Embed Size (px)
Citation preview

itochondria are far more than the power plants of our cells. Few people realize that these tiny structures play a central role in our physiology in various contexts and maintain a complex, synergistic relationship with the nuclear genome (see box on page 2). Molecular dermatology scientist Mark A. Birch-Machin, PhD, is among those who do. (Birch-Machin is Professor of Molecular Dermatology, Department of Derma-tology; Associate Dean, Newcastle University Institute of Cellular Medicine; Newcastle University, Newcastle upon Tyne, England.)
And in studying the functions of mitochondria in human skin, Birch-Machin recently made an eye-opening discovery
that is critically important to both mitochondrial and skin health in chronologic and photoaging. It concerns the unex-pected protective role of complex II—the diminutive, unassuming member of the respiratory enzyme chain that completes conversion of the energy from glucose into ATP (see box on page 7). The implications are profound for under-standing what can go wrong and why, and for developing therapeutic interventions to slow chronological aging, protect against photoaging, and reverse existing changes of concern.
Getting Hooked on Mitochondria— And Then the Skin
When Birch-Machin finished his PhD in molecular biology in 1986, he chose a postdoctoral fellowship with mitochondrial expert Professor Sir Doug Turnbull at Newcastle University in the U.K. Turnbull—now Director of the Wellcome Trust Centre for Mitochondrial Research there—was dedicated to uncover-ing the molecular mechanisms responsible for mitochondrial diseases. “I was very much impacted by the illnesses associ- ated with mitochondrial dysfunction,” Birch-Machin recalls. “Children with these diseases died very early, and it was devastating.” He has been committed to understanding mito-chondrial dysfunction ever since, with the ultimate goal of finding ways to correct it.
For the next decade Birch-Machin focused on pediatric mitochondrial myopathies, with assignments in the U.S., Canada, and then Paris. Along the way, he began to develop innovative techniques for gaining information about the mito-chondrial genome. Then, while he was at the Hôpital Necker for Sick Children in Paris, the Department of Dermatology at Newcastle University expressed interest in having him apply his research techniques to mitochondria in human skin.
As he considered this, Birch-Machin began to think about the skin’s role of “communicating with the environment— and I had a kind of epiphany,” he recalls. “I knew from my mitochondrial research in muscle and brain that mitochondria play a role in chronologic aging, which involves declining
(Continued on page 2)
DERMATOLOGY FOCUS
DERMATOLOGY FOCUS
™
VOL. 37 NO. 4 WINTER/SPRING 2019
A DERMATOLOGY FOUNDATION PUBLICATION
Also In This Issue
DF Honors Jeffrey P. Callen, MD
$2.74 Million in Research Funding for 2019
Sincere Thanks to 2018 Volunteers
SPONSORED BY ORTHO DERMATOLOGICS
The Mitochondria and Complex II—Linchpin for Skin Aging and Photoaging
M
PH OH
PL
OL
Thr
Val
D-Loop
CytB
ND6
ND5
ND4
ND4L
ND3
COXIII
COXIICOXI
ND2
ND1
16SRNA
12SRNA
AT
P6
AT
P8
Leu
Human mtDNA16,569bp
IleLight strandHeavy
strand
Met
LysAsp
Ser
CysAla
Gln
GlyArg
HisLeu
Ser
Trp
Tyr
Phe
Glu
Pro
Asn
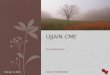
Mitochondrial genome (mtDNA). This schematic representation (not drawn to scale) of the double-stranded circular molecule notes the 37 genes it encodes, which involve components of the respiratory chain enzymes (except for Complex II, which is found in the nuclear genome). Note its economy of space, almost entirely (~93%) devoted to coding regions. (Reprinted with permission from AS Tulah & MA Birch-Machin. Mitochondrion. 2013;13:444–53.)

2 Winter/Spring 2019 Dermatology Foundation
metabolic energy and increasing oxidative stress. I also knew that mitochondria don’t repair very well,” he continues—“and it occurred to me that mitochondrial damage in the skin most likely increases measurably with sun exposure. I became really excited to study the role of mitochondria in skin aging, and also understand the effect that sun exposure has on this normal process. In my experience, no one had explored this before—and I wanted to do it.” Birch-Machin has focused on the skin ever since, expanding understanding in ways that will ultimately influence patient care.
mtDNA Damage—Biomarker of Cumulative UV Radiation Exposure
Specific properties of the mitochondrial genome had led Birch-Machin to hypothesize that mtDNA damage accurately reflects the cumulative impact of sun exposure. Mitochondrial genes lack the histone covering that is an important protector of nuclear genes, and their repair mechanisms are limited. The genome is also in close physical prox-imity to where superoxide generation—which occurs during UV exposure—takes place. So the mitochondrial genome is multiply vulnerable, and its limited repair capabilities allow damage to accumulate over time. The extent of this underlying damage, thou gh, is not manifest. Because there are a great many nonclonal mito-chondria within individual cells and multiple copies of the mitochondrial genome within each mitochondrion (see box below), there are usually enough molecules of functional mtDNA to compensate for those with mutations and maintain cell functions. But Birch-Machin suspected that assessing the
extent of these silent mutations should provide measurable evidence of UV-induced damage to mtDNA, and that the extent of damage would increase with increasing UV exposure—ie, it would be a highly sensitive biomarker of UV exposure in human skin.
Previous studies had examined the frequency of just a single common deletion. But Birch-Machin believed that a
complete picture was the only accurate way to begin. He and his team assessed 71 split-skin samples taken from body areas that were either unexposed, intermittently exposed, or highly sun exposed, and identified the full spectrum of mtDNA deletions in each skin sample. The number of deletions in the epidermis increased signifi-cantly as UV exposure increased, but mtDNA in the dermis showed no effect. Next, they focused on a single, rarely reported 3895 bp mtDNA deletion in age-matched skin samples, again from body areas with large differences in sun exposure. The frequency of this rare deletion increased in line with increasing UV exposure—this time in both the epidermis and dermis. Exposing cultured
human fibroblasts to a UVA+UVB light source confirmed this. The same rare mtDNA deletion appeared; then its presence increased in response to continued exposure.
Next, Birch-Machin and his team determined that the shorter UVR wavelengths (>320 nm) are primarily responsible for this mtDNA damage—the same part of the spectrum already implicated in both UVR-induced erythema and nuclear DNA damage in the skin. Under shorter-wavelength UVR, dermal fibroblasts turned out to be far more sensitive to
Mitochondria—The Tiny Organelles with the Huge Punch Back in the mists of evolutionary time, our mitochondria—the cellular organelles in our cytoplasm that produce 90% of
the chemical energy that our cells need to survive, and contribute substantially to other basic cellular functions—were independently dwelling purple photosynthetic bacteria. As eukaryotes evolved more than 1 billion years ago, these free-living bacteria became incorporated within them—the process of endosymbiosis—and developed a mutually dependent relationship. Their genomes, though, remained independent entities, and mitochondrial replication is independent of cell division. The human nuclear genome now contains 3 billion base pairs, with only about 2% actually coding for its 20,000 genes. The mito-chondrial genome (mtDNA) evolved in the opposite direction, contracting down to a 16.5-kb circular structure containing just 16,569 base pairs and 37 genes (see illustration on front cover). Unlike nuclear DNA, mtDNA is a model of efficiency, with no introns and no spacing between genes, so that almost all of it (~93%) represents a coding region. These dual-membrane mitochondria are rich in fats, proteins, and enzymes, but some of the proteins essential to their function—including the entire complex II respiratory enzyme (see box on page 7)—are produced by the cell, not by the mitochondria.
What this genome lacks in size, it makes up for in exceptional numbers. Excluding mature red blood cells, which are unique in lacking both a nucleus and mitochondria, the individual cellular presence of these organelles ranges from around 1,000 in cells with lower ATP needs to roughly 7,000 in individual human myocytes. Adding it all up, we contain roughly 500 trillion mitochondria, accounting for roughly 30% of our body weight. And each individual mitochondrion holds from 1 to 15 mtDNA molecules. Each cell’s population is not clonal, but includes normal—ie, wild-type—and various mutation-altered states. The presence of wild-type genomes is potent. “There can actually be quite profound deficiencies and damage present, but the remaining wild-type genomes will complement the damaged ones,” Birch-Machin explains. “In some cases, just 10% of the mitochondrial genomes need to be normal to make up for the deficiencies of the other 90%.”
Although mitochondria are best known as the cell’s powerhouse—converting the energy from glucose into ATP—this is just part of what they do. Among other things, they participate in cellular differentiation, cell growth, the cell cycle, apop-tosis, and steroid synthesis. They are platforms for intracellular signaling, regulators of innate immunity, modulators of stem cell activity, and are host to numerous biosynthetic and signaling processes that ultimately couple cellular metabolism to homeostatic regulatory mechanisms. Dysfunctional mitochondria are thus responsible for a number of human diseases and conditions. This past summer, mitochondrial research at the University of Southern California documented cross-regulation between the nuclear and mitochondrial genomes—noting that sometimes it’s the mitochondrial DNA in charge.
Mark A. Birch-Machin, PhD

sun-induced mtDNA damage than keratinocytes, a discovery that holds “important implications for disease and photodam-age mechanisms and for interventions,” Birch-Machin points out.
Complex II—Newly Recognized Importance in Skin The four respiratory chain enzymes—complex I through
complex IV—gradually transform the energy from glucose into ATP (see box on page 7). The byproducts of this process also make these enzymes the major generator of cellular oxidative stress. mtDNA vulnerability to this stress results in damage that in turn reduces the mitochondria’s ability to repair them-selves, which increases the production of mutations and dys-function, which further increases ROS production, which diminishes repair capabilities still further, producing addi- tional mutations…. This vicious cycle is thought to underlie the mitochondria’s contribution to aging, cancer, neurode- generation, and cell death in many tissues.
Birch-Machin and his group had already shown that UVA exposure increases both ROS production and mtDNA muta-tions in human skin. Now he wanted to begin exploring its role in this vicious cycle by identifying the most important sites of ROS production within the mitochondrial respiratory chain. Although he was not the first investigator to pose this question, he was among the very few to explore it in skin and the first to pursue it in human skin. Birch-Machin found this lack of attention to human skin quite surprising, “given that the skin is regularly exposed to the harmful UVA rays in sunlight.”
He and his team created multiple cultures of human ker-atinocytes (from the immortalized HaCaT cell line) and of fibroblasts (from neonatal foreskin). Each of the four respira-tory chain enzymes can be inhibited by several chemical agents, and Birch-Machin modified the individual cultures by adding, separately, each of these inhibitors. Then he exposed these cultures to doses of UVA irradiation that are comparable to normal outdoor exposure. Representative cultures were left unexposed as controls. The expectation was that among the various UVA-exposed cultures, the missing enzyme associated with the largest drop in UVA-induced ROS production would—under normal circumstances—be the largest contributor to ROS production.
The results took them in a very different direction. Complex II stood out—but not for producing the lion’s share
of ROS. Instead, it was unique for its ability to suppress ROS production, because inhibiting its activity increased ROS levels considerably.
Birch-Machin also engineered a comparison of young and aging tissues to see if the levels of these respiratory chain en-zymes change with age. Shrinking telomeres are considered to be a biomarker of aging, so he and his team used cultures grown from two versions of human fetal lung fibroblasts. The “youthful” tissue cultures were grown from fibroblasts engi-neered to overexpress the telomerase enzyme, which lengthens telomeres at the ends of nuclear genes. Because the unal-tered—wild-type—cells had shorter telomeres, in relative terms they represented aging tissue. Assessing the individual levels of complexes I–IV in the “young” and “aging” fibroblast cultures highlighted complex II again. It was the only respira-tory chain enzyme showing decreased activity in the “aging” lung fibroblasts. In line with this, recent data from a lab using mice to study aging skin in vivo had shown a decrease in complex II activity along with an increase in senescent cells in the skin as mice aged.
Birch-Machin realized for the first time that “the effect of complex II in human skin cells may be significantly more im-portant than previously thought.” It would explain why the activity of this tiny enzyme is approximately twofold greater in skin cells than in the liver, for example. Complex II also differs
www.dermatologyfoundation.org Winter/Spring 2019 3
Editors-in-Chief
Lindy Fox, MD – Professor of Dermatology University of California, San Francisco
Mary M. Tomayko, MD, PhD – Associate Professor of Dermatology Yale School of Medicine, New Haven, CT
Heidi A. Waldorf, MD – Director, Laser and Cosmetic Dermatology The Mount Sinai Medical Center, New York, NY
Executive Director Sandra Rahn Benz
Deputy Executive Director Christine M. Boris
Please address correspondence to: Editors-in-Chief, Dermatology Focus
c/o The Dermatology Foundation 1560 Sherman Avenue, Suite 500, Evanston, Illinois 60201 Tel: 847-328-2256 Fax: 847-328-0509 e-mail: [email protected]
Published for the Dermatology Foundation by
Robert B. Goetz—Designer, Production
Sheila Sperber Haas, PhD—Managing Editor, Writer
This issue of Dermatology Focus is distributed without charge through an educational grant from Ortho Dermatologics.
The opinions expressed in this publication do not necessarily reflect those of the Dermatology Foundation or Ortho Dermatologics. © Copyright 2019 by the Dermatology Foundation
DERMATOLOGY FOCUS A PUBLICATION OF THE DERMATOLOGY FOUNDATION Sponsored by Ortho Dermatologics A wholly owned subsidiary of Bausch Health Companies Inc.
Like us on Facebook
(Continued on page 4)
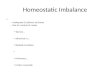
Complex II and the electron transport chain (ETC). This final step in ATP production involves the 4 respiratory enzymes. Complex II, although dramatically smaller than its family members, is the only one also active in the preceding phase—the Krebs cycle, in which it reduces ubiquinone. Thus, small changes in complex II translate to powerful impact. The ETC’s oxidative byproducts are indicated. (Reprinted with permission from K. Kandola et al. Int J Cosmetic Sci. 2015;37(Suppl 2):1–8.)

4 Winter/Spring 2019 Dermatology Foundation
from the other three respiratory chain enzymes in a fundamen-tal way. All of its subunits and assembling proteins are produced exclusively by the nuclear genome.
Pursuing the Aging Connection Birch-Machin wasted no time in following up on this ob-
servation that “younger” fetal lung fibroblasts contained more complex II than the “older” ones did. “It is highly important to understand the aging process in skin,” he emphasizes. “Skin is the largest organ of the body, acting as a protective barrier to a spectrum of external insults that includes UV radiation, infection, toxicity, and mechanical stress.” A better under- standing of the underlying biology will enable maintenance of skin health. And beyond this, “the skin is an organ that can be accessed and studied easily, and thus what is learned from this research may have profound relevance and application to aging in other body tissues,” he adds.
To explore the role of complex II in skin aging, Birch-Machin and his team worked with foreskin tissue (sun-
protected, eliminating any influence of UV exposure) from 27 males ranging from 6 to 72 years of age. They studied skin aging from two perspectives. Biological aging concerns the functional decline of the entire organism over time. Cellular senescence involves the transformation of proliferating cells to a state of irreversible growth arrest. On the positive side, senescence acts as an important tumor suppressive mecha-nism by preventing potentially malignant cells from undergoing replication; plus, senescent cells produce cytokines that aid wound healing. But senescent cells also have a number of significant negative effects—including ROS production and secretion of inflammatory cytokines—and thus are thought to be prominent in the aging process.
Biological aging: Birch-Machin and his team cultured fibroblasts and keratinocytes from each of these skin samples, then precisely calculated the activity level of complex II per unit of mitochondria in every culture. They also measured gene transcript expression and protein levels for complex II.
The Dermatology Foundation pays annual tribute to dermatologists whose exemplary capabilities and dedication have helped to make the specialty what it is today. Presentation of the 2018 awards was a highlight of the DF Annual Meeting on Saturday, March 2, 2019 in Washington, DC. The leaders and role models honored by their peers are:
Lifetime Career Educator Award—Jeffrey P. Callen, MD
Practitioner of the Year—Tina Alster, MD
Clark W. Finnerud Award—Jeffrey Sugarman, MD, PhD
(Drs. Alster and Sugarman will be highlighted in the next issue.)
2018 Lifetime Career Educator Award: Jeffrey P. Callen, MD Recognizing an academic dermatologist with a career-long history of dedicated service
as a mentor, role model, and inspirational teacher
DF Honors Excellence in Dermatology
“Dr. Callen is a true dermatology legend,” shared a colleague and mentee. “He is a change agent in our field, a sought-after educator, a national leader in the academy, and a devoted teacher and mentor who never fails to respond to any email from the countless individuals seeking his counsel.”
World-renowned medical dermatologist Dr. Jeffrey Callen—who chose to specialize in the highly challenging spectrum of collagen vascular diseases—has spent most of his career at the University of Louisville. He joined the faculty there in 1977 (and became the Chief of the Division of Dermatology in 1988), and has consistently main-
tained the ideals that have been critical to him from the outset. He gives his patients the best possible attention and compassionate care. He carries out research that improves the ability to understand, diagnose, and treat the collagen vascular diseases. Dr. Callen is also a well-known and respected teacher, taking advantage of any opportunity to provide what he believes will enable others to become the best dermatologists they can be. This includes his 30+ years of directing the residency program, lecturing, and mentoring young colleagues. Since arriving in Louisville, he has also maintained an ongoing lecture series to broaden the education of local doctors.
(Continued on page 6)
(Continued on top of page 5)

www.dermatologyfoundation.org Winter/Spring 2019 5
Dr. Callen notes that teaching has always
held special meaning for him. “It is deeply
rewarding because of the reach I have,” he
explains. “I love taking care of patients—but
when I am in my office my reach is
limited to the individual patient. When
I’m sharing information that will
help others be effective dermatolo-
gists, I hope to improve the quality
of a great many patients’ lives.”
Ironically, Dr. Callen had planned
to follow in his cardiologist father’s
footsteps. He was enjoying his final
year of internal medicine residency
at the University of Michigan and
eagerly anticipating a cardiology
fellowship when his dermatology
rotation began. “I was seeing patients
who had challenging problems that related a great
deal to internal medicine,” he recalls, “and this ex-
perience was fascinating.” Then Dr. Callen learned
that there would be a new dermatology chair and
a position was open for residency. He was encour-
aged to apply—and was accepted. ”It was not an
easy decision to give up that cardiology slot, but I
had been smitten by the complexity of dermatology
and the visual ability to make diagnoses,” he says.
“I was in the right place at the right time,”
Dr. Callen points out that ”my interest from
the start was this intersection between the external
and the internal.” He has shared what he has learned
in what have become definitive texts: Dermatological Signs of Systemic Disease, and Color Atlas of
Dermatology. One of Dr. Callen’s
special authorial enjoyments is
unearthing dermatology-relevant
information in the nondermatology
literature and reviewing it for the
dermatology community.
An exceptional number of official
accolades over his career attest to
Dr. Callen’s profound influence on
the field as one of the specialty’s
outstanding clinicians, scientists,
organizational thought leaders, and
teachers. His recent selection by the
AAD for the Master Dermatologist award also emphasizes his “extraordinary and
vast contributions through curriculum development
and authorship of hundreds of publications.”
Over the years, Dr. Callen has been instrumental
in training and teaching thousands of students and
colleagues. One colleague’s comment says it all:
“Quite simply, Dr. Callen has changed my life
as a physician, educator, and mentor. He has
single-handedly changed our field for the
better—and his impact will continue for
generations to come.”
2019 Leadership GalaThe Annual Leadership Gala is always eagerly
anticipated by Leaders Society, Annenberg Circle,
AC Sustaining, and Fitzpatrick Legacy Fund members.
The DF provides this special thank-you for their strong,
ongoing commitment to advancing the knowledge that
is essential to progress in patient care.
This year’s Gala, and the Young Leaders Pre-Gala,
were held the evening of March 3 at Washington DC’s
memorable National Museum of Women in the Arts.
The DF is grateful to the co-sponsors of this memorable event: Celgene Corporation; Galderma; Lilly USA, LLC; Ortho Dermatologics

Results were compared with complex IV, chosen as the control because—unlike com-plexes I and III—it is not directly linked to complex II within the electron transport chain. When the results were in, it became clear that complex II activity is pivotal to fibroblast func-tion—but not to keratinocytes.
To begin with, complex II activity was sub-stantially greater in fibroblasts than in ker-atinocytes, up to twice as high in cell cultures from younger donors. In addition, complex II activity decreased steadily with donor age—but only in fibroblasts (see graphs below). Because gene transcript expression and pro-tein levels for complex II also declined with age in fibroblasts, it appeared that in fibrob-lasts from this sun-protected area, the enzyme itself had not lost effectiveness with age but there was less and less of it. With the increasing loss of complex II’s protective actions, ROS-caused damage would exacerbate this diminishing activity. Complex IV showed no relation to age in either cell culture.
Senescence: When Birch-Machin and his team turned their attention to the relationship between senescence, complex II, and biologi-cal age in human skin, the results shed light on their observations with biological aging. Fibroblast cultures from 15 of the initial donors (ages 6–71 years) were separated into senescent and nonsenescent cell populations using the senescence biomarker lipofuscin, a wear-and-tear fluorescent pigment that is a remnant of the transition to senescence. As donor age increased, the number of senescent fibroblasts increased while the activity level of complex II decreased—but only in senes-cent fibroblasts. (Complex IV activity level in senescent fibroblasts was unrelated to donor
6 Winter/Spring 2019 Dermatology Foundation
AC Sustaining Generosity Continued to Grow
2018 New AC Sustaining Members, New Multi-Year Pledges
$75,000
Jeffrey P. Callen, MD Jean M. Holland, MD
James T. Sandwich, MD
$50,000
George Cotsarelis, MD Carol L. Huang, MD
$30,000
Erin E. Boh, MD, PhD Mathijs H. Brentjens, MD
Robert J. Pariser, MD
Stephen M. Purcell, DO Alan K. Silverman, MD
Barbara Dahl Wilson, MD
AC Sustaining members contribute $5,000 annually after completing the $25,000 Annenberg Circle commitment.
The Dermatology Foundation offers a special thank-you to those who made the significant decision to become a Sustaining
contributor or extend their Sustaining commitment years into the future. This exceptional generosity ensures the progress in
dermatology that will enable dermatologists to provide the best possible care for their patients. Sustaining members are
recognized according to their cumulative AC giving level.
Complex II pivotal to fibroblasts. In foreskin samples from males ranging from 6–72 years of age, complex II activity was highest in fibroblasts from the youngest donors and steadily decreased with age. There was no relationship in keratinocytes from these same samples. (Reprinted with permission from A Bowman & MA Birch-Machin. J Invest Dermatol. 2016;136:912–19.)
0.250 10 20 30 40 50 60 70 80
0.30
0.35
0.40
0.45
0.50Fibroblasts
Donor Age (years)
0 10 20 30 40 50 60 70 80Donor Age (years)
CII
/CS
Ac
tiv
ity
0.00
0.10
0.05
0.15
0.25
0.20
0.30
0.35Keratinocytes
CII
/CS
Ac
tiv
ity

www.dermatologyfoundation.org Winter/Spring 2019 7
age.) The surprise was that purely nonsenes-cent fibroblast cultures showed no correlation between aging and complex II activity.
These unexpected results refocused the initial picture. The age-related decrease in complex II activity observed in the original fibroblast cultures did not actually reflect the entire fibroblast population, but was specifi-cally a function of the senescent cell subset. Isolating the senescent fibroblasts for study emphasized that—in terms of mitochondrial complex II activity—senescent fibroblasts in the skin of older individuals are less efficient than those in younger individuals.
Human in vivo data will be required to confirm and flesh out the role of decreasing complex II activity in skin aging, and to clarify whether this loss is a cause or a consequence of aging—or both, as the vicious cycle of aging would predict. Any of these scenarios,
Founding Members (As of April 1, 2019)
The Dermatology Foundation Trustees are grateful to each
of the following members who have made an invaluable
commitment to progress in patient care through a
planned gift.
David R. Bickers, MD
Ronald R. Brancaccio, MD
Lisa A. Garner, MD
Karl V. Kaess, MD
James J. Leyden, MD
Tomoko Maeda-Chubachi, MD, PhD, MBA
Renée J. Mathur, MD
Elizabeth I. McBurney, MD
Kishwer S. Nehal, MD
Glenn A. Oclassen
Thomas G. Olsen, MD
Michael D. Tharp, MD
Bruce U. Wintroub, MD
A planned giving opportunity for DF members who wish to have a transformative impact
on the future of the specialty. The continuous pursuit of
new knowledge through research is essential for furthering the specialty and advancing the boundaries of care for every patient. Through the Dermatology Foundation’s new Visionary Society, members can ensure that
their field has the support essential to this progress far into the future. The Society is for those who wish to support the ongoing work
of the Foundation through an estate gift. Every contribution made through the Society is invested in the DF Research Endowment fund, which is managed to deliver reliable funding in perpetuity.
To join the Visionary Society, please contact the DF office at [email protected] or 847-328-2256 for the steps to follow in arranging your personal estate gift to the Foundation. All members confirming their planned gift in the 2019 calendar year will be recognized as Founders of the Visionary Society.
(Continued on page 8)
The Power of Complex II Complex II is tiny—only four subunits in size—but particularly power-
ful because it is involved in two phases of the progression from glucose to ATP, not just one. Yet mitochondrial researchers have learned this only recently. They had paid scant attention to complex II because it is so much smaller than the other respiratory chain enzymes, which contain from 10 to 45 subunits. But its minimal size disguises immense impact—far greater than that of the other three complexes—because it is involved in the Krebs cycle as well as the electron transport chain. “Because it is involved in two major metabolic pathways,” Birch-Machin explains, “a small change in this enzyme has a profound effect.”
There are three steps in producing ATP. The process begins with the release of energy from glucose. Then the Krebs—citric acid—cycle captures this energy and stores it in carrier molecules, enabled by complex II’s contribution of reduced ubiquinone. In the final stage of aerobic respiration—the electron transport stage—complexes I, III, and IV engineer the production of ATP and enable it to leave the mitochondria. This involves electron transfers, proton gradients, and oxygen, producing reactive oxygen species (ROS) as byproducts. Complex II participates by—as Birch-Machin has discovered—minimizing ROS production and damage. Chronic oxidative stress has been linked to a myriad of pathologies.

including direct DNA damage initiated by increased ROS production, is likely to increase overall mitochondrial dysfunction. And the result is decreased tissue function.
Testing Interventions Because antioxidant compounds neutralize ROS, thus
reducing or eliminating oxidative damage, this is a logical area to explore for candidates to support skin health and prevent further damage in the face of ROS-inducing conditions. Birch-Machin has begun evaluating candidates from medicinal plants and plant extracts as well as chemical molecules.
Clitoria ternatea L: Birch-Machin learned of C. ternatea—the butterfly pea plant—from Dr. Edward Okello, a neurology colleague who is also Executive Director of the Medicinal Plant Research Group. Indigenous to tropical Asia, the plant spread more widely across Asia and to Latin America and the East and West Indies, and has extensive traditional uses. One involves an herbal tea made from the colorful blue-and-white flower that is taken to protect the skin against age-related changes and sun- induced damage. Research on the plant’s biological activities have focused on the root, seeds, and leaf, but the flower was
recently found to contain anthocyanins, which are known antioxidants.
Birch-Machin incubated human keratinocyte cultures with the flower water extract (CTW), then rinsed them before expo-sure to hydrogen peroxide or UV. There was significantly less cytotoxicity and mtDNA damage after CTW treatment than in nontreated cells. A phytochemical analysis of the flower identifed major concentrations of polyacylated anthocyanins and flavonol glycosides, both with widely documented antiox-idant actions. Birch-Machin points out that the flower extract’s significant ability to protect against UV-induced mtDNA damage indicates a potential for preventing oxidative stress arising from mitochondrial dysfunction. Further research for therapeutic benefits is warranted. “We will also be studying additional Malaysian species, working in conjunction with Kew Gardens in London,” Birch-Machin says.
Antioxidant molecules: The first round of experiments compared the protective capability of two antioxidant molecules able to penetrate the mitochondria. MitoQ (mitoquinone)—a modified ubiquinone molecule developed
8 Winter/Spring 2019 Dermatology Foundation
(Continued on page 10)
DF Award to Further Diversity in Specialty“Diversity matters in medicine,” shared Chair Bruce U.
Wintroub, MD, at the Dermatology Foundation’s recent
Annual Meeting. “A more diverse physician workforce in derma-
tology can improve access and overall patient care for minority
populations that are currently underrepresented in our specialty.
Achieving a workforce that mirrors the race and ethnicity of every
community is an important long-term goal that can be furthered
by attracting more medical students from underrepresented
populations to the specialty.”
Last year, the Dermatology Foundation stepped up to this
important challenge and introduced the Diversity Research
Supplement Award. The 2018 awards were provided to eight
recent DF Career Development Award recipients to supplement
their efforts on existing research projects by providing a medical
student—one belonging to an underrepresented minority group
in medicine—with an in-depth investigative experience in
dermatology.
These awards produced uniformly enthusiastic feedback
from all mentees, who described eye-opening research and
mentorship experiences that carried exceptional value in
clarifying their desired path in medicine. As one student noted:
“I am grateful to the [DF] for affording me the opportunity to experience medicine as a researcher. It allowed me to further explore dermatology as a specialty, and has got me excited about the future of skin cancer inhibition and treatment strategies!”
The DF is proud to support an additional 10 Diversity
Research Supplement Awards this summer, and is honored
to contribute in this meaningful way to improving diversity
in the specialty.
Masaoki Kawasumi, MD, PhD & Kelsey N. Tuttle
Junko Takeshita, MD, PhD, MSCE & Alexis N. Holmes
Janis M. Taube, MD, MSc & J. Michael Bell
2018 Award Mentors / Mentees*
*3 of 8 pictured

www.dermatologyfoundation.org Winter/Spring 2019 9
“Thank You” to 2018 Leaders Society VolunteersThe DF Board of Trustees extends special appreciation to every one of these national campaign volunteers. They have each invested significant work to increase leadership giving in their area. Their concern for continued progress in patient care, and their gift of time and effort throughout 2018, helped to expand support for advancement in the specialty.
ALABAMA Chair Mark D. Herron, MD
Vice Chairs Gregory Bourgeois, MD J. Scott VanLoock, MD
ARIZONA Chair Lindsay Ackerman, MD
Vice Chair Anthony A. Nuara, MD, PhD
ARKANSAS Chair Henry K. Wong, MD, PhD
CALIFORNIA–BAY AREA Chair Eric S. Fromer, MD
Vice Chairs Anne Lynn S. Chang, MD Marlys S. Fassett, MD, PhD Bahram Razani, MD, PhD Roberto R. Ricardo-Gonzalez,
MD, PhD*
CALIFORNIA–LOS ANGELES Chair Jashin J. Wu, MD
CALIFORNIA–SAN DIEGO Chair Neal D. Bhatia, MD
COLORADO Chair Robert P. Dellavalle, MD, PhD
Vice Chair Peggy B. Liao, MD
CONNECTICUT Chair Christopher G. Bunick, MD, PhD
Vice Chairs Sean R. Christensen, MD, PhD Amanda Zubek, MD, PhD
FLORIDA Chair Conor P. Dolehide, MD
Vice Chair Kiran Motaparthi, MD
GEORGIA Chairs Travis W. Blalock, MD
Vice Chair Misty D. Caudell, MD
IDAHO Chair Ryan S. Owsley, MD
Vice Chair Gregory L. Wells, MD
INDIANA Chair Norma H. Schmitz, MD
IOWA Chair Kent D. Walker, MD
Vice Chairs Timothy G. Abrahamson, MD John H. Wollner, MD
KANSAS Chair Cameron West, MD
LOUISIANA Chair Amie Shannon, MD
Vice Chairs Rachel Dean, MD Kim Bui Drew, MD Stephen Klinger, MD* Frankie G. Rholdon, MD
MARYLAND–BALTIMORE Chair Saif U. Syed, MD
MASSACHUSETTS Chair Jennifer T. Huang, MD
Vice Chair Lynne J. Goldberg, MD
MICHIGAN Chair Dana L. Sachs, MD
MINNESOTA Chair Carilyn N. Wieland, MD
MISSOURI Vice Chair Tricia Missall, MD, PhD
NEW YORK–DOWNSTATE Vice Chairs Sherri K. Kaplan, MD Jennifer A. Stein, MD
NEW YORK–UPSTATE Chair Sherrif F. Ibrahim, MD, PhD
NORTH CAROLINA Chair William W. Huang, MD, MPH
Vice Chairs Elias E. Ayli, DO Russell A. Ball, MD Donna A. Culton, MD, PhD
OHIO–NORTH Chair Jonathan Bass, MD
Vice Chairs Jaye E. Benjamin, MD Neil J. Korman, MD, PhD John George Secrist, MD Stephen C. Somach, MD
OHIO–SOUTH Chair Shannon Campbell Trotter, DO
PENNSYLVANIA–EAST Chair Emily Y. Chu, MD, PhD
Vice Chairs Cynthia Bartus, MD Cory L. Simpson, MD, PhD
PENNSYLVANIA–WEST Vice Chair Renée J. Mathur, MD
RHODE ISLAND
Chair Leslie Robinson-Bostom, MD
SOUTH CAROLINA
Chair John C. Maize, Jr., MD
TEXAS–DALLAS Chair Travis W. Vandergriff, MD
Vice Chairs Jeri Beth Foshee, MD Robin A. Roberts, MD
TEXAS– SAN ANTONIO/AUSTIN Chair Allison J. Stocker, MD
Vice Chairs John Browning, MD Thomas L. Davis, MD Catherine L. Kowalewski, DO Keagan H. Lee, MD Vineet Mishra, MD
WASHINGTON Chair Jennifer M. Gardner, MD
Vice Chair Michi M. Shinohara, MD
WEST VIRGINIA Chair Stuart R. Lessin, MD
WISCONSIN Chair Kathleen S. Stokes, MD
Vice Chairs Melanie A. Clark, MD Julia Kasprzak, MD Abigail L. Taub, MD Yaohui Gloria Xu, MD, PhD
PEDIATRIC DERMATOLOGY CAMPAIGN Chair Yvonne E. Chiu, MD Vice Chairs Anna L. Bruckner, MD Kelly M. Cordoro, MD Erin F.D. Mathes, MD
DERMATOPATHOLOGY CAMPAIGN Chair Carrie L. Kovarik, MD Vice Chairs Ryan W. Hick, MD John T. Seykora, MD, PhD Karolyn A. Wanat, MD
*Enrolled three or more new LS members

10 Winter/Spring 2019 Dermatology Foundation
by Mike Murphy, PhD, Program Leader of the MRC Mito- chondrial Biology Unit, University of Cambridge, UK—is actively and exclusively attracted to mitochondria, and sufficiently small to penetrate the mitochondrial membrane. Tiron is a mitochondria-permeating and localized superoxide
scavenger and antioxidant and also chelates metals (including iron and titanium). Human fibroblast cultures were incu-bated with one or the other, then exposed to physiologic doses of UVA or to hydrogen peroxide. Tiron completely pre-vented ROS-induced mtDNA damage across the board. MitoQ reduced damage by 17% and 32%, respectively. (For UVA, see graphs at left.)
Birch-Machin suspected that Tiron’s complete elimination of ROS production indicated a protective effect extending beyond the mitochondria, and
further exploration also demonstrated complete protection of the nuclear genome from hydrogen peroxide-induced damage. MitoQ achieved 18%. Birch-Machin showed that these effects are completely independent of the Nrf2-signaling pathway,
2019 Awards: Supporting Research and Innovation
Thanks to the generosity and vision of its
many members and industry supporters, the
DF awarded $2.74 million in research support
for 59 innovative projects earlier this year.
Each project was carefully reviewed and selected
for its potential to advance patient care. A large
portion of the DF’s funding was allocated to its
highly effective Career Development Awards that
are intended for emerging investigators.
The DF also provided funding in two three-year
award categories for the promising research of
outstanding mid-career investigators, whose need
for research dollars continues to grow. The DF
was very pleased to announce the first new Sun
Pharma Research Award—devoted to projects
focused on highly challenging inflammatory skin
disease. The Stiefel Scholar Award, devoted to
skin cancer research, was bestowed on one new
recipient and one entering Year 2. The Foundation
is deeply grateful to Sun Pharma and to Charles
and Daneen Stiefel for their exceptionally
generous support of progress.
3-yearCareer
DevelopmentAwards
3-yearStiefel Scholar
Award forSkin Cancer
Research
1-yearFellowships
1-yearGrants
DiversityResearch
SupplementAwards
3-yearSun Pharma
Award for Inflammatory Skin Disease
Research
$2,255,000(41)
$200,000(2) $100,000
(1)$90,000
(3)$50,000
(10)$40,000
(2)
Preventing ROS in skin mitochondria. 2 mitochondria-penetrating molecules were evaluated in UVA-exposed human fibroblast cultures. The modified ubiquinone MitoQ (mitoquinone) reduced oxidative damage by 17%. Tiron—a localized superoxide scavenger, antioxidant, and metal chelator—completely eliminated ROS production. (Reprinted with permission from AO Oyewole et al. The FASEB J. 2014;28:485–94.)
0.0
0.5
1.0
1.5
2.0 ****
Fo
ld D
iffe
ren
ce C
(t)
0.0
0.5
1.0
1.5
2.0
Fo
ld D
iffe
ren
ce C
(t)
Control Tiron Tiron + UVA
UVAControl MitoQ MitoQ + UVA
UVA
(Continued on page 14)
Dr. Bruce U. Wintroub, DF Chair, announced the 2019 funding news at the DF membership meeting,
and congratulated all of the award recipients. “This is a significant milestone for each of you, and
we all look forward to watching the progress you bring to the specialty.”
$2.74 Million in Research Funding

CHART A COURSE
SYMPTOMATIC RELIEF
FOR ADULTS WITH PLAQUE PSORIASIS
TO
The e�cacy of Class 1 halobetasol with safety proven for up to 8 weeks of dosing1,2
BRYHALI and the check mark design are trademarks of Ortho Dermatologics’ a�liated entities. © 2018 All Rights Reserved. BRY.0025.USA.18 DISCOVER MORE AT BRYHALI.COM
STUDY RESULTS: 36.5% of patients in trial 1 and 38.4% in trial 2 achieved treatment success* at week 8 (primary endpoint) vs 8.1% and 12.0% of patients with vehicle, respectively (P<0.001 in both trials).2
STUDY DESIGN: The safety and e�cacy of BRYHALI Lotion were assessed in 2 prospective, multicenter, randomized, double-blind, phase 3 clinical trials in 430 adult patients with moderate-to-severe plaque psoriasis. Patients were treated with BRYHALI Lotion or vehicle lotion, applied once daily. Primary e�cacy endpoint was treatment success evaluated at week 8. Secondary e�cacy endpoint was treatment success evaluated at weeks 2, 4, 6, and 12 (4 weeks post treatment). Tertiary e�cacy endpoint was a 2-grade improvement from baseline at each time point for the individual signs of psoriasis (erythema, plaque elevation, and scaling).2
* Treatment success was de昀ned as at least a 2-grade improvement from baseline in the Investigator’s Global Assessment score, and a score of “clear” or “almost clear” (primary endpoint at week 8).2
References: 1. BRYHALI Lotion [prescribing information]. Bridgewater, NJ. Valeant Pharmaceuticals North America LLC. 2. Data on 昀le.
A NEW POTENCY CLASS OF STEROID LOTION
IndicationBRYHALI™ (halobetasol propionate) Lotion, 0.01% is a corticosteroid indicated for the topical treatment of plaque psoriasis in adults.
Important Safety Information Warnings and Precautions
• BRYHALI Lotion has been shown to suppress the hypothalamic-pituitary-adrenal (HPA) axis during treatment or upon cessation of treatment; periodic evaluation may be required.
• Systemic e昀ects of topical corticosteroids may also include Cushing’s syndrome, hyperglycemia, and glucosuria.
• Children may be more susceptible to systemic toxicity when treated with topical corticosteroids.
• Local adverse reactions may include atrophy, striae, telangiectasias, hypopigmentation, and allergic contact dermatitis. Some local adverse reactions may be irreversible.
• Use of topical corticosteroids may increase the risk of posterior subcapsular cataracts and glaucoma. If visual symptoms occur, consider referral to an ophthalmologist.
• Use an appropriate antimicrobial agent if a skin infection is present or occurs, and if prompt response is not seen, discontinue use until infection has been adequately treated.
• Discontinue BRYHALI Lotion if allergic contact dermatitis occurs.
Adverse Reactions• The most common adverse reactions (≥1%) were upper respiratory
tract infection, application site dermatitis, and hyperglycemia.
To report SUSPECTED ADVERSE REACTIONS, contact Customer Service at 1-800-321-4576 or FDA at 1-800-FDA-1088.
Please see Brief Summary of full Prescribing Information on following page.
2 PIVOTAL PHASE 3 TRIALS
Continued results 4 weeks post treatment1
Signi昀cant symptomatic relief as early as week 22
No increased epidermal atrophy observed through 8 weeks of treatment2
Local adverse reactions from topical corticosteroids may include atrophy, striae, telangiectasias, hypopigmentation and allergic contact
dermatitis. Some local adverse reactions may be irreversible.
POTENT TO SUPERPOTENT CLEARANCE1:
BRYHALI(�������������� �����)���� �������%
TM

BRIEF SUMMARY OF PRESCRIBING INFORMATIONThis brief summary does not include all the information needed to use BRYHALI safely and effectively. See full prescribing information for BRYHALI.
BRYHALI™ (halobetasol propionate) lotion, 0.01% for topical use Initial U.S. Approval: 1990
INDICATIONS AND USAGEBRYHALI™ (halobetasol propionate) Lotion, 0.01% is indicated for the topical treatment of plaque psoriasis in adults.
CONTRAINDICATIONSNone.
WARNINGS AND PRECAUTIONSHypothalamic-Pituitary-Adrenal (HPA) Axis SuppressionBRYHALI has been shown to suppress the hypothalamic-pituitary-adrenal (HPA) axis.Systemic effects of topical corticosteroids may include reversible HPA axis suppression with the potential for glucocorticosteroid insufficiency. This may occur during treatment or upon withdrawal of treatment with the topical corticosteroid.
The potential for hypothalamic-pituitary-adrenal (HPA) axis suppression with BRYHALI was evaluated in a study of 19 adult subjects with moderate to severe plaque psoriasis involving ≥20% of their body surface area (BSA). HPA axis suppression was reported for 1 (5.6%) subject at Week 4 and for 3 (15.8%) subjects at Week 8. All 3 subjects had normal HPA axis suppression test with discontinuation of treatment [see Clinical Pharmacology in full Prescribing Information].
Because of the potential for systemic absorption, use of topical corticosteroids, including BRYHALI, may require that patients be evaluated periodically for evidence of HPA axis suppression. Factors that predispose a patient using a topical corticosteroid to HPA axis suppression include the use of more potent corticosteroids, use over large surface areas, occlusive use, use on an altered skin barrier, concomitant use of multiple corticosteroid-containing products, liver failure, and young age. An adrenocorticotropic hormone (ACTH) stimulation test may be helpful in evaluating patients for HPA axis suppression.
If HPA axis suppression is documented, attempt to gradually withdraw the drug, reduce the frequency of application, or substitute a less potent steroid. Manifestations of adrenal insufficiency may require supplemental systemic corticosteroids. Recovery of HPA axis function is generally prompt and complete upon discontinuation of topical corticosteroids.
Systemic effects of topical corticosteroids may also include Cushing’s syndrome, hyperglycemia, and glucosuria. Use of more than one corticosteroid-containing product at the same time may increase the total systemic exposure to corticosteroids. Pediatric patients may be more susceptible than adults to systemic toxicity from the use of topical corticosteroids due to their larger surface-to-body mass ratios [see Use in Specific Populations].
Local Adverse ReactionsLocal adverse reactions from topical corticosteroids may include atrophy, striae, telangiectasias, burning, itching, irritation, dryness, folliculitis, acneiform eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, secondary infection, and miliaria. These may be more likely with occlusive use, prolonged use, or use of higher potency corticosteroids, including BRYHALI. Some local adverse reactions may be irreversible.
Concomitant Skin Infections Use an appropriate antimicrobial agent if a skin infection is present or develops. If a favorable response does not occur promptly, discontinue use of BRYHALI until the infection has been adequately treated.
Allergic Contact Dermatitis Allergic contact dermatitis with corticosteroids is usually diagnosed by observing failure to heal rather than noting a clinical exacerbation. Consider confirmation of a clinical diagnosis of allergic contact dermatitis by appropriate patch testing. Discontinue BRYHALI if allergic contact dermatitis occurs.
ADVERSE REACTIONSClinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
In randomized, double-blind, multicenter, vehicle-controlled clinical trials, 426 adults with plaque psoriasis were treated with BRYHALI and had post-baseline safety data. Subjects applied BRYHALI once daily for up to eight weeks. Table 1 presents adverse reactions that occurred in at least 1% of subjects treated with BRYHALI and more frequently than in vehicle-treated patients.
Table 1: Adverse Reactions Occurring in ≥1% of the Subjects Treated with BRYHALI through Week 8
BRYHALI (N=284)
Vehicle (N=142)
Adverse Reaction % %
Upper Respiratory Tract Infection 2% 1%
Application Site Dermatitis 1% 0
Hyperglycemia 1% 0
USE IN SPECIFIC POPULATIONSPregnancy
Risk SummaryThere are no available data on BRYHALI use in pregnant women to inform a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes.In animal reproduction studies, increased malformations, including cleft palate and omphalocele, were observed after oral administration of halobetasol propionate during organogenesis to pregnant rats and rabbits. The available data do not support relevant comparisons of systemic halobetasol propionate exposures achieved in the animal studies to exposures observed in humans after topical use of BRYHALI.
The background risk of major birth defects and miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2 to 4% and 15 to 20%, respectively.
Data
Animal DataHalobetasol propionate has been shown to cause malformations in rats and rabbits when given orally during organogenesis at doses of 0.04 to 0.1 mg/kg/day in rats and 0.01 mg/kg/day in rabbits. Halobetasol propionate was embryotoxic in rabbits but not in rats. Cleft palate was observed in both rats and rabbits. Omphalocele was seen in rats but not in rabbits.
Lactation
Risk SummaryThere are no data on the presence of halobetasol propionate or its metabolites in human milk, the effects on the breastfed infant, or the effects on milk production after treatment with BRYHALI.
Systemically administered corticosteroids appear in human milk and could suppress growth, interfere with endogenous corticosteroid production, or cause other untoward effects. It is not known whether topical administration of corticosteroids could result in sufficient systemic absorption to produce detectable quantities in human milk.
The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for BRYHALI and any potential adverse effects on the breastfed child from BRYHALI.
Clinical ConsiderationsAdvise breastfeeding women not to apply BRYHALI directly to the nipple and areola to avoid direct infant exposure.
Pediatric UseSafety and effectiveness of BRYHALI in pediatric patients under the age of 18 years have not been evaluated.
Because of higher skin surface area to body mass ratios, pediatric patients are at a greater risk than adults of HPA axis suppression and Cushing’s syndrome when they are treated with topical corticosteroids. They are therefore also at greater risk of adrenal insufficiency during or after withdrawal of treatment. Adverse reactions including striae have been reported with use of topical corticosteroids in infants and children [see Warnings and Precautions].
HPA axis suppression, Cushing’s syndrome, linear growth retardation, delayed weight gain, and intracranial hypertension have been reported in children receiving topical corticosteroids. Manifestations of adrenal suppression in children include low plasma cortisol levels and an absence of response to ACTH stimulation. Manifestations of intracranial hypertension include bulging fontanelles, headaches, and bilateral papilledema [see Warnings and Precautions].
Geriatric UseOf 284 subjects exposed to BRYHALI in clinical trials, 61 subjects were 65 years or older. Clinical trials of BRYHALI did not include sufficient numbers of subjects age 65 years and older to determine whether they respond differently from younger subjects.
NONCLINICAL TOXICOLOGYCarcinogenesis, Mutagenesis, Impairment of FertilityLong-term animal studies have not been performed to evaluate the carcinogenic potential of halobetasol propionate.
Halobetasol propionate was not genotoxic in the Ames assay, in the sister chromatid exchange test in Chinese hamster somatic cells, in chromosome aberration studies of germinal and somatic cells of rodents, or in a mammalian spot test. Positive mutagenicity effects were observed in a mouse lymphoma gene mutation assay in vitro and in a Chinese hamster micronucleus test.
Studies in rats following oral administration of halobetasol propionate at dose levels up to 0.05 mg/kg/day indicated no impairment of fertility or general reproductive performance.
PATIENT COUNSELING INFORMATIONAdvise the patient to read the FDA-approved patient labeling (Patient Information).
Manufactured for:Dow Pharmaceutical Sciences, a division of Valeant Pharmaceuticals North America LLC Bridgewater, NJ 08807 USA
By:Valeant Pharmaceuticals International, Inc. Laval, Quebec H7L 4A8, Canada U.S. Patent Numbers: 6,517,847 and 8,809,307BRYHALI is a trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.© 2018 Valeant Pharmaceuticals North America LLCBased on 9652102 November 2018 BRY.0032.USA.18

www.dermatologyfoundation.org Winter/Spring 2019 13
ALABAMA
Porcia Love, MD
Stephen E. Mason, MD
ARIZONA
Gary A. McCracken, MD
CALIFORNIA
Elizabeth E. Bailey, MD
Tina Bhutani, MD
Kerry L. Blacker, MD
Diana Camarillo, MD
Aileen Chang, MD
Yiyin E. Chen, MD, PhD
Bryan L. Gammon, MD
Ruby Ghadially, MD
Eleni Linos, MD, MPH, DrPH
Haley B. Naik, MD
Bahram Razani, MD, PhD
Sonal D. Shah, MD
Vernon R. Wilson, MD
COLORADO
Sylvia L. Brice, MD
CONNECTICUT
Marcus McFerren, MD, PhD
Caroline Nelson, MD
DISTRICT OF COLUMBIA
Ginette Hinds Okoye, MD
FLORIDA
Debra L. Bailey, MD
GEORGIA
Ross Campbell, MD Julia G. Girard, MD
ILLINOIS
Judith P. Knox, MD David A. Lorber, MD A. David Soleymani, MD
KANSAS
Cameron West, MD
LOUISIANA
Elizabeth Foley Bucher, MD Sarah E. Glorioso, MD Christel C. Malinski, MD Skylar Souyoul, MD Diane Trieu, MD
MAINE
Joshua D. Sparling, MD
MARYLAND
Lloyd S. Miller, MD, PhD Charlotte E. Modly, MD Rachel A. Schleichert, MD
MASSACHUSETTS
Kathryn E. Bowers, MD Anne-Sophie J. Gadenne, MD JiaDe Yu, MD
MICHIGAN
Christopher K. Bichakjian, MD Johann E. Gudjonsson, MD, PhD Christopher Schwimer, DO
MINNESOTA
Sarah S. Asch, MD
Lawrence E. Gibson, MD Kathleen J. Hectorne, MD Carilyn N. Wieland, MD
MISSOURI
Brian S. Kim, MD
NEBRASKA
Mary T. Finnegan, MD
NEW JERSEY
Lian-Jei Li, MD Marc Meulener, MD
NEW YORK
Randie Hee Kim, MD
NORTH CAROLINA
Adewole S. Adamson, MD
Dori Lee Hunt, MD Phillip M. Williford, MD
OHIO
John Ray Bernat, MD Conley W. Engstrom, MD Bruce P. Guido, MD Joyce A. Lender, MD Kirsten T. Lynch, MD John George Secrist, MD Harry L. Winfield, MD
OKLAHOMA
Christina G. Kendrick, MD
PENNSYLVANIA Daniel H. Kaplan, MD, PhD Joy H. Kunishige, MD Megan H. Noe, MD, MPH Steven A. Oberlender, MD, PhD Jennifer Sceppa, MD
SOUTH CAROLINA Dirk M. Elston, MD
SOUTH DAKOTA Mandi J. Greenway, MD
TENNESSEE Jami L. Miller, MD
TEXAS Benjamin F. Chong, MD, MSCS Melissa Mauskar, MD Nicole Owens, MD Susana C. Poliak, MD Christy Riddle, MD
UTAH Stephanie Z. Klein, MD Lindsay H. Wilson, MD
VIRGINIA Nicole Hayre, MD Katie Mercy, MD
WISCONSIN Pamela J. Butler, MD Melanie A. Clark, MD David L. Crosby, MD Abigail L. Taub, MD Kara Walton, MD
WYOMING Amber Robbins, MD
New Leaders Society Members Invest in Progress The DF Board of Trustees is pleased to recognize the Leaders Society members who joined their colleagues in 2018 to invest $1,500 annually to further the advancement of knowledge and patient care in dermatology. The Foundation appreciates their confidence in its ability to identify and support the research that will drive this progress for years to come.
Italics = Young Leader (5 years or less out of residency)
Jacqueline M. Junkins-Hopkins, MD

14 Winter/Spring 2019 Dermatology Foundation
which is known to provide cellular protec-tion against oxidative stress.
Tiron completely abrogated mito-chondrial and nuclear DNA damage in human skin cells exposed to these stres-sors. “We postulated that these profound in vitro antioxidant effects are attributable to the combination of its antioxidant and metal-chelating properties,” Birch-Machin explains. “It targets not just the ROS, but also the increased free intracellular metals that are released due to oxidative insults.” This points to the ideal therapeutic strategy of combining compounds with comple-mentary capabilities.
Conclusions It had first been speculated in the early
1970s that mitochondria play a key role in the aging process. Birch-Machin’s research in the skin “brings us one step closer to understanding how mitochondria may be contributing to this, with the hope of even-tually targeting areas of the mitochondria in an attempt to counteract the signs of aging,” he states. This includes his search for a way to maintain ideal levels of complex II as an endogenous ROS suppressor, and his con-tinuing work using Tiron as a preventive.
He is also expanding his pursuit of mtDNA involvement in skin health and disease. He is looking at mtDNA in the context of treating psoriasis, in the rela-
tionship between oxidative stress, nutritional status, and skin aging, and in the science and use of sunscreens.
Birch-Machin, though, is not mitochondria-centric. “The fascination and beauty for me,” he explains, “is the way the two genomes communicate and affect each other. Those who focus on just one of them and ignore the other—it’s at their peril,” he adds. “Our perspective should be a healthy balance between the two, as they are equally important.”
Suggested Readings Oyewole AO, Wilmot M-C, Fowler M, Birch-Machin MA.
“Comparing the effects of mitochondrial targeted and localized antioxidants with cellular antioxidants in human skin cells ex-posed to UVA and hydrogen peroxide.” FASEB J. 2014;28:485–94.
Bowman A, Birch-Machin MA. “Age-dependent decrease of mitochondrial complex II activity in human skin fibroblasts.” J Invest Dermatol. 2016;136:912–19.
Tulah AS, Birch-Machin MA. “Stressed out mitochondria: The role of mitochondria in ageing and cancer focusing on strategies and opportunities in human skin.” Mitochondrion. 2013;13:444–53.
Birch-Machin MS, Bowman A. “Oxidative stress and ageing.” Br J Dermatol. 2016;175(Suppl S2):26–9. ■
Annenberg Circle Welcomes Newest Members
The DF Board of Trustees is deeply grateful to the newest AC members. They each pledged $25,000 in 2018
to meet the critical need for supporting the research advances that are the platform for furthering patient care.
They join more than 600 colleagues in making this invaluable investment in the specialty’s future.
Fuad Abuabara, MD
Jonathan Bass, MD
Doris J. Day, MD
Matthew C. Fox, MD
Allan C. Harrington, MD
Michelle L. Juneau, MD
Mario E. Lacouture, MD
Rosemarie Liu, MD
Kiran Motaparthi, MD
Chad L. Prather, MD
Curt P. Samlaska, MD
John T. Seykora, MD, PhD
Michael J. Sharkey, MD
Jerald L. Sklar, MD
Cynthia R. Strohmeyer, MD
J. Scott VanLoock, MD
Special Gifts for Advancing Patient Care
Tribute and Honoraria contributions are an
effective, but often overlooked, way to support
research through the Dermatology Foundation
and enable the expansion of knowledge that is
the foundation of improvements in clinical care.
Tribute Contributions: A meaningful way to
increase the DF’s capacity for funding deserving
research projects is by memorializing or honoring
someone important to you—a family member,
special friend, or mentor.
Honoraria: A unique way to make your
member contribution this year is by arranging
to have your honoraria paid directly to the DF.
All such contributions to the DF are deeply
appreciated, and help maintain the momentum
of research and clinical progress in dermatology.
For more information on contributing gifts of this
kind, please call the DF office at 847.328.2256.
Coming in the Next Issue
• Highlights of the recent DF Annual Meeting
• Proceedings—Part I: summarizing the 2019 Clinical Symposia

www.dermatologyfoundation.org Winter/Spring 2019 15
2018 Corporate Honor Society Partners in Shaping Dermatology’s Future
The Dermatology Foundation is grateful to the following corporations for their generous contributions last year. Their support furthers the DF’s ability
to fund innovative research that shapes the future of dermatology.
Platinum Benefactors ($200,000 or more)
Gold Benefactor ($100,000 or more)
AbbVie
Silver Benefactors ($50,000 or more)
Lilly USA, LLC Janssen Novartis

Dermatology Focus c/o Dermatology Foundation 1560 Sherman Avenue, Suite 500 Evanston, Illinois 60201-4806
Non-Profit
U.S. Postage
PAID
Permit No. 236
Melrose Park, IL
VOL. 37 NO. 4 WINTER/SPRING 2019
A DERMATOLOGY FOUNDATION PUBLICATIONSPONSORED BY ORTHO DERMATOLOGICS
The DF Welcomes New President: Janet A. Fairley, MD
The Dermatology Foundation
is pleased to announce the Board
of Trustee’s election of Janet A.
Fairley, MD, to serve as its new
president. Dr. Fairley has been
a member of the DF for over 30
years, and an active volunteer
for nearly as many. She has con-
tributed her outstanding leadership
and perspective to a variety of
DF fundraising, research award,
and educational programs, including
co-chairing the annual DF Clinical
Symposia.
Dr. Fairley has been the John S. Strauss
Professor and Chair of the Department of
Dermatology at the University of
Iowa since 2007. She is also a
physician-scientist whose research
activities have focused on the
autoimmune blistering diseases.
One of her major goals has always
been to translate findings from the
laboratory into improved diagnostics
and/or therapies for patients.
Chairman Bruce U. Wintroub, MD,
warmly welcomed Dr. Fairley to
her new role. He added his sincere
thanks to outgoing president Kim B.
Yancey, MD, for his strong leadership as he
completed his term at the Annual Meeting of
Membership in Washington, DC.

![Mitochondrial DNA damage and atherosclerosis · 82 atherosclerosis development [12, 13] ... 164 dysfunctional mitochondria cardiolipin localises to the outer mitochondrial membrane,](https://img.pdfslide.us/doc/110x75/5fc3069c0498e3155071622c/mitochondrial-dna-damage-and-atherosclerosis-82-atherosclerosis-development-12.jpg)