Embed Size (px)
Citation preview

SSC Enhanced Recovery CollaborativePQI Summit - 11/19/2018
Angie Chan, Manager, GPSC

No disclosures

Overview
ƒ Enhanced Recovery programs are multi-modalperioperative care pathways designed to achieveearly recovery after surgical procedures.
ƒ Problem: Evidence supporting EnhancedRecovery has been growing for over 15 years,but the application of the pathway remainedinconsistent across BC.
ƒ Opportunity: Complication rates for electivecolorectal surgery patients could be vastlyimproved with a provincial strategy to helpspread the Enhanced Recovery pathway.

5Dimensionsof Scaling
Scaling Out(Beneficiaries)
Scaling Scree(New
Innovations)
Scaling Deep(Culture)
ScalingInfrastructure
(Capacity)
Scaling Up(Systems)
Ridell, Darcy & Michele-Lee Moore (2015)Tulloch, Gord (2018)
Here to There Consulting (2018)

IHI Collaborative Model akaBreakthrough Series Model
“An improvement method that relies on spreadand adaptation of existing knowledge to multiplesettings to accomplish a common aim.”- From Institute of Healthcare Improvement
ScalingOut

Vancouver Coastal Health 2014
Existing Knowledge:Enhanced Recovery Pathway
Active Patient InvolvementPre-operative Intra-operative Post-operative
Pre-admission education Active warming Early oral nutrition
Early discharge planning Opioid-sparing technique Early ambulation
Reduced fasting duration Surgical techniques Early catheter removal
Carbohydrate loading Avoidance of prophylacticNG tubes & drains
Use of chewing gum
No-selective bowel prep Goal-directed perioperative fluid management
Venous thromboembolismprophylaxis
Pain and nausea management
Antibiotic prophylaxisPre-warming
Audit of processes & outcomesMulti-disciplinary Team Involvement

Multiple settings:11 participating hospitals
BCEnhancedRecovery
Collaborative
NHA- MMH
VCH-VGH
PHC-SPH-MSJ
IslandHealth-NRGH-CRH
IH-KGH-RIH
FHA-RCH-LMH-SMH
UHNBC
RH, LGH
RJH, VGH, FPs
KBRH
ARH, RMH, PAH, FPs

Common Aim:Collaborative’s Goalsƒ 80% compliance on all pathway elements
ƒ 50% reduction in complication rates
ƒ Decrease hospital LOS
ƒ No significant change to readmission rates

Developmentof Frameworkand ChangePackage (i.e.
ERASprotocol)
Recruit &enroll teams
Pre-work
LS1Nov‘14
LS2Apr‘15
LS3Sep‘15
AP1 AP2 AP3
Dissemination:outcomes
congress (Jan’16), reports,evaluation
Holding thegains
Spread
P
DS
A
Supports:email, website, site visits, monthly reports,monthly team lead meetings, skill-building
webinars, Communities of Practice
IHI Breakthrough Series Model
P
DS
A P
DS
A
CollaborativeTopic
Selection
Assemblefaculty and
staffing
~ 6 months of prep~ 12 months of implementation

Participant Feedback
47% response rate

Outcomes
Baseline (n = 999) Jan-Dec 2015 (n=1123)
ComplicationRate
Length of Stay(days)
ReadmissionRate

Process Changes (%) Jan – Dec 2015 n=1123
Goal: 80% compliance on all pathway elements
ScalingScree
Provincialƒ Multidisciplinary, passionate leadershipƒ Inclusive Communities of PracticeHospitalƒ Hospital Teamwork: Core team + broaderengagement of everyone on pathwayƒ Staff educationPatientƒ Engage patient as partners in their careƒ Patient educationFun!
Supporting Culture ChangeScalingDeep

Sponsor: SSC
Advisory Panel:Anesthesia, Surgery,
Nursing/Adminmembers from 6
regional HAs
BC HipArthroplastyCollaborative
AnesthesiaCOP
2Patient
Partners
SurgeryCOP
Co-Chairs:Anesthesia,
Surgery,Nursing/QI
OrganizationalPartner:
BC Patient Safety& Quality Council
NursingCOP
NutritionCOP
ScalingInfrastructure
• SSC: data support funding• HA/Hospital: Staff time and
backfilling

Create and share resources
Patient Education Videos• applicable to many surgical
procedures• English, Cantonese, Mandarin,
Punjabi
Clinical Guidance Notes• Mechanical Bowel Preparation• Pre-operative Carbohydrate-
Loading• Goal-directed Fluid Therapy• Opioid-Sparing Technique
Network of Clinicians• champions• mentors• resource people
Data Set & Tools• Processes & Outcomes
Webinars• ERAS Basics• Process Mapping• Train-the-trainer• Post-op Pain• Run Charts• Enhanced Recovery in NSQIP
www.enhancedrecoverybc.ca• order sets• patient education materials• staff education materials• references• data definitions and data
collection tools• presentations• patient story video

ƒ Engagement of MOH, Provincial SurgicalExecutive Committee (PSEC), HA, and hospitalleaders
ƒ Spread of Enhanced Recovery pathway andpre-surgical optimization included in 2015-2018MOH Surgical Services Priorities
Supporting Policy ChangeScaling
Up

5Dimensionsof Scaling
Scaling Out(Beneficiaries)
Scaling Scree(New
Innovations)
Scaling Deep(Culture)
ScalingInfrastructure
(Capacity)
Scaling Up(Systems)
Ridell, Darcy & Michele-Lee Moore (2015)Tulloch, Gord (2018)
Here to There Consulting (2018)
Thank You!Angie ChanManagerCommunity Practice Designand EvaluationGPSC

PQI project Sustainabilityand spread
A physician perspective: Dr. Jason Wale, Island Health

I have no conflicts of interest to declare.
I receive no honorariums or finance.

Pre- PQI : My Office

Pre-PQI : My staff support

My PQI project from 2016/17: FentanylCrisis and ER response

My PQI project from 2016/17:
Problem Solution

Local success• More than 160 patients referred from VGH and RJH in
Victoria.
• NNT of 4.6 to achieve patients who are maintained intherapy at local addiction treatment centers.
PQI Funding is over….. Now what?

#1: Symbiosis -Use the health authority structure

How to make sustainable changes within HA
HA
PQI
PQI

#2: Relationships- Who will keep this going?
• HA sponsor involved to remove barriers tosustainability and spread.
• Identify the HA agents who are most interested inmaintaining your project.

#3: Celebrate Success
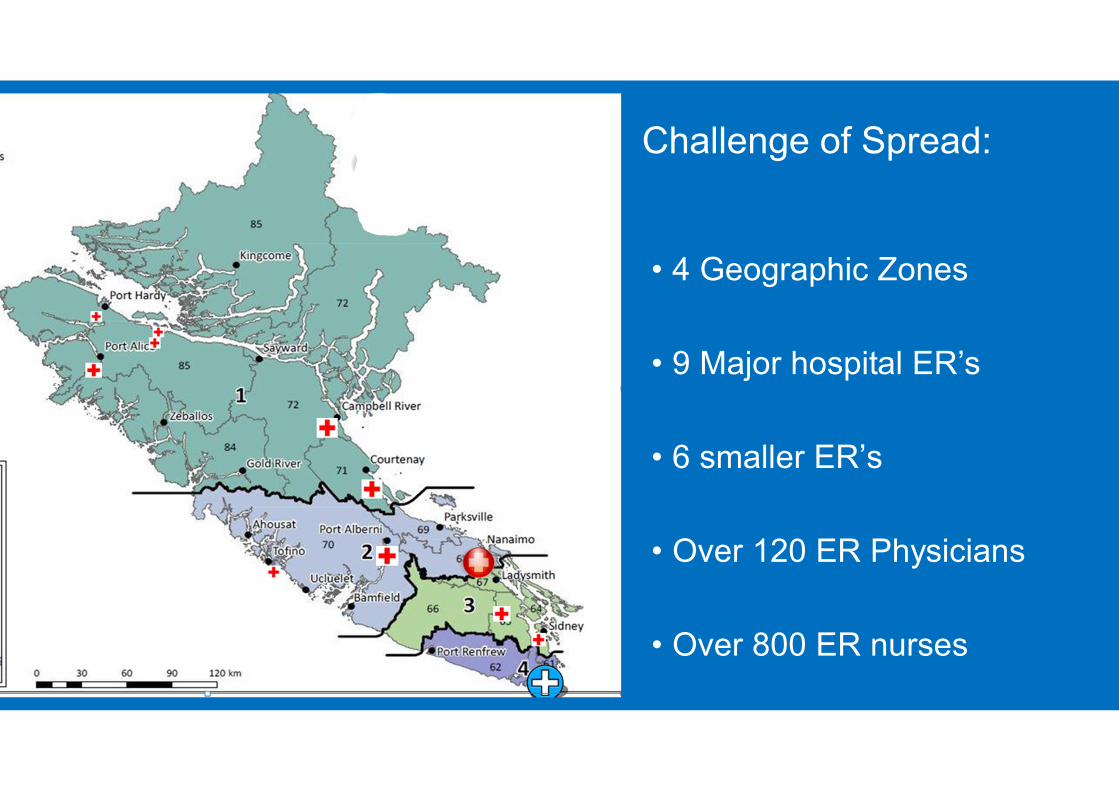
Local success• 4 Geographic Zones
• 9 Major hospital ER’s
• 6 smaller ER’s
• Over 120 ER Physicians
• Over 800 ER nurses
Challenge of Spread:

All of us have a spectrum of allegiance

People are most loyal to the smallest tribethat they belong to.
New Site for Spread
HealthAuthority
Need Local Champions.

The path ahead…? Fewer projects withmore support/integration
? Departmental/ Groupprojects
? Utilize FacilityEngagement and HealthSystem Redesignsynergy


Rapid Access to Consultative ExpertiseAn Innovative Model of Shared Care
November 19th, 2018
Margot Wilson, RN, MSNDirector, Shared Care & Digital Care/Virtual HealthProvidence Health Care

No Disclosures

Why RACE Came to Be atProvidence Health CareJoint partnership between Providence Health Care and the SharedCare Committee, in collaboration with Vancouver Coastal Health

The Problem
SomeSpecialties
areimpossibleto access!
We really need asimple way forcommunication Communication
is best when it’sdirectly
physician tophysician!
It seems the‘good olddays’ of
conversingin the
hallway aregone. Is
there a wayto bring that
back?
As a patient Iwant my doctorsto be connected
There just isn’t acommunication
network
In an urbansetting, it’s reallydifficult to know
the differentsubspecialties
Rapid Access to Consultative Expertise - RACE• One phone line with a selection of
specialty services• Request for urgent advice within 2
hours• Started at PHC in June 2010 with 5
services• Currently at 43 services• >40,000 calls• New Technology RACEApp+ started
July 2015• ~1000 calls per month• ~400 specialists• Many family physicians (800+ on
the app)

Current ServicesRegional• Cardiovascular Risk & Lipid Management• Eating Disorders -Psychiatry• Emergency Medicine• Endocrinology• General Cardiology• General Internal Medicine• General Pediatrics• Geriatric Psychiatry• Geriatrics• Hand and Upper Limb Orthopedic Conditions• Heart Failure• Infectious Diseases• Leg, Ankle, Foot Orthopedic Conditions• Nephrology• Neurology• Obstetrics & Gynecology• Ophthalmology• Otolaryngology/Ear, Nose & Throat• Parkinson’s Disease and other Movement
Disorders• Psychiatry – Adult• Radiology• Respirology• Rheumatology
Provincial Services• Addictions Medicine• Cardiac Transplant• Child & Adolescent Psychiatry• HIV Care, Treatment, and Prophylaxis• Medical Assistance in Dying Advice• Medical Refugee Health• Pediatric Gastroenterology• Pediatric Infectious Diseases• Pediatric Orthopedic Conditions• Pediatric Rheumatology• Perinatal Addictions• Perinatal Psychiatry• Physical Medicine and Rehabilitation• Sleep Disorders Service• Sexually Transmitted Infection• Thrombosis• Trans Gender Care• Tropical and Post-travel Medicine• Urology• Vascular Surgery

Metrics - 2012 Evaluation• 78% of calls answered
within 10 mins
• 90% are <15 min in length
• 60% avoided face-to-faceconsults
• 32% avoided ED visits
• Up to $200 cost avoidanceper call
• User-friendly 'decisionsupport tool'
• Improves clinicaljudgment
• Receive medicaleducation
• Increases knowledgecapacity

How RACE Impacts Family Practice

System Outcomes

RACEapp+• Search ‘RACEapp+’ on the app
store• www.raceapp.ca• Web based• Ability to exchange billing
information• Ability to add a professional photo• Specialists chooses preference on
how to receive the contact• Phone• SMS• Email
• Interaction is still voice to voice

Value for the Provider…
• Improves access to care
• Improves patient care
• Improves providerrelationships
• Patient CoordinationCosts Avoided
• Reduces ED Visits
“I find myself educatingpediatricians, GPs, and evenother psychiatrists aboutmore complicatedpsychiatric issues inchildren. Both sides of theconversation seem to enjoythe collaboration”
“I got confirmationthat the situationwas normal, and Ididn’t have tosubject the child toextra bloodwork oran ultrasound.”
“It has given mea level ofprofessionalsatisfaction,professionalempowermentand improvedpatient care.”
“The app isawesome, tap, tap,tap and I got a callback within a coupleof minutes”
“I learn something about thetypes of patients and resourcesavailable to front-line cliniciansand physicians, and they learnsomething about child andadolescent psychiatry”

Challenges of Spread andSustainability
• Expansion across specialties• Increased uptake by family physicians• Expansion across BC• Expansion across Canada• Creation of the App• Provincial governance• Provincial administration

One size does notfit all
Leverage Leadership
Keep is simple
Engage champions
“RACE in a BOX”
The reach ofrelationships
Talk about it
Avoid replacing wellestablished effectivecommunication lines
Respect what workswell
SpreadLearnings
Adaption notAdoption
Share everything
Remuneration
Marketing is key
The power ofpartnerships
Requires criteria for
specialist participation– Response time– collegial interaction– knowledge transfer

Ii
Provincial RACE Spread
Ii

National Spread• Canadian Foundation
for HealthcareImprovement (CFHI)Collaborative
• Canadian College ofFamily Physicians
• The Royal College ofPhysicians and Surgeonsof Canada
• Canada Health Infoway
Vancouver

Ii
RACE Triple Aim Potential
A) Enhance the care experience by:• providing knowledge transfer• improving the specialist/primary care interface
through improved communication• simplifying the patient journey
B) Improve Population Health• access to specialty care enhance• increase capacity of specialists
C) Control per capita cost of health care• reduce avoidable consults and emergency visits

Ii
“…I think the RACE program is awonderful idea because it will allowmy GP to access expertise on aspecific problem without my havingto be referred and having to wait anumber of months to see a specialistwhen perhaps only minor advicemight be needed….”
PatientPerspective






























