Embed Size (px)
Citation preview


Sponsors

Milan GuptaMD, FRCPC, FCCS, FACC, FAHA Associate Clinical Professor McMaster UniversityMedical Director, Canadian Collaborative Research NetworkBrampton, ON
Narendra Singh MD, FRCPC, FCCS, FACC, FAHADirector, Clinical Research, Atlanta Heart SpecialistsClinical Assistant Professor, Medical College of Georgia at Augusta UniversityClinician Scientist and Co-Director, Canadian Collaborative Research NetworkAtlanta, GA
Deepak BhattMD, MPH, FACC, FAHA, FSCAI, FESCExecutive Director, InterventionalCardiovascular Programs,Brigham andWomen’s Hospital Heart & Vascular CenterProfessor of Medicine Harvard Medical SchoolBoston, MA
Discussants

Housekeeping
You can take NOTES during the program by typing in the section under the slides.
Type your notes here…
Access your notes following the program in
My Account on the MD-Online website
Interact with the program through the tabs on the right of your screen.
You can ASK A QUESTION by selecting the tab on the right
By selecting OBTAIN MY CERTIFICATE you can complete the session evaluation and will receive a certificate confirming your attendance at this non-accredited session.
Your certificate will provide instruction on how you can claim
self-learning credits for your participation in this session

• These are remarkable times.
• We hope you and your loved ones are all safe and healthy.
• We thank all frontline health care workers for their dedication during this pandemic.
• For the first time in history, the live scientific sessions of the ACC were cancelled.
• Instead, ACC held a virtual meeting over 3 half days using a novel format.
• This program highlights the key clinical trials presented at ACC 2020, and explores the clinical implications for cardiovascular care.
Introduction


Heart failure
• VICTORIA• New data from PARAGON-HF
Lipids
• Homozygous FH• EPA levels in REDUCE-IT• New data from ODYSSEY Outcomes• Evolocumab for HIV patients
Peripheral arterial disease
• VOYAGER-PAD• COMPASS-DM
Structural heart disease
• Updates in TAVR
Key topics at ACC 2020

Heart failure
• VICTORIA• New data from PARAGON-HF
Lipids
• Homozygous FH• EPA levels in REDUCE-IT• New data from ODYSSEY Outcomes• Evolocumab for HIV patients
Peripheral arterial disease
• VOYAGER-PAD• COMPASS-DM
Structural heart disease
• Updates in TAVR
Key topics at ACC 2020

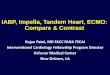
Cardiovascular deathHR 0.82 (0.69, 0.98); p=0.029
Worsening HF eventHR 0.70 (0.59, 0.83); p=0.00003
CV prognosis remains unacceptably poor in HFrEF
Dapagliflozin
Placebo
Dapagliflozin
Placebo
DAPA-HF study, 2019








ACC 2020: What You Need To Know







Discussion

Heart failure
• VICTORIA• New data from PARAGON-HF
Lipids
• Homozygous FH• EPA levels in REDUCE-IT• New data from ODYSSEY Outcomes• Evolocumab for HIV patients
Peripheral arterial disease
• VOYAGER-PAD• COMPASS-DM
Structural heart disease
• Updates in TAVR
Key topics at ACC 2020

Background
26
Hess…Hiatt et al. JACC 2020Jones…Fowkes et al. Circulation 2017Bonaca…Sabatine et al. JACC 2017 Bonaca…Morrow et al. Circulation 2016
N=393,017
Cum
ulat
ive
Inci
denc
e
Years from Index Revascularization
Risk in Patients Undergoing Peripheral Revascularization
Major Adverse Limb Events
4x risk of ALILong-term vs. no Revascularization
MACE
“Acute” Post Revascularization
“Stable”Phase
Outcomes in Patients with Acute Limb Ischemia
• Median hospitalization 8 days (IQR 5-15)
• ~4% die at presentation
• ~1/5 major amputation
• ~1/3 prolonged ICU stay
• ~3/4 major surgery
• Outcomes after hospitalization are poor with ~15% disabled or dead

VOYAGER PADVascular Outcomes Study of ASA Along with Rivaroxaban in Endovascular or Surgical Limb Revascularizations for Peripheral Artery Disease
Marc P. Bonaca, Rupert M. Bauersachs, Manesh R. Patel,Sonia S. Anand, Eike Sebastian Debus, Mark N. Nehler, FabrizioFanelli, Warren H. Capell, Nicole Jaeger, Lihong Diao, Connie N. Hess, JohnM. Kittelson, Lloyd P. Haskell, Scott D. Berkowitz, William R. Hiatt,for the VOYAGER PAD Steering Committee & Investigators
American College of Cardiology Virtual Scientific Sessions 2020 Late-Breaking Clinical TrialMarch 28, 2020

Trial Design
6,564 Patients with Symptomatic Lower Extremity PAD* Undergoing Peripheral Revascularization
Primary Efficacy Endpoint: Acute limb ischemia, major amputation of vascular etiology, myocardial infarction,
ischemic stroke or cardiovascular death
Principal Safety Outcome: TIMI Major Bleeding
Follow up Q6 Months, Event Driven, Median f/u 28 Months
Randomized 1:1 Double Blind
ASA 100 daily for all PatientsClopidogrel at Investigator’s Discretion
NCT02504216
Stratified by Revascularization Approach (Surgical or Endovascular)
and Use of Clopidogrel
*Ankle Brachial Index < 0.90 and
Imaging Evidence of Occlusive
Disease
Capell WH, Bonaca MP, Nehler MR…Hiatt WR. AHJ 2018
Rivaroxaban 2.5 mg twice daily Placebo

Primary Endpoint: Acute limb ischemia, major amputation for vascular cause, myocardial infarction, ischemic stroke, CV death

Primary Endpoint & Components
KM% 3 YearsRivaroxaban
N=3286
KM% 3 YearsPlaceboN=3278
HR(95% CI)
Primary Efficacy Outcome
17.3 19.9 0.85(0.76 – 0.96)
Acute Limb Ischemia
5.24 7.74 0.67(0.55 – 0.82)
Major Vascular Amputation
3.42 3.87 0.89(0.68 – 1.16)
Ischemic Stroke 2.70 3.01 0.87(0.63 – 1.19)
Myocardial Infarction
4.55 5.22 0.88(0.70 – 1.12)
CV Death 7.05 6.43 1.14(0.93 – 1.40)

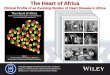
First Events Prevented / Caused for 10,000 Patients Treated* for 1 Year
-300 -200 -100 0 100 200 300
Favors Rivaroxaban 2.5 mg twice daily plus aspirin
Favors aspirin monotherapy
-181
-110
-20
-42
-19
-10
29
-6
0
Primary Efficacy Outcome
Acute Limb Ischemia
Major Amputation of Vascular Etiology
Myocardial Infarction
Ischemic Stroke
Cardiovascular Death
Principal Safety Outcome
Intracranial Hemorrhage
Fatal Bleeding
(-269 – -94)
(-165 – -56)
(-53 – 12)
(-84 – -1)
(-50 – 13)
(-48 – 28)
(-2 – 60)
(-22 – 11)
(-10 – 11)
*Efficacy and safety on-treatment

Summary & Conclusion
• In symptomatic PAD after revascularization, ~1 in 5 have acute limb ischemia, major amputation of vascular etiology, MI, ischemic stroke or cardiovascular death at 3 years
• In this population and setting, rivaroxaban 2.5 mg twice daily with aspirin compared to aspirin alone:
Significantly reduces this risk with…• Benefits apparent early and continued over time• Consistent benefit across major subgroups• Broad benefits including reductions in unplanned index limb revascularization
Increases bleeding: in VOYAGER PAD, there was a numerical increase in TIMI major bleeding and significantly increased ISTH major bleeding but no excess in intracranial or fatal bleeding
Prevents ~6 times as many ischemic events relative to bleeds caused in PAD patients after revascularization

VOYAGER PADEfficacy and Safety of Rivaroxaban in Patients with Symptomatic PAD undergoing Revascularization with and without Clopidogrel
William R. Hiatt, Marc P. Bonaca*, Manesh R. Patel, Mark R. Nehler, Eike Sebastian Debus, Sonia S. Anand, Warren H Capell, Lihong Diao, Nicole Jaeger, Connie N. Hess, Akos Ferenc Pap, Scott D. Berkowitz, Eva Muehlhofer, Lloyd Haskell, David Brasil, Juraf Madaric, Henrick Sillesen, David Szalay, Rupert Bauersachs on behalf of the VOYAGER PAD Investigators
American College of Cardiology Virtual Scientific Sessions 2020 Late-Breaking Clinical Trial29 March 2020

Primary EndpointAcute limb ischemia, major amputation for vascular cause, myocardial infarction, ischemic stroke, CV death

ISTH Major Bleeding With and Without Clopidogrel

Summary
• In patients with symptomatic PAD undergoing revascularization:
• The benefit of rivaroxaban plus aspirin versus aspirin alone is consistent regardless of background clopidogrel
• Primary efficacy endpoint HR ~0.85 with rivaroxaban regardless of clopidogrel with NNT < 50 with or without clopidogrel
• The safety of rivaroxaban plus aspirin versus aspirin alone is consistent regardless of background clopidogrel
• Principal safety outcome TIMI major bleeding HR ~1.3-1.5 regardless of clopidogrel with NNH > 90 with or without clopidogrel
• However, clopidogrel exposure was associated with higher rates of bleeding overall, particularly with longer durations (e.g. > 30 days)







Discussion

Heart failure
• VICTORIA• New data from PARAGON-HF
Lipids
• Homozygous FH• EPA levels in REDUCE-IT• New data from ODYSSEY Outcomes• Evolocumab for HIV patients
Peripheral arterial disease
• VOYAGER-PAD• COMPASS-DM
Structural heart disease
• Updates in TAVR
Key topics at ACC 2020

Alirocumab Efficacy And Safety In Adults With
Homozygous Familial Hypercholesterolemia
(ODYSSEY HoFH)
Dirk J. BlomUniversity of Cape Town, Cape Town, South Africa
Mariko Harada-Shiba, Paolo Rubba, Daniel Gaudet, John J.P. Kastelein, Min-Ji Charng, Robert Pordy,
Stephen Donahue, Shazia Ali, Yuping Dong, Nagwa Khilla, Marie Baccara-Dinet, Robert S. Rosenson

Background
• HoFH is characterized by extremely high LDL-C levels and early onset atherosclerotic cardiovascular disease despite treatment with conventional lipid lowering therapy1-3
• HoFH includes true homozygotes, compound heterozygotes and double heterozygotes1
• HoFH results from severely impaired LDLR function, most commonly due to mutations in both copies of the LDLR gene1
• Mutation in other genes of the LDLR pathway (APOB, PCSK9, and LDLRAP1) may also affect LDLR function1
APOB, gene encoding apolipoprotein B100; HoFH, homozygous familial hypercholesterolemia; LDL-C, low-density lipoprotein cholesterol; LDLR, low-density lipoprotein receptor; LDLR, gene encoding low-density lipoprotein receptor; LDLRAP, gene encoding low-density lipoprotein receptor adaptor protein 1; PCSK9, gene encoding proprotein convertase subtilisin/kexin type 9.1. Cuchel M et al. Eur Heart J. 2014;35:2146-2157. 2. Hovingh GK, Goldberg AC, Moriarty PM. J Clin Lipidol. 2017;11:602-616. 3. Raal FJ, Hovingh GK, Catapano AL. Atherosclerosis. 2018;277:483-492.

Baseline Characteristics
Alirocumab(n=45)
Placebo(n=24)
Age, years, mean (SD) 42.3 (14.1) 45.4 (15.8)
Male, n (%) 21 (46.7) 13 (54.2)
Race, n (%)
White 36 (80.0) 18 (75.0)
Black or African American 2 (4.4) 0
Asian 7 (15.6) 5 (20.8)
Body mass index, kg/m2, mean (SD) 25.1 (5.4) 25.1 (5.1)
History of CHD, n (%) 21 (46.7) 9 (37.5)CHD, coronary heart disease; SD, standard deviation.

Lipid-Lowering Therapy at Screeninga
n (%)Alirocumab
(n=45)Placebo(n=24)
Any statin 44 (97.8) 23 (95.8)
High-intensity statinb 38 (84.4) 21 (87.5)
Ezetimibe 31 (68.9) 19 (79.2)
Statin + ezetimibe 30 (66.7) 19 (79.2)
Lomitapide 7 (15.6) 3 (12.5)
Apheresis + other LLT 6 (13.3) 4 (16.7)
aA patient can be counted in several categories. bHigh-intensity statin corresponds to atorvastatin 40–80 mg daily or rosuvastatin 20–40 mg daily.

Baseline Lipids
Alirocumab(n=45)
Placebo(n=24)
LDL-C, mmol/L, mean (SD) 7.6 (4.0) 6.7 (4.6)
Non-HDL-C, mmol/L, mean (SD) 8.3 (4.1) 7.3 (4.6)
Apolipoprotein B, g/L, mean (SD) 1.9 (0.8) 1.7 (0.9)
HDL-C, mmol/L/L, mean (SD) 1.1 (0.4) 1.1 (0.3)
Triglycerides, mmol/L, median (Q1:Q3) 1.24 (0.9:1.8) 0.90 (0.7:1.4)
Lp(a), mg/dL, median (Q1:Q3) 36.0 (10.0:68.0) 32.5 (12.0:52.5)
Lp(a), lipoprotein (a); non-HDL-C, non-high-density lipoprotein cholesterol.

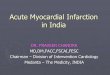
Primary Endpoint: LDL-C % Change vs. Placebo at Week 12a
-40
-30
-20
-10
0
10
20
0 4 8 12
LS m
ean
(SE)
per
cent
cha
nge
from
ba
selin
e in
LDL
-C (%
)
Time (weeks)aMixed effect model with repeated measures approach (intention-to-treat analysis).LS, least squares; SE, standard error.
LS mean difference (SE) versus placebo:–35.6 (7.8)%, P<0.0001
–26.9 (4.6)%−62.8 (14.0) mg/dL
8.6 (6.3)%8.9 (19.0) mg/dL
∆ Alirocumab 150 mg Q2W (n=45) ○ Placebo (n=24)
0.23 (0.49) mmol/L
- 1.62 (0.36) mmol/L

% Change in LDL-C at Week 12 by Genotype
-100
-80
-60
-40
-20
0
20
40
60
80
Chan
ge fr
om b
asel
ine
in L
DL-C
at
Wee
k 12
(%) *
**
**
Alirocumab 150 mg Q2WPlaceboNull/null (LDLR activity <2%)Single null LDLR variant
*†
† ††
†
No mutation identified
Double heterozygous(LDLR + APOB or PCSK9)
Homozygous (LDLR) Compound heterozygous (LDLR)
Heterozygous (LDLR + other benign
variants)Homozygous (LDLRAP1)
Homozygous (PCSK9)

Conclusions
• This is the largest randomized controlled interventional trial in HoFH patients to date
• Treatment with alirocumab resulted in a statistically significant and clinically meaningful reduction in LDL-C at Week 12 versus placebo
• Consistent reductions in LDL-C were observed from baseline to Week 12 for all subgroups, including patients on apheresis
• Alirocumab also significantly reduced ApoB, non-HDL-C, TC and Lp(a)
• LDL-C response more variable in patients with HoFH than in other forms of hypercholesterolemia
• Alirocumab was generally well tolerated with no distinct safety differences versus placebo

EPA Levels and Cardiovascular Outcomes in the Reduction of Cardiovascular Events
with Icosapent Ethyl–Intervention TrialDeepak L. Bhatt, MD, MPH, Michael Miller, MD, Ph. Gabriel Steg, MD,Eliot A. Brinton, MD, Terry A. Jacobson, MD, Steven B. Ketchum, PhD,
Rebecca A. Juliano, PhD, Lixia Jiao, PhD, Ralph T. Doyle, Jr., BA, Christina Copland, PhD,Richard L. Dunbar, MD, Craig Granowitz, MD, PhD, Fabrice MAC Martens, MD, PhD, Matthew Budoff, MD, John R. Nelson, MD, R. Preston Mason, PhD, Peter Libby, MD,
Paul Ridker, MD, Jean-Claude Tardif, MD, Christie M. Ballantyne, MD,
on Behalf of the REDUCE-IT Investigators

Bhatt DL, Steg PG, Miller M, et al. N Engl J Med. 2019; 380:11-22. Bhatt DL.AHA 2018, Chicago.
Primary Composite Endpoint:CV Death, MI, Stroke, Coronary Revasc, Unstable Angina
Key Secondary Composite Endpoint:CV Death, MI, Stroke
Primary and Key SecondaryComposite Endpoints
Icosapent Ethyl
Patie
nts
with
an
Even
t(%
)
0 1 2 3 4Years since Randomization
50
10 16.2%
Icosapent EthylPatie
nts
with
an
Even
t(%
)
0 1 2 3 4Years since Randomization
50
10
30Hazard Ratio, 0.75(95% CI, 0.68–0.83)
28.3% 30Hazard Ratio, 0.74(95% CI, 0.65–0.83)
20
RRR = 24.8%ARR = 4.8%NNT = 21 (95% CI, 15–33)
P=0.0000000123.0%
20
RRR = 26.5%ARR = 3.6%NNT = 28 (95% CI, 20–47)
P=0.0000006
20.0%

Eico
sape
ntae
noic
Aci
d (E
PA)
Icosapent Ethyl (N=4089) Placebo (N=4090) Between Group Difference
Visit
Median Observed
Values (µg/mL)
Median Absolute Change
from Baseline
Median % Change
from Baseline
Median% Change P-value
Median Observed
Values (µg/mL)
Median Absolute Change
from Baseline
Median % Change
from Baseline
Median% Change P-value
Median Absolute Change
from Baseline
Median % Change
from Baseline
Median % Change P-value
Baseline 26.1 26.1
Year 1 144 112.6 393.5 <0.0001 23.3 -2.9 -12.8 <0.0001 114.9 385.8 <0.0001
Year 2 169 137.3 478.6 <0.0001 28 0.5 2.8 <0.0001 137.1 457.4 <0.0001
Year 3 168 137.4 464.5 <0.0001 27.3 -0.1 -0.4 <0.0001 136.9 447.5 <0.0001
Year 4 162 132.6 452.1 <0.0001 26.2 -1.1 -5.2 0.15 133 439.8 <0.0001
Year 5 158 130.5 463.6 <0.0001 25.3 -0.5 -2 0.09 130.8 448.1 <0.0001
Last Visit 150 117.9 395.2 <0.0001 26.5 -0.9 -3.8 0.08 119 380.3 <0.0001
On-Treatment EPA Daily Average (derived)
135.2 103.9 363.9 <0.0001 27.7 0 0.2 <0.0001 103.8 347.7 <0.0001
Bhatt DL. ACC/WCC 2020, Chicago(virtual).
Levels of Eicosapentaenoic Acid (EPA) in Serum
Year 6 values are not included as the number of patients = 9.

Impact on the HR of Between-group Biomarker Differences (Icosapent Ethyl vs Placebo)
Primary Composite Endpoint Key Secondary Composite Endpoint
HR (95% CI) Significance P-value
HR (95% CI) Significance P-value
Overall Trial 0.75 (0.68–0.83) 0.00000001 0.74 (0.65–0.83) 0.0000006
Lipid/Biomarker Covariate
HR (95% CI)for Treatment Comparison
(Adjusting Covariate)Significance
P-value
HR (95% CI)for Treatment Comparison
(Adjusting Covariate)Significance
P-value
EPA (µg/mL) 1.03 (0.91–1.16) <0.0001 0.98 (0.84–1.14) <0.0001
Triglycerides (mg/dL) 0.77 (0.70–0.85) <0.0001 0.75 (0.66–0.85) <0.0001
LDL-C derived (mg/dL) 0.75 (0.68–0.83) 0.80 0.74 (0.65–0.84) 0.38
HDL Cholesterol-CDC (mg/dL) 0.73 (0.66–0.81) <0.0001 0.71 (0.63–0.80) <0.0001
Non-HDL Cholesterol (mg/dL) 0.78 (0.71–0.87) <0.0001 0.77 (0.68–0.87) <0.0001
Apolipoprotein B (mg/dL) 0.76 (0.69–0.84) 0.03 0.75 (0.66–0.85) 0.0004
hsCRP (mg/L) 0.76 (0.69–0.84) 0.004 0.74 (0.66–0.84) <0.0001
RLP-C (mg/dL) 0.78 (0.71–0.87) <0.0001 0.77 (0.68–0.87) <0.0001
Bhatt DL. ACC/WCC 2020, Chicago(virtual).
Stratified Analysis of Time to Primary Endpoint by Adjusting Time-Varying Covariates of Post-BaselineBiomarkers

Impact on the HR of Between-group Biomarker Differences (Icosapent Ethyl vs Placebo)
Primary Composite Endpoint Key Secondary Composite Endpoint
HR (95% CI) Significance P-value
HR (95% CI) Significance P-value
Overall Trial 0.75 (0.68–0.83) 0.00000001 0.74 (0.65–0.83) 0.0000006
Lipid/Biomarker Covariate
HR (95% CI)for Treatment Comparison
(Adjusting Covariate)Significance
P-value
HR (95% CI)for Treatment Comparison
(Adjusting Covariate)Significance
P-value
EPA (µg/mL) 1.03 (0.91–1.16) <0.0001 0.98 (0.84–1.14) <0.0001
Triglycerides (mg/dL) 0.77 (0.70–0.85) <0.0001 0.75 (0.66–0.85) <0.0001
LDL-C derived (mg/dL) 0.75 (0.68–0.83) 0.80 0.74 (0.65–0.84) 0.38
HDL Cholesterol-CDC (mg/dL) 0.73 (0.66–0.81) <0.0001 0.71 (0.63–0.80) <0.0001
Non-HDL Cholesterol (mg/dL) 0.78 (0.71–0.87) <0.0001 0.77 (0.68–0.87) <0.0001
Apolipoprotein B (mg/dL) 0.76 (0.69–0.84) 0.03 0.75 (0.66–0.85) 0.0004
hsCRP (mg/L) 0.76 (0.69–0.84) 0.004 0.74 (0.66–0.84) <0.0001
RLP-C (mg/dL) 0.78 (0.71–0.87) <0.0001 0.77 (0.68–0.87) <0.0001
Bhatt DL. ACC/WCC 2020, Chicago(virtual).
Stratified Analysis of Time to Primary Endpoint by Adjusting Time-Varying Covariates of Post-BaselineBiomarkers

Primary and Key Secondary Composite Endpoints, Cardiovascular Death, and Total Mortality by On-Treatment Serum EPA
100 200 300
AUC-Derived Daily Average EPA (µg/mL)
40026
2442 771 89 115212
2.0
Haz
ard
Ratio
: Ref
eren
ce to
EPA
= 2
6µg
/mL
0.2
0.
4
0.6
0.
8
1.0
1.
2
1.4
1.
61.
8
100 200 300
AUC-Derived Daily Average EPA (µg/mL)
40026
2471 789 94 125226
2.0
Haz
ard
Ratio
: Ref
eren
ce to
EPA
= 2
6µg
/mL
0.2
0.
4
0.6
0.
8
1.0
1.
2
1.4
1.
61.
8
2471 789 94 125225
2.0
Haz
ard
Ratio
: Ref
eren
ce to
EPA
= 2
6µg
/mL
0.2
0.
4
0.6
0.
8
1.0
1.
2
1.4
1.
61.
8
100 200 300
AUC-Derived Daily Average EPA (µg/mL)
40026100 200 300
AUC-Derived Daily Average EPA (µg/mL)
40026
2400 756 87 10No. ofPatients 5196
2.0
Haz
ard
Ratio
: Ref
eren
ce to
EPA
= 2
6µg
/mL
0.2
0.
4
0.6
0.
8
1.0
1.
2
1.4
1.
61.
8
Primary Endpoint1-5 Key Secondary Endpoint1-5 Cardiovascular Death1,2,4-6 TotalMortality1,2,4-6
P*<0.001 for all Dose-response hazard ratio 95% Confidence Interval (CI)
Note: Area under the curve (AUC)-derived daily average serum EPA (µg/mL) is the daily average of all available post baseline EPA measurements prior to the event. Dose-response hazard ratio (solid line) and95% CI (dotted lines) are estimated from the Cox proportional hazard model with a spline term for EPA and adjustment for randomization factors and statin compliance1, age2, sex3, baseline diabetes4, hsCRP5,treatment compliance6.*P value is <0.001 for both non-linear trend and for regressionslope.Bhatt DL. ACC/WCC 2020, Chicago (virtual).

Dose-Response of Hazard Ratio (95% CI) Primary Composite Endpoint by On-Treatment Serum EPA
Established Cardiovascular Disease or Diabetes with Risk Factors
40026
Haz
ard
Ratio
: Ref
eren
ce to
EPA
= 2
6µg
/mL
100 200 300
AUC-Derived Daily Average EPA (µg/mL)
1733 549 67 9No. of Patients 3765
1.0
2.0
0.2
0.4
0.6
0.8
1.2
1.4
1.6
1.8
40026 100 200 300
AUC-Derived Daily Average EPA (µg/mL)
667 207 20 11431
2.0
Haz
ard
Ratio
: Ref
eren
ce to
EPA
= 2
6µg
/mL
0.2
0.
4
0.6
0.
8
1.0
1.
2
1.4
1.
61.
8
1-5Primary Endpoint: Established Cardiovascular Disease
1-5Primary Endpoint: Diabetes with Risk Factors
P*<0.001 for all Dose-response hazard ratio 95% Confidence Interval (CI)
Note: Area under the curve (AUC)-derived daily average serum EPA (µg/mL) is the daily average of all available post baseline EPA measurements prior to the event. Dose-response hazard ratio (solid line) and95% CI (dotted lines) are estimated from the Cox proportional hazard model with a spline term for EPA and adjustment for randomization factors and statin compliance1, age2, sex3, baseline diabetes4, hsCRP5.*P value is <0.001 for both non-linear trend and for regressionslope.
Bhatt DL. ACC/WCC 2020, Chicago(virtual).

Compared with placebo, icosapent ethyl 4g/day significantly reduced first and total cardiovascular events by 25% and 30%, respectively.• These benefits were beyond what can be explained by the degree of
triglyceride or other biomarker changes
On-treatment EPA levels via icosapent ethyl correlate strongly with the primary endpoint, the key secondary endpoint, CV death, MI, stroke, coronary revascularization, unstable angina, sudden cardiac death, cardiac arrest, new heart failure, and all-cause mortality.
These data provide a mechanistic underpinning for the large risk reductions seen in multiple endpoints with icosapent ethyl in REDUCE-IT.
Bhatt DL. ACC/WCC 2020, Chicago(virtual).
Conclusions

61
OO Guidelines
Landmesser U, McGinniss J, Steg G, Bhatt DL, Bittner VA, Diaz R, Dilic M, Goodman SG, Harrington RA, Wouter Jukema J, Laucevicius A, Pecin I, Pordy
R, Poulsen SH, Roe MT, Szarek M, White HD, Zeiher AM, Schwartz GG, for the ODYSSEY OUTCOMES Investigators
ACC 2020 – Chicago, USAMarch 28–30, 2020
Achievement of New European Dyslipidemia-Guideline Low-Density Lipoprotein Cholesterol Treatment Goals
After Acute Coronary SyndromeInsights From ODYSSEY OUTCOMES

62
ACC 2020
62
OO Guidelines
• The 2019 ESC/EAS dyslipidemia guidelines have recalibrated targets of lipid-lowering therapy, particularly for secondary prevention.1
• In patients considered very high risk (including those with ACS) a LDL-C goal of <1.4 mmol/L (<55 mg/dL) is now recommended, with a goal of <1.0 mmol/L (40 mg/dL) for patients with recurrent cardiovascular events within 2 years.
• Using data from the ODYSSEY OUTCOMES trial,2 we examined how many patients achieved these new goals with the PCSK9 inhibitor alirocumab, and projected how many would have achieved the goals with the use of ezetimibe.
Background and Aim
ACS, acute coronary syndromes; EAS, European Atherosclerosis Society; ESC, European Society of Cardiology; LDL-C, low-density lipoprotein cholesterol, PCSK9, proprotein convertase subtilisin−kexin type 91. Mach F, et al. Eur Heart J. 2020;41:111-188; 2. Schwartz G, et al. NEJM. 2019;379:2097−107

63
ACC 2020
63
OO Guidelines
Results
• At baseline, 89% of patients received intensive statin treatment; 3% received ezetimibe.
• Median baseline LDL-C was 2.3 mmol/L [88.9 mg/dL] (interquartile range 1.9–2.7 [73.5 – 104.4 mg/dL])
54 77 101 124 147 170 193 217 240 263 286 309 333 356 379 402 425 449 472 495 518[mg/dL]

64
ACC 2020
64
OO Guidelines
Percent of patients who achieved LDL-C <1.4 mmol/L on at least 1 post-baseline measurement according to baseline LDL-C level
• Of the patients treated with alirocumab, 94.6% achieved LDL-C <1.4 mmol/L (<54 mg/dL) on at least one post-baseline measurement, compared with 17.3% in the placebo arm.

65
ACC 2020
65
OO Guidelines
Patients with prior ASCVD event who achieved LDL-C <1.0 mmol/L at any time post-baseline according to baseline LDL-C level
• Of patients with at least one prior ischemic cardiovascular event (in addition to the index ACS), 84% assigned to alirocumab achieved LDL-C <1.0 mmol/L (<39 mg/dL) at any time after baseline, compared with 3.7% with placebo








Discussion

Heart failure
• VICTORIA• New data from PARAGON-HF
Lipids
• Homozygous FH• EPA levels in REDUCE-IT• New data from ODYSSEY Outcomes• Evolocumab for HIV patients
Peripheral arterial disease
• VOYAGER-PAD• COMPASS-DM
Structural heart disease
• Updates in TAVR
Key topics at ACC 2020


Background
• Previous PARTNER trials have shown that TAVR was superior to standard therapy in extreme-risk patients and non-inferior to surgery in high- and intermediate-risk patients with aortic stenosis.
• Results from the PARTNER 3 Trial in low-risk patients demonstrated superiority for TAVR vs. surgery for the primary endpoint of death, stroke, or rehospitalization at 1 year.

Low Risk/TF ASSESSMENT by Heart Team(STS < 4%)
1:1 Randomization1000 Patients
TAVR(SAPIEN 3 THV)
Surgery(Surgical Bioprosthetic Valve)
Symptomatic Severe Aortic Stenosis
Follow-up: 30 days, 6 mos, and annually through 10 years
PRIMARY ENDPOINT: Composite of all-cause mortality, stroke, or CV re-hospitalization
at 1 year post-procedure
PARTNER 3 Study Design

Baseline Patient Characteristics
Demographics & Vascular Disease
TAVR(N=496)
Surgery(N=454)
Other Co-Morbidities
TAVR(N=496)
Surgery(N=454)
Age (years) 73.3 ± 5.8 73.6 ± 6.1 Diabetes 31.3% 30.2%
Male 67.5% 71.1% COPD (any) 5.1% 6.2%
BMI – kg/m2 30.7 ± 5.5 30.3 ± 5.1 Pulmonary Hypertension 4.6% 5.3%
STS Score 1.9 ± 0.7 1.9 ± 0.6 Creatinine > 2mg/dL 0.2% 0.2%
NYHA Class III or IV* 31.3% 23.8% Frailty (overall; > 2/4+) 0 0
Coronary Disease 27.7% 28.0% Atrial Fibrillation (h/o) 15.7% 18.8%
Prior CABG 3.0% 1.8% Permanent Pacemaker 2.4% 2.9%
Prior CVA 3.4% 5.1% Left Bundle Branch Block 3.0% 3.3%
Peripheral Vascular Disease 6.9% 7.3% Right Bundle Branch Block
10.3% 13.7%
% or mean ± SD*P = 0.01

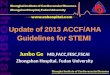
Primary Endpoint
0 6 12 18 24
496 462 452 436454 378 370 352
Number at risk:
TAVRSurgery
Months after Procedure
422339
TAVRSurgery
Dea
th, S
troke
, or R
ehos
p(%
)
11.5%
17.4%
0
10
20
HR [95% CI] = 0.63 [0.45, 0.88]
P = 0.007HR [95% CI] = 0.52 [0.35, 0.76]
P < 0.001
15.6%
8.5%
∆ 7.1%

Primary Endpoint
0 6 12 18 24
496 462 452 436454 378 370 352
Number at risk:
TAVRSurgery
Months after Procedure
422339
TAVRSurgery
Dea
th, S
troke
, or R
ehos
p(%
)
11.5%
17.4%
0
10
20
HR [95% CI] = 0.63 [0.45, 0.88]
P = 0.007HR [95% CI] =0.52 [0.35, 0.76]
P < 0.001
15.6%
8.5%
∆ 7.1%
∆ 5.9%


The PARTNER 3 TrialConclusions
In a defined population of severe symptomatic aortic stenosis patients who were at low surgical risk, TAVR (using the SAPIEN 3 valve) compared to surgery @ 2 years demonstrated:• Reduced primary endpoint events (37% reduction in death, stroke or
CV rehospitalization); BUT… More death and stroke events in TAVR patients from
1 to 2 years; no significant differences @ 2 years Reduced CV rehospitalizations favoring TAVR
• Increased valve thrombosis events in TAVR patients, esp. from 1 to 2 years
• Hemodynamic improvements and frequency of moderate or mild paravalvular regurgitation were unchanged between 1 and 2 years in both TAVR and surgery patients

Discussion

Program completion
By selecting OBTAIN MY CERTIFICATE you can complete the session evaluation and will receive a certificate confirming your attendance at this non-accredited session.
Your certificate will be sent to you by email upon completion.
Your certificate will provide instruction on how you can claim self-learning credits for your
participation in this session
Select this tab in the top right corner of your screen.

Program completion
Access your notes following the program in
My Account on the MD-Online website
Download these slides from the PROGRAM PAGE
on the MD-Online websiteLinks & Resources
Program Page

Sponsors