Embed Size (px)
Citation preview

ST. JOSEPH CENTER’S
CULINARY TRAINING PROGRAM
FREE professional cook training program
10-week program – 6 weeks in classroom and 4 weeks at externship placement Day classes (8 a.m. – 4 p.m.)
Hands-on culinary arts training in a new 1,500 square-foot teaching kitchen Classical French techniques in knife skills, stocks and sauces, cooking methods
Upcoming 2013 Start Dates: January 7, February 25, April 22, June 10
For more information and to download an application,
find the Culinary Training Program online at stjosephctr.org.
Call 310-396-6468 x355 or email [email protected] with questions.
204 Hampton Dr., Venice, CA 90291
St. Joseph Center’s Culinary Training Program
How to Apply to the Program
If you are eligible based on the program requirements and are interested in joining the program, please complete the application form (available for download on our website) in its entirety. Return your completed application to St. Joseph Center (ATTN: Culinary Training Program):
via email at [email protected],
via mail or in-person to 204 Hampton Drive, Venice, CA 90291, or via fax to 310-392-8042.
Upon receipt of your completed application, you will be contacted to schedule an in-person interview at St. Joseph Center. One interview date is held for each class, and the interview day includes group interviews, individual interviews, and kitchen practical interviews. A drug screen will be conducted as part of the application process. Please see below for application deadlines and program start dates. We accept applications year-round but are only able to schedule interviews for one class at a time.
Program Start Date Application Submission Deadline Monday, January 7, 2013 Monday, December 10, 2012 Monday, February 25, 2013 Monday, February 4, 2013 Monday, April 22, 2013 Monday, April 8, 2013 Monday, June 10, 2013 Monday, May 20, 2013 Monday, July 29, 2013 Monday, July 8, 2013 Monday, September 16, 2013 Monday, August 26, 2013 Monday, November 4, 2013 Monday, October 14, 2013
More information, including FAQs for applicants, is available on our website:
www.stjosephctr.org Click on “Programs” then “Culinary Training Program”
Contact us at 310-396-6468 x355 or [email protected] with questions.
ST. JOSEPH CENTER’S CULINARY TRAINING PROGRAM
Location: 204 Hampton Drive, Venice, CA 90291
310-396-6468 x355 – to apply for the program 310-396-6468 x354 –for Program Manager
Length of Program: 10 weeks Fees: No tuition; small cost of chef uniform. Applicants do not need a high school diploma or GED to participate in the program.
PROGRAM ELIGIBILITY REQUIREMENTS:
o Drug/alcohol free environment. Individuals invited to the orientation must have 90 days clean and sober at that time. You will be drug tested during the application process, and you must hold yourself accountable for drug testing at any point during the program. We do not recognize the use of medical marijuana.
o You will be required to disclose information concerning your legal history for externship
placement. No major crimes of violence with weapons, sexual assaults, terrorist or arsonist threats, identity theft, or warrants for arrest will be considered.
o Must be housed and able to maintain residence at same address throughout the 10 week program. o Able to read and write in English.
o Individuals must be at least 18 years old.
o Must be unemployed or underemployed.
o Valid CA driver’s license or CA I.D. card & valid Social Security card.
o Completion and written proof of tuberculosis test taken in the past six months (upon acceptance to the program).
o Must be in good enough physical condition to stand, move, bend, twist, kneel, and comfortably lift 50 lbs.
o Must be motivated to work and have an interest in the food service industry.
The interview takes place during the week preceding the start date of the program.
CLASS HOURS: (6 Weeks) Student must be available between 8:00 a.m. & 4:00 p.m. Monday to Thursday Monday 12:30 to 4:00 (unless you are scheduled for kitchen practicum at 8:00) Tuesday 12:30 to 4:00 (unless you are scheduled for kitchen practicum at 8:00) Wednesday 12:30 to 4:00 (unless you are scheduled for kitchen practicum at 8:00) Thursday 10:00 to 4:00 (unless you are scheduled for kitchen practicum at 8:00) Friday No Class (4 Week Externship/ 80 hours) Monday to Friday (4 hours each day) Hours vary depending on externship site. Some sites begin at 7:00 a.m.
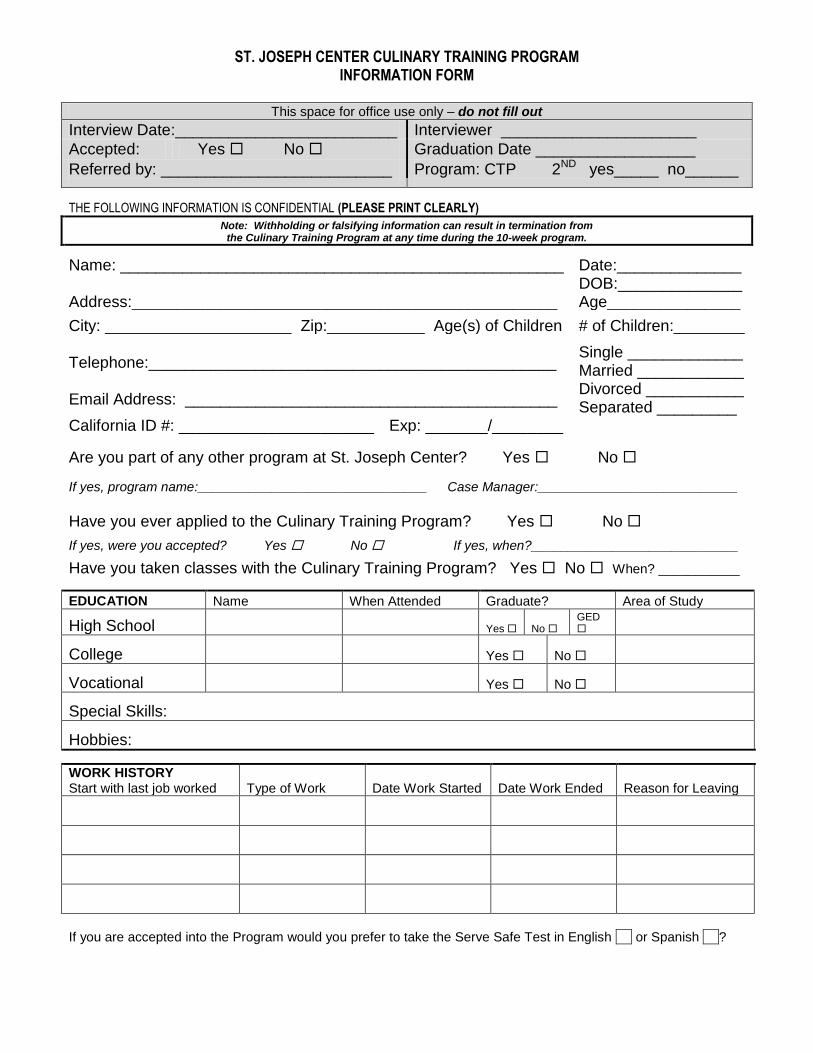
ST. JOSEPH CENTER CULINARY TRAINING PROGRAM INFORMATION FORM
This space for office use only – do not fill out
Interview Date:_________________________ Interviewer ______________________
Accepted: Yes No Graduation Date __________________
Referred by: __________________________ Program: CTP 2ND yes_____ no______
THE FOLLOWING INFORMATION IS CONFIDENTIAL (PLEASE PRINT CLEARLY) Note: Withholding or falsifying information can result in termination from
the Culinary Training Program at any time during the 10-week program.
Name: __________________________________________________ Date:______________
Address:________________________________________________ DOB:______________ Age_______________
City: _____________________ Zip:___________ Age(s) of Children # of Children:________ Telephone:______________________________________________ Email Address: __________________________________________
Single _____________ Married ____________ Divorced ___________ Separated _________ California ID #: ______________________ Exp: _______/________
Are you part of any other program at St. Joseph Center? Yes No
If yes, program name:_______________________________ Case Manager:___________________________
Have you ever applied to the Culinary Training Program? Yes No
If yes, were you accepted? Yes No If yes, when?____________________________
Have you taken classes with the Culinary Training Program? Yes No When? ___________
EDUCATION Name When Attended Graduate? Area of Study
High School Yes No GED
College Yes No
Vocational Yes No
Special Skills:
Hobbies:
WORK HISTORY Start with last job worked Type of Work Date Work Started Date Work Ended Reason for Leaving
If you are accepted into the Program would you prefer to take the Serve Safe Test in English or Spanish ?
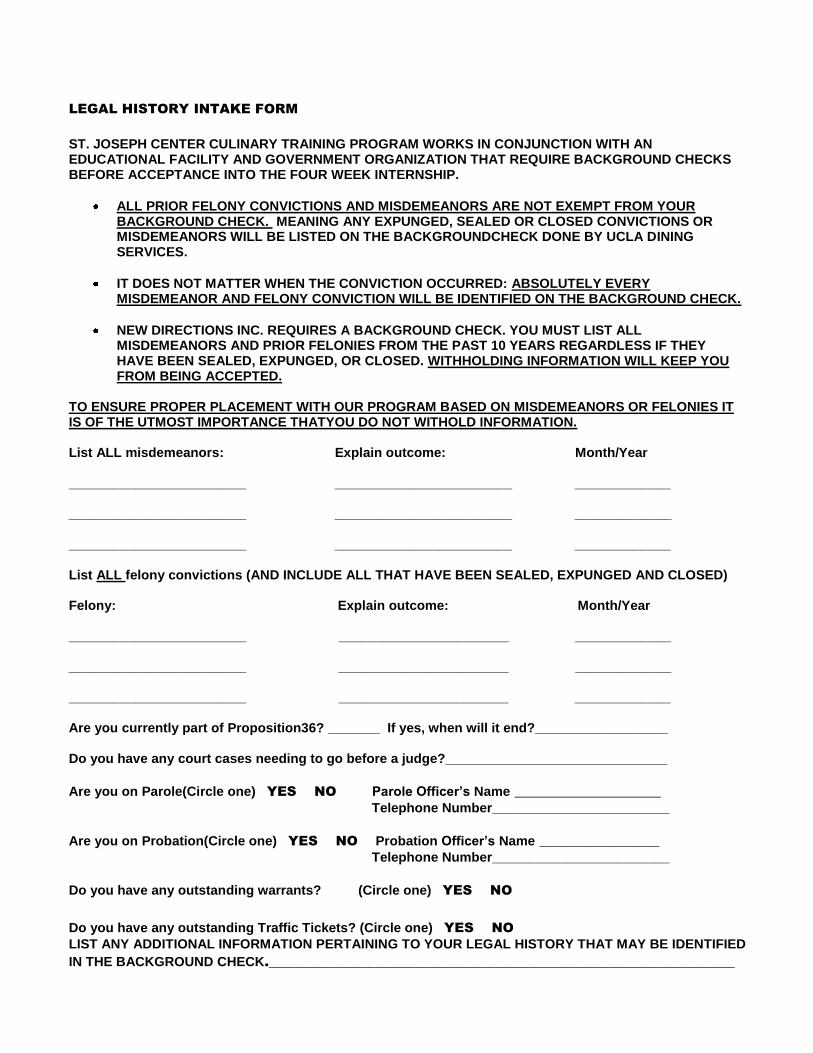
LEGAL HISTORY INTAKE FORM
ST. JOSEPH CENTER CULINARY TRAINING PROGRAM WORKS IN CONJUNCTION WITH AN EDUCATIONAL FACILITY AND GOVERNMENT ORGANIZATION THAT REQUIRE BACKGROUND CHECKS BEFORE ACCEPTANCE INTO THE FOUR WEEK INTERNSHIP.
ALL PRIOR FELONY CONVICTIONS AND MISDEMEANORS ARE NOT EXEMPT FROM YOUR BACKGROUND CHECK. MEANING ANY EXPUNGED, SEALED OR CLOSED CONVICTIONS OR MISDEMEANORS WILL BE LISTED ON THE BACKGROUNDCHECK DONE BY UCLA DINING SERVICES.
IT DOES NOT MATTER WHEN THE CONVICTION OCCURRED: ABSOLUTELY EVERY MISDEMEANOR AND FELONY CONVICTION WILL BE IDENTIFIED ON THE BACKGROUND CHECK.
NEW DIRECTIONS INC. REQUIRES A BACKGROUND CHECK. YOU MUST LIST ALL MISDEMEANORS AND PRIOR FELONIES FROM THE PAST 10 YEARS REGARDLESS IF THEY HAVE BEEN SEALED, EXPUNGED, OR CLOSED. WITHHOLDING INFORMATION WILL KEEP YOU FROM BEING ACCEPTED.
TO ENSURE PROPER PLACEMENT WITH OUR PROGRAM BASED ON MISDEMEANORS OR FELONIES IT IS OF THE UTMOST IMPORTANCE THATYOU DO NOT WITHOLD INFORMATION. List ALL misdemeanors: Explain outcome: Month/Year ________________________ ________________________ _____________ ________________________ ________________________ _____________ ________________________ ________________________ _____________ List ALL felony convictions (AND INCLUDE ALL THAT HAVE BEEN SEALED, EXPUNGED AND CLOSED) Felony: Explain outcome: Month/Year ________________________ _______________________ _____________ ________________________ _______________________ _____________ ________________________ _______________________ _____________ Are you currently part of Proposition36? _______ If yes, when will it end?__________________ Do you have any court cases needing to go before a judge?______________________________
Are you on Parole(Circle one) YES NO Parole Officer’s Name ______________________
Telephone Number________________________
Are you on Probation(Circle one) YES NO Probation Officer’s Name __________________
Telephone Number________________________
Do you have any outstanding warrants? (Circle one) YES NO
Do you have any outstanding Traffic Tickets? (Circle one) YES NO
LIST ANY ADDITIONAL INFORMATION PERTAINING TO YOUR LEGAL HISTORY THAT MAY BE IDENTIFIED
IN THE BACKGROUND CHECK.______________________________________________________________________
Why are you unemployed now? ___________________________________________________________ How long have you been unemployed? Months________ Years _________
Have you ever been fired? Yes No Explain:____________________________________
Have you attended or been referred to anger management classes in the past? Yes No
Explain: __________________________________________________________________________
INCOME - What is the source of your income?
Unemployment Benefits Yes No
Due to end (date): ____________________________________________
Program – circle one GAIN GR GROW SSI Dept of Aging (Title V) AFDC
Other – please specify ___________________________ Case manager__________________________________
Address ______________________________________ City ________________________________ Zip _______
Phone _______________________________________ FAX __________________________________________ When did income from this program begin? _________________________________
Will you continue to receive benefits during the 10 weeks of the program? Yes No
If not receiving income from one of the above programs, what will be source of income during class?
Employed? Yes No Supported by someone else? Yes No Your annual income_______________________ Your Spouse’s Income_________________________ If you live (and are supported by your parents) what is their combined income? _________________________
HOW DO YOU FEEL ABOUT MINIMUM WAGE? ___________________________________________________________________________________________ ___________________________________________________________________________________________
MEDICAL HISTORY
Do you plan to have any surgery within the next year? Yes No When? ______________
Do you plan to have any dental work within the next year? Yes No When? ______________
Previous Hospitalizations
____________________________________________ Date ______________
____________________________________________ Date ______________
____________________________________________ Date ______________
Physical Therapy
Date _____________ Condition ___________________________________________
Date _____________ Condition ___________________________________________
Currently working with physical therapist? Yes No
Back Injuries Yes No Explain___________________________________________________
Workers Comp Yes No Explain ___________________________________________________
Physical Limitations Yes No Explain ___________________________________________________
Work Restrictions Yes No Explain ___________________________________________________
Current Meds Yes No Explain ___________________________________________________
HISTORY OF PAST ILLNESS/INJURY – CIRCLE EACH ILLNESS/INJURY YOU HAVE HAD
Mumps
Chicken Pox
Broken Bones
Shingles
Mononucleosis
Sprains/dislocations
Meningitis
Scarlet Fever
Lacerations
(extensive)
Heart Disease
Heart Attack
Concussions
High Blood Pressure
Stroke
Knocked out
Diabetes
Thyroid Disease
Other Serious Injury
Anemia
Cancer
Auto Accident
Arthritis
Migraine Headaches
Feet (fallen arches)
Seizures
Nervous Breakdown
Bronchitis
Asthma
Hives/Hay fever
Hepatitis A
Hepatitis B
Comments for circled illnesses/injuries: ___________________________________________ ___________________________________________________________________________
Do you feel that you are physically able to work in a kitchen? (CIRLCE ONE) YES NO List any physical activities that you do________________________________________________________________________________
__________________________________________________________________________________________________________________________
MENTAL HEALTH HISTORY
Have mental health issues (depression, schizophrenia, etc.) prevented you from working in the past? Yes No
Have you ever been diagnosed with a mental illness? Yes No
If yes, are you currently under case management? Yes No
How long have you been under case management? _____________________________________________________________
Where do you receive case management? _____________________________________________________________
Mental Health case manager: ______________________________________ Tel. (______) _________ - ______________
Psychological Medication/s:
_____________________________ Prescribed for: _________________________________
_____________________________ Prescribed for: _________________________________
_____________________________ Prescribed for: _________________________________
Note: You must agree to stay under the care of your mental health case manager and agree to take all prescribed medication/s to be able to continue in the Culinary Training Program.
ALCOHOL AND DRUG USE
Do you drink alcohol? Yes No If yes, how much/how often? _______________________________
If no, are you in recovery? Yes No Time sober ________ Years _____ Months _____ Days ______
Have you ever used drugs? Yes No If yes, how much/how often? ______________________________
If yes, are you in recovery? Yes No Time clean __________Years _____ Months ______ Days _____
List drugs you have used ______________________________________________________________________
Have you ever attended 12-step meetings? Yes No Currently attending meetings? Yes No
Has drug or alcohol use kept you from working or caused you to be fired from a job? Yes No
Have you ever been unemployed for more than six months at a time? Yes No
If yes, explain:_______________________________________________________________________________
HOUSING
Are you currently homeless (living in transitional housing?) Yes No
If no, how long at your current residence? _________
Do you pay or contribute to the rent at the residence?
Yes No
Do you live with family? Yes No Do you live with friends? Yes No
If yes, please explain what circumstances caused you to move into transitional housing:
__________________________________________________________________________ __________________________________________________________________________ How many years have you been homeless (i.e., staying with a friend, living on the street, etc.) prior to moving into transitional housing? _________________________________________________________________________________________
Name of transitional institution where you currently reside:___________________________________________
How long have you been there? _________________ How long can you stay there? __________________
Do you plan to stay there during the 10-week program? Yes No
Previous transitional housing Location Dates of residence
___________________________________________ ____________________ ________ to _________
___________________________________________ ____________________ ________ to _________
___________________________________________ ____________________ ________ to _________
TRANSPORTATION
How do you plan to get to school? (circle one) Bus Car
Do you have a bus pass or income to provide it? Yes No Bus Route ____________
Have you ever used services from the Department of Rehabilitation? Yes No
Currently receiving services from the Department of Rehabilitation? Yes No
TRAINING PROGRAMS – List any free or low-cost training programs you have participated in
Name of program Dates Length of program Completed?
Can you provide proof of completion? Yes No MILITARY SERVICE Branch: _____________________
Years of Service: _______________
Discharge: _____________________
List ALL appointments such as court dates, medical, childcare, public social service, GROW, GAIN, parole, probation you have scheduled during the 10 weeks of the program between 8am to 5pm _______________________________________________________________ _______________________________________________________________
SUPPORT SYSTEMS
Family Member you are in contact with: ________________________________ Tel. (_____) ______-__________
Friends in the area: ____________________________________________ Tel. (_____) ______-__________
____________________________________________ Tel. (_____) ______-__________
____________________________________________ Tel. (_____) ______-__________
Church Yes No Civic/Social Group __________________________________
Describe in detail an example (within the past 6 months) when you participated as a team member. This does not need to be a work experience. A volunteer experience will also be accepted.
Describe in detail why you should be accepted into the Culinary Training Program ______________________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
I have answered the above questions and I understand that withholding or falsifying information can result in termination at any time from the Culinary Training Program during the 10-weeks.
Name (print) _____________________
Signature _____________________
Date _______________





























