Embed Size (px)
Citation preview

1223
Spine Imaging: History, Achievements,Remaining Frontiers
FJohn R. Hesselink Imaging the spine presents a special challenge. The vertebral column is a complex
bony structure. The vertebrae have irregular contours and shapes with multiplebony processes projecting in various directions. Moreover, the anatomic configu-rations of the vertebrae are different in the cervical, thoracic, and lumbosacralregions. This variable anatomy, along with the natural curvature of the spine, resultsin different orientations and complex angulations of joints and foramina, makingimaging difficult.
The vertebral column encloses the spinal canal, which serves as a protectiveconduit for vital neural elements, the spinal cord and nerve roots. Disease processesthat disrupt or compress the neural structures, although not often fatal, are majorcauses of morbidity and disability. Signs and symptoms of spinal disorders arecommon complaints.
Many imaging techniques have been applied to the spine and its contents,starting with plain films and tomography. Myelography, epidural venography, anddiskography were developed specifically to evaluate spinal disorders. Other imagingtechniques include radionuclide scanning, sonography, artenography, CT, and MRimaging. Each of these techniques has special merits and limitations for evaluatingcertain areas of the spine.
History
Plain Radiography
Plain radiography of the spine was made possible by the discovery of X-rays onNovember 8, 1 895, by Wilhelm Conrad Roentgen, Professor of Physics at theUniversity of Wurzburg, Germany. Dr. Roentgen presented his paper, “A New Kindof Rays” to the Wurzburg Physical-Medical Society on December 28, 1 895, andthe paper was printed in the Society’s Transactions in the final volume of 1 895 [11.
Owing to the low output of the early cathode-ray tubes, spine radiographsrequired imaging times of at least 15 mm. Roentgen’s discovery generated interestwithin the worldwide scientific community, and refinements of his crude equipmentfollowed rapidly. With development of high-voltage generators, finely focusedvacuum tubes with tungsten targets, and film-screen technology, plain radiographyof the spine achieved the quality to which we are accustomed today [1].
Received November 23, 1987; accepted afterrevision February 21, 1988.
‘Department of Radiology, University of Califor-nia, San Diego, Medical Center, 225 Dickinson St.,San Diego, CA 92103. Address reprint requests toJ. R. Hesselink.
AJR 150:1223-1229, Jun 19880361-803X/88/1 506-1 223C American Roentgen Ray Society
Tomography
The origins of tomography and credits for its development are not entirely clear.Between 1914 and 1930, a dozen or more investigators did some pioneering workwith this method, and it was added to the methods available to the radiologist. Inorder to obtain a tomogram, the X-ray source and film are rotated about a fulcrumduring the exposure to image a defined plane within a patient. Motion blurs the
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
CSF
LIB
& C
KM
/RSC
S M
GM
T o
n 11
/21/
14 f
rom
IP
addr
ess
169.
230.
243.
252.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

1224 HESSELINK AJR:150, June 1988
anatomy above and below the imaging plane. At first, linearmotion was used; later, more complex motions were devisedto get more complete blurring of unwanted structures [2].Tomography was used for many years to define complexvertebral fractures, to search for bone fragments within thespinal canal, and to look for subtle erosions of the corticalbone and associated periosteal reactions.
Myelography
Imaging of neural tissues within the spinal canal remainedelusive to standard techniques and led to the development ofmy�lography. The concept of myelography was first sug-gested by Dandy [3] in his classic 1 91 9 article on pneumo-encephalography. On the basis of his observations of theutility of subarachnoid air for diagnosing intracranial diseases,he stated that it was probable “that we shall be able to localizespinal cord tumors by means of intraspinal injections of air.”Two years later, in Sweden, Jacobeus [4] reported on thesuccessful localization of intraspinal tumors with “pneumo-myelography.” A report by Dandy [5] followed in 1 925 inwhich 1 0 spinal tumors were diagnosed with air myelography.
The next advance in myelography occurred in 1922, whenSicard and Forestier [6] inadvertently introduced iodized pop-pyseed oil (Lipiodol) into the subarachnoid space. They notedthat the oil moved freely in the subarachnoid space andrealized its potential for localizing spinal cord tumors. Owingto its high iodine content (40%), Lipiodol could be seenradiographically in very small quantities and rapidly becamethe preferred myelographic contrast agent. Unfortunately, theoil tended to form globules when mixed with CSF and had tobe removed completely because it was irritating to the piaarachnoid.
In 1 934, Mixter and Barr [7] published their classic articleon the herniated intervertebral disk as a cause of low backpain and sciatica. Within a short time after that report, thenumber of myelograms being obtained increased enormously.As a result, there was more concern about the arachnoiditisassociated with Lipiodol. Nonetheless, no better agent wasavailable, and because myelography had now become animportant diagnostic method, Lipiodol continued to be used.
It was not until 1 940 that a group of investigators at theUniversity of Rochester introduced Pantopaque (Lafayette,Lafayette, IN), and the first clinical report of this new agentappeared in 1 944 [8]. Pantopaque is much less viscous thanLipiodol, less prone to globule formation, and easier to injectand aspirate. Pantopaque is an oil and immiscible with CSF.It is absorbed extremely slowly and, unless removed, remainsin the subarachnoid space for many years. Because Panto-paque is less irritating to the meninges, it rapidly supplantedLipiodol and remained the myelographic medium of choice inthe United States and Great Britain for over 30 years.
With time, reports appeared in the literature of the devel-opment of arachnoiditis after Pantopaque myelography. Ad-mixture of blood with Pantopaque increases the risk of arach-noiditis, and a “bloody spinal tap” is a contraindication toinjection of the agent. Although symptomatic arachnoiditisafter Pantopaque myelography is rare, when it does occur, it
can be accompanied by incapacitating chronic back pain andneurologic dysfunction [9].
The first water-soluble agent for myelography, abrodil(Skiodan), was introduced in 1 931 by Arnell and Lidstrom[1 0]. Owing to its irritant effect on the spinal meninges, itnever gained popularity outside Scandinavia. Two otherwater-soluble contrast agents, Conray-60 and Dimer X, weredeveloped in the late 1 960s, but they were also associatedwith unacceptable toxicity. The first nonionic water-solubleagent to gain acceptance in the United States was metriz-amide (Amipaque, Nygaard, Oslo, Norway), which had beendeveloped in Norway. Although it was associated with someacute toxicity (including nausea, vomiting, occasional sei-zures, hallucinations, and aseptic meningitis), it did not carrythe risk of chronic debilitating arachnoiditis associated withPantopaque. Also, by use of proper technique and maintaininggood patient hydration, the side effects could be kept to aminimum [1 1]. More recently, even less toxic nonionic agentshave become available, including iohexol (Omnipaque, Win-throp-Breon, New York, NY) and iopamidol (Isovue, Squibb,Princeton, NJ), that have essentially replaced metrizamide[12, 13].
Diskography
A few other invasive techniques have been developed forevaluating degenerative disk disease. Lindblom [1 4] intro-duced diskography in 1 948. With this technique, a needle isintroduced into the central portion of the intervertebral diskand a small amount of contrast material is injected. Thecontrast material pools centrally in the nucleus pulposus of anormal disk. In a degenerated disk, the contrast materialassumes a more irregular, distorted shape and dissects intomore peripheral parts of the intervertebral disk. With theavailability of CT and MR, diskography is seldom performedtoday.
Epidural Venography
Epidural venography had a brief period of popularity in themiddle and late 1 970s. Via a femoral venous approach, cath-eters are manipulated into one or both ascending lumbarveins and contrast material is injected to outline the internalvertebral plexus. A herniated disk compresses and preventsfilling of the veins in the ventral epidural space [1 5]. At onetime, epidural venography was becoming competitive withmyelography and had its loyal proponents. Then, CT devel-oped so that it could provide high-resolution images of thespine with good soft-tissue contrast, and the argument overwhich of the invasive techniques was superior became moot.
Arteriography
Another vascular procedure, spinal angiography, has fewindications. Nevertheless, it is the definitive procedure forevaluating arteriovenous malformations of the spinal cord andwill likely remain so [16]. On occasion, arteriography is per-
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
CSF
LIB
& C
KM
/RSC
S M
GM
T o
n 11
/21/
14 f
rom
IP
addr
ess
169.
230.
243.
252.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:150, June 1988 SPINE IMAGING 1225
formed to identify the origin of the artery of Adamkiewiczbefore thoracic spine surgery. With refinements in techniqueand newer nonionic, water-soluble contrast agents, spinalangiography is a low-risk procedure.
Radionuclide Bone Scanning
An important imaging technique to augment the diagnosticworkup of spine disease is radionuclide bone scanning. It isthe most sensitive technique for the early detection of neo-plastic or inflammatory disease. On the other hand, the im-ages have low spatial resolution and low specificity for dis-ease. They cannot be used to distinguish either malignantfrom benign disease or neoplastic from inflammatory disease.Because the radiation dose is quite low and the entire skeletoncan be imaged at one time, radionuclide bone scanning is anideal screening technique [17].
Sonography
Because ultrasound cannot penetrate bone, the use ofsonography is limited to the unossified fetal spine and tothose patients in whom the posterior elements are deficientor have been removed. Sonography is used extensively toscreen for spinal dysraphism in the fetus and neonate [18].Also, intraoperative sonography after laminectomy helps de-fine the location and extent of cord tumors and cysts to guidesurgical removal [19].
CT
A new era of spine imaging began with the introduction ofCT in 1 973 by Dr. Godfrey Hounsfield [20]. The early clinicalinvestigations were performed by Ambrose [21] and his col-leagues. Although the first CT scanners were dedicated headunits, the potential for imaging spinal anatomy was recognizedimmediately. As soon as whole-body imagers became avail-able, they were applied to the spine.
CT is a sectional imaging technique that images primarilyin the axial plane. If closely spaced axial scans are obtained,images can be reformatted in a coronal, sagittal, or obliqueplane, but with lower resolution than with direct scanning[22]. The scanning gantry also can be tilted to obtain sectionsparallel to each intervertebral disk.
CT has much higher contrast resolution than conventionalradiographic techniques do. It provides superb detail of thebony elements and also clearly outlines soft-tissue/fat planes.For better visualization of intradural structures, the examin-ation can be supplemented with intrathecal contrast media[23]. A low-dose “CT myelographic study” has low morbiditybecause it requires only 3-5 ml of isotonic (180 mg/mI) water-soluble contrast material. Nevertheless, it does require aspinal tap, making it more invasive and lowering patientacceptance. IV contrast material is seldom used in conjunctionwith spine CT. It is helpful for examining spinal tumors andinflammatory disease. Some also advocate its use in thepostoperative patient to distinguish recurrent disk from epi-
dural scarring [24].
MR Imaging
The phenomenon of magnetic resonance was discoveredby Bloch [25] and Purcell et al. [26] in 1 946. MR spectroscopyevolved from their work and has been used extensively todetermine the chemical composition and structure of complexmolecules. It was not until 1 973 that Lauterbur [27] conceivedthe idea of constructing images from the MR signal. Techno-logic advances were slow in coming at first, but developmentaccelerated rapidly in the early 1980s. Multislice spin-echopulse sequences, higher field strengths, steeper gradients,and specialized surface coils are a few of the many develop-ments that led to high-quality spine images [28, 29]. Morerecently, gradient-echo pulse sequences have produced highsignal from CSF with relatively short acquisition times, result-ing in “myelogramlike images” [30]. Alternatively, high-reso-lution T2-weighted images of the cord can be obtained withCSF-gating techniques [31 , 32].
MR has several advantages over CT and is effectivelychallenging CT for supremacy in the diagnosis of diseases ofthe spine and spinal cord. MR does not use ionizing radiationand, as far as we know, is entirely without side effects. Imagescan be obtained in any desired imaging plane. It has evenhigher contrast resolution than CT does, so that the spinalcord and nerve roots in the subarachnoid space can bevisualized without the injection of IV or intrathecal contrastmaterial. On the other hand, MR is more costly, and patientswith cardiac pacemakers or intracranial aneurysm clips cannotbe scanned. Also, CT has superior spatial resolution andprovides better bone detail.
Although little signal is obtained from cortical bone, the fat-containing bone marrow yields high signal on Ti -weightedimages, so that disease processes that replace the bonemarrow of the vertebral bodies, such as tumor, inflammation,or reactive bone sclerosis, produce a negative defect that iseasily recognized. Epidural involvement and spinal cordcompression are seen better by MR than by myelography[33].
Achievements
Spine imaging has had a colorful history, starting with plainradiography, progressing to the era when myelography wasthe definitive procedure, and finally advancing to the lessinvasive, computerized sectional imaging techniques of today.Each imaging technique has had a part in elucidating diseaseprocesses affecting the spine. Along the way, great strideshave been made in correlating altered anatomy displayed byimaging studies with abnormal function and clinical syn-dromes.
With existing technology, a thorough examination of thespine can be performed. Plain films provide a global view ofthe bony elements, neural foramina, and facet joints. Congen-ital anomalies, fractures, malalignment of the vertebrae, de-gree of degenerative change, and gross bony destruction canbe identified (Fig. 1A). Moreover, the density of the bonesgives a clue about overall mineralization of the skeleton. Moreexquisite bone and soft-tissue detail are available with CTand MR (Fig. 1 B). Radionuclide bone scanning has the highest
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
CSF
LIB
& C
KM
/RSC
S M
GM
T o
n 11
/21/
14 f
rom
IP
addr
ess
169.
230.
243.
252.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

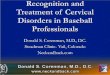
Fig. 2.-38-year-old woman with left-sided sciatica.A, Sagittal MR scan with gradient-echo pulse sequence shows soft-tissue mass Indenting ventral thecal sac (arrows) at L4-L5 level. Intervertebral disk
space is narrowed at that level; low signal intensity within disk represents either calcification or air. Disk at L5-Sl is degenerated also. Normal-appearingdisk is seen at L3-L4.
B, Ti-weighted image. Herniated disk (arrowheads) is outlined by epidural fat. Disk at L5-Si also protrudes posteriorly into spinal canal.C, Axial TI-weighted scan at L4-L5 level shows large fragment of disk material (arrows) in left anterolateral aspect of spinal canal, compressing thecal
sac and nerve roots.
1226 HESSELINK AJR:150, June 1988
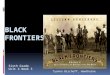
Fig. 1.-35-year-old woman with severe pso-riatic arthritis and progressive upper extremityweakness.
A, Lateral plain film shows marked anteriorsubluxation of Cl on C2. Also noted is promi-nence of soft tissues anterioriy (arrows).
B, Sagittal Ti-weighted MR scan shows mark-edly increased distance between anterior archof Cl and odontoid (white arrows). Upper cervi-cal cord (black arrow) is severely compressedbetween odontoid and posterior arch of Ci.
sensitivity for detecting metastatic deposits and inflammatorydisease [17].
Degenerative disk disease, a common cause of back pain,is imaged clearly with CT and MR. Degeneration of interver-tebral disks is associated with dehydration of the disk, result-ing in lower signal intensity on T2-weighted MR images. BothMR and CT have high sensitivity for detecting herniated disks;free fragments can be located accurately for presurgical plan-ning [28, 29, 34, 35] (Fig. 2).
Imaging of spinal cord disease remained elusive until MRwas developed. Other techniques, which used intrathecalcontrast material, relied on detecting alterations in the outercontours of the cord. MR imaging displays the internal archi-tecture of the cord, so that solid and cystic lesions can bedistinguished and diseases unassociated with mass effect
can be imaged. Cord tumors (Fig. 3), syringomyelia, traumaticinjuries (Fig. 4), multiple sclerosis, and congenital anomaliescan be seen with a clarity not previously possible [36-40].MR is providing new insights into disease mechanisms, prog-nosis, and effects of therapy [41-43].
On the basis of our knowledge and experience with spineimaging methods, algorithms can be devised for evaluatingspine disease, depending on the patient’s presenting symp-toms and the area of the spine to be examined. In the settingof trauma, plain films are mandatory. For more exquisite detailof vertebral fractures and to look for bone fragments in thespinal canal, CT is the preferred technique. Occasionally,tomograms are helpful to delineate nondisplaced fractures ofthe odontoid. MR is the definitive method for evaluatingassociated spinal cord injuries.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
CSF
LIB
& C
KM
/RSC
S M
GM
T o
n 11
/21/
14 f
rom
IP
addr
ess
169.
230.
243.
252.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:150, June 1988 SPINE IMAGING 1227
For nontraumatic disease, if the patient presents with amyelopathy or other symptoms of spinal cord disease, MR isthe procedure of choice. For patients with lumbar radicularpain, both plain CT and MR are very effective for evaluatingdiskogenic and spondylytic disease. MR is also recommendedfor screening the cervical and thoracic spine in patients withradicular-type symptoms. If the MR scan is not definitive andclinical suspicion of organic disease is high, then a CT mye-logram should be obtained. Standard myelography has fewindications today, except for cases of suspected arachnoiditisand leptomeningeal spread of tumor. As mentioned above,radionuclide bone scanning is important in both metastaticscreening and early detection of suspected infectious dis-eases.
Remaining Frontiers
Certainly, considerable progress has been made in imagingthe spine, unfolding some of the mysteries of disease proc-esses. Nevertheless, some areas of spinal diagnosis are stillchallenging the radiologist. For example, assessment of post-
Fig. 3.-3i-year-old woman with von Hippo-Undau disease, chronic dizziness, and recentnumbness of right neck, shoulder, and arm. Pro-ton-density-weighted sagittal MR scan of uppercervical region reveals cystic lesion (arrow.heads) in upper cervical cord, associated withwidening of cord. Exophytic soft-tissue compo-nent of lesion Is noted as high-signal-intensityarea more superiorly (arrows). At surgery, a he-mangloblastoma was found involving lowerbrainstem and upper cervical spinal cord.
Fig. 4.-2i-year-old man with cervical spinefracture. Decompressive laminectomy and car-vical fusion was performed. Sagittal Ti-weightedMR scan shows severe cord contusion (arrows)at C4 and C5 levels. Injured portion of cord Is oflow signal and has irregular, poorly definedmargins.
Fig. 5-46-year-old man with recurrent backpain 1 year after laminectomy and disk excisionat L4-L5 and U-Si levels.
A, Sagittal MR image shows herniated diskposteriorly (arrowheads) at L4-L5 level. Thinblack line outlines perimeter of disk fragment.Gray-appearing scar tissue (S) surrounds diskand extends inferiorly to U-Si level.
B, Axial T2-weighted Image confirms diskfragment (arrows) in ventrolateral aspect ofspinal canal.
operative back pain remains problematic for both MR andCT. Recurrent disk and postoperative scar are often isodenseon unenhanced CT. Contrast enhancement is helpful in somecases, because the postoperative scar will enhance but thedisk does not [24]. Unfortunately, enhancement of the scartissue is unpredictable, and distinction of scar from disk isoften unsatisfactory. Owing to its higher contrast resolution,MR seems to distinguish recurrent disk from scar better thanCT does [44]. The sagittal view is particularly helpful todetermine whether or not the soft-tissue abnormality is con-tiguous with the interspace. Also, in the postoperative back,retained or recurrent disk fragments often have a thin, low-signal line around the perimeter on T2-weighted images (Fig.5). The low-signal line most likely is due to a combination offibrous tissue and chronic hemorrhage. Preliminary investi-gations with IV gadolinium-DTPA (Magnavist, Berlex, CedarKnolls, NJ) suggest that this contrast agent, in conjunctionwith Ti -weighted imaging, will assist in distinguishing diskfrom scar [44, 45]. Like CT, the scar tissue enhances tohighlight the area of postoperative change. Some enhance-ment has also been noted around the perimeter of a diskfragment, but the central part of the disk does not enhance.
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
CSF
LIB
& C
KM
/RSC
S M
GM
T o
n 11
/21/
14 f
rom
IP
addr
ess
169.
230.
243.
252.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

1228 HESSELINK AJR:150, June 1988
Initial results are promising, and a multicenter investigation isin progress to determine the efficacy of gadolinium-enhancedMR in patients with postoperative back pain.
Another challenging area is the evaluation of subarachnoidprocesses, such as arachnoiditis or drop metastases from amalignant intracranial lesion. Myelography is quite sensitivefor imaging the subarachnoid space, but is tedious to performand invasive. Similarly, CT with intrathecal contrast enhance-ment requires a lumbar puncture, and imaging the entire spinein search of metastatic foci is not practical. MR is noninvasivebut has not proved to be sensitive for intradural extramedul-lary disease. Although gradient-echo sequences, cardiac-gated T2-weighted imaging, and flow-compensation pulsesequences have improved CSF contrast, the tumor nodulescan be small and difficult to see. Preliminary studies withgadolinium-DTPA have shown that the subarachnoid nodulesof tumor enhance brightly on Ti -weighted images [46]. It ishoped that further investigations will confirm the accuracy ofthis technique so that complete myelography of the spinalcolumn will no longer be necessary in these patients. Itremains to be seen whether MR, without or with gadolinium-DTPA, will be able to replace myelography for evaluatingarachnoiditis. Some specific MR findings have been identifiedin patients with arachnoiditis [47]. Fortunately, since Panto-paque has been replaced by nonionic, water-soluble agentsfor myelography, arachnoiditis has become much less corn-mon.
The potential of cine MR and other flow techniques hasbeen unexplored in the spine. Cine MR provides dynamicpictures of CSF flow within the cistemal spaces. CSF flow
studies may provide new insights into mechanisms of devel-opment of hydromyelia and synngomyelia. These studies maysuggest methods of prevention or new modes of therapy. Ina study of 1 6 patients with syringornyelia, Enzmann et al. [48]found that the presence of pulsations within a spinal cordcyst indicated a nonneoplastic cyst. They also noted a reduc-tion in pulsations after shunting the cysts, possibly indicatinga successful shunting procedure. Cine MR should also in-crease our general knowledge about CSF flow patternsaround the foramen magnum and within the spinal canal, andthe ways that these flow patterns vary with different physio-logic maneuvers and hydrodynamic changes within the intra-cranial cavity.
As mentioned earlier, MR has markedly improved the im-aging and diagnosis of spinal cord masses. Gadolinium-DTPAis also helpful in these cases for identification of enhancingnodules, distinction between cystic tumor and synngomyelia,and delineation of the extent of infiltrating spinal cord tumors[49, 50]. There is still much to be learned about other inflarn-matory and degenerative diseases of the spinal cord. MRcertainly can detect multiple sclerosis plaques, although itssensitivity has not been determined absolutely. DeLaPaz etal. [39] identified cord lesions as high-signal abnormalities onT2-weighted images in 32 of 44 MR studies in patients withhigh clinical suspicion of multiple sclerosis. Acute multiple
sclerosis plaques may also be associated with cord swellingand breakdown of the blood-brain barner. In a case of Devicdisease, another demyelinating disorder, Tashiro et al. [51]
noted acute cord swelling and progressive cord atrophy onfollow-up MR scans. In two cases of acute transverse myelitis,Menne et al. [52] observed cord swelling but no alteration ofsignal intensity on MR images. Finally, Sherman et al. [53]demonstrated cord atrophy in five of six patients with amy-otrophic lateral sclerosis. In three of those cases, the MRscans disclosed selective atrophy of the anterior portion ofthe spinal cord, sparing the dorsal columns. These data arepreliminary, and careful pathologic and neuroanatomic correl-ative studies are necessary to fully explore the potential ofMR in these diseases.
One of the more exciting frontiers is the study of metabo-lism with MR spectroscopy. Radionuclide bone scanning pro-vides a measure of bone metabolism, but tells nothing aboutcord metabolism or neural function. Such information is criticalin cases of cord ischemia and traumatic cord injuries. Detec-tion of anatomic distortion (Fig. 4), hemorrhage, and abnormalsignal intensity with MR imaging gives some clues about thepotential for recovery of neurologic function [54], but meta-bolic data have not been available with existing conventionaltechniques. Spectroscopy research has focused on skeletalmuscle, heart, liver, and brain [55, 56], so little data areavailable on the spinal cord. If MR spectroscopy can providea measure of cord metabolism, that information may helpassess cord injury and predict clinical outcome. Equally im-portant, metabolic data could serve as an important in vivoindicator to test the effectiveness of various therapies. At thepresent state-of-the-art, MR spectroscopy is not capable ofproviding reliable measurements of cord metabolism in aclinical setting; however, these investigations are being donein the laboratory. Vink et al. [57] demonstrated significantdecreases in pH and phosphocreatine/inorganic phosphateratios after cord trauma, and adenosine triphosphonate storesdisappeared from cord tissue by 3 hr after injury. In vivospectroscopic experiments are extremely complex and re-quire a collaborative effort between the physican, biochemist,and MR physicist. The medical community anxiously awaitsfurther progress in metabolic research.
REFERENCES
1 . Dewing SB. Modern radiology in historical perspective. Springfield, IL:
Thomas, 1962:23-41, 82-118, 125-139
2. Andrews JR. Planigraphy: introduction and history. AJR i936;36:575-5873. Dandy WE. Roentgenography of the brain after injection of air into the
spinal canal. Ann Surg i9i9;70:397-4034. Jacobeus HC. On insufflation of air into the spinal canal for diagnostic
purposes in cases of tumors in the spinal cord. Acta Med Scandi92i;21 :555-560
5. Dandy WE. Diagnosis and localization of spinal cord tumors. Ann Surgi925;81 :223-254
6. Sicard JA, Forestier J. Methode generale d’exploration radiologique parl’huite iodee (Upiodol). Ann Med lnterne (Paris) 1922;46:463-468
7. Mixter WJ, Barr JS. Rupture of the intervertebral disc with involvement ofthe spinal canal. N EnglJ Med i934;211 :210-215
8. Ramsey GH, French JD, Strain WH. lodinated organic compounds ascontrast media for radiographic diagnoses. IV. Pantopaque myelography.Radiology i944;43:236-240
9. Peterson HO. The hazards of myelography. Radiology l975;1 15:237-239
10. Arnell 5, Udstrom F. Myelography with Skiodan (abrodil). Acta Radiol
(Stockh) i93i;12:287-289
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
CSF
LIB
& C
KM
/RSC
S M
GM
T o
n 11
/21/
14 f
rom
IP
addr
ess
169.
230.
243.
252.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:150, June 1988 SPINE IMAGING 1229
1 1 . Sackett JF, Strother CM, Quaglieri CE, Javid JJ, Levin AB, Duff TA.
Metrizamide-CSF contrast medium. Analysis of clinical application in 215
patients. Radiology 1977;123:779-7821 2. Eldevik OP. Nakstad P. Kendall BE, Hindmarsh T. lohexol in lumbar
myelography: preliminary results from an open, noncomparative multicen-
ter clinical study. AJNR 1983;4:299-30113. Witwer G, Cacayorin ED, Bernstein AD, Hubballah MY, Yuan HA, Kieffer
SA. lopamidol and metrizamide for myelography: prospective double-blind
clinical trial. AJNR i984;5:403-407
1 4. Undblom K. Discography of dissecting transosseous rupture of disks inlumbar region. Acta Radiol 195i;36:12-16
1 5. Gargano FP, Meyer JD, Sheldon JJ. Transfemoral ascending lumbar
catheterization of the epidural veins in lumbar disk disease. Radiology
i974;1 11:329-33616. Djindjian R. Arteriography of the spinal cord. AJR i969;107:461-47817. Patton DD, Woolfenden J. Radionuclide bone scanning in diseases of the
spine. Radiol Clln North Am i977;2: 177-20218. Pretorius DH, Rumack CM, Manco-Johnson ML, et al. Specific skeletal
dysplasias in utero: sonographic diagnosis. Radiology i986;159:237-242
1 9. Dohrmann GJ, Rubin J. Dynamic intraoperative imaging and instrumenta-
tion of brain and spinal cord using ultrasound. Neurol Clin i985;3:425-437
20. Hounsfield GN. Computerized transverse axial scanning. Part I. Descriptionof system. Br J Radio! i973;46: 1016-1022
21 . Ambrose J. Computerized axial scanning. Part II. Clinical applicatiOn. Br JRadio! i973;46:1023-i047
22. Rothman SLG, Glenn WV. CT multiplanar reconstruction in 253 cases of
lumbar spondylolysis. AJNR i984;5: 81-9023. DiChiro G, Schellinger D. Computed tomography ofspinal cord after lumbar
intrathecal introduction of metrizamide (computed assisted myelography).Radiology i976;120: 101 -1 04
24. Teplick JG, Haskin ME. Intravenous contrast-enhanced CT of the postop-erative lumbar spine: improved identification of recurrent disk herniation,scar, arachnoiditis, and diskitis. AJNR 1984;5:373-383
25. Bloch F. Nuclear induction. Phys Rev i946;70:460-474
26. Purcell EM, Torrey HC, Pound RV. Resonance absorption by nuclearmagnetic moments in solids. Phys Rev 1946;69:37-38
27. Lauterbur PC. Image formation by induced local interactions: examplesemploying nuclear magnetic resonance. Nature i973;242: 190-191
28. MOdiC MT, Pavlicek W, Weinstein MA, et al. Magnetic resonance imaging
of intervertebral disk disease: clinical and pulse sequence considerations.Radiology i984;152: 103-111
29. Edelman RR, Shoukimas GM, Stark DD, et al. High resolution surface-coilimaging of lumbar disk disease. AJR i985;1 44:1123-1129
30. Perkins GP, Wehrli FW. CSF enhancement in short TR gradient-echoimages. Magn Reson Imaging l986;4:465-467
31 . Rubin JB, Enzmann DR, Wright A. CSF-gated MR imaging of the spine:
theory and clinical implementation. Radiology i987;163:784-79232. Enzmann DR, Rubin JB, Wright A. Use of cerebrospinal fluid gating to
improve T2-weighted images. Part I. The spinal cord. Radiologyi987;162:763-767
33. Smoker WRK, Godersky JC, Knutzon RK, Keyes WD, Norman D, Bergman
W. The role of MR imaging in evaluating metastatic spinal disease. AJNRi987;8:901-908
34. Haughton VM, Eldevik P0, Magnaes B, Amundsen P. A prospective
comparison of computed tomography and myelography in the diagnosis
of herniated lumbar disc.Radiology i982;142: 103-110
35. Firooznia H, Benjamin V, Kricheff II,Rafli M, Golimbu C. CT of lumbar
spine disk herniation: correlation with surgical findings. AJNR i984;5:91-
96; AJR i984;142:587-592
36. Williams AL, Haughton VM, Pojunas KW, Daniels DL, Kilgore DP. Differ-
entiation of intramedullary neoplasms and cysts by MR. AJNR 1987;8:527-532
37. Lee BCP, zimmerman RD, Manning JJ, Deck MD. MR imaging of syrin-gornyelia and hydromyelia. AJNR i985;6:221-228
38. Chakeres DW, Flickinger F, Bresnahan JC, Beattie MS. MR imaging ofacute spinal cord trauma. AJNR i987;8:5-10
39. DeLaPaz RL, FInds R, Norman D, Enzmann D. High field MRI of spinal
cord multiple sclerosis (abstr). Presented at the annual meeting of theSociety of Magnetic Resonance in Medicine, New York City, August 1987
40. Altman NR, Altman DH. MR imaging of spinal dysraphism. AJNR
i987;8:533-53841 . Quencer RM, El Gammal T, Cohen G. Syringomyelia associated with
intradural extramedullary masses of the spinal cord. AJNR i986;7:
143-148
42. Gebarski 55, Maynard FW, Gabrielsen TO, Knake JE, Latack JT, Hoff JT.Posttraumatic progressive myelopathy: clinical and radiologic correlation
employing MR imaging, delayed CT metrizamide myelography, and intra-operative sonography. Radiology i985;157:379-385
43. Regenbogen VS, Rogers LF, Atlas SW, Kim KS. Cervical spinal cordinjuries in patients with cervical spondylosis. AJR i986;146:277-284
44. Williams AL The postoperative spine: imaging update. Presented at theannual meeting of the American Society of Neuroradiology, New York City,
May 1987
45. Hueftle MG, Medic MT, Ross JS, et al. Postoperative epidural fibrosisversus recurrent disc hemiation in the lumbar spine: assessment with Gd-
DTPA enhanced MR imaging (abstr). Presented at the annual meeting of
the Radiological Society of North America, Chicago, December 198746. Sze G, Abramson A, Krol G, et al. Gadolinium-DTPA in the evaluation of
intradural extramedullary spinal disease. AJNR i988;9: 153-16347. Ross JS, Masaryk TJ, MOdIC MT, et al. MR imaging of lumbar arachnoiditis.
AJNR i987;8:885-89248. Enzmann DR, O’Donohue J, RubEn JB, Shuer L, Cogen P, Silverberg G.
CSF pulsations within nonneoplastic spinal cord cysts. AJNR l987;8:51 7-525
49. Jenkins JPR, Stack JP, Watson Y, Isherwood I. Magnetic resonanceimaging of spinal lesions: the role of gadolinium-DTPA (abstr). Presented
at the annual meeting of the Society of Magnetic Resonance in Medicine,New York City, August 1987
50. Bydder GM, Brown J, Niendort HP, Young IR. Enhancement of cervicalintraspinal tumors in MR imaging with intravenous gadolinium-DTPA. JComput Assist Tomogr i985;9:847-851
51 . Tashiro K, Ito K, Maruo Y, et al. MR imaging of the spinal cord in Devicdisease. JComputAssist Tomogr i987;11 :516-517
52. Merine D, Wang H, Kumar AJ, zinreich SJ, Rosenbaum AE. CT myelog-
raphy and MR imaging of acute transverse myelitis. J Comput AssistTomogr i987;1 I :606-608
53. Sherman JL, Drachman DB, Citrin CM. MR evaluation of amyotrophiclateral sclerosis (ALS). Presented at the annual meeting of the American
Society of Neuroradiology, New York City, May 198754. Kulkarni MV, McArdle CB, Kopanicky D, et al. Acute spinal cord injury: MR
imaging at 1 .5 T. Radiology i987;164:837-84355. Bottomley PA, Herfkens RJ, Smith LS, Bashore TM. Altered phosphate
metabolism in myocardial infarction. P-3i MR spectroscopy. Radiologyi987;165:703-707
56. Oberhaensli AD, Hilton-Jones D, Bore PJ, Radda GK. P-31 magneticresonance studies of human braln at 2T. Magn Reson Imaging
i986;4:417-41957. Vink R, Knoblach SM, Feden Al. 31P magnetic resonance spectroscopy of
traumatic spinal cord injury. Magn Reson Med i987;5:390-394
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by U
CSF
LIB
& C
KM
/RSC
S M
GM
T o
n 11
/21/
14 f
rom
IP
addr
ess
169.
230.
243.
252.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved