Embed Size (px)
Citation preview

34 I CARDIAC INTERVENTIONS TODAY I OCTOBER/NOVEMBER 2008
TECHNIQUES
Japanese operators are among the leading opera-
tors performing percutaneous coronary interven-
tion (PCI) for chronic total occlusion (CTO). The
reason for this is likely because Japanese operators
have been making continuous innovations and have
established new methodology in this field (eg, the
controlled antegrade and retrograde subintimal track-
ing [CART] technique). This article examines the stan-
dard Japanese techniques, including guidewire and
catheter selection.
CO RO N A RY A N G I O G R A P H Y F O R C TO P C I
To perform PCI for CTO, appropriate coronary
angiography (CAG) images must be taken. For exam-
ple, in a case of a CTO lesion in the right coronary
artery (RCA), angiograms focused on the occluded
portion must be taken. Generally, in cases of CTO in
the RCA, collaterals are often formed from the left
coronary artery (LCA). An angiography of the LCA
must consider the RCA as well as the LCA; otherwise,
a PCI for CTO cannot be performed (Figure 1).
Angiograms taken from various angles are also essen-
tial. Both the entrance and exit of the CTO must be
visualized on multiple planes, preferably perpendicu-
lar to each other. If possible, the CTO site should be
fixed in the center and visualized without panning
the table. Sometimes, certain “tricks” are necessary,
such as starting contralateral dye injection and wait-
ing until enough collateral flow is supplied before
taking angiograms by pressing the foot switch
(Figure 2).
CO R R E C T I N T E R P R E TAT I O N O F C AG
The next important step is to interpret the properly
acquired CAG images to confirm the entrance and exit
of the CTO and where the wire is to proceed between
these points. The occluded portion of a CTO lesion can-
not be visualized on CAG, but based on various pieces
of information, it is possible to anticipate the course of
the occluded vessel. Calcification and bridging collaterals
are good indicators to estimate the course of the vessel.
In many cases, the right channel is found in the occlud-
Standard Japanese CTO Technique
An step-by-step analysis of angiographic views, selection, and strategies for guidewire selection and use.
BY YASUSHI ASAKURA, MD
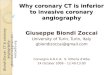
Figure 1. A case of CTO of the RCA (A). Angiography of the LCA in a case of CTO of the RCA (B). Due to panning to see the distal
side of the LCA, the distal side of the RCA cannot be observed. Angiography focused on the RCA.The exit of the CTO (arrow) is
clearly visible (C).
A B C

OCTOBER/NOVEMBER 2008 I CARDIAC INTERVENTIONS TODAY I 35
TECHNIQUES
ed portion. Often, microchannels are found in the vicini-
ty of the entrance and exit of the CTO. These channels
have to be differentiated from a bridging collateral. If a
side branch is found to originate from the channel, its
presence is a sign that the channel is likely to be the true
lumen (Figure 3).
In some cases, the true lumen exists like an island in
a river (Figure 2). Such an island does not necessarily
have a certain length. As shown in Figure 4, it may
merely be a remnant confluence area of two side
branches.
It goes without saying that PCI procedures per-
formed after obtaining such pieces of information
and those without them differ in their success rates.
Therefore, we perform thorough reading of the CAG
images before operation. First, we observe the
images repeatedly at normal speed. Then, we
observe all the frames one by one. We spend at least
more than half an hour—in many cases about 1
hour—for interpretation of CAG images.
CO N T R A L AT E R A L I N J E C T I O N
One difference among Japanese operators and
European and American operators is whether or not
to use contralateral angiography. Japanese operators
always perform contralateral angiography if it is nec-
essary to observe the distal side of the CTO. On the
contrary, I have experienced cases in Europe and the
US where PCI is performed without contralateral dye
injection (Figure 5). Performing a PCI procedure with-
out contralateral dye injection may result not only in
decreased success rates but may lead to serious com-
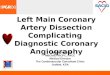
A B C
Figure 2. A case of CTO close to the ostium of the RCA (A).The exit of the CTO is located at the bifurcation of the posterolateral
branch and posterior descending branch (B). Starting dye injection before taking angiograms makes it possible to visualize the
mid-RCA via the right ventricular branch (C).
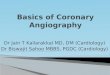
A B
Figure 3. CTO lesion in the proximal LAD (A).The channel indicated by the white arrows had the appearance of a bridging col-
lateral, and on the right anterior oblique caudal view, the true channel seemed to exist on the upper side, closer to the epicardi-
um (B). However, with a septal branch originating from this channel, it was likely to be the true lumen. In the present case, the
wire was first introduced to the epicardial side without success. After reading of the CAG for a second time, a soft wire was
advanced into this microchannel and revascularization was achieved successfully.

36 I CARDIAC INTERVENTIONS TODAY I OCTOBER/NOVEMBER 2008
TECHNIQUES
plications. The operators who will continue advancing
the balloon catheter or other devices would not
notice a perforation with the wire, and this would
result in massive bleeding and easily cause tampon-
ade.
Even with a contralateral angiography, it is some-
times not possible to obtain a sufficient view of the
distal side of the CTO. In such cases, it is necessary to
find a specific collateral channel. The most common
pattern is the conus branch connecting the left ante-
rior descending artery (LAD) and the RCA. Figure 6
shows a case of CTO at the ostium of the LAD. The
LAD is supplied with good collateral flow from the
RCA, but the exit of the CTO is not visualized. In this
case, dye was injected into the proximal LAD via the
conus branch, and to visualize the exit of the CTO,
selective angiography of the conus branch is neces-
sary. Sometimes, the distal part of the CTO in the
RCA is visualized via the conus branch (Figure 7). The
conus branch can originate from a different orifice
than the RCA, and in an angiography of the RCA, cau-
tion must be used not to overlook the collateral
channel. For angiography of this separate conus, an
internal mammary artery catheter is often appropri-
ate. In rare cases, there is a collateral route through
the atrial branch supplying the distal part of the RCA
(Figure 8). In any of these cases, it is difficult to hold
the catheter in place, and it is useful to have the
guidewire in place or to use a microcatheter for
angiography. If a microcatheter is used, as little as <1
mL of the contrast media is required. In many cases,
these collateral routes can be clearly visualized by the
multislice CT scan gaining increased recognition for
PCI for CTO in recent years.
C H O I C E A N D H A N D L I N G O F T H E
G U I D E W I R E
Decisive for success or failure of CTO PCI is whether
the guidewire can pass through the CTO lesion.
Therefore, the question of choice and maneuvering a
guidewire is of extreme importance. However, there is
no particular standard for selecting a guidewire. There
is no such guidewire with which any CTO lesion can be
crossed. Therefore, when choosing a guidewire to use,
the operator should use the one that he or she is most
used to. The X-treme (Asahi Intecc, Nagoya, Japan) is
the guidewire I use first in most cases of CTO. It does
not matter if you cannot see microchannels on angiog-
raphy because pathologically, CTO lesions have
microchannels in the occluded segment. The tapered-
tip X-treme is very good at tracing these channels. If a
microchannel is seen on angiography, the common
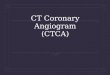
A B C D
A B C D
E
Figure 4. CTO at the ostial LAD (A).The exit of CTO is indicated by the arrow (B).The arrow indicates the point of confluence of
the RV branch and septal branch (C).The point of confluence was considered to be the LAD trunk so that the wire was
advanced aiming at this point (D).The wire crossed the lesion successfully (E).
Figure 5. CTO of the RCA (A). Although the RCA distal to the CTO lesion was not visualized, no contralateral dye injection was
performed. Unsuccessful PCI was associated with wire perforation and formation of a large hematoma (arrow) (B). Later, a sec-
ond attempt of PCI was made with contralateral dye injection (C). Revascularization was achieved successfully (D).

.014-inch wire with a plastic jacket is often most suited.
If the lesion cannot be crossed using such lubricous
wires, one should not hesitate to go on to the next
step. Once having entered the false lumen, it is unlikely
to find the true lumen with these wires. There is even
the risk of enlarging the subintimal space.
As the next choice of guidewire, I recommend the
Miracle series (Abbott Vascular, Santa Clara, CA).
When manipulating, never rotate the guidewire exces-
sively. It is recommended to repeat advancing and
retrieving the wire little by little. When retrieving the
guidewire, it is important to feel the magnitude of fric-
tion with your fingers. Depending on the lesion, nei-
ther too much nor too little friction is good.
Manipulation of the guidewire at the exit of the CTO
is also critical. Just before the guidewire penetrates the
distal end of the CTO, angiography from several angles
must be taken (Figure 9). If possible, this should be
done also immediately after perforation is completed.
The success rate of PCI depends very much on
whether such extra efforts are made. However, many
operators, including Japanese operators, fail to make
these efforts. In my view, excellent operators have the
following points in common with regard to their
choice and use of guidewire. First, they manipulate the
wires gently. Second, they are patient with the
guidewire once the choice is made and do not give up
easily. In contrast, operators with low success rates
decide too early to step up to the next wire, and I often
encounter cases in which a hard wire has entered the
false lumen. The third point is that these operators
know when to use the Asahi Confianza guidewire fami-
ly (Abbott Vascular). Japanese top operators are careful
about using these wires. Particularly in cases of a very
long CTO lesion, or if there are bends in the occluded
portion, a wire of the Confianza family should not be
used too early. The Miracle series (Abbott Vascular)
is more suited to cope with these types of lesions. It
is important to know the peculiarities of each wire
and use them at the most appropriate occasions.
I N T R AVA S C U L A R U LT R A S O U N D
Intravascular ultrasound (IVUS) is more frequently used
in Japan than in Europe and the US and in cases other
Figure 6. The LAD is occluded at the ostium shown with the arrow (spider view) (A).The LAD distal to the CTO lesion received
good collateral flow from the RCA (RAO view), however, the LAD proximal to the CTO showed a to-and-fro flow, and the exit of
the CTO was not visible (B). Selective angiography of the conus branch using a microcatheter clearly showed the exit of the
CTO (arrow) (spider view) (C).The wire was manipulated under selective angiography of the conus branch (D).
Figure 7. A case of CTO lesion in the proximal RCA (A).The exit of the CTO is near the bifurcation of posterolateral and posterior
descending branch (arrow) (B). Selective angiography of the conus branch having a different orifice than that of the RCA shows
the RCA trunk (arrow) (C). A microcatheter inserted in a diagnostic 6-F internal mammary artery catheter is used for angiogra-
phy of the conus branch. Final angiogram (D).
A B C D
A B C D
OCTOBER/NOVEMBER 2008 I CARDIAC INTERVENTIONS TODAY I 37
TECHNIQUES

38 I CARDIAC INTERVENTIONS TODAY I OCTOBER/NOVEMBER 2008
TECHNIQUES
than that of CTO. On a routine basis, we use both angiog-
raphy and IVUS to verify the PCI procedure that we have
performed. In cases of CTO treated with PCI, in particular,
IVUS shows us where and how the guidewire has actually
crossed the lesion. It also shows whether a false lumen
was created. Accumulation of such experience improves
our expertise in manipulation of guidewires.
Being familiar with the everyday use of IVUS makes our
technical wizardry possible to find the entrance to the
CTO with IVUS or to lead the guidewire that entered the
false lumen into the true lumen by IVUS-guided wiring.
M E D I C A L E CO N O M I C S A N D
S O C I A L B AC KG R O U N D
In Japan, PCI for CTO is performed more frequently
than in Europe and the US for other than scientific
reasons. The medical economic situation in Japan is
different from that of Europe and the US. The differ-
ence in insurance systems, in particular, is an impor-
tant factor. In many European countries and the US,
the payment of costs for PCI is made under the
prospective payment system in which the payment
amount for a particular medical service is predeter-
mined and fixed from the beginning. This means that
it is more profitable for the hospital if it performs PCI
procedures with as little device and contrasting agents
as possible. In many countries, doctors are paid more
for the more cases they have in their experience.
Under these circumstances, both hospitals and doc-
tors are happier if they treat a larger number of easier
cases. Difficult cases of CTO that would require longer
hours and more devices for PCI procedures are not
Figure 9. CTO in the proximal LAD (A). The
lesion was of little difficulty because the
length of the occlusion was short and without
bending and calcification. Before the wire
penetrates the exit of the CTO, it is important
to confirm whether the direction of the wire is
correct. In this case, the tip of the wire was
directed too downward in the right anterior
oblique cranial view (left) and too much to the left on the left anterior oblique cranial view (right) (B). Advancing the wire
without correcting the direction would have resulted in entering into the false lumen. The tip of the wire was directed into
the right position on multiple planes and confirmed on cine angiography (C). After penetration of the exit of the CTO, the
right position is confirmed on cine angiography (D). The wire must always be advanced with utmost caution. Final
angiogram (E).
Figure 8. CTO lesion in the proximal RCA (A).The RCA distal to the lesion was not visualized at all with angiography of the LCA
(B).The RCA was clearly visualized by selective angiography of the atrial branch (C). Final angiogram (D).
A
A
D E
B C
B C D

welcome. In Japan, on the contrary, payment for med-
ical services is made on a fee-for-service basis, which
means that the insurance will reimburse all costs for
any device used, and the difference between the
amount reimbursed by the insurance and the actual
amount paid becomes the profit of the hospital.
Furthermore, Japanese doctors are paid fixed salaries
so that the number of PCIs they perform is not reflect-
ed on the amount they receive. In other words, their
income and profit for the hospital do not suffer from
longer hours spent for one case of PCI. This means, in
Japan, the environment is friendlier if you want to use
PCI to treat patients with CTO.
The climate surrounding bypass surgery is also a fac-
tor leading to increased use of PCI for CTO. Although
the success rate of bypass surgery in Japan has
improved, until recently it was not satisfactory; a limit-
ed number of surgeons were achieving good results.
Under these circumstances, before the introduction of
drug-eluting stents, PCI for complicated lesions was
preferred over bypass surgery. Although bypass surgery
has been widely accepted by the general public in
Europe and the US, many Japanese people still shy
away from surgical operations and would rather avoid
them. These social factors lead to increased use of PCI
for CTO in Japan.
CO N C L U S I O N
PCI for CTO is employed more intensively in Japan
than in Europe and the US. While reasons of medical
economics and social background certainly play a role
in this development, we owe this to the top Japanese
operators, although limited in number, who have
achieved high success rates of PCI for CTO. The most
important factors leading to the high success rates are
their efforts in careful interpretation of CAG images
that are taken appropriately before the operation, gen-
tle manipulation of the guidewire and avoidance of
stepping up to other guidewires too easily, and their
daily attitude to never give up and do their best to
overcome the challenges they face. ■
Yasushi Asakura, MD, is Co-Director of
Cardiovascular Medicine, Toyohashi Heart Center in
Japan. He has disclosed that he holds no financial inter-
est in any product or manufacturer mentioned herein.
Dr. Asakura may be reached at +81-532-37-3377;
TECHNIQUES