Embed Size (px)
Citation preview
Speech Language-Pathology and the Professional Voice: An Overview
What does the SLP do?Does not provide special training: range, power,
control, stamina, esthetic qualityAnalyze Systematically the Vocal
Behaviors:Perceptual & Objective MeasuresAnalyze Vocational, Educationally, &
Psychosocial Factors of Vocal BehaviorsDesign & Implement an Individualized Program
for Modifying Vocal Behavior
Who are Professional Voice Users?
Use the voice for artistic expression Professional Singers Actors/Actresses Those seeking to become professional
singers or actors Excluded for this talk: Teacher, lawyer,
clergy
Levels of Vocal Usage
Elite Vocal Performer (Level I)- slight aberration of voice may have dire consequences: singers and actors, opera singer
Professional Voice User (Level II)- moderate vocal problem might prevent adequate job performance: clergy, teachers, lecturers,etc.
Non-Vocal Professional (Level III)- severe vocal problem would prevent adequate job performance: lawyers, physicians, businessmen, business women, etc.
Non-Vocal Non-Professional (Level IV)- vocal quality is not a prerequisite for adequate job performance: clerks, laborers.
Levels of Vocal Usage
The Vocal Tract: 4 Components "Generator”- breath support provided by the lungs. "Vibrator”- the larynx; specifically, the vocal folds
themselves.
"Resonator”- the space above the larynx, and includes most of the pharynx. (trained opera singer-produce resonance at 2,500 Hz).
"Articulator”-the tongue, lips, cheeks, teeth, and palate. Shapes sound from below into words and vocal gestures.
Anatomy & Physiology: Larynx
Laryngeal Cartilage's
Intrinsic & Extrinsic laryngeal Muscles
Vocal Fold Vibration: Speaking &
Singing
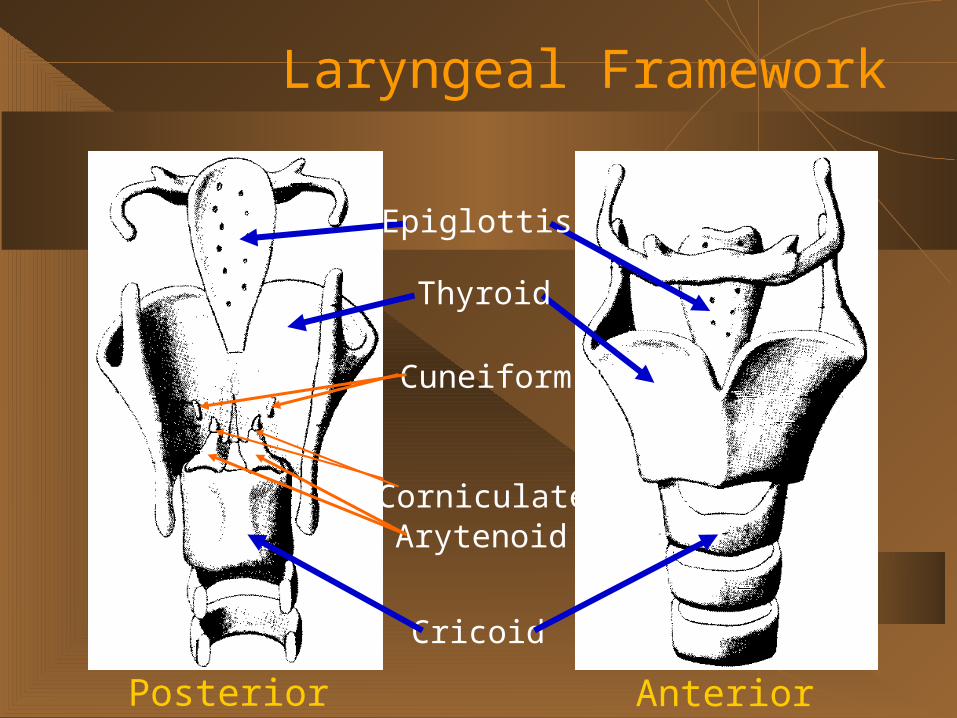
Laryngeal Framework
Posterior Anterior
Cricoid
Corniculate
Cuneiform
Arytenoid
Thyroid
Epiglottis
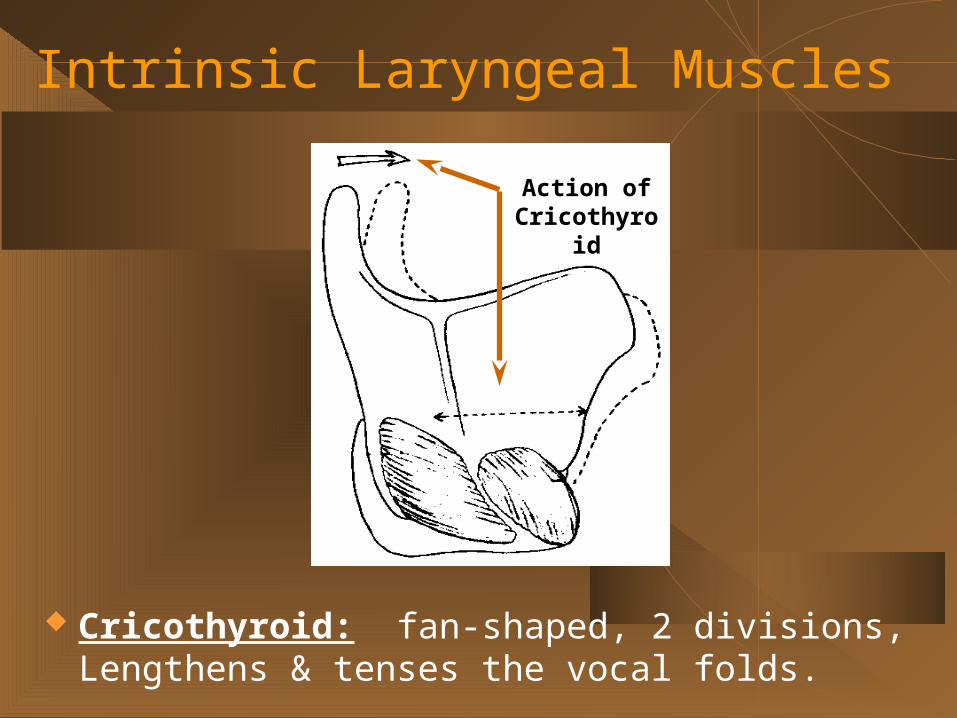
Intrinsic Laryngeal Muscles
Cricothyroid: fan-shaped, 2 divisions, Lengthens & tenses the vocal folds.
Action of Cricothyroid
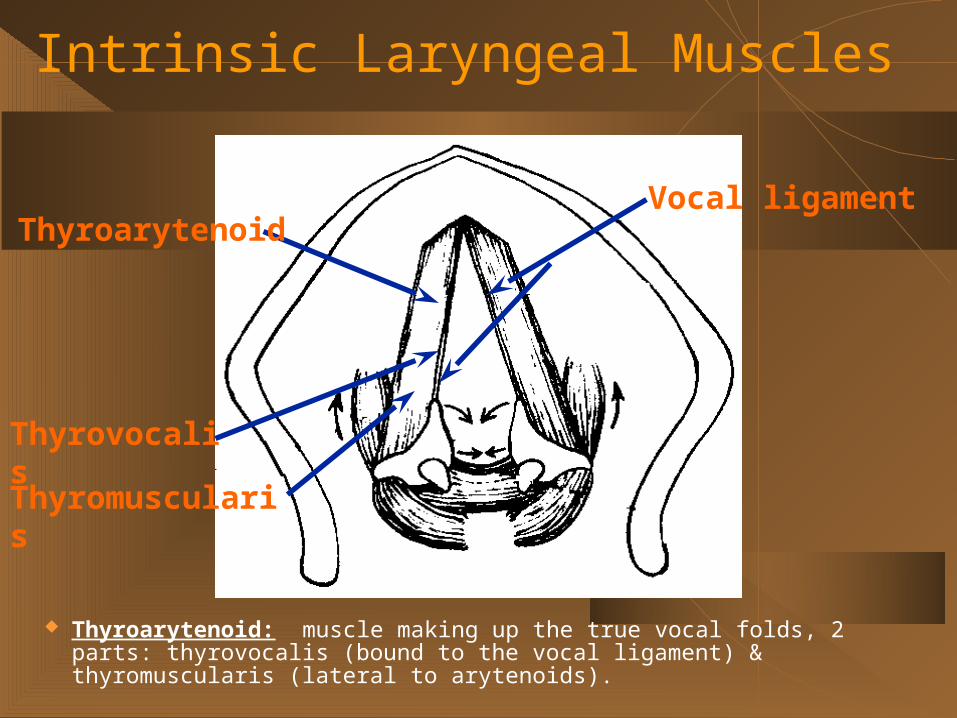
Intrinsic Laryngeal Muscles
Thyroarytenoid: muscle making up the true vocal folds, 2 parts: thyrovocalis (bound to the vocal ligament) & thyromuscularis (lateral to arytenoids).
ThyroarytenoidVocal ligament
Thyrovocalis
Thyromuscularis
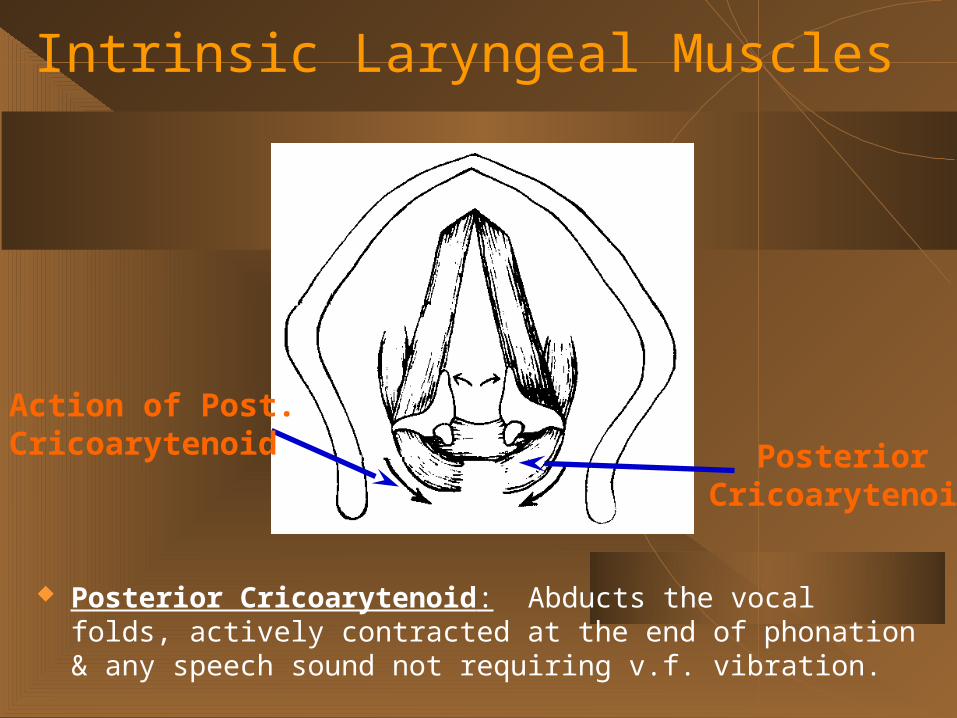
Intrinsic Laryngeal Muscles
Posterior Cricoarytenoid: Abducts the vocal folds, actively contracted at the end of phonation & any speech sound not requiring v.f. vibration.
PosteriorCricoarytenoid
Action of Post.Cricoarytenoid
Intrinsic Laryngeal Muscles
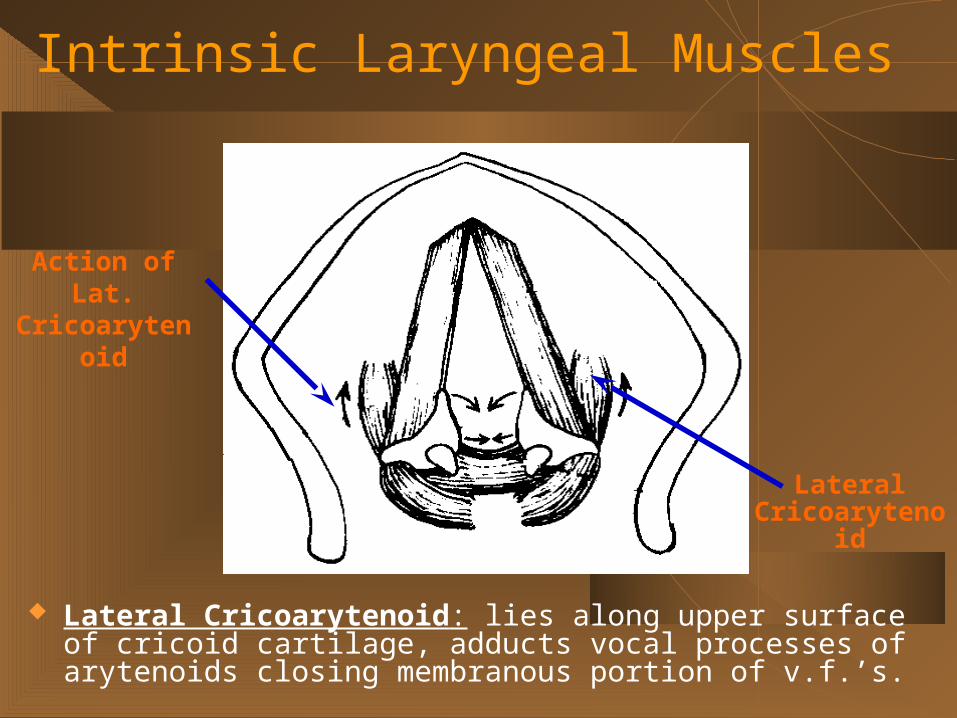
Lateral Cricoarytenoid: lies along upper surface of cricoid cartilage, adducts vocal processes of arytenoids closing membranous portion of v.f.’s.
Action of Lat.Cricoarytenoi
d
LateralCricoarytenoid
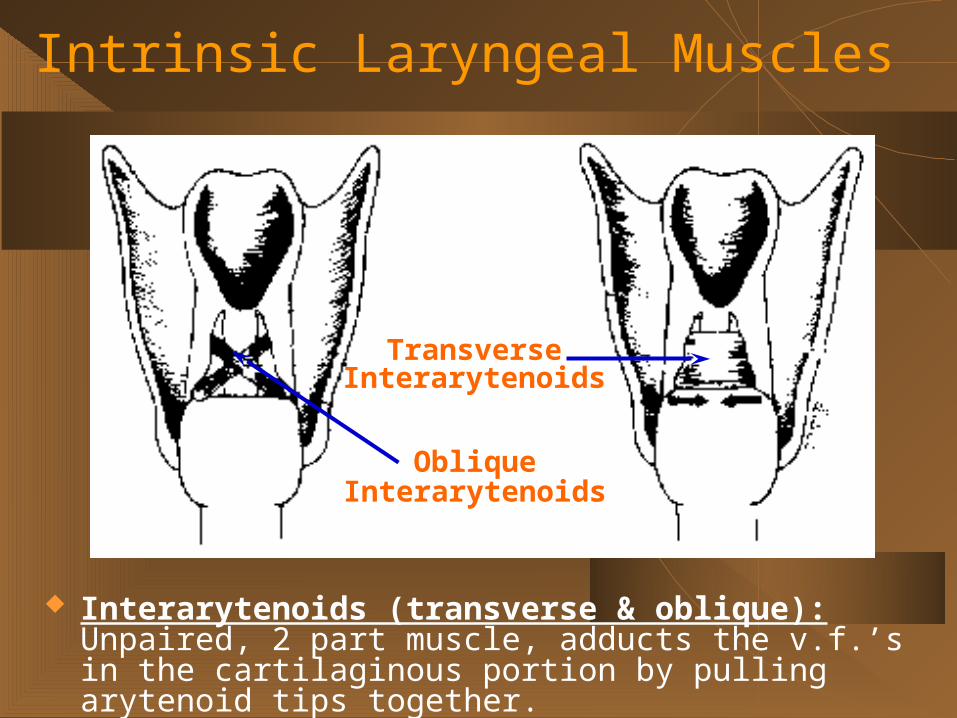
Interarytenoids (transverse & oblique): Unpaired, 2 part muscle, adducts the v.f.’s in the cartilaginous portion by pulling arytenoid tips together.
ObliqueInterarytenoids
TransverseInterarytenoids
Intrinsic Laryngeal Muscles

Extrinsic Laryngeal Muscles
Mastoid Tip
Mylohyoid
Hyoid Bone
Sternohyoid
Omohyoid
Sternum
Mandible
AnteriorDigastric
PosteriorDigastric
Stylohyoid
Thyrohyoid
Sternothyroid
Extrinsic Laryngeal Muscles
Three Main Purposes:
1) Fixation
2) Elevation
3) Depression Two major groups-
Suprahyoid & Infrahyoid Suprahyoid- one of the above
attachments lies above the larynx. Infrahyoid- one of the attachments lies
below the larynx.
Vocal Fold Vibration Vibratory cycle- single vibration of the vocal folds (or
glottal cycle)
“Begins when subglottal pressure (Ps ) overpowers
fold resistance just enough for the v.f.’s to first blow open.”
Opening phase: v.f. continue to blow apart
Closing phase: escape of air reduces Ps enough for
fold resistance to overpower airflow, then close.
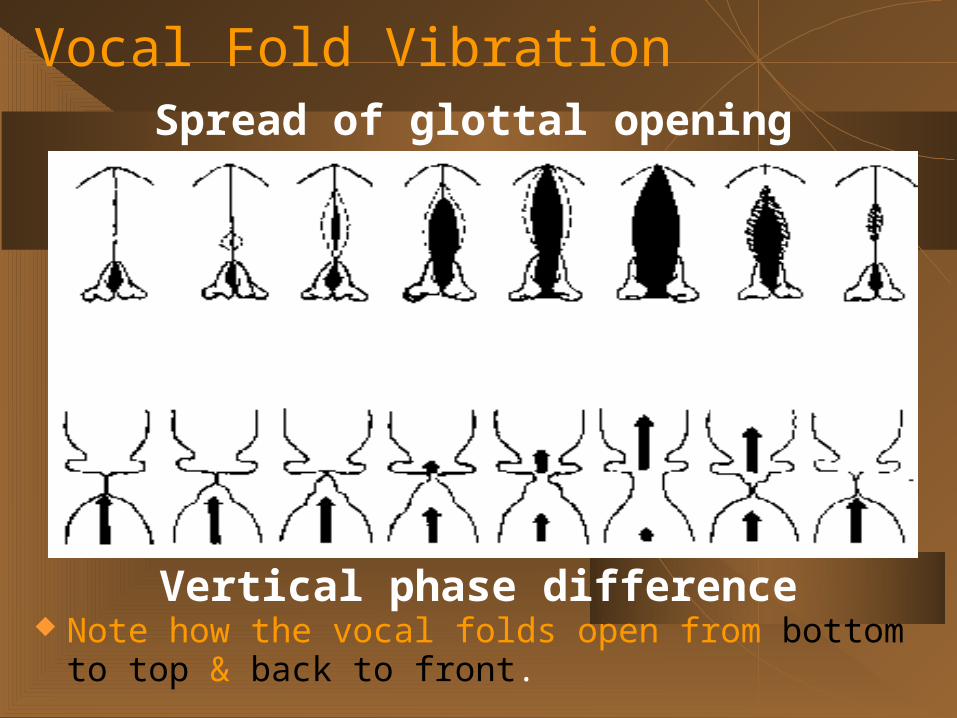
Vocal Fold Vibration
Note how the vocal folds open from bottom to top & back to front.
Spread of glottal opening
Vertical phase difference
Spread of glottal opening
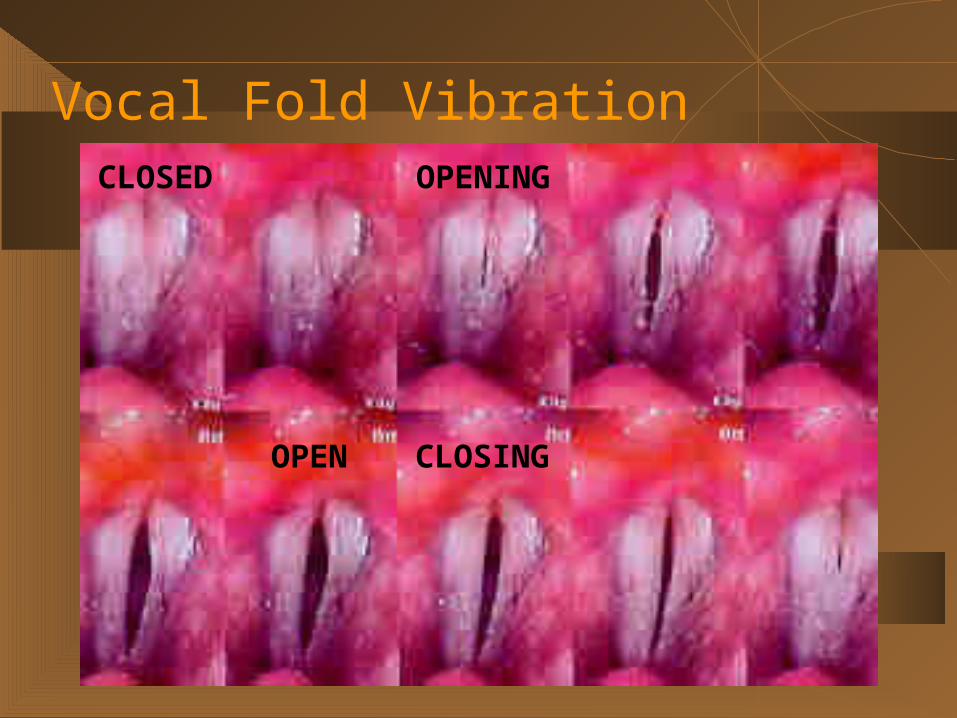
Vocal Fold Vibration
OPEN
CLOSED OPENING
CLOSING

Normal Vocal Folds
1.
2. 3. 4.
Vocal Abuse & Misuse
Hyperfunctional singing or speaking habits
Voice history taken to determine
speaking/singing patterns
Vocal techniques to reduce hyperfunctional
voice are discussed
Vocal Abuse & Misuse: Singing
Excessive muscle tension in tongue, neck, larynx Inadequate abdominal support Excessive volume Inadequate preparation
limited practice rehearsal of a difficult piece limited vocal training for a given role
Don’t go beyond your physical limits!
Vocal Abuse & Misuse: Speaking
Disassociation with speaking & singing voice is a common
abuse!
Support, muscular control, projection not applied to
speaking voice
Shouting, screaming (backstage, noisy rooms)
Conducting-Choral (Practice singing all parts)
Teaching singing (Long days, seated)
Vocal Abuse & Misuse: Speaking Loud talking, yelling, screaming Hard glottal attack Outside acceptable physiologic range Excessive coughing/throat clearing Grunting (lifting, exercising) Excessive talking Loud, hard laughing Voice production when folds are inflammed
Vocal Abuse & Misuse: Exposure
Alcohol consumption
Medications
Caffeine
Recreational drugs
Smoke
Reflux
Vocal Abuse & Misuse: Symptoms
Hoarseness
Vocal fatigue
Reduced range of phonation
Breathiness
Strain/Struggle voice
Disorders of Singing: Upper Respiratory Infection
Symptoms- Mucosal congestion Increased nasal secretions Nasal obstruction Pharyngitis Fever causing dehydration Productive or unproductive cough
Disorders of Singing: Upper Respiratory Infection Medications
Be knowledgeable about “over the counter remedies”
Avoid antihistamine (dry & thicken secretions) Early infection only Tefenadine & Astemizole (non sedating)
Mucolytic agents & decongestants give greatest relief
Sleepiness & anxiety
Avoid aspirin May cause vocal fold hemorrhage with coughing
Other therapies: Increase fluid intake
Those that don’t increase mucous production Nasal irrigation's
Thins secretions (saline) Singing only if no cord inflammation
Disorders of Singing: Upper Respiratory Infection
Disorders of Singing: Laryngitis URI may cause mucosal edema Voice rest considered Practice for short periods of time
Few brief rather than one long session Singing- Narrow pitch range Other vocalizations minimized or avoided No whispering or whistling
Gargling no help Steam inhalation is beneficial-
Decreases inflammations & reduces secretions
Performance during laryngitis Limit pitch range & volume
Disorders of Singing: Laryngitis

Laryngitis/ Edema
Disorders of Singing: Vocal Fold Hemorrhage
Can occur with URI, laryngitis or coughing Vocal abuse- Single episode of shouting etc. Women- Onset of menstrual cycle Strict vocal rest
Fibrosed tissue Frequent episodes- Prominent superficial blood
vessels Laser treatment
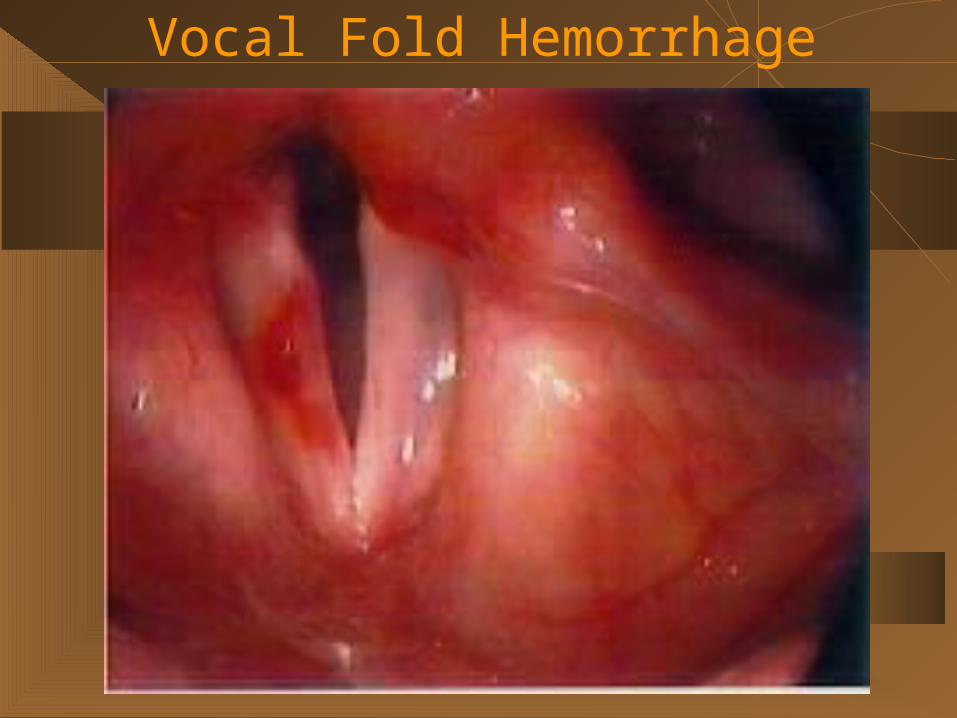
Vocal Fold Hemorrhage
Disorders of Singing: Vocal Fold Polyp Typically unilateral Anterior middle one-third of fold Broad based or sessile May cause mild-severe dysphonia Caused by misuse or abuse, smoking
(cigarettes or marijuana (worse)
Typical complaints: Harsh quality Diplophonia Loss of upper range
Therapy: Resolve with voice therapy Surgery-polypoidectomy
Disorders of Singing: Vocal Fold Polyp
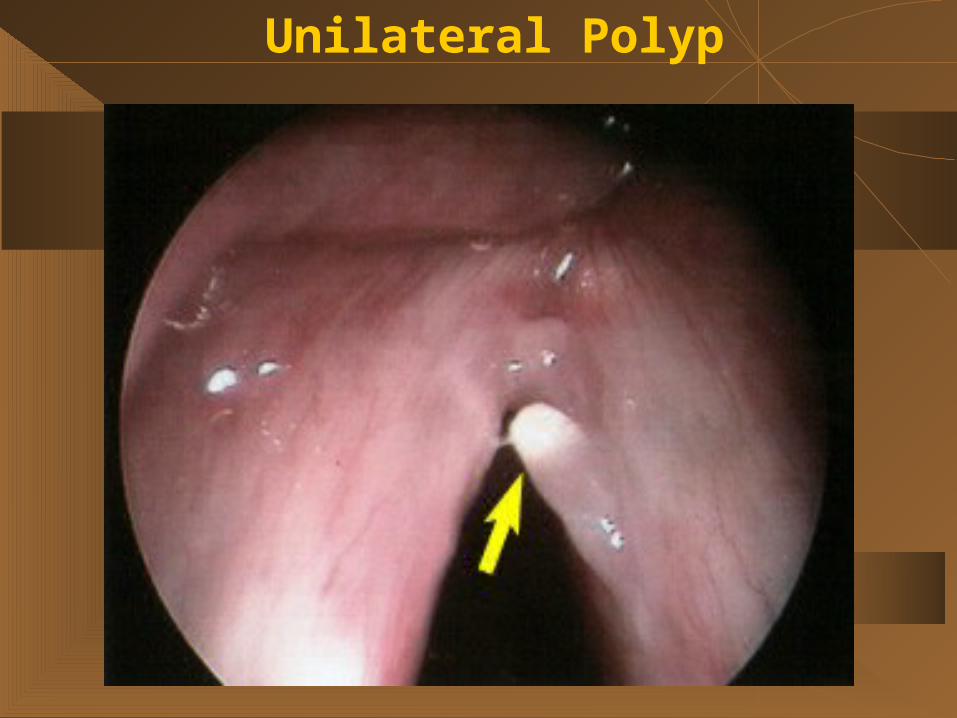
Unilateral Polyp
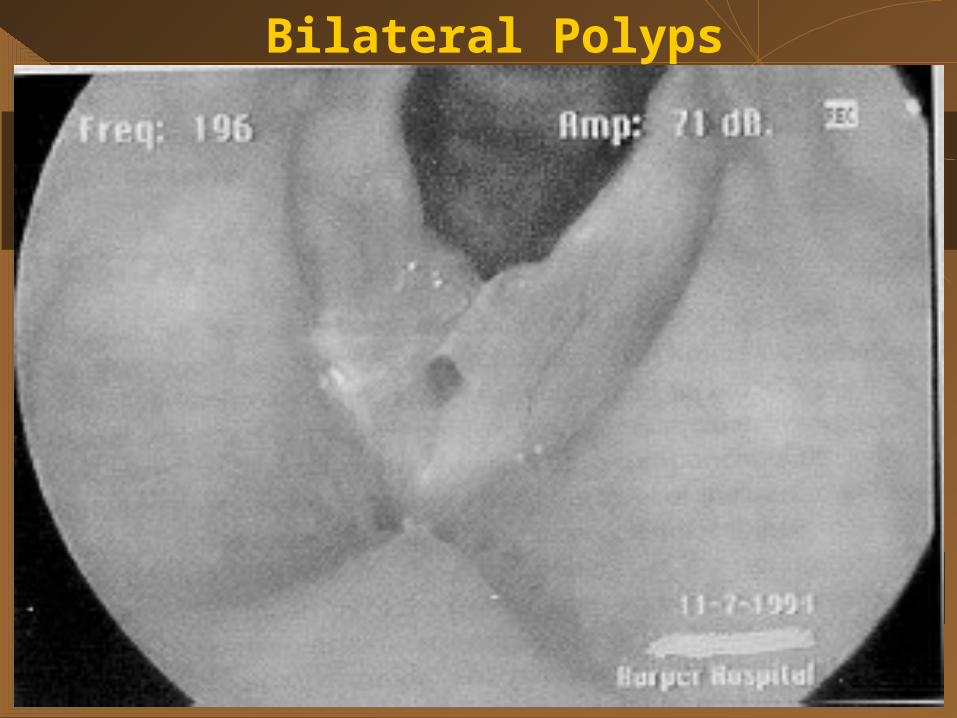
Bilateral Polyps
Disorders of Singing: Vocal Nodules Caused by overuse and abuse
Singing outside range Nonsinging activities (most often)
SpeakingJob environmentPlaying musical instrumentConductingTeaching
Other vocal abuses: Environment
NoiseSmokeDustPoorly ventilationLack of proper humidityPoor acoustics
Disorders of Singing: Vocal Nodules
Symptoms- Harsh, hoarse or breathy voice Loss of upper range
Treatment- 6-12 weeks of behavioral therapy If persist-surgery
Microlaryngeal- NO laser
Disorders of Singing: Vocal Nodules

Bilateral Singer’s Nodules
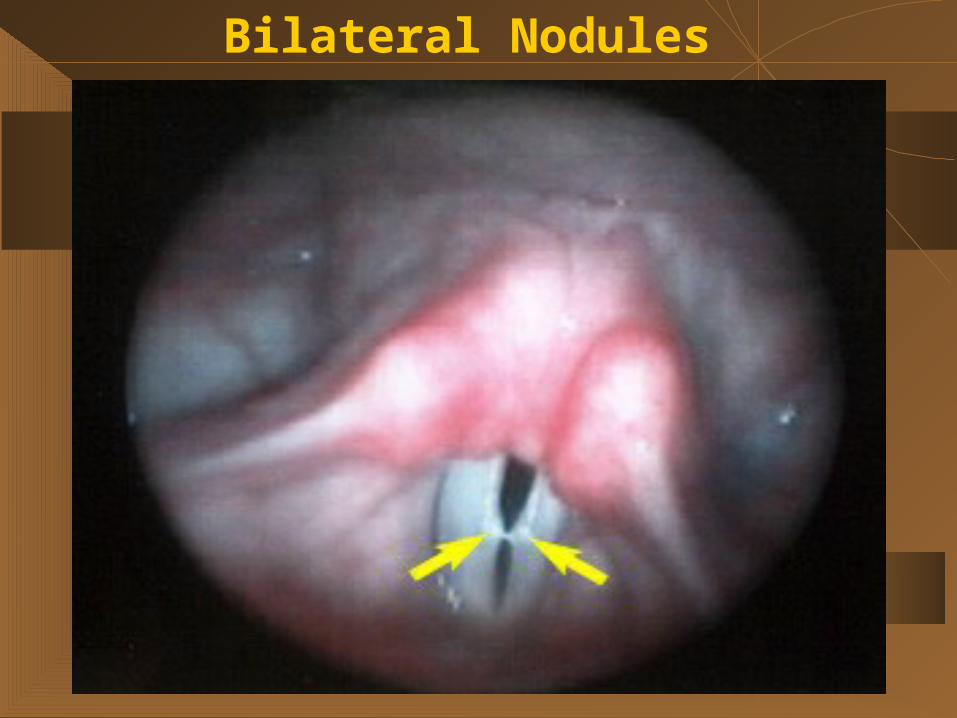
Bilateral Nodules
Prevalence of Disorder
Who Gets Voice Disorders?
45% are level I and II professional vocalists,
43% are level III and IV patients.
Remaining 12% are children
Disorders of Singing: Most Common Acute "emergencies":upper respiratory infection:
cold or stress-related.
Voice strain and/or extraesophageal reflux (the back flow of stomach contents).
Vocal abuse and misuse syndromes are common in professional voice
Disorders of Singing: Incidence Infectious and Inflammatory Conditions:
Laryngopharyngeal reflux (LPR)- 55%
Chronic tobacco use (smoking)- 25%
Upper respiratory infection- 15%
Vocal Misuse/Abuse Syndromes:
Muscle tension dysphonia(s)- 40%
Acute vocal abuse- 2%
Benign and Malignant Growths:
Reinke's edema- 16%
Vocal nodules- 8%
Granulomas- 7%
Papillomas- 4%
Carcinoma (Cancer)- 4%
Disorders of Singing: Incidence
Neuromuscular Disorders: Dystonia (spasmodic dysphonia)-8% Paralysis/paresis- 7% Degenerative conditions- 2%
Psychogenic Conditions: Conversion reactions- 2% Relapsing aphonia/dysphonia- 1%
Disorders of Singing: Incidence

10 Most Common Problems of Singers Poor Posture
Poor Breathing & Inappropriate Breath Support
Hard Glottal or "Aspirate" Attack
Poor Tone Quality
Limited Pitch Range, Difficulty in Register Transition
Lack of Flexibiltiy, Agility, Ease of Production, Endurance
Poor Articulation
Lack of Discipline, Commitment, Compliance
Poor Vocal Health, Hygiene, Vocal Abuse
Poor Self-Image, Lack of Confidence
Disorders of Singing: Treatment Concerns Successful treatment of voice disorders
depends on identification of "vocal needs" of each patient.
patient's professional and social needs and obligations.
different impact patients depending upon the patient's profession or "level of vocal usage."
How to save your voice: Avoid Abuse
1) Do nothing to your voice resulting in hoarseness and/or throat pain.
2) Avoid yelling or screaming to the point of causing hoarseness.
3) Avoid singing so loudly that you develop hoarseness, and avoid singing in situations that you cannot hear yourself singing.
4) Cold or laryngitis: do not try to talk or sing "over" the problem.
1) Careful using "character voices" not to strain, and use especially good breath support.
2) Do not alter your "normal" speaking voice to create an effect; avoid pitching your voice too low.
3) Avoid taking on roles you cannot do; don't attempt roles that are out of your range.
4) Avoid using long run-on sentences and a rapid speaking rate; good breath support for speech is as important as good breath support for singing.
How to save your voice: Avoid Misuse
How to save your voice: Avoid overuse
1) Examine your "vocal schedule" carefully. Your vocal demands are not of equal importance.
2) Avoid making a schedule that leaves no room for rest and recovery.
3) Use amplification when available and appropriate, especially for rehearsals.
How to save your voice: Monitor your diet/ life style.
1) Eat regularly, and eat a healthy diet.
2) Avoid fried and other fatty foods.
3) Avoid dehydration: drink plenty of water.
4) Avoid eating or drinking, particularly alcoholic
beverages, within three hours of bedtime.
5) Minimize consumption of caffeine-containing foods
and beverages.
6) Strictly avoid smoking or other tobacco consumption
7) Exercise regularly; aerobic exercise is best.
How to save your voice: Avoid unnecessary medications.
1)Avoid drying medications such as antihistamines.
2) Avoid anesthetic throat sprays.
Warming-Up the Voice Allowing time to warm-up
Singers develop distinctive warm-up regimens appropriate to their
personal needs
Warm-up the entire body with gentle physical exercise (e.g., stretching,
yoga, Tai Chi).
Begin vocalizing in the comfortable mid-range of the voice, and
gradually work out to the higher and lower extremes of pitch.
Test vocal register transitions during the warm-up. Exercises that
"blend" the "chest" ("heavy” laryngeal adjustment) and "head" ("light"
laryngeal adjustment) registers eventually produce a smooth passaggio.
Cooling Down the Voice
"warm-down" by vocalizing on "oo," for example). Singer using a "belting" voice, it is helpful to sing
in the "head" register (or falsetto)-stretches the vocal cords and alleviates laryngeal
tension Re-loosening the articulatory muscles, Massaging the jaw- the masseter, neck &
shoulders particularly the trapezius
Case Study: Opera Singer 2 days prior to Opera- Arrives in Tennessee
from Germany In 24 hours- Blocking, informal and dress
rehearsal Complaint- Mild changes in mid -range; not
noticed by others
Case Study: Examination Laryngeal videoendostroboscopy- revealed
moderately large immature bilateral vocal fold nodules
Cause: Sung during a cold 2 weeks prior
Case Study: Therapy Elimination of all unnecessary vocal usage
No cast partiesMinimal conversation
Transposition to a lower key was not an option Reduction of dynamic markings of solo parts Techniques used for 3 days of performance-
followed by 2 weeks of reduced vocal usage Problem was resolved