Embed Size (px)
Citation preview
Draft Definitions for CDISC August 20, 2014
Page 1 of 33
Standardized Definitions for Cardiovascular and Stroke Endpoint Events in Clinical Trials
Karen A. Hicks, H. M. James Hung, Kenneth W. Mahaffey, Roxana Mehran, Steven E. Nissen,
Norman L. Stockbridge, Shari L. Targum, Robert Temple; on behalf of the Standardized Data Collection for Cardiovascular Trials Initiative
TASK FORCE MEMBERS Chairpersons: Karen A. Hicks, Kenneth W. Mahaffey, Roxana Mehran, Steven E. Nissen Working Groups: Kenneth W. Mahaffey, Roxana Mehran, and Steven E. Nissen, Co-ordinators; Steve Bai, Steven S. Brooks, Paul Burton, Kenneth J. Cavanaugh, Bernard R. Chaitman, B. Christine Clark, Donald E. Cutlip, Akshay S. Desai, Michael J. Domanski, Billy Dunn, Andrew Farb, Heather D. Fitter, C. Michael Gibson, Karen A. Hicks, H. M. James Hung, Kachikwu Illoh, Ilan Irony, Michael R. Jaff, Cheri Janning, Hylton V. Joffe, Bron Kisler, Judith M. Kramer, Rebecca Kush, Martin J. Landray, Alexandra Lansky, John Lawrence, Jonathan G. Levine, Eldrin F. Lewis, A. Michael Lincoff, John R. Marler, Laura Mauri, Brian McCourt, John McMurray, Yale Mitchel, Jean Morgan, David A. Morrow, Christopher M. O’Connor, Mary H. Parks, Douglas Peddicord, Marc A. Pfeffer, Kenneth Rosenfield, Leonard Sacks, Cathy A. Sila, Benjamin M. Scirica, Karen Snowdon-Way, Scott D. Solomon, Steven R. Steinhubl, Norman L. Stockbridge, Ana Szarfman, Barbara E. Tardiff, Shari L. Targum, James E. Tcheng, John R. Teerlink, Robert Temple, Chris Tolk, Ellis F. Unger, Christopher J. White, Stephen D. Wiviott, and Bram Zuckerman With special thanks to Rhonda Bartley, Leanne Madre, and MariJo Mencini, Co-ordinators (Clinical Trials Transformation Initiative) and to Rachel E. Hartford, Anna Park, and Lori Anne Wachter, Co-ordinators (Food and Drug Administration).
Draft Definitions for CDISC August 20, 2014
Page 2 of 33
Table of Contents
Introduction ............................................................................................................................... 3 CHAPTER 1. Definition of Cardiovascular Death ................................................................... 4 CHAPTER 2. Definition of Non-Cardiovascular Death .......................................................... 7 CHAPTER 3. Definition of Undetermined Cause of Death ..................................................... 8 CHAPTER 4. Definition of Myocardial Infarction: Please also see 2012 Third Universal Definition of Myocardial Infarction. ........................................................................................... 9 CHAPTER 5. Definition of Hospitalization for Unstable Angina ......................................... 12 CHAPTER 6. Definition of Transient Ischemic Attack and Stroke ..................................... 14 CHAPTER 7. Definition of Heart Failure Event .................................................................... 16 CHAPTER 8. Interventional Cardiology Definitions ............................................................. 19 CHAPTER 9. Definition of Peripheral Vascular Intervention .............................................. 27 CHAPTER 10. Definition of Stent Thrombosis ...................................................................... 30 References .................................................................................................................................... 32
Draft Definitions for CDISC August 20, 2014
Page 3 of 33
Introduction 1 The purpose of this document is to provide a framework of definitions for cardiovascular and 2 stroke endpoints in clinical trials. These definitions are based on clinical and research expertise, 3 published guidelines and definitions, and our current understanding of the specific laboratory 4 tests, diagnostic tests, and imaging techniques used in clinical practice to diagnose these events. 5 6 It is recognized that definitions of cardiovascular and stroke endpoints may change over time, as 7 new biomarkers or other diagnostic tests become available, or as standards evolve and 8 perceptions of clinical importance become modified. 9 10 Endpoint definitions are necessary in clinical trials so that events are clearly characterized by 11 objective criteria and reported uniformly. However, some events may be complex and may not 12 neatly fulfill the specified criteria. Furthermore, within a large-scale, multicenter, international 13 study, some results may not be available because they were never measured by the physician 14 responsible for their care at the time, because the test was not available locally, or because the 15 results can no longer be found. In all cases, clinical judgment should be used to determine the 16 most likely cause of an event. Where the person performing the adjudication of an event is blind 17 to the treatment allocation, any errors will be random, rather than systematic. As a consequence, 18 any noise introduced by slight misclassifications of events will not bias the result towards one 19 arm or another, but may mask a true difference in effectiveness or safety or increase the chance 20 of concluding non-inferiority. 21 22 Advances in database technologies and statistical methodologies have created opportunities to 23 aggregate large trial datasets. If uniformly defined, events in drug development programs or 24 among different clinical trials may be analyzed more easily and trends and other safety signals 25 may be identified. More consistent definitions could improve the ability to estimate event rates 26 in a contemplated clinical trial. 27 28 All definitions have limitations and will not seem satisfactory for every case. The goal of this 29 document is to propose definitions that will be suitable for study endpoints in clinical trials and 30 as events of interest in assessing cardiovascular safety. 31 32 Keeping in mind the value and limitations of any type of standardization, the following 33 definitions are proposed to simplify the conduct of trials with cardiovascular outcomes and to 34 form a basis on which to design clinical trials. Flexibility in these definitions may be necessary 35 to address the particulars of a drug product, clinical trial, or study population. 36 37 This document includes ten chapters. Each chapter provides the definition for a particular 38 cardiovascular event. 39 40
Draft Definitions for CDISC August 20, 2014
Page 4 of 33
CHAPTER 1. Definition of Cardiovascular Death 41 42 Cardiovascular death includes death resulting from an acute myocardial infarction (MI), 43 sudden cardiac death, death due to heart failure (HF), death due to stroke, death due to 44 cardiovascular (CV) procedures, death due to CV hemorrhage, and death due to other CV causes. 45 46 Classifying CV mortality more specifically (MI, sudden death etc.) is usually not needed for 47 outcome trials. However, such classification is difficult because the classifications refer both to 48 underlying cause (e.g., acute MI) and to mode of death (sudden/arrhythmic, progression of HF), 49 and they overlap substantially. The following definitions can, however, be used if desired. 50 51 52 1. Death due to Acute Myocardial Infarction refers to a death by any cardiovascular 53
mechanism (e.g., arrhythmia, sudden death, heart failure, stroke, pulmonary embolus, 54 peripheral arterial disease) ≤ 30 days1 after a MI related to the immediate consequences of 55 the MI, such as progressive heart failure or recalcitrant arrhythmia. We note that there may 56 be assessable mechanisms of cardiovascular death during this time period, but for simplicity, 57 if the cardiovascular death occurs ≤ 30 days of the myocardial infarction, it will be 58 considered a death due to myocardial infarction. 59 60 Acute MI should be verified to the extent possible by the diagnostic criteria outlined for 61 acute MI (see Chapter 4) or by autopsy findings showing recent MI or recent coronary 62 thrombosis. 63 64 Death resulting from a procedure to treat a MI (percutaneous coronary intervention (PCI), 65 coronary artery bypass graft surgery (CABG)), or to treat a complication resulting from MI, 66 should also be considered death due to acute MI. 67 68 Death resulting from an elective coronary procedure to treat myocardial ischemia (i.e., 69 chronic stable angina) or death due to a MI that occurs as a direct consequence of a CV 70 investigation/procedure/operation should be considered as a death due to a CV procedure. 71
72 73
1The 30 day cut-off is arbitrary.

Draft Definitions for CDISC August 20, 2014
Page 5 of 33
2. Sudden Cardiac Death refers to a death that occurs unexpectedly, not following an acute 74 MI, and includes the following deaths: 75
76 a. Death witnessed and occurring without new or worsening symptoms 77
78 b. Death witnessed within 60 minutes of the onset of new or worsening cardiac symptoms, 79
unless the symptoms suggest acute MI 80 81
c. Death witnessed and attributed to an identified arrhythmia (e.g., captured on an 82 electrocardiographic (ECG) recording, witnessed on a monitor, or unwitnessed but found 83 on implantable cardioverter-defibrillator review) 84
85 d. Death after unsuccessful resuscitation from cardiac arrest (e.g., implantable cardioverter 86
defibrillator (ICD) unresponsive sudden cardiac death, pulseless electrical activity arrest) 87 88 e. Death after successful resuscitation from cardiac arrest and without identification of a 89
specific cardiac or non-cardiac etiology 90 91
f. Unwitnessed death in a subject seen alive and clinically stable ≤ 24 hours prior to being 92 found dead without any evidence supporting a specific non-cardiovascular cause of death 93 (information regarding the patient’s clinical status preceding death should be provided, if 94 available) 95
96 97 General Considerations 98 99 o Unless additional information suggests an alternate specific cause of death (e.g., Death 100
due to Other Cardiovascular Causes), if a patient is seen alive ≤ 24 hours of being found 101 dead, sudden cardiac death (criterion 2f) should be recorded. For patients who were not 102 observed alive within 24 hours of death, undetermined cause of death should be recorded 103 (e.g., a subject found dead in bed, but who had not been seen by family for several days). 104
105 106
107 3. Death due to Heart Failure refers to a death in association with clinically worsening 108
symptoms and/or signs of heart failure regardless of HF etiology (see Chapter 7). Deaths due 109 to heart failure can have various etiologies, including single or recurrent myocardial 110 infarctions, ischemic or non-ischemic cardiomyopathy, hypertension, or valvular disease. 111
112 4. Death due to Stroke refers to death after a stroke that is either a direct consequence of the 113
stroke or a complication of the stroke. Acute stroke should be verified to the extent possible 114 by the diagnostic criteria outlined for stroke (see Chapter 6). 115 116
5. Death due to Cardiovascular Procedures refers to death caused by the immediate 117 complications of a cardiac procedure. 118
119
Draft Definitions for CDISC August 20, 2014
Page 6 of 33
6. Death due to Cardiovascular Hemorrhage refers to death related to hemorrhage such as a 120 non-stroke intracranial hemorrhage (see Chapter 6), non-procedural or non-traumatic 121 vascular rupture (e.g., aortic aneurysm), or hemorrhage causing cardiac tamponade. 122
123 7. Death due to Other Cardiovascular Causes refers to a CV death not included in the above 124
categories but with a specific, known cause (e.g., pulmonary embolism or peripheral arterial 125 disease). 126
127 128
Draft Definitions for CDISC August 20, 2014
Page 7 of 33
CHAPTER 2. Definition of Non-Cardiovascular Death 129 130 131 Non-cardiovascular death is defined as any death with a specific cause that is not thought to be 132 cardiovascular in nature, as listed in Chapter 1. Detailed recommendations on the classification 133 of non-CV causes of death are beyond the scope of this document. The level of detail required 134 and the optimum classification will depend on the nature of the study population and the 135 anticipated number and type of non-CV deaths. Any specific anticipated safety concern should 136 be included as a separate cause of death. The following is a suggested list of non-CV causes of 137 death: 138 139
• Pulmonary 140 • Renal 141 • Gastrointestinal 142 • Hepatobiliary 143 • Pancreatic 144 • Infection (includes sepsis) 145 • Inflammatory (e.g., Systemic Inflammatory Response Syndrome (SIRS) / Immune 146
(including autoimmune) (may include anaphylaxis from environmental (e.g., food) 147 allergies) 148
• Hemorrhage that is neither cardiovascular bleeding or a stroke (see Chapter 1, Section 6, 149 and Chapter 6) 150
• Non-CV procedure or surgery 151 • Trauma 152 • Suicide 153 • Non-prescription drug reaction or overdose 154 • Prescription drug reaction or overdose (may include anaphylaxis) 155 • Neurological (non-cardiovascular) 156 • Malignancy 157 • Other non-CV, specify: _________________ 158
159 160 161 162 163
Draft Definitions for CDISC August 20, 2014
Page 8 of 33
CHAPTER 3. Definition of Undetermined Cause of Death 164 165 Undetermined Cause of Death refers to a death not attributable to one of the above categories 166 of CV death or to a non-CV cause. Inability to classify the cause of death may be due to lack of 167 information (e.g., the only available information is “patient died”) or when there is insufficient 168 supporting information or detail to assign the cause of death. In general, most deaths should be 169 classifiable as CV or non-CV, and the use of this category of death, therefore, should be 170 discouraged and should apply to few patients in well-run clinical trials. 171 172 A common analytic approach for cause of death analyses is to assume that all undetermined 173 cases are included in the CV category (e.g., presumed CV death, specifically “death due to other 174 CV causes”). Nevertheless, the appropriate classification and analysis of undetermined causes of 175 death depends on the population, the intervention under investigation, and the disease process. 176 The approach should be prespecified and described in the protocol and other trial documentation 177 such as the endpoint adjudication procedures and/or the statistical analysis plan. 178 179 180

Draft Definitions for CDISC August 20, 2014
Page 9 of 33
CHAPTER 4. Definition of Myocardial Infarction: Please also see 2012 Third Universal 181 Definition of Myocardial Infarction. 182 183 1. General Considerations 184
185 The term myocardial infarction (MI) should be used when there is evidence of myocardial 186 necrosis in a clinical setting consistent with myocardial ischemia. 187 188 In general, the diagnosis of MI requires the combination of: 189
• Evidence of myocardial necrosis (either changes in cardiac biomarkers or post-190 mortem pathological findings); and 191
• Supporting information derived from the clinical presentation, electrocardiographic 192 changes, or the results of myocardial or coronary artery imaging 193
194 The totality of the clinical, electrocardiographic, and cardiac biomarker information should 195 be considered to determine whether or not a MI has occurred. Specifically, timing and trends 196 in cardiac biomarkers and electrocardiographic information require careful analysis. The 197 adjudication of MI should also take into account the clinical setting in which the event 198 occurs. MI may be adjudicated for an event that has characteristics of a MI but which does 199 not meet the strict definition because biomarker or electrocardiographic results are not 200 available. 201
202 2. Criteria for Myocardial Infarction 203 204
a. Clinical Presentation 205 The clinical presentation should be consistent with diagnosis of myocardial ischemia and 206 infarction. Other findings that might support the diagnosis of MI should be taken into 207 account because a number of conditions are associated with elevations in cardiac 208 biomarkers (e.g., trauma, surgery, pacing, ablation, heart failure, hypertrophic 209 cardiomyopathy, pulmonary embolism, severe pulmonary hypertension, stroke or 210 subarachnoid hemorrhage, infiltrative and inflammatory disorders of cardiac muscle, 211 drug toxicity, burns, critical illness, extreme exertion, and chronic kidney disease). 212 Supporting information can also be considered from myocardial imaging and coronary 213 imaging. The totality of the data may help differentiate acute MI from the background 214 disease process. 215
216 b. Biomarker Elevations 217
For cardiac biomarkers, laboratories should report an upper reference limit (URL). If the 218 99th percentile of the upper reference limit (URL) from the respective laboratory 219 performing the assay is not available, then the URL for myocardial necrosis from the 220 laboratory should be used. If the 99th percentile of the URL or the URL for myocardial 221 necrosis is not available, the MI decision limit for the particular laboratory should be 222 used as the URL. Laboratories can also report both the 99th percentile of the upper 223 reference limit and the MI decision limit. Reference limits from the laboratory 224 performing the assay are preferred over the manufacturer’s listed reference limits in an 225
Draft Definitions for CDISC August 20, 2014
Page 10 of 33
assay’s instructions for use. In general, troponins are preferred. CK-MB should be used 226 if troponins are not available, and total CK may be used in the absence of CK-MB and 227 troponin. 228 229 For MI subtypes, different biomarker elevations for CK, CK-MB, or troponin will be 230 required. The specific criteria will be referenced to the URL. 231 232 In many studies, particularly those in which patients present acutely to hospitals which 233 are not participating sites, it is not practical to stipulate the use of a single biomarker or 234 assay, and the locally available results are to be used as the basis for adjudication. 235 However, if possible, using the same cardiac biomarker assay and preferably, a core 236 laboratory, for all measurements reduces inter-assay variability. 237 238 Since the prognostic significance of different types of myocardial infarctions (e.g., 239 periprocedural myocardial infarction versus spontaneous myocardial infarction) may be 240 different, consider evaluating outcomes for these subsets of patients separately. 241 242
c. Electrocardiogram (ECG) Changes 243 Electrocardiographic changes can be used to support or confirm a MI. Supporting 244 evidence may be ischemic changes and confirmatory information may be new Q waves. 245 246 • ECG manifestations of acute myocardial ischemia (in absence of left ventricular 247
hypertrophy (LVH) and left bundle branch block (LBBB)): 248 249
o ST elevation 250 New ST elevation at the J point in two contiguous leads with the cut-points: 251 ≥ 0.1 mV in all leads other than leads V2-V3 where the following cut-points 252 apply: ≥ 0.2 mV in men ≥ 40 years (≥ 0.25 mV in men < 40 years) or 253 ≥ 0.15 mV in women. 254
255 o ST depression and T-wave changes 256
New horizontal or down-sloping ST depression ≥ 0.05 mV in two contiguous 257 leads and/or new T inversion ≥ 0.1 mV in two contiguous leads with prominent R 258 wave or R/S ratio > 1. 259 260
The above ECG criteria illustrate patterns consistent with myocardial ischemia. In 261 patients with abnormal biomarkers, it is recognized that lesser ECG abnormalities 262 may represent an ischemic response and may be accepted under the category of 263 abnormal ECG findings. 264 265
Draft Definitions for CDISC August 20, 2014
Page 11 of 33
• Criteria for pathological Q-wave 266 267
o Any Q-wave in leads V2-V3 ≥ 0.02 seconds or QS complex in leads V2 and V3 268 o Q-wave ≥ 0.03 seconds and ≥ 0.1 mV deep or QS complex in leads I, II, aVL, 269
aVF, or V4-V6 in any two leads of a contiguous lead grouping (I, aVL; V1-V6; 270 II, III, and aVF)a 271
272 aThe same criteria are used for supplemental leads V7-V9, and for the Cabrera frontal 273 plane lead grouping. 274
275 • ECG changes associated with prior myocardial infarction 276
277 o Pathological Q-waves, as defined above 278 o R-wave ≥ 0.04 seconds in V1-V2 and R/S ≥ 1 with a concordant positive T-wave 279
in the absence of a conduction defect 280 281
• Criteria for prior myocardial infarction 282 Any one of the following criteria meets the diagnosis for prior MI: 283 o Pathological Q waves with or without symptoms in the absence of non-ischemic 284
causes 285 o Imaging evidence of a region of loss of viable myocardium that is thinned and 286
fails to contract, in the absence of a non-ischemic cause 287 o Pathological findings of a prior myocardial infarction 288
289
Draft Definitions for CDISC August 20, 2014
Page 12 of 33
CHAPTER 5. Definition of Hospitalization for Unstable Angina 290 291 292 Unstable angina requiring hospitalization is defined as 293 294 1. Ischemic discomfort (angina, or symptoms thought to be equivalent) ≥ 10 minutes in duration 295
occurring 296 • at rest, or 297 • in an accelerating pattern with frequent episodes associated with progressively 298
decreased exercise capacity. 299 300 AND 301 302 2. Prompting an unscheduled hospitalization within 24 hours of the most recent symptoms. 303
Hospitalization is defined as an admission to an inpatient unit or a visit to an emergency 304 department that results in at least a 24 hour stay (or a change in calendar date if the hospital 305 admission or discharge times are not available). 306
307 AND 308 309 3. At least one of the following: 310 311
a. New or worsening ST or T wave changes on resting ECG (in the absence of 312 confounders, such as LBBB or LVH) 313
314 • Transient ST elevation (duration < 20 minutes) 315
New ST elevation at the J point in two contiguous leads with the cut-points: ≥ 0.1 316 mV in all leads other than leads V2-V3 where the following cut-points apply: 317 ≥ 0.2 mV in men ≥ 40 years (≥ 0.25 mV in men < 40 years) or 318 ≥ 0.15 mV in women. 319
320 • ST depression and T-wave changes 321
New horizontal or down-sloping ST depression ≥ 0.05 mV in two contiguous 322 leads and/or new T inversion ≥ 0.3 mV in two contiguous leads with prominent 323 R wave or R/S ratio > 1. 324
325 326
b. Definite evidence of inducible myocardial ischemia as demonstrated by: 327 • an early positive exercise stress test, defined as ST elevation or ≥ 2 mm ST 328
depression prior to 5 mets 329 OR 330 • stress echocardiography (reversible wall motion abnormality) OR 331 • myocardial scintigraphy (reversible perfusion defect), OR 332 • MRI (myocardial perfusion deficit under pharmacologic stress). 333
334
Draft Definitions for CDISC August 20, 2014
Page 13 of 33
and believed to be responsible for the myocardial ischemic symptoms/signs. 335 336
c. Angiographic evidence of new or worse ≥ 70% lesion (≥ 50% for left main lesion) 337 and/or thrombus in an epicardial coronary artery that is believed to be responsible for 338 the myocardial ischemic symptoms/signs. 339
340 d. Need for coronary revascularization procedure (PCI or CABG) for the presumed 341
culprit lesion(s). This criterion would be fulfilled if revascularization was undertaken 342 during the unscheduled hospitalization, or subsequent to transfer to another institution 343 without interceding home discharge. 344
345 AND 346 347 4. Negative cardiac biomarkers and no evidence of acute MI 348 349 350 General Considerations 351
352 1. Escalation of pharmacotherapy for ischemia, such as intravenous nitrates or increasing 353
dosages of β-blockers, should be considered supportive but not diagnostic of unstable angina. 354 However, a typical presentation and admission to the hospital with escalation of 355 pharmacotherapy, without any of the additional findings listed under category 3, would be 356 insufficient to support classification as hospitalization for unstable angina. 357
358 2. If subjects are admitted with suspected unstable angina, and subsequent testing reveals a non-359
cardiac or non-ischemic etiology, this event should not be recorded as hospitalization for 360 unstable angina. Potential ischemic events meeting the criteria for myocardial infarction 361 should not be adjudicated as unstable angina. 362 363
3. Planned hospitalization or rehospitalization for performance of an elective revascularization 364 in patients who do not fulfill the criteria for unstable angina should not be considered a 365 hospitalization for unstable angina. For example, 366
367 • Hospitalization of a patient with stable exertional angina for coronary angiography 368
and PCI that is prompted by a positive outpatient stress test should not be considered 369 hospitalization for unstable angina. 370
371 • Rehospitalization of a patient meeting the criteria for unstable angina who was 372
stabilized, discharged, and subsequently readmitted for revascularization, does not 373 constitute a second hospitalization for unstable angina. 374
375 4. A patient who undergoes an elective catheterization where incidental coronary artery disease 376
is found and who subsequently undergoes coronary revascularization will not be considered 377 as meeting the hospitalization for unstable angina endpoint. 378
379 380
Draft Definitions for CDISC August 20, 2014
Page 14 of 33
CHAPTER 6. Definition of Transient Ischemic Attack and Stroke 381 382 Introduction 383 384 These definitions of Transient Ischemic Attack and Stroke apply to a wide range of 385 clinical trials. They are general, overarching, and widely applicable definitions combined 386 with a specific clinical measurement of disability. They are flexible in their application 387 and consistent with contemporary understanding of the pathophysiology of stroke. This 388 approach enables clinical trials to assess the clinically relevant consequences of vascular 389 brain injury for determining the safety or effectiveness of an intervention. 390 391 The distinction between a Transient Ischemic Attack and an Ischemic Stroke is the 392 presence of infarction. Persistence of symptoms is an acceptable indicator of acute 393 infarction. Thus, duration of symptom persistence that will be used to distinguish 394 between transient ischemia and acute infarction should be defined for any clinical trial in 395 which it is used. 396 397 In trials involving patients with stroke, evidence of vascular central nervous system 398 injury without recognized neurological dysfunction may be observed. Examples include 399 microhemorrhage, silent infarction, and silent hemorrhage. When encountered, the 400 clinical relevance of these findings may be unclear. If appropriate for a given clinical 401 trial, however, they should be precisely defined and categorized. 402 403 Subdural hematomas are intracranial hemorrhagic events and not strokes. 404 405 Transient Ischemic Attack 406 407 Transient ischemic attack (TIA) is defined as a transient episode of focal neurological 408 dysfunction caused by brain, spinal cord, or retinal ischemia, without acute infarction. 409 410 411 Stroke 412 413 Stroke is defined as an acute episode of focal or global neurological dysfunction caused 414 by brain, spinal cord, or retinal vascular injury as a result of hemorrhage or infarction. 415 416 Classification: 417 418
A. Ischemic Stroke 419 420 Ischemic stroke is defined as an acute episode of focal cerebral, spinal, or retinal 421 dysfunction caused by infarction of central nervous system tissue. 422 423
Draft Definitions for CDISC August 20, 2014
Page 15 of 33
Hemorrhage may be a consequence of ischemic stroke. In this situation, the 424 stroke is an ischemic stroke with hemorrhagic transformation and not a 425 hemorrhagic stroke. 426
427 B. Hemorrhagic Stroke 428
429 Hemorrhagic stroke is defined as an acute episode of focal or global cerebral or 430 spinal dysfunction caused by intraparenchymal, intraventricular, or subarachnoid 431 hemorrhage. 432
433 C. Undetermined Stroke 434
435 Undetermined stroke is defined as an acute episode of focal or global neurological 436 dysfunction caused by presumed brain, spinal cord, or retinal vascular injury as a 437 result of hemorrhage or infarction but with insufficient information to allow 438 categorization as A or B. 439 440 441
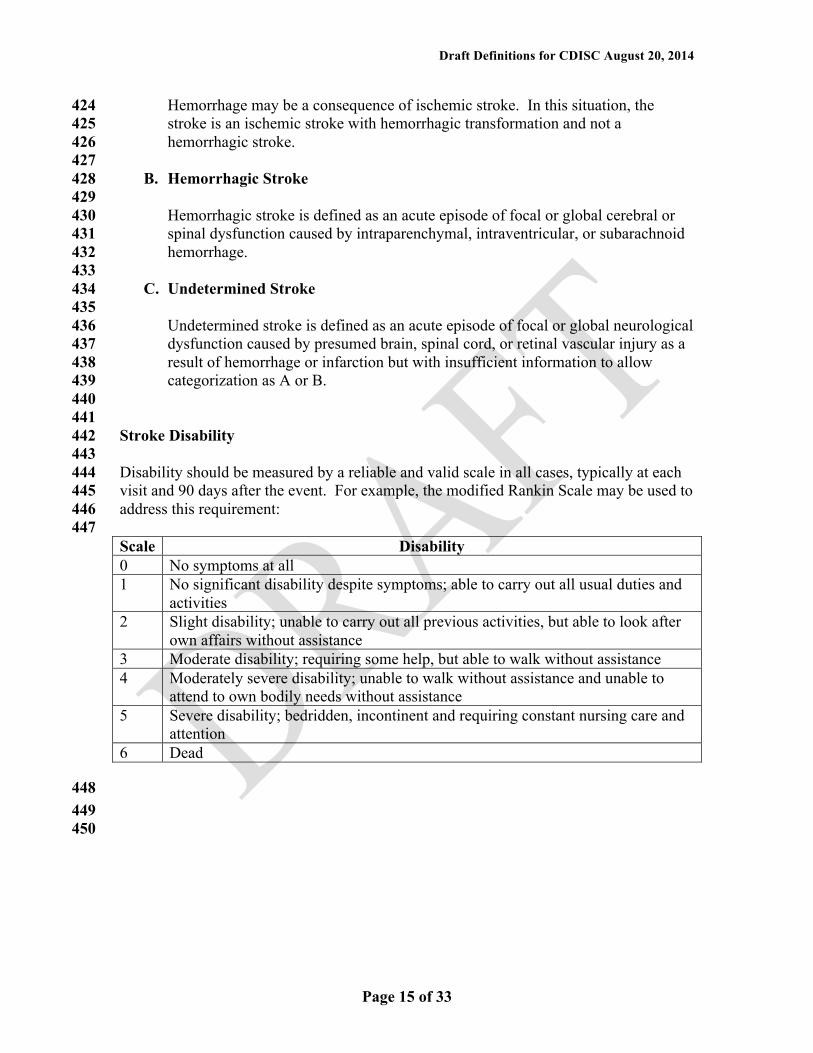
Stroke Disability 442 443 Disability should be measured by a reliable and valid scale in all cases, typically at each 444 visit and 90 days after the event. For example, the modified Rankin Scale may be used to 445 address this requirement: 446
447 Scale Disability 0 No symptoms at all 1 No significant disability despite symptoms; able to carry out all usual duties and
activities 2 Slight disability; unable to carry out all previous activities, but able to look after
own affairs without assistance 3 Moderate disability; requiring some help, but able to walk without assistance 4 Moderately severe disability; unable to walk without assistance and unable to
attend to own bodily needs without assistance 5 Severe disability; bedridden, incontinent and requiring constant nursing care and
attention 6 Dead
448 449 450
Draft Definitions for CDISC August 20, 2014
Page 16 of 33
CHAPTER 7. Definition of Heart Failure Event 451 452 453 A Heart Failure Event includes hospitalization for heart failure and may include urgent 454 outpatient visits. HF hospitalizations should remain delineated from urgent visits. If urgent 455 visits are included in the HF event endpoint, the number of urgent visits needs to be explicitly 456 presented separately from the hospitalizations. 457 458 A Heart Failure Hospitalization is defined as an event that meets ALL of the following 459 criteria: 460 461
1) The patient is admitted to the hospital with a primary diagnosis of HF 462 463 2) The patient’s length-of-stay in hospital extends for at least 24 hours (or a change in 464
calendar date if the hospital admission and discharge times are unavailable) 465 466 3) The patient exhibits documented new or worsening symptoms due to HF on presentation, 467
including at least ONE of the following: 468 469
a. Dyspnea (dyspnea with exertion, dyspnea at rest, orthopnea, paroxysmal 470 nocturnal dyspnea) 471
b. Decreased exercise tolerance 472 c. Fatigue 473 d. Other symptoms of worsened end-organ perfusion or volume overload (must be 474 specified and described by the protocol) 475 476
4) The patient has objective evidence of new or worsening HF, consisting of at least TWO 477 physical examination findings OR one physical examination finding and at least ONE 478 laboratory criterion), including: 479
480 a. Physical examination findings considered to be due to heart failure, including new 481
or worsened: 482 483
i. Peripheral edema 484 ii. Increasing abdominal distention or ascites (in the absence of primary hepatic 485
disease) 486 iii. Pulmonary rales/crackles/crepitations 487 iv. Increased jugular venous pressure and/or hepatojugular reflux 488 v. S3 gallop 489
vi. Clinically significant or rapid weight gain thought to be related to fluid 490 retention 491
Draft Definitions for CDISC August 20, 2014
Page 17 of 33
492 493 b. Laboratory evidence of new or worsening HF, if obtained within 24 hours of 494
presentation, including: 495 496
i. Increased B-type natriuretic peptide (BNP)/ N-terminal pro-BNP (NT-497 proBNP) concentrations consistent with decompensation of heart failure (such 498 as BNP > 500 pg/mL or NT-proBNP > 2,000 pg/mL). In patients with 499 chronically elevated natriuretic peptides, a significant increase should be 500 noted above baseline. 501
502 ii. Radiological evidence of pulmonary congestion 503
504 iii. Non-invasive diagnostic evidence of clinically significant elevated left- or 505
right-sided ventricular filling pressure or low cardiac output. For example, 506 echocardiographic criteria could include: E/e’ > 15 or D-dominant pulmonary 507 venous inflow pattern, plethoric inferior vena cava with minimal collapse on 508 inspiration, or decreased left ventricular outflow tract (LVOT) minute stroke 509 distance (time velocity integral (TVI)) 510
511 OR 512 513
iv. Invasive diagnostic evidence with right heart catheterization showing a 514 pulmonary capillary wedge pressure (pulmonary artery occlusion pressure) 515 ≥ 18 mmHg, central venous pressure ≥ 12 mmHg, or a cardiac index 516 < 2.2 L/min/m2 517
518 Note: All results from diagnostic tests should be reported, if available, even if 519 they do not meet the above criteria, because they provide important 520 information for the adjudication of these events. 521 522
5) The patient receives initiation or intensification of treatment specifically for HF, 523 including at least ONE of the following: 524
525 a. Augmentation in oral diuretic therapy 526 b. Intravenous diuretic or vasoactive agent (e.g., inotrope, vasopressor, or 527
vasodilator) 528 c. Mechanical or surgical intervention, including: 529
i. Mechanical circulatory support (e.g., intra-aortic balloon pump, ventricular 530 assist device, extracorporeal membrane oxygenation, total artificial heart) 531
ii. Mechanical fluid removal (e.g., ultrafiltration, hemofiltration, dialysis) 532 533
Draft Definitions for CDISC August 20, 2014
Page 18 of 33
An Urgent Heart Failure Visit is defined as an event that meets all of the following: 534 535
1) The patient has an urgent, unscheduled office/practice or emergency department visit for 536 a primary diagnosis of HF, but not meeting the criteria for a HF hospitalization 537
2) All signs and symptoms for HF hospitalization (i.e., 3) symptoms, 4) physical 538 examination findings/laboratory evidence of new or worsening HF, as indicated above) 539 must be met 540
3) The patient receives initiation or intensification of treatment specifically for HF, as 541 detailed in the above section with the exception of oral diuretic therapy, which will not be 542 sufficient 543
Draft Definitions for CDISC August 20, 2014
Page 19 of 33
CHAPTER 8. Interventional Cardiology Definitions 544 545 A. Clinical Definitions 546
547 1. Clinically-Driven Target Lesion Revascularization: Revascularization is clinically-548
driven if the target lesion diameter stenosis is > 50% by quantitative coronary 549 angiography (QCA) and the subject has clinical or functional ischemia which cannot be 550 explained by another native coronary or bypass graft lesion. Clinical or functional 551 ischemia includes any of the following: 552
553 a. A history of angina pectoris, presumably related to the target vessel 554 b. Objective signs of ischemia at rest (electrocardiographic changes) or during exercise 555
test (or equivalent), presumably related to the target vessel 556 c. Abnormal results of any invasive functional diagnostic test [e.g., coronary flow 557
reserve (CFR) or fractional flow reserve (FFR)] 558 559
Comment: Target lesion revascularization of a > 70% diameter stenosis by QCA in the 560 absence of the above signs or symptoms may be considered clinically-driven. 561 562 Comment: In the absence of QCA data or if a < 50% stenosis is present, TLR may be 563 considered clinically-driven by the Clinical Events Committee (CEC) if severe ischemic 564 signs and symptoms attributed to the target lesion are present. 565 566
2. Non-Target Lesion and Non-Target Lesion Revascularization: A lesion for which 567 revascularization is not attempted or one in which revascularization is performed using a 568 non-study device, respectively. 569
570 3. Non-Target Vessel and Non-Target Vessel Revascularization: A vessel for which 571
revascularization is not attempted or one in which revascularization is performed using a 572 non-study device, respectively. 573
574 4. Percutaneous Coronary Intervention (PCI) Status: 575
576 a. Elective: The procedure can be performed on an outpatient basis or during a 577
subsequent hospitalization without significant risk of myocardial infarction (MI) or 578 death. For stable in-patients, the procedure is being performed during this 579 hospitalization for convenience and ease of scheduling and NOT because the patient's 580 clinical situation demands the procedure prior to discharge. 581
582 b. Urgent: The procedure should be performed on an inpatient basis and prior to 583
discharge because of significant concerns that there is risk of myocardial ischemia, 584 MI, and/or death. Patients who are outpatients or in the emergency department at the 585 time that the cardiac catheterization is requested would warrant hospital admission 586 based on their clinical presentation. 587
588
Draft Definitions for CDISC August 20, 2014
Page 20 of 33
c. Emergency: The procedure should be performed as soon as possible because of 589 substantial concerns that ongoing myocardial ischemia and/or MI could lead to death. 590 "As soon as possible" refers to a patient who is of sufficient acuity that one would 591 cancel a scheduled case to perform this procedure immediately in the next available 592 room during business hours, or one would activate the on-call team were this to occur 593 during off-hours. 594
595 d. Salvage: The procedure is a last resort. The patient is in cardiogenic shock when the 596
PCI begins (i.e., the time at which the first guide wire or intracoronary device is 597 introduced into a coronary artery or bypass graft for the purpose of mechanical 598 revascularization) OR within the last ten minutes prior to the start of the case or 599 during the diagnostic portion of the case, the patient has also received chest 600 compressions or has been on unanticipated circulatory support (e.g., intra-aortic 601 balloon pump, extracorporeal membrane oxygenation, or cardiopulmonary support). 602
603 5. Percutaneous Coronary Intervention (PCI): Placement of an angioplasty guide wire, 604
balloon, or other device (e.g., stent, atherectomy catheter, brachytherapy delivery device, 605 or thrombectomy catheter) into a native coronary artery or coronary artery bypass graft 606 for the purpose of mechanical coronary revascularization. In the assessment of the 607 severity of coronary lesions with the use of intravascular ultrasound, coronary flow 608 reserve (CFR), or fractional flow reserve (FFR), insertion of a guide wire will NOT be 609 considered PCI. 610
611 6. Procedural Success: Achievement of < 30 % residual diameter stenosis of the target 612
lesion assessed by visual inspection or QCA and no in-hospital major adverse cardiac 613 events (MACE, a composite of death, MI, or repeat coronary revascularization of the 614 target lesion). Ideally, the assessment of the residual stenosis at the end of the procedure 615 should be performed by an angiographic core laboratory. 616 617 Comment: For some device interventions (e.g., balloon angioplasty), achievement of 618 < 50% diameter stenosis by visual inspection or QCA is an acceptable definition for 619 procedural success. 620
621 7. Target Lesion: Any lesion treated or attempted to be treated during the PCI with the 622
study device. The target lesion includes the arterial segment treated with the study device 623 (stent, in most cases) plus 5 mm proximal and 5 mm distal to the treatment site. 624
625 8. Target Lesion Failure (TLF): The composite of ischemia-driven revascularization of 626
the target lesion, MI related to the target vessel, or cardiac death related to the target 627 vessel. If it cannot be determined with certainty whether the MI or death was related to 628 the target vessel, it is considered a TLF. 629
630
Draft Definitions for CDISC August 20, 2014
Page 21 of 33
9. Target Lesion Revascularization (TLR): Any repeat percutaneous intervention of the 631 target lesion (including 5 mm proximal and 5 mm distal to the target lesion) or surgical 632 bypass of the target vessel performed for restenosis or other complication involving the 633 target lesion. In the assessment of TLR, angiograms should be assessed by an 634 angiographic core laboratory (if designated) and made available to the CEC for review 635 upon request. 636
637 10. Target Vessel: A major native coronary artery (e.g., left main coronary artery, left 638
anterior descending coronary artery, left circumflex coronary artery, or right coronary 639 artery) or bypass graft containing the target lesion. A native coronary artery target vessel 640 includes the arterial segments upstream and downstream to the target lesion plus major 641 side branches. 642
643 11. Target Vessel Failure (TVF): The composite of ischemia-driven revascularization of 644
the target vessel, MI related to the target vessel, or cardiac death related to the target 645 vessel. If it cannot be determined with certainty whether the MI or death was related to 646 the target vessel, it is considered a TVF. 647
648 12. Target Vessel, Non-Target Lesion, and Target Vessel, Non-Target Lesion 649
Revascularization: Any lesion or revascularization of a lesion in the target vessel other 650 than the target lesion, respectively. 651
652 13. Target Vessel Revascularization (TVR): Any repeat percutaneous intervention or 653
surgical bypass of any segment of the target vessel. In the assessment of TVR, 654 angiograms should be assessed by an angiographic core laboratory (if designated) and 655 made available to the CEC for review upon request. 656
657 14. Vascular Complications: 658
• Access site hematoma: Development of a new, localized collection of blood at a 659 vascular access site sufficient to produce a palpable mass within 72 hours of a 660 procedure. 661
• Arteriovenous fistula: Development of a new, unintended communication between 662 an artery and a vein occurring at a vascular access site within 72 hours of a procedure. 663
• Peripheral ischemia: Development of new arterial insufficiency sufficient to 664 produce clinical signs or symptoms of ischemia (pallor, pain, paresthesia) distal to a 665 vascular access site within 72 hours of a procedure. 666
• Peripheral nerve injury: Development of new sensory or motor loss of peripheral 667 nerve function from external nerve compression (e.g., as a result of positioning during 668 a procedure), or internal compression or direct nerve damage from the procedure, 669 occurring within 72 hours of a procedure. 670
• Pseudoaneurysm: Development of a new localized collection of blood with a 671 persistent communication (neck) originating at a vascular access site and occurring 672 within 72h of a procedure. 673
• Retroperitoneal hemorrhage: Development of new bleeding into the 674 retroperitoneal space originating at a vascular access site and occurring within 72 675 hours of a procedure. 676
677
Draft Definitions for CDISC August 20, 2014
Page 22 of 33
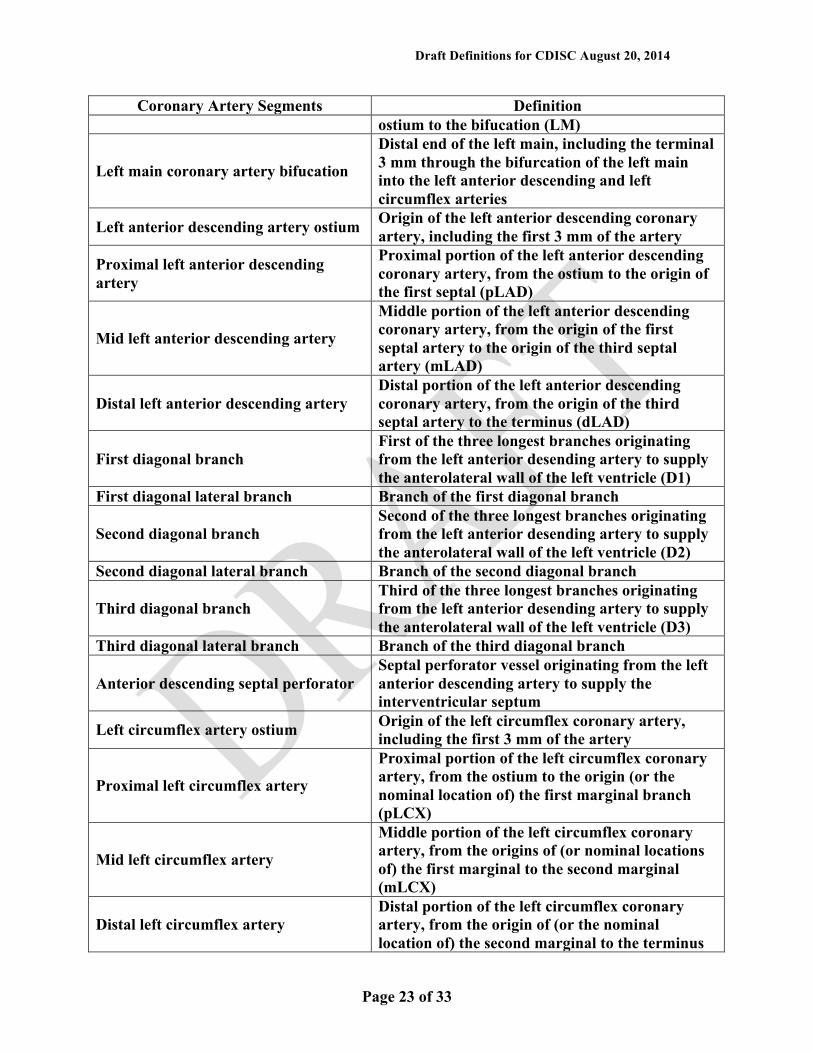
B. Angiographic Definitions 678 679
1. Abrupt Closure: New intra-procedural severely reduced flow (TIMI grade 0-1) within 680 the target vessel that persists and requires intervention by stenting or other treatment, or 681 results in MI or death. Abrupt closure requires an association with a vascular dissection, 682 thrombus, or severe spasm at the treatment site or within the instrumented vessel. 683
684 2. Coronary Lesions Treated 685
686 Coronary Artery Segments Definition
Right coronary artery ostium Origin of the right coronary artery, including the first 3 mm of the artery
Proximal right coronary artery
Proximal portion of the right coronary artery, from the ostium of the right coronary artery to the origin of the first right ventricular branch (pRCA)
Mid right coronary artery Middle portion of the right coronary artery, from the origin of the first right ventricular branch to the acute margin (mRCA)
Distal right coronary artery Distal portion of the right coronary artery, from the acute margin to the origin of the posterior descending artery (dRCA)
Right posterior descending artery
In right dominant and mixed circulations, the vessel that runs in the posterior interventricular groove and supplies septal perforator branches (PDA)
Posterolateral segmental artery
In right dominant circulations, the distal continuation of the right coronary artery in the posterior atrioventricular groove after the origin of the right posterior descending artery (PLSA)
First right posterolateral branch In right dominant circulations, the first posterolateral branch originating from the right posterior atrioventricular artery (RPL1)
Second right posterolateral branch In right dominant circulations, the second posterolateral branch originating from the right posterior atrioventricular artery (RPL2)
Third right posterolateral branch In right dominant circulations, the third posterolateral branch originating from the right posterior atrioventricular artery (RPL3)
Posterior descending septal perforator Septal perforator vessel originating from the posterior descending artery
Right ventricular branch Branch arising from the right coronary artery to supply the right ventricular wall (RV)
Left main coronary artery ostium Origin of the left coronary artery, including the first 3 mm of the artery
Left main coronary artery body Body of the left main coronary artery, from the
Draft Definitions for CDISC August 20, 2014
Page 23 of 33
Coronary Artery Segments Definition ostium to the bifucation (LM)
Left main coronary artery bifucation
Distal end of the left main, including the terminal 3 mm through the bifurcation of the left main into the left anterior descending and left circumflex arteries
Left anterior descending artery ostium Origin of the left anterior descending coronary artery, including the first 3 mm of the artery
Proximal left anterior descending artery
Proximal portion of the left anterior descending coronary artery, from the ostium to the origin of the first septal (pLAD)
Mid left anterior descending artery
Middle portion of the left anterior descending coronary artery, from the origin of the first septal artery to the origin of the third septal artery (mLAD)
Distal left anterior descending artery Distal portion of the left anterior descending coronary artery, from the origin of the third septal artery to the terminus (dLAD)
First diagonal branch First of the three longest branches originating from the left anterior desending artery to supply the anterolateral wall of the left ventricle (D1)
First diagonal lateral branch Branch of the first diagonal branch
Second diagonal branch Second of the three longest branches originating from the left anterior desending artery to supply the anterolateral wall of the left ventricle (D2)
Second diagonal lateral branch Branch of the second diagonal branch
Third diagonal branch Third of the three longest branches originating from the left anterior desending artery to supply the anterolateral wall of the left ventricle (D3)
Third diagonal lateral branch Branch of the third diagonal branch
Anterior descending septal perforator Septal perforator vessel originating from the left anterior descending artery to supply the interventricular septum
Left circumflex artery ostium Origin of the left circumflex coronary artery, including the first 3 mm of the artery
Proximal left circumflex artery
Proximal portion of the left circumflex coronary artery, from the ostium to the origin (or the nominal location of) the first marginal branch (pLCX)
Mid left circumflex artery
Middle portion of the left circumflex coronary artery, from the origins of (or nominal locations of) the first marginal to the second marginal (mLCX)
Distal left circumflex artery Distal portion of the left circumflex coronary artery, from the origin of (or the nominal location of) the second marginal to the terminus
Draft Definitions for CDISC August 20, 2014
Page 24 of 33
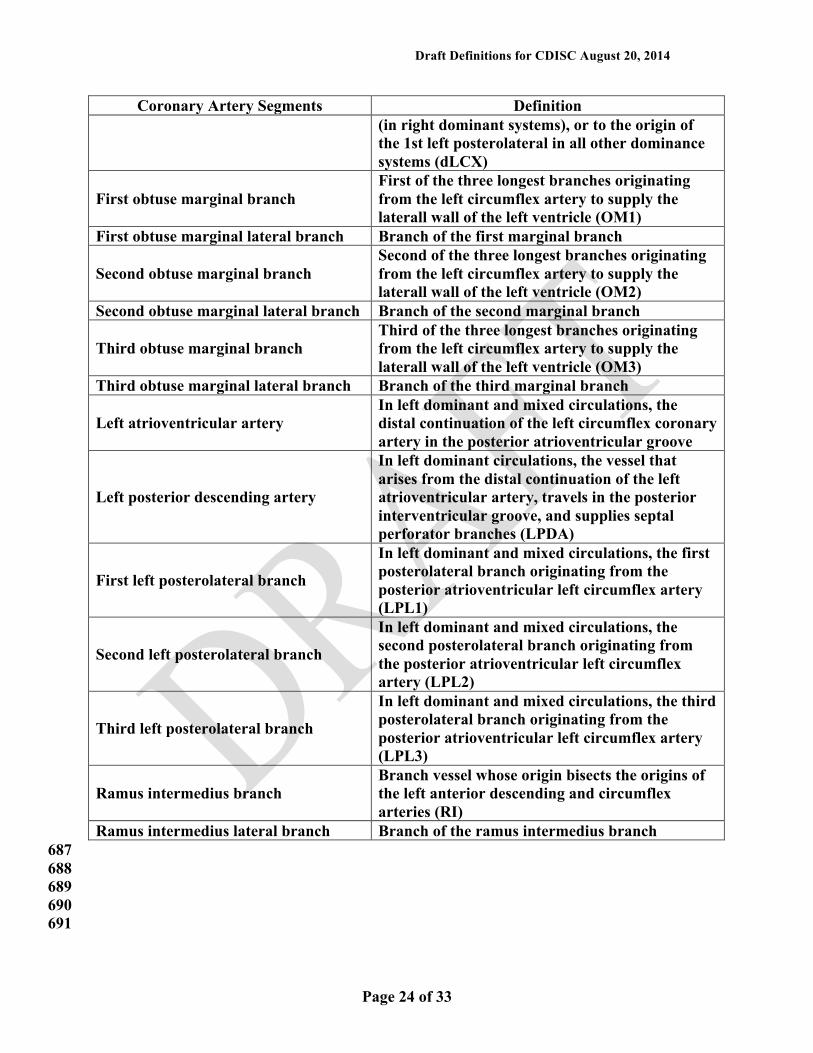
Coronary Artery Segments Definition (in right dominant systems), or to the origin of the 1st left posterolateral in all other dominance systems (dLCX)
First obtuse marginal branch First of the three longest branches originating from the left circumflex artery to supply the laterall wall of the left ventricle (OM1)
First obtuse marginal lateral branch Branch of the first marginal branch
Second obtuse marginal branch Second of the three longest branches originating from the left circumflex artery to supply the laterall wall of the left ventricle (OM2)
Second obtuse marginal lateral branch Branch of the second marginal branch
Third obtuse marginal branch Third of the three longest branches originating from the left circumflex artery to supply the laterall wall of the left ventricle (OM3)
Third obtuse marginal lateral branch Branch of the third marginal branch
Left atrioventricular artery In left dominant and mixed circulations, the distal continuation of the left circumflex coronary artery in the posterior atrioventricular groove
Left posterior descending artery
In left dominant circulations, the vessel that arises from the distal continuation of the left atrioventricular artery, travels in the posterior interventricular groove, and supplies septal perforator branches (LPDA)
First left posterolateral branch
In left dominant and mixed circulations, the first posterolateral branch originating from the posterior atrioventricular left circumflex artery (LPL1)
Second left posterolateral branch
In left dominant and mixed circulations, the second posterolateral branch originating from the posterior atrioventricular left circumflex artery (LPL2)
Third left posterolateral branch
In left dominant and mixed circulations, the third posterolateral branch originating from the posterior atrioventricular left circumflex artery (LPL3)
Ramus intermedius branch Branch vessel whose origin bisects the origins of the left anterior descending and circumflex arteries (RI)
Ramus intermedius lateral branch Branch of the ramus intermedius branch 687
688 689
690 691
Draft Definitions for CDISC August 20, 2014
Page 25 of 33
3. Dissection: 692 Based on the National Heart, Lung, and Blood Institute (NHLBI) Dissection 693 Classification System: 694 • Grade A: Minor radiolucencies within the lumen during contrast injection with no 695
persistence after dye clearance 696 • Grade B: Parallel tracts or double lumen separated by a radiolucent area during 697
contrast injection with no persistence after dye clearance 698 • Grade C: Extraluminal cap with persistence of contrast after dye clearance from the 699
lumen 700 • Grade D: Spiral luminal filling defect with delayed but complete distal flow 701 • Grade E: New persistent filling defect with delayed antegrade flow 702 • Grade F: Non-A-E types with total coronary occlusion and no distal antegrade flow 703 Note: Grade E and F dissections may represent thrombus 704
705 4. Late Loss: Minimum lumen diameter (MLD) assessed at follow-up angiography minus 706
the MLD assessed immediately after the index procedure. MLDs are measured by QCA. 707 708 5. Minimum Lumen Diameter (MLD): The mean minimum lumen diameter (typically 709
measured in-lesion, in-stent, and in-segment) derived from two orthogonal views by 710 QCA. 711
712 6. No Reflow: An acute reduction in coronary flow (TIMI grade 0-1) in the absence of 713
dissection, thrombus, spasm, or high-grade residual stenosis at the original target lesion. 714 715 7. Percent Diameter Stenosis (% DS): The value calculated as 100 x (1 – MLD/RVD) 716
using the mean values determined by QCA from two orthogonal views (when possible). 717 718 8. Reference Vessel Diameter (RVD): Defined as the average of normal segments within 719
10 mm proximal and 10 mm distal to the target lesion from two orthogonal views using 720 QCA. 721
722 723
Draft Definitions for CDISC August 20, 2014
Page 26 of 33
9. Restenosis: Re-narrowing of the vessel following the treatment of a prior stenosis 724 725
• Binary restenosis: A diameter stenosis of > 50% at the previously treated lesion site, 726 including the originally treated site plus the adjacent vascular segments 5 mm 727 proximal and 5 mm distal to the site. 728
729 • In-stent restenosis (ISR): A previously stented lesion with a > 50% diameter. 730
stenosis. 731 732
10. Thrombus (Angiographic): A discrete, mobile, intraluminal filling defect with defined 733 borders with or without associated contrast staining. 734
735 11. TIMI (Thrombolysis in Myocardial Infarction) Flow Grades: 736 737
• Grade 0 (no perfusion): There is no antegrade flow beyond the point of occlusion. 738 739 • Grade 1 (penetration without perfusion): The contrast material passes beyond the 740
area of obstruction but “hangs up” and fails to opacify the entire coronary bed distal 741 to the obstruction for the duration of the cineangiographic filming sequence. 742
743 • Grade 2 (partial perfusion): The contrast material passes across the obstruction and 744
opacifies the coronary bed distal to the obstruction. However, the rate of entry of 745 contrast material into the vessel distal to the obstruction or its rate of clearance from 746 the distal bed (or both) is perceptibly slower than its entry into or clearance from 747 comparable areas not perfused by the previously occluded vessel (e.g., the opposite 748 coronary artery or the coronary bed proximal to the obstruction). 749
750 • Grade 3 (complete perfusion): Antegrade flow into the bed distal to the obstruction 751
occurs as promptly as antegrade flow into the bed proximal to the obstruction and 752 clearance of contrast material from the involved bed is as rapid as from an uninvolved 753 bed in the same vessel or the opposite artery.. 754
755 12. Vessels 756
• Left main coronary artery (LMCA) 757 • Left anterior descending artery (LAD) with septal and diagonal branches 758 • Left circumflex artery (LCX) with obtuse marginal branches 759 • Ramus intermedius artery 760 • Right coronary artery (RCA) and any of its branches 761 • Posterior descending artery 762 • Saphenous vein bypass graft(s) 763 • Arterial bypass graft(s): Right internal mammary graft, left internal mammary graft, 764
radial artery graft, and gastroepiploic artery graft. 765 766
767 768 769
770
Draft Definitions for CDISC August 20, 2014
Page 27 of 33
CHAPTER 9. Definition of Peripheral Vascular Intervention 771 772 773 1. Peripheral Vascular Intervention (PVI): Peripheral vascular intervention2 is a catheter-774
based or open surgical procedure designed to improve arterial or venous blood flow or 775 otherwise modify or revise vascular conduits. Procedures may include, but are not limited to, 776 percutaneous transluminal balloon angioplasty, stent placement, thrombectomy, 777 embolectomy, atherectomy, dissection repair, aneurysm exclusion, treatment of dialysis 778 conduits, placement of various devices, intravascular thrombolysis or other 779 pharmacotherapies, and open surgical bypass or revision. 780
781 In general, the intention to perform percutaneous peripheral vascular intervention is denoted 782 by the insertion of a guide wire into a peripheral artery or vein. 783 784 The target vessel(s) and the type of revascularization procedure (e.g., surgical bypass, 785 thrombectomy, endarterectomy, percutaneous transluminal angioplasty, stent placement, 786 thromboembolectomy, and thrombolysis) should be specified and recorded. For the sake of 787 simplicity, this definition applies to the extracranial carotid artery and other non-cardiac 788 arteries and veins and excludes the intracranial vessels and lymphatics. 789 790
2. Procedural Success: In the case of percutaneous intervention for obstructive lesions, 791 procedural success is defined as the achievement of a satisfactory final residual diameter 792 stenosis by angiography at the end of the procedure (and without flow limiting dissection or 793 hemodynamically significant translesional pressure gradient). The specific parameter for 794 final percent residual stenosis is typically between < 30% and < 50%; selection of the 795 appropriate percentage may vary depending upon the specific intervention applied, the 796 vascular territory, and anticipated or desired therapeutic response. Procedural success also 797 implies absence of in-hospital major adverse events (e.g., death, stroke, myocardial 798 infarction, acute onset of limb ischemia, need for urgent/emergent vascular surgery, and 799 other procedure-specific major adverse events). The balloon inflation, stent placement, or 800 other therapeutic intervention may be preceded by use of adjunctive devices (e.g., 801 percutaneous mechanical thrombectomy, directional or rotational atherectomy, laser, and 802 chronic total occlusion crossing device), as predefined in the protocol. 803
804 3. Procedural Status: Non-Elective and Elective: 805
806 a. Non-Elective: Non-elective procedures include emergent and urgent procedures. A non-807
elective procedure is a procedure that is performed without delay, because there is 808 clinical consensus that the procedure should occur imminently. Non-elective procedures 809 imply a degree of instability of the patient, urgency of the medical condition, or 810 instability of the threatening lesion. 811
812
2 We note that peripheral vascular disease includes veins, arteries, and lymphatics. However, for simplicity,
this definition will focus on peripheral artery and venous interventions.
Draft Definitions for CDISC August 20, 2014
Page 28 of 33
• Emergent: A procedure that is performed immediately because of the acute nature 813 of the medical condition (e.g., acute limb ischemia, acute aortic dissection), and the 814 increased morbidity or mortality associated with a temporal delay in treatment. 815
816 • Urgent: An urgent procedure is one that is not an emergency but is required to be 817
performed on a timely basis (≤ 24 hrs) (e.g., a patient who has been stabilized 818 following initial treatment of acute limb ischemia, and there is clinical consensus that 819 a definitive procedure should occur within the next 24 hours). 820
821 b. Elective: An elective procedure is one that is scheduled and is performed on a patient 822
with stable disease, or in whom there is no urgency and/or increased morbidity or 823 mortality associated with a planned procedure. 824
825 4. Target Lesion: A target lesion is any vascular segment treated or attempted to be treated 826
during the trial procedure with the index device. The target lesion is the treated segment 827 starting 10 mm proximal and ending 10 mm distal to the index device or therapy (stent, 828 balloon, atherectomy catheter, or aortic stent-graft). 829
830 5. Target Vessel: A target vessel is any vessel (e.g., non-cardiac or non-intracranial) that 831
contains the target lesion treated with the study device. The target vessel includes the target 832 lesion as well as the entire length of native vessel upstream and downstream from the target 833 lesion, including side branches. For the arteries of the leg, the vasculature is divided into 3 834 vessel “levels:” aorto-iliac, femoral-popliteal, and tibial-crural. 835
836 6. Non-Target Lesion and Non-Target Lesion Revascularization: A lesion for which 837
revascularization is not attempted or one in which revascularization is performed using a 838 non-study device, respectively. 839
840 7. Non-Target Vessel and Non-Target Vessel Revascularization: A vessel for which 841
revascularization is not attempted or one in which revascularization is performed using a 842 non-study device, respectively. 843
844 8. Target Vessel, Non-Target Lesion and Target Vessel, Non-Target Lesion 845
Revascularization: Any lesion or revascularization of a lesion in the target vessel other than 846 the target lesion, respectively. 847
848 9. Target Lesion Revascularization (TLR): Target lesion revascularization is any repeat 849
intervention of the target lesion (including 10 mm proximal and 10 mm distal to the index 850 device, as target lesion is defined above) or surgical intervention/bypass of the target vessel 851 performed for restenosis or other complication involving the target lesion. In the assessment 852 of TLR, angiograms should be assessed by an angiographic core laboratory (if designated). 853 Angiograms (and core laboratory assessment thereof) and other source documentation should 854 be made available to the CEC for review upon request. 855
856 857

Draft Definitions for CDISC August 20, 2014
Page 29 of 33
10. Target Vessel Revascularization (TVR): Target vessel revascularization is any repeat 858 intervention or surgical bypass of any segment of the target vessel. In the assessment of 859 TVR, angiograms should be assessed by an angiographic core laboratory (if designated). 860 Angiograms (and core laboratory assessment thereof) and other source documentation should 861 be made available to the CEC for review upon request. 862 863
11. Clinically-Driven Target Lesion Revascularization: Clinically-driven target lesion 864 revascularization is defined as target lesion revascularization performed due to target lesion 865 diameter stenosis > 50% AND either evidence of clinical or functional ischemia (e.g. 866 recurrent/progressive intermittent claudication, critical limb ischemia) OR recurrence of the 867 clinical syndrome for which the initial procedure was performed. Clinically-driven target 868 lesion revascularization occurs in the absence of protocol-directed surveillance ultrasound or 869 angiography. 870
871 12. Vessel Patency: Vessel patency at a given time point will be determined by the absence of 872
clinically-driven target lesion revascularization and/or absence of recurrent target lesion 873 diameter stenosis > 50% by imaging (e.g., invasive angiography or most commonly, duplex 874 ultrasonography). If patency data are incorporated within the primary endpoint of a clinical 875 trial, the angiographic images or duplex ultrasonographic images should be assessed by 876 appropriate core laboratories and made available to the CEC for review upon request. 877
878 13. Restenosis: Re-narrowing of the artery following the treatment of a prior stenosis 879 880
• Binary restenosis: A diameter stenosis of > 50% at the previously treated lesion site, 881 including the originally treated site plus the adjacent vascular segments 10 mm proximal 882 and 10 mm distal to the site (or as otherwise defined by the protocol, as noted above). 883
884 • In-stent restenosis (ISR): A previously stented lesion that has > 50% diameter stenosis. 885
886
887
Draft Definitions for CDISC August 20, 2014
Page 30 of 33
CHAPTER 10. Definition of Stent Thrombosis 888 889 890 Stent Thrombosis: Timing 891 892 Stent thrombosis should be reported as a cumulative value over time and at the various 893 individual time points as specified below. Time 0 is defined as the time point after the guiding 894 catheter has been removed and the subject has left the cardiac catheterization laboratory. 895
896 Stent Thrombosis: Timing 897 Acute stent thrombosis1 0-24 hours post stent implantation Subacute stent thrombosis1 > 24 hours – 30 days post stent implantation Late stent thrombosis2 > 30 days – 1 year post stent implantation Very late stent thrombosis2 > 1 year post stent implantation 1Acute or subacute can also be replaced by the term early stent thrombosis. Early stent thrombosis (0-30 days) will be used herein.
2Includes “primary” as well as “secondary” late stent thrombosis; “secondary” late stent thrombosis is a stent thrombosis after a target lesion revascularization. 898 899 Stent Thrombosis: Categories 900 901 We propose three categories of evidence to define stent thrombosis, as follows: 902 903 1. Definite Stent Thrombosis 904
905 Definite stent thrombosis is considered to have occurred by either angiographic or 906 pathological confirmation: 907
908 a. Angiographic confirmation of stent thrombosis3 909
910 • The presence of a thrombus4 that originates in the stent or in the segment 5 mm 911
proximal or distal to the stent and presence of at least 1 of the following criteria 912 within a 48-hour time window: 913
914 o Acute onset of ischemic symptoms at rest 915
916 o New ischemic ECG changes that suggest acute ischemia 917 918 o Typical rise and fall in cardiac biomarkers (refer to definition of spontaneous MI) 919
3The incidental angiographic documentation of stent occlusion in the absence of clinical signs or symptoms is
not considered a confirmed stent thrombosis (silent occlusion). 4Intracoronary thrombus
Draft Definitions for CDISC August 20, 2014
Page 31 of 33
o Nonocclusive thrombus 920 Intracoronary thrombus is defined as a (spheric, ovoid, or irregular) noncalcified 921 filling defect or lucency surrounded by contrast material (on 3 sides or within a 922 coronary stenosis) seen in multiple projections, or persistence of contrast material 923 within the lumen, or a visible embolization of intraluminal material downstream 924
925 o Occlusive thrombus 926
TIMI 0 or TIMI 1 intrastent or proximal to a stent up to the most adjacent 927 proximal side branch or main branch (if originates from the side branch). 928
929 b. Pathological Confirmation of Stent Thrombosis 930
931 Evidence of recent thrombus within the stent determined at autopsy or via examination of 932 tissue retrieved following thrombectomy. 933
934 2. Probable Stent Thrombosis 935 936
Clinical definition of probable stent thrombosis is considered to have occurred after 937 intracoronary stenting in the following cases: 938 939 a. Any unexplained death within the first 30 days5 940 941 b. Irrespective of the time after the index procedure, any MI that is related to documented 942
acute ischemia in the territory of the implanted stent without angiographic confirmation 943 of stent thrombosis and in the absence of any other obvious cause 944
945 3. Possible Stent Thrombosis 946
947 Clinical definition of possible stent thrombosis is considered to have occurred with any 948 unexplained death from 30 days after intracoronary stenting until end of trial follow-up. 949
950
5For studies with ST-elevation MI population, one may consider the exclusion of unexplained death within 30 days as evidence of probable stent thrombosis
Draft Definitions for CDISC August 20, 2014
Page 32 of 33
References 951 952 1. ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non ST-953
Elevation Myocardial Infarction: Executive Summary. A Report of the American College of 954 Cardiology/American Heart Association Task Force on Practice Guidelines (Writing 955 Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable 956 Angina/Non ST-Elevation Myocardial Infarction): Developed in Collaboration with the 957 American College of Emergency Physicians, the Society for Cardiovascular Angiography 958 and Interventions, and the Society of Thoracic Surgeons: Endorsed by the American 959 Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic 960 Emergency Medicine, Circulation, 2007, 116:803-877. 961
962 2. 2012 ACCF/AHA Focused Update of the Guideline for the Management of Patients With 963
Unstable Angina/Non-ST-Elevation Myocardial Infarction (Updating the 2007 Guideline and 964 Replacing the 2011 Focused Update). A Report of the American College of Cardiology 965 Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll 966 Cardiol, 2012, 60(7):645-81. 967
968 3. 2009 Focused Update Incorporated Into the ACC/AHA 2005 Guidelines for the Diagnosis 969
and Management of Heart Failure in Adults. A Report of the American College of 970 Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, 971 J Am Coll Cardiol, 2009, 53(15):e1-90. 972
973 4. Campeau L, Grading of angina pectoris (letter), Circulation, 1976, 54:522-23. 974 975 5. Cutlip DE, S Windecker, R Mehran, A Boam, DJ Cohen, G-A van Es, PG Steg, M-A Morel, 976
L Mauri, P Vranckx, E McFadden, A Lansky, M Hamon, MW Krucoff, PW Serruys and on 977 behalf of the Academic Research Consortium. Clinical Endpoints in Coronary Stent Trials: 978 A Case for Standardized Definitions, Circulation, 2007, 115:2344-2351. 979
980 6. Easton JD, Saver JL, Albers GW, Alberts MJ, Chaturvedi S, Feldmann E, Hatsukami TS, 981
Higashida RT, Johnston SC, Kidwell CS, Lutsep HL, Miller E, Sacco RL. Definition and 982 Evaluation of Transient Ischemic Attack, A Scientific Statement for Healthcare Professionals 983 from the American Heart Association; American Stroke Association Stroke Council; Council 984 on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and 985 Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on 986 Peripheral Vascular Disease, Stroke, 2009 Jun; 40(6):2276-93. Epub 2009 May 7. Review. 987
988 7. ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008. 989
The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of 990 the European Society of Cardiology. Developed in collaboration with the Heart Failure 991 Association of the ESC (HFA) and endorsed by the European Society of Intensive Care 992 Medicine (ESICM), European Journal of Heart Failure, 2008, 10:933-989. 993
994 8. Hiatt WR, Goldstone J, Smith, Jr. SC, McDermott M, Moneta G, Oka R, Newman AB, 995
Pearce WH, and for Writing Group 1. Atherosclerotic Peripheral Vascular Disease 996 Symposium II: Nomenclature for Vascular Diseases, Circulation, 2008, 118:2826-2829. 997
998
Draft Definitions for CDISC August 20, 2014
Page 33 of 33
999 9. Thygesen, Kristian, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, and White HD on 1000
behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of 1001 Myocardial Infarction, Third Universal Definition of Myocardial Infarction. Circulation, 1002 2012, 126:2020-2035 (published online August 24, 2012). 1003
1004 10. Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, and White HD: the Writing 1005
Group on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition 1006 of Myocardial Infarction. Third Universal Definition of Myocardial Infarction. Expert 1007 Consensus Document. J Am Coll Cardiol, 2012, 60(16):1581-1598 (published online 1008 October 16, 2012). 1009
1010 11. Hunt SA, Abraham WT, Chin MH, et al. 2009 Focused Update Incorporated into the 1011
ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults. 1012 A Report of the American College of Cardiology Foundation/American Heart Association 1013 Task Force on Practice Guidelines Developed in Collaboration With the International Society 1014 for Heart and Lung Transplantation. J Am Coll Cardiol. 2009;53:e1-e90. 1015
1016 12. Jneid H, Anderson JL, Wright RS, et al. 2012 ACCF/AHA Focused Update of the Guideline 1017
for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial 1018 Infarction (Updating the 2007 Guideline and Replacing the 2011 Focused Update). A Report 1019 of the American College of Cardiology Foundation/American Heart Association Task Force 1020 on Practice Guidelines. J Am Coll Cardiol. 2012;60:645-81. 1021
1022 13. Cannon CP, Brindis RG, Chaitman BR, et al. 2013 ACCF/AHA Key Data Elements and 1023
Definitions for Measuring the Clinical Management and Outcomes of Patients with Acute 1024 Coronary Syndromes and Coronary Artery Disease. A Report of the American College of 1025 Cardiology Foundation/American Heart Association Task Force on Clinical Data Standards 1026 (Writing Committee to Develop Acute Coronary Syndromes and Coronary Artery Disease 1027 Clinical Data Standards). J Am Coll Cardiol. 2013;12:65-105. 1028
1029 14. Creager MA, Belkin M, Bluth EI, et al. 2012 ACCF/AHA/ACR/SCAI/SIR/STS/SVM/SVN/ 1030
SVS Key Data Elements and Definitions for Peripheral Atherosclerotic Vascular Disease. A 1031 Report of the American College of Cardioogy Foundation/American Heart Association Task 1032 Force on Clinical Data Standards (Writing Committee to Develop Clinical Data Standards for 1033 Peripheral Atherosclerotic Vascular Disease). J Am Coll Cardiol. 2012;59:294-357. 1034
1035 15. O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA Guideline for the 1036
Management of ST-Elevation Myocardial Infarction. A Report of the American College of 1037 Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J 1038 Am Coll Cardiol. 2013;61:e78-140. 1039
1040 16. Sacco RL, Kasner SE, Broderick JP, et al. An Updated Definition of Stroke for the 21st 1041
Century. A Statement for Healthcare Professionals from the American Heart 1042 Association/American Stroke Association. Stroke. 2013;44:2064-89. 1043
1044 17. Zannad F, Garcia AA, Anker SD, et al. Clinical Outcome Endpoints in Heart Failure Trials: 1045
a European Society of Cardiology Heart Failure Association Consensus Document. Eur J 1046 Heart Fail. 2013;15(10):1082-1094. 1047






















![PAYGo PERFORM KPI Kick-Off [FINAL] - GOGLA• KPI Technical Guide: definitions of selected key performance indicators • Taxonomy: standardized qualitatively categorizing different](https://img.pdfslide.us/doc/110x75/5f0de8d77e708231d43caea7/paygo-perform-kpi-kick-off-final-gogla-a-kpi-technical-guide-definitions.jpg)





