Embed Size (px)
Citation preview

Journal of the American Academy of Orthopaedic Surgeons188
Before the introduction of modernantibiotic therapy, mortality inpatients with vertebral osteomyelitiswas as high as 25%.1 Antibiotictherapy combined with surgicaldébridement and stabilization hasdecreased mortality to less than 5%to 15%.2-4 Early diagnosis also hasimproved outcomes by facilitatingrapid initiation of antibiotic treat-ment and preventing abscess forma-tion, structural instability, and neu-rologic deterioration.
Spinal infections are evaluatedaccording to their location, the path-ogen or pathogens involved, route ofthe infection, age of the patient, andimmune status of the host. The loca-tion of the infection may involve theosseous vertebra, the intervertebraldisk, the epidural space, or the sur-rounding soft tissues. The pathogensare usually either bacterial or fungal;however, the widespread use ofbroad-spectrum antibiotics and theincreasing number of immunocom-promised patients have led to infec-tions with unusual organisms.
A systematic approach must betaken in the diagnosis and treat-ment of each type of spinal infec-tion. The presentation and efficacyof the various elements of the initialevaluation differ markedly for acutehematogenous infection, granulom-atous spinal infection, pediatrichematogenous diskitis, epiduralabscess, and postoperative spinalinfection.
Pathophysiology of SpinalInfection
Pyogenic vertebral osteomyelitis is abacterial infection that can arisefrom a number of sources�directinoculation, contiguous spread froman adjacent infection, or hematoge-nous seeding. Direct inoculationcan result from penetrating injuriesor from percutaneous or open spinalprocedures (eg, chemonucleolysis,diskography, diskectomy) done onthe intervertebral disk. Local spreadof bacteria or fungi can occur fol-
lowing intra-abdominal and retro-peritoneal abscesses. Althoughlocal spread from direct inoculationof bacteria into the spinal canal islikely to become more prevalent asthe number of spinal proceduresincreases, hematogenous seeding ofinfection is still by far the most com-mon mechanism of spinal infection.Potential sources of pathogenicorganisms include skin and soft-tissue infections, infected vascularaccess sites, and the urinary tract.
The two major theories for hema-togenous dissemination are thevenous theory and the arteriolartheory. Batson5 developed thevenous theory using both live ani-mal and human cadaveric models.He demonstrated retrograde flowfrom the pelvic venous plexus to theperivertebral venous plexus viavalveless meningorrhachidian veins.In the arteriolar theory, Wiley andTrueta6 proposed that bacteria canbecome lodged in the end-arteriolar
Dr. Tay is Assistant Professor, Department ofOrthopaedic Surgery, University of Californiaat San Francisco, San Francisco GeneralHospital, San Francisco, CA. Dr. Deckey isAttending Surgeon, Southern CaliforniaComplex Spine and Scoliosis Center, Whittier,CA. Dr. Hu is Associate Professor, Depart-ment of Orthopaedic Surgery, University ofCalifornia at San Francisco.
Reprint requests: Dr. Tay, 3A36, 1001 PotreroAvenue, San Francisco, CA 94110.
Copyright 2002 by the American Academy ofOrthopaedic Surgeons.
Abstract
Spinal infections can occur in a variety of clinical situations. Their presenta-tion ranges from the infant with diskitis who is unwilling to crawl or walk tothe adult who develops an infection after a spinal procedure. The most commontypes of spinal infections are hematogenous bacterial or fungal infections, pedi-atric diskitis, epidural abscess, and postoperative infections. Prompt and accu-rate diagnosis of spinal infections, the cornerstone of treatment, requires a highindex of suspicion in at-risk patients and the appropriate evaluation to identifythe organism and determine the extent of infection. Neurologic function andspinal stability also should be carefully evaluated. The goals of therapy shouldinclude eradicating the infection, relieving pain, preserving or restoring neuro-logic function, improving nutrition, and maintaining spinal stability.
J Am Acad Orthop Surg 2002;10:188-197
Spinal Infections
Bobby K-B Tay, MD, Jeffrey Deckey, MD, and Serena S. Hu, MD

Bobby K-B Tay, MD, et al
Vol 10, No 3, May/June 2002 189
network near the vertebral endplate. Both mechanisms are likelysignificant in the establishment ofan infectious focus in the spinal col-umn. In the cervical spine, an ex-tensive prevertebral pharyngealvenous plexus also may act as aconduit for the spread of bacteria.7
Local spread of infection canoccur in a number of ways. Oncethe infection is established adjacentto the end plate of one vertebralbody, it can rupture through thatstructure into the adjoining disk andinfect the next vertebral body. Thedisk material is relatively avascularand is rapidly destroyed by the bac-terial enzymes (Fig. 1). In the cervi-cal spine, if the infection penetratesthe prevertebral fascia, it can extendinto the mediastinum or into thesupraclavicular fossa, markedlyincreasing the extent and severity ofthe process. From the lumbar spine,abscess formation may track alongthe psoas muscle and into the but-tock (piriformis fossa), the perianalregion, the groin, or even the pop-liteal fossa. The extension of infec-tion from the vertebral body or diskinto the spinal canal may result in anepidural abscess or even bacterialmeningitis. Destruction of the ver-tebral body and intervertebral diskcan potentially lead to instabilityand collapse. In addition, with col-lapse of the vertebral body, infectedbone or granulation tissue may beretropulsed into the spinal canal,causing neural compression or vas-cular occlusion. With pyogenicosteomyelitis, the lumbar spine ismore commonly affected than thethoracic or cervical spine.8
The pathogenesis of spinal infec-tion differs markedly between chil-dren and adults because of anatomicdifferences in the vascular anatomyof the vertebrae. In children, vascu-lar channels cross the cartilaginousgrowth plate and end within thenucleus pulposus. These channelsprovide pathways for direct inocu-lation of organisms into the avascu-
lar nucleus pulposus. Since thesevascular channels are not present inadults, the direct seeding of the diskdoes not occur, but rather spreadingoccurs by direct extension with rup-ture of the infective focus throughthe end plate into the disk.
Neurologic deterioration can be adevastating consequence of spinalinfection. A number of differentfactors can cause neural deficit.Direct spread of infected materialinto the spinal canal can produce anepidural abscess that may compressthe neural elements or cause throm-bosis or infarction of the regionalvascular supply to the spinal cord.Direct hematogenous spread rarelyresults in epidural abscess withoutthe presence of associated diskitis orosteomyelitis. Pathologic fracturecan occur, with associated extrusionof either infected material or bony
elements into the spinal canal.Kyphosis and/or spinal instabilityresulting from destruction of thedisk, vertebral bone, and posteriorstabilizing structures can causeneural impingement. Eismont et al4
reported several additional risk fac-tors that predispose to neurologicdeterioration: diabetes, rheumatoidarthritis, steroid use, advanced age,a more cephalad level of infection(ie, high thoracic or cervical), andinfection with Staphylococcus spe-cies.
The pathophysiology of granulom-atous spinal infection differs fromthat of pyogenic infections. Themost common form of granuloma-tous disease of the spine is causedby Mycobacterium tuberculosis (Pott�sdisease). Although endemic inmany developing countries, tuber-culosis (TB) was nearly eradicated in
A B
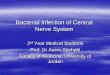
Figure 1 A 56-year-old man presented with severe back pain following a urologic proce-dure. He had an elevated ESR but no leukocytosis. A, T1-weighted sagittal MR image ofthe lumbar spine shows severe edema of the L3-4 disk and adjacent soft tissues. B, T2-weighted sagittal MR image shows high signal intensity in the L3-4 disk and adjacent ver-tebral bodies, consistent with pyogenic diskitis and osteomyelitis. Cultures obtained froma CT-guided biopsy of the disk space grew Staphylococcus aureus.

Spinal Infections
Journal of the American Academy of Orthopaedic Surgeons190
the United States; however, therehas been a recent resurgence of TBwith resistant strains and in patientswith human immunodeficiencyvirus (HIV). Although less than 10%of patients with TB have skeletalinvolvement, 50% of the skeletal in-volvement occurs in the spine.Depending on the series, between10% and 61% of patients presentwith or develop a neurologicdeficit.9
With TB, the primary route ofinfection to the spine is hematoge-nous from a pulmonary or geni-tourinary source, although directspread from adjacent structures canoccur. Three major patterns of spi-nal vertebral body involvementhave been documented: peridiscal,central, and anterior.10 The mostcommon form, peridiscal, occursadjacent to the vertebral end plateand spreads around a single inter-vertebral disk. Extension to the ad-jacent vertebra occurs as the granu-lomatous abscess material tracksbeneath the anterior longitudinalligament. Unlike the situation inpyogenic infections, the interverte-bral disk is usually spared. Centralinvolvement occurs in the middleof the vertebral body and can be
mistaken for a tumor. Destructionof the vertebral body will then leadto spinal deformity. Anteriorinvolvement begins beneath theanterior longitudinal ligament,causing scalloping of the vertebralbody (Fig. 2). In contrast withperidiscal involvement, whichaffects a single motion segment,anterior involvement can producea spinal abscess that extends overmultiple levels. Primary involve-ment of the posterior structures isuncommon. Regionally, the tho-racic spine is most often involved,followed by the lumbar spine andcervical spine. Paraspinal exten-sion with abscess formation is com-mon and can occur at any level.
Spinal infections can be classifiedas acute, subacute, or chronic de-pending on the duration of symp-toms. Symptoms that have persistedfor <3 weeks are acute; those lastingfrom 3 weeks to 3 months are sub-acute. Chronic infections last >3months and either are caused byindolent organisms, are granuloma-tous in nature, or are incompletelytreated (eg, infections with resistantorganisms, or the presence of for-eign material in the area of infec-tion).
Clinical Evaluation
Pyogenic VertebralOsteomyelitis
Pyogenic vertebral osteomyelitisis more common in males than infemales and also more common inelderly populations.2,11 However,the incidence of infection is increas-ing in younger age groups in popu-lations with intravenous drug abuseor immunocompromise after organtransplantation or chemotherapy.Accordingly, spinal infection shouldbe considered in the differentialdiagnosis of acute-onset spinal painin patients older than 50 years orwith diabetes, rheumatoid arthritis,immunocompromise (from medical illness or pharmacologic immuno-suppression), or a history of intra-venous drug abuse.
The clinical presentation of ver-tebral osteomyelitis depends on thelocation of the infection, the viru-lence of the organism, and the im-mune status of the host. Back orneck pain is the most consistentsymptom of pyogenic infection.Observed in >90% of patients, thepain is often quite severe and isassociated with notable paraspinalmuscle spasm. The pain may occur
A B C D
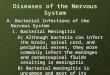
Figure 2 A 33-year-old woman presented with back pain of several months� duration. A, Anteroposterior radiograph shows collapse ofthe vertebral body and paraspinal soft-tissue shadow (arrowheads). B, Lateral radiograph also shows collapse and interior scalloping(arrow). C, Sagittal T1-weighted MR image shows a large anterior abscess, extensive vertebral body involvement, and relative sparing ofdisk spaces. D, The patient underwent CT-guided biopsy and aspiration with placement of a pigtail catheter for 1 week to drain thisabscess. She underwent anti-TB treatment for 1 year, with resolution of pain and no development of deformity.

Bobby K-B Tay, MD, et al
Vol 10, No 3, May/June 2002 191
at night and is usually present re-gardless of activity level. Radicularleg or arm pain is less common butmay be present with neurologicinvolvement, which occurs in lessthen 10% of patients. Fevers aredocumented in approximately 50% of the affected population.12
Weight loss is common but maynot be easily recognized by patientsbecause it may occur slowly over aperiod of weeks to months beforethe infection is diagnosed andtreated.
The presence of other signs orsymptoms depends on the extent ofthe infectious process. A patientwith a psoas abscess may have painwith hip extension. Cervical abscessformation may lead to torticollis ordysphagia. Radiculopathy, myelop-athy, or even complete paralysis canoccur with neural compression as aresult of abscess, instability, orspinal deformity. Direct spread ofthe infection into the epidural spacecan cause meningitis.
Gram-positive organisms are re-sponsible for the majority of verte-bral column infections in both adultsand children, with Staphylococcusaureus accounting for >50%. Infec-tion with gram-negative organismssuch as Escherichia coli, Pseudomonas,and Proteus may occur followinggenitourinary infections or proce-dures. Intravenous drug abusers arealso prone to Pseudomonas infections.Anaerobic infections may be en-countered in patients with diabetesor following penetrating trauma.Low-virulence organisms such ascoagulase-negative staphylococciand Streptococcus viridans may causeindolent infections. These organ-isms may not be detected unlessblood cultures are held for morethan 10 days and should not be dis-regarded as contaminants in thepresence of clinical infection. Salmo-nella, presumably from an intestinalsource, can cause vertebral osteo-myelitis in children with sickle cellanemia.
Laboratory StudiesLaboratory studies may be useful
but are usually nonspecific. Thewhite blood cell count will be ele-vated in approximately half thecases of acute pyogenic osteomye-litis but typically is normal in thepresence of subacute or chronicinfection. The erythrocyte sedimen-tation rate (ESR) is a more sensitivetest and is elevated in >90% of pa-tients. The C-reactive protein (CRP)level, an acute-phase reactant with amuch quicker normalization time,may be more helpful in followingthe course of treatment than theESR. A rapid decrease in the CRPlevel indicates an adequate responseto treatment and can help determinewhen to switch from intravenous tooral antibiotics. Blood cultures maybe negative in up to 75% of patients,particularly if the infection involvesa low-virulence organism. It isextremely important to delay antibi-otic therapy until appropriate cul-tures have been obtained unless thepatient is septic and critically ill.Even then, blood and urine culturesshould be obtained before the ad-ministration of antibiotics.
Evaluation of laboratory measure-ments for malnutrition is as impor-tant as the diagnostic tests that detectthe presence of infection. Weightloss >30% of ideal body weight dur-ing the course of the infection in-dicates severe malnutrition. Otherlaboratory measurements that areassociated with severe malnutritioninclude a serum albumin level of <3g/dL, serum transferrin measure-ment of <150 µg/dL, and an absolutelymphocyte count of <800/mL. Al-though it is a measurement less com-monly used in orthopaedics, a 24-hour urinary creatinine excretion of<10.5 mg in men or <5.8 mg inwomen indicates a negative nitrogenbalance associated with malnutrition.
BiopsyThe definitive diagnosis of spinal
pyogenic osteomyelitis requires
identification of the organismthrough a positive blood culture orfrom a biopsy and culture of theinfected site. Blood cultures may bediagnostic in as few as 25% to 33%of cases.2 Cultures taken duringfever spikes may provide betterdiagnostic results. Biopsy of theinfected area is often necessary toinitiate the appropriate antibioticregimen. Other sources of obviousinfection, such as the urine, mustalso be cultured. Spinal biopsiesmay be done percutaneously, usingcomputed tomography (CT) or fluo-roscopy to localize the focus of infec-tion. The accuracy of closed biopsytechniques varies and has beenreported to be about 70%.13 Key fac-tors may be insufficient tissueretrieval or administration of antibi-otics prior to biopsy. A core sampleobtained from a Craig biopsy needlefor bone or a TruCut (Baxter Trave-nol, Deerfield, IL) or similar needlefor soft tissue is preferable to fine-needle aspiration except when anabscess cavity is present. Antibioticsmust not be started until the biopsyis done and sufficient tissue is ob-tained for culture, gram stain, andhistology. If a diagnosis is not con-firmed on the first attempt, a secondclosed biopsy should be consideredbefore open biopsy is done.
An open biopsy is indicatedwhen needle biopsy fails to identifyan organism, when the infection isinaccessible by standard closedtechniques, or when there is markedstructural damage with neurologiccompromise. Open biopsies arediagnostic in >80% of cases.14 Mini-mally invasive techniques, such as alaparoscopic or thoracoscopic ap-proach, may be considered when thatapproach is appropriate to decreasethe morbidity of the procedure.
Biopsies should be sent for gramstain, acid-fast stain, and aerobic,anaerobic, fungal, and TB cultures.Bacterial cultures should be main-tained for 10 days to detect low-vir-ulence organisms. Histologic stud-

Spinal Infections
Journal of the American Academy of Orthopaedic Surgeons192
ies also should be done, if possible,to detect metabolic or neoplasticprocesses. If tissue is available,pathologic examination should beconducted to differentiate betweenacute and chronic infection and tohelp detect the presence of acid-fastbacilli and fungal elements. Thedevelopment of polymerase chainreaction as a diagnostic tool has fa-cilitated rapid detection of the in-fecting agent, especially when indo-lent and low-virulence organisms areinvolved.15,16 However, technicalproblems with cross-contaminationcan lead to false-positive results.
TuberculosisThe clinical presentation of a
patient with a tuberculous spinalinfection is highly variable. As withpyogenic infections, back pain is themost common symptom; however,it is usually less severe than in apyogenic infection. Patients withchronic infection also may experi-ence weight loss, malaise, fevers,and night sweats. Kyphotic defor-mities, neurologic deficits, or cuta-neous sinuses may occur after pro-longed or very severe infections.Neurologic deficit can occur fromepidural extension of the tubercu-lous infection, from destruction ofbone with retropulsion of infectedmaterial into the spinal canal, orfrom progressive kyphotic defor-mity. Elderly patients appear to beat higher risk for developing a neu-rologic deficit. The differential diag-nosis of spinal infection includes primary and metastatic tumors; in-fections with atypical bacteria suchas Actinomyces, Nocardia, and Bru-cella; infections with atypical myco-bacteria; and fungal infections suchas coccidioidomycosis, blastomyco-sis, cryptomycosis, candidiasis, andaspergillosis. Immunocompromisedpatients are at risk for developinginfections with atypical mycobacte-ria. Fungal infections also havebecome more common with theincreasing use of broad-spectrum
antibiotics, especially in combinationwith central venous catheters forparenteral nutrition (Fig. 3).
Suspicion of a mycobacterialinfection is the basis for establishingthe diagnosis. Patients from South-east Asia or South America, prisonpopulations, and frequenters ofhomeless shelters are at high risk forcontracting TB. A patient with afamily member or household con-tact with TB also should be consid-ered as at high risk. Laboratory testsare usually nonspecific. A leukocy-tosis may or may not be present.The ESR may be normal in up to25% of cases. Although the purifiedprotein derivative skin test can helpdetect active infection or past expo-sure to TB, the test is not fully reli-able because of false-negative resultsthat can occur in the malnourishedand the immunocompromised.Polymerase chain reaction for detec-tion of tuberculous infection holdsgreat promise for a faster diagnosis.
Pediatric DiskitisThe highly variable clinical pre-
sentation of a child with diskitis maylead to delays in recognition anddiagnosis. Active children mayoften associate the onset of pain withsome activity or minor trauma. Inthe absence of systemic symptomsof infection, further workup is nec-essary if the pain does not resolve in1 to 2 weeks. In general, however,vertebral infection should be sus-pected when the child has a low-grade fever and pain, refuses to bearweight, or assumes a flexed positionof the spine. The patient also maycomplain of abdominal pain. Thesenonspecific findings are more com-mon in children over the age of 5years.17-19 In contrast, infants aremore likely to be systemically ill.Older children are more likely to beable to identify the spine as thesource of pain. Although uncom-mon, these same symptoms can beobserved with spinal tumors in chil-dren, such as Ewing�s sarcoma.
The white blood cell count mayor may not be elevated, but the ESRis usually mildly elevated and theCRP level, markedly elevated.Infants typically will demonstrate aleukocytosis and elevated ESR.20
Blood cultures can be positive inup to 50% of cases.19
Acute infections are more likelyto yield positive blood cultures.19
Certainly the child who appears illand febrile should have all possiblesources of infection cultured. If abiopsy is needed, it can be doneunder CT guidance; a 60% to 70%yield rate for infectious lesions canbe expected.21 If a trial of antibioticswas initiated prior to biopsy with-out response, antibiotics should besuspended for 3 to 4 days before theprocedure to ensure greater accuracyfrom the cultures.
A B
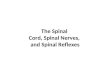
Figure 3 A 40-year-old woman withrheumatoid arthritis and chronic steroiduse developed severe back pain and para-plegia after treatment with broad-spectrumantibiotics for necrotizing fasciitis. A,Lateral radiograph of the lumbar spineshows bony destruction of the end platesof L2 and L3. B, T2-weighted sagittal MRimage of the lumbar spine demonstratesdiskitis and vertebral osteomyelitis at L2-3,with severe canal stenosis from an epiduralcollection (arrowhead). Cultures taken atthe time of anterior débridement were con-sistent with a Candida infection. The pa-tient obtained pain relief and improvementin motor function after aggressive anteriordébridement and reconstruction with anautogenous tricortical iliac graft and 6weeks� administration of intravenous lipo-somal amphotericin B.

Bobby K-B Tay, MD, et al
Vol 10, No 3, May/June 2002 193
Epidural AbscessThe presence of a spinal epidural
abscess is usually associated withthe occurrence of diskitis or verte-bral osteomyelitis. Rarely does anepidural abscess occur hematoge-nously without spinal involvement.This condition is caused by directseeding of bacteria into the epiduralvenous plexus, in contrast with themore common route of local exten-sion from adjacent disk or bone. Inthe absence of diskitis or vertebralosteomyelitis, an epidural abscesscan be difficult to diagnose and canprogress rapidly, with devastatingconsequences; prompt diagnosisand early treatment are critical inthese rare cases. Risk factors for thedevelopment of epidural abscessinclude history of intravenous druguse, diabetes, trauma, obesity, per-cutaneous or open procedures (eg,spinal surgery, nerve or epiduralblock, or diskography), HIV, andrenal failure.22-26 Patients may pre-sent with back pain, progressiveneurologic deficit, or fever. Al-though leukocytosis may not bepresent, the ESR is almost alwayselevated.
Radiographic Evaluation
Imaging studies are crucial to local-ize the infection, assess the extent ofinvolvement, and determine theresponse to treatment. Radiographsmay demonstrate progressive osteo-lysis and end plate destruction,often best seen on the anteroposteriorview (Fig. 2, A). As the disease pro-gresses, the disk space narrows andeventually collapses (Fig. 3). Plainradiographs, however, may notdemonstrate abnormal findings forup to several weeks after the pro-cess has begun. Soft-tissue exten-sion must be suspected in the pres-ence of an abnormal psoas shadow,widening of the mediastinum (Fig.2, A), or enlargement of the retro-pharyngeal soft-tissue shadow. The
presence of gas in the soft tissuessuggests an infection with an anaer-obic organism.
In contrast with pyogenic infec-tions, skeletal radiographs in atuberculous infection often demon-strate vertebral destruction withrelative preservation of the diskspaces. As the infection progress-es, the disk is also destroyed and akyphotic deformity may be present,especially in the thoracic spine. Achest radiograph always should beobtained to assess for active pul-monary disease.
In pediatric diskitis, radiographsof the spine should be assessed fordisk space narrowing, end plate ero-sions, bony destruction, and para-vertebral soft-tissue swelling. Thesechanges may not occur for severaldays or weeks after onset of symp-toms. They usually persist, eventu-ally leading to disk space narrowingor autofusion.18,27 Although latekyphosis is rarely seen in pediatricspinal infections, a notable exceptionis infantile osteomyelitis, which gen-erally is associated with more initialbony destruction and resembles con-genital kyphosis in late stages.20
Radionuclide studies can bemuch more sensitive than radio-graphs in detecting early infections.Technetium 99m bone scintigraphyis sensitive (~90%) but nonspecific,especially in adults with degener-ative joint disease.28 Because thestudy is dependent on local bloodflow, false-negative results haveoccurred in areas of relative ische-mia in very young and elderly pa-tients. In pediatric vertebral osteo-myelitis, the technetium 99m bonescan is positive in 74% to 100% ofcases,17,19 facilitating earlier diagno-sis of diskitis in children. Wenger etal19 showed that use of bone scansallowed diskitis to be diagnosed anaverage of 8.3 days earlier thanwithout.
When used in conjunction withtechnetium 99m scans, gallium 67citrate scans have high sensitivity
and specificity in detecting foci ofinfection. The tracer, an analog offerritin, is secreted by leukocytes atsites of infection. Gallium scans alsonormalize during the recovery phaseand may be used to follow treatmentresponse. This test, however, maynot be effective in leukopenic pa-tients and may not detect low-viru-lence organisms. Indium 111-labeledscans have a poor sensitivity in ver-tebral osteomyelitis (17%) and arenot recommended.29
CT is useful in delineating theextent of bony destruction and soft-tissue extension and is helpful in pre-operative planning. However, thestatus of the neural elements cannotbe accurately assessed without theuse of myelographic dye, which iscontraindicated in suspected infec-tion because it places the patient atrisk for developing meningitis orarachnoiditis. Although the CT scanwith intravenous contrast also candemonstrate soft-tissue extension,distinction between abscess andgranulation tissue may be difficult.
Magnetic resonance imaging(MRI) is the modality of choice inthe diagnosis and evaluation ofspinal infections because it providesexcellent imaging of the soft tissue,neural elements, and inflammatorychanges in the bone (Figs. 2, B and 3, C). MRI has an extremely highsensitivity (96%) and specificity(93%) in detecting infections of thevertebral column.28 It is noninva-sive, allows detection of paraverte-bral and epidural extension, andclearly visualizes neurologic struc-tures. T1-weighted sequencesdemonstrate decreased signal in-tensity in both the vertebral bodyand disk from edema. T2-weightedimages show increased signal inten-sity in both the vertebral body anddisk with loss of the normal intranu-clear cleft (Fig. 1).
The administration of gadoliniumin combination with MRI improvesresolution and allows an infectiousprocess to be distinguished from

Spinal Infections
Journal of the American Academy of Orthopaedic Surgeons194
degenerative changes of the endplate and intervertebral disk (Fig. 4).The vascular-based enhancementalso allows differentiation of anepidural granulation from an epi-dural abscess. An epidural massmay be isointense or hypointenseon T1-weighted images, shows highsignal on T2-weighted images, andmay show peripheral enhancementvisible with gadolinium.30 Short T1inversion recovery sequences oftencan help to differentiate an infectionfrom other pathologic entities. Evenwith MRI, however, granulomatousinfections can be difficult to distin-guish from tumors of the spine.Thus, a biopsy is often required tomake a definitive diagnosis.
Treatment
Pyogenic InfectionsThe goals for treatment of spinal
infections should be to establish adiagnosis and identify the pathogen,eradicate the infection, prevent orminimize neurologic involvement,maintain spinal stability, and pro-vide an adequate nutritional state to combat infection. Establishing a diagnosis and identifying thepathogen is of primary importance.Once the organism has been identi-fied, intravenous antibiotic therapyshould be initiated according to theculture results and sensitivities. Acourse of 2 to 6 weeks of parenteralantibiotics is usually recommended.This is followed by a course of oralantibiotics, depending on the viru-lence of the organism, susceptibilityof the host, and other factors, such asretained hardware. Conversion tooral antibiotics should be made onlywith clinical improvement, normal-ization of the ESR and CRP level, orresolution of the infection as demon-strated in imaging studies.
In addition to antibiotic therapy,immobilization, rest, and proper nu-trition are recommended. Moldedcontact braces are effective in the
lumbar region, whereas a halo or arigid cervicothoracic orthosis maybe required for cervical osteomye-litis. Immobilization of the affectedarea aids in pain relief and helpsprevent deformity.
Surgery is indicated in five cir-cumstances: to obtain a tissue diag-nosis after a failed closed needlebiopsy or from a location inaccessi-ble by closed methods; for drainageof an abscess that is causing sepsisor neurologic deficit; to treat neuro-logic deficit secondary to compres-sion either by the infection (abscessor granulation) or structural de-struction; for structural instability ordeformity; or for failure of medicalmanagement to reduce persistentsymptoms or elevated laboratorymeasurements.
The location of the infection andthe intended purpose of the surgeryoften dictate the surgical approach.Because the majority of these infec-tions involve the vertebral body andthe disk, an anterior approach ismost commonly used to maximizeaccess to the infected tissue. A pos-terolateral approach to the thoracicspine may be considered in certaininstances, or a costotransversectomyif only culture, biopsy, or abscess
drainage is necessary. Because theseand endoscopic approaches avoidthoracotomy, they may cause lessmorbidity in the medically fragilepatient.
If an anterior approach is usedfor débridement and decompressionof the spinal canal, reconstructionshould be done with an autogenousstructural graft, such as tricorticaliliac crest or middle third of thefibula. Iliac crest is preferable be-cause of the abundant amount ofcancellous bone. Fresh-frozen allo-grafts in combination with autoge-nous bone may be considered forstructural support, but structuralautogenous bone grafts are pre-ferred. Vascularized bone graftshave gained popularity during thelast decade because of their intrinsicblood supply and faster rate of in-corporation. In the thoracolumbarjunction, a vascularized rib graftmay be used, and in the lumbarspine, vascularized rib or iliacgrafts.31-34 Recently, titanium surgi-cal mesh filled with autogenousbone has been used as an alternativeto structural autogenous graft.Depending on the degree of preop-erative kyphosis and length of thereconstruction, a posterior fusion
A B C
Figure 4 A 38-year-old man with HIV and a CD4 cell count of 20 presented with backpain of several weeks� duration and no radiculopathy. A, T1-weighted sagittal MR imageshows edema at the L5-S1 disk space and adjacent end plates. The asterisk (*) indicates anepidural collection consistent with an epidural abscess. B, T1-weighted gadolinium-enhanced sagittal MR image shows uptake at the L5-S1 disk space and the epidural collec-tion. C, T2-weighted sagittal MR image shows no notable canal compromise by the anteri-or collection. However, there is severe destruction of the adjacent bone of L5 and S1.
*

Bobby K-B Tay, MD, et al
Vol 10, No 3, May/June 2002 195
with instrumentation may be re-quired to adequately stabilize thespine. This is usually undertaken 1to 2 weeks after the initial surgicaldébridement. The staging of theprocedures allows for an interval ofintravenous antibiotics and opti-mization of medical and nutritionalparameters before placement of theinstrumentation.
Hyperalimentation is an effectiveway to maximize the patient�s nutri-tional status before and after surgeryand between stages. The infectionplaces the patient in a catabolic statebecause of metabolic losses that haveoccurred before the diagnosis of in-fection is made. The goal of nutri-tional supplementation is to restorethe patient to the premorbid nutri-tional status. Nutrition consultationand monitoring of laboratory mea-surements are helpful in reaching apositive nitrogen balance. Theseinclude achieving a serum albuminlevel >3 g/dL, an absolute lympho-cyte count >800/mL, and a 24-hoururine creatinine excretion >10.5 mgin men and >5.8 mg in women.
TuberculosisOnce the diagnosis of a tubercu-
lous infection is established, ag-gressive treatment is necessary toeradicate the infection. A four-drugregimen of isoniazid, rifampin,ethambutol, and pyrazinamide isused as first-line therapy for 6months. The response to treatmentis assessed by routine clinical ex-aminations and radiographs. Theemergence of multidrug-resistantmycobacteria will provide furtherchallenges in the treatment of theseinfections in the future.
Indications for surgery in tuber-cular infections are the same as forpyogenic infections. The most com-mon surgical technique, the HongKong procedure, involves débride-ment of infected bone, decompres-sion of the spinal canal, and correc-tion of the kyphotic deformity usingstructural grafting35 (Fig. 5). Addi-
tional posterior fusion with instru-mentation also may be required.The second procedure can be eitherstaged or done on the same day,depending on the tolerance of thepatient. Autogenous iliac crest orfibula is ideal for structural grafting.Rib graft alone has been shown tobe inadequate unless a vascularizedrib is used to accelerate the rate ofincorporation. The Hong Kong pro-cedure is preferred over anterior
débridement alone because theaddition of an anterior strut correctsand prevents progressive kyphoticdeformity. Laminectomy withoutadjunctive stabilization is contra-indicated because damage to theposterior structures in the presenceof weakened anterior structures willlead to progressive kyphosis andneurologic injury.
Failure of medical treatment ordevelopment of neurologic deficit is
A B
C D
Figure 5 A 22-year-old woman presented with a long history of back pain.Anteroposterior (A) and lateral (B) radiographs show erosion and partial collapse of theT12 vertebral body (arrow). C, T1-weighted MR image demonstrates extensive anteriorand posterior column involvement. Because of atypical MR image findings, a posteriorbiopsy was performed, which revealed TB. D, Postoperative lateral radiograph. Becauseof partial collapse and extensive involvement, the patient underwent anterior reconstruc-tion using autogenous rib graft.

Spinal Infections
Journal of the American Academy of Orthopaedic Surgeons196
a clear indication for surgicaldébridement, decompression, andstabilization. Early decompressionwill maximize the patient�s func-tional recovery. A more chronicneurologic deficit due to cord com-pression over structural deformityalso may be treated with decom-pression and stabilization. How-ever, the prognosis for neurologicrecovery in the face of chronicdeficits is not as optimistic.
Pediatric DiskitisWhether diskitis in children is
infectious or inflammatory in originremains controversial. Althoughthe recommended treatment willvary depending on the suspectedorigin, immobilization with castingor bracing is uniformly recommend-ed. The use of antibiotics has beencontroversial, with satisfactoryresults reported in several studiesregardless whether a patientreceived antibiotics. Scoles andQuinn18 reported that all patientswere asymptomatic at the time ofhospital discharge, whether or notantibiotics were administered. Inaddition, none of these patients hada relapse. In contrast, Ring andWenger36 observed that patientstreated with intravenous antibioticsfor at least 6 days had a more rapidresolution of symptoms and thelowest likelihood of developingrecurrent symptoms. Oral antibi-otics or no treatment were morelikely to lead to prolonged or recur-rent symptoms. Based on their
experience, they felt that a shortcourse of parenteral antibiotics wasmore likely to result in rapid reliefof symptoms and a lower incidenceof recurrent symptoms. Crawford etal17 reserved antibiotics for patientswho failed to respond to immobili-zation, bed rest, traction, or casting.
Epidural AbscessSurgical drainage is almost uni-
versally recommended for treatmentof an epidural abscess (Fig. 4). Con-servative management of epiduralabscesses, however, may be appro-priate if the patient has no neurologicdeficit, if the involvement is exten-sive, if the patient is not expected tosurvive surgery, or if paralysis hasbeen present for >48 hours so thatneurologic improvement would beunlikely.26,30 For example, patientswith lumbar involvement, no neuralcompromise, and diagnostic cul-tures can be effectively treated withintravenous antibiotics. As withosteomyelitis, from 2 to 6 weeks ofintravenous antibiotics is usuallyrecommended. An extended periodof oral antibiotics may be necessarydepending on the immunocompe-tency of the patient and the sensi-tivity of the organism.
Patients with neurologic deterio-ration are best managed with surgi-cal decompression and débridementin addition to antibiotic therapy.Anterior abscesses, particularlywith vertebral body involvement,should have anterior débridement.This can be done using either an
open or endoscopic approach. Pos-teriorly located infections can beadequately treated by a laminec-tomy. Patients with extensive in-volvement can be treated throughmultilevel laminectomies. However,care should be taken not to removemore bone than is indicated fordecompression because of the risk ofpostlaminectomy deformity. Promptand aggressive treatment of neuro-logic compression appears to favor-ably affect neurologic recovery.26
Summary
The most common types of verte-bral osteomyelitis are hematoge-nous bacterial or fungal infections(pyogenic or granulomatous), pedi-atric diskitis, epidural abscess, andpostoperative infections. Successfuldiagnosis and treatment depend onan appropriate index of suspicion.The optimal management of pa-tients with spinal infection requiresunderstanding the circumstancesthat resulted in the infection, theorganism involved, and the degreeof bony and neurologic compro-mise. Early detection and medicaltreatment may obviate the need forsurgical intervention. When surgi-cal débridement is indicated, itsprompt initiation appears to resultin good clinical outcomes. In addi-tion, maximizing the patient�s nutri-tional status with hyperalimentationimproves the outcomes of both med-ical and surgical treatment.
References
1. Guri JP: Pyogenic osteomyelitis of thespine: Differential diagnosis throughclinical and radiographic observations.J Bone Joint Surg Am 1946;28:29-39.
2. Carragee EJ: Pyogenic vertebral osteo-myelitis. J Bone Joint Surg Am 1997;79:874-880.
3. Garcia A Jr, Grantham SA: Hematoge-nous pyogenic vertebral osteomyelitis.J Bone Joint Surg Am 1960;42:429-436.
4. Eismont FJ, Bohlman HH, Soni PL,Goldberg VM, Freehafer AA: Pyogenicand fungal vertebral osteomyelitis withparalysis. J Bone Joint Surg Am 1983;65:19-29.
5. Batson OV: The vertebral system ofveins as a means for cancer dissemina-tion. Prog Clin Cancer 1967;3:1-18.
6. Wiley AM, Trueta J: The vascular anat-omy of the spine and its relationship to
pyogenic vertebral osteomyelitis. J BoneJoint Surg Br 1959;41:796-809.
7. Parke WW, Rothman RH, Brown MD:The pharyngovertebral veins: Ananatomical rationale for Grisel�s syn-drome. J Bone Joint Surg Am 1984;66:568-574.
8. Sapico FL, Montgomerie JZ: Vertebralosteomyelitis. Infect Dis Clin North Am1990;4:539-550.

Bobby K-B Tay, MD, et al
Vol 10, No 3, May/June 2002 197
9. Boachie-Adjei O, Squillante RG:Tuberculosis of the spine. Orthop ClinNorth Am 1996;27:95-103.
10. Doub HP, Badgley CE: The roentgensigns of tuberculosis of the vertebralbody. AJR Am J Roentgenol 1932;27:827-837.
11. Krogsgaard MR, Wagn P, Bengtsson J:Epidemiology of acute vertebralosteomyelitis in Denmark: 137 cases inDenmark 1978-1982, compared tocases reported to the National PatientRegister 1991-1993. Acta Orthop Scand1998;69:513-517.
12. Torda AJ, Gottlieb T, Bradbury R:Pyogenic vertebral osteomyelitis:Analysis of 20 cases and review. ClinInfect Dis 1995;20:320-328.
13. Kornblum MB, Wesolowski DP,Fischgrund JS, Herkowitz HN: Com-puted tomography-guided biopsy ofthe spine: A review of 103 patients.Spine 1998;23:81-85.
14. Sapico FL, Montgomerie JZ: Pyogenicvertebral osteomyelitis: Report of ninecases and review of the literature. RevInfect Dis 1979;1:754-776.
15. Berk RH, Yazici M, Atabey N, Oz-damar OS, Pabuccuoglu U, Alici E:Detection of Mycobacterium tuberculosisin formaldehyde solution-fixed, paraf-fin-embedded tissue by polymerasechain reaction in Pott�s disease. Spine1996;21:1991-1995.
16. Meier A, Persing DH, Finken M,Bottger EC: Elimination of contami-nating DNA within polymerase chainreaction reagents: Implications for ageneral approach to detection ofuncultured pathogens. J Clin Microbiol1993;31:646-652.
17. Crawford AH, Kucharzyk DW, Ruda
R, Smitherman HC Jr: Diskitis in chil-dren. Clin Orthop 1991;266:70-79.
18. Scoles PV, Quinn TP: Intervertebraldiscitis in children and adolescents.Clin Orthop 1982;162:31-36.
19. Wenger DR, Bobechko WP, Gilday DL:The spectrum of intervertebral disc-space infection in children. J Bone JointSurg Am 1978;60:100-108.
20. Eismont FJ, Bohlman HH, Soni PL,Goldberg VM, Freehafer AA: Verte-bral osteomyelitis in infants. J BoneJoint Surg Br 1982;64:32-35.
21. Omarini LP, Garcia J: CT-guided per-cutaneous puncture-biopsy of thespine: Review of 104 cases [French].Schweiz Med Wochenschr 1993;123:2191-2197.
22. Junila J, Niinimaki T, Tervonen O:Epidural abscess after lumbar discog-raphy: A case report. Spine 1997;22:2191-2193.
23. Kindler CH, Seeberger MD, StaenderSE: Epidural abscess complicatingepidural anesthesia and analgesia.Acta Anaesthesiol Scand 1998;42:614-620.
24. Knight JW, Cordingley JJ, Palazzo MG:Epidural abscess following epiduralsteroid and local anaesthetic injection.Anaesthesia 1997;52:576-578.
25. Prendergast H, Jerrard D, O�Connell J:Atypical presentations of epiduralabscess in intravenous drug abusers.Am J Emerg Med 1997;15:158-160.
26. Sampath P, Rigamonti D: Spinalepidural abscess: A review of epidemiol-ogy, diagnosis, and treatment. J SpinalDisord 1999;12:89-93.
27. Song KS, Ogden JA, Ganey T, GuideraKJ: Contiguous discitis and osteomye-litis in children. J Pediatr Orthop 1997;
17:470-477.28. Modic MT, Feiglin DH, Piraino DW, et
al: Vertebral osteomyelitis: Assessmentusing MR. Radiology 1985;157:157-166.
29. Whalen JL, Brown ML, McLeod R,Fitzgerald RH Jr: Limitations of indi-um leukocyte imaging for the diagno-sis of spine infections. Spine 1991;16:193-197.
30. Lang IM, Hughes DG, Jenkins JP, StClair Forbes W, McKenna F: MR im-aging appearances of cervical epiduralabscess. Clin Radiol 1995;50:466-471.
31. Ikeda K, Yokoyama M, Okada K,Tomita K, Yoshimura M: Long-termfollow-up of the vascularized iliac bonegraft. Microsurgery 1998;18:419-423.
32. Hayashi A, Maruyama Y, Okajima Y,Motegi M: Vascularized iliac bonegraft based on a pedicle of upper lum-bar vessels for anterior fusion of thethoraco-lumbar spine. Br J Plast Surg1994;47:425-430.
33. Mosheiff R, Meyer S, Floman Y, KaplanL, Eid A, Cohen I: Anterior vascular-ized rib strut graft in the treatment ofPott�s disease in the young child. BullHosp Jt Dis 1993;53:61-65.
34. Lascombes P, Grosdidier G, Olry R,Thomas C: Anatomical basis of the an-terior vertebral graft using a pediculatedrib. Surg Radiol Anat 1991;13:259-263.
35. A controlled trial of anterior spinalfusion and debridement in the surgicalmanagement of tuberculosis of thespine in patients on standard chemo-therapy: A study in Hong Kong. Br JSurg 1974;61:853-866.
36. Ring D, Wenger DR: Pyogenic infec-tious spondylitis in children: The evo-lution to current thought. Am J Orthop1996;25:342-348.