Embed Size (px)
Citation preview
State and Federal Health Care Legislation
Lawrence MassaMinnesota Hospital Association
May 17, 2012

The good news continues ….
Well … not so fast …

Place picture here
State Health Care Legislation
Click icon to add picture
State Issues:Community benefit
Passed repeal legislation keeping hospitals’ community benefit activities locally determined.• Unanimous support in House and Senate• Repeal of new rider language from 2011 • Funding language for Statewide Health Improvement
Project (SHIP) remains
State Issues:Provider Peer Grouping
Passed a Provider Peer Grouping “fix-up” language in same bill as community benefit.• Allows providers to verify their data• Requires better risk adjustment for high cost services
like trauma, medical education and neo-natal ICU• Creates a stakeholder/expert advisory committee• Expands scope of appeals (peer group, calculations,
methodology and data)• Requires use of most current data available• Eliminates requirement that health plans use PPG in
product design
State Issues:HHS Omnibus Bill
Allow Medicaid coverage for inpatient mental health services delivered by a physician assistant acting under psychiatrist’s supervision
Further restriction on release of medical records• Expands liability for unauthorized, intentional access via
record locator service• Requires study by Department of Health to examine
capability of detecting unauthorized attempts to view a patient’s medical records
Establishes a 10-day window for DHS prior authorization for PT/OT, speech, audiology and mental health services, otherwise authorized
State Issues:HHS Omnibus Bill
Restores Emergency Medical Assistance coverage for dialysis and cancer treatments
Repeals Minn. Rule that required physician authentication (signature) of verbal/emergency orders within 24 hours
State Issues:Radiation Therapy
The current moratorium in 14 counties stays in place until 2014
After 2014, can’t build a new radiation facility within 7 miles from a current facility
Maintained the requirement that any new radiation facility must be built in collaboration with a hospital
State Issues:Miscellaneous
Enacted a new felony-level offense for intentional deprivation of a vulnerable adult.• Provides affirmative defenses for caregivers acting in good
faith Amended MN’s No-Fault Auto Insurance statute.
• Restricts the use of “runners and cappers” which can generate inappropriate health care services.
• $20,000 in medical coverage remains in place. Newborn screening bill responds to court ruling
• Opt-out for testing• Opt-in for allowing MDH to store sample for 18 years
Other policy issues raised but not enacted
Interstate Nurse Licensure Compact Partial restoration of Medical Education Research
Costs (MERC) Health Insurance Exchange 1-year restoration of 5% cut to outpatient
provider rates Leapfrog mandate
Other policy issues raised but not enacted
Mandatory nurse-to-patient staffing ratios• Bills introduced (SF 2182; HF 2618)• MHA successful at keeping bills from getting hearings
in either House or Senate• Major, contentious issue for 2012 elections and 2013
sessiono MN hospitals already provide safest, highest quality care in
the countryo Mandated ratios not shown to improve care safety or qualityo Hospitals need flexibility to staff for patient acuity and
caregivers’ experience/skill levelo Mandated ratios increase the cost of care significantly
Place picture here
Attorney General Agreement
Current Requirements:Based on 2005 agreement &2007 extension
Cap on charges to uninsured• Uninsured pay amount equal to what hospital’s “Most
Favored Insurer” pays Adopt charity care and debt collection policies Limit debt collection litigation (and litigation-like)
• Limit on garnishment, contingency fees, credit bureau reports
• Requires senior corporate officer review at each step of litigation process
Modifications in new extension
5-year extension Modify Attorney General contact information on
hospital collection notices so patients contact hospital first, then AG if issue is unresolved
Clarify that hospitals may respond to patient inquiries verbally, not just in writing

Place picture hereFederal Issues
Federal budget not getting any prettier
Rep. Paul Ryan budget proposal• Shift Medicare to voucher program• Shift Medicaid to block grant
Debt ceiling deal from 2011 called for 2% across-the-board cuts• Goes into effect Jan. 1, 2013• Includes Medicare and critical access hospitals• Will not apply to Medicaid
President Obama proposed additional hospital and provider cuts
Critical Access Hospitalsno longer “under the radar”
President proposed cutting payments 1% President proposed eliminating CAH status for
hospitals within ten miles of another hospital• Others proposed 20 miles
Independent Payment Advisory Board pending• 15 members appointed by the President• Required to cut $13 billion in six years from
CAHs, physicians or other non-hospital providers (while physician sustainable growth rate cuts remain unresolved)

Health Reform:Trends and
Speculations
ACA in Limbo
Meanwhile . . .
States are spending hundreds of millions of dollars in federal grant funds to construct health insurance exchanges
Insurance plans extended coverage to dependent children up to age 26
Minnesota expanded Medicaid to cover childless adults up to 75% of FPL
All dependent on legality of ACA
Health care reform initiatives in Minnesota
Gov. Dayton began early Medicaid enrollment• 100,000+ people eligible for Medicaid coverage• Decrease uninsured population by 28,000; decrease
underinsured population by 75,000• Medicaid is more meaningful coverage with statewide
access to providers Gov. Dayton building health insurance exchange
• Using more than $36 million in federal grants• Controversy with GOP legislators over authority to spend
federal grants without enabling legislation• State must make substantial progress on Exchange by 2013
or federal government will run MN’s Exchange
Health Care Home:Minnesota’s medical home model
Requires certification by the state Multiple payers participating
• Medicaid• State employees• Medicare• Commercial
Care coordination fee varies based on number of chronic/complex conditions from $10/month for 2 conditions to $60 (Medicaid) or $45/month (Medicare) for 10 conditions
Health Care Home:Minnesota’s medical home model
150 clinics certified in MN so far• Provide care for 438,000 non-Medicare
patients, although many, many fewerhave enrolled to receive health care home services
• Total Medicaid care coordination fee payments to providers are much smaller than predicted because of lower-than expected enrollment
Bundled payments
Lump payment for services patient receives from multiple providers for same episode or condition
Flexibility in program • Benefits providers assembling bundles• Makes it more difficult to for other providers to
discern what works, best practices, etc. Integrated or collaborative providers have
better opportunity to succeed
Bundled Payments
MHA members applying for CMS’ Bundled Payment program• MHA-led consortium of 8 hospitals
CentraCare Fairview Southdale Fairview RidgesFairview UMMC North Memorial RegionsPark Nicollet St. Luke’s
• Other MHA members submitting applicationsEssentia HealthEast Mayo
Accountable Care Organizations Group of providers that agree to care for an entire
population of patients & achieve quality and cost thresholds
Medicare proposed Shared Savings Program• Min. 5,000 Medicare beneficiaries• 33 quality measures required to be reported
• 2-4% savings threshold before eligible for shared savings bonus
• Withhold of 25% of any savings bonus• soon
Accountable Care Organizations
MHA seeking rural ACO modelsfrom CMS Center for Innovation
Micro-ACOs• Specify smaller region, subpopulation of patients
(e.g., dual eligibles), and less financial risk• Focus on total cost of care coordination, not
necessarily total cost of care delivery Uncoupled-ACOs
• Non-hospital-provider ACO within community/region• Allow CAH to retain cost-based reimbursement• Create financial rewards for ACO/community
providers based on total cost (including hospitalization) and quality

Three Minnesota health systems certified as Pioneer ACOs by CMS
• Allina Hospitals & Clinics
• Fairview Health Services
• Park Nicollet Health Services(also participated in Physician Group Practice demonstration)
Accountable Care Organizations
Accountable Care OrganizationsMedicaid
Demonstration projects on the horizon• State issued Request for Proposals (RFP), which gave
hospitals more flexibility• Contract negotiations on-going• Nine applicants
CentraCare Children’s Hospitals EssentiaFairview FQHCs in Twin Cities Mayo ClinicNorth Memorial Park NicolletAllina
Hennepin County has similar, ambitious project • Includes corrections, social services, courts, etc. as well
as health care in total cost of care calculation
Examples of ACO considerationsfor potential partnerships
Potential provider/partner must• Meet defined performance measures on quality,
experience and cost• Have capability to use ACO network’s resources and
optimize transitions of care• Share clinical and financial data with ACO• Commit to use ACO’s analytics, metrics• Participate in case review and performance
improvement discussions• Use or refer to other ACO network providers• Help reduce ACO network’s readmissions
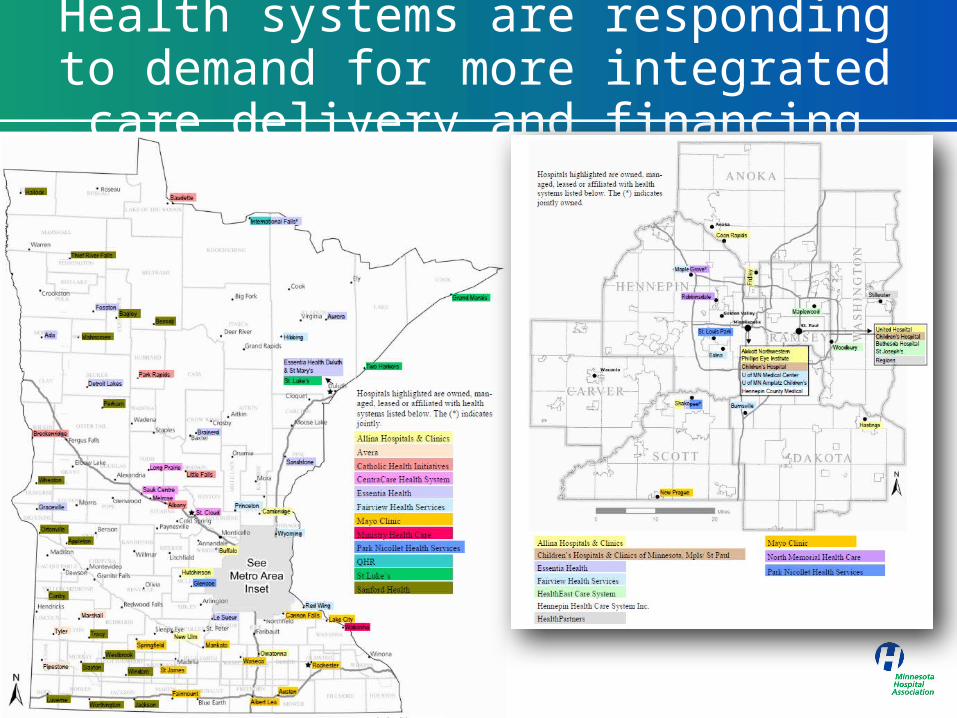
Health systems are responding to demand for more integrated care delivery and financing

Questions&
Discussion