Embed Size (px)
Citation preview

Acta Otorrinolaringol Esp. 2012;63(3):241---243
www.elsevier.es/otorrino
CASE STUDY
Spinal-esophageal Fistula in a Patient Treated With ConcurrentChemotherapy and Radiotherapy�
Álvaro Cordero-Jiménez,∗ Rafael Tenor-Serrano, Carlos Munoz-Palza,José Rafael Solano-Romero
Servicio de Otorrinolaringología, Hospital Clínico Universitario Virgen de la Victoria, Málaga, Spain
KEYWORDSSpinal esophagealfistula;Radiotherapy adverseeffects;Extradural abscess
Abstract We present the case of a 56-year-old male patient with a history of glottic carcinomatreated with concurrent chemotherapy and radiotherapy in complete remission, who went tohospital with severe neck pain, upper right limb weakness and dysphagia. Physical examinationshowed neck stiffness as well. Spondylitis at C6---C7 spinal level with extradural abscess forma-tion was diagnosed by MRI. Barium radiography revealed an esophageal ulcer with a posteriorsinus path. Conservative treatment was given with percutaneous gastrostomy and antibiotics.The patient’s symptoms improved and the fistula and the abscess had disappeared in the laterMRI control studies.© 2010 Elsevier España, S.L. All rights reserved.
PALABRAS CLAVEFístulaesófago-raquídea;Efectos adversosradioterapia;Absceso extradural
Fístula esófago-espondilorraquídea en paciente tratado con radioterapiay quimioterapia
Resumen Varón de 56 anos con antecedente de carcinoma glótico tratado con quimioterapiay radioterapia concomitante en remisión completa. Acude a urgencias por cervicalgia intensa,paresia de miembro superior derecho y disfagia. La exploración física muestra además rigidezcervical. Se realiza resonancia magnética donde se objetiva espondilitis a nivel vertebral C6-C7
con formación de un absceso extradural que comprime la médula. Un tránsito baritado mues-tra una úlcera esofágica con trayecto fistuloso posterior. Se realiza tratamiento conservadorcon gastrostomía percutánea y antibioticoterapia. El paciente mejora ostensiblemente de sussíntomas y en los estudios de imagen de control se objetiva la desaparición de la fístula.© 2010 Elsevier España, S.L. Todos los derechos reservados.� Please cite this article as: Cordero-Jiménez Á, et al. Fístulaesófago-espondilorraquídea en paciente tratado con radioterapiay quimioterapia. Acta Otorrinolaringol Esp. 2012;63:241---3.
∗ Corresponding author.E-mail address: [email protected]
(Á. Cordero-Jiménez).
I
Cfocii
2173-5735/$ – see front matter © 2010 Elsevier España, S.L. All rights re
ntroduction
lassically, 4 major complications have been describedollowing radiotherapy treatment for laryngeal cancer:
edema of the laryngeal mucosa, radiodermatitis, peri-hondritis and cartilage radionecrosis.1 However, advancesn radiotherapy treatment planning have decreased theirncidence. We report a patient treated with radiotherapyserved.

242 Á. Cordero-Jiménez et al.
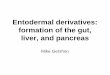
Figure 1 T1: sagittal T1-weighted MRI section showing a change in the normal signal of the vertebral bodies from C1 to T2,compatible with fat replacement after radiotherapy. We highlight a pathological enhancement of the body of C6 (arrow) indicatings showg to sp
apte
C
TgtTa
bhm
2cnrawbtt(olfiilsr
eptract disappeared on the control MRI scan. The patient wasable to restart oral feeding.
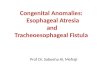
Figure 2 Coronal T1-weighted MRI with Gd section showing a
pondylitis at this level. T2: sagittal T2-weighted MRI section
oing from C2 to T1. This indicates ischaemia at this level due
nd chemotherapy for glottic squamous cell cancer, whoresented a fistula as a rare complication. This created con-inuity from the pharynx to the spinal canal, causing anpidural abscess at this level.
linical Case
he patient was a 56-year old male who attended the Emer-ency Service due to fever and severe cervical pain radiatingo the right upper limb (RUL) which decreased mobility.hese symptoms were accompanied by dysphagia to solidsnd liquids.
As pathological background of interest, the patient hadeen treated for a T3N1M0 glottic squamous carcinoma andad received concurrent radiotherapy and chemotherapy 2onths earlier.On examination, the patient presented RUL paresis of
/5 with proximal predominance, preserved sensitivity andervical stiffness. We performed laryngeal endoscopy andoted a fixed and oedematous right hemilarynx, with slighteduction of the glottic lumen. The patient was admittednd underwent a cervical spine MRI scan (Figs. 1 and 2),hich revealed an epidural collection affecting one verte-ral body and spinal cord involvement. This image appearedo rule out metastatic involvement and pointed to infec-ious complications. We also conducted a barium radiographFig. 3), which revealed an ulcer on the posterior wallf the pharyngoesophageal segment and a posterior fistu-ous tract. We established a diagnosis of pharyngeal---spinalstula as the source of the epidural abscess, which was
ndirectly responsible for spinal cord compression and neuro-ogical symptoms. We also conducted an electromyographictudy which revealed polyradiculometameric or anterioroot involvement at the level of the right C5---C7.
soCc
ing a diffuse involvement of the spine, with a signal increaseinal cord compression.
The patient showed clinical improvement after par-nteral antibiotic therapy and removal of oral feeding. Thearavertebral collection and, subsequently, the fistulous
trong meningeal enhancement from C2 to T1. It is possible tobserve a right, extramedullary collection of about 3 cm from5 to C7, presumably epidural, with a thickness of 1 cm andompressing the spine.

Spinal-esophageal Fistula in a Patient Treated with Concurrent C
iBts
rtoattc
rpt
cgd
C
T
R
1
2
3
4
5
Figure 3 Pharyngoesophageal barium radiograph showing afistulous tract in the posterior direction.
Discussion
The goal of radiation therapy is to administer a dose whichis both sufficient and evenly distributed within the tumourwhile minimising side effects in healthy adjacent tissues.2
Side effects include those with an acute or early onset,occurring approximately 2 weeks after starting radiationtherapy, and those with a chronic or late-onset, appear-ing several months after completion of treatment. Thefirst group is due to the manifestations of toxicity in rapid
renewal tissues (skin and mucous membranes). The sec-ond group appears in relation with the involvement of slowrenewal tissues (vascular endothelium, connective tissue,muscle, bone) and determines the appearance of tissue6
hemotherapy and Radiotherapy 243
schaemia, fibrosis, dystrophy, torpid ulcers and necrosis.2
ased on this, hyperbaric oxygen therapy has been used inhe treatment of laryngeal cartilage radionecrosis, since iteems to increase tissue vascularisation.3,4
In the present case we found a late-onset side effect ofadiotherapy, in which fibrosis and tissue ischaemia condi-ioned a weakening of the cervical fasciae and the formationf a fistulous tract. Normally, the cervical fasciae act as
limiting barrier in deep cervical infections. However, inhis case they had lost this barrier function and the infec-ion was able to progress to the vertebral body and spinalanal.
The treatment of late-onset necrosis or ulcers afteradiotherapy often requires surgical treatment. In ouratient, conservative treatment with antibiotics and discon-inuation of oral feeding was sufficient.
Although the literature reviewed contains numerousases of chondroradionecrosis after radiotherapy for laryn-eal squamous cancer,5,6 we did not find the complicationescribed.
onflict of Interests
he authors have no conflicts of interest to declare.
eferences
. Lederman M. Radiation therapy in cancer of the larynx. JAMA.1972;221:1253---4.
. Ferrer Albiach C, Dualde Beltrán D, Morillo Macías V. Radioterapiaen otorrinolaringología: bases del tratamiento, procedimientosy efectos secundarios. In: Suárez C, Gil-Carcedo LM, Marco J,Medina JE, Ortega P, Trinidad J, editors. Tratado de Otorrino-laringología y Cirugía de Cabeza y Cuello. Tomo I. 2. a ediciónMadrid: Editorial Médica Panamericana; 2007. p. 115---26.
. Zbären P, Caversaccio M, Thoeny HC. Radionecrosis or tumorrecurrence after radiation of laryngeal and hypopharyngeal car-cinomas. Otolaryngol Head Neck Surg. 2006;135:838---43.
. Narozny W, Sicko Z, Kot J, Stankiewicz C, Przewozry T,Kuczkowski J. Hyperbaric oxygen therapy in the treatment ofcomplication of irradiation in head and neck area. UnderseaHyperb Med. 2005;32:103---10.
. Shimizu N, Okamoto H, Fukuda T, Yane K, Hosoi H. Late laryn-geal radionecrosis in severe arteriosclerosis. J Laryngol Otol.
2005;119:922---5.. Sancho E, Escorial O, Cortés JM, Rivas P, Millán J, VallésH. Condrorradionecrosis laríngea. Acta Otorrinolaringol Esp.2003;54:123---6.