
The two largest former clients (public or private sector) for whom the vendor provided
similar services to those sought in this ITN.
The Department will contact each reference. The vendor does not need to send the
reference form to its references.
References will not be accepted from:
Current employees of DMS.
Former employees of DMS within the past three (3) years.
Persons currently or formerly employed by the vendor’s organization.
Board members of the vendor’s organization.
Relatives.
Corporations based solely in a foreign country.
A member of the vendor’s organization, who has written, completed and submitted the form on behalf of the reference.
Vendors should complete the each following table in its entirety.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 90
Information Reference #1
Company Name
Contact Person
Title
Address
City
State
Telephone Number
Email Address
Size of Account/
Covered Lives
Contract Period
Brief Summary of
Services

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 91
Information Reference #2
Company Name
Contact Person
Title
Address
City
State
Telephone Number
Email Address
Size of Account/
Covered Lives
Contract Period
Brief Summary of
Services

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 92
Information Reference #3
Company Name
Contact Person
Title
Address
City
State
Telephone Number
Email Address
Size of Account/
Covered Lives
Contract Period
Brief Summary of
Services

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 93
Information Reference #4
Company Name
Contact Person
Title
Address
City
State
Telephone Number
Email Address
Size of Account/
Covered Lives
Contract Period
Brief Summary of
Services

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 94
Section 9 Technical Information
Instructions: Provide a response to each of the following Technical reply questions and
requests for information by restating the item and providing vendor’s response below the item
in at least 11 pt Calibri, Arial or Times New Roman blue font. Failure to submit a response to a
question or request for information may disqualify the vendor from further consideration.
This section will be scored pursuant to subsection 4.3.1 (“Scoring of Technical Information”) of
this ITN.
1. Describe the characteristics of vendor’s business model, health management, network
management and any other operational functions that set vendor apart from other
vendors. Topics may include, but are not limited to:
a. The approaches and value enhancements vendor offers that could mean best value for
the State;
b. Centers of excellence, transplant networks and other health care arrangements that
focus on quality of care and cost avoidance;
c. How vendor maximizes the use of State of Florida residents, state products (produced
and/or purchased within the State of Florida) and other Florida-based businesses in
delivering the Services; and
d. Expectations for the future direction of the organization.
2. Describe vendor's experience in providing health plan benefits. Topics may include, but are
not limited to:
a. Type of health plan administered and complexity/customization of the health plan;
b. Governance model;
c. Number of lives covered;
d. Types of clinical, disease, and utilization management programs; how candidates are
determined; level of participation in such programs and their impact on health risk and
cost containment;
e. After hours care (e.g., nurse line, urgent care centers)
f. How administering a self-insured plan differs from administering vendor’s insured
blocks; and
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 95
g. Options for members outside of the network.
3. Describe vendor's network development model and contracting strategy in Florida. Topics
may include, but are not limited to:
a. Impact to the vendor’s network by taking on the State’s covered population;
b. Discounts and average reimbursement rates;
c. Impact of geography on network discounts;
d. Stability of the network (e.g., annual physician turnover – gross, not net of additions);
e. The provider credentialing process;
f. Provider quality measures and controls;
g. How provider satisfaction is measured;
h. Reasons for member dissatisfaction with the network or providers, steps taken to
improve or correct such reasons and how the level of member satisfaction prompts
changes in the network contracting strategy; and
i. If reply includes rental networks: how, where and how long rental networks have been
used; “a” through “h” of this question for rental networks; and cost containment
monitoring and strategies for rental networks.
4. Describe the protocols in place that ensure personal health information remains secure.
Topics may include, but are not limited to:
a. Monitoring of all electronic systems and personnel;
b. Established processes and fail safes to mitigate breaches;
c. Resolution, notification and reparation protocols when a breach is discovered;
d. Protocols that ensure no offshoring of or offshore access to any protected data; and
e. Security protocols for call center employees, correspondence tracking system and
process, and electronic systems that access or store protected data.
5. Describe the customer service call center. Topics may include, but are not limited to:
a. Location of call center, hours of operation, and number of representatives assigned to
State’s account;

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 96
b. Training, minimum qualifications, experience and turnover of representatives;
c. Languages customer service unit can support (other than English) and how that support
is provided (i.e., language line or vendor call center representatives);
d. Year-to-date call targets and actual statistics (e.g., abandonment rate, speed to answer);
e. Call recording system; documentation of calls; and timeframe and manner to furnish call
recordings or notes to the department;
f. Online chatting, email capabilities, and other electronic access capabilities;
g. Customer satisfaction survey methodology and recent survey with results from a group
similar in size and composition to the State;
h. Any quality improvement activities initiated as a result of Enrollee satisfaction surveys;
i. Explain whether customer service representatives will be dedicated and exclusive. If not,
explain the ratio of representatives to Members.
j. Describe the services Members can access via the web, smartphone applications or
other electronic devices?
6. Describe claims processing. Topics may include, but are not limited to:
a. Training, minimum qualifications, experience and turnover of medical claims processors;
b. Location of claims administration office, and number of processors assigned to this
account and if these claims processors can be an exclusively dedicated unit;
c. Year-to-date targets and actual statistics for clean claims processing turnaround time
and accuracy;
d. Threshold under which claims processors can approve a claim for payment;
e. Coordination of benefits process, including with Medicare and worker’s compensation;
f. Methodology for reimbursing a non-participating hospital-based provider (radiologists,
pathologists, anesthesiologists, emergency room physicians, neo-natal physicians, etc.);
g. Protocols and/or tools to ensure claims are processed accurately and timely;
h. Ability to recognize fraudulent claims, abuse and other fraudulent actions and vendor’s
process for addressing:
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 97
i. The procedure for handling emergency admission requests;
j. Describe vendor's procedures for handling and resolving claim inquiries from Members;
k. Describe vendor's procedures for handling and resolving claim inquiries from the
Department;
7. Describe clinical services. Topics may include, but are not limited to:
a. Training, minimum qualifications, experience and turnover of the case management
staff assigned to the this account;
b. Case management model and processes;
c. How the case management program integrates with other care management programs
such as utilization review and quality management; and
d. Accreditations vendor’s care management program currently holds, or is in the process
of pursuing.
8. Provide a detailed Implementation Plan that clearly demonstrates the vendor's ability to
meet the Department's requirements to have a fully functioning program in place and
operable on January 1, 2017.
a. Include a list of specific implementation tasks/transition protocols and a time table for
initiation and completion of such tasks, beginning with the contract award and
continuing through the effective date of operation (January 1, 2017). The
Implementation Plan should be specific about requirements for information transfer as
well as any services or assistance required from the State during implementation.
b. Indicate the critical dates that must be met to keep the Implementation Plan on
schedule. Include the processes that shall be reviewed, including system testing,
information required from the incumbent, historical claims data and format, and plan
documents.
c. Describe any anticipated major transition issues during implementation.
d. Describe vendor's procedures and processes for handling transition of care during the
transition period for the new contract.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 98
Section 10 Service and Program Information
Instructions: Provide a response to the following questions and requests for information.
Failure to provide response to any request below may result in rejection of the vendor’s reply.
The vendor’s response to this section will not be scored.
SUPPORT SERVICES
1. Provide a sample of a new Enrollee communications package in section 10 of the reply,
including how to locate providers, how to use network services and how to access
member services.
2. How many written complaints/grievances were received by vendor per 1,000 Enrollees
during 2014, what were the top five, and how were they resolved?
3. Provide a complete description (including a flowchart) of vendor's proposed 2017
member appeals process for medical services including external reviews.
NETWORK ACCESS MANAGEMENT
4. Provide vendor's average historical discount rates for the following provider types, for
the proposed HMO network:
Calendar Year 2013
Calendar Year 2014 Calendar Year 2015
through July 31
Primary Care
Physicians
Obstetricians and
Gynecologists
Pediatricians
Other Specialists
Acute Care Facilities
Urgent Care Facilities
Hospitals

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 99
5. Provide a profile of vendor's business in Florida for the last three (3) calendar years:
Calendar Year 2012 Calendar Year 2013 Calendar Year 2014
Number of Primary
Care Physicians
Number of
Obstetricians and
Gynecologists
Number of
Pediatricians
Number of Other
Specialists
Number of Acute
Care Facilities
Number of Urgent
Care Facilities
6. For vendor's proposed network for the State, what percent of participating primary care
physicians and specialists are currently closed to new patients?
7. For vendor's proposed network for the State of Florida, what percent of participating
PCPs and specialists were closed to new patients for Calendar Year 2014?
8. Explain how a provider can be nominated to be considered for inclusion in the network.
9. What percentage of network PCPs are board certified?
10. What percentage of network specialists are board certified?
11. Describe any ongoing or upcoming provider and facility contract negotiations that may
result in a network change over the next 12 months.
12. Describe how vendor monitors waiting times for patients seeking appointments,
including the average number of working days between the date an appointment is
made and the date of the actual visit for both non-emergency care and urgent care.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 100
13. Describe the vendor's specialist referral process.
14. Do network physicians (or their staff) assist in arranging for services such as home
health care, hospice, skilled nursing, durable medical equipment and mental
health/chemical dependency? If yes, describe the process and their roles including how
often vendor meets to educate physician staff on pre-certification/pre-authorization
requirements and other Plan-specific benefits and processes.
15. Describe the procedures to be used to ensure that hospital-based physicians (radiology,
anesthesiology, emergency, pathology, etc.) are paid at the negotiated hospital based
network pricing.
16. Describe, if applicable, any financial incentives or disincentives to network providers
that are tied to utilization goals, specialty referrals, quality of care outcomes, or other
performance results and include risk sharing arrangements. Explain how financial
incentives are paid, if applicable.
17. Describe any penalties to which providers will be subject for failure to pre-certify non-
emergency admissions.
18. Describe any other penalties to which providers will be subject for failure to adhere to
utilization management policies.
19. How much notice are providers contractually required to give if they elect to terminate
a contract with vendor?
20. What happens to Members receiving ongoing treatment from a network provider who
elects to terminate a contract with vendor?
21. Describe what actions are taken to recruit individual providers or another group practice
for the network in place of terminated providers, including how often vendor initiates a
needs assessment.
22. Explain if vendor anticipates changes in 2017 reimbursement policies for out-patient,
free-standing facilities; inpatient hospital; or laboratory services.
23. What utilization controls are in place with vendor’s network providers to reduce the
number of unnecessary services being performed?
24. What happens in the self-funded scenario when a hospital based non-participating
provider administers services?

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 101
25. Describe the procedure in place for covering emergency care services performed by
non-network facilities.
26. Describe vendor's process to perform provider profiling or other quality measures to
identify providers with patterns of over/under treatment to Enrollees and the actions
taken to address such patterns.
27. Explain if vendor has any ownership interest in or if vendor is involved in the operations
of any network outpatient facilities.
28. Explain if vendor partially owns, or subcontracts any part of vendor's network (i.e.
chiropractic, behavioral health, etc.). If yes, describe.
MENTAL HEALTH/SUBSTANCE ABUSE
29. Does the vendor subcontract for mental health/substance abuse care? If yes, identify
the organization and provide a detailed description of their program and vendor's
relationship to the Subcontractor.
30. Provide a detailed description of the mental health/substance abuse access and triage
process.
31. Describe vendor's mental health/substance abuse case management service from
structural and functional perspectives and how these lend to long-term stability of an
Enrollee.
TRANSPLANT NETWORK
32. Describe how vendor handles transplants (i.e., through a transplant network or vendor's
network).
33. Describe how Members access the transplant network (i.e., physician referral, utilization
or medical management review, direct access).
34. Provide a list of transplant procedures available within the network.
35. Describe how transplant costs are monitored and mitigated.
CENTERS OF EXCELLENCE
36. Describe all high-risk and/or high-technology services coordinated with the Centers of
Excellence. Provide the names and locations for vendor's top five (5) Centers of
Excellence by volume.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 102
37. How are patients utilizing Centers of Excellence case managed? (i.e. Are they
coordinated separately from other catastrophic cases?)
38. What are the financial arrangements for the Centers of Excellence?
39. Specify if the vendor is aware of any changes in the coming year to vendor's current
Centers of Excellence arrangements.
DATA PROCESSING / INTERFACE
40. Describe vendor's system update process.
41. Describe any electronic system changes planned for the contract term.
42. How often are the systems backup and disaster recovery procedures tested?
43. When were the systems last tested and what were the results?
42. Describe how claims, customer service, case management, and utilization review
systems are linked.
43. Describe how vendor's claims system automatically matches claims with utilization
management information.
44. Describe vendor's online reporting tool ad hoc reporting capabilities.
45. Explain the vendor’s process for routine maintenance of all systems to be used for this
contract.
CLINICAL SERVICES
46. Provide (as attachments) biographies of the medical management staff to be assigned
to this account.
47. What is the nurse/patient ratio for the utilization and case management programs?
48. Describe the access Members have to a nurse-line for counseling/support.
WELLNESS PROGRAM
49. Describe any program offerings vendor's organization has for health/fitness promotions
that can be provided at no additional cost to the State and comply with current plan
design and Florida law.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 103
50. Describe any program offerings vendor's organization has for health
assessment/screening, which can be provided at no additional cost to the State and
comply with current plan design.
51. Describe any program offerings vendor's organization has for wellness, which can be
provided at no additional cost to the State and comply with current plan design.
DISEASE MANAGEMENT
52. Describe each disease management program, how Members are identified and
contacted for participation, and Member access to support services.
53. Describe how reminders are sent to patients and/or physicians to encourage
appropriate health actions.
54. Describe how vendor will transition Enrollees who are undergoing treatment for chronic
and/or catastrophic conditions to vendor's plan.
QUALITY OF CARE
55. Describe how vendor measures the quality of care received by its Enrollees.
56. Describe any quality improvement initiatives undertaken in the last twelve (12) months.
57. Describe vendor's approach to assessing the effectiveness of its Quality Management
programs for both clinical services within the network and administrative operations of
the health plan.
58. Describe the role and content of quality management training programs for health plan
staff, providers and their administrative staffs.
AUDITS
59. Describe vendor's policy and procedures for auditing hospital bills/claims.
60. Describe vendor's internal audit staff duties, how frequently internal are audits
performed, and the frequency for which claims processing function audits are
performed by an external auditing firm.
61. Overall, what percent of claims are subject to internal audit?
62. What is the typical audit size?

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 104
63. Describe in detail how are claims selected for audit (e.g., random by the system, fixed
percent per day, fixed number per day per week, diagnosis, dollar amount).
64. Describe vendor's method of selecting claims for internal quality review.
65. Describe any processor actions and/or claim characteristics that automatically trigger a
review.
66. What percentage of claims is reviewed on a daily basis for accuracy of payment?
SUBROGATION
67. Describe in detail vendor’s subrogation processes and procedures.
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 105
Section 11 Recommended Solutions and Alternatives
Instructions: Provide a response to the following questions and requests for information.
Failure to provide response to any request below may result in rejection of the vendor’s reply.
The vendor’s response to this section will not be scored. This ideas and items submitted by
vendors in response to this section may be used during negotiations.
1. Provide any proposed service alternatives or recommendations to improve the delivery
of services to Members, for example, telemedicine, accountable care organizations,
centers of excellence, etc.
2. As allowed under current law, propose innovative approaches the Department could
consider to manage member health risk and mitigate rising health care costs. Discuss
cost, return on investment based on actual experience in vendor’s book of business and
impacts on member health based on vendor’s book of business medical claims
experience trend.
3. Provide a discussion of vendor's willingness and experience in implementing, staffing,
and maintaining an on-site clinic.
4. If replying for a fully-insured arrangement, describe vendor’s pharmacy benefits
management program. Briefly discuss the following topics
a. Name of vendor’s contracted pharmacy benefits manager (PBM), if applicable;
b. Which pharmacy management services are performed in-house, if any, and those
out-sourced to the PBM;
c. The type of preferred drug list (open, partially restricted or closed), and explain the
medical necessity approval process;
d. Types and impacts of pharmacy management protocols (e.g., step therapy and prior
authorization) on prescription drug costs and medical costs;
e. How prescription drug information is integrated into a managed care approach,
including how data is stored, what outcomes can be tracked, how results can be
reported (with respect to each medical condition;
f. How physician prescribing is managed; and
g. How insuring the pharmacy benefits would provide best value to the State and to
Members.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 106
5. If replying for a fully-insured arrangement, describe vendor’s experience providing
Medicare Advantage Prescription Drug (MAPD) plans in Florida. Briefly discuss the
following topics:
a. Vendor’s ability to offer the State’s Plan;
b. Counties in which the MAPD is available; and
c. The most recent CMS plan quality and performance ratings.
6. If replying for a fully insured arrangement, based on the targeted loss ratios provided in
Attachment C-5, briefly describe the vendor’s policy on reimbursing the State for a Plan
Year, if any, in which the actual loss ratio is less than the targeted loss ratio proposed.
Describe how the timing and amount of reimbursement are determined.
7. If replying for a self-insured arrangement, provide a discussion of vendor's experience in
establishing contract terms based off of vendor-calculated claims target guarantee and
risk corridor. By way of example from the current PPO TPA contract:
a. Projected and Target Claims Cost Vendor’s Projected and Target Claims Cost is based on the following Enrollee
types: (i) Active Employees, (ii) Early Retirees, (iii) Medicare eligible Retirees, and
(iv) COBRA. The Projected and Target Claims Cost includes in-network and out-
of-network claims, and excludes prescription drugs (except for those drugs
included in medical claims).
For each Plan Year after 2017, the Projected and Target Claims Cost will be
based on the actual total paid claims incurred in the prior Plan Year for all
Members by Enrollee type plus the Paid Claims Expected Trend.
Projected and Target Claims Costs (aggregate dollars) = Active + Pre-Medicare +
Medicare + COBRA.
b. Allowable Adjustment Factors Allowable Adjustment Factors will be used to develop mutually agreed upon
annual adjustments to the Paid Claims Expected Trend for each subsequent
Plan Year based on changes in enrollment, demographics and plan changes
which may impact total paid claims.
c. Paid Claims Expected Trend The amount of trend used to determine the claims target will be based, in part,
on the trend letter provided by the vendor to the Department for the Estimating

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 107
Conference held in either January or February of the respective Plan Year. The
trend letter will be based on claims paid in the previous Plan Year. The Parties
will use the Allowable Adjustment Factors and the trend letter to develop a
mutually agreed upon “Paid Claims Expected Trend.”
d. Claims Target Guarantee No later than March 31 of the respective Plan Year, the vendor shall provide a
Claims Target Guarantee for the respective Plan Year (using the Projected and
Target Claims Cost and mutually agreed upon Paid Claims Expected Trend) on a
total aggregate basis. Medicare Subscribers shall not be included in the Claims
Target Guarantee.
The Claims Target Guarantee will be assessed annually based on the receipt of
the Annual Claims Target Guarantee Report. The PEPM basis guarantee
amount will be calculated by dividing the aggregate Claims Target Guarantee
by the average actual enrollment for the preceding Plan Year. The Department
will compute (excluding Medicare as noted above) the actual paid claims and
divide by the average actual enrollment for the preceding Plan Year to
establish the “Realized PEPM Claims.” The risk corridor established by the
Claims Target Guarantee will be compared to the Realized PEPM Claims. If the
Realized PEPM Claims exceed the risk corridor of the Claims Target Guarantee,
the vendor shall remit the appropriate amount to the Department no more
than 15 Calendar Days after the receipt of the annual report.
i. Vendor Calculations
Claims Target Guarantee = Projected and Target Claims
Cost (Active + Early Retiree + COBRA Only) + Paid Claims
Expected Trend (Delivered in January or February)
Risk Corridor = Claims Target Guarantee * Risk Corridor (Delivered to
Department by March 31 of Plan Year)
Risk Corridor (PEPM) = Risk Corridor / Actual Average
Enrollment (Enrollees) (Computed after end of Plan Year)
ii. DSGI Calculations
“Realized PEPM Claims” = (Actual Spend for Plan Year –
Claims amounts over $750,000)/ Actual Average Enrollment
(Enrollees) (computed after end of Plan Year)
If “Realized PEPM Claims” > Risk Corridor (PEPM); Multiply the amount

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 108
in excess of the risk corridor (PEPM) by Average Actual Enrollment and
vendor is responsible to remit entire amount above the risk corridor to
Department, limited to a maximum of percentage of the
Administrative Fees paid in the respective Plan Year.
8. If replying for a self-insured arrangement, provide a discussion of vendor's experience in
establishing contract terms for average network discounts for each of the primary
categories: inpatient facility, outpatient facility, specialist, primary care, and ancillary
services.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 109
Section 12 Network Information
Instructions: Provide the information required in Attachment B-1 through B-7. Failure to
provide the information requested below may result in rejection of the vendor’s reply. The
vendor’s response to this section will be scored.
Vendors are required to submit fully completed Attachment Forms B-1 through B-7 in native
file format on a CD-ROM or “thumb drive.” Please follow the instructions in Attachment B.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 110
Section 13 Financial Reply
Instructions: Provide the information required in Attachment C. Failure to provide the
information requested will result in rejection of the vendor’s reply. The vendor’s response to
this section will be scored.
Vendors are required to submit fully completed Attachment Forms C-1 through C-7 in native
file format on a CD-ROM or “thumb drive.” Please follow the instructions in Attachment C.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 111
Section 14 Purchasing Forms
The following forms (Form 1 and Form 2) included in this section must be completed and
attached in their entirety with the signature of the vendor’s authorized agent and included in
Tab 14. Failure to complete, sign, and/or return these documents with replies by the
submission deadline may result in rejection of the reply.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 112
Form 1: Vendor Certification
As the person authorized to sign on behalf of ___________________________________
[vendor name], I certify the following.
1. The above-named vendor understands that all information provided by and
representations made by the vendor are material and will be relied on by the
Department in awarding the contract. The Department reserves the right to investigate
all representations and any other information the Department deems pertinent. Any
misstatement will be treated as fraudulent concealment from the Department of true
facts relating to the submission of the reply. A misrepresentation will be punishable by
law, including but not limited to chapter 817, Florida Statutes. Accordingly, all
information and representations contained in this reply are true and accurate to the
best of my knowledge, and no modifications have been made to this ITN section 14
forms submitted with the vendor’s reply.
2. The above-named vendor has not been placed within the last thirty-six (36) months on
the Department’s Convicted vendor List or on a similar list maintained by any other
governmental entity.
3. The above-named vendor is not currently under suspension of debarment by the State
of Florida or any other governmental entity.
4. The above-named vendor and its affiliates, subsidiaries, directors, officers, and
employees are not currently under any known investigation by any governmental
authority and have not in the last ten (10) years been convicted or found liable for any
act prohibited by law in any jurisdiction involving conspiracy or collusion with respect to
bidding on any public contract.
5. The above-named vendor has not been defaulted by the State of Florida under any
contract.
6. The above-named vendor has fully informed the Department in writing of all convictions
of the vendor; its affiliates (as defined in subsection 287.133(1)(a), Florida Statutes); and
all directors, officers, and employees of the firm and its affiliates for violation of state or
federal antitrust laws with respect to a public contract for violation of any state or
federal law involving fraud, bribery, collusion, conspiracy, or material misrepresentation
with respect to a public contract. This includes disclosure of the names of current

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 113
employees who were convicted of contract crimes while in the employ of another
company.
7. Neither vendor nor any person associated with it in the capacity of owner, partner,
director, officer, principal, investigator, project director, manager, auditor or position
involving the administration of federal funds:
a. Has within the preceding three (3) years been convicted of or had a civil judgment
rendered against them or is presently indicated for or otherwise criminally or civilly
charged for commission of fraud or a criminal offense in connection with obtaining,
attempting to obtain or performing a federal, state or local government transaction
or public contract; violation of federal or state falsification or destruction of records,
making false statements or receiving stolen property; or
b. Has within a three-year (3) period preceding this certification had one or more
federal, state or local government contracts terminated for cause or default.
8. The submission is made in good faith and not pursuant to any agreement or discussion
with, or inducement from, any firm or person to submit a complementary or
noncompetitive reply.
9. Vendor has made a diligent inquiry of its employees and agents responsible for
preparing, approving or submitting the reply and has been advised by each of them that
he or she has not participated in any communication, consultation, discussion,
agreement, collusion, act or other conduct inconsistent with any of the statements and
representations made in the reply.
10. The prices and amounts have been arrived at independently and without consultation,
communication or agreement with any other vendor or potential vendor; neither the
prices nor the amounts, actual or approximate, have been disclosed to any vendor or
potential vendor and they will not be disclosed before the ITN opening.
11. No attempt has been made or will be made to induce any firm or persons to refrain
from submitting a reply for the contract, or to submit a price(s) higher that the prices in
this reply, or to submit any intentionally high or noncompetitive price(s) or other form
of complementary reply.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 114
_________________ , its affiliates, subsidiaries, officers, director, and employees
(Name of Firm)
are not currently under investigation, by any governmental agency and have not in the
last three years been convicted or found liable for any act prohibited by state or federal
law in any jurisdiction, involving conspiracy or collusion with respect to the reply, on any
public contract, except as follows:
Signature of Authorized Representative:
Name:
Title:
Date: , 2015
Mailing Address:
Email Address:
Telephone:

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 115
Form 2: Notice of Conflict of Interest
Company or Entity Name
For the purpose of participating in the solicitation process and complying with the provisions of
chapter 112 of the Florida Statutes, the undersigned corporate officer states as follows:
The persons listed below are corporate officers, directors or agents and are currently
employees of the State of Florida or one of its agencies:
The persons listed below are current State employees who own an interest of ten percent or
more in the company/entity named above:
Dated this day of 2015.
Name of Organization:
Signed by:
Print Name
being duly sworn deposes and says that the information herein is true and sufficiently
complete so as not to be misleading.
Subscribed and sworn before me this day of 2015.
Notary Public:
My Commission
Expires:

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 116
Section 15 Attachments
Following are the attachments to this ITN:
Attachment A: Draft Contract – provided as a separate document
Attachment B: Network Information – provided as a separate spreadsheet
Attachment C: Financial Reply – provided as a separate spreadsheet
Attachment D: Census File – see subsection 1.8 of the ITN regarding how to obtain this
file
Attachment E: Confidentiality and Non-Disclosure Agreement – included in this section
Attachment F: Notice of Intent to Submit a Reply – included in this section
Attachment G: Claims Utilization – see subsection 1.8 of the ITN regarding how to obtain
this file
Attachment H: Covered Benefits and Services – included in this section

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 117
Attachment E: Confidentiality and Non-Disclosure Agreement
This Confidential and Non-Disclosure Agreement (the “Agreement”) is made this ____ day of ______
2015, by and between ____________________________________ hereinafter referred to as “the
vendor” and the State of Florida Department of Management Services, hereinafter referred to as “the
State.”
The vendor warrants and represents that it intends to submit a Reply in response to the State
solicitation entitled ITN No. DMS 15/16-005 HMO Services (ITN). The State must provide the Vendor
with access to certain confidential information (Confidential Information) including, but not limited to,
demographic and identifying information on the State’s eligible member population and plan utilization
data related to this procurement. This information includes data that is considered Protected Health
Information as defined in 45 C.F.R. § 160.103, Health Insurance Portability and Accountability Act of
1996 (HIPAA), as amended. All such information provided by the State during this procurement process
shall be considered Confidential Information regardless of the form, format, or media upon which or in
which such information is contained or provided, regardless of whether it is oral, written, electronic, or
any other form, and regardless of whether the information is marked as Confidential Information. As a
condition for its receipt and further access to the Confidential Information, Vendor agrees as follows:
1. Vendor will not copy, disclose, publish, release, transfer, disseminate or use for any purpose in
any form any Confidential Information received under this ITN, except in connection with the
preparation of its Reply to this ITN.
2. Vendor shall be liable for any violations by any of its employees who are provided or given
access to Confidential Information or any incidental access obtained by unauthorized persons
while in its control.
3. Vendor shall abide by the following procedures in handling the States’ Confidential Information:
a. Upon receipt of the data, the Vendor will password protect the Confidential
Information.
b. Vendor’s employees needing access to the State’s Confidential Information will be
informed that:
i. They are not to share the password or the State’s Confidential Information with
any unauthorized person;
ii. At the end of the solicitation process they will delete the State’s Confidential
Information from any laptop, desktop or any other electronic shared system
under their control and destroy any paper copies of such Confidential
Information; and
iii. They must confirm to the Vendor that they have so deleted or destroyed the
Confidential Information.
c. Files and passwords will be provided separately to appropriate users.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 118
d. Vendor will maintain the list of persons granted access (Access List) to the State’s
Confidential Information. Employees expected to have access to the State’s Confidential
Information are to be listed in the chart on page 3 of this attachment. Vendor will
update the list at the time it submits its Reply.
4. Vendor shall destroy the Confidential Information, including any copies, remaining in its
possession within the later of five business days of the State’s notice of an intended award in
connection with this solicitation or the conclusion of any legal proceeding or protest regarding
the procurement and shall provide a certification and a final Access List to the procurement
officer as defined in the ITN that it has complied with this requirement. If the Vendor does not
submit a Reply, the Vendor shall destroy the Confidential Information including any copies by
the time Replies are due and shall provide a certification and Access List to the procurement
officer that it has complied with this requirement on or before the due date for Replies. Vendor
acknowledges that the disclosure of the Confidential Information may cause irreparable harm to
the State and agrees that the State may obtain an injunction to prevent the disclosure, copying,
or other impermissible use of the Confidential Information. The State’s rights and remedies
hereunder are cumulative and the State expressly reserves any and all rights, remedies, claims
and actions that it may have now or in the future to protect the Confidential Information and/or
to seek damages for the Vendor’s failure to comply with the requirements of this Agreement.
5. In the event the State suffers any losses, damages, liabilities, expenses or costs (including by way
of example only, attorney’s fees and disbursements) that are attributable, in whole or in part to
any failure by the Vendor or any employee of the Vendor to comply with the requirements of
this Agreement, Vendor shall hold harmless and indemnify the State and the State of Florida
from and against any such losses, damages, liabilities, expenses and/or costs.
6. This Agreement shall be governed by the laws of the State of Florida. The Vendor consents to
personal jurisdiction in Florida state court, and exclusive venue shall be Leon County, Florida.
7. The individual signing below warrants and represents that they are fully authorized to bind the
Vendor to the terms and conditions specified in this Agreement.
Vendor: _____________________________________________________________
By: _____________________________________________________________________
Print Name: ______________________________________________________________
Title: ___________________________________________________________________
Address: ________________________________________________________________
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 119
VENDOR’S EMPLOYEES WHO WILL BE GIVEN ACCESS TO THE
CONFIDENTIAL INFORMATION
Printed Name,
Address of Individual
Signature of
Individual
Date
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 120
Attachment F: Notice of Intent to Submit a Reply
__________________________ informs the Florida Department of Management Services of its Enter Legal Name of Vendor
intent to respond to the solicitation titled ITN No. DMS 15/16-005 for Insured Health
Maintenance Organization Benefits and Self-Insured Health Plan Services.
Complete ALL Information Below
Name of Authorized Representative: ________________________________
Title of Authorized Representative: _________________________________
Signature of Authorized Representative: _____________________________
Date: __________________________ Date of Signature
Address: _____________________________________ Enter Street or PO Address for Delivery of Attachments D and G
_____________________________________ Enter City, State and ZIP Code for Delivery of Attachments D and G
Telephone No: (____) _____- ______
E-mail Address: __________________________

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 121
Attachment H: Covered Benefits and Services
SCHEDULE OF MEMBER COST SHARE
Benefit Description Cost to Member
Standard Plan Health Investor Plan
Deductible (Per Calendar Year)
None $1,300 Single
$2,600 Family (not to exceed $1,300
per covered person)
Medical Out-of-Pocket Maximum (Per Calendar Year)
Includes covered medical expenses only.
$1,500 Single
$3,000 Family (not to exceed
$1,500 per Member)
See below Global Out-of-Pocket Max
Global Out-of-Pocket Maximum including Rx (Per Calendar Year)
Includes covered expenses for both medical and prescription drugs or Rx only.
$6,850 Single
$13,700 Family (not to exceed
$6,850 per Member)
$3,000 Single
$6,000 Family (not to exceed $3,000
Member)
Preventive Care
Preventive health care (including screening mammograms) and immunization benefits for all covered members shall be age and gender based in accordance with the current grade A and B recommendations of the U.S. Preventive Services Task Force as provided by the Patient Protection and Affordable Care Act and medical policy guidelines established by [vendor] for preventive services.
No Charge No Charge
Not Subject to Deductible
Primary Care Physician
Services at participating doctor’s offices include, but are not limited to:
Routine office visits
Minor surgical procedures
Medical hearing examinations
$20 per visit
20% of the contracted rate
after you pay Deductible
Specialty Care Physician Services
Office visits, consultation, diagnosis and treatment
$40 per visit 20% of the contracted rate
after you pay Deductible
Hospital Pre-authorization is required for inpatient care, which at participating Hospitals includes:
$250 per admission; 100%
coverage
20% of the contracted rate
after you pay

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 122
SCHEDULE OF MEMBER COST SHARE
Benefit Description Cost to Member
Standard Plan Health Investor Plan
Room and board – unlimited days (semi-private)
Physician’s, specialist’s and surgeon’s services
Anesthesia, use of operating and recovery rooms, oxygen, drugs and medication
Intensive care unit and other special units, general and special duty nursing
Laboratory and diagnostic imaging
Required special diets
Radiation and inhalation therapies
thereafter Deductible
Surgery Outpatient
Inpatient Treating physician must obtain authorization from the Health Plan prior to surgery including preparation services and treatment.
No Charge
$250 per admission; 100%
coverage thereafter
20% of the contracted rate
after you pay Deductible
Vision Benefits Annual eye exam
Primary Care Physician
Specialist Services (office visits, refractions) o Participating optometrist and
ophthalmologist
$20 Copayment $40 Copayment
20% of the contracted rate
after you pay Deductible
Outpatient Laboratory and X-ray
Diagnostic Tests
CAT scan, PET scan, MRI
Outpatient Laboratory Tests
Mammograms
No Charge 20% of the contracted rate
after you pay Deductible. No
Charge for mammograms or
preventive diagnostic tests
and services
Emergency Services Copayment waived if admitted. Emergency room at participating Hospitals, facilities and/or Physicians Hospital and/or referring or admitting physician must call the Health Plan as soon as possible and within 24 hours of
$100 Copayment 20% of the contracted rate
after you pay Deductible
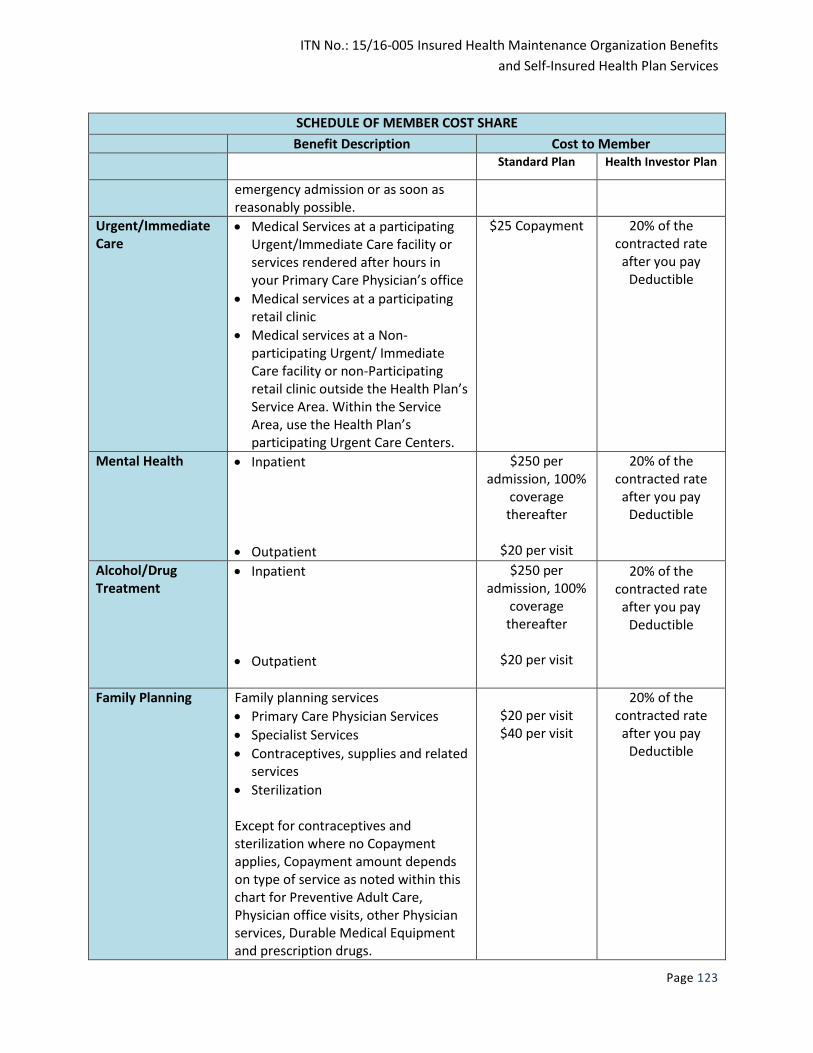
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 123
SCHEDULE OF MEMBER COST SHARE
Benefit Description Cost to Member
Standard Plan Health Investor Plan
emergency admission or as soon as reasonably possible.
Urgent/Immediate Care
Medical Services at a participating Urgent/Immediate Care facility or services rendered after hours in your Primary Care Physician’s office
Medical services at a participating retail clinic
Medical services at a Non-participating Urgent/ Immediate Care facility or non-Participating retail clinic outside the Health Plan’s Service Area. Within the Service Area, use the Health Plan’s participating Urgent Care Centers.
$25 Copayment 20% of the contracted rate
after you pay Deductible
Mental Health Inpatient
Outpatient
$250 per admission, 100%
coverage thereafter
$20 per visit
20% of the contracted rate
after you pay Deductible
Alcohol/Drug Treatment
Inpatient
Outpatient
$250 per admission, 100%
coverage thereafter
$20 per visit
20% of the contracted rate
after you pay Deductible
Family Planning Family planning services
Primary Care Physician Services
Specialist Services
Contraceptives, supplies and related services
Sterilization Except for contraceptives and sterilization where no Copayment applies, Copayment amount depends on type of service as noted within this chart for Preventive Adult Care, Physician office visits, other Physician services, Durable Medical Equipment and prescription drugs.
$20 per visit $40 per visit
20% of the contracted rate
after you pay Deductible

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 124
SCHEDULE OF MEMBER COST SHARE
Benefit Description Cost to Member
Standard Plan Health Investor Plan
Maternity Care
Outpatient
Inpatient
$40 per visit. If
billed as a global fee, then first
visit only.
$250 per admission, 100%
coverage thereafter
Allergy Treatments Injections
Primary Care Physician Services
Specialist Services Skin Testing
Primary Care Physician Services
Specialist Services
$20 per visit $40 per visit
$20 per visit $40 per visit
20% of the contracted rate
after you pay Deductible
Ambulance When pre-authorized or in the case of an emergency
No Charge
20% of the contracted rate
after you pay Deductible
Autism Spectrum Disorder, Diagnosis and Treatment of
Applied Behavior Analysis Services
Physical, speech or occupational therapy
$40 per visit 20% of the contracted rate
after you pay Deductible
Home Health Care
Per Occurrence No Charge 20% of the contracted rate
after you pay Deductible
Durable Medical Equipment
Per Device No Charge 20% of the contracted rate
after you pay Deductible
Rehabilitative Services
Outpatient Services limited to 60 visits per injury
$40 per visit 20% of the contracted rate
after you pay

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 125
SCHEDULE OF MEMBER COST SHARE
Benefit Description Cost to Member
Standard Plan Health Investor Plan
Deductible
Skilled Nursing Facilities
Pre-authorization required
Up to 60 days maximum per calendar year
No Charge 20% of the contracted rate
after you pay Deductible
Prosthetic or Orthotic Devices
Per Device No Charge 20% of the contracted rate
after you pay Deductible
Prescription Drugs CVS/caremark
Participating Retail Pharmacy (up to a 30-day supply)
Generic
Brand Name, Preferred
Brand Name, Non-Preferred Participating Retail Pharmacy (up to a 90-day supply)
Generic
Brand Name, Preferred
Brand Name, Non-Preferred Mail Order Pharmacy (up to a 90-day supply)
Generic
Brand Name, Preferred
Brand Name, Non-Preferred
$7 $30 $50
$14 $60
$100
$14 $60
$100
After you pay Deductible:
30% 30% 50%
If a generic is available and you, rather than your Physician, request the brand name drug, your cost is the brand Copayment (or Coinsurance if HIHP) plus the difference in the Plan’s cost between brand name and the generic. For oral cancer treatment medications, your cost is the lesser of the appropriate Copay (or Coinsurance if HIHP) or $50.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 126
COVERED BENEFITS AND SERVICES
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
Ambulance Transportation and Service
Ambulance service to the nearest Hospital
Ambulance service to a Health Plan Member’s home or skilled nursing facility
Ambulance service from a Hospital which is unable to provide proper care to the nearest Hospital that can provide proper care
For services by boat, airplane or helicopter o When the pick-up point is inaccessible by ground
transportation o When the travel distance involved in getting the Health
Plan Member to the nearest Hospital that can provide proper care is too far for medical safety
o When speed in excess of ground vehicle speed is critical for medical safety
Anesthesia Services
Both inpatient and outpatient
Autism Spectrum Disorder
Diagnosis and treatment through speech therapy, occupational therapy, physical therapy, and Applied Behavior Analysis services for an individual under 18 years of age or an individual 18 years of age or older who is in high school who has been diagnosed as having a developmental disability at 8 years of age or younger.
Coverage includes well-baby and well-child screening for diagnosing the presence of Autism Spectrum Disorder, speech therapy, occupational therapy, physical therapy, and Applied Behavior Analysis. Applied Behavior Analysis is covered when provided by Applied Behavioral Analysts, psychologists, clinical social workers, and others within the scope of their license.
Coverage limited to services prescribed by the Health Plan Member’s treating physician in accordance with a treatment plan. The required treatment plan includes, but is not limited to, a diagnosis; proposed treatment by type, frequency and duration of treatment; anticipated outcomes stated as goals; frequency with which treatment plan will be updated; and a signature from the treating physician.
Covered as required by sections 627.6686 and 641.31098, Florida Statutes, and as further amended by state and federal law.
Developmental Disability means a disorder or syndrome that is: 1) attributable to a mental disability, cerebral palsy, autism, spina bifida, or Prader-Willi syndrome, 2) manifests before the age of 18, and 3) constitutes a substantial handicap that can reasonably be expected to continue indefinitely.
Bone Marrow Transplants If the particular use of the procedure is determined to be accepted within the appropriate oncological specialty and not Experimental pursuant to rules adopted by the Florida

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 127
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
Agency for Health Care Administration.
Includes costs associated with the donor-patient
Cancer Services
Diagnosis and Treatment Includes both inpatient and outpatient diagnostic tests and
treatment (including anti-cancer medications administered by Network providers), including cancer clinical trials as set forth in the Florida Clinical Trial Compact. Does not include Experimental or Investigational Treatment.
Cleft Lip and Cleft Palate Treatment and services for children under 18 years, including medical, dental, speech therapy, audiology and nutrition services only as required by sections 627.64193 and 641.31(35), Florida Statutes.
Clinical Trials Includes routine patient care costs incurred by an insured individual who participates in approved Phase I, II, III or IV clinical trials relating to cancer and other life threatening diseases if those services, including drugs, items and devices, would otherwise be covered under the plan or contract for an insured person not enrolled in a clinical trial program. Experimental treatment is excluded.
Child Health Supervision Services Services include a physical examination, developmental assessment and anticipatory guidance, and immunizations and laboratory tests, consistent with the recommendations for Preventive Pediatric Health Care of the American Academy of Pediatrics.
Services as defined by the Patient Protection and Affordable Care Act.
Contraceptive Supplies
Insertion and removal of IUD
Diaphragm
Insertion and removal of contraceptive implants
Contraceptive injections
Oral contraceptives
With respect to Women’s Preventive Services (see also Preventive Services), and to the extent required by federal law, coverage is limited to at least one form of contraception in each of the eighteen methods identified in FDA’s most current Birth Control Guide and limited to generic products, when available. o Contraceptive methods – Medical
Barrier: Diaphragm Implanted: IUD Sterilization: Tubal ligations
o Contraceptive methods – Pharmacy Hormonal: All generic oral contraceptives
Other contraceptives may be covered based on medical necessity.
The Plan pays 100 percent of the Network allowed amount.
For additional information on medical coverage, please call the Health Plan’s Member Services Department listed in the

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 128
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
contact section within this document. For additional information on prescription coverage, please call CVS/caremark at 1-877-531-4793.
Cosmetic Surgery
Plastic and reconstructive
Reduction mammoplasty
Repair or alleviation of damage if the result of an accident, which is a sudden, unintentional, and unexpected event or force
Correction of a congenital anomaly for an eligible dependent
Correction of an abnormal bodily function for an area of the body which was altered by the treatment of a disease
All stages of reconstruction of a breast on which a mastectomy was performed in accordance with federal law. However, if there is no evidence of malignancy, such reconstruction and initial prosthetic device shall only be covered if received within two years after the date of the mastectomy.
Dental Care and Accidental Dental Injury Accidental Dental Injury - an injury to sound natural teeth caused by a sudden, unintentional, and unexpected event or force. This term does not include injuries to the mouth, structures within the oral cavity, or injuries to natural teeth caused by biting or chewing, surgery, or treatment for a disease or illness. Sound Natural Tooth - a tooth that is whole or properly restored (restoration with amalgams only) and is not in need of the treatment provided for any reason other than an Accidental Dental Injury. For purposes of this Plan, a tooth previously restored with a crown inlay, inlay or porcelain restoration, or treated by endodontics, is not considered a sound natural tooth.
Only in cases of Dental Care provided to a person under age 8 if the dental condition is likely to result in a medical condition if left untreated and if the child’s dentist and physician determine dental treatment in a Hospital or surgical center is necessary.
Accidental dental injury coverage is limited as defined. General Dental Care is not covered as stated in the Exclusion section of this document.
Benefits for accidental dental injury are limited to care and treatment rendered within 120 days of an accidental dental injury.
Dermatology Services Direct access (without referral or authorization) for up to five office visits annually, including minor procedures and testing, to a Network dermatologist, as required by sections 627.6472(16) and 641.31(33) Florida Statutes.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 129
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
Diabetes and pre-diabetes Treatment
All medically appropriate and necessary equipment, supplies and outpatient self-management training and educational services used to treat pre-diabetes and diabetes, if the treating physician or a physician who specializes in the treatment of diabetes certifies that such services are necessary.
Certain diabetic equipment and supplies are covered through the Health Plan. Those not covered by the Health Plan may be covered by the Prescription Drug Plan. See Prescription Drug Plan section within this document for additional information.
Doctor’s Care
Office visits
Medical treatment in Hospital or outpatient facility or surgery (other than office visit), which includes anesthesia services, concurrent physician care (surgical assistance provided by another physician) and consultations.
Child health supervision services
Adult preventive Medical Services
Allergy treatment – including testing, desensitization therapy and allergy immunotherapy, which includes hyposensitization serum when administered by a health care provider.
Diagnostic procedures, lab tests or x-rays, including their interpretation, for the treatment of a covered condition
For concurrent physician care and surgical assistance: o The additional physician must actively participate in the
treatment o The condition involves more than one body system or is
so severe or complex that one physician cannot provide the care unassisted
o The physicians have different specialties or have the same specialty with different sub-specialties
o Must be authorized by the Health Plan Member’s PCP or the Health Plan
For consultations: o The ordering physician must request the consultation o Consulting physician shall prepare a written report
Durable Medical Equipment
For the care and treatment of a condition covered under this Plan, the Plan shall either rent or purchase medical equipment and supplies including, but not limited to: o Trusses, braces, walkers,
canes, crutches, casts and splints
o Occlusal guards, bite or
Durable Medical Equipment: o Shall not serve as a comfort, hygiene, or convenience
item o Shall not be used for the sole purpose of exercise o Shall not be used by any other party o Shall have been manufactured specifically for medical
use o Shall not include shoe buildups, shoe orthotics, shoe
braces or shoe supports unless the shoe is attached to a brace
o Shall not include water therapy devices, modification to

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 130
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
dental splints, repositioning devices, and TMJ models for the treatment of temporomandibular joint (TMJ) syndrome
o Commode chairs, bedpans/urinals, decubitus care equipment, and ostomy and urinary products
o Oxygen and rental of equipment for the administration of oxygen, ventilator or other mechanical equipment for the treatment of respiratory paralysis or insufficiency
o Ambulatory home uterine activity monitoring devices (AHUM)
o Wheelchairs, Hospital beds, lumbar-sacral-orthosis (LSO) and thoracic-lumbar-sacral-orthosis (TLSO) braces, and traction equipment
o Other medical equipment and supplies as determined to be Medically Necessary
motor vehicles and/or homes or similar items
Emergency Care
Coverage, without prior authorization, for screening and stabilization based on determination by either an in-Network or non-Network provider
Eye Care
Routine or refractive eye examinations as part of the adult preventive medical care or child health supervision services benefit
For eyeglasses or contact lenses: o Limited to the first pair following an accident to the eye
or cataract surgery o Includes the examination for the prescribing or fitting
thereof o For treatment of a covered condition:
Aphakic patients and soft lenses or sclera shells
Following an injury, disease or accident
Family Planning Services Includes counseling and information on birth control, sex education and the prevention of sexually transmitted

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 131
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
diseases.
Hearing Tests Only when associated with a covered ear surgery, in accordance with child and adult preventive health care benefits, or for the diagnosis of a covered condition.
Hearing tests to determine if a hearing aid is needed are not covered.
Hemodialysis for Renal Disease Includes equipment, training and medical supplies for home dialysis and dialysis centers.
Home Health Care
Services by a home health care agency for a Health Plan Member confined and convalescing at home for a covered condition
Home health care services include: o Part-time, intermittent or
continuous nursing care by registered nurses or licensed practical nurses, nurse registries or home health agencies;
o Physical, speech, occupational and respiratory therapy, and infusion therapy
o Medical appliances, equipment, laboratory services, supplies, drugs, and medicines prescribed by the treating physician and other covered services provided by or for a home health agency through a licensed nurse registry or by an independent nurse licensed under chapter 464, Florida Statutes, to the extent that they would have been covered if the person had been confined in a Hospital
For approval of Home Health Care Services by your PCP or the Plan: o The treating physician must submit a home health care
plan of treatment to your PCP o The plan of treatment must document that home health
care is Medically Necessary and that the services are being provided in lieu of hospitalization or continued hospitalization
o Home health care benefits would be less costly than confinement to a Hospital or skilled nursing facility
Services which shall not be covered under this benefit include: o Any service that would not have been covered had the
Health Plan Member been confined to a Hospital o Services which are solely for the convenience of the
Health Plan Member
Therapy is subject to outpatient Limitations described under rehabilitative services
A visit is limited to a period of two hours or less.
Hospice Care
In-home care Hospice treatment program shall:
o Meet the standards outlined by the National Hospice

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 132
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
o Physician services o Physical, respiratory,
massage, speech and occupational therapy if approved by the Plan
o Medical supplies, drugs and appliances
o Home health aide services o Part-time or intermittent
nursing care by a registered nurse (RN) or licensed practical nurse (LPN) or Private Duty Nursing service
o Oxygen o Infusion Therapy
Hospice Inpatient Care o Room and board and general
nursing care o Inpatient care services same
as inpatient Hospital care o Same covered services as in-
home and outpatient hospice care
o Includes care for pain control or acute chronic symptom management
Hospice outpatient care o Physician services o Laboratory, x-ray, and
diagnostic testing o Ambulance service o Same covered services as in-
home hospice care
Association o Be recognized as an approved hospice program by the
Health Plan o Be licensed, certified, and registered as required by
Florida law, and o Be directed by the Health Plan Member’s PCP or the
Health Plan and coordinated by a registered nurse with a treatment plan that provides an organized system of hospice facility care, uses a hospice team and has around-the-clock care available
For hospice care: o Counseling of terminally ill patients whose doctor has
certified that they have less than one year to live o Primary Care Physician (PCP) must submit a written
hospice care plan or program o Treating physician must submit a life expectancy
certification o All hospice care expenses shall be approved in writing
by the Health Plan on behalf of the Plan o While in the hospice program, plan benefits for
expenses related to the terminal illness are covered by the hospice provider
o Limited to 210 calendar days per lifetime
Hospital Inpatient Care
Hospital room, board and general nursing care for a semi-private room the Plan determines that a private room is Medically Necessary
Room, board and treatment in an intensive, progressive, cardiac or neonatal care unit
Other necessary services and supplies including, but not limited
Services and supplies must be furnished at a Network Hospital and must be authorized by the Primary Care Physician or the Plan in order to be covered. Exceptions to this include emergency services and other special circumstances, as approved by the Health Plan.
Excludes services and supplies provided when the Health Plan Member is admitted to a Hospital or other facility primarily to provide rehabilitative services.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 133
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
to:
Use of operating room, labor room, delivery room and recovery room
Drugs and medicines used by the patient
Intravenous solutions
Dressings, ordinary casts, splints and trusses
Anesthesia and related supplies
Transfusion supplies and services including blood, blood plasma and serum albumin, if not replaced
Respiratory therapy, including oxygen
Diagnostic services, including radiology, ultrasound, laboratory, pathology, and approved machine testing such as electrocardiograms and electroencephalograms
Basal metabolism examinations
X-ray, including therapy
Diathermy
All covered rehabilitative services
Immunizations
Includes flu shots See Preventive Services.
Mammograms
Screening
Diagnostic service
One baseline mammogram for women age 35 through 39
One mammogram every one to two years – ages 40 through 49
One mammogram every year – age 50 and over
At any age if deemed Medically Necessary (diagnostic)
Maternity Care
Pre-natal and post-natal care and monitoring of the mother
Delivery in a Hospital or birth center
Postpartum care
Newborn care and assessment (one time), including initial exam from pediatrician
Medically Necessary clinical tests and immunizations
Covered Hospital stays for the mother and newborn child will be no less than: o 48 hours for a normal delivery o 96 hours for a Cesarean-section delivery unless agreed
to by the provider and the patient
With respect to Women’s Preventive Services, coverage for breast feeding supplies is: o Limited to one manual breast pump per birth

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 134
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
Routine well-baby nursery services
Midwife services
Breastfeeding support, supplies and counseling
Mental Health, Alcoholism and Substance Abuse Care
Inpatient
Outpatient
Treatment program must be accredited by the Joint Commission or approved by the State.
Providers must be licensed in accordance with applicable law.
For inpatient care: o Alcoholism and substance abuse care includes
detoxification.
For outpatient care: o Mental health and nervous disorders treatment
includes diagnostic evaluation, psychiatric treatment, and individual and group therapy. For learning and behavioral disabilities or mental
disability, coverage is limited to evaluation and diagnosis.
Newborn Care
Coverage includes, but is not limited to: o Coverage for injury or
sickness, including Medically Necessary care or treatment for medically diagnosed congenital defects, birth abnormalities or prematurity.
o The transportation costs of the newborn to and from the nearest available facility appropriately staffed and equipped to treat the newborn’s condition. Such transportation shall be certified by the attending physician as necessary to protect the health and safety of the newborn child.
Coverage for the unenrolled newborn child of a covered eligible Health Plan Member is limited to well-baby Hospital nursery services.
Newborn must be enrolled in the Health Plan within 60 days of the birth to be covered for other services.
Nutrition Counseling
Nursing Services
Nursing care by a registered nurse (RN) or licensed practical
Includes inpatient Private Duty Nursing when authorized by the Plan.
Includes Home Health Care Services and Hospice Services.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 135
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
nurse (LPN)
Oral Surgery
Surgical treatment of non-dental injury to teeth, fractured or dislocated jaw, excision of tumors, cysts, abscesses and lesions of the mouth and surgical treatment of temporomandibular joint (TMJ) syndrome
Treatment of bones or joints of the jaw or facial region as required by section 641.31094, Florida Statutes, when Medically Necessary for conditions caused by congenital or developmental deformity, disease or injury
Does not include care or treatment of the teeth or gums, intraoral prosthetic devices or surgical procedures for cosmetic purposes.
Organ Transplants
Services, care and treatment received for or in connection with the approved transplantation of the following human tissue and organs: o Heart o Heart/lung o Lung o Liver o Kidney o Kidney/pancreas o Bone marrow o Cornea
Covered services include: o Organ acquisition and donor
costs. However, donor costs shall not be payable under this Plan if they are payable in whole or in part by any other insurance health plan, organization or person other than the donor’s family or estate.
Transplantation includes pre-transplant, transplant and post-discharge services, and treatment of complications after
To have a transplant covered: o Prior approval for the transplant must be obtained by
the Health Plan Member’s Participating PCP in advance of the Health Plan Member’s initial evaluation for the procedure;
o The Health Plan shall be given the opportunity to evaluate the clinical results of the evaluation. Such evaluation and approval shall be based on written criteria and procedures established by the Plan; and
o The facility in which the pre-transplant services, transplant procedure and post-discharge services will be performed must be licensed as a transplant facility and authorized by the Health Plan.
Transplant services shall not be covered when: o Expenses are eligible to be paid under any private or
public research fund, government program, or other funding program, whether or not such funding was applied for or received;
o The expense relates to the transplantation of any non-human organ or tissue;
o The service or supply is in connection with the implant of an artificial organ, including the implant of the artificial organ;
o The organ is sold rather than donated to the person; o The expense relates to the donation or acquisition of an
organ for a recipient who is not covered by the Plan except in the case of the donor costs for bone marrow transplants; or

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 136
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
transplantation
For bone marrow transplants: o Includes the harvesting,
transplantation and chemotherapy components
o Donor costs are covered in the same way as costs for the Health Plan Member, including Limitations and non-covered services
o A denied transplant is performed; this includes follow-up care, immunosuppressive drugs, and complications of such transplant
The following services and supplies shall not be covered: o Artificial heart devices used as a bridge to transplant; o Drugs used in connection with diagnosis or treatment
leading to a transplant when such drugs have not received FDA approval for such use; or
o Any service or supply in connection with identification of a donor from a local, state, or national listing.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 137
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
Outpatient Care
Treatment as an outpatient in a Hospital, a health care provider’s office, an ambulatory surgical center or other licensed outpatient health care facility
Clinical laboratory services
Services for outpatient surgery and outpatient treatment of an injury
Includes Medically Necessary supplies provided or used by the facility during the surgery or treatment, such as: o Use of operating room, and
recovery room o Use of covered drugs and
medicines used by the patient o Intravenous solutions,
dressings, ordinary casts, splints and trusses
o Anesthesia, related supplies and their administration
o Transfusion supplies and services including blood, blood plasma and serum albumin, if not replaced
o Respiratory therapy, including oxygen
o Diagnostic services, including radiology, ultrasound, laboratory, pathology, and approved machine testing such as electrocardiograms and electroencephalograms
o Basal metabolism examinations
o X-ray, including therapy o Diathermy o Services provided by a
birthing center licensed pursuant to section 383.30-383.335, Florida Statutes
Other covered necessary services and supplies

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 138
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
Pathologist Services
Both inpatient and outpatient
Pre-admission Tests Tests shall be: o Ordered or authorized by the Health Plan Member’s
PCP; and o Performed in a facility accepted by the Hospital and the
Health Plan in lieu of the same tests which would normally be done while Hospital confined.
Preventive Services
Additional Women’s Preventive Services: to the extent required by federal law; the following services are covered for all female Health Plan Members: o Human papillomavirus (HPV)
testing; o Counseling for sexually
transmitted infections; o Counseling and screening for
human immune-deficiency virus (HIV);
o Counseling and screening for interpersonal and domestic violence;
o Screening for gestational diabetes;
o Counseling and support for breastfeeding and supplies (limited to one breast pump per birth); and
Annual well woman visits expanded to include prenatal care, contraceptive counseling and at least one form of contraception in each of the eighteen methods identified in FDA’s most current Birth Control Guide and limited to generic products, when available (see Contraceptive Services)
Preventive Medical Services will be as defined by the Patient Protection and Affordable Care Act, which include: o Evidence-based items or services that have in effect a
rating of “A” or “B” in the current recommendations of the United States Preventive Services Task Force;
o Assessment of the risk of falls for older adults is included during the preventive care wellness examination or evaluation and management (E&M) visit;
o Immunizations that have in effect a recommendation from the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention with respect to the individual involved.
o With respect to infants, children, and adolescents, evidence-informed preventive care and screenings are provided to the extent required by the comprehensive guidelines supported by the Health Resources and Services Administration.
o With respect to Women’s Preventive Health Services, coverage is provided to the extent mandated by federal law.
o For additional information on immunizations and preventive health care services go to: www.healthcare.gov www.uspreventiveservicestaskforce.org/uspstf/us
psabrecs.htm www.healthcare.gov/law/resources/regulations/w
omensprevention.html, and www.healthcare.gov/new/factsheets/2010/09/aff
ordable_care_act_immunization.html
Prostheses and Orthotic Devices
Initial placement of the most cost effective prosthetic or orthotic device, fitting, adjustments and repair
Replacements covered if due to growth or change and approved by the Plan as Medically Necessary.
Shoe orthotics shall be covered only when attached to a brace.
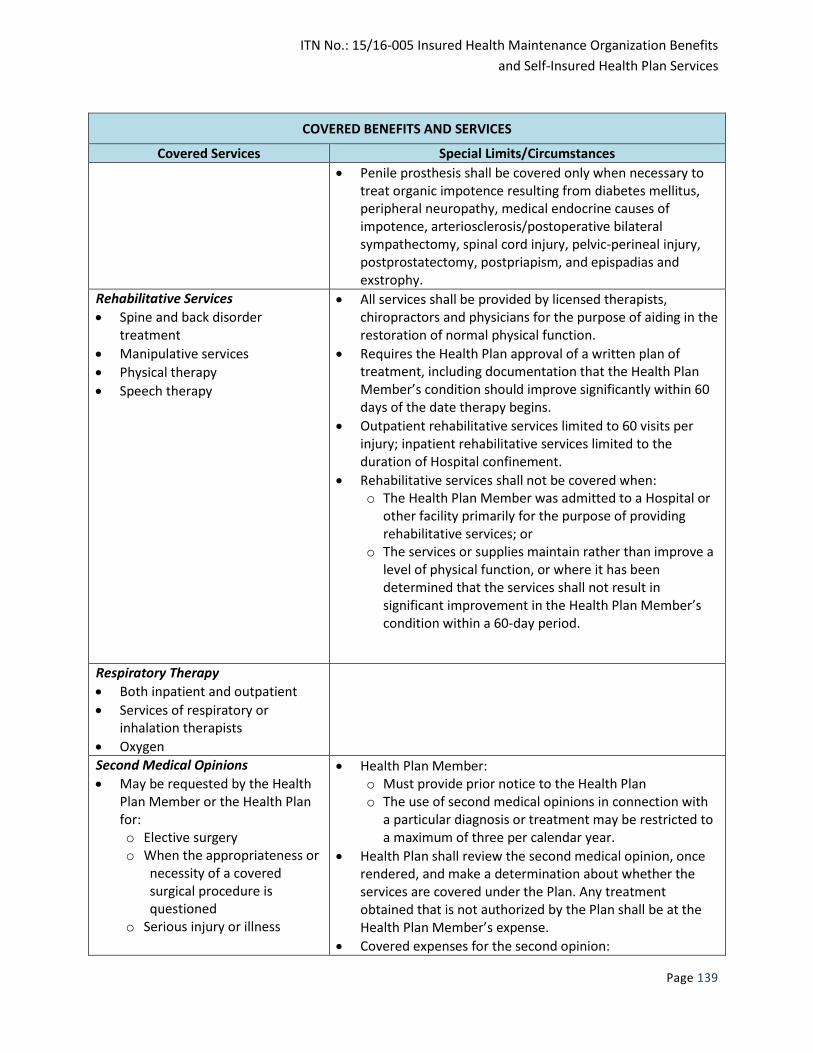
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 139
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
Penile prosthesis shall be covered only when necessary to treat organic impotence resulting from diabetes mellitus, peripheral neuropathy, medical endocrine causes of impotence, arteriosclerosis/postoperative bilateral sympathectomy, spinal cord injury, pelvic-perineal injury, postprostatectomy, postpriapism, and epispadias and exstrophy.
Rehabilitative Services
Spine and back disorder treatment
Manipulative services
Physical therapy
Speech therapy
All services shall be provided by licensed therapists, chiropractors and physicians for the purpose of aiding in the restoration of normal physical function.
Requires the Health Plan approval of a written plan of treatment, including documentation that the Health Plan Member’s condition should improve significantly within 60 days of the date therapy begins.
Outpatient rehabilitative services limited to 60 visits per injury; inpatient rehabilitative services limited to the duration of Hospital confinement.
Rehabilitative services shall not be covered when: o The Health Plan Member was admitted to a Hospital or
other facility primarily for the purpose of providing rehabilitative services; or
o The services or supplies maintain rather than improve a level of physical function, or where it has been determined that the services shall not result in significant improvement in the Health Plan Member’s condition within a 60-day period.
Respiratory Therapy
Both inpatient and outpatient
Services of respiratory or inhalation therapists
Oxygen
Second Medical Opinions
May be requested by the Health Plan Member or the Health Plan for: o Elective surgery o When the appropriateness or
necessity of a covered surgical procedure is questioned
o Serious injury or illness
Health Plan Member: o Must provide prior notice to the Health Plan o The use of second medical opinions in connection with
a particular diagnosis or treatment may be restricted to a maximum of three per calendar year.
Health Plan shall review the second medical opinion, once rendered, and make a determination about whether the services are covered under the Plan. Any treatment obtained that is not authorized by the Plan shall be at the Health Plan Member’s expense.
Covered expenses for the second opinion:

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 140
COVERED BENEFITS AND SERVICES
Covered Services Special Limits/Circumstances
o If a Network physician is selected, the only cost to the Health Plan Member will be the applicable Copayment/Coinsurance.
o If a non-Network physician is selected, the Health Plan Member may be required to pay for up to 40 percent of the usual and customary charges for those services in the community where they were rendered as determined by the Health Plan.
Skilled Nursing Facility Care
Room, board and general nursing care
Services and supplies for necessary treatment
Primary Care Physician (PCP) or the Health Plan shall approve a written plan of treatment
Health Plan Member must require skilled care for a condition (or a related condition) which was treated in the hospital and such care can be provided at a skilled nursing facility in lieu of hospitalization or continued hospitalization
The Health Plan Member must be admitted to the facility immediately following discharge from the Hospital
Skilled nursing care or services are provided on a daily basis
Limited to 60 days of confinement per calendar year
Services shall be ordered by and provided under the direction of a physician
Surgical Procedures
Both inpatient and outpatient
Surgical Sterilization Limited to tubal ligations and vasectomies
Tobacco Cessation Products Tobacco screening, cessation counseling and tobacco cessation medications, including prescription and over-the-counter medications, when prescribed by a health care provider and that have a current rating of A or B by the United States Preventive Services Task Force.
Wigs Covered only when hair loss is caused by chemotherapy, radiation therapy, or cranial surgery. Coverage is limited to a maximum payment of $40 for one wig and fitting in the 12 months following treatment or surgery.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 141
Limitations and Exclusions
The following services and supplies are excluded from coverage under this Plan unless a specific
exception is noted. Exceptions may be subject to certain coverage Limitations.
LIMITATIONS AND EXCLUSIONS
Abortion Which is elective, performed at any time during a pregnancy.
Acupuncture Services, supplies, care or treatment in connection with acupuncture (except when used in lieu of an anesthetic agent for covered surgery).
Arch Supports Orthopedic shoes, sneakers, or support hose, or similar type devices/appliances, regardless of intended use.
Autologous transfusion In which blood is removed from a donor and stored before it is returned to the donor's circulation.
Autopsy
Biofeedback services And other forms of self-care or self-help training and any related diagnostic testing, hypnosis, meditation, mind expansion, elective psychotherapy such as Gestalt therapy, transactional analysis, transcendental meditation, Z-therapy, and Erhard seminar training (EST).
Complications of non-covered services
Including the diagnosis or treatment of any condition which arises as a complication of a non-covered service.
Cosmetic surgery/services Including plastic and reconstructive surgery (except as noted as a covered service), dental care, and any other service and supply to improve the Health Plan Member’s appearance or self-perception.
Costs incurred by the Plan related to…
Health care services resulting from accidental bodily injuries arising out of a motor vehicle accident to the extent such services are payable under any medical expense provision of any automobile insurance policy, and telephone consultations, failure to keep a scheduled appointment or complete any form and/or medical information.
Custodial care Including any service or supply of a custodial nature primarily intended to assist the Health Plan Member in the activities of daily living. This includes rest homes (facilities), nursing homes, skilled nursing facility, home health aides (sitters), home mothers, domestic maid services and respite care. Also includes services and supplies that are furnished mainly to train or assist in the activities of daily living, such as bathing, feeding, dressing, walking and taking oral medications. “Custodial Care” also means services and supplies that can be safely and adequately provided by persons other than licensed Health Professionals, such as dressing changes and catheter care, or that ambulatory patients customarily provide for themselves, such as ostomy care, administering insulin and

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 142
LIMITATIONS AND EXCLUSIONS
measuring and recording urine and blood sugar levels.
Dental care Or any treatment relating to the teeth, jaws, or adjacent structures (e.g.
periodontium), including but not limited to extraction or cleaning of the
teeth; implants, braces, crowns, bridges, fillings, dentures, x-rays,
periodontal, orthodontic treatment; rapid palatial expanders;
continuous passive motion (CPM) devices.
Dietary regimens Treatments, food, food substitutes, vitamins or exercise programs for
reducing or controlling weight.
Experimental/Investigational
or Not Medically Necessary
Treatment
With the exception of routine care in connection with a clinical trial in
cancer, pursuant to the Florida Clinical Trial Compact and the Patient
Protection and Affordable Care Act.
Eye care Including the purchase, examination, or fitting of eyeglasses or contact lenses, except as specifically provided for in the covered benefits section;
Radial keratotomy, myopic keratomileusis, and any surgery which involves corneal tissue for the purpose of altering, modifying, or correcting myopia, hyperopia, or astigmatic error; and
Training or orthoptics, including eye exercises.
Foot care (routine) Including any service or supply in connection with foot care in the
absence of disease, injury or accident. This Exclusion includes, but is not
limited to, treatment of bunions, flat feet, fallen arches, and chronic
foot strain, removal of warts, corns, or calluses, or trimming of toenails,
unless determined by the Plan to be Medically Necessary.
Gender reassignment or
modification services and
supplies
Genetic tests To determine paternity or sex of a child.
Hearing aids External or implantable or the examination, including hearing tests, for
the prescription or fitting of hearing aids, including tinnitus maskers.
Human Growth Hormone For diagnosis and/or treatment of idiopathic short stature.
Hypnotism Medical hypnotherapy or hypnotic anesthesia.
Immunizations and physical
examinations
When required for travel, or when needed for school, employment,
insurance or governmental licensing, except insofar as such
immunizations and examinations are within the scope of, and coincide
with, the periodic health assessment examination and/or state law
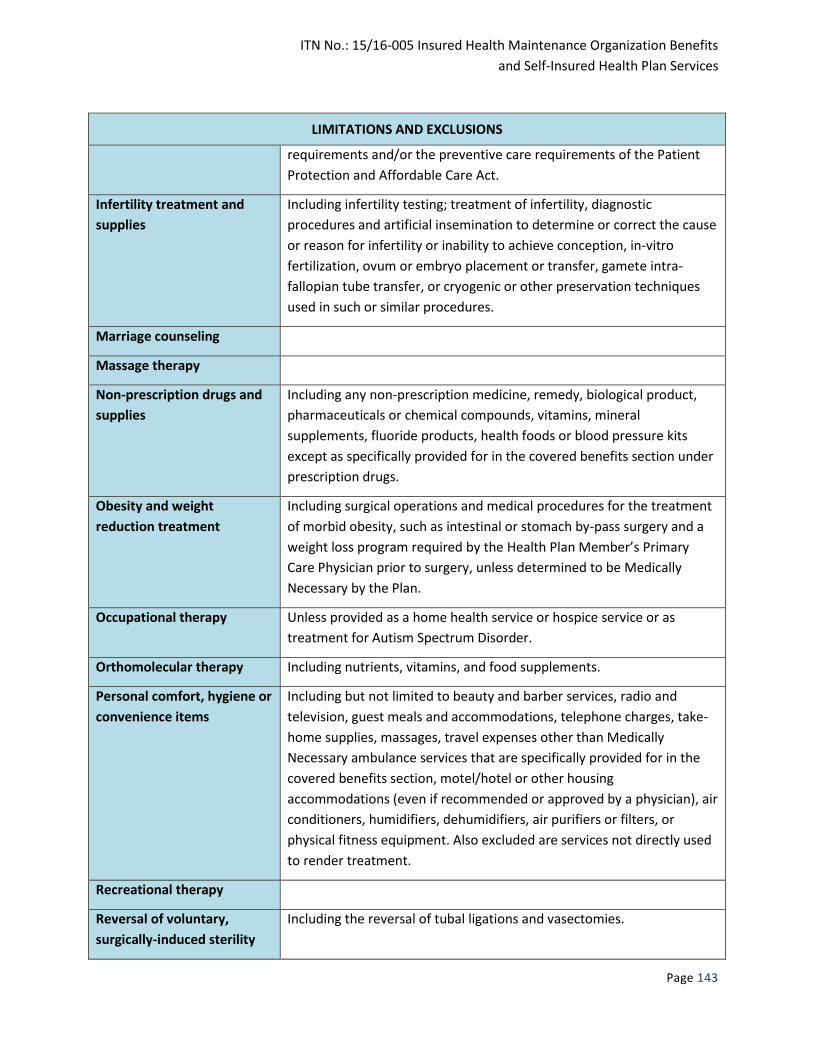
ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 143
LIMITATIONS AND EXCLUSIONS
requirements and/or the preventive care requirements of the Patient
Protection and Affordable Care Act.
Infertility treatment and
supplies
Including infertility testing; treatment of infertility, diagnostic
procedures and artificial insemination to determine or correct the cause
or reason for infertility or inability to achieve conception, in-vitro
fertilization, ovum or embryo placement or transfer, gamete intra-
fallopian tube transfer, or cryogenic or other preservation techniques
used in such or similar procedures.
Marriage counseling
Massage therapy
Non-prescription drugs and
supplies
Including any non-prescription medicine, remedy, biological product,
pharmaceuticals or chemical compounds, vitamins, mineral
supplements, fluoride products, health foods or blood pressure kits
except as specifically provided for in the covered benefits section under
prescription drugs.
Obesity and weight
reduction treatment
Including surgical operations and medical procedures for the treatment
of morbid obesity, such as intestinal or stomach by-pass surgery and a
weight loss program required by the Health Plan Member’s Primary
Care Physician prior to surgery, unless determined to be Medically
Necessary by the Plan.
Occupational therapy Unless provided as a home health service or hospice service or as
treatment for Autism Spectrum Disorder.
Orthomolecular therapy Including nutrients, vitamins, and food supplements.
Personal comfort, hygiene or
convenience items
Including but not limited to beauty and barber services, radio and
television, guest meals and accommodations, telephone charges, take-
home supplies, massages, travel expenses other than Medically
Necessary ambulance services that are specifically provided for in the
covered benefits section, motel/hotel or other housing
accommodations (even if recommended or approved by a physician), air
conditioners, humidifiers, dehumidifiers, air purifiers or filters, or
physical fitness equipment. Also excluded are services not directly used
to render treatment.
Recreational therapy
Reversal of voluntary,
surgically-induced sterility
Including the reversal of tubal ligations and vasectomies.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 144
LIMITATIONS AND EXCLUSIONS
Sexual deviations, disorders
or psychosexual
dysfunctions services and
supplies
Sleep therapy
Tobacco cessation programs
and products
Including any service or supply to eliminate or reduce a dependency on,
or addiction to, tobacco including but not limited to nicotine withdrawal
programs, vapor and e-cigarettes, nicotine gum, patches, lozenges, or
inhalers, unless specifically provided by law.
Training and educational
programs
Including programs primarily for pain management or vocational
rehabilitation unless specifically provided by law.
Volunteer services Or services which would normally be provided free of charge to a Health
Plan Member.
Weight control/weight loss
programs
Work related condition
services
To the extent the Health Plan Member is covered or required to be covered by a workers’ compensation law. If the Health Plan Member enters into a settlement giving up rights to recover past or future medical benefits under a workers’ compensation law, this Plan shall not cover past or future Medical Services that are the subject of or related to that settlement. In addition, if the Health Plan Member is covered by a workers’ compensation program that limits benefits if other than specified health care providers are used and the Health Plan Member receives care or services from a health care provider not specified by the program, the Health Plan shall not cover the balance of any costs remaining after the program has paid.
Additional Exclusions
include, but are not limited
to:
Bulk powders, bulk chemicals, and proprietary bases used in compounded medications and over-the-counter products used in compounded medications.
Services or supplies not Medically Necessary as determined by the Plan and/or the Prescription Drug Plan clinical staff and the State.
Services or supplies that are not specifically listed in the covered benefits section unless such services are specifically required by state or federal law.
Court ordered care or treatment, unless otherwise covered by this Plan, including testing required as a condition of parole or probation;
Testing for aptitude, ability, intelligence or interest.

ITN No.: 15/16-005 Insured Health Maintenance Organization Benefits
and Self-Insured Health Plan Services
Page 145
LIMITATIONS AND EXCLUSIONS
Treatment of a condition resulting from:
War or an act of war, whether declared or not;
Participation in any act which would constitute a riot or rebellion, or commission of a crime punishable as a felony;
Engaging in an illegal occupation;
Services in the armed forces;
Services or supplies received prior to a Health Plan Member’s effective date or received on or after the date a Health Plan Member’s coverage terminates under this Plan, unless coverage is extended in accordance with extension of benefit provisions;
Services provided by a physician or other health care provider who normally resides in the Health Plan Member’s home;
Services rendered from a medical or dental department maintained by or on behalf of a public health entity;
Non-medical conditions related to hyperkinetic syndromes, learning disabilities, intellectual disability, or inpatient confinement for environmental change;
Services or supplies supplied at no charge, or determined by the Plan not to be the most cost-effective setting, procedure or treatment.
The following services:
o Social work
o Bereavement and pastoral
o Financial
o Legal
o Dietary counseling
o Day care
o Homemaker and chore
o Funeral