Embed Size (px)
Citation preview
Standardized Testing11.14.13Barthel ADL IndexBerg Balance ScaleDynamic Gait IndexFunctional ReachTimed Up and Go Test (TUG)Tinetti AssessmentSpeech Assessments
Barthel ADL Index
Guidelines
• 1. The index should be used as a record of what a patient does, not as a record of what a patient could do.
• 2. The main aim is to establish degree of independence from any help, physical or verbal, however minor and for whatever reason.
• 3. The need for supervision renders the patient not independent.
• 4. A patient's performance should be established using the best available evidence. Asking the patient, friends/relatives and nurses are the usual sources, but direct observation and common sense are also important. However direct testing is not needed.
• 5. Usually the patient's performance over the preceding 24-48 hours is important, but occasionally longer periods will be relevant.
• 6. Middle categories imply that the patient supplies over 50 per cent of the effort.
• 7. Use of aids to be independent is allowed.

Scoring
• Higher scores reflect greater independence.
• In the original version, a patient who scores 100 is continent; independent in feeding, dressing, getting in and out of bed, and bathing; can walk at least one block; and can ascend and descend stairs without help.
• A score of 0–20 suggests total dependence, 21–60 severe dependence, 61–90 moderate dependence and 91–99 slight dependence. In the 15-item version, a score of 60 is commonly considered to be the threshold score for marked dependence.
References:• Shah S, Vanclay F, Cooper B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J Clin Epidemiol
1989;42:703–9.
• 10. Granger CV, Sherwood CC, Greer DS. Functional status measures in a comprehensive stroke care program. Arch Phys Med Rehabil 1977;58:555–61.
FEEDING
• 0 = unable
• 5 = needs help cutting, spreading butter, etc., or requires modified diet
• 10 = independent
Feeding
• • Able to eat any normal food (not only soft food). Food cooked and served by others, but not cut up.
• • 'Help' = food cut up, patient feeds self.
BATHING
• 0 = dependent
• 5 = independent (or in shower)
Bathing
• • Usually the most difficult activity.
• • Must get in and out unsupervised, and wash self.
• • Independent in shower = 'independent' if unsupervised/unaided.

GROOMING
• 0 = needs to help with personal care
• 5 = independent face/hair/teeth/shaving (implements provided)
Grooming (preceding 24 – 48 hours)
• • Refers to personal hygiene: doing teeth, fitting false teeth, doing hair, shaving, washing face. Implements can be provided by helper.

DRESSING
• 0 = dependent
• 5 = needs help but can do about half unaided
• 10 = independent (including buttons, zips, laces, etc.)
Dressing
• • Should be able to select and put on all clothes, which may be adapted.
• • 'Half' = help with buttons, zips, etc. (check!), but can put on some garments alone.

BOWELS
• 0 = incontinent (or needs to be given enemas)
• 5 = occasional accident
• 10 = continent
Bowels (preceding week)
• • If needs enema from nurse, then 'incontinent.'
• • 'Occasional' = once a week.
BLADDER
• 0 = incontinent, or catheterized and unable to manage alone
• 5 = occasional accident
• 10 = continent
Bladder (preceding week)
• • 'Occasional' = less than once a day.
• • A catheterized patient who can completely manage the catheter alone is registered as 'continent.'

TOILET USE
• 0 = dependent
• 5 = needs some help, but can do something alone
• 10 = independent (on and off, dressing, wiping)
Toilet use
• • Should be able to reach toilet/commode, undress sufficiently, clean self, dress, and leave.
• • 'With help' = can wipe self and do some other of above.
TRANSFERS (BED TO CHAIR AND BACK)
• 0 = unable, no sitting balance
• 5 = major help (one or two people, physical), can sit
• 10 = minor help (verbal or physical)
• 15 = independent
Transfer
• • From bed to chair and back.
• • 'Dependent' = NO sitting balance (unable to sit); two people to lift.
• • 'Major help' = one strong/skilled, or two normal people. Can sit up.
• • 'Minor help' = one person easily, OR needs any supervision for safety.
MOBILITY (ON LEVEL SURFACES)
• 0 = immobile or < 50 yards
• 5 = wheelchair independent, including corners, > 50 yards
• 10 = walks with help of one person (verbal or physical) > 50 yards
• 15 = independent (but may use any aid; for example, stick) > 50 yards
Mobility
• • Refers to mobility about house or ward, indoors. May use aid. If in wheelchair, must negotiate corners/doors
• unaided.
• • 'Help' = by one untrained person, including supervision/moral support.
• 50 yards=150 feet

STAIRS
• 0 = unable
• 5 = needs help (verbal, physical, carrying aid)
• 10 = independent
Stairs
• • Must carry any walking aid used to be independent.

Additional Considerations
Bowels (preceding week)• • If needs enema from nurse, then 'incontinent.'• • 'Occasional' = once a week.Bladder (preceding week)• • 'Occasional' = less than once a day.• • A catheterized patient who can completely manage the catheter alone is
registered as 'continent.'Grooming (preceding 24 – 48 hours)• • Refers to personal hygiene: doing teeth, fitting false teeth, doing hair, shaving,
washing face. Implements can be provided by helper.Toilet use• • Should be able to reach toilet/commode, undress sufficiently, clean self, dress,
and leave.• • 'With help' = can wipe self and do some other of above.Feeding• • Able to eat any normal food (not only soft food). Food cooked and served by
others, but not cut up.• • 'Help' = food cut up, patient feeds self.

Additional Considerations part 2
Transfer• • From bed to chair and back.• • 'Dependent' = NO sitting balance (unable to sit); two people to lift.• • 'Major help' = one strong/skilled, or two normal people. Can sit up.• • 'Minor help' = one person easily, OR needs any supervision for safety.Mobility• • Refers to mobility about house or ward, indoors. May use aid. If in wheelchair, must
negotiate corners/doors• unaided.• • 'Help' = by one untrained person, including supervision/moral support.Dressing• • Should be able to select and put on all clothes, which may be adapted.• • 'Half' = help with buttons, zips, etc. (check!), but can put on some garments alone.Stairs• • Must carry any walking aid used to be independent.Bathing• • Usually the most difficult activity.• • Must get in and out unsupervised, and wash self.• • Independent in shower = 'independent' if unsupervised/unaided.

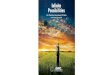
Barthel ADL Index Complete

Berg Balance Scale
• Description: 14-item scale designed to measure balance of the older adult in a clinical setting.
• Equipment needed: Ruler, 2 standard chairs (one with arm rests, one without)
• Footstool or step, Stopwatch or wristwatch, 15 ft walkway
• Completion Time: 15-20 minutes
• Scoring: A five-point ordinal scale, ranging from 0-4. “0” indicates the lowest level of function and “4” the highest level of function. Total Score = 56
• Interpretation: 41-56 = low fall risk
21-40 = medium fall risk
0 –20 = high fall risk

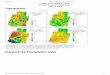
Berg Balance Scale Scores
General Instructions
• Please document each task and/or give instructions as written. When scoring, please record the lowest response category that applies for each item.
• In most items, the subject is asked to maintain a given position for a specific time. Progressively more points are deducted if:• the time or distance requirements are not met• the subject’s performance warrants supervision• the subject touches an external support or receives assistance from the examiner
• Subject should understand that they must maintain their balance while attempting the tasks. The choices of which leg to stand on or how far to reach are left to the subject. Poor judgment will adversely influence the performance and the scoring.
• Equipment required for testing is a stopwatch or watch with a second hand, and a ruler or other indicator of 2, 5, and 10 inches. Chairs used during testing should be a reasonable height. Either a step or a stool of average step height may be used for item # 12.
SITTING TO STANDING
INSTRUCTIONS: Please stand up. Try not to use your hand for support.
• ( ) 4 able to stand without using hands and stabilize independently
• ( ) 3 able to stand independently using hands
• ( ) 2 able to stand using hands after several tries
• ( ) 1 needs minimal aid to stand or stabilize
• ( ) 0 needs moderate or maximal assist to stand

STANDING UNSUPPORTED
• INSTRUCTIONS: Please stand for two minutes without holding on.
• ( ) 4 able to stand safely for 2 minutes
• ( ) 3 able to stand 2 minutes with supervision
• ( ) 2 able to stand 30 seconds unsupported
• ( ) 1 needs several tries to stand 30 seconds unsupported
• ( ) 0 unable to stand 30 seconds unsupported
• If a subject is able to stand 2 minutes unsupported, score full points for sitting unsupported. Proceed to item #4.

SITTING WITH BACK UNSUPPORTED BUT FEET SUPPORTED ON FLOOR OR ON A STOOL
INSTRUCTIONS: Please sit with arms folded for 2 minutes.
• ( ) 4 able to sit safely and securely for 2 minutes
• ( ) 3 able to sit 2 minutes under supervision
• ( ) 2 able to able to sit 30 seconds
• ( ) 1 able to sit 10 seconds
• ( ) 0 unable to sit without support 10 seconds

STANDING TO SITTING
INSTRUCTIONS: Please sit down.
• ( ) 4 sits safely with minimal use of hands
• ( ) 3 controls descent by using hands
• ( ) 2 uses back of legs against chair to control descent
• ( ) 1 sits independently but has uncontrolled descent
• ( ) 0 needs assist to sit

TRANSFERS
INSTRUCTIONS: Arrange chair(s) for pivot transfer. Ask subject to transfer one way toward a seat with armrests and one way toward a seat without armrests. You may use two chairs (one with and one without armrests) or a bed and a chair.
• ( ) 4 able to transfer safely with minor use of hands
• ( ) 3 able to transfer safely definite need of hands
• ( ) 2 able to transfer with verbal cuing and/or supervision
• ( ) 1 needs one person to assist
• ( ) 0 needs two people to assist or supervise to be safe
STANDING UNSUPPORTED WITH EYES CLOSED
INSTRUCTIONS: Please close your eyes and stand still for 10 seconds.
• ( ) 4 able to stand 10 seconds safely
• ( ) 3 able to stand 10 seconds with supervision
• ( ) 2 able to stand 3 seconds
• ( ) 1 unable to keep eyes closed 3 seconds but stays safely
• ( ) 0 needs help to keep from falling

STANDING UNSUPPORTED WITH FEET TOGETHERINSTRUCTIONS: Place your feet together and stand without holding on.
• ( ) 4 able to place feet together independently and stand 1 minute safely
• ( ) 3 able to place feet together independently and stand 1 minute with supervision
• ( ) 2 able to place feet together independently but unable to hold for 30 seconds
• ( ) 1 needs help to attain position but able to stand 15 seconds feet together
• ( ) 0 needs help to attain position and unable to hold for 15 seconds

REACHING FORWARD WITH OUTSTRETCHED ARM WHILE STANDING
INSTRUCTIONS: Lift arm to 90 degrees. Stretch out your fingers and reach forward as far as you can. (Examiner places a ruler at the end of fingertips when arm is at 90 degrees. Fingers should not touch the ruler while reaching forward. The recorded measure is the distance forward that the fingers reach while the subject is in the most forward lean position. When possible, ask subject to use both arms when reaching to avoid rotation of the trunk.)
• ( ) 4 can reach forward confidently 25 cm (10 inches)
• ( ) 3 can reach forward 12 cm (5 inches)
• ( ) 2 can reach forward 5 cm (2 inches)
• ( ) 1 reaches forward but needs supervision
• ( ) 0 loses balance while trying/requires external support

PICK UP OBJECT FROM THE FLOOR FROM A STANDING POSITION
INSTRUCTIONS: Pick up the shoe/slipper, which is place in front of your feet.
• ( ) 4 able to pick up slipper safely and easily
• ( ) 3 able to pick up slipper but needs supervision
• ( ) 2 unable to pick up but reaches 2-5 cm(1-2 inches) from slipper and keeps balance independently
• ( ) 1 unable to pick up and needs supervision while trying
• ( ) 0 unable to try/needs assist to keep from losing balance or falling

TURNING TO LOOK BEHIND OVER LEFT AND RIGHT SHOULDERS WHILE STANDING
INSTRUCTIONS: Turn to look directly behind you over toward the left shoulder. Repeat to the right. Examiner may pick an object to look at directly behind the subject to encourage a better twist turn.
• ( ) 4 looks behind from both sides and weight shifts well
• ( ) 3 looks behind one side only other side shows less weight shift
• ( ) 2 turns sideways only but maintains balance
• ( ) 1 needs supervision when turning
• ( ) 0 needs assist to keep from losing balance or falling

TURN 360 DEGREES
INSTRUCTIONS: Turn completely around in a full circle. Pause. Then turn a full circle in the other direction.
• ( ) 4 able to turn 360 degrees safely in 4 seconds or less
• ( ) 3 able to turn 360 degrees safely one side only 4 seconds or less
• ( ) 2 able to turn 360 degrees safely but slowly
• ( ) 1 needs close supervision or verbal cuing
• ( ) 0 needs assistance while turning
PLACE ALTERNATE FOOT ON STEP OR STOOL WHILE STANDING UNSUPPORTED
INSTRUCTIONS: Place each foot alternately on the step/stool. Continue until each foot has touch the step/stool four times.
• ( ) 4 able to stand independently and safely and complete 8 steps in 20 seconds
• ( ) 3 able to stand independently and complete 8 steps in > 20 seconds
• ( ) 2 able to complete 4 steps without aid with supervision
• ( ) 1 able to complete > 2 steps needs minimal assist
• ( ) 0 needs assistance to keep from falling/unable to try

STANDING UNSUPPORTED ONE FOOT IN FRONT
INSTRUCTIONS: (DEMONSTRATE TO SUBJECT) Place one foot directly in front of the other. If you feel that you cannot place your foot directly in front, try to step far enough ahead that the heel of your forward foot is ahead of the toes of the other foot. (To score 3 points, the length of the step should exceed the length of the other foot and the width of the stance should approximate the subject’s normal stride width.)
• ( ) 4 able to place foot tandem independently and hold 30 seconds
• ( ) 3 able to place foot ahead independently and hold 30 seconds
• ( ) 2 able to take small step independently and hold 30 seconds
• ( ) 1 needs help to step but can hold 15 seconds
• ( ) 0 loses balance while stepping or standing

STANDING ON ONE LEG
INSTRUCTIONS: Stand on one leg as long as you can without holding on.
• ( ) 4 able to lift leg independently and hold > 10 seconds
• ( ) 3 able to lift leg independently and hold 5-10 seconds
• ( ) 2 able to lift leg independently and hold ≥ 3 seconds
• ( ) 1 tries to lift leg unable to hold 3 seconds but remains standing independently.
• ( ) 0 unable to try of needs assist to prevent fall

Berg Balance Complete
Dynamic Gait Index
• Description: Developed to assess the likelihood of falling in older adults. Designed to test eight facets of gait.
• Equipment needed: Box (Shoebox), Cones (2), Stairs, 20’ walkway, 15” wide
• Completion Time: 15 minutes
• Scoring: A four-point ordinal scale, ranging from 0-3. “0” indicates the lowest level of function and “3” the highest level of function.
• Total Score = 24
• Interpretation: < 19/24 = predictive of falls risk in community dwelling elderly
> 22/24 = safe ambulators

1. Gait level surface _____
• Instructions: Walk at your normal speed from here to the next mark (20’)
• Grading: Mark the lowest category that applies.
• (3) Normal: Walks 20’, no assistive devices, good sped, no evidence for imbalance, normal gait pattern
• (2) Mild Impairment: Walks 20’, uses assistive devices, slower speed, mild gait deviations.
• (1) Moderate Impairment: Walks 20’, slow speed, abnormal gait pattern, evidence for imbalance.
• (0) Severe Impairment: Cannot walk 20’ without assistance, severe gait deviations or imbalance.

2. Change in gait speed _____
• Instructions: Begin walking at your normal pace (for 5’), when I tell you “go,” walk as fast as you can (for 5’). When I tell you “slow,” walk as slowly as you can (for 5’).
• Grading: Mark the lowest category that applies.• (3) Normal: Able to smoothly change walking speed without loss of
balance or gait deviation. Shows a significant difference in walking speeds between normal, fast and slow speeds.
• (2) Mild Impairment: Is able to change speed but demonstrates mild gait deviations, or not gait deviations but unable to achieve a significant change in velocity, or uses an assistive device.
• (1) Moderate Impairment: Makes only minor adjustments to walking speed, or accomplishes a change in speed with significant gait deviations, or changes speed but has significant gait deviations, or changes speed but loses balance but is able to recover and continue walking.
• (0) Severe Impairment: Cannot change speeds, or loses balance and has to reach for wall or be caught.
3. Gait with horizontal head turns _____
• Instructions: Begin walking at your normal pace. When I tell you to “look right,” keep walking straight, but turn your head to the right. Keep looking to the right until I tell you, “look left,” then keep walking straight and turn your head to the left. Keep your head to the left until I tell you “look straight,“ then keep walking straight, but return your head to the center.
• Grading: Mark the lowest category that applies.• (3) Normal: Performs head turns smoothly with no change in gait.• (2) Mild Impairment: Performs head turns smoothly with slight
change in gait velocity, i.e., minor disruption to smooth gait path or uses walking aid.
• (1) Moderate Impairment: Performs head turns with moderate change in gait velocity, slows down, staggers but recovers, can continue to walk.
• (0) Severe Impairment: Performs task with severe disruption of gait, i.e., staggers
• outside 15” path, loses balance, stops, reaches for wall.

4. Gait with vertical head turns _____
• Instructions: Begin walking at your normal pace. When I tell you to “look up,” keep walking straight, but tip your head up. Keep looking up until I tell you, “look down,” then keep walking straight and tip your head down. Keep your head down until I tell you “look straight,“ then keep walking straight, but return your head to the center.
• Grading: Mark the lowest category that applies.• (3) Normal: Performs head turns smoothly with no change in gait.• (2) Mild Impairment: Performs head turns smoothly with slight
change in gait velocity, i.e., minor disruption to smooth gait path or uses walking aid.
• (1) Moderate Impairment: Performs head turns with moderate change in gait velocity, slows down, staggers but recovers, can continue to walk.
• (0) Severe Impairment: Performs task with severe disruption of gait, i.e., staggers
• outside 15” path, loses balance, stops, reaches for wall.

5. Gait and pivot turn _____
• Instructions: Begin walking at your normal pace. When I tell you, “turn and stop,” turn as quickly as you can to face the opposite direction and stop.
• Grading: Mark the lowest category that applies.
• (3) Normal: Pivot turns safely within 3 seconds and stops quickly with no loss of balance.
• (2) Mild Impairment: Pivot turns safely in > 3 seconds and stops with no loss of balance.
• (1) Moderate Impairment: Turns slowly, requires verbal cueing, requires several small steps to catch balance following turn and stop.
• (0) Severe Impairment: Cannot turn safely, requires assistance to turn and stop.
6. Step over obstacle ____
• Instructions: Begin walking at your normal speed. When you come to the shoebox, step over it, not around it, and keep walking.
• Grading: Mark the lowest category that applies.
• (3) Normal: Is able to step over the box without changing gait speed, no evidence of imbalance.
• (2) Mild Impairment: Is able to step over box, but must slow down and adjust steps to clear box safely.
• (1) Moderate Impairment: Is able to step over box but must stop, then step over. May require verbal cueing.
• (0) Severe Impairment: Cannot perform without assistance.
7. Step around obstacles _____
• Instructions: Begin walking at normal speed. When you come to the first cone (about 6’ away), walk around the right side of it. When you come to the second cone (6’ past first cone), walk around it to the left.
• Grading: Mark the lowest category that applies.
• (3) Normal: Is able to walk around cones safely without changing gait speed; no evidence of imbalance.
• (2) Mild Impairment: Is able to step around both cones, but must slow down and adjust steps to clear cones.
• (1) Moderate Impairment: Is able to clear cones but must significantly slow, speed to accomplish task, or requires verbal cueing.
• (0) Severe Impairment: Unable to clear cones, walks into one or both cones, or requires physical assistance.

8. Steps _____
• Instructions: Walk up these stairs as you would at home, i.e., using the railing if necessary. At the top, turn around and walk down.
• Grading: Mark the lowest category that applies.
• (3) Normal: Alternating feet, no rail.
• (2) Mild Impairment: Alternating feet, must use rail.
• (1) Moderate Impairment: Two feet to a stair, must use rail.
• (0) Severe Impairment: Cannot do safely.

Dynamic Gait Index Complete

Functional Reach
• Functional Reach is item #8 in the Berg Balance Scale • Directions: • Using a yardstick mounted on the wall at shoulder height, ask the subject to
position themselves close to, but not touching the wall with their arm outstretched and hand fisted. Take note of the starting position by determining what number the MCP joints line up with on the yardstick. Have the subject reach as far forward as possible in a plane parallel with the measuring device.
• They are free to use various reaching strategies. Take note of the end position of the MCP joints against the ruler, and record the difference between the starting and ending position numbers. If they move their feet, that trial must be discarded and the trial repeated. Guard the subject as the task is performed to prevent a fall. Subjects are given two practice trials, and then their performance on an additional three trials is recorded and averaged.
• Scores less than 6 or 7 inches indicate limited functional balance. Most health individuals with adequate functional balance can reach 10 inches or more.
• Reference:Duncan P, Weiner D, Chandler J, et al. Functional reach: a new clinical measure of balance. J of Gerontol 1990; 45: M192-197.

Instructions to the patient:
• Please reach as far forward as you can without losing your balance. Keep your feet on the floor. You are not allowed to touch the wall or the ruler as you reach. You will have two practice trials and then I will record the distance that you reach forward.
• HINT: to prevent a starting position with the scapula protracted, have the person hold both arms out horizontally. If the fingers match, they are not protracting. Then lower the non-testing arm and begin the test.

Criteria to stop the test:
• The patient’s feet lifted up from the floor or they fell forward. Most patients fall forward with this test. The therapist should guard from the front as that is the direction that you reach forward.
Functional Reach Complete
Timed Up and Go (TUG) Test
Description of the Instrument
Patients are timed (in seconds) when performing the TUG—3 conditions
• 1. TUG alone-from sitting in a chair, stand up, walk 3 meters, turn around, walk back, and sit down..
• 2. TUG Cognitive-complete the task while counting backwards from a randomly selected number between 20 and 100.
• 3. TUG Manual-complete the task while carrying a full cup of water.
The time taken to complete the task is strongly correlated to level of functional mobility, (i.e. the more time taken, the more dependent in activities of daily living).
Norm Values
• TUG Alone is 13.5 seconds or longer with an overall correct prediction rate of 90%;
• TUG Manual (while carrying a glass of water) is 14.5 seconds or longer with a 90% correct prediction rate;
• TUG Cognitive (while counting backwards) is 15.0 seconds or longer with an overall correct prediction rate of 87%.
• Reference: • Lundlin-Olsson, L., Nyberg, L., & Gustafson, Y. (1998). Attention, frailty, and falls: the effect of a manual task on basic mobilty. Journal of
the American Geriatrics Society, 46, 758-761.• Podsiadlo, D., & Richardson, S. (1991). The timed “up & go”: A test of basic functional mobility for frail elderly persons. Journal of the
American Geriatrics Society, 39, 142-148.• Shumway-Cook, A., Brauer, S., & Woollacott, M. (2000). Predicting the probability for falls in community-dwelling older adults using the
timed up & go test. Physical Therapy, 80(9), 896-903.• Lusardi, M.M. (2004). Functional Performance in Community Living Older Adults. Journal of Geriatric Physical Therapy, 26(3), 14-22.
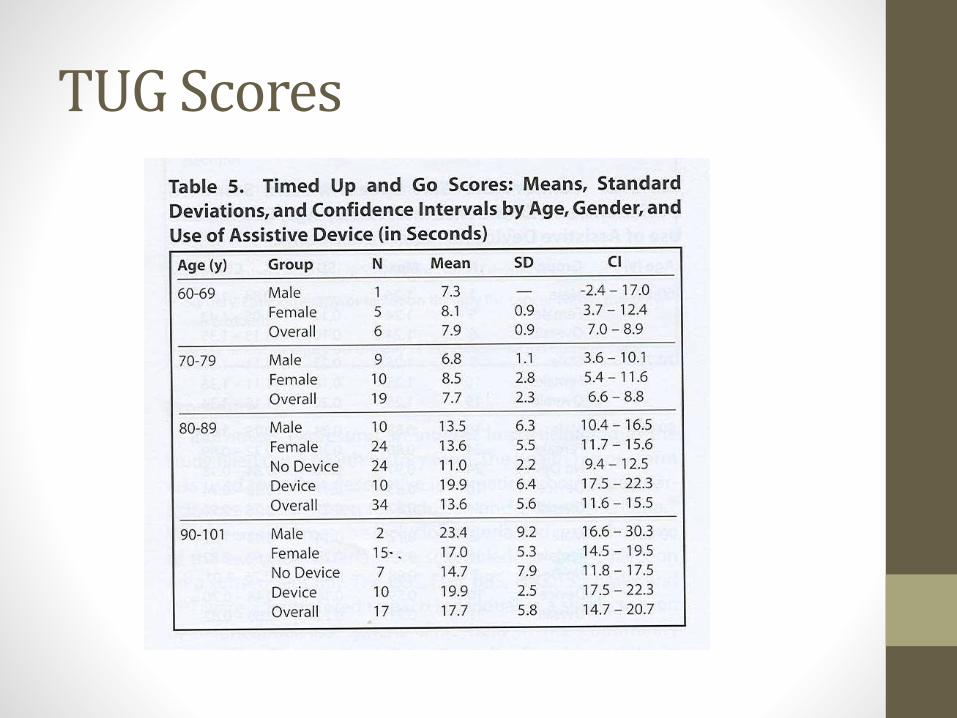
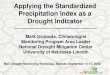
TUG Scores

Directions
The timed “Up and Go” test measures, in seconds, the time taken by an individual to stand up from a standard arm chair (approximate seat height of 46 cm [18in], arm height 65 cm [25.6 in]), walk a distance of 3 meters (118 inches, approximately 10 feet), turn, walk back to the chair, and sit down. The subject wears their regular footwear and uses their customary walking aid (none, cane, walker). No physical assistance is given. They start with their back against the chair, their arms resting on the armrests, and their walking aid at hand. They are instructed that, on the word “go” they are to get up and walk at your normal pace to a line on the floor 3 meters away, turn, return to the chair and sit down again. The subject walks through the test once before being timed in order to become familiar with the test. Either a stopwatch or a wristwatch with a second hand can be used to time the trial.

Instructions to the Patient
• “When I say ‘go’ I want you to stand up and walk to the line, turn and then walk back to the chair and sit down again. Walk at your normal pace.”

TUG Complete
Tinetti AssessmentDescription:The Tinetti assessment tool is an easily administered task-oriented test that measures an older adult’s gait and balance abilities.
Equipment needed: Hard armless chairStopwatch or wristwatch 15 ft walkway
Completion Time: 10-15 minutes
Scoring: A three-point ordinal scale, ranging from 0-2. “0” indicates the highest level of impairment and “2” the individuals independence.
Total Balance Score = 16Total Gait Score = 12Total Test Score = 28
Interpretation: 25-28 = low fall risk19-24 = medium fall risk< 19 = high fall risk
Reference:Tinetti ME. Performance-oriented assessment of mobility problems in elderly patients. JAGS 1986; 34: 119-126. (Scoring description: PT Bulletin Feb. 10, 1993)

Tinetti Assessment BalanceSITTING BALANCELeans or slides in chair = 0; Steady, safe =1
ARISES Unable without help = 0; Able, uses arms to help = 1; Able without using arms = 2
ATTEMPTS TO RISE Unable without help = 0; Able, requires > 1 attempt = 1;
Able on first attempt = 2
IMMEDIATE STANDING BALANCE (first 5 seconds)Unsteady (moves feet, sway, swaggers) = 0; Steady but uses support = 1; Steady without support = 2
STANDING BALANCEUnsteady = 0; Steady but > 4 inch BOS and requires support = 1;
Narrow stance without support = 2
STERNAL NUDGE (feet close together)Begins to fall = 0; Staggers, grabs, catches self = 1; Steady = 2
EYES CLOSED (feet close together)Unsteady = 0; Steady = 1
TURNING 360°Discontinuous steps = 0; Continuous steps = 1
TURNING 360°Unsteady (grabs, staggers) = 0; Steady = 1
SITTING DOWNUnsafe (misjudges distance, falls) = 0; Uses arms or not a smooth motion = 1; Safe, smooth motion = 2

Tinetti Assessment GaitGAIT INITIATION (immediate after told “go”)Any hesitancy, multiple attempts to start = 0; No hesitancy = 1
STEP LENGTH R swing foot passes L stance leg = 1; L swing foot passes R stance leg = 1
FOOT CLEARANCER foot completely clears floor = 1; L foot completely clears floor = 1
STEP SYMMETRYR and L step length unequal = 0; R and L step length equal = 1
STEP CONTINUITY Stopping or discontinuity between steps = 0; Steps appear continuous = 1
PATH (excursion) Marked deviation = 0; Mild/moderate deviation or uses device = 1; Straight without assistive device = 2
TRUNK Marked sway or uses assistive device = 0; No sway, but knee or trunk flexion or spreads arms out while walking = 1;None of above deviations = 2
BASE OF SUPPORTHeels apart = 0; Heels almost touching with gait = 1
Tinetti Assessment Complete

Speech Therapy Tests
• Arizona Battery for Communication Disorders of Dementia (ABCD)• Boston Diagnostic Aphasia Examination (BDAE-3)• Boston Naming Test Brief Cognitive Rating Scale (BCRS)• Frenchay Dysarthria Assessment • FROMAJE (Function, Reasoning, Orientation, Memory, Arithmetic,
Judgment, and Emotion)• Functional Linguistic Communication Inventory (FLCI) • Functional Staging Assessment Global Deterioration Scale (GDS) • Mini Mental Status Exam (MMSE) included• NIH Stroke Scale Ross Information Processing Assessment - Geriatric
(RIPA-G) • SLUMS Examination (St Louis University Mental Status Examination)
included• Bedside Evaluation of Dysphagia (bed)• MASA: Mann Assessment of Swallowing Ability • Test of Oral Structures (TOSF)

Mini Mental Status Exam
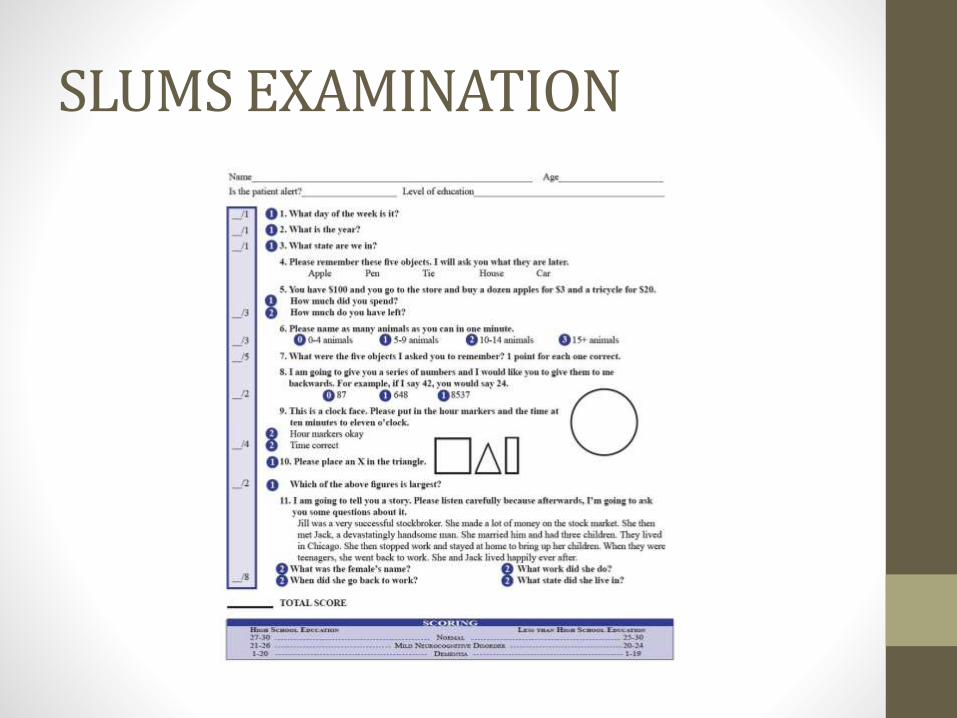
SLUMS EXAMINATION