-
What even is Surgo? 80th Anniversary Special Edition
2015; 87:3
-
Anxious about your exams?
Revise with PasTest for up-to-date content created for your
medical school exams
Online revision for your OSCEs, PSA, SJT & Finals1000s of
exam-format questions specific to Glasgows exams, along with
videos, tutorials, spot diagnosis clips, podcasts and free
mobile app.
Try before you buy with free 2-week demos for Finals &
OSCEs
www.pastest.co.uk
Starting from 10 for 6 months access
10 OFFMedical Student Finalswith this discount code
SURGO10
25% OFF PasTest booksPlus free UK postage for all online
subscribers!
-
..
ADDRESSES AND PAPERS
History of Surgo
by Tom H. Baddeley
Medical News
by Jamie Henderson
Madness at Arkham Asylum
by Dr Colm Hennessy
Playing the Supervisor Game
by Trung Ton
How to Get the Most Out of Clinical Placement
by Tom Ainge
Losing Our NHS
by Michaela Jewson
ADDRESSES AND PAPERS
The Lectured Become the Lecturers
by Jenna Woods
Happenings in MedChir
by Tom Baddeley
We Ballsed it Up
by Year Club Beta
Transverse Acetabular Ligament
by Craig R Johnstone
SHITS
by Daniel Taylor-Sweet
Ethics Case
by GUGPS
It has been a busy semester for the Surgo
committee. 1st and 2nd years have almost completed
their studies and are now preparing for the upcoming
exams . 3rd and 4th years made it through their
notorious clinical exams and are now starting their
placement and specialities blocks. Finally the 5th
years are starting p4p and becoming actual, legit
doctors...there really is no rest for a medical student!
(Apart from Intercal).
Surgo is celebrating its 80th (Oak)
anniversary this year and is ready to lighten-up your
coffee break. Due to popular demand, we start with
the history and the formation of Surgo to ask the
ageless question of what even is Surgo. Following
this, Jamie gives us a summary of recent medical
news and former Surgo editor and psychiatrist Dr
Colm Hennessey gives us a portrayal of psychiatry in
the media based on the Batman universe. Since half
the medical school is on placement at the moment,
Trung has enlightened us in how to play the
supervisor game and Tom Ainge (ft. beta-17 year
club) helps us get the most out of clinical placements.
Michaela confirms her distaste for the Tories in a
shocking reveal of the creeping privatisation in the
NHS (a must-read). Dan sticks to his strengths and
gives us the abstract of Surgo's next clinical trial:
SHITS (Surgo's highly interesting toilet trial). But
wait, there's more! An ethical case from the Glasgow
University General Practice Society, Jenna's inquiry
into if attendance should be monitored in lectures, an
abstract from Craig Johnstone, a review of the 3rd
year ball and finally a summary of recent Med-Chir
events. Enjoy!
Tom Baddeley, Editor of Surgo
Editorial
-
Many a student at Glasgow Medical School
has asked themselves this eternal question:
what even is Surgo? Surgo is 80 years old
this year and so I feel we all deserve a
clarification of how Surgo came to be. Lets
start from the very beginning
Despite the University of Glasgow being
founded in 1451 it did not have a dedicated
medical faculty until the end of the 18th
century; anyone who wanted to become a
doctor had to travel to Italy or the
Netherlands for university. The medical
profession in Glasgow during the 16th
century was: one physician, six barber
surgeons and two midwives, so not enough
to support a population of 7000. Glasgow
back then had terrible weather, no
sanitation and was rife with leprosy and
other infectious diseases, so much like it is
now! Lepers were sent to St Ninians Croft,
a hospital near present-day Gorbals. Here
they were looked after but had to wear a
long gown with hood and sleeves closed at
the fingertips and rattling clappers if they
wanted to leave the hospital, to warn
others of their presence. After several
outbreaks of leprosy and syphilis, the
powers in charge decided that the
University and the Clergy appoint someone
to be in charge of the medical faculty in
Glasgow. They decided on Maister Peter
Lowe, who settled in Glasgow in 1598.
This high-achieving man was trained in
Paris and had 22 years of experience of
battlefield medicine whilst working with the
French and Spanish armies. He was
employed and founded the Faculty of
Physicians and Surgeons, Glasgow on the
3rd June 1603.
The Medico-Chirurgical Society of Glasgow
was founded in 1802 but it wasnt until
1934 when the idea arose that the society
should have a medical journal. The first
steps were taken by Mr Uytman and
several other medical students who looked
into how much it would cost to run and set
up. Mr Uytman was the Med-Chir
treasurer at the time and offered the idea
at a meeting on the 22 November 1934. Mr
Leckie was president and supported the
motion, appointing the members who
proposed Surgo as the initial committee. A
star was born.
The first issue went to print in January
1935 and here are the opening words of the
editorial:
At a time when the Medico-Chirurgical
Society of Glasgow University, by means of
its numerous progressive activities, has
definitely established itself as one of the
most important influences upon the life of
the medical students of the university this
year the membership exceeds the five
hundred mark it is particularly fitting that
the society should have considered
publishing a medical journal.
Mr Uytman then goes on to outline the
three aims (I feel we have pretty much
stuck to them):
1. In the first place, Surgo provides a
means of publication of papers written
by students.
2. Secondly, Surgo will provide an
excellent medium for the orderly,
original and articulate expression of
student opinion on all matters of
medical interest
3. Thirdly, Surgo is intended to be a
source of information. Surgo as the
instrument of the society will satisfy a
long felt want in the matter of
publishing items of news both local
and general, which are of interest to
the medical student.
As it turns out, Surgo means I arise in
Latin; this is because Surgo arose like a
phoenix from the ashes of a former
publication called The Scalpel which
allegedly had to be shut down due to it
containing gross personalities and articles
calculated to excite feelings dangerous to
the security of the college. They were
probably proposing inflammatory ideas
such as accepting women into medical
school.
Surgo went on sale for 5 shillings a year,
so roughly 12 in our money. Surgo also
had companies pay for advertising space,
much like now. But this was before the
age of multinational healthcare companies
and old so Surgo editions featured adverts
from private companies for surgical tools,
prosthetic limbs etc. as well as household
names like Guinness and Tennents. The
advert below is advertising hernia trusses
and surgical belts. The shop itself
occupied 249 Buchanan Street, where
Topshop is now and having tried to fit into
Topman jeans in the past I can imagine
hernia belts are not too dissimilar. During
World War 2 Glasgow medical school found
it difficult to produce doctors fast enough
for the war effort, there were a number of
articles published discussing whether the
course should be shortened or if extra
semesters should be brought in to 1st and
2nd years. They also discuss how Glasgow
is the only Scottish university with no
military training; this could be the liberal
anti-war spirit of Glasgow coming through
or maybe just the med school hadnt got
round to organising it yetwho knows.
During the war and the post war period,
Surgo struggled to find sponsors and the
wartime paper shortage almost ended it for
good, but plucky old Surgo powered on
through.
Whilst reading through old issues of Surgo
and old Med-Chir minutes from the last
century, I unfortunately sensed a level of
underlying sexism. An example of this is
just after when women were officially
allowed to enter the GUU in 1977, Med-
Chir organised a field day in 1978 where
there was debating, sports at Garscube and
snooker and darts in the mens union.
The rules officially state men only as
players and spectators for the snooker and
darts, so I can guess where Med-Chir stood
on the mixed-sex union dispute. However
there was a beer drinking competition and
night out in the Savoy Centre afterwards,
all sponsored by MPS - which sounds more
like the Med-Chir we all know.
Surgo was much like it is now from the
1980s onwards with the same light-hearted
look on life as a medical student. It has
had its ups and downs but for a student
magazine to be celebrating its 80th
anniversary, it must be something special.
As long as Glasgow has a medical school I
believe it is important that Surgo should
exist to act as an impartial judge, holding
the medical school accountable if needed
and to allow medical students to voice their
opinions. In doing this Im sure Surgo will
be celebrating its 160th anniversary in 80
years time.
What even is Surgo? by Tom Baddeley
-
MEDICAL NEWS
Scottish hospitals show improvement in mortality People dont go
into hospital to die; at least that is the idea. But inevitably
patients do. This can be due the result of the condition of the
patient on
admittance, but some deaths can be prevented by improving care
and not
causing harm (beneficence and non-maleficence). It was with this
aim that the
Scottish Patient Safety Programme (SPSP) was set up. It has seen
a reduction in
the Hospital Standardised Mortality Ratios (HSMR) of 16.3% over
the whole of
Scotland. The Southern General managed to reduce its HSMR by
more than
20%: the target for the end of 2015.
Attractive Men Are Selfish Resear che rs f r om Brune l
University have found that
attractive men are more likely to
be less generous and favour
equality less than their less
attractive counterparts; the
same could not be said of
women. Therefore there is a
lesson to all; be careful who you
go on dates with. You may end
up paying for it.
Chocolates on wards at high risk Dont leave food, particularly
chocolate, around
a ward as they will vanish quickly. A
multicentre trial, published in the BMJ, has
found that the half-life of a chocolate on a ward
is remarkably small - 1hr 39 minutes. It takes
only 12 minutes for a box of chocolates to be
opened. The main culprits in this study were
health care assistants and nursing staff,
composing 28% of consumers; doctors didnt
fair too well either, coming third overall. So
next time you grab a Quality Street on a ward
be careful, someone may well be watching you!
Hold the press, binge drinking is over In a report from the
Office of National Statistics (think grey suits and lots of SPSS),
they have reported that binge drinking is waning in the UK, with
more people than ever being teetotal. Young people (
-
Madness at
Arkham Asylum
rkham Asylum looms high over Gotham.
Or sometimes it sits on an island in the
bay. Or is dwarfed by the modern buildings
around it. Or maybe it becomes part of the city,
a segment where anarchy reigns. While the
details vary, one fact always remains: its where
the bad people are. Where the murderers,
anarchists and freaks of the Batman world are
sent after being captured by the Dark Knight.
There they stay for a while, contained,
sometimes experimented on. They are never
cured, never successfully helped. Sometimes
they are discharged by misguided staff,
sometimes the staff even help them escape.
Because they always escape, and return to
their life of crime, and then return to Arkham a
while later. No one gets better at Arkham, no
good is ever truly done. The patients do not
recover, and society is never safeguarded.
Gotham is indeed where the bad people are.
n the wide pantheon of superheroes, no
character or title has paid as much lip
service to the medical speciality of psychiatry
as Batman has. The hero himself, irrespective
of the portrayal, is always fuelled by trauma
the murder of his parents, and a fear of bats.
His villains are often described as mad, or
s c h i z o p h r e n i c ( i n c l u d i n g t h e g r e a
t
misunderstanding of schizophrenia as spilt
personality, personified by Harvey Two-Face
Dent). He has even faced a remarkable number
of evil psychiatrists over the years: Harleen
Harley Quinn Quinzell, Jonathan Scarecrow
Crane, Dr Hugo Strange, and others. Not only
are bad people held in the citys secure
psychiatric hospital, but the madness is
seemingly contagious, regularly spreading to
the abusive and incompetent staff. Even the
origins of Arkham lie in madness: the name
itself comes from the Cthulhu mythos of HP
Lovecraft , whose arcane tales told of
otherworldly insanities forever pushing in on
reality. And old Jeremiah Arkham himself, the
architect and founder of the hospital, fell to
madness, shuffling through the halls of the
institution he built.
atman is not unique in its portrayal of
mental illness as being synonymous with
evil and danger, but it is perhaps remarkable in
its unreconstructed and profligate portrayal.
The institution itself entered the Batman comic
book in the early 1970s, at a time when
psychiatry was recovering from the excesses of
institutionalisation and the barbarism of the
lobotomy era. Effective medications were by
t h e n a v a i l a b l e , a n d t h e a g e o f d e -
institutionalisation was beginning. But the
image of psychiatry, then as now, was still one
of custody and madness. Arkham thus became
a super-villain take of One Flew Over the
Cuckoos Nest, where no one ever recovers and
people are contained rather than treated.
owhere is the Arkham Effect greater
than in the character of The Joker.
Batmans greatest villain, he serves as an
anarchistic riposte to Batmans fascistic
leanings. The Joker is unpredictable, unhinged
and extremely dangerous. He has taken the
A
I
B
N
-
lives of countless Gothamites, including
(during the Death in the Family storyline)
Batmans young ward, Robin. But despite his
leanings towards anarchy, he is a methodical
criminal mastermind. There is no hint in his
portrayal that he is depressed, or bipolar.
Although unhinged, his mind maintains a
consistency of thought and action that is not in
keeping with psychosis. There have been
instances of catatonia (most notable in Frank
Millers The Dark Knight Returns). But, if any
diagnosis were to stick with The Joker, it would
be psychopathy.
f Scotland has an institution equivalent to
Arkham Asylum, it would be The State
Hospital at Carstairs. I have worked there
myself. Rather than a gothic building of spires
and watchtowers, it is a series of modern flat-
roofed buildings set on a remote and windy
patch of central belt countryside. As opposed to
being a chaotic and abusive place, it is a
controlled and contained environment. To be
sent to Carstairs, one must generally have a
significant mental health problem in addition
to requiring a high-secure environment. As a
rule the focus is on recovery (if possible)
enabling the patient to move to a less-secure
environment. There are medications, therapy
groups, passes to the community. The other
fact that sets Carstairs apart from Arkham is
that The Joker would never get in. Because
psychopathy, by virtue of not being a treatable
mental illness, is the domain of the Scottish
prison system.
here is one other particularly troubling
aspect of The Joker, and that is the fate of
his psychiatrist Dr Harleen Quinzel. It is
something of a trope in popular culture that
psychiatrists fall in love with their patients, but
Dr Quinzels case is even more troubling: she
styles herself after him, becoming a deranged
super-villain named Harley Quinn, and begins
a life of crime and terrorism specifically to
garner the affections of The Joker. It is here
that one of the most troubling aspects of
stigma is personified: that mental illness is in
some way contagious, and that spending time
with the mad can make oneself insane.
hen I decided to become a psychiatrist,
there were a few comments that I grew
tired of hearing pretty quickly. Some people,
including relatives, worried about my safety;
that the dangerous patients would turn on
me. Others joked I would become mad myself.
Finally people asked why I did not want to be a
real doctor, as if I was abandoning medicine
for imprisonment and mysticism. Stigma is not
just damaging to our patients, who must
contend not just with mental illness but also
with the fear and ignorance of society. Stigma
is also directed towards psychiatrists
themselves, who are frequently regarded as
bizarre, unhinged, and perhaps inferior to their
medical colleagues.
t is hard to judge the effect of constructs
such as Arkham Asylum on stigma towards
psychiatry. Of course Arkham is one (albeit
central) part of the Batman mythology, and
Batman is only one (very well-known)
character. What Arkham Asylum is, though, is
part of a wider trend of portrayal of psychiatry
in the media. And while stigma is a wide issue,
it has its beginnings in the public perception of
mental illness. Arkham looms large in comic
books, videogames and movies. People who
grow up on Batman become aware of it, and
this terrifying and nasty environment must
surely become internalised, one of many
impressions to be called upon when they
encounter mental illness in the future. And
there it will remain: gothic environments, scary
patients, evil staff, and no recovery.
I
T
W
I
Cby Dr olm Hennessy ST6 in Child and Adolescent Psychiatry
Former Surgo Editor
H
-
PLAYING THE SUPERVISOR
THE ENIGMA
So its nearly the end of week 3 of 5 of your placement and youre
starting to wonder, when will I meet my supervisor? Why haven't
they replied to my five thousand emails asking to meet?
The enigma is clearly a busy doctor who hardly has time for
themselves l e t a lone a med ica l s tudent ! Sometimes even their
own secretary will have no idea where they have ran off to. Or they
have a secret hate of students constantly wanting their signature
and clogging up their inbox.
DO NOT FEAR!.. Continue on with your block as you would do and
make sure you have al l your necessary cases and documents ready to
present to the Enigma in the most concise and speedy manner. Be
ready with all necessary online forms ready to be signed before you
lose track of your supervisor for another week.
THE KEEN BEAN
The keen supervisor is the one who really wants the most out of
you, and would have you by their side at all times. Forget all
teaching, friends, lunch...your supervisor is now your life, your
heart and soul of your 5 week placement. They want you there at
every clinic, MDT, ward round, theatre list...all in the name of
teaching you. This could be the best clinical exposure of your e n
t i r e m e d i c a l c a r e e r b u t consequently the most
tiring!
Supervisors are still human beings, and understand you may need
a breather from time to time so do not fear to ask if you need to
get away. However stick by them as much as you can and you will
definitely reap the benefits of good knowledge and that end of
block assessment form signed off!
Starting clinical placements can be a daunting experience come
third year and beyond. It is a completely different to those PBL
and VS sessions; a sense of freedom and responsibility rains over
you as you step onto those busy wards. However, as much as you want
placement to be your own learning experience, the ultimate fate of
whether or not you have to cancel all summer/elective plans and
resit a placement is up to one person - your supervisor!
Supervisors come in a variety of flavours in the world of
clinical placement; each one has their own style and attitude to
supervising. It is up to you to use your own judgement on how to
get the most out of your supervisor, and how to play the supervisor
game.
Here are some supervisor personas you might encounter:
THE OLD SKOOL REBEL
2 portfolio cases, mini cexs and CBDs?! Not in my clinic! The
Rebel has their own ways of teaching you the ways of medicine and
will not stick by the jurisdiction of the medical school clinical
years guidebook! There are a variety of ways in which the rules can
be bent to their will. Some supervisors may not require any
portfolio cases, others may demand a case a week. Some will not
give a damn about your reflection and how the case has made you a
better person, while others will think you are a cold hearted
monster if you didnt mention the social aspects of a patients
life.
One golden rule here is do as youre told, or else your chances
of a sign off will be in jeopardy!
GAME
by Trung Ton
-
THE SPECIALIST
Now all consultants have a special interest. But this kind of
supervisor wants it be your special interest too and will have
nothing else you have to offer. Even if it is something youre not
particularly interested, there is no escaping the subject now.
Everything you do will revolve around this topic and you just have
to accept your fate.
Best thing to do is to stick by it and you might even learn
something that may come in handy in the future. (regardless of the
fact you have neglected all 200 other ILOs of the block)
THE LAID BACK ONE
The dream situation has arisen in your block; A supervisor who
knows exactly what a medical student needs in a clinical placement.
These supervisors will respond with haste to your emails, meet you
at any convenient time and give you total control of your learning
experience.
All you have to do is to keep your work up to good standard and
you will be getting that sign off in the easiest manner
possible.
At the end of the day, it is up to you to make the most out (or
very little) of your clinical placements and your supervisor is
just there to ensure you are keeping up to standard with your
practice. Some top tips for the supervisor game: Contact your
supervisor as soon as you start to arrange a meeting Get all your
assessments done sooner rather than later Try to show face and
attend your supervisors clinics etc (if they permit - this is a
good way of getting things signed off too) Enjoy clinical placement
and make it your own personal learning experience - (you will be
getting paid to do it before you know it!)
WANT MORE USEFUL INFORMATION LIKE THIS? Dont forget to check out
Surgos very own website at
www.surgoglasgow.com
-
How to get the most
out of clinical
placements
It is time to step up to the fold and do some proper medicine.
You all must be excited and probably a bit nervous about going on
clinical placements. You should however, remember that these years
will be some of the most exciting moments of your education.
Meeting real patients, solving real problems and doing real
medicine.
This guide is about what you can do to make the most of your
time on placements. We arent talking about having parties in the
onsite accommodation; we are talking about getting slick with
clinical skills and history taking skills. Placements are where you
learn to practice, practice, practice medicine.
In conjunction with Alna Robb we have developed this guide to
help you operate effectively and gain as much experience in
clinical skills as possible.
Before we get started
Placements will vary between hospitals, but they all will be
following the same objectives and themes. Pay attention to their
introduction they give you at your hospital, and dont forget to
read the Guide to Clinical Years. Doing both of these will put you
in good stead for understanding what is expected of you in clinical
years.
Getting the work done!
In order to be competent you need to perform each the procedures
expected of you five times, you can find a list of these in the
clinical skills logbook (If you still have it) or online via vale
or the e-portfolio. Have a list in your
notepad or Smartphone and a plan for the day of what you would
like to get done. Get all of these signed off and logged on your
e-portfolio/vale.
So what can I do?
You can do almost any clinical procedure so long as you have
been trained to do it and are supervised by a qualified medical
professional. So ask your supervisor what you want to do, ask if
you can watch them doing it and then get them to supervise you
doing it!
The Surgical block For those who like scalpels and sutures, this
will be an invaluable experience, for the rest of us, just try not
to faint at the sight of blood. This should be a very enlightening
experience as many of you will have never stepped into an operating
theatre before.
-
STOP, Hand washing time!
As a first initial priority, get your hand washing technique
assessed and get it mastered properly, youll be surprised how many
slip up on this basic skill. This is especially important on the
surgical block.
Injection technique
On the surgical block your subcutaneous injection technique
competency can be completed very easily as most patients receive
subcut heparin when on the wards. These injections usually occur at
about 0800 and 1800, nursing staff usually do these, but if you
have a chat with the lead nurse (in some hospitals still called the
ward sister) you should be able to get trained to do them and
perform some yourself. In about 2-3 drug rounds you should have
completed competency
In terms of intramuscular injections, you may get the
opportunity to do these before the patient goes into theatre but
you will need to check with the nursing staff beforehand.
Urinary Catheterisation
Most patients will be catheterised in theatre, so try and get as
much theatre time as possible. You will be shown meticulous aseptic
technique and the procedure will generally be easier, as the
patient wont be conscious when having a tube passed up their
urethra (as you can imagine this is very uncomfortable).
Follow the patient through
their operation
One of the best learning opportunities to do in the surgical
block is to follow a patient though surgery. You can gain a number
of key skills and see the hospital machine in action. Here is a
step by step guide as to what to do. Dont forget permission,
training and supervision must be adhered to at all steps:
1. If possible, look at the theatre list for the day and ask
permission from your consultant to follow a patient though their
journey. Pick a patient who is likely to be in theatre for a few
hours.
2. Get permission to follow the patient though the journey from
the patient the day before the surgery.
3. Get your own history from the patient and enquire
with your consultant what procedure he/she is having done.
4. Revise your anatomy/physiology regarding the
procedure the night before, as the surgeon may ask you
questions.
5. The next day be on the ward well before the patient is due
their operation. Give your phone number to the ward sister to call
you if timings change.
6. Observe the surgical checklist that is carried out
before the patient leaves for surgery and escort the patient to
theatre. Hopefully the theatre reception and staff will have been
informed you will be following the patient through theatre.
7. Observe the handover of the patient.
8. Go change into theatre scrubs and meet your patient before
they head into the anaesthetics room. If you
-
have been following the patient thus far, they may consent to
you performing a cannulation under the anaesthetists
supervision.
9. You then may have the option to stay with the anaesthetist
and scrub in to theatre
10. Observe, and perform a surgical scrub (handwashing
skill up!) under supervision of the theatre staff. You will also
be shown how to Gown up following aseptic technique.
11. You may be able to catheterise the patient under
supervision, once the patient is under. If you are really lucky you
might be able to do a few surgical clips or sutures!
12. After the operation, accompany the patient into the
recovery room and help with observations (see the observations
section). You will see how intensive these are investigated post
theatre.
13. You will also learn in the recovery room oxygen therapy
technique (masks, observing ABGs, pulse oximetry) and other skills
such as IV drug therapy and ECG procedure and interpretation.
14. Once the patient is ready to return to the ward,
accompany the patient back there and observe the handover to the
ward staff. You could also try having a go at this under
Supervision.
The Medical block This is where you can get the majority of your
skills polished that you already know, whilst gaining many new ones
( These can also be applied to the surgical block too).
Observations
Basic observations such as Pulse, BP, RR, ECG, GCS, urine output
and early warning scores are basic clinical skills, however you
should try to learn them in context of a patients condition. When
you have free time on the wards, offer to the ward sister/nurses to
do the observations for 20 minutes or so. You may call doing these
Basic but learning to recognise patterns in a patients condition
will be an invaluable skill in clinical practice, not to mention
you will become very slick at the basic procedures, and the
examiners like that!
Nasogastric tubing
The time to look out for NG tubing in particular is on the GI,
pancreatic and surgical wards. The nursing students usually have
dibs on the first few but if you inform the sister on the ward that
you would like to do one, usually you will get the chance to do
about one per week. Even if they say no, ask if you can watch, and
still improve your skills.
Venepuncture
Your consultant can usually give you some opportunities to do
this, but If the phlebotomist is on the ward taking blood, ask them
if you can perform a few. The phlebotomist has a time schedule to
keep and wont let you perform too many, but get a few under your
belt and youll be well on your way to clinical competency.
-
ECGs
Whilst on placement get yourself some time spent at the cardiac
clinic, patients here will have an ECG performed on admission, you
can learn how to perform, do one yourself and practice interpreting
them. You should be able to get all five ticked off before you even
leave the unit!
Histories
These will be the meat and gravy of your placement, do them
frequently and often. Patients will have had histories taken from
them on admission but you can perform some yourself, be aware to
ask the ward sisters before doing this. Tell the patient why you
want to take their history, otherwise they may get annoyed about
being repeatedly interrogated. Tell them you are still learning and
that you would like some objective feedback. You could use a
feedback form from the VS com skills sessions in order to make this
easier and have a record of this. Check your clinical skills
logbook for the list of histories to take.
These include but are not limited to: Respiratory, CVS,
Neurological, GI, Rhemo/Ortho, Endocrine, Renal/urinary.
Quickfire Questions
Can I go to A&E?
Yes, some days during your five week block, your consultant may
be on call for A&E or acute recieving. You might be starting
later in the day but be working later when called to A&E.
Whilst in A&E dont panic, play by the rules (do exactly what
the staff ask of you, you may be helping with procedures) and
remember your ABCs.
Will we be expected to be in 9-5?
It depends on your hospital, but you may be in 9-5 or even
later!
Are we expected to do weekends?
As a rule no, but if you wish to do so, make your consultant
aware and they should be able to help you. You could use this time
to catch up on your clinical skills youre lacking in.
Should I bring chocolates to the nurses to make them like
me?
Please dont, the best thing you can do is to be polite, friendly
and respectful (there is no Nurse/Doctor/Auxiliary/Med Student
hierarchy.)
Do I need to revise/study anything beforehand?
Your supervisor should be directing you in your learning, but
use your experiences to highlight areas for you to look into. If
you are following a patient through surgery, read up on the anatomy
and physiology related to the procedure beforehand. Watch the
clinical skills podcasts if you are unsure how to do any of the
core clinical skills.
-
]
So, there we go, a whistle-stop guide to clinical placements. We
hope this helps you in your endeavours. Have fun, enjoy yourselves
and be some great doctors!
A production by the 2017 Beta year club; Author: Tom Ainge
Image attributions:
https://medicalhumour.files.wordpress.com/2012/09/warning-medical-student-who-wants-to-take-your-history.jpg?w=914
http://news.bbcimg.co.uk/media/images/60028000/jpg/_60028231_m5200213-hospital_hygiene.jpg
http://www.telegraph.co.uk/news/worldnews/northamerica/usa/11197280/Operation-inventor-needs-money-for-his-own-operation.html
http://www.excellenceinjections.com/subcutaneous-injections/
http://www.theredlist.fr/media/database/films/tv-series/sitcom-and-soap/2000/scrubs/005-scrubs-theredlist.jpg
http://www.osceskills.com/e-learning/subjects/intravenous-cannulation/
General tips for placements
x Make yourself visible on the wards to the ward sisters. Ask
them if there are any procedures you can do/help with (it may help
to give them a short list of the things you want to do)
x Be polite to the staff, people love to teach so express you
love to learn x Be on time, five minute rule! x Have a checklist of
things you want to do each day/week and have a plan x If you cant
do a procedure watch it and gain experience x There is always
something to do on the wards, tell the nurses if you want to do
things x Above all have fun on placements
-
Losing Our NHS Here goes another rage article. I challenge you
to read this article and not be shocked, sickened and appalled. The
2010 election campaigns of all political parties may have differed,
but all major parties seemed to stand united in a pledge to protect
our NHS both in quality and budget. David Cameron promised No cuts
to frontline services, real-terms increases to the NHS budget, and
no more top-down reorganisations. Within weeks he began to break
these promises. In the shadows; hidden behind euphemism, carefully
worded contracts and cheery hospital visits; the Conservatives have
spent the last 4 years making the NHS ready for sale.
Following the general election, 2011 marked the first fall in a
decade and the biggest fall in NHS approval ratings in three
decades, the ratings fell from 70% to 58%. Government ministers
slating of the NHS in order to justify their reforms no doubt must
have a role to play in this. The current coalition has starved the
NHS and then taken to the headlines asking why it isnt performing
as well. It would indeed seem a very clever plan to create a
situation in which the NHS cannot perform to meet its targets,
criticise it for failing and then begin to talk of ways to fix it.
Ways like, I dont know, of fering deals to private companies? It
seems our health service has fallen victim to a smear c a m p a i g
n , s m e a r e d w i t h b a d headlines in a preparation to be
served to the bidder with the most connections. If you want to look
for who is gaining from this then look no further than Westminster
itself. 1 in 4 Conservative Peers have recent or present financial
connections to companies or individuals involved in healthcare;
Andrew Lansley himself has received at least two donations from
individuals in private healthcare; Nearly 40% of GPs on Clinical
Commissioning Groups have an interest in selling products they are
commissioning. This is just the
beginning of a list of shocking statistics linking MPs to
private healthcare companies and suggesting ulterior motive for
awarding private companies NHS contracts.
All of this begs the question, how are firms making profit from
NHS services that we are struggling to provide? Many of the
companies being considered and sometimes awarded these contracts
have previously come under fire for substandard care in care homes
and hospitals. If these companies do decide that the services they
have chosen do not work as a business decision, they able to pick
up and drop services as they please w i t h l i t t l e c o n s e q
u e n c e o r accountability, for example the return of
Hinchingbrooke Hospital to the NHS after the private company
running it failed to meet standards and came under scrutiny. There
is no such get out clause for the NHS to cut short the contract if
the private firms fail to provide an adequate service.
In a recent scandal, Alliance medical has recently won a 10 year
contract to provide diagnostic services despite their bid costing 7
million more than a bid from NHS trusts. When looking for an
explanation for this, I can probably give you less than three
guesses until you get it right. It cannot be confirmed but David
Cameron has not yet revealed if ex-
m in i s t e r S i r Ma l co lm R i fk ind influenced the deal
with Alliance Medical, the Tory MP who actually sits on the board
of the private healthcare provider has since resigned as an MP
after having been found accepting cash for access. 70% of contracts
put out to tender are now won by private firms. This arrangement is
even more worrying when coupled with the fact that the most recent
contracts set performance targets and standards after deals are
signed and the contract is won.
As shocking as the actions of the government is the cover up.
The conservatives have recently deleted every article, speech and
press release released before the last election from their website.
Is this as they have said an effort to make the site easier to read
or an effort to sweep under the rug the totality of the promises
they have broken to date? Since the coalition has been in power we
have lost: 5,870 NHS nurses, 7,968 hospital beds, a third of
ambulance stations to name a few. The massive top down
reorganisation that has occurred just weeks after the Tories
promised it would not has diverted approximately 3 billion away
from patient care.
My opinion? We wont have an NHS anymore if we have another term
of conservatives in parliament.
by Michaela Jewson
-
Do#you#have#a#very#particular#set#of#skills?
We#will#nd#you#and#you#will#write#for#us.#if$you$would$like$to.$$There$is$no$pressure$for$a$long$term$commitment.$We$
appreciate$all$enthusiastic$contributions$and$ideas!$Contact:#[email protected]
-
Free * e-learning modules* worldwide elective protection
Discountson medical textbooks
24 HourMedicolegaladvice line
FreeOSCE revision
resources
Free medicolegalpublications
Free
For more information about MPS, please visit
www.mps.org.uk/student or call 0845 900 0022
www.facebook.com/mpsmedicalstudent
MEDICAL PROTECTION SOCIETYPROFESSIONAL SUPPORT AND EXPERT
ADVICE
The Medical Protection Society Limited. A company limited by
guarantee. Registered in England No. 36142 at 33 Cavendish Square,
London, W1G 0PS. MPS is not an insurance company. All the benefi ts
of membership of MPS are discretionary as set out in the Memorandum
and Articles of Association. VAT number 524 251475. MPS1059
05/13
Choice medical students
The Right
for
MPS1059_FRESHERS ADVERT_HALFPAGE.indd 1 31/07/2013 10:34
w w w . c r c p r e s s . c o m
e s s e n t i a l
MeDiCalrevision
15% discount on all revision books. Just visit:
http://bit.ly/CrCrevision15 to automatically receive your
discount
and get FREE worldwide delivery. expires 31/12/2015
-
surgoglasgow.com
The Lectured Become the Lecturers But should we be forced to
endure them?
Sound familiar? Above is an article from a 1977 edition of
Surgo. How many of us have complained about a lecture? It seems
that the use of the slide projector (or PowerPoint) as a
psychological weapon is just as common now, in 2015, as it was when
most of our lecturers were, themselves, being lectured.
What is proposed in the article above, is the beginning of the
whole PBL idea - self directed learning. All of us spend the first
two years here doing PBL, then progress to CBL to learn how to
proceed with the care of our future
patients. However, most of you will agree, it is only with
lectures to complement this learning that we are able to become
good clinicians.
Having said this, lectures do not suit everyone, so Surgo asks
you this:
Do you think attendance should be taken in lectures and why?
Please email your opinions to the editor at
[email protected] and we will incorporate the best answers
into the next issue.
-
Happenings in MedChir
SCRUBBY! A solid effort all round from the 492
attendees of Scrubby 2015! The blue tide
filled up the beer bar, Viper and pubs
across the city. Despite it being Friday
the 13th no one was injured, although a
7 year old Govan resident did take a
swing at a first year (he probably had it
coming). A personal highlight was a
rammed Bellrock Bar singing along to
Whitney Houston.
MedChir Revue Oh what a night! Talent was abundant and came in
many forms including a particularly jovial Irish Dancing act. Jesse
Dawson, Prof Walters and Alna Robb were the judges; euphemisms and
sexual innuendos firing left, right and centre, though mostly in
the direction of Alna. Med-Chir provided a satirical clinical
skills session with 5th year Anna Yule as Alna, which thankfully
went down well. An all-round excellent night and bring on next
year!
Welcome Back Pub Quiz
Surgos first ever legit event went
pretty much as planned and the
winning team won the enviable prize
of out-of-date Subway vouchers. Who
says we dont treat you right? First
Year Rep Shereif knocking over a table
covered in pints was pretty funny,
such a waste of Tennents though. We
also put old issues of Surgo to good
use, as shown by the big Munn
himself
www.surgoglasgow.com
-
Three bells, three barfs, one burn.
Here is this years 3rd year ball
experience in a nutshell.
After months of p lanning and
anticipation, the halfway ball took
place from 11th to 13th of February in
MacDonald Cardrona Hotel, Peebles.
We were all sick of spending our
nights in the Study Landscape eating
food from the reduced section in M&S,
and listening to those students
claiming they know literally nothing
yet somehow always seem to get on
the honours list. With everyone
looking forward to it for so long could
it possibly live up to expectation? One
hundred and eighty medics drunk for
two daysof course it did!
With most of us having far too many
at the Beer Bar after Tuesday's MEQ
and with THREE students ringing the
bell (cheers to Michael, Cameron and
Iain), it was somewhat remarkable
that we all made it for the buses the
next day. We got off to a shaky start
Sam, Caitlin and Ross decided to
paint the buses with a cheeky bit of
vomit on the way to the hotel, however
we soon settled in to our fancy digs
and had a lovely time listening to
singer/songwriter Tony McHugh and
enjoying a hard earned pint.
A game of Ring of Fire was started
almost as soon as we arrived to the
hotel and within the hour people were
well on their way. Joe was drunk by
3pm and with each passing sentence
became more and more Welsh. The
Kings cup was overflowing with
champagne, vodka and fair amounts
of pubic hair.
T h e f i r s t n i g h t w a s t h e m e d
Superheroes and Supervillains. Some
people really made an effort with their
costumes Anna Leersen dressed as
Sauron, but most of the other girls
dressed as Poison Ivy. Other people
dressed up as someone who cant hold
their drink and real ly true to
character, passed out at the dinner
table. The night came to an end with a
DJ serenading us with classics such
as Angels by Robbie Williams, the
anthem of our year.
Sometime during these festivities Iain
MacLeod and Lewis Walker decided
they should race down the corridor to
see who was the fastest, but we all
know both men can only last 15
seconds anyway. Iain was first to
cross the finish line, but face-planted
the ground in triumph and gave
himself carpet burn down the left side
of his face as a reward. Maybe it is
good that he nearly lost his left eye as
Sam got locked out of his room in his
birthday suit and the night porter had
to be fetched to save him from this
compromising situation.
There was a bit of an altercation on
the upper floors when Dominic Waugh
was left with a bit of periorbital
swelling too we are not sure what
the relationship between ocular
injuries and the hotel is but well keep
an eye out for more information. The
second afternoon was a lot more
chilled out some people went to the
pool, others took 6 hours to play 18
holes of golf, and we had rented out
sumo suits for those who were a bit
more daring. Some keen beans, who
obviously didnt drink enough the
night before, even went to the gym!
Here there was more grunting than a
pig orgy as Dominic Waugh was lifting
in front of the mirror to improve his
pectoral muscles, which allegedly can
spurt whipped cream on demand.
During the evening we had a drinks
reception and a lovely three course
meal. This was followed by a ceilidh in
which Jordan Newport looked like
Ricky Martin on coke. At one point he
nearly dislocated Annas arms from
her sockets. There was a beautiful
rendition at the end of Auld Lang
Syne, Loch Lomond, and of course
Angels (again). Following that we
danced the night away to hits from
Britney Spears to Kanye West. It was
great to see David swaying around to
the beat and sweating profusely. At
around 4am most peoples legs had
given up on them and we retired for
the evening.
Friday morning was a day of great
regret and we all left feeling sad and
hungover, or in my case still drunk;
making those who made the bus look
like extras from The Walking Dead.
Unfortunately some poor souls didnt
make the bus on time (Catherine,
Maria and Abi) and we are told they
are still trying to hitchhike home.
So that was the Ball in a nutshell. It
seems like there wasnt a great deal of
scandal but unfortunately our lawyers
have advised against including those
stories. Beta -2017 Year Club would
like to thank everyone who came and
also those who supported our events
during the year. We had a ball!
By Year Club Beta 2017
WE
BALLSED IT UP
-
Introduction The transverse acetabular ligament (TAL) is a
poorly understood aspect of the hip with limited morphological
description in the reviewed literature. It is often used as a
landmark for orientation of the acetabular component in total hip
arthroplasty (THA) but its suitability is debated. The aim of the
current study was to investigate the morphology of the TAL. It was
hypothesised that the current description in the literature is
insufficient.
Materials and methods Seven dry bone hemi-pelves were
reconstructed using a microscribe and rhinoceros 4.0 3D software.
Hips (n=3; F=2) were dissected to expose the TAL. The TAL was
removed and a footprint taken of its perimeter and attachment sites
for measurements. 3D models of the
dissected acetabuli with an outline of the TAL and attachment
sites were created as for dry bones.
Results The TAL extended beyond the acetabular notch, around the
circumference of the acetabular rim. Two attachment sites were
identified in each specimen in the superior half of the acetabular
rim; one anterior and one posterior. In one specimen, an additional
attachment site was identified on the posterior horn. TAL length in
each specimen as measured from 2D digital photographs were 132mm,
117mm and 179mm, with attachment areas of 215mm2, 150mm2 and
350mm2, respectively. There was marked variation in ligament
breadth between and within individual specimens, ranging from 2.6
to 5.3mm and 3.2 to 6.3mm in the smallest and largest specimens
respectively. Discussion Contrary to previous literature, the TAL
was found to extend far beyond the acetabular notch, and its
attachment sites were found more superiorly on the acetabular rim
than previously described. The unexpected length may explain
disagreements surrounding its use as an anatomical landmark.
Further biomechanical research may determine which part if any of
the ligament the acetabular component should be orientated
against.
True Facts about the Hip
It takes about 3000N of force to fracture a hip. A car hitting
you at 30mph transfers about 21000N into you.
Gorham's Disease is a rare disease causing osteolysis, thus
rendering the patient boneless.
In the early 1970s, DJ Kool Herc coined the term Hip hop to
describe his epic funk block parties in the Bronx.
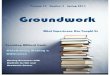
Clinical Anatomy of the Transverse Acetabular Ligament
Craig R JohnstoneSupervised by Dr Quentin Fogg
Transverse acetabular ligament
Acetabulum
Ligament of femoral head
-
Background
One in five Britons will have commenced a new diet at the
start of the year, in a vain attempt to shed pounds and help
sculpt a perfect beach bod. Many of these people attempt a
celebrity diet that they have read about in the high impact
nutritional journal Cosmo. SHITS is less concerned with
the effect of the diet or the amount of weight they lose but
far more interested in how the diets affect their poop. We
aim to assess the effect of commencing a celebrity diet on
poop quality and quantity. No study has investigated this
area before. Prior to commencing investigation into the
diets
effect on poop we aim to determine the most commonly
occurring celebrity diets online.
Methods
SHITS will comprise of two parts; Part 1: diet selection and
Part 2: diet's effect on poop.
Part 1 will include an initial Google search will be
completed
to find popular celebrity diets, which will be recorded.
A preliminary list of diets will be created for analysis.
Any
diet designed to be completed with an adjunctive exercise
program will be excluded from further analysis as will any
diet involving the consumption of dangerous or illegal
substances.
Following application of exclusion criteria a subsequent
Google search will be completed on the diets identified and
the five diets returning the largest number of Google search
results will be selected for study.
Results
Five diets were selected for study. The most popular diets
were: Gluten free diet [61,400,000 results], Sugar free
diet [51,200,000 results], Raw food diet [32,200,000
results], 5:2 diet [20,000,000 results] and Paleo
diet [13,700,000 results].
Conclusion
The wide variety of celebrity diets listed on the Internet
shows a trend for diets to be based on removing certain food
groups from ones diet.
Another trend can be seen in the rise of diets encouraging
eating foods that are uncooked, natural or unprocessed.
It is unclear on how the selected diets will affect the
participants' poop. SHITS: Part 2 will investigate this.
Paleo?5:2 Diet?
Gluten free?
Raw food?
DETO
X
Sugar FreeGo for a run?
Part 1 : Diet Selection
Daniel Taylor-Sweet1
1University of Glasgow, Glasgow, Scotland
March, 2015
Funding: No funding was received or applied for. Conflicting
Interests: None Ethical Approval: Applied for ethical approval from
MedChir Ethics Committee, pending approval.
SHITSSurgos Highly Interesting Toilet
Study
An analysis of the most commonly occurring celebrity diets on
Google.
-
CONTACT GUGPS: Facebook: Glasgow University General Practice
Society/ Email: [email protected] President: Mita
Dhullipala
Glasgow University General Practice Society: ETHICS CASE!
Hello! Welcome to Glasgow Medical Schools latest society. GUGPS
hopes to get
more of you interested and thinking about a career in general
practice. We have lots of exciting events planned for next year, so
watch this space for more information!
Ethics is a huge part of general practice, and those of you that
choose a career as a family physician will be faced with ethical
dilemmas on a regular basis. So GUGPS
have decided to team up with SURGO and get you all thinking
about ethics a bit more, by giving you an ethical case to solve in
every issue! Well point you in the
right direction with some questions- and in the next issue- well
tell you what the best solution would be (the solution that will
let you keep your job!)
The Case: Oliver Klozoff and the Foreign Liaison
Oliver Klozoff, a 27-year-old CEO consults with you, complaining
of dysuria following a trip abroad for business. Both he and his
wife Emma are patients of the practice.
Investigation reveals the presence of a Chlamydia infection. At
your next appointment you suggest that Oliver should tell Emma
about this problem, because if she is not diagnosed, treated and
followed up she could suffer long term harm. Oliver refuses, saying
that their marriage is already in difficulty and this would be the
'final
straw'. He also refuses to use condoms because he feels that
Emma would be suspicious. When you challenge him about the threat
to the health of Emma, he asks
you to take a swab from her on some pretext, and then treat any
infection that you discover.
Questions-
1) Would you go along with Mr. Klozoff's suggestion?
2) What other options do you have? 3) Would the situation be any
different if Emma was not your patient?
4) Would your decision be any different if the infection was
Candida instead of Chlamydia?
-
Exclusive access to The Electives Network (TEN) website. Free
guide to elective planning. Professional indemnity for your
clinical practice during your elective.*
Medico-legal advice and guidance. Elective reports and
videos.
Taken an elective photo that youre proud of?
Why not enter our competition.
For details on how to enter and the prizes available
go to themdu.com
We can help
Planning your elective?
* Contact our membership team before you go. Visit
themdu.com/yourelective for full benefits for students on
elective.
MDU Services Limited (MDUSL) is authorised and regulated by the
Financial Conduct Authority for insurance mediation and consumer
credit activities only. MDUSL is an agent for The Medical Defence
Union Limited (MDU). MDU is not an insurance company. The benefits
of MDU membership are all discretionary and are subject to the
Memorandum and Articles of Association. Visit themdu.com for the
latest information of the benefits included in membership.MDU
Services Limited, registered in England 3957086. Registered Office:
230 Blackfriars Road, London SE1 8PJ. 2014 STU211-d-1407
Follow us@the_mdu
Find usmdu student
Watch usmdu videoConnect with us
Apply for membership
0800 716 376
themdu.com
[email protected]