Embed Size (px)
Citation preview
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 1
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Stable Life Concepts
Applied Behavior Analysis (ABA)
Parent Intake Packet
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 2
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Table of Contents Welcome .................................................................................................................................................................. 4
Staff ......................................................................................................................................................................... 4
What is ABA? ........................................................................................................................................................................ 5
What Is Required To Start ABA Services? ................................................................................................................................ 6
Types of Services Stable Life Concepts Provides .......................................................................................................... 7
Center-based 1:1 Therapy .................................................................................................................................................... 7
Community based or school based 1:1 Therapy ................................................................................................................. 7
Home based 1:1 Therapy ...................................................................................................................................................... 7
Equine-Assisted ABA Therapy ............................................................................................................................................. 7
Functional Behavior Assessment (FBA) ............................................................................................................................... 7
Parent Training..................................................................................................................................................................... 7
Financial Information .................................................................................................................................................. 8
Rules and Regulations................................................................................................................................................ 8
Scheduling And Sessions ....................................................................................................................................................... 8
Absences, Vacations And Holidays .......................................................................................................................................... 8
Illness Policy .......................................................................................................................................................................... 9
Observation Of Client ................................................................................................................................................. 9
Medical Information .................................................................................................................................................. 10
Photography and Video ............................................................................................................................................ 10
Required Documentation........................................................................................................................................ 11
Insurance Rates of Service ..................................................................................................................................... 11
Cancellation Policy and Fees ................................................................................................................................. 11
Release Form .......................................................................................................................................................... 12
Service Agreement and Consent Form....................................................................................................................... 14
Services Offered .................................................................................................................................................................. 14
Appointments ...................................................................................................................................................................... 14
Confidentiality, Records, and Release Of Information .............................................................................................................. 14
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 3
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
To Protect Client From Harm ................................................................................................................................................. 14
Professional Consulatations .................................................................................................................................................. 15
Records .............................................................................................................................................................................. 15
Payment For Services .......................................................................................................................................................... 15
Health Care Insurance .......................................................................................................................................................... 15
Professional Records ........................................................................................................................................................... 15
Client Rights ........................................................................................................................................................................ 15
Contacting Us ...................................................................................................................................................................... 16
Consent .............................................................................................................................................................................. 16
Client Confidentiality Contact Form ............................................................................................................................ 17
Informed Consent For Services ................................................................................................................................. 18
Release, Indemnification and Hold Harmless Agreement for Transportation .......................................................... 19
Child Intake Questionnaire ........................................................................................................................................ 20
Child Information .................................................................................................................................................................. 20
School Information ............................................................................................................................................................... 20
Family Information ................................................................................................................................................................ 21
Types of Programs ............................................................................................................................................................... 22
Siblings ............................................................................................................................................................................... 22
Developmental History .......................................................................................................................................................... 23
Social Skills ......................................................................................................................................................................... 24
Self Care ............................................................................................................................................................................. 25
Daily Routines ..................................................................................................................................................................... 25
Allergies .............................................................................................................................................................................. 26
Medications ......................................................................................................................................................................... 26
Related Services .................................................................................................................................................................. 27
Behaviors of Concern ........................................................................................................................................................... 27
Extra-Curricular Activities ...................................................................................................................................................... 29
Appendix A: Permission Slips .................................................................................................................................... 30
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 4
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
PARTICIPANTS MEDICAL HISTORY & PHYSICIAN’S STATEMENT ......................................................................... 33
AUTHORIZATION FOR EMERGENCY MEDICAL TREATMENT ................................................................................ 34
Shining Star Program Waiver .................................................................................................................................... 37
Welcome Thank you for your interest in Stable Life Concepts ABA services. We hope that you will find all information helpful and are excited to be a part of your journey. Our primary focus is to provide your child and your family with quality services that are collaborative, innovative and all-encompassing. Integrity, safety, and accountability are of the utmost importance. Please review all information attached concerning Stable Life Concepts policies and procedures, processes, and services. Fill out all of the attached patient history and background information before the scheduled assessment in order to expedite the process. All information will be used to create an appropriate treatment plan that will allow for success now and in the future. If at any point you need assistance, please do not hesitate to contact us via phone call, text, or email. We look forward to working with you and and your child. Stable Life Concepts Staff
Staff Please feel free to contact any staff member below to begin services or ask questions pertaining to the process. Lindsey Emmons-Owner and Business Director 254-449-1405, [email protected] Stephanie Emmons-Owner, Clinical Director and Equine Services Director 512-800-2961,[email protected]
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 5
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
What is ABA? Applied Behavior Analysis (ABA) is an evidence-based approach to creating meaningful or socially significant behavior change. New skills and behaviors are taught while existing behaviors are modified. ABA focuses on behaviors that are observable and measurable, with respect to their function. This is determined through the collection of data that involves antecedents and consequences, which are events that occur directly before and after the behavior of interest. This approach utilizes principles of reinforcement, to increase skills that are functional and socially significant throughout the child’s daily life. ABA not only teaches these skills, but also promotes maintenance and generalization of the skills. ABA also serves to decrease behaviors that may interfere with learning, such as tantrums, aggression, or stereotypy. Treatment plans are developed to facilitate learning based on the individualized need of each child. Areas that we work on include (but are not limited to):
Language and Functional Communication: Communicating needs/wants to others
Independent Play: Playing alone without assistance
Social Skills: Interacting with others
Imitation: Imitating behaviors or vocalizations of others
Gross/Fine Motor Skills: Control over balance and body movement
Listener Responding: Attending and responding to spoken words
Visual/Perceptual Skills: Interpreting things he/she sees visually
Self-help Skills: Skills such as dressing, grooming, feeding, toilet training
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 6
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
What Is Required To Start ABA Services? 1. Completed Intake Packet: any other evaluations or reports would be helpful
2. Intake Interview
3. If insurance is involved then pre-authorization is required prior to any evaluation, therapy or other services being provided
4. Assessments completed by Stable Life Concepts and parents
5. Meeting with Clinical Supervisor to discuss treatment goals and program plan
6. Arrangement of therapy schedule
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 7
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Types of Services Stable Life Concepts Provides Center-based 1:1 Therapy Stable Life Concepts provides a center-based program in which basic skills are taught to each child to enhance learning. Each child participates in 1:1 sessions with a BCBA, BCaBA, or Registered Behavior Technician based upon his or her individual programming created by the BCBA.
Community based or school based 1:1 Therapy Once prerequisite skills are mastered in the center-based environment, these skills will be utilized and tested for generalization in the community and school environments.
Home based 1:1 Therapy To ensure all skills are generalized and parents and family members are able to successfully implement the plan at home, some in home based services will be recommended.
Equine-Assisted ABA Therapy Clients have the opportunity to work on current goals in a unique environment where skills will be demonstrated and tested with horses. An Equine Specialist and a variety of horses will be a part of this team. Horsemanship skills will be a part of this program.
Functional Behavior Assessment (FBA) This is designed for children who may have behaviors that are interfering with their ability to learn. An analysis of the behavior of concern will be completed via parent interview and direct observation. Once the analysis is conducted, a plan will be written to address the behaviors of concern. Parent Training All ABA services include a component of parent training. In order for center-based ABA therapy to have lasting effects, parents must assist the child with bringing the skills he or she learns at the center to other natural environments, especially in the home and community settings. Parent education and trainings will be available through Stable Life Concepts. Participation by parents, guardians, or caretakers is not only encouraged but expected for any program to be successful.
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 8
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Financial Information Stable Life Concepts is willing to participate with any major insurance provider in the State of Texas. We are currently working on Network Credentialing with the following providers: BCBS, Scott and White, United, Aetna, and Cigna. Please contact us to find out if we are currently providers for your insurance company. We also take self-pay. We accept payment via check or credit cards (Visa, MasterCard or Discover). All fees are based on the service performed including copays.
Rules and Regulations
Scheduling And Sessions Sessions for ABA therapy are typically scheduled in 2-3 hour blocks. The research demonstrates that longer sessions result in greater retention of skills and mastery is sustained. The parent or legal guardian is not required to be present during the therapy session but should arrive 10 minutes prior to the end of the session for consultation with the therapist. Please provide 30 days notice on significant changes to ABA scheduling in order to facilitate consistency in service delivery. This may include a request for change in schedule, long vacation, or termination of services. Sessions will involve direct services with the client, time to prep materials, data collection, and time to discuss the session with the parent.
Absences, Vacations And Holidays 1. I/We understand that in the event of inclement weather, all programs at Stable Life Concepts will follow the local
public school’s procedures. I/ We further understand that the Clinical Director has the discretion to cancel appointments due to exigent circumstances if needed even if the schools have not closed.
2. Stable Life Concepts has scheduled vacation and holidays where all services will be canceled. I/We understand
that we will be provided with a calendar of those scheduled days in advance. 3. I/We understand that requests for leaves of absence or extended vacation from the program must be submitted with
at least 30 days’ notice and will be reviewed by the Clinical Director. Upon approval, arrangements will be made on a case by case basis.
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 9
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Illness Policy 1. I/We understand that if my child’s temperature is at or above 100 degrees I/we will be contacted and that my/our
child will be required to be picked up.
2. I/We understand that my child must be fever free for a minimum of 24 hours before returning to therapy, without the aid of any fever reducing substance.
3. I/We understand the I/we will be called to pick up my child from therapy or home therapy sessions ended, if he/she has two (2) or more unexpected instances of diarrhea. I/We understand that my/our child will not be permitted to resume therapy until 24 hours have passed with no diarrhea instances.
4. I/We understand that I/we will be called to pick up my child from therapy or home therapy sessions ended, if he/she has one (1) or more instances of vomiting. I/We understand that my/our child will not be allowed to resume therapy until 24 hours have passed with no instances of vomiting.
5. I/We understand that I/we may bring my/our child to therapy if he/she has a common cold (slight occasional cough, clear runny nose, occasional sneezing). I/we further understand that if my/our child has discharge of any other color than clear, my/our child will not be seen for therapy.
6. I/We understand that if my/our child has any rash other than a mild diaper rash I/we must bring a not from the doctor stating the rash is not contagious.
7. I/We understand that by law my/our child is not permitted to be seen for therapy if he/she has contracted a communicable disease. Examples of communicable diseases are (but not limited to): Conjunctivitis (Pink eye), Impetigo, Hepatitis A, Scabies, Ringworm, Infections Diarrhea, Chicken Pox, Scarlet Fever, Lice, and Strep Throat. I/we understand that if my/our child is thought to have a communicable disease I/we will be contacted and that my/our child will not be permitted to be seen for therapy. I/we further understand that my/our child will not be permitted to attend therapy until a doctor’s note has been provided stating that my/our child is no longer contagious.
Observation Of Client 1. I/We understand that my/our child could be videotaped while receiving therapy from Stable Life Concepts for the
purpose of training staff members and/or receiving video updates on my/our child’s progress. I/We understand that any video will be kept confidential.
2. I/We understand that professionals, other clients, potential clients, staff, and therapists in training will occasionally be observing therapy. In these cases I/we will be informed of the purpose of the observation.
3. I/We understand that I/ We may view my/our child while he/she is receiving therapy. In addition I/we may be asked to observe procedures in order to promote generalization.
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 10
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Medical Information 1. I/We understand that I/we have agreed to release my/our child’s medical and psychological records to Stable Life
Concepts. Releasing these records will allow us Stable to review my/our child’s diagnosis, developmental, medical, levels of intellectual, behavioral, and social functioning as well as their medical history.
2. I/ We understand that I/we give Stable Life Concepts permission to seek medical assistance for my/our child in case of an emergency. Medical attention will be sought without my/our verbal permission if I/we are either unreachable, time is of the essence, or other unforeseeable circumstances arise.
3. I/we understand that there are medical conditions, as well as certain medications (such as insulin), that the staff of
Stable Life Concepts is not qualified to deal with and/or administer. If a medical condition arises that the staff is NOT able to handle, my child may not be able to be seen by the staff.
Photography and Video It is beneficial to use photographs and videos of the clients within the therapeutic setting. It can also be helpful to use client photographs and videos in presentations, educational materials, and trainings. Please indicate below your consent for Stable Life Concepts to take and use pictures and/or videos of your child for these purposes. Declining consent will not affect your access to therapy in any way.
Please Circle: Center Use Public Use
Declined Consent
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 11
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Required Documentation
Qualifying Diagnosis
Primary Care Manager Referral
IEP/504 (if applicable)
Authorization (Insurance)
Insurance Rates of Service
Assessment- $500.00
BCBA-$125.00 per hour
RBT-$50.00 per hour
Copays per policy Cancellation Policy and Fees If written notice for cancellation of a session is not received 24 hours prior to the scheduled session, documentation for a no call/no show will be applied. If more than 3 no call/no shows are documented, the fourth and any cancelation thereafter will result in a $50.00 fee. This ensures consistent and quality service are provided to our clients. Signature Agreement for Rules and Regulations of Stable Life Concepts: ______________________________________________ _____________________ Signature (Parent/ Guardian #1) Date ______________________________________________ _____________________ Signature (Parent/ Guardian #2) Date
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 12
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Release Form REQUEST/AUTHORIZATION TO RELEASE CONFIDENTIAL MEDICAL AND MENTAL HEALTH RECORDS AND INFORMATION
SOURCE OF INFORMATION Person or facility: ______________________________________________________________________ Address: ______________________________________________________________________ _______________________________________________ Phone #: ____-____-______ IDENTIFYING INFORMATION Name: ______________________________________________________________________ Address: ______________________________________________________________________ ______________________________________________________________________ Phone #: ____-____-______ DOB:_______________ Social Security #:______________ Parent/Guardian: ______________________________________________________________________ Address: ______________________________________________________________________ _______________________________________________ Phone #: ____-____-______ I hereby authorize the source named above to send the records marked below to Stable Life Concepts at the address listed above. ____ Inpatient or outpatient treatment records for physical and/or psychological, psychiatric, or emotional illness: ____ Psychological evaluation(s) or testing records, and behavioral observations or checklists completed by and staff member or by the client. ____ Psychiatric evaluations, reports, or treatment notes ____ Treatment plans, recovery plans, aftercare plans ____ Admission and discharge summaries ____ Social histories, assessments with diagnosis, prognoses, recommendations, and all similar documents ____ Information about how the client’s condition affects or has affected his or her ability to complete tasks, activities of daily living, or ability to work. ____ Workshop reports and other vocational evaluations and reports. ____ Billing records ____ Academic or educational reports ____ Report of teachers/staff observations ____ Achievement and other test results Other: ______________________________________________________________________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 13
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
I further authorize the source named above to speak by telephone with staff of Stable Life Concepts about the reasons for my/the client’s referral, and the relevant history or diagnosis, and other similar information that can assist with my/the client’s receiving treatment or being evaluated. _____________________________________ _______________________________ Signature Printed Name Date _____________________________________ _______________________________ Signature of parent/guardian Printed Name Date

400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 14
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Service Agreement and Consent Form This document contains important information about our professional services and business policies. It also contains summary information about the Health Information and Portability and Accountability Act (HIPPA), a federal law that provides privacy protections and client rights with regard to the use and disclosure of your Protected Health Information (PHI) used for the purpose of treatment, payment, and health care operations. HIPPA requires that we provide you with a Notice of Privacy Practices for use and disclosure of PHI for treatment, payment and health care operations. The Notice, which is attached to this Agreement, explains HIPPA and its application to your personal health information in greater detail. The law requires that we obtain your signature acknowledging that we have provided you with the information. Although these documents are long and sometimes complex, it is very important that you read them carefully and that you ask questions you have about the procedures at any time. When you sign this document, it will also represent an agreement between us. You may revoke this agreement in writing at any time. That revocation will be binding on us unless we have taken action in reliance on it; if there are obligation imposed on us by your health insurer in order to process or substantiate claims made under your policy; or if you have not satisfied any financial obligations you have incurred. If you have any questions or concerns, please feel free to discuss them with us.
Services Offered We will provide services specifically designed to help you and/or your minor child, or otherwise provide you with referrals to other professionals. Our behavioral services consist primarily of individual behavioral and skill assessments and short and long-term ABA service provision to youth in the autism spectrum but are not limited to those areas.
Appointments Except for rare emergencies, we will see your child at the time scheduled. We understand that circumstances (such as illness or family emergency) may arise which necessitate the occasional cancellation of appointments. In these cases, in order to avoid any misunderstanding, we ask that you give us as much notice as possible. This will allow us to offer your time to another person. You will be charged the standard hourly rate (see below) for appointments missed or canceled with less than 24 hours’ notice. Please note that most insurance companies will not reimburse you for missed appointments and you remain responsible for these charges. 75% attendance is required to maintain services. 3 or more no call/no shows will result in termination of services.
Confidentiality, Records, and Release Of Information All services are confidential except to the extent that you provide us with written authorization to release specified information to specific individuals, or under other conditions and us mandated by Texas and Federal law and our professional codes of conduct/ethics. These exceptions are discussed below.
To Protect Client From Harm If we have reason to suspect that a minor, elderly, or disabled person is being abused, we are required to report this (and any additional information upon request) to the appropriate state agency. If we believe that a client is threatening serious

400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 15
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
harm to him/herself or others, we are required to take protective actions which could include notifying the police, an intended victim, a minor’s parents, or others who could provide protection, or seek appropriate hospitalization.
Professional Consulatations Psychologists and Behavior Analysts routinely consult about cases with other professionals. In so doing, we make every effort to avoid revealing the identity of our clients, and any consulting professionals are also required to refrain from disclosing any information we reveal to them.
Records We will review all testing results during our feedback session, and offer you opportunities to ask questions and discuss the results with us. You will receive a written report that summarizes the findings. This report will include a summary and interpretation of all individual testing, as well as impressions from individual observations and consultations conducted as a part of a comprehensive individual evaluation. Upon your request, we are happy to provide you with a written summary of our impressions from other meetings, consultations, or observations as well.
Payment For Services If necessary, we may seek assistance from an outside party in order to collect payment for services rendered to you. In such cases, any disclosures are limited to the minimum that is necessary to achieve the purpose. Copays are the responsibility of the beneficiary.
Health Care Insurance If we do not file your insurance claims at this time, we will provide you with statements that you may submit to your insurance carrier or complete any forms as required by your insurance carrier in order to obtain reimbursement for out-of-network providers. In order to assist you with obtaining reimbursement for our services, your insurance carrier may require that we provide a clinical diagnosis, or additional clinical information such as treatment plans or summaries, copies of your child’s entire Clinical Record. In such situations, we will make every effort to release only the minimum information about you and your child that is necessary for the purpose requested. By signing this Agreement, you agree that we can provide requested information toyour carrier if/when you choose to file a claim for any services that we have provided to you or your child.
Professional Records You should be aware that, pursuant to HIPPA, we keep clients’ Protected Health Information in two sets of professional records. One set contains the Clinical Record and the other the professionals personal notes.
Client Rights HIPPA provides you with several rights with regards to your Clinical Record and disclosures of protected health information. These rights include requesting that we amend your records; requesting that we amend your record; requesting restrictions on what information from your Clinical Record is disclosed to others; requesting an accounting of most disclosures of
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 16
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
protected health information that you have neither consented to nor authorized; determining the location to which protected information disclosures are sent; having any complaints you make about your policies and procedures recorded in your records; and the right to a paper copy of the Agreement; the attached Notice Form, and our privacy policies and procedures.
Contacting Us Given their many professional commitments, our professionals are often not immediately available by telephone. If you need to leave a message, we will make every effort to return your call promptly (within 24-48 hours with the exception of holidays and weekends). If you are difficult to reach, please leave some times when you will be available.
Consent Your signature(s) below indicates that you have read the information in this document and agree to be bound by its terms, and that you have received the HIPPA notice from described above or have been offered a copy and declined. Consent by all parents/legal guardians (those with legal custody) is required. _____________________________________ ____________ Client/Child’s Name Date ___________________________________ _______________________________ Parent/Guardian #1 Name Parent/Guardian #2 Name ___________________________________ _______________________________ Parent/Guardian #1 Signature Parent/Guardian #2 Signature
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 17
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Client Confidentiality Contact Form Client confidentiality is a top priority for Stable Life Concepts. Therefore, it is important that you provide us with the following information to ensure there is no violation of your privacy. In the event that I, ____________________________________________, am unable to be reached, Stable Life Concepts may leave information with the following: _______Other Adult in Household (Name):_______________________________________ _______On Home Voice Mail (#): _____________________________________________ _______On Cell Phone (#): _________________________________________________ _______I may be reached at my work number: ___________________________________ _______May leave a message at work on my voice mail: _____________________________ _______Other: (Please describe): _____________________________________________ _______Text:____________________________________________________________ OPT OUT (Initials) ____________. In the event that I am unable to be reached, Stable Life Concepts MAY NOT leave information with anyone but myself. I understand that if the status of any of the above information changes, it will be my responsibility to inform the staff of Stable Life Concepts. Parent’s Signature: __________________________________ Date: ________________

400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 18
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Informed Consent For Services I, ______________________________, as a parent or guardian, give my consent for Stable Life Concepts to provide behavior analytic services to my child, _____________________________, in accordance with the ethical guidelines proposed by the Behavior Analytic Certification Board (BACB). I also understand that I may withdraw my consent and terminate treatment at anytime and for any reason. I understand that any information provided in this intake as well as any information obtained at any point during the interview process or course of treatment, is kept strictly confidential in accordance with HIPAA regulation guidelines and the law. I understand that Board Certified Behavior Analysts are bound to strict ethical guidelines of practice and that any issues of concern that may arise throughout the treatment process that are out of the behavior analyst’s area of experience may result in referrals to a more appropriate agency or individual. Signature: ______________________________________ Date: ___________________ Printed Name: ______________________________ Name of Client: _________________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 19
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Release, Indemnification and Hold Harmless Agreement for Transportation As a necessary and indispensable part of my being allowed to participate in Equine-Assisted ABA, community outings, field trips, and other necessary transportation sponsored by Stable Life Concepts, I do hereby agree and represent, on my behalf and on behalf of my heirs, personal and legal representatives, successors, assigns, employees, dependents, and associates as follows: I , ______________________________ willingly assume any and all risks and danger inherent with or incidental to myself and my minor child, ____________________________ participation in all sessions and travel to and from the stables, other community locations, or classes, and any and all activities in connection with any such activities sponsored by Stable Life Concepts. I understand and accept that accidents occur, although Stable Life Concepts will make every attempt to maintain the utmost safety for all parties involved. In any event and regardless of the nature of any injury, damage, or loss that I may suffer or that may accrue to the benefit of or damage to any of the persons named above, no claim or demand will be made on or against you, Stable Life Concepts, or on or against any of the agents, representatives, associates, employees, or contractors of Stable Life Concepts. I give permission for my child to be transported to and from the below activities by staff or contractors of Stable Life Concepts: ______Stables ______ School ______Community Outings ______ Medical Needs (Clinics/ER/Hospital) ______Field Trips ______Other This agreement is knowingly, willingly and freely given, and I fully understand and agree that it is a release and waiver of certain rights I may have and shall act as a complete bar against any claims that might otherwise be brought. I have been given a copy of this agreement, which I have read and I understand and acknowledge its terms. Its contents have also been explained to me. I understand the consequences of my signature to this agreement. Signature of Parent: ___________________________________ Date: ______________ Print Name: ___________________________________________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 20
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Child Intake Questionnaire The following questionnaire is to be completed by the child’s parent or legal guardian. This form has been designed to provide essential information before your initial appointment in order to make the most productive and efficient use of our time. Please feel free to add any additional information which you think may be helpful in understanding your child. Stable Life Concepts will hold information provided by you as strictly confidential and will only be released in accordance with HIPPA guidelines and as mandated by law. PLEASE PRINT
Child Information
School Information If your child has been in Special Education, please circle any of the following that they may have had:
504 Plan IEP
Psychological Evaluation
Behavior Intervention Plan Occupational Therapy Evaluation Physical Therapy Evaluation
Adaptive Technology Evaluation Speech Therapy Evaluation Other:
Child’s name: ______________________________________ DOB: _________________ Age: ____________ Male: ______ Female: ______ Address: _________________________ City: ______________ State: ____ Zip: _____ Phone: ______________________________________ Type: _____________________
School District: _______________________ Name of School: ______________________ Grade: ___________ Date enrolled: ________________ Date of IEP: _______________ Placement: _____ Mainstream _____ Inclusion _____ Resource ____ Other: ___________ Days and times of attendance: ________________________________________________ Teacher (s): _____________________________________________________________ Contact Information: _______________________________________________________ Did the teacher report any problems? (please explain): ____________________________________________________________________________________________________________________________________________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 21
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Family Information
Mother’s/guardian’s name: _________________________________________________ Occupation: ____________________________________________________________ Address (if different from client): ____________________________________________ City: _______________________ State: _____ Zip: _______ Phone: ________________________________________ Type: __________________ Email address: __________________________________________________________
Father’s/guardian’s name: _________________________________________________ Occupation: ____________________________________________________________ Address (if different from client): ____________________________________________ City: _______________________ State: _____ Zip: _______ Phone: ________________________________________ Type: __________________ Email address: __________________________________________________________
Marital status of parents: _____ Married _____ Separated _____ Divorced _____ Single Parent (s) with custody of child: _____________________________________________ Step-parents: __________________________________________________________ Was child adopted? ____ Yes ____ No Referred by: ___________________________________________________________
Insurance Provider:________________________________________________________ Provider Number: ___________________________ Contact Number: _________________ If Military: Sponsor _______________________________________________________ Sponsor Rank: ____________ Sponsor SSN: ____________________________________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 22
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Types of Programs (Please mark all that are of interest):
Siblings
Name Age Relationship Living
at Home
School Grade
OTHERS: Please list any others who currently live in your home.
Name Age Relationship Years Living in Home
Center-based ABA Therapy: _______ Home-based ABA Therapy: _______ Equine-Assisted ABA Therapy: _______ Social Skills Group Therapy: _______ FBA Only: ______ Consult with schools/other: _______
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 23
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Developmental History Please indicate the age at which your child did the following:
Milestone Age
Rolled over consistently
Sat up unsupported
Stood
Crawled
Walked unassisted
Said 1st word intelligible to strangers
Said two-three word phrases
Used sentences regularly
Toilet trained during the day
Dry through the night (6+ months)
Dressed self
Fed self
Colored
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 24
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
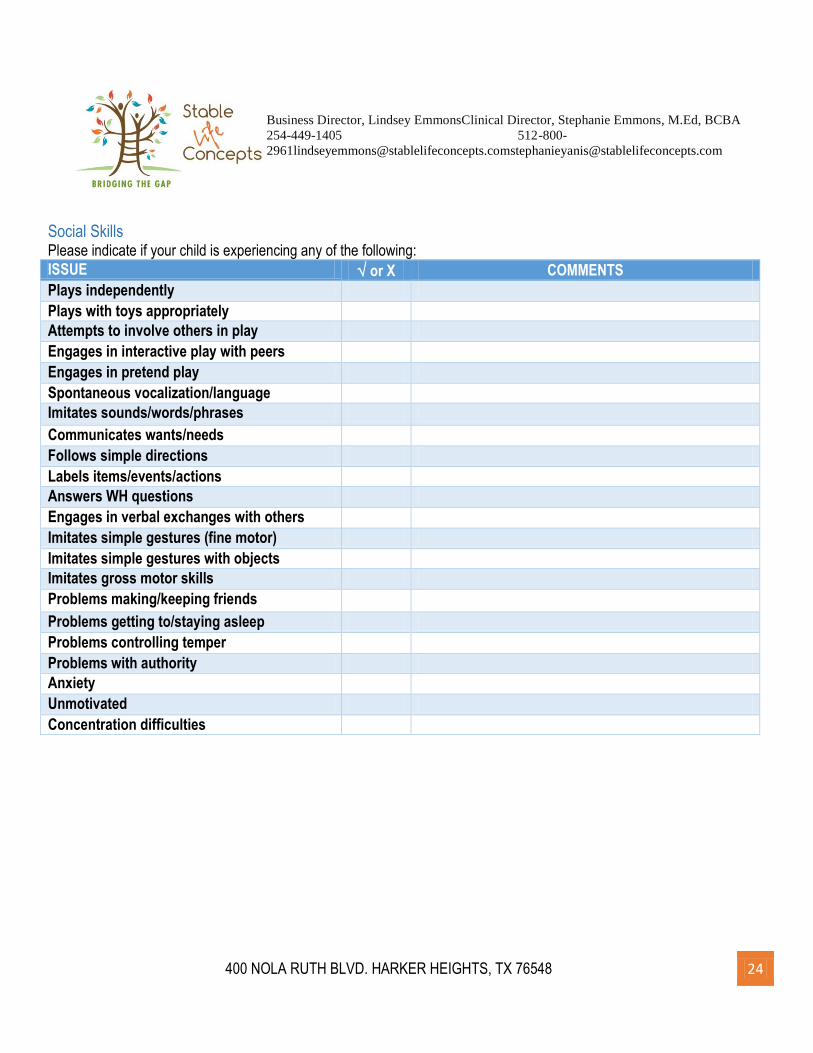
Social Skills Please indicate if your child is experiencing any of the following:
ISSUE or X COMMENTS
Plays independently
Plays with toys appropriately
Attempts to involve others in play
Engages in interactive play with peers
Engages in pretend play
Spontaneous vocalization/language
Imitates sounds/words/phrases
Communicates wants/needs
Follows simple directions
Labels items/events/actions
Answers WH questions
Engages in verbal exchanges with others
Imitates simple gestures (fine motor)
Imitates simple gestures with objects
Imitates gross motor skills
Problems making/keeping friends
Problems getting to/staying asleep
Problems controlling temper
Problems with authority
Anxiety
Unmotivated
Concentration difficulties
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 25
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
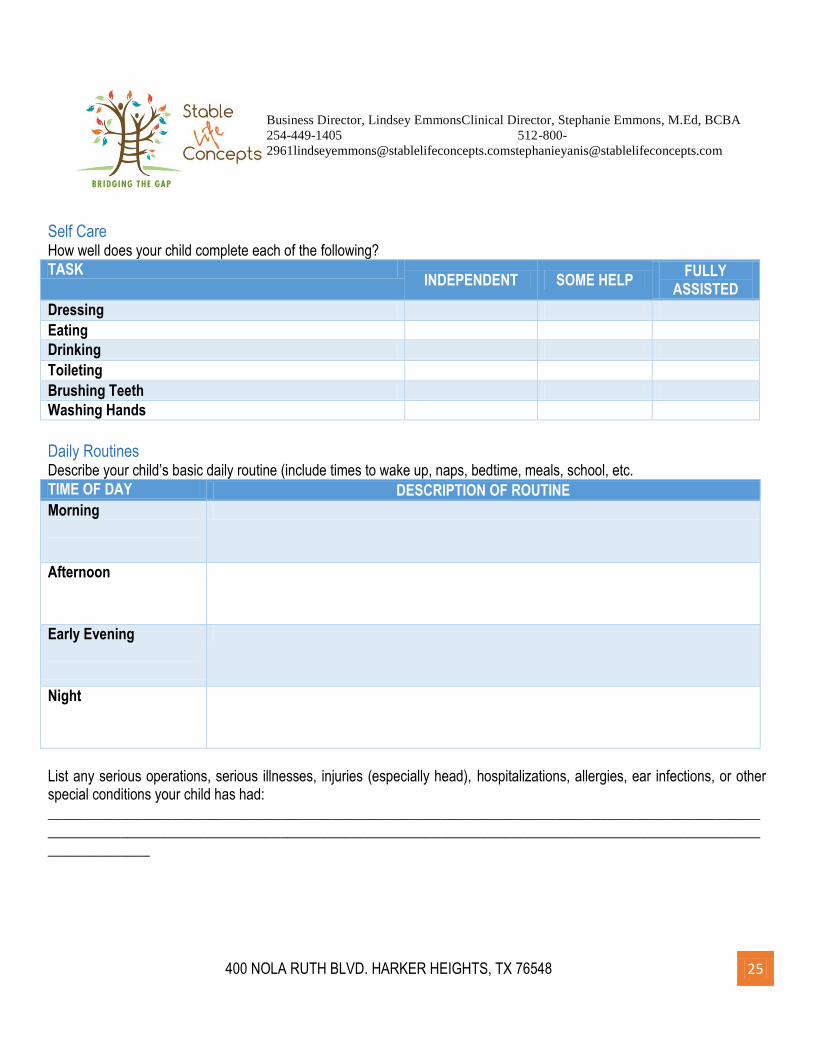
Self Care How well does your child complete each of the following?
TASK INDEPENDENT SOME HELP
FULLY ASSISTED
Dressing
Eating
Drinking
Toileting
Brushing Teeth
Washing Hands
Daily Routines Describe your child’s basic daily routine (include times to wake up, naps, bedtime, meals, school, etc.
TIME OF DAY DESCRIPTION OF ROUTINE
Morning
Afternoon
Early Evening
Night
List any serious operations, serious illnesses, injuries (especially head), hospitalizations, allergies, ear infections, or other special conditions your child has had: __________________________________________________________________________________________________________________________________________________________________________________________________________________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 26
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
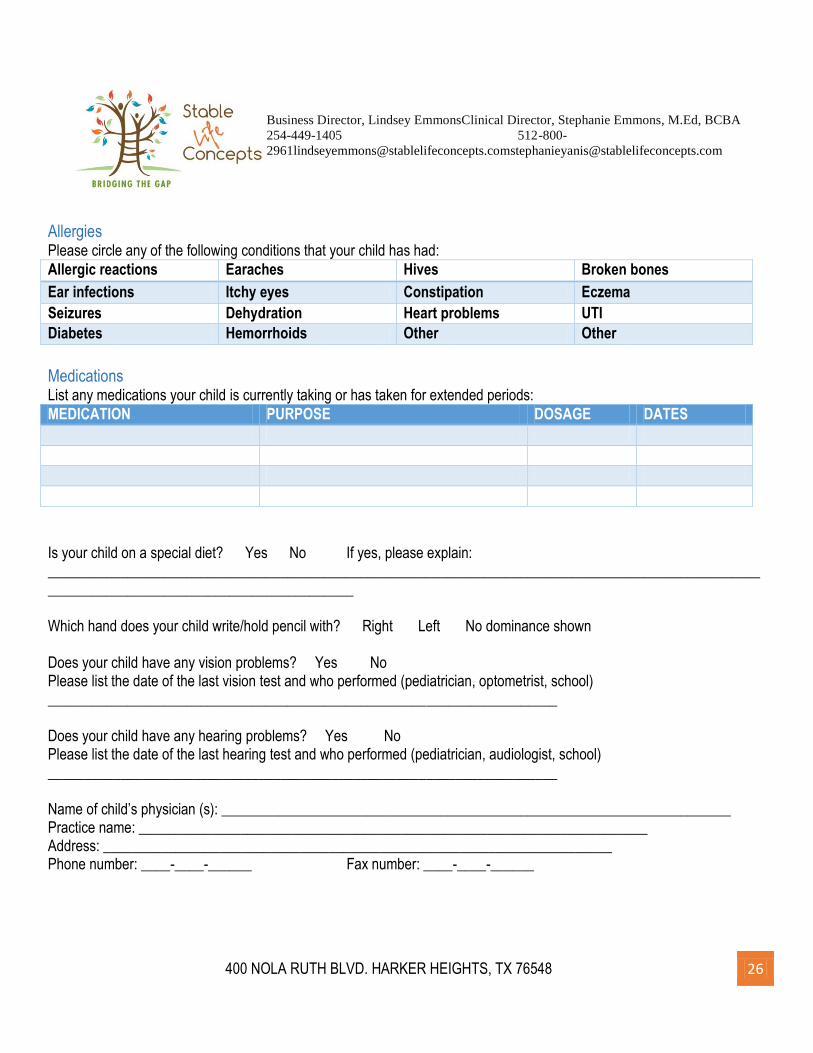
Allergies Please circle any of the following conditions that your child has had:
Allergic reactions Earaches Hives Broken bones
Ear infections Itchy eyes Constipation Eczema
Seizures Dehydration Heart problems UTI
Diabetes Hemorrhoids Other Other
Medications List any medications your child is currently taking or has taken for extended periods:
MEDICATION PURPOSE DOSAGE DATES
Is your child on a special diet? Yes No If yes, please explain: ____________________________________________________________________________________________________________________________________________ Which hand does your child write/hold pencil with? Right Left No dominance shown Does your child have any vision problems? Yes No Please list the date of the last vision test and who performed (pediatrician, optometrist, school) ______________________________________________________________________ Does your child have any hearing problems? Yes No Please list the date of the last hearing test and who performed (pediatrician, audiologist, school) ______________________________________________________________________ Name of child’s physician (s): ______________________________________________________________________ Practice name: ______________________________________________________________________ Address: ______________________________________________________________________ Phone number: ____-____-______ Fax number: ____-____-______
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 27
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
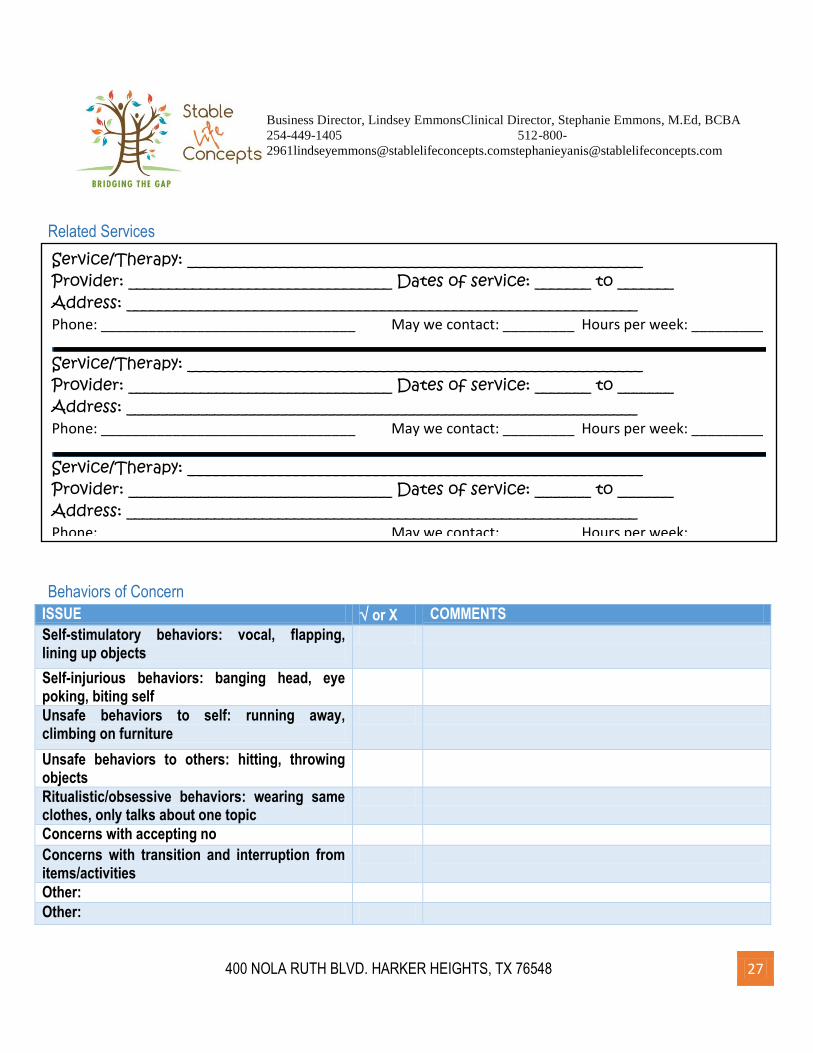
Related Services
Behaviors of Concern
ISSUE or X COMMENTS
Self-stimulatory behaviors: vocal, flapping, lining up objects
Self-injurious behaviors: banging head, eye poking, biting self
Unsafe behaviors to self: running away, climbing on furniture
Unsafe behaviors to others: hitting, throwing objects
Ritualistic/obsessive behaviors: wearing same clothes, only talks about one topic
Concerns with accepting no
Concerns with transition and interruption from items/activities
Other:
Other:
Service/Therapy: _________________________________________________________ Provider: _________________________________ Dates of service: _______ to _______ Address: ________________________________________________________________ Phone: ________________________________ May we contact: _________ Hours per week: _________
Service/Therapy: _________________________________________________________ Provider: _________________________________ Dates of service: _______ to _______ Address: ________________________________________________________________ Phone: ________________________________ May we contact: _________ Hours per week: _________
Service/Therapy: _________________________________________________________ Provider: _________________________________ Dates of service: _______ to _______ Address: ________________________________________________________________ Phone: ________________________________ May we contact: _________ Hours per week: _________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 28
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
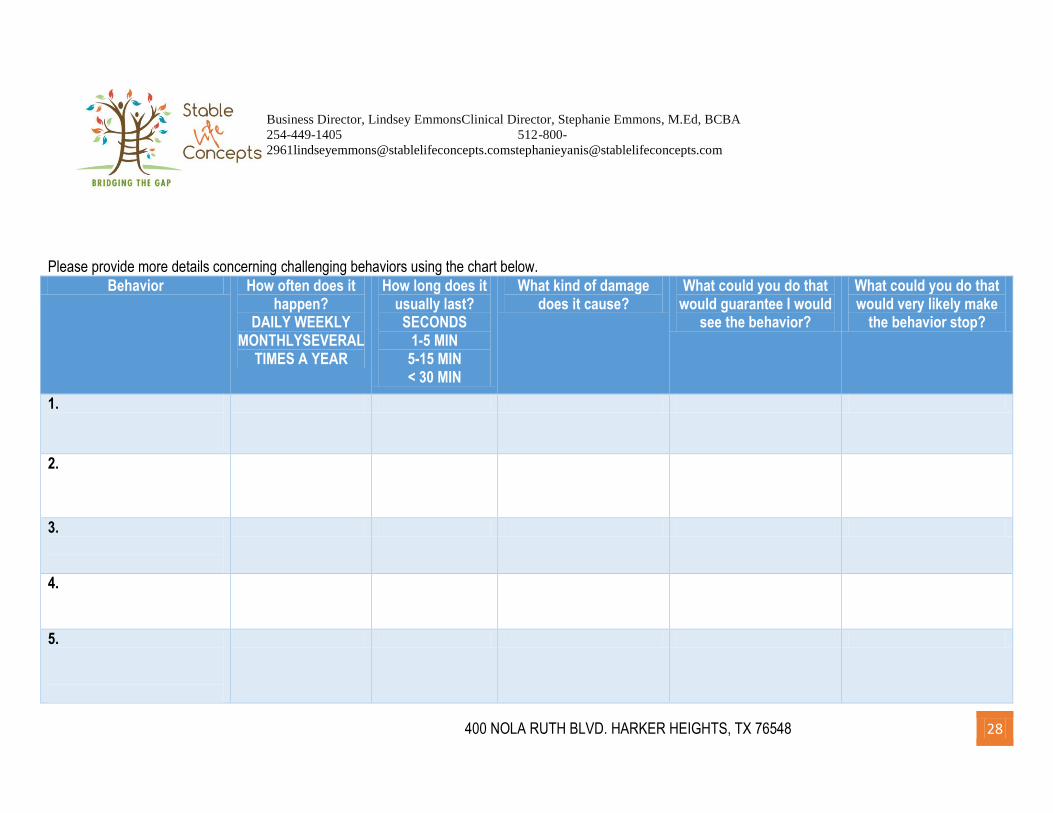
Please provide more details concerning challenging behaviors using the chart below.
Behavior How often does it happen?
DAILY WEEKLY MONTHLYSEVERAL
TIMES A YEAR
How long does it usually last?
SECONDS 1-5 MIN
5-15 MIN < 30 MIN
What kind of damage does it cause?
What could you do that would guarantee I would
see the behavior?
What could you do that would very likely make
the behavior stop?
1.
2.
3.
4.
5.
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 29
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Please list any fears or non-preferred items/activities your child may have: ____________________________________________________________________________________________________________________________________________ Please list any reinforcers your child may have: ____________________________________________________________________________________________________________________________________________
Extra-Curricular Activities Please indicate any extra-curricular activities, including sports, clubs, hobbies, lessons, etc.:
Football Karate Dance (Type)
Baseball Piano Music (Type)
Cheerleading Scouts Gymnastics
Basketball Soccer Other:
Any other information that may by useful: ______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 30
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Appendix A: Permission Slips
ACKNOWLEDGMENT AND ACCEPTANCE EQUINE ASSISTED ABA Equine Assisted ABA Therapy is experiential, offering clients a unique opportunity to be both mentally and physically involved in their own development. Participants learn about themselves and others by participating in activities with the horses, peers and therapists. Stable Life Concepts, LLC Equine-Assisted Therapy sessions are treatment team guided; a collaborative effort between a certified therapist, an Equine Specialist and horses to foster development in all areas for our clients. You will be provided suggestions and feedback from this treatment team. A certified therapist and equine specialist team are in the arena with the client making observations and providing feedback during the session and after the activity is completed. Please initial: _____________ By signing you are acknowledging that you understand and accept that the Equine Specialist present and involved during your child’s sessions is not a Board Certified Behavior Analyst but is certified through an equine specialty (EAGALA, CHA, OK Corral, PATH) and is a vital and functional part of your treatment team. Signature:________________________________________ Date: _____________ By signing you are acknowledging that you understood, accept and consent to the presence and involvement of an Equine Specialist during your child’s sessions. Signature:________________________________________ Date: _____________ This Equine Activity Liability Release, Waiver of Right to Sue and Assumption of All Risks Agreement (“this Agreement”) is hereby given by the undersigned (i) Stable Life Concepts LLC, any therapist representing Stable Life, (ii) to the sponsor as agent for and for the benefit of each owner of land upon which an equine activity to which this Agreement relates is conducted (“owner”), and (iii) to each partner, officer, agent, employee, subscriber, member, h ier, personal representative, successor and assign of the sponsor and of each owner (who also shall be included within the words “sponsor” or “owner” as their relationships may determine) and provides as follows: In consideration for the opportunities provided by the sponsor and each owner to the undersigned (including any minor in whose behalf the undersigned signs this Agreement) (the “participant”) for the enjoyment of equine activities as participant, the participant, including any minor participant for whom he signs this Agreement, hereby agrees as follows:
1. This Agreement is given in part under the Texas Equine Limited Liability Act (Section1. Title 4, Civil Practices and
Remedies Code, Chapter 87. Liability for Equine Activities.) as it may now provide or be hereafter amended (the
“Act”). All terms defined by the Act shall have the same meaning herein, and the Act is hereby incorporated in this
Agreement by reference. This Agreement shall be so construed as to provide to the sponsor and each owner the
fullest protections of a release, waiver of right to sue and assumptions of all risks that is afforded by the Act, by
other applicable statutes and by general law.
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 31
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
2. The participant hereby acknowledges that he has full and complete notice and understanding of the Act and of all
the risks inherent in equine activities which may cause, contribute to or result in the death or personal injury of the
participant or damage to the participant’s property (the “Risks”). These risks include, but are not limited to: (I) the
propensity of equines to behave in ways that may result in injury, harm, or death to persons on or around them; (ii)
the unpredictability of an equine’s reaction to such things as sounds, sudden movement, and unfamiliar objects,
persons, or other animals; (iii) certain hazards such as surface and subsurface conditions, (iv) collisions with other
animals or objects, (v) the potential of participant acting in a negligent manner that may contribute to injury to the
participants or others, such as failing to maintain control over the equine or not acting within the participant’s ability;
(vi) the propensity of an equine to behave in dangerous ways or to trip and/or fall, (vii) the inability of anyone
whomsoever to predict or foresee an equine’s reaction to excitement, weather conditions, sound, movements,
objects, vehicles, persons, animals, reptiles, birds or insects, and the effects of such reactions, (viii) the hazards of
surface or subsurface conditions, including but not limited to objects or conditions on, under or protruding from the
surface both latent and patent; (ix) the hazards which rocks, fences, trees, stumps, logs, bridges, ditches, bodies of
water, debris and obstacles, and any equine activity in connection therewith, may foreseeably or unforeseeably
present, (x) the dangers of being struck by an equine, (xiv) any negligent act or omission by the sponsor or any
owner which causes or results in the death or personal injury of the participant or damage to the participant’s
property; and (xi) all other risks associated with horses, [handling horses,] and related activities.
3. The participant hereby RELEASES and WAIVES all rights which he may have or hereafter have against the
sponsor and each owner for injury, loss, damage or death which is any way resulting from the intrinsic dangers of
equine activities and/or associated with Risks enumerated in Paragraph 2 above; he does hereby WAIVE his right
to sue or to bring any action against the sponsor and each owner in connection therewith; he agrees to INDEMNIFY
and DEFEND the sponsor and each owner from and to HOLD the sponsor and each owner HARMLESS against
any such suit or action including reimbursement of legal fees associated with the defense of any claim; and he
hereby expressly ASSUMES ALL RISKS AND DANGERS of injury, loss, damage or death which are in any way
resulting from the intrinsic dangers of equine activities and/or associated with the Risks enumerated in paragraph 2
above, including an act or omission that constitutes negligence for the safety of the participant by the sponsor, any
owner or any other person.
Please initial: ______________
4. The participant hereby authorizes and consents to any emergency medical care which may at the time appear
reasonably appropriate under the circumstances as a result of injury or sickness caused by or incurred in the
course of an equine activity.
5. This Agreement shall remain valid and in full force and effect from and after the date opposite the signature of the
Participant until expressly revoked by the Participant in a written notice personally delivered to the sponsor.
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 32
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
6. To the extent possible, this Agreement shall be construed in such manner as will render it, and each provision of it,
fully enforceable; but if any provision of this Agreement shall be unenforceable such provision (or so much thereof
as is unenforceable) shall be deleted and the remainder of this Agreement shall continue in full force and effect.
7. If the Agreement is executed by the undersigned for and on behalf of a minor participant named below, the
undersigned hereby warrants and represents that he is in fact the legal parent or guardian of such minor, with full
rights of custody and control; that this Agreement is given on behalf of and is intended to be binding upon said
minor participant, his heirs, personal representatives, successors and assigns; and the undersigned further agrees
that this Agreement shall also be as fully binding on the undersigned as if it were entered into solely on this own
behalf.
8. This Agreement shall be binding upon the heirs, personal representatives, successors and assigns of the
participant and the undersigned.
I HAVE FULLY READ AND FULLY UNDERSTAND THE FOREGOING EQUINE LIABILITY RELEASE, WAIVER
OF RIGHT TO SUE AND ASSUMPTIONS OF ALL RISKS. I HAVE CONSULTED AND RELIED UPON MY OWN
ADVISORS ON ALL QUESTIONS IN CONNECTION THEREWITH, AND I HAVE NOT RELIED UP THE
SPONSOR/PROFESSIONAL, ANY OWNER OR THE EQUINE ACTIVITY SPONSOR FOR ANY ADVICE OR
EXPLANATIONIN CONNECTION THEREWITH.
Print name: ___________________________________________
Signature:________________________________________ Date: _____________
FOR MINORS UNDER 18 YEARS OF AGE
Printed name of minor: __________________________________________________________
Printed name of Legal Guardian: ___________________________________________________
Signature of Parent or Legal Guardian: ______________________________________________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 33
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
PARTICIPANTS MEDICAL HISTORY & PHYSICIAN’S STATEMENT
Name: __________________________________________________________________
Address: __________________________________________________________________
Parent or Guardian: __________________________________________________________________
DOB: _______ Height: _______ Weight: _______ Tetanus Shot: Yes / No Date: _______
Current Medications: ____________________________________________________________
Please circle any of the following areas to indicate that the participant has a problem and/or surgeries in those
areas.
Allergies Auditory Visual Speech Cardiac Circulatory Pulmonary Diabetes
Muscular Orthopedic Learning Disability Neurological Mental/Psychological Impairment
Other: __________________________________________________________________
Special Precautions/Needs: __________________________________________________________________
I have filled out this medical information sheet to the best of my knowledge. I understand the Equine Assisted ABA
Therapy may be physically challenging and I take full responsibility for decided whether or not my minor child,
should participate. By signing this form, I am accepting the physical nature of EA-Therapy and am agreeing for my
minor child to participate.
Signature of Parent or Guardian: _________________________ Date: __________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 34
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
AUTHORIZATION FOR EMERGENCY MEDICAL TREATMENT
Physician’s Name: ________________________ Medical Facility: ____________________ Health Insurance Co: _____________________ Insured: ____________________ Policy #: __________ (please attach a copy of the front and back of your insurance card to this form) Allergies to medications: ______________________________________ If yes, please comment using back of form if necessary) Other allergies: ______________________________________________________________________ In the event of an emergency, contact: Name: __________________________ Relation: _____________ Phone: _____________ Name: _________________________ Relation: _____________ Phone: _____________ In the event emergency medical aid/treatment is required due to illness or injury during the process of receiving services, or while being on the property of the agency, I authorize Stable Life Concepts, agents and/or staff to:
1. Secure and retain medical treatment and transportation if needed; and
2. Release client records upon request to the authorized individual or agency involved in the medical emergency
treatment.
Consent Plan: This authorization includes x-ray, surgery, hospitalization, medication and any treatment procedure deemed “life saving” by the physician. This provision will only be invoked if the person(s) above is unable to be reached. Consent Signature: ________________________________________ Date: ___________ Client, Parent or Legal Guardian signed in the presence of program personnel. Program Personnel Initials: ___________________________ Date: _________________ Non-consent Plan: I do not give my consent for emergency medical treatment/aid in the case of illness or injury during the process of receiving services or while being on the property of the agency. In the event emergency treatment/aid is required, I wish the following procedures to take place: ______________________________________________________________________ Non-Consent Signature: ___________________________________ Date: ____________ Client, Parent or Legal Guardian signed in the presence or program personnel Program Personnel Initials: _______________________________ Date: ______________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 35
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Sunscreen Application Waiver
As the parent or guardian of ___________________________ I recognize that too much sunlight may increase my ch ild’s risk of getting skin cancer or other skin disorders in the future. Therefore, I give my permission for personnel at Stable life Concepts to apply a sunscreen product of SPF-15 or higher to my child, as specified below, when he or she will be playing outside. I understand that sunscreen may be applied to the exposed skin, including but not limited to the face, tops of the ears, nose and bare shoulders, arms and legs. Please check all of the following that apply: __ I do not know of any allergies my child has to sunscreen __ Staff may use the sunscreen of their choice following the directions and recommendations printed on the bottle. __ For medical purposes please do NOT apply sunscreen to the following areas of my child’s body: ____________________________________________________ __ My child is allergic to some sunscreen. Please only use the following brands: ____________________________________________________ __ I have provided the following sunscreen for use on my child: ____________________________________ Parent/Guardian Print: _______________________________ Parent/Guardian Signature: _______________________________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 36
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
SLC is pleased to announce the start of our social groups. Each social group will meet once a month for 2-3 hours. We will meet at the clinic for 30 minutes to complete a social skills lesson from the Social Thinking Curriculum. We will then proceed to a local community setting to work on the skills previously taught and current ABA goals in your child’s program. Each child will have a therapist to work with to ensure we maximize our time while on our community outing. We have some outings in mind, but please feel free to make suggestions should you like help in a certain setting. The therapists will provide transportation during this time. You may use that time to run errands or relax as we will take care of all needs during the social group sessions. During some sessions, we may offer parent training in which we will invite you to join us. SLC will cover most costs for the activities. If we choose a bigger outing, we may ask for assistance in paying for the outing. We will inform you in advance so you have time to make a decision on participation. We are excited to begin this new journey with all of you.
SLC Staff http://www.socialthinking.com/ Please sign the permission slip below and return to your child’s therapist.
I, ________________________, give my child, _________________________, permission to participate in the Social Skills group and all activities involved. My child, ___________________________, has permission to be transported by SLC staff during these sessions. ________________________________________ ____________________________ Signature Date Suggestions: _______________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________
400 NOLA RUTH BLVD. HARKER HEIGHTS, TX 76548 37
Business Director, Lindsey EmmonsClinical Director, Stephanie Emmons, M.Ed, BCBA
254-449-1405 512-800-
[email protected]@stablelifeconcepts.com
Shining Star Program Waiver
We are very excited to announce our Shining Star Program with Spotlight Dance Company. This program will allow children with special needs to participate in a dance class that will be held on a consistent basis. Dance classes will allow us to work on improving brain activity, strength and flexibility, making friends, body awareness, reducing anxiety, cultural awareness, providing a creative outlet and having FUN. If you have more questions about this program please don't hesitate to speak with one of us.
I, ______________________________, as a parent or guardian, give my consent for my child, _____________________________, to attend and participate in Shining Star Dance Classes with Spotlight Dance Company. I also understand that I may withdraw my consent and terminate at anytime and for any reason.
I understand that any transportation given by Stable Life Concepts was authorized in my signing of the Release, Indemnification and Hold Harmless Agreement for Transportation.
I understand and accept that accidents occur, although Stable Life Concepts will make every attempt to maintain the utmost safety for all parties involved. In any event and regardless of the nature of any injury, damage, or loss that I may suffer or that may accrue to the benefit of or damage to any of the persons named above, no claim or demand will be made on or against you, Stable Life Concepts, or on or against any of the agents, representatives, associates, employees, or contractors of Stable Life Concepts. Signature: ______________________________________ Date: ___________________
Printed Name: ______________________________ Name of Client: _________________





























