Embed Size (px)
Citation preview

J Neurosurg: Spine / Volume 16 / June 2012
J Neurosurg Spine 16:523–531, 2012
523
Spinal AVMs are complex neurosurgical lesions that can be categorized according to location. Intramed-ullary, or glomus, spinal AVMs are rare entities lo-
cated within the spinal cord parenchyma. They may be supplied by single or multiple feeding arteries that arise from branches of the anterior and/or posterior spinal arter-ies. Underlying clinical pathophysiology is attributed to venous hypertension, vascular steal, and/or hemorrhage. Presenting signs and symptoms include pain, paresthe-
sias, myelopathy, and paresis or paralysis.3–6,10,11,14,20,22,
23,25–27 Glomus spinal AVMs share similar angioarchitec-tural characteristics with intracranial AVMs. We have previously categorized intramedullary spinal AVMs into compact and diffuse subtypes.22 The vast majority of glo-mus AVMs are diffuse, possessing both intraparenchy-mal and extrapial components that are amenable to pial resection.
Various treatment modalities including conservative observation,16 endovascular embolization,1,2,6,7,9,11,13,14,17–19,
25,26 radiation therapy,21 and microsurgical resection3–5,10,
12,15,20,22,24,25,28,29 have been attempted. At most tertiary centers, preoperative embolization followed by microsur-
Microsurgical management of glomus spinal arteriovenous malformations: pial resection technique
Clinical article
GreGory J. Velat, M.D., SteVe W. ChanG, M.D., aDib a. abla, M.D., Felipe C. albuquerque, M.D., CaMeron G. MCDouGall, M.D., anD robert F. Spetzler, M.D.Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona
Object. Intramedullary, or glomus, spinal arteriovenous malformations (AVMs) are rare vascular lesions ame-nable to resection with or without adjuvant embolization. The authors retrospectively reviewed the senior author’s (R.F.S.’s) surgical series of intramedullary spinal AVMs to evaluate clinical and radiographic outcomes.
Methods. Detailed chart and radiographic reviews were performed for all patients with intramedullary spinal AVMs who underwent surgical treatment between 1994 and 2011. Presenting and follow-up neurological examina-tion results were obtained and graded using the modified Rankin Scale (mRS) and McCormick Scale. Surgical tech-nique, outcomes, complications, and long-term angiographic studies were reviewed.
Results. During the study period, 20 patients (10 males and 10 females) underwent resection of glomus spinal AVMs. The mean age at presentation was 30 ± 17 years (range 7–62 years). The location of the AVMs was as follows: cervical spine (n = 10), thoracic spine (n = 9), and cervicothoracic junction (n = 1). The most common presenting signs and symptoms included paresis or paralysis (65%), paresthesias (40%), and myelopathy (40%). Perioperative embolization was performed in the majority (60%) of patients. Pial AVM resection was performed in 17 cases (85%). Angiographically verified AVM obliteration was achieved in 15 patients (75%). At a mean follow-up duration of 45.4 ± 52.4 months (range 2–176 months), 14 patients (70%) remained functionally independent (mRS and McCormick Scale scores ≤ 2). One perioperative complication occurred, yielding a surgical morbidity rate of 5%. Three symp-tomatic spinal cord tetherings occurred at a mean of 5.7 years after AVM resection. No neurological decline was observed after endovascular and surgical interventions. No deaths occurred. Long-term angiographic follow-up data were available for 9 patients (40%) at a mean of 67.6 ± 60.3 months (range 5–176 months) following AVM resection. Durable AVM obliteration was documented in 5 (83%) of 6 patients.
Conclusions. Intramedullary AVMs may be safely resected with satisfactory clinical and angiographic results. The pial resection technique, which provides subtotal AVM nidus resection, effectively devascularized these lesions, as confirmed on postoperative angiography, without violating the spinal cord parenchyma, thereby potentially reduc-ing iatrogenic injury.(http://thejns.org/doi/abs/10.3171/2012.3.SPINE11982)
Key WorDS • arteriovenous malformation • embolization • glomus • intramedullary • spinal surgery • technique
Abbreviations used in this paper: AVM = arteriovenous malfor-mation; mRS = modified Rankin Scale; NBCA = N-butyl cyanoac-rylate.

G. J. Velat et al.
524 J Neurosurg: Spine / Volume 16 / June 2012
gical resection is the preferred treatment. We retrospec-tively reviewed the clinical and radiographic outcomes of our series of spinal glomus AVMs while highlighting a pial resection technique that minimizes parenchymal dissection. This technique, which provides subtotal AVM nidus resection, effectively devascularizes glomus AVMs, as confirmed on postoperative angiography.
MethodsData obtained from all patients treated by the senior
author (R.F.S.) who underwent microsurgical treatment of spinal vascular malformations between January 1994 and April 2011 were reviewed from a prospectively main-tained database. During this period, the pial resection technique was preferentially employed for glomus spinal AVMs with nidi that crossed a pial surface. Myelotomy was reserved for significant intramedullary hematomas, syringes, or AVMs whose nidi remained entirely intrapa-renchymal. Detailed retrospective chart and radiographic reviews included only patients with intramedullary glo-mus spinal AVMs affecting the cervical and/or thoracic spines. Patients harboring arteriovenous fistulas, juve-nile or metameric AVMs, and AVMs affecting the conus medullaris and/or cauda equina were excluded from anal-ysis. Patient demographic factors, medical comorbidities, presenting signs and symptoms, and results of baseline neurological examinations were obtained through de-tailed chart reviews. Scores based on the mRS and Mc-Cormick Scales were assigned to each patient at presen-tation. Pretreatment MRI and spinal angiography studies were reviewed. Operative records were studied closely, focusing primarily on microsurgical technique. For many patients, surgical videos were available for review. Ad-juvant treatment records, including endovascular emboli-zation, were reviewed in detail. Postoperative (within 24 hours of resection) and long-term spinal angiograms were evaluated by the senior author and endovascular neuro-surgeons at our institution (F.C.A. and C.G.M.). Function-al status was measured using the mRS and McCormick Scale at last clinical follow-up. In cases of limited clinical follow-up, telephone interviews were conducted.
ResultsDuring the study period, 20 patients (10 males and
10 females) underwent microsurgical resection of glomus spinal AVMs. Most patients were referred from other ter-tiary care centers throughout the US and from abroad. The mean age at presentation was 30 ± 17 years (range 7–62 years). The most commonly affected spinal segment was cervical (n = 10 cases [50%]) followed by thoracic (n = 9 cases [45%]). One AVM (5%) spanned the cervico-thoracic junction. Three flow-related aneurysms were ob-served (intranidal, Cases 1 and 19; feeding artery, Case 8) (Table 1). The associated aneurysm in Case 1 was excised successfully along with the AVM nidus during the same surgical setting. The feeding artery aneurysm in Case 8 was embolized before resection. The patient in Case 19 underwent embolization of an intranidal AVM aneurysm elsewhere before undergoing treatment at our institution.
PresentationPresenting signs and symptoms are detailed in Table
1. The most common presentations—paresis, paralysis, or both—occurred in 13 patients (65%). Other present-ing signs and symptoms included paresthesias (40%), my-elopathy (40%), bowel and/or bladder incontinence (15%), and intractable pain (10%). Three patients (Cases 9, 10, and 19) presented with hemorrhage. Acute subarachnoid and subdural blood products were observed in Cases 9 and 19, whereas in Case 10 the patient presented with a large intramedullary hematoma. All 3 patients experi-enced acute neurological decline. The timing of symptom onset ranged from several days to 3 years. In Cases 14, 17, and 19, the patients were cared for at outside institutions before undergoing treatment at our center. The patient in Case 14 was left with residual weakness of the left lower extremity after undergoing subtotal AVM resection at an outside institution. He presented to our center with an 18-month history of progressive bilateral lower-extremity paresis, spasticity, and bowel/bladder incontinence 13 years after his initial surgery. The patient in Case 17 un-derwent conservative treatment at an outside facility after she presented with moderate paraparesis and a lower tho-racic intramedullary spinal AVM. She sought treatment at our institution 4 years after diagnosis, when, over the course of several months, she had begun to experience progressive myelopathy and bilateral lower-extremity paresthesias. The patient in Case 19 was transferred to our center after embolization of an associated intranidal aneurysm at the referring hospital.
Microsurgical TechniqueIn most cases surgery was performed via a posterior
approach (Table 1). Typically, we used a multilevel lam-inoplasty extending a single level above and below the AVM nidus. The senior author (R.F.S.) prefers lamino-plasty over laminectomy to protect the underlying neural elements and to facilitate future operative exposures, if required. For laterally situated lesions, the laminotomy should extend to the ipsilateral pedicle or pars interar-ticularis to improve lateral exposure. The dural opening should likewise be tailored to the AVM location. A para-median posterior durotomy was most commonly used in this series. For cases in which additional anterolateral exposure was achieved after performing costotransver-sectomy (Cases 12, 14, and 19), the durotomy was made laterally between the ventral and dorsal nerve rootlets. Dorsal nerve rootlets were sacrificed in selected cases with routine sectioning of dentate ligaments to further augment anterolateral exposure.
Careful inspection of the spinal cord and its associ-ated vasculature is critical to achieving optimal surgical results. Draining veins are typically easier to identify grossly on the surface of the spinal cord than feeding ar-teries. Associated arterial or intranidal aneurysms may be identified. It is often difficult to clearly define the an-gioarchitecture of these complex lesions. Intraoperative indocyanine green videoangiography is very helpful in identifying feeding arterial pedicles and early draining veins. Repeated indocyanine green videoangiography

J Neurosurg: Spine / Volume 16 / June 2012
Resection technique for glomus spinal AVMs
525
at various time points during the AVM resection helps identify residual, early-filling pedicles that are then oblit-erated. Embolic material casts from endovascular embo-lization also help to identify associated feeding arteries, allowing the surgeon to correlate the surgical anatomy with the AVM angioarchitecture.
Pial Resection TechniqueMicrosurgical resection of spinal AVMs varies by
institution. The senior author (R.F.S.) prefers to resect feeding arteries before sacrifice of draining veins, simi-lar to intracranial AVMs. Other surgeons, however, have described clinical success with resection of venous ele-ments first.3 In the senior author’s early series of spinal AVMs, intraparenchymal components were resected via myelotomy tailored to the location of the lesion. Four classic myelotomies were used: midline dorsal, dorsal
root entry zone, lateral, and anterior midline. Over the past 2 decades, the senior author has adopted a pial resec-tion technique that minimizes entry into the spinal cord parenchyma (as illustrated in Fig. 1 and Videos 1 and 2).
ViDeo 1. Case 6. Resection of an intramedullary C-5 glomus AVM (1.9 × 0.9 × 0.9 cm) in a 12-year-old boy who presented with progressive bilateral upper-extremity paresis and paresthe-sias. Preoperative embolization was not performed because of the proximity of the anterior spinal artery arising from the right thyrocervical artery feeder supplying the AVM nidus. The AVM was devascularized using the pial resection technique. Left-sided C-5 sensory rootlets intimately involved with the AVM were sacrificed. Postoperative angiography confirmed complete AVM obliteration. At the 20-month clinical follow-up visit, the patient’s symptoms had completely resolved. Used with permis-sion from Barrow Neurological Institute. Click here to view with Media Player. Click here to view with Quicktime.
TABLE 1: Summary of demographics, presentations, treatments, and perioperative results*
Case No.
Age (yrs), Sex
AVMLocation Presentation
PreopEmbolization Surgical Approach
AVM Oblitera- tion on Postop Angiography
1 38, M T4–5 myelopathy w/ bowel/bladder incontinence no T3–6 laminoplasties yes 2 26, F C2–3 myelopathy w/ bilat upper-extremity pares-
thesiasno C2–4 laminoplasties yes
3 12, F C4–5 spastic quadriparesis yes C3–6 laminoplasties yes 4 51, F C3–5 spastic quadriparesis yes C2–6 laminoplasties yes† 5 9, M C6–7 ipsilat paresthesias & monoparesis no C6–7 laminoplasties yes 6 12, M C5–6 bilat upper-extremity paresis & paresthesias no C4–6 laminoplasties yes 7 62, M C3–4 ipsilat hemiparesis yes C3–4 laminoplasties yes 8 13, M T9–10 myelopathy yes T8–10 laminoplasties yes 9 17, M C5–6 SAH; bilat lower-extremity paresis yes C5–7 laminoplasties yes10 18, M C5–6 IPH; ipsilat hemiparesis yes C4–6 laminoplasties w/ midline posterior
myelotomy to evacuate intramedullary hematoma
no
11 45, M T5–7 bilat lower-extremity paresis & paresthesias no T3–8 laminoplasties‡ yes12 22, F T8–9 pain, bilat lower-extremity paralysis w/
bowel/bladder incontinenceyes lt T8–9 costotransversectomy w/ midline
anterior myelotomyyes
13 34, F C7–T1 pain, ipsilat paresthesias yes C6–T2 laminoplasties no14 29, M T2–6 myelopathy, spastic paraparesis w/ bowel/
bladder incontinenceno lt T3–5 costotransversectomies w/ mid-
line anterior myelotomy‡yes
15 23, F C-3 ipsilateral spastic hemiparesis yes C2–3 laminoplasties no16 48, F C-2 myelopathy w/ ipsilat hemibody paresthe-
siasyes C1–3 laminoplasties no
17 32, F T-11 myelopathy w/ bilat lower-extremity pares- thesias
no T10–12 laminoplasties yes
18 51, F T-5 bilat lower-extremity paresthesias yes staged T3–7 laminoplasties & transtho- racic approach
no
19 7, M T-8 SAH; myelopathy w/ bilat lower-extremity paresis
yes§ T7–9 laminoplasties & lt T-8 costotrans- versectomy
yes
20 52, F T4–5 myelopathy w/ bilat lower-extremity paresis no T3–6 laminoplasties yes
* IPH = intraparenchymal hemorrhage; SAH = subarachnoid hemorrhage.† Indicates AVM obliteration after postoperative (< 24-hour) residual embolization.‡ Indicates 2 operations.§ Embolization performed at outside hospital.

G. J. Velat et al.
526 J Neurosurg: Spine / Volume 16 / June 2012
ViDeo 2. Case 2. Resection of a glomus C2–3 spinal AVM (1.3 × 1 × 0.9 cm) in a 26-year-old woman who presented with progressive bilateral upper-extremity paresthesias and hyper-reflexia. Preoperative embolization was unsuccessful due to the extreme tortuosity of the feeding arterial pedicle, which arose from the right vertebral artery. Complete AVM obliteration, achieved using the pial resection technique, was confirmed on postoperative angiography. At the 4-month clinical follow-up visit, the patient continued to be neurologically stable. Used with permission from Barrow Neurological Institute. Click here to view with Media Player. Click here to view with Quicktime.
In this technique, which has been previously described,25 feeding arteries and draining veins are coagulated and divided along the spinal cord surface while minimiz-ing subpial dissection. For reasons yet to be fully eluci-
dated, and in direct contrast to brain AVMs, interruption of the spinal AVM angioarchitecture provides sufficient devascularization of glomus AVMs (as verified on post-operative angiography) to alleviate venous hypertension, prevent bleeding, and improve neurological function. A representative case example is provided in Fig. 2, which illustrates a C-5 glomus spinal AVM in a young boy that was successfully obliterated using the pial resection tech-nique. Currently at our institution, myelotomy is reserved for the evacuation of intraparenchymal hematomas, fen-estration of associated spinal syringes, or for the rare compact midline glomus AVM whose nidus is completely intraparenchymal. In this series, the pial resection tech-nique was used in 17 (85%) of 20 cases. Resection of in-traparenchymal anteriorly located AVMs was performed via an anterior midline myelotomy in Cases 12 and 14. A posterior midline myelotomy was performed in Case 10 to evacuate a large intraparenchymal hematoma.
Endovascular EmbolizationEmbolization plays an integral part in the surgical
management of intramedullary spinal AVMs. It proves particularly useful in reducing blood supply from ante-riorly located feeding arteries that can complicate mi-crosurgical resection from posterior or posterolateral ap-proaches. Embolization was attempted in all 20 patients in this series but was successful in only 12 cases (60%). The contribution of feeding arteries to the anterior spi-nal artery precluded successful embolization in 4 patients (Cases 1, 5, 6, and 20). Four additional intramedullary AVMs were supplied by either small-caliber or extremely tortuous vessels that prevented optimal microcatheter positioning to allow safe embolization (Cases 2, 11, 14, and 17). Polyvinyl alcohol particles and NBCA were used early in the series, and Onyx was preferentially used in cases managed in the last 5 years. An associated feeding artery aneurysm was embolized before resection in Case 8. The patient in Case 19 underwent embolization of an intranidal aneurysm at the referring hospital before being transferred. A median of 2 arterial feeders were emboli-zed over a single treatment session. There were no direct complications related to embolization.
Angiographic Results and Long-Term Radiographic Follow-Up
Postoperative spinal angiography was performed in all 20 patients within 24 hours of surgery (Table 1). Com-plete AVM obliteration was ultimately achieved in 15 cases (75%) after combined endovascular and microsur-gical therapies. Two patients (Cases 11 and 14) required multiple resections to obliterate their respective AVMs. The patient in Case 4 underwent postoperative NBCA embolization of a small residual left thyrocervical feed-ing artery branch after subtotal resection of a complex cervical intramedullary spinal AVM to achieve complete obliteration. (As shown in Table 1, this patient also re-ceived preoperative embolization.) Long-term follow-up angiographic studies were available for 9 patients (45%) (at a mean interval of 67.6 ± 60.3 months (range 5-176 months) as denoted in Table 2. Durable AVM obliteration
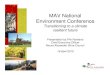
Fig. 1. Upper: Illustration of a glomus spinal AVM affecting the posterior spinal cord. The AVM nidus extends through the spinal pa-renchyma into the extrapial space. Associated feeding arteries arising from the posterior spinal arteries, intranidal aneurysms, and arterialized draining veins are present. Lower: The extrapial portion of the AVM nidus has been resected, leaving the parenchymal portion of the ni-dus. Despite subtotal nidal resection, the glomus spinal AVM has been essentially devascularized and obliterated. Used with permission from Barrow Neurological Institute.

J Neurosurg: Spine / Volume 16 / June 2012
Resection technique for glomus spinal AVMs
527
was observed in 5 (83%) of 6 patients with long-term an-giographic follow-up. In 3 patients (Cases 10, 13, and 18), the appearance of known residual AVM components at long-term angiographic follow-up was stable. The patient in Case 11 developed a new left vertebral artery feeder to his thoracic AVM, which had previously been obliterated following a 2-stage posterior resection. The blood supply to the AVM in this case was minimal, and the patient is being followed conservatively and has not experienced any new neurological deficits.
Clinical OutcomesClinical outcomes were assessed at presentation to
our institution and at the time of last clinical follow-up us-ing the mRS and McCormick Scale (Table 3). The mean follow-up period, as calculated from the time of AVM
resection, was 45.4 ± 52.4 months (range 2–176 months). The median and mean mRS scores at presentation were similar (median 3, mean 2.9 ± 1.1), as were the McCor-mick Scale scores (median 3, mean 2.9 ± 1.0). Clinical improvement was validated within the cohort based on improved mRS and McCormick Scale scores at last fol-low-up (median and mean mRS scores 2 and 2.2 ± 1.2, respectively; median and mean McCormick Scale scores 2 and 2.3 ± 1.0, respectively). Independent functional sta-tus (defined as mRS and/or McCormick Scale scores ≤ 2) was observed in 9 patients (45%) at presentation and in 14 patients (70%) at last clinical evaluation (p = 0.2) (Fig. 3). No patients suffered clinical deterioration following endovascular and/or surgical interventions.
One perioperative complication occurred, yielding an immediate complication rate of 5%. The patient in
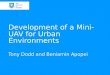
Fig. 2. Case 6. A 12-year-old boy presented with progressive bilateral upper-extremity paresis and paresthesias. A and B: Sagittal and axial MRI scans showing characteristic flow voids and extensive edema consistent with the intramedullary C-5 spinal AVM (arrow). C: Preoperative anteroposterior angiogram confirming arterial supply to the AVM via a right thyrocervical feeder (arrow). Embolization was not performed due to some contribution of this arterial pedicle to the anterior spinal artery (ar-rowhead). D: Intraoperative photograph acquired following C4–6 laminoplasties, illustrating an extensive extrapial AVM nidus involving the posterolateral surface of the spinal cord. E: Indocyanine green videoangiography demonstrating early filling of the extrapial AVM nidus. F: The pial resection technique was performed to devascularize the extrapial AVM nidus. Sharp dissection was used to expose vascular pedicles that traverse the spinal cord parenchyma (arrows) prior to coagulation and division. G: The extrapial portion of the AVM nidus has been resected along the posterolateral margin of the spinal cord. H: Indocyanine green videoangiography confirming resection of the extrapial AVM nidus. I: Postoperative anteroposterior angiogram of the right thyrocervical artery verifying complete AVM obliteration despite the subtotal nidal resection achieved using the pial resec-tion technique. Figures 1D–H used with permission from Barrow Neurological Institute.

G. J. Velat et al.
528 J Neurosurg: Spine / Volume 16 / June 2012
Case 12 developed a CSF pleural fistula after undergoing a 2-level costotransversectomy for resection of a thoracic intramedullary AVM. There was no evidence of pleural violation during the operation. The fistula resolved after placement of a lumboperitoneal shunt. The overall long-term complication rate was 15% (3 of 20 patients) (Table 3). Three delayed symptomatic spinal cord tetherings oc-curred at a mean interval of 5.7 years following surgery. The patient in Case 5 developed subtle worsening of par-
esthesias without motor deficits 13 months after a lower cervical intramedullary spinal AVM was excised. Repeat imaging showed evidence of increased T2-weighted sig-nal change within the spinal cord and extensive scar tis-sue formation. The patient underwent detethering, and his symptoms resolved over several weeks. The patient in Case 11 experienced delayed-onset leg paresthesias 41 months after staged AVM resection. After detethering surgery, his symptoms resolved within 1 month. Like-wise, the patient in Case 18 developed worsening bilateral lower-extremity paresthesias 15 years after staged subto-tal resection of a thoracic intramedullary AVM. Follow-up MRI showed extensive tethering and formation of a syrinx. The spinal cord was detethered, the syrinx was fenestrated via a posterior approach, and the paresthesias resolved clinically.
DiscussionIntramedullary, or glomus, spinal AVMs are rare vas-
cular lesions. Their complex angioarchitecture renders potential treatment options especially challenging for the neurosurgeon. Over the years, a gradual paradigm shift in the management of these lesions has occurred. Con-servative observation has been replaced by endovascular embolization and resection. Despite recent technological advances in endovascular devices and techniques, intra-medullary AVMs are not always amenable to emboliza-tion. Feeding arterial branches may supply critical spinal
TABLE 3: Summary of neurological status at presentation and follow-up, follow-up duration, and operative complications*
CaseNo.
mRS Score McCormick Score Clinical Fol- low-Up (mos) Op ComplicationsPresentation Follow-Up Presentation Follow-Up
1 3 2 3 2 2 none 2 2 1 2 2 4 none 3 4 3 4 3 11 none 4 3 1 3 2 10 none 5 2 2 2 2 13 delayed development of TSC 12 mos after AVM resection 6 2 2 2 2 20 none 7 3 2 3 2 75 none 8 4 4 4 4 38 none 9 4 2 4 2 36 none10 4 3 4 3 116 none11 4 3 4 3 98 delayed development of TSC 41 mos after AVM resection 12 5 5 5 5 12 CSF-pleura fistula requiring LP shunt placement13 2 2 2 2 115 none14 4 4 3 3 126 none15 3 2 3 2 24 none16 2 1 2 1 12 none17 2 1 2 1 12 none18 2 1 2 1 176 delayed development of TSC & associated syrinx 15 yrs after AVM
resection19 2 1 2 2 5 none20 1 1 2 2 2 none
* LP = lumboperitoneal; TSC = tethered spinal cord.
TABLE 2: Long-term angiographic results
CaseNo.
Angiographic Follow-Up (mos) Residual or Recurrent AVM
5 13 none 8 38 none 9 36 none10 116 stable residual supply from rt vertebral & rt
T-5 segmental arteries11 98 new small feeder supplied by lt vertebral ar-
tery13 115 stable residual supply from lt superior inter-
costal artery17 12 none18 176 2 small stable feeders from lt T-8 segmental
artery19 5 none

J Neurosurg: Spine / Volume 16 / June 2012
Resection technique for glomus spinal AVMs
529
cord vascular elements, such as the anterior spinal artery or the artery of Adamkiewicz. In cases of arterial elo-quence, provocative testing with a combination of amytal and cardiac lidocaine may be performed. In our series, embolization was aborted if changes were observed in somatosensory and/or motor evoked potentials. Vessel tortuousity may also limit the interventionalist’s ability to selectively insert a microcatheter into feeding arterial pedicles. Eight (40%) of our 20 patients did not undergo preoperative AVM embolization for these reasons.
Evidence in the literature suggests that clinical signs and symptoms may improve after complete or subtotal embolization. Results from endovascular embolization of glomus spinal AVMs vary. Riché et al.17 embolized 17 in-tramedullary spinal AVMs involving the anterior spinal artery. Nine patients (53%) improved during the follow-up period, while 5 remained neurologically stable. In 3 patients deterioration occurred after treatment; this yield-ed a periprocedural complication rate of 17.6%. Using ei-ther polyvinyl alcohol particles or acrylic glue, Rodesch and colleagues19 embolized 19 intramedullary spinal AVMs supplied by arterial pedicles arising from the an-terior spinal artery. At last clinical follow-up, 53% of pa-tients improved neurologically despite a relatively high periprocedural complication rate (27%). A retrospective update published by the same group in 2003 detailed an improved AVM obliteration rate of 16%, with more than a 50% reduction in AVM shunting in 86% of the patients treated with acrylic glue.18 More recently, Corkill et al.6 embolized 17 glomus AVMs using Onyx. Three intra-procedural complications occurred: 2 extradural hemor-rhages and 1 perforation of a feeding vessel resulting in subarachnoid hemorrhage, eventual vasospasm, and sub-sequent spinal cord infarction. Immediate postemboliza-tion angiography confirmed AVM obliteration in 6 pa-tients (37.5%). Despite a low rate of AVM obliteration, 14 patients (82%) had improved clinical function at a mean follow-up period of 24.3 months. Another group achieved complete intramedullary spinal AVM obliteration after
Onyx embolization in 4 (80%) of 5 patients at a mean an-giographic follow-up period of 8.2 months, with 1 spinal cord infarction.11 Scant data are available regarding the durability of glomus AVM embolization. Using polyvinyl alcohol particles for embolization, Hall et al.8 observed a 67% recanalization rate within 2 months of treating 3 intramedullary AVMs.
Microsurgical resection with or without adjuvant embolization remains the mainstay treatment for symp-tomatic glomus spinal AVMs. The vast majority of these lesions may be approached posteriorly despite involve-ment of anterior spinal elements.3–5,15 Direct anterior or anterolateral approaches have been described.12,28 Lami-noplasties were performed in 18 (90%) of 20 patients in the present series. Sufficient anterolateral exposure can be obtained by exposing the posterior elements eccentric to the side of the lesion, sectioning the dentate ligaments, and sacrificing the dorsal nerve rootlets if necessary (par-ticularly in the thoracic spine). The spinal cord can be gently rolled laterally, without causing neurological se-quelae, to augment anterior exposure. Posterolateral ap-proaches may provide additional exposure to the anterior spinal elements, allowing enhanced extirpation of these lesions.
Early in this series, costotransversectomy was per-formed as a stand-alone approach in 2 patients. The pa-tient in Case 12 had an anteriorly located intramedullary AVM that was resected via a left-sided T8–9 costotrans-versectomy and midline anterior myelotomy. The patient in Case 14 underwent a 3-level costotransversectomy for resection of a similar anterior intramedullary AVM. The left T-3 and T-4 dorsal rootlets were sacrificed to allow rotation of the spinal cord. A midline anterior myelotomy was performed. This patient required a second opera-tion, in which the same approach was used within several days of the original surgery to achieve complete AVM obliteration. One additional patient (Case 19) underwent a 1-level costotransversectomy to augment anterolateral ex-posure after multilevel laminoplasties. One direct lateral approach was performed in this series (Case 18). A staged transthoracic exposure followed by posterior laminoplas-ty was used to subtotally resect a complex intramedullary AVM using the pial technique. Although adequate expo-sure of the AVM was obtained through the transthoracic exposure, the increased working distance made the AVM resection particularly challenging.
A summary of results for contemporary intramedul-lary spinal AVM surgical series is shown in Table 4. Ad-junctive embolization was used in most of the series. Rates of AVM obliteration ranged from 70% to 100%. Many of the series, however, failed to report how AVM oblit-eration was determined. We maintain that postoperative spinal angiography is the only definitive way to confirm complete eradication. The 75% obliteration rate observed in the present series falls within the results published by other groups. Our series did not include conus medullaris AVMs, which are often more amenable to resection and surgical cure. Our single perioperative complication com-pares favorably to complication rates published by other groups. Likewise, functional independence was achieved in 70% of our patients at a mean clinical follow-up pe-riod of 45 months. Two patients (Cases 8 and 12), who
Fig. 3. Bar graph depicting independent (mRS and McCormick Scale scores ≤ 2) and dependent functional status at presentation and last clinical follow-up. The values on the y axis represent the number of patients.

G. J. Velat et al.
530 J Neurosurg: Spine / Volume 16 / June 2012
presented with severe neurological deficits and functional dependence, did not improve despite AVM obliteration.
Limited information on long-term postoperative complications is available in the literature. Three of our patients presented with symptomatic spinal cord tether-ing at a mean of 5.7 years after AVM resection. Paresthe-sias were the presenting symptom in all 3 patients. After the patients underwent cord detethering, their symptoms resolved over the course of several weeks to months. This observation reinforces the need for long-term clinical and radiographic follow-up in such cases, even in the setting of complete AVM eradication. Delayed recurrence of a previously obliterated AVM occurred in 1 patient (Case 11) more than 8 years after surgery. The recurrence was discovered on a follow-up spinal angiogram 4.5 years af-ter the spinal cord detethering procedure. We are con-servatively following the small AVM recurrence because the patient remains neurologically stable. Such late recur-rences have been reported years after initial AVM eradi-cation.5
Over the past 3 decades, microsurgical resection techniques for intramedullary spinal AVMs have evolved. Traditional myelotomy, which places critical spinal ele-ments at risk, may not be necessary in selected cases of glomus spinal AVMs that cross a pial surface. Satisfac-tory radiographic and clinical results can be achieved by occluding the AVM vessels as they enter the pia mater rather than by following them into the spinal cord pa-renchyma. This technique simply interrupts feeding and draining AVM vessels. Thus far, we have not encountered significant bleeding, spinal infarctions, or neurological deterioration when using this technique, a fact that stands in dramatic contrast to intracranial AVMs, where subtotal nidal resection results in uncontrollable bleeding.
Major limitations of our study include its retrospec-tive nature and the incomplete long-term angiographic follow-up. In general, we attempt to obtain a repeat spinal angiogram 12 months after surgery. Four patients in our series are scheduled to undergo 12-month follow-up an-giography in the near future. Other patients were lost to follow-up, a common problem for many tertiary referral institutions.
ConclusionsIntramedullary spinal AVMs are complex lesions
amenable to combined endovascular embolization fol-lowed by resection. Despite varied clinical presentations, patients tend to improve after treatment, even those with residual AVM components. The pial resection technique effectively devascularizes critical feeding and draining vasculature and leads to satisfactory clinical and angio-graphic results. This technique avoids entry into the spi-nal cord parenchyma and is ideal for the more common laterally located glomus-type AVMs.
Disclosure
Dr. Spetzler is a consultant for Zeiss; has direct stock ownership in Boston Scientific, DicomGrid, EmergeMD, Neurovasc, Synerget-ics, Stereotaxis, RSB Spine, iCO Therapeutics, and Katalyst/Kogent; and receives royalties from Codman and Stryker.
Author contributions to the study and manuscript preparation include the following. Conception and design: Spetzler, Velat. Acquisition of data: Velat. Analysis and interpretation of data: Spetz-ler, Velat, Abla, Chang. Drafting the article: Velat. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Spetzler. Statistical analysis: Velat. Administrative/technical/material support: Spetzler. Study supervision: Spetzler.
References
1. Ausman JI, Gold LH, Tadavarthy SM, Amplatz K, Chou SN: Intraparenchymal embolization for obliteration of an intra-medullary AVM of the spinal cord. Technical note. J Neuro-surg 47:119–125, 1977
2. Biondi A, Merland JJ, Hodes JE, Aymard A, Reizine D: An-eurysms of spinal arteries associated with intramedullary ar-teriovenous malformations. II. Results of AVM endovascular treatment and hemodynamic considerations. AJNR Am J Neuroradiol 13:923–931, 1992
3. Boström A, Krings T, Hans FJ, Schramm J, Thron AK, Gils-bach JM: Spinal glomus-type arteriovenous malformations: microsurgical treatment in 20 cases. Clinical article. J Neu-rosurg Spine 10:423–429, 2009
4. Cogen P, Stein BM: Spinal cord arteriovenous malformations with significant intramedullary components. J Neurosurg 59: 471–478, 1983
TABLE 4: Summary of results, complications, outcomes, and follow-up duration of recent surgical series for intramedullary spinal AVMs*
Authors & YearNo. of Cases
Adjuvant Emboli- zation
Periop AVM Obliteration Rate (imaging modality)
Periop Complication
Rate (%)Good or Independent
Outcome (%)Mean Follow-
Up (yrs)
Cogen & Stein, 1983 6 no NA NA 83 5 Rosenblum et al., 1987 14 yes NA NA NA NAConnolly et al., 1998 15 yes 93% (angiography) 7 67 8.9 Ushikoshi et al., 2000 10 yes 70% (NA) NA NA 7.5 Zozulya et al., 2006 30 yes 100% (NA) NA 87 NABoström et al., 2009 12 yes 83% (8 angiography, 2
MRI)8 80 (2 patients lost to
follow-up)3.9
present study 20 yes 75% (angiography) 5 70 3.8
* NA = not applicable.

J Neurosurg: Spine / Volume 16 / June 2012
Resection technique for glomus spinal AVMs
531
5. Connolly ES Jr, Zubay GP, McCormick PC, Stein BM: The posterior approach to a series of glomus (Type II) intramedul-lary spinal cord arteriovenous malformations. Neurosurgery 42:774–786, 1998
6. Corkill RA, Mitsos AP, Molyneux AJ: Embolization of spinal intramedullary arteriovenous malformations using the liquid embolic agent, Onyx: a single-center experience in a series of 17 patients. J Neurosurg Spine 7:478–485, 2007
7. Djindjian R, Merland JJ, Djindjian M, Houdart R: [Emboliza-tion in the treatment of medullary arteriovenous malforma-tions in 38 cases (author’s transl).] Neuroradiology 16:428–429, 1978 (Fr)
8. Hall WA, Oldfield EH, Doppman JL: Recanalization of spinal arteriovenous malformations following embolization. J Neu-rosurg 70:714–720, 1989
9. Horton JA, Latchaw RE, Gold LH, Pang D: Embolization of intramedullary arteriovenous malformations of the spinal cord. AJNR Am J Neuroradiol 7:113–118, 1986
10. Kim LJ, Spetzler RF: Classification and surgical management of spinal arteriovenous lesions: arteriovenous fistulae and ar-teriovenous malformations. Neurosurgery 59 (5 Suppl 3): S195–S201, 2006
11. Lv X, Li Y, Yang X, Jiang C, Wu Z: Endovascular emboliza-tion for symptomatic perimedullary AVF and intramedullary AVM: a series and a literature review. Neuroradiology [epub ahead of print], 2011
12. MacFarlane MR, Burn PJ, Evison J: Excision of high and mid cervical spinal cord arteriovenous malformations by anterior operation. J Clin Neurosci 12:71–79, 2005
13. Molyneux AJ, Coley SC: Embolization of spinal cord arterio-venous malformations with an ethylene vinyl alcohol copo-lymer dissolved in dimethyl sulfoxide (Onyx liquid embolic system). Report of two cases. J Neurosurg 93 (2 Suppl): 304–308, 2000
14. Niimi Y, Berenstein A, Setton A, Pryor J: Symptoms,Vascular anatomy and endovascular treatment of spinal cord arterio-venous malformations. Interv Neuroradiol 6 (Suppl 1):199–202, 2000
15. Ohata K, Takami T, El-Naggar A, Morino M, Nishio A, In-oue Y, et al: Posterior approach for cervical intramedullary arteriovenous malformation with diffuse-type nidus. Report of three cases. J Neurosurg 91 (1 Suppl):105–111, 1999
16. Panciani PP, Fontanella M, Crobeddu E, Schatlo B, Bergui M, Ducati A: Spontaneous occlusion of a spinal arteriovenous malformation: is treatment always necessary? Case report. J Neu rosurg Spine 12:397–401, 2010
17. Riché MC, Melki JP, Merland JJ: Embolization of spinal cord vascular malformations via the anterior spinal artery. AJNR Am J Neuroradiol 4:378–381, 1983
18. Rodesch G, Hurth M, Alvarez H, David P, Tadie M, Lasjaunias P: Embolization of spinal cord arteriovenous shunts: morpho-logical and clinical follow-up and results—review of 69 con-secutive cases. Neurosurgery 53:40–50, 2003
19. Rodesch G, Hurth M, Alvarez H, Lasjaunias P: Embolisation of spinal cord arteriovenous malformations with glue through the anterior spinal axis. Review of 20 cases. Interv Neurora-diol 3:131–143, 1997
20. Rosenblum B, Oldfield EH, Doppman JL, Di Chiro G: Spinal
arteriovenous malformations: a comparison of dural arterio-venous fistulas and intradural AVM’s in 81 patients. J Neuro-surg 67:795–802, 1987
21. Sinclair J, Chang SD, Gibbs IC, Adler JR Jr: Multisession Cy-berKnife radiosurgery for intramedullary spinal cord arterio-venous malformations. Neurosurgery 58:1081–1089, 2006
22. Spetzler RF, Detwiler PW, Riina HA, Porter RW: Modified classification of spinal cord vascular lesions. J Neurosurg 96 (2 Suppl):145–156, 2002
23. Srivatanakul K, Songsaeng D, Ozanne A, Toulgoat F, Lasjau-nias P: Spinal arteriovenous malformation associated with syringomyelia. Report of 4 cases. J Neurosurg Spine 10: 436–442, 2009
24. Tai PA, Tu YK, Liu HM: Surgical treatment of spinal arte-riovenous malformations: vascular anatomy and surgical out-come. J Formos Med Assoc 100:389–396, 2001
25. Ushikoshi S, Hida K, Kikuchi Y, Iwasaki Y, Miyasaka K, Abe H: Treatment of intramedullary arteriovenous malformations of the spinal cord. Interv Neuroradiol 6 (Suppl 1):203–207, 2000
26. Veznedaroglu E, Nelson PK, Jabbour PM, Rosenwasser RH: Endovascular treatment of spinal cord arteriovenous malfor-mations. Neurosurgery 59 (5 Suppl 3):S202–S209, 2006
27. Vodoff MV, Gilbert B, Le Breton F, Rodesch G, Laroche C, Lagarrigue JF, et al: [Paraplegia and medullary arteriovenous malformation. Role of surgery, corticosteroids and emboliza-tion.] Arch Pediatr 8:608–610, 2001 (Fr)
28. Williams FC, Zabramski JM, Spetzler RF, Rekate HL: An-terolateral transthoracic transvertebral resection of an intra-medullary spinal arteriovenous malformation. Case report. J Neurosurg 74:1004–1008, 1991
29. Zozulya YP, Slin’ko EI, Al-Qashqish II: Spinal arteriovenous malformations: new classification and surgical treatment. Neu rosurg Focus 20(5):E7, 2006
Manuscript submitted November 14, 2011.Accepted March 13, 2012.Please include this information when citing this paper: pub-
lished online April 6, 2012; DOI: 10.3171/2012.3.SPINE11982.Supplemental online information:
Video 1: http://mfile.akamai.com/21490/wmv/digitalwbc.download. akamai.com/21492/wm.digitalsource-na-regional/spine11-982_video_1.asx (Media Player).http://mfile.akamai.com/21488/mov/digitalwbc.download.akamai.com/21492/qt.digitalsource-global/spine11-982_video_1.mov (Quicktime).Video 2: http://mfile.akamai.com/21490/wmv/digitalwbc.download. akamai.com/21492/wm.digitalsource-na-regional/spine11-982_video_2.asx (Media Player).http://mfile.akamai.com/21488/mov/digitalwbc.download.akamai.com/21492/qt.digitalsource-global/spine11-982_video_2.mov (Quicktime).
Address correspondence to: Robert F. Spetzler, M.D., Neurosci-ence Publications, Barrow Neurological Institute, St. Joseph’s Hos-pital and Medical Center, 350 West Thomas Road, Phoenix, Arizona 85013. email: [email protected].