Embed Size (px)
Citation preview

WHAT’S NEW IN
“SPORT”
CONCUSSION
Mitchell Shulman MDCM FRCPC CSPQEmergency Department, MUHCAssistant Professor, Dept of Surgery
COPYRIGHT © 2017 BY
SEA COURSES INC.
All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means – graphic, electronic, or mechanical,
including photocopying, recording, or information storage and retrieval systems without prior written
permission of Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or participant’s statements, materials, acts or omissions.

CME FACULTY
DISCLOSURE
Dr. Shulman has no affiliation
with the manufacturer of any
commercial product or provider
of any commercial service
discussed in this CME activity.

HOT TOPIC!
• 250,000 - 300,000 / yr
• High risk of recurrence
• Long term dysfunction eg: Mohamed Ali, Paul Kariya, Troy Aikman
• Annual cost (US) > $1 billion
• >98% of sports related head injuries: concussions
• Misunderstanding still common

CLINICAL DILEMMA
• No proven acute treatment. Injury must run its course
• Final outcome may take years.
Severity unknown until it`s resolved
• UncertaintyAbout when it`s safe to return to competition.
• Multiple criteria / guidelines. Based on subjective clinical factors and durationof impairment
The Glasgow Coma Scale Isn’t Enough!

WHAT WE’LL COVER
1. Definitions
2. What Happens (Pathophysiology)
3. Evaluation
4. Management
5. What We Know and Don`t Know
6. Prevention
OLD DEFINITION
“A reversible injury to the brain
due to traumatic forces, resulting
in amnesia and/or loss of
consciousness.”

CURRENT DEFINITION
Concussion: brain injury
A complex pathophysiological process affecting the
brain, induced by biomechanical forces
(direct blow to head, face, neck; or, elsewhere on body with an
impulsive force transmitted to the head)
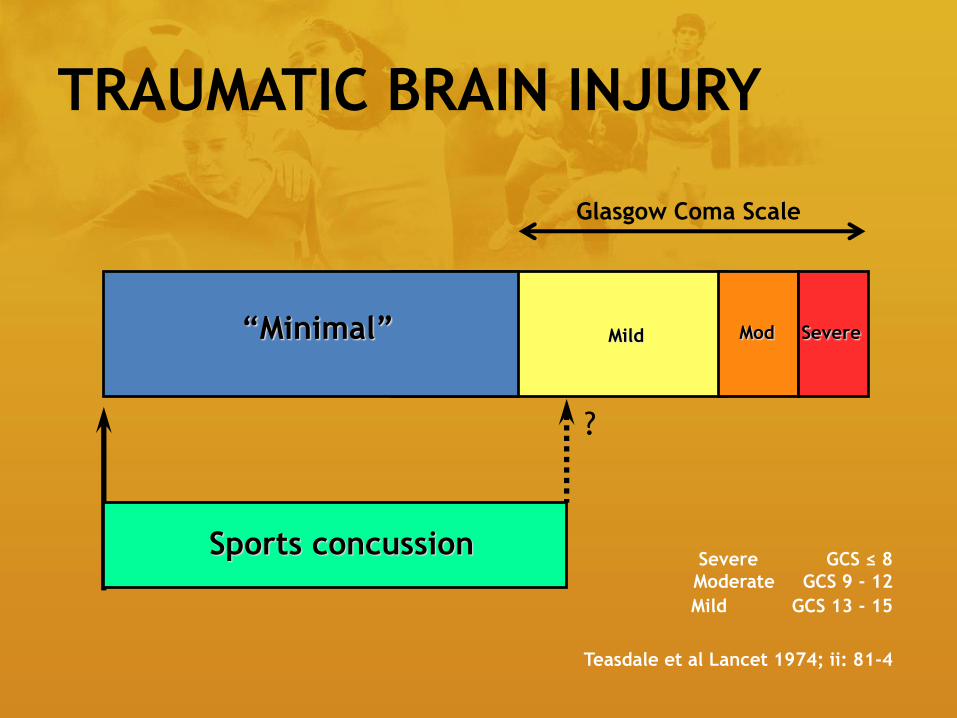
TRAUMATIC BRAIN INJURY
ModMild Severe
Severe GCS ≤ 8
Moderate GCS 9 - 12
Mild GCS 13 - 15
Teasdale et al Lancet 1974; ii: 81-4
Sports concussion
?
“Minimal”
Glasgow Coma Scale

GLASGOW COMA SCALE

P.E.A.R.L.S.
• Don’t need:period of unconsciousness
direct hit to head
amnesia
• Must have: concussion related symptomsnormal CT / MRI
Repeated sub-clinical head accelerations will likely
become part of the definition in the near future.

WHAT WE’LL COVER
1. Definitions
2. What Happens (Pathophysiology)
3. Evaluation
4. Management
5. What We Know and Don`t Know
6. Prevention

NOT JUST A BUMP
ON THE HEAD!
Mild TBI: tri-phasic process
*Hyperglycolysis (hours-days)
*Metabolic depression (days-weeks)
*Metabolic recovery (days-weeks-mos.)
WHAT WE’LL COVER
1. Definitions
2. What Happens (Pathophysiology)
3. Evaluation
4. Management
5. What We Know and Don`t Know
6. Prevention

EVALUATION OF
ACUTE CONCUSSION
• Evaluate player onsite: Standard Emergency
Principles apply Exclude c-spine injury
• Safely removed
• First aid, then assess concussion
(SCAT3 / other sideline assessment tools)
• DO NOT LEAVE PLAYER ALONE
Serial monitoring
• NOT ALLOWED TO RETURN TO PLAY
On day of injury
Player shows ANY features of a concussion
on field / sidelines

DIAGNOSISPhysical Signs of Mild TBI
• Any loss of consciousness
• Retrograde or anterograde amnesia
• Seizure at time of impact
• Vacant stare
• Inability to focus (easily distracted)
• Slurred speech, slow to answer questionsDelayed verbal / motor responses, slowed reaction times
• Disoriented, unsteady gait
• Memory deficits, personality changeEmotionally unstable, inappropriate behavior, irritability

DIAGNOSISSymptoms
• Headache (nearly always present)
• Dizziness, vertigo, drowsiness
• Lack of awareness“Just not feeling right”, Feeling like “in a fog”
• Nausea, vomiting
• Loss of balance
• Feeling dazed, “dinghy”
• Ringing in the ears (tinnitus)
• Blurred or double vision (diplopia)
• Insomnia

P.E.A.R.L.S.
• High index of suspicion -based on mechanism of injury
-velocity
-damage (in-car, helmet, to surrounding area, etc.)
• Athletes will under report symptoms (lie!)
to stay in the event
WHEN IN DOUBT, SIT THEM
OUT!

DETAILED CLINICAL ASSESSMENT
OUTLINED IN SCAT3 /CHILD SCAT3
Developed by SCAT3 Subcommittee (Meeuwisse, McCrory, Dvorak, Echemendia, Guskiewicz Iverson,
Johnston, McCrea, Putukian, Raftery, Schneider)

EVALUATION (EMERGENCY / OFFICE)
• Individual clinical decision
• Medical assessment:
History detailed
Neurological examination
(including mental status, cognitive
functioning, gait, balance)
• Improvement or deterioration since injury?
(info from parents, coaches, teammates, eyewitness)
• Emergent neuroimaging?
(exclude structural abnormality)
• Neuro-psych testing? ImPACT: Immediate Post-Concussion Assessment and
Cognitive Testing

CT / MRI ?• Especially when suspicion of intra-cerebral
or structural lesion:
• Focal neurologic deficit
• Evidence of significant impact
• Seizure activity > 1 minute
• Worsening symptoms
• Prolonged alteration in consciousness
• Persistent symptoms (fails to improve over 2 -3 weeks)
*Other modalities (eg. fMRI) correlate with symptom severity and
recovery. Although not routinely used, may provide additional
insight.
Alternative imaging technologies: still too early in their
development in concussion. Not recommended except research
setting
WHAT WE’LL COVER
1. Definitions
2. What Happens (Pathophysiology)
3. Evaluation
4. Management
5. What We Know and Don`t Know
6. Prevention
PROGNOSIS
• 80-90% resolve in 7-10 days
• May take longer in children / adolescents

>3 previous concussions:
9x amnesia (either anterograde / retrograde)
and post concussion symptoms
Retrograde amnesia: 10x poor outcome
Anterograde amnesia: 4.2x poor outcome
L.O.C. not predictive of outcome!!!

MANAGEMENT
• Rest until acute symptoms resolve
Physical Rest No training, playing, exercise, weights
Beware of exertion with activities of daily living
Cognitive Rest No television, extensive reading, video games
Caution re: daytime sleep
MANAGEMENT
• Expect gradual resolution w/in 7-10 days
• Gradual return to school
and social activities
that doesn’t result in
significant exacerbation of symptoms
• Then step-wise return to sport / play

RECOVERED?
• “Feels fine”
• Always ask:
1.“On a scale of 0 to 100%, how do you feel?”
2.“What makes you not100% ?”
3. Symptom Checklist – SCAT3
4. Are they confident to return to play?
5. Has their equipment been replaced /
upgraded?

RETURN TO PLAY
• Level 1: No activity, complete rest. once asymptomatic proceed to level 2
• Level 2: Light aerobic exercise (eg walking / stationary cycling)
• Level 3: Sport-specific training (eg. hockey: skating; soccer: running; racing: family car)
• Level 4: Return to sport (supervised private practice; attention to consistent, competitivetimes or abilities)
• Level 5: Return to competition (under observation during practice then competition)
Any re-occurrence of symptoms, athlete goes back to previous level!!!!
• school first, then sports
• 24 hours per step (~ 1 week for full protocol)
• If recurrence of symptoms at any stage: return to previous asymptomatic
level, resume after 24 hr period of rest

WHAT WE’LL COVER
1. Definitions
2. What Happens (Pathophysiology)
3. Evaluation
4. Management
5. What We Know and Don`t Know
6. Prevention

WE STILL DON’T KNOW
• How many mild TBI’s are too many?
• When is brain really back to normal?
• Is there effective pharmacotherapy?
• Why some athletes are “brain injury prone”?
Age /development
Kids / women are more vulnerable
Genetics (seems to run in families)
Role of other conditions (migraine, ADD)

WE KNOW
• Mild TBI can have long term effects
• Most (but not all) recover quickly
• Age may be important in recovery
• Neuropsychological testing: a useful tool
• Management should involve multiple
components
• Total inactivity is bad but, activity too soon is
also bad
• Psychological support and education make a
difference
WHAT WE’LL COVER
1. Definitions
2. What Happens (Pathophysiology)
3. Evaluation
4. Management
5. What We Know and Don`t Know
6. Prevention

PREVENTION
• Protective equipment
• Mouthguards:
benefit: preventing oral injury
no evidence: concussion reduction
• Head gear / helmets:
reduction in biomechanical forces
not translated to reduction in concussion
reduce head / facial injury

OTHER ISSUES
• Education / Awareness
• Rule changes• If mechanism clear
• Compensatory Behaviour• Use of protective equipment may change
behavior
• Violence / Aggression• Violent behavior that increases concussion risk
must be eliminated
• Promote fair play / respect

PREVENTION
• Reduce risk of falls
• Car seats / seat belts

P.E.A.R.L.S.
• Don’t need:period of unconsciousness
direct hit to head
amnesia
• Must have: concussion related symptoms
normal CT / MRI

P.E.A.R.L.S.
• High index of suspicion -based on mechanism of injury
-velocity
-damage (in-car, helmet, to surrounding area, etc.)
• Athletes will under report symptoms to
stay in the event
WHEN IN DOUBT, SIT THEM
OUT!