Embed Size (px)
DESCRIPTION
Citation preview

Evaluation andManagement of AcuteIschemic Stroke
Pooja Khatri, MD, MSc
ABSTRACTPurpose of Review: This review provides an overview of emergent evaluation of thestroke patient with an emphasis on practical issues regarding ischemic stroke treatment.Recent Findings: The IV recombinant tissue-type plasminogen activator (rtPA)treatment window has been expanded from 3 to 4.5 hours from symptom onset.The evidence for better outcomes with more rapid initiation of reperfusion therapies isvery strong. Adjunctive endovascular therapy has not been shown to benefit allpatients with moderate or severe strokes, and investigations are underway to identifysubgroups that may benefit from this approach. Endovascular therapy should beconsidered for patients who are ineligible for IV rtPA and can begin treatment within6 hours of stroke onset.Summary: Effective emergent evaluation of a stroke patient requires well-organizedsystems that maximize speed of assessment and administration of appropriatetherapies, including IV rtPA and endovascular therapies.
Continuum (Minneap Minn) 2014;20(2):283–295.
INTRODUCTIONThis article provides a practical over-view regarding the emergent evalua-tion of a patient with acute ischemicstroke, including the decision toadminister acute reperfusion therapyand other acute supportive care.It should be noted that ‘‘acute re-perfusion therapy’’ refers to treat-ment aimed at emergently restoringblood flow in the acutely occludedcerebral artery, and may consist of IVthrombolysis and/or specific endovas-cular interventions such as intra-arterial thrombolysis or mechanicalembolectomy.
This discussion is framed aroundthe most recent American HeartAssociation/American Stroke Associ-ation guidelines, which serve as use-ful and comprehensive references tothe reader.1
EMERGENT EVALUATION OFTHE POTENTIAL ACUTEREPERFUSION CANDIDATERapid evaluation and treatment iscritical for the best outcomes. Thishas been shown both in the setting ofIV thrombolysis (IV recombinanttissue-type plasminogen activator[rtPA]) and endovascular therapy.With IV rtPA, the number needed totreat to prevent one death or signifi-cant disability is 8 when treatingwithin 3 hours of symptom onset,and 14 when treating from 3 to 4.5hours.2,3 Figure 1-1 demonstrates theodds of good outcome with IV rtPAtreatment among subjects pooledfrom major trials to date.4 It has alsobeen demonstrated that every 30-minute delay in acute reperfusionleads to a 10% relative reduction inthe likelihood of a good outcome.5
Address correspondenceto Dr Pooja Khatri, Departmentof Neurology, University ofCincinnati, 260 Stetson Street,ML 0525, Cincinnati, OH45267-0525,[email protected].
Relationship Disclosure:
Dr Khatri has receivedresearch grants from theNIH and research supportfrom Penumbra Inc andGenentech, Inc.
Unlabeled Use ofProducts/InvestigationalUse Disclosure:Dr Khatri discusses the use ofIV tissue plasminogen activatorfor minor stroke and ofendovascular therapy for stroketreatment, neither of which areapproved by the US Food andDrug Administration.
* 2014, American Academyof Neurology.
283Continuum (Minneap Minn) 2014;20(2):283–295 www.ContinuumJournal.com
Review Article
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

A patient should receive IV rtPAwithin 1 hour of arrival to an emergencydepartment (and sooner is better) withthe following goals.6
& Emergency department physiciansees patient within 10 minutesof arrival
& Stroke consultant is notifiedwithin 15 minutes of arrival
& CT scan is completed within25 minutes of arrival
& CT is interpreted within 45minutes of arrival
Strategies likely to increase thespeed of treatment include earlystroke-team notification (preferably be-fore or concurrent with CT scan per-formance); storage of rtPA in theemergency department; recognitionthat glucose level is the only necessarylaboratory result if no clinical suspicionfor bleeding diathesis is present; andmixing of IV rtPA (1:1 ratio with sterilewater or normal saline) early.
DECISION TO ADMINISTERACUTE REPERFUSION THERAPYThe following information is neededfrom the emergency department uponinitial consultation to guide clinicaldecision making.
& Time that patient was last knownto be well
& Any significant medical history& A brief neurologic examination
(ideally theNIH Stroke Scale [NIHSS])& Glucose level (finger stick) and any
other significant laboratory results& Current blood pressure& Results of acute brain imaging,
typically CT scan, when available
Each of these points and their rolein decision making are described insubsequent sections.
TimeThe patient’s ‘‘last known well’’ timedetermines potential treatment options.
KEY POINTS
h Rapid evaluation andtreatment are critical forthe best outcomes.
h A patient should receiveIV recombinanttissue-type plasminogenactivator within 1 hourof arrival to anemergency department(and sooner is better).
FIGURE 1-1 Odds of good outcome based on stroke onset to treatment time. Pooledanalysis of European Cooperative Acute Stroke Study (ECASS), AlteplaseThrombolysis for Acute Noninterventional Therapy in Ischaemic Stroke
(ATLANTIS), National Institute of Neurological Disorders and Stroke (NINDS), andEchoplanar Imaging Thrombolytic Evaluation Trial (EPITHET) subjects demonstrates thatlater onset to treatment times lead to lower odds of a treatment effect of IV rtPAcompared with placebo. Treatment beyond 270 minutes appears to have no benefit.
Reprinted with permission from Lees KR, et al, Lancet.4B 2010 Elsevier. www.sciencedirect.com/science/
article/pii/S0140673610604916.
284 www.ContinuumJournal.com April 2014
Acute Stroke
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

It is important to distinguish the timelast known well from the time that thestroke deficits were first discovered, asdemonstrated by Case 1-1.
IV thrombolysis, specifically usingrtPA, should be considered for patientsfor whom it can be administered within4.5 hours of onset. IV rtPA (at the doseof 0.9 mg/kg, maximum dose 90 mg,with 10% given as an initial bolus) hasbeen shown to improve clinical out-comes for patients within 3 hours ofonset by two randomized trials (jointlyreferred to as the National Institutes ofNeurological Disorders and Stroke[NINDS] tPA Stroke Study),2 and within3 to 4.5 hours by one randomized trial
(European Cooperative Acute StrokeStudy III).3 Specifically, within 3 hoursof onset, despite a 6% increased risk ofsymptomatic intracranial hemorrhage,the overall absolute benefit of treatmentis a 13% lower rate of significant dis-ability (defined as a modified RankinScale of 0 or 1). This benefit is estimatedto be as high as 33% for any improve-ment in the spectrum of independenceto severe disability or death; Figure 1-27
illustrates potential treatment effects.8
Several community cohorts,9 pooledanalyses of other IV rtPA trials,4 and the3-hour subgroup of the Third Interna-tional Stroke Trial (IST-3) providefurther supportive evidence.10 Of note,
KEY POINT
h IV thrombolysis,specifically usingrecombinant tissue-typeplasminogen activator,should be consideredfor patients for whom itcan be administeredwithin 4.5 hours ofonset of stroke deficits.
Case 1-1A 78-year-old woman with a history of diabetes mellitus presented to theemergency department with acute left-sided weakness at 4:00 PM. Herhusband had called 9-1-1 immediately upon identifying her symptoms at3:30 PM. Emergency medical services (EMS) had promptly evaluated thepatient and brought her to the stroke-ready emergency department.En route, EMS had prenotified the hospital, where a CT scan wasperformed upon the patient’s arrival. The CT scan showed minimal earlyischemic changes and no intracranial hemorrhage. The patient’sfinger-stick glucose level was 95 mg/dL, and her examination revealed lefthemiplegia and anosognosia. Her husband reported that her onlymedication was metformin and she had no recent surgeries or prior historyof intracranial hemorrhage. However, upon further discussion regardingthe time of onset with the stroke clinician, it became clear that, while thepatient’s symptoms were discovered at 3:30 PM, her husband had last seenher well before he left for work at 9:00 AM. The patient reported feelingfine until her husband came home. Her cell phone was checked, and shehad not spoken to anyone that day. Her neighbor was called by the husband,and the patient had not been witnessed to be well by anyone else since9:00 AM. Thus, it was 7 hours from last known well at this point, and IVrecombinant tissue-type plasminogen activator (rtPA) was not administered.
Comment. In this case, if the patient had not had anosognosia, it mayhave been appropriate to identify the last known well time based on thepatient’s own history. However, given her lack of appreciation for herdeficit, her report could not be trusted. A normal CT scan has not beendemonstrated to identify patients who might benefit from IV rtPAregardless of time from last known well. However, an active and promisingarea of investigation is to develop imaging markers that can identifypatients who will benefit from IV rtPA treatment based on physiologictime. Had it not been for the unknown and potentially greater than4.5-hour time of onset, the patient in this case would have been eligiblefor IV rtPA.
285Continuum (Minneap Minn) 2014;20(2):283–295 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

the US Food and Drug Administrationhas only approved the 3-hour timewindow for IV rtPA, whereas clinicalguidelines recommend treatment upto 4.5 hours based on the currentevidence.1 It should also be noted thatno other lytic agent, such as reteplaseor tenecteplase, has been demonstratedas an effective treatment for acuteischemic stroke.
Endovascular therapy for IV re-combinant tissue-type plasminogenactivatorYineligible patients. For pa-tients ineligible for IV rtPA (because
of, for example, time of onset,coagulopathy, or recent surgery) whohave significant stroke deficits (typically,an NIHSS score of 8 or higher),endovascular therapy should be consid-ered if treatment can be initiated within6 hours (Case 1-2). Indirect evidence,including the Prolyse in Acute CerebralThromboembolism (PROACT) II trialof recombinant prourokinase and theMiddle Cerebral Artery Embolism LocalFibrinolytic Intervention Trial (MELT)of urokinase,11Y13 suggests that intra-arterial rtPA initiated within 6 hours ofonset will lead to better clinical out-comes than supportive care alone (ie,no reperfusion therapy). More recentevidence suggests that endovasculardevices open major arterial occlusionsmore effectively, leading to their fre-quent clinical use in this setting; spe-cifically, the most recent generation ofmechanical embolectomy devices, in-cluding the Penumbra Aspiration Sys-tem, the Solitaire Stent Retriever, andthe TREVO2 Stent Retriever, reportrevascularization rates exceeding80%.14Y16 Comparable safety and effi-cacy between IV rtPA within 3 hoursversus endovascular therapy within 6hours in the SYNTHESIS trial also sup-ports the approach for IV rtPAYineligiblepatients who present early.17 Case seriesdata also suggest reasonable safety forthe use of intra-arterial thrombolysis inthe nonneurosurgical postoperative set-ting.18 Devices available in the UnitedStates are shown in Figure 1-4.
The role of imaging selection toidentify patients beyond 6 hours fromonset who will benefit from acutereperfusion therapies remains to bedetermined. A phase 2b study, theMechanical Retrieval and Recanalizationof Stroke Clots Using Embolectomy(MR RESCUE) trial, tested the penum-bral hypothesis.19 A favorable CT-basedor magnetic resonanceYbased penum-bral selection pattern was defined as a
KEY POINT
h For patients ineligiblefor IV recombinanttissue-type plasminogenactivator who havesignificant strokedeficits (typically, an NIHStroke Scale score of 8or greater), endovasculartherapy should beconsidered if treatmentcan be initiated within6 hours.
FIGURE 1-2 Changes in final outcome as a result of intravenousrecombinant tissue-type plasminogen activator(IV rtPA) treatment within 3 hours of onset.
Reprinted from Saver JL, Medscape.7emedicine.
medscape.com/article/1160840-overview.
286 www.ContinuumJournal.com April 2014
Acute Stroke
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
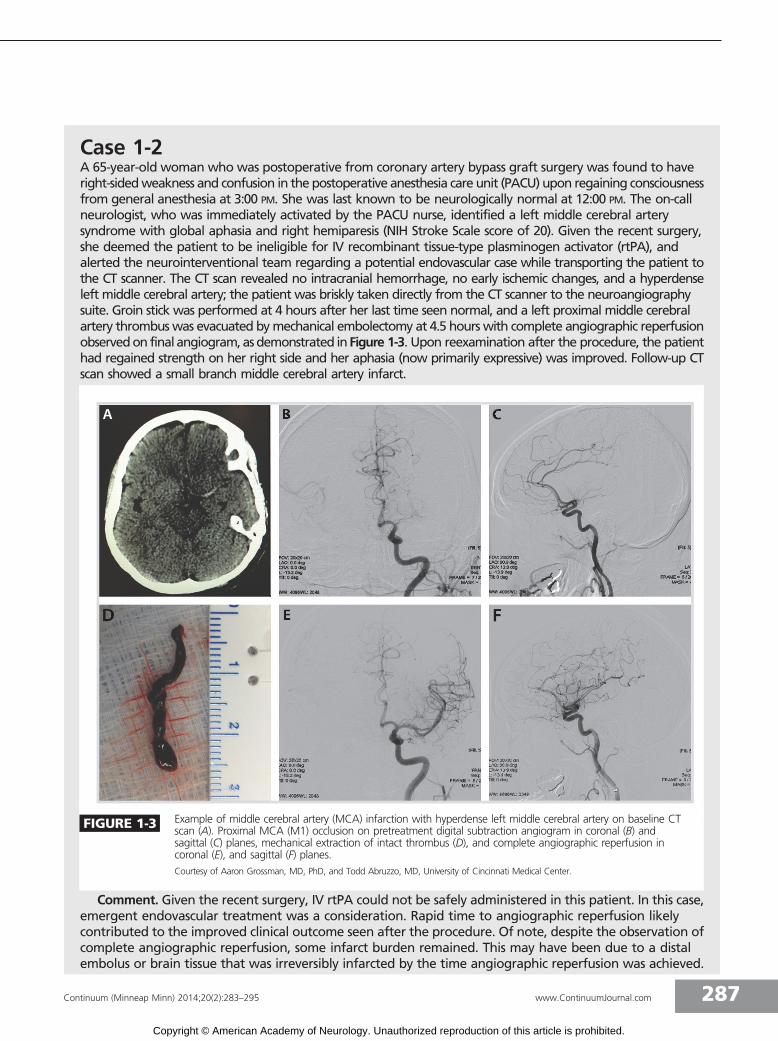
Case 1-2A 65-year-old woman who was postoperative from coronary artery bypass graft surgery was found to haveright-sidedweakness and confusion in thepostoperative anesthesia care unit (PACU) upon regaining consciousnessfrom general anesthesia at 3:00 PM. She was last known to be neurologically normal at 12:00 PM. The on-callneurologist, who was immediately activated by the PACU nurse, identified a left middle cerebral arterysyndrome with global aphasia and right hemiparesis (NIH Stroke Scale score of 20). Given the recent surgery,she deemed the patient to be ineligible for IV recombinant tissue-type plasminogen activator (rtPA), andalerted the neurointerventional team regarding a potential endovascular case while transporting the patient tothe CT scanner. The CT scan revealed no intracranial hemorrhage, no early ischemic changes, and a hyperdenseleft middle cerebral artery; the patient was briskly taken directly from the CT scanner to the neuroangiographysuite. Groin stick was performed at 4 hours after her last time seen normal, and a left proximal middle cerebralartery thrombuswas evacuated bymechanical embolectomy at 4.5 hours with complete angiographic reperfusionobservedon final angiogram,asdemonstrated inFigure 1-3. Upon reexamination after the procedure, the patienthad regained strength on her right side and her aphasia (now primarily expressive) was improved. Follow-up CTscan showed a small branch middle cerebral artery infarct.
Comment. Given the recent surgery, IV rtPA could not be safely administered in this patient. In this case,emergent endovascular treatment was a consideration. Rapid time to angiographic reperfusion likelycontributed to the improved clinical outcome seen after the procedure. Of note, despite the observation ofcomplete angiographic reperfusion, some infarct burden remained. This may have been due to a distalembolus or brain tissue that was irreversibly infarcted by the time angiographic reperfusion was achieved.
FIGURE 1-3 Example of middle cerebral artery (MCA) infarction with hyperdense left middle cerebral artery on baseline CTscan (A). Proximal MCA (M1) occlusion on pretreatment digital subtraction angiogram in coronal (B) andsagittal (C) planes, mechanical extraction of intact thrombus (D), and complete angiographic reperfusion incoronal (E), and sagittal (F) planes.
Courtesy of Aaron Grossman, MD, PhD, and Todd Abruzzo, MD, University of Cincinnati Medical Center.
287Continuum (Minneap Minn) 2014;20(2):283–295 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

predicted infarct core comprising 70%or more of ‘‘at-risk’’ tissue as identifiedby a complex voxel-by-voxel algorithm,and incorporating baseline NIHSS scorefor the CT-based cases as well. Patientsfor whom endovascular treatment couldbe initiated within 8 hours of symptomonset were randomized to mechanicalembolectomy versus supportive care,and stratified by the presence of penum-bra. The presence of penumbra did notdiscriminate between subjects who woulddifferentially benefit from mechanical em-bolectomy, but did predict better clinicaloutcomes among those with penumbraregardless of treatment arm. Evidence fornewer definitions of penumbra, and itsuse beyond 8 hours from onset, arelimited to nonrandomized cohort studiesof treated patients only.20,21 These single-arm trials are unable to discriminatebetween a predictor of treatment effectand a marker of better clinical outcomeregardless of treatment. This is an activearea of investigation, and several plannedand ongoing randomized trials will likelyinform this discussion in the future.22
Medical HistoryIn addition to eligibility based on timefrom onset, acute reperfusion treat-ment options are further determinedby eliciting key medical history.
IV rtPA exclusion criteria and relativecontraindications are listed in Box 1-1.1
A consensus definition of deficits thatshould typically be considered disabling(regardless of total NIHSS score) isshown in Table 1-1.
Based on limited evidence, poten-tial eligibility for endovascular therapyin IV rtPAYineligible patients mightinclude age younger than 85 years,NIHSS greater than or equal to 8, andtreatment within 6 hours of onset.1,10,11
Brief Examination and NIHSSThe examination helps the cliniciandetermine that the patient is indeedhaving a stroke and gauge its severity.The NIHSS score, in particular, is a usefulway to describe and follow the patient’sexamination (Appendix A). All clinicianswho care for stroke patients in theacute setting should be NIHSS certified
KEY POINTS
h Rapidly improvingdeficits should not beconsidered acontraindication unlessthe remaining deficitis minor.
h Additional exclusioncriteria for IVrecombinant tissue-typeplasminogen activatorwithin the 3- to4.5-hour time windowinclude a history ofstroke and diabetesmellitus, NIH StrokeScale score greater than25, age greater than80 years, and warfarinuse (regardless ofinternational normalizedratio value).
h All clinicians who carefor stroke patients in theacute setting should beNIH Stroke Scalecertified.
FIGURE 1-4 Devices cleared by the US Food and Drug Administration for acute stroke clot removal: A, Merci Retriever; B, Solitairestent retriever; C, Penumbra aspiration system; and D, TREVO2 stent retriever.
Panel A courtesy of Concentric Medical, Inc; Panel B courtesy of Covidien; Panel C courtesy of Penumbra, Inc; Panel D courtesy of Stryker.
288 www.ContinuumJournal.com April 2014
Acute Stroke
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

BOX 1-1 IV rtPA Exclusion and Relative Contraindication Criteria
Key IV rtPA Exclusion Criteria
& Stroke or significant head trauma within 3 months
& Major surgery or serious trauma within 14 days
& Gastrointestinal or urinary hemorrhage within 21 days
& Arterial puncture at a noncompressible site within 7 days
& History of intracranial hemorrhage
& Intracranial neoplasm, arteriovenous malformation, or aneurysm) Some experts consider treating patients with remotely secured or unruptured aneurysms
& Symptoms of subarachnoid hemorrhage
& Active internal bleeding
& Pretreatment blood pressure with systolic 9185 mm Hg or diastolic 9110 mm Hg
& Clear and large hypodensity on CT scan
& Current bleeding diathesis including
) International normalized ratio (INR) 91.7) Heparin within 48 hours resulting in abnormal partial thromboplastin time (PTT)) Platelets G100,000/mm3
) Direct thrombin inhibitor (eg, dabigatran) or factor Xa inhibitor (eg, rivaroxaban, apixaban)use within 48 hours
h Optimal laboratory testing thresholds for safe IV recombinant tissue-type plasminogenactivator (rtPA) use in this setting remain to be determined and are an area of activeinvestigation.
& Serum glucose G50
) If persistent symptoms after correction, or infarct is verified/supported by imaging, most expertswould consider IV rtPA treatment.
Relative Contraindications for IV rtPA1
& Minor deficit) Rapidly improving deficits should not be considered a contraindication unless the remainingdeficit is minor.23
) A common definition of minor deficits is an NIH Stroke Scale (NIHSS) score e5 and not clearlydisabling.
) A consensus definition of deficits that should typically be considered disabling (regardless of totalNIHSS score) is shown in Table 1-1.
& Myocardial infarction in the past 3 months) Some experienced centers treat this as a contraindication only if the myocardial infarction issubacute and transmural, or other signs suggest a high risk of hemopericardium, such as clinicalor ECG evidence of pericarditis.
) Concurrent acute myocardial infarction may benefit from IV rtPA as well and should beconsidered in consultation with a cardiologist; however, only lower stroke dosing of 0.9 mg/kg(not higher cardiac dosing of approximately 1.1 mg/kg) should be used in this setting.
& Seizure at presentation) If stroke is verified by imaging, IV rtPA treatment should be considered. However, the severity ofconcurrent stroke must be judged in the context of ictal/postictal presentation.
& Pregnancy) Must weigh risks and benefits in the individual circumstances.
Continued on next page
289Continuum (Minneap Minn) 2014;20(2):283–295 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

(http://nihss-english.trainingcampus.net/uas/modules/trees/windex.aspx).However, emergency physicians arenot always NIHSS trained, and a de-scriptive examination can be usedto estimate the NIHSS score andthereby the severity of the stroke in thatcircumstance.
Treating a stroke mimic, such asa complicated migraine or seizure,with IV rtPA is inevitable sometimes.Fortunately, the risk of intracranialhemorrhage when treating a strokemimic with IV rtPA inadvertently isextremely low (less than 1%) based oncase series of tPA-treated strokemimics and the cardiology literature.24
Therefore, time to treatment shouldnot be lost with ancillary testing suchas MRI or CT angiography if strokeseems likely but not definitive.
The role of adjunctive endovasculartreatment for severe IV rtPAYtreatedischemic strokes remains to be deter-mined. The only randomized trial ofthe combined IV rtPA/endovascularapproach to date, the InterventionalManagement of Stroke (IMS) III trial,did not demonstrate its superiorityover IV rtPA alone among subjects of18 to 83 years of age with severestrokes (NIHSS score of 8 or higher),although safety parameters werecomparable.25 The trial results alsosuggested that the clinical benefit ofsuccessful flow restoration may be lostbeyond 7 hours from stroke onset inthe average patient. It has been hy-pothesized that subgroups of patientsmay benefit from endovascular therapy,such as those with the most severedeficits (eg, an NIHSS score greater than
KEY POINTS
h The risk of intracranialhemorrhage whentreating a stroke mimicwith IV recombinanttissue-type plasminogenactivator inadvertentlyis extremely low (lessthan 1%).
h The combined IV/endovascular approachin all patients with anNIH Stroke Scale scoreof 8 or greater is notsuperior to IVrecombinant tissue-typeplasminogen activatoralone despitecomparable safety.
BOX 1-1 IV rtPA Exclusion and Relative Contraindication Criteria (continued)
Additional Exclusion Criteria for IV rtPA Within the 3- to 4.5-Hour Time Window1
& History of stroke AND diabetes mellitus
& NIHSS score 925
& Age 980 years old
& On warfarin (regardless of INR value)
TABLE 1-1 Proposed Operational Definition of Disabling Deficitsa,b
The following typically should be considered disabling deficits:
Complete hemianopsia (Q2 on NIH Stroke Scale [NIHSS] question 3), or
Severe aphasia (Q2 on NIHSS question 9), or
Visual or sensory extinction (Q1 on NIHSS question 11), or
Any weakness limiting sustained effort against gravity (Q2 on NIHSSquestion 6 or 7),
Any deficits that lead to a total NIHSS 95, or
Any remaining deficit considered potentially disabling in the view of thepatient and the treating practitioner. Clinical judgment is required.
a Reprinted with permission from Re-examining Acute Eligibility for Thrombolysis (TREAT) TaskForce, Stroke.23 stroke.ahajournals.org/content/44/9/2500.abstract.
b All neurologic deficits present at the time of the treatment decision should be considered inthe context of individual risk and benefit, as well as the patient’s baseline functional status.
290 www.ContinuumJournal.com April 2014
Acute Stroke
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

20), patients with demonstrated largeproximal arterial occlusions (such asinternal carotid artery terminusocclusionsor occlusions that are greater than 8 mmin length), and those whose occlusionsare recanalizedmore rapidly or effectively.Several randomized trials of more selec-tive patient subgroups are nowunderway.
Glucose and Other LaboratoryResultsTesting for serum glucose level isnecessary before the IV rtPA treatmentdecision.1 This should take minimaltime when performed by finger stickand is often done by EMS en route.This test allows the clinician to excludestroke mimics of hypoglycemia orhyperglycemia. If the hypoglycemicpatient’s symptoms resolve after glu-cose administration, then IV rtPA maynot be indicated. Hyperglycemia canpresent with choreiform movementsthat can be mistaken for stroke symp-toms. Experts generally believe thatneither hypoglycemia nor hyperglyce-mia should preclude IV rtPA treatmentif the deficits are believed to be causedby concurrent ischemia.
Other laboratory results should be so-licited if available, but they are not ne-cessary. In particular, INR, PTT, andplatelet count will help determine IV rtPAeligibility. However, IV rtPA administrationshould not be delayed for any laboratoryresult other than finger-stick glucoselevel unless a clinical suspicion for anabnormality exists. Fewer than three in1000 patients will have unsuspectedthrombocytopenia,26 and fewer than fourin 1000 patients will have an unsus-pected INR greater than 1.7.27
Blood PressureBlood pressure is generally maintainedrelatively high after acute ischemicstroke. In the setting of cerebral ischemia,a loss of cerebral autoregulation occurssuch that systemic blood pressures
directly affect cerebral perfusion pres-sure. In this setting, increased systemicblood pressure will improve blood flowto the cerebral infarct, often via collateralblood vessels, and thereby may reducethe extent of irreversible ischemia.
The upper limits of blood pressurecontrol are dictated by the decision ofwhether to administer acute reperfu-sion therapy. The blood pressuremust be less than 185 mm Hg systolicand 110 mm Hg diastolic for IV rtPAeligibility, and must be maintainedbelow 180/105 mm Hg during andafter IV rtPA administration. Gentleblood pressure reduction can usuallybe achieved with labetalol 10 mg IV. Ifthis dose is not enough, then it mightbe doubled. If no response occurs, anicardipine infusion (5 mg per hourIV, titrate up by 2.5 mg per hour every5 to 15 minutes, maximum 15 mg perhour) may be needed and typicallyachieves the blood pressure goals. Ifnicardipine is not available, or contra-indications exist for this or labetalol,another consideration is IV enalaprilat3.25 mg to 6.5 mg.
Acute Brain ImagingImaging of the brain parenchyma servesthe primary role of ruling out intracranialhemorrhage, including intracerebral,subarachnoid, and epidural/subdural lo-cations. At most centers, a noncontrastCT scan is the most rapid modalityavailable, although some centers mayuse limited MRI (specifically consistingof diffusion-weighted imaging [DWI],either susceptibility-weighted [SW] im-aging or gradient echo [GRE] se-quences, and fluid-attenuated inversionrecovery [FLAIR] sequences) if rapidlyavailable. Rarely, an acute CT scan willreveal a large and clear hypodensity thatwill lead to questioning the time ofonset of the stroke and the possibilityof an undiagnosed subacute stroke,both of which would contraindicate IV
KEY POINT
h One should not delay IVrecombinant tissue-typeplasminogen activatoradministration for anylaboratory result otherthan finger-stick glucoselevel unless a clinicalsuspicion for anabnormality exists.
291Continuum (Minneap Minn) 2014;20(2):283–295 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

rtPA. Subtle changes may also be seenon CT scan, such as loss of gray-whitedifferentiation or sulcal effacement, tosupport the diagnosis of ischemicstroke. While subtle ischemic changeson CT scan are not contraindications toacute reperfusion therapy, they doportend worse outcomes comparedwith those with lesser acute ischemicchanges on CT scan.28
Advanced imaging, specifically headand neck vascular imaging with CTangiography or magnetic resonanceangiography, can be valuable in plan-ning the approach to endovasculartherapy if indicated, determining theetiology of stroke for secondary pre-vention (eg, carotid endarterectomy),or obtaining supportive evidence foran ischemic stroke diagnosis. Usingthis as a first-line imaging approach forall ‘‘rule-out stroke patients’’ in anemergency department is likely to beinappropriate, given the additionalradiation exposure to a diverse groupof patients. In settings where an expertphysician triages stroke patients, CTangiography or magnetic resonanceangiography may be useful in selectedcases (ie, IV rtPAYineligible patients whoarrive in the emergency departmentearly) to identify symptomatic occlu-sions amenable to acute endovasculartherapy while the neurointerventionalteam is being mobilized. In all cases,advanced neuroimaging should not de-lay the administration of IV rtPA.
To date, there is no known role forother forms of advanced imaging,such as perfusion studies with CTperfusion or magnetic resonanceperfusion-weighted imaging, to selectpatients for acute reperfusion thera-pies. In particular, no data havesupported the utility of identifyingpenumbra (ie, brain at risk for infarc-tion without reperfusion) for IV rtPAdecisions, as the majority of thesepatients will have penumbra within
4.5 hours, and the role of penumbralimaging for selecting patients for acutereperfusion treatment beyond 4.5 hoursremains to be determined (as discussedearlier in this review).
POSTREPERFUSION THERAPYCAREStandard post-tPA management for thefirst 24 hours includes the following:
& admission to a step-down orintensive care unit
& maintenance of nothing-by-mouth(NPO) status until dysphagiascreening is performed to avoidaspiration pneumonia
& administration of isotonic IV fluids(not dextrose containing becauseof risk of hyperglycemia)
& blood pressure and neurologicmonitoring every 15 minutes for2 hours, then every 30 minutesfor 6 hours, then every hour for16 hours after treatment
& aggressive blood pressure treatmentif systolic blood pressure is greaterthan 180 mm Hg or diastolic bloodpressure is greater than 105 mm Hg
& emergent CT scan of the brain ifneurologic decline, acute increasein blood pressure, nausea, vomiting,or new headache is present to ruleout hemorrhagic transformation
& repeat brain imaging at 24 hoursto assess for asymptomatichemorrhage and to allow initiationof antiplatelet therapy
OTHER ACUTE ISCHEMICSTROKE MANAGEMENTCONSIDERATIONSBlood Pressure in Patients WithNo Reperfusion TherapiesData are very limited to dictate theoptimal blood pressure in this set-ting. Experts generally recommendpermissive hypertension if tolerated
KEY POINTS
h Subtle ischemic changeson CT scan are notcontraindications toacute reperfusiontherapy.
h Standard postYtissueplasminogen activatormanagement for thefirst 24 hours includesaggressive blood pressuretreatment if systolic bloodpressure is greater than180 mm Hg or diastolicblood pressure is greaterthan 105 mm Hg.
292 www.ContinuumJournal.com April 2014
Acute Stroke
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

(up to 220/120 mm Hg) in the non-reperfusion therapy setting and con-sideration of lowering blood pressureby 15% over the first 24 hours.1
Less commonly, blood pressuremay be low in the acute setting, andstroke deficits may improve with raisingthe pressure. Most experts will attemptIV fluid boluses to raise blood pressurein the setting of relative hypotensionand see if stroke symptoms improvewith this intervention. If the strokedeficits appear to be pressure depen-dent, more aggressive blood pressuresupport with pressors may be consid-ered. Evidence for the role of pressorsin the acute stroke setting is limited,however.
Glucose in the Acute SettingHyperglycemia (greater than 140 mg/dL)during the first 24 hours after stroke is apoor prognostic indicator.Whether acutecorrection will lead to better clinical out-comes after stroke is unknown. Currentrecommendations are to treat hyper-glycemia to achieve a level lower than180 mg/dL, and stricter glucose controlis under study in a major randomizedclinical trial.1
Antithrombotic Therapy in theAcute SettingAspirin should be initiated within 48hours in all patients and is typicallyinitiated in the emergency departmentif no acute reperfusion therapy isadministered. If IV rtPA or acuteendovascular therapy is administered,aspirin is initiated at approximately 24hours and only after confirmation of nohemorrhagic transformation on the24-hour CT scan. Early aspirin treat-ment leads to a 1% absolute reductionof stroke over the next 2 weeks.29,30
Recent evidence from a randomizedtrial in China of TIA and minor strokepatients who were not treated with IVtPA has suggested that short-term
combined aspirin and clopidogrel admin-istration may better prevent early strokerecurrence in minor strokes or TIAs, andfurther randomized study is currentlyunderway in the United States.31
It is well established that acuteanticoagulation (including unfractionatedand low-molecular-weight heparin)does not improve clinical outcomesafter acute ischemic stroke comparedwith antiplatelet therapy in unselectedpatients. There may be a role for acuteanticoagulation in specific circum-stances in which early stroke recurrencerisk is high, but clinical data are lacking.
SUMMARYIn summary, effective emergent evalua-tion of a stroke patient requires well-organized systems that maximize speedof assessment and administration ofappropriate therapies. This article pro-vides a practical overview of this pro-cess, and the reader is referred to theAmerican Heart Association/AmericanStroke Association clinical guidelinesfor more detailed discussions. Whenthese systems cannot appropriately beimplemented at a given hospital, it isimperative that triage and bypass plansbe implemented to maximize clinicaloutcomes after stroke.
REFERENCES1. Jauch EC, Saver JL, Adams HP, et al.
Guidelines for the early management ofpatients with acute ischemic stroke: a guidelinefor healthcare professionals from theAmerican Heart Association/American StrokeAssociation. Stroke 2013;44(3):870Y947.
2. Tissue plasminogen activator for acuteischemic stroke. The National Institute ofNeurological Disorders and Stroke rt-PAStroke StudyGroup.N Engl JMed1995;333(24):1581Y1587.
3. Hacke W, Donnan G, Fieschi C, et al;ATLANTIS Trials Investigators; ECASS TrialsInvestigators; NINDS rt-PA Study GroupInvestigators. Association of outcome with
KEY POINTS
h Experts generallyrecommend permissivehypertension if tolerated(up to 220/120 mm Hg)in the nonreperfusiontherapy setting.
h Current recommendationsare to treat hyperglycemiato a level lower than180 mg/dL.
h Early aspirin treatmentleads to a 1% absolutereduction of stroke overthe next 2 weeks.
h Short-term combinedaspirin and clopidogreladministration maybetter prevent earlystroke recurrence inminor strokes or TIAs.
293Continuum (Minneap Minn) 2014;20(2):283–295 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

early stroke treatment: pooled analysis ofATLANTIS, ECASS, and NINDS rt-PA stroketrials. Lancet 2004;363(9411):768Y774.
4. Lees KR, Bluhmki E, von Kummer R, et al.Time to treatment with intravenousalteplase and outcome in stroke: an updatedpooled analysis of ECASS, ATLANTIS, NINDS,and EPITHET trials. Lancet2010;375(9727):1695Y1703.
5. Khatri P, Abruzzo T, Yeatts SD, et al. Goodclinical outcome after ischemic stroke withsuccessful revascularization is time-dependent.Neurology 2009;73(13):1066Y1072.
6. Marler JR, Jones PW, Emr W. Proceedings ofa national symposium on rapid identificationand treatment of acute stroke. Bethesda,MD: The National Institute of NeurologicDisorders and Stroke (NINDS), NationalInstitutes of Health, 1997;97:4239.
7. Saver JL. Thrombolytic therapy in stroke.Medscape. emedicine.medscape.com/article/1160840-overview. Updated September 18,2012. Accessed February 6, 2014.
8. Gadhia J, Starkman S, Ovbiagele B, et al.Assessment and improvement of figures tovisually convey benefit and risk of strokethrombolysis. Stroke 2010;41(2):300Y306.
9. Graham GD. Tissue plasminogen activatorfor acute ischemic stroke in clinical practice:a meta-analysis of safety data. Stroke2003;34(12):2847Y2850.
10. The IST3 Collaborative Group. The benefitsand harms of intravenous thrombolysis withrecombinant tissue plasminogen activatorwithin 6 h of acute ischaemic stroke (thethird international stroke trial [IST-3]): arandomised controlled trial. Lancet2012;379(9834):2352Y2363.
11. Furlan A, Higashida R, Wechsler L, et al.Intra-arterial prourokinase for acuteischemic stroke. The PROACT II study: arandomized controlled trial. Prolyse inacute cerebral thromboembolism. JAMA1999;282(21):2003Y2011.
12. Ogawa A, Mori E, Minematsu K, et al.Randomized trial of intraarterial infusion ofurokinase within 6 hours of middle cerebralartery stroke: the middle cerebral arteryembolism local fibrinolytic interventiontrial (MELT) Japan. Stroke 2007;38(10):2633Y2639.
13. Fields JD, Khatri P, Nesbit GM, et al.Meta-analysis of randomized intra-arterialthrombolytic trials for the treatment ofacute stroke due to middle cerebral arteryocclusion. JNeurointerv Surg2011;3(2):151Y155.
14. Nogueira RG, Lutsep HL, Gupta R, et al.Trevo versusMerci retrievers for thrombectomy
revascularisation of large vessel occlusions inacute ischaemic stroke (TREVO 2): a randomisedtrial. Lancet 2012;380(9849):1231Y1240.
15. Saver JL, Jahan R, Levy EI, et al. Solitaire flowrestoration device versus the Merci Retrieverin patients with acute ischaemic stroke(SWIFT): a randomised, parallel-group,non-inferiority trial. Lancet 2012;380(9849):1241Y1249.
16. Bose A, Henkes H, Alfke K, et al. ThePenumbra System: a mechanical device forthe treatment of acute stroke due tothromboembolism. AJNR Am J Neuroradiol2008;29(7):1409Y1413.
17. Ciccone A, Valvassori L, Nichelatti M, et al.Endovascular treatment for acute ischemicstroke. N Engl J Med 2013;368(10):904Y913.
18. Chalela JA, Katzan I, LiebeskindDS, et al. Safetyof intra-arterial thrombolysis in the postoperativeperiod. Stroke 2001;32(6), 1365Y1369.
19. Kidwell CS, Jahan R, Gornbein J, et al. A trialof imaging selection and endovasculartreatment for ischemic stroke. N Engl J Med2013;368(10):914Y923.
20. Lansberg MG, Straka M, Kemp S, et al. MRIprofile and response to endovascularreperfusion after stroke (DEFUSE 2): aprospective cohort study. Lancet Neurol2012;11(10):860Y867.
21. Jovin TG, Liebeskind DS, Gupta R, et al.Imaging-based endovascular therapy foracute ischemic stroke due to proximalintracranial anterior circulation occlusiontreated beyond 8 hours from time last seenwell: retrospective multicenter analysis of237 consecutive patients. Stroke 2011;42(8):2206Y2211.
22. Parsons MW, Albers GW. MR RESCUE: is theglass half-full or half-empty? Stroke2013;44(7):2055Y2057.
23. The Re-examining Acute Eligibility forThrombolysis (TREAT) Task Force; Levine SR,Khatri P, Broderick JP, et al. Review, historicalcontext, and clarifications of the NINDSrt-PA stroke trials exclusion criteria part 1:rapidly improving stroke symptoms. Stroke2013;44(7):2055Y2057.
24. Tsivgoulis G, Alexandrov AV, Chang J, et al.Safety and outcomes of intravenousthrombolysis in stroke mimics: a 6-year,single-care center study and a pooledanalysis of reported series. Stroke2011;42(6):1771Y1774.
25. Broderick JP, Palesch YY, Demchuk AM,et al. Endovascular therapy after intravenoust-PA versus t-PA alone for stroke. N Engl JMed 2013;368(10):893Y903.
294 www.ContinuumJournal.com April 2014
Acute Stroke
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

26. Cucchiara BL, Jackson B, Weiner M, MesseSR. Usefulness of checking platelet countbefore thrombolysis in acute ischemicstroke. Stroke 2007;38(5):1639Y1640.
27. Rost NS, Masrur S, Pervez MA, et al.Unsuspected coagulopathy rarely preventsIV thrombolysis in acute ischemic stroke.Neurology 2009;73(23):1957Y1962.
28. Demchuk AM, Hill MD, Barber PA, et al.Importance of early ischemic computedtomography changes using ASPECTS inNINDS rtPA Stroke Study. Stroke 2005;36(10):2110Y2115.
29. CAST: randomized placebo-controlled trialof early aspirin use in 20,000 patients withacute ischaemic stroke. CAST (Chinese AcuteStroke Trial) Collaborative Group. Lancet1997;349(9066):1641Y1649.
30. The International StrokeTrial (IST): a randomisedtrial of aspirin, subcutaneous heparin, both, orneitheramong19435patientswithacute ischaemicstroke. Lancet 1997;349(9065):1569Y1581.
31. Wang Y, Wang Y, Zhao X, et al. Clopidogrelwith aspirin in acute minor stroke ortransient ischemic attack. N Engl J Med2013;369(1):11Y19.
295Continuum (Minneap Minn) 2014;20(2):283–295 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.




























