Embed Size (px)
Citation preview

RESEARCH ARTICLE Open Access
Stakeholder perspectives on theeffectiveness of the Victorian SaltReduction Partnership: a qualitative studyEmalie Rosewarne1*, Wai-Kwan Chislett1, Briar McKenzie1, Jenny Reimers2, Kellie-Ann Jolly3, Kirstan Corben2,Kathy Trieu1 and Jacqui Webster1
Abstract
Background: Interventions to reduce population salt intake are feasible and cost-effective. The Victorian SaltReduction Partnership implemented a complex, multi-faceted salt reduction intervention between 2014 and 2020 inthe Australian state of Victoria. This study aimed to understand stakeholder perspectives on the effectiveness of theVictorian Salt Reduction Partnership.
Methods: Semi-structured interviews were conducted with Partnership and food industry stakeholders. TheConsolidated Framework for Implementation Research was adapted for the Partnership intervention and used toguide the qualitative analysis.
Results: Fourteen Partnership and seven food industry stakeholders were interviewed. The Partnership was viewedas essential for intervention planning and decision-making and an enabler for intervention delivery. The goals ofcapacity building and collaborative action were perceived to have been achieved. The implementation teamexecuted intended intervention activities and outputs, with some adaptations to strategy. Barriers and enablers toimplementation were identified by interviewees, such as compatibility of individual, organisational and Partnershipvalues and building positive relationships between the Partnership and food industry, respectively. Legal, political,social, environmental, technological and economic factors affecting intervention design, delivery and outcomeswere identified.
Conclusions: Establishing a Partnership with diverse skills and experience facilitated collaborative action, capacitybuilding and execution of the intervention. Monitoring and evaluating implementation informed strategyadaptations, which allowed optimisation of Partnership strategy. The importance of developing strongcommunication networks between strategic and implementation-levels was a key lesson.
Keywords: Salt reduction, Public health nutrition, Stakeholder perspectives, Population intervention
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence: [email protected] George Institute for Global Health, The University of New South Wales,Sydney, NSW 2006, AustraliaFull list of author information is available at the end of the article
Rosewarne et al. BMC Nutrition (2021) 7:12 https://doi.org/10.1186/s40795-021-00414-6
BackgroundSalt reduction interventions have been identified as feas-ible, cost-effective approaches to reduce the non-communicable disease burden attributable to excess saltconsumption [1, 2]. Global estimates suggest salt intakeis double the recommended daily maximum amount of5 g per day [2, 3]. In 2017, diets high in salt resulted inalmost 3.2 million deaths and more than 70 million dis-ability adjusted life years (DALYs) globally [4]. High saltintakes cause high blood pressure, which was the attrib-utable factor in more than 10 million global deaths and381 million DALYs [4]. In an effort to reduce the salt-related non-communicable disease burden, in 2013,United Nations Member States committed to the globaltarget of a 30% relative reduction in average populationsalt intake by 2025 [5].Despite this commitment, coordinated efforts to re-
duce salt intake in many countries, including Australia,have been lacking [6, 7]. In the state of Victoria, salt in-take was estimated at 8.9 g/day in adults [8] and 6.7 g/day in children [9], with men and boys consuminghigher amounts than women and girls [8, 9] and bothadults and children exceeding the recommended max-imum salt intake [2]. To coordinate actions to reducesalt intake, in 2014 the Victorian Salt Reduction Partner-ship (referred to as the Partnership) was established bythe Victorian Health Promotion Foundation (VicHealth)
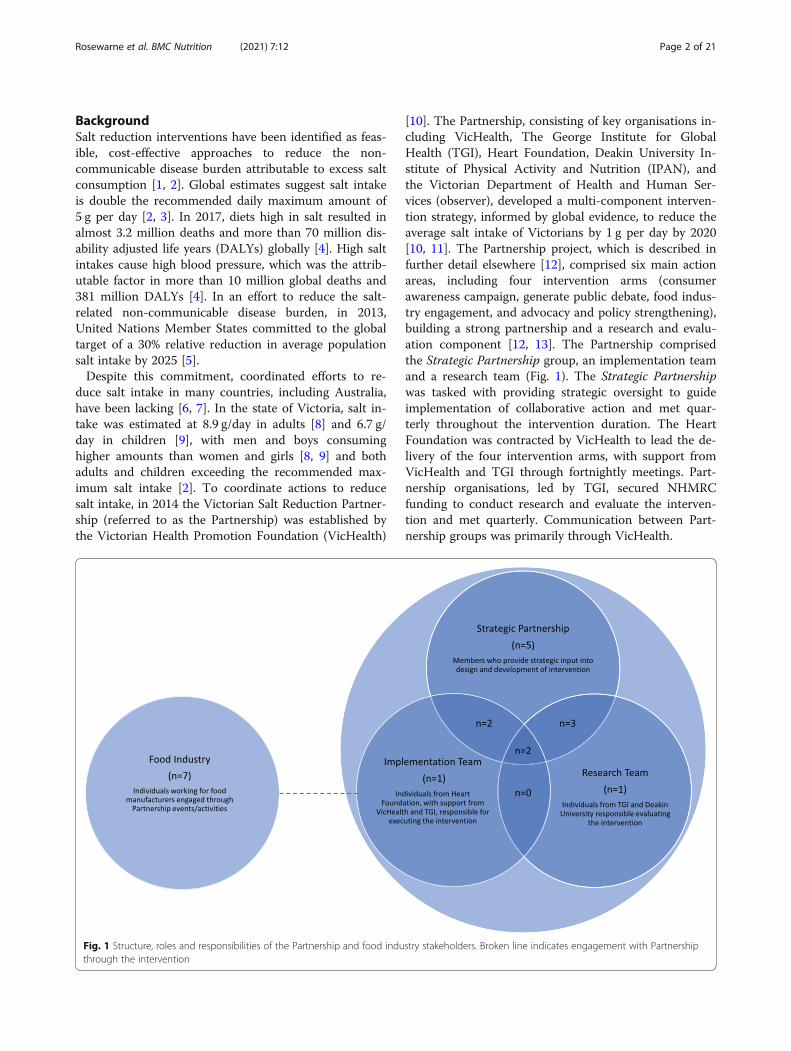
[10]. The Partnership, consisting of key organisations in-cluding VicHealth, The George Institute for GlobalHealth (TGI), Heart Foundation, Deakin University In-stitute of Physical Activity and Nutrition (IPAN), andthe Victorian Department of Health and Human Ser-vices (observer), developed a multi-component interven-tion strategy, informed by global evidence, to reduce theaverage salt intake of Victorians by 1 g per day by 2020[10, 11]. The Partnership project, which is described infurther detail elsewhere [12], comprised six main actionareas, including four intervention arms (consumerawareness campaign, generate public debate, food indus-try engagement, and advocacy and policy strengthening),building a strong partnership and a research and evalu-ation component [12, 13]. The Partnership comprisedthe Strategic Partnership group, an implementation teamand a research team (Fig. 1). The Strategic Partnershipwas tasked with providing strategic oversight to guideimplementation of collaborative action and met quar-terly throughout the intervention duration. The HeartFoundation was contracted by VicHealth to lead the de-livery of the four intervention arms, with support fromVicHealth and TGI through fortnightly meetings. Part-nership organisations, led by TGI, secured NHMRCfunding to conduct research and evaluate the interven-tion and met quarterly. Communication between Part-nership groups was primarily through VicHealth.
Fig. 1 Structure, roles and responsibilities of the Partnership and food industry stakeholders. Broken line indicates engagement with Partnershipthrough the intervention
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 2 of 21

To monitor and evaluate the effectiveness of the inter-vention, a comprehensive process and outcome evalu-ation was designed, as described in the protocol [12].The aim of the process evaluation was to examine thereach, dose, fidelity, context, adoption and effectivenessof the intervention. This was done through the collec-tion of routine administrative and cost data, impact as-sessments of consumer campaigns, product categoryreports, industry engagement, and advocacy activities,and analysis of stakeholder perspectives [12]. Semi-structured stakeholder interviews were conducted withkey stakeholders at two timepoints: (1) in the earlystages of intervention implementation (March to May2017 [14]) and (2) towards the end of the intervention(May to December 2019). This paper reports on the in-terviews undertaken in 2019. The primary objective wasto understand stakeholder perceptions of the effective-ness of the Partnership in achieving its intended roleand delivering a salt reduction intervention. Key lessonsand learnings generated from this research will be usedwith a view to contributing to greater understanding ofhow strategic partnerships can facilitate implementationof public health and nutrition interventions through col-laborative action and capacity building.
MethodsSample and recruitmentPotential participants were stakeholders involved in de-signing and/or delivering the Partnership intervention orengaged through the Partnership intervention, includingthe food industry, identified by VicHealth and the HeartFoundation. A letter of invitation to participate, along withthe participant information sheet and consent form, wasemailed to the VicHealth’s Partnership member contactlist in April 2019, and Heart Foundation food industrycontact list in August 2019. Participants agreed to partici-pate by return email, including returning a signed consentform and agreeing to an interview time. Interviews wereconducted from May to December 2019, either in personor online using Skype for Business or Zoom.
InterviewsSemi-structured interviews were conducted by two re-searchers, E.R., a PhD candidate and dietitian at TGIwho was not directly involved in the Partnership, andW-K.C., a research assistant at TGI who was not previ-ously involved in the project. The survey instrument waspreviously developed for interim stakeholder interviewsin 2017 to understand perceived barriers and enablers tointervention implementation [14] and was built on in-struments used in similar studies [15, 16]. Questionscentred on understanding the Partnership (effectiveness,structure and function), the process of executing theintervention, and internal and external factors affecting
intervention design, delivery and outcomes. Questionswere asked about each participant’s roles and their per-ceptions on delivery and fulfilment of their roles. Thesemi-structured approach allowed interviewers to adaptthe questions based on each participant’s involvement inthe Partnership, which enabled deeper knowledge in spe-cific areas. Probing questions were asked to gain moreinformation where necessary.Interviews were audio recorded using a phone and lap-
top. Permission to record was sought from participantsin the consent form and verbally at the beginning of theinterview. The interviews were manually transcribed byMurray Transcription.
Data analysisParticipants were characterised according to their in-volvement in the Partnership: Members of the StrategicPartnership (SP), implementation team (I) and/or re-search team (R); or food industry stakeholder engagedthrough the Partnership intervention (Fig. 1).Transcripts were de-identified and imported into NVivo
for data management. Transcripts were thematically ana-lysed by one researcher (E.R.), using a combination of de-ductive and inductive methods, with input from theresearch team (W-K.C., B.M., K.T. and J.W.). The Consol-idated Framework for Implementation Research (CFIR),was used to guide the qualitative analysis of the interviewsto better understand factors affecting program implemen-tation [17] within the context of the main process evalu-ation framework [12]. The CFIR is a comprehensiveframework designed for evaluations of interventions tounderstand the effectiveness of intervention implementa-tion and specifically “what factors influenced implementa-tion and how implementation influenced performance ofthe intervention” [17]. The CFIR consists of five domains:Intervention characteristics (e.g. design and developmentof the intervention), outer setting (contextual factors af-fecting intervention design, implementation and outcomese.g. political and social factors), inner setting (e.g. net-works and communication within the Partnership),characteristics of individuals (e.g. knowledge and beliefsabout the intervention) and the process of implementation(e.g. execution of the intervention). To enable a more in-depth analysis of the CFIR process domain, elements ofthe broader process evaluation framework were incorpo-rated [11]. Constructs included in this analysis were:Stakeholder perceptions on achieving intervention aims(e.g. reach and dose), and fidelity and quality of the inter-vention. The CFIR domains and adapted constructs usedin this analysis are displayed in Table 1. To ensure allmeaningful data were captured, an inductive approach,line-by-line transcript analysis, was used to identifythemes not already captured by the framework [18].
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 3 of 21

Ethics and consentThis study was approved by the University of SydneyHuman Ethics Research Committee (2016/770). Writteninformed consent was obtained from all participantsprior to the interview.
ResultsSampleTwenty-four stakeholders from 11 partner organisationsand 19 food industry stakeholders were invited to beinterviewed. Sixteen Partnership stakeholders agreed tobe interviewed, two declined as they felt they were notan active member of the partnership, one declined asthey felt a colleague (already invited) was best placed toparticipate, two were no longer with their organisation,and three did not respond. An additional two stake-holders agreed to participate however did not completethe interview process. Seven food industry stakeholdersagreed to be interviewed, two declined as they no longerworked for the company engaged by the Partnership,and ten did not respond.
In total, 14 Partnership stakeholders and seven foodindustry stakeholders were interviewed. Of the Partner-ship stakeholders interviewed, 12 were part of the Stra-tegic Partnership, five were part of the implementationteam and eight were part of the research team. Sevenparticipants were members of more than one group andtwo were members of all three groups (Fig. 1). Of theseven food industry stakeholders, one was employed bya major retailer and 6 were from large food manufactur-ing companies [19]. The average duration for Partner-ship interviews was 39 min and for industry interviewswas 30min. In general, food industry stakeholders wereonly able to speak about the industry engagement armand were not aware of the broader Partnership strategy.In the subsequent sections, we describe the key themes
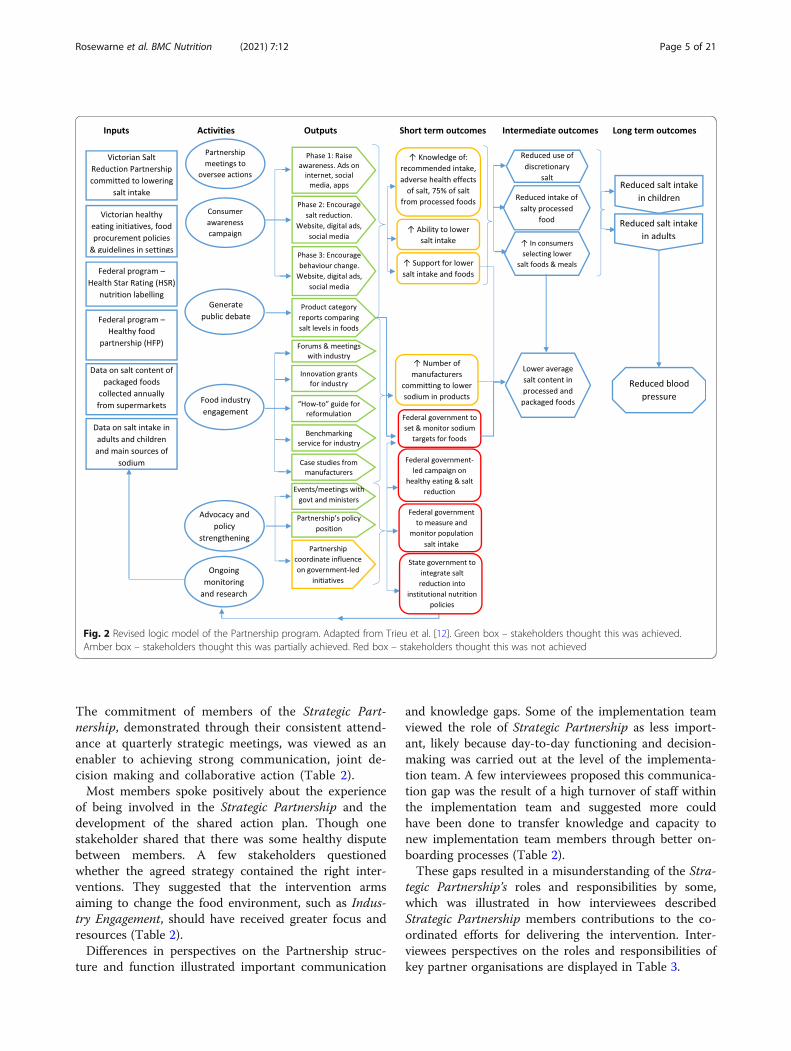
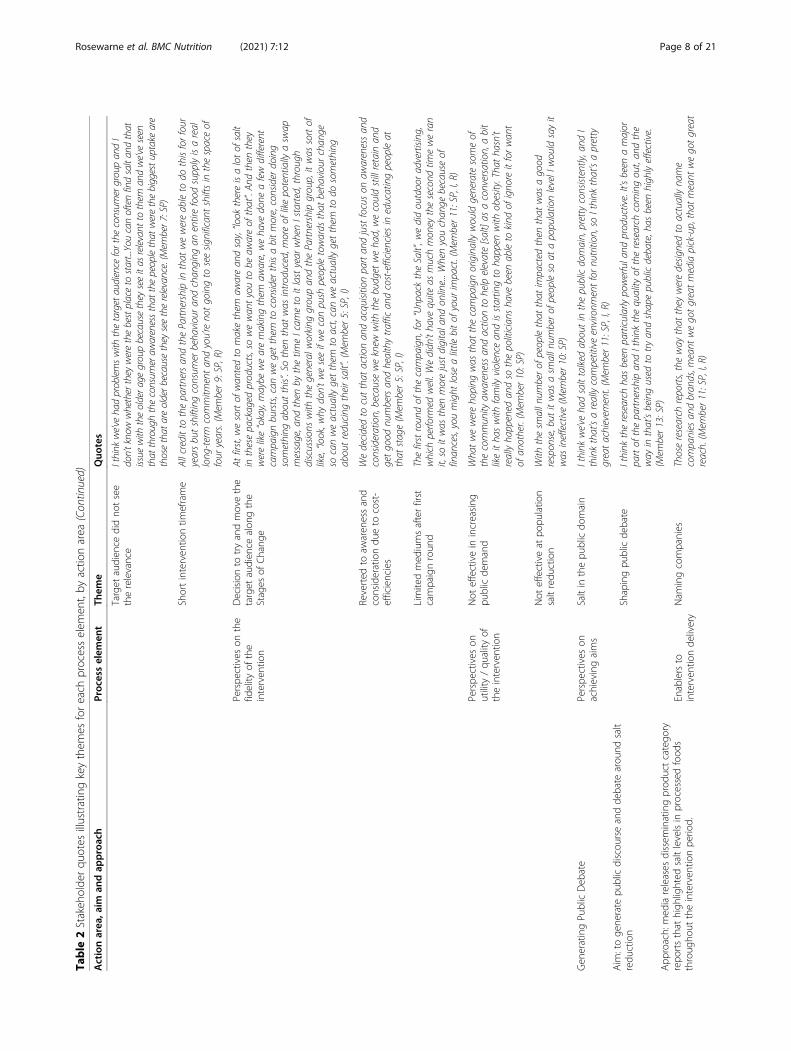
from the stakeholder interviews using the CFIR adaptedconstructs with supportive quotes. Themes are organisedas follows: (1) the Partnership (inner setting, interven-tion characteristics and individual characteristics), (2)execution of the four intervention arms includingachieving intervention aims (e.g. reach and dose), en-ablers and barriers to execution, and fidelity and qualityof the intervention (process), (3) contextual factors af-fecting intervention design, delivery and outcomes (outersetting). An overview of the Partnership program, andstakeholders’ perceptions on the effectiveness of theintervention, is illustrated in the revised project logicmodel (Fig. 2).
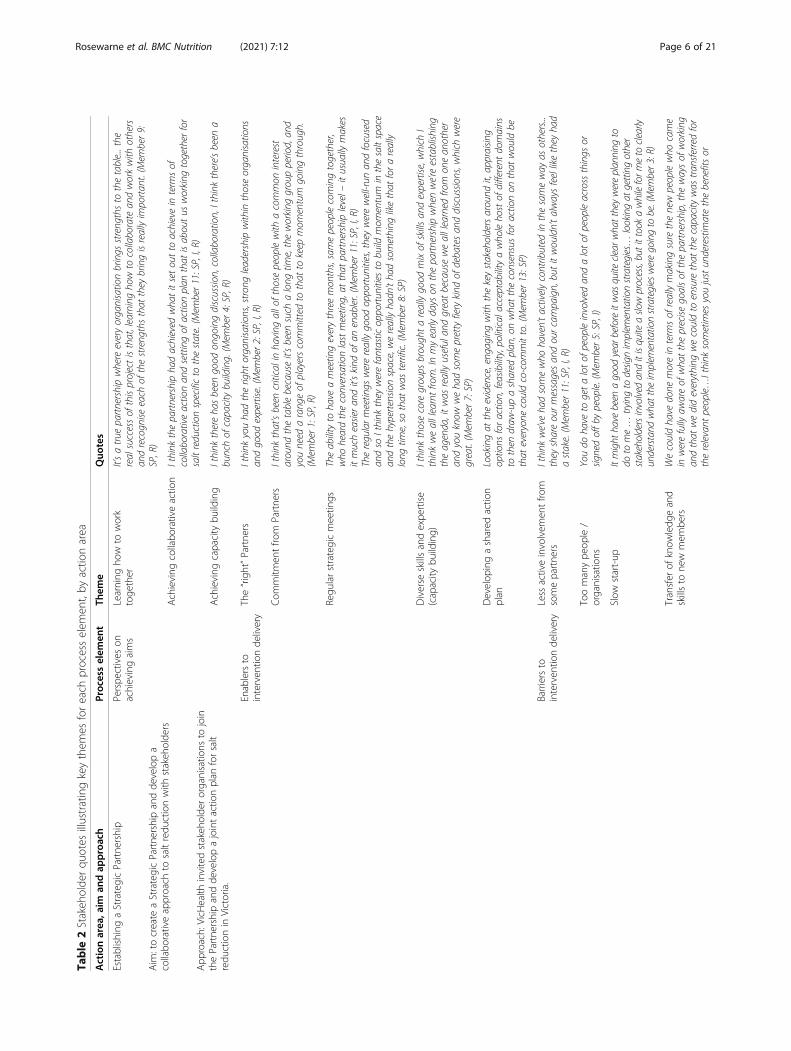
The PartnershipPerceived effectiveness, structure and function of theStrategic PartnershipThe establishment of the Strategic Partnership was de-scribed as one of the biggest successes of the project.Stakeholders believed that the Strategic Partnership waseffective in achieving its goals of capacity buildingthrough the transfer of knowledge, skills and expertisebetween members, and collaborative action through thedevelopment and execution of a shared action plan. TheStrategic Partnership was viewed by most as essential forintervention planning and decision-making processesthat underpinned the execution of the intervention andperceived to be a “background enabler” for interventiondelivery (Table 2).Interviewees felt that having the “right” organisa-
tions and individuals involved, with a diverse range ofskills and expertise, and creating a positive learningclimate, where they were able to share ideas and pro-vide input into the strategy, were important compo-nents for designing and delivering a feasible,evidence-based salt reduction intervention in Victoria.Strong engagement from organisational leaders andsalt champions were enablers for establishing and sus-taining momentum and enthusiasm for the project.
Table 1 Consolidated Framework for Implementation Research(CFIR) domains and adapted constructs
Domains Adapted constructsa
Interventioncharacteristics
Intervention design and development
Relative advantage
Adaptability
Outer setting Cosmopolitanism
External policies and incentives: National level,state level
Other outer setting factors: Political context,socio-cultural factors, environmental factors,technological factors.
Inner setting Structural characteristics: Partnership structure,organisational roles and responsibilities,changes in personnel, organisational changes
Networks and communications: Collaboration,communication
Implementation: Compatibility, learning climate
Readiness for implementation: Available resources
Characteristics ofindividuals
Knowledge and beliefs about the intervention
Self-efficacy
Individual identification with Partnership
Process Planning
Engaging the right stakeholders: Opinion leaders,formally appointed internal implementationleaders, champions, external change agents
Executing the intervention: Achieving goals,enablers and barriers to delivery, fidelity,utility/quality
Reflecting and evaluatingaBold indicates additional construct
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 4 of 21
The commitment of members of the Strategic Part-nership, demonstrated through their consistent attend-ance at quarterly strategic meetings, was viewed as anenabler to achieving strong communication, joint de-cision making and collaborative action (Table 2).Most members spoke positively about the experience
of being involved in the Strategic Partnership and thedevelopment of the shared action plan. Though onestakeholder shared that there was some healthy disputebetween members. A few stakeholders questionedwhether the agreed strategy contained the right inter-ventions. They suggested that the intervention armsaiming to change the food environment, such as Indus-try Engagement, should have received greater focus andresources (Table 2).Differences in perspectives on the Partnership struc-
ture and function illustrated important communication
and knowledge gaps. Some of the implementation teamviewed the role of Strategic Partnership as less import-ant, likely because day-to-day functioning and decision-making was carried out at the level of the implementa-tion team. A few interviewees proposed this communica-tion gap was the result of a high turnover of staff withinthe implementation team and suggested more couldhave been done to transfer knowledge and capacity tonew implementation team members through better on-boarding processes (Table 2).These gaps resulted in a misunderstanding of the Stra-
tegic Partnership’s roles and responsibilities by some,which was illustrated in how interviewees describedStrategic Partnership members contributions to the co-ordinated efforts for delivering the intervention. Inter-viewees perspectives on the roles and responsibilities ofkey partner organisations are displayed in Table 3.
Fig. 2 Revised logic model of the Partnership program. Adapted from Trieu et al. [12]. Green box – stakeholders thought this was achieved.Amber box – stakeholders thought this was partially achieved. Red box – stakeholders thought this was not achieved
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 5 of 21
Table
2Stakeh
olde
rqu
otes
illustratingkeythem
esforeach
processelem
ent,by
actio
narea
Actionarea
,aim
andap
proach
Proc
esselem
ent
Them
eQuo
tes
Establishing
aStrategicPartne
rship
Aim
:tocreate
aStrategicPartne
rshipandde
velopa
collabo
rativeapproach
tosaltredu
ctionwith
stakeh
olde
rs
App
roach:VicH
ealth
invitedstakeh
olde
rorganisatio
nsto
join
thePartne
rshipandde
velopajointactio
nplan
forsalt
redu
ctionin
Victoria.
Perspe
ctives
onachievingaims
Learning
how
towork
toge
ther
It’satrue
partnershipwhereeveryorganisationbrings
streng
thsto
thetable...the
realsuccessof
thisprojectisthat,learningho
wto
collaborate
andworkwith
others
andrecogn
iseeach
ofthestreng
thsthat
they
bringisreallyimportan
t.(M
ember9:
SP,R)
Achieving
collabo
rativeactio
nIthink
thepartnershipha
dachieved
wha
titsetoutto
achievein
term
sof
collaborativeactionan
dsettingof
actionplan
that
isaboutus
working
togetherfor
saltreductionspecificto
thestate.(M
ember11:SP,I,R)
Achieving
capacity
building
Ithink
thereha
sbeen
good
ongoingdiscussio
n,collaboration,Ithink
there’sbeen
abunchof
capacitybuilding.(M
ember4:SP,R)
Enablersto
interven
tionde
livery
The“right”Partne
rsIthink
youha
dtheright
organisations,stron
gleadershipwithin
thoseorganisations
andgood
expertise.(Mem
ber2:SP,I,R)
Com
mitm
entfro
mPartne
rsIthink
that’sbeen
criticalinha
ving
allo
ftho
sepeoplewith
acommon
interest
around
thetablebecauseit’sbeen
such
along
time,theworking
groupperiod,an
dyouneed
arang
eof
playerscommitted
tothat
tokeep
mom
entum
goingthrough.
(Mem
ber1:SP,R)
Regu
larstrategicmeetin
gsTheabilityto
have
ameetingeverythreemon
ths,samepeoplecomingtogether,
who
heardtheconversationlastmeeting,at
that
partnershiplevel–
itusually
makes
itmucheasieran
dit’skind
ofan
enabler.(M
ember11:SP,I,R)
Theregularmeetings
werereallygood
opportun
ities,theywerewell-run
andfocused
andso
Ithink
they
werefantastic
opportun
ities
tobuild
mom
entum
inthesaltspace
andthehypertensio
nspace,wereallyha
dn’tha
dsomething
likethat
forareally
long
time,so
that
was
terrific.(M
ember8:SP)
Diverse
skillsandexpe
rtise
(capacity
building)
Ithink
thosecoregroups
brough
tareallygood
mixof
skillsan
dexpertise,w
hich
Ithinkwealllearntfro
m.Inmyearly
days
onthepartnershipwhenwe’reestablish
ing
theagenda,itwas
reallyusefulan
dgreatbecausewealllearned
from
onean
other
andyouknow
weha
dsomeprettyfierykind
ofdebatesan
ddiscussio
ns,w
hich
were
great.(M
ember7:SP)
Develop
ingashared
actio
nplan
Lookingat
theevidence,eng
agingwith
thekeystakeholdersaround
it,appraisin
goptions
foraction,feasibility,politicala
cceptabilityawho
leho
stof
different
domains
tothen
draw
-upashared
plan
,onwha
ttheconsensusforactionon
that
wouldbe
that
everyone
couldco-com
mitto.(Mem
ber13:SP)
Barriersto
interven
tionde
livery
Less
activeinvolvem
entfro
msomepartne
rsIthink
we’ve
hadsomewho
haven’tactivelycontributed
inthesameway
asothers...
they
shareourmessagesan
dourcampaign,butitwouldn’talwaysfeellikethey
had
astake.(M
ember11:SP,I,R)
Toomanype
ople/
organisatio
nsYoudo
have
togetalotof
peopleinvolved
andalotof
peopleacrossthings
orsig
nedoffb
ypeople.(Mem
ber5:SP,I)
Slow
start-up
Itmight
have
been
agood
year
beforeitwas
quite
clearw
hatthey
wereplanning
todo
tome…
tryingto
desig
nimplem
entationstrategies…
lookingat
gettingother
stakeholdersinvolved
anditisquite
aslowprocess,butittook
awhileform
eto
clearly
understand
whatthe
implem
entationstrategies
weregoingto
be.(Mem
ber3:R)
Transfer
ofknow
ledg
eand
skillsto
new
mem
bers
Wecouldha
vedone
moreinterm
sof
reallymakingsurethenewpeoplewho
came
inwerefully
awareof
wha
ttheprecise
goalsof
thepartnership,thewaysof
working
andthat
wedideverything
wecouldto
ensurethat
thecapacitywas
tran
sferredfor
therelevant
people…Ithink
sometimes
youjustun
derestimatethebenefitsor
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 6 of 21
Table
2Stakeh
olde
rqu
otes
illustratingkeythem
esforeach
processelem
ent,by
actio
narea
(Con
tinued)
Actionarea
,aim
andap
proach
Proc
esselem
ent
Them
eQuo
tes
stopping
,takingstock,makingsurethat
absolutelyeverybodyin
thepartnershipis
onthesamepage
andha
sallthe
relevant
background
inform
ationan
dknow
ledge
andskillsin
orderto
ensurethat
theprojectcontinueson
thesametrack,an
dIthink
potentially
wecouldha
vespentsomemoretim
edoingthat.(Mem
ber2:SP,I,R)
Barriersto
achieving
outcom
esThe“right”interven
tion
Ithink
theHeartFoun
dationto
theextent
that
itdelivered
anintervention,did
deliveran
interventionprettyeffectively,butwhethertheinterventionwas
the
interventionthat
needed
deliveringIthink
isakeyquestion.(M
ember4:SP,R)
Everyone’spassiona
tewho
was
around
thetableon
thisissue
andof
course
you’re
goingto
have
someheat,and
that’spartof
it,itshouldn’talljustbe
smooth
sailing
,youneed
peopleto
question,challeng
ewhetheryouneed
theconsum
erpieceor
doyoujustfocuson
thefood
reform
ulationor
doyoudo
thedebate
andthepolicies?
(Mem
ber7:SP)
Perspe
ctives
onthe
fidelity
ofthe
interven
tion
Chang
esto
Partne
rship
mem
bers
Anu
mberof
otherplayersha
vecomeon
asit’sdeem
edrelevant
that
they
can
contribute,an
dobviously
they
have
aninterestin
thisarea.(Mem
ber1:SP,R)
Perspe
ctives
onutility/qu
ality
ofthe
interven
tion
EffectivePartne
rship
It’sbeen
reallyeffectiveto
have
thesedifferent
organisations
with
different
skillsets
working
socloselytogether.(Mem
ber21:SP,I)
Enablerto
interven
tion
delivery
ThePartnership’sabackground
enabler.(M
ember12:SP)
RaisingCon
sumer
Awaren
ess
Aim
:toincrease
publicaw
aren
essof
saltintakes,saltand
health,d
ietary
sourcesof
saltandstep
sto
redu
cesaltintake.
App
roach:athree-ph
asedigitalcam
paignthat
targeted
pri-
maryfood
providerswith
infamilies
with
prim
aryscho
ol-
aged
children.
Perspe
ctives
onachievingaims
Positiveachievem
ents,g
iven
limitatio
nsWith
thecampaign,they’vedone
well,giventhebudget
andallthe
otherfactors,
that
was
alwaysgoingto
makethat
atoughtask.(Mem
ber10:SP)
Goo
dreachandrecallwith
inthetarget
audien
ceNearly
50%
ofthetarget
marketswerereachedwith
thiscampaignacrossthethree
yearsthat
wedidan
intervention,which
ishu
ge,and
then
ofthat,82%
ofthat
are
recalling
oneof
ourtopkeymessagesaboutthat
there’sprocessedfood
ishigh
salt,
that
they
need
tobe
readinglabelsan
dlookingforlowersaltoptions,and
eating
fresh
isbest.So,there’ssomereallygood
positiveoutcom
esan
dthey
were
achievem
entsagainstobjectives.(Mem
ber21:SP,I)
Limitedim
pact
onge
neral
popu
latio
nThemetricswe’ve
goton
awareness-raising
wereprom
ising
andthat’sgreatbut
Deakin’sresearch
wouldsaywe’reno
tchan
ging
know
ledge,attitudes
andbeha
viours
onageneralpublic
levelbut
potentially
with
that
target
marketof
campaignwe
have
raisedaw
areness.(M
ember11:SP,I,R)
Con
certed
campaign
Wewereableto
runaconcertedcampaignforfour
yearsaround
gettingVictorians
toreduce
theirsaltintake
-Ithink
that
was
ahu
geachievem
ent.(M
ember9:SP,R)
Enablersto
interven
tionde
livery
Utilisingearntmed
iato
increase
reach
Whilst
allour
paidadvertising
focusedon
Victoria,allof
ourorganicsocialan
dearnt
mediawas
alln
ationa
l,so
wereachedfarbeyond
that.(Mem
ber21:SP,I)
Barriersto
interven
tionde
livery
Limitedmed
iums
Look
Ithink
[thereach]
islim
itedto
somedegree
becauseit’son
lysocialmedia…
there’sno
broaderbrush...w
eha
ven’tgotadiversity
ofmediums.(M
ember7:SP)
Weakmessaging
Our
callto
actionin
ourconsum
eraw
arenessha
sperhapsno
tbeen
asstrong
asit
could’ve
been.(Mem
ber7:SP)
Barriersto
achieving
outcom
esInability
tocut-throug
hothe
rnu
trition
message
sIthink
thetarget
audience
that
weweretargetingwas
problematicinthat
they’re
beingbombarded
byallsortsof
messagesaround
wha
tto
feed
theirkids
andho
wto
feed
theirkids
andho
wto
getthem
exercisin
gor
howto
maintaintheirhealth.
So,Ithinkthereweresomechalleng
esin
perhapsthetarget
audience
that
we
selected.(Mem
ber9:SP,R)
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 7 of 21
Table
2Stakeh
olde
rqu
otes
illustratingkeythem
esforeach
processelem
ent,by
actio
narea
(Con
tinued)
Actionarea
,aim
andap
proach
Proc
esselem
ent
Them
eQuo
tes
Target
audien
cedidno
tsee
therelevance
Ithink
we’vehadproblemswith
thetargetaudience
forthe
consum
ergroupandI
don’tknowwhetherthey
werethebestplaceto
start...You
canoftenfindsaltandthat
issue
with
theoldera
gegroupbecausethey
seeitas
relevant
tothem
andwe’veseen
that
throughtheconsum
eraw
arenessthat
thepeoplethat
werethebiggestu
ptakeare
thosethat
areolderb
ecause
they
seetherelevance.(Mem
ber7:SP)
Shortinterven
tiontim
eframe
Allcreditto
thepartnersan
dthePartnershipin
that
wewereableto
dothisforfour
yearsbutshiftingconsum
erbeha
viouran
dchan
ging
anentirefood
supplyisareal
long
-term
commitm
entan
dyou’reno
tgoingto
seesig
nifican
tshiftsin
thespaceof
four
years.(M
ember9:SP,R)
Perspe
ctives
onthe
fidelity
ofthe
interven
tion
Decisionto
tryandmovethe
target
audien
cealon
gthe
Stages
ofChang
e
Atfirst,w
esortof
wan
tedto
makethem
awarean
dsay,“look
thereisalotof
salt
inthesepackaged
products,sowewan
tyouto
beaw
areof
that”.An
dthen
they
werelike“okay,maybe
wearemakingthem
aware,weha
vedone
afewdifferent
campaignbursts,can
wegetthem
toconsiderthisabitmore,considerdoing
something
aboutthis”.Sothen
that
was
introduced,m
oreof
likepotentially
asw
apmessage,and
then
bythetim
eIcam
eto
itlastyear
whenIstarted,through
discussio
nswith
thegeneralw
orking
groupan
dthePartnershipgroup,itwas
sortof
like,“look,w
hydon’tweseeifwecanpush
peopletowards
that
beha
viourchan
geso
canweactuallygetthem
toact,canweactuallygetthem
todo
something
aboutreducing
theirsalt”.(Mem
ber5:SP,I)
Reverted
toaw
aren
essand
considerationdu
eto
cost-
efficiencies
Wedecidedto
cutthat
actionan
dacquisitionpartan
djustfocuson
awarenessan
dconsideration,becauseweknew
with
thebudget
weha
d,wecouldstillretain
and
getgood
numbersan
dhealthytraffic
andcost-efficiencies
ineducatingpeopleat
that
stage(M
ember5:SP,I)
Limitedmed
iumsafterfirst
campaignroun
dThefirstroun
dof
thecampaign,for“Unp
acktheSalt”,w
edidoutdooradvertising
,which
perfo
rmed
well.Wedidn
’tha
vequite
asmuchmon
eythesecond
timeweran
it,so
itwas
then
morejustdigitaland
online...Whenyouchan
gebecauseof
finan
ces,youmight
lose
alittle
bitof
your
impact.(Mem
ber11:SP,I,R)
Perspe
ctives
onutility
/qu
ality
oftheinterven
tion
Not
effectivein
increasing
publicde
mand
Wha
twewereho
ping
was
that
thecampaignoriginallywouldgenerate
someof
thecommun
ityaw
arenessan
dactionto
helpelevate[salt]as
aconversation,abit
likeitha
swith
family
violence
andisstartingto
happen
with
obesity.Tha
tha
sn’t
reallyha
ppened
andso
thepoliticians
have
been
ableto
kind
ofigno
reitforwan
tof
another.(M
ember10:SP)
Not
effectiveat
popu
latio
nsaltredu
ction
With
thesm
alln
umberof
peoplethat
that
impacted
then
that
was
agood
respon
se,but
itwas
asm
alln
umberof
peopleso
atapopulationlevelIwouldsayit
was
ineffective(M
ember10:SP)
Gen
eratingPu
blicDeb
ate
Aim
:toge
nerate
publicdiscou
rseandde
bate
arou
ndsalt
redu
ction
App
roach:med
iareleases
dissem
inatingprod
uctcatego
ryrepo
rtsthat
high
lighted
saltlevelsin
processedfood
sthroug
hout
theinterven
tionpe
riod.
Perspe
ctives
onachievingaims
Saltin
thepu
blicdo
main
Ithink
we’ve
hadsalttalked
aboutin
thepublicdomain,prettyconsistently,and
Ithinkthat’sareallycompetitiveenvironm
entfornu
trition
,soIthink
that’sapretty
greatachievem
ent.(M
ember11:SP,I,R)
Shapingpu
blicde
bate
Ithink
theresearch
hasbeen
particularlypowerfuland
productive.It’sbeen
amajor
partof
thepartnershipan
dIthink
thequality
oftheresearch
comingout,an
dthe
way
inthat’sbeingused
totryan
dshapepublicdebate,has
been
high
lyeffective.
(Mem
ber13:SP)
Enablersto
interven
tionde
livery
Nam
ingcompanies
Thoseresearch
reports,theway
that
they
weredesig
nedto
actuallyna
me
companies
andbran
ds,m
eant
wegotgreatmediapick-up,that
meant
wegotgreat
reach.(M
ember11:SP,I,R)
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 8 of 21
Table
2Stakeh
olde
rqu
otes
illustratingkeythem
esforeach
processelem
ent,by
actio
narea
(Con
tinued)
Actionarea
,aim
andap
proach
Proc
esselem
ent
Them
eQuo
tes
Barriersto
interven
tionde
livery
Alignm
entof
organisatio
nal
andPartne
rshipview
sTheHeartFoun
dationis,
asaremostorganisations
areno
w,shifting
away
from
the
nutrientsfocus…
toamorewho
le-fo
odapproach.So,wecertainlyyesfeltsometen-
sions
there…
whenwe’relookingat
food
categories(M
ember21:SP,I)
Someof
thefood
categoriesthat
VicHealth
andtheGeorgeInstitute
wouldha
veliked
togo
outwith
didn
’tsit
wellw
iththeHeartFoun
dation’sph
ilosoph
y,so
[the
Partnership]
couldn
’tpursue
thoseopportun
ities.(Mem
ber21:SP,I,R)
Barriersto
achieving
outcom
esCrowde
dnu
trition
space
Thenewspapersarefullof
debatesabout‘cleaneating,’and
caffeinewillgive
you
thisan
dyour
processedfatswillgive
youthat,w
eused
totalkaboutfatsan
dno
wwe’retalkingaboutsugars.Inthat
context,talkingaboutsaltitwas
alwaysgoingto
struggleto
getcutthrough.(M
ember13:SP)
Perspe
ctives
onthe
fidelity
ofthe
interven
tion
Chang
esin
thede
sign
ofthe
interven
tion
Ifweno
wwentinto
desig
ning
this,
we’dgo
inwith
theintentionof
implem
entation
lookinglikeitendedup...Ittook
awhileto
getto
that...thisidea
ifyoubenchm
ark
industryaround
anu
trient
oraround
thehealthinessof
theirproducts,you
can
leverage
them
forpublicaw
arenessan
dfood
industryengagementan
dpotentially
governmentpolicyengagementdepend
ingon
wha
tthepoliticalland
scapeis.
That’s
akeylesson
.(Mem
ber11:SP,I,R)
Perspe
ctives
onutility/qu
ality
ofthe
interven
tion
Engaging
med
ia,ind
ustryand
policymakers
Wha
t’sbeen
reallyeffectiveha
sbeen
theproductcategoryreports,which
theGeorge
Institute
hasdone.These
regularreports,which
basicallylook
atsaltlevelsof
certain
foods,weusethoseforstrategicadvocacy
togetmediaattention...itraises
awarenessof
thepublican
dourpolicymakers,butitalso
enablesus
toliaise
directly
with
thefood
companies
toraise
theiraw
areness...and
invite
them
tothetable,an
dto
developstrategies
totryan
dreduce
salt...that’sworkedrelativelywell.(M
ember
2:SP,I,R)
Scalability
Thisconceptof
doingthesesurveyson
food
grou
psan
dresurveyingeveryfew
yearsan
dthat
namingan
dsham
ingof
individu
alprod
ucts,brilliant,
absolutely
criticalan
dIreckon
that
was
something
that
wou
ldbe
scaled
upan
dareally
valuab
lepieceof
work.
Ithou
ghtthat
approa
chwas
very
impo
rtan
t.(M
ember8:
SP)
Inno
vativeapproaches
with
food
indu
stry
Aim
:Toredu
cesaltlevelsin
packaged
andprocessedfood
sby
supp
ortin
gfood
manufacturersto
reform
ulate.
App
roach:Engage
food
indu
stry
throug
heven
tsand
meetin
gs,d
evelop
resources,services
andgrants,and
prod
ucecase
stud
ies.
Perspe
ctives
onachievingaims
Establishing
relatio
nships
We’ve
been
successfulin
developing
reallystrong
relationships
with
someof
Australia’smajor
food
man
ufacturers(M
ember6:I)
Und
erstanding
reform
ulation
practices
Wesetoutto
engage
with
topman
ufacturersan
dun
derstand
wha
t’sha
ppening
within
thesebusin
essesan
dthen
toshow
case
theirpractice,where
itwas
available
andtryan
dhelpthosewho
aren’t,an
dIthink
weha
vedefinitelyachieved
allof
thosethings
(Mem
ber21:SP,I)
Develop
ingsupp
ortive
resourcesandservices
Andwealso
wereableto,asaresultof
working
with
[thefood
industry],developa
guideto
supportparticularlytheVictorian-basedobjectives
that
weoriginallyha
dat
theoutset
oftheproject.So
that
guidewas
something
wecoulddevelopforthese
smallerto
medium
man
ufacturersbasedin
Victoriaan
dthat’sbeen
shared
with
them
throughvarious
networks.Soyes,Ithink
we’ve
definitelyachieved
thoseout-
comes.(Mem
ber21:SP,I)
Chang
esto
thefood
supp
lyHow
effectivewillactivity
that
haskind
ofsped
upin
thelastyear
ortwobe
inactuallygettingsaltlevelsdownin
thetim
ethat
we’remeasuring?...Ifyoulooked
atitright
now,I’m
notsureifwecouldseethat
thefood
supplyha
salreadyshifted.
(Mem
ber1:SP,R)
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 9 of 21
Table
2Stakeh
olde
rqu
otes
illustratingkeythem
esforeach
processelem
ent,by
actio
narea
(Con
tinued)
Actionarea
,aim
andap
proach
Proc
esselem
ent
Them
eQuo
tes
Enablersto
interven
tionde
livery
Buildingpo
sitiverelatio
nships
Your
overalla
imwas
toreallysupportman
ufacturersan
dyouwan
tedto
provideus
with
thereform
ulationguide,youha
dan
eventthat
was
really,really
supportiveof
companies
who
weredoingthings
welland
that
reallyhelped
usto
getinvolved.
(Industry15)
Barriersto
interven
tionde
livery
Uncertainty
ofrolesand
authority
Thisisha
ppeningat
Federallevelan
dthereforewha
tisourrolean
dwha
tisour
authority
interm
sof
industryengagement.So,Ithinkitwas
that
lack
ofclarity
ofroles,an
dwheredo
wefit
andwha
t’sourauthority,Ithinkthat
was
probablyon
eof
thebarriers.(Mem
ber2:SP,I,R)
Slow
startto
implem
entatio
nEngaging
with
food
industryat
thestartmay
have
been
abitslo
wbutIpersona
llydon’tha
veexperienceengaging
with
food
industry.O
therpeopleat
thetableha
vesome,butIthink
it’stakenawhileto
probablycomeup
with
theworking
plan
ofwha
tisthebestapproach
toengage
with
that
target
group.(M
ember1:SP,R)
Perspe
ctives
onthe
fidelity
ofthe
interven
tion
Chang
esto
theplansdu
eto
new
know
ledg
eand
inno
vatio
n
OverallthePartnershipha
sbeen
soopen
totrialand
erroran
dthelevelo
finno
vationin
term
sof
let’s
trythisan
dlet’s
trythat.The
resourcesthat
have
been
developedby
thepartnershipforindustry,w
eneverenvisagedthat
atthebeginn
ing.
Who
wouldha
veenvisagedtwoyearsagothat
wewouldha
vefinish
edthisproject
with
aho
wto
guide,benchm
arking
reportsan
dgran
ts?(M
ember6:I)
Chang
esto
thetarget
audien
ceto
effect
more
change
Wechan
gedha
lf-way
throughinregardsto
ourthinking
around
who
weshouldtar-
get....Ifweha
dbeen
thinking
atthestartaround
howcanweeffectthemost
chan
gean
dtarget
thebigon
eswith
thesefood
categoryreportsan
dthen
howdo
weeffectthemostchan
gein
Victoriaby
providingtoolsan
dresourcesan
dcontacts
forsm
alltomedium,tha
twouldha
vebeen
anice
roun
dbran
dfro
mthestart.
(Mem
ber21:SP,I)
Perspe
ctives
onutility/qu
ality
ofthe
interven
tion
‘ReformulationReadiness’
Guide
Thereform
ulationreadinessguide...Ithink
that
isagreatresource
that
was
putout...
Weha
dalotof
good
feedback
from
different
areasof
oursupplychainan
dfood
techno
logistsaround
that
guide,so
justreallyhelpful.(Industry17)
Indu
stry-cen
tred
even
tsIt’sprobablythefirsttim
eweha
veseen
apublichealth
organisationrunan
industry
eventan
dbe
supportive...youun
derstand
theworkwearedoing,an
dyou’rewilling
tosupportitan
dhigh
light
wherecompanies
aredoingwell(Industry15)
Casestud
ies
Smallerbusin
esses...theyneed
toseewha
twe’redoingan
dthey
need
tolearnfro
mus
andifthey
seecase
studiesfro
mus,tha
tcanreallyhelp
them
shapetheir
nutrition
strategy,soIthink
it’sapositiveforthoseotherindustryplayersan
dalso
consum
ersto
seewha
twe’redoingan
dobviously
governmentto
seewha
twe’re
doing(Industry17)
Benchm
arking
service
TheGeorgeInstitute
was
offeringthosereportswhich
couldtake
onecompanies’
productsan
dcompareitto
theentirecategory...Ithink
that’sreallyvaluableas
well
becauseyouknow
,allcompanies
aregoingto
beinterested
toknow
wha
ttheir
competitorsaredoing.(Industry16)
Reform
ulationgrants
Thesaltreductiongran
ts,Ithinkthat’sshow
ingreallystrong
leadershipan
dshow
ing
food
man
ufacturersthat
thereissupportan
dthereareresourcesavailableto
dothis.
(Mem
ber6:I)
One
-to-on
emeetin
gsWe’ve
been
able
toun
dertakeover
20on
eon
oneenga
gementmeetin
gswhich
have
revealed
alotof
insigh
tan
dinform
ationarou
ndthedriversfor
reform
ulationan
dthecurrentob
staclesan
dissues
that
food
man
ufacturers
are
still
facing
.(M
ember6:
I)
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 10 of 21
Table
2Stakeh
olde
rqu
otes
illustratingkeythem
esforeach
processelem
ent,by
actio
narea
(Con
tinued)
Actionarea
,aim
andap
proach
Proc
esselem
ent
Them
eQuo
tes
Advocacyandpo
licystreng
then
ing
Aim
:to“stren
gthe
nhe
althypo
licies”to
improvethefood
environm
ent,includ
ingfood
reform
ulationprog
ramsand
institu
tionaln
utritionpo
licies.
App
roach:Engaging
governmen
tstakeh
olde
rs,creatinga
policypo
sitio
nstatem
entandinfluen
cing
governmen
tinitiatives.
Perspe
ctives
onachievingaims
Did
notachievepo
licychange
Ireckonifwe’djustgone,“Youknow
wha
t,to
makean
impactin
Victoriawha
twe
need
todo
isweneed
tochan
gethings
nationa
lly,”wejustspentallofo
urtim
ean
deffortjustfocusin
gon
bringing
theVictorianStategovernment,regulators,
poweran
dinfluence
tobear
onCa
nberra
andindeed
ontheotherstates,toactually
chan
gethings
forthewho
lecoun
try,maybe
that
wouldha
vebeen
moresuccessful.
(Mem
ber4:SP,R)
Whilst
wemight
notha
veseen
policychan
ge,w
e’ve
definitelycontinuedthe
conversationan
dputsupportbehind
it.(M
ember21:SP,I)
Supp
ortedalreadyplanne
dactivities
Ifeelliketheadvocacy
activities
probablyha
vejustaddedastrong
supporterbase
around
things
that
werein-train.(Mem
ber11:SP,I,R)
Enablersto
interven
tionde
livery
Develop
ingablueprint
Wedevelopedthecallto
actiondocument.Ithink
was
agreatoutput
anda
deliverable...it’sprobablythefirst-timeorganisations
have
gottogetherto
actually
getsomeform
ofconsensus,ablueprinton
wha
tweneed
goingforward.(M
ember
7:SP)
Barriersto
interven
tionde
livery
Lack
ofallocatio
nof
rolesand
respon
sibilities
Wedevelopedaclearstatem
ent,which
outlineswha
tthekeyasks
ofthestrategic
partnershipwere,butthen
wedidn
’tidentifypeerrolesor
allocate
specific
respon
sibilitiesto
thedifferent
partnershipmem
bersin
term
sof
who
was
goingto
take
that
forward.(M
ember2:SP,I,R)
Uncertainty
arou
ndow
nership
andleadership
Ithink
oneof
thechalleng
esof
thePartnership,whenyou’ve
gotmultiple
organisations,a
lotof
streng
ths,butthen
you’ve
gotacertaindegree
ofwho
’sow
ning
it,leading,drivingit,an
dwho
’sgoingto
makethosecalls
andwho
’sgoing
togetthecreditforit.Which
isun
fortun
atelythepoliticsworking
anyw
herean
dI
thinkthat’sprobablyheldsomeof
theprogressback
inthat
policyadvocacy
space
becausemixed
inwith
alltha
tpoliticalcontext.(M
ember10:SP)
Barriersto
achieving
outcom
esPo
liticalclim
ate
There’sbeen
somegood
workbutas
awho
leitprobablyha
sn’tquite
hadthe
impactat
thestatean
dfederallevelas
wewouldha
vewan
ted.That’sno
tnecessarily
becauseof
thefaultof
anyof
thepartners,it’s
partlybecauseof
the
politicalconversations
andagendasoutwheresaltisan
dyoucan’tmakean
issue
popularwith
politicians
ifthey
don’twan
titto
bean
dthere’sno
tapublicpush.
(Mem
ber10:SP)
Perspe
ctives
onthe
fidelity
ofthe
interven
tion
Shift
from
targetingstate
governmen
tto
fede
ral
governmen
t
Upun
tilprobablyJune
2018,w
ewereadvocatingat
astatelevel,an
dthen
we
shifted,w
ethough
titwas
moreof
ana
tiona
l,afederalissue...so
wewrote
anew
plan
(Mem
ber21:SP,I)
Attheverybeginn
ingof
theproject,itwas
veryVictoriafocused…
butalon
gthe
way
thedecisio
nwas
made…
it’sana
tiona
lthing
,ifthey’re
goingto
makethat
policy,it’sgoingto
beFederalpolicy.(M
ember5:SP,I,R)
Perspe
ctives
onutility
/qu
ality
oftheinterven
tion
Jointadvocacy
Therearelotsof
benefitsto
apartnershipworking
togetheron
strategicadvocacy
andIthink
we’ve
utilisedthat
quite
wellonsomeoccasio
ns,but
perhapsno
tas
well
aswecouldthrougho
utthewho
leproject,an
dIthink
thisisprobablyachalleng
eforthesesortsof
partnerships
ingeneral.(M
ember2:SP,I,R)
Advocacyasks
documen
tSomepeoplemight
saywelltha
t’sthestatem
entof
theobviousbutto
have
itas
adocumentthere,to
hand
-out
togovernmentsan
dto
useas
andadvocacy
toolwas
amileston
e.(M
ember8:SP)
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 11 of 21

Execution of the four intervention armsThe intervention action areas, process domains, keythemes and stakeholder quotes relating to the executionof the intervention are displayed in Table 2.
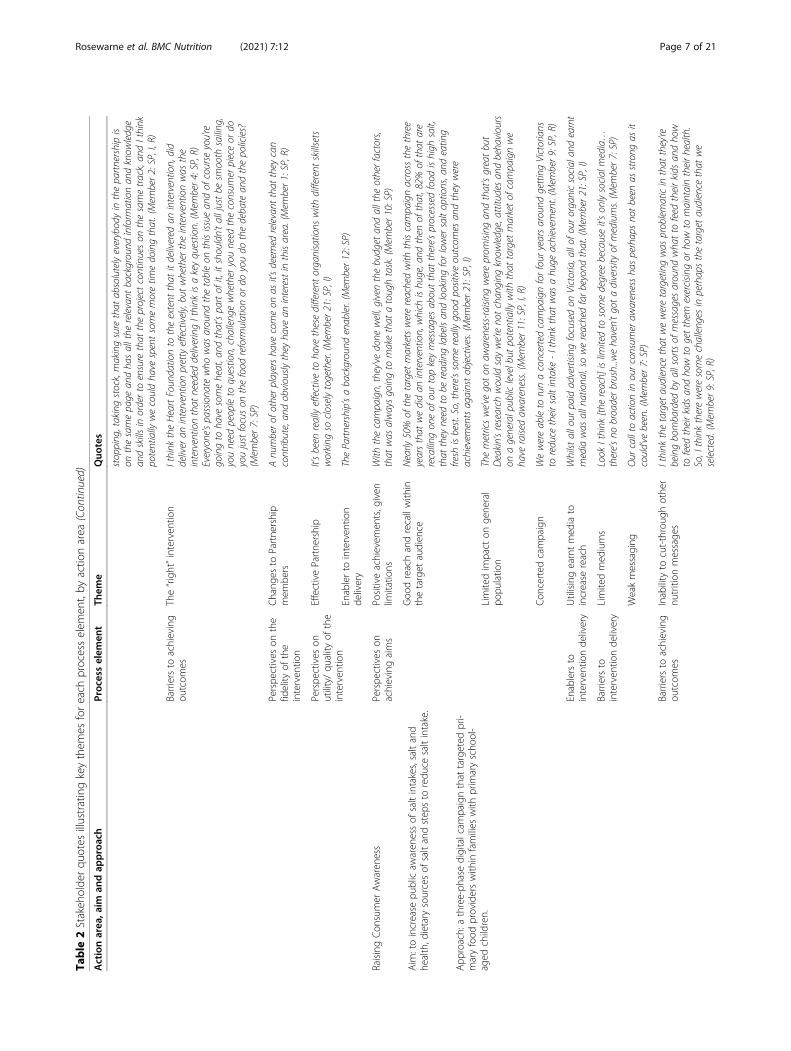
Consumer awareness campaignStakeholder perceptions on the effectiveness of the Con-sumer Awareness campaign were mixed. Stakeholders in-volved in, or overseeing, intervention delivery sharedthat a digital campaign was strategically chosen for itscost effectiveness and efficiency in reaching the targetaudience. Eight interviewees expressed that the reachwas “adequate” given the constraints of the chosen ap-proach, including the budget, timeframe and target audi-ence. Some of the intervention team shared specificachievements of the campaign, such as high recall of thekey messages within the target population (Table 2).However, overall, many felt the campaign was limited
and did not have enough reach. Two participants statedthat the campaign was ineffective in making a meaning-ful contribution to the overall Partnership goal of a one-gram reduction in population salt intake. Amongst thosewho expressed scepticism towards the campaign’s effect-iveness, challenges in delivering this intervention armand engaging the targeted population were discussed.Five reasons were suggested by interviewees: (1) The tar-get audience did not see the relevance for them becauseof the perception that high blood pressure was an olderperson’s problem; (2) the target audience was “bom-barded” with digital health messaging from othersources; (3) absence of hard-hitting campaign messagingthat did not “cut-through” other digital health messagesthat flooded media and social media spaces; and (4) lim-ited campaign mediums (digital only) as a result of tight
budgets; and (5) the intervention timeframe was tooshort (Table 2).
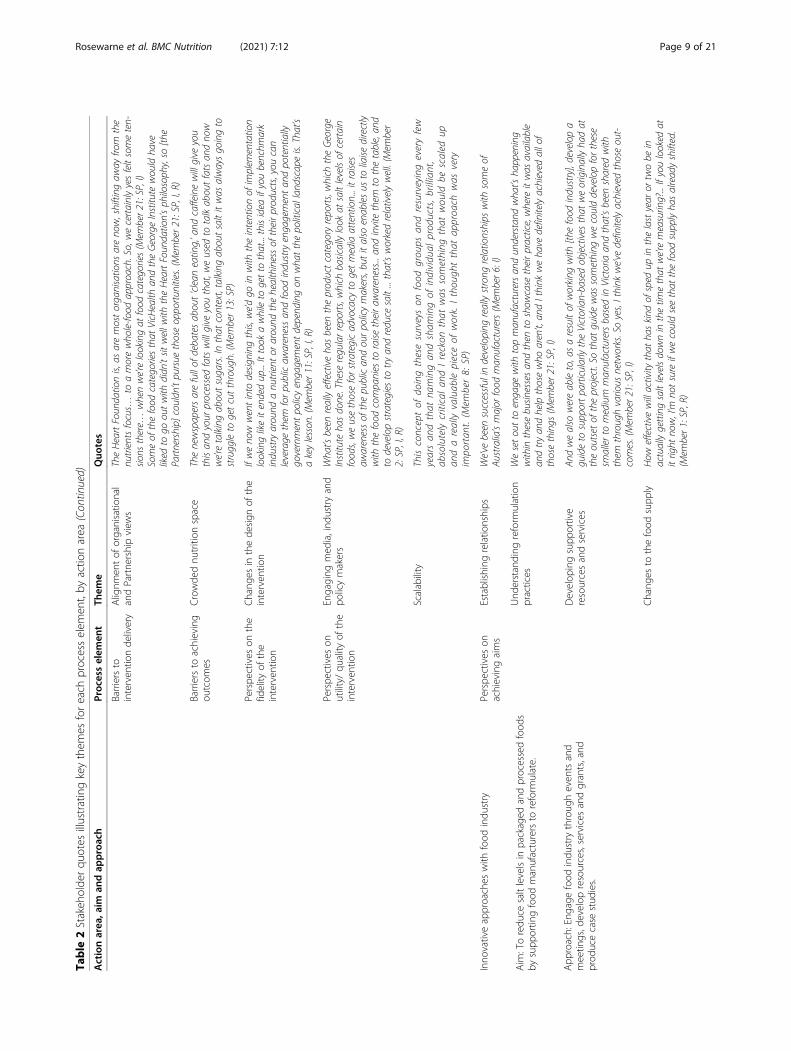
Generate public debateThe primary mechanism used to generate public debatewas perceived by interviewees to be an effective centrallever for consumer awareness raising, engaging the foodindustry and pursuing advocacy and policy asks throughmedia advocacy strategies. One stakeholder shared howthe strategy was developed overtime and many inter-viewees didn’t differentiate it from the ConsumerAwareness arm. Ten Partnership members discussed theutility of the product category reports in engaging mediaand industry. The reports were perceived to be a “starperformer”, achieving more media and industry engage-ment than anticipated, and at low cost (Table 2).However, the majority of interviewees (10 Partnership
stakeholders and three food industry stakeholders) alsoacknowledged a competitive media environment, whichwas “full of debates about ‘clean eating’” and “sugar”, assomething that potentially hindered impact. Implemen-tation team members identified that some individualsand organisations had changed focus from salt as a sin-gle nutrient towards general healthy eating principles, asa challenge that had created a misalignment between in-dividual, organisational and Partnership objectives andvalues resulting in friction between some members.These “tensions” were resolved; however, delivery of thisintervention arm was slowed and perceived as “challen-ging” at times (Table 2).
Food industry engagementThe Industry Engagement strategy was viewed as effect-ive in terms of innovative approaches to industry en-gagement and creating positive relationships between
Table 3 Organisational roles and responsibilities, as described by interviewees
Organisation Roles and responsibilities
VicHealth VicHealth has clearly set direction and part of the reason we’ve had that role is because we have funded theimplementation. (Member 11: SP, I, R)
Heart Foundation Heart Foundation was awarded a contract by VicHealth to deliver three areas of the intervention, being consumerawareness, advocacy and industry engagement (Member 21: SP, I)
The George Institute The George Institute was engaged for strategic advice and also as a research partner and subsequently built anNHMRC partnership grant around the work which the partners were engaged on (Member 13: SP)As we move forward, we have been supporting the Heart Foundation in terms of the intervention’s strategy.(Member 2: SP, I, R)
IPAN at Deakin University Much of our work has been collecting that baseline and end data for surveys in regards to knowledge, attitudesand behaviours have shifted on salt consumption throughout after this intervention, as well as actual salt intakein children and adults. (Member 1: SP, R)
Department of Health and HumanServices Victoria
Providing strategic advice and promoting the project broadly… contributing funding… government rep. (Member12: SP)
Other organisations on the StrategicPartnership
Attend four meetings a year, we’re just looking for their input, looking for their contribution, looking for where theymight be able to amplify communication messages (Member 11: SP, I, R)All of the aspects of the partnership plan were developed through consultation with myself and the other strategicleaders. (Member 13: SP)
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 12 of 21

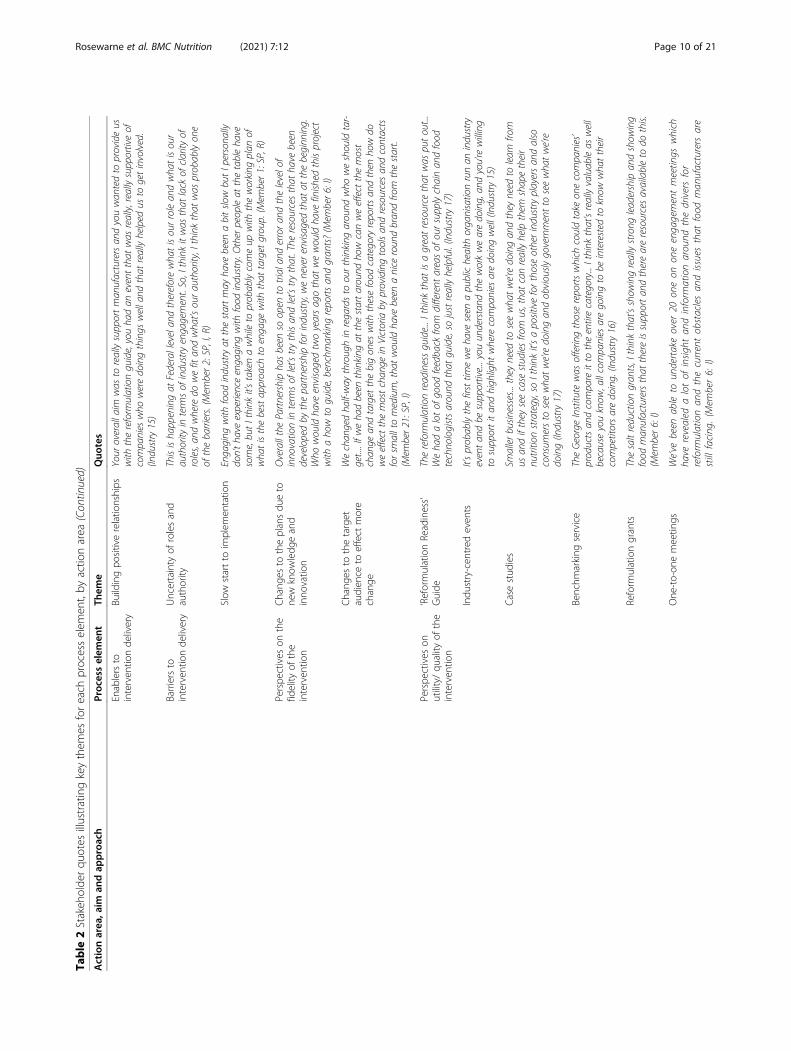
public health organisations and the food industry. How-ever, both strategic partnership members and programimplementers identified challenges, including perceivedchanges to the strategy during the intervention (Table 2).Stakeholders cited a slow start to implementation of thisintervention arm. A few suggested this was due to aninitial lack of understanding of the food industry, how toengage them and which organisation would be respon-sible. Some interviewees said that the focus initially wason supporting small-to-medium manufacturers inVictoria to reformulate processed foods, but this waslater expanded to include national and internationalmanufacturers, in order to have an impact on the Aus-tralian food supply (Table 2).Stakeholders spoke positively about the learning ex-
perience and the process of adapting the strategy to ad-dress industry needs identified throughout theintervention. Both Partnership members and food indus-try stakeholders spoke of the strong positive relation-ships that were created. One-to-one meetings were seenas important for building rapport and a two-way ex-change of knowledge between the Partnership and foodindustry. Interviewees discussed how through thesemeetings, new knowledge and understanding of industrylevers and capabilities were gained, which enabled thePartnership to adapt the industry engagement strategyto utilise levers and create services and resources to fillidentified gaps in capabilities. This included: (1) the de-velopment of a guide for reformulation to support com-panies to undertake reformulation, (2) a benchmarkingservice to assess the nutritional profile of products andcompare to competitors and to sodium targets, and (3)grants for small-to-medium manufacturers to financiallysupport reformulation. In addition to increasing cap-acity, interviewees shared that the Partnership was ableto demonstrate supportiveness of companies’ positiveprogress towards sodium reduction through public casestudies and showcases at events. This was perceived tofurther facilitate relationship building and help overcomethe “us and them mentality” between public health orga-nisations and the food industry (Table 2).
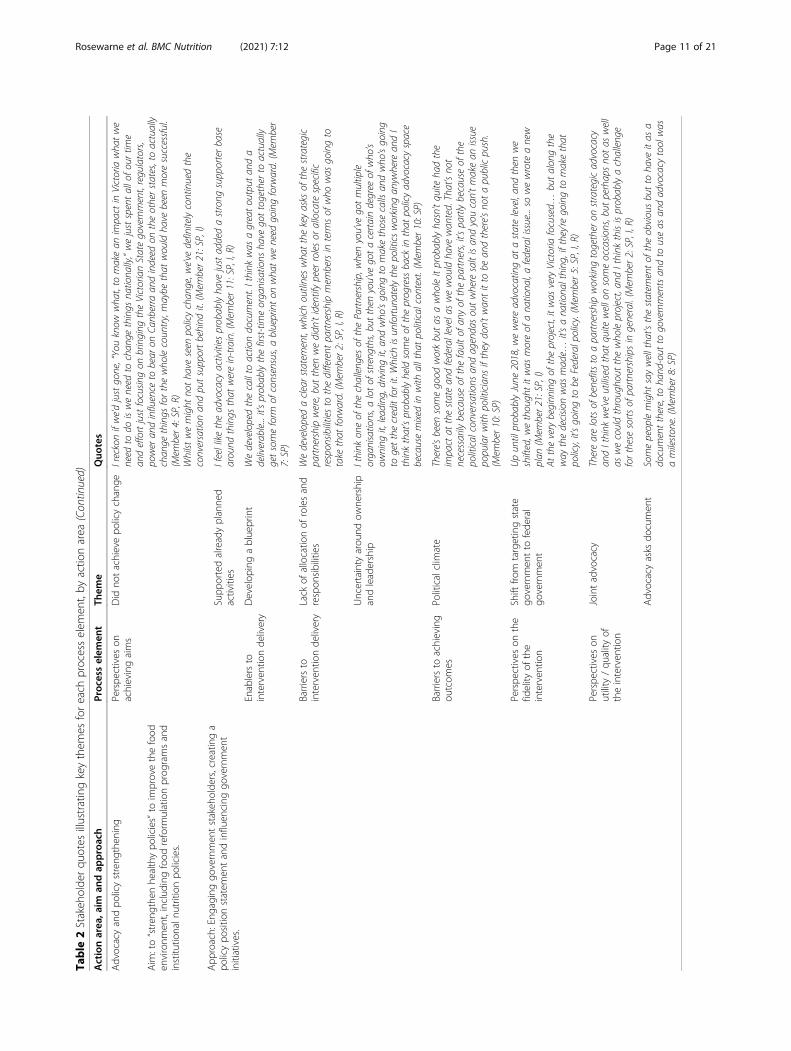
Advocacy and policy strengtheningStakeholder perspectives on the effectiveness of the Advo-cacy and Policy Strengthening arm were mixed, likely dueto differences in understanding of the intended objectivesand strategy. Two program implementers shared how thepolicy and advocacy activities were initially carried out ata state-level, however the Partnership identified that keylevers for certain food policies were at different levels ofgovernment and that there was a mis-match between whatwas planned and what was achievable at a state-level. Spe-cifically, stakeholders spoke about food reformulation pro-grams being a federal matter and many suggested this
advocacy could have been more successful if it had a na-tional focus from the outset, though some recognised thechallenges associated with the funding coming from thestate for a Victorian-specific intervention (Table 2). Con-trastingly, one strategic member spoke of the plannedstrategy as always intending to target both the federal andstate governments and two strategic members shared thatvery little progress was made towards integrating salt re-duction into state-based policies, including institutionalnutrition policies.Participants talked about the development of an ad-
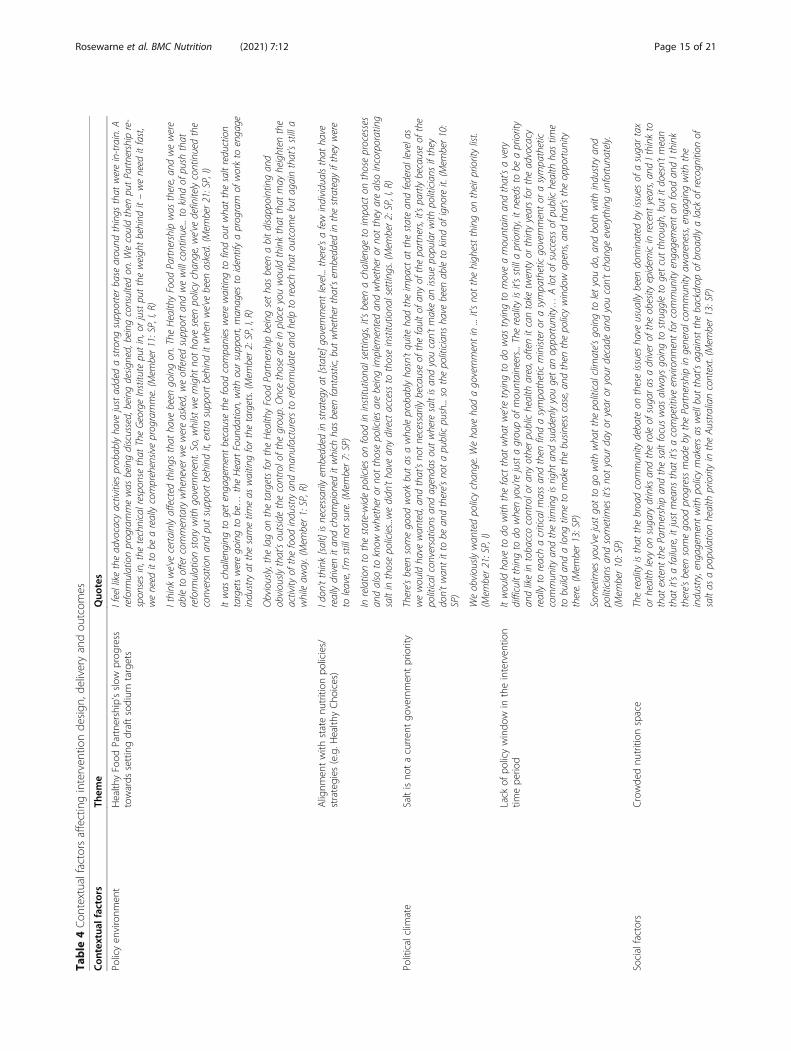
vocacy asks document, that was perceived to be vitalin bringing the organisations together and forging aconsensus on the way forward for the Partnership.However, the utility of the document, and indeed theoverall strategy, was a contested topic, with someviewing it as a “milestone” and others a “statement ofthe obvious”. Many shared how the Partnership had“affected things that have been going on”, such asproviding feedback on the draft sodium reduction tar-gets proposed by the Australian federal government’sHealthy Food Partnership in 2018 (Table 4). However,some stated the main advocacy ask of getting thegovernment to establish targets for salt was notachieved within the intervention period. Many identi-fied a lack of coordinated advocacy actions and clearallocation of roles and responsibilities to have hin-dered intervention delivery. Uncertainty regardingwhich organisation was driving the strategy and whenorganisations were advocating as part of the Partner-ship or alone were suggested to have held up inter-vention delivery and led to sparse communication ofadvocacy activities between members, resulting in alack of coordinated action. The lack of allocation ofroles created uncertainty amongst individual membersas to who was responsible for carrying out the advo-cacy activities and who was responsible for makingsure they were executed (Table 2).
Contextual factors affecting intervention design, deliveryand outcomesStakeholders identified legal, political, social, environ-mental, technological and economic factors affectingintervention design, delivery and outcomes. Key themesand supporting quotes are provided in Table 4.The state and national food policy environments were
frequently discussed and perceived to shape the inter-vention design, hinder intervention delivery and preventthe Partnership achieving outcomes. At the state level,attempts to embed salt as a priority in current institu-tional nutrition policies (e.g. schools, hospitals and pub-lic sector workplaces) were thought by one stakeholderto be hindered by an inability to access relevant organi-sations to understand what programs were being
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 13 of 21

implemented and a lack of available data on implemen-tation or effectiveness. At the national level, slow pro-gress by the government’s Healthy Food Partnership insetting and implementing nutrient reformulation targetswas viewed as a barrier to effective action in two ways.Firstly, the announcement of the Healthy Food Partner-ship and its proposed program of work in 2016, requiredthe Partnership to adapt the Advocacy and Policy strat-egy to the shift in the policy environment. Subsequently,the slow progress in setting targets, including a lengthypublic consultation, impeded further advocacy attemptsfor policy change within the intervention timeframe.Secondly, the slow progress in target setting hindered In-dustry Engagement by the Partnership. Participants indi-cated that if targets had been in place there would havebeen an acceleration of industry reformulation activityand higher demand for the Partnership to support com-panies to reduce salt in food, and ultimately a greaterimpact on the food supply. Although one participantstated that the Partnership was able to put in place astrategy and “identify a program of work to engage in-dustry at the same time as waiting for the targets”(Member 2) (Table 4).The political and social climate was viewed as not con-
ducive to achieving Partnership aims. Many stakeholdersspoke about “a lack of recognition of salt as a populationhealth priority in the Australian context” (Member 13).Some speculated that a crowded and competitive nutri-tion space in the public domain hindered the Partner-ship from achieving political and social traction, withsugar and obesity being more “top of mind” issues. Somespoke of the link between consumer demand and gov-ernment and industry action. They suggested that a lackof public push for policy change continues to allow poli-ticians to ignore salt as a health priority and a lack ofpublic demand for healthy foods continues to allow in-dustry to produce processed foods high in salt. A fewstakeholders viewed a key role of the Partnership to becontinued advocacy on the importance of salt reductionto consumers, government and industry, building a busi-ness case for when policy window opens (Table 4).
DiscussionThis research, based on in-depth interviews with 14Partnership members and seven food industry stake-holders, has provided valuable insights into stakeholderperceptions on a partnership approach to implementinga salt reduction intervention. Use of CFIR enabled un-derstanding of factors affecting program implementationand how these factors were perceived to influence Part-nership effectiveness. This has added to our knowledgeon successes and challenges of working as a partnershipto deliver a multi-faceted public health intervention andprovided valuable lessons for future initiatives.
The PartnershipStakeholders viewed the establishment of the Partner-ship as essential for intervention planning, design anddevelopment, and an enabler for intervention delivery.Previous nutrition coalitions in Australia have tended tobe homogenous in knowledge and skills with mostmembers being from a nutrition background [20];whereas, effective health partnerships engage diversemembers who bring a wide range of skill sets and know-ledge [21, 22]. Consistent with this perspective, Partner-ship members viewed their diversity as a strength. ThePartnership brought together skills and expertise in di-verse areas such as communications, campaign manage-ment, public health interventions, disease preventionand treatment, advocacy and research. By working to-gether, an effective and diverse partnership can achievebetter outcomes than any individual or organisation canalone by sharing knowledge and skills, more-efficientlyutilising available resources and executing joint activities[23]. Interviewees described how the diversity within thegroup facilitated the cultivation of a positive learning cli-mate and they spoke positively about their ability to con-tribute to the strategy and their role in executing thePartnership’s plan. Thus, the effectiveness of interven-tion implementation was facilitated by the establishmentof a Partnership with diverse members who were able tocontribute their knowledge, skills and expertise, whichenabled effective collaborative action and interventionexecution.
Execution of the interventionThe interviewees felt the planned activities of each inter-vention arm were executed and the intended outputswere generated, though some recalled adaptations andadditions over the implementation period, and this wasviewed as an achievement. However, there were variedbeliefs regarding the translation of outputs to anticipatedoutcomes across the intervention arms [12]. This mayreflect the delay between outputs and outcomes com-monly seen in public health and policy interventions,but is also likely due to (1) internal factors, such as Part-nership communication networks, (2) contextual factors,such as the social and political context, and (3) interven-tion fidelity, which were highlighted in the interviews.
Communication networks within the PartnershipThe Partnership demonstrated some common featuresof effective collaborative frameworks, such as membercommitment, communication structures, openness,planning, a shared vision, and clear decision-makingprocesses [24]. For example, interviewees described clearbenefits associated with being a member of the Partner-ship, such as fulfilling organisational health promotiongoals, which were important in facilitating commitment
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 14 of 21
Table
4Con
textualfactorsaffectinginterven
tionde
sign
,deliveryandou
tcom
es
Con
textua
lfactors
Them
eQuo
tes
Policyen
vironm
ent
Health
yFood
Partne
rship’sslow
prog
ress
towards
settingdraftsodium
targets
Ifeelliketheadvocacy
activities
probablyha
vejustaddedastrong
supporterbase
around
things
that
werein-train.A
reform
ulationprogrammewas
beingdiscussed,beingdesig
ned,beingconsultedon
.Wecouldthen
putPartnershipre-
spon
sesin,the
technicalresponsethat
TheGeorgeInstitute
putin,orjustputtheweigh
tbehind
it–weneed
itfast,
weneed
itto
beareallycomprehensiveprogramme.(M
ember11:SP,I,R)
Ithink
we’ve
certainlyaffected
things
that
have
been
goingon
.The
HealthyFood
Partnershipwas
there,an
dwewere
ableto
offercommentarywheneverwewereasked,weofferedsupportan
dwewillcontinue...to
kind
ofpush
that
reform
ulationstorywith
government.So,w
hilst
wemight
notha
veseen
policychan
ge,w
e’ve
definitelycontinuedthe
conversationan
dputsupportbehind
it,extrasupportbehind
itwhenwe’ve
been
asked.(M
ember21:SP,I)
Itwas
challeng
ingto
getengagementbecausethefood
companies
werewaitingto
findoutwha
tthesaltreduction
targetsweregoingto
be…
theHeartFoun
dation,with
oursupport,man
ages
toidentifyaprogram
ofworkto
engage
industryat
thesametim
eas
waitingforthetargets.(M
ember2:SP,I,R)
Obviously,the
lagon
thetargetsfortheHealthyFood
Partnershipbeingsetha
sbeen
abitdisappointingan
dobviously
that’soutsidethecontrolofthe
group.Oncethosearein
placeyouwouldthinkthat
that
may
heighten
the
activity
ofthefood
industryan
dman
ufacturersto
reform
ulatean
dhelpto
reachthat
outcom
ebutagainthat’sstilla
whileaw
ay.(Mem
ber1:SP,R)
Alignm
entwith
statenu
trition
policies/
strategies
(e.g.H
ealth
yCho
ices)
Idon
’tthink[salt]isnecessarily
embedded
instrategy
at[state]governmentlevel...
there’safewindividualsthat
have
reallydriven
itan
dcham
pion
editwhich
hasbeen
fantastic,but
whetherthat’sem
bedded
inthestrategy
ifthey
were
toleave,I’m
stillno
tsure.(Mem
ber7:SP)
Inrelationto
thestate-widepolicieson
food
ininstitutiona
lsettings,it’s
been
achalleng
eto
impacton
thoseprocesses
andalso
toknow
whetheror
notthosepoliciesarebeingimplem
entedan
dwhetheror
notthey
arealso
incorporating
saltin
thosepolicies...wedidn
’tha
vean
ydirectaccessto
thoseinstitutiona
lsettings.(Mem
ber2:SP,I,R)
Politicalclim
ate
Saltisno
tacurren
tgo
vernmen
tpriority
There’sbeen
somegood
workbutas
awho
leprobablyha
sn’tquite
hadtheimpactat
thestatean
dfederallevelas
wewouldha
vewan
ted,an
dthat’sno
tnecessarily
becauseof
thefaultof
anyof
thepartners,it’s
partlybecauseof
the
politicalconversations
andagendasoutwheresaltisan
dyoucan’tmakean
issue
popularwith
politicians
ifthey
don’twan
titto
bean
dthere’sno
tapublicpush...so
thepoliticians
have
been
ableto
kind
ofigno
reit.(M
ember10:
SP)
Weobviously
wan
tedpolicychan
ge.W
eha
veha
dagovernmentin
...it’sno
tthehigh
estthingon
theirprioritylist.
(Mem
ber21:SP,I)
Lack
ofpo
licywindo
win
theinterven
tion
timepe
riod
Itwouldha
veto
dowith
thefactthat
wha
twe’retrying
todo
was
trying
tomoveamountainan
dthat’savery
difficultthingto
dowhenyou’rejustagroupof
mountaineers...The
reality
isit’sstillapriority,itneedsto
beapriority
andlikein
tobaccocontroloran
yotherpublichealth
area,oftenitcantake
twentyor
thirtyyearsfortheadvocacy
reallyto
reachacriticalm
assan
dthen
findasympatheticministeror
asympatheticgovernmentor
asympathetic
commun
ityan
dthetim
ingisright
andsuddenlyyougetan
opportun
ity…
Alotof
successof
publichealth
hastim
eto
build
andalong
timeto
makethebusin
esscase,and
then
thepolicywindowopens,an
dthat’stheopportun
itythere.(M
ember13:SP)
Sometimes
you’ve
justgotto
gowith
wha
tthepoliticalclimate’sgoingto
letyoudo,and
both
with
industryan
dpoliticians
andsometimes
it’sno
tyour
dayor
year
oryour
decade
andyoucan’tchan
geeverything
unfortun
ately.
(Mem
ber10:SP)
Socialfactors
Crowde
dnu
trition
space
Thereality
isthat
thebroadcommun
itydebate
ontheseissuesha
veusually
been
dominated
byissuesof
asugartax
orhealth
levy
onsugarydrinks
andtheroleof
sugaras
adriverof
theobesity
epidem
icin
recent
years,an
dIthink
tothat
extent
thePartnershipan
dthesaltfocuswas
alwaysgoingto
struggleto
getcutthrough,butitdoesn’tmean
that
it’safailure,itjustmeans
that
it’sacompetitiveenvironm
entforcommun
ityengagementon
food
andIthink
there’sbeen
somegood
progressmadeby
thePartnershipin
generalcom
mun
ityaw
areness,engaging
with
the
industry,eng
agem
entwith
policymakersas
wellbut
that’sagainstthebackdrop
ofbroadlyalack
ofrecogn
ition
ofsaltas
apopulationhealth
priorityin
theAu
straliancontext.(M
ember13:SP)
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 15 of 21
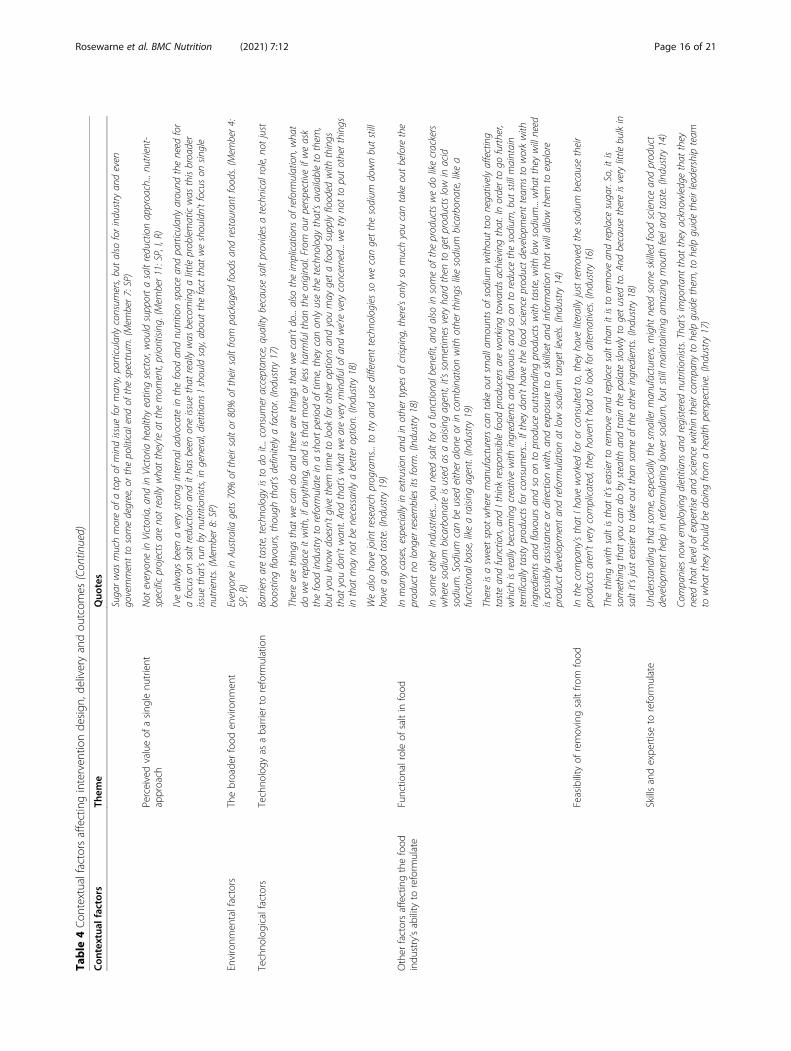
Table
4Con
textualfactorsaffectinginterven
tionde
sign
,deliveryandou
tcom
es(Con
tinued)
Con
textua
lfactors
Them
eQuo
tes
Sugarwas
muchmoreof
atopof
mindissue
forman
y,particularlyconsum
ers,butalso
forindustryan
deven
governmentto
somedegree,orthepolitical
endof
thespectrum
.(Mem
ber7:SP)
Perceivedvalueof
asing
lenu
trient
approach
Not
everyone
inVictoria,and
inVictoriahealthyeatingsector,w
ouldsupportasaltreductionapproach...nu
trient-
specificprojectsareno
treallywha
tthey’re
atthemom
ent,prioritising
.(Mem
ber11:SP,I,R)
I’vealwaysbeen
averystrong
internaladvocate
inthefood
andnu
trition
spacean
dparticularlyaround
theneed
for
afocuson
saltreductionan
ditha
sbeen
oneissue
that
reallywas
becomingalittle
problematicwas
thisbroader
issue
that’srunby
nutrition
ists,in
general,dietitian
sIsho
uldsay,aboutthefactthat
weshouldn’tfocuson
single
nutrients.(M
ember8:SP)
Environm
entalfactors
Thebroade
rfood
environm
ent
Everyone
inAu
stralia
gets70%
oftheirsaltor
80%
oftheirsaltfro
mpackaged
foodsan
drestaurant
foods.(M
ember4:
SP,R)
Techno
logicalfactors
Techno
logy
asabarrierto
reform
ulation
Barriersaretaste,techno
logy
isto
doit...consum
eracceptan
ce,qualitybecausesaltprovides
atechnicalrole,no
tjust
boostingflavours,though
that’sdefinitelyafactor.(Industry17)
Therearethings
that
wecando
andtherearethings
that
wecan’tdo...also
theimplications
ofreform
ulation,wha
tdo
wereplaceitwith,ifa
nything,an
disthat
moreor
lessha
rmfultha
ntheoriginal.From
ourperspectiveifweask
thefood
industryto
reform
ulatein
ashortperiodof
time,they
canon
lyusethetechno
logy
that’savailableto
them
,butyouknow
doesn’tgive
them
timeto
look
forotheroptions
andyoumay
getafood
supplyflooded
with
things
that
youdon’twan
t.An
dthat’swha
tweareverymindfulof
andwe’reveryconcerned...wetryno
tto
putotherthings
inthat
may
notbe
necessarily
abetteroption.(Industry18)
Wealso
have
jointresearch
programs...totryan
dusedifferent
techno
logies
sowecangetthesodium
downbutstill
have
agood
taste.(Industry19)
Other
factorsaffectingthefood
indu
stry’sability
toreform
ulate
Functio
nalroleof
saltin
food
Inman
ycases,especiallyin
extrusionan
din
othertypesof
crisp
ing,there’son
lyso
muchyoucantake
outbeforethe
productno
long
erresembles
itsform
.(Industry18)
Insomeotherindustries...you
need
saltforafunctiona
lbenefit,an
dalso
insomeof
theproductswedo
likecrackers
wheresodium
bicarbon
ateisused
asaraising
agent,it’ssometimes
veryha
rdthen
togetproductslowin
acid
sodium
.Sodium
canbe
used
eitheralon
eor
incombina
tionwith
otherthings
likesodium
bicarbon
ate,likea
functiona
lbase,likearaising
agent.(Industry19)
Thereisasw
eetspot
where
man
ufacturerscantake
outsm
allamountsof
sodium
withouttoonegativelyaffecting
tastean
dfunction,an
dIthink
respon
siblefood
producersareworking
towards
achievingthat.Inorderto
gofurther,
which
isreallybecomingcreativewith
ingredientsan
dflavoursan
dso
onto
reduce
thesodium
,but
stillmaintain
terrifically
tastyproductsforconsum
ers...Iftheydon’tha
vethefood
scienceproductdevelopm
entteam
sto
workwith
ingredientsan
dflavoursan
dso
onto
produceoutstand
ingproductswith
taste,with
lowsodium
...wha
tthey
willneed
ispossiblyassistanceor
directionwith,and
exposureto
askillsetan
dinform
ationthat
willallowthem
toexplore
productdevelopm
entan
dreform
ulationat
lowsodium
target
levels.
(Industry14)
Feasibility
ofremovingsaltfro
mfood
Inthecompany’sthat
Ihaveworkedforor
consultedto,theyha
veliterallyjustremoved
thesodium
becausetheir
productsaren’tverycomplicated,theyha
ven’tha
dto
look
foralternatives.(Industry16)
Thethingwith
saltisthat
it’seasierto
removean
dreplacesaltthan
itisto
removean
dreplacesugar.So,itis
something
that
youcando
bystealth
andtrainthepalate
slowlyto
getused
to.A
ndbecausethereisverylittle
bulkin
saltit’sjusteasierto
take
outthan
someof
theotheringredients.(Industry18)
Skillsandexpe
rtiseto
reform
ulate
Und
erstan
ding
that
some,especiallythesm
allerman
ufacturers,m
ight
need
someskilled
food
sciencean
dproduct
developm
enthelpin
reform
ulatinglowersodium
,but
stillmaintaining
amazingmouth
feelan
dtaste.(Industry14)
Companies
nowem
ployingdietitian
san
dregistered
nutrition
ists.That’simportan
tthat
they
acknow
ledgethat
they
need
that
levelofexpertisean
dsciencewithin
theircompany
tohelpguidethem
,tohelpguidetheirleadershipteam
towha
tthey
shouldbe
doingfro
mahealth
perspective.(Industry17)
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 16 of 21
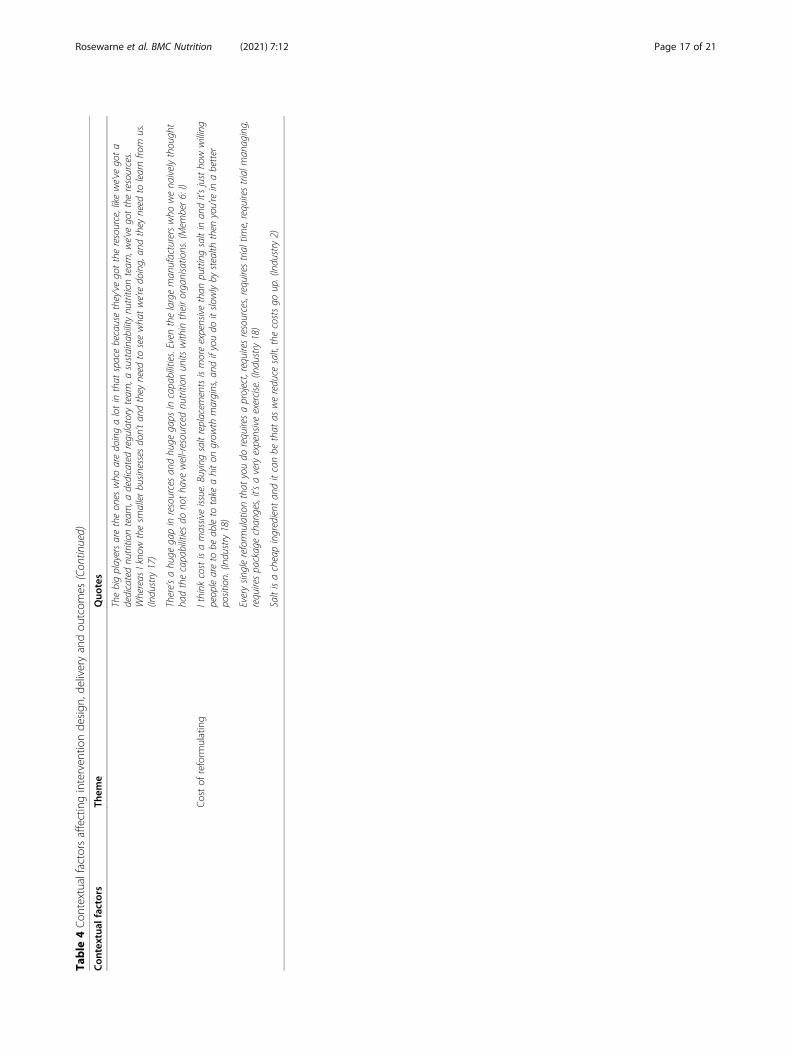
Table
4Con
textualfactorsaffectinginterven
tionde
sign
,deliveryandou
tcom
es(Con
tinued)
Con
textua
lfactors
Them
eQuo
tes
Thebigplayersaretheon
eswho
aredoingalotin
that
spacebecausethey’vegottheresource,likewe’ve
gota
dedicatednu
trition
team
,adedicatedregulatoryteam
,asustaina
bilitynu
trition
team
,we’ve
gottheresources.
Whereas
Ikno
wthesm
allerbusin
essesdon’tan
dthey
need
toseewha
twe’redoing,an
dthey
need
tolearnfro
mus.
(Industry17)
There’sahu
gegapin
resourcesan
dhu
gegaps
incapabilities.Even
thelargeman
ufacturerswho
wena
ivelythough
tha
dthecapabilitiesdo
notha
vewell-resourced
nutrition
units
within
theirorganisations.(Mem
ber6:I)
Costof
reform
ulating
Ithink
costisamassiveissue.Buyingsaltreplacem
entsismoreexpensivethan
puttingsaltin
andit’sjustho
wwilling
peopleareto
beableto
take
ahiton
grow
thmargins,and
ifyoudo
itslo
wlyby
stealth
then
you’rein
abetter
position.(Industry18)
Everysin
glereform
ulationthat
youdo
requiresaproject,requiresresources,requirestrialtime,requirestrialm
anaging,
requirespackagechan
ges,it’saveryexpensiveexercise.(Industry18)
Saltisacheapingredient
anditcanbe
that
aswereduce
salt,thecostsgo
up.(Industry2)
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 17 of 21
to the Partnership and collaborative working [23, 25].Stakeholders also described some qualities that couldhave been improved. Interviewees discussed communi-cation challenges encountered between members work-ing at the strategic level and program implementers.Despite quarterly strategic meetings, there was a lack oflack of clarity around the overall vision of the interven-tion, with stakeholders from these distinct groups hold-ing different views of action area aims and objectives,and individual’s roles and responsibilities [22]. Hunterand Perkins propose that a lack of connection betweenmembers at the strategic-level and implementation-levelis a barrier to effective partnership working due to a lackof transfer of knowledge, skills and expertise betweengroups [26]. They found that strategic partners were fo-cused on achieving the strategic goals and targets, whilethose involved in intervention delivery operated in amore organic way, distinct from the objectives set at thestrategic level [26]. This was evident within the currentPartnership. Strategic-level members mostly spoke aboutachieving strategic aims and objectives that were deter-mined at the outset, some of which were viewed as tooambitious; while program implementers seemed to havevaried understandings of the strategic goals and weremore focused on meeting organisational and individualcontractual obligations (e.g. key performance indicators).The disparity between individuals’ perspectives on Part-nership goals highlights a crucial gap between the expec-tations of the strategic partners and the ability of theprogram implementers to respond.Furthermore, program implementers and strategic
partnership members held different perspectives on eachother’s roles. For example, strategic leaders viewed theirrole as central to the intervention design and delivery,while program implementers thought of the role of stra-tegic partners as less important. Program implementersshared details about their decision-making processes,which tended to be made at the implementation teamlevel and independently of the strategic goals. These de-cisions, combined with staff turnover and poor handoverwithin the implementation team, resulted in subsequentchanges to the intervention plan and ultimately changedthe ways in which the intervention team thought aboutand executed the overall Partnership plan. Given sharedunderstanding of clear aims and objectives, and delega-tion of roles and responsibilities, are factors that facili-tate Partnership functioning [25, 26], the differences inindividual perspectives that were highlighted in the in-terviews, may have reduced the effectiveness of the Part-nership. Without having a solid understanding of theanticipated outcomes, the intervention team were work-ing towards generating the outputs they were contractedto produce rather than striving to achieve the plannedstrategic outcomes through the outputs [26, 27]. This
highlights the need for partnerships to ensure relation-ships and the transfer of knowledge and skills are main-tained between those at strategic levels and thoseresponsible for intervention delivery [26].
Contextual factorsThe importance of planning and implementing an ap-propriate intervention for the context was highlighted,as well as planning within the constraints of a chosenintervention approach, such as within the limitations ofa voluntary state-based program. This salt reductionproject utilised a partnership approach to execute afour-armed salt reduction intervention plus monitoringand evaluation. Around the world, countries are employ-ing multi-dimensional salt reduction strategies to reduceexcessive population-level salt intakes and the associateddisease burden [28]. The Partnership approach com-prised evidence-based salt reduction strategies that havebeen previously identified, including: Measuring andmonitoring salt use and knowledge, attitudes and behav-iours of Victorians and salt levels in the Australian foodsupply, engaging the food industry to reformulate prod-ucts, influencing the establishment of sodium targets forfoods and front-of-pack labelling in Australia, consumereducation to empower individuals to change their saltuse behaviours and supporting the creation of healthyfood environments in public institutions [29]. Simplyimplementing a multi-faceted evidence-based interven-tion is not enough to achieve public health outcomes ina complex real-world setting where contextual factorsare at play [27]. Tseng suggests it is not just about whatworks, but “what works for whom, under what condi-tions and at what cost” [30]. Two key challenges wereidentified: executing a salt reduction strategy within oneAustralian state from a state-based perspective and lackof available policy levers stemming from the delegationof power between state/territory governments and theCommonwealth government in Australia. Legislative andregulatory responsibilities for health policy and healthcare are split between state and Federal governments[31], which has resulted in challenges executing publichealth responses both now and in the past [32]. The de-livery of the Policy and Advocacy arm was hindered bycomplexities around this division of power, where somedesired activities needed to be executed at the federal-level (e.g. advocating for sodium targets) and others atthe state-level (e.g. integrating salt reduction into institu-tional nutrition policies). Partnership resources for thisintervention arm were divided and stretched betweenthe two approaches, and ultimately this resulted in agreater focus on Federal government advocacy and in-attention to the state-based goal. Notably, at the Federallevel, the few government strategies that have aimed toimprove population diets have been voluntary and are
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 18 of 21

unlikely to have much impact [33, 34], even though sys-tematic reviews and modelling studies suggestmandatory or legislative approaches may be more effect-ive [35, 36]. Regardless of this, through its program, thePartnership was able to engage with the food industry,including successfully building positive relationships andfacilitating reformulation [7], in the absence of regula-tion. This example demonstrates that the Partnershipapproach and strategy could be a useful model for theGovernment to adopt. A key lesson from the Partnershipwas the need to understand the context of the interven-tion – the legal and political mechanisms that influencepublic health agendas – in order to plan an appropriateintervention that fits within the context and engageswith these mechanisms, prior to commencing theintervention.Further to this, the political and social climates were
viewed as barriers to achieving planned outcomes; par-ticularly policy change, given the lack of public and pol-itical push for salt reduction. To achieve nutrition policychange, gaining public support, and demonstrating it topolicymakers, is crucial for generating political will [37].As a newly-formed coalition, the Partnership firstlyneeded to gain credibility and trust from the public [37].This is often hard for nutrition coalitions to achieve asthere is a perception from the public that the nutritionmessage is constantly changing and there is lack of con-sensus among nutrition professionals [37]. Members be-lieved a focus on salt reduction alone made it difficult tocompete with more topical issues such as sugar andobesity. The public nutrition space was described as“crowded” by mixed messaging from various specialinterest groups making it difficult for the intervention’smessages to stand out and for the Partnership to build acredible reputation, which likely limited its influence onpublic will. Interestingly, even with substantial supportand longer-term advocacy efforts, public health and nu-trition professionals have not managed to influence thegovernment to implement a national nutrition policy[38]. It is important to note, that the Partnership wasable to influence the government’s sodium target settingprocess, and subsequent to the intervention (May 2020),the government announced 27 sodium reduction targets[39]. This suggests public health and nutrition coalitionscan influence policies already on policymakers’ agendasbut illustrates the challenge in generating the public andpolitical will needed to get policies onto decision-makers’ agendas.
Fidelity of the interventionA monitoring and evaluation process was actualised to en-sure intervention fidelity and generate the evidenceneeded to support decision-making to optimise the effect-iveness of the Partnership intervention throughout the
implementation period. Our analysis revealed that theprogram implementers were able to incorporate feedbackand adapt components of the intervention plan in re-sponse to Partnership monitoring and evaluation efforts[14]. For example, the need for a more strategic approachthat would have greater impact on the food supply by tar-geting both small and medium businesses as well as largermanufacturers through a variety of different engagementmethods was identified in an interim assessment [14]. Ef-fective partnerships have clear strategic plans, which aresupported by robust monitoring and evaluation proce-dures, to determine how the partnership is performingand how intervention delivery is going throughout theintervention to establish if any modifications are needed[26]. Planned and unplanned adaptations are often madeprior to interventions (e.g. for a specific audience or con-text) and during interventions (e.g. to optimise effective-ness) [40]. Adaptations to intervention plans can have apositive or negative impact on the intervention’s effective-ness [41, 42]. Following the intervention, stakeholdersviewed the food industry strategy adaptation as one of thekey successes and a facilitator in achieving Partnershipoutcomes. However, not all recommended changes wereexecuted by the implementation team, which suggeststhere were missed opportunities to increase the impact ofthe Partnership intervention. For instance, in 2017 and2019 stakeholders identified a need for stronger, strategicconsumer-messaging that conveyed the serious healthrisks of high salt [14]; however, perceptions on thestrength of awareness-raising messages remained un-changed throughout the interventions. Program imple-menters did not comment on why such feedback was notincorporated; however, this was potentially due to achange in key personnel. They did speak about an unsuc-cessful attempt to shift consumers along the Transtheore-tical Model stages of change [43] through the threecampaign waves. While the Transtheoretical Model canbe applied to public health interventions to try to acceler-ate the rate of behaviour change, only a small proportionof the population will be willing to contemplate making achange and an even smaller proportion will be ready totake action within the intervention timeframe, leading tovaried successes in changing dietary behaviour in popula-tions [44]. This is an example of prioritising interventionfidelity over adaptation and optimisation, and raises ques-tions about whether the Partnership could have made fur-ther progress towards its consumer awareness goals if theinterim feedback had been applied.
Strengths and limitationsThe strengths of this study include that the interviewtool had been previously used for the 2017 interviews[14] and was built on survey instruments used in previ-ous studies [15, 16]. The semi-structured approach
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 19 of 21

allowed interviewers to ask tailored questions to eachinterviewee given their involvement in the Partnershipand ask probing questions to gain further informationbased on participant responses. The qualitative analysiswas guided by the CFIR, which facilitated the identifica-tion and understanding of the internal and contextualfactors that influenced intervention implementation andeffectiveness [17]. Some limitations are noted. Althoughall Partnership members were invited to participate andthere was a variety of strategic, implementation and re-search members, only 14/24 (58%) Partnership membersagreed to participate and most interviewees were fromorganisations involved in implementation or evaluation.All food manufacturers engaged by the implementationteam were also invited to participate, however only 7/19(37%) stakeholders agreed to participate, and these inter-viewees were from larger companies and their experi-ences may not be representative of all companiesengaged.
ConclusionsThe establishment of a Partnership with diverse skillsand experience facilitated collaborative action and inter-vention delivery. Monitoring and evaluating implemen-tation informed strategy adaptations which allowedoptimisation of Partnership strategy. Future partnershipsshould consider the importance of developing strongcommunication networks, particularly between strategicand implementation-levels, interventions that fit thecontext and utilise available contextual mechanisms, andthe balance between intervention adaptation and main-taining intervention fidelity.
AbbreviationsDALY: Disability-adjusted life year; TGI: The George Institute for Global Health;IPAN: Institute for Physical Activity and Nutrition; SGSA: State government orstatutory agency; CFIR: Consolidated framework for implementation research
AcknowledgementsThe authors wish to thank the interviewees for participating in the study.
Authors’ contributionsE.R., B.M., K.T., J.R. and J.W. contributed to the design of the study. E.R. andW-K.C. conducted the interviews. E.R. analysed and interpreted the data anddrafted the manuscript. All authors, E.R., W-K.C., B.M., J.R., K-A.J., K.C., K.T. andJ.W., contributed to the final manuscript by providing input into the inter-pretation of the data, reviewing, and editing the manuscript. All authors haveread and approved the final manuscript.
FundingThis study was funded by a National Health and Medical Research CouncilProject Partnership Grant (APP1111457) with additional funding from theVictorian Health Promotion Foundation. ER is supported by a University ofNew South Wales University Postgraduate Award (UPA) and George InstituteTop-Up Scholarship. BM is supported by a UNSW Scientia PhD scholarship.KT is supported by an Early Career Fellowship from the National Health andMedical Research Council of Australia (APP1161597) and a Postdoctoral Fel-lowship from the National Heart Foundation of Australia (Award ID 102140).JW is supported by a National Heart Foundation Future Leaders Fellowship II(#102039), a NHMRC CRE on food policy interventions to reduce salt(#1117300) and NHMRC project grants (#1052555 and #1111457).
Availability of data and materialsThe datasets used and/or analysed during the current study are availablefrom the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participateThis study was approved by the University of Sydney Human Ethics ResearchCommittee (2016/770) and performed in accordance with the Declaration ofHelsinki. Written informed consent was obtained from all participants priorto the interview.
Consent for publicationNot applicable.
Competing interestsJ.W. is Director of the World Health Organization (WHO) Collaborating Centreon Population Salt Reduction. VicHealth initiated and funded the VictorianSalt Reduction Partnership, J.R. and K.C. were not involved in interviewingstakeholders, analysing the data or reporting the results. All other authorsdeclare that they have no competing interests.
Author details1The George Institute for Global Health, The University of New South Wales,Sydney, NSW 2006, Australia. 2Victorian Health Promotion Foundation,Melbourne, VIC 3053, Australia. 3National Heart Foundation of Australia,Melbourne, VIC 3008, Australia.
Received: 12 November 2020 Accepted: 18 February 2021
References1. World Health Organization. ‘Best buys’ and other recommended
interventions for the prevention and control of noncommunicable diseases.Updated (2017) Appendix 3 of the global action plan for the preventionand control of noncommunicable diseases 2013–2020. Geneva: WorldHealth Organization; 2017.
2. World Health Organization. Guideline: sodium intake for adults and children.Geneva: World Health Organization; 2012.
3. Powles J, Fahimi S, Micha R, Khatibzadeh S, Shi P, Ezzati M, et al. Global,regional and national sodium intakes in 1990 and 2010: a systematicanalysis of 24 h urinary sodium excretion and dietary surveys worldwide.BMJ Open. 2013;3(12):e003733.
4. Institute for Health Metrics and Evaluation (IHME). GBD Compare DataVisualization. Seattle: IHME, University of Washington; 2017. Available from:https://vizhub.healthdata.org/gbd-compare/
5. World Health Organization. Global status report on noncommunicablediseases 2014. Geneva: World Health Organization; 2014. Available from:https://apps.who.int/iris/bitstream/handle/10665/148114/9789241564854_eng.pdf;jsessionid=98B7854EE6D6173E4848891BECFF3D27?sequence=1
6. Webster J, Trieu K, Dunford E, Nowson C, Jolly K-A, Greenland R, et al. Saltreduction in Australia: from advocacy to action. Cardiovasc Diagn Ther.2015;5:207–18.
7. Rosewarne E, Trieu K, Farrand C, Reimers J, Potter J, Davidson C, et al.Unpack the salt: an assessment of the Victorian salt reduction Partnership’smedia advocacy activities to highlight the salt content of different foods.Nutr J. 2020;19(1):102.
8. Bolton KA, Webster J, Dunford EK, Jan S, Woodward M, Bolam B, et al.Sources of dietary sodium and implications for a state-wide salt reductionprogram in Victoria, Australia. Br J Nutr. 2020;123(10):1165–75.
9. Grimes CA, Riddell LJ, Campbell KJ, Beckford K, Baxter JR, He FJ, et al.Dietary intake and sources of sodium and potassium among Australianschoolchildren: results from the cross-sectional salt and other nutrients inchildren (SONIC) study. J BMJ open. 2017;7(10):e016639.
10. Victorian Health Promotion Foundation (VicHealth). Salt Reduction inVictoria. Melbourne: VicHealth; 2017. Available from: https://www.vichealth.vic.gov.au/programs-and-projects/salt-reduction
11. Christoforou A, Trieu K, Land M-A, Bolam B, Webster J. State-level andcommunity-level salt reduction initiatives: a systematic review of globalprogrammes and their impact. J Epidemiol Community Health. 2016;70(11):1140–50.
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 20 of 21
12. Trieu K, Jan S, Woodward M, Grimes C, Bolam B, Nowson C, et al. Protocolfor the process evaluation of a complex, statewide intervention to reducesalt intake in Victoria, Australia. Nutrients. 2018;10(8):998.
13. Victorian Health Promotion Foundation (VicHealth). State of Salt: The case forsalt reduction in Victoria. Melbourne: VicHealth; 2015. Available from: https://www.vichealth.vic.gov.au/media-and-resources/publications/state-of-salt
14. McKenzie B, Trieu K, Grimes CA, Reimers J, Webster J. Understandingbarriers and enablers to state action on salt: analysis of stakeholderperceptions of the VicHealth salt reduction partnership. Nutrients. 2019;11(1):184.
15. Trieu K, Webster J, Jan S, Hope S, Naseri T, Ieremia M, et al. Processevaluation of Samoa’s national salt reduction strategy (MASIMA): whatinterventions can be successfully replicated in lower-income countries?Implement Sci. 2018;13(1):107.
16. Webster J, Pillay A, Suku A, Gohil P, Santos J, Schultz J, et al. Processevaluation and costing of a multifaceted population-wide intervention toreduce salt consumption in Fiji. Nutrients. 2018;10(2):155.
17. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC.Fostering implementation of health services research findings into practice:a consolidated framework for advancing implementation science.Implement Sci. 2009;4(1):50.
18. Bradley EH, Curry LA, Devers KJ. Qualitative data analysis for health servicesresearch: developing taxonomy, themes, and theory. Health Serv Res. 2007;42(4):1758–72.
19. Food & Drink Business. Australia's top 100 Food & Drink Companies 2019.Food & Drink Business November–December 2019; 2019. p. 29–57.
20. Cullerton K, Donnet T, Lee A, Gallegos D. Exploring power and influence innutrition policy in Australia. Obes Rev. 2016;17(12):1218–25.
21. Willis C, Greene J, Abramowicz A, Riley B. Strengthening the evidence andaction on multi-sectoral partnerships in public health: an action researchinitiative. Chronic Dis Injuries Canada. 2016;36(6):101.
22. Baker EA, Wilkerson R, Brennan LK. Identifying the Role of CommunityPartnerships in Creating Change to Support Active Living. Am J Prev Med.2012;43(5, Supplement 4):S290–S9.
23. Butterfoss FD, Kegler M. The community coalition action theory. In:DiClemente RJ, RAC, editors. Emerging theories in health promotionpractice and research. 2nd ed. San Francisco: Jossey-Bass; 2009. p. 237–76.
24. Willis C, Greene J, Riley B. Understanding and improving multi-Sectoralpartnerships for chronic disease prevention: blending conceptual andpractical insights. Evid Policy. 2017;13(4):623.
25. Taylor-Robinson DC, Lloyd-Williams F, Orton L, Moonan M, O'Flaherty M,Capewell S. Barriers to partnership working in public health: a qualitativestudy. PLoS One. 2012;7(1):e29536.
26. Hunter D, Perkins N. Partnership working in public health: the implicationsfor governance of a systems approach. J Health Serv Res Policy. 2012;17(2_suppl):45–52.
27. Wandersman A, Alia K, Cook BS, Hsu LL, Ramaswamy R. Evidence-basedinterventions are necessary but not sufficient for achieving outcomesin each setting in a complex world: empowerment evaluation, gettingto outcomes, and demonstrating accountability. Am J Eval. 2016;37(4):544–61.
28. Trieu K, Neal B, Hawkes C, Dunford E, Campbell N, Rodriguez-Fernandez R,et al. Salt reduction initiatives around the world - a systematic review ofProgress towards the global target. Plos One. 2015;10(7):e0130247.
29. World Health Organization. SHAKE the Salt Habit. The SHAKE TechnicalPackage for Salt Reduction. Geneva: World Health Organization; 2016.Available from: https://apps.who.int/iris/bitstream/handle/10665/250135/9789241511346-eng.pdf;jsessionid=8FB361AB384DFE9F6F6732A2A3F4FBCE?sequence=1
30. Tseng V. Evidence at the crossroads pt. 11: The next generation ofevidence-based policy. New York: William T Grant Foundation; 2016.
31. Parkin A, Summers J, Woodward DF. Government, politics, power and policyin Australia. Melbourne: Pearson Australia Group; 2006.
32. Moloney K, Moloney S. Australian quarantine policy: from centralization tocoordination with mid-pandemic COVID-19 shifts. Public Adm Rev. 2020;80(4):671–82.
33. Jones A, Shahid M, Neal B. Uptake of Australia’s health star rating system.Nutrients. 2018;10(8):997.
34. Rosewarne E, Huang L, Farrand C, Coyle D, Pettigrew S, Jones A, et al.Assessing the healthy food Partnership’s proposed nutrient reformulationtargets for foods and beverages in Australia. Nutrients. 2020;12(5):1346.
35. Hyseni L, Elliot-Green A, Lloyd-Williams F, Kypridemos C, O'Flaherty M,McGill R, et al. Systematic review of dietary salt reduction policies: evidencefor an effectiveness hierarchy? Plos One. 2017;12(5):e0177535.
36. Nghiem N, Blakely T, Cobiac LJ, Pearson AL, Wilson N. Health and economicimpacts of eight different dietary salt reduction interventions. Plos One.2015;10(4):e0123915.
37. Cullerton K, Donnet T, Lee A, Gallegos D. Effective advocacy strategies forinfluencing government nutrition policy: a conceptual model. Int J BehavNutr Phys Act. 2018;15(1):83.
38. Public Health Association of Australia (PHAA). National Nutrition Policy.Policy Position Statement. Canberra: PHAA; 2018. Available from: https://www.phaa.net.au/documents/item/3287
39. Healthy Food Partnership. Reformulation Targets. Canberra: Commonwealthof Australia; 2020. Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/reformulation-targets
40. Escoffery C, Lebow-Skelley E, Haardoerfer R, Boing E, Udelson H, Wood R,et al. A systematic review of adaptations of evidence-based public healthinterventions globally. Implement Sci. 2018;13(1):125.
41. Bopp M, Saunders RP, Lattimore D. The tug-of-war: fidelity versusadaptation throughout the health promotion program life cycle. J PrimPrev. 2013;34(3):193–207.
42. Pérez D, Van der Stuyft P, del Carmen ZM, Castro M, Lefèvre P. A modifiedtheoretical framework to assess implementation fidelity of adaptive publichealth interventions. Implement Sci. 2015;11(1):91.
43. Prochaska JO, DiClemente CC. The transtheoretical approach. HandbookPsychother Integration. 2005;2:147–71.
44. Greene GW, Rossi SR, Rossi JS, Velicer WF. Dietary applications of the stagesof change model. J Acad Nutr Diet. 1999;99(6):673.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Rosewarne et al. BMC Nutrition (2021) 7:12 Page 21 of 21





























