Embed Size (px)
Citation preview

Starving Away Stubborn Seizures:
Food for Thought on the Ketogenic Diet for Refractory Epilepsy in Children
Bernadette Espiritu, Pharm.D. PGY1 Pharmacy Resident
Children’s Hospital of San Antonio The University of Texas Health Science Center at San Antonio
The University of Texas at Austin College of Pharmacy
April 17, 2015
Learning Objectives
1. Discuss the background, dietary composition, adverse effects, and challenges of the ketogenic diet2. Describe the pharmacist’s role in the management of the ketogenic diet patient3. Evaluate the literature regarding use of the ketogenic diet in pediatric refractory epilepsy4. Formulate an evidence-based strategy deciding the role of the ketogenic diet in the management of
pediatric refractory epilepsy compared to alternative pharmacotherapy

Espiritu | 1
I. Definitions A. Seizure1-3
i. Clinical manifestation of excessive, synchronous abnormal electrical activity of neurons in the cerebral cortex
ii. Interferes with normal functioning iii. Due to shift in normal balance of excitation and inhibition in the central nervous
system a. Glutamate is the major excitatory neurotransmitter b. γ-aminobutyric acid (GABA) is the major inhibitory neurotransmitter
B. Epilepsy2,3
i. > 2 unprovoked afebrile seizures > 24 hours apart ii. Diagnosis of an epilepsy syndrome
iii. Recurrent seizures due to chronic, underlying process C. Refractory epilepsy4,5
i. Inadequate seizure control despite appropriate therapy with > 2 antiepileptic drugs (AEDs) at maximally tolerated doses for 18 months to 2 years
ii. Adequate seizure control with unacceptable drug-related adverse effects II. Epidemiology
A. Seizures affect 4-10% of children at some point in their lifetime7 i. Approximately 150,000 children experience new-onset seizure annually
ii. Only 30,000 children with new-onset seizure will develop epilepsy B. Currently 326,000 children with a diagnosis of epilepsy in the United States4,7,8
i. 60-70% of children become seizure free with moderate doses of one or two AEDs8 ii. Estimated 10-40% will continue to have seizures despite optimal management with
AEDs4 iii. Approximately one-third of epilepsy will be refractory4
PEDIATRIC EPILEPSY
Figure 1. International League Against Epilepsy (ILAE) Classification of Seizures6

Espiritu | 2
III. Prognosis and comorbidities2,5 A. Cognitive deficits and abnormalities B. Psychiatric comorbidities C. Non-fatal injuries D. Risk of death is 2-3 times greater in patients with epilepsy
i. Underlying etiologies of seizure ii. Accidents
iii. Status epilepticus iv. Sudden unexpected death in epileptic patients (SUDEP)
IV. Treatment A. Goal of therapy is improved quality of life3,8
i. Elimination or reduction in seizures ii. Minimize adverse effects from therapy
iii. Manage comorbid conditions a. Address underlying conditions contributing to epilepsy b. Depression, anxiety, pain, sleep disorders
B. Approach to refractory epilepsy3-5 i. Non-pharmacologic
a. Avoid triggers b. Surgical intervention c. Vagal nerve stimulation d. Dietary therapy
ii. Pharmacologic
I. Background9-11 A. Mimics the biochemical changes that occur during the starvation state leading to ketosis B. Majority of calories from fat, with moderate protein and very low carbohydrate
i. Calories initially limited to 80-90% of daily recommended needs ii. Adjusted to accommodate ideal growth and patient safety
iii. Historically included fluid restriction, though no longer done in practice
Table 1. Potential uses of KD11,12
Epilepsy Weight loss Autism Brain tumors Depression Narcolepsy Alzheimer’s disease
Traumatic brain injury Parkinson’s syndrome Amyotrophic lateral sclerosis Migraines Sleep disorders Schizophrenia Post-anoxic brain disorders
II. History in epilepsy
A. Early history of KD13-15 i. Fasting for epilepsy recorded by Hippocrates in 5th century BC
ii. Gospel of Matthew describes Jesus curing epileptic boy with “fasting and prayer”
THE KETOGENIC DIET (KD)

Espiritu | 3
B. Modern history of KD9,14-16 i. 1911: French physicians, Guelpa and Marie, author first scientific report of fasting
for epilepsy ii. 1921: Dr. R.M. Wilder at the Mayo Clinic proposes diet to mimic fasting state
iii. 1938: Phenytoin discovered; decline in use of KD iv. 1971: Medium-chain triglyceride diet introduced v. 1994: Resurgence of KD due to success in Charlie Abrahams15
a. Charlie was 2-year old son of a Hollywood producer who experienced intractable myoclonic, generalized tonic, and tonic-clonic seizures
b. Gained national attention for successful use of KD to control his seizures c. The Charlie Foundation created for KD and epilepsy d. Made-for-television movie based on Charlie’s experience with KD
vi. 2008: First randomized, controlled trial of KD17 III. Starvation state18,19
A. Body forced to metabolize fatty acids B. Brain dependent on formation of ketone bodies in the liver, transported over blood-brain
barrier i. β-hydroxybutyrate (BHOB)
ii. Acetoacetate (ACAC)
IV. Mechanism of action9,18 A. Despite decades of use, mechanism of action remains elusive B. Many postulated mechanisms, though likely a combination of simultaneous mechanisms C. Hypothesized mechanisms9,11,18,21
i. Ketone bodies/ketosis a. ACAC and acetone have anticonvulsant properties
1. Demonstrated in animal models 2. Acetone levels elevated in brains of patients treated with KD
b. BHOB structurally similar to GABA c. Consumption of oxaloacetate in ketotic state shunts glutamate to GABA
synthesis
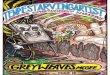
Figure 2. Production of ketones by the liver and utilization by the brain20

Espiritu | 4
Figure 3. Proposed mechanism of KD by opening of KATP channels23
ii. Lack of glucose limits ability of brain to generate and promote seizure activity iii. Direct anti-seizure activity of polyunsaturated fatty acids produced while on KD iv. Opening of ATP-sensitive potassium (KATP) channels22
a. KATP channels normally inhibited by high intracellular ATP b. Shift away from glycolytic ATP production allows KATP channels to open c. Open KATP channels reduce neuronal excitability in the substantia nigra
V. Dietary composition9,11,24 A. Classic KD
i. Diet allotted in a 4:1 fat to carbohydrate/protein ratio per weight ii. Lower ratios (3:1 or 2:1) may be used in younger children
iii. Oldest and most studied diet B. Medium-chain triglycerides (MCT) diet
i. MCT more ketogenic than long-chain triglycerides (LCT) ii. Greater allowance for protein and carbohydrates
iii. MCT sources include coconut oil, palm kernel oil, whole milk, butter C. Modified Atkins diet
i. More tolerable than classic KD and MCT diet ii. Carbohydrate restricted, unlimited protein, fat, and fluids
a. Carbohydrate initially limited to 10 grams b. Planned increase to 15-20 grams of carbohydrates/day in 1-3 months c. Fats highly encouraged

Espiritu | 5
VI. Tolerability (Appendix A) A. Not a “natural” treatment for epilepsy13
i. Parents should not start the diet without medical guidance ii. Should be initiated and monitored by a physician working with the health-care
team B. Compliance11
i. Difficult to tolerate a. 40-50% will discontinue diet within first 6 months9 b. Requires accurate measurement of all components of the diet c. Hidden sources of carbohydrates in diet and other products d. Strict compliance is necessary for benefits of the diet
1. Small lapses are enough to stop ketosis9 a. Not finishing a meal b. Consuming too much carbohydrate or protein
2. Non-compliance may lead to seizures ii. More palatable diets available11
a. Less restrictions and adverse effects b. Modified Atkins diet c. MCT diet
iii. All-liquid formulations of the diet are available for infants and enterally fed children a. Easier to implement b. More compliance and greater efficacy25
iv. When attempted, should be tried for at least 3 months v. Patients who respond to and tolerate diet should continue for at least 2 years
VII. Safety A. Adverse effects11,13,21,24
i. Initiation phase11,24 a. Dehydration b. Hypoglycemia c. Vomiting
Figure 4. Comparison of the calorie composition of the typical American diet and dietary therapies for epilepsy11,19,24

Espiritu | 6
ii. Maintenance phase a. Gastrointestinal11,21,24
1. Constipation 2. Exacerbation of gastroesophageal reflux disease (GERD)
b. Nephrolithiasis11,13,21,24 1. 3-10% experience nephrolithiasis 2. Prevent with adequate hydration and avoidance of medications
that may cause nephrolithiasis 3. Oral potassium citrate may decrease prevalence
c. Hypertriglyceridemia11,13,21,24 1. Particularly in first six months 2. Kwiterivoch et al. studied effect on lipid profile after six months of
diet26 a. Significant increase in total cholesterol, low-density
lipoprotein, very low-density lipoprotein, and triglycerides b. Significant decrease in high-density lipoprotein
3. Used successfully in children with pre-existing hyperlipidemia d. Growth/nutrition11,13,16,21
1. Significant reduction in height and weight after prolonged use 2. Catch-up growth observed after diet discontinuation27 3. Increased risk of bone fractures 4. All children on KD must receive supplements
a. Vitamins and minerals (including trace minerals) b. Calcium and vitamin D c. Oral citrates and carnitine optional
B. Contraindications11,24 i. Relative contraindications: patients who have more curative alternatives, difficulty
with compliance, or comorbidities that may be exacerbated by KD ii. Absolute contraindications: inborn errors of metabolism where biochemical
changes due to KD are dangerous
Table 2. Relative and absolute contraindications of KD11,24
Relative Absolute
• Epilepsy surgery candidates • Failure to thrive/poor nutritional status • Special diet needs/preferences • Parent/caregiver noncompliance • Medical conditions aggravated by diet
• Primary carnitine deficiency • Carnitine palmitoyltransferase I or II deficiency • Carnitine translocase deficiency • Fatty oxidation defects • Porphyria • Pyruvate carboxylase deficiency

Espiritu | 7
I. Combined with AEDs
A. Evidence supporting pharmacodynamics interactions between KD and AEDs is weak24 B. Valproic acid24,28
i. Valproic acid is a short-chain fatty acid ii. Enhanced fatty acid oxidation with KD may enhance valproic acid-related
hepatotoxicity iii. Carnitine deficiency24
a. Both valproic acid and KD alone cause carnitine deficiency b. May be worsened in combination
C. Carbonic anhydrase inhibition i. Metabolic acidosis24
a. Carbonic anhydrase inhibitors (CAIs), topiramate and zonisamide, may worsen transient metabolic acidosis associated with KD
b. Serum bicarbonate 1. Monitor when initiating KD with topiramate and/or zonisamide 2. Supplement with bicarbonate in clinically symptomatic patients
ii. Nephrolithiasis21 a. CAIs increase risk of nephrolithiasis b. Monitor patients carefully when initiating KD c. Consider empiric oral citrates
D. Phenobarbital28 i. Elimination slower in acidotic state, resulting in higher levels
ii. Patients on phenobarbital may not respond as well to KD II. Medications containing carbohydrates (Appendix B)28,29
A. Formulations of AEDs and other medications may contain carbohydrates or sugar additives28-30
i. “Sugar-free” products may still contain other carbohydrate fillers ii. IV fluids, TPNs, diluents
B. Strategies for reducing carbohydrate content of medications29,30 i. Liquids > chewable/disintegrating tablets > tablets/capsules in carbohydrate
content a. Crush tablets or open capsules of products able to be crushed or opened b. Generics may contain more carbohydrate fillers than brand name products c. IV formulations may be given orally
ii. Avoid dextrose containing diluents, if alternatives compatible III. Pharmacologic management and prevention of adverse effects10
A. Proton-pump inhibitors for GERD B. Potassium citrate to prevent nephrolithiasis C. Vitamin and mineral supplementation D. Constipation management
IV. Alternative to AEDs A. Good responders to KD may discontinue AEDs31
i. Possible seizure exacerbations when AEDs are weaned ii. During withdrawal while on KD, phenobarbital and benzodiazepines are most
associated with breakthrough seizures B. Must weigh benefits of starting KD versus trying another AED
ROLE OF A PHARMACIST IN KD

Espiritu | 8
Figure 4. Mechanisms of action of AEDs32
I. When should KD be considered over alternative AEDs in pediatric patients with refractory epilepsy? II. International Ketogenic Diet Study Group24
A. Neurologists and dieticians commissioned by The Charlie Foundation B. Recommend strong consideration of KD after 2-3 failed AEDs
III. Approach to pharmacotherapy in refractory epilepsy
A. Address causes for treatment failure5,8 i. Inappropriate choice of first-line AED
ii. Poor compliance iii. Lifestyle factors iv. Intolerable adverse effects
B. Considerations in AED selection5,8,33 i. Seizure/epilepsy type (Appendix C)
ii. Adverse effects (Appendix D) iii. Drug interactions iv. Cost v. Pharmacokinetics & drug monitoring
CLINICAL QUESTION

Espiritu | 9
IV. Efficacy in epilepsy trials A. Efficacy measures8,34
i. Mean percentage (%) of baseline a. Compares baseline seizure control against seizure control after
intervention b. Often involves total number of seizures before and after intervention
ii. 50% responder rate8 a. Proportion of patients with more than 50% reduction in seizures b. Common efficacy measure reported in literature and randomized,
controlled trials c. Patients will be considered “responders” or “non-responders” based on
50% responder rate iii. 90% responder rate
a. Proportion of patients with more than 90% reduction in seizures b. Corresponds to “very good” responders
iv. Seizure freedom a. Patients experiencing freedom from seizures b. Corresponds to total or complete response to therapy
B. Efficacy of pharmacotherapy in refractory epilepsy5,35 i. 15-20% of patients may achieve > 6 months of seizure remission with additional
drug trials ii. 30-40% of refractory patients will receive > 50% reduction in seizure frequency with
adjunctive polytherapy iii. Average drop-out rates in most AED trials for refractory epilepsy range from 5-10%
Table 3. Efficacy of AEDs in adjunctive treatment of refractory epilepsy35-42
AED 50% Responder Rate AED 50 % Responder Rate
Clobazam 43-65% Pregabalin 14-51%
Felbamate 33-56% Rufinamide 28.2-46.7%
Gabapentin 34.4% Tiagabine 25%
Lamotrigine 33-45% Topiramate 20-88%
Lacosamide 38-41% Valproic Acid 50-60%
Levetiracitam 27-52% Vigabatrin 28-80%
Oxcarbazepine 41% Zonisamide 26-67%

Espiritu | 10
Neal EG et al. The ketogenic diet for the treatment of childhood epilepsy: a randomized controlled trial. Lancet Neuro. 2008;7:500-06.17
Overview
Objective To investigate whether there are clear benefits in terms of seizure control in children with epilepsy who were treated with the classic KD for 3 months compared with a control group of children whose treatment did not change
Trial Design Open-label, parallel-group, randomized-controlled trial in the United Kingdom (UK)
Patients
Inclusion Criteria
Age between 2-16 years
Daily seizures or > 7 seizures per week
Non-responder to > 2 AEDs
Not previously treated with KD
Exclusion Criteria
History of: o Hyperlipidemia o Nephrolithiasis o Organic-acid-deficiency syndromes
Outcomes
Primary
% change in baseline seizures
Proportion of children with: o >90% reduction in seizures o >50% reduction in seizures
Secondary
Tolerability of diet o Adverse effects o Compliance o Growth
Interventions
Children randomly assigned to start diet immediately after 4-week baseline (diet group) or delayed by 3 months after 4-week baseline (control group)
Control group remained on regular diet with no changes in AEDs
Diet group given an individual KD based on child’s food preferences with no changes in AEDs
KD started at home, non-fasting o 2:1 ratio to begin, with initiation to 3:1 or 4:1 over 1-2 weeks as tolerated o Diets supplemented with vitamins and minerals
Patients reviewed outpatient at 6 weeks and 3 months with telephone calls between visits
Seizures frequency assessed and recorded by parents daily during baseline and study period
Statistical Analysis
Sample size of 47 patients per group needed to detect a 25% difference in mean percentage of baseline seizures significant at 5% with 90% power
Mean % of baseline seizures compared with unpaired t-test; verified with Mann-Whitey U test
Multiple linear regression to assess association between diet and % baseline seizures taking into account baseline characteristics of age group and gender
Fisher’s exact test for calculating difference in diet and control groups for responder rates of 50% or 90% seizure reduction
Unpaired t-test comparing mean % of baseline seizures between diet and control group for generalized and focal seizures
Results
Baseline characteristics
Provided table of baseline characteristics for gender and age but no clear analysis o Most children in diet group in 2-6 year age group (N=37), followed by 7-11 year age group
(N=27) and the 12-16 year age group (N=9)
6 children on no epilepsy medications at entry, 20 children on one medication, 53 children on 2 medications, and 54 children on 3 medications o No mention of how many failed AED treatments prior to enrollment
Epilepsy types and syndromes similar in control and diet groups
Mean of 13.3 seizures/day in KD group and 10.1 seizures/day in control group
LITERATURE REVIEW

Espiritu | 11
Primary outcomes
16 patients (8 from each group) dropped out before study period began
26 patients (11 from KD group and 15 from control group) not included in final analysis due to drop-outs or inadequate data after study period began
Table 4. Comparison of seizures as percentage of baseline after 3 months
Outcome Diet group (N=54) Control group (N=49) p-value
Mean % of baseline seizures (95% CI) 62.0 (50-74%) 136.9% (105-169%) <0.0001
Median % of baseline seizures (SD, IQR)
47.7% (43, 0-200%)
106.3% (111, 28-575%)
-----
Difference in mean % of baseline seizures remained significant after accounting for outliers o Linear regression model: difference between mean % baseline seizures increased to 76.6%
(95% CI 44.4-108.9; p<0.0001) o Removal of extreme outliers in control group: difference between mean % baseline seizures
reduced to 50.9% (95% CI 30-7-71.2%; p<0.0001)
No significant differences found when comparing mean % of baseline seizures for generalized or focal seizures in either the control or diet group
Table 5. Responder rate in diet group vs control group
Outcome Diet group (N=73) Control group (N=72) p-value
>90% reduction in seizures 5 (7%) 0 (0%) 0.0582
>50% reduction in seizures 28 (38%) 4 (6%) <0.0001
<50% reduction in seizures 45 (62%) 68 (94%) <0.0001
Secondary outcomes
Adverse effects in the diet group included constipation (33%), constipation requiring medication (24%), lack of energy (24%), vomiting (25%), hunger (22%), diarrhea (13%), and abdominal pain (9%)
10 patients withdrew from dietary treatment o 3 due to parental unhappiness with restrictions, 2 due to behavioral food refusal, 1 due to
increased seizures and 4 due to adverse effects (extreme drowsiness, vomiting, diarrhea, and constipation)
One patient, who remained on the diet, had evidence of nephrolithiasis treated with potassium citrate
Conclusions
Author’s conclusions
The diet has efficacy and should be included in management of children with drug-resistant epilepsy. Side effects should be considered alongside with the risk/benefit of other treatments.
Critique
Strengths
Randomized, controlled
Enrollment achieved power
Responder rates reported as intention-to-treat
Results robust after accounting for outliers
Limitations
Non-blinded
Compared with placebo
Subjective recording of seizures and adverse effects
No details on failed AEDs
Per-protocol with high drop-out rate
Cultural diet differences
Lacked clear analysis of baseline characteristics
Take-home points
First randomized, controlled trial of KD
High number of drop-outs and non-starters
Effective in reducing seizures but not without adverse effects/intolerability
No data on number of failed AEDs
Cultural diet differences

Espiritu | 12
Sharma S et al. Use of the modified Atkins diet for treatment of refractory childhood epilepsy: a randomized controlled trial. Epilepsia. 2013;54(3):481-486.43
Overview
Objective To evaluate the efficacy of the modified Atkins diet in a randomized controlled trial in children with refractory epilepsy
Trial Design Open-label, parallel-group, randomized-controlled trial in India
Patients
Inclusion Criteria
Age between 2-14 years
Daily seizures or > 7 seizures per week
Failure of > 3 AEDs
Exclusion Criteria
Known/suspected inborn errors of metabolism
Systemic illness
Motivational issues with family
Outcomes
Primary
% change in seizure frequency compared to baseline
Proportion of children with: o Seizure freedom o >90% reduction in seizures o >50% reduction in seizures
Secondary
Tolerability of diet
Adverse effects
Interventions
Assigned to modified Atkins diet group or control group (no diet changes)
4-week baseline observation period followed by study period o Recorded daily seizure log by parents (seizure type, duration, and frequency)
Both groups remained on same AEDs during 3 month trial period and throughout the study, unless medically indicated
Intervention arm began modified Atkins diet as outpatients at end of baseline period o Carbohydrate intake of 10 grams/day o Intake of fats encouraged o Calories and protein intake not restricted o Received sugar-free, fat-soluble vitamin supplement and calcium supplement o Recipes provided, based on patient’s dietary habits (e.g. vegetarian) o Urine ketones checked by parents daily during the first week and twice weekly thereafter
Reviewed as outpatients at 1, 2, and 3 months
Three-day dietary intake chart reviewed at each visit in diet group to calculate carbohydrate and calorie intake, and to reinforce compliance
Tolerability and adverse effects evaluated by parental interview
Statistical Analysis
Calculated sample size of 48 in each group to detect 25% difference in primary outcome at 5% with 90% power
All analysis intention-to-treat
Drop outs were treated as worst case scenario in the treatment group (0% seizure control) and as best case scenario in the control group (100% seizure control)
Mean % of seizures compared with unpaired t-test/Mann-Whitney U test
Responder rates (seizure freedom, >50% and >90% seizure reduction) compared using Fisher’s exact test
Results
Baseline characteristics
102 children enrolled (diet group=50, control group=52)
No significant differences in baseline characteristics between groups
Average age of 4.7 years in diet group and 5.2 years in control group
Median of 5 (range 3-9) AEDs tried in diet group; median of 4 (range 3-9) tried in control group)
Median of 3 ongoing AEDs (range 2-4) in both groups during study period

Espiritu | 13
Primary outcomes
No significant differences in response between epilepsy syndromes Table 6. Seizure outcome at 3 months
Diet group (N=50)
Control group (N=52)
p-value
Mean % of seizures compared to baseline 59 ± 54 (95% CI 44-74.5)
95.5 (95% CI, 82-109)
0.003
Median % of seizures as compared to baseline (IQR) 37 100 0.003
>90 % responder rate 30% 7.7% 0.003
>50% responder rate 52% 11.5% 0.001
Proportion of children seizure free 10% 5.8% (drop-outs) -----
Secondary outcomes
Adverse effects in the diet group included constipation (46%), anorexia (18%), vomiting (10%), lethargy (6%), lower respiratory tract infections (4%), hyperammonemic encephalopathy (2%)
4 patients discontinued the diet o 3 due to adverse effects (2 with frequent chest infections, 1 for hyperammonemic
encephalopathy 1 week after starting the diet) o 1 child discontinued because family found diet too restrictive
Older children complained that diet was too restrictive and difficult
Diet more difficult to tolerate in patients with dietary restrictions (vegetarians)
Conclusions
Author’s conclusions
The modified Atkins diet was found to be effective and well tolerated in children with refractory epilepsy. However, the diet does have adverse effects, and careful medical supervision is warranted.
Critique
Strengths
Randomized, controlled
Enrollment achieved power
Intention-to-treat analysis
Limitations
Non-blinded
Compared with placebo
Excluded families with “motivational issues”
Cultural diet differences
Subjective recording of seizures and adverse effects
Take-home points
Diet effective in reducing seizures, though not without adverse effects
50% responder rate = 52%
Average of 4-5 failed AEDs before starting treatment
Difficult to tolerate in older children and patients with diet restrictions
Cultural dietary differences

Espiritu | 14
Kossoff EH et al. A randomized, crossover comparison of daily carbohydrate limits using the modified Atkins diet. Epilepsy Behav. 2007;10(3):432-6.44
Overview
Objective To identify the ideal starting limit of carbohydrates on the modified Atkins diet to maximize efficacy, ketosis, and tolerability
Trial Design Prospective, randomized, crossover study in the United States (US)
Patients
Inclusion Criteria
Age between 3-18 years
Failure of > 2 AEDs
At least daily, countable seizures
Exclusion Criteria
Use of Atkins diet < 7 days previously
Known hypercholesterolemia, kidney dysfunction, or heart disease
Recent (<1 year)/current use of KD
BMI <3% for age
Outcomes
Primary
Proportion of children with: o Seizure freedom o >90% reduction in seizures o >50% reduction in seizures
Secondary
Ketosis
Tolerability of diet
Adverse effects
Interventions
Patients randomized to begin diet with 10 grams or 20 grams per day o Baseline blood counts, fasting lipid profile, comprehensive metabolic profile, urine calcium
and creatinine levels obtained o 3-day pre-diet food record analyzed o Diet explained to families in hour long visit o Monthly calendar to record seizures daily, ketones semi-weekly, and weight weekly o Frequent contact with physician and dietitians via phone and e-mail o Each patient received multivitamin and calcium supplement o At 3 months, patients were crossed over to opposite amount (i.e. 10 gram 20 gram, 20
gram 10 gram)
Children evaluated at baseline, 3 months and 6 months o Urine ketones checked semi-weekly and urine/laboratory tests repeated at 3 months and 6
months o Medication changes allowed after 2 weeks if requested by families o Families given the option to continue diet with carbohydrate limit of their choice, or
discontinue diet after 6 months
Statistical Analysis
Calculated total number of 20 patients needed to show difference of 20% between group assuming a 40% dropout rate
Categorical data analyzed with Fisher’s exact test
Medians compared using Wilcoxon two-sample test; means with paired two-sample t test
Significance level set at P=0.05
Intention-to-treat analysis
Results
Baseline characteristics
N=20 (10 patients in each carbohydrate group)
No differences in baseline characteristics between groups
Average age of 7.5 years in 10 gram group and 9.8 years in 20 gram group
Average number of 6 AEDs previously tried in each group
Average of 2 concurrent AEDs in each group
4 patients previously attempted on KD with no reported improvement (randomized 2 patients to each group)

Espiritu | 15
Primary outcomes
Table 7. Seizure outcomes at 1, 3, and 6 months
10 gram group (N=10) 20 gram group (N=10) p-value
1 month >50% seizure reduction 6 (60%) 4 (40%) 0.33
>90% seizure reduction 0 (0%) 1 (10%) 0.50
3 months >50% seizure reduction 6 (60%) 1 (10%) 0.03
>90% seizure reduction 3 (30%) 0 (0%) 0.10
6 months >50% seizure reduction 5 (50%) 5 (50%) 0.67
>90% seizure reduction 3 (30%) 4 (40%) 0.50
Secondary outcomes
Table 8. Tolerability outcomes in diet group
10 gram group (N=10) 20 gram group (N=10) p-value
Diet duration (in months) 9.0 (3-22) 4.5 (0-19) 0.12
Number completing 6-month study 7 (70%) 5 (50%) 0.33
Of the 12 patients who completed the study, 9 decided to continue on modified Atkins diet after 6 months
4 patients reported significant constipation while on diet
Conclusions
Author’s conclusions
A starting carbohydrate limit of 10 grams/day for children starting the modified Atkins diet may be ideal, with a planned increase to 20 grams/day after 3 months. The study adds further prospective evidence for the efficacy and safety of the modified Atkins diet for refractory pediatric seizures.
Critique
Strengths
Randomized
Enrollment achieved
Intention-to-treat analysis
Conducted in the US
Data on number of failed AEDs
Limitations
Non-blinded, not controlled
Subjective recording of seizures
Small sample
High drop-out rate
Take-home points
Diet effective in reducing seizures (50% responder rate of 10-60%)
High drop-out rates suggest poor tolerability
Average of 6 failed AEDs before starting diet
Conducted in the United States
I. Summary of literature
A. Responder rate (>50% reduction in seizures) i. Range from 10-60% in prospective, randomized trials
ii. 38-52% in prospective, randomized, controlled trials B. Average of 4-6 AEDs tried prior to trying KD C. Tolerability
i. Most common side effects are gastrointestinal, particularly constipation ii. High drop-out rates, particularly in the UK and US
iii. More difficult to tolerate in older patients and those with diet restrictions D. Lack of head-to-head trials comparing alternative AED and KD in refractory epilepsy, or
starting KD earlier in management II. KD treatment
A. Effective treatment for pediatric refractory epilepsy B. Requires strict compliance to achieve benefits C. Pharmacists can play a role in the management of a child on KD
SUMMARY

Espiritu | 16
I. Recommendations A. Due to availability and efficacy of alternative AEDs, KD should not be considered in most
children until failure of at least 4 AEDs i. Difficulties with tolerability and compliance limit use of KD
ii. High drop-out rates in studies iii. Alternative AEDs or polytherapy should be considered first in refractory epilepsy
B. Considerations of starting KD vs. AED i. Type of seizure/epilepsy syndrome
ii. Patient age iii. Diet preferences and cultural considerations iv. Family compliance and motivation v. Cost
vi. Enteral feeding vii. Adverse effects of KD and AEDs
viii. Concurrent medications ix. Available alternative treatment(s)
II. Future directions A. Discovering mechanism of KD may provide targets for future AEDs B. Head-to-head trials of KD vs. starting another AED C. Trials of KD earlier in treatment
RECOMMENDATIONS

Espiritu | 17
1. Welty TE, Faught E. Chapter 30. Epilepsy. In: Chisholm-Burns MA, Kolesar JM, Malone PM, ed. Pharmacotherapy Principles and Practice. 2nd ed. New York, NY: McGraw-Hill; 2010:521-539.
2. Lowenstein DH. Chapter 369. Epilepsy. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson J, Loscalzo J, ed. Harrison's Principles Of Internal Medicine. 18th ed. New York, NY: McGraw-Hill; 2012. Available at: http://accesspharmacy.mhmedical.com.ezproxy.lib.utexas.edu/content.aspx?sectionid=40727185&bookid=331. Accessed March 6, 2015.
3. Rogers SJ, Cavazos JE. Chapter 40. Epilepsy. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L, ed. Pharmacotherapy: A Pathophysiologic Approach. 9th ed. New York, NY: McGraw-Hill; 2014. Available at: http://accesspharmacy.mhmedical.com.ezproxy.lib.utexas.edu/content.aspx?sectionid=45310490&bookid=689&Resultclick=2. Accessed March 3, 2015.
4. Go C, Snead OC. Pharmacologically intractable epilepsy in children: diagnosis and preoperative evaluation. Neurosurg Focus. 2008;25(3):E2.
5. Schuele SU, Lüders HO. Intractable epilepsy: management and therapeutic alternatives. Lancet Neurol. 2008;7(6):514-24.
6. Berg AT, Berkovic SF, Brodie MJ, et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE Commission on Classification and Terminology, 2005-2009. Epilepsia. 2010;51(4):676-85.
7. Agarwal M, Fox SM. Pediatric seizures. Emerg Med Clin North Am. 2013;31(3):733-54. 8. Raspall-Chaure M, Neville BG, Scott RC. The medical management of the epilepsies in children: conceptual and
practical considerations. Lancet Neurol. 2008;7(1):57-69. 9. Greener M. Food for thought: the ketogenic diet for epilepsy. Prog Neuro Psychiatry. 2014 May/June. 18(3): 6-9. 10. Kossoff EH, Zupec-Kania BA, Rho JM. Ketogenic diets: an update for child neurologists. J Child Neurol. 2009;24(8):979-
88. 11. Sharma S, Jain P. The ketogenic diet and other dietary treatments for refractory epilepsy in children. Ann Indian Acad
Neurol. 2014;17(3):253-8. 12. Barañano KW, Hartman AL. The ketogenic diet: uses in epilepsy and other neurologic illnesses. Curr Treat Options
Neurol. 2008;10(6):410-9. 13. Sinha SR, Kossoff EH. The ketogenic diet. Neurologist. 2005;11(3):161-70. 14. Wheless JW. Chapter 2. History and Origin of the Ketogenic Diet. In: Stafstrom C, Rho J, ed. Epilepsy and the
Ketogenic Diet. 1st ed. Totowa, NJ: Humana Press, Inc.; 2004:31-5 15. Wheless JW. History of the ketogenic diet. Epilepsia. 2008;49 Suppl 8:3-5 16. Papandreou D, Pavlou E, Kalimeri E, Mavromichalis I. The ketogenic diet in children with epilepsy. Br J Nutr.
2006;95(1):5-13. 17. Neal EG, Chaffe H, Schwartz RH, et al. The ketogenic diet for the treatment of childhood epilepsy: a randomised
controlled trial. Lancet Neurol. 2008;7(6):500-6. 18. Kim DY, Rho JM. The ketogenic diet and epilepsy. Curr Opin Clin Nutr Metab Care. 2008;11(2):113-20. 19. Nordli DR, De Vivo DC. Chapter 14. Effects of the Ketogenic Diet on Cerebral Energy Metabolism. In: Stafstrom C, Rho
J, ed. Epilepsy and the Ketogenic Diet. 1st ed. Totowa, NJ: Humana Press, Inc.; 2004:179-80. 20. Melø TM, Nehlig A, Sonnewald U. Neuronal-glial interactions in rats fed a ketogenic diet. Neurochem Int. 2006;48(6-
7):498-507. 21. Huffman J, Kossoff EH. State of the ketogenic diet(s) in epilepsy. Curr Neurol Neurosci Rep. 2006;6(4):332-40. 22. Hartman AL, Gasior M, Vining EP, Rogawski MA. The neuropharmacology of the ketogenic diet. Pediatr Neurol.
2007;36(5):281-92. 23. Yellen G. Neuronal Metabolism and Excitability. Gary Yellen's Lab at Harvard Medical School Neurobiology. 2015.
Available at: http://yellen.hms.harvard.edu/images/Yellen001.jpg. Accessed March 14, 2015. 24. Kossoff EH, Zupec-Kania BA, Amark PE, et al. Optimal clinical management of children receiving the ketogenic diet:
recommendations of the International Ketogenic Diet Study Group. Epilepsia. 2009;50(2):304-17. 25. Kossoff EH, Mcgrogan JR, Freeman JM. Benefits of an all-liquid ketogenic diet. Epilepsia. 2004;45(9):1163. 26. Kwiterovich PO, Vining EP, Pyzik P, et al. Effect of a high-fat ketogenic diet on plasma levels of lipids, lipoproteins, and
apolipoproteins in children. JAMA. 2003;290(7):912-20.
REFERENCES

Espiritu | 18
27. Kim JT, Kang HC, Song JE, et al. Catch-up growth after long-term implementation and weaning from ketogenic diet in pediatric epileptic patients. Clin Nutr. 2013;32(1):98-103.
28. Lebel D, Morin C, Laberge M, Achim N, et al. The carbohydrate and caloric content of concomitant medications for children with epilepsy on the ketogenic diet. Can J Neurol Sci. 2001;28(4):322-40.
29. Misiewicz Runyon A, So TY. The use of ketogenic diet in pediatric patients with epilepsy. ISRN Pediatr. 2012;2012:263139.
30. Feldstein TJ. Carbohydrate and alcohol content of 200 oral liquid medications for use in patients receiving ketogenic diets. Pediatrics. 1996;97(4):506-11.
31. Kossoff EH, Pyzik PL, Mcgrogan JR, Rubenstein JE. The impact of early versus late anticonvulsant reduction after ketogenic diet initiation. Epilepsy Behav. 2004;5(4):499-502.
32. Löscher W, Schmidt D. Epilepsy: perampanel-new promise for refractory epilepsy? Nat Rev Neurol. 2012;8(12):661-2. 33. Sullivan JE, Dlugos DJ. Antiepileptic drug monotherapy: pediatric concerns. Semin Pediatr Neurol. 2005;12(2):88-96. 34. Ben-Menachem E, Sander JW, Privitera M, Gilliam F. Measuring outcomes of treatment with antiepileptic drugs in
clinical trials. Epilepsy Behav. 2010;18(1-2):24-30. 35. French JA, Kanner AM, Bautista J, et al. Efficacy and tolerability of the new antiepileptic drugs, II: Treatment of
refractory epilepsy: report of the TTA and QSS Subcommittees of the American Academy of Neurology and the American Epilepsy Society. Epilepsia. 2004;45(5):410-23.
36. Barnes SE, Bower BD. Sodium valproate in the treatment of intractable childhood epilepsy. Dev Med Child Neurol. 1975;17(2):175-81.
37. Chu-Shore CJ, Thiele EA. New drugs for pediatric epilepsy. Semin Pediatr Neurol. 2010;17(4):214-23. 38. Hwang H, Kim KJ. New antiepileptic drugs in pediatric epilepsy. Brain Dev. 2008;30(9):549-55. 39. Jarrar RG, Buchhalter JR. Therapeutics in pediatric epilepsy, Part 1: The new antiepileptic drugs and the ketogenic
diet. Mayo Clin Proc. 2003;78(3):359-70. 40. Keene DL, Metrakos K, Watters GV, Sherwin A. Sodium valproate in the treatment of the intractable childhood
epileptic. Can J Neurol Sci. 1982;9(3):307-11. 41. Khurana DS, Riviello J, Helmers S, et al. Efficacy of gabapentin therapy in children with refractory partial seizures. J
Pediatr. 1996;128(6):829-33. 42. Verrotti A, Loiacono G, Coppola G, et al. Pharmacotherapy for children and adolescents with epilepsy. Expert Opin
Pharmacother. 2011;12(2):175-94. 43. Sharma S, Sankhyan N, Gulati S, Agarwala A. Use of the modified Atkins diet for treatment of refractory childhood
epilepsy: a randomized controlled trial. Epilepsia. 2013;54(3):481-6. 44. Kossoff EH, Turner Z, Bluml RM, et al. A randomized, crossover comparison of daily carbohydrate limits using the
modified Atkins diet. Epilepsy Behav. 2007;10(3):432-6. 45. Kalra V, Seth R, Mishra D, Saha NC. Clobazam in refractory childhood epilepsy. Indian J Pediatr. 2010;77(3):263-6.
APPENDICES
Appendix A. Example of Typical 4:1 KD Meal using 1100 kcal/day10
Breakfast Lunch Dinner Snack
90 g ketogenic pudding 44 g cream cheese 13 g eggs 29 g heavy cream
40 g 36% heavy cream 8 g MCT oil Dark meat chicken salad
20 g dark meat chicken 8 g mayonnaise
20 g avocado
35 g 36% heavy cream Ground beef and cheese
11 g ground beef 10 g cheese 8 g butter
26 g cooked broccoli 11 g butter
Ketogenic chocolate 3 g cocoa 6 g butter 6 g coconut oil

Espiritu | 19
Appendix B. Carbohydrate content of antibiotics, AEDs, and over-the-counter medications28-30
Medication (Brand Name) Dosage Unit Grams of carbohydrate per dosage unit
Over-the-counter pain medications
Acetaminophen liquid suspension (Tylenol®) 160 mg/5 mL 5 grams/5 mL
Ibuprofen suspension (Motrin®) 100 mg/5 mL 0.63 grams/5 mL
Antibiotics
Amoxicillin oral suspension (Amoxil®) 400 mg/5 mL 1.88 grams/5 mL
Azithromycin oral suspension (Zithromax®) 100 mg/5 mL 3.86 grams/5 mL
Cephalexin oral suspension (Keflex®) 250 mg/5 mL 3.03 grams/5 mL
AEDs
Carbamazepine suspension (Tegretol®) 100 mg/5 mL 2.65 grams/5 mL
Gabapentin tablets (Neurontin®) 100 mg 0.03 grams
Lamotrigine tablets (Lamictal) 25 mg 0.03 grams
Levetiracetam oral solution (Keppra®) 100 mg/mL 0.3 grams/mL
Phenobarbital elixir 20 mg/5 mL 3.4 grams/5 mL
Phenytoin suspension (Dilantin®) 125 mg/5 mL 1.39 grams/5 mL
Topiramate tablets (Topamax®) 25 mg 0.04 grams
Valproic acid syrup (Depakene®) 250 mg/5 mL 4.5 grams/5 mL
Multivitamins
Poly-vi-sol® ---- 4.25 grams/5 mL
Appendix C. Recommended AEDs according to epilepsy syndrome8
Epilepsy Syndrome First-line AEDs Alternative AEDs Do not use (may worsen)
Childhood absence epilepsy Ethosuximide Lamotrigine Valproate
Levetiracetam Topiramate
Carbamezepine Oxcarbazepine Phenytoin Tiagabine Vigabatrin
Juvenile absence epilepsy Lamotrigine Valproate
Levetiracitam Topiramate
Juvenile myoclonic epilepsy Lamotrigine Valproate
Clobazam Clonazepam Levetiracitam Topiramate
Epilepsy with generalized tonic-clonic seizures
Carbamazepine Lamotrigine Topiramate Valproate
Levetiracetam Clobazam Oxcarbazepine Phenobarbital Phenytoin Primidone
Tiagabine Vigabatrin
Focal epilepsies: cryptogenic or symptomatic
Carbamazepine Lamotrigine Oxcarbazepine Valproate Topiramate
Clobazam Gabapentin Levetiracetam Phenytoin Tiagabine Clonazepam Phenobarbital Primidone

Espiritu | 20
Appendix D. Adverse reactions in AEDs for refractory epilepsy38,40,42,45
AED Adverse Reactions
Clobazam Sedation, hyperactivity, behavioral problems, irritability, fatigue, salivation, weight gain, sleep disturbances
Felbamate Anorexia, weight loss, insomnia, gait disturbance, aplastic anemia, hepatotoxicity
Gabapentin Emotional lability, aggression, hyperactivity, weight gain, somnolence, dizziness, dyspepsia, constipation, nausea, fatigue, ataxia
Lamotrigine Dizziness, sedation, headache, diplopia, ataxia, skin rash
Lacosamide Dizziness, headache, nausea, diplopia
Levetiracitam Somnolence, asthenia, headache, anorexia, noninvasive infections, hostility, emotional lability, nervousness, depersonalization, psychotic behavior
Oxcarbazepine Dizziness, diplopia, nausea, ataxia, hyponatremia
Pregabalin Dizziness, somnolence, ataxia, weight gain, euphoric effects
Rufinamide Dizziness, fatigue, headache, somnolence, nausea
Tiagabine Dizziness, asthenia, tremor, fatigue, nervousness
Topiramate Somnolence, fatigue, problems with concentration and word finding, difficulty with memory, decreased appetite and weight loss, nervousness, headache, asthenia
Valproic Acid Weight gain, vomiting, tremor, nausea, thrombocytopenia, impaired coagulation, drowsiness alopecia, encephalopathy, hyperammonemia
Vigabatrin Peripheral visual-field defect, hyperactivity, irritability, aggression, self-injurious behavior, self-defiance, weight gain, facial edema, headache, drowsiness, insomnia, ataxia, somnolence, stupor
Zonisamide Sleepiness, loss of appetite, weight loss, ataxia, oligohydrosis, hyperthermia
Appendix C (continued). Recommended AEDs according to epilepsy syndrome8
Infantile spasms Vigabatrin
Clobazam Clonazepam Valproate Topiramate
Carbamezapine Oxcarbazepine
Benign epilepsy with centrotemoral spikes or occipital paroxysms
Carbamazepine Lamotrigine Oxcarbazepine Valproate
Levetiracetam Topiramate
Dravet syndrome
Clobazam Clonazepam Valproate Topiramate
Levetiracetam Phenobarbital
Carbamazpeine Lamotrigine Oxcarbazepine Vigabatrin
Continuous spike wave of slow sleep
Clobazam Clonazepam Ethosuximide Lamotrigine Valproate
Levetiracetam Topiramate
Carbamazepine Oxcarbazepine Vigabatrin
Lennox-Gastaut syndrome Lamotrigine Valproate Topiramate
Clobazam Clonazepam Ethosuximide Levetiracetam Felbamate
Carbamazepine Oxcarbazepine
Landau-Kleffner syndrome Lamotrigine Valproate
Levetiracetam Topiramate
Carbamazepine Oxcarbazepine
Myoclonic astatic epilepsy
Clobazam Clonazepam Valproate Topiramate
Lamotrigine Levetiracetam
Carbamazepine Oxcarbazepine