Embed Size (px)
Citation preview
Annaliesa S Anderson PhD FAAM
Pfizer Vaccine Research and Development
Disclosure: ASA is employed by Pfizer and previous employee of Merck. ASA owns stock in both companies
Staphylococcus aureus Vaccines
Outline
Medical need
Vaccine Development
Technical and Clinical Assessment
Challenges Associated with Vaccine Development
2
3
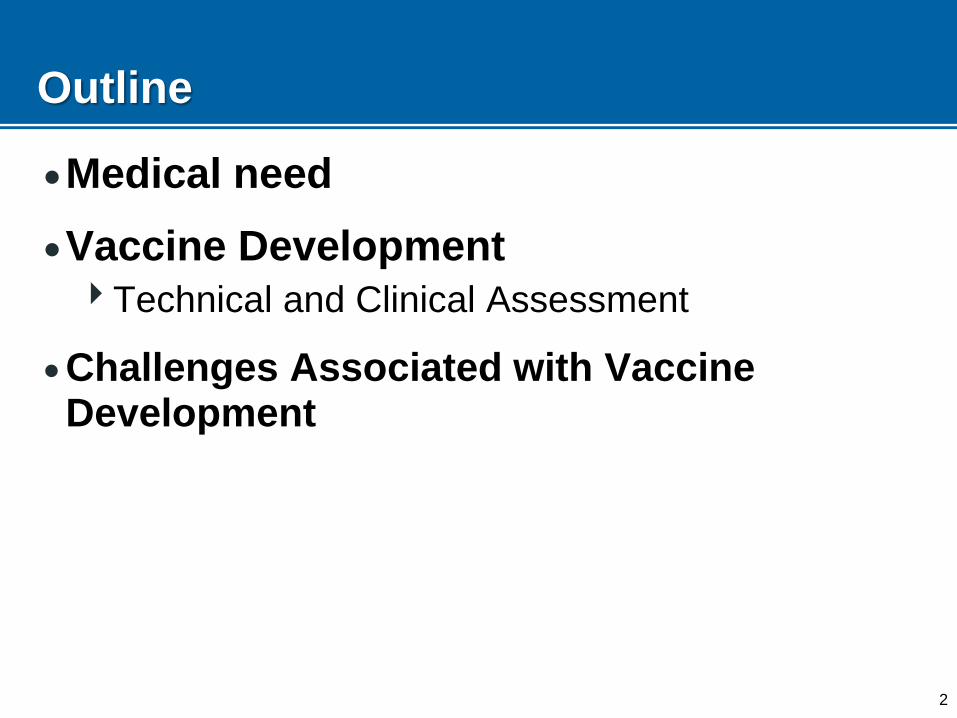
Medical Need for a S. aureus Vaccine
S. aureus is a leading cause of morbidity and mortality in both healthcare-associated and community settings1
1Allegranzi et al. Lancet 2011: 377: 228-41
|4
Medical Need for a S. aureus Vaccine
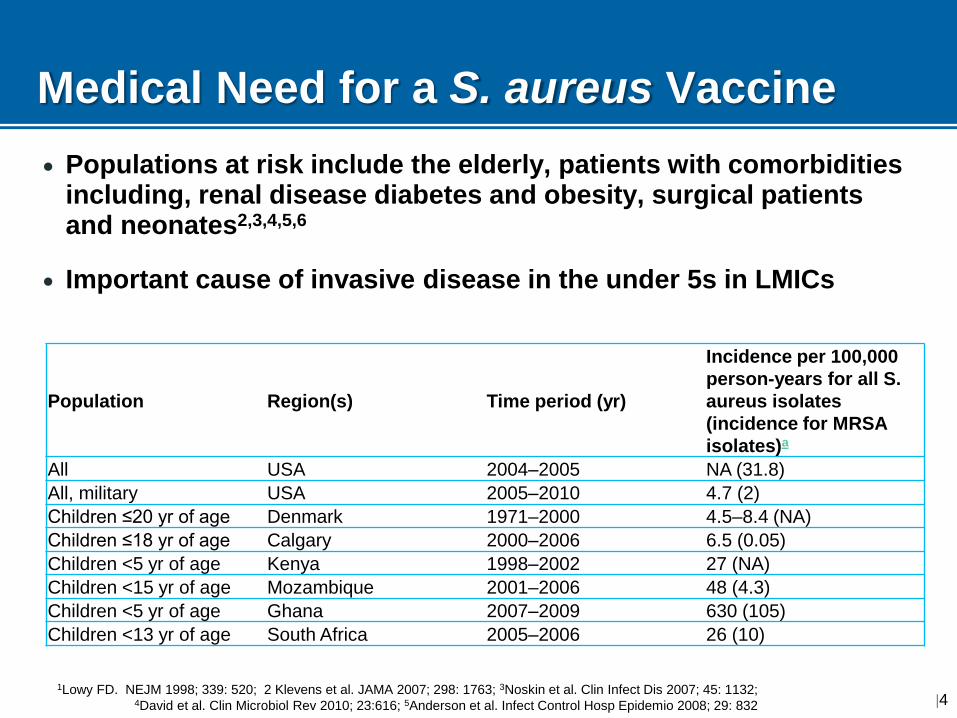
Populations at risk include the elderly, patients with comorbidities including, renal disease diabetes and obesity, surgical patients and neonates2,3,4,5,6
Important cause of invasive disease in the under 5s in LMICs
1Lowy FD. NEJM 1998; 339: 520; 2 Klevens et al. JAMA 2007; 298: 1763; 3Noskin et al. Clin Infect Dis 2007; 45: 1132; 4David et al. Clin Microbiol Rev 2010; 23:616; 5Anderson et al. Infect Control Hosp Epidemio 2008; 29: 832
Population Region(s) Time period (yr)
Incidence per 100,000
person-years for all S.
aureus isolates
(incidence for MRSA
isolates)a
All USA 2004–2005 NA (31.8)
All, military USA 2005–2010 4.7 (2)
Children ≤20 yr of age Denmark 1971–2000 4.5–8.4 (NA)
Children ≤18 yr of age Calgary 2000–2006 6.5 (0.05)
Children <5 yr of age Kenya 1998–2002 27 (NA)
Children <15 yr of age Mozambique 2001–2006 48 (4.3)
Children <5 yr of age Ghana 2007–2009 630 (105)
Children <13 yr of age South Africa 2005–2006 26 (10)
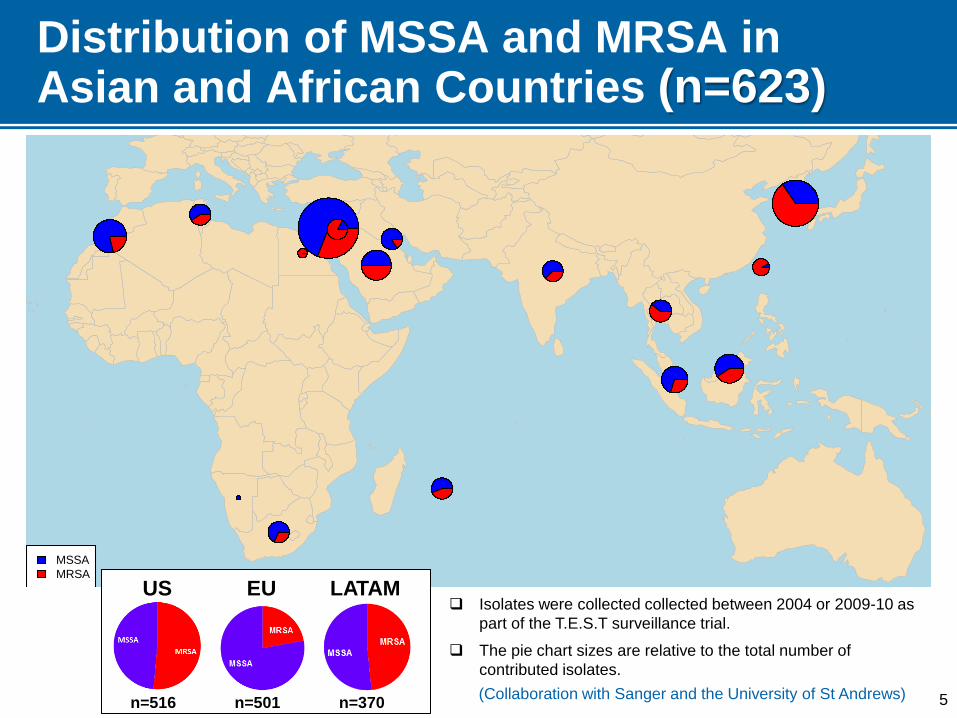
Distribution of MSSA and MRSA in Asian and African Countries (n=623)
MSSA
MRSA
Isolates were collected collected between 2004 or 2009-10 as
part of the T.E.S.T surveillance trial.
The pie chart sizes are relative to the total number of
contributed isolates.
(Collaboration with Sanger and the University of St Andrews)
US EU LATAM
n=516 n=501 n=370 5
6
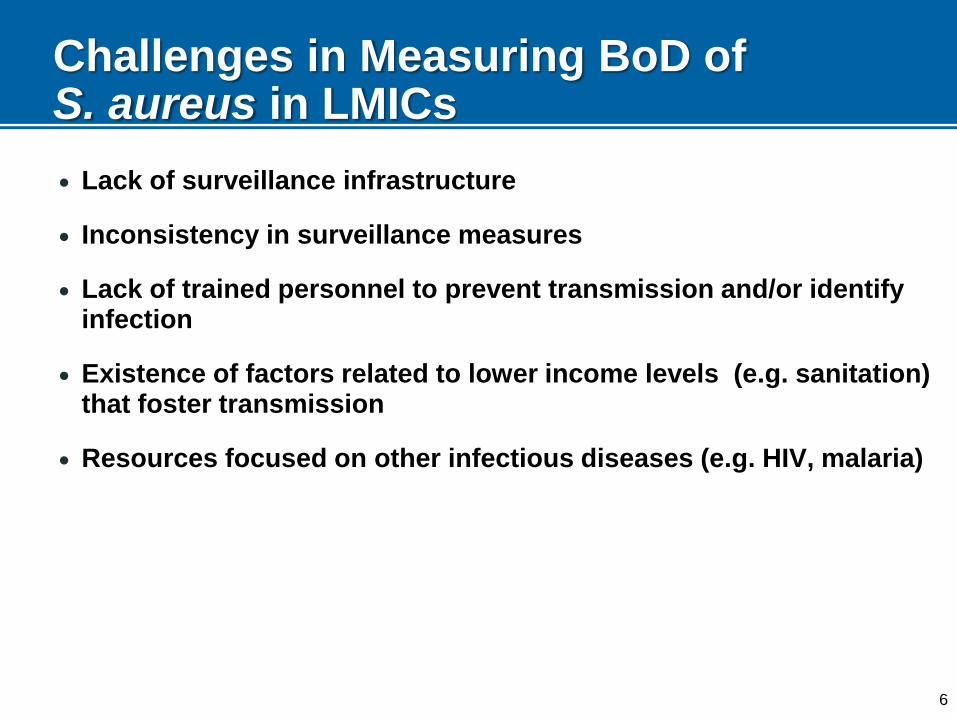
Challenges in Measuring BoD of S. aureus in LMICs
Lack of surveillance infrastructure
Inconsistency in surveillance measures
Lack of trained personnel to prevent transmission and/or identify infection
Existence of factors related to lower income levels (e.g. sanitation) that foster transmission
Resources focused on other infectious diseases (e.g. HIV, malaria)
S. aureus Vaccines Update
8
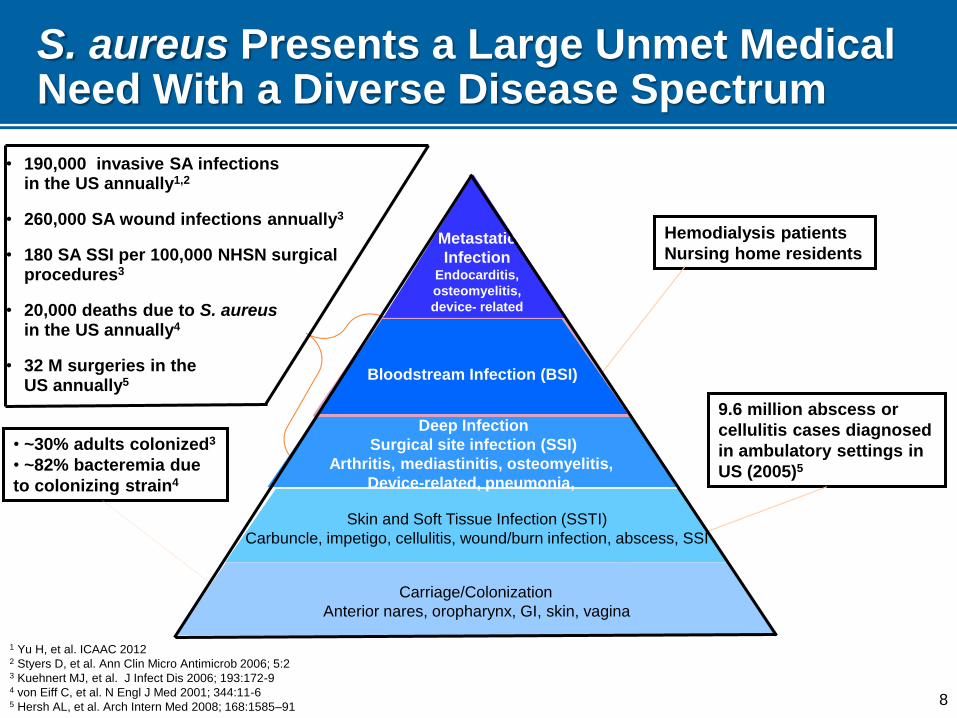
S. aureus Presents a Large Unmet Medical Need With a Diverse Disease Spectrum
• ~30% adults colonized3
• ~82% bacteremia due
to colonizing strain4
9.6 million abscess or
cellulitis cases diagnosed
in ambulatory settings in
US (2005)5
Hemodialysis patients
Nursing home residents
Skin and Soft Tissue Infection (SSTI)
Carbuncle, impetigo, cellulitis, wound/burn infection, abscess, SSI
Deep Infection
Surgical site infection (SSI)
Arthritis, mediastinitis, osteomyelitis,
Device-related, pneumonia,
Bloodstream Infection (BSI)
Carriage/Colonization
Anterior nares, oropharynx, GI, skin, vagina
Metastatic
Infection Endocarditis,
osteomyelitis,
device- related
1 Yu H, et al. ICAAC 2012 2 Styers D, et al. Ann Clin Micro Antimicrob 2006; 5:2 3 Kuehnert MJ, et al. J Infect Dis 2006; 193:172-9 4 von Eiff C, et al. N Engl J Med 2001; 344:11-6 5 Hersh AL, et al. Arch Intern Med 2008; 168:1585–91
• 190,000 invasive SA infections in the US annually1,2
• 260,000 SA wound infections annually3
• 180 SA SSI per 100,000 NHSN surgical procedures3
• 20,000 deaths due to S. aureus in the US annually4
• 32 M surgeries in the US annually5
9
S. aureus is a Challenging Vaccine Target
Highly successful commensal organism (25-33% of humans colonized)1,2
Diverse array of virulence factors facilitate colonization and evasion of host immune response3,4
Toxins
Adhesion factors
Nutrient scavenging
Capsular polysaccharides to evade phagocytosis
Antibody and complement interference factors
Most humans fail to generate functional antibodies against S. aureus following natural infection4
No existing correlate for protection
Extensive strain diversity3
1Kluytmans et al. Clin Microbiol Rev 1997; 10: 505; 2Lowy FD. NEJM 1998; 339: 520; 3Liu, GY.
Pediatric Research 2009; 65: 71R; 4Scully et al. Fronteirs in Immunology 2014; 5: 1
10
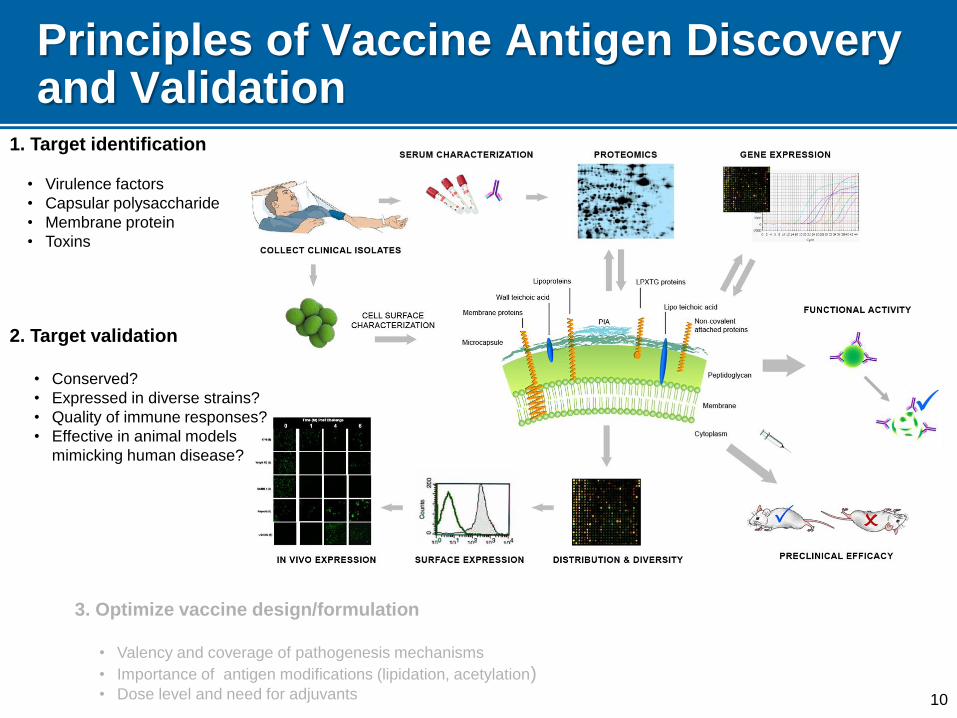
Principles of Vaccine Antigen Discovery and Validation
3. Optimize vaccine design/formulation
• Valency and coverage of pathogenesis mechanisms
• Importance of antigen modifications (lipidation, acetylation) • Dose level and need for adjuvants
2. Target validation
• Conserved?
• Expressed in diverse strains?
• Quality of immune responses?
• Effective in animal models
mimicking human disease?
1. Target identification
• Virulence factors
• Capsular polysaccharide
• Membrane protein
• Toxins
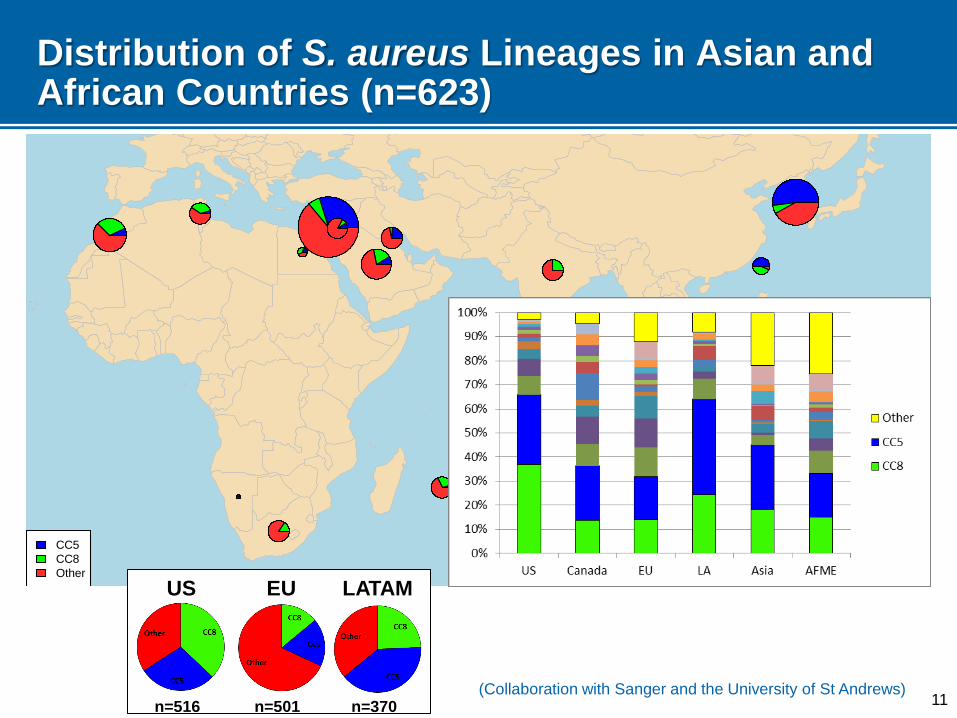
Distribution of S. aureus Lineages in Asian and African Countries (n=623)
CC5
CC8
Other
US EU LATAM
n=516 n=501 n=370 (Collaboration with Sanger and the University of St Andrews)
11
12
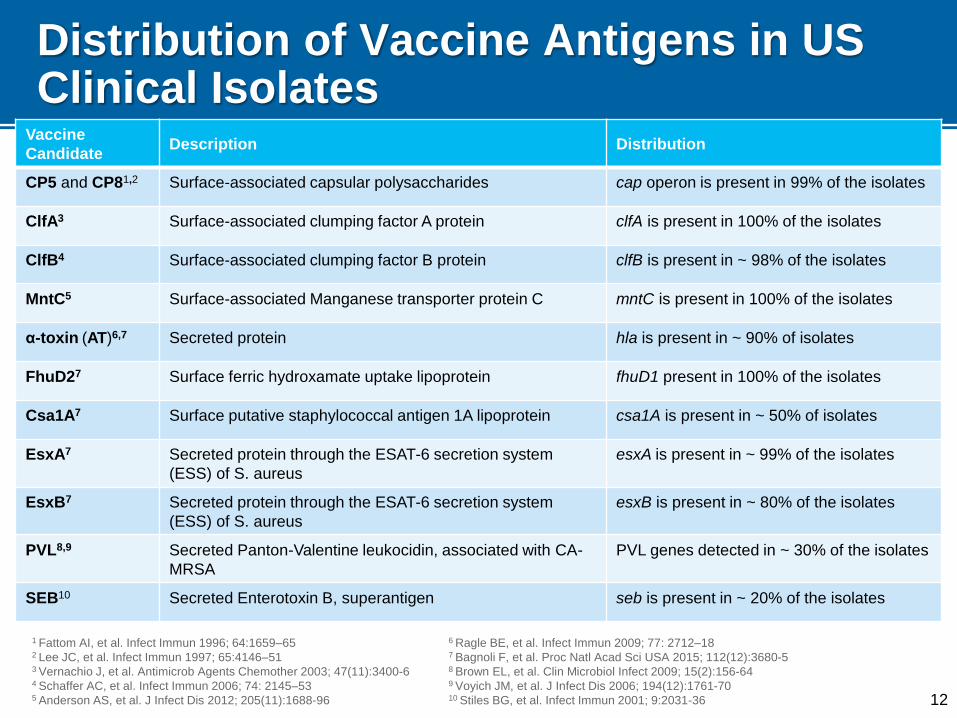
Distribution of Vaccine Antigens in US Clinical Isolates
Vaccine
Candidate Description Distribution
CP5 and CP81,2 Surface-associated capsular polysaccharides cap operon is present in 99% of the isolates
ClfA3 Surface-associated clumping factor A protein clfA is present in 100% of the isolates
ClfB4 Surface-associated clumping factor B protein clfB is present in ~ 98% of the isolates
MntC5 Surface-associated Manganese transporter protein C mntC is present in 100% of the isolates
α-toxin (AT)6,7 Secreted protein hla is present in ~ 90% of isolates
FhuD27 Surface ferric hydroxamate uptake lipoprotein fhuD1 present in 100% of the isolates
Csa1A7 Surface putative staphylococcal antigen 1A lipoprotein csa1A is present in ~ 50% of isolates
EsxA7 Secreted protein through the ESAT-6 secretion system
(ESS) of S. aureus
esxA is present in ~ 99% of the isolates
EsxB7 Secreted protein through the ESAT-6 secretion system
(ESS) of S. aureus
esxB is present in ~ 80% of the isolates
PVL8,9 Secreted Panton-Valentine leukocidin, associated with CA-
MRSA
PVL genes detected in ~ 30% of the isolates
SEB10 Secreted Enterotoxin B, superantigen seb is present in ~ 20% of the isolates
1 Fattom AI, et al. Infect Immun 1996; 64:1659–65 2 Lee JC, et al. Infect Immun 1997; 65:4146–51 3 Vernachio J, et al. Antimicrob Agents Chemother 2003; 47(11):3400-6
4 Schaffer AC, et al. Infect Immun 2006; 74: 2145–53 5 Anderson AS, et al. J Infect Dis 2012; 205(11):1688-96
6 Ragle BE, et al. Infect Immun 2009; 77: 2712–18 7 Bagnoli F, et al. Proc Natl Acad Sci USA 2015; 112(12):3680-5 8 Brown EL, et al. Clin Microbiol Infect 2009; 15(2):156-64 9 Voyich JM, et al. J Infect Dis 2006; 194(12):1761-70 10 Stiles BG, et al. Infect Immun 2001; 9:2031-36
13
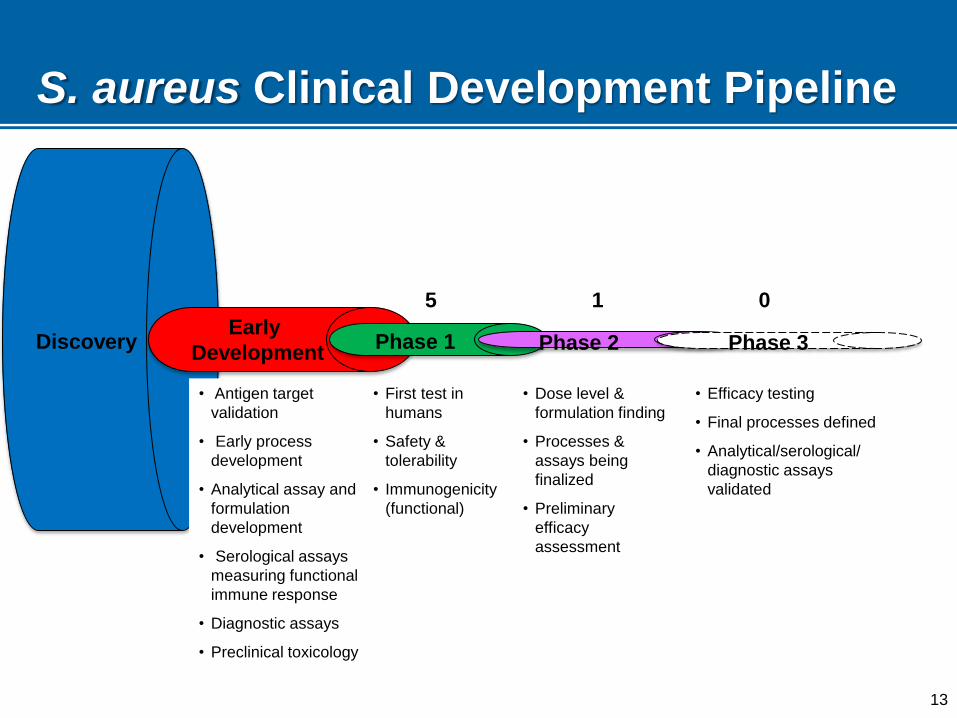
S. aureus Clinical Development Pipeline
• First test in
humans
• Safety &
tolerability
• Immunogenicity
(functional)
• Dose level &
formulation finding
• Processes &
assays being
finalized
• Preliminary
efficacy
assessment
• Efficacy testing
• Final processes defined
• Analytical/serological/
diagnostic assays
validated
Discovery Early
Development Phase 1 Phase 2
• Antigen target
validation
• Early process
development
• Analytical assay and
formulation
development
• Serological assays
measuring functional
immune response
• Diagnostic assays
• Preclinical toxicology
Phase 3
5 1 0
14
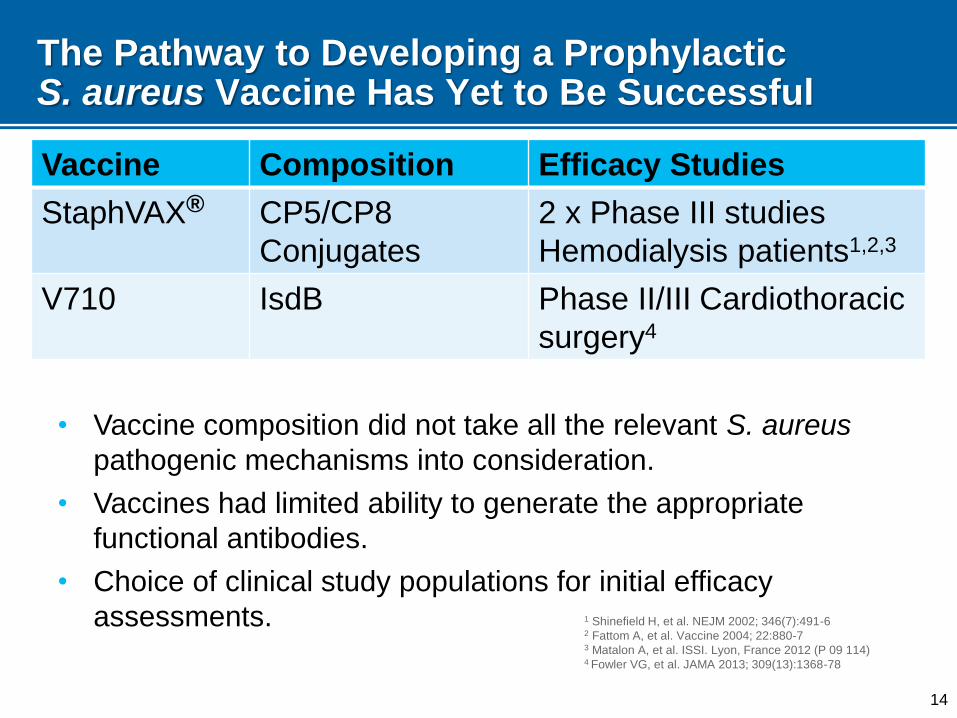
The Pathway to Developing a Prophylactic S. aureus Vaccine Has Yet to Be Successful
Vaccine Composition Efficacy Studies
StaphVAX® CP5/CP8
Conjugates
2 x Phase III studies
Hemodialysis patients1,2,3
V710 IsdB Phase II/III Cardiothoracic
surgery4
• Vaccine composition did not take all the relevant S. aureus
pathogenic mechanisms into consideration.
• Vaccines had limited ability to generate the appropriate
functional antibodies.
• Choice of clinical study populations for initial efficacy
assessments. 1 Shinefield H, et al. NEJM 2002; 346(7):491-6 2 Fattom A, et al. Vaccine 2004; 22:880-7 3 Matalon A, et al. ISSI. Lyon, France 2012 (P 09 114) 4 Fowler VG, et al. JAMA 2013; 309(13):1368-78
15
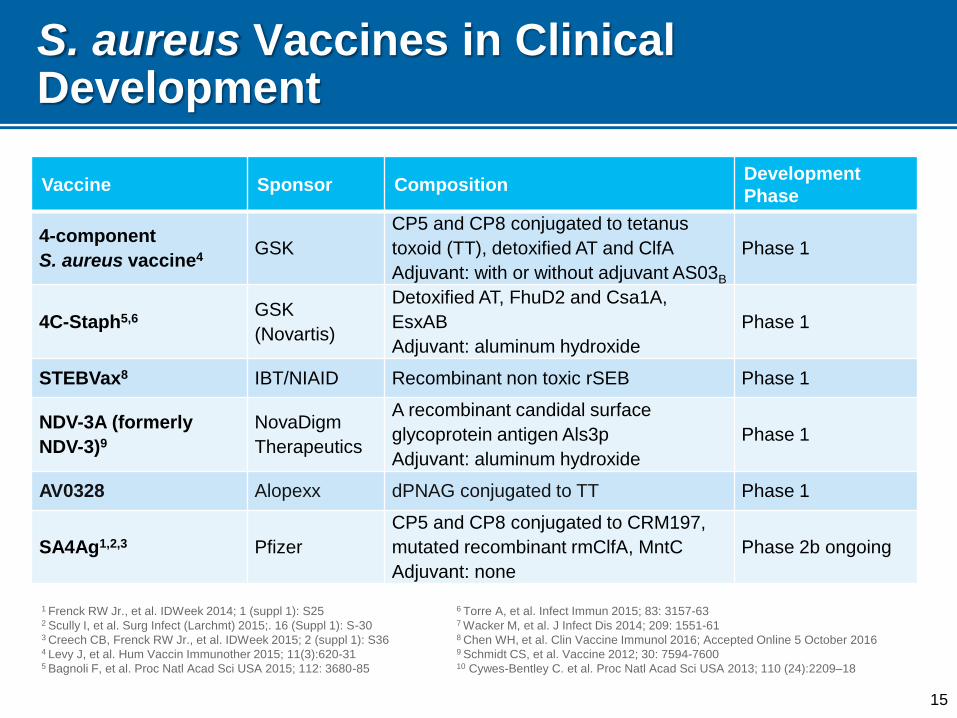
S. aureus Vaccines in Clinical Development
Vaccine Sponsor Composition Development
Phase
4-component
S. aureus vaccine4 GSK
CP5 and CP8 conjugated to tetanus
toxoid (TT), detoxified AT and ClfA
Adjuvant: with or without adjuvant AS03B
Phase 1
4C-Staph5,6 GSK
(Novartis)
Detoxified AT, FhuD2 and Csa1A,
EsxAB
Adjuvant: aluminum hydroxide
Phase 1
STEBVax8 IBT/NIAID Recombinant non toxic rSEB Phase 1
NDV-3A (formerly
NDV-3)9
NovaDigm
Therapeutics
A recombinant candidal surface
glycoprotein antigen Als3p
Adjuvant: aluminum hydroxide
Phase 1
AV0328 Alopexx dPNAG conjugated to TT Phase 1
SA4Ag1,2,3 Pfizer
CP5 and CP8 conjugated to CRM197,
mutated recombinant rmClfA, MntC
Adjuvant: none
Phase 2b ongoing
1 Frenck RW Jr., et al. IDWeek 2014; 1 (suppl 1): S25 2 Scully I, et al. Surg Infect (Larchmt) 2015;. 16 (Suppl 1): S-30 3 Creech CB, Frenck RW Jr., et al. IDWeek 2015; 2 (suppl 1): S36 4 Levy J, et al. Hum Vaccin Immunother 2015; 11(3):620-31 5 Bagnoli F, et al. Proc Natl Acad Sci USA 2015; 112: 3680-85
6 Torre A, et al. Infect Immun 2015; 83: 3157-63 7 Wacker M, et al. J Infect Dis 2014; 209: 1551-61 8 Chen WH, et al. Clin Vaccine Immunol 2016; Accepted Online 5 October 2016 9 Schmidt CS, et al. Vaccine 2012; 30: 7594-7600 10 Cywes-Bentley C. et al. Proc Natl Acad Sci USA 2013; 110 (24):2209–18
16
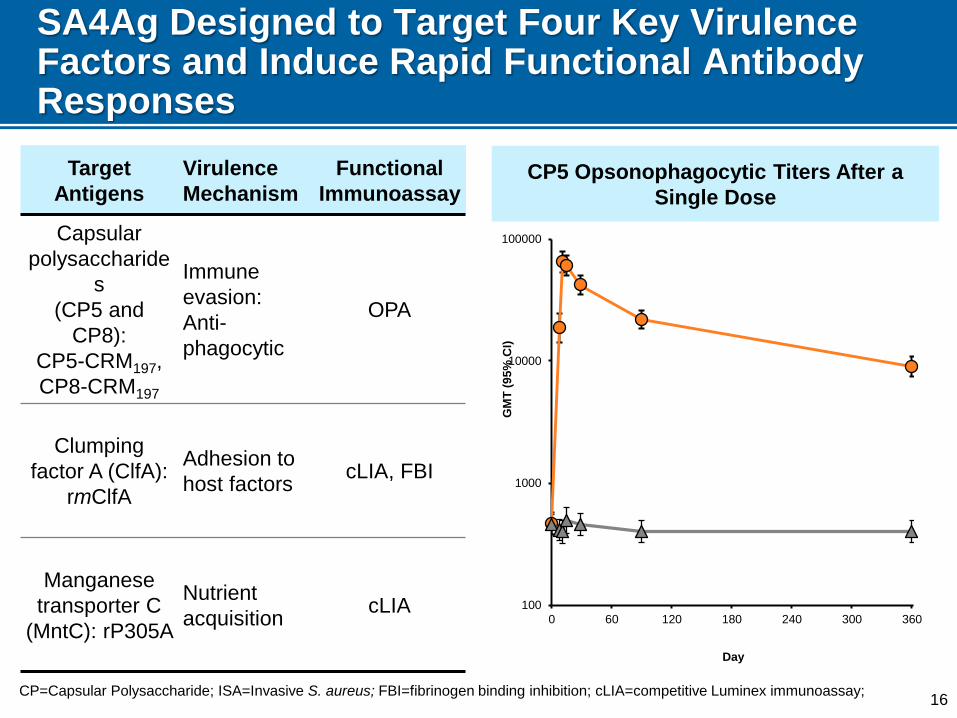
CP5 Opsonophagocytic Titers After a
Single Dose
SA4Ag Designed to Target Four Key Virulence Factors and Induce Rapid Functional Antibody Responses
Target
Antigens
Virulence
Mechanism
Functional
Immunoassay
Capsular
polysaccharide
s
(CP5 and
CP8):
CP5-CRM197,
CP8-CRM197
Immune
evasion:
Anti-
phagocytic
OPA
Clumping
factor A (ClfA):
rmClfA
Adhesion to
host factors cLIA, FBI
Manganese
transporter C
(MntC): rP305A
Nutrient
acquisition cLIA
CP=Capsular Polysaccharide; ISA=Invasive S. aureus; FBI=fibrinogen binding inhibition; cLIA=competitive Luminex immunoassay;
100
1000
10000
100000
0 60 120 180 240 300 360
GM
T (
95
% C
I)
Day
17
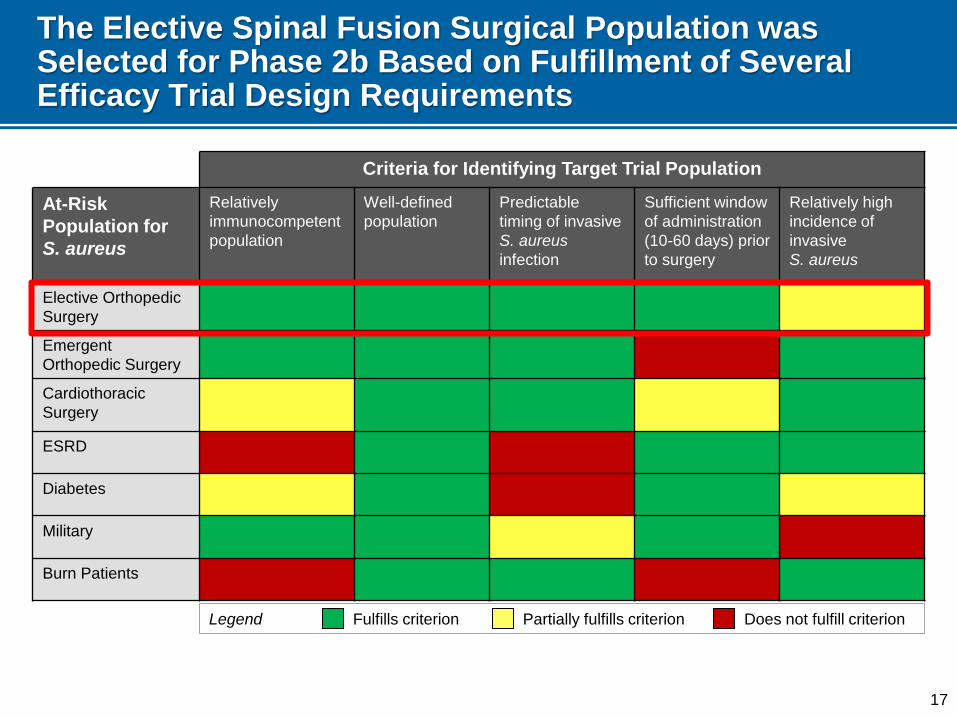
The Elective Spinal Fusion Surgical Population was Selected for Phase 2b Based on Fulfillment of Several Efficacy Trial Design Requirements
ILLUSTRATIVE
Legend Fulfills criterion Does not fulfill criterion Partially fulfills criterion
Criteria for Identifying Target Trial Population
At-Risk
Population for
S. aureus
Relatively
immunocompetent
population
Well-defined
population
Predictable
timing of invasive
S. aureus
infection
Sufficient window
of administration
(10-60 days) prior
to surgery
Relatively high
incidence of
invasive
S. aureus
Elective Orthopedic
Surgery
Emergent
Orthopedic Surgery
Cardiothoracic
Surgery
ESRD
Diabetes
Military
Burn Patients
18
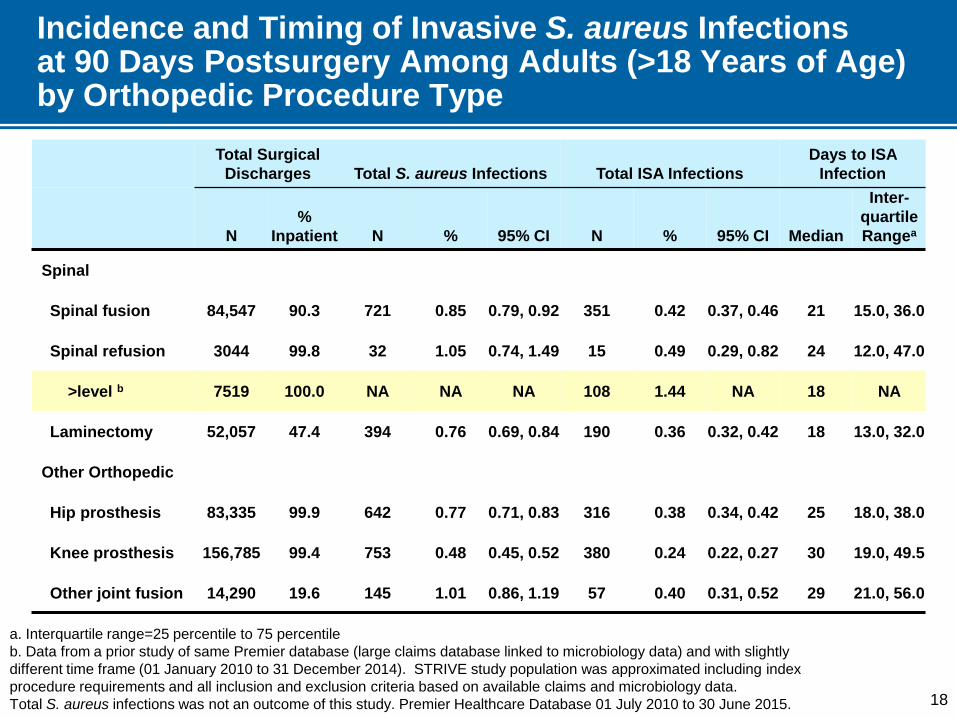
Incidence and Timing of Invasive S. aureus Infections at 90 Days Postsurgery Among Adults (>18 Years of Age) by Orthopedic Procedure Type
Total Surgical
Discharges Total S. aureus Infections Total ISA Infections
Days to ISA
Infection
N
%
Inpatient N % 95% CI N % 95% CI Median
Inter-
quartile
Rangea
Spinal
Spinal fusion 84,547 90.3 721 0.85 0.79, 0.92 351 0.42 0.37, 0.46 21 15.0, 36.0
Spinal refusion 3044 99.8 32 1.05 0.74, 1.49 15 0.49 0.29, 0.82 24 12.0, 47.0
>level b 7519 100.0 NA NA NA 108 1.44 NA 18 NA
Laminectomy 52,057 47.4 394 0.76 0.69, 0.84 190 0.36 0.32, 0.42 18 13.0, 32.0
Other Orthopedic
Hip prosthesis 83,335 99.9 642 0.77 0.71, 0.83 316 0.38 0.34, 0.42 25 18.0, 38.0
Knee prosthesis 156,785 99.4 753 0.48 0.45, 0.52 380 0.24 0.22, 0.27 30 19.0, 49.5
Other joint fusion 14,290 19.6 145 1.01 0.86, 1.19 57 0.40 0.31, 0.52 29 21.0, 56.0
a. Interquartile range=25 percentile to 75 percentile
b. Data from a prior study of same Premier database (large claims database linked to microbiology data) and with slightly
different time frame (01 January 2010 to 31 December 2014). STRIVE study population was approximated including index
procedure requirements and all inclusion and exclusion criteria based on available claims and microbiology data.
Total S. aureus infections was not an outcome of this study. Premier Healthcare Database 01 July 2010 to 30 June 2015.
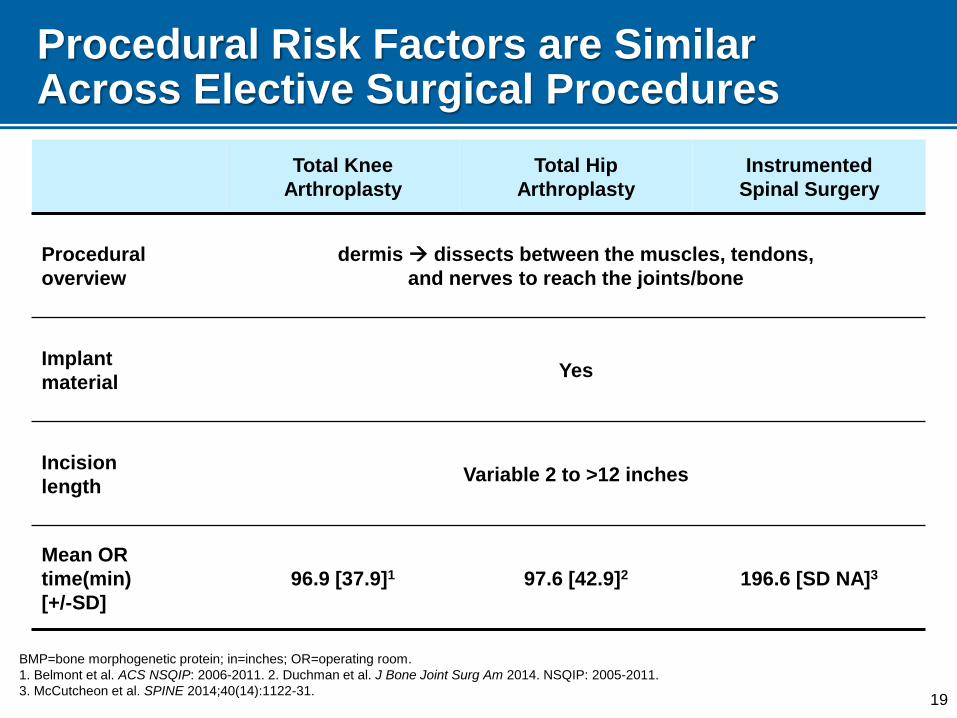
Procedural Risk Factors are Similar Across Elective Surgical Procedures
Total Knee
Arthroplasty
Total Hip
Arthroplasty
Instrumented
Spinal Surgery
Procedural
overview
dermis dissects between the muscles, tendons,
and nerves to reach the joints/bone
Implant
material Yes
Incision
length Variable 2 to >12 inches
Mean OR
time(min)
[+/-SD]
96.9 [37.9]1 97.6 [42.9]2 196.6 [SD NA]3
19
BMP=bone morphogenetic protein; in=inches; OR=operating room.
1. Belmont et al. ACS NSQIP: 2006-2011. 2. Duchman et al. J Bone Joint Surg Am 2014. NSQIP: 2005-2011.
3. McCutcheon et al. SPINE 2014;40(14):1122-31.
20
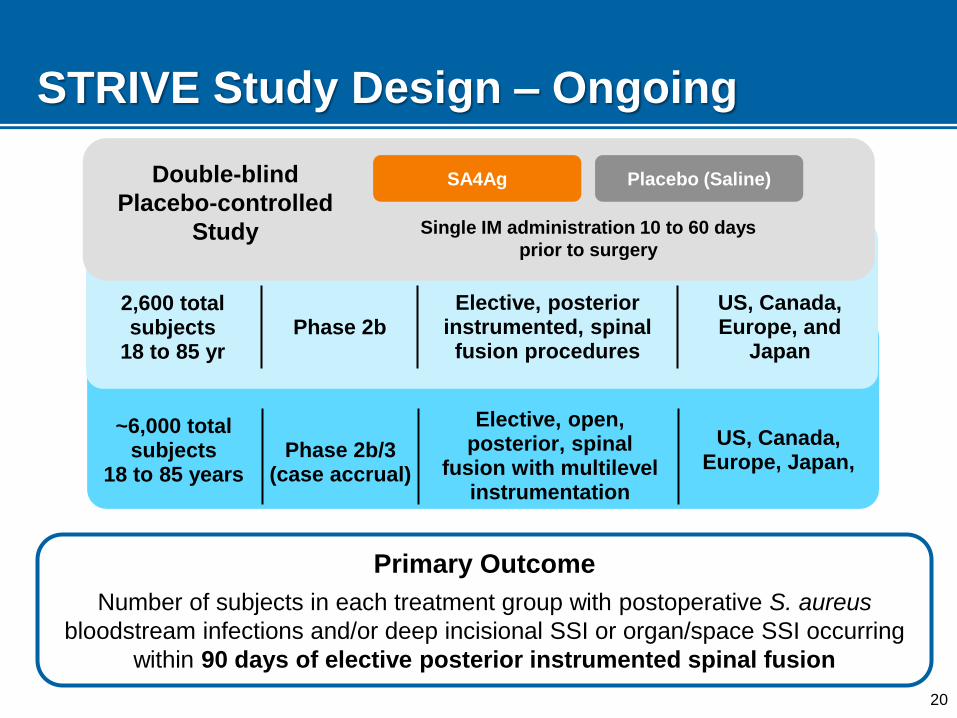
~6,000 total subjects
18 to 85 years Phase 2b/3
(case accrual)
Elective, open, posterior, spinal
fusion with multilevel instrumentation
US, Canada, Europe, Japan,
STRIVE Study Design – Ongoing
Primary Outcome
Number of subjects in each treatment group with postoperative S. aureus
bloodstream infections and/or deep incisional SSI or organ/space SSI occurring
within 90 days of elective posterior instrumented spinal fusion
2,600 total subjects
18 to 85 yr Phase 2b
Elective, posterior instrumented, spinal fusion procedures
US, Canada, Europe, and
Japan
SA4Ag Placebo (Saline)
Single IM administration 10 to 60 days
prior to surgery
Double-blind
Placebo-controlled
Study
Challenges for Developing a
S. aureus Vaccine
22
Preclinical Challenges
Target of bacterial virulence factors that are essential to the pathogenesis of the organism
What are relevant antigens: single vs multiple
Relevant animal models that may predict response/efficacy in humans
23
Immunological Challenges
Incomplete understanding of host immunity needed to confer protection
Lack of known correlate/s of protection
Assessment of immune response in humans: functional and/or killing antibodies
24
Development Challenges
Dynamic and dramatic changes in epidemiology of SA infection
Surveillance systems targeting MRSA only
Prior vaccine failures in phase 3 clinical programs add additional obstacles
Clinical endpoints requirements
Identification of the right population for efficient assessment of VE
Relatively high S. aureus infection rate
Immunocompetence
Ability to vaccinate prior to period of risk
S. aureus disease presents during a predictable time
25
Summary
Medical need
S. aureus causes a broad range of diseases in different populations
Comprehensive disease data is limited in all regions
Vaccine Development
Technical feasibility
‒ Preclinical data has not been predictive of efficacy
‒ Correlates are not available
‒ Multi antigen formulation that neutralize key virulence mechanisms is likely important
Clinical development feasibility
‒ Despite the recognized medical need, clinical populations are not straightforward
Thank you to
Naglaa Mohamed
Lisa Weiss
Alvaro Quintana
Alejandra Gurtman
David Swerdlow
26