Embed Size (px)
Citation preview

Central JSM Neurosurgery and Spine
Cite this article: Faried A, Hidayat I, Yudoyono F, Dahlan RH, Arifin MZ (2015) Spondylitis Tuberculosis in Neurosurgery Department Bandung Indonesia. JSM Neurosurg Spine 3(3): 1059.
*Corresponding authorAhmad Faried, Department of Neurosurgery, Faculty of Medicine, Universitas Padjadjaran–Dr. Hasan Sadikin Hospital, Jl. Pasteur No. 38, Bandung 40161, West Java,
Submitted: 11 April 2015
Accepted: 13 July 2015
Published: 14 July 2015
Copyright© 2015 Faried et al.
OPEN ACCESS
Keywords•Spondylitis tuberculosis•Weakness of lower extremity•Neurosurgery
Research Article
Spondylitis Tuberculosis in Neurosurgery Department Bandung IndonesiaAhmad Faried1*, Imam Hidayat2, Farid Yudoyono1, Rully Hanafi Dahlan1 and Muhammad Zafrullah Arifin1
1Department of Neurosurgery, Universitas Padjadjaran–Dr. Hasan Sadikin Hospital, Indonesia2Department of Neurosurgery, Universitas Syiah Kuala-Dr. Zainal Abidin Hospital, Indonesia
Abstract
Spondylitis TB is an infection of Mycobacterium TB involving the spine. The course of spondylitis TB is relatively indolent (without pain), thus early diagnosis is challenging. This study was conducted to evaluate the clinical presentation and the goal of surgery in twelve patients who had been operated for spondylitis tuberculosis (TB) in the Department of Neurosurgery, Faculty of Medicine, Universitas Padjadjaran–Dr. Hasan Sadikin Hospital, Bandung, Indonesia between May 2012–2013 were reviewed retrospectively. This study analized the medical records of patients operated in our center. A clinical examination, spinal X-Ray, computed tomography scans were obtained before and after the operation is examined. Final diagnosis was based on histological characteristics and polymerase chain reaction (PCR) result of the Mycobacterium TB bacteria. The chief complaint of spondylitis TB patients admitted or consulted to our center is lower limb weakness. There were 12 cases of spondylitis TB (5 women and 7 men with a ratio of 1: 1.4). The average age was 34.3 (the youngest patient was 17 years old and the oldest was 56 years) with a standard deviation ± 9.9. The infected spines are: one patient in the cervical, eight patients in thoracal and three patients in lumbar. The chief complaint of spondylitis TB patients admitted or consulted is lower limb weakness (83.3%). Gibbus is observed in 83.3% of patients. Anterior cervical discectomy and fusion was performed in 1 case and posterior was used in 11 cases. A comprehensive history taking, along with correct sampling using various imaging modalities and PCR, will certainly lead to the diagnosis of spondylitis TB. It must be noted that neurological deficit due to spinal tuberculosis is reversible in majority of cases, especially if decompression is achieved promptly.
INTRODUCTIONSpinal tuberculosis infection, or commonly referred as
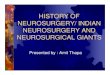
spondylitis tuberculosis (TB) or vertebral osteomyelitis tuberculosis or Pott’s disease [1], caused by the Mycobacterium tuberculosis bacteria that attacks the corpus vertebrae, potentially causing serious morbidity, including neurological deficits and permanent spine deformity. The most common deformity is kyphotic deformity, known as the gibbus. The diagnosis is usually established at advanced stage, where severe spinal deformity and neurological deficits such as paraplegia are evident [2,3].
Indonesia is ranked after India and China as country with most population infected by TB [4]. Approximately 20% of pulmonary TB infection will spread outside the lung (extrapulmonary TB) [5]. Eleven percent of extrapulmonary TB is osteoarticular TB, and approximately half of the patients have spinal TB infection
[6]. The management of spondylitis TB in general includes anti-TB drugs, immobilization with or without surgical intervention.
This study was conducted in order to evaluate the clinical presentation and the goal of surgery in 12 cases of patients with spondylitis TB treated in the Department of Neurosurgery, Faculty of Medicine, Universitas Padjadjaran (FK UNPAD)–Dr. Hasan Sadikin, Hospital (RSHS), Bandung from 2012-2013.
METHODSThis research was a retrospective cohort study examining
the medical records of spondylitis TB patients operated in the Department of Neurosurgery, FK UNPAD–RSHS in May 2012–May 2013. A clinical examination, spinal X-Ray, and computed tomography (CT) scans were obtained before and after the operation is performed (Figure 1). Final diagnosis was achieved based on histological characteristics and outcome of polymerase

Central
Faried et al. (2015)Email:
JSM Neurosurg Spine 3(3): 1059 (2015) 2/4
chain reaction (PCR) of the Mycobacterium Tuberculosis bacteria.
SURGICAL CONSIDERATIONSIndications for surgery in acute spondylitis TB [7,8].
1. Progressive neurologic deficit.
2. Progressive increase of spinal deformity (more than ±40⁰ of segmental kyphosis, anteroposterior or lateral translation).
3. Conservative treatments futile including point 1 and 2 above.
4. Severe pain due to abscess or spinal instability.
5. Uncertain diagnosis: this could be an inability to obtain microbiological diagnosis from microscopy, culture or even via detection of mycobacterium DNA using PCR.
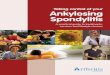
Patients were operated in prone position under general anesthesia. Septic and aseptic and draping was performed, the operation site marking was then infiltrated with 10 ml of 1% xylocaine with adrenaline to minimize bleeding. A posterior midline approach was commonly used. The dissection was carried out in the subperiosteal plane to allow decent bony part identification. In the patient with cold abscess (Figure 2), the posterolateral extra pleural (costotransversectomy) approach was used to decompress the cord and remove necrotic materials within the body and disc using curettes, and paraspinal abscess was drained. The spine was stabilized using transpedicular screw and rod system (Figure 3), the wound was closed layer by layer after securing haemostasis without a drain. Surrounding muscles were injected with 20 mg of bupivacaine to reduce post-operative pain and muscle spasm. Anterior surgery (anterior cervical discectomy and fusion; ACDF) was performed in one case (Table 1).
RESULTSThere were 12 cases of spondylitis TB in this study (five
women and seven men with a ratio of 1: 1.4). The average age of the patients was 34.3 (the youngest patient was 17 years old and the oldest was 56 years) with a standard deviation (SD) ± 9.9.
Figure 1 Clinical picture that showing gibbus. Posterior deformity of the spine is shown in response to vertebral kypothic angulation.
Figure 2 T1-weighted and T2-weighted sagittal MRI images of thoracic spine showing destruction due to spinal TB of thoracal 7-8 (T7-T8) with some preservation of the disc (A and B). T2-weighted axial and coronal MRI of same patient showing paravertebral abcess (C and D).
Figure 3 Intra-operative photograph of bilateral partial laminectomy (A). Abcess lesion following debridement (B).
The infected spine are: one patient in the cervical, eight patients in thoracal and three patients in lumbar. The chief complaint of spondylitis TB patients admitted or consulted is lower limb weakness (83.3%). Gibbus is observed in 83.3% of patients. ACDF was performed in 1 case and posterior was used in 11 cases (Table 1). Diagnosis is based on histological characteristic (hematoxylin and eosin staining) and laboratory tests using PCR; the DNA samples were amplified using primers IS6110 with product result 123 base pairs (bp). Forward and reverse primer IS6110 consists of:
IS6110 forward: (5’ – CCT GCG AGC GTA GGC GTC GG– 3’)

Central
Faried et al. (2015)Email:
JSM Neurosurg Spine 3(3): 1059 (2015) 3/4
IS6110 reverse : (5’ – CTC GTC CAG CGC CGC TTC GG – 3’)
PCR is highly accurate with a sensitivity of 80-98%, a specificity of 98% [9] and rapid scan times (> 24 hours).
DISCUSSIONWorld Health Organization (WHO) has set TB as world
emergency issues. WHO estimates that there are approximately eight million new cases annually and two million deaths each year. If the problem is not managed, WHO predicts that there will be approximately 200 million people infected by TB and 35 million deaths may be encountered in 2000 to 2020 [4].
Recently, Murdaca and colleagues emerged a very serious issue that tell us how the administration of pro-infammatory cytokine inhibitor, such as tumor necriting factor (TNF)-alpha inhibitor, for chronic immune-mediated diseases appears to be responsible (adverse event) for re-activation of latent-
tuberculosis (LTB) and the overall risk of opportunistic infections [10]. Murdaca and colleagues suggested that the clinician must have patient’s medical history, Mantoux test and chest x-ray should always be done before TNFalpha inhibitor consider to be given to the patient with chronic immune-mediated diseases [10]. In Indonesia, TNFalpha inhibitor for chronic immune-mediated diseases (such as rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, and other inflammatory arthritis) is not our national protocol and will not covered by our national insurance; therefore no LTB associated with TNFalpha inhibitor therapy reported in our country. The message that they want to underline is that, the clinician should be aware of TB in subjects undergoing TNFalpha inhibitor therapy, especially in countries with a high prevalence of TB, such us in Indonesia.
Clinical manifestations of spondylitis TB are relatively indolent (without the pain) [9]. The patients usually complaint unspecific local pain in the infected area of the vertebra. Infection begins in the subchondral epiphyseal vertebral area then extends to the bone ossification center that may devitalized the bone due to TB bacilli exotoxin that may cause loss of extracellular matrix also spread locally to the subligament longitudinal area. TB germ induce inflammatory reaction and the formation of granulation tissue. This granulation will start damaging and erodes the cartilage and even bone tissue resulting in demineralization and then spread to the disc that has a poor blood supply. This process may lead to deformity known kyphotic gibbus (83.3% patients are presented with gibbus in this study).
Spondylitis TB is most commonly located in thoracal areas, as many as 71% [11]; 66.7% in this study. The main artery that affects the spinal cord in thoracal segments is most frequently located in the left vertebrae thorakal 8 to lumbar 3. Thrombosis of this artery may cause paraplegia. Another factor to be taken into account is the relatively large diameter of the spinal canal compared with vertebral canal. Lumbar vertebrae intumesensia begin to widen as high as ± vertebrae thoracal 10, where vertebral canal in the area is relatively small. As vertebral canal in the first lumbar vertebra is large, it provides more space to move when there is compression on the anterior part. This may explain why paraplegia is common in vertebral thoracal lesions.
Gulhane Askeri Tip Academics (GATA) classification determines the best therapy for the patient. This classification system is based on clinical and radiological criteria, including: abscess formation, disc degeneration, vertebral collapse, kyphosis, sagittal angulation, vertebral instability and neurological symptoms; spondylitis TB is divided into three types (GATA I, II, and III) [12]. Surgical intervention is performed on patients with GATA IB-III. Meanwhile, the only contraindication of surgery is heart and lung failure.
The management of spondylitis TB aims to: (i) eradicate TB germs using anti-TB drugs, (ii) Improve the patient’s general condition, (iii) prevent or correct deformity, using decompression and stabilization, (iv) Prevent or treat complications such as neurological deficit such as paraplegi [13]. Treatment of spondylitis TB is generally divided into two parts that can be initiated concurrently, medical and surgical. Medical treatment is fundamental, whereas surgery and complementary medical therapy varies among patients [14]. Although medical treatment
Figure 4 The final histopathological finding revealed TB infection that shown as the accumulation of the epitheloid granulomas, datia langhans cells, and caseous necrosis (magnifition 50x).
Figure 5 Polychain reaction (PCR) results. The IS6110 primers amplify a fragment of MTB with a length of 123 base pair (bp).

Central
Faried et al. (2015)Email:
JSM Neurosurg Spine 3(3): 1059 (2015) 4/4
Faried A, Hidayat I, Yudoyono F, Dahlan RH, Arifin MZ (2015) Spondylitis Tuberculosis in Neurosurgery Department Bandung Indonesia. JSM Neurosurg Spine 3(3): 1059.
Cite this article
is the core therapy in the management of spondylitis TB patients, surgery play an important role in spondylitis TB cases with cold abscess, tuberculosis lesions, paraplegia, kyphosis progressive or bone or disc herniation in the neural canal. In this study, surgical therapy was performed in 83.3% of patients with cold abscess.
There are several surgical approaches; including (a) Anterior approach where abscess can be evacuated, necrotic substances can be disposed, anterior decompression of the spinal cord can be achieved. Tissue for histopathological examination and culture may be obtained easily and kyphosis can be corrected or stabilized with autogenous bone graft, (b) Posterior approach; indicated in cases where posterior elements are involved and posterior stabilization is needed before anterior decompression and arthrodesis, as well as in patients with stable or minimal spinal deformity with intramedullary tuberculoma or epidural abscess present. In this study, surgery was conducted, using posterior approach, due to progressive neurologic deficits and the progressive increase of spinal deformity (91.7%).
CONCLUSIONA comprehensive history taking, along with correct sampling
using various imaging modalities and PCR, will certainly lead to the diagnosis of spondylitis TB. It must be noted that neurological deficit due to spinal tuberculosis is reversible in majority of cases, especially if decompression is achieved promptly. Appropriate fusion and stabilization may prevent pain and late deformity.
CONSENTInformed consent was obtained from each patient on May
2012–2013 for publication of this study and any accompaning images
AUTHORS’ CONTRIBUTIONSAF, IH, FY, RHD and MZA had examined, treated, observed,
and followed up the subject of this research. AF, FY and RHD performed all the operation on the patient. All authors participated in writing the manuscript. All authors has read and approved of the final manuscript.
ACKNOWLEDGEMENTThe authors would like to thank to Agung B. Sutiono from
Department of Neurosurgery, Faculty of Medicine, Universitas Padjadjaran-Dr. Hasan Sadikin Hospital, Bandung, for fruitful of discussions.
REFERENCES1. Sai Kiran NA, Vaishya S, Kale SS, Sharma BS, Mahapatra AK. Surgical
results in patients with tuberculosis of the spine and severe lower-extremity motor deficits: a retrospective study of 48 patients. J Neurosurg Spine. 2007; 6: 320-326.
2. Cormican L, Hammal R, Messenger J, Milburn HJ. Current difficulties in the diagnosis and management of spinal tuberculosis. Postgrad Med J. 2006; 82: 46-51.
3. Sinan T, Al-Khawari H, Ismail M, Ben-Nakhi A, Sheikh M. Spinal tuberculosis: CT and MRI feature. Ann Saudi Med. 2004; 24: 437-441.
4. WHO. Global tuberculosis control-epidemiology, strategy, financing.
5. Agarwal P, Rathi P, Verma R, Pradhan CG. Tuberculous spondilitis: `Global lesion’. Special issues on Tuberculosis. Bombay Hospital Journal. 1999.
6. Leibert E, Haralambou G. Tuberculosis. In: Rom WN and Garay S, eds. Spinal tuberculosis. Lippincott, Williams and Wilkins. 2004: 565–577.
7. Mak KC, Cheung KM. Surgical treatment of acute TB spondylitis: indications and outcomes. Eur Spine J. 2013; 22: 603-611.
8. Bhavuk Garg, Pankaj Kandwal, Upendra Bidre Nagaraja, Ankur Goswami, Arvind Jayaswal. Anterior versus posterior procedure for surgical treatment of thoracolumbar tuberculosis: A retrospective analysis. Indian J Orthop. 2012; 46: 165–170.
9. Agrawal V, Patgaonkar PR, Nagariya SP. Tuberculosis of spine. J Craniovertebr Junction Spine. 2010; 1: 74-85.
10. Murdaca G, Spanò F, Contatore M, Guastalla A, Penza E, Magnani O, et al. Infection risk associated with anti-TNF-α agents: a review. Expert Opin Drug Saf. 2015; 14: 571-582.
11. Albar Z. Medical treatment of Spinal Tuberculosis. Cermin Dunia Kedokteran. 2002; 137: 29.
12. Oguz E, Sehirlioglu A, Altinmakas M, Ozturk C, Komurcu M, Solakoglu C, et al. A new classification and guide for surgical treatment of spinal tuberculosis. International Orthopaedics (SICOT). 2008; 32: 127–133.
13. Infectious and noninfectious inflammatory disease affecting the spine. In: Byrne TN, Benzel EC, Waxman SG (eds). Disease of the Spine and Spinal Cord. Oxford University Press. 2000: 325–335.
14. Nataprawira HM, Rahim AH, Dewi MM, Ismail Y. Comparative between operative and conservative therapy in spondylitis tuberculosis in Hasan Sadikin Hospital, Bandung. Majalah Kedokteran Indonesia 2010; 60: 318–332.
![Ankylosing spondylitis and related conditions - NHS Wales1].pdf · Condition Ankylosing spondylitis Ankylosing spondylitis and related conditions This booklet provides information](https://img.pdfslide.us/doc/110x75/5d53eb2788c993a4728b841d/ankylosing-spondylitis-and-related-conditions-nhs-1pdf-condition-ankylosing.jpg)