Embed Size (px)
Citation preview

Standard 4:Medication Safety
Graham Bedford, Margaret Duguid
Accrediting Agencies Surveyor Workshop, 11 July 2012

Why have a standard about medication safety?
Medications are the most prevalent health therapy in Australia
Estimated 1.5million adverse medicine events annually, resulting in at least 400,000 GP visits and 140,000 hospital admissions1
Adverse medicines events associated with:2 • 38% of readmissions to hospital
• 33% ED attendances
Acute care medication errors:• 2 – 5% of drug charts contain prescribing errors3
• 5 – 18% of doses medicines administered in error3
• 18% of IV infusions administered incorrectly (>75% rate errors)4
Medication errors a major cause of patient harm
Errors are preventable

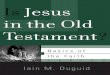
Dispensing11%
Prescribing
39%
Administering
38%
52% of prescribing errors reach the patient - Pharmacists and nurses prevent errors
Transcription
12%
Only 2% of administration errors intercepted.
Why have a standard about medication safety?
Where do errors occur ? 5

Causes of medication errors
Systems failures• Environment
- frequent interruptions – slips, lapses• Insufficient information
• Patient information, medicines information• Poorly written medication orders
• Poor design of medication forms, electronic systems
• Look-alike sound-alike names
• Similar packaging
• Poor medicines storage
Poor teamwork, communication with colleagues, patients
Lack of knowledge

Standard 4 – Medication Safety
The Medication Safety Standard describes the elements of a safe medication management system.
It requires hospitals to have in place strategies and systems known to reduce the risk of common causes of medication error.
• standardisation and systemisation of processes
• improving clinical workforce and clinician-patient communication
• using technology to support information recording and transfer
• providing better access to patient information and clinical decision support at the point of care.

Standard 4 – Medication Safety
Clinical leaders and senior managers of a health service organisation implement systems to reduce the occurrence of medication incidents, and improve the safety and quality of medicine use. Clinicians and other members of the workforce use the systems to safely manage medicines.
Two overarching Standards:• Standard 1: Governance for Safety and Quality
• Standard 2: Partnering with Consumers

Five criteria (Part 1)
1. Governance and systems for medication safety• Health service organisations have mechanisms for the safe
prescribing, dispensing, supplying, administering, storing, manufacturing, compounding and monitoring of the effects of medicines.
2. Documentation of patient information• The clinical workforce accurately records a patient’s
medication history and this history is available throughout the episode of care.
3. Medication management processes• The clinical workforce is supported for the prescribing,
dispensing, supplying, administering, storing, manufacturing, compounding and monitoring of medicines.

Five criteria (Part 2)
4. Continuity of medication management• The clinician provides a complete list of a patient’s medicines
to the receiving clinician and patient when handing over care or changing medicines.
5. Communicating with patients and carers• The clinical workforce informs patients about their options,
risks and responsibilities for an agreed medication management plan.

1. Governance and systems for med safety
4.1:Developing and implementing governance arrangements and organisation policies, procedures and/or protocols for medication safety, which are consistent with national and jurisdictional legislative requirements, policies and guidelines.
Why?• Systems for safe and high quality medications need
organisational support and executive and clinical leadership to be successful
• Robust clinical governance frameworks and processes for evaluation, audit and feedback are important for the improvement of medication management systems.

1. Governance and systems for med safety
4.1:Developing and implementing governance arrangements and organisation policies, procedures and/or protocols for medication safety, which are consistent with national and jurisdictional legislative requirements, policies and guidelines.
What?
Identify suitable individual / group / committee to take responsibility for governance of medication safety system (4.1.1)
• Drug and Therapeutics, Management Committee
• Reporting to safety and quality governance, executive
• Terms of reference could include:
monitoring the safety and quality of medicines use in the facility
conducting interventions to improve the safety and quality
managing adverse drug reactions and medication incidents
establishing a medication safety risk register
informing staff about medicines use issues, policies etc Consumer

1. Governance and systems for med safety
4.1:Developing and implementing governance arrangements (cónt’d)
What?• Incorporate medication safety into strategic and
operational plans, safety and quality risk registers (4.1.1)
• Monitor the impact of interventions
• Training programs for staff
Medication safety risks, strategies to reduce the risks
Staff attendance at training
Completing NIMC on line learning module
Completion of NPS medication safetymodules (in progress)
.

1. Governance and systems for med safety
4.1:Developing and implementing governance arrangements and organisation policies, procedures and/or protocols (cont’d)
What?• Develop and implement medication policies and
procedures across the organisation (4.1.2):• Consistent with legislative requirements• Readily accessible, version control with review date• Examples:- list of medicines approved for use in the facility (formulary)
- prescribing policies and guidelines
- procedures for administering medicines, independent checking
- procedure for checking patient identification
- use of the NIMC and ancillary charts
• Audits of compliance

1. Governance and systems for med safety
Source. APAC Guiding principles to achieve continuity of medication management 2005 6

1. Governance and systems for med safety

1. Governance and systems for med safety
4.2: Undertaking a regular, comprehensive assessment of medication use systems to identify risks to patient safety and implementing system changes to address the identified risks
Why?• Evaluation of medication management systems to identify
areas of risk, determine changes required and prioritise areas for improvement
• Ongoing monitoring needed to track changes over time and ensure that systems operate effectively

1. Governance and systems for med safety
4.2: Undertaking a regular, comprehensive assessment of medication use systems to identify risks to patient safety and implementing system changes to address the identified risks
What?• Adopt, or develop, and implement processes for assessing the
safety of the medication system (4.2.1)• Use a structured tool e.g. Medication Safety Self
Assessment7
- Multidisciplinary team- Every three years
• NIMC national audit• Failure Modes Effects Analysis

1. Governance and systems for med safety
4.2: Undertaking a regular, comprehensive assessment of medication use systems to identify risks to patient safety and implementing system changes to address the identified risks
What?• Respond to assessment findings to improve performance
(4.2.2)• Action plan or risk register with actions• Quality improvements implemented and evaluated
- Audits- Indicators e.g. Indicators for Quality Use of Medicines in
Australian Hospitals 7, State performance measures• Communication with workforce

1. Governance and systems for med safety
4.3: Authorising the relevant clinical workforce to prescribe, dispense and administer medications
Why?• To ensure that only staff with the competence and
authority to do so can prescribe, dispense and administer medicines
• Staff work within their scope of practice

1. Governance and systems for med safety
4.3: Authorising the relevant clinical workforce to prescribe, dispense and administer medications
What?• Develop a system to:
• identify areas where specific authorization is required to prescribe, dispense or administer medicines; and
• verify and maintain register/log of individual clinicians with qualifications and competencies(4.3.1)
• Review the use of the system. Identify if system breached (4.3.2)
• Identify actions to strengthen the system, address any breaches (4.3.3)

1. Governance and systems for med safety
4.4: Using a robust organisation-wide system of reporting, investigating and managing change to respond to medication incidents
Why?• Medication incidents are the second most commonly
reported incidents in Australian hospital incident monitoring systems
• To learn about the safety of the medication management process by reviewing incident reports, analysing and investigating incidents causing, or with the potential to cause, patient harm.
See also Standard 1.14

1. Governance and systems for med safety
4.4: Using a robust organisation-wide system of reporting, investigating and managing change to respond to medication incidents
What?
Implement a mechanism for staff to report medication incidents and for incidents to be analysed, investigated and reported to the medication safety governance group (4.4.1)
Review reports to identify trends, causes (4.4.1)• Involve clinical staff, medication sub-committee
Identify actions to reduce risk of recurrence (4.4.2)• Medication safety risk register with actions
• Safety and/or quality improvement plan
• Report to quality/patient safety committee
• Feedback to staff

1. Governance and systems for med safety
4.5: Undertaking quality improvement activities to enhance the safety of medicines use
Why?• To reduce harm to patients from known risks by
implementing and measuring the effect of quality improvement activities outlined in the medication safety quality improvement plan, risk register.
• These activities may include actions recommended to address risks identified from:
• Medication incident management system, RCA reports,• State, national or international medication safety notices/alerts, • Medication Safety Self Assessments• NIMC audit.

1. Governance and systems for med safety
4.5: Undertaking quality improvement activities to enhance the safety of medicines use
What?• Assess the performance of the medication management
system and evaluate effectiveness of changes (4.5.1): • Indicators e.g. Indicators for Quality Use of Medicines, state
performance measures• IHI Global Trigger Tool (identify adverse medicines events and areas
for improvement in the medication management system)• Auditing implementation of recommendations, safety alerts
- Recommendations for labelling of injectable fluids, lines and medicines
- National alerts e.g. potassium, vincristine alerts- State medication safety alerts

Prescribing errors – unclear, incorrect ordersAdministration documentationPharmacists’ documentation
1. Governance and systems for med safety

1. Governance and systems for med safety
4.5: Undertaking quality improvement activities to enhance the safety of medicines use
What?• Use information from 4.5.1 to identify further improvement activities
required to increase the safety and effectiveness of medicines use (4.5.2)
• Implement recommendations/alerts• Standardisation of work practices and products:
- Use pre-mixed solutions or preloaded syringes for injectable high risk medicines
- Standardise dosing protocols, medication checking procedures- Implement policies, procedures and workforce training to support
standardisation• Use infusion pumps with IV safety software (“smart pump” technology) and
drug libraries • Implement oral dispensers for oral liquid medicines

1. Governance and systems for med safety

2. Documentation of patient information
The clinical workforce accurately records a patient’s medication history and this history is available throughout the episode of care

2. Documentation of patient information
4.6: The clinical workforce taking an accurate medication history when a patient presents to a health service organisation, or as early as possible in the episode of care, which is then available at the point of care
Why?• The medication history is used as the basis for
therapeutic decision making, for ensuring continuity of regular medicines while a patient is in hospital and to identify adverse medicines events.
• Medication histories are often incomplete (10 – 67% have errors) and a cause of error and harm 9.

2. Documentation of patient information
4.6: The clinical workforce taking an accurate medication history when a patient presents to a health service organisation, or as early as possible in the episode of care, which is then available at the point of care
What?• Clinicians document a “Best Possible Medication History”
by interviewing patient/carer and verifying history with at least one other source. (4.6.1)
• Clinicians trained in taking a BPMH
• Standard form with prompts to elicit history (manual/electronic)
e.g. National Medication Management Plan or equivalent

2. Documentation of patient information
Keep the MMP together with the current NIMC Electronic system allows history to be viewed when prescribing
Clinicians can access the medication historyand clinical information required for safe prescribing at the point of prescribing (4.6.2)

Medication Management Plan supports workforce :
Taking a complete and accurate medication history (BPMH) (4.6.1)
Documenting ADRs on admission, if ADR occurs during episode of care (4.7.1)
Reconciling discrepancies between history and medication orders (4.8.1)
2. Documentation of patient information

2. Documentation of patient information
4.7: The clinical workforce documenting the patient’s previously known adverse drug reactions on initial presentation and updating this if an adverse reaction to a medicine occurs during the episode of care
Why?• Prevent avoidable harm from administration of a
medicines to which the patient has a known allergy or adverse reaction
• Communicate complete allergy/adverse drug reaction history to next care provider
• Contribute to post marketing surveillance of medicines

2. Documentation of patient information
4.7: The clinical workforce documenting the patient’s previously known adverse drug reactions on initial presentation and updating this if an adverse reaction to a medicine occurs during the episode of care
What?• Clinicians obtain and document a history of allergies and
adverse drug reactions (ADRs) when patients are admitted (4.7.1)
• Reduce risk of adverse reactions (4.7.2) by:• Recording information on the medication chart (NIMC) or in
electronic record - information available when medicines are prescribed, dispensed or administered
• Updating clinical record when ADR experienced during episode of care
• Informing GP and patient in discharge documentation• Monitoring documentation through audits, indicators (Indicator 3.2
Indicators for QUM in Australian Hospitals)

2. Documentation of patient information
4.7: The clinical workforce documenting the patient’s previously known adverse drug reactions (cont’d)
What?• System encourages and supports clinicians to report
adverse reactions:• Within in organisation for consideration by the Medication
Safety Governance Groupo Review ADRs reported and feedback information to staff in
medication safety or drug bulletins, at staff in-service session, grand rounds
• To Therapeutic Goods Administration (4.7.3)- Facility to report ADRs to TGA online - Number of ADRs reported to TGA

2. Documentation of patient information
4.8: The clinical workforce reviewing the patient’s current medication orders against their medication history and prescriber’s medication plan, and reconciling any discrepancies (Developmental)
Why?• Studies show that 30 – 70% patients admitted to hospitals
have ≥ 1 discrepancy between medicines taken at home and medicines ordered on admission 10
• The process of reconciling medicines ordered with the medication history (BPMH) reduces by >50% the errors and adverse events that occur when care is transferred e.g. when patient admitted, transferred internally or discharged

2. Documentation of patient information
4.8: The clinical workforce reconciling discrepancies between patient’s current medication orders and medication history
What?• Implement a formal structured process to ensure all patients admitted
to the health service receive accurate and timely medication reconciliation at admission, transfer of care and on discharge. (4.8.1)
• Procedures assigning responsibilities• Training staff• Using a standard form to document medicines reconciled
- National Medication Management Plan, equiv or e-version- NIMC Medicines taken prior to presentation section
• Prioritise patients >65 years, multiple medicines/morbidities, high risk medicines if resources limited
• Audits of rate and quality of reconciliation

37
. . .
Medication Management Plan+ implementation resources
MATCH UP Medicines Resources
2. Documentation of patient information
2. Documentation of patient information

3. Medication management processes
The clinical workforce is supported for the prescribing, administering, storing, manufacturing, compounding and monitoring of medicines

3. Medication management processes
2.9: Ensuring that current and accurate medicines information and decision support tools are readily available to the clinical workforce when making clinical decisions related to medicines use
Why?• Lack of knowledge about medicines, lack of access to up
to date protocols/guidelines are factors known to contribute to medication errors and harm.
• The availability of decision support tools when medicines are prescribed, dispensed and administered improves the safety and quality of medicines use.

3. Medication management processes
4.9: Ensuring that current and accurate medicines information and decision support tools are readily available (cont’d)
What?• Implement and maintain up-to-date medicines information
resources and decision support tools (manual or electronic) that are accessible to staff in clinical areas (at point of care) (4.9.1)
• formulary information, prescribing requirements, approval systems• reference texts• policies, protocols and guidelines• dosing calculators• drug interaction databases• guidelines for safe administration of specific medicines (eg administering
medicines via enteral tubes)• antibiotic approval systems

Hospital protocols, guidelines
3. Medication management processes
SHPA Australian Injectable Drugs HandbookSHPA Don’t Rush to Crush Handbook

3. Medication management processes
4.9: Ensuring that current and accurate medicines information and decision support tools are readily available (cont’d)
What?• Regular review of the use and content of clinical information and
decision support tools, to ensure that resources are current, and are endorsed for use within the organisation (4.9.2)
• Drug & Therapeutics Committee minutes/documentation• Risk assessment of drug information domain in MSSA
• Take action to improve clinical information and decision support tools where a need is identified based on review (4.9.3)
• Drug & Therapeutics Committee minutes• Examples of improvements

3. Medication management processes
4.10: Ensuring that medicines are distributed and stored securely, safely and in accordance with the manufacturer’s directions, legislation, jurisdictional orders and operational directives
Why?• Product integrity is maintained, medicines stored safely,
and waste minimised
• Distribution systems are responsive to clinical demand in order for medicines to be available for patient care in a timely manner.

3. Medication management processes
4.10: Ensuring that medicines are distributed and stored securely, safely (cont’d)
What?• Regular review and risk assessment of medicines storage
and distribution across the organisation.(4.10.1)
• As part of overall self assessment• Audit against policies, procedures• Observation audits and “walk arounds”• Review medication incidents

3. Medication management processes
4.10: Ensuring that medicines are distributed and stored securely, safely (Cont’d)
What?• Actions to reduce risks (including confusion with look
alike sound alike names) (4.10.2)• Policies and procedures• Safe handling and disposal of S8 medicines, cytotoxic products
and hazardous substances• Use of bar code scanners (dispensing, distribution)• Physical separation of products (e.g. look-alike, sound-alike
products) • Use of Tall Man lettering (e-systems, infusion pump libraries,
shelving, packaging)• Purchasing for safety• Safer distribution systems• Staff communication, alerts,
bulletins

3. Medication management processes
4.10: Ensuring that medicines are distributed and stored securely, safely (cont’d)
What?• Temperature sensitive medicines are monitored and integrity of
temperature-sensitive medicines maintained (4.10.3)• Temperatures measured, recorded, reviewed
• Workforce disposes of unused, unwanted or expired medicines, in accordance with legislative and jurisdictional requirements (4.10.4)
• S8 medicines audits• Disposal of cytotoxic products and hazardous substances (WHS
issues)• Monitoring disposal of unused, unwanted or expired medicines
(4.10.5)• Compliance with policy for disposal• Wastage

3. Medication management processes
4.11: Identifying high risk medicines in the organisation and ensuring they are stored, prescribed, dispensed and administered safely
High risk medicines - PINCH (Potassium, Insulin, Narcotics(S8s),Chemotherapy, Heparin (anticoagulants)
What? • Undertake an assessment of how high risk medicines are
managed within the organisation (4.11.1)• audits• incident analysis• risk assessment tools• drug usage evaluation programs• collaborative projects• benchmarking activities.

3. Medication management processes
4.11: Identifying high risk medicines in the organisation and ensuring they are stored, prescribed, dispensed and administered safely

Audits of compliance
3. Medication management processes

3. Medication management processes
4.11: Identifying high risk medicines in the organisation and ensuring they are stored, prescribed, dispensed and administered safely
What?• Put systems in place to minimise the risk of error (4.11.2)
• List of high risk medicines available to staff• Policies, procedures and protocols • Guidelines for prescribing, dispensing, administering and
monitoring specific high risk medicines such as anticoagulants, chemotherapy, opioids, insulin
• Pre-loaded infusions potassium, heparin• Training on awareness of high risk meds• Implement safety alerts on high risk medicines• Monitor improvement activities

4. Continuity of medication management
4.12: Ensuring a current comprehensive list of medicines, and the reason(s) for any change, is provided to the receiving clinician and the patient during any clinical handovers
Why?• 60% of patients have ≥ 3 changes during their hospital
stay 11
• Adverse drug events occur in up to 20% after discharge 11
• Patients with ≥ 1 medicine left off their discharge summary are 2.3 times more likely to be readmitted 12
• Providing an accurate list of current medicines at handover decreases medication errors and adverse events

4. Continuity of medication management
4.12: Ensuring a current comprehensive list of medicines, and the reason(s) for any change, is provided to the receiving clinician and the patient during any clinical handovers
What?• Implement and maintain a system that supports
clinicians to generate accurate and comprehensive medicines lists and explanations for changes when transferring care (4.12.1)
• Policies and procedures for medicines handover• Process of reconciling medicines list with medication history
(BPMH), discharge medicines dispensed and current medication orders (on medication chart)
• Audit of discharge summaries that include medicines list, reasons for any changes

4. Continuity of medication management
4.12: Ensuring a current comprehensive list of medicines, and the reason(s) for any change, is provided to the receiving clinician and the patient during any clinical handovers
What?• List of medicines to be continued on discharge along
with explanations of changes provided to:• Patient / carer (with counselling)(4.12.2)
- Audit clinical records (pharmacy)• Receiving clinician (4.12.3)
- Audit of discharge summaries that include medicines list, reasons for any changes
- Use of MMP and NIMC at internal transfer

4. Continuity of medication management
4.12: Ensuring a current comprehensive list of medicines, and the reason(s) for any change, is provided to the receiving clinician and the patient during any clinical handovers
What?• Increase number of patients and receiving clinicians
provided with a current list when care transferred (4.12.4)
• Communication to staff, patients
5.3 Percentage of discharge summaries that include medication therapy changes and explanations for changes

5. Communicating with patients and carers
The clinical workforce informs patients about their options, risks and responsibilities for an agreed medication management plan.
Developmental

5. Communicating with patients and carers
4.13: The clinical workforce informing patients and carers about medication treatment options, benefits and associated risks
Why?• Patients and carers require sufficient information
about treatment options to make informed choices about their medicines, and adhere to agreed treatment plans
• Failure to achieve informed agreement to the prescription can result in non-adherence

5. Communicating with patients and carers
4.13: The clinical workforce informing patients and carers about medication treatment options, benefits and associated risks
What?• Implement systems that support the
provision of patient specific medicines information when medication treatment options are discussed (4.13.1)
• Consumer Medicines Information provided (documented on MMP, in clinical notes)
• Consumer information on specific medications, for example anticoagulants, chemotherapy
• Patient specific medicines information accessible in clinical areas (4.13.2)
• Hard copy or soft copy

5. Communicating with patients and carers
4.14: Developing a medication management plan in partnership with patients and carers
Why?• 30 – 50% medicines prescribed for long term conditions
not used as prescribed 11
• Failure to achieve informed agreement or identify and provide support that patient needs to manage their medicines can lead to non-adherence can occur 11
• The medication management (action) plan is intended to support health professionals and patients/carers in developing strategies to manage medicines safely and achieve treatment goals

5. Communicating with patients and carers
4.14: Developing a medication management plan in partnership with patients and carers
What?• Undertake assessment of the patient’s medication risks to
identify medication management issues• Use Medication Risk Identification section on National Medication
Management Plan
• Develop a medication management (action) plan that establishes treatment goals and specifies actions required to achieve medication management goals (4.14.1).
- List of medicines, allergies, administration aids- Goals of therapy, action to achieve goals
• Communicate plan to patient and with the patient’s consent to other relevant health care professionals

5. Communicating with patients and carers
4.15: Providing current medicines information to patients in a format that meets their needs whenever new medicines are prescribed or dispensed
Why?• Patients and carers require information in a form they
understand and can use to assist them to use their medicines safely and effectively

5. Communicating with patients and carers
4.15: Providing current medicines information to patients in a format that meets their needs whenever new medicines are prescribed or dispensed
What?• Identify medicines information resources that are in a format
that can be used and understood by patients and carers when new medicines are prescribed/supplied or medicines changed(4.15.1)
- Similar evidence to 4.14.3- Interpreter services available for CALD patients- Written information in patients own language e.g.
multilingual medicines lists • Improve medicines information provided in response to
patient feedback (4.15.2)- Action in response for complaints, patient survey

Communicating with patients and carers

Resources
Australian Commission on Safety and Quality in Health Care – Medication Safety http://www.safetyandquality.gov.au/our-work/medication-safety/
State and Territory Medication Safety Committees/sites
Clinical Excellence Commission – High risk medicines program
http://www.cec.health.nsw.gov.au/programs/high-risk-medicines
New South Wales Health Medication Management Strategy
http://www.health.nsw.gov.au/quality/medsafe/index.asp
Victorian Health Department Quality Use of Medicines
http://www.health.vic.gov.au/qum/index.htm
Western Australian Department of Health Medication Safety
http://www.safetyandquality.health.wa.gov.au/medication/index.cfm

Resources
Audit, indicators and assessment tools
Canadian Patient Safety Institute. Safer Healthcare Now! Medication reconciliation Measures
www.saferhealthcarenow.ca/EN/Interventions/medrec/Pages/measurement.aspx
Clinical Excellence Commission, NSW Therapeutic Advisory Group Inc. Medication Safety Self Assessment® for Australian Hospitals, 2007. www.mssa.cec.health.nsw.gov.au/MSSA_introduction.html
Clinical Excellence Commission, NSW Therapeutic Advisory Group Inc Medication Safety Self Assessment ® for Antithrombotic Therapy in Australian Hospitals. www.mssa.cec.health.nsw.gov.au/at2/MSSAT_introduction.html
Continuity in Medication Management – a Handbook for South Australian Hospitals November 2010. Appendix 3: SA APAC Key Performance Indicators.
www.sahealth.sa.gov.au/wps/wcm/connect/e055bd8044fd8fc2aff7efcfa5ded0ab/Pharmaceutical+Reform+Handbook+V7_Print+version.pdf?MOD=AJPERES&CACHEID=e055bd8044fd8fc2aff7efcfa5ded0ab
Institute for healthcare Improvement Failure Modes and Effects Analysis Template http://app.ihi.org/Workspace/tools/fmea/

Resources
Audit, indicators and assessment tools (Cont’d)
ISMP Canada: International Medication Safety Self Assessment for Oncology 2012 www.cec.health.nsw.gov.au/programs/mssa
NSW TAG. Indicators for Quality Use of Medicines in Australian Hospitals www.ciap.health.nsw.gov.au/nswtag/documents/publications/QUMIndicators/Manual0408.pdf
SQuIRe Plus Guide: Medication Reconciliation Audit Tool January 2012 www.safetyandquality.health.wa.gov.au/docs/squire/Medication_Reconciliation_Audit_Tool_Guidelines.pdf
Patient and carer tools and resources
ACSQHC Medication reconciliation consumer resources.
http://www.safetyandquality.gov.au/our-work/medication-safety/
Institute of Safe Medication Practices Consumer website
www.ismp.org/consumers/default.asp, www.consumermedsafety.org
NPS Better Choices, Better Health. Medicines information for consumers
http://www.nps.org.au/consumers.
WA Health Consumers’ Council: Patient First Guide (March 2012)
http://www.health.wa.gov.au/docreg/education/population/OA004305_patient_first_book.pdf

Resources
Education resources
ACSQHC Medication Management Plan Flash training tool with audio voice over
hwww.safetyandquality.gov.au/our-work/medication-safety/medication-reconciliation/nmmp/
http://whqlibdoc.who.int/publications/2011/9789241501958_eng.pdf
National Inpatient Chart On- line Training Course www.nps.org.au/health_professionals/online_learning/NIMC
NPS Better Choices Better Health National Prescribing Curriculum on line training www.nps.org.au/health_professionals/online_learning/national_prescribing_curriculum
NPS, NSW TAG Medication Safety e-Learning Modules
http://www.nps.org.au/health_professionals/online_learning
NPS Better Choices, Better Health Quality use of medicines on line training courses
http://www.nps.org.au/health_professionals/online_learning/qum
World Health Organization. Improving Medication Safety. WHO Patient Safety Curriculum Guide: Multiprofessional Edition, 2011. http://www.who.int/patientsafety/education/curriculum/en/index.html

Summary
Ensuring that competent clinicians safety prescribe, dispense and administer appropriate medicines to informed patients and carers is an essential element of safe and high quality care.
Purpose of the Standard is to improve outcomes for patients by ensuring that there is a systematic approach to medicines management and safety
Outcomes to be achieved are clear – methods to get there will vary depending on context
www.safetyandquality.gov.au

Summary
Ensuring that competent clinicians safety prescribe, dispense and administer appropriate medicines to informed patients and carers is an essential element of safe and high quality care.
Purpose of the Standard is to improve outcomes for patients by ensuring that there is a systematic approach to medicines management and safety
Outcomes to be achieved are clear – methods to get there will vary depending on context
www.safetyandquality.gov.au

References
1. Roughead EE Lexchin A. Adverse Drug Events: counting is not enough, action is needed. Medical Journal of Australia2006;184(7):315-6
2. Easton K, Morgan T, Williamson M. Medication safety in the community: A review of the literature. National Prescribing Service, June 2009
3. Australian Council for Safety and Quality in Health care. Second national Report of Patient Safety – Improving Medication Safety. Canberra 2002
4. Roughead EE, Semple SJ Medication safety in acute care in Australia: where are we now?. Part 1: a review of the extent and causes of medication problems 2002-2008 ANZ Health Policy 2009, 6:18
5. Leape L et al Systems analysis of adverse drug events JAMA 1995;271:35-43
6. Australian Pharmaceutical Advisory Council. Guiding principles to achieve continuity of medication management .2005
7. Clinical Excellence Commission, NSW Therapeutic Advisory Group Inc. Medication Safety Self Assessment® for Australian Hospitals, 2007. www.mssa.cec.health.nsw.gov.au/MSSA_introduction.html
8. NSW TAG. Indicators for Quality Use of Medicines in Australian Hospitals www.ciap.health.nsw.gov.au/nswtag/documents/publications/QUMIndicators/Manual0408.pdf
9. Tam V, Knowles S, Cornish P, Fine N, Marchesano R, Etchells E. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. CMAJ 2005;173(5):510-15.
10. NICE. Technical patient safety solutions for medicines reconciliation on admission of adults to hospital. London. National Institute for health and Clinical Excellence, 2007.
11. NICE. Medicines adherence – involinmg patients in decisions about prescribed medicines and supporting adherence Clinical Guideline CG 76 – January 2009
12. Stowasser DA, Stowasser M, Collins DM. A randomsied controlled trial of medication liaison services – patient outcomes. J Pharmacy Practice and Research 2002;32:133-40