Embed Size (px)
Citation preview

From the VVA 23298-From the VVA 23298-Address coCommonwe0510. E-ma© 2009 El1527-3369doi:10.1053
Staff Nurses Working Together to Improve Carefor Late-preterm Infants
Brenda Baker, MN, RNc, CNS, Jacqueline McGrath, PhD, RN, FNAP, FAAN,Robin Lawson, MS, RNc, Theresa Liverman, MS, RN and Stephen Cohen, MD
Late-preterm infants have unique nursing care needs th
at require attention for the infant to transition easily tothe newborn phase of life. With limited physiological reserves to respond to stress, the focus of nursing care isearly recognition of stress and conservation of reserves. Evaluating current nursing practices compared withevidence-based practices can reveal what may seem to be minor practices that can have significant negativeeffects on care of the late-preterm infant. Involving all members of the health care team to increase awarenessof the issues surrounding this unique population can lead to staff development and united efforts that improveoutcomes for the late-preterm infant.Keywords: Staff development; Late-preterm infant; Thermoregulation; Discharge teaching
Staff development can often be facilitated by participation inthe integration of evidence-based practice (EBP). Evidence-based practice is a problem-solving approach to the delivery ofcare that integrates research findings from well-designedstudies (best evidence) with a clinician's practical expertiseand the preferences of the patient population and uses thisknowledge to guide clinical decision making. Researchfindings indicate that EBP results in substantially improvedoutcomes for patients.1-2
Using EBP strategies to improve outcomes for the patientpopulation of interest identified by the staff can be veryimportant in decision making surrounding changes in routinepractices that affect how staff members work together to make adifference. There are many barriers to the implementation ofEBP; however, involving staff nurses in the process fromidentification of the problem to implementation of newpractices and evaluation of the results can facilitate the uptakeof new practices as well as developing the critical thinkingstrategies of the staff as a whole. This article provides anexample of how EBP can be used as a strategy to help staffmembers work together to solve patient care problems andimprove outcomes.
irginia Commonwealth University Health System, Richmond,0510.irginia Commonwealth University, School of Nursing, Richmond,0510.rrespondence to Brenda Baker, MN, RNc, CNS, Virginiaalth University, P.O. Box 980510, Richmond, VA 23298-il: [email protected] Inc. All rights reserved./09/0903-0312$36.00/0/j.nainr.2009.06.002
BackgroundLate-preterm infants (LPIs) have unique nursing care needs
that require immediate attention for the infant to transition easilythrough the newborn phase of life. With limited physiologicalreserves to respond to cold stress, the demands of suck-swallow-breath, and glycemic control, these infants require an environ-ment that conserves resources while providing support as thepriority of care. Current professional literature has clearlyidentified the population of LPIs as a growing concern withneeds specific to their gestation. The March of Dimes3 and theAssociation of Women's Health, Obstetric, and NeonatalNursing (AWHONN)4 have clearly outlined the risks thispopulation of infants are susceptible to and a model of care thatpromotes transition and conservation of physiological reserves.Translating best practice guidelines into day-to-day practicepresents a challenge to both nursing and the medical team.
Late-preterm infants are defined as infants born between 34and 36 completed weeks' gestation. Late-preterm infantsaccount for 9% of all births and 70% of preterm births in theUnited States.6 Reasons cited for the increase in late-pretermbirth include the increased use of reproductive technology,increased rate of multifetal pregnancies, closer fetal surveillance,increased cesarean section rate, and advanced maternal age.5
Late-preterm infants have a mortality rate of 7.7 per 1000 livebirths, three times higher than that of term infants.3 Late-preterm infants are also more likely to require readmission or toseek care in the emergency department than term infants do.Discharge within the first 48 hours of life compounds the risksthe LPI faces. The American Academy of Pediatrics recommendsthat early discharge be limited to infants of singleton birth, bornbetween 38 and 42 weeks' gestation, with a birth weightappropriate for gestational age, and meeting all other discharge
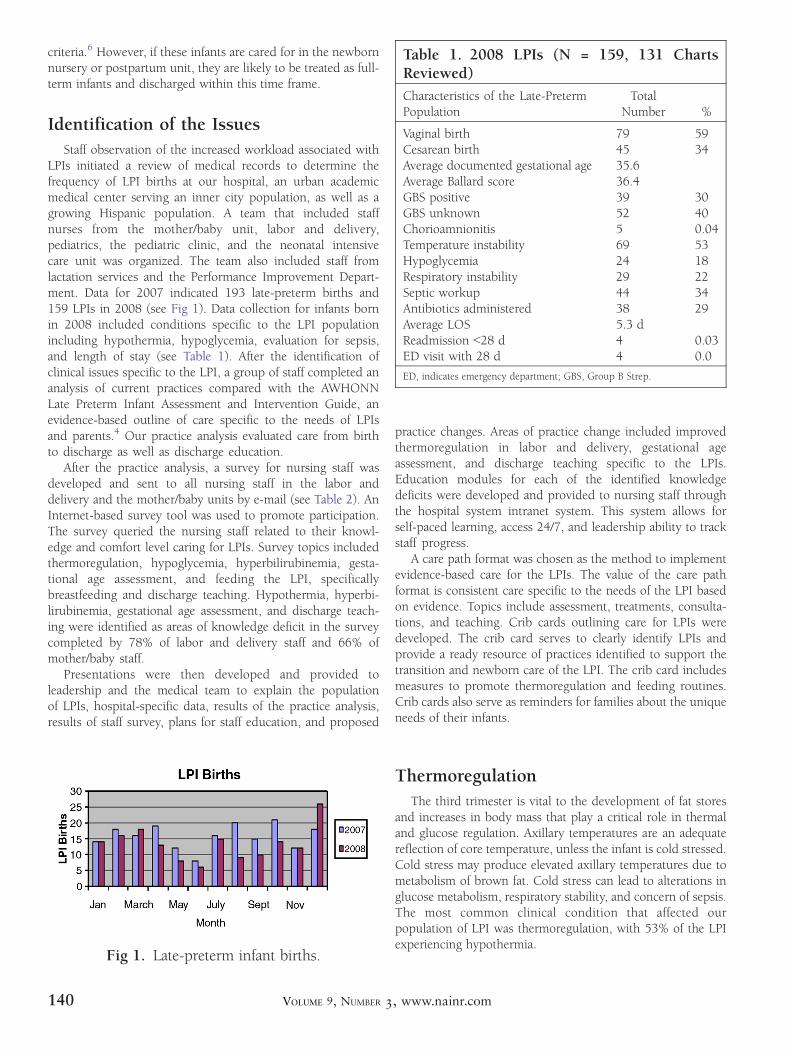
Table 1. 2008 LPIs (N = 159, 131 ChartsReviewed)Characteristics of the Late-PretermPopulation
TotalNumber %
Vaginal birth 79 59Cesarean birth 45 34Average documented gestational age 35.6Average Ballard score 36.4GBS positive 39 30GBS unknown 52 40Chorioamnionitis 5 0.04Temperature instability 69 53Hypoglycemia 24 18Respiratory instability 29 22Septic workup 44 34Antibiotics administered 38 29Average LOS 5.3 dReadmission b28 d 4 0.03ED visit with 28 d 4 0.0
ED, indicates emergency department; GBS, Group B Strep.
criteria.6 However, if these infants are cared for in the newbornnursery or postpartum unit, they are likely to be treated as full-term infants and discharged within this time frame.
Identification of the IssuesStaff observation of the increased workload associated with
LPIs initiated a review of medical records to determine thefrequency of LPI births at our hospital, an urban academicmedical center serving an inner city population, as well as agrowing Hispanic population. A team that included staffnurses from the mother/baby unit, labor and delivery,pediatrics, the pediatric clinic, and the neonatal intensivecare unit was organized. The team also included staff fromlactation services and the Performance Improvement Depart-ment. Data for 2007 indicated 193 late-preterm births and159 LPIs in 2008 (see Fig 1). Data collection for infants bornin 2008 included conditions specific to the LPI populationincluding hypothermia, hypoglycemia, evaluation for sepsis,and length of stay (see Table 1). After the identification ofclinical issues specific to the LPI, a group of staff completed ananalysis of current practices compared with the AWHONNLate Preterm Infant Assessment and Intervention Guide, anevidence-based outline of care specific to the needs of LPIsand parents.4 Our practice analysis evaluated care from birthto discharge as well as discharge education.
After the practice analysis, a survey for nursing staff wasdeveloped and sent to all nursing staff in the labor anddelivery and the mother/baby units by e-mail (see Table 2). AnInternet-based survey tool was used to promote participation.The survey queried the nursing staff related to their knowl-edge and comfort level caring for LPIs. Survey topics includedthermoregulation, hypoglycemia, hyperbilirubinemia, gesta-tional age assessment, and feeding the LPI, specificallybreastfeeding and discharge teaching. Hypothermia, hyperbi-lirubinemia, gestational age assessment, and discharge teach-ing were identified as areas of knowledge deficit in the surveycompleted by 78% of labor and delivery staff and 66% ofmother/baby staff.
Presentations were then developed and provided toleadership and the medical team to explain the populationof LPIs, hospital-specific data, results of the practice analysis,results of staff survey, plans for staff education, and proposed
Fig 1. Late-preterm infant births.
140 VOLUME 9, NUMBER 3
practice changes. Areas of practice change included improvedthermoregulation in labor and delivery, gestational ageassessment, and discharge teaching specific to the LPIs.Education modules for each of the identified knowledgedeficits were developed and provided to nursing staff throughthe hospital system intranet system. This system allows forself-paced learning, access 24/7, and leadership ability to trackstaff progress.
A care path format was chosen as the method to implementevidence-based care for the LPIs. The value of the care pathformat is consistent care specific to the needs of the LPI basedon evidence. Topics include assessment, treatments, consulta-tions, and teaching. Crib cards outlining care for LPIs weredeveloped. The crib card serves to clearly identify LPIs andprovide a ready resource of practices identified to support thetransition and newborn care of the LPI. The crib card includesmeasures to promote thermoregulation and feeding routines.Crib cards also serve as reminders for families about the uniqueneeds of their infants.
ThermoregulationThe third trimester is vital to the development of fat stores
and increases in body mass that play a critical role in thermaland glucose regulation. Axillary temperatures are an adequatereflection of core temperature, unless the infant is cold stressed.Cold stress may produce elevated axillary temperatures due tometabolism of brown fat. Cold stress can lead to alterations inglucose metabolism, respiratory stability, and concern of sepsis.The most common clinical condition that affected ourpopulation of LPI was thermoregulation, with 53% of the LPIexperiencing hypothermia.
, www.nainr.com

Table 2. LPI Staff Survey1. Your comfort level in caring for the LPI is best described as:Very comfortable Comfortable Neither Uncomfortable Very Uncomfortable2. Your level of knowledge of thermoregulation of the LPI is best described as:Very knowledgeable Knowledgeable Knowledge deficit3. Your level of knowledge related to physical assessment of the LPI is best described as:Very knowledgeable Knowledgeable Knowledge deficit4. Your level of knowledge related to jaundice/hyperbilirubinemia in the LPI is best described as:Very knowledgeable Knowledgeable Knowledge deficit5. Your comfort level assisting LPI mothers with breastfeeding is best described as:Very comfortable Comfortable Neither Uncomfortable Very Uncomfortable6. Your level of knowledge related to gestation age assessment in the LPI is best described as:Very knowledgeable Knowledgeable Knowledge deficit7. Your knowledge level of discharge teaching for the LPI is best described as:Very knowledgeable Knowledgeable Knowledge deficit8. Your knowledge of glucose management in the LPI is best described as:Very knowledgeable Knowledgeable Knowledge deficit9. What practice changes would improve outcomes for LPIs?
A literature review of neonatal thermoregulation wascompleted, and practice changes were identified. Practiceimprovements included identification of the LPI beforebirth and initiating interventions immediately aimed atthermoregulation.7-9 Labor and delivery nurses began consis-tently double wrapping LPIs in warmed blankets and dressing ina diaper, shirt, and hat. Any infant with a temperature less than97.7°F was transferred to the mother/baby unit early to providecloser monitoring. Another significant finding showed thatmother's who had delivered by cesarean section frequently hadlow temperatures postoperative. Labor and delivery nursesquestioned the practice of a fluid bolus before surgery as a reasonfor maternal hypothermia and a possible factor contributing tonewborn hypothermia. An improvement project was initiated inlabor and delivery to review maternal temperatures post-operatively in relation to the amount of intravenous fluidsadministered before and during a cesarean section; this is anongoing project, and results are not yet available.
Other seemingly minor practices in the transition periodincluded reweighing newborns when admitted to the mother/baby unit and how the first bath was done. Reweighing was aduplicate work exposing already thermally unstable infants tofurther cold stress. Reweighing was eliminated from routine care.The AWHONN Neonatal Skin Care Guidelines were used toestablish best practices for the initial bath and subsequent baths.10
Extensive staff education was provided on the topic ofthermoregulation, includingmethods for obtaining temperatures,rewarming techniques, and signs and symptoms of cold stress.
Gestational Age AssessmentReview of clinical data and staff survey information indicated
a need for gestational age assessment. Prenatal gestational ageassessment found in prenatal records compared with Ballardscores during the transition period often varied by more than aweek. The New Ballard Gestational Age assessment toolavailable online was used as part of the education module on
NEWBORN & INFANT NURSING
gestational age assessment.11 Pediatric residents and attendingphysicians also participated in gestational assessment education.
Discharge Teaching Needs for theLate-Preterm Family
Nursing staff survey findings indicated a need for moreinformation related to the specific needs of LPIs to preparefamilies for discharge. A patient education tool specific to theneeds of the LPI was developed as well as staff guidelines fordischarge teaching. Nursing approached every encounter withthe family was an opportunity to teach and prepare fordischarge. Routine newborn discharge teaching addressedhyperthermia, but not hypothermia, a much more commonrisk factor for the LPI. Discharge teaching for the LPIs stresseshow to take a temperature, signs and symptoms of dehydration,and detailed education on feeding LPIs.12-14 Lactation con-sultants are a routine part of the team caring for LPIs, providingeducation and support specific to the mother and LPI needs.
According to published guidelines from the AmericanAcademy of Pediatrics,15 the LPI should have a car seat testbefore discharge, to monitor for apnea, bradycardia, and oxygendesaturation. It is estimated that 12% of LPIs will experienceapneic, bradycardic episodes and decline in oxygen desatura-tion while placed in an infant car seat.16-17 Car seat testingbefore discharge has been added to routine care for the LPI.Resources for alternative care seats are also available for infantsidentified by a car seat test to be at risk.
Other Results of Nursing Changesin Practice
Medical staff also supported our focus on the late-pretermpopulation. During weekly rounds to review departmentstatistics, all births less than 39 weeks are reviewed. Inductions
141REVIEWS, SEPTEMBER 2009

of labor and cesarean sections at less than 39 weeks are viewedfor clinical appropriateness. Through consistent education andawareness of the impact of birth in the late-preterm period, aconsistent message has been conveyed to the medical staff. Themedical staff has embraced this effort by participating in datareview and identification of additional medical team practiceissues contributing to late-preterm births.
Efforts to reduce the incidence of late-preterm birth andimprove the care provided to the late-preterm population arestill in the development phase. Improvements have been seen insuch as decrease in the number of LPIs born at our hospital, aswell as improvements in specific clinical issues includingthermoregulation and gestational age assessment. Our effortswill continue to focus on care that is evidence based andsupports the LPIs' transition. The nursing staff has grown in theability to identify a problem and use EBP strategies to improvepatient outcomes.
References1. McGinty J, Anderson G. Predictors of physician compliance
with American Heart Association guidelines for acutemyocardial infarction. Crit Care Nurs Q 2008;31:161-172.
2. Shortell SM, Rundall TG, Hsu J. Improving patient care bylinking evidence-based medicine and evidence-based man-agement. JAMA 2007;298:673-676.
3. March of Dimes. Late preterm birth: every week matters.Intranet 2007. Available at: URL: http://www.marchofdimes.com/files/MP_Late_Preterm_Birth-Every_Week_Matters_3-24-06.pdf.
4. Santa-Donato A, Medoff-Cooper B, Bakewell-Sachs S, AskinDF, Rosenberg S. Late Preterm Infant Assessment Guide.Washington, DC: AWHONN; 2008.
5. Engle WA, Tomashek KM, Wallman C. “Late-preterm”infants: a population at risk. Pediatrics 2007;120:1390-1401.
6. Tomashek KM, Shapiro-Mendoza CK, Weiss J, et al. Earlydischarge among late preterm and term newborns and
142 VOLUME 9, NUMBER 3
risk of neonatal morbidity. Semin Perinatol 2006;30:61-68.
7. Laptook A, Jackson GL. Cold stress and hypoglycemia inthe late preterm (“near term”) infant: impact on nurseryadmission. Semin Perinatol 2006;30:24-27.
8. Thoerner AL. Neonatal induced hypothermia. NewbornInfant Nurs Rev 2007;7:95-99.
9. McGrath JM. Procedure #: 190 neonatal thermoregulation.In: Verger J, Lebet R, editors. AACN Procedure Manual forPediatric Acute and Critical Care. American Association ofCritical Care Nurses. St Louis, MO: Elsevier; 2007.p. 1390-1398.
10. Lund CH, Kuller J, Raines DA, Ecklund S, ArchambaultME, O'Flaherty P. Neonatal Skin Care: Evidence-BasedClinical Practice Guideline. 2nd ed. Washington, DC:AWHONN; 2007.
11. Gestational age assessment. In: Tappero EP, Honeyfield ME,editors. Physical Assessment of the Newborn: A Compre-hensive Approach to the Art of Physical Examination.3th ed. Santa Rosa, CA: NICU Ink; 2003.
12. Jorgensen AM. Late preterm birth: a rising trend (part oneof a two-part series). Nurs Womens Health 2008;12:309-317.
13. Jorgensen AM. Late preterm infants: clinical complicationsand risk (part two of a two-part series). Nurs Women'sHealth 2008;12:318-331.
14. McGrath JM. “He's just a little small:” helping families tounderstand implications of caring for a late preterm infant.Newborn Infant Nurs Rev 2007;7:120-121.
15. American Academy of Pediatrics Committee on Injury andPoison Prevention. Safe transportation of newborns athospital discharge. Pediatrics 1999;104:986-989.
16. Tedeschi L. The challenge of positional car seat testing inhealthy near-term neonates. Newborn Infant Nurs Rev2007;7:100-105.
17. Waltsman K. The importance of positioning the near-terminfant for sleep, play and development. Newborn InfantNurs Rev 2007;7:76-81.
, www.nainr.com





























