Embed Size (px)
Citation preview
Spiritual Care to the Veteran
Expanding CompetencyBrynn White, MDiv, BCC
Coatesville VA
Jennifer Wortmann, PhD
Mental Health and Chaplaincy
VA Mid-Atlantic MIRECC
Introductions and brief poll:
● How many veterans in the room?
● How many VA or Military chaplains in the room?
● How many of you regularly work with veterans? How frequently?
● What is your current knowledge of military and veteran culture? [(1)
Very little; (2) Some; (3) Very much]
● How comfortable do you feel tending to the spiritual wounds of
war? [(1) Uncomfortable; (2) Somewhat Comfortable; (3) Comfortable]
Demographics: Theaters of War
Citation: http://www.defenselink.mil/news/casualty/pdf
● “Global War on Terror(ism)” (GWOT):
○ OEF...KIA: 2,216 (Afghanistan) KIA: 131 (other location);
WIA: 20,057 (Afghanistan); WIA: 39 (other location)
○ OIF...KIA: 4,410; WIA: 31,957
○ OND...KIA: 73; WIA: 295
● Gulf Wars (Desert Storm and Desert Shield: 1990-1991)
● Vietnam
● Korean
● World Wars
Demographics: ● ~ 1.3 million active duty; ~ 800,000 reservists currently serving
● Currently about 19 million veterans in the US
● 50 percent served by VHA● https://www.va.gov/COMMUNITYCARE/docs/pubfiles/factsheets/VHA-FS_MISSION-Act.pdf
● How to become a provider: https://www.va.gov/communitycare/providers/resources.asp
● Specifics:
○ ~ 17 million Male service members
○ > 500,000 Female service members (up from 159,810 in
2001)
○ ~ 2 million Female veterans
○ > 1 million LGBTQ veterans
Demographics: by groups
● Total population of veterans is predicted (based on
data) to decline from about 20 to 13.6 million by 2037
● As of 2017, largest veteran cohort is the Gulf War
veteran group at 7.2 million (Vietnam 6.6 million)
● About 1.2 OEF/OIF/OND veterans access care through
VHA (about 2.0 million OEF/OIF/OND veterans total)
https://www.va.gov/vetdata/docs/Demographics/New_Vetpop_Model/Vetpop_Infographic_Final31.pdf
https://www.publichealth.va.gov/docs/epidemiology/healthcare-utilization-report-fy2015-qtr3.pdf#
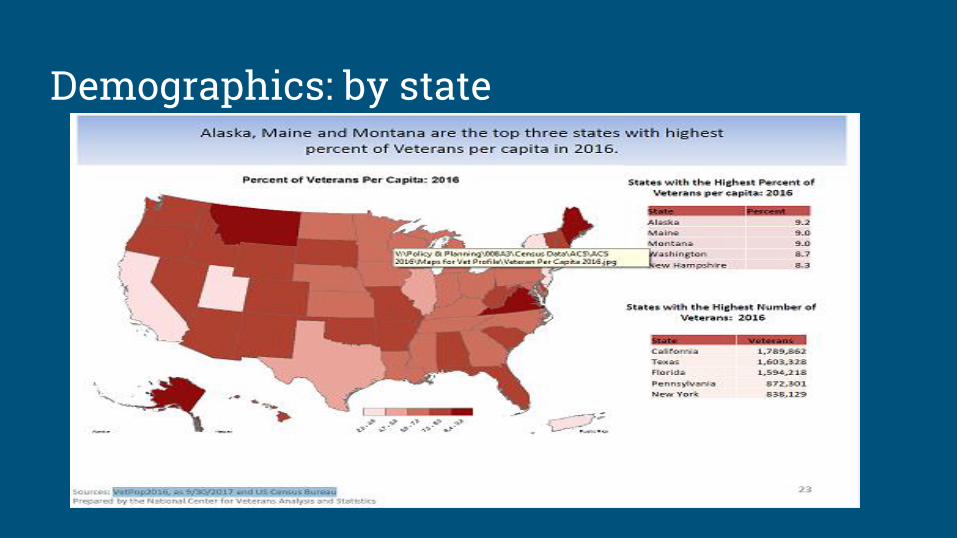
Demographics: by state
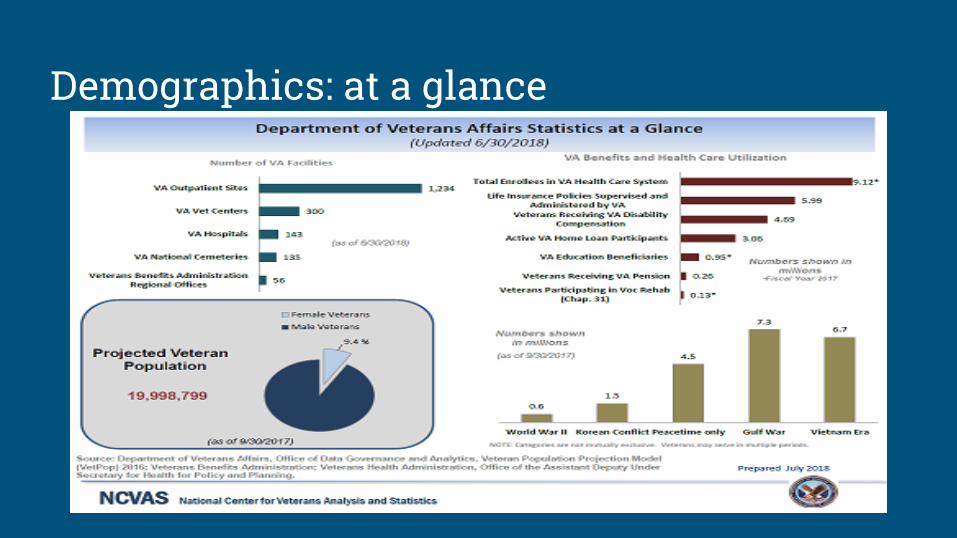
Demographics: at a glance
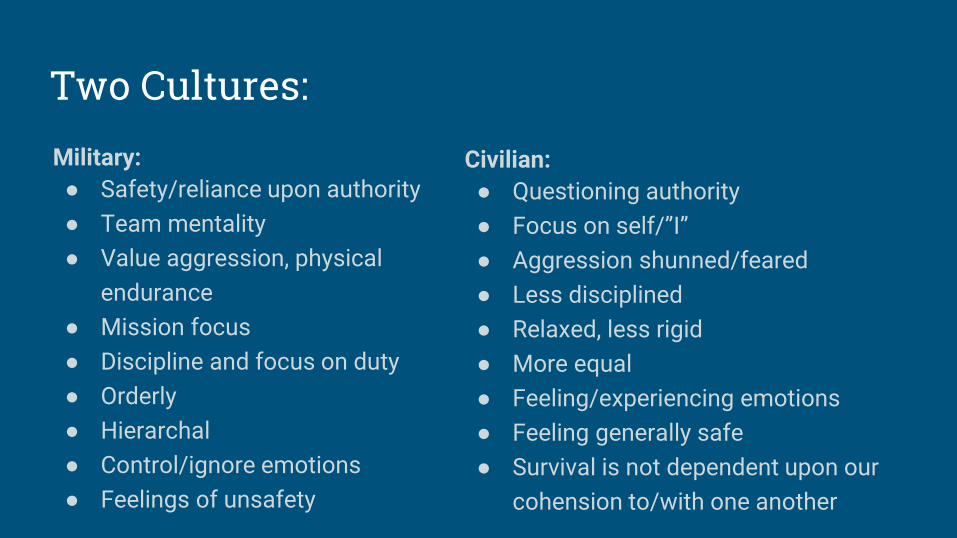
Two Cultures:Military:
● Safety/reliance upon authority
● Team mentality
● Value aggression, physical
endurance
● Mission focus
● Discipline and focus on duty
● Orderly
● Hierarchal
● Control/ignore emotions
● Feelings of unsafety
Civilian:
● Questioning authority
● Focus on self/”I”
● Aggression shunned/feared
● Less disciplined
● Relaxed, less rigid
● More equal
● Feeling/experiencing emotions
● Feeling generally safe
● Survival is not dependent upon our
cohension to/with one another
Two Cultures:
● These were highly trained men and women who carried enormous responsibilities while serving (experienced great worth/value);
● Most elite-trained force in the world;● Had a great sense of purpose and mission while
serving;● Knew their role and where they fit and what was
expected of them;● Sense of commitment and great discipline
Two Cultures: Re-integration
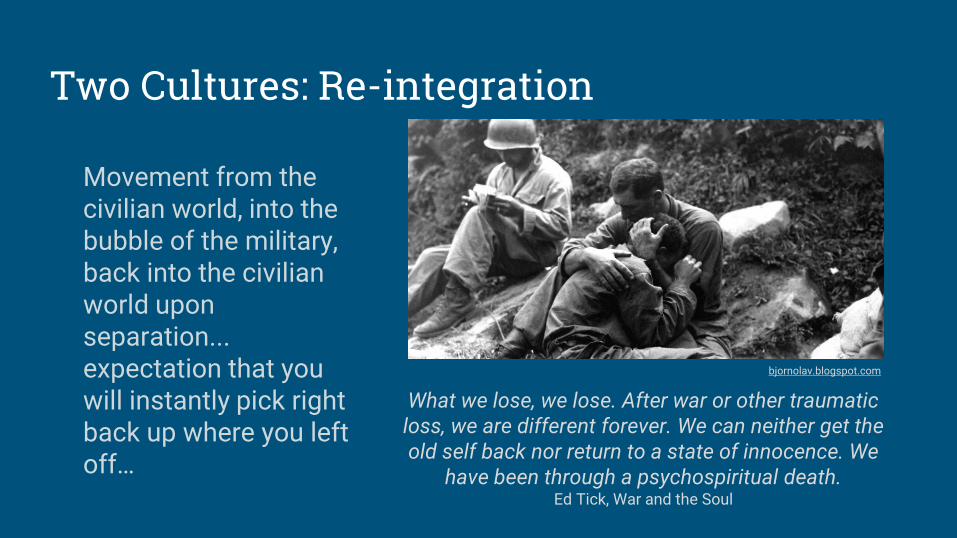
Movement from the civilian world, into the bubble of the military, back into the civilian world upon separation...expectation that you will instantly pick right back up where you left off…
What we lose, we lose. After war or other traumatic loss, we are different forever. We can neither get the old self back nor return to a state of innocence. We
have been through a psychospiritual death.Ed Tick, War and the Soul
bjornolav.blogspot.com
Separating and Integrating challenges:● Returning home becomes disorienting, i.e. new routine, loss of schedule/discipline,
fitting in, issues that now must be faced (trauma, isolation, others not understanding, etc)
● Person will not be the same as they were when they first enlisted● Whether in combat or not, likely to endure higher levels of stress and vigilance ● Existential questions arise around meaning, purpose, identity, theodicy, often without
a safe space in which to articulate or explore these issues● Identity formation (“Who am I now?” becomes vexing after separating)● Great many who dreamed of becoming “lifers” (What about the future
now?=grief/loss)● Many important skills necessary for survival in combat do not compute in civilian life,
(i.e., being a tank driver, weapons specialist, counter IED, prison interrogator, etc. →“Now I’m stocking shelves in the grocery store”)
Trauma: Non-Combat and Combat
Non-Combat:
● Just because one doesn’t see
combat doesn’t mean there is not
trauma
● Trauma during boot camp—
emotional, physical, sexual
● Many separate from service
stateside after experiencing trauma
Combat:
● Face-to-face combat
● Operating drones, radio, etc.
● Retrieving blown up equipment
● Handling and “bagging” human remains
● Seeing dead bodies/comrades blown
up or killed
● Killing civilian operatives (women,
children) or innocent bystanders
*Types of exposure to trauma determines risk of mental health challenges after separation*
Trauma: TBI, MI, PTSD, MST● Traumatic Brain Injury (TBI)● Moral Injury (MI)● Post Traumatic Stress Disorder
(PTSD)● Military Sexual Trauma (MST)
○ Happens to both men and women service members
○ 1 in 4 women report at least one incidence of MST
○ 1 in 100 men report at least one incidence of MST
○ Not uncommon to hear an MST survivor was also a survivor of childhood sexual abuse
○ Hotline for women survivors: 1-855-VA-WOMEN
livescience.com
Trauma: SuicideSuicide is a national health concern that affects all Americans
https://www.mentalhealth.va.gov/suicide_prevention/What to look for: ● Loss of interest● Hoarding medicine/buying a gun● Feeling like a burden● Withdrawal from family and friends● Feeling humiliated● “I just wish I were dead”● Hopelessness/loss of reasons to live
○ More suicide-related resources will be provided today○ VETERANS CRISIS LINE: 1-800-273-8255, press 1
Trauma: Suicide
Trauma: Homelessness, MH, and SUD
● 1 in 10 homeless adults are veterans
○ 1 in 5 homeless men
● 68% reside in principal cities
○ 32% reside in suburban/rural areas
● Needs:
○ Half have disabilities or serious mental illness (SMI)
○ 70% have substance abuse problems
National Coalition of Homeless Veterans
Trauma: Impacts on spirituality
● Weakened faith, less comfort(Currier, Drescher, & Harris, 2014; Fontana & Rosenheck, 2004)
● Religion doesn’t mean as much to me as it did when I went in
● Life means nothing; life is cheap
(Flipse Vargas et al., 2013)
● Fewer spiritual experiences, more problems with forgiveness
(Currier, Drescher, & Harris, 2014)
Trauma: Spiritual coping (“negative”)
● Distress, Struggle● Feel that God has let you down
● View God as unkind
● Feel abandoned by God
(Exline et al., 2014; Wood et al., 2010)
● Felt punished by God …
● Questioned the power of God
(Pargament et al., 2000)
● Associated with poorer mental health in veterans
(Aflakseir & Coleman, 2009; Currier, Drescher, & Harris, 2014; Witvliet et al., 2004)
Trauma: Spiritual coping (“positive”)
● Benevolent reappraisal
● Collaboration with God
● Seeking spiritual support, connection
● Religious purification
● A journey● Conservation or transformation
(Pargament, 2007)
Trauma: Seeking spiritual support
● People who are suffering turn to clergy and chaplains(Bonner et al., 2013; Morgan et al., 2016; Nieuwsma et al., 2014; Wang et al.,
2003)
● Issues like guilt, loss of faith, and loss of meaning lead to seeking care
from both mental health professionals and chaplains
(Fontana & Rosenheck, 2005; Morgan et al., 2016)
● Problems with forgiveness → PTS; Forgiveness → Quality of life
(Currier, Drescher, & Harris, 2014; Currier et al., 2016)
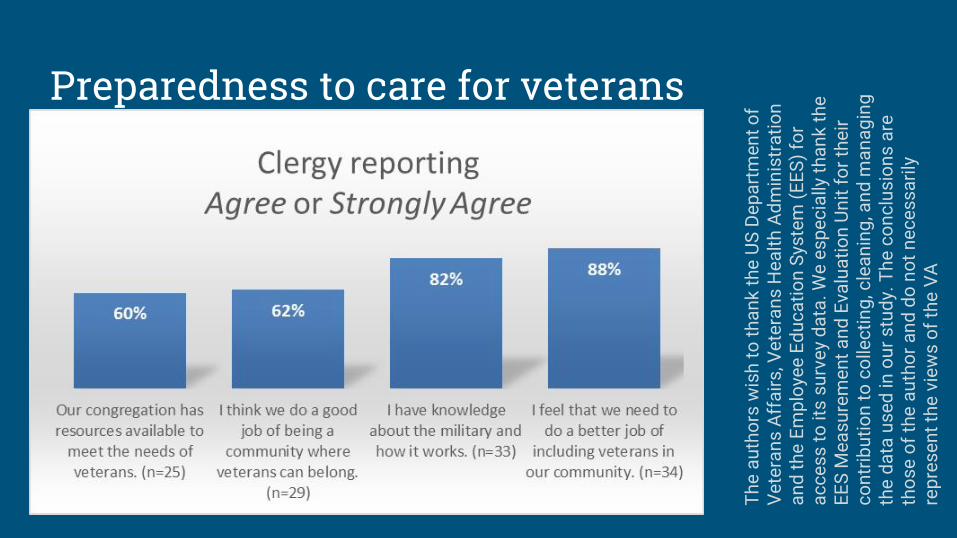
Preparedness to care for veterans
Th
e a
uth
ors
wis
h t
o t
ha
nk
th
e U
S D
ep
art
me
nt
of
Ve
tera
ns
Aff
air
s, V
ete
ran
s H
ea
lth
Ad
min
istr
ati
on
a
nd
th
e E
mp
loye
e E
du
ca
tio
n S
yste
m (
EE
S)
for
ac
ce
ss
to
its
su
rve
y d
ata
. W
e e
sp
ec
ially
th
an
k t
he
E
ES
Me
as
ure
me
nt
an
d E
valu
ati
on
Un
it f
or
the
ir
co
ntr
ibu
tio
n t
o c
olle
cti
ng
, cle
an
ing
, an
d m
an
ag
ing
th
e d
ata
us
ed
in o
ur
stu
dy.
Th
e c
on
clu
sio
ns
are
th
os
e o
f th
e a
uth
or
an
d d
o n
ot
ne
ce
ss
ari
ly
rep
res
en
t th
e v
iew
s o
f th
e V
A
Layers of trauma
● Psychological, Cognitive, Behavioral,
Interpersonal, Physical, Emotional,
Spiritual...
● “...trauma...can cause much deeper inflictions and afflictions than just physiological or psychological harm, for there may also be wounds affecting the ‘soul’ that are far more difficult to heal.”
(“Moral Injury, Spiritual Care and the Role of Chaplains: An Exploratory Scoping Review of Literature and Resources”)
nationalgeographic.com
Spiritual reactions to trauma:Spiritual wounds of war/Moral Injury (MI)
○ Anytime we transgress our values or mores through our own actions, or bear witness to such, by another
○ Brings theme of worth/value to the surface-question worthiness (or possibility of forgiveness)
○ Shatters one’s sense of self and worldview-may lead to apathy of meaning, purpose, life, and spiritual connection/comfort
Spiritual reactions to trauma:
● Moral injury affects one’s “interiority” (John O’Donohue): Why is moral injury so crippling?
● Why is treating moral injury from a spiritually-oriented disposition essential to beginning to foster healing?
wong42.weebly.com
Spiritual reactions to trauma:Symptoms associated with spiritual injuries (MI):● PTSD● Depression● Isolation/less social support● Poorer social/work adjustment● Hopelessness, pessimism, anger● Suicide risk● Shame, guilt, anxiety
“In addition to poorer mental health and adjustment, quantitative and qualitative research has demonstrated negative spiritual impacts of moral injury.”
Wortmann, J. H., Eisen, E., Hundert, C., Jordan, A. H., Smith, M. W., Nash, W. P., & Litz, B. T. (2017). “Spiritual Features of War-Related Moral Injury: A Primer for Clinicians.”
Spiritual reactions to trauma:● Feelings of guilt
● Loss of once-meaningful beliefs/values● Feeling damaged/defective/flawed● Confusion about core ethical beliefs● Altered sense of meaning/purpose● Existential and theodicy struggles● Feeling ineffective, despair, hopelessness● Grief and loss● “Who am I now?”● Confusion about God: character, presence, unconditional love,
etc.
Spiritual reactions to trauma:
“… many veterans do not believe their moral struggles are psychological illnesses needing
treatment. Instead, they experience their feelings as a profound spiritual crisis that has changed
them, perhaps beyond repair”(Brock and Lettini 51).
Spiritual reactions to trauma:
● Research shows that service men and women struggle to reconcile their previous religious beliefs with traumatic, war-time experiences
● Over half of those feel as if they have abandoned their religious framework altogetherFontana & Rosenheck, 2005 pinterest.com
Spiritual responses to trauma: role of the spiritual
“Spirituality is the art
of transfiguration.”John O’Donohue
“Suffering ceases to be
suffering in some way at
the moment it finds a
meaning.” Viktor Frankl99inspiration.com
Spiritual responses to trauma: role of the Spiritual● Finding meaning and purpose in
life
● Path toward our wholeness
● Moving beyond our smaller, lesser
selves into embodiment of our
Essence/Soul
● Moving toward our best, highest,
most authentic self
● More about relationship (with Self,
Other, Nature, the Sacred)
● More about exploring our inner
landscaping and makeup
● Integrating mind, body, and Soul
● Honoring interdependence and
interconnectedness
● Both a practice and a “beingness”—
moving beyond external
“doingness”/thinking
Elevating Our Consciousness
Spiritual responses to trauma:
● Veterans, because of military culture, often feel safer with clergy and chaplains (confidential, off the record, non-clinical diagnosis, etc.)
● Clergy seen as less stigmatizing, less threatening
● Maladaptive: Magical thinking, diminishing the role of the MH/clinical, avoiding diagnoses (“prayer will save me,” etc)
● Strong connection between weakened spirituality, increased guilt/shame, and decrease of meaning/purpose in life
Spiritual responses to trauma:Effect of Trauma: Spiritual Intervention:
Isolation and withdrawal Build connections and supportive health community
Guilt Practice self-forgiveness and compassion
Anger Forgiveness as movement away from hostility
Foreshortened future and loss of interest
Honoring and being present within “the now”
Hypervigilance and anxiety Meditation
Spiritual responses to trauma: sufferingSuffering: must change our orientation to it
How can suffering be valuable?○ Suffering as a teacher○ The shadow side of our love, our values, our beliefs ○ Mining the riches of our suffering vs. “fix me” therapeutic culture○ “Changing our relationship” to the pain vs. striving to rid ourselves of
it (automatically begins to alleviate suffering)○ “What I’m not willing to have, I will” (ACT maxim)○ Taking seriously that trauma can yield growth and is invitation to
grappling with theological beliefs that were handed-down/never fully integrated
○ When engaged, can lead to rebirth after psycho-spiritual death
Spiritual responses to trauma: guilt
● Holding nonjudgmental, loving, brave space: must validated the feeling and the experience instead of brushing it off as “war”
● Guilt: mainly experienced as a “bad” feeling-what about it is good?○ Moral compass, signpost when we go astray○ Helps us to be more compassionate, loving, empathetic○ More likely to extend grace/mercy to the other when we have
experienced acute guilt from our own mistakes○ Able to fully see/accept our own humanity (perfection as illusion that
creates suffering)○ Learning to hold the guilt reverently/tenderly, like a child, as it is
something that is informing our growth (while also acknowledging the pain)
Spiritual responses to trauma: confessionConfession:
Cathartic-why?○ Externalizes what was internally
toxic○ Involves accepting and owning full
responsibility○ Initiates the healing process○ Can then begin to learn from vs.
avoid/be controlled by○ Can experience non-judgment and
love from the listener(s)○ Validation from others through
similar “sins” or errors99inspiration.com
Spiritual responses to trauma: confession
“Many are alienated from their own spiritual center, from others, and
ultimately from God. A person in this condition has lost his sense of self as a
loving, moral human being. The only remedy is to regain a sense of self in
loving relationships with others, to experience another transformation of self-perception...A decisive step in the
journey out of the spiritual night...is...the acceptance of responsibility for one’s own actions.” (Mahedy, William P. Out of the Night: the Spiritual
Journey of Vietnam Vets. Knoxville, Radiz, 1986)
huiho.org
Spiritual responses to trauma: reconciliationMost major religions hold space for the healing effects of reconciliation:● Reconcile with one’s Self, Higher Power, the Other, and the community
○ Mindfulness of one’s actions that can both inflict pain and yield healing;○ Being granted absolution by an authority figure representing the Sacred○ Making amends or paying penance (not as punishment but as reminder of one’s
innate goodness)● Initiates the meaning-making process:
○ “I now understand that I endured this so that I might warn/teach others about it in the future.”
○ Rediscovery of deeper meaning and purpose ● Religious sacraments: opportunity to take hard look at why we engage in the sacraments/
rituals and what role they can play in our healing and integration (within Self and the community)
● “Both/and”: understanding and owning both our goodness and our shadow (our light and our dark); recognizing our internal parts vs. Essence (perception of self vs. “self as context”)
Evidence-Based Practices (EBPs): MIThree EBPs that dovetail well with chaplaincy:● Motivational Interviewing (MI): “A collaborative, goal-oriented style of communication with
particular attention to the language of change, designed to strengthen personal motivation for and commitment to a specific goal by eliciting and exploring the person’s own reasons for change within an atmosphere of acceptance and compassion.” (Miller and Rollnick, 410)○ Focus on one’s readiness/willingness to change○ Asking gentle, directional questions (contemplative) vs. offering answers (“guiding”
vs. “directing” or “following”)○ Four movements: engaging, focusing, evoking, and planning (respecting patient’s
autonomy and not steering where I think patient needs to go)○ OARS: Open questions, Affirming, Reflecting, and Summarizing○ Doesn’t join with the client around the “but,” but joins around the place of potential
willingness to change:■ Avoids strengthening the person’s reluctance/arguments for change■ Instead, offers engagement, empowerment, openness, and understanding
Evidence-Based Practices (EBPs): PSTThree EBPs that dovetail well with chaplaincy:● Problem-Solving Therapy (PST) aims to:
○ Enhance one’s adaptability to problems in life (problems are normal part of life);○ Offer “effective implementation of specific problem-solving behaviors” (Nezu, Nezu,
D’Zurilla, 3)● Used to treat: depression, anxiety, emotional distress, SI, cancer, heart disease, diabetes,
stroke, TBI, PTSD, schizophrenia● Aims: “positive problem orientation” and “planful problem solving,” while minimizing
“negative problem orientation, avoidant problem solving, and impulsive/careless reactions” (15-16)
● Four “toolkits”:○ Problem-solving multitasking (overcoming cognitive overload)○ Stop, slow down, think, act (SSTA): (overcoming emotional dysregulation and
maladaptive problem solving under stress)○ Healthy thinking and positive imagery (overcoming negative thinking and low
motivation)○ Planful problem solving (effectively problem solving)
Evidence-Based Practices (EBPs): ACT
● Acceptance and Commitment Therapy
● Works so well with chaplaincy, there’s even a book for clergy!
Evidence-Based Practices (EBPs): ACT
Psychological Flexibility:“The process of contacting the present
moment fully as a conscious human being and persisting or changing behavior in the service of chosen
values.”
Potential intersections with spirituality:
● Openness● Balance/groundedness● Connected to Essence/Self, other,
nature, and the sacred (if applicable)
● Innate understanding of interdependence/interconnectedness
● Working from love, compassion, kindness (toward self also)
● Embodying values/morals● Acceptance of what is vs.
struggling against● Present, aware, conscious
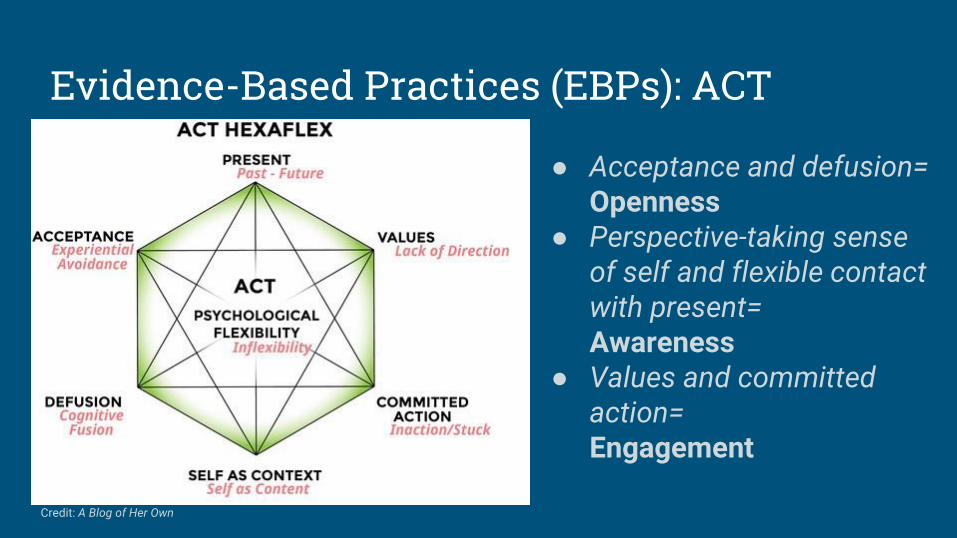
Evidence-Based Practices (EBPs): ACT
● Acceptance and defusion=Openness
● Perspective-taking sense of self and flexible contact with present=Awareness
● Values and committed action=Engagement
Credit: A Blog of Her Own

EBPs and Collaboration• Principle-based EBPs
• Different than delivering therapy package as a licensed provider
• Seek training opportunitiesPST: https://www.veterantraining.va.gov/
movingforward/
MI: https://motivationalinterviewing.org/motivational-interviewing-training
• Mental Health Integration for Chaplain Services (MHICS)
http://www.mirecc.va.gov/MIRECC/mentalhealthandchaplaincy/MHICS.asp
Collaborating with Mental Health Colleagues
• Get to know one another
• Role clarification/scope of practice
• Formal process: screening and referral

Resources: CollaboratingBridging Mental Health and Chaplaincy (≈ 1 hour each)
➢ “Why do it?”
➢ “Knowing Our Stories”
➢ “Opening a Dialogue”
Learning Collaborative (≈ 1 hour each)
➢ “Establishing Awareness”
➢ “Communicating and
Coordinating Care”
➢ “Formalizing Systematic Processes”Videos available at: https://www.mirecc.va.gov/mentalhealthandchaplaincy/

Resources: Collaborating, Veterans, and Mental Health
Clergy & Faith Communities
Clergy (≈ 1 hour each)
➢ “Signposts Toward Collaboration”
➢ “Abiding with Those Who Suffer”
Faith Communities (≈ 20 minutes each)
➢ “Partners in Care”
➢ “Trauma”
➢ “Moral Injury”
➢ “Belonging”
Videos available at:https://www.mirecc.va.gov/mentalhealthandchaplaincy/
community.asp
Contact us at [email protected]

Resources: Military Military Specialty Certification for BCCs:
http://www.professionalchaplains.org/
Resources: Suicide
In addition to previous suicide prevention resources:
Faith. Hope. Life.
Program through the National Action Alliance for Suicide Prevention-effort to get faith communities involved in suicide prevention
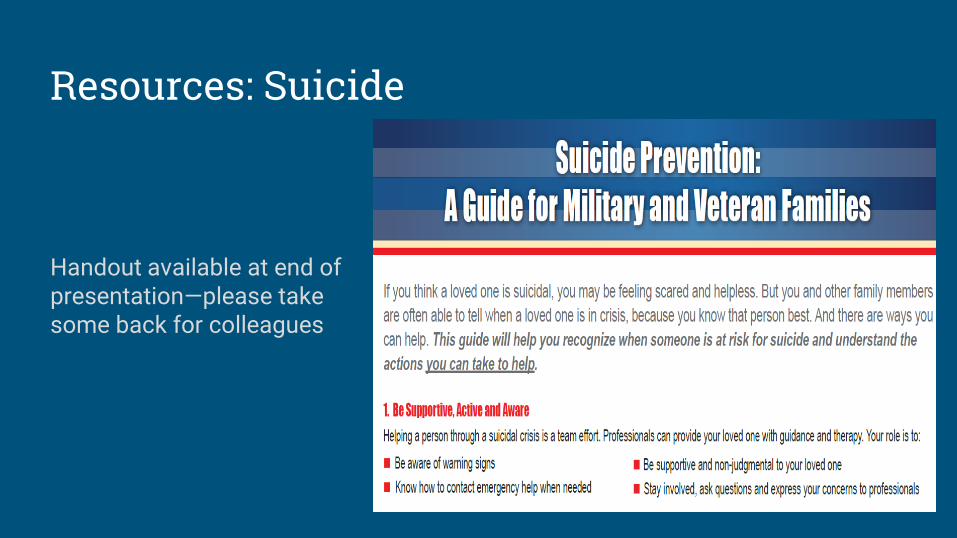
Resources: Suicide
Handout available at end of presentation—please take some back for colleagues
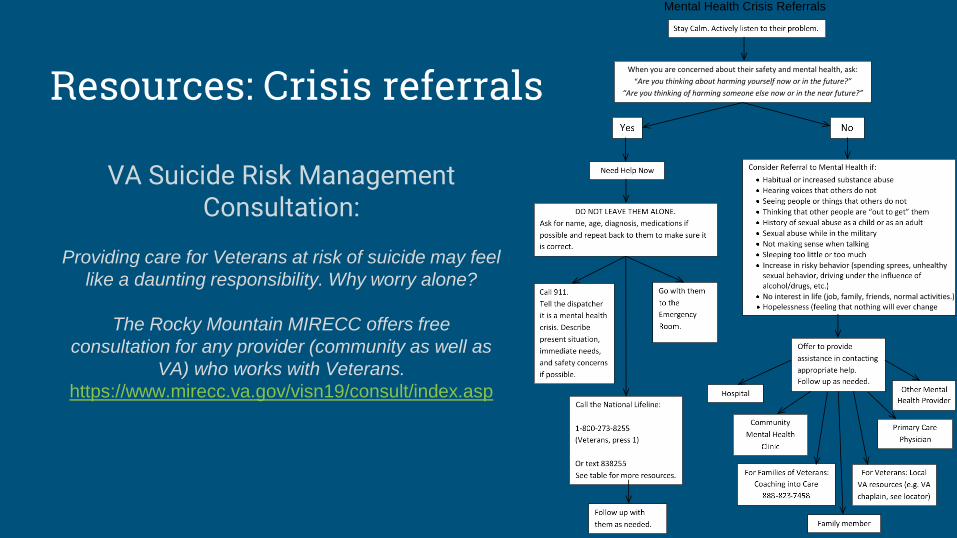
Resources: Crisis referrals
Mental Health Crisis Referrals
VA Suicide Risk Management Consultation:
Providing care for Veterans at risk of suicide may feel
like a daunting responsibility. Why worry alone?
The Rocky Mountain MIRECC offers free
consultation for any provider (community as well as
VA) who works with Veterans.
https://www.mirecc.va.gov/visn19/consult/index.asp
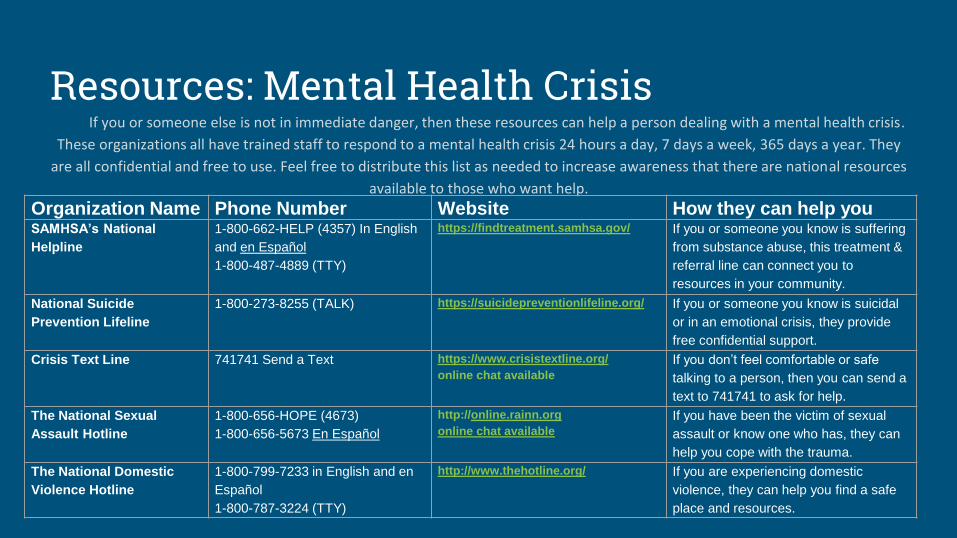
Resources: Mental Health CrisisIf you or someone else is not in immediate danger, then these resources can help a person dealing with a mental health crisis.
These organizations all have trained staff to respond to a mental health crisis 24 hours a day, 7 days a week, 365 days a year. They
are all confidential and free to use. Feel free to distribute this list as needed to increase awareness that there are national resources
available to those who want help.
Organization Name Phone Number Website How they can help youSAMHSA’s National
Helpline
1-800-662-HELP (4357) In English
and en Español
1-800-487-4889 (TTY)
https://findtreatment.samhsa.gov/ If you or someone you know is suffering
from substance abuse, this treatment &
referral line can connect you to
resources in your community.
National Suicide
Prevention Lifeline
1-800-273-8255 (TALK) https://suicidepreventionlifeline.org/ If you or someone you know is suicidal
or in an emotional crisis, they provide
free confidential support.
Crisis Text Line 741741 Send a Text https://www.crisistextline.org/
online chat available
If you don’t feel comfortable or safe
talking to a person, then you can send a
text to 741741 to ask for help.
The National Sexual
Assault Hotline
1-800-656-HOPE (4673)
1-800-656-5673 En Español
http://online.rainn.org
online chat available
If you have been the victim of sexual
assault or know one who has, they can
help you cope with the trauma.
The National Domestic
Violence Hotline
1-800-799-7233 in English and en
Español
1-800-787-3224 (TTY)
http://www.thehotline.org/ If you are experiencing domestic
violence, they can help you find a safe
place and resources.
Resources: Mental Health and Spirituality
National Alliance on Mental Illness (NAMI) FaithNet-https://www.nami.org/faithnet
A network of members, friends, clergy and congregations who encourage faith communities to be welcoming and supportive of people living with mental illness.
Resources: Veteran Care
Veterans Resource locator –https://www.veteranscrisisline.net/GetHelp/ResourceLocator.aspx
VA Locations –https://www.va.gov/directory/guide/allstate.asp
Coaching into Care -https://www.mirecc.va.gov/coaching/
A national telephone service of the VA which aims to educate, support, and empower family members and friends who are seeking care or services for a Veteran.

Questions?
Contact us:
Works Cited:● Aflakseir, A., & Coleman, P. G. (2009). The influence of religious coping on the mental health of disabled Iranian
war veterans. Mental Health, Religion & Culture, 12, 175-190.
● Bonner, L. M., Lanto, A. B., Bolkan, C., Watson, G. S., Campbell, D. G., Chaney, E. F., ... & Rubenstein, L. V. (2013).
Help-seeking from clergy and spiritual counselors among veterans with depression and PTSD in primary care.
Journal of Religion and Health, 52, 707-718.
● Brock, Nakashima Rita and Gabriella Lettini. Soul Repair: Recovering from Moral Injury after War. Boston, Beacon,
2012.
● Carey, Lindsay B., Timothy J. Hodgson, Lillian Krikheli, Rachel Y. Soh, Annie-Rose Armour, Taranjeet K. Singh,
Cassandra G. Impiombato, “Moral Injury, Spiritual Care and the Role of Chaplains: An Exploratory Scoping Review
of Literature and Resources” (2016) J Relig Hea lth, 55: 1218-1245
● Currier, J. M., Drescher, K. D., & Harris, J. I. (2014). Spiritual functioning among veterans seeking residential
treatment for PTSD: A matched control group study. Spirituality in Clinical Practice, 1(1), 3-15.
● Currier, J. M., Holland, J. M., Drescher, K., & Foy, D. (2015). Initial psychometric evaluation of th Moral Injury
Questionnaire—Military version. Clinical psychology & psychotherapy, 22, 54–63.
● Exline, J. J., Pargament, K. I., Grubbs, J. B., & Yali, A. M. (2014). The Religious and Spiritual Struggles Scale:
Development and initial validation. Psychology of Religion and Spirituality, 6(3), 208.
● Flipse Vargas, A., Hanson, T., Kraus, D., Drescher, K., & Foy, D. (2013). Moral injury themes in combat veterans’
narrative responses from the National Vietnam Veterans’ Readjustment Study. Traumatology, 19(3), 243-250.
Works Cited:● Fontana, A., & Rosenheck, R. (2004). “Trauma, change in strength of religious faith, and mental health service use
among veterans treated for PTSD.” J Nerv Ment Dis, 192(9), 579-584.
● Fontana, A., & Rosenheck, R. (2005). The role of loss of meaning in the pursuit of treatment for posttraumatic
stress disorder. Journal of Traumatic Stress, 18(2), 133-136.
● Goalder, James S., PhD and John Bailey, Mdiv (2018) Military Culture and the Wounds of War. PowerPoint
presentation within Community Clergy Training Program.
● Hayes, Steven C. and Jason Lillis. Acceptance and Commitment Therapy. Washington, APA, 2012.
● Kopacz, Marek S., April L. Connery, Todd M. Bishop, Craig J. Bryan, Kent D. Drescher, Joseph M. Currier, Wilfred R.
Pigeon (2016) “Moral Injury: A New Challenge for Complementary and Alternative Medicine,” Complementary
Therapies in Medicine, 24, 29-33.
● Lagace, Raymond R. and William D. Smith, PhD (2013) Coming Home: Developing a Theological Response for
Returning Combat Veterans. PowerPoint presentation at Togus, ME VA.
● Mahedy, William P. Out of the Night: the Spiritual Journey of Vietnam Vets. Knoxville, Radix, 1986
● Miller, William R. & Stephen Rollnick. Motivational Interviewing: Helping People Change. New York, Guilford, 2013.
● Morgan, J. K., Hourani, L., Lane, M. E., & Tueller, S. (2016). Help-seeking behaviors among active-duty military
personnel: utilization of chaplains and other mental health service providers. Journal of health care chaplaincy, 22,
102-117.
● Nezu, Arthur M., Christine Maguth Nezu, Thomas J. D’Zurilla. Problem-Solving Therapy: a Treatment Manual. New
York, Springer, 2013.
Works Cited:● Nieuwsma, J. A., Fortune-Greeley, A. K., Jackson, G. L., Meador, K. G., Beckham, J. C., & Elbogen, E. B. (2014).
Pastoral care use among post-9/11 veterans who screen positive for mental health problems. Psychological
services, 11, 300-308.
● Pargament, K. I. (2007). Spiritually integrated psychotherapy: Understanding and addressing the sacred. New
York, NY US: Guilford Press.
● Pargament, K. I., Koenig, H. G., & Perez, L. M. (2000). The many methods of religious coping: Development and
initial validation of the RCOPE. Journal of Clinical Psychology, 56, 519-543.
● Tick, Ed. War and the Soul. Wheaton, Quest, 2005.
● Suzette Bremault-Phillips, Lori-Ann R. Sacrey, Joanne Olson, Jeanne Weis, & Terry Cherwick (2016) “Measures of
Spirituality for Use in Military Contexts: A Scoping Review,” Journal of Military, Veteran and Family Health, 2(1)
55-69.
● Wang, P. S., Berglund, P. A., & Kessler, R. C. (2003). Patterns and correlates of contacting clergy for mental
disorders in the United States. Health services research, 38(2), 647-673.
● Witvliet, C. V. O., Phipps, K. A., Feldman, M. E., & Beckham, J. C. (2004). Posttraumatic mental and physical
health correlates of forgiveness and religious coping in military veterans. Journal of Traumatic Stress, 17, 269-
273.
● Wood, B. T., Worthington Jr., E., Exline, J., Yali, A., Aten, J. D., & McMinn, M. R. (2010). Development, refinement,
and psychometric properties of the Attitudes toward God Scale (ATGS-9). Psychology of Religion and Spirituality,
2(3), 148-167. doi:10.1037/a0018753
Works Cited:● Wortmann, J. H., Eisen, E., Hundert, C., Jordan, A. H., Smith, M. W., Nash, W. P., & Litz, B. T. (2017). “Spiritual
Features of War-Related Moral Injury: A Primer for Clinicians.” Retrieved from
http://www.dartmouth.edu/~ajordan/papers/Wortmann%20et%20al.%20-
%20Spiritual%20Features%20of%20Moral%20Injury.pdf
● https://www.womenshealth.va.gov/WOMENSHEALTH/outreachmaterials/mentalhealth/substance_abuse.asp
● https://dod.defense.gov/News/Casualty-Status/
● https://www.va.gov/vetdata/docs/Demographics/New_Vetpop_Model/Vetpop_Infographic_Final31.pdf
● https://www.publichealth.va.gov/docs/epidemiology/healthcare-utilization-report-fy2015-qtr3.pdf#






























