Embed Size (px)
Citation preview
© TrustHCS 2019© TrustHCS 2019
Presented by:
Nena Scott, PHd, MSEd, RHIA, CCS, CCS-P, CCDS, CRC
Spinal Procedures: A Coding Walk-Through
© TrustHCS 2019
Objectives
At the completion of this presentation the learner will:
• Review the anatomy of spine
• Review ICD-10-PCS and CPT coding guidelines and coding clinics for spinal procedures
• Assign ICD-10-PCS and CPT codes to coding scenarios for spinal procedures
© TrustHCS 2019© TrustHCS 2019
Anatomy
© TrustHCS 2019
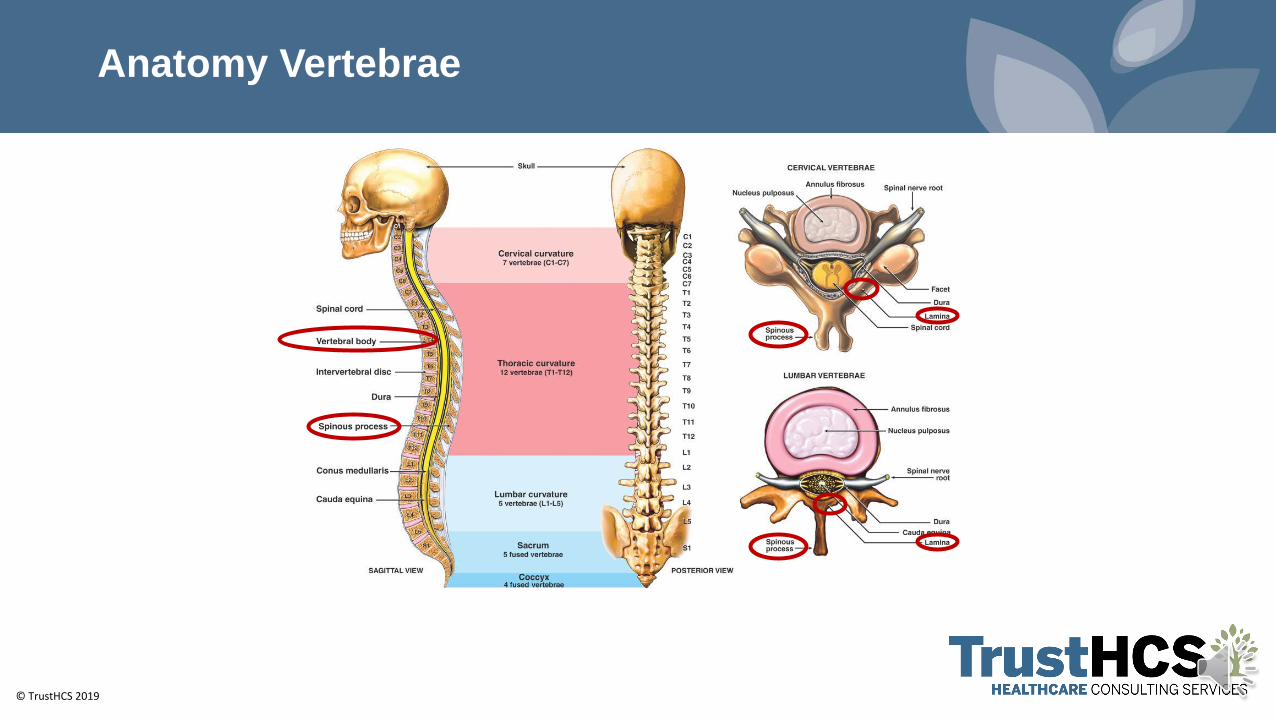
Anatomy Vertebrae
© TrustHCS 2019
Spinal Fusion and Anatomy

© TrustHCS 2019© TrustHCS 2019
Common Terminology
© TrustHCS 2019
Common - Medical Terms
• Spondylolisthesis – forward displacement of one vertebra over another
• Spondylosis – (arthritis) with or without myelopathy (any functional disturbance or pathological change in the spinal cord) or radiculopathy (disorder of the spinal nerve roots)
• Degenerative Disc Disorders (DDD) - with or without myelopathy or radiculopathy
• Spinal Instability – unstable spine due to disc disorders
• Spinal Stenosis – narrowing of the vertebral canal, nerve root canals, or intervertebral foramina, caused by encroachment of bone upon the space
© TrustHCS 2019
Common - Spinal Procedures
• Discectomy - removal of a herniated intervertebral disc
• Laminectomy - removal of the thin bony plate on the back of the vertebra called the laminae to increase space within the spinal canal and relieve pressure
• Laminotomy - removal of a portion of the vertebral arch (lamina) that covers the spinal cord
• Foraminotomy - removal of bone or tissue at/in the passageway (called the neuroforamen) where nerve roots branch off the spinal cord and exit the spinal column
© TrustHCS 2019
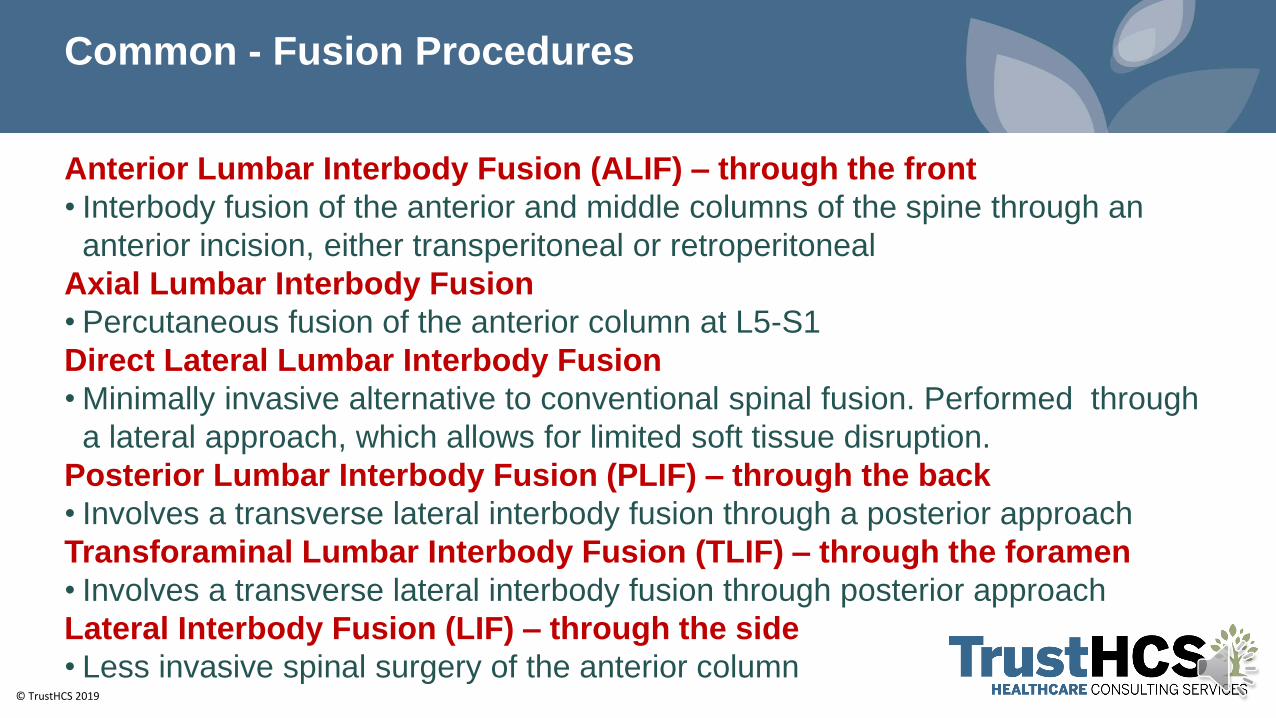
Common - Fusion Procedures
Anterior Lumbar Interbody Fusion (ALIF) – through the front
• Interbody fusion of the anterior and middle columns of the spine through an
anterior incision, either transperitoneal or retroperitoneal
Axial Lumbar Interbody Fusion
• Percutaneous fusion of the anterior column at L5-S1
Direct Lateral Lumbar Interbody Fusion
• Minimally invasive alternative to conventional spinal fusion. Performed through
a lateral approach, which allows for limited soft tissue disruption.
Posterior Lumbar Interbody Fusion (PLIF) – through the back
• Involves a transverse lateral interbody fusion through a posterior approach
Transforaminal Lumbar Interbody Fusion (TLIF) – through the foramen
• Involves a transverse lateral interbody fusion through posterior approach
Lateral Interbody Fusion (LIF) – through the side
• Less invasive spinal surgery of the anterior column
© TrustHCS 2019
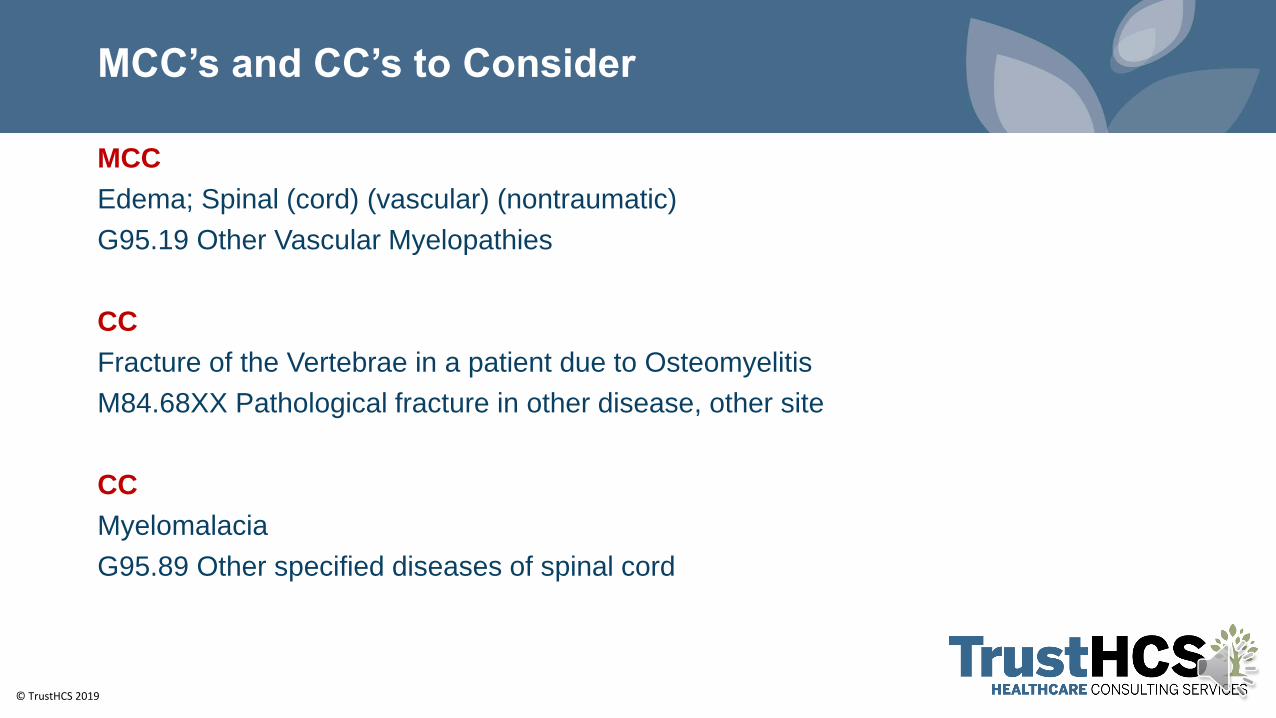
MCC’s and CC’s to Consider
MCC
Edema; Spinal (cord) (vascular) (nontraumatic)
G95.19 Other Vascular Myelopathies
CC
Fracture of the Vertebrae in a patient due to Osteomyelitis
M84.68XX Pathological fracture in other disease, other site
CC
Myelomalacia
G95.89 Other specified diseases of spinal cord
© TrustHCS 2019© TrustHCS 2019
ICD-10-PCS
© TrustHCS 2019
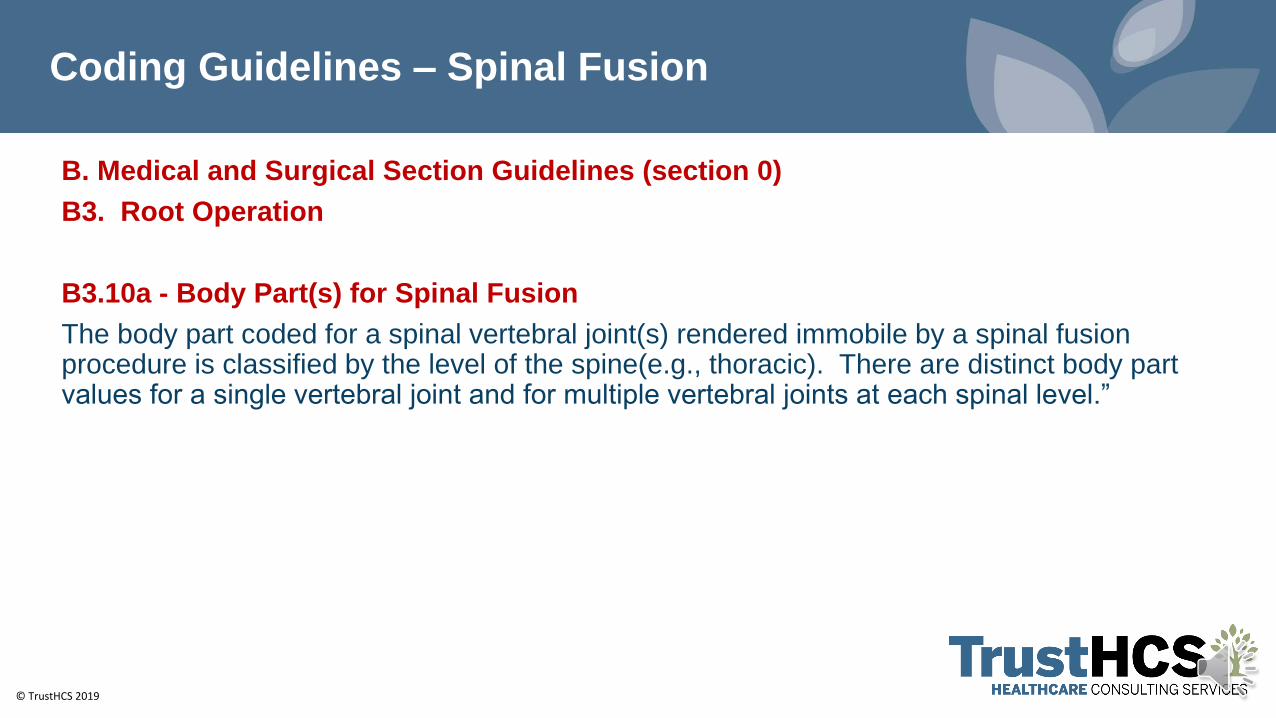
Coding Guidelines – Spinal Fusion
B. Medical and Surgical Section Guidelines (section 0)
B3. Root Operation
B3.10a - Body Part(s) for Spinal Fusion
The body part coded for a spinal vertebral joint(s) rendered immobile by a spinal fusion procedure is classified by the level of the spine(e.g., thoracic). There are distinct body part values for a single vertebral joint and for multiple vertebral joints at each spinal level.”
© TrustHCS 2019
Character 4 – Body Part
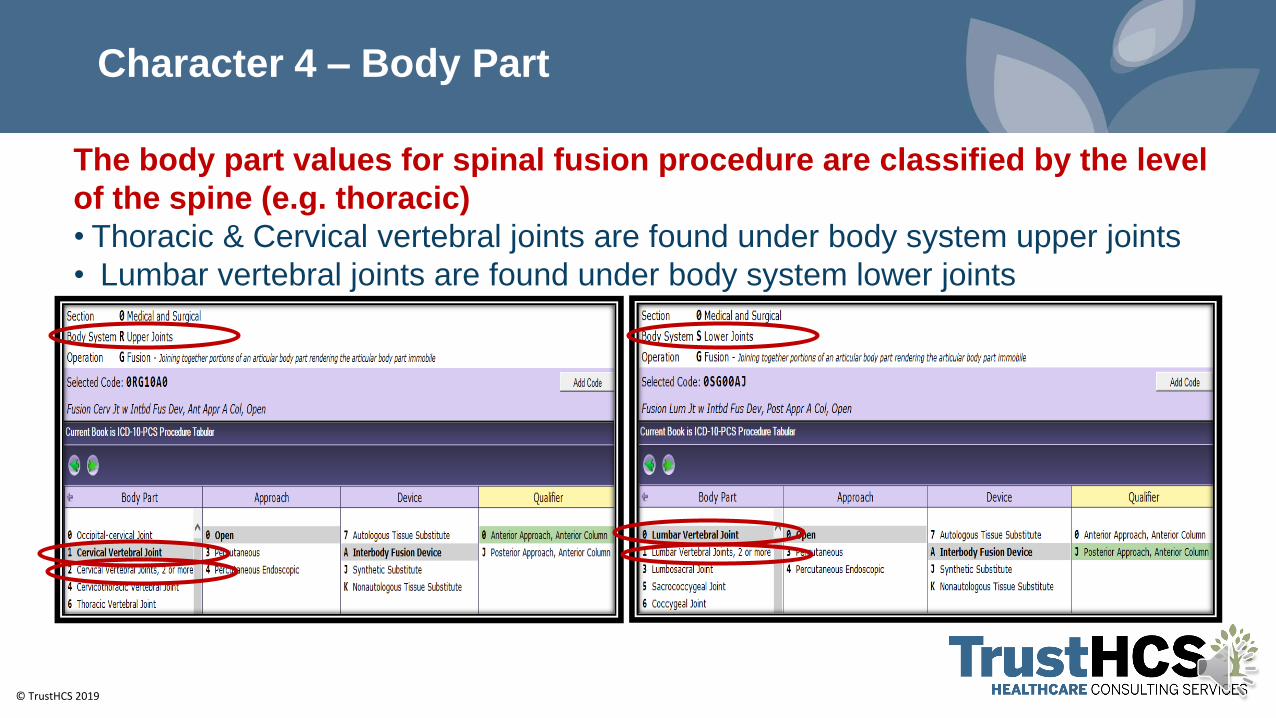
The body part values for spinal fusion procedure are classified by the level
of the spine (e.g. thoracic)
• Thoracic & Cervical vertebral joints are found under body system upper joints
• Lumbar vertebral joints are found under body system lower joints
© TrustHCS 2019
Character 6 - Device
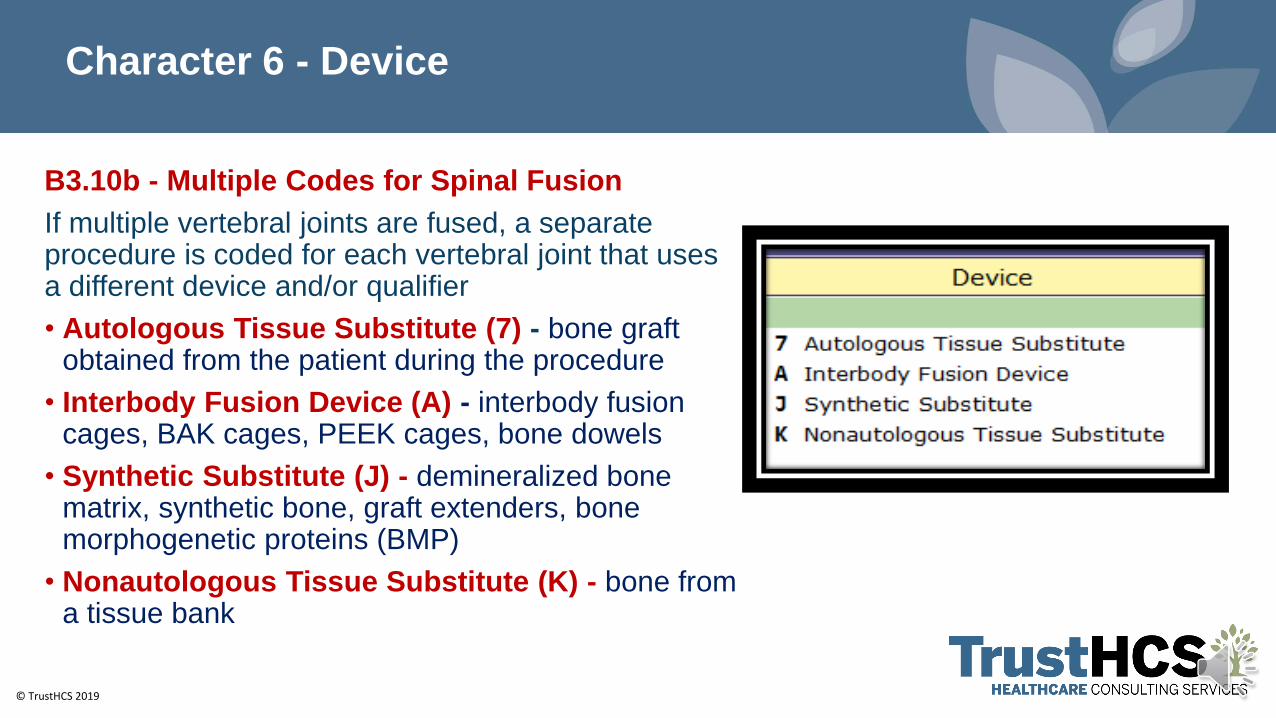
B3.10b - Multiple Codes for Spinal Fusion
If multiple vertebral joints are fused, a separate procedure is coded for each vertebral joint that uses a different device and/or qualifier
• Autologous Tissue Substitute (7) - bone graft obtained from the patient during the procedure
• Interbody Fusion Device (A) - interbody fusion cages, BAK cages, PEEK cages, bone dowels
• Synthetic Substitute (J) - demineralized bone matrix, synthetic bone, graft extenders, bone morphogenetic proteins (BMP)
• Nonautologous Tissue Substitute (K) - bone from a tissue bank
© TrustHCS 2019
Character 6 - Device
Combinations of devices and materials are often used on a vertebral joint to
render the joint immobile. When combinations of devices are used on the
same vertebral joint, the device value coded for the procedure is as follows:
• If an interbody fusion device is used to render the joint immobile (alone or
containing other material like bone graft), the procedure is coded with the
device value Interbody Fusion Device
• If bone graft is the only device used to render the joint immobile, the
procedure is coded with the device value Nonautologous Tissue Substitute or
Autologous Tissue Substitute
• If a mixture of autologous and nonautologous bone graft (with or without
biological or synthetic extenders or binders) is used to render the joint
immobile, code the procedure with the device value Autologous Tissue
Substitute
© TrustHCS 2019
Character 7 - Qualifier
• Anterior Approach, Anterior Column (0)
• Entry through the front of the body to perform a procedure on the body of the vertebra or disc
• Posterior Approach, Posterior Column (1)
• Entry through the back of the body to perform a procedure on the vertebral foramen, spinous process, facets and/or lamina
• Posterior Approach, Anterior Column (J)
• Entry through the back of the body to perform a procedure on the body of the vertebra or the disc
© TrustHCS 2019
Spinal Fusions –What Should be Coded Separately?
• Separate procedure for each vertebral joint that uses a different device and/or qualifier
• Bone harvested for a spinal fusion from a different anatomical site
• Discectomy performed at the time of a spinal fusion
• Partial removal of the disc should be reported using root operation excision
• Total discectomy is performed it should be reported using root operation resection
• Decompression laminectomy performed to treat a separately documented diagnosis of spinal stenosis
© TrustHCS 2019
Spinal Fusions –What Should NOT be Coded Separately?
• Instrumentation (rods, plates, screws)
• Foraminotomy
• Laminectomy performed to reach site of the procedure

© TrustHCS 2019© TrustHCS 2019
CPT
© TrustHCS 2019
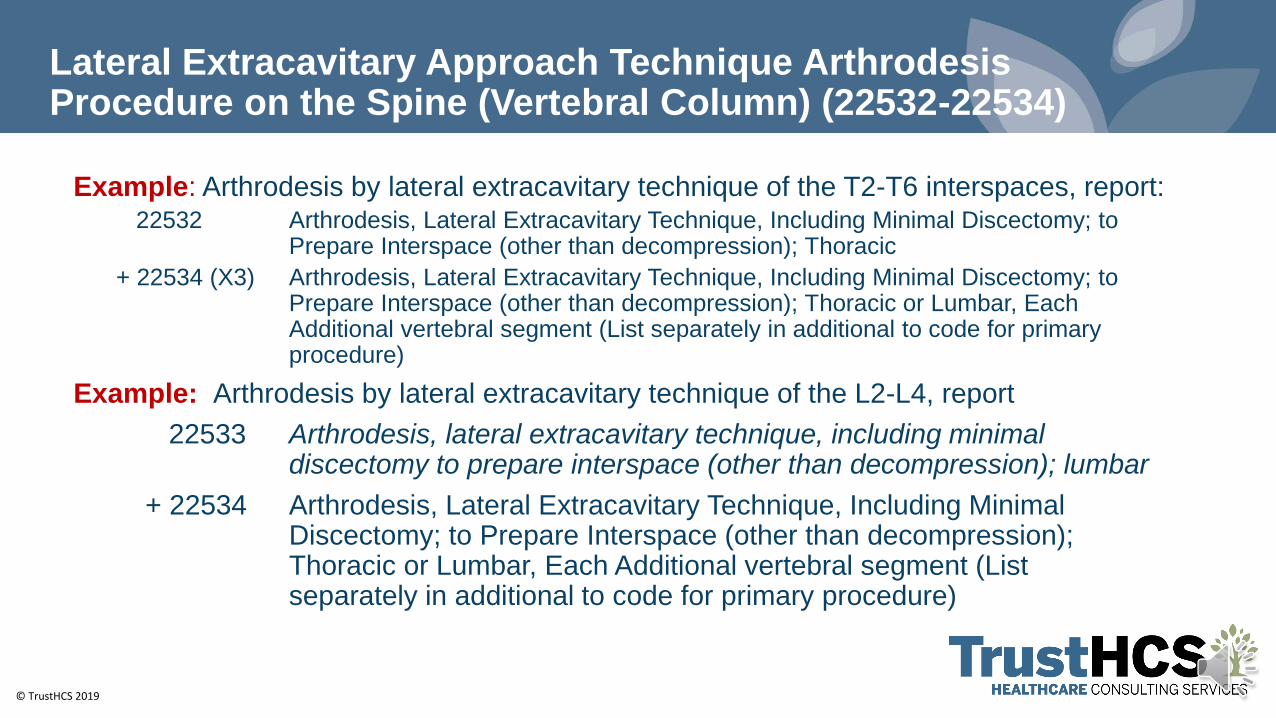
Lateral Extracavitary Approach Technique Arthrodesis Procedure on the Spine (Vertebral Column) (22532-22534)
Example: Arthrodesis by lateral extracavitary technique of the T2-T6 interspaces, report:22532 Arthrodesis, Lateral Extracavitary Technique, Including Minimal Discectomy; to
Prepare Interspace (other than decompression); Thoracic
+ 22534 (X3) Arthrodesis, Lateral Extracavitary Technique, Including Minimal Discectomy; to Prepare Interspace (other than decompression); Thoracic or Lumbar, Each Additional vertebral segment (List separately in additional to code for primary procedure)
Example: Arthrodesis by lateral extracavitary technique of the L2-L4, report
22533 Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than decompression); lumbar
+ 22534 Arthrodesis, Lateral Extracavitary Technique, Including Minimal Discectomy; to Prepare Interspace (other than decompression); Thoracic or Lumbar, Each Additional vertebral segment (List separately in additional to code for primary procedure)
© TrustHCS 2019
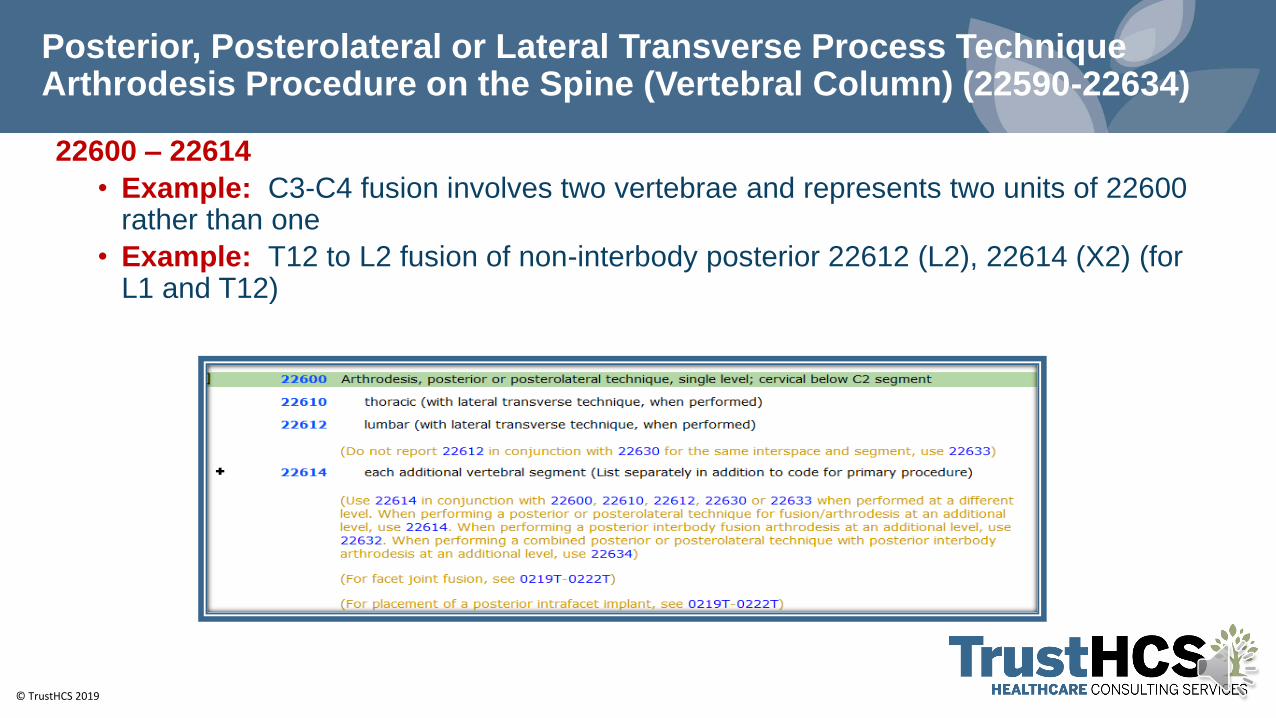
Posterior, Posterolateral or Lateral Transverse Process Technique Arthrodesis Procedure on the Spine (Vertebral Column) (22590-22634)
22600 – 22614
• Example: C3-C4 fusion involves two vertebrae and represents two units of 22600 rather than one
• Example: T12 to L2 fusion of non-interbody posterior 22612 (L2), 22614 (X2) (for L1 and T12)
© TrustHCS 2019
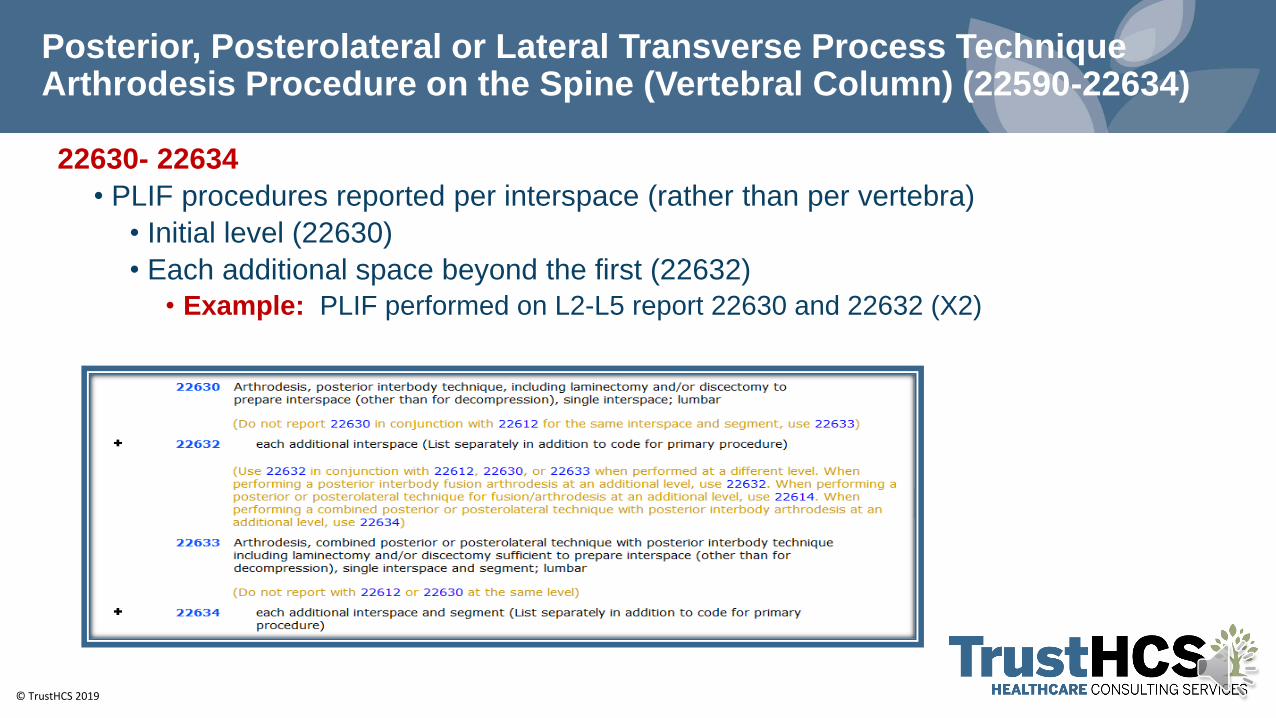
Posterior, Posterolateral or Lateral Transverse Process Technique Arthrodesis Procedure on the Spine (Vertebral Column) (22590-22634)
22630- 22634
• PLIF procedures reported per interspace (rather than per vertebra)
• Initial level (22630)
• Each additional space beyond the first (22632)
• Example: PLIF performed on L2-L5 report 22630 and 22632 (X2)
© TrustHCS 2019
Anterior or Anterolateral Approach Technique Arthrodesis Procedures on the Spine (Vertebral Column) (22548-22586)
Anterior approach – patient supine (lying face up) and access the spine through an incision in the front of the body
• To access the upper cervical vertebrae C1-C2 occurs through the mouth (transoral or extraoral) (22548)
• To access the cervical vertebrae below C2 via anterior approach, the surgeon makes an incision in the neck, just below the jaw line (22554)
• To access the thoracic vertebrae the exact location may vary according to the vertebrae the surgeon addresses (22556)
• To access the lumbar vertebrae the incision is placed over the abdomen, reaching the spine through either a transperitoneal (through the abdomen) or retroperitoneal (behind the abdomen) exposure. (Commonly referred to as ALIF) (22558)
• Each additional interspace use an additional code (22585)
• Procedures included and not coded separately minimal discectomy
• Procedures coded separately for placement of bone grafts (20930-20938) and instrumentation (22840-22851)
© TrustHCS 2019© TrustHCS 2019
Coding Clinic Review
© TrustHCS 2019
Coding Clinic – Spinal Fusion
Clarification: Spinal Fusion Procedures without Bone Graft
Coding Clinic for ICD-10-CM/PCS, First Quarter 2018: Page 22
Summary:
Answer:
• Specific guideline for spinal fusion that goes beyond the basic root operation definition of
"Fusion." While the root operation of "fusion" does not require the use of bone graft, the spinal
fusion guideline indicates that a spinal fusion requires bone graft
• As of October 1, 2018, the device value "Z, No device" was deleted from table ORG, fusion of
upper joints and table OSG, fusion of lower joints.
• The codes were clinically invalid because a fusion procedure always requires some type of
device (for example, instrumentation with bone graft or bone graft alone) to facilitate the fusion of
the joints.
© TrustHCS 2019
Decompression of Spinal Cord and Placement of Instrumentation
Coding Clinic, Second Quarter 2017: Page 23
Summary
Review documentation to determine if fusion was performed
• Spinal fusion involves the use of bone graft or bone graft substitute, which can be done with or without instrumentation
• Instrumentation alone does not constitute a spinal fusion
• Insertion of rods and screws is not the same as the placement of a pedicle-based stabilization device
• Device value "Spinal stabilization device, pedicle based" - value is only used for specific stabilization systems
© TrustHCS 2019
Coding Clinic – Spinal Fusion
Cervical Spinal Fusion, Decompression and Placement of Interfacet Stabilization Device
Coding Clinic for ICD-10-CM/PCS, Second Quarter 2019: Page 19
Decompressive Laminectomy of Both Spinal Cord and Nerve Roots
Coding Clinic for ICD-10-CM/PCS, First Quarter 2019: Page 28
Decompressive Laminectomy (Release of Spinal Cord versus Release of Spinal Meninges)
Coding Clinic for ICD-10-CM/PCS, Third Quarter 2018: Page 30
Decompressive Laminectomy/Foraminotomy and Lumbar Discectomy
Coding Clinic, Second Quarter 2016: Page 16
Removal of Longitudinal Ligament to Decompress Cervical Nerve Root
Coding Clinic, Second Quarter 2016: Page 17
© TrustHCS 2019© TrustHCS 2019
Example Scenario’s
© TrustHCS 2019
Scenario #1
Preoperative DiagnosesHerniated nucleus pulposus, C5-6Bilateral cervical radiculopathy
Postoperative DiagnosesHerniated nucleus pulposus, C5-6Bilateral cervical radiculopathy
Procedures
Anterior C5-6 discectomy with decompression of spinal cord & bilateral nerve roots
Anterior interbody fusion C5-6 and PEEK interbody device C5-6 using locally
obtained bone with demineralized bone matrix and Zavation plating
© TrustHCS 2019
Scenario #1
With the patient supine, general anesthesia was induced, and endotracheal intubation was
performed. The neck was prepped and draped. A time-out was undertaken; all participants
concurred. Standards oblique incision was made on the left side of the neck. Platysma was
incised. Sternomastoid was retracted laterally and taken to the esophagus medially. I came
down to the prevertebral fascia. Needle markers were placed. Correct level was identified.
I now carried out anterior discectomies at C5-6. I used the distraction screws to open the
interspace. There was clear neural compression. It was worse on the left than on the right
side.
Following through decompression and total discectomy, I carried out interbody fusion. I
used PEEK interbody device. This was filled with locally obtained bone and demineralized
bone matrix. I then supplemented this with an anterior Zavation plate. Excellent screw
fixation was achieved at C5 and C6. Excellent position was noted intraoperatively and on x-
ray. There had been no change on monitoring. Blood loss was minimal. The wound was
now irrigated and closed in layers. The patient was extubated and returned to the recovery
room in good condition.

© TrustHCS 2019
Fusion
© TrustHCS 2019
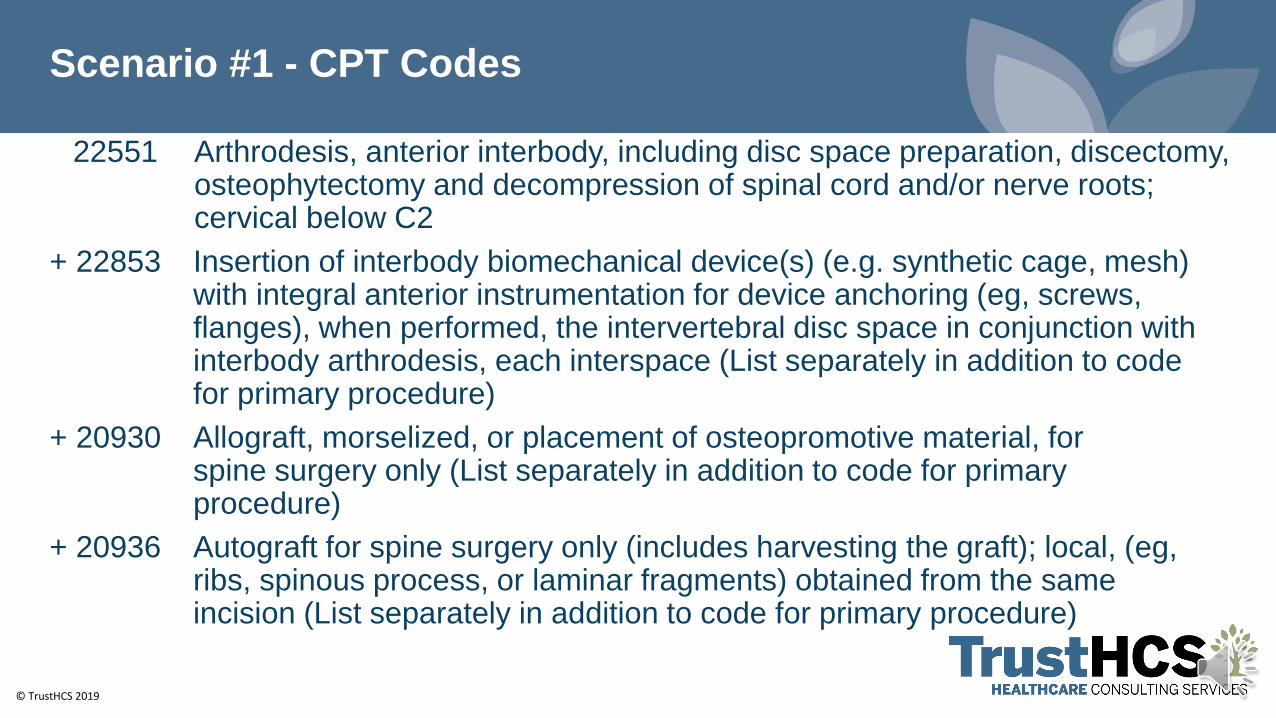
Scenario #1 - CPT Codes
22551 Arthrodesis, anterior interbody, including disc space preparation, discectomy, osteophytectomy and decompression of spinal cord and/or nerve roots; cervical below C2
+ 22853 Insertion of interbody biomechanical device(s) (e.g. synthetic cage, mesh) with integral anterior instrumentation for device anchoring (eg, screws, flanges), when performed, the intervertebral disc space in conjunction with interbody arthrodesis, each interspace (List separately in addition to code for primary procedure)
+ 20930 Allograft, morselized, or placement of osteopromotive material, for spine surgery only (List separately in addition to code for primary procedure)
+ 20936 Autograft for spine surgery only (includes harvesting the graft); local, (eg, ribs, spinous process, or laminar fragments) obtained from the same incision (List separately in addition to code for primary procedure)
© TrustHCS 2019
Scenario #1 – ICD-10-PCS
© TrustHCS 2019
Scenario #1 – ICD-10-PCS
© TrustHCS 2019
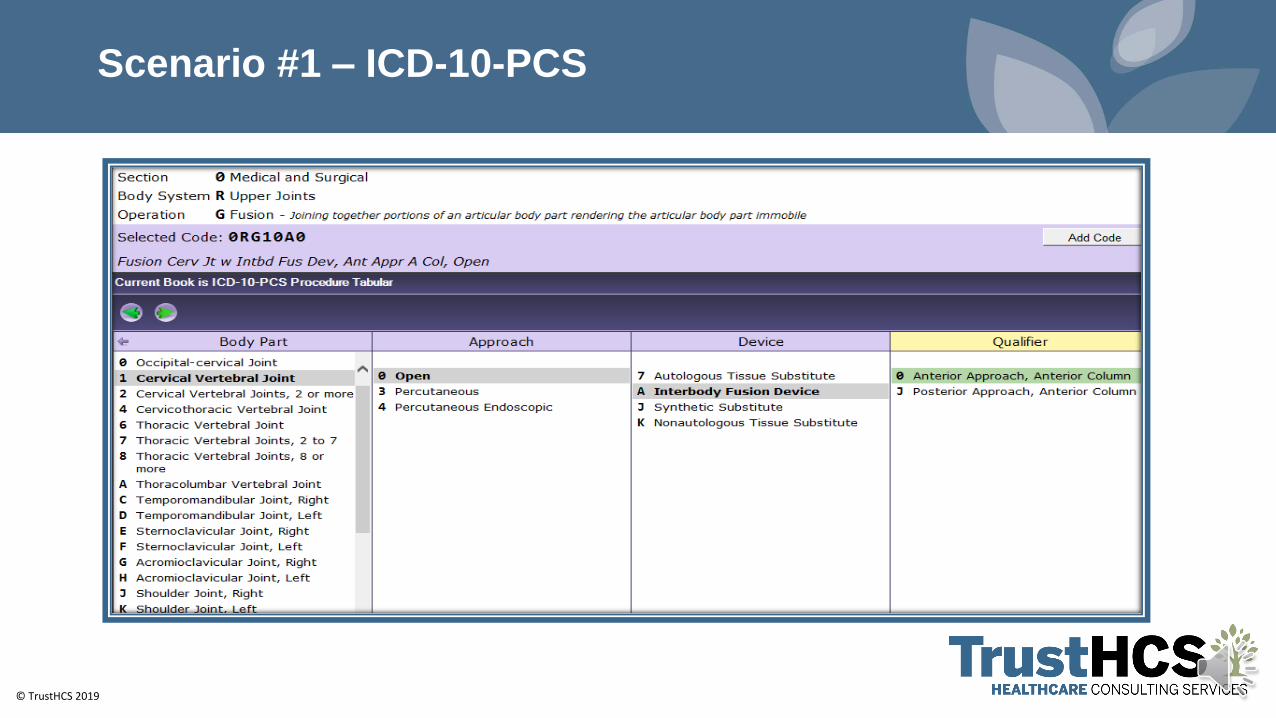
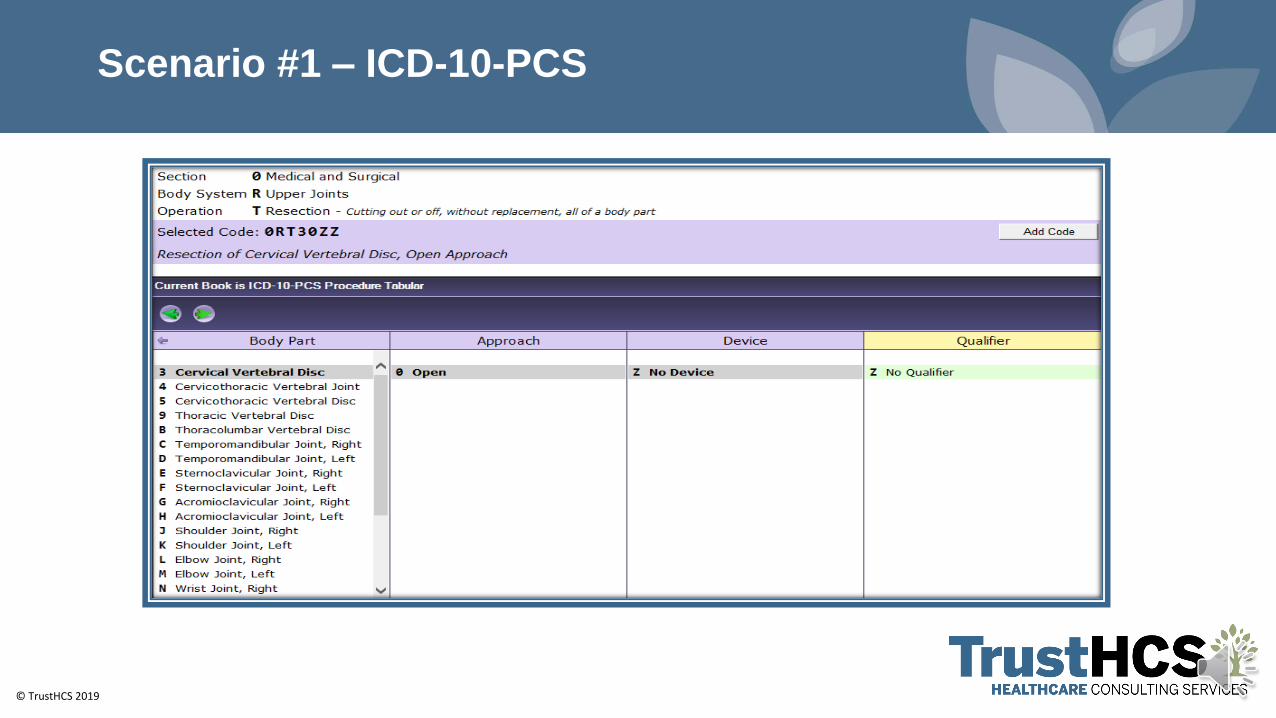
Scenario #1 – ICD-10-PCS – Summary
0RG10A0 Fusion Cervical Joint with Interbody Fusion Device, Anterior Approach, Anterior Column, Open
0RT30ZZ Resection of Cervical Vertebral Disc, Open Approach
© TrustHCS 2019
Scenario #2
Preoperative DiagnosesT12-L1 Left Herniated DiscThoracic MyelopathyT12 Radiculopathy
Postoperative DiagnosesT12-L1 Left Herniated DiscThoracic MyelopathyT12 Radiculopathy
Procedures
1. T12-L1 Complete Left Facetectomy, central laminectomy, partial transpedicular
decompression and discectomy, decompression of spinal cord
2. T12-L1 Fusion with instrumentation, pedicle screws and rods bilaterally
3. Posterior arthrosis T12-L1 with laminectomy bone, allograft, bone marrow aspirate, BMP
4. Mayfield clamp headholder
5. Left bone marrow aspirate
© TrustHCS 2019
Scenario #2
Findings
The patient has significant compression of the nerve root and spinal cord at the T12-L1 level on the left
Indication
Patient is a 44-year-old male who presents with left upper thigh numbness, erectile dysfunction, weakness of his left iliopsoas due to the large extruded T12-L1 herniate disc. The spine cord was deformed from the T12-L1 disc herniation. The patient’s symptoms were progressive. The risk were discussed, and the patient agree to proceed.
The patient was brought to the preop area. IV lines, ted stockings and SCDs were placed. The patient was brought into the OR and underwent general endotracheal tube intubation performed by anesthesia. EMG/SSEP needles were inserted in the scalp, upper extremities and lower extremities. The Head was supported to avoid pressure on the eyes (Mayfield-Antibiotic added to pins). Antibiotic ointment was added to the pins. The patient was positioned prone on the operative table. Appropriate padding was placed on the chest and pelvis, the knees were bent and he feet elevated pillows the arms were supported and padded and taped down.
© TrustHCS 2019
Scenario #2
The thoracic and lumbar sacral area was prepped and draped in standard fashion. Under fluoroscopic guidance the incision was marked at the T12-L1 level. The incision was infiltrated with local anesthetic. The incision was made with a #10 scalpel. The levels were confirmed under fluoroscopy. The Bovie was used for hemostasis and to incise the fascia. The Cobb was used to help dissect the muscle. The McCullough retractor was placed. The levels were confirmed under fluoroscopy. A drill was used to perform a central laminotomy, after removing the interspinous ligament between T12 and L1. Facetectomy of T12-L1 on left including a pars as well as both superior and inferior facets. Once the ligament was identified, I used an angled curette to incise the ligament. This was followed using the 2 and 3 Kerrison to remove the ligament exposing the central and lateral recess of the spinal cord. Immediately evident was the nerve root in addition to slight deformation of the thecal sac. Intraoperative ultrasound was performed identifying a hyperechogenic mass deforming the spinal cord at T12-L1 on the left. The microscope was brought into position. Under microscopic dissection I performed a transpedicular resection of the superior part of the L1 pedicle down to the T12-L1 disc. At this point the nerve was decompressed from the spinal cord at the T12-L1.
© TrustHCS 2019
Scenario #2
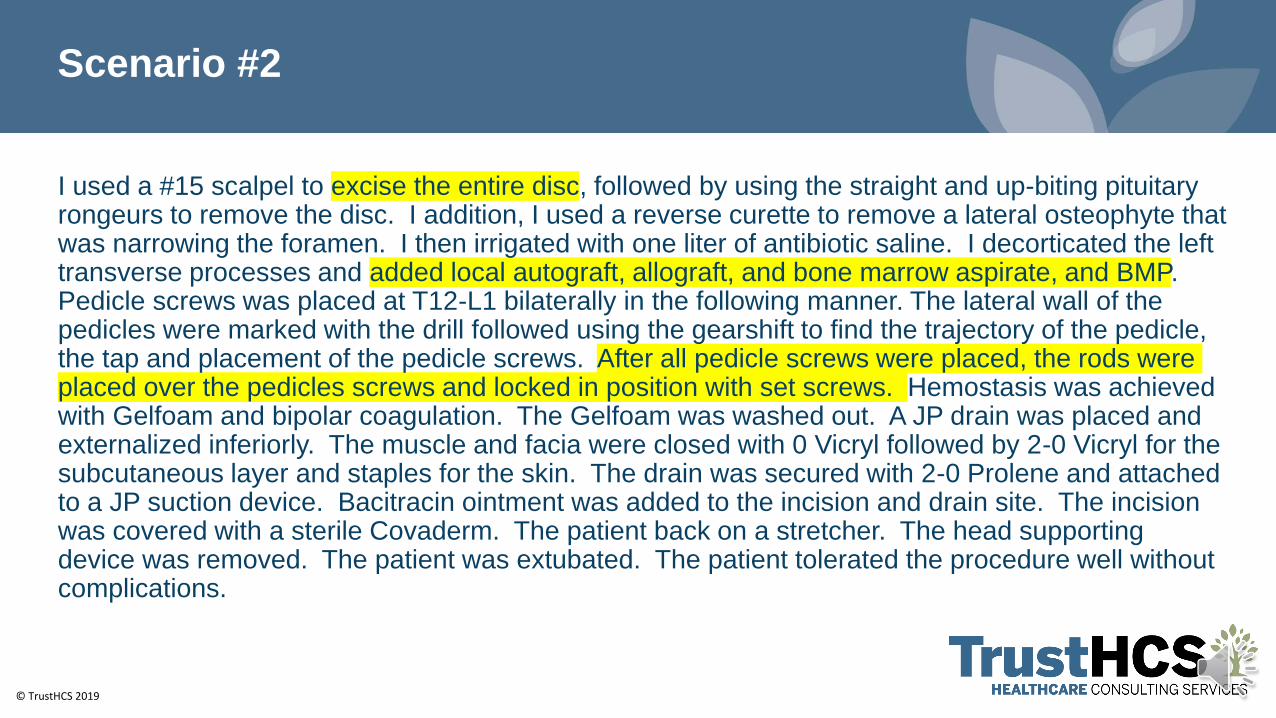
I used a #15 scalpel to excise the entire disc, followed by using the straight and up-biting pituitary rongeurs to remove the disc. I addition, I used a reverse curette to remove a lateral osteophyte that was narrowing the foramen. I then irrigated with one liter of antibiotic saline. I decorticated the left transverse processes and added local autograft, allograft, and bone marrow aspirate, and BMP. Pedicle screws was placed at T12-L1 bilaterally in the following manner. The lateral wall of the pedicles were marked with the drill followed using the gearshift to find the trajectory of the pedicle, the tap and placement of the pedicle screws. After all pedicle screws were placed, the rods were placed over the pedicles screws and locked in position with set screws. Hemostasis was achieved with Gelfoam and bipolar coagulation. The Gelfoam was washed out. A JP drain was placed and externalized inferiorly. The muscle and facia were closed with 0 Vicryl followed by 2-0 Vicryl for the subcutaneous layer and staples for the skin. The drain was secured with 2-0 Prolene and attached to a JP suction device. Bacitracin ointment was added to the incision and drain site. The incision was covered with a sterile Covaderm. The patient back on a stretcher. The head supporting device was removed. The patient was extubated. The patient tolerated the procedure well without complications.
© TrustHCS 2019
Scenario #2 - CPT Codes
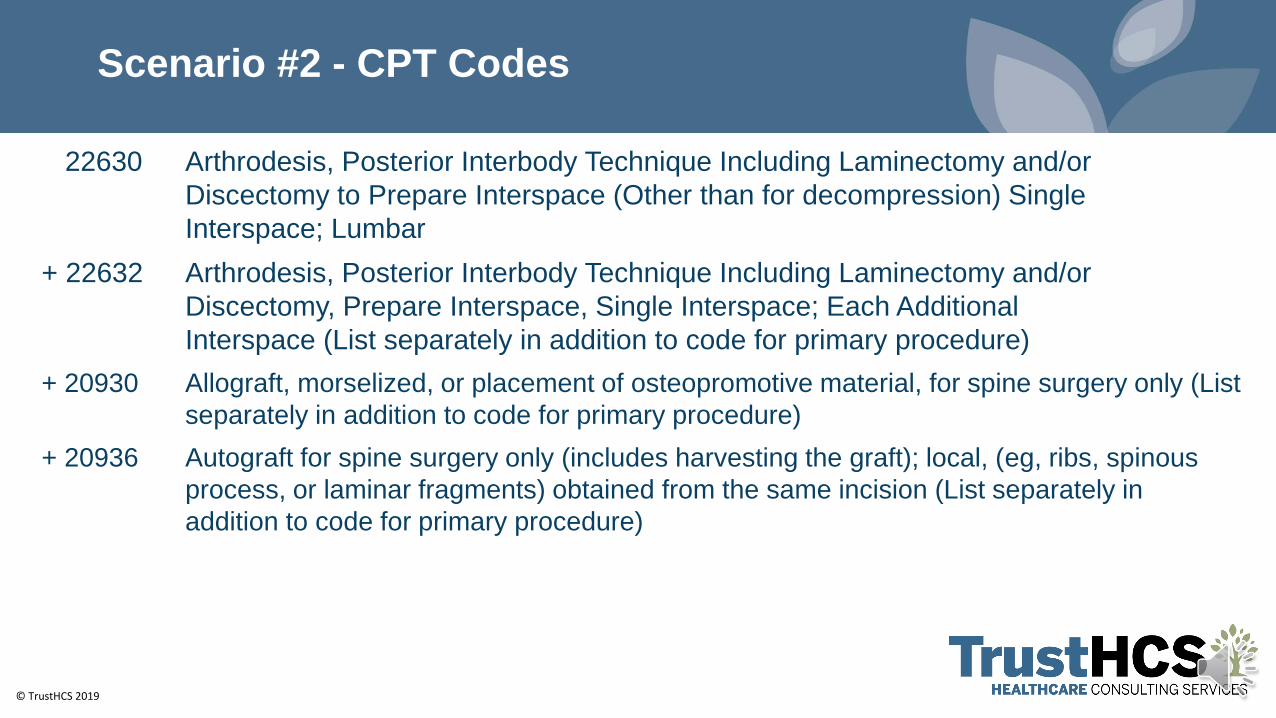
22630 Arthrodesis, Posterior Interbody Technique Including Laminectomy and/or
Discectomy to Prepare Interspace (Other than for decompression) Single
Interspace; Lumbar
+ 22632 Arthrodesis, Posterior Interbody Technique Including Laminectomy and/or
Discectomy, Prepare Interspace, Single Interspace; Each Additional
Interspace (List separately in addition to code for primary procedure)
+ 20930 Allograft, morselized, or placement of osteopromotive material, for spine surgery only (List
separately in addition to code for primary procedure)
+ 20936 Autograft for spine surgery only (includes harvesting the graft); local, (eg, ribs, spinous
process, or laminar fragments) obtained from the same incision (List separately in
addition to code for primary procedure)
© TrustHCS 2019
Scenario #2 – ICD-10-PCS
© TrustHCS 2019
Scenario #2 – ICD-10-PCS
© TrustHCS 2019
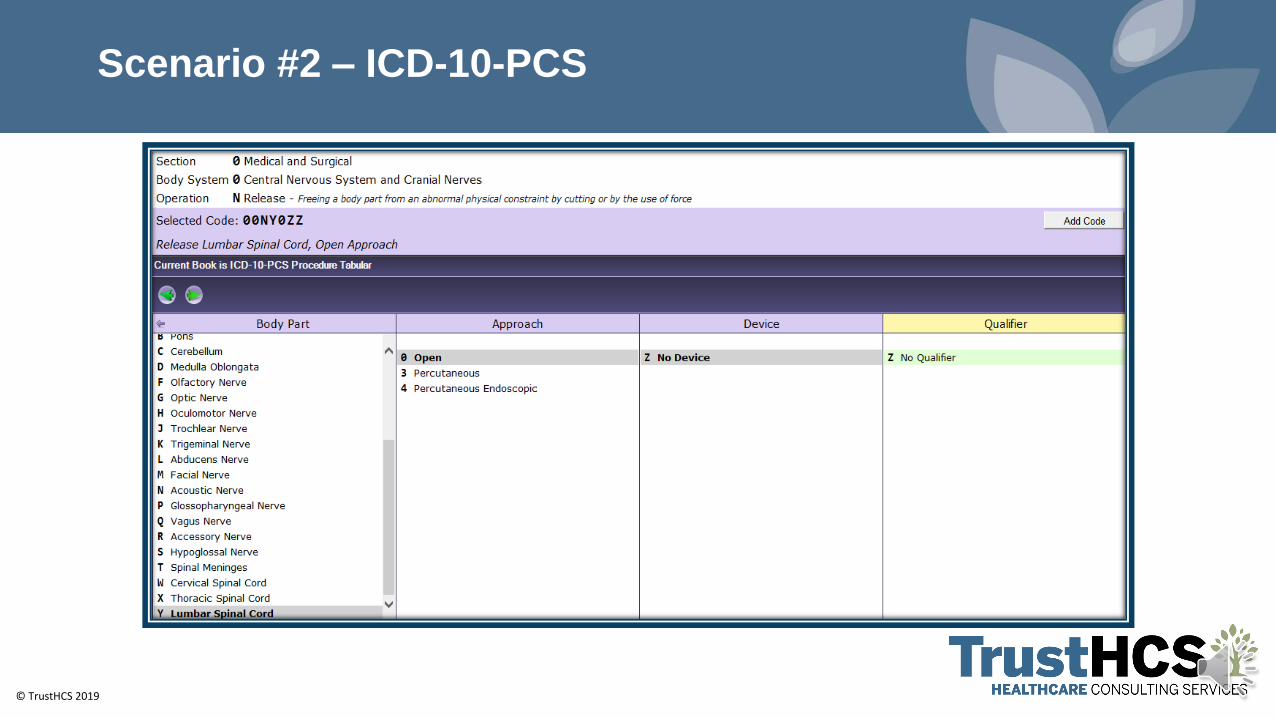
Scenario #2 – ICD-10-PCS
© TrustHCS 2019
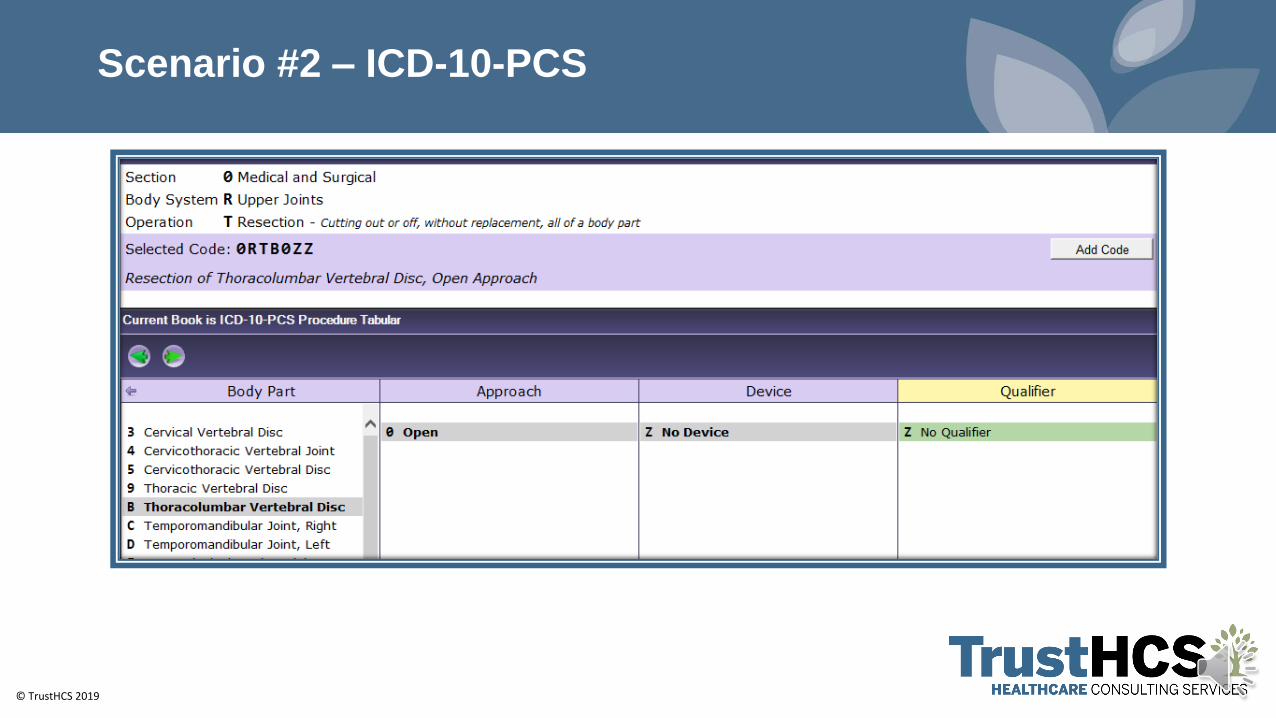
Scenario #2 – ICD-10-PCS
© TrustHCS 2019
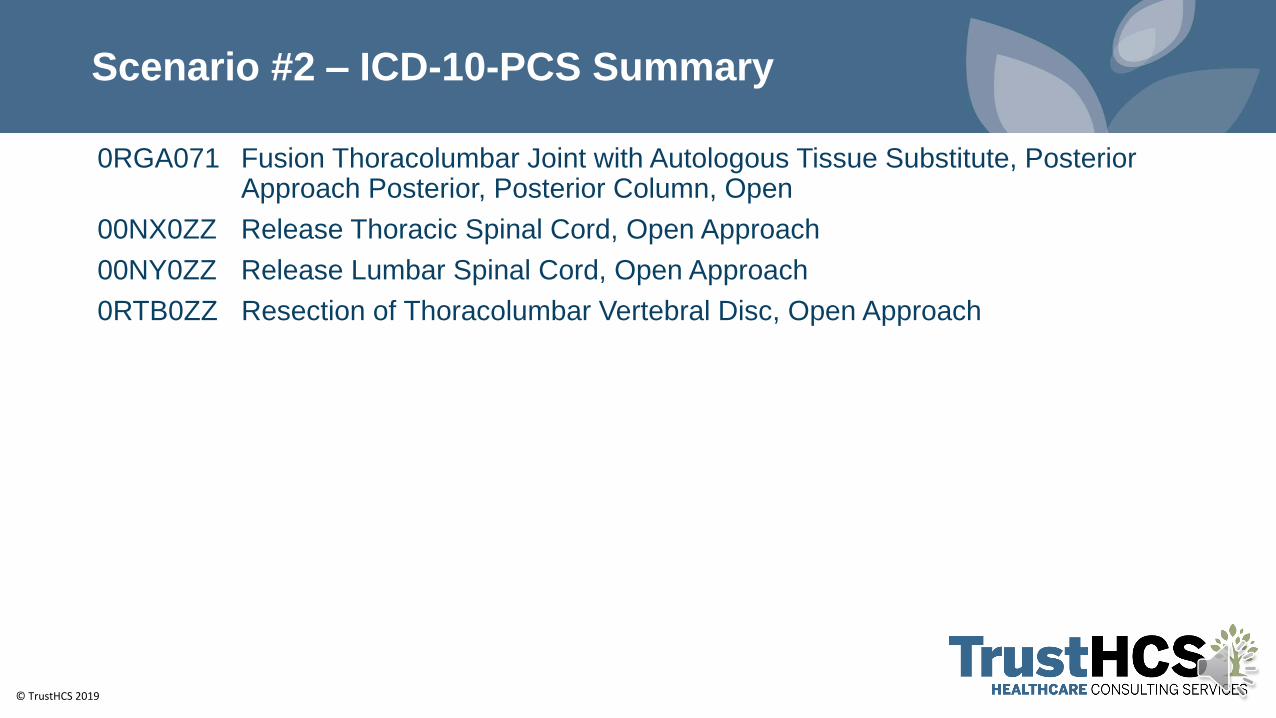
Scenario #2 – ICD-10-PCS Summary
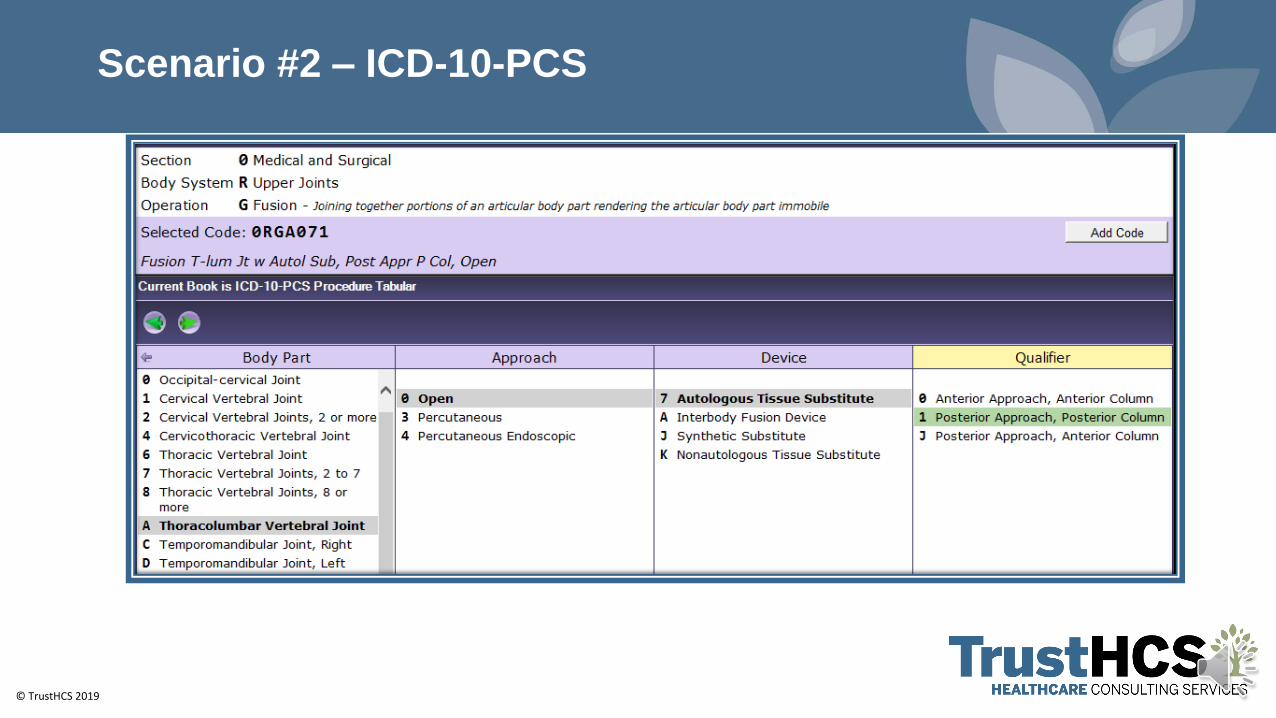
0RGA071 Fusion Thoracolumbar Joint with Autologous Tissue Substitute, Posterior Approach Posterior, Posterior Column, Open
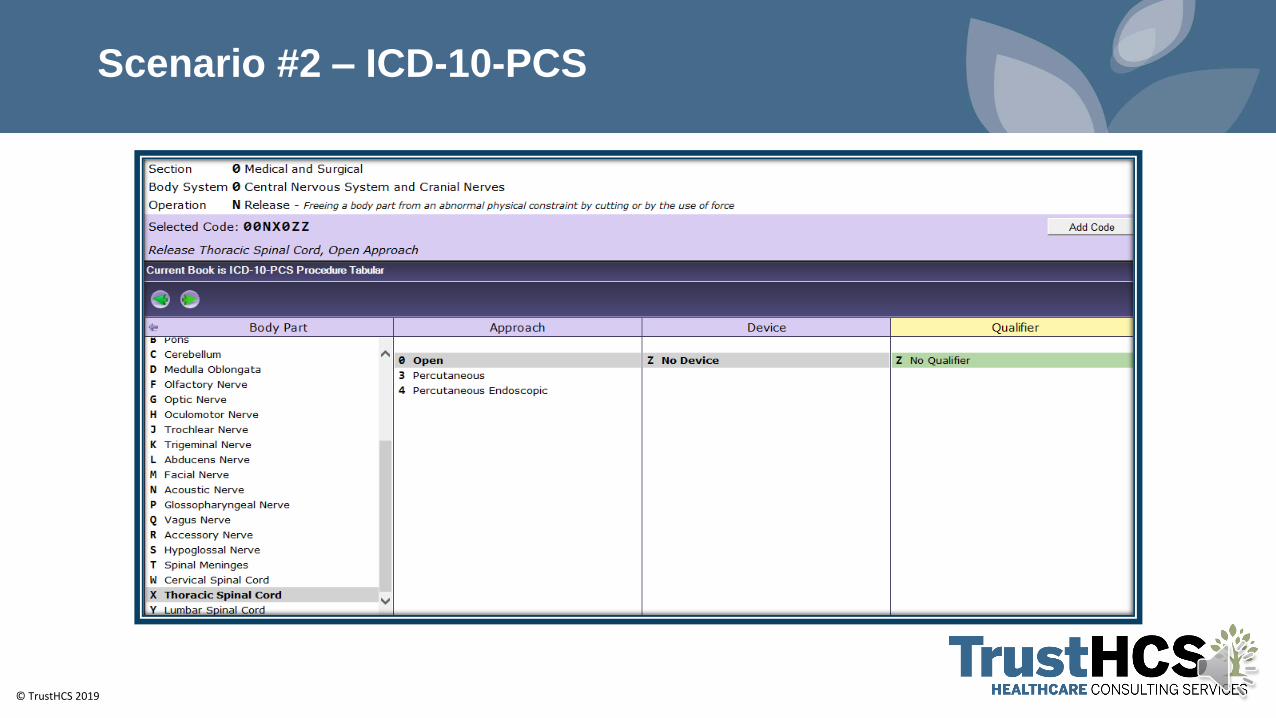
00NX0ZZ Release Thoracic Spinal Cord, Open Approach
00NY0ZZ Release Lumbar Spinal Cord, Open Approach
0RTB0ZZ Resection of Thoracolumbar Vertebral Disc, Open Approach
© TrustHCS 2019
Coding Clinic – Spinal Fusion
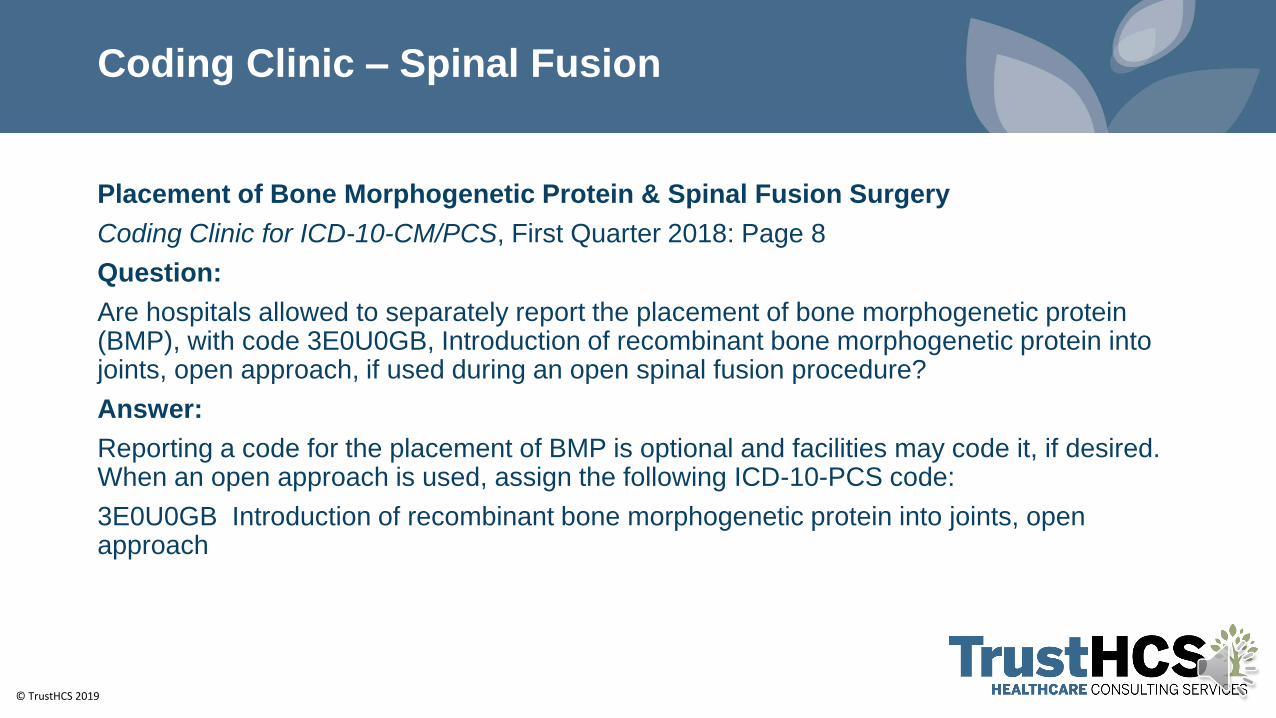
Placement of Bone Morphogenetic Protein & Spinal Fusion Surgery
Coding Clinic for ICD-10-CM/PCS, First Quarter 2018: Page 8
Question:
Are hospitals allowed to separately report the placement of bone morphogenetic protein (BMP), with code 3E0U0GB, Introduction of recombinant bone morphogenetic protein into joints, open approach, if used during an open spinal fusion procedure?
Answer:
Reporting a code for the placement of BMP is optional and facilities may code it, if desired. When an open approach is used, assign the following ICD-10-PCS code:
3E0U0GB Introduction of recombinant bone morphogenetic protein into joints, open approach
© TrustHCS 2019
Scenario #3
Preoperative and Postoperative DiagnosesGeneral spondylolisthesisLumbar stenosisNeurogenic claudicationHerniated disk, L4-L5Lumbar radiculopathy, left L4-L5Degenerative scoliosis
Procedures
Laminectomy L3, L4, L5 secondary to stenosis
Posterior spinal fusion L3-L4 secondary to instability
Non segmental instrumentation L3-L4
Correction of deformity
© TrustHCS 2019
Scenario #3
Indication
This is a 68-year-old female with severe neurogenic claudication, failed conservative treatment,
tincture, time, anti-inflammatory medications, injections. MRI confirms a general spondylolisthesis,
L3-L4 with scoliosis as well as neural foraminal narrowing at L4-L5 with what looks like acute disk
herniation on the left. Plan decompression, stabilization L3-L4 decompression L4-L5 No
guarantee given to outcome. We discussed adjacent segmental issues of infection 3% CSF leak,
nerve root injury, and imponderables.
Description of Procedure
The patient was brought to the operating room and underwent general anesthesia without difficulty,
rolled into the prone position on Jackson frame, arm placed in 90-90. Appropriate timeout was
performed. The back was the prepped and draped in normal fashion using aseptic technique.
Midline incision as carried from L3-L5 confirmed with C-arm, carried down through the
subcutaneous tissue, identifying the fascia. The fascia entered. Subperiosteal dissection
performed exposing lamina, L3, L4, and L5 body on the left and L3-L4 on the right transverse
process were identified. The L2-L3 facets were identified and protected.
© TrustHCS 2019
Scenario #3
The L3-L4 facets were stripped of soft tissue as well as using a narrow Leksell to remove the cartilage. Lateral C-arm was then brought in and 2 pedicle screws placed at L3, 2 at L4 using a sharp trocar, bone pedicle probe and a ball-tip to make sure there was a base at each pedicle, 6.2 X 45 mm screws. AP and lateral C-arm excellent and all above 14 milliamps on EMGs. I then performed a laminotomy at L4-L5 using a 2-3 Kerrison, I did extensive medial facetectomy that allowed me elevate ligamentum remove it to make sure central lateral recess structures were decompressed. I did enter the disk space; it was more of a degenerative type disc. I did not find an acute disk herniation. I did an extensive foraminotomy to make sure the Murphy ball was placed on the foramen without difficulty and I was convinced the nerve was fully decompressed. Gelfoam was placed over that defect. I then did a L3-L4 laminotomy. This was carried through the midline and out laterally to do a complete facetectomy secondary to severe foraminal narrowing. The ligament was elevated past midline incision lateral and central recess structures were decompressed and out through the foramen make sure that the nerve root was completely decompressed. I did not place a spacer.
© TrustHCS 2019
Scenario #3
The space was severely collapsed down and the way her dura was bulging out laterally I felt it would be difficult to put a spacer without having Dural injury. I did use some Tisseel at the end of the case to cover the dura just because I did not like the way it was building out laterally and exposed. There was no Dural injury noted. Screw heads were reamed, 3D heads placed prelordosed dose a 3/5 on the right, 30/40 in the left and I did use a distractor for correction of scoliosis and make sure the foramen was completely decompressed. Everything torqued appropriately through the case, irrigated out copiously with a weak Betadine solution, a gram of vancomycin powder. Fascia was closed with a locked PDS suture, skin 2-0 Vicryl and 3-0 Monocryl, Steri-Strips, sterile dressing was placed, taken to recovery room in stable condition. No complications noted.
© TrustHCS 2019
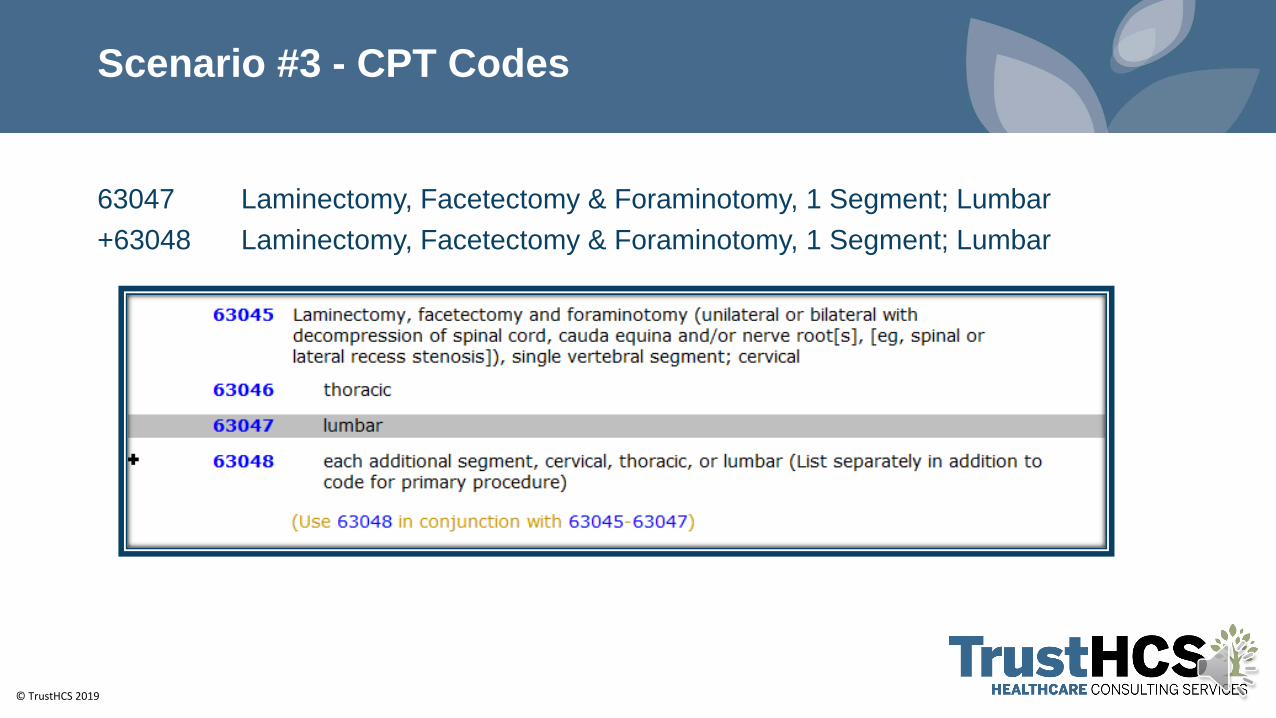
Scenario #3 - CPT Codes
63047 Laminectomy, Facetectomy & Foraminotomy, 1 Segment; Lumbar
+63048 Laminectomy, Facetectomy & Foraminotomy, 1 Segment; Lumbar
© TrustHCS 2019
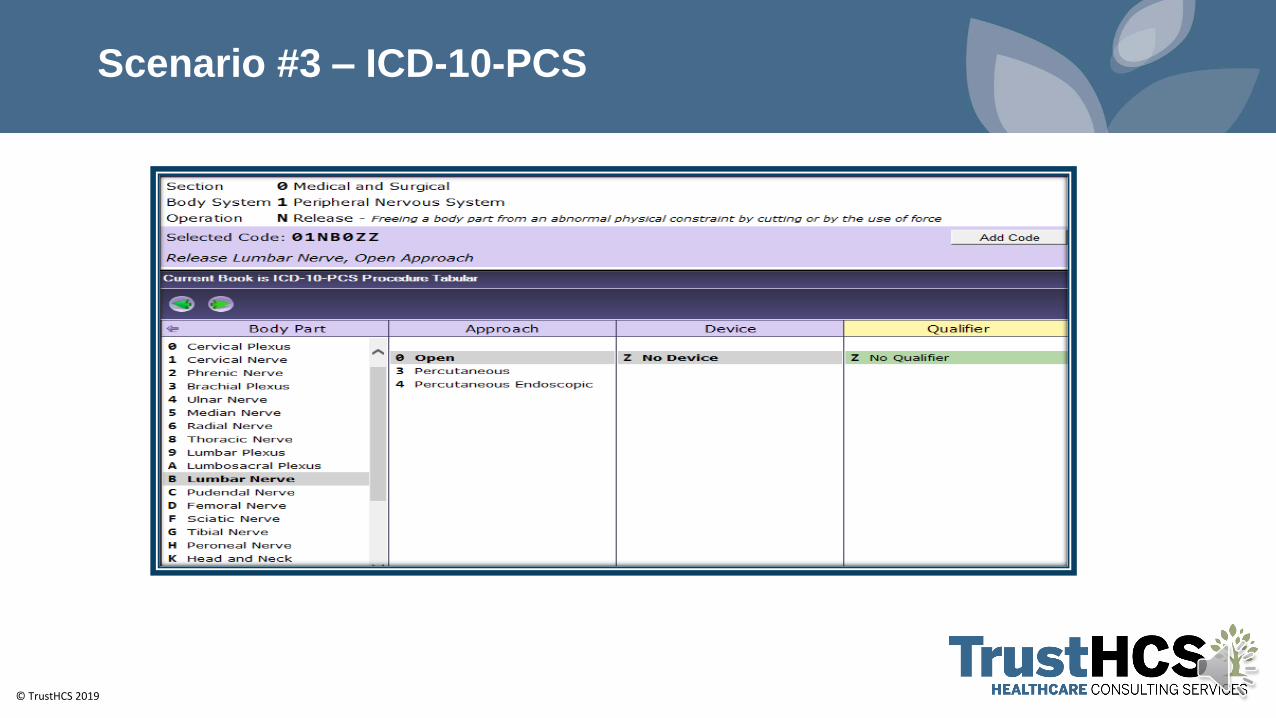
Scenario #3 – ICD-10-PCS
© TrustHCS 2019
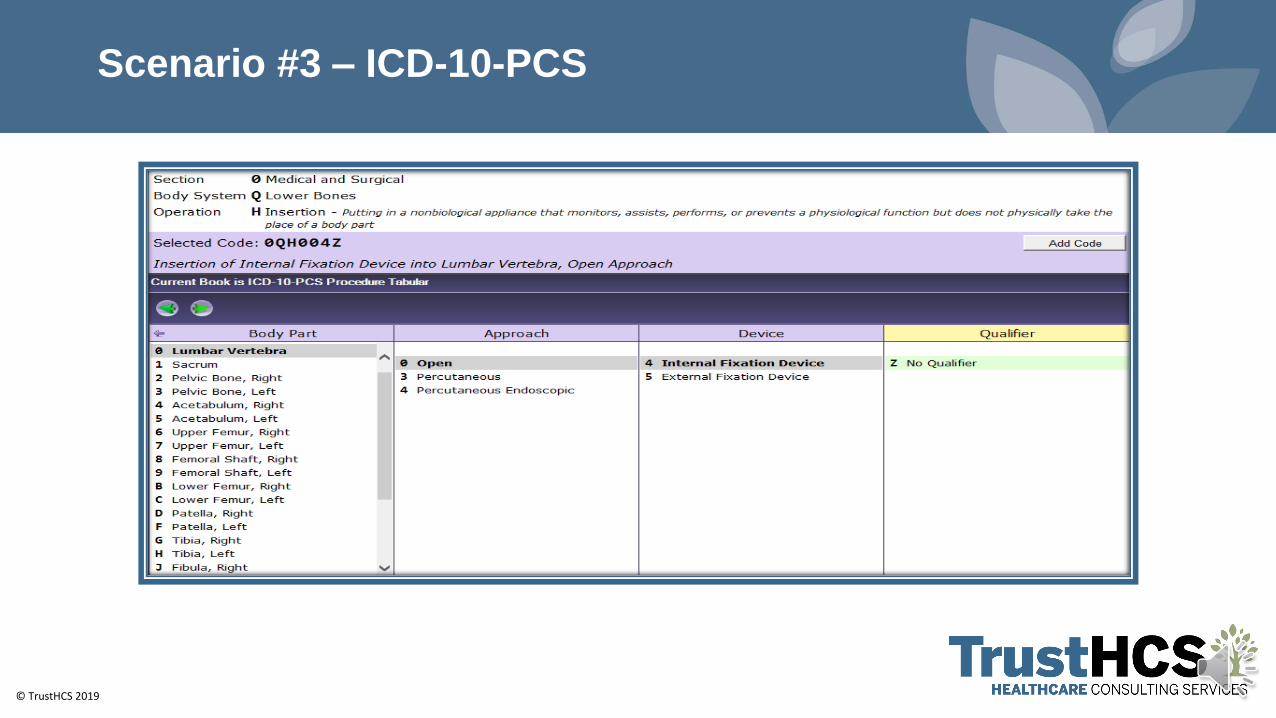
Scenario #3 – ICD-10-PCS
© TrustHCS 2019
Scenario #3 – ICD-10-PCS - Summary
01NB0ZZ Release Lumbar Nerve, Open Approach
0QH004Z Insertion of Internal Fixation Device into Lumbar Vertebra, Open Approach
© TrustHCS 2019© TrustHCS 2019
Thank You!!Nena Scott, PhD, MSEd, RHIA, CCS, CCS-P, CCDS, CRC
Director, Coding Quality and Professional Development
Phone: 662-210-2805
www.TrustHCS.com
Read our blog: http://www.trusthcs.com/blog/
© TrustHCS 2019
References
2020 Current Procedural Terminology (CPT) Professional Edition. American Medical Association.
Nucleus Medical Media: Medical Video, Animation, Illustration. (n.d.). Retrieved from http://www.nucleuscatalog.com