Embed Size (px)
Citation preview
The Journal of Emergency Medicine, Vol. 45, No. 2, pp. e35–e40, 2013Copyright � 2013 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/$ - see front matter
http://dx.doi.org/10.1016/j.jemermed.2013.03.034
RECEIVED: 29 AACCEPTED: 27 M
ClinicalCommunications: Adults
ST-ELEVATION MYOCARDIAL INFARCTION IN THE PRESENCE OF BIVENTRICULARPACED RHYTHM
Keerthana Karumbaiah, MD and Bassam Omar, MD, PHD
Division of Cardiology, University of South Alabama Medical Center, Mobile, AlabamaReprint Address: Keerthana Karumbaiah, MD, Division of Cardiology, University of South Alabama, 2451 Fillingim Street, Mobile, AL 36617
, Abstract—Background: In the diagnosis of acute myo-cardial infarction (AMI), the presence of baseline left bundlebranch block or a permanent pacemaker rhythm posesa challenge. Objective: We present a case report highlight-ing this challenge, along with a review of pertinent litera-ture. Case Report: A 70-year-old female with knownsevere idiopathic dilated cardiomyopathy andmoderate cor-onary artery disease who was status post�biventricularpacemaker/implantable cardioverter defibrillator insertionwas brought to our institution via Emergency Medical Ser-vices with recurrent firing of her implantable cardioverterdefibrillator and syncope. After stabilization in the Emer-gency Department and treatment with intravenous amio-darone, the patient admitted to having ongoing chestpains. The electrocardiogram revealed evidence of biven-tricular pacing with superimposed ST-segment elevationsin the anterolateral leads indicative of myocardial injury.She underwent prompt angiography, thrombectomy, andbare-metal stent insertion to a totally occluded proximalleft anterior descending coronary artery, with resolution ofher chest pain and improvement in the ST-segment changes.Conclusions: Despite proposed criteria that aid in the recog-nition of AMI with underlying left bundle branch block andpaced rhythm; the advent of new pacing modalities and thepotential variability of pacing sites impose additional diag-nostic challenges requiring higher level of suspicion andbetter physician awareness. � 2013 Elsevier Inc.
, Keywords—STEMI; myocardial infarction; pacedrhythm; biventricular pacing; right ventricular pacing;electrocardiography
ugust 2012; FINAL SUBMISSION RECEIVED: 14 Decarch 2013
e35
INTRODUCTION
ST-segment elevation myocardial infarction (STEMI) isa serious condition requiring prompt electrocardiographicrecognition because prognosis is highly dependent ontimely reperfusion (1). The electrocardiographic mani-festations are, for the most part, obvious and readilyrecognizable (2). However, in the presence of baseline ab-normalities on the electrocardiogram (ECG), such as bun-dle branch blocks, especially left bundle branch block(LBBB), or a permanent pacemaker rhythm, the electro-cardiographic diagnosis becomes challenging and re-quires additional skills and a high level of suspicion (3).We report a case of anterolateral MI in a patient with bi-ventricular pacing, which presents another challenge be-cause such devices are increasingly implanted incombination with an implantable cardioverter defibrilla-tor (ICD) in patients with congestive heart failure, whoare expected to pace the majority of the time to reap thebenefits of synchronization.
CASE REPORT
A 70-year-old female with known severe idiopathic di-lated cardiomyopathy was brought to our EmergencyDepartment (ED) by Emergency Medical Services afteran episode of loss of consciousness at home, followedby firing of her ICD. Two and a half years earlier, she
ember 2012;
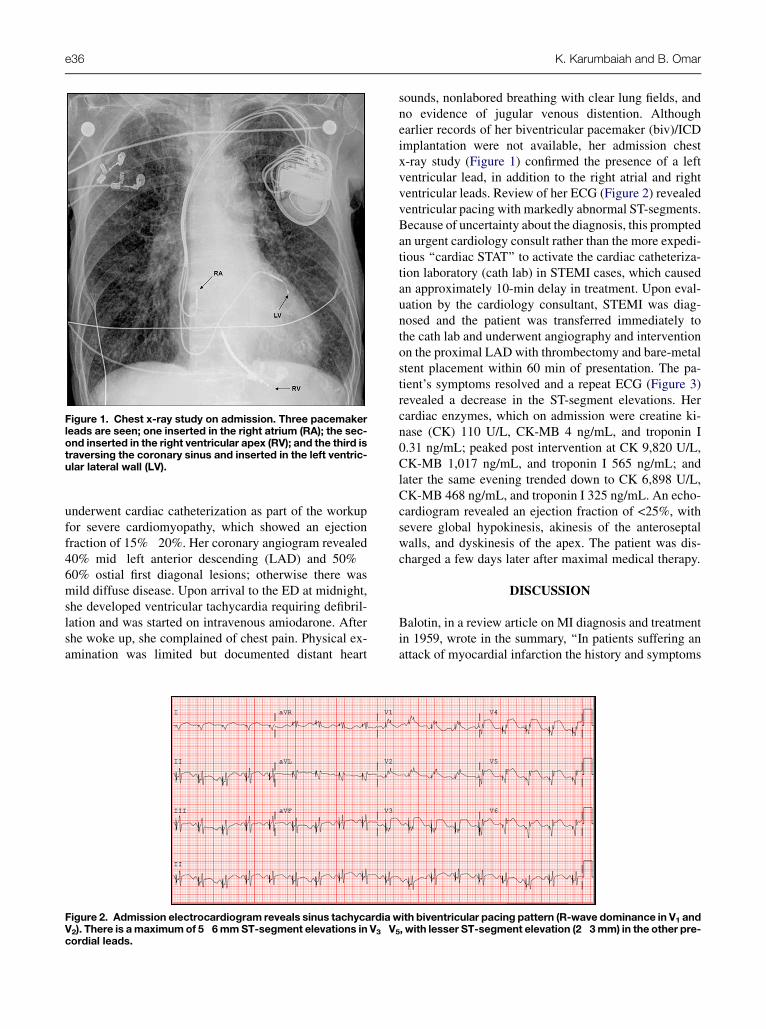
Figure 1. Chest x-ray study on admission. Three pacemakerleads are seen; one inserted in the right atrium (RA); the sec-ond inserted in the right ventricular apex (RV); and the third istraversing the coronary sinus and inserted in the left ventric-ular lateral wall (LV).
e36 K. Karumbaiah and B. Omar
underwent cardiac catheterization as part of the workupfor severe cardiomyopathy, which showed an ejectionfraction of 15%�20%. Her coronary angiogram revealed40% mid�left anterior descending (LAD) and 50%�60% ostial first diagonal lesions; otherwise there wasmild diffuse disease. Upon arrival to the ED at midnight,she developed ventricular tachycardia requiring defibril-lation and was started on intravenous amiodarone. Aftershe woke up, she complained of chest pain. Physical ex-amination was limited but documented distant heart
Figure 2. Admission electrocardiogram reveals sinus tachycardia wV2). There is amaximumof 5�6mmST-segment elevations in V3�Vcordial leads.
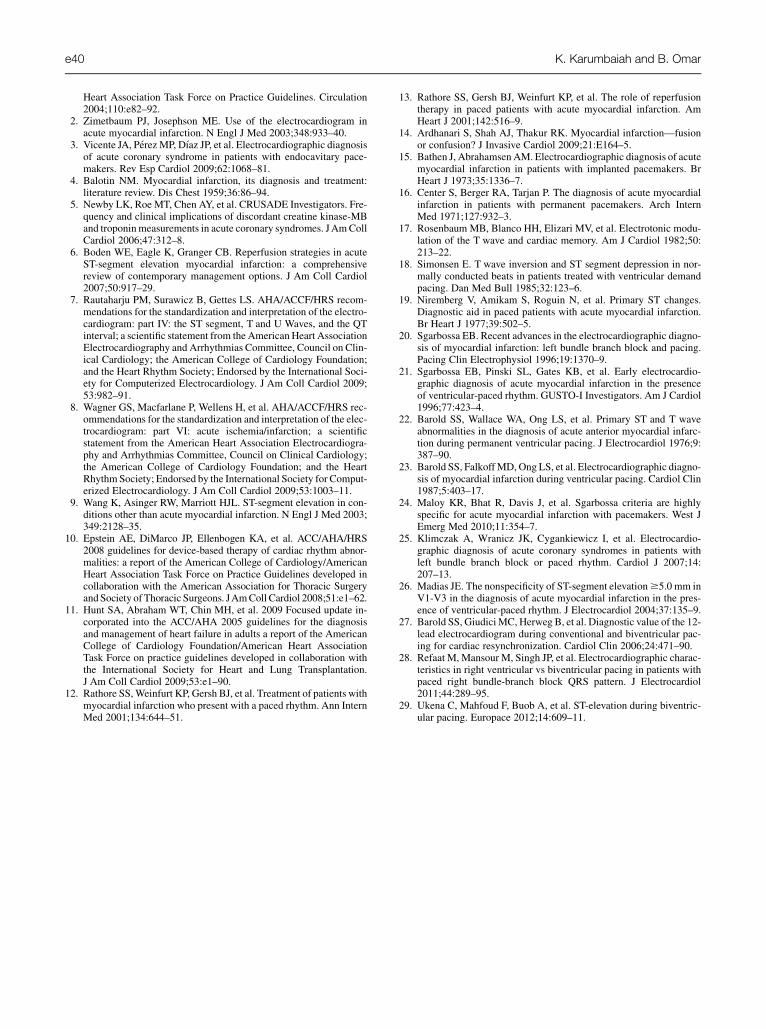
sounds, nonlabored breathing with clear lung fields, andno evidence of jugular venous distention. Althoughearlier records of her biventricular pacemaker (biv)/ICDimplantation were not available, her admission chestx-ray study (Figure 1) confirmed the presence of a leftventricular lead, in addition to the right atrial and rightventricular leads. Review of her ECG (Figure 2) revealedventricular pacing with markedly abnormal ST-segments.Because of uncertainty about the diagnosis, this promptedan urgent cardiology consult rather than the more expedi-tious ‘‘cardiac STAT’’ to activate the cardiac catheteriza-tion laboratory (cath lab) in STEMI cases, which causedan approximately 10-min delay in treatment. Upon eval-uation by the cardiology consultant, STEMI was diag-nosed and the patient was transferred immediately tothe cath lab and underwent angiography and interventionon the proximal LAD with thrombectomy and bare-metalstent placement within 60 min of presentation. The pa-tient’s symptoms resolved and a repeat ECG (Figure 3)revealed a decrease in the ST-segment elevations. Hercardiac enzymes, which on admission were creatine ki-nase (CK) 110 U/L, CK-MB 4 ng/mL, and troponin I0.31 ng/mL; peaked post intervention at CK 9,820 U/L,CK-MB 1,017 ng/mL, and troponin I 565 ng/mL; andlater the same evening trended down to CK 6,898 U/L,CK-MB 468 ng/mL, and troponin I 325 ng/mL. An echo-cardiogram revealed an ejection fraction of <25%, withsevere global hypokinesis, akinesis of the anteroseptalwalls, and dyskinesis of the apex. The patient was dis-charged a few days later after maximal medical therapy.
DISCUSSION
Balotin, in a review article on MI diagnosis and treatmentin 1959, wrote in the summary, ‘‘In patients suffering anattack of myocardial infarction the history and symptoms
ith biventricular pacing pattern (R-wave dominance in V1 and
5, with lesser ST-segment elevation (2�3mm) in the other pre-
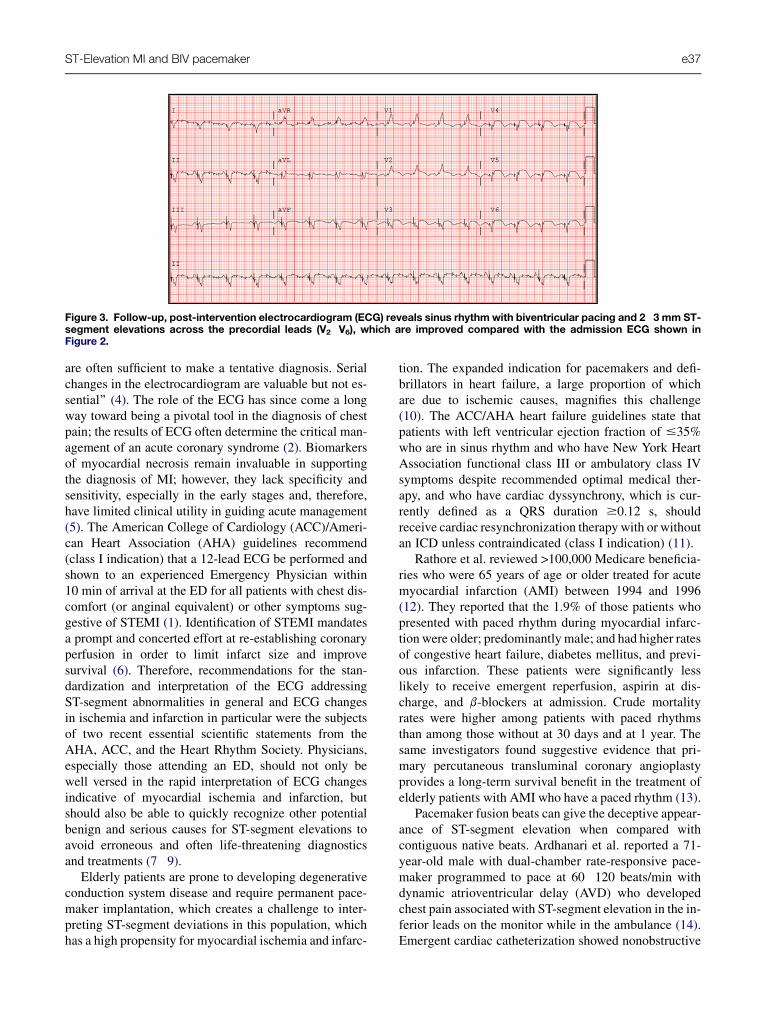
Figure 3. Follow-up, post-intervention electrocardiogram (ECG) reveals sinus rhythmwith biventricular pacing and 2�3 mm ST-segment elevations across the precordial leads (V2�V6), which are improved compared with the admission ECG shown inFigure 2.
ST-Elevation MI and BIV pacemaker e37
are often sufficient to make a tentative diagnosis. Serialchanges in the electrocardiogram are valuable but not es-sential’’ (4). The role of the ECG has since come a longway toward being a pivotal tool in the diagnosis of chestpain; the results of ECG often determine the critical man-agement of an acute coronary syndrome (2). Biomarkersof myocardial necrosis remain invaluable in supportingthe diagnosis of MI; however, they lack specificity andsensitivity, especially in the early stages and, therefore,have limited clinical utility in guiding acute management(5). The American College of Cardiology (ACC)/Ameri-can Heart Association (AHA) guidelines recommend(class I indication) that a 12-lead ECG be performed andshown to an experienced Emergency Physician within10 min of arrival at the ED for all patients with chest dis-comfort (or anginal equivalent) or other symptoms sug-gestive of STEMI (1). Identification of STEMI mandatesa prompt and concerted effort at re-establishing coronaryperfusion in order to limit infarct size and improvesurvival (6). Therefore, recommendations for the stan-dardization and interpretation of the ECG addressingST-segment abnormalities in general and ECG changesin ischemia and infarction in particular were the subjectsof two recent essential scientific statements from theAHA, ACC, and the Heart Rhythm Society. Physicians,especially those attending an ED, should not only bewell versed in the rapid interpretation of ECG changesindicative of myocardial ischemia and infarction, butshould also be able to quickly recognize other potentialbenign and serious causes for ST-segment elevations toavoid erroneous and often life-threatening diagnosticsand treatments (7�9).
Elderly patients are prone to developing degenerativeconduction system disease and require permanent pace-maker implantation, which creates a challenge to inter-preting ST-segment deviations in this population, whichhas a high propensity for myocardial ischemia and infarc-
tion. The expanded indication for pacemakers and defi-brillators in heart failure, a large proportion of whichare due to ischemic causes, magnifies this challenge(10). The ACC/AHA heart failure guidelines state thatpatients with left ventricular ejection fraction of #35%who are in sinus rhythm and who have New York HeartAssociation functional class III or ambulatory class IVsymptoms despite recommended optimal medical ther-apy, and who have cardiac dyssynchrony, which is cur-rently defined as a QRS duration $0.12 s, shouldreceive cardiac resynchronization therapy with or withoutan ICD unless contraindicated (class I indication) (11).
Rathore et al. reviewed >100,000 Medicare beneficia-ries who were 65 years of age or older treated for acutemyocardial infarction (AMI) between 1994 and 1996(12). They reported that the 1.9% of those patients whopresented with paced rhythm during myocardial infarc-tion were older; predominantly male; and had higher ratesof congestive heart failure, diabetes mellitus, and previ-ous infarction. These patients were significantly lesslikely to receive emergent reperfusion, aspirin at dis-charge, and b-blockers at admission. Crude mortalityrates were higher among patients with paced rhythmsthan among those without at 30 days and at 1 year. Thesame investigators found suggestive evidence that pri-mary percutaneous transluminal coronary angioplastyprovides a long-term survival benefit in the treatment ofelderly patients with AMI who have a paced rhythm (13).
Pacemaker fusion beats can give the deceptive appear-ance of ST-segment elevation when compared withcontiguous native beats. Ardhanari et al. reported a 71-year-old male with dual-chamber rate-responsive pace-maker programmed to pace at 60�120 beats/min withdynamic atrioventricular delay (AVD) who developedchest pain associated with ST-segment elevation in the in-ferior leads on the monitor while in the ambulance (14).Emergent cardiac catheterization showed nonobstructive

e38 K. Karumbaiah and B. Omar
coronary disease. Analysis of the rhythm strips from theambulance revealed intermittent and varying degrees ofST-segment elevation in the inferior leads caused by ven-tricular fusion, evidenced by the presence of a ventricularpacing artifact and the QRS complex being a hybrid ofnormal and paced beats. Rate-responsive dual-chamberpacing with dynamic AVDwas responsible for generatingvarying degrees of fusion because of competition with thepatient’s normal AV conduction. Ventricular fusion wasnot recognized because the bipolar pacing artifactswere inconspicuous.
Earlier attempts at diagnosingmyocardial infarction inthe setting of a paced rhythm focused on the identificationof any spontaneous, nonpaced beats, or by shorting outthe pacemaker (15,16). However, in patients who arepacemaker-dependent, such an approach can be unsafeand likely misleading due to the potentially ischemic-appearing native beats caused by ‘‘cardiac memory’’rather than ischemia (17,18). Niremberg et al. describedprimary ST-segment changes, consisting of ST-segmentelevations of at least 2 mm with a convex shape and al-ways located in the same leads in which they appear onconducted sinus beats, as diagnostic of myocardial infarc-tion in 94% of patients (19). Sgarbossa et al. assessed theclassic electrocardiographic criteria for AMI in the pres-ence of ventricular paced rhythm used by previous inves-tigators in 17 patients enrolled in the GUSTO-I trial(Global Utilization of Streptokinase and t-PA for Oc-cluded Coronary Arteries-I) who had permanent ventric-ular pacing and confirmed MI (19�23). They found threecriteria which were highly specific for AMI (summarizedin Table 1): 1) ST-segment elevation $5-mm in leadsthat had predominantly negative QRS complexes (sensi-tivity 53%, specificity 88%); 2) ST-segment elevation$1-mm in leads with a predominantly positive QRScomplex (sensitivity 18%, specificity 94%); and 3) ST-segment depression$1-mm in leads V1, V2, and V3 (sen-sitivity 29%, specificity 82%). The latter could representeither posterior ‘‘Q wave’’ infarction or ‘‘ST-segment de-pression (subendocardial)’’ infarct. Maloy and colleagues
Table 1. Summary of the Criteria for Acute MyocardialInfarction in the Presence of Ventricular PacedRhythm Reported by Sgarbossa et al. (20,21)
ST Deviation Sensitivity (%) Specificity (%)
$5-mm ST elevation in leadswith predominantly negativeQRS complexes
53 88
$1-mm ST elevation in leadswith predominantly positiveQRS complexes
18 94
$1-mm ST depression in V1, V2,
and V3 (acute posterior MI vs.subendocardial MI)
29 82
MI = myocardial infarction.
confirmed the usefulness of the Sgarbossa criteria in 57patients with AMI and ventricular paced rhythm andfound that ST-segment elevation $5-mm in leads thathad predominantly negative QRS complexes had 99%specificity for the diagnosis of AMI (24).
Klimczak et al. reviewed the electrocardiographic di-agnosis of acute coronary syndromes in patients withLBBB or paced rhythm and concluded that the presentcriteria for recognition of AMI in patients with pace-makers has serious limitations, with a need for additionalprospective studies that include larger population of pa-tients with new methods of pacing and alternative locali-zations of electrodes (25). They conceded that thismethod (together with a typical medical history) is stillthe simplest, cheapest, and most available form of anearly diagnosis of AMI. Madias, on the other hand, chal-lenged the specificity of the ST-segment elevation $5mm in V1�V3 in the diagnosis of AMI in the presenceof ventricular paced rhythm because it is also encoun-tered in patients with pacemakers and QRS complexesof large amplitudes in those leads, but without an AMI(26). He suggested that the magnitude of ST-segmentelevation in leads V1�V3 be normalized for the corre-sponding QRS amplitude.
Barold et al. reviewed the electrocardiographic mani-festations of various pacing modalities and pacemakerlead positions, including traditional right ventricular(RV) pacing and biventricular pacing (27). Whether in-tentional or inadvertent, nontraditional lead positionscause patterns on the 12-lead ECG that deviate from themore familiar apical RV pacing (Table 2) and, therefore,can impact the recognition of ischemic changes using theusual electrocardiographic criteria. In biventricular pace-makers, traditionally the R wave in V1 can be expected tobe dominant when the RV lead is implanted in the apex;however, this dominance may be lost when the RV lead isimplanted in the outflow tract. The QRS complex is rela-tively narrower than during single-chamber pacing. Api-cal RV pacing, for various reasons, can sometimes resultin a right bundle branch block (RBBB) QRS pattern,which is difficult to differentiate from biventricular pac-ing. Refaat et al. found approximately 17% of patientswith RV pacing had RBBB QRS morphology (28).They noted that, in contrast to biventricular pacing, RVpacing with RBBBQRSmorphology often exhibited pos-itive concordance in the precordial leads; qR configura-tion in lead V1; and late QRS transition beyond lead V3.
The R-wave dominance in lead V1, and often lead V2,in biventricular paced rhythm means that ST-segmentelevation in these leads will be concordant. Therefore,ST-segment elevation $1-mm should be considered ab-normal and indicative of injury in these leads. This is incontrast to RV apical pacing, where these leads exhibitpredominantly negative QRS complexes and therefore

Table 2. Electrocardiogram Features of Right Ventricular, Left Ventricular, and Biventricular Pacing with Variable PacemakerLead Positions as Described by Barold et al. (27)
VentricularChamber Lead Position Expected ECG Features
Potential Pattern During Anterior orInferior STEMI (Lateral or PosteriorSTEMI Depend on QRS Direction)
RV Apical (conventional) LBBB pattern; negative in II, III, aVF;no qR in I; superior axis
$5-mm ST elevation in anterior MI$5-mm ST elevation in inferior MI
RV Mid-septal (lead displacement fromRV apex to mid-septum)
LBBB pattern; negative in II, III, aVF;qR in I, aVL; superior axis
$5-mm ST elevation in anterior MI$5-mm ST elevation in inferior MI
RV Outflow tract pacing LBBB pattern; positive in II, III, aVF;qR in I; aVL; right inferior axis
$5-mm ST elevation in anterior MI$1-mm ST elevation in inferior MI
LV LV endocardium (lead destined to theRV apex, passed through ASD/PFO or subclavian arteryinadvertently)
RBBB pattern; axis depends onpacing site
$1-mm ST elevation in anterior MIInferior MI varies depending on axis
LV Basal LV (coronary sinus posterior orposterolateral vein; proper positionfor resynchronization pacing)
RBBB pattern; dominant R-wavesV1�V6; right inferior axis
$1-mm ST elevation in anterior MI$1-mm ST elevation in inferior MI
LV Basal LV (lead, meant forresynchronization, placed incoronary sinus middle or greatanterior vein inadvertently)
LBBB, depending on site ofstimulation
$5-mm ST elevation in anterior MIInferior MI varies depending on axis
RV and LV (biv) Basal LV; apical RV Positive V1; negative in II, III, aVF; q orQS in I; right superior axis
$1-mm ST elevation in anterior MI$5-mm ST elevation in inferior MI
RV and LV (biv) Basal LV; RV outflow tract Negative V1; positive in II, III, aVF;right inferior axis; q or QS in I; rightinferior axis
$5-mm ST elevation in anterior MI$1-mm ST elevation in inferior MI
ASD = atrial septal defect; biv = biventricular; ECG = electrocardiogram; LBBB = left bundle branch block; LV = left ventricular; MI = myo-cardial infarction; PFO = patent foramen ovale; RBBB = right bundle branch block; RV = right ventricular; STEMI = ST-segment elevationmyocardial infarction.
ST-Elevation MI and BIV pacemaker e39
$5-mm ST-segment elevation is requisite for AMI diag-nosis. In our patient, although ST-segment elevationsapproximated or exceeded 5-mm in leads V3 to V5
(Figure 2), this was not the case in leads V1 and V2, whichexhibited smaller, but concordant, ST-segment eleva-tions. One potential reason for the less impressiveST-segment elevation in V1 and V2 could have been thelocation of the injury, having spared part of the septum,as proximal septal perforators were patent on the pre-intervention angiogram. In a similar report by Ukenaand colleagues, a 53-year-old man with severe cardiomy-opathy and an implanted biv/ICD device was treated foranterior myocardial infarction (29). Less than 5-mmST-segment elevations were observed in I, II, aVL, andV3–V6, which were concordant with the paced QRS com-plexes. Their diagnosis was facilitated by comparisonwith a previous ECG. Despite the lack of a baselineECG in our patient, the ST-segment changes were over-whelmingly abnormal, even in the discordant leads, V3
to V6, especially given the extent of ST-segment devia-tions in comparison with the overall small amplitude ofthe QRS complexes (26).
CONCLUSIONS
The ECG remains the cornerstone for the diagnosis andtimely decision making in AMI. Its utility, however, has
often been blurred by the presence of underlying ab-normalities that can mask the classic anticipated ST-segment elevation. Criteria have been proposed to aidin the diagnosis of AMIwith underlying LBBB and pacedrhythm. Biventricular pacing, and the potential variabilityof pacing sites, causes ECG patterns different from con-ventional RV apical pacing, which can impact the re-cognition of myocardial infarction. Providers should notdismiss an ECG with paced rhythm as uninterpretable,nor should they rely on a computerized ECG interpreta-tion, which often shies away from calling any abnormal-ities in the setting of a paced rhythm. The paucity of casesof myocardial infarction with unconventional pacingmakes it more difficult for providers to become familiarwith such abnormal patterns so that they can make swiftdiagnosis and implement timely therapy. Simulation soft-ware that creates various patterns of ST-elevation in un-conventional paced rhythms for the purpose of teachingand more robust computerized ECG interpretation algo-rithms that can detect subtle electrocardiographic STchanges in paced rhythms can help alleviate this problem.
REFERENCES
1. Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelinesfor the management of patients with ST-elevation myocardial in-farction: a report of the American College of Cardiology/American
e40 K. Karumbaiah and B. Omar
Heart Association Task Force on Practice Guidelines. Circulation2004;110:e82–92.
2. Zimetbaum PJ, Josephson ME. Use of the electrocardiogram inacute myocardial infarction. N Engl J Med 2003;348:933–40.
3. Vicente JA, Perez MP, Dıaz JP, et al. Electrocardiographic diagnosisof acute coronary syndrome in patients with endocavitary pace-makers. Rev Esp Cardiol 2009;62:1068–81.
4. Balotin NM. Myocardial infarction, its diagnosis and treatment:literature review. Dis Chest 1959;36:86–94.
5. Newby LK, Roe MT, Chen AY, et al. CRUSADE Investigators. Fre-quency and clinical implications of discordant creatine kinase-MBand troponinmeasurements in acute coronary syndromes. JAmCollCardiol 2006;47:312–8.
6. Boden WE, Eagle K, Granger CB. Reperfusion strategies in acuteST-segment elevation myocardial infarction: a comprehensivereview of contemporary management options. J Am Coll Cardiol2007;50:917–29.
7. Rautaharju PM, Surawicz B, Gettes LS. AHA/ACCF/HRS recom-mendations for the standardization and interpretation of the electro-cardiogram: part IV: the ST segment, T and U Waves, and the QTinterval; a scientific statement from the American Heart AssociationElectrocardiography and Arrhythmias Committee, Council on Clin-ical Cardiology; the American College of Cardiology Foundation;and the Heart Rhythm Society; Endorsed by the International Soci-ety for Computerized Electrocardiology. J Am Coll Cardiol 2009;53:982–91.
8. Wagner GS, Macfarlane P, Wellens H, et al. AHA/ACCF/HRS rec-ommendations for the standardization and interpretation of the elec-trocardiogram: part VI: acute ischemia/infarction; a scientificstatement from the American Heart Association Electrocardiogra-phy and Arrhythmias Committee, Council on Clinical Cardiology;the American College of Cardiology Foundation; and the HeartRhythmSociety; Endorsed by the International Society for Comput-erized Electrocardiology. J Am Coll Cardiol 2009;53:1003–11.
9. Wang K, Asinger RW, Marriott HJL. ST-segment elevation in con-ditions other than acute myocardial infarction. N Engl J Med 2003;349:2128–35.
10. Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS2008 guidelines for device-based therapy of cardiac rhythm abnor-malities: a report of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines developed incollaboration with the American Association for Thoracic SurgeryandSociety of Thoracic Surgeons. JAmColl Cardiol 2008;51:e1–62.
11. Hunt SA, Abraham WT, Chin MH, et al. 2009 Focused update in-corporated into the ACC/AHA 2005 guidelines for the diagnosisand management of heart failure in adults a report of the AmericanCollege of Cardiology Foundation/American Heart AssociationTask Force on practice guidelines developed in collaboration withthe International Society for Heart and Lung Transplantation.J Am Coll Cardiol 2009;53:e1–90.
12. Rathore SS,Weinfurt KP, Gersh BJ, et al. Treatment of patients withmyocardial infarction who present with a paced rhythm. Ann InternMed 2001;134:644–51.
13. Rathore SS, Gersh BJ, Weinfurt KP, et al. The role of reperfusiontherapy in paced patients with acute myocardial infarction. AmHeart J 2001;142:516–9.
14. Ardhanari S, Shah AJ, Thakur RK. Myocardial infarction—fusionor confusion? J Invasive Cardiol 2009;21:E164–5.
15. Bathen J, AbrahamsenAM. Electrocardiographic diagnosis of acutemyocardial infarction in patients with implanted pacemakers. BrHeart J 1973;35:1336–7.
16. Center S, Berger RA, Tarjan P. The diagnosis of acute myocardialinfarction in patients with permanent pacemakers. Arch InternMed 1971;127:932–3.
17. Rosenbaum MB, Blanco HH, Elizari MV, et al. Electrotonic modu-lation of the T wave and cardiac memory. Am J Cardiol 1982;50:213–22.
18. Simonsen E. T wave inversion and ST segment depression in nor-mally conducted beats in patients treated with ventricular demandpacing. Dan Med Bull 1985;32:123–6.
19. Niremberg V, Amikam S, Roguin N, et al. Primary ST changes.Diagnostic aid in paced patients with acute myocardial infarction.Br Heart J 1977;39:502–5.
20. Sgarbossa EB. Recent advances in the electrocardiographic diagno-sis of myocardial infarction: left bundle branch block and pacing.Pacing Clin Electrophysiol 1996;19:1370–9.
21. Sgarbossa EB, Pinski SL, Gates KB, et al. Early electrocardio-graphic diagnosis of acute myocardial infarction in the presenceof ventricular-paced rhythm. GUSTO-I Investigators. Am J Cardiol1996;77:423–4.
22. Barold SS, Wallace WA, Ong LS, et al. Primary ST and T waveabnormalities in the diagnosis of acute anterior myocardial infarc-tion during permanent ventricular pacing. J Electrocardiol 1976;9:387–90.
23. Barold SS, FalkoffMD, Ong LS, et al. Electrocardiographic diagno-sis of myocardial infarction during ventricular pacing. Cardiol Clin1987;5:403–17.
24. Maloy KR, Bhat R, Davis J, et al. Sgarbossa criteria are highlyspecific for acute myocardial infarction with pacemakers. West JEmerg Med 2010;11:354–7.
25. Klimczak A, Wranicz JK, Cygankiewicz I, et al. Electrocardio-graphic diagnosis of acute coronary syndromes in patients withleft bundle branch block or paced rhythm. Cardiol J 2007;14:207–13.
26. Madias JE. The nonspecificity of ST-segment elevation$5.0 mm inV1-V3 in the diagnosis of acute myocardial infarction in the pres-ence of ventricular-paced rhythm. J Electrocardiol 2004;37:135–9.
27. Barold SS, GiudiciMC, Herweg B, et al. Diagnostic value of the 12-lead electrocardiogram during conventional and biventricular pac-ing for cardiac resynchronization. Cardiol Clin 2006;24:471–90.
28. Refaat M, Mansour M, Singh JP, et al. Electrocardiographic charac-teristics in right ventricular vs biventricular pacing in patients withpaced right bundle-branch block QRS pattern. J Electrocardiol2011;44:289–95.
29. Ukena C, Mahfoud F, Buob A, et al. ST-elevation during biventric-ular pacing. Europace 2012;14:609–11.