Embed Size (px)
Citation preview
CHHS18/110
Canberra Hospital and Health ServicesClinical Procedure Spinal Injury Management of the Adult Contents
Contents....................................................................................................................................1
Purpose.....................................................................................................................................3
Scope........................................................................................................................................ 3
Section 1 - Spinal Immobilisation..............................................................................................4
1.1 Logrolling.........................................................................................................................4
1.2 Head Immobilisation.......................................................................................................5
1.3 Trauma Soft Collars.........................................................................................................8
1.4 Cervical Spine Clearance in the Trauma Patient..............................................................8
1.5 Spinal Orthosis..............................................................................................................10
1.6 Bedrest Management....................................................................................................13
1.7 Spinal Traction...............................................................................................................14
Section 2 – Spinal Surgery.......................................................................................................19
2.1 Pre-operative................................................................................................................ 19
2.2 Post-operative...............................................................................................................20
2.3 Anterior Cervical Discectomy and Fusion (ACDF)..........................................................21
Section 3 - Spinal Observations and Assessment....................................................................21
3.1 Spinal Injury Management and Treatment Plan............................................................21
3.2 Traumatic Spinal Injury and Spinal Surgery Observations.............................................22
Implementation...................................................................................................................... 24
Related Policies, Procedures, Guidelines and Legislation.......................................................24
References.............................................................................................................................. 25
Definition of Terms................................................................................................................. 27
Search Terms.......................................................................................................................... 27
Attachments............................................................................................................................28
Attachment 1 Level of precaution required - assessed using the definitions for the 3 Protocol Groups..................................................................................................................29
Attachment 2: The Canadian C-Spine Rule..........................................................................31
Attachment 3: Spinal precaution for the unconscious trauma patient...............................32
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 1 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
Attachment 4: Spinal precautions for the alert (GCS> 15) trauma patient.........................33
Attachment 5: Indications for the use MRI in the management of patients with a potential spinal injury.........................................................................................................................34
Attachment 6: Spinal injury management and treatment pla.............................................35
Attachment 7: Traumatic spinal injury and spinal surgery observation chart.....................36
Attachment 8: Motor Grading Scale....................................................................................38
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 2 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/110
Purpose
The purpose of the Spinal Management Clinical Procedure is to outline the process for optimal care and management of spinal injuries and disorders in adult patients of Canberra Hospital and Health Services
This procedure provides information for any clinicians who care for patients with a spinal injury or requiring spinal surgery in the acute hospital setting.
Standardisation of practice means delivery of best practice, continuity of care and optimal clinical outcomes for the patients of the Canberra Hospital and Health Services.
Back to Table of Contents
Scope
This clinical procedure is applicable to all Canberra Hospital and Health Services (CHHS) patients who have presented with a suspected spinal injury, those who have had radiological confirmation of a spinal injury and patients admitted for surgical management of a spinal disorder.
The document applies to staff working within their scope of practice including: Medical staff Registered and Enrolled Nurses Tertiary students under supervision Allied Health Professionals all
Consultants responsible for clearance of the cervical spine following review and reporting of the appropriate cervical spine imaging by a consultant radiologist or senior radiology registrar: Neurosurgeon (or senior neurosurgical registrar/fellow) General/Trauma surgeon Intensive Care Physician Emergency Physician Orthopaedic spine surgeon A registrar from the above specialties after discussion with their senior consultant.
ALERT: In the consideration of spinal precautions and logrolling, head immobilisation should
only be performed by Medical Officers or Registered Nurses, on completion of the appropriate training. Student nurses, medical students and wardsman to assist under strict guidance and supervision.
Back to Table of Contents
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 3 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
Section 1 - Spinal Immobilisation
Spinal immobilisation in trauma is practiced in the management of potential and actual spinal injuries. It is usually initiated in the pre hospital setting before being maintained up to the point of medical clearance within the hospital setting. Immobilisation procedures include surgical fixation, orthosis application, spinal logrolls and traction including Gardner Well Tongs and Halo and Vest.
Evidence suggests that over 5% of patients admitted presenting with a spinal injury experience the onset or worsening of neurological symptoms once they reach hospital. This is not only attributed to worsening ischaemia or spinal cord oedema but also to inadequate immobilisation of the spine. In addition to protecting the patient from worsening injury, immobilisation also plays a role in controlling pain associated with column fractures and soft tissue injuries (Attachment 1).
The main aims of care for patients with a potential or confirmed spinal injury are to prevent further spinal injury, prevent complications from immobilisation and timely clearance of the spine. The level of precaution required can be assessed using the definitions for the 3 Protocol Groups outlined in Attachment 1.
1.1 Logrolling Logrolling is performed to provide pressure area care, examine skin integrity, assess for further injury, during thoracolumbar spinal clearance and to protect the airway in the instance of vomiting etc. The main aim of this technique is to support and maintain the natural anatomical alignment of the spine.
The number of staff required and the technique itself is dependent on the level of injury. This should be identified from medical documentation in the patient’s clinical record or in the instance of potential spinal injury; guided by the trauma team leader.
1. The patient should be supine and anatomically aligned prior to commencement of the logrolling procedure
2. Explain the procedure to the patient, asking them to lie still, cross their arms across their chest to prevent twisting motion and refrain from assisting
3. Ensure any lines or medical devices i.e. indwelling catheters, intercostal catheters, are clear and reposition them where necessary to avoid dislodgement
4. If the patient is intubated or has a tracheostomy tube, airway suctioning prior to log rolling is recommended to prevent coughing and anatomical misalignment
5. Position the bed at a suitable height for staff, if cervical precautions required the height should be suitable for the ‘head holder’
6. Assistant 1, the assistant supporting the upper body, place one hand over the patient’s shoulder to support the posterior chest area, and the other hand around the patient’s hips
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 4 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/110
7. Assistant 2, the assistant supporting the patient’s abdomen and lower limbs, overlaps with assistant 1 to place one hand under the patient’s back, and the other hand over the patient’s thigh
8. The ‘head holder’, the clinician who leads the roll, directs assistants 1 and 2 when the roll will be initiated (ON the count of three)
9. Again, on direction from the ‘head holder’, the patient is turned in anatomical alignment in one smooth action
10. Assistant 3 completes the planned activity (pressure area care etc.)11. The head holder will direct the assistants to either return the patient to the supine
position (ON the count of three) or to support the patient in a lateral position with wedge pillows. The patient should be left in correct anatomical alignment
12. Consider whether the intubated patient or patient with a tracheostomy requires further suctioning post roll.
1.2 Head ImmobilisationPrior to cervical spine clearance or when a cervical injury has been diagnosed, a patient’s head should be immobilised during a log-roll, position change or when a cervical collar is removed.
The main aim is to maintain the patient’s head in anatomical alignment and prevent flexion, extension and lateral tilting. The patients head is always held from the top of the bed
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 5 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
however there are other techniques such as head and trapezius holds depending on clinician preference and environmental constraints.
1. If a collar is insitu, ensure that it is well fitted prior to commencement of roll2. Head Hold: The thumb and forefingers of both hands are extended allowing the rest of
the fingers to shrug the occiput. The forefingers are folded along the line of the sternocleidomastoid muscle and the thumbs provide support along the angle of the jaw.
If the patient is intubated the hand which is supporting the opposite side to which is being rolled on, can support the endotracheal tube
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 6 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
Trapezius Hold: With the forearms in a supinated position and with the thumbs extended, slide the fingers under the trapezius muscles bilaterally with thumbs resting over the clavicles (and alongside the collar if insitu). In this hold, the forearms are used to immobilise/support the patient’s head during the log-roll.
3. The ‘head holder’ is the team leader throughout the process of logrolling. They must ensure that all assistants are in correct position and ready to commence
4. Once assured that all assistants are ready, call ‘on my count of three: a. one, two, three, and roll should occur ON three
5. This process repeats on return to resting position – ‘back on my count of three;a. one, two, three’
6. The ‘head holder’ must continue to support the head until completion of the procedure or for as long as the patient is being repositioned, i.e. slide sheet up the bed
ALERT.Clinicians should always be aware of the risk of neurogenic shock in severe acute spinal injury with possible cord involvement. Neurogenic Shock, is defined as vascular hypotension with associated bradycardia usually resulting from traumatic disruption of the sympathetic outflow between (T) 1 and Lumbar (L) 2 and the subsequent unopposed vagal tone. The degree of risk is related to the severity of neurological injury but clinicians should be vigilant as neurogenic shock can progress to cardiac arrest.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 7 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
1.3 Trauma Soft CollarsMajor trauma patients are considered to have sustained spinal trauma until proven otherwise and are immobilised as a precaution. Injuries to the cervical spine occur in2-6.6% of major trauma patients, and of the patients with missed or delayed diagnosis of cervical spine injury, 70% had altered levels of consciousness.
The potential spinal patient must be immobilised and a temporary soft collar is applied at the trauma scene to physically and consciously acknowledge the possibility of a spinal injury but also dramatically reduce the risks associated with a rigid hard collar such as pressure injury, raised intracranial pressure, ventilation impairment and patient discomfort/anxiety.
The only contraindication for the application of soft collars would be if the patient with a potential spinal injury was uncooperative with spinal precautions due to confusion, in which case they should have it changed to a Miami J for greater control of the neck and to optimise patient safety.
On arrival to The Canberra Hospital patients with this collar insitu must be managed with full spinal precautions as outlined in Section 1.1 and 1.2. Until their cervical spine has either been cleared of injury, at which time they should have their collar removed and precautions lifted; or an injury has been diagnosed and they should be changed to a Miami J collar or to other longer term immobilisation (Section 1.5, 1.7).
1.4 Cervical Spine Clearance in the Trauma Patient1. All unconscious trauma patients and conscious trauma patients where cervical injury is
highly suspected, must have spinal precautions instituted upon arrival to the Emergency Department (ED) (Attachment 1).
2. Full spinal precaution for the unconscious patient until cervical Computer Tomography (CT) performed, cleared and documented (logrolling continues without head hold until thoracolumbar X-Ray also performed, cleared and documented). (Attachment 3)
3. In alert (Glasgow Coma Scale (GCS) 15) trauma patients with a suspected cervical spine injury Clinical exam should follow Canadian C-Spine rule. (Attachment 2)
Canadian C-Spine Rule (Attachment 2)
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 8 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
Patients considered of being at high risk of cervical spine (c-spine) injury - radiography is recommended: Age >65 years Dangerous Mechanism or
a. Fall from elevated height (>2m/5 stairs)b. Axial load to the headc. High speed Motor Vehicle Accident (MVA) (>100km/hr), rollover or ejectiond. Motorised recreational vehicle collisione. Push bike accident
Paraesthesia in extremities
If the following criteria are met the patient is at low risk but still mandates radiography. Rear ending MVA which was either:
a. Pushed into oncoming trafficb. Hit by a bus or large vehiclec. Hit at high speedd. Caused rollover
Cannot sit up in ED comfortably Cannot ambulate comfortably Had immediate onset of neck pain at time of accident Has midline c-spine tenderness
4. If answering NO to the above criteria, the patient may be safe for range of motion assessment. Assess the patient’s ability to actively rotate the neck 45° left and right; if unable, the patient requires radiography, if able, the c-spine is cleared.
There should be a high index of suspicion and a low threshold for imaging when examining patients with pre-existing conditions such as ankylosing spondylitis, previous c-spine surgery or fractures.
5. Where clinical exam is unreliable or where radiographic assessment is required, a CT scan from occiput to T4 should be performed
6. Magnetic Resonance Imaging (MRI) may be required if CT images are abnormal, if midline tenderness is present or if neurological signs are present
7. Clinically insignificant injury, as deemed by Shock Trauma or Neurosurgery, may result in c-spine clearance
8. Only once c-spine clearance is clearly documented in patient’s clinical record by one of the following may the position restrictions be lifted and collar removed: Neurosurgeon (or senior neurosurgical registrar/fellow) General/Trauma surgeon Intensive Care Physician Emergency Physician Orthopaedic spinal surgeon A registrar from the above specialties only after discussion with their senior
consultant*
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 9 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
If imaging is abnormal, clinically significant or an unstable injury exists; the patient will be referred for consultation by Neurosurgery
9. If it is expected that a patient will require a cervical collar for >24hrs, a Miami J collar should be fitted by the physiotherapist, medical officer or registered nurse, on completion of the appropriate training (see section 1.5)
10. A Spinal Management Plan (Attachment 5) should be completed by neurosurgical or shock/trauma registrar or consultant outlining appropriate management and restrictions.
1.5 Spinal OrthosisSpinal Orthoses (brace, splint, or other artificial external device serving to support the spine) are prescribed to patients as an immobilisation device during the diagnostic phase (in the instance of possible cervical injury) and for stabilisation and management of a confirmed fracture. Appropriate orthosis are prescribed by Neurosurgical or Shock/Trauma registrars/consultants and should be suitably fitted by qualified Physiotherapists, Medical Officers or Registered Nurses.
Miami J CollarSuspected and confirmed cervical injuries are managed with the application of a cervical collar. 1. For a conscious and cooperative patient, a soft collar with the alert sticker “C-spine Not
Cleared” will be applied in the pre hospital setting which is used to consciously and physically acknowledge a potential c-spine injury and to prompt the use of spinal precautions when repositioning, but not to immobilise. It is felt that a fully awake and alert patient will stabilise their own spine, with muscle spasm and pain providing adequate immobilisation and the risks associated with rigid trauma collars eliminated. These soft collars remain insitu until the c-spine has been cleared, in which case they can be removed, or until an injury has been confirmed.
2. For a patient with a decreased level of consciousness or who is uncooperative, a rigid trauma collar will be fitted in the pre hospital setting.
3. If an injury has been radiographically confirmed, or a patient has had a rigid trauma collar on within 4 hours of admission, a Miami J collar should be fitted. Extended application of rigid collars can cause pressure injuries, increase intracranial pressure, restrict venous return, increase patient discomfort and aspiration risk.
Initially, a Miami J collar should be fitted by the physiotherapist, medical officer or registered nurse, on completion of the appropriate training and worn for the time prescribed by the treating/consulting Neurosurgeon.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 10 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/110
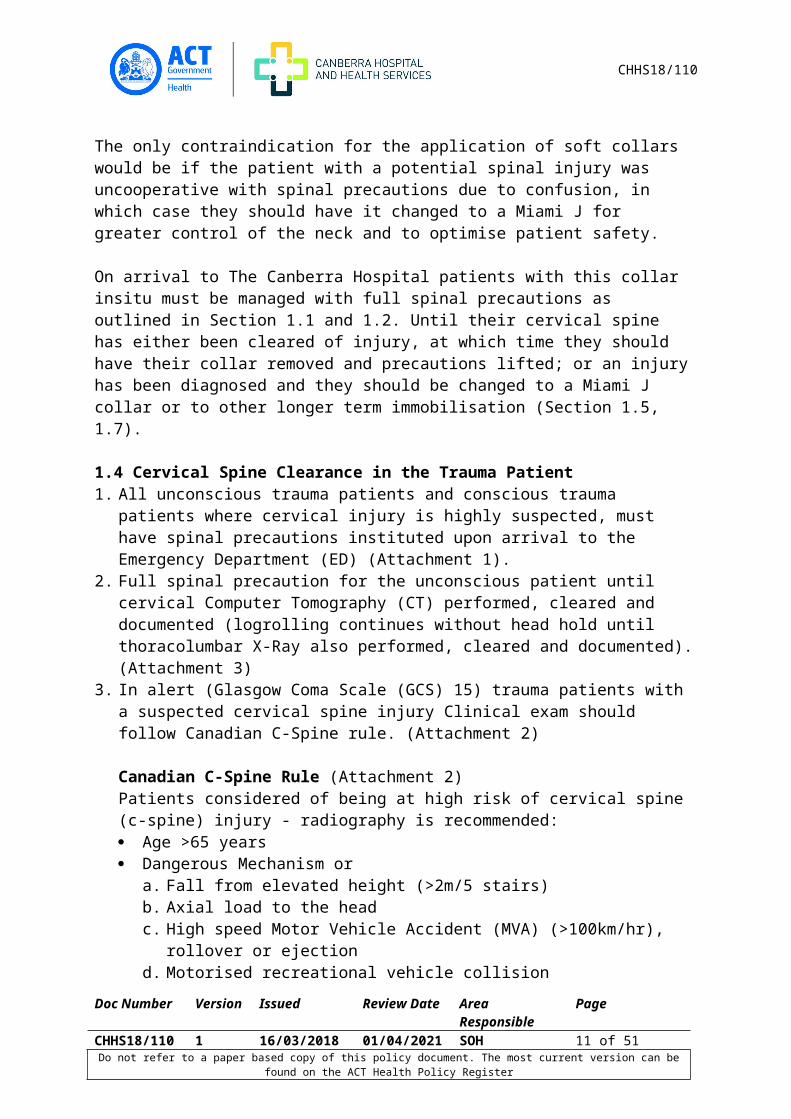
1. Size it up: Use your fingers to observe and determine the vertical distance between the highest point of the trapezius and the top of the chin when the head is in the desired treatment alignment.
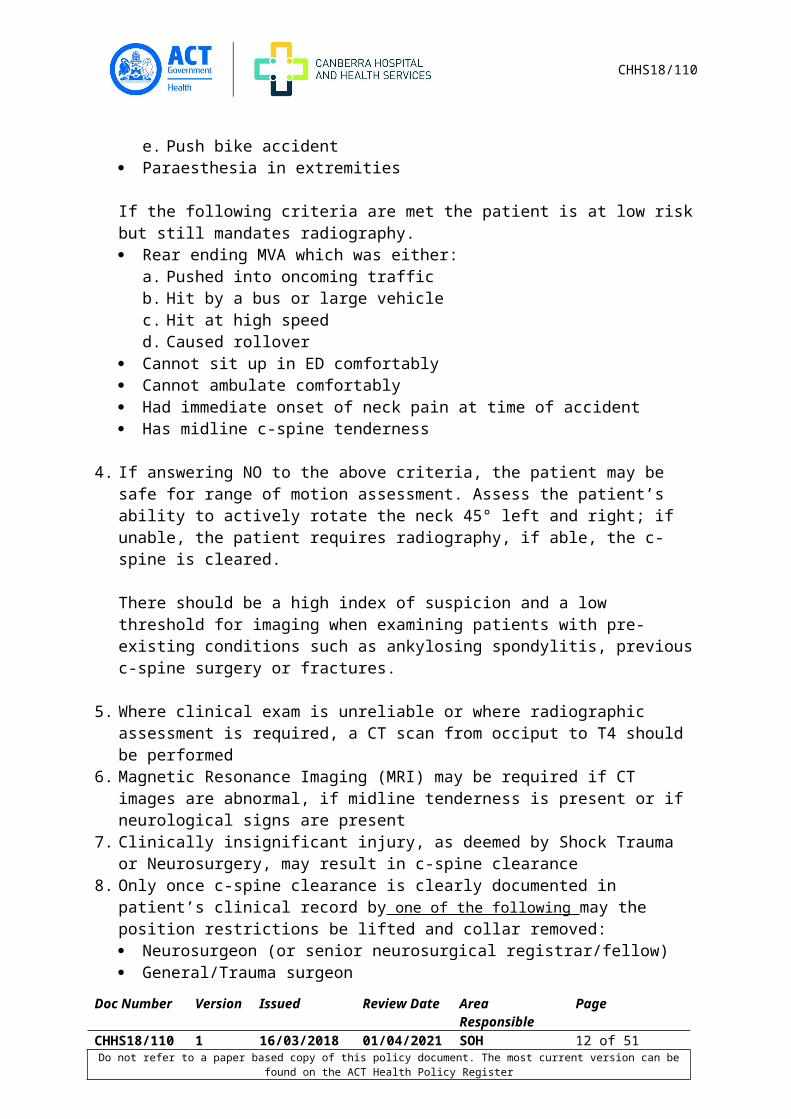
2. Select appropriate collar size by using the distance observed in step 1 and corresponding it to the distance from the top of the Velcro strap to the bottom edge of the collar plastic.
3. Miami J sizes are phenotype-driven according to sizing silhouettes and come in Adult Tall, Regular, Short as well as specialty sizes Stout, Super Short and Extra Small.
4. Two persons are needed for initial collar placement: one to maintain the patient’s head and neck in proper alignment, the second to fit the collar.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 11 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/110
5. Remove any pillows from behind the patient’s head. Position patient with arms to the side, shoulders down and head centrally aligned.
6. Slide the Back Piece behind the patient’s neck and centre it. To avoid pushing/pulling on the patient, push down into the mattress during slide and avoid towels or other materials which will increase friction. Ensure the blue Sorbatex™ padding extends beyond the edge of the hard plastic.
7. To apply the front, flare the sides out, slide it up the chest wall and ‘scoop’ up to achieve a neat fit under the chin. Caution must be taken to ensure that the head is not extended during this process.
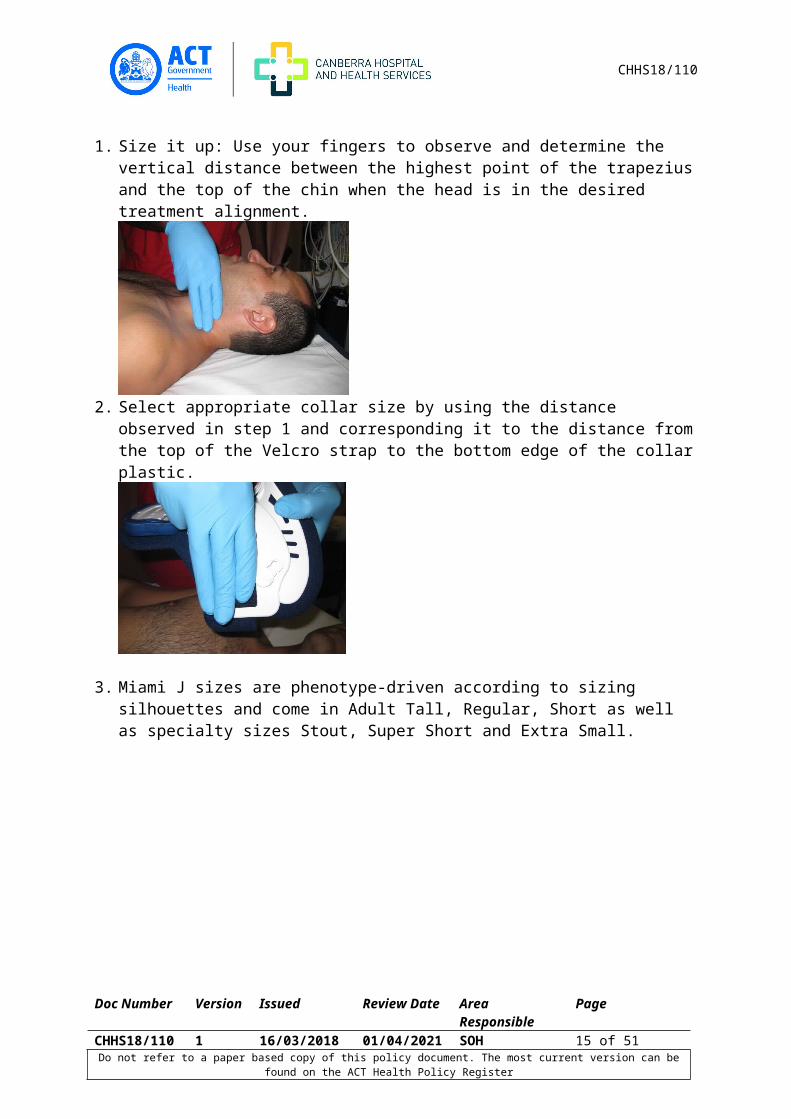
8. Orient the sides of the collar up, away from the trapezius, and toward the ears.9. Place the front of collar inside the back, lining the blue Velcro straps up with the ‘buddy’
Velcro on the collar
10. Tighten straps alternately, one at a time, ensuring that they finish up equal in length (an indication that both the front and back are centred to the midline).
If the patient can slip his/her chin inside the collar, it is clear indication that it is not snug enough and proper alignment is not being maintained.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 12 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
11. Miami J collars should be removed DAILY, at a minimum, to inspect skin integrity and change the blue Sorbatex padding. Each patient should have 2 sets of padding to be interchangeable, when removed they should be washed in warm soapy water, rinsed and air dried (a mechanical dryer will shrink the pads) ready to use the next day.
12. Any removal of the collar should be in supine position and two people required, one to maintain alignment and one to provide cares (unless otherwise specified in ‘CHHS Spinal Management Plan’ by the neurosurgical registrar).
Pressure injuries can easily occur underneath the Miami J collar, especially on bony prominences such as sternum, clavicles and occiput as well as trapezius. Underlying skin should be inspected for redness or signs of pressure injury when collar removed or patient reporting any irritation. Any areas of redness should have management strategies applied as soon as they are observed. Check blue Sorbatex padding is covering rigid plastic edges Ensure Velcro straps are aligned with buddy Velcro so ensuring appropriate fit Apply mepilex border dressings to reddened or irritated areas to offload pressure.
Bulkier dressings such as combine will increase pressure and should be avoided. If pressure injury noted, follow normal procedure including referral to Tissue Viability
Unit and completing RiskMan.
Thoracic, Lumbar and Sacral OrthosisFor management of confirmed thoracic, lumbar and sacral fractures, orthoses may be prescribed. The type of orthosis will differ depending on the level of injury, as well as restrictions for donning and doffing dependant on stability of fracture (and specified in CHHS Spinal Management Plan by a neurosurgical consultant, registrar or nursing Team Leader. (Attachment 5)). These braces will be fitted by a physiotherapist who has completed the appropriate competency. Daily donning and doffing of brace in line with prescription attended by Nursing Staff, physiotherapists or medical officers who have completed the competency.
1.6 Bedrest ManagementNon operative management of spinal fractures may include a period of bedrest at the prescription of the neurosurgical consultant and will be documented on the Spinal Injury Management and Treatment Plan (Attachment 5) along with associated bed mobility restrictions.1. Provide patient education regarding bed rest procedure and orientate to ward routines.
Inform of risks associated with extended periods of bedrest and educate on deep breathing and coughing exercises, VTE and Pressure Injury prevention. Include signs and symptoms to be aware of and to report to nursing staff. (i.e. tender calf muscles, shortness of breath)
2. Nurse patient resting in bed with head of bed height and whole bed tilt as directed by surgeon
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 13 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
ALERT.Spinal patients are not to have alternating air mattress unless approved by neurosurgical team.
3. Step down vital sign observations and spinal observations as suitable. Any decrease to observation frequency should only be after consultation with surgical team. Measure patient for TED’s and apply, ensure these are worn every shift
4. Ensure regular aperients charted and commence bowel chart to ensure bowels open consistently. Notify > 2 days of bowels not open to treating team and consider enema
5. If suitable for portable bedbath (as documented on the Spinal Injury Management and Treatment Plan (attachment 6)) offer this to patient as option for personal care – encourage independence where able
6. Monitor patient for signs of depression or inability to cope with treatment plan. Notify team if suspected and consider Psychology referral for coping strategies
7. Ensure physiotherapist aware of planned date to mobilise so that appropriate orthosis may be measured for and sourced if required.
1.7 Spinal TractionGardner Wells Tongs Applied either in the neurosurgical acute care unit or in the operating theatre, Gardner Wells Tongs are indicated in cases of facet subluxation or dislocation, and in burst-type fractures. Gardner Wells Tongs immobilise the cervical vertebrae, reduce a fracture and/or dislocation, reduce pressure on the spinal cord in the instance of a burst fracture and provide relief from the pain associated with malalignment.
Equipment Traction bed with head bar and pulley. Gardner Wells Tongs Double cord Local anaesthetic Betadine Blue under pads Clippers Syringes and needles Tap water Leukoplast strapping Weight bag and S hook Sterile gloves and gown Sand bags x 2
Procedures1. Consent is obtained by attending Registrar or consultant2. Assess the patient’s level of understanding of the immobilisation process and educate
the patient and significant others about the immobilisation process.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 14 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/110
3. Facilitate preparation of the patient by ascertaining the type of traction prescribed by the treating MO
4. Administer premedication/analgesia as prescribed5. Position the patient in the supine position in centre of the bed to ensure the line of pull
will be correctly set up6. The scalp may be clipped in the temporal region superior to the ear depending on
preference. The scalp is prepared with Betadine and the insertion sites are infiltrated with local anaesthetic. The tongs are positioned by the MO with the sterile points contacting the skin at the predetermined sites of placement. The points are then advanced until the position of the spring-loaded points shows that the proper pressure is being exerted. An assistant may be necessary to hold the metal ring of the tong. Weights are applied via a double cord to reduce the fracture-dislocation. A cervical spine x-ray may be obtained to evaluate vertebrae alignment.
7. Position either head bar/pulley at the head of the traction bed ensuring the line of pull will be in alignment with the cervical spine
8. Apply traction by tying a double cord (two separate cords) to the tongs and passing it straight over the pulley. Tie double cord to S-hook and attach weight. Ensure the correct weight is applied and that the weight hangs freely if the height of the bed is adjusted. Secure knots by taping the loose end to the main body of the rope as taping the actual knot will make observation and adjustments difficult.
9. The MO may request that the bed be tilted with the foot down to maintain counter traction
10. Monitor neurological status including spinal observations (Attachment 7) and vital signs hourly for 4 hours and then Q4/24 for duration (or more frequently if prescribed and documented in the patient’s clinical record)
11. Inspect pin sites each shift. Clean with normal saline, monitor for any signs of infection and report these to MO
12. MO should document specific instructions for patient log roll. Ensure Q3/24 turns for pressure injury prevention following spinal precautions outlined in Section 1.2 (NOTE: traction is NOT to be removed when rolling patient. Attend normal c-spine precautions including head hold whilst maintaining traction)
13. Apply anti-embolic stockings and sequential compression devices, encourage deep breathing and leg exercises. Educate patient on the signs and symptoms of VTE and pressure injuries
14. Administer low dose Heparin, analgesia, aperients and antispasmodics as prescribed by the MO
15. Patients with Gardner Wells tongs will have progressive cervical spine x-rays which can be done on the ward with a mobile x-ray. If patient is required to move anywhere within the hospital they require a registered nurse escort and traction should never be removed without specific documentation from a consultant or registrar and even then, manual traction must be applied.
16. Refer for consult with Physiotherapist, Social Worker, Dietician, speech pathologist and Occupational Therapist
17. If patient has cervical surgery ensure all relevant equipment for Gardner Wells tongs is returned to the ward from the Operating Theatre.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 15 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
Crown Halo and VestCrown halo and vest is utilised as a non-operative stabilisation of unstable high cervical spine fractures. They provide precise positional control of the cervical spine while allowing early mobilisation and shorter hospital stay for the patient.
Equipment1. Pre-packaged halo ring (measured for size as per below), including bolts and halo clamps2. Pre-packaged vest with synthetic liner (measured for size as per below) including
transverse bars, connectors and bolts3. Tape measure and sizing chart4. Positioning spoon5. Titanium skull pins with locking nuts x 5 (1 pack)6. Hair clippers7. Local anaesthetic, drawing up needle and syringes8. Basic dressing pack with extra gauze squares9. Sterile gloves10. Torque pin driver and wrench (kept in Neurosurgical Registrar’s office)11. Ossur (manufacturer) ‘Patient Information Manual’
Procedure1. Explain the procedure to the patient.2. Gain consent3. Measure the greatest circumference of the skull (about ½” above the ears)
4. Choose the appropriate size Ossur halo ring as per table below
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 16 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
ALERTWith proper placement of the tongs and continuous traction, the patient should have only minimal pain which should be relieved by medication. Notify MO immediately if the patient experiences undue discomfort or change in neurological status. Muscle spasms are a common discomfort rather than pain – notify MO to consider diazepam.
CHHS18/110
5.SIZE CHART
_______________________________________________________________________________
SIZE HEAD CIRCUMFERENCESMALL 43-51 cmSTANDARD 51-59 cmLARGE 59-66cm
6. Measure the patient’s chest circumference at the xyphoid process.
7. If patient has a pendulous abdomen, measure around the widest part of the costal margin and the sternal length to ensure appropriate fit.
8. Choose applicable Ossur vest size as per table below.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 17 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/110
SIZE CHART_____________________________________________________________________________SIZE Chest CircumferenceX-SMALL 50-66 cmSMALL 66-84 cmSMALL/MEDIUM 81-92 cmMEDIUM 84-102 cmMEDIUM/Large 96-107 cmLARGE 102-117cmX LARGE 117-132 cm
9. Administer analgesia/premedication as ordered and reassess/administer as required during the application process
10. The positioning spoon may be placed under the patient using spinal precautions.11. Before moving a patient on whom a crown/halo vest has been applied, 15mins post
application, the MO will re-torque the skull pins using the four remaining torque limiting caps and then secure the locking nuts on all four pins against the crown/halo using the wrench. A final check of all the bolts for tightness is performed
12. The MO will then re-torque the skull pins further using the torque pin driver at 24 and 48 hours after initial application and every 2 to 3 weeks during treatment process
13. Patient to remain resting in bed with restrictions as documented by the MO until post procedure X-Ray has been performed to confirm correct alignment
14. Monitor spinal observations (Attachment 7) and vital sign observations 1/24 for 4 hours then 4/24 for 24 hours if stable unless otherwise requested by MO. Ensure patient is aware of the need to report pain and sensory changes post procedure.
15. Await documented clearance from MO before mobilising the patient. Once cleared patients should get out of bed by rolling onto their side at the edge of the bed, and dropping their legs off the edge and pushing sideways with their elbow and hand at the same time. This method puts less stress on the front pins. Spinal observations should be attended at time of mobilisation and then two hours post, if stable then may be ceased.
16. Pin sites are cleaned daily using normal saline and gauze swabs or may be cleaned with shampoo on hair washing days (conditioner should not be used). Provide patient education on performing this daily at home once discharged. If patient unable to, refer to Community Nursing on discharge or educate family members
17. Observe pin sites and educate the patient on reporting any of the following: Inflammation, swelling and/or discharge Tracking (open area where the skin has pulled away from the pin) Pain or tenderness around the pin site Clicking noise reported by the patient
18. It is important to keep the patient’s skin and fleece liner as clean as possible because the liner should not be changed unless it is medically necessary. No soap, lotion or powder should be used under the vest because it cannot be adequately removed and may irritate the skin. To wash the skin under the vest, use a fibrella wipe that has been wrung out in warm water. Pull it back and forth in a drying motion beneath both front and back
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 18 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
portions of the vest. The skin under the vest should be inspected daily with a torch in order to detect pressure areas. Extra fleece or foam may be inserted to relieve pressure points that may occur when the patient assumes certain positions. Try to keep the synthetic vest liner dry at all times, however if the lining gets wet, dry it with a hair dryer on a cool setting.
19. If the vest liner should get soiled it may have to be changed by the MO.
20. The patient can shower rest of the body using a hand held shower hose or have a sponge bath. If the patient is mobile they can have a shallow bath, ensuring that the bottom of the vest is protected with plastic.
21. Provide the patient with the Ossur ‘Patient Information Manual’
Back to Table of Contents
Section 2 – Spinal Surgery
Pre and post-operative procedure for the management of patients who are undergoing either elective surgery for a disorder of the spine (excluding Anterior Cervical Discectomy and Fusion), or following surgical management of an acute spinal injury.
2.1 Pre-operative1. Explain the procedure to the patient and ensure identification label is on wrist2. Nurse patient in accordance with spinal management plan documented by registrar or
consultant and assist with log rolling as required3. Ensure consent is signed – re consent will have to be completed if original was signed
>24 hours previously4. If not already collected in pre-admission clinic, ensure that the following routine bloods
have been collected and that results are available prior to the patient going to theatre: Full blood count (FBC), urea, electrolytes and creatinine (UEC), blood glucose level
(BGL), full coagulation profile (FCP), Group & Hold5. Check bowels open recently, if not, consider aperients prior to theatre6. Check and record full set of vital sign observations and baseline spinal observations
(Attachment 6). Note any pre-existing neurological deficit7. Weigh patient and document8. Give pre-operative education as well as instructions regarding deep breathing and
coughing exercises, VTE and Pressure Injury prevention
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 19 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
ALERTLiners should not be changed, if it can be avoided, as loosening of the superstructure (vest) carries a risk of spinal malalignment.
AlertShould the patient require CPR while wearing the vest, the anterior portion of the vest must be removed. Unscrew the bottom knobs on the anterior portion of the vest to release to waist straps, place hand above the red line and bend the lower section away.
CHHS18/110
9. Fast from midnight (or as per CHHS ‘Fasting Guidelines – for patients undergoing procedures requiring sedation or anaesthesia), ensure appropriate intravenous therapy is charted and IVC insitu
10. Perform pre-operative patient wash and dress in inpatient gown11. Measure patient for TED’s and assist patient putting them on 12. Ensure adequate amount of patient labels 13. Complete Pre-operative Checklist.
Back to Table of Contents
2.2 Post-operativeIn addition to general post-operative care outlined in CHHS Post-operative Care and Handover Guideline
1. Attend spinal observations (attachment 7) ½ hourly x 2 hours Q1/24 x 4 hours, then if stable Q4/24
ALERT.Progressive neurological deterioration resulting from cord compression is a surgical emergency. Notify MO if any deterioration in limb movement, power or sensation.
2. Nurse patient resting in bed with head of bed height as directed by surgeon. Post-operative spinal patients are not to have alternating air mattress unless approved by neurosurgical team.
3. If staples insitu - replace dressing on day 2 with opsite, can be reinforced with combine and mefix if large amounts of ooze < 24 hrs postop. Monitor for potential CSF leak if postop ooze present
NOTE: If dermabond insitu – do not apply any dressings.
ALERT.If a dural puncture has occurred, patient may need to rest in bed, lying flat for ≥48hrs or as specified by Surgeon. Strict wound checks and monitoring for CSF leak is required.
4. Surgical drains generally removed day 1 unless high output post operatively or specified otherwise by neurosurgical team. Remove drain when ordered in accordance with CHHS Drain Management Clinical Procedure.
5. Encourage deep breathing, coughing and leg exercises, ensure TED stockings and sequential compression devices (SCD) insitu and source SCD pump from Central Equipment Store.
6. If patient cannot move self in bed, ensure appropriate Pressure Injury Prevention management strategies have been implemented and regular skin checks attended.
7. Routine post-op bloods – Day 1 – FBC, UEC.8. Mobilisation – as per surgeon’s orders in ‘Post-operative Instructions’. 9. Record bowels daily and respond early to concurrent days of bowels not open.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 20 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
10. Remove staples day 7-14, as directed by neurosurgeon11. Provide patient education regarding avoiding heavy lifting, avoiding long car journeys,
and driving restrictions for 4-6 weeks12. Discharge day 2-713. Patient will follow up with consultant in 6 weeks with spinal X-Ray, appointments
arranged by discharging MOBack to Table of Contents
2.3 Anterior Cervical Discectomy and Fusion (ACDF)In addition to the post-operative risks and management of spinal surgery outlined in section 1.2, patients who have undergone a Cervical Discectomy and Fusion with an anterior approach are at risk of localised oedema or haematoma which may cause obstruction of swallowing and potentially obstruction of airway resulting in a medical emergency.
First 12 hours postop1. Supervise patient during oral intake, observing for any signs of dysphagia or possible
aspiration. If any concerning signs cease oral intake, report to surgical team immediately for review and consider speech pathology
2. Closely assess airway patency and escalate any dyspnoea or stridor to surgical team immediately
3. Report any new or increasing hoarseness of voice or visible swelling immediately.4. Monitor exudrain hourly, ensuring patency of drainage will reduce the risk of
haematoma formation. Report sudden large volumes of frank drainage to surgical team and otherwise manage as per CHHS Drain Management Clinical Procedure.
ALERT. Airway obstruction from haemorrhage or oedema has rapidity of onset, potential for catastrophic consequences and requires an urgent need to act to ensure positive patient outcomes.
Back to Table of Contents
Section 3 - Spinal Observations and Assessment
3.1 Spinal Injury Management and Treatment PlanThe Spinal Injury Management and Treatment Plan form (Attachment 6) was developed to provide appropriate, safe and consistent care to patients with a spinal injury. This tool, which aids clinical handover, outlines restrictions placed on patient’s mobility, orthosis prescribed, donning and doffing orders and progress with patient education for discharge planning. This form is a clinical order and restrictions documented should be strictly adhered to. 1. To be completed by Surgical Consultant or Registrar only. Nursing Team Leader may
complete form only when restrictions have already been documented by the surgical team in the patient’s clinical record
2. Should be completed within 4 hours of admission to the inpatient setting.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 21 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
3. Updated as soon as patient’s condition changes and restrictions lifted OR further restrictions placed on mobility. New form to be completed and previous form voided and filed within the patient’s clinical record
4. To remain within the front of the patient’s bedside clinical folder and to accompany the patient throughout the organisation, i.e. ward to ward transfer, medical imaging.
3.2 Traumatic Spinal Injury and Spinal Surgery ObservationsThe Traumatic Spinal Injury and Spinal Surgery Observation chart (Attachment 7) is designed to objectively assess motor and sensory nerve function in patients with a spinal injury or who have undergone a spinal surgery. The aim is to identify any neurological compromise as a complication or deterioration in the patient’s condition, to provide documented baseline function prior to a spinal procedure and to confirm stability or improvement.
Procedure 1. To be commenced on admission to the Emergency Department, Post Anaesthetic
Recovery Unit (PACU) or the ward.2. For traumatic spinal injury - performed hourly until surgical fixation or treatment plan
documented. If for conservative management/bedrest, perform Q4/24 until stable for 72 hours then cease with clarification from neurosurgical team and nursing team leader. If for conservative management/orthosis, perform at time of first mobilised then after a further hour, continue Q4/24 until standing X-Ray reviewed and cleared by neurosurgical team post
3. Pre-operative elective spinal surgery – perform one baseline assessment4. Post-operative – ½ hourly for 2 hours, hourly for 4 hours then Q4/24 hourly until stable
for 72 hours or ceased with clarification from neurosurgical team or nursing team leader5. Begin with documenting level of injury or levels of surgery in the space provided
together with the need for traction or orthosis6. Based on dermatome map, if level above and including T3, both upper and lower motor
and sensory assessments required. If level below T3, only lower limb motor and sensory assessment required and upper limb section can be crossed out.
7. When a region cannot be assessed for other reasons i.e. limb amputation, traction, mark the corresponding box with ‘NT’ (not testable) and document the reason in the patient’s clinical record.
Motor Assessment (attachment 7)The following exercises must be performed to test motor function in the upper and lower limbs. After each exercise, a numerical score should be recorded for each muscle group using the Motor Grading Scale (0-5) (appendix 8)
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 22 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
Upper:1. Gain patient consent2. Shoulder Abduction – Place supporting hand on the patients shoulder and resisting hand
on the wrist/forearm. Ask patient to lift arm out from body, as they lift arm, apply resistance downward. Assessing the Deltoid muscle and axillary nerve (nerve root C5/C6)
3. Elbow Flexion – Place supporting hand on patients bent elbow and resisting hand on lateral wrist. Ask patient to flex arm towards the face and apply resistance downward. Assessing Biceps Brachii muscle a musculocutaneous nerve (nerve root C5/C6)
4. Elbow Extension - Place supporting hand on patient’s bent elbow and resisting hand on medial wrist. Ask patient to straighten arm and apply resistance in opposite direction. Assessing Tricep muscle and radial nerve (nerve root C5/C6/C7)
5. Wrist Flexion – Support patient’s forearm and ask them to make a fist and flex wrist upwards. Apply resistance downwards in attempt to straighten wrist. Assessing Flexor Capri Radialis and Flexor Capri Ulnaris and radial nerve (nerve root C7/C8)
6. Wrist Extension – Support patients forearm and ask them to make a fist and extend wrist downwards. Apply resistance upwards in attempt to straighten wrist. Assessing Extensor Carpi Ulnaris/ Radialis and Biceps plus radial nerve (nerve root C8/T1)
7. Finger Flexion – Curl the patient’s finger around yours (in a ‘monkey grip’) and ask the patient to resist you straightening their fingers. Pull gently in attempt to straighten fingers. Assessing Flexor Digitorum superficialis, Profundus muscles and Median and Ulnar nerve (nerve root C8)
8. Finger Abduction – Support patient’s wrist, ask patient to place their palm down and spread the fingers. Apply resistance on index and little finger attempting to bring them together. Assessing first Dorsal Interosseous muscles and Ulnar nerve (nerve root T1)
Lower:1. Gain patient consent2. Hip Flexion – Ask patient to bend their knee, place supporting hand underneath the
lower leg and apply resistance downwards through lower thigh/knee asking patient to bring knee up towards face. Assessing Iliopsoas muscle and lumbar sacral plexus (nerve root L1/L2)
3. Knee Flexion – ask patient to bend their knee, place supporting hand on lower thigh/knee, asking the patient to bend their knee further (bring heel to buttocks) and apply opposing force. Assessing hamstring muscle and sciatic nerve (nerve roots L5/S1)
4. Knee Extension – Ask patient to bend their knee, place supporting hand underneath knee and ask them to kick lower leg up straightening knee, apply opposite force. Assessing Quadricep femoris and femoral nerve (nerve root L3/L4)
5. Ankle Dorsiflexion – Place supporting hand on lower leg, ask patient to flex foot up, toes towards face and apply opposite resistance. Assessing anterior tibialis muscle and deep peroneal nerve (nerve roots L4/L5)
6. Ankle Plantar Flexion – place supporting hand on lower leg, ask patient point toes downwards, apply opposite resistance on ball of foot. Assessing gastrocnemius muscle and posterior tibial nerve (nerve root S1/S2)
7. Ankle Inversion – place supporting hand on lower leg and with feet hip width apart, ask patient to bring big toes towards the midline keeping legs still, inverting the ankle. Place
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 23 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
resistance on medial foot. Assessing tibialis posterior muscle and tibial nerve (nerve roots L4/L5)
8. Ankle Eversion - place supporting hand on lower leg and with feet hip width apart, ask patient to bring foot away from the midline keeping legs still, everting the ankle. Place resistance on lateral foot. Assessing peroneus longus and brevis muscles and superficial peroneal nerve (nerve roots L5/S1)
Sensory Assessment1. Gain patient consent2. Using hand touch, assess both medial and lateral limb and gain patient feedback. 3. Examiner should assess bilateral limbs simultaneously to identify subtle differences or
deficits. 4. Observations should be documented as an ‘X’ for present, tingling/pins and needles or
no sensation/numb.5. Specifics should be then documented in patient clinical record
Back to Table of Contents
Implementation
This document will be added to the orientation programs of applicable clinical areas. It will be published on the CHHS Policy and Guidance register and available for viewing or download by any ACT Health CHHS employee. Its contents will be presented in area specific in-services and referred to when completing relevant clinical competencies.
Back to Table of Contents
Related Policies, Procedures, Guidelines and Legislation
Policies Health Directorate Nursing and Midwifery Continuing Competence Policy Consent and Treatment CHHS Patient Identification and Procedure Matching Policy Modified Early Warning Scores (MEWS) Patient Controlled Analgesia (PCA) Management
Procedures CHHS Healthcare Associated Infections Clinical Procedure CHHS Aseptic Non Touch Technique CHHS Venous Thromboembolism (VTE) Prevention Procedure
Guidelines CHHS Fasting Guidelines – Elective and Emergency Surgery CHHS Post-operative Care and Handover
Legislation
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 24 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/110
Health Records (Privacy and Access) Act 1997 Human Rights Act 2004 Work Health and Safety Act 2011
Back to Table of Contents
References
1. American Association of Neurological Surgeons & the Congress of Neurological Surgeons (2001) Pre-hospital cervical spine immobilisation following trauma, Disorders of the Spine and Peripheral Nerves, American Association of Neurological Surgeons & the Congress of Neurological Surgeons, Chicago
2. Kwan I, Bunn F & Roberts I (2001) Spinal immobilisation for trauma patients (Review), The Cochrane Collaboration, 4:1-15
3. Flynn A V & Sinclair M (2005) Exploring the relationship between nursing protocols and nursing practice in an Irish intensive care unit, International Journal of Nursing Practice, 11(4):142-149
4. Clancy M (1999) Clearing the cervical spine of adult victims of trauma, Journal of Accident & Emergency Medicine, 16:208-214
5. Hedger A (2002) Clearance of cervical spines in adult trauma patients, Journal of Neurosurgical Nursing, 34:331-336
6. Morris CG, Mullan B (2004) Clearing the cervical spine after polytrauma: Implementing unified management for unconscious victims in the intensive care unit, Anaesthesia, 59:755-761
7. Hoffman JR, Mower WR, Wolfson AB et al (2000) Validity of a set of clinical criteria to rule out injury to the cervical spine with blunt trauma, New England Journal of Medicine, 343:94-99
8. Hoffman JR, Wolfson AB, Todd K & Mower WR (1998) Selective cervical spine radiography in blunt trauma: Methodology of the National Emergency X-Radiography Utilisation Study (NEXUS), Annuals of Emergency Medicine, 32:461-469
9. Marion DW, Domeier R, Dunham CM, Luchette FA, Haid R & Erwood SC (1999) Practice Parameter For Identifying Cervical Spine Instability Following Trauma: EAST Trauma Practice Guideline, Journal of Trauma, 44(6):941-956
10. Ackland H (2006) The Alfred Spinal Clearance Management Protocol, National Trauma Research Institute, accessed online at: http://www.ntri.com.au/events/13/SPINAL_CLEARANCE_MANAGEMENT_PROTOCOL.pdf
11. Ajani AE, Cooper DJ, Scheinkestrel CD, Laidlaw J, Tuxen DV. Optimal assessment of cervical spine trauma in critical ill patients: A prospective evaluation. Anaesth. Intensive Care. 1998;26:487-491.
12. Demetriades D, Charalambides BS, Chahwan S et al. Non-skeletal cervical spine injuries: Epidemiology and diagnostic pitfalls. J.Trauma. 2000;48:724-727.
13. Schenarts PJ, Diaz J, Kaiser C et al. Prospective comparison of admission computed tomographic scan and plain films of the upper cervical spine in trauma patients with altered mental status. J.Trauma. 2001;51:663-669.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 25 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/110
14. Pasquale M, Fabian TC. Practice management guidelines for trauma: EAST ad hoc committee on guideline development- identifying cervical spine instability after trauma. J. Trauma. 1998;44:941-956.
15. Hendy GW, Wolfson AB, Mower WR et al. Spinal cord injury without radiographic abnormality: Results of the National Emergency X-Radiography Utilisation study in blunt cervical trauma. J.Trauma. 2002;53:1-4.
16. Hills MM, Deane SA. Head injury and facial injury: Is there an increased risk of cervical spine injury? J Trauma. 1993;34:549-554.
17. Holly LT, Kelly DF, Counelis GJ et al. Cervical spine trauma associated with moderate and severe head injury: incidence, risk factors and injury characteristics. J Neurosurg. 2002;96:285-291.
18. Surgeons, A.C.O, 2012. Advanced Trauma Life Support: Program for Doctors. 9th ed. American College of Surgeons: A.C.O.S.T. Committee, Chicago: 366.
19. Iida H, Tachibana S, Kitahara T et al. Association of head trauma with cervical spine injury, spinal cord injury or both. J Trauma. 1999;46:450-452.
20. Bucholz RW, Burkhead WZ, Graham W, Petty C. Occult cervical spine injuries in fatal traffic accidents. J Trauma. 1979;19:768-791.
21. Reid DC, Henderson R, Saboe L et al. Etiology and clinical course of missed spine fractures. J. Trauma. 1987;27:980-986.
22. Davis JW, Phreaner DL, Hoyt DB. The aetiology of missed cervical spine injuries. J. Trauma. 1993;34:342-346.
23. Webster B, Giunti G, Young A et al. Work-related tetraplegia: Causes of injury and annual medical costs. Spinal Cord. 2004;42:240-247.
24. Webber-Jones JE, Thomas CA, Bordeaux RE Jnr. The management and prevention of rigid cervical collar complications. Orthop.Nurs. 2002;21:19-28.
25. Stiell IG, Clement CM, McKnight RD, Wells GA, Brison R, Schull M, Rowe B, Worthington J, Eisenhauer M, Cass D, Greenberg G, MacPhail I, Dreyer J, Lee J, Bandiera G, Reardon M, Holroyd B, Lesiuk H. (2003) Comparative Validation of the Canadian C-Spine Rule and the NEXUS Low-Risk Criteria in Alert and Stable Trauma Patients. New Engl J Med, 349:2510-8
26. Spivak, J et al, 1995. Thoracolumbar Spine Trauma: II Principles of Management, Journal of American Academy of Orthopeadic Surgery. 3(6): p. 353-360.
27. Posterior Lumbar Discectomy: Mayfield Brain and Spine, Revised Bohinski, R (2016). Accessed from http://www.mayfieldclinic.com/PE-LumDiscectomy.htm
28. Hickey, J, 2014. The Clinical Practice of Neurological and Neurosurgical Nursing. (7th Ed) Lippincott, Williams and Wilkins: Philadelphia, New York and Sydney.
29. Aidlen, JP, Caiati, J, Daniels, AH, Palumbo, MA and Thakur, NG, 2012. Airway Compromise Due to Wound Hematoma Following Anterior Cervical Spine Surgery, Open Orthopaedic Journal; 6: 108-113.
30. Trivedi, JM, 2002. Spinal trauma: therapy—options and outcomes. European Journal of Radiology; 42 (2), pages 127-134.
31. Kang, M, Vaccaro, A, & Vives, MJ (2003). The Halo Vest: Principles Of Application and Management Of Complications, The Journal of Spinal Cord Medicine, 26 (3), 186-192
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 26 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
32. Clinical Quality and Patient Safety Unit, Queensland Ambulance Service (2016). Clinical Practice Procedures: Trauma/Cervical Collar. Accessed from http://ambulance.qld.gov.au/clinical.html
Back to Table of Contents
Definition of Terms
Discectomy – A discectomy is the surgical removal of herniated disc material that is pressing on a nerve root or the spinal cord
Foraminotomy – the vertebral foramen or space is made larger to remove pressure on the nerve root.
Laminectomy – partial or total removal of one or more vertebral lamina to expose the spinal canal for treatment of compression, fracture, dislocation, tumour or herniated disc.
Rhizolysis – freeing of the nerve thereby establishing blood flow to the nerve root to relieve radiculopathy.
Spinal Fusion - performed by a neurosurgeon in the operating theatre and involves the fixation of an unstable segment of the spine, using bone grafts and/or metal plates and screws. Fusion is performed to limit movement and/or stabilise the spine at a particular level in the cases of Spondylolisthesis, fractures, lesions or deformity
ACDF - A herniated disc in the cervical spine can be removed through an anterior approach (the front of the neck) to relieve spinal cord or nerve root pressure and alleviate corresponding pain, weakness, numbness, and tingling. A bone graft, which is usually taken from the iliac crest, is then inserted to stabilise. Indications for this procedure are: herniated disc, degenerative disease, bone spurs, cervical stenosis and spondylosis.
Dysphagia – swallowing deficit
Back to Table of Contents
Search Terms
Spine, microdiscectomy, brace, orthosis, fusion, laminectomy, traction, trauma, PLIF, vertebrae, halo, cervical, disc, logroll, Gardner-wells, fracture, spinal, precaution, bedrest, clowards, discectomy, head hold, observations, rhizolysis, c-spine, ACDF, foraminotomy, collar, Miami J, spinal injury
Back to Table of Contents
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 27 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
Attachments
Attachment 1 Level of precaution required - assessed using the definitions for the 3 Protocol GroupsAttachment 2: The Canadian C-Spine RuleAttachment 3: Spinal precaution for the unconscious trauma patientAttachment 4: Spinal precautions for the alert (GCS> 15) trauma patientAttachment 5: Indications for the use MRI in the management of patients with a potential spinal injuryAttachment 6: Spinal Injury Management and Treatment PlanAttachment 7: Traumatic spinal injury and spinal surgery observation chartAttachment 8: Motor Grading Scale
Disclaimer: This document has been developed by ACT Health, Canberra Hospital and Health Services specifically for its own use. Use of this document and any reliance on the information contained therein by any third party is at his or her own risk and ACT Health assumes no responsibility whatsoever.
Policy Team ONLY to complete the following:Date Amended Section Amended Divisional Approval Final Approval16/03/2018 Complete Review Daniel Wood, A/g ED
SOHCHHS Policy Committee
This document supersedes the following: Document Number Document NameCHHS14/053 Care of Adult Patients with Potential Spinal Injury
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 28 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
Attachment 1 Level of precaution required - assessed using the definitions for the 3 Protocol Groups
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 29 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
Arrive to ED / ICU with prehospital Hard Collar
Triage / Primary SurveyIf no immediate life threats
then hard collar replaced with soft collar.
Spinal Clearance Assessment using Canadian
C spine Rules (see flow Chart). Thoracolumbar spine assessed clinically
Arrives with prehospital soft collar
Spinal precautions maintained: Soft collar + sandbags/ rolled
towels log roll In line stabilisation for
transfers / procedures
Whole Spine Cleared Clinically
CT Cervical Spine +/- thoraco-lumber imaging *
Self presents with Neck Injury or pain
after trauma
Spine not cleared
Spinal precautions maintained: Soft collar with sandbags or rolled towels log roll In line stabilisation for transfers /
procedures
No further spinal precautions required
Follow Adult spinal injury management Protocol (see flow chart)
* = CT is the investigation of choice for potential cervical spine and thoracic spine injuries. The use of
NEXUS criteria is not an appropriate
basis to proceed to CT. The patient must be evaluated using Canadian C
spine rules.
Obtunded Patient?
Initial Management of Adult Patients with Potential spinal injuries
CHHS18/110
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 30 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
Attachment 2: The Canadian C-Spine Rule
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 31 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
UNCONSCIOUS MAJOR TRAUMA PATIENT
Apply soft collar & spinal precautions
MSCT with reconstructions:Whole spine - E.A.M. to sacrum (sagittal,
axial & coronal reformats
Imaging abnormal
C-spine cleared Films reviewed by
appropriate Consultant AND Radiologist
+/- MRI
Imaging normal
Collar off & cease position restrictions, clearly
documenting assessment and decision making
CHHS18/110
Attachment 3: Spinal precaution for the unconscious trauma patient
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 32 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CONSCIOUS MAJOR TRAUMA PATIENT
Soft collar insituApply spinal precautions
Canadian C-Spine Rule*:Alert (GCS 15)
Stable trauma patient
Any high risk factor which mandates radiography?Age >65 orDangerous mechanism ^ orParesthaesia in extremities
C-spine cleared
Any low risk factor which allows safe assessment of range of motion?Simple rear end MVCSitting position in ED orAmbulatory at any time orDelayed onset of neck pain i.e. not immediate onset of neck pain orAbsence of midline c-spine tenderness
Radiography:CT occiput to T4
Collar off & cease position restrictions, clearly documenting assessment and decision making
Able to actively rotate neck?45o left and right
^ Dangerous mechanism Fall from elevated height (>2 m/5 stairs)Axial load to the head (e.g. diving)MVC high speed (>100km/hr), rollover, ejectionMotorised recreational vehiclesPedal cyclist collisionParaesthesia in extremities^^ Simple rear end MVC excludes:Pushed into oncoming trafficHit by a bus or large vehicleRolloverHit by high speed vehicle^^^ Delayed:i.e. not immediate onset of neck pain
No
Yes
Yes
No
*Rule NOT applicable if:Non-trauma patientGCS <15Unstable vital signsAge <16 yearsAcute paralysisKnown vertebral diseasePrevious c-spine surgery
Yes
Able
Unable
CHHS18/110
Attachment 4: Spinal precautions for the alert (GCS> 15) trauma patient
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 33 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
Attachment 5: Indications for the use MRI in the management of patients with a potential spinal injury
Attachment 6: Spinal injury management and treatment planAttachment 7: Traumatic spinal injury and spinal surgery observation chart
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 34 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
MAJOR TRAUMA CONSCIOUS
Cervical CTE.A.M. to the top of T4 (saggital, axial & coronal reformats)
Review by Radiologist & senior ED Consultant
Clinical evidence of spinal cord injury
MRI when stable
Normal imaging but symptomatic
Clinical examination and review
MRI if indicated
MAJOR TRAUMA UNCONSCIOUS
Cervical CTE.A.M. toT4/5 (saggital, axial & coronal reformats)
Normal imaging Abnormal imaging
Stop +/- MRI only if clinically indicated
+/- MRI when stable
MAJOR TRAUMA & SPINAL CORD INJURY
Cervical CTE.A.M. toT4/5 (saggital, axial & coronal reformats)
MRI ASAP
CHHS18/110
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 35 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/110
Attachment 8: Motor Grading Scale
Doc Number Version Issued Review Date Area Responsible PageCHHS18/110 1 16/03/2018 01/04/2021 SOH 36 of 36
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register






















![€¦ · Web viewMarion Cross School Parent Handbook [Type text][Type text][Type text] 8](https://img.pdfslide.us/doc/110x75/5b8348d97f8b9a7d3a8c8367/-web-viewmarion-cross-school-parent-handbook-type-texttype-texttype-text.jpg)