Embed Size (px)
Citation preview
Spinal Decompression Surgery
Medical Coverage Policy
Effective Date: 01/01/2012 Revision Date: 01/01/2012 Review Date: 09/22/2011 Policy Number: CLPD-0483-009
Page: 1 of 20
Change Summary: Updated Provider Claims Codes
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
Disclaimer Description Coverage Determination Background
Medical Alternatives Provider Claims Codes Medical Terms References
Disclaimer
State and federal law, as well as contract language, including definitions and specific inclusions/ exclusions, take precedence over clinical policy and must be considered first in determining eligibility for coverage. Coverage may also differ for our Medicare and/or Medicaid members based on any applicable Centers for Medicare & Medicaid Services (CMS) coverage statements including National Coverage Determinations (NCD), Local Medical Review Policies (LMRP), and/or Local Coverage Determinations. See the CMS web site at http://www.cms.hhs.gov/. The member's health plan benefits, in effect on the date services are rendered, must be used. Clinical policy is not intended to preempt the judgment of the reviewing Medical Director or dictate to providers how to practice medicine. Providers are expected to exercise their medical judgment in rendering the most appropriate care. Identification of selected brand names of devices, tests, and procedures in a Medical Coverage Policy are for reference only and is not an endorsement of any one device, test or procedure over another. Clinical technology is constantly evolving, and we reserve the right to review and update this policy periodically. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any shape or form or by any means, electronic, mechanical, photocopying, or otherwise, without permission from Humana Inc.
Description Spinal decompression surgery is a general term that refers to various procedures intended to relieve symptoms caused by pressure or compression on the spinal cord and/or nerve roots. Depending on the location and cause of the compression, this may be accomplished by performing a discectomy, laminectomy, laminotomy, foraminotomy, foraminectomy, corpectomy, facetectomy, spinal fusion (for information regarding spinal fusions, please refer to Spinal Fusion Surgery (Cervical and Lumbar) Medical Coverage Policy), or a combination of these procedures. Discectomy (diskectomy) is the most common surgical treatment for ruptured or herniated discs, particularly of the lumbar spine, though it may also be used on the cervical or thoracic spine. During a discectomy, the surgeon removes the section of the disc that is protruding from the disc wall and also any other disc fragments that may be pressing on a nerve root or the spinal cord. A discectomy may be “open” or it may be performed microscopically (known as a microdiscectomy). Both procedures allow for direct visualization of the vertebra, disc, and other surrounding structures. The microdiscectomy utilizes
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 2 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
a special microscope or magnifying instrument to view the disc and nerves, which makes it possible to remove the disc material through a smaller incision. This smaller incision reduces the risk of damage to the surrounding tissues, which decreases the potential complications. An arthroscopic microdiscectomy, also known as a percutaneous endoscopic discectomy, has been proposed as another alternative to the traditional open procedure or the microdiscectomy. A cannula is inserted near the spine through which an endoscope and very small surgical instruments are then inserted. The herniated portion of the disc can then be removed. This procedure does not allow direct visualization of the disc or surrounding tissues. Examples of a device used in an arthroscopic microdiscectomy/percutaneous endoscopic discectomy would include, but may not be limited to, the Yeung Endoscopic Spinal System (Y.E.S.S.) or the AccuraScope DND. (Please refer to the Coverage Limitations section). Automated percutaneous lumbar discectomy (APLD) or automated percutaneous mechanical lumbar discectomy is another newer approach for surgical treatment of herniated discs. In this procedure, under fluoroscopic guidance, a cannula is inserted into the disc; an automated cutting and aspiration device is then inserted through the cannula and the disc material is removed. An example of a device used for this type of procedure includes, but may not be limited to, the Stryker Dekompressor Lumbar Discectomy Probe. (Please refer to the Coverage Limitations section). Laser discectomy is also known as laser-assisted discectomy, laser disc decompression or laser-assisted disc decompression (LADD). Though this procedure is called a discectomy, it does not actually remove the disc, but utilizes a laser to “vaporize” a small portion of the nucleus pulposus in order to decompress a herniated disc. Laser discectomy may be performed either percutaneously or laparoscopically. (Please refer to the Coverage Limitations section). Percutaneous laser discectomy is performed under a local anesthetic. Under x-ray (fluoroscopic) guidance, a needle is inserted through the skin into the disc. A flexible quartz fiber is then threaded through the needle and into the disc, which delivers the laser energy. (Please refer to the Coverage Limitations section).
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 3 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
In a laparoscopic laser discectomy, the procedure is done through a laparoscope, which allows visualization of the disc, disc space, and other structures. The annulus of the disc is opened and is then excised with a laser device which was inserted through the laparoscope. (Please refer to the Coverage Limitations section). Foraminectomy and foraminotomy – these procedures are performed to expand the openings (foramen) for the nerve roots to exit the spinal cord by removing some bone and other tissue. A foraminectomy or foraminotomy is often performed on an individual who has arthritis, a lateral disc herniation, or spinal stenosis. The term foraminectomy is used to refer to a procedure that removes a large amount of bone and tissue, and foraminotomy when a smaller amount is removed. A microsurgical anterior foraminotomy is a more recently developed procedure for the treatment of cervical radiculopathy as a result of a narrowing of the foramen. Microsurgical instruments are used through a small incision, which is proposed as a way to decrease damage to surrounding tissue and/or the lamina or facets. Laminectomy and laminotomy – these procedures involve removal of a small part of the bony arches of the spinal canal, called the lamina, which increases the size of the spinal canal. A laminectomy or laminotomy is most commonly performed for a diagnosis of spinal stenosis. During a laminectomy the entire lamina is removed. In a laminotomy, only a portion of the lamina is removed. These procedures are also often done with either a discectomy or a foraminectomy/foraminotomy. Minimally invasive approaches for laminectomy, laminotomy, foraminectomy, or foraminotomy have also proposed as a newer treatment option by some surgeons. They may utilize either an endoscopic or laparoscopic approach for the procedure. Additionally, percutaneous procedures have also been proposed as an alternative surgical approach for laminectomy, laminotomy, foraminectomy, or foraminotomy. The percutaneous procedures are generally performed in an outpatient setting with the individual awake but sedated. One example of a percutaneous decompression procedure for spinal stenosis is the MILD® procedure, which utilizes trocars to access the area of stenosis. (Please refer to the Coverage Limitations section).
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 4 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Laminoplasty is a variation that may be used in an effort to lessen the chance of deformity that can develop when a facetectomy or laminectomy is performed alone. In a laminoplasty the laminae are split and then held apart by bone struts, sutures, or other techniques, in order to enlarge the spinal canal diameter. This procedure is usually performed on the cervical spine. A corpectomy is a procedure to remove the body of a vertebra, as well as the disc. This is most commonly performed in the cervical (neck area) spine, and is in conjunction with a fusion. Please note: For information regarding other back pain treatments or procedures, please refer to the following medical coverage policies: Electrothermal Intradiscal Therapies Medical Coverage Policy, Neuroablative Techniques for Chronic Spinal Pain Medical Coverage Policy, Interspinous Process Decompression Spacers (X-Stop®) Medical Coverage Policy, Percutaneous Vertebroplasty, Kyphoplasty (Balloon-Assisted Vertebroplasty), Sacroplasty Medical Coverage Policy, Spinal Fusion Surgery (Cervical and Lumbar) Medical Coverage Policy, Injections for Pain Conditions Medical Coverage Policy, or Dynamic Spinal Stabilization Devices Medical Coverage Policy.
Coverage Determination
Humana members may be eligible under the Plan for discectomy (including microdiscectomy) of the cervical, thoracic, or lumbar spine for the following indications:
Evidence of myelopathy confirmed by imaging studies (e.g., computed tomography [CT] scan or magnetic resonance imaging [MRI]) with corresponding clinical symptoms (including, but may not be limited to, bowel or bladder incontinence, clumsiness of hands, frequent falls, urinary urgency) and corresponding objective neurologic signs (including, but may not be limited to, hyperreflexia, Hoffman sign, increased tone or spasticity); OR
Rapidly progressive neurologic signs/symptoms of lumbar spine compression confirmed by imaging studies (e.g., CT scan or MRI); OR
Spinal fractures confirmed by imaging studies (e.g., CT scan or MRI); OR
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 5 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Spinal infection confirmed by imaging studies (e.g., CT scan or MRI); OR
Spinal tumor confirmed by imaging studies (e.g., CT scan or MRI); OR
Herniated disc, confirmed by imaging studies (e.g., MRI or myelogram); AND
Radicular* pain that has persisted despite appropriate conservative treatment (e.g., rest, medications, physical therapy, etc.).
*Lumbar (low back) radicular pain typically radiates to the level of the knee or more distally and is associated with segmental nerve root impingement. Cervical (neck) radicular pain typically radiates down one or both arms and is associated with segmental nerve root impingement. Humana members may be eligible under the Plan for a cervical laminectomy, laminotomy, foraminectomy, foraminotomy, or a foraminolaminectomy for the following indications:
Congenital cervical spinal stenosis; OR
Cord compression as result of rheumatoid arthritis (usually performed with a spinal fusion) (please refer to Spinal Fusion Surgery (Cervical and Lumbar) Medical Coverage Policy) ; OR
Degenerative spondylolisthesis (usually performed with a spinal fusion) (please refer to Spinal Fusion Surgery (Cervical and Lumbar) Medical Coverage Policy) ; OR
Evidence of myelopathy confirmed by imaging studies (e.g., CT scan or MRI) with corresponding clinical symptoms (including, but may not be limited to, bowel or bladder incontinence, clumsiness of hands, frequent falls, urinary urgency) and corresponding objective neurologic signs (including, but may not be limited to, hyperreflexia, Hoffman sign, increased tone or spasticity); OR
Ossification of posterior longitudinal ligament (three or more levels) with cord compression confirmed by imaging studies (e.g., CT scan, MRI, or myelogram); OR
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 6 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Spinal fractures confirmed by imaging studies (e.g., CT scan or MRI); OR
Spinal infection confirmed by imaging studies (e.g., CT scan or MRI); OR
Spinal injury from epidural hematoma; OR
Spinal injury from foreign bodies; OR
Spinal tumor confirmed by imaging studies (e.g., CT scan or MRI); OR
Herniated disc or spinal stenosis at the level corresponding with clinical findings confirmed by imaging studies (e.g., magnetic resonance imaging (MRI) or myelogram); AND
Physical and neurological abnormalities suggestive of nerve root or spinal cord compression (e.g., weakness, sensory loss, reflex change); AND
Radicular* pain that has persisted despite appropriate conservative treatment (e.g., rest, medications, physical therapy, etc.).
Humana members may be eligible under the Plan for a lumbar laminectomy, laminotomy, foraminectomy, foraminotomy, or a foraminolaminectomy for the following indications:
Cauda equina syndrome (bowel or bladder dysfunction, bilateral lower extremity weakness/numbness/decreased sensation, saddle anesthesia) confirmed by imaging studies (e.g., computed tomography (CT) scan or MRI); OR
Rapidly progressive neurologic signs/symptoms of lumbar spine compression confirmed by imaging studies (e.g., CT scan or MRI); OR
Spinal fractures confirmed by imaging studies (e.g., CT scan or MRI); OR
Spinal infection confirmed by imaging studies (e.g., CT scan or MRI); OR
Spinal injury from epidural hematoma; OR
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 7 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Spinal injury from foreign bodies; OR
Spinal tumor confirmed by imaging studies (e.g., CT scan or MRI); OR
Spondylolisthesis (usually performed with a spinal fusion) (please refer to Spinal Fusion Surgery (Cervical and Lumbar) Medical Coverage Policy) ; OR
Herniated disc or spinal stenosis at the level corresponding with clinical findings confirmed by imaging studies (e.g., magnetic resonance imaging (MRI) or myelogram); AND
Physical and/or neurological abnormalities suggestive of nerve root or spinal cord compression (e.g., weakness, sensory loss, reflex change); AND
Radicular* pain that has persisted despite appropriate conservative treatment (e.g., rest, medications, physical therapy, etc.).
Humana members may be eligible under the Plan for a thoracic or sacral laminectomy, laminotomy, foraminectomy, foraminotomy, or a foraminolaminectomy for the following indications:
Spinal fractures confirmed by imaging studies (e.g., CT scan or MRI); OR
Spinal infection confirmed by imaging studies (e.g., CT scan or MRI); OR
Spinal injury from epidural hematoma; OR
Spinal injury from foreign bodies; OR
Spinal tumor confirmed by imaging studies (e.g., CT scan or MRI). Humana members may be eligible under the Plan for a laminoplasty for severe cervical spinal stenosis at multiple (greater than or equal to three) levels with compressive myelopathy. Humana members may be eligible under the Plan for a corpectomy for spinal cord or nerve root compression due to ossification of the posterior longitudinal ligament (if treated anteriorly), vertebral fractures or tumors in the cervical, thoracic, or lumbar regions.
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 8 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Coverage Limitations
Note: A minimally invasive approach (laparoscopic or endoscopic) to spinal decompression surgery is considered integral to the primary procedure and would not be subject to additional reimbursement on the part of the surgeon or the facility. This would include, but may not be limited to, the use of the METRx® system (X-tube), a tubular microdiskectomy, microendoscopic discectomy (MED), or a microsurgical anterior foraminotomy. Additionally, robotic-assisted surgery and/or robotic guidance systems (e.g., Renaissance™ system) is considered integral to the primary procedure and not separately reimbursable. Humana members may NOT be eligible under the Plan for discectomy (including microdiscectomy) for any indications other than those listed above (in the coverage determinations section). These technologies are considered experimental/investigational or NOT medically necessary if they are not utilized in accordance with nationally recognized standards of medical practice and/or identified as safe, widely used and generally accepted as effective for the proposed use as reported in nationally recognized peer-reviewed medical literature published in the English language. Humana members may NOT be eligible under the Plan for any other type of discectomy procedure, including, but not limited to the following:
Arthroscopic microdiscectomy (also known as percutaneous endoscopic discectomy), including but may not be limited to the Yeung Endoscopic Spinal System or the AccuraScope DND; OR
Automated percutaneous lumbar discectomy (APLD) ( also known as automated percutaneous mechanical lumbar discectomy), including but may not be limited to the Stryker Dekompressor Lumbar Discectomy Probe; OR
Laser discectomy, regardless of approach, including percutaneous laser discectomy, laser-assisted discectomy, laser disc decompression or laser-assisted disc decompression; OR
Percutaneous discectomy techniques not previously listed.
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 9 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
These technologies are considered experimental/investigational as they are not identified as widely used and generally accepted for the proposed use as reported in nationally recognized peer-reviewed medical literature published in the English language. Humana members may NOT be eligible under the Plan for laminectomy, laminotomy, foraminectomy, foraminotomy, foraminolaminectomy, laminoplasty, or corpectomy for any indications other than those listed above (in the coverage determinations section). These technologies are considered experimental/investigational or NOT medically necessary if they are not utilized in accordance with nationally recognized standards of medical practice and/or identified as safe, widely used and generally accepted as effective for the proposed use as reported in nationally recognized peer-reviewed medical literature published in the English language. Humana members may NOT be eligible under the Plan for any other type of laminectomy, laminotomy, foraminectomy, foraminotomy, foraminolaminectomy, laminoplasty, or corpectomy procedure including but not limited to the following:
ANY percutaneous laminectomy, laminotomy, foraminectomy, foraminotomy, foraminolaminectomy, laminoplasty, or corpectomy, including but not limited to the MILD® procedure; OR
Laser laminectomy These technologies are considered experimental/investigational as they are not identified as widely used and generally accepted for the proposed use as reported in nationally recognized peer-reviewed medical literature published in the English language.
Background You can learn more about neck or back pain, degenerative disc disease, spinal stenosis, and other spinal conditions from the following sites:
National Institute of Neurological Disorders and Stroke (NINDS) - http://www.ninds.nih.gov
National Library of Medicine - http://www.nlm.nih.gov
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 10 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
North American Spine Society (NASS) - http://www.spine.org
Medical Alternatives
Alternatives to discectomy include, but may not be limited to, the following:
Physical Therapy (please refer to Physical Therapy and Occupational Therapy Medical Coverage Policy)
Prescription drug therapy may be appropriate for this condition
Therapeutic pain injections (e.g., epidural steroid injections) (please refer to Injections for Pain Conditions Medical Coverage Policy).
Alternatives to laser discectomy, arthroscopic microdiscectomy, or APLD include, but may not be limited to, the following:
Discectomy (“standard”, traditional approach, i.e., open or microdiscectomy)
Physical Therapy (please refer to Physical Therapy and Occupational Therapy Medical Coverage Policy)
Prescription drug therapy may be appropriate for this condition
Therapeutic pain injections (e.g., epidural steroid injections) (please refer to Injections for Pain Conditions Medical Coverage Policy).
Alternatives to laminectomy, laminotomy, foraminectomy, foraminotomy, or foraminolaminectomy include, but may not be limited to the following:
Physical Therapy (please refer to Physical Therapy and Occupational Therapy Medical Coverage Policy)
Prescription drug therapy may be appropriate for this condition
Therapeutic pain injections (e.g., epidural steroid injections) (please refer to Injections for Pain Conditions Medical Coverage Policy).
Alternatives to laminoplasty include, but may not be limited to the following:
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 11 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Physical Therapy (please refer to Physical Therapy and Occupational Therapy Medical Coverage Policy)
Prescription drug therapy may be appropriate for this condition
Therapeutic pain injections (e.g., epidural steroid injections) (please refer to Injections for Pain Conditions Medical Coverage Policy)
Spinal fusion (please refer to Spinal Fusion Surgery Medical Coverage Policy).
Alternatives to corpectomy include, but may not be limited to the following:
Physical Therapy (please refer to Physical Therapy and Occupational Therapy Medical Coverage Policy)
Prescription drug therapy may be appropriate for this condition
Therapeutic pain injections (e.g., epidural steroid injections) (please refer to Injections for Pain Conditions Medical Coverage Policy)
Spinal fusion (please refer to Spinal Fusion Surgery Medical Coverage Policy).
Alternatives to microsurgical anterior foraminotomy include, but may not be limited to the following:
Foraminotomy using a “traditional” approach
Physical Therapy (please refer to Physical Therapy and Occupational Therapy Medical Coverage Policy)
Prescription drug therapy may be appropriate for this condition
Therapeutic pain injections (e.g., epidural steroid injections) (please refer to Injections for Pain Conditions Medical Coverage Policy).
Alternatives to endoscopic laser laminectomy include, but may not be limited to the following:
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 12 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
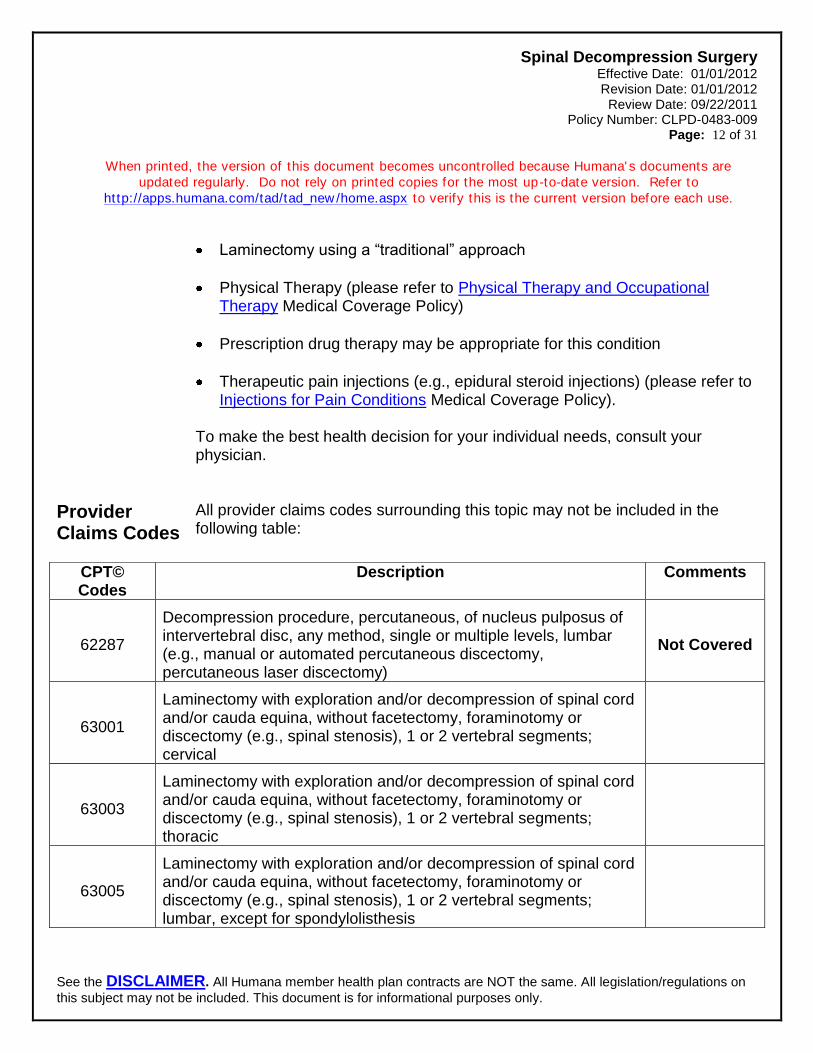
Laminectomy using a “traditional” approach
Physical Therapy (please refer to Physical Therapy and Occupational Therapy Medical Coverage Policy)
Prescription drug therapy may be appropriate for this condition
Therapeutic pain injections (e.g., epidural steroid injections) (please refer to Injections for Pain Conditions Medical Coverage Policy).
To make the best health decision for your individual needs, consult your physician.
Provider Claims Codes
All provider claims codes surrounding this topic may not be included in the following table:
CPT© Codes
Description Comments
62287
Decompression procedure, percutaneous, of nucleus pulposus of intervertebral disc, any method, single or multiple levels, lumbar (e.g., manual or automated percutaneous discectomy, percutaneous laser discectomy)
Not Covered
63001
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (e.g., spinal stenosis), 1 or 2 vertebral segments; cervical
63003
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (e.g., spinal stenosis), 1 or 2 vertebral segments; thoracic
63005
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (e.g., spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 13 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
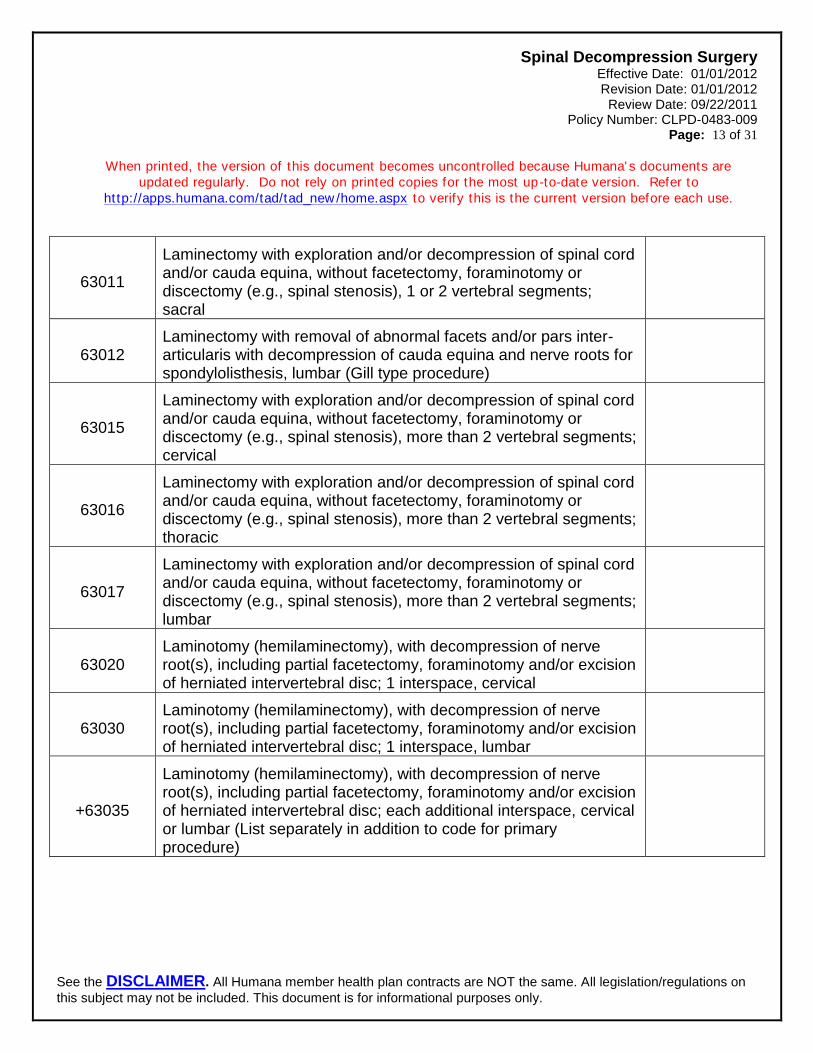
63011
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (e.g., spinal stenosis), 1 or 2 vertebral segments; sacral
63012 Laminectomy with removal of abnormal facets and/or pars inter-articularis with decompression of cauda equina and nerve roots for spondylolisthesis, lumbar (Gill type procedure)
63015
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (e.g., spinal stenosis), more than 2 vertebral segments; cervical
63016
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (e.g., spinal stenosis), more than 2 vertebral segments; thoracic
63017
Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (e.g., spinal stenosis), more than 2 vertebral segments; lumbar
63020 Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, cervical
63030 Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar
+63035
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; each additional interspace, cervical or lumbar (List separately in addition to code for primary procedure)
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 14 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
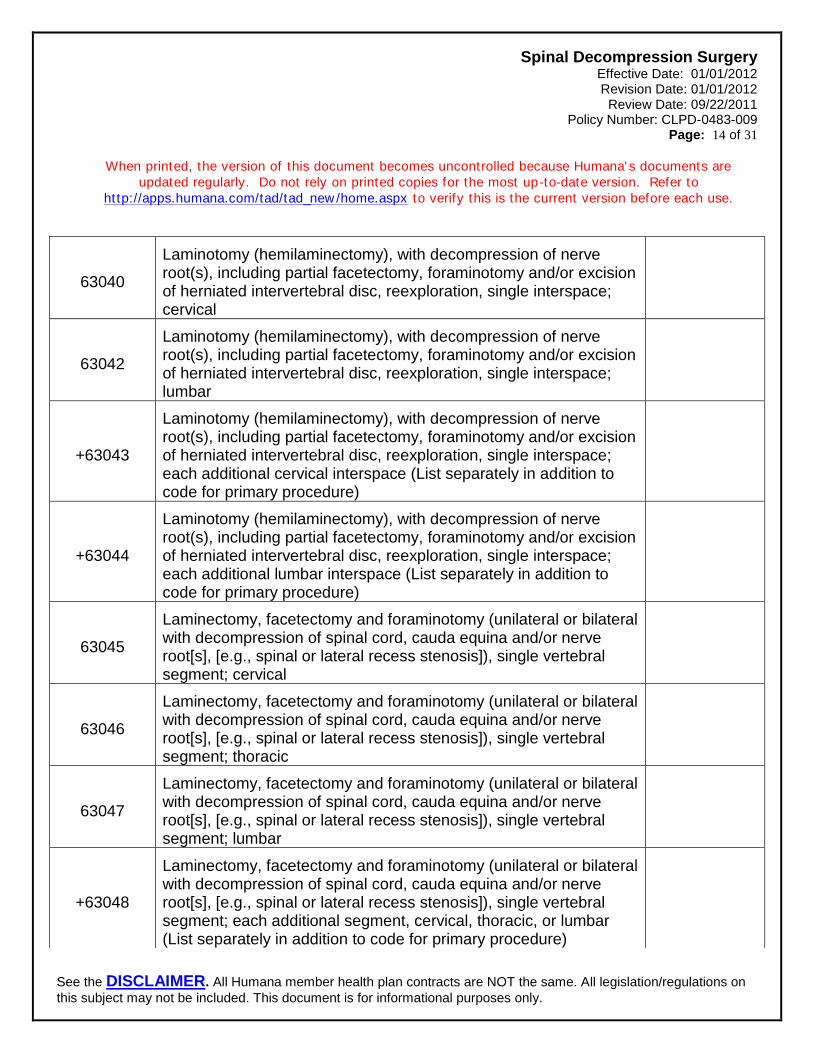
63040
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc, reexploration, single interspace; cervical
63042
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc, reexploration, single interspace; lumbar
+63043
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc, reexploration, single interspace; each additional cervical interspace (List separately in addition to code for primary procedure)
+63044
Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc, reexploration, single interspace; each additional lumbar interspace (List separately in addition to code for primary procedure)
63045
Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [e.g., spinal or lateral recess stenosis]), single vertebral segment; cervical
63046
Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [e.g., spinal or lateral recess stenosis]), single vertebral segment; thoracic
63047
Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [e.g., spinal or lateral recess stenosis]), single vertebral segment; lumbar
+63048
Laminectomy, facetectomy and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], [e.g., spinal or lateral recess stenosis]), single vertebral segment; each additional segment, cervical, thoracic, or lumbar (List separately in addition to code for primary procedure)
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 15 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
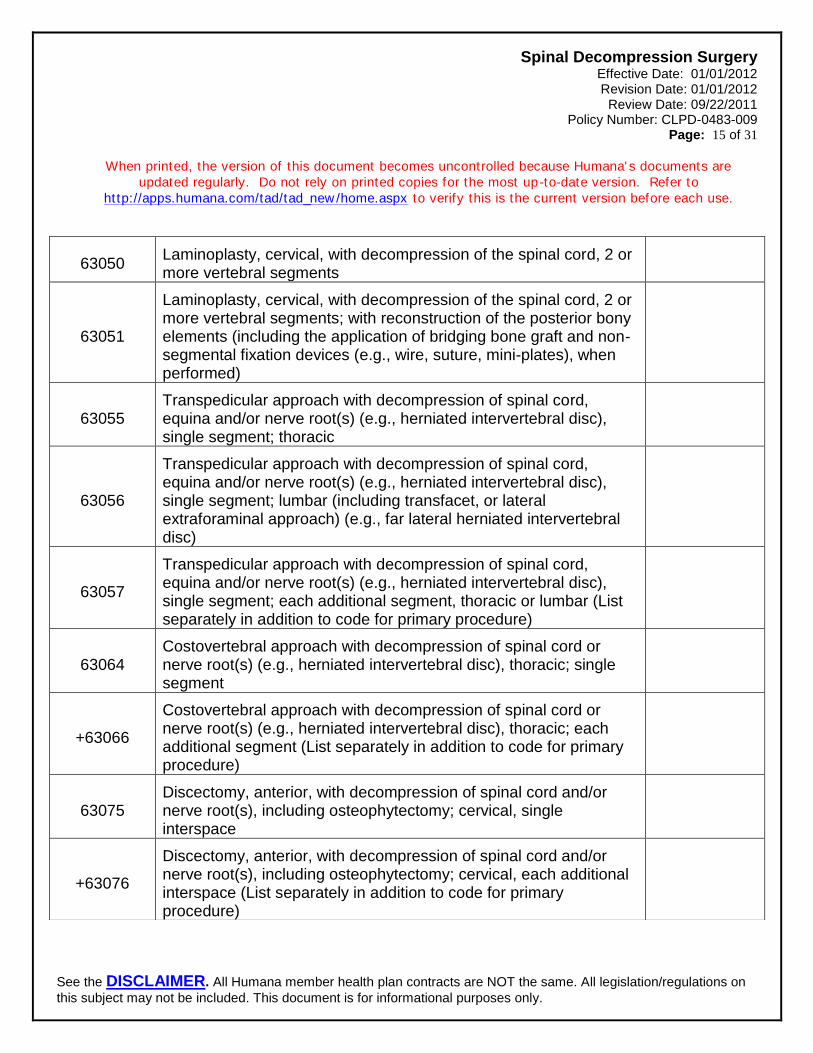
63050 Laminoplasty, cervical, with decompression of the spinal cord, 2 or more vertebral segments
63051
Laminoplasty, cervical, with decompression of the spinal cord, 2 or more vertebral segments; with reconstruction of the posterior bony elements (including the application of bridging bone graft and non-segmental fixation devices (e.g., wire, suture, mini-plates), when performed)
63055 Transpedicular approach with decompression of spinal cord, equina and/or nerve root(s) (e.g., herniated intervertebral disc), single segment; thoracic
63056
Transpedicular approach with decompression of spinal cord, equina and/or nerve root(s) (e.g., herniated intervertebral disc), single segment; lumbar (including transfacet, or lateral extraforaminal approach) (e.g., far lateral herniated intervertebral disc)
63057
Transpedicular approach with decompression of spinal cord, equina and/or nerve root(s) (e.g., herniated intervertebral disc), single segment; each additional segment, thoracic or lumbar (List separately in addition to code for primary procedure)
63064 Costovertebral approach with decompression of spinal cord or nerve root(s) (e.g., herniated intervertebral disc), thoracic; single segment
+63066
Costovertebral approach with decompression of spinal cord or nerve root(s) (e.g., herniated intervertebral disc), thoracic; each additional segment (List separately in addition to code for primary procedure)
63075 Discectomy, anterior, with decompression of spinal cord and/or nerve root(s), including osteophytectomy; cervical, single interspace
+63076
Discectomy, anterior, with decompression of spinal cord and/or nerve root(s), including osteophytectomy; cervical, each additional interspace (List separately in addition to code for primary procedure)
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 16 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
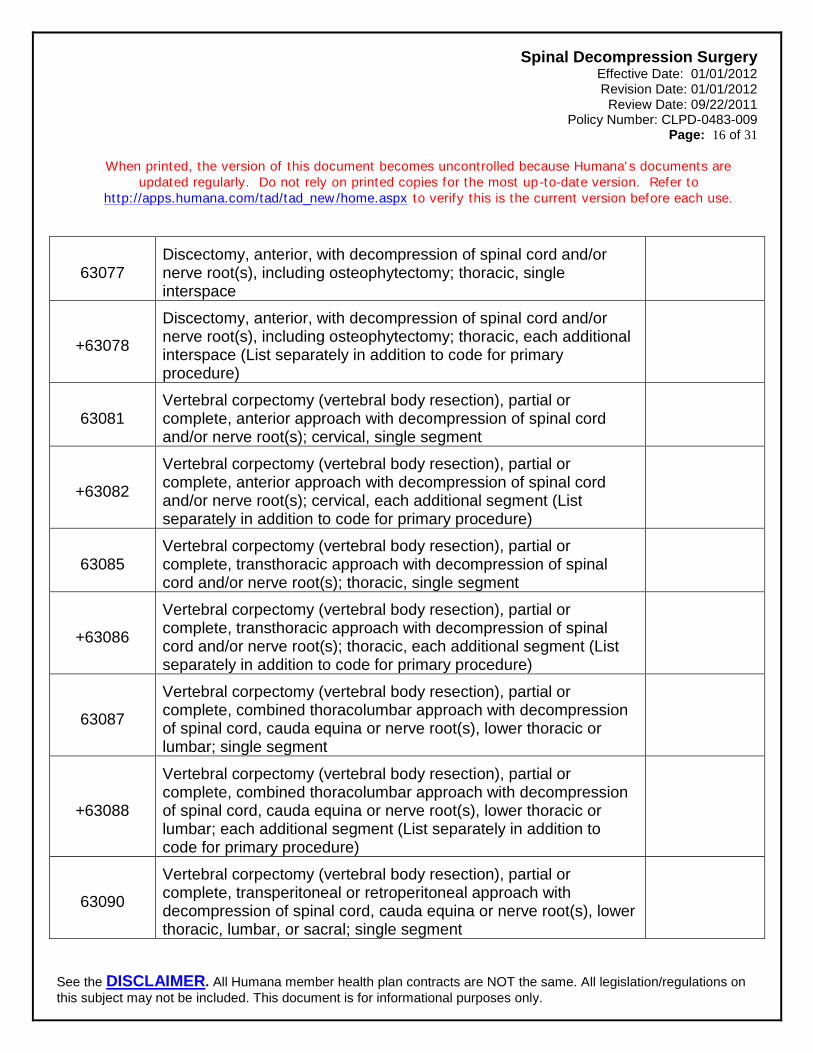
63077 Discectomy, anterior, with decompression of spinal cord and/or nerve root(s), including osteophytectomy; thoracic, single interspace
+63078
Discectomy, anterior, with decompression of spinal cord and/or nerve root(s), including osteophytectomy; thoracic, each additional interspace (List separately in addition to code for primary procedure)
63081 Vertebral corpectomy (vertebral body resection), partial or complete, anterior approach with decompression of spinal cord and/or nerve root(s); cervical, single segment
+63082
Vertebral corpectomy (vertebral body resection), partial or complete, anterior approach with decompression of spinal cord and/or nerve root(s); cervical, each additional segment (List separately in addition to code for primary procedure)
63085 Vertebral corpectomy (vertebral body resection), partial or complete, transthoracic approach with decompression of spinal cord and/or nerve root(s); thoracic, single segment
+63086
Vertebral corpectomy (vertebral body resection), partial or complete, transthoracic approach with decompression of spinal cord and/or nerve root(s); thoracic, each additional segment (List separately in addition to code for primary procedure)
63087
Vertebral corpectomy (vertebral body resection), partial or complete, combined thoracolumbar approach with decompression of spinal cord, cauda equina or nerve root(s), lower thoracic or lumbar; single segment
+63088
Vertebral corpectomy (vertebral body resection), partial or complete, combined thoracolumbar approach with decompression of spinal cord, cauda equina or nerve root(s), lower thoracic or lumbar; each additional segment (List separately in addition to code for primary procedure)
63090
Vertebral corpectomy (vertebral body resection), partial or complete, transperitoneal or retroperitoneal approach with decompression of spinal cord, cauda equina or nerve root(s), lower thoracic, lumbar, or sacral; single segment
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 17 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
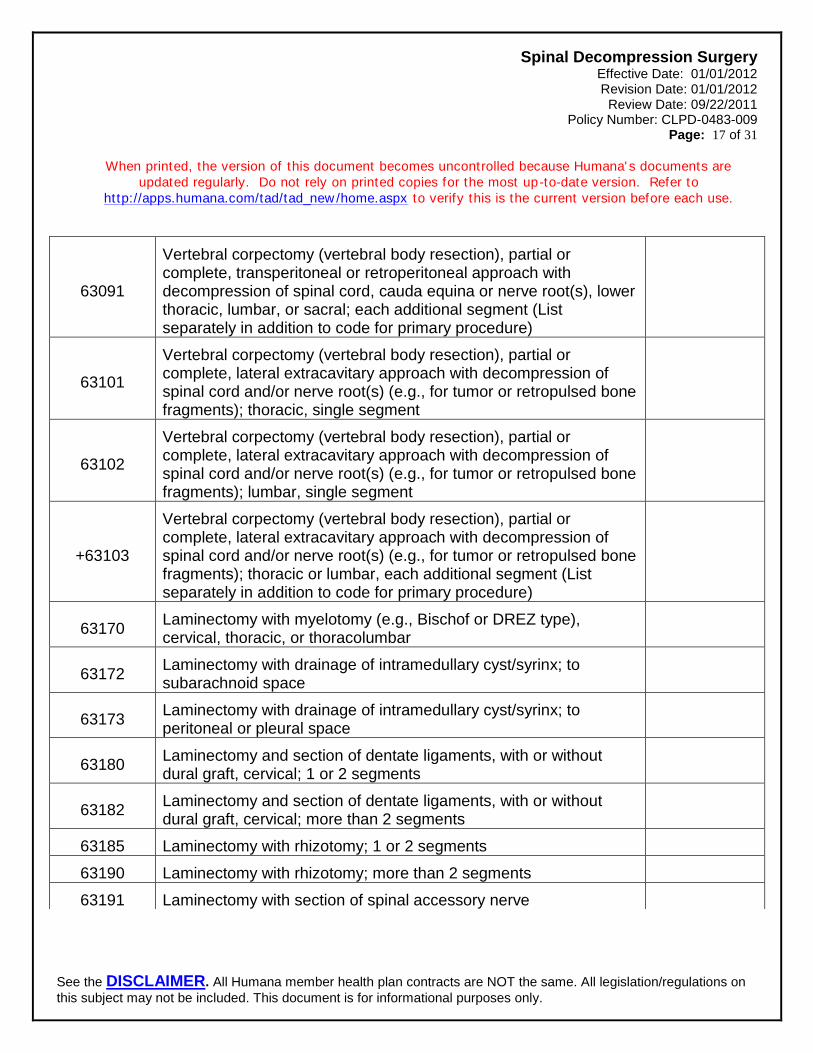
63091
Vertebral corpectomy (vertebral body resection), partial or complete, transperitoneal or retroperitoneal approach with decompression of spinal cord, cauda equina or nerve root(s), lower thoracic, lumbar, or sacral; each additional segment (List separately in addition to code for primary procedure)
63101
Vertebral corpectomy (vertebral body resection), partial or complete, lateral extracavitary approach with decompression of spinal cord and/or nerve root(s) (e.g., for tumor or retropulsed bone fragments); thoracic, single segment
63102
Vertebral corpectomy (vertebral body resection), partial or complete, lateral extracavitary approach with decompression of spinal cord and/or nerve root(s) (e.g., for tumor or retropulsed bone fragments); lumbar, single segment
+63103
Vertebral corpectomy (vertebral body resection), partial or complete, lateral extracavitary approach with decompression of spinal cord and/or nerve root(s) (e.g., for tumor or retropulsed bone fragments); thoracic or lumbar, each additional segment (List separately in addition to code for primary procedure)
63170 Laminectomy with myelotomy (e.g., Bischof or DREZ type), cervical, thoracic, or thoracolumbar
63172 Laminectomy with drainage of intramedullary cyst/syrinx; to subarachnoid space
63173 Laminectomy with drainage of intramedullary cyst/syrinx; to peritoneal or pleural space
63180 Laminectomy and section of dentate ligaments, with or without dural graft, cervical; 1 or 2 segments
63182 Laminectomy and section of dentate ligaments, with or without dural graft, cervical; more than 2 segments
63185 Laminectomy with rhizotomy; 1 or 2 segments
63190 Laminectomy with rhizotomy; more than 2 segments
63191 Laminectomy with section of spinal accessory nerve
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 18 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
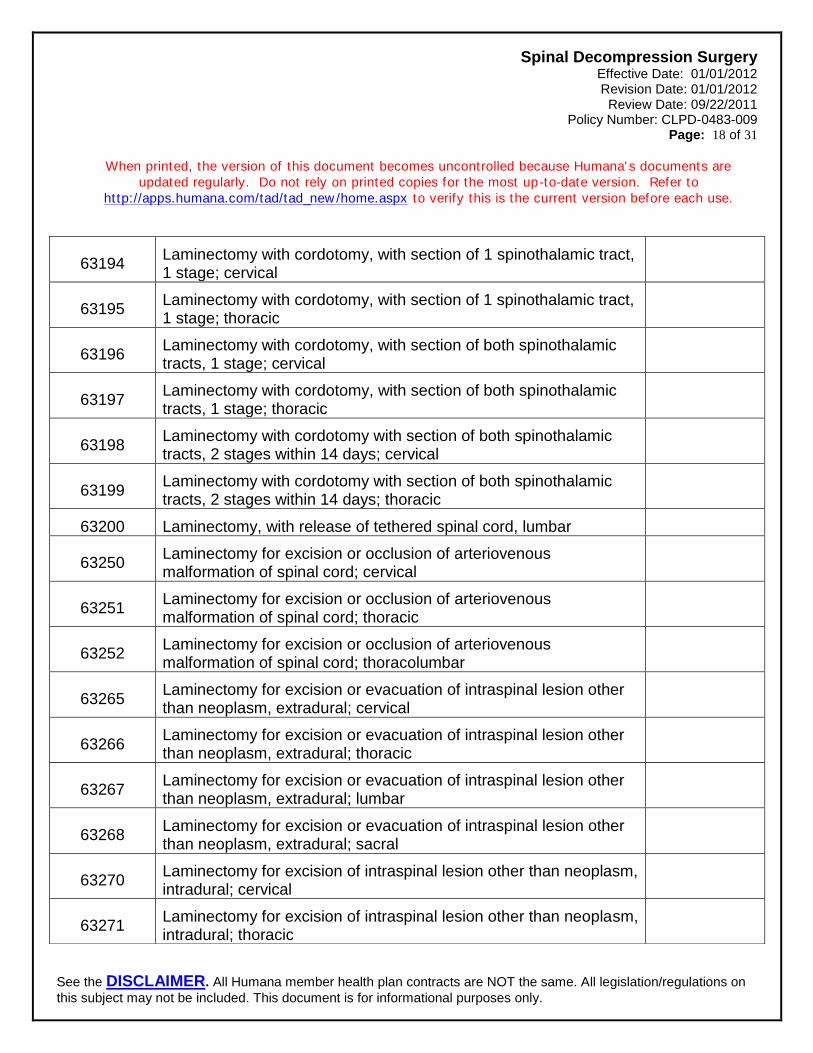
63194 Laminectomy with cordotomy, with section of 1 spinothalamic tract, 1 stage; cervical
63195 Laminectomy with cordotomy, with section of 1 spinothalamic tract, 1 stage; thoracic
63196 Laminectomy with cordotomy, with section of both spinothalamic tracts, 1 stage; cervical
63197 Laminectomy with cordotomy, with section of both spinothalamic tracts, 1 stage; thoracic
63198 Laminectomy with cordotomy with section of both spinothalamic tracts, 2 stages within 14 days; cervical
63199 Laminectomy with cordotomy with section of both spinothalamic tracts, 2 stages within 14 days; thoracic
63200 Laminectomy, with release of tethered spinal cord, lumbar
63250 Laminectomy for excision or occlusion of arteriovenous malformation of spinal cord; cervical
63251 Laminectomy for excision or occlusion of arteriovenous malformation of spinal cord; thoracic
63252 Laminectomy for excision or occlusion of arteriovenous malformation of spinal cord; thoracolumbar
63265 Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; cervical
63266 Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; thoracic
63267 Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; lumbar
63268 Laminectomy for excision or evacuation of intraspinal lesion other than neoplasm, extradural; sacral
63270 Laminectomy for excision of intraspinal lesion other than neoplasm, intradural; cervical
63271 Laminectomy for excision of intraspinal lesion other than neoplasm, intradural; thoracic
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 19 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
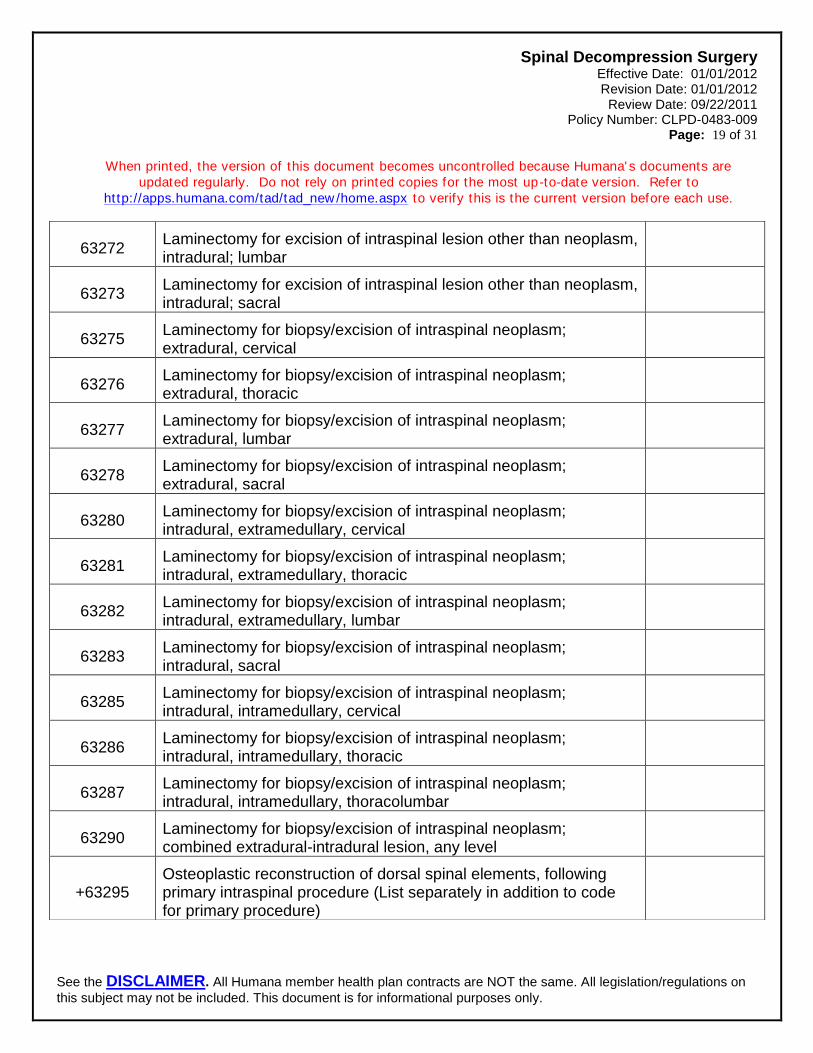
63272 Laminectomy for excision of intraspinal lesion other than neoplasm, intradural; lumbar
63273 Laminectomy for excision of intraspinal lesion other than neoplasm, intradural; sacral
63275 Laminectomy for biopsy/excision of intraspinal neoplasm; extradural, cervical
63276 Laminectomy for biopsy/excision of intraspinal neoplasm; extradural, thoracic
63277 Laminectomy for biopsy/excision of intraspinal neoplasm; extradural, lumbar
63278 Laminectomy for biopsy/excision of intraspinal neoplasm; extradural, sacral
63280 Laminectomy for biopsy/excision of intraspinal neoplasm; intradural, extramedullary, cervical
63281 Laminectomy for biopsy/excision of intraspinal neoplasm; intradural, extramedullary, thoracic
63282 Laminectomy for biopsy/excision of intraspinal neoplasm; intradural, extramedullary, lumbar
63283 Laminectomy for biopsy/excision of intraspinal neoplasm; intradural, sacral
63285 Laminectomy for biopsy/excision of intraspinal neoplasm; intradural, intramedullary, cervical
63286 Laminectomy for biopsy/excision of intraspinal neoplasm; intradural, intramedullary, thoracic
63287 Laminectomy for biopsy/excision of intraspinal neoplasm; intradural, intramedullary, thoracolumbar
63290 Laminectomy for biopsy/excision of intraspinal neoplasm; combined extradural-intradural lesion, any level
+63295 Osteoplastic reconstruction of dorsal spinal elements, following primary intraspinal procedure (List separately in addition to code for primary procedure)
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 20 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
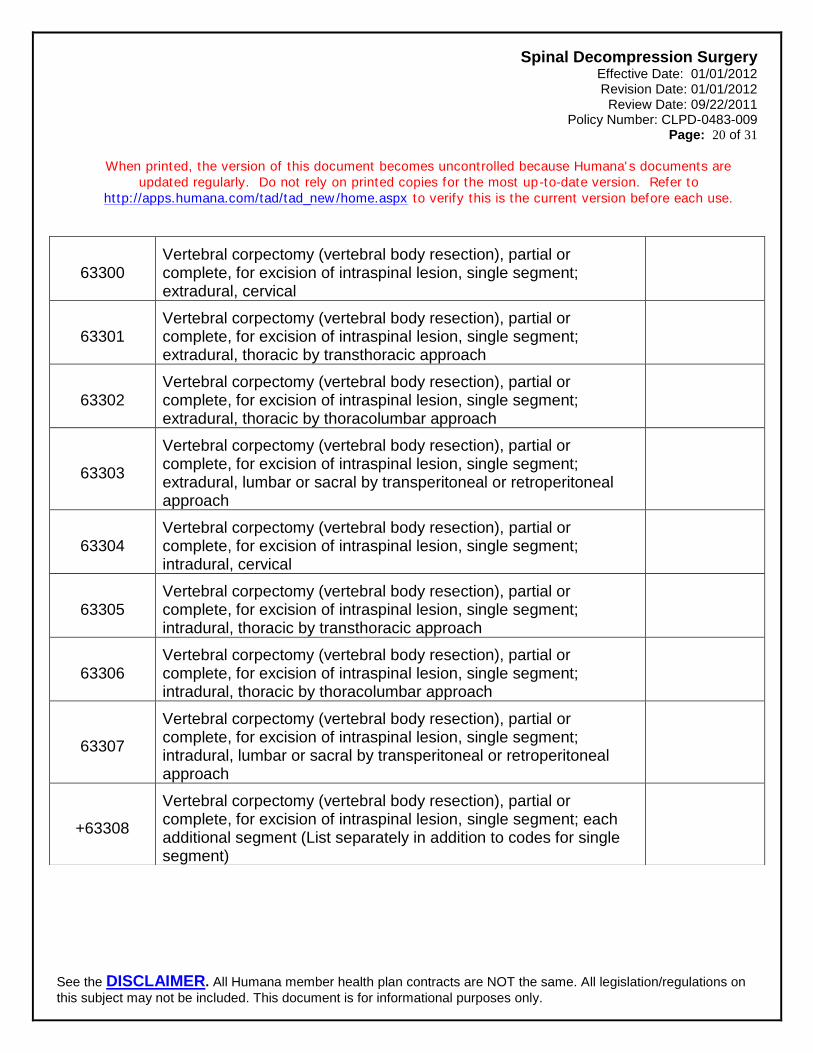
63300 Vertebral corpectomy (vertebral body resection), partial or complete, for excision of intraspinal lesion, single segment; extradural, cervical
63301 Vertebral corpectomy (vertebral body resection), partial or complete, for excision of intraspinal lesion, single segment; extradural, thoracic by transthoracic approach
63302 Vertebral corpectomy (vertebral body resection), partial or complete, for excision of intraspinal lesion, single segment; extradural, thoracic by thoracolumbar approach
63303
Vertebral corpectomy (vertebral body resection), partial or complete, for excision of intraspinal lesion, single segment; extradural, lumbar or sacral by transperitoneal or retroperitoneal approach
63304 Vertebral corpectomy (vertebral body resection), partial or complete, for excision of intraspinal lesion, single segment; intradural, cervical
63305 Vertebral corpectomy (vertebral body resection), partial or complete, for excision of intraspinal lesion, single segment; intradural, thoracic by transthoracic approach
63306 Vertebral corpectomy (vertebral body resection), partial or complete, for excision of intraspinal lesion, single segment; intradural, thoracic by thoracolumbar approach
63307
Vertebral corpectomy (vertebral body resection), partial or complete, for excision of intraspinal lesion, single segment; intradural, lumbar or sacral by transperitoneal or retroperitoneal approach
+63308
Vertebral corpectomy (vertebral body resection), partial or complete, for excision of intraspinal lesion, single segment; each additional segment (List separately in addition to codes for single segment)
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 21 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
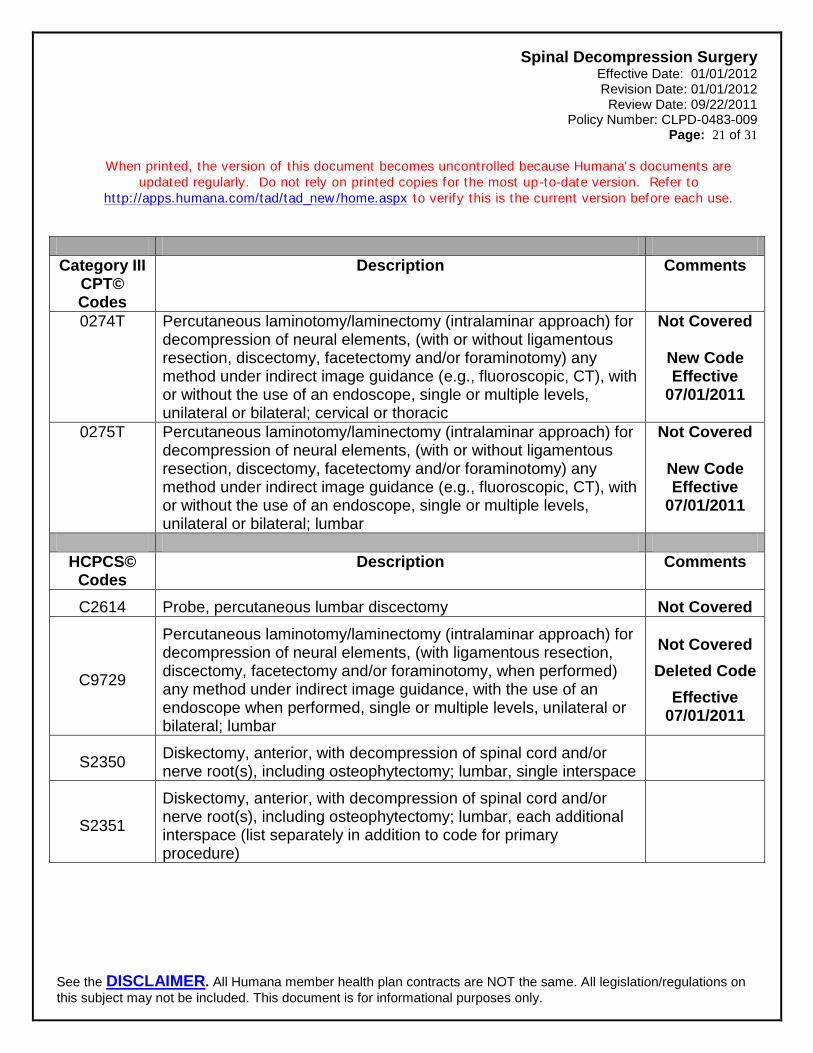
Category III CPT© Codes
Description Comments
0274T Percutaneous laminotomy/laminectomy (intralaminar approach) for decompression of neural elements, (with or without ligamentous resection, discectomy, facetectomy and/or foraminotomy) any method under indirect image guidance (e.g., fluoroscopic, CT), with or without the use of an endoscope, single or multiple levels, unilateral or bilateral; cervical or thoracic
Not Covered
New Code Effective
07/01/2011
0275T Percutaneous laminotomy/laminectomy (intralaminar approach) for decompression of neural elements, (with or without ligamentous resection, discectomy, facetectomy and/or foraminotomy) any method under indirect image guidance (e.g., fluoroscopic, CT), with or without the use of an endoscope, single or multiple levels, unilateral or bilateral; lumbar
Not Covered
New Code Effective
07/01/2011
HCPCS© Codes
Description Comments
C2614 Probe, percutaneous lumbar discectomy Not Covered
C9729
Percutaneous laminotomy/laminectomy (intralaminar approach) for decompression of neural elements, (with ligamentous resection, discectomy, facetectomy and/or foraminotomy, when performed) any method under indirect image guidance, with the use of an endoscope when performed, single or multiple levels, unilateral or bilateral; lumbar
Not Covered
Deleted Code
Effective 07/01/2011
S2350 Diskectomy, anterior, with decompression of spinal cord and/or nerve root(s), including osteophytectomy; lumbar, single interspace
S2351
Diskectomy, anterior, with decompression of spinal cord and/or nerve root(s), including osteophytectomy; lumbar, each additional interspace (list separately in addition to code for primary procedure)
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 22 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Medical Terms
Anesthetic - Medication used before or during surgery or a medical procedure that prevents pain from being felt, or provides decreased consciousness. Annulus - The outer ring of a vertebral disc. Anterior - Front of the body. Arthritis - Inflammation of a joint, which causes pain, swelling, and stiffness. Bilateral - Occurring on or affecting both sides of the body. Cannula - A small flexible tube inserted into the body, often for draining off fluid, delivery of medication, or to provide a pathway for surgical instruments. Cervical - Describes the upper spine (neck) area. Chronic - Persisting over a long period of time or marked by frequent recurrence. Computed Tomography (CT) Scan - Special radiographic technique that uses a computer to assimilate multiple X-ray images into a two-dimensional cross-
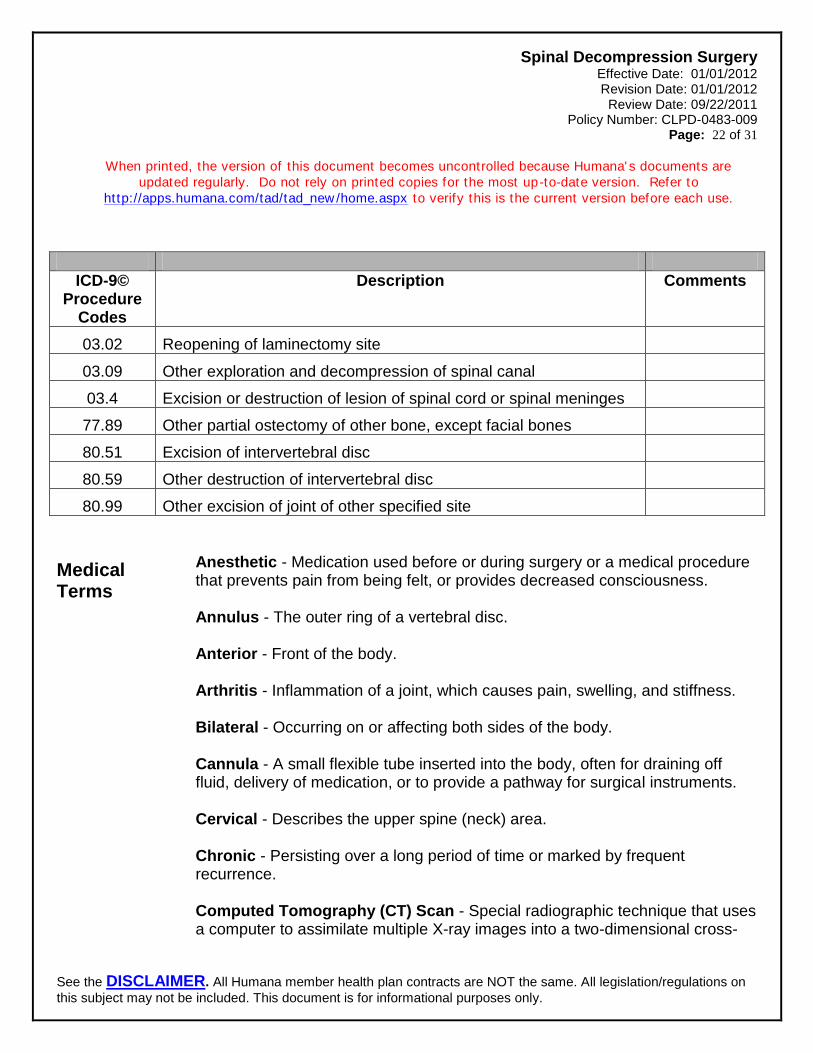
ICD-9© Procedure
Codes
Description Comments
03.02 Reopening of laminectomy site
03.09 Other exploration and decompression of spinal canal
03.4 Excision or destruction of lesion of spinal cord or spinal meninges
77.89 Other partial ostectomy of other bone, except facial bones
80.51 Excision of intervertebral disc
80.59 Other destruction of intervertebral disc
80.99 Other excision of joint of other specified site
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 23 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
sectional image. Distal - Located away from the center of the body. Dysfunction - A disturbance, impairment or abnormality of the functioning of an organ. Epidural Steroid Injection - An injection of a steroid into the epidural space (space where spinal fluid circulates around the spinal cord) to help relieve spinal pain that may be caused by pressure on a spinal nerve root. Excise - Surgical removal of tissue or a body part. Extremity - Lower or upper limb, such as the leg or arm. Facet - Small, smooth area on a bone or other hard surface. Foramen - An opening, a hole or passageway in a bone for blood vessels or nerves. Fluoroscopy - Procedure that utilizes an imaging device (X-ray) to view structures in the body in real time, or “live,” rather than waiting for film to be developed and interpreted. Herniated Disc - Also known as a “slipped disc,” is a rupture of the inner part of the disc into the spinal canal. Hoffmann Sign - Used to assess patients with symptoms of myelopathy. The test is done by quickly snapping or flicking the patient's middle fingernail. The test is positive for spinal cord compression when the tip of the index finger, ring finger, and/or thumb suddenly flex in response. Hyperreflexia - Exaggerated response of the deep tendon reflexes, usually resulting from injury to the central nervous system or metabolic disease. Incontinence - Involuntary loss of bladder or bowel. Lamina - Thin plate, sheet, or layer.
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 24 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Laparoscope - A thin, tube-like instrument with a light and lens for viewing; it may also have a tool to remove tissue or perform other types of surgery. Lateral - Refers to movement to the side. Ligament - Fibrous connective tissue at a joint that connects one bone to another. Lumbar - Lower section of the spine (the low back). Magnetic Resonance Imaging (MRI) - Special imaging technique that is utilized to image internal structures of the body; utilizes high powered magnetic fields rather than X-rays to produce the images. Myelogram - Diagnostic test that injects radiographic contrast media (dye) into the area surrounding the spinal cord and nerves; is used to diagnose disorders of the spinal canal and cord, such as nerve compression. Myelopathy - A disturbance of the spinal cord that results in loss of sensation and mobility; most commonly caused by spinal stenosis, which is a progressive narrowing of the spinal canal. Nerve Root - One of thirty-one pairs of nerves that come off each side of the spinal cord. Neurological - Related to the nervous system. Nucleus Pulposus - The jelly-like substance in the center of a spinal disc. Ossification - Condition of being altered into a hard bony substance. Percutaneous - A surgery or procedure done percutaneously is to access the organs or tissue via a needle puncture of the skin, rather than an “open” approach made by a scalpel. Physical Therapy - Treatment of physical dysfunction or injury by therapeutic exercise and the application of modalities, intended to restore or facilitate normal function or development. Posterior - Toward the back of the body.
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 25 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Posterior Longitudinal Ligament - A ligament that binds the vertebrae and vertebral disks together into a columnar unit. Radiculopathy - Irritation and inflammation of a spinal nerve root, resulting in pain, muscle weakness, and/or numbness and tingling. Renaissance™ System - A robotic guidance system, which is a designed to increase surgical safety and accuracy of spinal procedures by using image-based planning and guided instrumentation to guide the surgeon to the exact location. Rheumatoid Arthritis - A type of arthritis that affects the lining of the joints, resulting in hot, painful, swollen and deformed joints; the body’s immune system attacks the joints; long term it can affect the internal organs. Sacral - Refers to the sacrum, which is the triangular shaped bone at the base of the spine. Saddle Anesthesia - Decreased sensation (feeling) to the buttocks, perineum, and inner surfaces of the thighs. Spinal Fusion - Surgery to connect (graft) the spinal bones together to prevent movement and relieve pain. Thoracic - Used to describe the middle section of the spine or the chest region. Trauma - An injury. Vertebrae - One of the 33 bones in the cervical, thoracic and lumbar regions that make up the spinal column.
References
California Technology Assessment Forum (CTAF) Website. Percutaneous laser disc decompression for treatment of lumbar disc prolapse. June 18, 2008. Available at: http://www.ctaf.org. Accessed September 6, 2011. Chopko B, Caraway D. MiDAS I (mild® decompression alternative to open surgery): a preliminary report of a prospective, multi-center clinical study. Pain Physician. 2010; 13:369-378.
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 26 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Chou R, Loeser J, Owens D, et al. Interventional therapies, surgery, and interdisciplinary rehabilitation for low back pain - an evidence-based clinical practice guideline from the American Pain Society. Spine. 2009; 34:1066-1077. Deer T, Kapural L. New image-guided ultra-minimally invasive lumbar decompression method: the mild® procedure. Pain Physician. 2010; 13:35-41. ECRI Institute. Custom Hotline Response. Laser discectomy for the treatment of herniated lumbar discs. March 8, 2011. Available at: https://www.ecri.org. Accessed August 26, 2011. ECRI Institute. Custom Hotline Response. Surgical devices for annulus fibrosus repair after spinal surgery. December 2, 2010. Available at: https://www.ecri.org. Accessed August 26, 2011. ECRI Institute. Custom Hotline Response (ARCHIVED). Surgical decompression procedures for degenerative spinal stenosis and spondylolisthesis. November 20, 2009. Available at: https://www.ecri.org. Accessed August 26, 2011. ECRI Institute. Custom Hotline Response (ARCHIVED). Percutaneous cervical discectomy for disc herniation. January 30, 2009. Available at: https://www.ecri.org. Accessed August 26, 2011. ECRI Institute. Emerging Technology Report. Percutaneous disc decompression for cervical disc herniation. December 28, 2009. Available at: https://www.ecri.org. Accessed August 26, 2011. ECRI Institute. Evidence Report. Laser discectomy for the treatment of herniated lumbar discs. December 2004. Available at: https://www.ecri.org. Accessed August 26, 2011. ECRI Institute. Health Technology Forecast. Spinal stenosis. September 10, 2009. Available at: https://www.ecri.org. Accessed August 26, 2011. Erginousakis D, Filippiadis D, Malagari A, et al. Comparative prospective randomized study comparing conservative treatment and percutaneous disk decompression for treatment of intervertebral disk herniation. Radiology. 2011; 260:487-493.
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 27 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Hayes, Winifred S. Directory Report (ARCHIVED). Automated percutaneous lumbar discectomy. May 10, 2010. Available at: http://www.hayesinc.com. Accessed August 26, 2011. Hayes, Winifred S. Health Technology Brief. Endoscopic laser-assisted discectomy for cervical disc herniation. March 1, 2011. Available at: http://www.hayesinc.com. Accessed August 26, 2011. Hayes, Winifred S. Health Technology Brief. Laminotomy for lumbar spinal stenosis. December 3, 2010. Available at: http://www.hayesinc.com. Accessed August 26, 2011. Hayes, Winifred S. Health Technology Brief (ARCHIVED). Arthroscopic microdiscectomy for lumbar disc herniation. June 17, 2009. Available at: http://www.hayesinc.com. Accessed August 26, 2011. Hayes, Winfred S. News Service. Surgical treatment of spinal stenosis yields more benefit than nonsurgical alternatives. February 24, 2008. Available at: http://www.hayesinc.com. Accessed August 26, 2011. Hayes, Winifred S. News Service. Trends in surgical procedures in treating spinal stenosis in older patients. April 22, 2010. Available at: http://www.hayesinc.com. Accessed August 26, 2011. Hayes, Winifred S. Search and Summary. Arthroscopic microdiscectomy for lumbar disc herniation. August 4, 2011. Available at: http://www.hayesinc.com. Accessed August 26, 2011 Hayes, Winifred S. Search and Summary. Laminotomy (hemilaminectomy) for spinal stenosis. August 12, 2010. Available at: http://www.hayesinc.com. Accessed August 26, 2011. Hayes, Winifred S. Search and Summary (ARCHIVED). Minimally invasive lumbar decompression (mild®; Vertos Medical Inc.) for lumbar spinal stenosis. March 2, 2010. Available at: http://www.hayesinc.com. Accessed August 26, 2011.
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 28 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
Institute for Clinical and Economic Review (ICER) Website. Management options for patients with low back disorders. June 24, 2011. Available at: http://www.icer-review.org. Accessed September 6, 2011. Institute for Clinical Systems Improvement Website. Health care guideline: adult low back pain. Fourteenth Edition. November 2010. Available at: http://www.icsi.org. Accessed September 6, 2011. Manchikanti L, Boswell M, Singh V, et al. Comprehensive evidence-based guidelines for interventional techniques in the management of chronic spinal pain. American Society of Interventional Pain Physicians (ASIPP). Pain Physician. 2009; 12: 699-802. Milliman Care Guidelines® 15th Edition. Automated percutaneous diskectomy (APLD), low back pain. Available at: http://cgi.careguidelines.com/login-careweb.htm. Accessed September 6, 2011. Milliman Care Guidelines® 15th Edition. Cervical diskectomy or microdiskectomy, foraminotomy, laminotomy. Available at: http://cgi.careguidelines.com/login-careweb.htm. Accessed September 6, 2011. Milliman Care Guidelines® 15th Edition. Cervical laminectomy. Available at: http://cgi.careguidelines.com/login-careweb.htm. Accessed September 6, 2011. Milliman Care Guidelines® 15th Edition. Lumbar diskectomy, foraminotomy, or laminotomy. Available at: http://cgi.careguidelines.com/login-careweb.htm. Accessed September 6, 2011. Milliman Care Guidelines® 15th Edition. Lumbar laminectomy. Available at: http://cgi.careguidelines.com/login-careweb.htm. Accessed September 6, 2011. National Guideline Clearinghouse Website. American Association of Neurological Surgeons (AANS). Cervical laminoforaminotomy for the treatment of cervical degenerative radiculopathy. August 2009. Available at: http://www.guideline.gov. Accessed September 6, 2011.
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 29 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
National Guideline Clearinghouse Website. American Association of Neurological Surgeons (AANS). Cervical surgical techniques for the treatment of cervical spondylotic myelopathy. August 2009. Available at: http://www.guideline.gov. Accessed September 6, 2011. National Guideline Clearinghouse Website. American Association of Neurological Surgeons (AANS). Techniques for anterior cervical decompression for radiculopathy. August 2009. Available at: http://www.guideline.gov. Accessed September 6, 2011. National Guideline Clearinghouse Website. American College of Occupational and Environmental Medicine (ACOEM). Occupational medicine practice guidelines: evaluation and management of common health problems and functional recovery in workers: low back disorders. 2007. Available at: http://www.guideline.gov. Accessed September 6, 2011. National Guideline Clearinghouse Website. Washington State Department of Labor Industries. Work-related acute cauda equina syndrome (CES) diagnosis and treatment. August 2009. Available at: http://www.guideline.gov. Accessed September 6, 2011. National Guideline Clearinghouse Website. Work Loss Data Institute (WLDI). Low back – lumbar & thoracic (acute & chronic). 2011. Available at: http://www.guideline.gov. Accessed September 6, 2011. National Guideline Clearinghouse Website. Work Loss Data Institute (WLDI). Neck and upper back (acute & chronic). 2011. Available at: http://www.guideline.gov. Accessed September 6, 2011. National Institute for Clinical Excellence (NICE) Website. Automated percutaneous mechanical lumbar discectomy. November 2005. Available at: http://www.nice.org.uk. Accessed September 6, 2011. National Institute for Clinical Excellence (NICE) Website. Endoscopic laser foraminoplasty. December 2003. Available at: http://www.nice.org.uk. Accessed September 6, 2011. National Institute for Clinical Excellence (NICE) Website. Percutaneous endoscopic laser cervical discectomy. June 2009. Available at: http://www.nice.org.uk. Accessed September 6, 2011.
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 30 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
National Institute for Clinical Excellence (NICE) Website. Percutaneous endoscopic laser lumbar discectomy. May 2009. Available at: http://www.nice.org.uk. Accessed September 6, 2011. National Institute for Clinical Excellence (NICE) Website. Percutaneous endoscopic laser thoracic discectomy. May 2004. Available at: http://www.nice.org.uk. Accessed September 6, 2011. North American Spine Society (NASS) Website. Evidence-based clinical guidelines for multidisciplinary spine care – diagnosis and treatment of cervical radiculopathy from degenerative disorders. 2010. Available at: http://www.spine.org. Accessed September 6, 2011. North American Spine Society (NASS) Website. Evidence-based clinical guidelines for multidisciplinary spine care – diagnosis and treatment of degenerative lumbar spondylolisthesis. 2008. Available at: http://www.spine.org. Accessed September 6, 2011. North American Spine Society (NASS) Website. Evidence-based clinical guidelines for multidisciplinary spine care – diagnosis and treatment of degenerative lumbar stenosis. January 2007. Available at: http://www.spine.org. Accessed September 6, 2011. UpToDate® Website. Cervical spondylotic myelopathy. May 2011. Available at: https://www.uptodate.com/home/index.html. Accessed September 6, 2011. UpToDate® Website. Lumbar spinal stenosis: treatments and prognosis. June 9, 2011. Available at: https://www.uptodate.com/home/index.html. Accessed September 6, 2011. UpToDate® Website. Lumbosacral radiculopathy: prognosis and treatment. May 2011. Available at: https://www.uptodate.com/home/index.html. Accessed September 6, 2011. UpToDate® Website. Subacute and chronic low back pain: surgical treatment. May 2011. Available at: https://www.uptodate.com/home/index.html. Accessed September 6, 2011.
Spinal Decompression Surgery Effective Date: 01/01/2012
Revision Date: 01/01/2012 Review Date: 09/22/2011
Policy Number: CLPD-0483-009 Page: 31 of 31
When printed, the version of this document becomes uncontrolled because Humana' s documents are
updated regularly. Do not rely on printed copies for the most up-to-date version. Refer to
http://apps.humana.com/tad/tad_new /home.aspx to verify this is the current version before each use.
See the DISCLAIMER. All Humana member health plan contracts are NOT the same. All legislation/regulations on
this subject may not be included. This document is for informational purposes only.
UpToDate® Website. Treatment of cervical radiculopathy. May 2011. Available at: https://www.uptodate.com/home/index.html. Accessed September 6, 2011. Washington State Department of Labor and Industries Website. Medical treatment guidelines. Review criteria for cervical surgery for entrapment of a single nerve root. June 2004. Available at: http://www.lni.wa.gov/.
Washington State Department of Labor and Industries Website. Medical treatment guidelines. Review criteria for entrapment of a single lumbar nerve root. March 1992. Available at: http://www.lni.wa.gov/.