Embed Size (px)
Citation preview

Stable patterns of AH block arising from longitudinaldissociation and reentry within the superfused rabbitAV junction
Eugene Patterson & Benjamin J. Scherlag &
Ralph Lazzara
Received: 13 January 2009 /Accepted: 24 November 2009 /Published online: 4 February 2010# Springer Science+Business Media, LLC 2010
AbstractIntroduction Multiple forms of antegrade AH Wenckebachblock (WB) observed in 14 of 221 superfused rabbit AVjunctions.Methods Bipolar and microelectrode recordings were usedto examine the mechanism of multiple forms of AH WB.Results Each of the 14 preparations demonstrated typical3:2 and 2:1 AV block, but also demonstrated longitudinaldissociation within the slow pathway input (N=11) orcompact AV node (N=3). A 3:2 WB in one pathway and1:1 conduction in a parallel pathway summated to provideantegrade conduction of the third atrial beat. Retrogradeconduction (reentry) blocked conduction of the fourthimpulse (4:3 block). A 5:4 block was similarly observed,with summation providing for antegrade AH activation ofthe third and fourth atrial beats. Retrograde activationobserved with the fourth beat, terminated antegradeconduction of the fifth beat.Conclusions The studies demonstrate multiple AH WBpatterns consistent with rate-dependent longitudinal disso-ciation, summation of dissociated AV conduction pathways,and retrograde conduction block within the AV junction.
Keywords Wenckebach block . Atrioventricularconduction . Longitudinal dissociation . Reentry . AV node .
Wenckebach conduction
1 Introduction
Increasing the atrial heart rate in mammalian hearts initiallyproduces a graded slowing of conduction through the AVjunction evidenced as a prolongation of the atrial-Hisbundle (AH) activation interval [1]. Further increases inthe atrial heart rate produce second degree AV blockevidenced first as 3:2 Wenckebach AV conduction blockand then as 2:1 AV conduction block [1, 2]. The site ofcommon 3:2 Wenckebach block has largely been ascribedto the “AV node”, with little regard paid to an exactanatomic location of the slowed conduction and block (i.e.,slow pathway input, fast pathway input, compact AV node,etc.). Although the slowing of AH conduction andWenckebach block occurs within a complex anatomicarrangement of myocardial cells with disparate electricalproperties, in vitro studies using the superfused rabbit AVjunction [3–5] and studies of the intact canine heart [5–8],have demonstrated that conduction slowing within theslow AV conduction pathway and 3:2 Wenckebach AVblock are most commonly determined by posterior/inferiortransitional cell inputs to the compact AV node. The site ofstable 2:1 AV block is determined by the anteriortransitional cell input to the compact AV node [3–8].Although these patterns of AV conduction block arenormal properties of the AV junction tissues in the rabbitand dog, there is little information available as to theelectrophysiologic bases and anatomic sites determiningthe less commonly observed, more complicated patterns ofAV Wenckebach block, such as 4:3 and 5:4 Wenckebachblock (WB).
In the present studies, we examined the bases for AVand VA conduction block in 221 superfused rabbit AVjunction preparations studied using local bipolar elec-trode and intracellular microelectrode recordings, con-
E. Patterson (*) :B. J. Scherlag :R. LazzaraOU Medical Center, and DVA Medical Center,The University of Oklahoma Health Sciences Center,6E 103 ET CARI, 1200 Everett Drive,Oklahoma City, OK 73104, USAe-mail: [email protected]
J Interv Card Electrophysiol (2010) 28:5–18DOI 10.1007/s10840-009-9462-z

firming earlier observations of the anatomic sites andelectrophysiologic bases for common 3:2 Wenckebachand 2:1 AV block and examining the hypothesis thatlocalized reentry within the superfused rabbit AVjunction may provide a basis for the less commonlyobserved, more complicated 4:3, 4:2, and 5:4 patterns ofAV block observed in mammalian species.
2 Methods
2.1 Experimental preparations
Adult New Zealand rabbits of either sex weighing 2.5–4 kgwere anesthetized with sodium pentobarbital (30 mg/kgIV). The heart was removed and rinsed in Tyrode’s solution(in mmol/L; NaCl, 130; KCl, 4.05; MgCl2, 1.0; NaHCO3,20; NaH2PO4, 1.0; glucose, 5.5; and CaCl2, 1.35) bubbledwith 95% oxygen: 5% CO2 (pH=7.4). The right atrium andAV junction were pinned in a 20 ml Lucite chamber andsuperfused at 20 ml/min (36°). Both extracellular bipolarelectrodes (0.10 mm diameter insulated silver wires, 1 mmapart) and intracellular glass microelectrodes (1.0 mmdiameter filled with 3 M KCl having a tip resistance of 5-30 MΩ) were used to record from various anatomic siteswithin the preparation [3–5]. Bipolar electrograms wererecorded from the posterior/inferior AV nodal input (termedthe slow pathway (SP)), transitional cells of the anterior fastAV nodal input (fast pathway, (FP)), and the proximal Hisbundle (HB) in each experiment. Pacing stimuli wereintroduced from the high right atrium (4 ms duration at2–3× diastolic voltage) using a Grass S-88 stimulator.Bipolar electrograms were individually amplified andfiltered at 1–5000 Hz. Permanent recordings were obtainedat a paper speed of 100 mm/s using a Gould Windografrecorder. Microelectrode recordings at the various locations(8–26 sites, mean=12 sites) were made individually andaligned from stable recordings made at the same pacedcycle lengths and at different times, but during the samerhythm as verified by the multiple extracellular bipolarelectrode recordings made at different anatomic sites. Allexperiments were approved by the Institutional AnimalCare and Use Committees of the University of OklahomaHealth Sciences Center and the Oklahoma City Departmentof Veterans Affairs Medical Center.
2.2 Statistics
Data are expressed as the mean±standard error of the mean.Differences between groups were determined by analysis ofvariance for paired or unpaired data as appropriate followedby a Student–Neuman–Keuls test. Criterion for significancewas p<0.05.
3 Results
3.1 Normal AV conduction in the superfused rabbit AVjunction
A total of 221 rabbit AV preparations were studied atdecreasing 1–2-ms-paced intervals from the sinus heart rateuntil 2:1 AV conduction block was observed (169±12 ms).Initial 2:1 AH conduction block (slow pathway input, N=4;compact AV node, N=11; fast pathway input, N=206) waspreceded by 3:2 Wenckebach AV conduction block in 197preparations (186±13 ms). AV pre-excitation mediated byan extension of fast pathway transitional fibers bypassingthe compact AV node and connecting to the His bundle wasobserved in seven preparations as described previously [5].Common 3:2 AV WB was observed to occur within thecompact AV node at a longer cycle length than transitionalcell input (slow pathway input), with 1:1 conductionmaintained within both the anterior and posterior/inferiorAV nodal inputs in 11 preparations at a paced cycle lengthof 170±10 ms. The most common site of 3:2 AV conductionblock was within transitional fibers of the posterior/inferiorAV nodal input (slow pathway input) lying between thetricuspid valve and the tendon of Todaro. Initial 3:2 blockwithin transitional cell fibers of the posterior/inferior AVnodal input was observed in 186 of 221 rabbit AV junctionpreparations studied and in 186 of the 197 preparationsdemonstrating 3:2 AV block with rapid high right atrialpacing, at a paced cycle length of 188±12 ms. Furtherdecreases in the high right atrial paced cycle length produced2:1 block mediated primarily within the anterior AV nodalinputs (N=186) at a cycle length of 160±14 ms. The patternof block development observed within all the rabbit AVjunction preparations is described in a flow chart (Fig. 1).
WB (3:2) within the slow pathway input was observedover a 26±2.7 ms duration window of paced atrial cyclelengths followed by 2:1 conduction block, either withintransitional cells of the anterior AV nodal input (N=20),transitional cells of the posterior/inferior AV nodal input(N=158), or within the compact AV node (N=8). As the atrialcycle length was decreased within the interval producing 3:2WB, the site of Wenckebach block within the slow pathwayinput moved proximally, from a site near its insertion into thecompact AV node, towards the coronary sinus os.
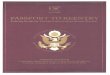
An example of the most common mode of 3:2 AH WBwithin transitional cells of the slow pathway input (160 mscycle length) is shown in Fig. 2. At paced atrial cyclelengths of 145 to 159 ms, the site of 3:2 Wenckebachmoves to more proximal sites within the slow pathwayinput, closer to the coronary sinus os (not shown). The siteof AV conduction block then shifts when 2:1 blockdevelops within transitional fibers of the anterior fastpathway input (142 ms cycle length; Fig. 2). The site of
6 J Interv Card Electrophysiol (2010) 28:5–18

2:1 block moves successively to more superior sites alongthe anterior AV nodal input with decreases in the pacedatrial cycle length (not shown) [4, 5, 7, 9, 10]. A secondexample of 3:2 WB observed within transitional cells of theposterior/slow pathway input is shown in Fig. 3.
3.2 Normal HA conduction
Retrograde HA conduction was demonstrated in 209 of 221superfused rabbit preparations. Earliest atrial exit within theposterior/slow pathway input was observed in 18 of the 209preparations demonstrating HA conduction with earliest atrialexit observed along the fast pathway input in the remaininganimals. An AV nodal bypass tract consisting of transitionaltissues from the fast pathway input directly attaching to theHis bundle was observed in 22 of 221 preparations. Theobservation of direct HA connections bypassing the compactAV node has been previously reported [5].
3.3 Multiple forms of AV WB
Three different stable and reproducible patterns of ante-grade AH Wenckebach conduction block were observed in
the present studies, 3:2, 4:3, and 5:4 conduction block.Although other uncommon patterns of Wenckebach con-duction blocks, i.e., 6:5 and 7:6, were also occasionallyobserved, the patterns were neither reproducible norsufficiently sustained as to allow systemic investigationand multiple microelectrode recordings to be performedduring stable WB. All three stable patterns of antegradeWB (3:2, 4:3, and 5:4 block) were observed in three AVjunction preparations. Both 3:2 and 5:4 antegrade WB werepresent in two preparations and both 3:2 and 4:3 antegradeWB were present in eight preparations. Two sites of stable3:2 block (slow pathway input and compact AV node) wereobserved in two preparations.
In order for the compact AV node to be (1) the site of 3:2AV WB conduction block, and (2) the site for slowconduction, summation, and reentry to produce 4:3 or 5:4conduction block, the slow pathway input/posterior transi-tional cell input must demonstrate 3° conduction blockwhile the fast pathway input retains 1:1 compact AV nodalactivation. This allows the compact AV node to be the sitefor 3:2, 4:3, and 5:4 AV conduction block. This uncommonobservation is clearly demonstrated in Figs. 3 and 4, andallows the compact AV node to be the site of WB, slow
AV Preexcitation(N = 7)
Posterior "SP"(N = 2)
Anterior "FP"(N = 13)
Compact AVN Node(N = 2)
2:1 AV Block Only(N = 17)
4:3 Block Observed(N = 8)
4:3 and 5:4 Block Observed(N = 3)
5:4 Block Observed(N = 2)
3:2 Block in Posterior SP(N = 186)
3:2 Block in Compact AV Node(N = 11)
3:2 WB Block Preceding 2:1 AV Block(N = 197)
Conduction Through Compact AV Node(N = 214)
Rabbit AV Junction PreparationsAH Conduction (N = 221)
No HA Conduction(N = 12)
SP Exit(N = 18)
FP Exit(N = 169)
Supernormal VA ConductionFP Exit - H-A < 10 msec - (N = 22)
Rabbit AV Junctional PreparationsHA Conduction (N = 221)
Fig. 1 Antegrade and retrograde conduction in the superfused rabbitAV junction—antegrade (AH; upper panel) and retrograde (HA; lowerpanel) conduction were evaluated in 221 consecutive superfusedrabbit AV junction preparations. Antegrade AH pre-excitation bypass-ing the compact AV node was present in seven preparations with AHWB mediated within the anterior slow pathway at paced cycle lengths<the cycle length producing high grade 3:1 or greater block in theextranodal pathway. In 17 of the remaining 214 preparations, AH WBwas not observed and only 2:1 AH block could be elicited withpacing. The 2:1 AH block was observed within the posterior/inferiortransitional cell input (slow pathway) in two preparations, the anterior(fast pathway) in 13 preparations, and within the compact AV node in
two preparations. AH WB (3:2) within the normal antegrade AVconduction pathway was predominately mediated by transitional cellsof the anterior slow pathway input with 3:2 WB rarely mediatedwithin the compact AV node (N=11). Although no retrograde HAconduction (N=12), earliest atrial activation from the anterior slowpathway (N=18), and retrograde activation via a rapidly conductingHis-fast pathway connection (N=22) were observed, each of thesuperfused rabbit AV junction preparations demonstrating stable 4:3and 5:4 WB also demonstrated earliest retrograde atrial activationposterior/inferior to the compact AV node along the fast pathway inputto the compact AV node
J Interv Card Electrophysiol (2010) 28:5–18 7
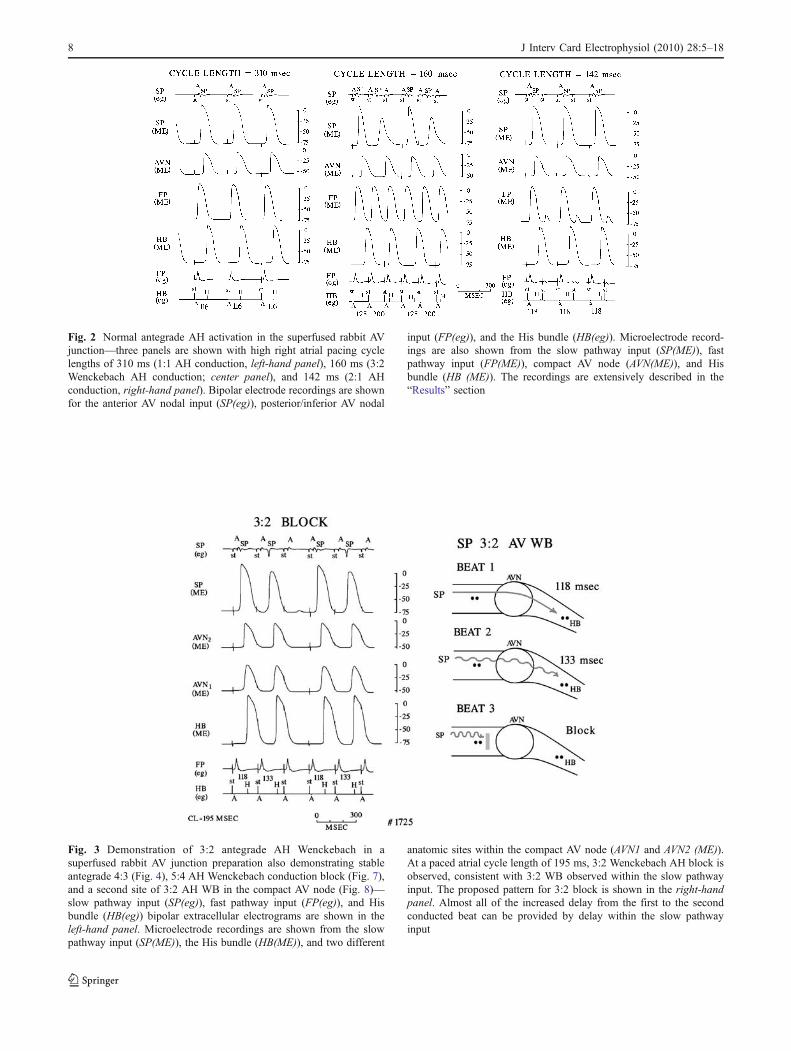
Fig. 2 Normal antegrade AH activation in the superfused rabbit AVjunction—three panels are shown with high right atrial pacing cyclelengths of 310 ms (1:1 AH conduction, left-hand panel), 160 ms (3:2Wenckebach AH conduction; center panel), and 142 ms (2:1 AHconduction, right-hand panel). Bipolar electrode recordings are shownfor the anterior AV nodal input (SP(eg)), posterior/inferior AV nodal
input (FP(eg)), and the His bundle (HB(eg)). Microelectrode record-ings are also shown from the slow pathway input (SP(ME)), fastpathway input (FP(ME)), compact AV node (AVN(ME)), and Hisbundle (HB (ME)). The recordings are extensively described in the“Results” section
Fig. 3 Demonstration of 3:2 antegrade AH Wenckebach in asuperfused rabbit AV junction preparation also demonstrating stableantegrade 4:3 (Fig. 4), 5:4 AH Wenckebach conduction block (Fig. 7),and a second site of 3:2 AH WB in the compact AV node (Fig. 8)—slow pathway input (SP(eg)), fast pathway input (FP(eg)), and Hisbundle (HB(eg)) bipolar extracellular electrograms are shown in theleft-hand panel. Microelectrode recordings are shown from the slowpathway input (SP(ME)), the His bundle (HB(ME)), and two different
anatomic sites within the compact AV node (AVN1 and AVN2 (ME)).At a paced atrial cycle length of 195 ms, 3:2 Wenckebach AH block isobserved, consistent with 3:2 WB observed within the slow pathwayinput. The proposed pattern for 3:2 block is shown in the right-handpanel. Almost all of the increased delay from the first to the secondconducted beat can be provided by delay within the slow pathwayinput
8 J Interv Card Electrophysiol (2010) 28:5–18

conduction, summation, and reentry. Pure 3:2 Wenckebachblock in the compact AV node is observed in Fig. 8.
3.4 Mechanism of 4:3 AH conduction block
Longitudinal dissociation within transitional cells of theposterior/inferior AV nodal input (slow pathway input; N=10) or the compact AV node (N=3) was an essentialrequirement for 4:3 WB. A 4:3 Antegrade AH Wenckebachconduction was observed during longitudinal dissociation,when 3:2 AH WB conduction was maintained within thefunctional AH conduction pathway and dissociated local1:1 activation was maintained within the second conductionpathway. AH activation for the first two beats of the four-beat pattern was maintained within the functional AHpathway demonstrating 3:2 WB and delayed AH conduc-tion. Antegrade penetration of the third beat of local 1:1activation into the functional AH conduction pathway wasallowed by block of the third atrial beat at a more proximalsite. Antegrade penetration (reentry) maintains antegradeAH conduction. Retrograde conduction of the reentrant beatAH activation prevents subsequent atrial activation of bothantegrade conduction pathways.
An example of 4:3 antegrade AH block mediated byreentry within the compact AV node is shown in Fig. 4. Themore common example of 4:3 AH WB mediated intransitional fibers of a longitudinally dissociated posterior/inferior slow pathway input is shown in Fig. 5. Althoughthe anatomic sites for 4:3 WB differ, it is a commonreentrant mechanism during sustained 3:2 WB that produ-ces 4:3 conduction block at both anatomic sites. A 3:2Wenckebach conduction block within the slow pathwayinput at a slightly longer cycle length than producing a 4:3Wenckebach conduction block at the same anatomic site isshown in Fig. 6.
3.5 Mechanism of antegrade 5:4 Wenckebach conductionblock
Longitudinal dissociation with the AV conduction axis,either within transitional cells of the posterior/inferior AVnodal input (slow pathway input; N=3) or the compact AVnode (N=3), was an essential requirement for 5:4 WB. Both4:3 and 5:4 WB can be observed during localized 3:2antegrade WB in one dissociated pathway providing AHconduction with 1:1 activation of a second dissociated
Fig. 4 Demonstration of 4:3 antegrade AH Wenckebach in asuperfused rabbit AV junction preparation—the present recordingsare from the same preparation as shown in Figs. 3, 7, and 8. At apaced atrial cycle length of 185 ms, local 2:1 block is present in theslow pathway input with 3° block to the compact AV node. Slowpathway activation occurs after activation of the compact AV node,demonstrating a shift in compact AV nodal activation from the slowpathway to the fast pathway input. Conduction within the compact AVnode is dissociated into two pathways, one demonstrating innate 3:2
WB (AVN1) and a second one maintaining 1:1 activation withconduction block to the His bundle (AVN2). Conduction of the third(fusion) beat results from the summation of AVN1 and AVN2pathways. The summation is dependent upon the delayed activationof the third beat of the AV Wenckebach pathway allowing reentry ofthe AVN1 pathway. Activation of both AVN1 and AVN2 pathways bythe third paced beat prevents antegrade activation of the compact AVnode by the fourth atrial paced beat
J Interv Card Electrophysiol (2010) 28:5–18 9

Fig. 5 A 4:3 WB within a dissociated slow pathway input in thesuperfused rabbit AV nodal preparation—localized reentry within adissociated slow pathway input—WB (4:3) is present at a paced atrialcycle length of 185 ms. The first and second conducted beats areassociated with slow pathway activation via SP2. The third conductedbeat results from reactivation of SP2 from the SP1 pathway. The thirdbeat of SP1 thus produces both antegrade activation of the compact
AV node and His bundle as well as retrograde activation of SP1preventing activation of both antegrade pathways by the fourth pacedatrial beat. Note that the more proximal SP electrogram is activated byall five atrial beats while antegrade block is observed in both SP1 andSP2, distal to the SP electrogram recording site. Recordings from thesame preparation during 3:2 AH WB are shown in Fig. 6
Fig. 6 A 3:2 WB within adissociated slow pathway inputin the superfused rabbit AVnodal preparation—–at a pacedatrial cycle length of 213 ms,longitudinal dissociation ispresent within the slow pathwayinput. The SP1 pathway micro-electrode (ME) and bipolarelectrogram (SP(eg)) demon-strate 1:1 activation with atrialpacing, with 3:2 AH WB deter-mined within the SP2 micro-electrode recording (ME2)).Most of the AH delay observedduring WB is determined withinthe slow pathway input, withlittle difference in the AVN1 andAVN2 microelectrode record-ings and His bundle activation(bipolar electrode HB(eg) andmicroelectrode (ME) recordings)for the first and second con-ducted beats
10 J Interv Card Electrophysiol (2010) 28:5–18

pathway. Although both 4:3 and 5:4 AH Wenckebach wereobserved in three preparations, 5:4 AH WB was observedin two preparations in the absence of stable 4:3 AH block.Each example of 3:2, 4:3, and 5:4 Wenckebach conductionblock demonstrated typical block, with successive progres-sion of AH intervals within a WB sequence (Table 1).
The longitudinal dissociation giving rise to 5:4 WB canoccur within either the compact AV node or the posterior/inferior AV nodal input. Progressive AH conduction delayduring the first and second paced atrial beats of a 5:4 AHconduction occurs via the functional AH pathway main-taining 3:2 AH WB. Summation of the third atrial pacedbeat is slowly conducted within the functional AHconduction pathway, producing antegrade AH activationwithout retrograde penetration along the functional AHconduction pathway. Even slower conduction of the next,fourth paced atrial beat along the AH conduction pathwayallows even later entrance of the dissociated 1:1 conductionpathway into the AH conduction pathway, this timeallowing both antegrade and retrograde penetration alongthe functional AH conduction pathway. Antegrade penetra-tion maintains AH activation of a fourth atrial paced beatwhile retrograde penetration terminates atrial activation ofboth antegrade conduction pathways. An example of 5:4AH WB observed in conjunction with dissociated conduc-tion pathways within the compact AV node is shown inFig. 7. Evidence for underlying 3:2 WB as a basis forreentry and 4:3 and 5:4 block is shown in Fig. 8 when aslightly longer paced cycle length demonstrates 3:2 AHWB within the compact AV node.
3.6 Mechanism of antegrade 4:2 conduction block (twoatrial beats producing his bundle activation followed by twoblocked beats)
A 4:2 conduction block (two consecutive atrial beatsconducted to the His bundle followed by two blocked atrialbeats) was observed in one preparation. The two conductedatrial beats were observed during 3:2 WB in the antegradeslow pathway input although the second dissociated slowpathway input conducted into and blocked within thecompact AV node. Evidence for this dissociated andblocked posterior/inferior AV nodal input is seen in SP2and NH2 microelectrode recordings in Fig. 9 at a pacedatrial cycle length of 180 ms, with subthreshold activation
of NH2 consistent with compact AV nodal activation via theSP2 input. At a slightly longer paced atrial cycle length of185 ms (Fig. 10), SP1 activation is maintained withantegrade conduction block apparent between the NHrecording of the compact AV node and the His bundle.Delayed activation of NH2 is observed with retrogradeactivation of the N region of the compact AVN (doublepotential of AVN recording). This retrograde activation ofthe compact AV node and slow pathway input preventsantegrade AH activation via both SP1 and SP2 slowpathway inputs. This is evidenced by the absence of bothmicroelectrode and bipolar electrogram recordings in theslow pathway recordings (Fig. 10).
4 Discussion
4.1 The functional and anatomic differentiation of tissuescontained within the AV junction
We have chosen the definition of the compact AV nodeused by Tawara [11]; a 1–2-mm oval whirl of irregularlyarranged fibers in the rabbit, located at the apex of thetriangle of Koch. We do not include the bridging fibers [11]or nodal extensions containing neurofilament [12] as part ofthe AV node. These are considered as AV nodal inputsbased upon both anatomic location and electrophysiologicproperties. Functionally, the compact AV nodal fibers (1)are more depolarized (a resting membrane potential≥62 mV), (2) have a smaller Vmax (<35 V/s), (3) have anaction potential amplitude (<62 mV with atrial stimulation),and (3) do not respond to intracellular stimulation(≤5,000 nA) [13, 14].
4.2 Previously proposed models of AV Wenckebachconduction
In a review article published in 1989 by Kinoshita andKonishi [15], three basic mechanisms were proposed toprovide for antegrade AV Wenckebach periodicity. We havekept the same elements, but slightly modified the proposedAV conduction pathway as follow; (1) inherently depressedexcitability and decremental conduction, (2) depressedconduction by incorporation of an inexcitable gap, or (3)localized longitudinal dissociation and reentry.
AH 1 (msec) AH 2 (msec) AH 3 (msec) AH 4 (msec)
3:2 Wenckebach block (N=197) 99±9 172±6 – –
4:3 Wenckebach block (N=11) 108±8 171±7 188±5 –
5:4 Wenckebach block (N=5) 90±9 137±10 162±11 186±12
Table 1 AH intervals duringperiodic Wenckebach block
J Interv Card Electrophysiol (2010) 28:5–18 11

Fig. 7 Demonstration of 5:4antegrade AH Wenckebach in asuperfused rabbit AV junctionpreparation—the present record-ings are from the same prepara-tion as shown in Figs. 3, 4, and8. At a paced atrial cycle lengthof 190 ms, 2:1 block is presentin the slow pathway input. Slowpathway activation occurs afteractivation of the compact AVnode, demonstrating a shift incompact AV nodal activationhas shifted from the slow path-way to the fast pathway input.Two AV nodal conduction path-ways are present. In the AVN2pathway, beats 1, 2, and 3 areblocked within the compactAVN. Beat 3 summates with thethird beat of the AVN1 pathway,activating the His bundle. Beat 4AVN1 also summates with beat4 AVN2, but penetrates retro-gradely to prevent activation ofboth AVN1 and AVN2 pathways(beat 5)
Fig. 8 A 3:2 AH WB within the compact AV node Wenckebach in asuperfused rabbit AV junction preparation—the present recordings arefrom the same preparation as shown in Figs. 3, 4, and 7. At a pacedatrial cycle length of 200 ms, 2:1 block is present in the slow pathwayinput. Slow pathway activation occurs after activation of the compactAV node, demonstrating a shift in compact AV nodal activation hasshifted from the slow pathway to the fast pathway input. Two AV
nodal conduction pathways are present. In the AVN1 pathway, beats 1,2, and 3 are blocked within the compact AVN. A 3:2 AH WB isdetermined at a second site within the compact AV node. The cyclelength and site of 3:2 AH WB are different for the same AV junctionpreparation (Fig. 3 and the present figure). Conduction is maintainedthrough the slow pathway input in Fig. 3 and through the fast pathwayinput in the present figure
12 J Interv Card Electrophysiol (2010) 28:5–18

4.3 Mechanism one—depressed excitabilityand decremental conduction
Depressed excitability and decremental conduction arewell-documented properties of isolated single rabbit AVnodal cells [16] and N cell recordings from the superfusedrabbit AV junction [4, 17, 18]. Progressive development of5:4 to 4:3 to 3:2 to 2:1 block in isolated rabbit AN cells[16] or 4:3 to 3:2 to 2:1 conduction block in the isolatedsuperfused rabbit AV junction [17] as well as in intactdennervated dog hearts in vivo [19] have been reported withsmall incremental decreases in the paced cycle length. Eachrhythm is observed over a narrow window of paced cyclelengths. Decremental conduction is also observed withinthe transitional cell inputs into the compact AV nodes [3, 4,7, 10, 13, 14] and may provide the most common anatomicsites for Wenckebach conduction block in the superfusedrabbit AV junction [3, 4, 10, 13] as well as the intact canineheart [6, 8, 14]. Although depressed cellular excitability iscapable of providing the decremental conduction needed toprogress from successively from 5:4 to 4:3 to 3:2 to 2:1periodic conduction block, the progression of conduction ismost reproducible within single cells Small beat-to-beatchanges in excitability resulting from autonomic influencesor cell-to-cell coupling may limit the reproducibility and
sustainability of complex Wenckebach patterns resultingfrom small beat-to-beat changes in excitability.
4.4 Mechanism two—conduction across an inexcitable gapwithin the AV conduction axis
The incorporation of an inexcitable gap within the AV axisis another mechanism capable of producing progressivecomplicated but stable patterns of AH Wenckebach period-icity. This mechanism has been extensively modeled andstudied in canine and sheep Purkinje fibers [20–22].Depressed excitability and post-repolarization refractorinessare common features of both mechanism one and mecha-nism two. Although the anatomic basis, the location, andthe electrophysiologic bases for the depressed excitability/decremental conduction observed with an incorporatedinexcitable gap can be clearly distinguished betweenmechanism one and two, an inexcitable gap may providea more stable foundation for a zone of depressed excitabil-ity that is less sensitive to small changes in autonomic toneor cell-to-cell coupling. Investigators have even proposedthat such an inexcitable gap may exist within the normalAV node [23]. Such a mechanism would however stillprovide for a progression from 5:4 to 4:3 to 3:2 to 2:1 blockoccurring as the atrial cycle length is incrementally
Fig. 9 A 3:2 block within the slow pathway input of a superfusedrabbit AV junction preparation demonstrating longitudinal dissociatedantegrade pathways extending into the compact AV node—electricalrecordings are from the same rabbit AV junction preparation as shownin Fig. 10. At a paced atrial cycle length of 180 ms, longitudinaldissociation is present within the anterior slow pathway input. A 3:2WB is present in one pathway (SP1), associated with 3:2 AHconduction. Dissociated 1:1 activation is present in the SP2 pathway.
Activation of both pathways can be seen in the bipolar electroderecordings from the slow pathway input (SP(eg)). The non-conductedsubthreshold potential observed within microelectrode potentialrecorded from the NH region of the compact AV node (NH2) suggestspenetration of one potential AH pathway into the compact AV nodeeven though no microelectrode recording associated with a separatepathway was recorded within the N cells of the compact AV node
J Interv Card Electrophysiol (2010) 28:5–18 13

decreased, but would be inconsistent with our observationsof 3:2 WB preceding 5:4 and 4:3 Wenckebach conductionblock as the paced atrial cycle length is reduced. Moreover,longitudinal dissociation and reentry can provide for theprogression of 3:2 to 4:3 to 4:2 conduction block asobserved in the superfused rabbit AV junction.
4.5 Mechanism three—longitudinal dissociationand localized reentry: a proposed model for 4:3 and 4:2conduction block in the superfused rabbit AV preparation
In 188 of 221 superfused rabbit AV junction preparations,the principal site of AV conduction block was provided bythe transitional cells of the posterior/inferior AV nodalinput. In 186 of 188 examples, AV conduction block wasinitially observed as 3:2 WB within transitional cells of theposterior/inferior AV nodal input. It is important to note theobservation that as the paced atrial cycle length is decreasedwithin the window of paced atrial rates producing 3:2 WBin the posterior/inferior AV nodal input (or analogouslywithin the compact AV node), the site of block moves to amore proximal site, towards the coronary sinus os. This hasbeen previously described for 3:2 WB within the posterior/inferior AV nodal input in the superfused canine AV
junction [7] as well as for 2:1 block observed within theanterior AV nodal input in the superfused [7], isolatedperfused [14], and intact canine heart in vivo [14]. Themore proximal movement of 3:2 WB is an essentialcomponent in the proposed reentry mechanism as it allowsthe distal penetration of 1:1 antegrade conduction within aparallel and dissociated transitional cell or AV nodalconduction pathway into the functional AH conductionpathway. The proximal movement of the site of block alsoallows retrograde activation of the same functional AHconduction pathway. Stable, complex forms of antegradeAH WB were not observed in an absence of (1) longitudinaldissociation and (2) co-existing 3:2 WB in one of the twodissociated antegrade AH conduction pathways.
Our proposed model for 4:3 conduction block is shownin the left-hand panel of Fig. 11. Essential characteristics ofthe model are:
1. Longitudinal dissociation of the slow pathway input orcompact AV node into two conduction pathways
2. A 3:2 conduction block within a functional AHconduction pathway and 1:1 conduction within asecond dissociated pathway that blocks and fails toconduct to the His bundle
Fig. 10 A 4:2 AH conduction block resulting from combined 3:2 WBand reentry within the compact AV node—electrical recordings arefrom the same rabbit AV junction preparation as shown in Fig. 9. At apaced atrial cycle length of 185 ms, longitudinal dissociation ispresent within the anterior slow pathway input. For the first threepaced atrial beats, 3:2 WB is present in one pathway (SP1) anddissociated 1:1 activation is present in the SP2 pathway. Unlike Fig. 9,at the longer cycle length, the slow pathway input does not determine3:2 AH block. A 3:2 block is determined within the compact AV node(AVN and NH2 microelectrode recordings). Reentry within the NH
region following the third atrial beat (which fails to conductantegradely to the His bundle) conducts retrogradely to the slowpathway input to extinguish atrial activation of the compact AV nodeand His bundle by blocking conduction of the fourth paced atrial beat.The site of 3:2 block progressed distally within the slow pathwayinput at an atrial cycle length of 185 ms (Fig. 10) vs. 180 ms (Fig. 9)as the action potential amplitude of the third paced atrial beat (SP2) isincreased and the bipolar electrode recording site now records bothSP1 and SP2 activation
14 J Interv Card Electrophysiol (2010) 28:5–18

3. Proximal movement of the site of 3:2 conduction blockas the paced cycle length is decreased allows more distalpenetration of 1:1 conduction from the non-functionalAH conduction pathway into the functional AH conduc-tion pathway following the blocked third beat
4. Antegrade penetration of the third atrial beat from thedissociated, non-functional conduction pathway intothe functional AH conduction pathway activates the Hisbundle while retrograde conduction within the samedissociated pathway prevents activation of both ante-grade pathways by the fourth atrial paced beat.
A 4:2 conduction block can occur by a similarmechanism to 4:3 conduction block (right-hand panel ofFig. 10). The difference between 4:3 and 4:2 block is based
upon the penetration of activation from the third pacedatrial beat of the dissociated pathway into the functionalAH conduction pathway conducting only retrogradely, withantegrade conduction block of the third atrial beat. The thirdpaced atrial beat thus fails to activate the His bundle, butconducts retrogradely to prevent activation of both antegradeconduction pathways by the fourth paced atrial beat.
4.6 Mechanism four—longitudinal dissociationand localized reentry: proposed model of 5:4 conductionblock in the superfused rabbit AV preparation
Our proposed model for antegrade 5:4 AH conduction isshown in the right-hand panel of Fig. 11. The proposedreentrant mechanism for 5:4 conduction block is similar to
Beat 1
Beat 2
Beat 3
Beat 4
Beat 5
4:3 Block 5:4 Block
Fig. 11 Diagrams demonstrating proposed patterns for 4:3 and 5:4block in the rabbit AV Junction—two proposed forms of uncommonAV WB are shown, 4:3 WB (left-hand panel) and 5:4 WB (right-handpanel). Both patterns are dependent upon (1) longitudinal dissociationwithin the slow pathway input or compact AV node and (2) 3:2 AVblock occurring within one of the two dissociated AV pathways. With4:3 WB, 3:2 WB with AH conduction is maintained within one of thetwo dissociated pathways. A 1:1 conduction is observed within thesecond dissociated pathway, with complete AH conduction blockobserved for the first two beats. Proximal block within the 3:2Wenckebach conduction block pathway is observed with the thirdatrial beat, allowing both antegrade and retrograde penetration fromthe 1:1 conduction pathway into the AH conduction pathway. Thispenetration into the AH conduction pathway results in antegrade AHactivation as well as retrograde conduction into both antegradeconduction pathways. This retrograde penetration extinguishes atrialactivation of both antegrade pathways by the fourth atrial beat,producing AH conduction block (left-hand panel). A 4:2 block, asobserved in Figs. 9 and 10, is similar to 4:3 WB, but is observed whenonly retrograde activation of the AH conduction pathway is observedwith the third atrial beat, and antegrade conduction block is observedfurther downstream in the AH conduction pathway. With 5:4 WB
(right-hand panel), 3:2 WB with AH conduction os maintained withinone of the two dissociated pathways, providing AH conduction of thefirst two atrial beats. For the first two beats, 1:1 activation failing topropagate is maintained within the second dissociated pathway. Slowconduction within the AH conduction pathway is observed with thethird atrial beat, summating with antegrade activation from thepreviously dissociated 1:1 conduction pathway. In the absence ofsummation from activation of the second dissociated pathway,conduction block would have occurred distal to entrance site forelectrical activity from the 1:1 conduction pathway, and 3:2 AH WBwould have been observed. Because summation of the two pathwayswas observed, retrograde penetration was not observed into eitheractivation pathway. Conduction of a fourth atrial beat is observed inboth activation pathways, with proximal conduction block observed inthe pathway previously demonstrating 3:2 block. More proximal blockin the AH conduction pathway allows both antegrade and retrogradepenetration from the 1:1 conduction pathway into the AH conductionpathway. The antegrade penetration into the AH conduction pathwayresults in antegrade AH activation and the retrograde penetrationextinguishes atrial activation of both antegrade pathways by the fifthatrial beat, producing AH conduction block (right-hand panel)
J Interv Card Electrophysiol (2010) 28:5–18 15

the proposed mechanism for 4:3 conduction block in (1) arequirement for two parallel dissociated antegrade conduc-tion pathways, (2) the maintenance of 3:2 conduction blockin the functional AH conduction pathway, and (3) 1:1conduction in a parallel activation pathway failing toconduct to the His bundle. A 5:4 Conduction block isobserved at shorter paced atrial cycle lengths than thoseproducing 3:2 AH conduction block. When 5:4, 4:3, and3:2 AH conduction block are each present, 5:4 AHconduction block is observed at a rate intermediate between3:2 conduction block and 4:3 conduction block, anobservation consistent with our proposed reentry mecha-nism and inconsistent with the progression of 5:4 to 4:3to 3:2 conduction block observed with mechanisms oneand two.
Atrial beats one and two with progressive delay areconducted to the His bundle by the same proposedmechanism for 4:3 and 5:4 block. A 3:2 AH Wenckebachis observed in a one dissociated, but functional AHconduction pathway with 1:1 activation maintained in asecond dissociated and non-functional AH conductionpathway. The more proximal site of 3:2 conduction blockin the functional AH conduction pattern at the shorter cyclelength than producing sustained 3:2 AH WB allows theantegrade penetration of 1:1 conduction from the dissoci-ated pathway into the functional AH conduction pathway,summating the electrical activity of both pathways with thethird atrial paced beat, and facilitating antegrade AHconduction of the third atrial beat that would otherwiseblocked. Critical timing of activation in the two pathwaysallow antegrade summation of activity for the third atrialbeat without permitting retrograde penetration into thefunctional AH conduction pathway. The fourth paced atrialbeat blocks even more proximal to the site of block foratrial beat three, allowing both antegrade and retrogradeconduction of the 1:1 conduction pathway into thefunctional AH conduction pathway. As observed with thethird atrial paced beat in 4:3 block, the fourth atrial beat in5:4 block conducts antegradely to activate the His bundleand conducts retrogradely to prevent antegrade activation ofboth antegrade activation pathways by the fifth atrial pacedbeat. The timing of 5:4 block allowing summation of thethird beat, antegrade and retrograde penetration of thefourth atrial paced beat is more critical than observed with4:3 block resulting in a smaller 5±0.7 ms window for 5:4block than the 12±2.3 ms window observed for 4:3conduction block (p<0.01). The windows for both uncom-mon forms of AH block are also smaller than the windowsproducing common 3:2 WB in the slow pathway input(26±2.7 ms; p<0.001 vs. 5:4 block, p<0.01 vs. 4:3 block).
We also proposed that the same mechanism of summa-tion and reentry providing for 5:4 block may produce 6:5,7:6, etc. patterns of Wenckebach AV block. The pacing
window would be smaller and homogenous conductionmore critical in maintaining the more complex patterns,leading to less stability. The small size of the availablecircuits in the rabbit compared to the dog and man may alsoprovide a less stable substrate for 6:5 and 7:6 AHconduction patterns in the rabbit.
4.7 Complex forms of AV Wenckebach conduction blockin man
In contrast to the common observation of 3:2 AHWenckebach conduction in the superfused rabbit AVjunction, stable 3:2, 4:3, and 5:4 AV Wenckebach conduc-tion block can be observed in normal human hearts. A 5:4WB and more complicated conduction blocks are mostoften “atypical” and do not fit a pattern of progressive beat-to-beat AV conduction prior to conduction block [24]. Ineach instance, in the present study in the rabbit, WB (3:2,4:3, and 5:4) was typical, with increased AH successiveconducted AH intervals prior to block.
In the rabbit, only 3:2 AH Wenckebach was a stable andcommon form of AH Wenckebach within the posterior/inferior AV nodal input. The 3:2 conduction block wasalmost exclusively due to slow, decremental conductionwithin the posterior/inferior AV nodal (slow pathway)input. A 4:3 WB was unusual and occurred only as aconsequence of longitudinal dissociation and localizedreentry within the posterior/inferior AV nodal input or thecompact AV node. In larger species such as man [24] andthe dennervated intact canine heart in situ [19], stable 4:3AH conduction block is a more commonly observedrhythm. The longer slow pathway input and larger compactAV node may facilitate the ability to maintain slowdecremental conduction, and allow larger temporal win-dows capable of sustaining prolonged 5:4 and 4:3 conduc-tion patterns with atrial pacing. Sustained 4:3 WB in therabbit may be possible only over a narrow range of cyclelengths that are, in a practical sense, unattainable. Smallbeat-to-beat variations in conduction velocity and conduc-tion pathway may further impinge on this small windowmaking sustained patterns of 4:3 block resulting fromdepressed excitability much more difficult to maintain than3:2 WB.
4.8 Clinical implications—reentry as a basis for WB in man
A 1:1 atria activation can be maintained with ventricularstimulation in humans [25] and the dog [26]. Decreasingthe paced ventricular cycle length initiates VAWenckebachconduction. As the retrograde AV conduction delay reachesa critical value, retrograde Wenckebach conduction isterminated by a reentrant ventricular beat. Concealedreentry contributes to retrograde Wenckebach conduction
16 J Interv Card Electrophysiol (2010) 28:5–18

block via a collision of the paced retrograde impulse andreentrant impulse within the AV node. Despite the presentevidence supportive of reentry as a basis for complicatedWB in the rabbit, it is uncertain if a similar mechanismcould be manifested during antegrade AH activation andprovide for more complicated Wenckebach conductionintervals presently attributed to slow, decremental conduc-tion within the posterior/inferior AV nodal (slow pathway)input and compact AV node in humans. Further investiga-tion would however appear warranted.
4.9 Limitations
The limited number of recording sites used in the presentstudies, especially true for a complex anatomic andfunctional structure such as the compact AV node, cannotprovide conclusive evidence of localized block and reentryas a basis for WB. The evidence for dissociation ofantegrade conduction into multiple pathways, the retrogrademovement of WB with a shortening of the paced cyclelength, and the abrupt termination of antegrade conductionof a subsequent beat to subthreshold activation are eachconsistent with the presented hypothesis of localizedreentry, and thus must be considered as a credibleexplanation for complicated patterns of WB observed inthe rabbit and other mammalian species.
5 Conclusion
The present results demonstrate (1) longitudinal dissocia-tion, (2) underlying 3:2 AH Wenckebach conduction, and(3) localized reentry within the antegrade AH conductionpathway as a basis for 4:3 and 5:4 Wenckebach conductionblock in the superfused rabbit AV junction. The reentrantprocess can be observed both within transitional fibers ofthe slow pathway input and within the compact AV node.The same processes observed in the rabbit may provide forsome complex forms of antegrade AV Wenckebach con-duction observed in man.
Acknowledgments Supported by a research grant from theAmerican Heart Association, Heartland Affiliate
References
1. Mobitz, W. (1924). Uber die unvollstandige storang der erren-gungsuberleitung zwischen vorhof und krammer des menschli-chen herzens. Zeitschrift für Die Gesamte Experimentelle Medizin,41, 180–237.
2. Scherlag, B. J., Lau, S. H., Helfant, R., Berkowitz, W. D., Stein,E., & Damato, A. N. (1969). Catheter technique for recording Hisbundle activity in man. Circulation, 39, 13–18.
3. Patterson, E., & Scherlag, B. J. (1999). Longitudinal dissociationwithin the posterior AV nodal input of the rabbit: a substrate forAV nodal reentry. Circulation, 99, 143–155.
4. Patterson, E., & Scherlag, B. J. (2001). Functional anatomy of AVconduction: changing concepts in the ablation era. Journal ofElectrocardiology, 34, 135–141.
5. Patterson, E., & Scherlag, B. J. (2004). Fast pathway-His bundleconnections in the rabbit heart. Journal of Interventional CardiacElectrophysiology, 10, 121–129.
6. Antz, M., Scherlag, B. J., Otomo, K., Pitha, J., Tondo, C.,Patterson, E., et al. (1998). Evidence for multiple atrio-A-V nodalinputs in the normal dog heart. Journal of CardiovascularElectrophysiology, 9, 395–408.
7. Patterson, S. B. J. (2002). Decremental conduction in the posteriorand anterior AV nodal inputs. J Interven Cardiac Electrophysiol,7, 137–148.
8. Hirao, K., Scherlag, B. J., Poty, H., Otomo, K., Tondo, C., Antz,M., et al. (1997). Electrophysiology of the atrio-nodal inputs andexits in the normal dog heart: radiofrequency ablation using anepicardial approach. Journal of Cardiovascular Electrophysiolo-gy, 8, 904–905.
9. Zhang, Y., Bharati, S., Mowry, K. A., Zhung, S., Tchou, P. J., &Mazgalev, T. N. (2001). His electrogram alternans reveal dual-wavefront input into and longitudinal dissociation within thebundle of His. Circulation, 104, 832–838.
10. Patterson, E., & Scherlag, B. J. (2002). Anatomic andfunctional fast atrioventricular conduction pathway. Journal ofCardiovascular Electrophysiology, 13, 945–949.
11. Tawara, S. (1906). Das reizleitungssytem des saugetierher-zens. Eine anatomisch-histologische studie uber das atrioven-trikularbundel und die purkinjeschen faden. Jena GustavFisher; translated Summa K, Shimada M, Imperial CollegePress.
12. Li, J., Greener, I. D., Inada, S., Nikolski, V. P., Yamamoto, M.,Hancox, J. C., et al. (2008). Computer three-dimensionalreconstruction of the atrioventricular node. Circulation Research,102, 975–985.
13. Antz, M., Scherlag, B. J., Patterson, E., Otomo, K., Tondo, C.,Pitha, J., et al. (1997). Electrophysiology of the right anteriorapproach to the atrioventricular node: Studies in vivo and in theisolated perfused dog heart. Journal of Cardiovascular Electro-physiology, 8, 47–61.
14. Patterson, E., & Scherlag, B. J. (2005). Delineation of AVconduction pathways by selective surgical transection: effects onantegrade and retrograde transmission. Journal of InterventionalCardiac Electrophysiology, 13, 95–105.
15. Kinoshita, S., & Konishi, G. (1989). Mechanisms of atypicalatrioventricular Wenckebach periodicity; a theoretical modelderived from the concepts of inhomogeneous excitability andelectronically mediated conduction. Journal of Electrocardiology,22, 227–233.
16. Hoshino, K., Anumonwo, J., Delmar, M., & Jalife, J. (1990).Wenckebach periodicity in single atrioventricular nodal cells fromthe rabbit heart. Circulation, 82, 2201–2216.
17. Watanabe, Y., & Dreifus, L. S. (1967). Second degree atrioven-tricular block. Cardiovascular Research, 1, 150–158.
18. Merideth, J., Mendez, C., Mueller, W. J., & Moe, G. K. (1968).Electrical excitability of atrioventricular nodal cells. CirculationResearch, 23, 69–85.
19. SImson, M., Spear, J. F., & Moore, E. N. (1978). Electrophysi-ologic studies on atrioventricular nodal Wenckebach cycles.American Journal of Cardiology, 41, 244–258.
20. Antzelevitch, C., & Moe, G. K. (1981). Electrotonically-mediateddelayed conduction and reentry in relation to “slow responses” tomammalian ventricular conducting tissue. Circulation Research,49, 1129–1139.
J Interv Card Electrophysiol (2010) 28:5–18 17

21. Antzelevitch, C., & Moe, G. K. (1983). Electrotonic inhibitionand summation of impulse conduction in mammalian Purkinjefibers. American Journal of Physiology, 245, H42–H53.
22. Davidenko, J. M., & Antzelevitch, C. (1986). Electrophysiologicalmechanisms underlying rate-dependent changes of refractorinessin normal and segmentally-depressed canine Purkinje fibers: thecharacteristics of pos-repolarization refractoriness. CirculationResearch, 58, 257–268.
23. Meijler, F. L., & Fisch, C. (1989). Does the atrioventricular nodeconduct? British Heart Journal, 61, 309–315.
24. Friedman, H. S., Gomes, J. A. C., & Haft, J. I. (1975). An analysisof Wenckebach periodicity. Journal of Electrocardiology, 8, 307–315.
25. Gallagher, J. J., Damato, A. N., Varghese, P. J., & Lau, S. H.(1973). Manifest and concealed reentry; a mechanism of A-Vnodal Wenckebach in man. Circulation, 47, 752–757.
26. Damato, A. N., Varghese, P. J., Lau, S. H., Gallagher, J. J., &Bobb, G. A. (1972). Manifest and concealed reentry; a mechanismof AV nodal Wenckebach phenomenon. Circulation Research, 30,283–292.
18 J Interv Card Electrophysiol (2010) 28:5–18