Embed Size (px)
Citation preview

DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
httpwwwneurologyorgcontent83156fullhtmllocated on the World Wide Web at
The online version of this article along with updated information and services is
Neurology All rights reserved Print ISSN 0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright copy 2014 American Academy of
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology
Lidia MVR Moura MDMouhsin M Shafi MD
PhDMarcus Ng MDSandipan Pati MDSydney S Cash MD
PhDAndrew J Cole MDDaniel Brian Hoch MD
PhDEric S Rosenthal MDM Brandon Westover
MD PhD
Correspondence toDr Westovermwestovermghharvardedu
Supplemental dataat Neurologyorg
Spectrogram screening of adult EEGs issensitive and efficient
ABSTRACT
Objective Quantitatively evaluate whether screening with compressed spectral arrays (CSAs) is apractical and time-effective protocol for assisting expert review of continuous EEG (cEEG) stud-ies in hospitalized adults
Methods Three neurophysiologists reviewed the reported findings of the first 30 minutes of 118cEEGs then used CSA to guide subsequent review (ldquoCSA-guided reviewrdquo protocol) Reviewersviewed 120 seconds of raw EEG data surrounding suspicious CSA segments The same neuro-physiologists performed independent page-by-page visual interpretation (ldquoconventional reviewrdquo)of all cEEGs Independent conventional review by 2 additional more experienced neurophysiol-ogists served as a gold standard We compared review times and detection rates for seizures andother pathologic patterns relative to conventional review
Results A total of 2092 hours of cEEG data were reviewed Average times to review 24 hours ofcEEG data were 8 (64) minutes for CSA-guided review vs 38 (617) minutes for conventionalreview (p 0005) Studies containing seizures required longer review 10 (64) minutes for CSA-guided review vs 44 (620) minutes for conventional review (p 0005) CSA-guided review wassensitive for seizures (873) periodic epileptiform discharges (100) rhythmic delta activity(971) focal slowing (987) generalized slowing (100) and epileptiform discharges(885)
Conclusions CSA-guided review reduces cEEG review time by 78 with minimal loss of sensi-tivity compared with conventional review
Classification of evidence This study provides Class IV evidence that screening of cEEG withCSAs efficiently and accurately identifies seizures and other EEG abnormalities as comparedwith standard cEEG visual interpretation Neurologyreg 20148356ndash64
GLOSSARYcEEG 5 continuous EEG CSA 5 compressed spectral array ESE 5 electrographic status epilepticus MGH 5 Massachu-setts General Hospital
Many studies have shown that nonconvulsive seizures are common in critically ill patients1211
Consequently there has recently been a marked increase in the use of continuous EEG (cEEG)monitoring12ndash15 cEEG findings are often dynamic and have immediate management implica-tions thus requiring frequent review Quantitative EEG tools are increasingly used to expeditedata review particularly in centers with large monitoring volumes1617 In particular compressedspectral arrays (CSAs spectrograms) display 2 to 8 hours of cEEG in a single color map whichmay allow electroencephalographers (EEGers) to screen long periods quickly to determinewhich segments require further direct review of the primary EEG data Furthermore certainEEG features such as voltage asymmetries abrupt changes such as movement artifacts andseizures gradual trends in background activity1819 and changes in patterns of recurrent cyclicseizures may be easily recognized using CSA20
Despite increasingly widespread clinical adoption the empirical performance of CSA-basedcEEG review has received little rigorous study We hypothesized that the time required for
From the Department of Neurology (LMVRM MN SP SSC AJC DBH ESR MBW) Epilepsy Service Massachusetts GeneralHospital Boston and Department of Neurology (MMS) Division of Epilepsy Beth Israel Deaconess Medical Center Boston MA
Go to Neurologyorg for full disclosures Funding information and disclosures deemed relevant by the authors if any are provided at the end of the article
56 copy 2014 American Academy of Neurology
expert review of selected segments of rawcEEG data when guided by CSA-based screen-ing is less than that required for conventionalreview of the entire raw cEEG without mean-ingfully compromising sensitivity for seizuresor other critical findings
METHODS Level of evidence The aim of this Class IV evi-
dence study was to determine whether screening of cEEG with
CSA efficiently and accurately identifies seizures and other
EEG abnormalities as compared with conventional unaided
visual interpretation
Study design We conducted a retrospective review of critical
care cEEGs and medical records at the Massachusetts General
Hospital (MGH) between September 2011 and February 2012
(figures e-1 and e-2 on the Neurologyreg Web site at Neurologyorg)
All cEEGs were ordered by treating physicians (rather than as part of a
protocol) and all cEEGs included were performed for the purpose of
seizure surveillance in acutely ill patients
Patient cohort Among 370 consecutive patients monitored
between September 2011 and February 2012 118 patients met
the following inclusion criteria (1) older than 18 years of age
(2) duration $8 hours (3) admitted for an acute illness (rather
than electively) and (4) the primary indication for ordering cEEG
was a suspicion for seizures Demographic and other clinical
information was obtained from the electronic medical record
General cEEG data review protocol The CSA review group
was composed of 3 EEGers at the fellowship stage of clinical EEG
subspecialty training (readers AndashC) but with at least 6 months of
cEEG experience The same records were also independently
reviewed by the same EEGers (readers AndashC) and 2 attending
clinical neurophysiologists (readers D and E) using conventional
page-by-page visual analysis The findings of the readers at the
attending level served as the ldquogold standardrdquo while the
conventional review by readers AndashC allowed for comparison of
time to review All readers used CSA in daily clinical practice and
were trained in American Clinical Neurophysiology Societyrsquos
intensive care unit cEEG terminology21 Readers A B and C
reviewed 44 37 and 37 cEEGs using the CSA protocol and
66 44 and 8 cEEGs using conventional review respectively
Reviewers D and E reviewed 58 and 60 EEGs respectively
using conventional review For cEEGs lasting 24 hours only
the first 24 hours were reviewed
Detailed descriptions of the CSA-guided and conventional
visual (gold standard) cEEG review protocols technical details
of cEEG recordings and configuration of CSA displays and rea-
sons for selecting CSA over alternative quantitative EEG methods
are provided in the online supplemental material (sections A and
B) An example of the CSA display is provided in figure 1
Statistical analysis for primary aim The primary outcome
measures of this study were time taken for readers AndashC to review
each cEEG study using the CSA-guided cEEG review protocol
compared with conventional page-by-page EEG review and
detection sensitivity for seizures The significance of differences
in review times between the methods of cEEG review was assessed
using a paired t test
Statistical analysis for secondary aims Detection sensitivity
for seizures periodic epileptiform discharges nonperiodic epi-
leptiform discharges focal slowing generalized slowing and
rhythmic delta activity were calculated for reviewers AndashC using
CSA-guided cEEG review relative to the findings of the gold
standard reviewers D and E who relied on conventional page-
by-page EEG review In addition we analyzed detection
sensitivity for electrographic status epilepticus (ESE) For this
study ESE was said to be present when either (1) the maximum
seizure duration (max duration) was 5 minutes or (2)
the minimum average interseizure interval within any hour of
monitoring was 5 minutes ESE was said to have been
ldquodetectedrdquo by CSA-guided review when either all seizures
lasting 5 minutes were detected or when 50 of all
seizures were detected (for cases in which all seizures were
briefer than 5 minutes) otherwise ESE was considered to
have been ldquomissedrdquo
The relationship between review time (per 24 hours of cEEG
recording) and seizure detection sensitivity using CSA-guided
review was assessed using Spearman correlation analysis Calcula-
tions and graphs were generated using Microsoft Excel and Stata
The relation between total seizure burden and percentage of seiz-
ures missed was assessed using a Pearson correlation coefficient
and a t test was used to compare the mean percentages of missed
seizures (for cases lacking status epilepticus) in cases with seizures
with brief vs longer average durations
Standard protocol approvals registrations and patientconsents This retrospective study was conducted under a protocol
approved by the MGH institutional review board Informed consent
was not required
RESULTS Demographic and clinical data for the118 selected patients are summarized in table e-1The 118 cEEGs included 40 with seizures and com-prised a total of 2092 hours of cEEG data and 1192seizures Among the 40 cases with seizures 475(1940) met study criteria for ESE either by havingone or more seizures lasting 5 minutes (74 ofcases [1419]) or by having an average hourly inter-seizure interval5 minutes in duration (25 of cases[519]) (table 1)
Table e-2 summarizes the time-savings analysisThe time required for review of intermittent rawcEEG guided by CSA was substantially less than forconventional complete review of the entire cEEGwithout CSA guidance Average times to review 24hours of cEEG data were 8 (64) minutes for CSA-guided review and 38 (617) minutes for conven-tional review (p 0005) Significant time savingswere also found considering only studies containingseizures (adjusted for 24 hours) 10 (64) minutes forCSA-guided review and 44 (620) minutes for con-ventional review (p 0005) (figure 2)
CSA-guided cEEG review identified all patientswith seizures and detected 873 of all individual seiz-ures among the cohort That is reviewers detected atleast one seizure in every record that contained seizures(as determined by gold-standard conventional EEGreview by readers D and E) however in records withmultiple electrographic seizures some seizures weremissed by CSA-guided review The overall sensitivityof CSA-guided review (figure 3) was as follows seizures873 (10411192) periodic epileptiform discharges
Neurology 83 July 1 2014 57
100 (4343) rhythmic delta activity 971 (3435)focal slowing 987 (7677) generalized slowing100 (100100) and epileptiform discharges 885(6170) No cases of ESE went undetected by CSA-guided review (table 1) all seizures lasting5 minuteswere detected and in cases of ESE without any seizureslasting 5 minutes the lowest seizure detection ratewas 86 (95111)
Excluding cases with ESE due to prolonged (5-minute) seizures (of which all were detected seeabove) we found an inverse relationship betweennumber of seizures per cEEG and number of missedseizures (more seizures were missed in EEGs withhigher total seizure counts Pearson correlation coef-ficient 073 p 5 00001) In addition dividing the21 cases without ESE into cases with brief (averageduration 1 minute) vs longer seizures we foundthat the mean percentage of missed seizures was twiceas high in the group with brief seizures 13 (SD 22)vs 65 (SD 12) respectively (t test p 5 001)
Differences in detection rates for seizures andother patterns between readers in the CSA-guidedreview group were modest and not clinically signifi-cant (table e-3) A detailed discussion of differencesbetween detection performance characteristics among
reviewers A B and C in the CSA-guided reviewgroup is provided in the online supplemental material(section C) An example of the CSA display obscuredby artifact is provided in figure 4
There was no significant correlation between sei-zure detection sensitivity (CSA protocol) and timeto review 24 hours of cEEG (Spearman r R2 [40]013 p 5 041) suggesting that CSA-guided re-viewers adjusted review time on a case-by-case basisto maintain sensitivity In addition linear regressionof the time to review each file as a function of theordering in which cEEG was reviewed by a particularreader revealed no significant trend suggesting thatthe time to review a cEEG study was stable for eachreader throughout the study
DISCUSSION The main finding of this study is thatCSA-based screening of cEEG recordings inhospitalized adults can substantially reduce averagereview time without significantly sacrificingsensitivity for seizures and other critical findingsrelative to conventional page-by-page review CSA-guided screening identified 100 of cEEGrecordings containing seizures all cases of ESE andtended to miss seizures only in records with
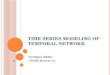
Figure 1 CSA display
Top screen Two-hour segments of CSA power data were displayed from top to bottom in a spectrogrammontage There arebrief periods with increased power in the high-frequency band over the left hemisphere highlighting suspicious regions Bot-tom screen Raw cEEG data cEEG 5 continuous EEG CSA 5 compressed spectral array
58 Neurology 83 July 1 2014
Table 1 Descriptive statistics for patients with seizures
Patient No of seizures No detected Detected No missed Missed Min duration Mean duration Max duration Max rate Min ISI Max ESE present ESE detected
1 1 1 100 0 0 05 05 05 1 mdash 1
2 1 1 100 0 0 9408 9408 9408 1 mdash 100 X X
3 1 1 100 0 0 21 21 21 1 mdash 4
4 1 1 100 0 0 18 18 18 1 mdash 3
5 1 1 100 0 0 184 184 184 1 mdash 31 X X
6 1 1 100 0 0 22 22 22 1 mdash 4
7 1 1 100 0 0 03 03 03 1 mdash 1
8 2 2 100 0 0 100 124 147 1 900 25 X X
9 2 2 100 0 0 05 06 06 1 1200 1
10 3 2 67 1 33 11 11 19 1 350 0
11 3 1 33 2 67 02 04 10 1 620 1
12 3 3 100 0 0 03 19 35 2 300 6
13 3 3 100 0 0 04 04 05 1 700 1
14 3 3 100 0 0 01 01 134 1 50 3 X X
15 4 3 75 1 25 03 04 05 3 200 3
16 8 8 100 0 0 08 13 18 4 150 11
17 9 6 67 3 33 06 41 71 1 660 12 X X
18 10 10 100 0 0 03 04 09 9 67 7
19 14 11 79 3 21 07 06 111 3 200 100 X X
20 14 14 100 0 0 04 22 89 7 86 15 X X
21 20 12 60 8 40 10 1123 9124 4 150 100 X X
22 23 22 96 1 4 04 17 73 6 100 16 X X
23 25 15 60 10 40 05 05 27 7 86 1
24 28 27 96 1 4 04 06 07 2 300 2
25 28 20 71 8 29 09 22 22 3 200 4
26 29 14 48 15 52 04 20 68 5 120 29 X X
27 30 28 93 2 7 25 48 69 3 200 31 X X
28 33 33 100 0 0 02 04 07 6 100 2
29 37 36 97 1 3 10 12 14 4 150 4
30 46 46 100 0 0 10 19 19 5 120 3
31 47 47 100 0 0 08 11 15 5 120 2
32 48 48 100 0 0 01 02 02 25 24 1 X X
Continued
Neurology
83
July12
014
59
multiple seizures attaining an overall detection rate of87 in 25 of the time required for conventionalreview This finding was established in a largecollection of unselected recordings from patientswith a broad range of neurologic conditionsMoreover the cEEG review procedure was clinicallypractical Our data suggest that CSA-guided reviewis an acceptable alternative to the current standardpractice of page-by-page review of all data for cEEGmonitoring in critically ill adults
In the minority of cases in which CSA-guidedreview missed seizures misses tended to represent asmall fraction of a high seizure burden Missed seiz-ures also tended to occur more often in patients withbriefer seizures We speculate that misses can be ex-plained in part by the intrinsic difficulty of drawinga line between patterns on the ldquoictal-interictal contin-uumrdquo and ldquodefinite seizuresrdquo Efforts to increase in-terrater agreement on seizure patterns may furtherimprove performance of CSA-guided review
Our findings in adults are similar to those ofsmaller studies in pediatric populations1820 Onestudy using CSA and amplitude-integrated EEG in23 pediatric cEEGs (17 with seizures 10 without)found a sensitivity for seizure detection with CSA of83320 Another study in 8 neonates (26ndash44weeks) found that envelope trends enabled experi-enced users to detect 88 of prolonged seizureswhile detection rates for brief or slowly evolvingneonatal seizures were only 40 and 2022 sug-gesting that compressed EEG may be useful in somebut not all neonates In contrast with the presentstudy in both of these pediatric studies reviewerswere not permitted to correlate compressed datafindings with the primary EEG data This differencemay have contributed to lower detection sensitivitiesrelative to the present study
The present study investigated sensitivity and effi-ciency (time savings) of CSA as to guide cEEGreview placing minimal emphasis on specificity(low false-positive detection rates) This choicetreats CSA as a screening tool which cannot be per-formed without simultaneous review of raw cEEGdata rather than as a primary modality for cEEGinterpretation Suspicious CSA patterns must befrequently correlated with raw EEG data to distin-guish seizures from state changes periodic patternsand artifacts This back-and-forth dynamic allowscEEG review to be adaptive such that after an ini-tial careful correlation of raw cEEG with CSA pat-terns (including a careful visual analysis of thecEEG background) during the initial 30-minuteperiod reviewers are able to rapidly distinguishartifacts from true physiologic changes This initialreview enables subsequent review to proceed morequickly
Tab
le1
Con
tinu
ed
Pat
ient
No
ofse
izur
esNo
det
ecte
dDet
ecte
d
No
misse
dMisse
d
Min
dur
ation
Mea
ndur
ation
Max
dur
ation
Max
rate
Min
ISI
Max
ESE
pre
sent
ESE
det
ecte
d
33
53
52
98
12
02
40
154
12
50
27
XX
34
54
52
96
24
01
03
06
30
20
2X
X
35
57
20
35
37
65
02
86
2921
35
17
100
XX
36
76
74
97
23
15
25
34
16
38
13
XX
37
99
95
96
44
00
44
436
30
20
84
XX
38
111
95
86
16
14
02
07
30
19
32
15
XX
39
121
104
86
17
14
02
05
11
2242
2
40
151
132
87
19
13
01
13
29
21
29
21
XX
Abb
reviations
ESE
5elec
trog
raph
icstatus
epile
pticus
ISI5
interseizu
reinterval
Min
duration
5minim
umse
izure
duration
(inminutes
)max
duration
5max
imum
seizure
duration
(inminutes
)max
rate
5max
imum
numbe
rof
seizures
that
occu
rred
during
any
hour
ofmon
itoring
min
ISI5
minim
umav
erag
eISIfor
anyho
urdu
ring
mon
itoring
define
das
theminim
umav
erag
edu
ration
betw
eenco
nsec
utivese
izures
withinan
yho
urof
mon
itoring(in
patien
tswith1se
izure)m
ax
5max
imum
percen
tage
ofan
yho
urdu
ring
mon
itoringthat
was
occu
pied
byse
izureac
tivityP
atientsareso
rted
bynu
mbe
rof
seizures
that
occu
rred
during
mon
itoring
Detec
ted
andmisse
d
give
thepe
rcen
tage
ofse
izures
detected
ormisse
dby
compr
esse
dsp
ectral
arrayndash
guided
review
protoc
ol(relativeto
thepa
ge-by-pa
gereview
gold
stan
dard
)For
this
stud
yapa
tien
twas
said
toha
veESE
ifeither
(1)t
hemax
imum
seizuredu
ration
was
5
minutes
or(2)t
heminim
umho
urly
averag
eISIw
as5
minutes
60 Neurology 83 July 1 2014
In keeping with a prior study by our group23
CSA-guided review had excellent sensitivity for thepresence of other common critical ldquointerictalrdquo find-ings including focal (987) and generalized (100)slowing periodic discharges (100) and rhythmicdelta activity (971) compared with conventionalpage-by-page EEG review Similarly sensitivity forthe presence of sporadic epileptiform discharges wasreasonably high (885) The high sensitivity fornonseizure findings is not necessarily because these
patterns produce distinct CSA signatures For exam-ple epileptiform discharges being brief typicallyshow no obvious footprint in the 2-hour CSA displayused in our protocol Rather these patterns are abun-dant enough to be detected even by very limitedreview of the primary EEG data that occurs duringCSA-guided review
The early stage of cEEG training of the CSAreview group merits comment This selection of read-ers was intended to reflect the practice at many ter-tiary care centers of relying on clinical fellows formost first-line cEEG interpretation The use of train-ees might produce conservative estimates of sensitiv-ity as sensitivity should improve with experienceBy contrast our gold-standard EEG reviewers wereexperienced attending-level clinical EEGers to ensurevalidity of the gold standard
Our protocol relied on 2-hour CSA windowsWe chose to display 5 CSA panels (left and right lat-eral and parasagittal chains and hemispheric asym-metry spectrogram) Including additional CSApanels higher time resolution (eg 30-minute win-dows) and possibly other compressed-data formats(eg amplitude integrated EEG rhythmicity meas-ures) might have produced higher seizure detectionrates However increasing data volume might com-promise efficiency by producing cognitive overloadFurther research is necessary to determine whichquantitative EEG instruments alone and in combi-nation present the best cognitive match for humanEEG reviewers
Some have suggested that nurses EEG technolo-gists and residents can be trained to review CSA datato flag regions for direct review by physician ex-perts2021 These efforts are important because cEEGpatterns in the acutely ill are dynamic and requireprompt action However nonexpert CSA-basedscreening (without immediate visual confirmation)may yield more false alarms which might place addi-tional burdens on neurophysiologists charged withfollowing up on such alerts In the current studyconstant correlation of CSA patterns with the under-lying EEG was critical in achieving high sensitivityand efficiency and direct visual confirmation by atrained expert remains an essential step to determin-ing which cEEG patterns are significant rather thanartifactual or incidental
Our results are subject to several limitationsFirst our study is a single-center retrospectivereview and a larger multi-institutional prospectivetrial is needed to establish the validity and general-izability of our findings Second CSA cannot escapethe inherent limitations of scalp EEG including thefact that not all seizures may be detectable on scalpEEG For example exquisitely focal seizures maybe detectable only with invasive monitoring and
Figure 2 Time-savings group analysis
Comparison histograms of the time taken to review a given record with the assistance ofCSA (blue bars) and without (red) (A) All studies reviewed by readers AndashC using CSA guid-ance vs conventional review (B) All studies that contained seizures Studies were rankordered from the shortest to longest review time The average time to review 24 hours ofcEEG data when CSA was used was 8 (64) minutes whereas conventional review took 38(617) minutes on average (A) These were statistically different between the groups (p
0005) (B) If seizures were present time savings was more marked CSA review 10(64) minutes and conventional 44 (620) minutes (p 0005) The figure is truncated at60 minutes For 14 studies reading with conventional review took more than 60 minutesTimes to review for these outliers were 622 623 635 636 637 646 652 660 673716 724 750 958 and 1016 in chart A and 958 750 724 716 673 652 646636 635 623 and 622 in chart B Times to review were normalized to a standard dura-tion of 24 hours of cEEG ie all reported times are expressed as time spent per 24 hours ofEEG data cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 61
seizure activity of low amplitude frequency orduration or seizures in the presence of ldquomalig-nantrdquo-appearing background activity may be diffi-cult to discern even on careful inspection of the rawcEEG Third while our results suggest that patternsmeeting the strict definition of definite electro-graphic seizures24 can be identified readily border-zone rhythmic and periodic EEG patterns failing toqualify as definite electrographic seizures may nev-ertheless be symptomatic and require treatment insome cases Determination of the clinical signifi-cance of such cases is possible only by clinical cor-relation eg to determine whether the pattern inquestion reliably correlates with signssymptomsand whether the patient improves with treatmentIn such cases CSA-guided review may not signifi-cantly reduce the total time required for interpreta-tion Fourth it should be emphasized that ourestimate of approximately 75 time savings appliesonly to the part of EEG review after careful directconventional visual analysis of the initial 30 minutesof data As stated above there are reasons to believethat the familiarity with the cEEG provided by thisinitial review is critical to both time savings andsensitivity of subsequent CSA-guided screeningFifth not all centers have access to software or read-ing stations such as those used to view CSA in thisstudy However such centers may be less likely toperform large-scale cEEG and may thus be betterable to review their studies without relying on CSA-based screening Sixth some centers employ dedi-cated technicians to monitor and screen for seizures
allowing physicians to focus only on suspicious seg-ments perhaps obviating the advantage (for physi-cians) of CSA-guided review Seventh some centersemploy screening of CSA (andor other measures)by nurses and electroneurodiagnostic technologistsfollowed by page-by-page EEG review by a physi-cian in fellowship training or another electroneur-odiagnostic technician followed by complete ortargeted review by an attending-level neurophysiol-ogist This approach of triple EEG review whiletime-consuming and resource-intensive is arguablythe least likely to miss any significant findingsFurther outcome-oriented research is needed todetermine the optimal approach among these alter-natives Eighth it must be emphasized that theCSA-guided review protocol proposed here is notintended as a substitute for visual review by trainedexpert clinicians and indeed expert visual review ofprimary cEEG data is an indispensable componentof the present CSA-guided protocol Lastly the re-sults of the present study apply only in the criticalcare setting They have no obvious direct relevanceto diagnostic long-term video EEG monitoring forassessment of chronic epilepsy particularly for thepresurgical workup In such patients interictalspikes may be infrequent but very clinically impor-tant necessitating careful time-consuming visualsearch and patients may undergo days of cEEGrecording to detect even a small number of seizureson which neurosurgical decisions are based In thissetting missing one seizure can have significantclinical consequences
Figure 3 Sensitivity analysis for seizures and other abnormal patterns
The overall sensitivity of CSA-guided review and conventional review of reviewers AndashC is shown relative to the gold-standard findings of readers D and E seizures 873 (10411192) PDs 100 (4343) RDA 971 (3435) FS987 (7677) GS 100 (100100) and EDs 885 (6170) By definition the gold-standard conventional review groupdetected 100 of all seizures and common abnormal patterns CSA 5 compressed spectral array ED 5 epileptiformdischarge FS 5 focal slowing GS 5 generalized slowing PD 5 periodic epileptiform discharge RDA 5 rhythmic deltaactivity
62 Neurology 83 July 1 2014
Finally it remains to be determined whether thetime savings achievable by CSA-guided review ismeaningful in either clinical or cost-effectivenessterms In many cases initial identification of EEGevents represents only one part of providing criticalcare cEEG services Other responsibilities whichmay be even more time-consuming include clinicalcorrelation of EEG findings including bedside exam-ination as needed to determine their significanceevaluation of changes in medications frequent com-munication with clinical teams to report findingsand to make EEG-related management recommenda-tions and writing EEG reports Nevertheless if vali-dated our results may justify replacing at least thefront-line conventional page-by-page EEG reviewarguably the most time-sensitive stage of EEG analy-sis by the more efficient CSA-based screening proce-dure presented herein
Our results suggest that CSA-guided cEEG reviewcan enable significantly faster interpretation withoutsubstantial loss of sensitivity for critical findings in thevast majority of cases While intensive care unit out-come measures were not explored in this study thedemonstration that CSA-guided review enables rapid
and accurate evaluation of critical EEG findings (suchas the presence of seizures or nonconvulsive status epi-lepticus) suggests that this protocol may positively affectpatient care by allowing more timely management de-cisions in response to critical cEEG events
AUTHOR CONTRIBUTIONSLMVRM MMS and MBW conceptualized and designed the study
LMVRM (MGH clinical neurophysiology fellow) and MBW (faculty
with the MGH Epilepsy Service) completed the statistical analysis LMV
RM MMS and MBW drafted the original manuscript LMVRM
SP and MN contributed to the data production and collection SSC
AJC DBH MMS ESR and MBW reviewed and revised the
manuscript
STUDY FUNDINGNo targeted funding reported
DISCLOSUREL Moura reports no disclosures relevant to the manuscript M Shafi
received support from Harvard Catalyst KL2 MeRIT program M Ng
and S Pati report no disclosures relevant to the manuscript S Cash
A Cole and D Hoch received support from NIHNeurological Disor-
ders and Stroke NS062092 E Rosenthal reports no disclosures relevant
to the manuscript M Westover received support from the American
Brain Foundation Go to Neurologyorg for full disclosures
Received May 22 2013 Accepted in final form March 25 2014
Figure 4 CSA display obscured by artifact
Top screen Two-hour segments of CSA display as described in figure 3 Bottom screen Raw cEEG data as described infigure 3 cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 63
REFERENCES1 Vespa PM Nuwer MR Juhaacutesz C et al Early detection of
vasospasm after acute subarachnoid hemorrhage using con-
tinuous EEG ICU monitoring Electroencephalogr Clin
Neurophysiol 1997103607ndash615
2 Schreiber JM Zelleke T Gaillard WD et al Continuous
video EEG for patients with acute encephalopathy in a
pediatric intensive care unit Neurocrit Care 201217
31ndash38
3 Pandian JD Cascino GD So EL et al Digital video-
electroencephalographic monitoring in the neurological-
neurosurgical intensive care unit Arch Neurol 200461
1090ndash1094
4 Cloostermans MC Van Meulen FB Eertman CJ et al
Continuous electroencephalography monitoring for early
prediction of neurological outcome in postanoxic patients
after cardiac arrest a prospective cohort study Crit Care
Med 2012402867ndash2875
5 Rudin D Grize L Schindler C et al High prevalence of
nonconvulsive and subtle status epilepticus in an ICU of a
tertiary care center a three-year observational cohort
study Epilepsy Res 201196140ndash150
6 Young GB Doig GS Continuous EEG monitoring in
comatose intensive care patients epileptiform activity in
etiologically distinct groups Neurocrit Care 200525ndash10
7 Young GB Continuous EEG monitoring in the ICU
Acta Neurol Scand 200611467ndash68
8 Claassen J Mayer SA Kowalski RG et al Detection of
electrographic seizures with continuous EEG monitoring
in critically ill patients Neurology 2004621743ndash1748
9 Vespa PM Nuwer MR Nenov V et al Increased inci-
dence and impact of nonconvulsive and convulsive seizures
after traumatic brain injury as detected by continuous elec-
troencephalographic monitoring J Neurosurg 199991
750ndash760
10 Towne AR Waterhouse EJ Boggs JG et al Prevalence of
nonconvulsive status epilepticus in comatose patients
Neurology 200054340ndash345
11 Talwar D Torres F Continuous electrophysiologic mon-
itoring of cerebral function in the pediatric intensive care
unit Pediatr Neurol 19884137ndash147
12 Claassen J Hirsch LJ Kreiter KT et al Quantitative con-
tinuous EEG for detecting delayed cerebral ischemia in
patients with poor-grade subarachnoid hemorrhage Clin
Neurophysiol 20041152699ndash2710
13 Carrera E Claassen J Oddo M et al Continuous electroen-
cephalographic monitoring in critically ill patients with central
nervous system infections Arch Neurol 2008651612ndash1618
14 Sutter R Fuhr P Grize L et al Continuous video-EEG
monitoring increases detection rate of nonconvulsive status
epilepticus in the ICU Epilepsia 201152453ndash457
15 Claassen J Hirsch LJ Frontera JA et al Prognostic sig-
nificance of continuous EEG monitoring in patients with
poor-grade subarachnoid hemorrhage Neurocrit Care
20064103ndash112
16 Nuwer MR Quantitative EEG analysis in clinical settings
Brain Topogr 19968201ndash208
17 Nuwer M Assessment of digital EEG quantitative EEG
and EEG brain mapping report of the American Academy
of Neurology and the American Clinical Neurophysiology
Society Neurology 199749277ndash292
18 Shah AK Agarwal R Carhuapoma JR Loeb JA Com-
pressed EEG pattern analysis for critically ill
neurological-neurosurgical patients Neurocrit Care
20065124ndash133
19 Bricolo A Turazzi S Faccioli F et al Clinical application
of compressed spectral array in long-term EEG monitoring
of comatose patients Electroencephalogr Clin Neurophy-
siol 197845211ndash225
20 Stewart CP Otsubo H Ochi A et al Seizure identification in
the ICU using quantitative EEG displays Neurology 2010
751501ndash1508
21 Hirsch LJ LaRoche SM Gaspard N et al American Clin-
ical Neurophysiology Societyrsquos Standardized Critical Care
EEG Terminology 2012 version J Clin Neurophysiol
2013301ndash27
22 Abend NS Dlugos D Herman S Neonatal seizure detec-
tion using multichannel display of envelope trend Epilep-
sia 200849349ndash352
23 Williamson CA Wahlster S Shafi MM Westover MB
Sensitivity of compressed spectral arrays for detecting seiz-
ures in acutely ill adults Neurocrit Care 20142032ndash39
24 Young GB Jordan KG Doig GS An assessment of non-
convulsive seizures in the intensive care unit using contin-
uous EEG monitoring an investigation of variables
associated with mortality Neurology 19964783ndash89
Free Michael J Fox DVD Video on Parkinsonrsquos DiseaseThe AAN and the American Brain Foundation present actor and Parkinsonrsquos disease patientMichael J Fox hosting Parkinsonrsquos Disease A Guide for Patients and Families This new patienteducation video is now available free to members and the public either on DVD or online Thefree DVD can be ordered while supplies last by visiting AANcomviewPatientEducationVideos orcalling (800) 879-1960 The video can be viewed online at YouTubecomAANChannel with otherpatient education DVDs produced by the AAN
64 Neurology 83 July 1 2014
DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
ServicesUpdated Information amp
httpwwwneurologyorgcontent83156fullhtmlincluding high resolution figures can be found at
Supplementary Material
00000000537DC1htmlhttpwwwneurologyorgcontentsuppl20140629WNL00000Supplementary material can be found at
References
httpwwwneurologyorgcontent83156fullhtmlref-list-1at This article cites 24 articles 5 of which you can access for free
Subspecialty Collections
httpwwwneurologyorgcgicollectionhealth_care_reformHealth care reform
reshttpwwwneurologyorgcgicollectioneeg_see_epilepsy-seizuEEG see EpilepsySeizures
httpwwwneurologyorgcgicollectioncritical_careCritical carefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

Lidia MVR Moura MDMouhsin M Shafi MD
PhDMarcus Ng MDSandipan Pati MDSydney S Cash MD
PhDAndrew J Cole MDDaniel Brian Hoch MD
PhDEric S Rosenthal MDM Brandon Westover
MD PhD
Correspondence toDr Westovermwestovermghharvardedu
Supplemental dataat Neurologyorg
Spectrogram screening of adult EEGs issensitive and efficient
ABSTRACT
Objective Quantitatively evaluate whether screening with compressed spectral arrays (CSAs) is apractical and time-effective protocol for assisting expert review of continuous EEG (cEEG) stud-ies in hospitalized adults
Methods Three neurophysiologists reviewed the reported findings of the first 30 minutes of 118cEEGs then used CSA to guide subsequent review (ldquoCSA-guided reviewrdquo protocol) Reviewersviewed 120 seconds of raw EEG data surrounding suspicious CSA segments The same neuro-physiologists performed independent page-by-page visual interpretation (ldquoconventional reviewrdquo)of all cEEGs Independent conventional review by 2 additional more experienced neurophysiol-ogists served as a gold standard We compared review times and detection rates for seizures andother pathologic patterns relative to conventional review
Results A total of 2092 hours of cEEG data were reviewed Average times to review 24 hours ofcEEG data were 8 (64) minutes for CSA-guided review vs 38 (617) minutes for conventionalreview (p 0005) Studies containing seizures required longer review 10 (64) minutes for CSA-guided review vs 44 (620) minutes for conventional review (p 0005) CSA-guided review wassensitive for seizures (873) periodic epileptiform discharges (100) rhythmic delta activity(971) focal slowing (987) generalized slowing (100) and epileptiform discharges(885)
Conclusions CSA-guided review reduces cEEG review time by 78 with minimal loss of sensi-tivity compared with conventional review
Classification of evidence This study provides Class IV evidence that screening of cEEG withCSAs efficiently and accurately identifies seizures and other EEG abnormalities as comparedwith standard cEEG visual interpretation Neurologyreg 20148356ndash64
GLOSSARYcEEG 5 continuous EEG CSA 5 compressed spectral array ESE 5 electrographic status epilepticus MGH 5 Massachu-setts General Hospital
Many studies have shown that nonconvulsive seizures are common in critically ill patients1211
Consequently there has recently been a marked increase in the use of continuous EEG (cEEG)monitoring12ndash15 cEEG findings are often dynamic and have immediate management implica-tions thus requiring frequent review Quantitative EEG tools are increasingly used to expeditedata review particularly in centers with large monitoring volumes1617 In particular compressedspectral arrays (CSAs spectrograms) display 2 to 8 hours of cEEG in a single color map whichmay allow electroencephalographers (EEGers) to screen long periods quickly to determinewhich segments require further direct review of the primary EEG data Furthermore certainEEG features such as voltage asymmetries abrupt changes such as movement artifacts andseizures gradual trends in background activity1819 and changes in patterns of recurrent cyclicseizures may be easily recognized using CSA20
Despite increasingly widespread clinical adoption the empirical performance of CSA-basedcEEG review has received little rigorous study We hypothesized that the time required for
From the Department of Neurology (LMVRM MN SP SSC AJC DBH ESR MBW) Epilepsy Service Massachusetts GeneralHospital Boston and Department of Neurology (MMS) Division of Epilepsy Beth Israel Deaconess Medical Center Boston MA
Go to Neurologyorg for full disclosures Funding information and disclosures deemed relevant by the authors if any are provided at the end of the article
56 copy 2014 American Academy of Neurology
expert review of selected segments of rawcEEG data when guided by CSA-based screen-ing is less than that required for conventionalreview of the entire raw cEEG without mean-ingfully compromising sensitivity for seizuresor other critical findings
METHODS Level of evidence The aim of this Class IV evi-
dence study was to determine whether screening of cEEG with
CSA efficiently and accurately identifies seizures and other
EEG abnormalities as compared with conventional unaided
visual interpretation
Study design We conducted a retrospective review of critical
care cEEGs and medical records at the Massachusetts General
Hospital (MGH) between September 2011 and February 2012
(figures e-1 and e-2 on the Neurologyreg Web site at Neurologyorg)
All cEEGs were ordered by treating physicians (rather than as part of a
protocol) and all cEEGs included were performed for the purpose of
seizure surveillance in acutely ill patients
Patient cohort Among 370 consecutive patients monitored
between September 2011 and February 2012 118 patients met
the following inclusion criteria (1) older than 18 years of age
(2) duration $8 hours (3) admitted for an acute illness (rather
than electively) and (4) the primary indication for ordering cEEG
was a suspicion for seizures Demographic and other clinical
information was obtained from the electronic medical record
General cEEG data review protocol The CSA review group
was composed of 3 EEGers at the fellowship stage of clinical EEG
subspecialty training (readers AndashC) but with at least 6 months of
cEEG experience The same records were also independently
reviewed by the same EEGers (readers AndashC) and 2 attending
clinical neurophysiologists (readers D and E) using conventional
page-by-page visual analysis The findings of the readers at the
attending level served as the ldquogold standardrdquo while the
conventional review by readers AndashC allowed for comparison of
time to review All readers used CSA in daily clinical practice and
were trained in American Clinical Neurophysiology Societyrsquos
intensive care unit cEEG terminology21 Readers A B and C
reviewed 44 37 and 37 cEEGs using the CSA protocol and
66 44 and 8 cEEGs using conventional review respectively
Reviewers D and E reviewed 58 and 60 EEGs respectively
using conventional review For cEEGs lasting 24 hours only
the first 24 hours were reviewed
Detailed descriptions of the CSA-guided and conventional
visual (gold standard) cEEG review protocols technical details
of cEEG recordings and configuration of CSA displays and rea-
sons for selecting CSA over alternative quantitative EEG methods
are provided in the online supplemental material (sections A and
B) An example of the CSA display is provided in figure 1
Statistical analysis for primary aim The primary outcome
measures of this study were time taken for readers AndashC to review
each cEEG study using the CSA-guided cEEG review protocol
compared with conventional page-by-page EEG review and
detection sensitivity for seizures The significance of differences
in review times between the methods of cEEG review was assessed
using a paired t test
Statistical analysis for secondary aims Detection sensitivity
for seizures periodic epileptiform discharges nonperiodic epi-
leptiform discharges focal slowing generalized slowing and
rhythmic delta activity were calculated for reviewers AndashC using
CSA-guided cEEG review relative to the findings of the gold
standard reviewers D and E who relied on conventional page-
by-page EEG review In addition we analyzed detection
sensitivity for electrographic status epilepticus (ESE) For this
study ESE was said to be present when either (1) the maximum
seizure duration (max duration) was 5 minutes or (2)
the minimum average interseizure interval within any hour of
monitoring was 5 minutes ESE was said to have been
ldquodetectedrdquo by CSA-guided review when either all seizures
lasting 5 minutes were detected or when 50 of all
seizures were detected (for cases in which all seizures were
briefer than 5 minutes) otherwise ESE was considered to
have been ldquomissedrdquo
The relationship between review time (per 24 hours of cEEG
recording) and seizure detection sensitivity using CSA-guided
review was assessed using Spearman correlation analysis Calcula-
tions and graphs were generated using Microsoft Excel and Stata
The relation between total seizure burden and percentage of seiz-
ures missed was assessed using a Pearson correlation coefficient
and a t test was used to compare the mean percentages of missed
seizures (for cases lacking status epilepticus) in cases with seizures
with brief vs longer average durations
Standard protocol approvals registrations and patientconsents This retrospective study was conducted under a protocol
approved by the MGH institutional review board Informed consent
was not required
RESULTS Demographic and clinical data for the118 selected patients are summarized in table e-1The 118 cEEGs included 40 with seizures and com-prised a total of 2092 hours of cEEG data and 1192seizures Among the 40 cases with seizures 475(1940) met study criteria for ESE either by havingone or more seizures lasting 5 minutes (74 ofcases [1419]) or by having an average hourly inter-seizure interval5 minutes in duration (25 of cases[519]) (table 1)
Table e-2 summarizes the time-savings analysisThe time required for review of intermittent rawcEEG guided by CSA was substantially less than forconventional complete review of the entire cEEGwithout CSA guidance Average times to review 24hours of cEEG data were 8 (64) minutes for CSA-guided review and 38 (617) minutes for conven-tional review (p 0005) Significant time savingswere also found considering only studies containingseizures (adjusted for 24 hours) 10 (64) minutes forCSA-guided review and 44 (620) minutes for con-ventional review (p 0005) (figure 2)
CSA-guided cEEG review identified all patientswith seizures and detected 873 of all individual seiz-ures among the cohort That is reviewers detected atleast one seizure in every record that contained seizures(as determined by gold-standard conventional EEGreview by readers D and E) however in records withmultiple electrographic seizures some seizures weremissed by CSA-guided review The overall sensitivityof CSA-guided review (figure 3) was as follows seizures873 (10411192) periodic epileptiform discharges
Neurology 83 July 1 2014 57
100 (4343) rhythmic delta activity 971 (3435)focal slowing 987 (7677) generalized slowing100 (100100) and epileptiform discharges 885(6170) No cases of ESE went undetected by CSA-guided review (table 1) all seizures lasting5 minuteswere detected and in cases of ESE without any seizureslasting 5 minutes the lowest seizure detection ratewas 86 (95111)
Excluding cases with ESE due to prolonged (5-minute) seizures (of which all were detected seeabove) we found an inverse relationship betweennumber of seizures per cEEG and number of missedseizures (more seizures were missed in EEGs withhigher total seizure counts Pearson correlation coef-ficient 073 p 5 00001) In addition dividing the21 cases without ESE into cases with brief (averageduration 1 minute) vs longer seizures we foundthat the mean percentage of missed seizures was twiceas high in the group with brief seizures 13 (SD 22)vs 65 (SD 12) respectively (t test p 5 001)
Differences in detection rates for seizures andother patterns between readers in the CSA-guidedreview group were modest and not clinically signifi-cant (table e-3) A detailed discussion of differencesbetween detection performance characteristics among
reviewers A B and C in the CSA-guided reviewgroup is provided in the online supplemental material(section C) An example of the CSA display obscuredby artifact is provided in figure 4
There was no significant correlation between sei-zure detection sensitivity (CSA protocol) and timeto review 24 hours of cEEG (Spearman r R2 [40]013 p 5 041) suggesting that CSA-guided re-viewers adjusted review time on a case-by-case basisto maintain sensitivity In addition linear regressionof the time to review each file as a function of theordering in which cEEG was reviewed by a particularreader revealed no significant trend suggesting thatthe time to review a cEEG study was stable for eachreader throughout the study
DISCUSSION The main finding of this study is thatCSA-based screening of cEEG recordings inhospitalized adults can substantially reduce averagereview time without significantly sacrificingsensitivity for seizures and other critical findingsrelative to conventional page-by-page review CSA-guided screening identified 100 of cEEGrecordings containing seizures all cases of ESE andtended to miss seizures only in records with
Figure 1 CSA display
Top screen Two-hour segments of CSA power data were displayed from top to bottom in a spectrogrammontage There arebrief periods with increased power in the high-frequency band over the left hemisphere highlighting suspicious regions Bot-tom screen Raw cEEG data cEEG 5 continuous EEG CSA 5 compressed spectral array
58 Neurology 83 July 1 2014
Table 1 Descriptive statistics for patients with seizures
Patient No of seizures No detected Detected No missed Missed Min duration Mean duration Max duration Max rate Min ISI Max ESE present ESE detected
1 1 1 100 0 0 05 05 05 1 mdash 1
2 1 1 100 0 0 9408 9408 9408 1 mdash 100 X X
3 1 1 100 0 0 21 21 21 1 mdash 4
4 1 1 100 0 0 18 18 18 1 mdash 3
5 1 1 100 0 0 184 184 184 1 mdash 31 X X
6 1 1 100 0 0 22 22 22 1 mdash 4
7 1 1 100 0 0 03 03 03 1 mdash 1
8 2 2 100 0 0 100 124 147 1 900 25 X X
9 2 2 100 0 0 05 06 06 1 1200 1
10 3 2 67 1 33 11 11 19 1 350 0
11 3 1 33 2 67 02 04 10 1 620 1
12 3 3 100 0 0 03 19 35 2 300 6
13 3 3 100 0 0 04 04 05 1 700 1
14 3 3 100 0 0 01 01 134 1 50 3 X X
15 4 3 75 1 25 03 04 05 3 200 3
16 8 8 100 0 0 08 13 18 4 150 11
17 9 6 67 3 33 06 41 71 1 660 12 X X
18 10 10 100 0 0 03 04 09 9 67 7
19 14 11 79 3 21 07 06 111 3 200 100 X X
20 14 14 100 0 0 04 22 89 7 86 15 X X
21 20 12 60 8 40 10 1123 9124 4 150 100 X X
22 23 22 96 1 4 04 17 73 6 100 16 X X
23 25 15 60 10 40 05 05 27 7 86 1
24 28 27 96 1 4 04 06 07 2 300 2
25 28 20 71 8 29 09 22 22 3 200 4
26 29 14 48 15 52 04 20 68 5 120 29 X X
27 30 28 93 2 7 25 48 69 3 200 31 X X
28 33 33 100 0 0 02 04 07 6 100 2
29 37 36 97 1 3 10 12 14 4 150 4
30 46 46 100 0 0 10 19 19 5 120 3
31 47 47 100 0 0 08 11 15 5 120 2
32 48 48 100 0 0 01 02 02 25 24 1 X X
Continued
Neurology
83
July12
014
59
multiple seizures attaining an overall detection rate of87 in 25 of the time required for conventionalreview This finding was established in a largecollection of unselected recordings from patientswith a broad range of neurologic conditionsMoreover the cEEG review procedure was clinicallypractical Our data suggest that CSA-guided reviewis an acceptable alternative to the current standardpractice of page-by-page review of all data for cEEGmonitoring in critically ill adults
In the minority of cases in which CSA-guidedreview missed seizures misses tended to represent asmall fraction of a high seizure burden Missed seiz-ures also tended to occur more often in patients withbriefer seizures We speculate that misses can be ex-plained in part by the intrinsic difficulty of drawinga line between patterns on the ldquoictal-interictal contin-uumrdquo and ldquodefinite seizuresrdquo Efforts to increase in-terrater agreement on seizure patterns may furtherimprove performance of CSA-guided review
Our findings in adults are similar to those ofsmaller studies in pediatric populations1820 Onestudy using CSA and amplitude-integrated EEG in23 pediatric cEEGs (17 with seizures 10 without)found a sensitivity for seizure detection with CSA of83320 Another study in 8 neonates (26ndash44weeks) found that envelope trends enabled experi-enced users to detect 88 of prolonged seizureswhile detection rates for brief or slowly evolvingneonatal seizures were only 40 and 2022 sug-gesting that compressed EEG may be useful in somebut not all neonates In contrast with the presentstudy in both of these pediatric studies reviewerswere not permitted to correlate compressed datafindings with the primary EEG data This differencemay have contributed to lower detection sensitivitiesrelative to the present study
The present study investigated sensitivity and effi-ciency (time savings) of CSA as to guide cEEGreview placing minimal emphasis on specificity(low false-positive detection rates) This choicetreats CSA as a screening tool which cannot be per-formed without simultaneous review of raw cEEGdata rather than as a primary modality for cEEGinterpretation Suspicious CSA patterns must befrequently correlated with raw EEG data to distin-guish seizures from state changes periodic patternsand artifacts This back-and-forth dynamic allowscEEG review to be adaptive such that after an ini-tial careful correlation of raw cEEG with CSA pat-terns (including a careful visual analysis of thecEEG background) during the initial 30-minuteperiod reviewers are able to rapidly distinguishartifacts from true physiologic changes This initialreview enables subsequent review to proceed morequickly
Tab
le1
Con
tinu
ed
Pat
ient
No
ofse
izur
esNo
det
ecte
dDet
ecte
d
No
misse
dMisse
d
Min
dur
ation
Mea
ndur
ation
Max
dur
ation
Max
rate
Min
ISI
Max
ESE
pre
sent
ESE
det
ecte
d
33
53
52
98
12
02
40
154
12
50
27
XX
34
54
52
96
24
01
03
06
30
20
2X
X
35
57
20
35
37
65
02
86
2921
35
17
100
XX
36
76
74
97
23
15
25
34
16
38
13
XX
37
99
95
96
44
00
44
436
30
20
84
XX
38
111
95
86
16
14
02
07
30
19
32
15
XX
39
121
104
86
17
14
02
05
11
2242
2
40
151
132
87
19
13
01
13
29
21
29
21
XX
Abb
reviations
ESE
5elec
trog
raph
icstatus
epile
pticus
ISI5
interseizu
reinterval
Min
duration
5minim
umse
izure
duration
(inminutes
)max
duration
5max
imum
seizure
duration
(inminutes
)max
rate
5max
imum
numbe
rof
seizures
that
occu
rred
during
any
hour
ofmon
itoring
min
ISI5
minim
umav
erag
eISIfor
anyho
urdu
ring
mon
itoring
define
das
theminim
umav
erag
edu
ration
betw
eenco
nsec
utivese
izures
withinan
yho
urof
mon
itoring(in
patien
tswith1se
izure)m
ax
5max
imum
percen
tage
ofan
yho
urdu
ring
mon
itoringthat
was
occu
pied
byse
izureac
tivityP
atientsareso
rted
bynu
mbe
rof
seizures
that
occu
rred
during
mon
itoring
Detec
ted
andmisse
d
give
thepe
rcen
tage
ofse
izures
detected
ormisse
dby
compr
esse
dsp
ectral
arrayndash
guided
review
protoc
ol(relativeto
thepa
ge-by-pa
gereview
gold
stan
dard
)For
this
stud
yapa
tien
twas
said
toha
veESE
ifeither
(1)t
hemax
imum
seizuredu
ration
was
5
minutes
or(2)t
heminim
umho
urly
averag
eISIw
as5
minutes
60 Neurology 83 July 1 2014
In keeping with a prior study by our group23
CSA-guided review had excellent sensitivity for thepresence of other common critical ldquointerictalrdquo find-ings including focal (987) and generalized (100)slowing periodic discharges (100) and rhythmicdelta activity (971) compared with conventionalpage-by-page EEG review Similarly sensitivity forthe presence of sporadic epileptiform discharges wasreasonably high (885) The high sensitivity fornonseizure findings is not necessarily because these
patterns produce distinct CSA signatures For exam-ple epileptiform discharges being brief typicallyshow no obvious footprint in the 2-hour CSA displayused in our protocol Rather these patterns are abun-dant enough to be detected even by very limitedreview of the primary EEG data that occurs duringCSA-guided review
The early stage of cEEG training of the CSAreview group merits comment This selection of read-ers was intended to reflect the practice at many ter-tiary care centers of relying on clinical fellows formost first-line cEEG interpretation The use of train-ees might produce conservative estimates of sensitiv-ity as sensitivity should improve with experienceBy contrast our gold-standard EEG reviewers wereexperienced attending-level clinical EEGers to ensurevalidity of the gold standard
Our protocol relied on 2-hour CSA windowsWe chose to display 5 CSA panels (left and right lat-eral and parasagittal chains and hemispheric asym-metry spectrogram) Including additional CSApanels higher time resolution (eg 30-minute win-dows) and possibly other compressed-data formats(eg amplitude integrated EEG rhythmicity meas-ures) might have produced higher seizure detectionrates However increasing data volume might com-promise efficiency by producing cognitive overloadFurther research is necessary to determine whichquantitative EEG instruments alone and in combi-nation present the best cognitive match for humanEEG reviewers
Some have suggested that nurses EEG technolo-gists and residents can be trained to review CSA datato flag regions for direct review by physician ex-perts2021 These efforts are important because cEEGpatterns in the acutely ill are dynamic and requireprompt action However nonexpert CSA-basedscreening (without immediate visual confirmation)may yield more false alarms which might place addi-tional burdens on neurophysiologists charged withfollowing up on such alerts In the current studyconstant correlation of CSA patterns with the under-lying EEG was critical in achieving high sensitivityand efficiency and direct visual confirmation by atrained expert remains an essential step to determin-ing which cEEG patterns are significant rather thanartifactual or incidental
Our results are subject to several limitationsFirst our study is a single-center retrospectivereview and a larger multi-institutional prospectivetrial is needed to establish the validity and general-izability of our findings Second CSA cannot escapethe inherent limitations of scalp EEG including thefact that not all seizures may be detectable on scalpEEG For example exquisitely focal seizures maybe detectable only with invasive monitoring and
Figure 2 Time-savings group analysis
Comparison histograms of the time taken to review a given record with the assistance ofCSA (blue bars) and without (red) (A) All studies reviewed by readers AndashC using CSA guid-ance vs conventional review (B) All studies that contained seizures Studies were rankordered from the shortest to longest review time The average time to review 24 hours ofcEEG data when CSA was used was 8 (64) minutes whereas conventional review took 38(617) minutes on average (A) These were statistically different between the groups (p
0005) (B) If seizures were present time savings was more marked CSA review 10(64) minutes and conventional 44 (620) minutes (p 0005) The figure is truncated at60 minutes For 14 studies reading with conventional review took more than 60 minutesTimes to review for these outliers were 622 623 635 636 637 646 652 660 673716 724 750 958 and 1016 in chart A and 958 750 724 716 673 652 646636 635 623 and 622 in chart B Times to review were normalized to a standard dura-tion of 24 hours of cEEG ie all reported times are expressed as time spent per 24 hours ofEEG data cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 61
seizure activity of low amplitude frequency orduration or seizures in the presence of ldquomalig-nantrdquo-appearing background activity may be diffi-cult to discern even on careful inspection of the rawcEEG Third while our results suggest that patternsmeeting the strict definition of definite electro-graphic seizures24 can be identified readily border-zone rhythmic and periodic EEG patterns failing toqualify as definite electrographic seizures may nev-ertheless be symptomatic and require treatment insome cases Determination of the clinical signifi-cance of such cases is possible only by clinical cor-relation eg to determine whether the pattern inquestion reliably correlates with signssymptomsand whether the patient improves with treatmentIn such cases CSA-guided review may not signifi-cantly reduce the total time required for interpreta-tion Fourth it should be emphasized that ourestimate of approximately 75 time savings appliesonly to the part of EEG review after careful directconventional visual analysis of the initial 30 minutesof data As stated above there are reasons to believethat the familiarity with the cEEG provided by thisinitial review is critical to both time savings andsensitivity of subsequent CSA-guided screeningFifth not all centers have access to software or read-ing stations such as those used to view CSA in thisstudy However such centers may be less likely toperform large-scale cEEG and may thus be betterable to review their studies without relying on CSA-based screening Sixth some centers employ dedi-cated technicians to monitor and screen for seizures
allowing physicians to focus only on suspicious seg-ments perhaps obviating the advantage (for physi-cians) of CSA-guided review Seventh some centersemploy screening of CSA (andor other measures)by nurses and electroneurodiagnostic technologistsfollowed by page-by-page EEG review by a physi-cian in fellowship training or another electroneur-odiagnostic technician followed by complete ortargeted review by an attending-level neurophysiol-ogist This approach of triple EEG review whiletime-consuming and resource-intensive is arguablythe least likely to miss any significant findingsFurther outcome-oriented research is needed todetermine the optimal approach among these alter-natives Eighth it must be emphasized that theCSA-guided review protocol proposed here is notintended as a substitute for visual review by trainedexpert clinicians and indeed expert visual review ofprimary cEEG data is an indispensable componentof the present CSA-guided protocol Lastly the re-sults of the present study apply only in the criticalcare setting They have no obvious direct relevanceto diagnostic long-term video EEG monitoring forassessment of chronic epilepsy particularly for thepresurgical workup In such patients interictalspikes may be infrequent but very clinically impor-tant necessitating careful time-consuming visualsearch and patients may undergo days of cEEGrecording to detect even a small number of seizureson which neurosurgical decisions are based In thissetting missing one seizure can have significantclinical consequences
Figure 3 Sensitivity analysis for seizures and other abnormal patterns
The overall sensitivity of CSA-guided review and conventional review of reviewers AndashC is shown relative to the gold-standard findings of readers D and E seizures 873 (10411192) PDs 100 (4343) RDA 971 (3435) FS987 (7677) GS 100 (100100) and EDs 885 (6170) By definition the gold-standard conventional review groupdetected 100 of all seizures and common abnormal patterns CSA 5 compressed spectral array ED 5 epileptiformdischarge FS 5 focal slowing GS 5 generalized slowing PD 5 periodic epileptiform discharge RDA 5 rhythmic deltaactivity
62 Neurology 83 July 1 2014
Finally it remains to be determined whether thetime savings achievable by CSA-guided review ismeaningful in either clinical or cost-effectivenessterms In many cases initial identification of EEGevents represents only one part of providing criticalcare cEEG services Other responsibilities whichmay be even more time-consuming include clinicalcorrelation of EEG findings including bedside exam-ination as needed to determine their significanceevaluation of changes in medications frequent com-munication with clinical teams to report findingsand to make EEG-related management recommenda-tions and writing EEG reports Nevertheless if vali-dated our results may justify replacing at least thefront-line conventional page-by-page EEG reviewarguably the most time-sensitive stage of EEG analy-sis by the more efficient CSA-based screening proce-dure presented herein
Our results suggest that CSA-guided cEEG reviewcan enable significantly faster interpretation withoutsubstantial loss of sensitivity for critical findings in thevast majority of cases While intensive care unit out-come measures were not explored in this study thedemonstration that CSA-guided review enables rapid
and accurate evaluation of critical EEG findings (suchas the presence of seizures or nonconvulsive status epi-lepticus) suggests that this protocol may positively affectpatient care by allowing more timely management de-cisions in response to critical cEEG events
AUTHOR CONTRIBUTIONSLMVRM MMS and MBW conceptualized and designed the study
LMVRM (MGH clinical neurophysiology fellow) and MBW (faculty
with the MGH Epilepsy Service) completed the statistical analysis LMV
RM MMS and MBW drafted the original manuscript LMVRM
SP and MN contributed to the data production and collection SSC
AJC DBH MMS ESR and MBW reviewed and revised the
manuscript
STUDY FUNDINGNo targeted funding reported
DISCLOSUREL Moura reports no disclosures relevant to the manuscript M Shafi
received support from Harvard Catalyst KL2 MeRIT program M Ng
and S Pati report no disclosures relevant to the manuscript S Cash
A Cole and D Hoch received support from NIHNeurological Disor-
ders and Stroke NS062092 E Rosenthal reports no disclosures relevant
to the manuscript M Westover received support from the American
Brain Foundation Go to Neurologyorg for full disclosures
Received May 22 2013 Accepted in final form March 25 2014
Figure 4 CSA display obscured by artifact
Top screen Two-hour segments of CSA display as described in figure 3 Bottom screen Raw cEEG data as described infigure 3 cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 63
REFERENCES1 Vespa PM Nuwer MR Juhaacutesz C et al Early detection of
vasospasm after acute subarachnoid hemorrhage using con-
tinuous EEG ICU monitoring Electroencephalogr Clin
Neurophysiol 1997103607ndash615
2 Schreiber JM Zelleke T Gaillard WD et al Continuous
video EEG for patients with acute encephalopathy in a
pediatric intensive care unit Neurocrit Care 201217
31ndash38
3 Pandian JD Cascino GD So EL et al Digital video-
electroencephalographic monitoring in the neurological-
neurosurgical intensive care unit Arch Neurol 200461
1090ndash1094
4 Cloostermans MC Van Meulen FB Eertman CJ et al
Continuous electroencephalography monitoring for early
prediction of neurological outcome in postanoxic patients
after cardiac arrest a prospective cohort study Crit Care
Med 2012402867ndash2875
5 Rudin D Grize L Schindler C et al High prevalence of
nonconvulsive and subtle status epilepticus in an ICU of a
tertiary care center a three-year observational cohort
study Epilepsy Res 201196140ndash150
6 Young GB Doig GS Continuous EEG monitoring in
comatose intensive care patients epileptiform activity in
etiologically distinct groups Neurocrit Care 200525ndash10
7 Young GB Continuous EEG monitoring in the ICU
Acta Neurol Scand 200611467ndash68
8 Claassen J Mayer SA Kowalski RG et al Detection of
electrographic seizures with continuous EEG monitoring
in critically ill patients Neurology 2004621743ndash1748
9 Vespa PM Nuwer MR Nenov V et al Increased inci-
dence and impact of nonconvulsive and convulsive seizures
after traumatic brain injury as detected by continuous elec-
troencephalographic monitoring J Neurosurg 199991
750ndash760
10 Towne AR Waterhouse EJ Boggs JG et al Prevalence of
nonconvulsive status epilepticus in comatose patients
Neurology 200054340ndash345
11 Talwar D Torres F Continuous electrophysiologic mon-
itoring of cerebral function in the pediatric intensive care
unit Pediatr Neurol 19884137ndash147
12 Claassen J Hirsch LJ Kreiter KT et al Quantitative con-
tinuous EEG for detecting delayed cerebral ischemia in
patients with poor-grade subarachnoid hemorrhage Clin
Neurophysiol 20041152699ndash2710
13 Carrera E Claassen J Oddo M et al Continuous electroen-
cephalographic monitoring in critically ill patients with central
nervous system infections Arch Neurol 2008651612ndash1618
14 Sutter R Fuhr P Grize L et al Continuous video-EEG
monitoring increases detection rate of nonconvulsive status
epilepticus in the ICU Epilepsia 201152453ndash457
15 Claassen J Hirsch LJ Frontera JA et al Prognostic sig-
nificance of continuous EEG monitoring in patients with
poor-grade subarachnoid hemorrhage Neurocrit Care
20064103ndash112
16 Nuwer MR Quantitative EEG analysis in clinical settings
Brain Topogr 19968201ndash208
17 Nuwer M Assessment of digital EEG quantitative EEG
and EEG brain mapping report of the American Academy
of Neurology and the American Clinical Neurophysiology
Society Neurology 199749277ndash292
18 Shah AK Agarwal R Carhuapoma JR Loeb JA Com-
pressed EEG pattern analysis for critically ill
neurological-neurosurgical patients Neurocrit Care
20065124ndash133
19 Bricolo A Turazzi S Faccioli F et al Clinical application
of compressed spectral array in long-term EEG monitoring
of comatose patients Electroencephalogr Clin Neurophy-
siol 197845211ndash225
20 Stewart CP Otsubo H Ochi A et al Seizure identification in
the ICU using quantitative EEG displays Neurology 2010
751501ndash1508
21 Hirsch LJ LaRoche SM Gaspard N et al American Clin-
ical Neurophysiology Societyrsquos Standardized Critical Care
EEG Terminology 2012 version J Clin Neurophysiol
2013301ndash27
22 Abend NS Dlugos D Herman S Neonatal seizure detec-
tion using multichannel display of envelope trend Epilep-
sia 200849349ndash352
23 Williamson CA Wahlster S Shafi MM Westover MB
Sensitivity of compressed spectral arrays for detecting seiz-
ures in acutely ill adults Neurocrit Care 20142032ndash39
24 Young GB Jordan KG Doig GS An assessment of non-
convulsive seizures in the intensive care unit using contin-
uous EEG monitoring an investigation of variables
associated with mortality Neurology 19964783ndash89
Free Michael J Fox DVD Video on Parkinsonrsquos DiseaseThe AAN and the American Brain Foundation present actor and Parkinsonrsquos disease patientMichael J Fox hosting Parkinsonrsquos Disease A Guide for Patients and Families This new patienteducation video is now available free to members and the public either on DVD or online Thefree DVD can be ordered while supplies last by visiting AANcomviewPatientEducationVideos orcalling (800) 879-1960 The video can be viewed online at YouTubecomAANChannel with otherpatient education DVDs produced by the AAN
64 Neurology 83 July 1 2014
DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
ServicesUpdated Information amp
httpwwwneurologyorgcontent83156fullhtmlincluding high resolution figures can be found at
Supplementary Material
00000000537DC1htmlhttpwwwneurologyorgcontentsuppl20140629WNL00000Supplementary material can be found at
References
httpwwwneurologyorgcontent83156fullhtmlref-list-1at This article cites 24 articles 5 of which you can access for free
Subspecialty Collections
httpwwwneurologyorgcgicollectionhealth_care_reformHealth care reform
reshttpwwwneurologyorgcgicollectioneeg_see_epilepsy-seizuEEG see EpilepsySeizures
httpwwwneurologyorgcgicollectioncritical_careCritical carefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

expert review of selected segments of rawcEEG data when guided by CSA-based screen-ing is less than that required for conventionalreview of the entire raw cEEG without mean-ingfully compromising sensitivity for seizuresor other critical findings
METHODS Level of evidence The aim of this Class IV evi-
dence study was to determine whether screening of cEEG with
CSA efficiently and accurately identifies seizures and other
EEG abnormalities as compared with conventional unaided
visual interpretation
Study design We conducted a retrospective review of critical
care cEEGs and medical records at the Massachusetts General
Hospital (MGH) between September 2011 and February 2012
(figures e-1 and e-2 on the Neurologyreg Web site at Neurologyorg)
All cEEGs were ordered by treating physicians (rather than as part of a
protocol) and all cEEGs included were performed for the purpose of
seizure surveillance in acutely ill patients
Patient cohort Among 370 consecutive patients monitored
between September 2011 and February 2012 118 patients met
the following inclusion criteria (1) older than 18 years of age
(2) duration $8 hours (3) admitted for an acute illness (rather
than electively) and (4) the primary indication for ordering cEEG
was a suspicion for seizures Demographic and other clinical
information was obtained from the electronic medical record
General cEEG data review protocol The CSA review group
was composed of 3 EEGers at the fellowship stage of clinical EEG
subspecialty training (readers AndashC) but with at least 6 months of
cEEG experience The same records were also independently
reviewed by the same EEGers (readers AndashC) and 2 attending
clinical neurophysiologists (readers D and E) using conventional
page-by-page visual analysis The findings of the readers at the
attending level served as the ldquogold standardrdquo while the
conventional review by readers AndashC allowed for comparison of
time to review All readers used CSA in daily clinical practice and
were trained in American Clinical Neurophysiology Societyrsquos
intensive care unit cEEG terminology21 Readers A B and C
reviewed 44 37 and 37 cEEGs using the CSA protocol and
66 44 and 8 cEEGs using conventional review respectively
Reviewers D and E reviewed 58 and 60 EEGs respectively
using conventional review For cEEGs lasting 24 hours only
the first 24 hours were reviewed
Detailed descriptions of the CSA-guided and conventional
visual (gold standard) cEEG review protocols technical details
of cEEG recordings and configuration of CSA displays and rea-
sons for selecting CSA over alternative quantitative EEG methods
are provided in the online supplemental material (sections A and
B) An example of the CSA display is provided in figure 1
Statistical analysis for primary aim The primary outcome
measures of this study were time taken for readers AndashC to review
each cEEG study using the CSA-guided cEEG review protocol
compared with conventional page-by-page EEG review and
detection sensitivity for seizures The significance of differences
in review times between the methods of cEEG review was assessed
using a paired t test
Statistical analysis for secondary aims Detection sensitivity
for seizures periodic epileptiform discharges nonperiodic epi-
leptiform discharges focal slowing generalized slowing and
rhythmic delta activity were calculated for reviewers AndashC using
CSA-guided cEEG review relative to the findings of the gold
standard reviewers D and E who relied on conventional page-
by-page EEG review In addition we analyzed detection
sensitivity for electrographic status epilepticus (ESE) For this
study ESE was said to be present when either (1) the maximum
seizure duration (max duration) was 5 minutes or (2)
the minimum average interseizure interval within any hour of
monitoring was 5 minutes ESE was said to have been
ldquodetectedrdquo by CSA-guided review when either all seizures
lasting 5 minutes were detected or when 50 of all
seizures were detected (for cases in which all seizures were
briefer than 5 minutes) otherwise ESE was considered to
have been ldquomissedrdquo
The relationship between review time (per 24 hours of cEEG
recording) and seizure detection sensitivity using CSA-guided
review was assessed using Spearman correlation analysis Calcula-
tions and graphs were generated using Microsoft Excel and Stata
The relation between total seizure burden and percentage of seiz-
ures missed was assessed using a Pearson correlation coefficient
and a t test was used to compare the mean percentages of missed
seizures (for cases lacking status epilepticus) in cases with seizures
with brief vs longer average durations
Standard protocol approvals registrations and patientconsents This retrospective study was conducted under a protocol
approved by the MGH institutional review board Informed consent
was not required
RESULTS Demographic and clinical data for the118 selected patients are summarized in table e-1The 118 cEEGs included 40 with seizures and com-prised a total of 2092 hours of cEEG data and 1192seizures Among the 40 cases with seizures 475(1940) met study criteria for ESE either by havingone or more seizures lasting 5 minutes (74 ofcases [1419]) or by having an average hourly inter-seizure interval5 minutes in duration (25 of cases[519]) (table 1)
Table e-2 summarizes the time-savings analysisThe time required for review of intermittent rawcEEG guided by CSA was substantially less than forconventional complete review of the entire cEEGwithout CSA guidance Average times to review 24hours of cEEG data were 8 (64) minutes for CSA-guided review and 38 (617) minutes for conven-tional review (p 0005) Significant time savingswere also found considering only studies containingseizures (adjusted for 24 hours) 10 (64) minutes forCSA-guided review and 44 (620) minutes for con-ventional review (p 0005) (figure 2)
CSA-guided cEEG review identified all patientswith seizures and detected 873 of all individual seiz-ures among the cohort That is reviewers detected atleast one seizure in every record that contained seizures(as determined by gold-standard conventional EEGreview by readers D and E) however in records withmultiple electrographic seizures some seizures weremissed by CSA-guided review The overall sensitivityof CSA-guided review (figure 3) was as follows seizures873 (10411192) periodic epileptiform discharges
Neurology 83 July 1 2014 57
100 (4343) rhythmic delta activity 971 (3435)focal slowing 987 (7677) generalized slowing100 (100100) and epileptiform discharges 885(6170) No cases of ESE went undetected by CSA-guided review (table 1) all seizures lasting5 minuteswere detected and in cases of ESE without any seizureslasting 5 minutes the lowest seizure detection ratewas 86 (95111)
Excluding cases with ESE due to prolonged (5-minute) seizures (of which all were detected seeabove) we found an inverse relationship betweennumber of seizures per cEEG and number of missedseizures (more seizures were missed in EEGs withhigher total seizure counts Pearson correlation coef-ficient 073 p 5 00001) In addition dividing the21 cases without ESE into cases with brief (averageduration 1 minute) vs longer seizures we foundthat the mean percentage of missed seizures was twiceas high in the group with brief seizures 13 (SD 22)vs 65 (SD 12) respectively (t test p 5 001)
Differences in detection rates for seizures andother patterns between readers in the CSA-guidedreview group were modest and not clinically signifi-cant (table e-3) A detailed discussion of differencesbetween detection performance characteristics among
reviewers A B and C in the CSA-guided reviewgroup is provided in the online supplemental material(section C) An example of the CSA display obscuredby artifact is provided in figure 4
There was no significant correlation between sei-zure detection sensitivity (CSA protocol) and timeto review 24 hours of cEEG (Spearman r R2 [40]013 p 5 041) suggesting that CSA-guided re-viewers adjusted review time on a case-by-case basisto maintain sensitivity In addition linear regressionof the time to review each file as a function of theordering in which cEEG was reviewed by a particularreader revealed no significant trend suggesting thatthe time to review a cEEG study was stable for eachreader throughout the study
DISCUSSION The main finding of this study is thatCSA-based screening of cEEG recordings inhospitalized adults can substantially reduce averagereview time without significantly sacrificingsensitivity for seizures and other critical findingsrelative to conventional page-by-page review CSA-guided screening identified 100 of cEEGrecordings containing seizures all cases of ESE andtended to miss seizures only in records with
Figure 1 CSA display
Top screen Two-hour segments of CSA power data were displayed from top to bottom in a spectrogrammontage There arebrief periods with increased power in the high-frequency band over the left hemisphere highlighting suspicious regions Bot-tom screen Raw cEEG data cEEG 5 continuous EEG CSA 5 compressed spectral array
58 Neurology 83 July 1 2014
Table 1 Descriptive statistics for patients with seizures
Patient No of seizures No detected Detected No missed Missed Min duration Mean duration Max duration Max rate Min ISI Max ESE present ESE detected
1 1 1 100 0 0 05 05 05 1 mdash 1
2 1 1 100 0 0 9408 9408 9408 1 mdash 100 X X
3 1 1 100 0 0 21 21 21 1 mdash 4
4 1 1 100 0 0 18 18 18 1 mdash 3
5 1 1 100 0 0 184 184 184 1 mdash 31 X X
6 1 1 100 0 0 22 22 22 1 mdash 4
7 1 1 100 0 0 03 03 03 1 mdash 1
8 2 2 100 0 0 100 124 147 1 900 25 X X
9 2 2 100 0 0 05 06 06 1 1200 1
10 3 2 67 1 33 11 11 19 1 350 0
11 3 1 33 2 67 02 04 10 1 620 1
12 3 3 100 0 0 03 19 35 2 300 6
13 3 3 100 0 0 04 04 05 1 700 1
14 3 3 100 0 0 01 01 134 1 50 3 X X
15 4 3 75 1 25 03 04 05 3 200 3
16 8 8 100 0 0 08 13 18 4 150 11
17 9 6 67 3 33 06 41 71 1 660 12 X X
18 10 10 100 0 0 03 04 09 9 67 7
19 14 11 79 3 21 07 06 111 3 200 100 X X
20 14 14 100 0 0 04 22 89 7 86 15 X X
21 20 12 60 8 40 10 1123 9124 4 150 100 X X
22 23 22 96 1 4 04 17 73 6 100 16 X X
23 25 15 60 10 40 05 05 27 7 86 1
24 28 27 96 1 4 04 06 07 2 300 2
25 28 20 71 8 29 09 22 22 3 200 4
26 29 14 48 15 52 04 20 68 5 120 29 X X
27 30 28 93 2 7 25 48 69 3 200 31 X X
28 33 33 100 0 0 02 04 07 6 100 2
29 37 36 97 1 3 10 12 14 4 150 4
30 46 46 100 0 0 10 19 19 5 120 3
31 47 47 100 0 0 08 11 15 5 120 2
32 48 48 100 0 0 01 02 02 25 24 1 X X
Continued
Neurology
83
July12
014
59
multiple seizures attaining an overall detection rate of87 in 25 of the time required for conventionalreview This finding was established in a largecollection of unselected recordings from patientswith a broad range of neurologic conditionsMoreover the cEEG review procedure was clinicallypractical Our data suggest that CSA-guided reviewis an acceptable alternative to the current standardpractice of page-by-page review of all data for cEEGmonitoring in critically ill adults
In the minority of cases in which CSA-guidedreview missed seizures misses tended to represent asmall fraction of a high seizure burden Missed seiz-ures also tended to occur more often in patients withbriefer seizures We speculate that misses can be ex-plained in part by the intrinsic difficulty of drawinga line between patterns on the ldquoictal-interictal contin-uumrdquo and ldquodefinite seizuresrdquo Efforts to increase in-terrater agreement on seizure patterns may furtherimprove performance of CSA-guided review
Our findings in adults are similar to those ofsmaller studies in pediatric populations1820 Onestudy using CSA and amplitude-integrated EEG in23 pediatric cEEGs (17 with seizures 10 without)found a sensitivity for seizure detection with CSA of83320 Another study in 8 neonates (26ndash44weeks) found that envelope trends enabled experi-enced users to detect 88 of prolonged seizureswhile detection rates for brief or slowly evolvingneonatal seizures were only 40 and 2022 sug-gesting that compressed EEG may be useful in somebut not all neonates In contrast with the presentstudy in both of these pediatric studies reviewerswere not permitted to correlate compressed datafindings with the primary EEG data This differencemay have contributed to lower detection sensitivitiesrelative to the present study
The present study investigated sensitivity and effi-ciency (time savings) of CSA as to guide cEEGreview placing minimal emphasis on specificity(low false-positive detection rates) This choicetreats CSA as a screening tool which cannot be per-formed without simultaneous review of raw cEEGdata rather than as a primary modality for cEEGinterpretation Suspicious CSA patterns must befrequently correlated with raw EEG data to distin-guish seizures from state changes periodic patternsand artifacts This back-and-forth dynamic allowscEEG review to be adaptive such that after an ini-tial careful correlation of raw cEEG with CSA pat-terns (including a careful visual analysis of thecEEG background) during the initial 30-minuteperiod reviewers are able to rapidly distinguishartifacts from true physiologic changes This initialreview enables subsequent review to proceed morequickly
Tab
le1
Con
tinu
ed
Pat
ient
No
ofse
izur
esNo
det
ecte
dDet
ecte
d
No
misse
dMisse
d
Min
dur
ation
Mea
ndur
ation
Max
dur
ation
Max
rate
Min
ISI
Max
ESE
pre
sent
ESE
det
ecte
d
33
53
52
98
12
02
40
154
12
50
27
XX
34
54
52
96
24
01
03
06
30
20
2X
X
35
57
20
35
37
65
02
86
2921
35
17
100
XX
36
76
74
97
23
15
25
34
16
38
13
XX
37
99
95
96
44
00
44
436
30
20
84
XX
38
111
95
86
16
14
02
07
30
19
32
15
XX
39
121
104
86
17
14
02
05
11
2242
2
40
151
132
87
19
13
01
13
29
21
29
21
XX
Abb
reviations
ESE
5elec
trog
raph
icstatus
epile
pticus
ISI5
interseizu
reinterval
Min
duration
5minim
umse
izure
duration
(inminutes
)max
duration
5max
imum
seizure
duration
(inminutes
)max
rate
5max
imum
numbe
rof
seizures
that
occu
rred
during
any
hour
ofmon
itoring
min
ISI5
minim
umav
erag
eISIfor
anyho
urdu
ring
mon
itoring
define
das
theminim
umav
erag
edu
ration
betw
eenco
nsec
utivese
izures
withinan
yho
urof
mon
itoring(in
patien
tswith1se
izure)m
ax
5max
imum
percen
tage
ofan
yho
urdu
ring
mon
itoringthat
was
occu
pied
byse
izureac
tivityP
atientsareso
rted
bynu
mbe
rof
seizures
that
occu
rred
during
mon
itoring
Detec
ted
andmisse
d
give
thepe
rcen
tage
ofse
izures
detected
ormisse
dby
compr
esse
dsp
ectral
arrayndash
guided
review
protoc
ol(relativeto
thepa
ge-by-pa
gereview
gold
stan
dard
)For
this
stud
yapa
tien
twas
said
toha
veESE
ifeither
(1)t
hemax
imum
seizuredu
ration
was
5
minutes
or(2)t
heminim
umho
urly
averag
eISIw
as5
minutes
60 Neurology 83 July 1 2014
In keeping with a prior study by our group23
CSA-guided review had excellent sensitivity for thepresence of other common critical ldquointerictalrdquo find-ings including focal (987) and generalized (100)slowing periodic discharges (100) and rhythmicdelta activity (971) compared with conventionalpage-by-page EEG review Similarly sensitivity forthe presence of sporadic epileptiform discharges wasreasonably high (885) The high sensitivity fornonseizure findings is not necessarily because these
patterns produce distinct CSA signatures For exam-ple epileptiform discharges being brief typicallyshow no obvious footprint in the 2-hour CSA displayused in our protocol Rather these patterns are abun-dant enough to be detected even by very limitedreview of the primary EEG data that occurs duringCSA-guided review
The early stage of cEEG training of the CSAreview group merits comment This selection of read-ers was intended to reflect the practice at many ter-tiary care centers of relying on clinical fellows formost first-line cEEG interpretation The use of train-ees might produce conservative estimates of sensitiv-ity as sensitivity should improve with experienceBy contrast our gold-standard EEG reviewers wereexperienced attending-level clinical EEGers to ensurevalidity of the gold standard
Our protocol relied on 2-hour CSA windowsWe chose to display 5 CSA panels (left and right lat-eral and parasagittal chains and hemispheric asym-metry spectrogram) Including additional CSApanels higher time resolution (eg 30-minute win-dows) and possibly other compressed-data formats(eg amplitude integrated EEG rhythmicity meas-ures) might have produced higher seizure detectionrates However increasing data volume might com-promise efficiency by producing cognitive overloadFurther research is necessary to determine whichquantitative EEG instruments alone and in combi-nation present the best cognitive match for humanEEG reviewers
Some have suggested that nurses EEG technolo-gists and residents can be trained to review CSA datato flag regions for direct review by physician ex-perts2021 These efforts are important because cEEGpatterns in the acutely ill are dynamic and requireprompt action However nonexpert CSA-basedscreening (without immediate visual confirmation)may yield more false alarms which might place addi-tional burdens on neurophysiologists charged withfollowing up on such alerts In the current studyconstant correlation of CSA patterns with the under-lying EEG was critical in achieving high sensitivityand efficiency and direct visual confirmation by atrained expert remains an essential step to determin-ing which cEEG patterns are significant rather thanartifactual or incidental
Our results are subject to several limitationsFirst our study is a single-center retrospectivereview and a larger multi-institutional prospectivetrial is needed to establish the validity and general-izability of our findings Second CSA cannot escapethe inherent limitations of scalp EEG including thefact that not all seizures may be detectable on scalpEEG For example exquisitely focal seizures maybe detectable only with invasive monitoring and
Figure 2 Time-savings group analysis
Comparison histograms of the time taken to review a given record with the assistance ofCSA (blue bars) and without (red) (A) All studies reviewed by readers AndashC using CSA guid-ance vs conventional review (B) All studies that contained seizures Studies were rankordered from the shortest to longest review time The average time to review 24 hours ofcEEG data when CSA was used was 8 (64) minutes whereas conventional review took 38(617) minutes on average (A) These were statistically different between the groups (p
0005) (B) If seizures were present time savings was more marked CSA review 10(64) minutes and conventional 44 (620) minutes (p 0005) The figure is truncated at60 minutes For 14 studies reading with conventional review took more than 60 minutesTimes to review for these outliers were 622 623 635 636 637 646 652 660 673716 724 750 958 and 1016 in chart A and 958 750 724 716 673 652 646636 635 623 and 622 in chart B Times to review were normalized to a standard dura-tion of 24 hours of cEEG ie all reported times are expressed as time spent per 24 hours ofEEG data cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 61
seizure activity of low amplitude frequency orduration or seizures in the presence of ldquomalig-nantrdquo-appearing background activity may be diffi-cult to discern even on careful inspection of the rawcEEG Third while our results suggest that patternsmeeting the strict definition of definite electro-graphic seizures24 can be identified readily border-zone rhythmic and periodic EEG patterns failing toqualify as definite electrographic seizures may nev-ertheless be symptomatic and require treatment insome cases Determination of the clinical signifi-cance of such cases is possible only by clinical cor-relation eg to determine whether the pattern inquestion reliably correlates with signssymptomsand whether the patient improves with treatmentIn such cases CSA-guided review may not signifi-cantly reduce the total time required for interpreta-tion Fourth it should be emphasized that ourestimate of approximately 75 time savings appliesonly to the part of EEG review after careful directconventional visual analysis of the initial 30 minutesof data As stated above there are reasons to believethat the familiarity with the cEEG provided by thisinitial review is critical to both time savings andsensitivity of subsequent CSA-guided screeningFifth not all centers have access to software or read-ing stations such as those used to view CSA in thisstudy However such centers may be less likely toperform large-scale cEEG and may thus be betterable to review their studies without relying on CSA-based screening Sixth some centers employ dedi-cated technicians to monitor and screen for seizures
allowing physicians to focus only on suspicious seg-ments perhaps obviating the advantage (for physi-cians) of CSA-guided review Seventh some centersemploy screening of CSA (andor other measures)by nurses and electroneurodiagnostic technologistsfollowed by page-by-page EEG review by a physi-cian in fellowship training or another electroneur-odiagnostic technician followed by complete ortargeted review by an attending-level neurophysiol-ogist This approach of triple EEG review whiletime-consuming and resource-intensive is arguablythe least likely to miss any significant findingsFurther outcome-oriented research is needed todetermine the optimal approach among these alter-natives Eighth it must be emphasized that theCSA-guided review protocol proposed here is notintended as a substitute for visual review by trainedexpert clinicians and indeed expert visual review ofprimary cEEG data is an indispensable componentof the present CSA-guided protocol Lastly the re-sults of the present study apply only in the criticalcare setting They have no obvious direct relevanceto diagnostic long-term video EEG monitoring forassessment of chronic epilepsy particularly for thepresurgical workup In such patients interictalspikes may be infrequent but very clinically impor-tant necessitating careful time-consuming visualsearch and patients may undergo days of cEEGrecording to detect even a small number of seizureson which neurosurgical decisions are based In thissetting missing one seizure can have significantclinical consequences
Figure 3 Sensitivity analysis for seizures and other abnormal patterns
The overall sensitivity of CSA-guided review and conventional review of reviewers AndashC is shown relative to the gold-standard findings of readers D and E seizures 873 (10411192) PDs 100 (4343) RDA 971 (3435) FS987 (7677) GS 100 (100100) and EDs 885 (6170) By definition the gold-standard conventional review groupdetected 100 of all seizures and common abnormal patterns CSA 5 compressed spectral array ED 5 epileptiformdischarge FS 5 focal slowing GS 5 generalized slowing PD 5 periodic epileptiform discharge RDA 5 rhythmic deltaactivity
62 Neurology 83 July 1 2014
Finally it remains to be determined whether thetime savings achievable by CSA-guided review ismeaningful in either clinical or cost-effectivenessterms In many cases initial identification of EEGevents represents only one part of providing criticalcare cEEG services Other responsibilities whichmay be even more time-consuming include clinicalcorrelation of EEG findings including bedside exam-ination as needed to determine their significanceevaluation of changes in medications frequent com-munication with clinical teams to report findingsand to make EEG-related management recommenda-tions and writing EEG reports Nevertheless if vali-dated our results may justify replacing at least thefront-line conventional page-by-page EEG reviewarguably the most time-sensitive stage of EEG analy-sis by the more efficient CSA-based screening proce-dure presented herein
Our results suggest that CSA-guided cEEG reviewcan enable significantly faster interpretation withoutsubstantial loss of sensitivity for critical findings in thevast majority of cases While intensive care unit out-come measures were not explored in this study thedemonstration that CSA-guided review enables rapid
and accurate evaluation of critical EEG findings (suchas the presence of seizures or nonconvulsive status epi-lepticus) suggests that this protocol may positively affectpatient care by allowing more timely management de-cisions in response to critical cEEG events
AUTHOR CONTRIBUTIONSLMVRM MMS and MBW conceptualized and designed the study
LMVRM (MGH clinical neurophysiology fellow) and MBW (faculty
with the MGH Epilepsy Service) completed the statistical analysis LMV
RM MMS and MBW drafted the original manuscript LMVRM
SP and MN contributed to the data production and collection SSC
AJC DBH MMS ESR and MBW reviewed and revised the
manuscript
STUDY FUNDINGNo targeted funding reported
DISCLOSUREL Moura reports no disclosures relevant to the manuscript M Shafi
received support from Harvard Catalyst KL2 MeRIT program M Ng
and S Pati report no disclosures relevant to the manuscript S Cash
A Cole and D Hoch received support from NIHNeurological Disor-
ders and Stroke NS062092 E Rosenthal reports no disclosures relevant
to the manuscript M Westover received support from the American
Brain Foundation Go to Neurologyorg for full disclosures
Received May 22 2013 Accepted in final form March 25 2014
Figure 4 CSA display obscured by artifact
Top screen Two-hour segments of CSA display as described in figure 3 Bottom screen Raw cEEG data as described infigure 3 cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 63
REFERENCES1 Vespa PM Nuwer MR Juhaacutesz C et al Early detection of
vasospasm after acute subarachnoid hemorrhage using con-
tinuous EEG ICU monitoring Electroencephalogr Clin
Neurophysiol 1997103607ndash615
2 Schreiber JM Zelleke T Gaillard WD et al Continuous
video EEG for patients with acute encephalopathy in a
pediatric intensive care unit Neurocrit Care 201217
31ndash38
3 Pandian JD Cascino GD So EL et al Digital video-
electroencephalographic monitoring in the neurological-
neurosurgical intensive care unit Arch Neurol 200461
1090ndash1094
4 Cloostermans MC Van Meulen FB Eertman CJ et al
Continuous electroencephalography monitoring for early
prediction of neurological outcome in postanoxic patients
after cardiac arrest a prospective cohort study Crit Care
Med 2012402867ndash2875
5 Rudin D Grize L Schindler C et al High prevalence of
nonconvulsive and subtle status epilepticus in an ICU of a
tertiary care center a three-year observational cohort
study Epilepsy Res 201196140ndash150
6 Young GB Doig GS Continuous EEG monitoring in
comatose intensive care patients epileptiform activity in
etiologically distinct groups Neurocrit Care 200525ndash10
7 Young GB Continuous EEG monitoring in the ICU
Acta Neurol Scand 200611467ndash68
8 Claassen J Mayer SA Kowalski RG et al Detection of
electrographic seizures with continuous EEG monitoring
in critically ill patients Neurology 2004621743ndash1748
9 Vespa PM Nuwer MR Nenov V et al Increased inci-
dence and impact of nonconvulsive and convulsive seizures
after traumatic brain injury as detected by continuous elec-
troencephalographic monitoring J Neurosurg 199991
750ndash760
10 Towne AR Waterhouse EJ Boggs JG et al Prevalence of
nonconvulsive status epilepticus in comatose patients
Neurology 200054340ndash345
11 Talwar D Torres F Continuous electrophysiologic mon-
itoring of cerebral function in the pediatric intensive care
unit Pediatr Neurol 19884137ndash147
12 Claassen J Hirsch LJ Kreiter KT et al Quantitative con-
tinuous EEG for detecting delayed cerebral ischemia in
patients with poor-grade subarachnoid hemorrhage Clin
Neurophysiol 20041152699ndash2710
13 Carrera E Claassen J Oddo M et al Continuous electroen-
cephalographic monitoring in critically ill patients with central
nervous system infections Arch Neurol 2008651612ndash1618
14 Sutter R Fuhr P Grize L et al Continuous video-EEG
monitoring increases detection rate of nonconvulsive status
epilepticus in the ICU Epilepsia 201152453ndash457
15 Claassen J Hirsch LJ Frontera JA et al Prognostic sig-
nificance of continuous EEG monitoring in patients with
poor-grade subarachnoid hemorrhage Neurocrit Care
20064103ndash112
16 Nuwer MR Quantitative EEG analysis in clinical settings
Brain Topogr 19968201ndash208
17 Nuwer M Assessment of digital EEG quantitative EEG
and EEG brain mapping report of the American Academy
of Neurology and the American Clinical Neurophysiology
Society Neurology 199749277ndash292
18 Shah AK Agarwal R Carhuapoma JR Loeb JA Com-
pressed EEG pattern analysis for critically ill
neurological-neurosurgical patients Neurocrit Care
20065124ndash133
19 Bricolo A Turazzi S Faccioli F et al Clinical application
of compressed spectral array in long-term EEG monitoring
of comatose patients Electroencephalogr Clin Neurophy-
siol 197845211ndash225
20 Stewart CP Otsubo H Ochi A et al Seizure identification in
the ICU using quantitative EEG displays Neurology 2010
751501ndash1508
21 Hirsch LJ LaRoche SM Gaspard N et al American Clin-
ical Neurophysiology Societyrsquos Standardized Critical Care
EEG Terminology 2012 version J Clin Neurophysiol
2013301ndash27
22 Abend NS Dlugos D Herman S Neonatal seizure detec-
tion using multichannel display of envelope trend Epilep-
sia 200849349ndash352
23 Williamson CA Wahlster S Shafi MM Westover MB
Sensitivity of compressed spectral arrays for detecting seiz-
ures in acutely ill adults Neurocrit Care 20142032ndash39
24 Young GB Jordan KG Doig GS An assessment of non-
convulsive seizures in the intensive care unit using contin-
uous EEG monitoring an investigation of variables
associated with mortality Neurology 19964783ndash89
Free Michael J Fox DVD Video on Parkinsonrsquos DiseaseThe AAN and the American Brain Foundation present actor and Parkinsonrsquos disease patientMichael J Fox hosting Parkinsonrsquos Disease A Guide for Patients and Families This new patienteducation video is now available free to members and the public either on DVD or online Thefree DVD can be ordered while supplies last by visiting AANcomviewPatientEducationVideos orcalling (800) 879-1960 The video can be viewed online at YouTubecomAANChannel with otherpatient education DVDs produced by the AAN
64 Neurology 83 July 1 2014
DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
ServicesUpdated Information amp
httpwwwneurologyorgcontent83156fullhtmlincluding high resolution figures can be found at
Supplementary Material
00000000537DC1htmlhttpwwwneurologyorgcontentsuppl20140629WNL00000Supplementary material can be found at
References
httpwwwneurologyorgcontent83156fullhtmlref-list-1at This article cites 24 articles 5 of which you can access for free
Subspecialty Collections
httpwwwneurologyorgcgicollectionhealth_care_reformHealth care reform
reshttpwwwneurologyorgcgicollectioneeg_see_epilepsy-seizuEEG see EpilepsySeizures
httpwwwneurologyorgcgicollectioncritical_careCritical carefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

100 (4343) rhythmic delta activity 971 (3435)focal slowing 987 (7677) generalized slowing100 (100100) and epileptiform discharges 885(6170) No cases of ESE went undetected by CSA-guided review (table 1) all seizures lasting5 minuteswere detected and in cases of ESE without any seizureslasting 5 minutes the lowest seizure detection ratewas 86 (95111)
Excluding cases with ESE due to prolonged (5-minute) seizures (of which all were detected seeabove) we found an inverse relationship betweennumber of seizures per cEEG and number of missedseizures (more seizures were missed in EEGs withhigher total seizure counts Pearson correlation coef-ficient 073 p 5 00001) In addition dividing the21 cases without ESE into cases with brief (averageduration 1 minute) vs longer seizures we foundthat the mean percentage of missed seizures was twiceas high in the group with brief seizures 13 (SD 22)vs 65 (SD 12) respectively (t test p 5 001)
Differences in detection rates for seizures andother patterns between readers in the CSA-guidedreview group were modest and not clinically signifi-cant (table e-3) A detailed discussion of differencesbetween detection performance characteristics among
reviewers A B and C in the CSA-guided reviewgroup is provided in the online supplemental material(section C) An example of the CSA display obscuredby artifact is provided in figure 4
There was no significant correlation between sei-zure detection sensitivity (CSA protocol) and timeto review 24 hours of cEEG (Spearman r R2 [40]013 p 5 041) suggesting that CSA-guided re-viewers adjusted review time on a case-by-case basisto maintain sensitivity In addition linear regressionof the time to review each file as a function of theordering in which cEEG was reviewed by a particularreader revealed no significant trend suggesting thatthe time to review a cEEG study was stable for eachreader throughout the study
DISCUSSION The main finding of this study is thatCSA-based screening of cEEG recordings inhospitalized adults can substantially reduce averagereview time without significantly sacrificingsensitivity for seizures and other critical findingsrelative to conventional page-by-page review CSA-guided screening identified 100 of cEEGrecordings containing seizures all cases of ESE andtended to miss seizures only in records with
Figure 1 CSA display
Top screen Two-hour segments of CSA power data were displayed from top to bottom in a spectrogrammontage There arebrief periods with increased power in the high-frequency band over the left hemisphere highlighting suspicious regions Bot-tom screen Raw cEEG data cEEG 5 continuous EEG CSA 5 compressed spectral array
58 Neurology 83 July 1 2014
Table 1 Descriptive statistics for patients with seizures
Patient No of seizures No detected Detected No missed Missed Min duration Mean duration Max duration Max rate Min ISI Max ESE present ESE detected
1 1 1 100 0 0 05 05 05 1 mdash 1
2 1 1 100 0 0 9408 9408 9408 1 mdash 100 X X
3 1 1 100 0 0 21 21 21 1 mdash 4
4 1 1 100 0 0 18 18 18 1 mdash 3
5 1 1 100 0 0 184 184 184 1 mdash 31 X X
6 1 1 100 0 0 22 22 22 1 mdash 4
7 1 1 100 0 0 03 03 03 1 mdash 1
8 2 2 100 0 0 100 124 147 1 900 25 X X
9 2 2 100 0 0 05 06 06 1 1200 1
10 3 2 67 1 33 11 11 19 1 350 0
11 3 1 33 2 67 02 04 10 1 620 1
12 3 3 100 0 0 03 19 35 2 300 6
13 3 3 100 0 0 04 04 05 1 700 1
14 3 3 100 0 0 01 01 134 1 50 3 X X
15 4 3 75 1 25 03 04 05 3 200 3
16 8 8 100 0 0 08 13 18 4 150 11
17 9 6 67 3 33 06 41 71 1 660 12 X X
18 10 10 100 0 0 03 04 09 9 67 7
19 14 11 79 3 21 07 06 111 3 200 100 X X
20 14 14 100 0 0 04 22 89 7 86 15 X X
21 20 12 60 8 40 10 1123 9124 4 150 100 X X
22 23 22 96 1 4 04 17 73 6 100 16 X X
23 25 15 60 10 40 05 05 27 7 86 1
24 28 27 96 1 4 04 06 07 2 300 2
25 28 20 71 8 29 09 22 22 3 200 4
26 29 14 48 15 52 04 20 68 5 120 29 X X
27 30 28 93 2 7 25 48 69 3 200 31 X X
28 33 33 100 0 0 02 04 07 6 100 2
29 37 36 97 1 3 10 12 14 4 150 4
30 46 46 100 0 0 10 19 19 5 120 3
31 47 47 100 0 0 08 11 15 5 120 2
32 48 48 100 0 0 01 02 02 25 24 1 X X
Continued
Neurology
83
July12
014
59
multiple seizures attaining an overall detection rate of87 in 25 of the time required for conventionalreview This finding was established in a largecollection of unselected recordings from patientswith a broad range of neurologic conditionsMoreover the cEEG review procedure was clinicallypractical Our data suggest that CSA-guided reviewis an acceptable alternative to the current standardpractice of page-by-page review of all data for cEEGmonitoring in critically ill adults
In the minority of cases in which CSA-guidedreview missed seizures misses tended to represent asmall fraction of a high seizure burden Missed seiz-ures also tended to occur more often in patients withbriefer seizures We speculate that misses can be ex-plained in part by the intrinsic difficulty of drawinga line between patterns on the ldquoictal-interictal contin-uumrdquo and ldquodefinite seizuresrdquo Efforts to increase in-terrater agreement on seizure patterns may furtherimprove performance of CSA-guided review
Our findings in adults are similar to those ofsmaller studies in pediatric populations1820 Onestudy using CSA and amplitude-integrated EEG in23 pediatric cEEGs (17 with seizures 10 without)found a sensitivity for seizure detection with CSA of83320 Another study in 8 neonates (26ndash44weeks) found that envelope trends enabled experi-enced users to detect 88 of prolonged seizureswhile detection rates for brief or slowly evolvingneonatal seizures were only 40 and 2022 sug-gesting that compressed EEG may be useful in somebut not all neonates In contrast with the presentstudy in both of these pediatric studies reviewerswere not permitted to correlate compressed datafindings with the primary EEG data This differencemay have contributed to lower detection sensitivitiesrelative to the present study
The present study investigated sensitivity and effi-ciency (time savings) of CSA as to guide cEEGreview placing minimal emphasis on specificity(low false-positive detection rates) This choicetreats CSA as a screening tool which cannot be per-formed without simultaneous review of raw cEEGdata rather than as a primary modality for cEEGinterpretation Suspicious CSA patterns must befrequently correlated with raw EEG data to distin-guish seizures from state changes periodic patternsand artifacts This back-and-forth dynamic allowscEEG review to be adaptive such that after an ini-tial careful correlation of raw cEEG with CSA pat-terns (including a careful visual analysis of thecEEG background) during the initial 30-minuteperiod reviewers are able to rapidly distinguishartifacts from true physiologic changes This initialreview enables subsequent review to proceed morequickly
Tab
le1
Con
tinu
ed
Pat
ient
No
ofse
izur
esNo
det
ecte
dDet
ecte
d
No
misse
dMisse
d
Min
dur
ation
Mea
ndur
ation
Max
dur
ation
Max
rate
Min
ISI
Max
ESE
pre
sent
ESE
det
ecte
d
33
53
52
98
12
02
40
154
12
50
27
XX
34
54
52
96
24
01
03
06
30
20
2X
X
35
57
20
35
37
65
02
86
2921
35
17
100
XX
36
76
74
97
23
15
25
34
16
38
13
XX
37
99
95
96
44
00
44
436
30
20
84
XX
38
111
95
86
16
14
02
07
30
19
32
15
XX
39
121
104
86
17
14
02
05
11
2242
2
40
151
132
87
19
13
01
13
29
21
29
21
XX
Abb
reviations
ESE
5elec
trog
raph
icstatus
epile
pticus
ISI5
interseizu
reinterval
Min
duration
5minim
umse
izure
duration
(inminutes
)max
duration
5max
imum
seizure
duration
(inminutes
)max
rate
5max
imum
numbe
rof
seizures
that
occu
rred
during
any
hour
ofmon
itoring
min
ISI5
minim
umav
erag
eISIfor
anyho
urdu
ring
mon
itoring
define
das
theminim
umav
erag
edu
ration
betw
eenco
nsec
utivese
izures
withinan
yho
urof
mon
itoring(in
patien
tswith1se
izure)m
ax
5max
imum
percen
tage
ofan
yho
urdu
ring
mon
itoringthat
was
occu
pied
byse
izureac
tivityP
atientsareso
rted
bynu
mbe
rof
seizures
that
occu
rred
during
mon
itoring
Detec
ted
andmisse
d
give
thepe
rcen
tage
ofse
izures
detected
ormisse
dby
compr
esse
dsp
ectral
arrayndash
guided
review
protoc
ol(relativeto
thepa
ge-by-pa
gereview
gold
stan
dard
)For
this
stud
yapa
tien
twas
said
toha
veESE
ifeither
(1)t
hemax
imum
seizuredu
ration
was
5
minutes
or(2)t
heminim
umho
urly
averag
eISIw
as5
minutes
60 Neurology 83 July 1 2014
In keeping with a prior study by our group23
CSA-guided review had excellent sensitivity for thepresence of other common critical ldquointerictalrdquo find-ings including focal (987) and generalized (100)slowing periodic discharges (100) and rhythmicdelta activity (971) compared with conventionalpage-by-page EEG review Similarly sensitivity forthe presence of sporadic epileptiform discharges wasreasonably high (885) The high sensitivity fornonseizure findings is not necessarily because these
patterns produce distinct CSA signatures For exam-ple epileptiform discharges being brief typicallyshow no obvious footprint in the 2-hour CSA displayused in our protocol Rather these patterns are abun-dant enough to be detected even by very limitedreview of the primary EEG data that occurs duringCSA-guided review
The early stage of cEEG training of the CSAreview group merits comment This selection of read-ers was intended to reflect the practice at many ter-tiary care centers of relying on clinical fellows formost first-line cEEG interpretation The use of train-ees might produce conservative estimates of sensitiv-ity as sensitivity should improve with experienceBy contrast our gold-standard EEG reviewers wereexperienced attending-level clinical EEGers to ensurevalidity of the gold standard
Our protocol relied on 2-hour CSA windowsWe chose to display 5 CSA panels (left and right lat-eral and parasagittal chains and hemispheric asym-metry spectrogram) Including additional CSApanels higher time resolution (eg 30-minute win-dows) and possibly other compressed-data formats(eg amplitude integrated EEG rhythmicity meas-ures) might have produced higher seizure detectionrates However increasing data volume might com-promise efficiency by producing cognitive overloadFurther research is necessary to determine whichquantitative EEG instruments alone and in combi-nation present the best cognitive match for humanEEG reviewers
Some have suggested that nurses EEG technolo-gists and residents can be trained to review CSA datato flag regions for direct review by physician ex-perts2021 These efforts are important because cEEGpatterns in the acutely ill are dynamic and requireprompt action However nonexpert CSA-basedscreening (without immediate visual confirmation)may yield more false alarms which might place addi-tional burdens on neurophysiologists charged withfollowing up on such alerts In the current studyconstant correlation of CSA patterns with the under-lying EEG was critical in achieving high sensitivityand efficiency and direct visual confirmation by atrained expert remains an essential step to determin-ing which cEEG patterns are significant rather thanartifactual or incidental
Our results are subject to several limitationsFirst our study is a single-center retrospectivereview and a larger multi-institutional prospectivetrial is needed to establish the validity and general-izability of our findings Second CSA cannot escapethe inherent limitations of scalp EEG including thefact that not all seizures may be detectable on scalpEEG For example exquisitely focal seizures maybe detectable only with invasive monitoring and
Figure 2 Time-savings group analysis
Comparison histograms of the time taken to review a given record with the assistance ofCSA (blue bars) and without (red) (A) All studies reviewed by readers AndashC using CSA guid-ance vs conventional review (B) All studies that contained seizures Studies were rankordered from the shortest to longest review time The average time to review 24 hours ofcEEG data when CSA was used was 8 (64) minutes whereas conventional review took 38(617) minutes on average (A) These were statistically different between the groups (p
0005) (B) If seizures were present time savings was more marked CSA review 10(64) minutes and conventional 44 (620) minutes (p 0005) The figure is truncated at60 minutes For 14 studies reading with conventional review took more than 60 minutesTimes to review for these outliers were 622 623 635 636 637 646 652 660 673716 724 750 958 and 1016 in chart A and 958 750 724 716 673 652 646636 635 623 and 622 in chart B Times to review were normalized to a standard dura-tion of 24 hours of cEEG ie all reported times are expressed as time spent per 24 hours ofEEG data cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 61
seizure activity of low amplitude frequency orduration or seizures in the presence of ldquomalig-nantrdquo-appearing background activity may be diffi-cult to discern even on careful inspection of the rawcEEG Third while our results suggest that patternsmeeting the strict definition of definite electro-graphic seizures24 can be identified readily border-zone rhythmic and periodic EEG patterns failing toqualify as definite electrographic seizures may nev-ertheless be symptomatic and require treatment insome cases Determination of the clinical signifi-cance of such cases is possible only by clinical cor-relation eg to determine whether the pattern inquestion reliably correlates with signssymptomsand whether the patient improves with treatmentIn such cases CSA-guided review may not signifi-cantly reduce the total time required for interpreta-tion Fourth it should be emphasized that ourestimate of approximately 75 time savings appliesonly to the part of EEG review after careful directconventional visual analysis of the initial 30 minutesof data As stated above there are reasons to believethat the familiarity with the cEEG provided by thisinitial review is critical to both time savings andsensitivity of subsequent CSA-guided screeningFifth not all centers have access to software or read-ing stations such as those used to view CSA in thisstudy However such centers may be less likely toperform large-scale cEEG and may thus be betterable to review their studies without relying on CSA-based screening Sixth some centers employ dedi-cated technicians to monitor and screen for seizures
allowing physicians to focus only on suspicious seg-ments perhaps obviating the advantage (for physi-cians) of CSA-guided review Seventh some centersemploy screening of CSA (andor other measures)by nurses and electroneurodiagnostic technologistsfollowed by page-by-page EEG review by a physi-cian in fellowship training or another electroneur-odiagnostic technician followed by complete ortargeted review by an attending-level neurophysiol-ogist This approach of triple EEG review whiletime-consuming and resource-intensive is arguablythe least likely to miss any significant findingsFurther outcome-oriented research is needed todetermine the optimal approach among these alter-natives Eighth it must be emphasized that theCSA-guided review protocol proposed here is notintended as a substitute for visual review by trainedexpert clinicians and indeed expert visual review ofprimary cEEG data is an indispensable componentof the present CSA-guided protocol Lastly the re-sults of the present study apply only in the criticalcare setting They have no obvious direct relevanceto diagnostic long-term video EEG monitoring forassessment of chronic epilepsy particularly for thepresurgical workup In such patients interictalspikes may be infrequent but very clinically impor-tant necessitating careful time-consuming visualsearch and patients may undergo days of cEEGrecording to detect even a small number of seizureson which neurosurgical decisions are based In thissetting missing one seizure can have significantclinical consequences
Figure 3 Sensitivity analysis for seizures and other abnormal patterns
The overall sensitivity of CSA-guided review and conventional review of reviewers AndashC is shown relative to the gold-standard findings of readers D and E seizures 873 (10411192) PDs 100 (4343) RDA 971 (3435) FS987 (7677) GS 100 (100100) and EDs 885 (6170) By definition the gold-standard conventional review groupdetected 100 of all seizures and common abnormal patterns CSA 5 compressed spectral array ED 5 epileptiformdischarge FS 5 focal slowing GS 5 generalized slowing PD 5 periodic epileptiform discharge RDA 5 rhythmic deltaactivity
62 Neurology 83 July 1 2014
Finally it remains to be determined whether thetime savings achievable by CSA-guided review ismeaningful in either clinical or cost-effectivenessterms In many cases initial identification of EEGevents represents only one part of providing criticalcare cEEG services Other responsibilities whichmay be even more time-consuming include clinicalcorrelation of EEG findings including bedside exam-ination as needed to determine their significanceevaluation of changes in medications frequent com-munication with clinical teams to report findingsand to make EEG-related management recommenda-tions and writing EEG reports Nevertheless if vali-dated our results may justify replacing at least thefront-line conventional page-by-page EEG reviewarguably the most time-sensitive stage of EEG analy-sis by the more efficient CSA-based screening proce-dure presented herein
Our results suggest that CSA-guided cEEG reviewcan enable significantly faster interpretation withoutsubstantial loss of sensitivity for critical findings in thevast majority of cases While intensive care unit out-come measures were not explored in this study thedemonstration that CSA-guided review enables rapid
and accurate evaluation of critical EEG findings (suchas the presence of seizures or nonconvulsive status epi-lepticus) suggests that this protocol may positively affectpatient care by allowing more timely management de-cisions in response to critical cEEG events
AUTHOR CONTRIBUTIONSLMVRM MMS and MBW conceptualized and designed the study
LMVRM (MGH clinical neurophysiology fellow) and MBW (faculty
with the MGH Epilepsy Service) completed the statistical analysis LMV
RM MMS and MBW drafted the original manuscript LMVRM
SP and MN contributed to the data production and collection SSC
AJC DBH MMS ESR and MBW reviewed and revised the
manuscript
STUDY FUNDINGNo targeted funding reported
DISCLOSUREL Moura reports no disclosures relevant to the manuscript M Shafi
received support from Harvard Catalyst KL2 MeRIT program M Ng
and S Pati report no disclosures relevant to the manuscript S Cash
A Cole and D Hoch received support from NIHNeurological Disor-
ders and Stroke NS062092 E Rosenthal reports no disclosures relevant
to the manuscript M Westover received support from the American
Brain Foundation Go to Neurologyorg for full disclosures
Received May 22 2013 Accepted in final form March 25 2014
Figure 4 CSA display obscured by artifact
Top screen Two-hour segments of CSA display as described in figure 3 Bottom screen Raw cEEG data as described infigure 3 cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 63
REFERENCES1 Vespa PM Nuwer MR Juhaacutesz C et al Early detection of
vasospasm after acute subarachnoid hemorrhage using con-
tinuous EEG ICU monitoring Electroencephalogr Clin
Neurophysiol 1997103607ndash615
2 Schreiber JM Zelleke T Gaillard WD et al Continuous
video EEG for patients with acute encephalopathy in a
pediatric intensive care unit Neurocrit Care 201217
31ndash38
3 Pandian JD Cascino GD So EL et al Digital video-
electroencephalographic monitoring in the neurological-
neurosurgical intensive care unit Arch Neurol 200461
1090ndash1094
4 Cloostermans MC Van Meulen FB Eertman CJ et al
Continuous electroencephalography monitoring for early
prediction of neurological outcome in postanoxic patients
after cardiac arrest a prospective cohort study Crit Care
Med 2012402867ndash2875
5 Rudin D Grize L Schindler C et al High prevalence of
nonconvulsive and subtle status epilepticus in an ICU of a
tertiary care center a three-year observational cohort
study Epilepsy Res 201196140ndash150
6 Young GB Doig GS Continuous EEG monitoring in
comatose intensive care patients epileptiform activity in
etiologically distinct groups Neurocrit Care 200525ndash10
7 Young GB Continuous EEG monitoring in the ICU
Acta Neurol Scand 200611467ndash68
8 Claassen J Mayer SA Kowalski RG et al Detection of
electrographic seizures with continuous EEG monitoring
in critically ill patients Neurology 2004621743ndash1748
9 Vespa PM Nuwer MR Nenov V et al Increased inci-
dence and impact of nonconvulsive and convulsive seizures
after traumatic brain injury as detected by continuous elec-
troencephalographic monitoring J Neurosurg 199991
750ndash760
10 Towne AR Waterhouse EJ Boggs JG et al Prevalence of
nonconvulsive status epilepticus in comatose patients
Neurology 200054340ndash345
11 Talwar D Torres F Continuous electrophysiologic mon-
itoring of cerebral function in the pediatric intensive care
unit Pediatr Neurol 19884137ndash147
12 Claassen J Hirsch LJ Kreiter KT et al Quantitative con-
tinuous EEG for detecting delayed cerebral ischemia in
patients with poor-grade subarachnoid hemorrhage Clin
Neurophysiol 20041152699ndash2710
13 Carrera E Claassen J Oddo M et al Continuous electroen-
cephalographic monitoring in critically ill patients with central
nervous system infections Arch Neurol 2008651612ndash1618
14 Sutter R Fuhr P Grize L et al Continuous video-EEG
monitoring increases detection rate of nonconvulsive status
epilepticus in the ICU Epilepsia 201152453ndash457
15 Claassen J Hirsch LJ Frontera JA et al Prognostic sig-
nificance of continuous EEG monitoring in patients with
poor-grade subarachnoid hemorrhage Neurocrit Care
20064103ndash112
16 Nuwer MR Quantitative EEG analysis in clinical settings
Brain Topogr 19968201ndash208
17 Nuwer M Assessment of digital EEG quantitative EEG
and EEG brain mapping report of the American Academy
of Neurology and the American Clinical Neurophysiology
Society Neurology 199749277ndash292
18 Shah AK Agarwal R Carhuapoma JR Loeb JA Com-
pressed EEG pattern analysis for critically ill
neurological-neurosurgical patients Neurocrit Care
20065124ndash133
19 Bricolo A Turazzi S Faccioli F et al Clinical application
of compressed spectral array in long-term EEG monitoring
of comatose patients Electroencephalogr Clin Neurophy-
siol 197845211ndash225
20 Stewart CP Otsubo H Ochi A et al Seizure identification in
the ICU using quantitative EEG displays Neurology 2010
751501ndash1508
21 Hirsch LJ LaRoche SM Gaspard N et al American Clin-
ical Neurophysiology Societyrsquos Standardized Critical Care
EEG Terminology 2012 version J Clin Neurophysiol
2013301ndash27
22 Abend NS Dlugos D Herman S Neonatal seizure detec-
tion using multichannel display of envelope trend Epilep-
sia 200849349ndash352
23 Williamson CA Wahlster S Shafi MM Westover MB
Sensitivity of compressed spectral arrays for detecting seiz-
ures in acutely ill adults Neurocrit Care 20142032ndash39
24 Young GB Jordan KG Doig GS An assessment of non-
convulsive seizures in the intensive care unit using contin-
uous EEG monitoring an investigation of variables
associated with mortality Neurology 19964783ndash89
Free Michael J Fox DVD Video on Parkinsonrsquos DiseaseThe AAN and the American Brain Foundation present actor and Parkinsonrsquos disease patientMichael J Fox hosting Parkinsonrsquos Disease A Guide for Patients and Families This new patienteducation video is now available free to members and the public either on DVD or online Thefree DVD can be ordered while supplies last by visiting AANcomviewPatientEducationVideos orcalling (800) 879-1960 The video can be viewed online at YouTubecomAANChannel with otherpatient education DVDs produced by the AAN
64 Neurology 83 July 1 2014
DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
ServicesUpdated Information amp
httpwwwneurologyorgcontent83156fullhtmlincluding high resolution figures can be found at
Supplementary Material
00000000537DC1htmlhttpwwwneurologyorgcontentsuppl20140629WNL00000Supplementary material can be found at
References
httpwwwneurologyorgcontent83156fullhtmlref-list-1at This article cites 24 articles 5 of which you can access for free
Subspecialty Collections
httpwwwneurologyorgcgicollectionhealth_care_reformHealth care reform
reshttpwwwneurologyorgcgicollectioneeg_see_epilepsy-seizuEEG see EpilepsySeizures
httpwwwneurologyorgcgicollectioncritical_careCritical carefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

Table 1 Descriptive statistics for patients with seizures
Patient No of seizures No detected Detected No missed Missed Min duration Mean duration Max duration Max rate Min ISI Max ESE present ESE detected
1 1 1 100 0 0 05 05 05 1 mdash 1
2 1 1 100 0 0 9408 9408 9408 1 mdash 100 X X
3 1 1 100 0 0 21 21 21 1 mdash 4
4 1 1 100 0 0 18 18 18 1 mdash 3
5 1 1 100 0 0 184 184 184 1 mdash 31 X X
6 1 1 100 0 0 22 22 22 1 mdash 4
7 1 1 100 0 0 03 03 03 1 mdash 1
8 2 2 100 0 0 100 124 147 1 900 25 X X
9 2 2 100 0 0 05 06 06 1 1200 1
10 3 2 67 1 33 11 11 19 1 350 0
11 3 1 33 2 67 02 04 10 1 620 1
12 3 3 100 0 0 03 19 35 2 300 6
13 3 3 100 0 0 04 04 05 1 700 1
14 3 3 100 0 0 01 01 134 1 50 3 X X
15 4 3 75 1 25 03 04 05 3 200 3
16 8 8 100 0 0 08 13 18 4 150 11
17 9 6 67 3 33 06 41 71 1 660 12 X X
18 10 10 100 0 0 03 04 09 9 67 7
19 14 11 79 3 21 07 06 111 3 200 100 X X
20 14 14 100 0 0 04 22 89 7 86 15 X X
21 20 12 60 8 40 10 1123 9124 4 150 100 X X
22 23 22 96 1 4 04 17 73 6 100 16 X X
23 25 15 60 10 40 05 05 27 7 86 1
24 28 27 96 1 4 04 06 07 2 300 2
25 28 20 71 8 29 09 22 22 3 200 4
26 29 14 48 15 52 04 20 68 5 120 29 X X
27 30 28 93 2 7 25 48 69 3 200 31 X X
28 33 33 100 0 0 02 04 07 6 100 2
29 37 36 97 1 3 10 12 14 4 150 4
30 46 46 100 0 0 10 19 19 5 120 3
31 47 47 100 0 0 08 11 15 5 120 2
32 48 48 100 0 0 01 02 02 25 24 1 X X
Continued
Neurology
83
July12
014
59
multiple seizures attaining an overall detection rate of87 in 25 of the time required for conventionalreview This finding was established in a largecollection of unselected recordings from patientswith a broad range of neurologic conditionsMoreover the cEEG review procedure was clinicallypractical Our data suggest that CSA-guided reviewis an acceptable alternative to the current standardpractice of page-by-page review of all data for cEEGmonitoring in critically ill adults
In the minority of cases in which CSA-guidedreview missed seizures misses tended to represent asmall fraction of a high seizure burden Missed seiz-ures also tended to occur more often in patients withbriefer seizures We speculate that misses can be ex-plained in part by the intrinsic difficulty of drawinga line between patterns on the ldquoictal-interictal contin-uumrdquo and ldquodefinite seizuresrdquo Efforts to increase in-terrater agreement on seizure patterns may furtherimprove performance of CSA-guided review
Our findings in adults are similar to those ofsmaller studies in pediatric populations1820 Onestudy using CSA and amplitude-integrated EEG in23 pediatric cEEGs (17 with seizures 10 without)found a sensitivity for seizure detection with CSA of83320 Another study in 8 neonates (26ndash44weeks) found that envelope trends enabled experi-enced users to detect 88 of prolonged seizureswhile detection rates for brief or slowly evolvingneonatal seizures were only 40 and 2022 sug-gesting that compressed EEG may be useful in somebut not all neonates In contrast with the presentstudy in both of these pediatric studies reviewerswere not permitted to correlate compressed datafindings with the primary EEG data This differencemay have contributed to lower detection sensitivitiesrelative to the present study
The present study investigated sensitivity and effi-ciency (time savings) of CSA as to guide cEEGreview placing minimal emphasis on specificity(low false-positive detection rates) This choicetreats CSA as a screening tool which cannot be per-formed without simultaneous review of raw cEEGdata rather than as a primary modality for cEEGinterpretation Suspicious CSA patterns must befrequently correlated with raw EEG data to distin-guish seizures from state changes periodic patternsand artifacts This back-and-forth dynamic allowscEEG review to be adaptive such that after an ini-tial careful correlation of raw cEEG with CSA pat-terns (including a careful visual analysis of thecEEG background) during the initial 30-minuteperiod reviewers are able to rapidly distinguishartifacts from true physiologic changes This initialreview enables subsequent review to proceed morequickly
Tab
le1
Con
tinu
ed
Pat
ient
No
ofse
izur
esNo
det
ecte
dDet
ecte
d
No
misse
dMisse
d
Min
dur
ation
Mea
ndur
ation
Max
dur
ation
Max
rate
Min
ISI
Max
ESE
pre
sent
ESE
det
ecte
d
33
53
52
98
12
02
40
154
12
50
27
XX
34
54
52
96
24
01
03
06
30
20
2X
X
35
57
20
35
37
65
02
86
2921
35
17
100
XX
36
76
74
97
23
15
25
34
16
38
13
XX
37
99
95
96
44
00
44
436
30
20
84
XX
38
111
95
86
16
14
02
07
30
19
32
15
XX
39
121
104
86
17
14
02
05
11
2242
2
40
151
132
87
19
13
01
13
29
21
29
21
XX
Abb
reviations
ESE
5elec
trog
raph
icstatus
epile
pticus
ISI5
interseizu
reinterval
Min
duration
5minim
umse
izure
duration
(inminutes
)max
duration
5max
imum
seizure
duration
(inminutes
)max
rate
5max
imum
numbe
rof
seizures
that
occu
rred
during
any
hour
ofmon
itoring
min
ISI5
minim
umav
erag
eISIfor
anyho
urdu
ring
mon
itoring
define
das
theminim
umav
erag
edu
ration
betw
eenco
nsec
utivese
izures
withinan
yho
urof
mon
itoring(in
patien
tswith1se
izure)m
ax
5max
imum
percen
tage
ofan
yho
urdu
ring
mon
itoringthat
was
occu
pied
byse
izureac
tivityP
atientsareso
rted
bynu
mbe
rof
seizures
that
occu
rred
during
mon
itoring
Detec
ted
andmisse
d
give
thepe
rcen
tage
ofse
izures
detected
ormisse
dby
compr
esse
dsp
ectral
arrayndash
guided
review
protoc
ol(relativeto
thepa
ge-by-pa
gereview
gold
stan
dard
)For
this
stud
yapa
tien
twas
said
toha
veESE
ifeither
(1)t
hemax
imum
seizuredu
ration
was
5
minutes
or(2)t
heminim
umho
urly
averag
eISIw
as5
minutes
60 Neurology 83 July 1 2014
In keeping with a prior study by our group23
CSA-guided review had excellent sensitivity for thepresence of other common critical ldquointerictalrdquo find-ings including focal (987) and generalized (100)slowing periodic discharges (100) and rhythmicdelta activity (971) compared with conventionalpage-by-page EEG review Similarly sensitivity forthe presence of sporadic epileptiform discharges wasreasonably high (885) The high sensitivity fornonseizure findings is not necessarily because these
patterns produce distinct CSA signatures For exam-ple epileptiform discharges being brief typicallyshow no obvious footprint in the 2-hour CSA displayused in our protocol Rather these patterns are abun-dant enough to be detected even by very limitedreview of the primary EEG data that occurs duringCSA-guided review
The early stage of cEEG training of the CSAreview group merits comment This selection of read-ers was intended to reflect the practice at many ter-tiary care centers of relying on clinical fellows formost first-line cEEG interpretation The use of train-ees might produce conservative estimates of sensitiv-ity as sensitivity should improve with experienceBy contrast our gold-standard EEG reviewers wereexperienced attending-level clinical EEGers to ensurevalidity of the gold standard
Our protocol relied on 2-hour CSA windowsWe chose to display 5 CSA panels (left and right lat-eral and parasagittal chains and hemispheric asym-metry spectrogram) Including additional CSApanels higher time resolution (eg 30-minute win-dows) and possibly other compressed-data formats(eg amplitude integrated EEG rhythmicity meas-ures) might have produced higher seizure detectionrates However increasing data volume might com-promise efficiency by producing cognitive overloadFurther research is necessary to determine whichquantitative EEG instruments alone and in combi-nation present the best cognitive match for humanEEG reviewers
Some have suggested that nurses EEG technolo-gists and residents can be trained to review CSA datato flag regions for direct review by physician ex-perts2021 These efforts are important because cEEGpatterns in the acutely ill are dynamic and requireprompt action However nonexpert CSA-basedscreening (without immediate visual confirmation)may yield more false alarms which might place addi-tional burdens on neurophysiologists charged withfollowing up on such alerts In the current studyconstant correlation of CSA patterns with the under-lying EEG was critical in achieving high sensitivityand efficiency and direct visual confirmation by atrained expert remains an essential step to determin-ing which cEEG patterns are significant rather thanartifactual or incidental
Our results are subject to several limitationsFirst our study is a single-center retrospectivereview and a larger multi-institutional prospectivetrial is needed to establish the validity and general-izability of our findings Second CSA cannot escapethe inherent limitations of scalp EEG including thefact that not all seizures may be detectable on scalpEEG For example exquisitely focal seizures maybe detectable only with invasive monitoring and
Figure 2 Time-savings group analysis
Comparison histograms of the time taken to review a given record with the assistance ofCSA (blue bars) and without (red) (A) All studies reviewed by readers AndashC using CSA guid-ance vs conventional review (B) All studies that contained seizures Studies were rankordered from the shortest to longest review time The average time to review 24 hours ofcEEG data when CSA was used was 8 (64) minutes whereas conventional review took 38(617) minutes on average (A) These were statistically different between the groups (p
0005) (B) If seizures were present time savings was more marked CSA review 10(64) minutes and conventional 44 (620) minutes (p 0005) The figure is truncated at60 minutes For 14 studies reading with conventional review took more than 60 minutesTimes to review for these outliers were 622 623 635 636 637 646 652 660 673716 724 750 958 and 1016 in chart A and 958 750 724 716 673 652 646636 635 623 and 622 in chart B Times to review were normalized to a standard dura-tion of 24 hours of cEEG ie all reported times are expressed as time spent per 24 hours ofEEG data cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 61
seizure activity of low amplitude frequency orduration or seizures in the presence of ldquomalig-nantrdquo-appearing background activity may be diffi-cult to discern even on careful inspection of the rawcEEG Third while our results suggest that patternsmeeting the strict definition of definite electro-graphic seizures24 can be identified readily border-zone rhythmic and periodic EEG patterns failing toqualify as definite electrographic seizures may nev-ertheless be symptomatic and require treatment insome cases Determination of the clinical signifi-cance of such cases is possible only by clinical cor-relation eg to determine whether the pattern inquestion reliably correlates with signssymptomsand whether the patient improves with treatmentIn such cases CSA-guided review may not signifi-cantly reduce the total time required for interpreta-tion Fourth it should be emphasized that ourestimate of approximately 75 time savings appliesonly to the part of EEG review after careful directconventional visual analysis of the initial 30 minutesof data As stated above there are reasons to believethat the familiarity with the cEEG provided by thisinitial review is critical to both time savings andsensitivity of subsequent CSA-guided screeningFifth not all centers have access to software or read-ing stations such as those used to view CSA in thisstudy However such centers may be less likely toperform large-scale cEEG and may thus be betterable to review their studies without relying on CSA-based screening Sixth some centers employ dedi-cated technicians to monitor and screen for seizures
allowing physicians to focus only on suspicious seg-ments perhaps obviating the advantage (for physi-cians) of CSA-guided review Seventh some centersemploy screening of CSA (andor other measures)by nurses and electroneurodiagnostic technologistsfollowed by page-by-page EEG review by a physi-cian in fellowship training or another electroneur-odiagnostic technician followed by complete ortargeted review by an attending-level neurophysiol-ogist This approach of triple EEG review whiletime-consuming and resource-intensive is arguablythe least likely to miss any significant findingsFurther outcome-oriented research is needed todetermine the optimal approach among these alter-natives Eighth it must be emphasized that theCSA-guided review protocol proposed here is notintended as a substitute for visual review by trainedexpert clinicians and indeed expert visual review ofprimary cEEG data is an indispensable componentof the present CSA-guided protocol Lastly the re-sults of the present study apply only in the criticalcare setting They have no obvious direct relevanceto diagnostic long-term video EEG monitoring forassessment of chronic epilepsy particularly for thepresurgical workup In such patients interictalspikes may be infrequent but very clinically impor-tant necessitating careful time-consuming visualsearch and patients may undergo days of cEEGrecording to detect even a small number of seizureson which neurosurgical decisions are based In thissetting missing one seizure can have significantclinical consequences
Figure 3 Sensitivity analysis for seizures and other abnormal patterns
The overall sensitivity of CSA-guided review and conventional review of reviewers AndashC is shown relative to the gold-standard findings of readers D and E seizures 873 (10411192) PDs 100 (4343) RDA 971 (3435) FS987 (7677) GS 100 (100100) and EDs 885 (6170) By definition the gold-standard conventional review groupdetected 100 of all seizures and common abnormal patterns CSA 5 compressed spectral array ED 5 epileptiformdischarge FS 5 focal slowing GS 5 generalized slowing PD 5 periodic epileptiform discharge RDA 5 rhythmic deltaactivity
62 Neurology 83 July 1 2014
Finally it remains to be determined whether thetime savings achievable by CSA-guided review ismeaningful in either clinical or cost-effectivenessterms In many cases initial identification of EEGevents represents only one part of providing criticalcare cEEG services Other responsibilities whichmay be even more time-consuming include clinicalcorrelation of EEG findings including bedside exam-ination as needed to determine their significanceevaluation of changes in medications frequent com-munication with clinical teams to report findingsand to make EEG-related management recommenda-tions and writing EEG reports Nevertheless if vali-dated our results may justify replacing at least thefront-line conventional page-by-page EEG reviewarguably the most time-sensitive stage of EEG analy-sis by the more efficient CSA-based screening proce-dure presented herein
Our results suggest that CSA-guided cEEG reviewcan enable significantly faster interpretation withoutsubstantial loss of sensitivity for critical findings in thevast majority of cases While intensive care unit out-come measures were not explored in this study thedemonstration that CSA-guided review enables rapid
and accurate evaluation of critical EEG findings (suchas the presence of seizures or nonconvulsive status epi-lepticus) suggests that this protocol may positively affectpatient care by allowing more timely management de-cisions in response to critical cEEG events
AUTHOR CONTRIBUTIONSLMVRM MMS and MBW conceptualized and designed the study
LMVRM (MGH clinical neurophysiology fellow) and MBW (faculty
with the MGH Epilepsy Service) completed the statistical analysis LMV
RM MMS and MBW drafted the original manuscript LMVRM
SP and MN contributed to the data production and collection SSC
AJC DBH MMS ESR and MBW reviewed and revised the
manuscript
STUDY FUNDINGNo targeted funding reported
DISCLOSUREL Moura reports no disclosures relevant to the manuscript M Shafi
received support from Harvard Catalyst KL2 MeRIT program M Ng
and S Pati report no disclosures relevant to the manuscript S Cash
A Cole and D Hoch received support from NIHNeurological Disor-
ders and Stroke NS062092 E Rosenthal reports no disclosures relevant
to the manuscript M Westover received support from the American
Brain Foundation Go to Neurologyorg for full disclosures
Received May 22 2013 Accepted in final form March 25 2014
Figure 4 CSA display obscured by artifact
Top screen Two-hour segments of CSA display as described in figure 3 Bottom screen Raw cEEG data as described infigure 3 cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 63
REFERENCES1 Vespa PM Nuwer MR Juhaacutesz C et al Early detection of
vasospasm after acute subarachnoid hemorrhage using con-
tinuous EEG ICU monitoring Electroencephalogr Clin
Neurophysiol 1997103607ndash615
2 Schreiber JM Zelleke T Gaillard WD et al Continuous
video EEG for patients with acute encephalopathy in a
pediatric intensive care unit Neurocrit Care 201217
31ndash38
3 Pandian JD Cascino GD So EL et al Digital video-
electroencephalographic monitoring in the neurological-
neurosurgical intensive care unit Arch Neurol 200461
1090ndash1094
4 Cloostermans MC Van Meulen FB Eertman CJ et al
Continuous electroencephalography monitoring for early
prediction of neurological outcome in postanoxic patients
after cardiac arrest a prospective cohort study Crit Care
Med 2012402867ndash2875
5 Rudin D Grize L Schindler C et al High prevalence of
nonconvulsive and subtle status epilepticus in an ICU of a
tertiary care center a three-year observational cohort
study Epilepsy Res 201196140ndash150
6 Young GB Doig GS Continuous EEG monitoring in
comatose intensive care patients epileptiform activity in
etiologically distinct groups Neurocrit Care 200525ndash10
7 Young GB Continuous EEG monitoring in the ICU
Acta Neurol Scand 200611467ndash68
8 Claassen J Mayer SA Kowalski RG et al Detection of
electrographic seizures with continuous EEG monitoring
in critically ill patients Neurology 2004621743ndash1748
9 Vespa PM Nuwer MR Nenov V et al Increased inci-
dence and impact of nonconvulsive and convulsive seizures
after traumatic brain injury as detected by continuous elec-
troencephalographic monitoring J Neurosurg 199991
750ndash760
10 Towne AR Waterhouse EJ Boggs JG et al Prevalence of
nonconvulsive status epilepticus in comatose patients
Neurology 200054340ndash345
11 Talwar D Torres F Continuous electrophysiologic mon-
itoring of cerebral function in the pediatric intensive care
unit Pediatr Neurol 19884137ndash147
12 Claassen J Hirsch LJ Kreiter KT et al Quantitative con-
tinuous EEG for detecting delayed cerebral ischemia in
patients with poor-grade subarachnoid hemorrhage Clin
Neurophysiol 20041152699ndash2710
13 Carrera E Claassen J Oddo M et al Continuous electroen-
cephalographic monitoring in critically ill patients with central
nervous system infections Arch Neurol 2008651612ndash1618
14 Sutter R Fuhr P Grize L et al Continuous video-EEG
monitoring increases detection rate of nonconvulsive status
epilepticus in the ICU Epilepsia 201152453ndash457
15 Claassen J Hirsch LJ Frontera JA et al Prognostic sig-
nificance of continuous EEG monitoring in patients with
poor-grade subarachnoid hemorrhage Neurocrit Care
20064103ndash112
16 Nuwer MR Quantitative EEG analysis in clinical settings
Brain Topogr 19968201ndash208
17 Nuwer M Assessment of digital EEG quantitative EEG
and EEG brain mapping report of the American Academy
of Neurology and the American Clinical Neurophysiology
Society Neurology 199749277ndash292
18 Shah AK Agarwal R Carhuapoma JR Loeb JA Com-
pressed EEG pattern analysis for critically ill
neurological-neurosurgical patients Neurocrit Care
20065124ndash133
19 Bricolo A Turazzi S Faccioli F et al Clinical application
of compressed spectral array in long-term EEG monitoring
of comatose patients Electroencephalogr Clin Neurophy-
siol 197845211ndash225
20 Stewart CP Otsubo H Ochi A et al Seizure identification in
the ICU using quantitative EEG displays Neurology 2010
751501ndash1508
21 Hirsch LJ LaRoche SM Gaspard N et al American Clin-
ical Neurophysiology Societyrsquos Standardized Critical Care
EEG Terminology 2012 version J Clin Neurophysiol
2013301ndash27
22 Abend NS Dlugos D Herman S Neonatal seizure detec-
tion using multichannel display of envelope trend Epilep-
sia 200849349ndash352
23 Williamson CA Wahlster S Shafi MM Westover MB
Sensitivity of compressed spectral arrays for detecting seiz-
ures in acutely ill adults Neurocrit Care 20142032ndash39
24 Young GB Jordan KG Doig GS An assessment of non-
convulsive seizures in the intensive care unit using contin-
uous EEG monitoring an investigation of variables
associated with mortality Neurology 19964783ndash89
Free Michael J Fox DVD Video on Parkinsonrsquos DiseaseThe AAN and the American Brain Foundation present actor and Parkinsonrsquos disease patientMichael J Fox hosting Parkinsonrsquos Disease A Guide for Patients and Families This new patienteducation video is now available free to members and the public either on DVD or online Thefree DVD can be ordered while supplies last by visiting AANcomviewPatientEducationVideos orcalling (800) 879-1960 The video can be viewed online at YouTubecomAANChannel with otherpatient education DVDs produced by the AAN
64 Neurology 83 July 1 2014
DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
ServicesUpdated Information amp
httpwwwneurologyorgcontent83156fullhtmlincluding high resolution figures can be found at
Supplementary Material
00000000537DC1htmlhttpwwwneurologyorgcontentsuppl20140629WNL00000Supplementary material can be found at
References
httpwwwneurologyorgcontent83156fullhtmlref-list-1at This article cites 24 articles 5 of which you can access for free
Subspecialty Collections
httpwwwneurologyorgcgicollectionhealth_care_reformHealth care reform
reshttpwwwneurologyorgcgicollectioneeg_see_epilepsy-seizuEEG see EpilepsySeizures
httpwwwneurologyorgcgicollectioncritical_careCritical carefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

multiple seizures attaining an overall detection rate of87 in 25 of the time required for conventionalreview This finding was established in a largecollection of unselected recordings from patientswith a broad range of neurologic conditionsMoreover the cEEG review procedure was clinicallypractical Our data suggest that CSA-guided reviewis an acceptable alternative to the current standardpractice of page-by-page review of all data for cEEGmonitoring in critically ill adults
In the minority of cases in which CSA-guidedreview missed seizures misses tended to represent asmall fraction of a high seizure burden Missed seiz-ures also tended to occur more often in patients withbriefer seizures We speculate that misses can be ex-plained in part by the intrinsic difficulty of drawinga line between patterns on the ldquoictal-interictal contin-uumrdquo and ldquodefinite seizuresrdquo Efforts to increase in-terrater agreement on seizure patterns may furtherimprove performance of CSA-guided review
Our findings in adults are similar to those ofsmaller studies in pediatric populations1820 Onestudy using CSA and amplitude-integrated EEG in23 pediatric cEEGs (17 with seizures 10 without)found a sensitivity for seizure detection with CSA of83320 Another study in 8 neonates (26ndash44weeks) found that envelope trends enabled experi-enced users to detect 88 of prolonged seizureswhile detection rates for brief or slowly evolvingneonatal seizures were only 40 and 2022 sug-gesting that compressed EEG may be useful in somebut not all neonates In contrast with the presentstudy in both of these pediatric studies reviewerswere not permitted to correlate compressed datafindings with the primary EEG data This differencemay have contributed to lower detection sensitivitiesrelative to the present study
The present study investigated sensitivity and effi-ciency (time savings) of CSA as to guide cEEGreview placing minimal emphasis on specificity(low false-positive detection rates) This choicetreats CSA as a screening tool which cannot be per-formed without simultaneous review of raw cEEGdata rather than as a primary modality for cEEGinterpretation Suspicious CSA patterns must befrequently correlated with raw EEG data to distin-guish seizures from state changes periodic patternsand artifacts This back-and-forth dynamic allowscEEG review to be adaptive such that after an ini-tial careful correlation of raw cEEG with CSA pat-terns (including a careful visual analysis of thecEEG background) during the initial 30-minuteperiod reviewers are able to rapidly distinguishartifacts from true physiologic changes This initialreview enables subsequent review to proceed morequickly
Tab
le1
Con
tinu
ed
Pat
ient
No
ofse
izur
esNo
det
ecte
dDet
ecte
d
No
misse
dMisse
d
Min
dur
ation
Mea
ndur
ation
Max
dur
ation
Max
rate
Min
ISI
Max
ESE
pre
sent
ESE
det
ecte
d
33
53
52
98
12
02
40
154
12
50
27
XX
34
54
52
96
24
01
03
06
30
20
2X
X
35
57
20
35
37
65
02
86
2921
35
17
100
XX
36
76
74
97
23
15
25
34
16
38
13
XX
37
99
95
96
44
00
44
436
30
20
84
XX
38
111
95
86
16
14
02
07
30
19
32
15
XX
39
121
104
86
17
14
02
05
11
2242
2
40
151
132
87
19
13
01
13
29
21
29
21
XX
Abb
reviations
ESE
5elec
trog
raph
icstatus
epile
pticus
ISI5
interseizu
reinterval
Min
duration
5minim
umse
izure
duration
(inminutes
)max
duration
5max
imum
seizure
duration
(inminutes
)max
rate
5max
imum
numbe
rof
seizures
that
occu
rred
during
any
hour
ofmon
itoring
min
ISI5
minim
umav
erag
eISIfor
anyho
urdu
ring
mon
itoring
define
das
theminim
umav
erag
edu
ration
betw
eenco
nsec
utivese
izures
withinan
yho
urof
mon
itoring(in
patien
tswith1se
izure)m
ax
5max
imum
percen
tage
ofan
yho
urdu
ring
mon
itoringthat
was
occu
pied
byse
izureac
tivityP
atientsareso
rted
bynu
mbe
rof
seizures
that
occu
rred
during
mon
itoring
Detec
ted
andmisse
d
give
thepe
rcen
tage
ofse
izures
detected
ormisse
dby
compr
esse
dsp
ectral
arrayndash
guided
review
protoc
ol(relativeto
thepa
ge-by-pa
gereview
gold
stan
dard
)For
this
stud
yapa
tien
twas
said
toha
veESE
ifeither
(1)t
hemax
imum
seizuredu
ration
was
5
minutes
or(2)t
heminim
umho
urly
averag
eISIw
as5
minutes
60 Neurology 83 July 1 2014
In keeping with a prior study by our group23
CSA-guided review had excellent sensitivity for thepresence of other common critical ldquointerictalrdquo find-ings including focal (987) and generalized (100)slowing periodic discharges (100) and rhythmicdelta activity (971) compared with conventionalpage-by-page EEG review Similarly sensitivity forthe presence of sporadic epileptiform discharges wasreasonably high (885) The high sensitivity fornonseizure findings is not necessarily because these
patterns produce distinct CSA signatures For exam-ple epileptiform discharges being brief typicallyshow no obvious footprint in the 2-hour CSA displayused in our protocol Rather these patterns are abun-dant enough to be detected even by very limitedreview of the primary EEG data that occurs duringCSA-guided review
The early stage of cEEG training of the CSAreview group merits comment This selection of read-ers was intended to reflect the practice at many ter-tiary care centers of relying on clinical fellows formost first-line cEEG interpretation The use of train-ees might produce conservative estimates of sensitiv-ity as sensitivity should improve with experienceBy contrast our gold-standard EEG reviewers wereexperienced attending-level clinical EEGers to ensurevalidity of the gold standard
Our protocol relied on 2-hour CSA windowsWe chose to display 5 CSA panels (left and right lat-eral and parasagittal chains and hemispheric asym-metry spectrogram) Including additional CSApanels higher time resolution (eg 30-minute win-dows) and possibly other compressed-data formats(eg amplitude integrated EEG rhythmicity meas-ures) might have produced higher seizure detectionrates However increasing data volume might com-promise efficiency by producing cognitive overloadFurther research is necessary to determine whichquantitative EEG instruments alone and in combi-nation present the best cognitive match for humanEEG reviewers
Some have suggested that nurses EEG technolo-gists and residents can be trained to review CSA datato flag regions for direct review by physician ex-perts2021 These efforts are important because cEEGpatterns in the acutely ill are dynamic and requireprompt action However nonexpert CSA-basedscreening (without immediate visual confirmation)may yield more false alarms which might place addi-tional burdens on neurophysiologists charged withfollowing up on such alerts In the current studyconstant correlation of CSA patterns with the under-lying EEG was critical in achieving high sensitivityand efficiency and direct visual confirmation by atrained expert remains an essential step to determin-ing which cEEG patterns are significant rather thanartifactual or incidental
Our results are subject to several limitationsFirst our study is a single-center retrospectivereview and a larger multi-institutional prospectivetrial is needed to establish the validity and general-izability of our findings Second CSA cannot escapethe inherent limitations of scalp EEG including thefact that not all seizures may be detectable on scalpEEG For example exquisitely focal seizures maybe detectable only with invasive monitoring and
Figure 2 Time-savings group analysis
Comparison histograms of the time taken to review a given record with the assistance ofCSA (blue bars) and without (red) (A) All studies reviewed by readers AndashC using CSA guid-ance vs conventional review (B) All studies that contained seizures Studies were rankordered from the shortest to longest review time The average time to review 24 hours ofcEEG data when CSA was used was 8 (64) minutes whereas conventional review took 38(617) minutes on average (A) These were statistically different between the groups (p
0005) (B) If seizures were present time savings was more marked CSA review 10(64) minutes and conventional 44 (620) minutes (p 0005) The figure is truncated at60 minutes For 14 studies reading with conventional review took more than 60 minutesTimes to review for these outliers were 622 623 635 636 637 646 652 660 673716 724 750 958 and 1016 in chart A and 958 750 724 716 673 652 646636 635 623 and 622 in chart B Times to review were normalized to a standard dura-tion of 24 hours of cEEG ie all reported times are expressed as time spent per 24 hours ofEEG data cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 61
seizure activity of low amplitude frequency orduration or seizures in the presence of ldquomalig-nantrdquo-appearing background activity may be diffi-cult to discern even on careful inspection of the rawcEEG Third while our results suggest that patternsmeeting the strict definition of definite electro-graphic seizures24 can be identified readily border-zone rhythmic and periodic EEG patterns failing toqualify as definite electrographic seizures may nev-ertheless be symptomatic and require treatment insome cases Determination of the clinical signifi-cance of such cases is possible only by clinical cor-relation eg to determine whether the pattern inquestion reliably correlates with signssymptomsand whether the patient improves with treatmentIn such cases CSA-guided review may not signifi-cantly reduce the total time required for interpreta-tion Fourth it should be emphasized that ourestimate of approximately 75 time savings appliesonly to the part of EEG review after careful directconventional visual analysis of the initial 30 minutesof data As stated above there are reasons to believethat the familiarity with the cEEG provided by thisinitial review is critical to both time savings andsensitivity of subsequent CSA-guided screeningFifth not all centers have access to software or read-ing stations such as those used to view CSA in thisstudy However such centers may be less likely toperform large-scale cEEG and may thus be betterable to review their studies without relying on CSA-based screening Sixth some centers employ dedi-cated technicians to monitor and screen for seizures
allowing physicians to focus only on suspicious seg-ments perhaps obviating the advantage (for physi-cians) of CSA-guided review Seventh some centersemploy screening of CSA (andor other measures)by nurses and electroneurodiagnostic technologistsfollowed by page-by-page EEG review by a physi-cian in fellowship training or another electroneur-odiagnostic technician followed by complete ortargeted review by an attending-level neurophysiol-ogist This approach of triple EEG review whiletime-consuming and resource-intensive is arguablythe least likely to miss any significant findingsFurther outcome-oriented research is needed todetermine the optimal approach among these alter-natives Eighth it must be emphasized that theCSA-guided review protocol proposed here is notintended as a substitute for visual review by trainedexpert clinicians and indeed expert visual review ofprimary cEEG data is an indispensable componentof the present CSA-guided protocol Lastly the re-sults of the present study apply only in the criticalcare setting They have no obvious direct relevanceto diagnostic long-term video EEG monitoring forassessment of chronic epilepsy particularly for thepresurgical workup In such patients interictalspikes may be infrequent but very clinically impor-tant necessitating careful time-consuming visualsearch and patients may undergo days of cEEGrecording to detect even a small number of seizureson which neurosurgical decisions are based In thissetting missing one seizure can have significantclinical consequences
Figure 3 Sensitivity analysis for seizures and other abnormal patterns
The overall sensitivity of CSA-guided review and conventional review of reviewers AndashC is shown relative to the gold-standard findings of readers D and E seizures 873 (10411192) PDs 100 (4343) RDA 971 (3435) FS987 (7677) GS 100 (100100) and EDs 885 (6170) By definition the gold-standard conventional review groupdetected 100 of all seizures and common abnormal patterns CSA 5 compressed spectral array ED 5 epileptiformdischarge FS 5 focal slowing GS 5 generalized slowing PD 5 periodic epileptiform discharge RDA 5 rhythmic deltaactivity
62 Neurology 83 July 1 2014
Finally it remains to be determined whether thetime savings achievable by CSA-guided review ismeaningful in either clinical or cost-effectivenessterms In many cases initial identification of EEGevents represents only one part of providing criticalcare cEEG services Other responsibilities whichmay be even more time-consuming include clinicalcorrelation of EEG findings including bedside exam-ination as needed to determine their significanceevaluation of changes in medications frequent com-munication with clinical teams to report findingsand to make EEG-related management recommenda-tions and writing EEG reports Nevertheless if vali-dated our results may justify replacing at least thefront-line conventional page-by-page EEG reviewarguably the most time-sensitive stage of EEG analy-sis by the more efficient CSA-based screening proce-dure presented herein
Our results suggest that CSA-guided cEEG reviewcan enable significantly faster interpretation withoutsubstantial loss of sensitivity for critical findings in thevast majority of cases While intensive care unit out-come measures were not explored in this study thedemonstration that CSA-guided review enables rapid
and accurate evaluation of critical EEG findings (suchas the presence of seizures or nonconvulsive status epi-lepticus) suggests that this protocol may positively affectpatient care by allowing more timely management de-cisions in response to critical cEEG events
AUTHOR CONTRIBUTIONSLMVRM MMS and MBW conceptualized and designed the study
LMVRM (MGH clinical neurophysiology fellow) and MBW (faculty
with the MGH Epilepsy Service) completed the statistical analysis LMV
RM MMS and MBW drafted the original manuscript LMVRM
SP and MN contributed to the data production and collection SSC
AJC DBH MMS ESR and MBW reviewed and revised the
manuscript
STUDY FUNDINGNo targeted funding reported
DISCLOSUREL Moura reports no disclosures relevant to the manuscript M Shafi
received support from Harvard Catalyst KL2 MeRIT program M Ng
and S Pati report no disclosures relevant to the manuscript S Cash
A Cole and D Hoch received support from NIHNeurological Disor-
ders and Stroke NS062092 E Rosenthal reports no disclosures relevant
to the manuscript M Westover received support from the American
Brain Foundation Go to Neurologyorg for full disclosures
Received May 22 2013 Accepted in final form March 25 2014
Figure 4 CSA display obscured by artifact
Top screen Two-hour segments of CSA display as described in figure 3 Bottom screen Raw cEEG data as described infigure 3 cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 63
REFERENCES1 Vespa PM Nuwer MR Juhaacutesz C et al Early detection of
vasospasm after acute subarachnoid hemorrhage using con-
tinuous EEG ICU monitoring Electroencephalogr Clin
Neurophysiol 1997103607ndash615
2 Schreiber JM Zelleke T Gaillard WD et al Continuous
video EEG for patients with acute encephalopathy in a
pediatric intensive care unit Neurocrit Care 201217
31ndash38
3 Pandian JD Cascino GD So EL et al Digital video-
electroencephalographic monitoring in the neurological-
neurosurgical intensive care unit Arch Neurol 200461
1090ndash1094
4 Cloostermans MC Van Meulen FB Eertman CJ et al
Continuous electroencephalography monitoring for early
prediction of neurological outcome in postanoxic patients
after cardiac arrest a prospective cohort study Crit Care
Med 2012402867ndash2875
5 Rudin D Grize L Schindler C et al High prevalence of
nonconvulsive and subtle status epilepticus in an ICU of a
tertiary care center a three-year observational cohort
study Epilepsy Res 201196140ndash150
6 Young GB Doig GS Continuous EEG monitoring in
comatose intensive care patients epileptiform activity in
etiologically distinct groups Neurocrit Care 200525ndash10
7 Young GB Continuous EEG monitoring in the ICU
Acta Neurol Scand 200611467ndash68
8 Claassen J Mayer SA Kowalski RG et al Detection of
electrographic seizures with continuous EEG monitoring
in critically ill patients Neurology 2004621743ndash1748
9 Vespa PM Nuwer MR Nenov V et al Increased inci-
dence and impact of nonconvulsive and convulsive seizures
after traumatic brain injury as detected by continuous elec-
troencephalographic monitoring J Neurosurg 199991
750ndash760
10 Towne AR Waterhouse EJ Boggs JG et al Prevalence of
nonconvulsive status epilepticus in comatose patients
Neurology 200054340ndash345
11 Talwar D Torres F Continuous electrophysiologic mon-
itoring of cerebral function in the pediatric intensive care
unit Pediatr Neurol 19884137ndash147
12 Claassen J Hirsch LJ Kreiter KT et al Quantitative con-
tinuous EEG for detecting delayed cerebral ischemia in
patients with poor-grade subarachnoid hemorrhage Clin
Neurophysiol 20041152699ndash2710
13 Carrera E Claassen J Oddo M et al Continuous electroen-
cephalographic monitoring in critically ill patients with central
nervous system infections Arch Neurol 2008651612ndash1618
14 Sutter R Fuhr P Grize L et al Continuous video-EEG
monitoring increases detection rate of nonconvulsive status
epilepticus in the ICU Epilepsia 201152453ndash457
15 Claassen J Hirsch LJ Frontera JA et al Prognostic sig-
nificance of continuous EEG monitoring in patients with
poor-grade subarachnoid hemorrhage Neurocrit Care
20064103ndash112
16 Nuwer MR Quantitative EEG analysis in clinical settings
Brain Topogr 19968201ndash208
17 Nuwer M Assessment of digital EEG quantitative EEG
and EEG brain mapping report of the American Academy
of Neurology and the American Clinical Neurophysiology
Society Neurology 199749277ndash292
18 Shah AK Agarwal R Carhuapoma JR Loeb JA Com-
pressed EEG pattern analysis for critically ill
neurological-neurosurgical patients Neurocrit Care
20065124ndash133
19 Bricolo A Turazzi S Faccioli F et al Clinical application
of compressed spectral array in long-term EEG monitoring
of comatose patients Electroencephalogr Clin Neurophy-
siol 197845211ndash225
20 Stewart CP Otsubo H Ochi A et al Seizure identification in
the ICU using quantitative EEG displays Neurology 2010
751501ndash1508
21 Hirsch LJ LaRoche SM Gaspard N et al American Clin-
ical Neurophysiology Societyrsquos Standardized Critical Care
EEG Terminology 2012 version J Clin Neurophysiol
2013301ndash27
22 Abend NS Dlugos D Herman S Neonatal seizure detec-
tion using multichannel display of envelope trend Epilep-
sia 200849349ndash352
23 Williamson CA Wahlster S Shafi MM Westover MB
Sensitivity of compressed spectral arrays for detecting seiz-
ures in acutely ill adults Neurocrit Care 20142032ndash39
24 Young GB Jordan KG Doig GS An assessment of non-
convulsive seizures in the intensive care unit using contin-
uous EEG monitoring an investigation of variables
associated with mortality Neurology 19964783ndash89
Free Michael J Fox DVD Video on Parkinsonrsquos DiseaseThe AAN and the American Brain Foundation present actor and Parkinsonrsquos disease patientMichael J Fox hosting Parkinsonrsquos Disease A Guide for Patients and Families This new patienteducation video is now available free to members and the public either on DVD or online Thefree DVD can be ordered while supplies last by visiting AANcomviewPatientEducationVideos orcalling (800) 879-1960 The video can be viewed online at YouTubecomAANChannel with otherpatient education DVDs produced by the AAN
64 Neurology 83 July 1 2014
DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
ServicesUpdated Information amp
httpwwwneurologyorgcontent83156fullhtmlincluding high resolution figures can be found at
Supplementary Material
00000000537DC1htmlhttpwwwneurologyorgcontentsuppl20140629WNL00000Supplementary material can be found at
References
httpwwwneurologyorgcontent83156fullhtmlref-list-1at This article cites 24 articles 5 of which you can access for free
Subspecialty Collections
httpwwwneurologyorgcgicollectionhealth_care_reformHealth care reform
reshttpwwwneurologyorgcgicollectioneeg_see_epilepsy-seizuEEG see EpilepsySeizures
httpwwwneurologyorgcgicollectioncritical_careCritical carefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

In keeping with a prior study by our group23
CSA-guided review had excellent sensitivity for thepresence of other common critical ldquointerictalrdquo find-ings including focal (987) and generalized (100)slowing periodic discharges (100) and rhythmicdelta activity (971) compared with conventionalpage-by-page EEG review Similarly sensitivity forthe presence of sporadic epileptiform discharges wasreasonably high (885) The high sensitivity fornonseizure findings is not necessarily because these
patterns produce distinct CSA signatures For exam-ple epileptiform discharges being brief typicallyshow no obvious footprint in the 2-hour CSA displayused in our protocol Rather these patterns are abun-dant enough to be detected even by very limitedreview of the primary EEG data that occurs duringCSA-guided review
The early stage of cEEG training of the CSAreview group merits comment This selection of read-ers was intended to reflect the practice at many ter-tiary care centers of relying on clinical fellows formost first-line cEEG interpretation The use of train-ees might produce conservative estimates of sensitiv-ity as sensitivity should improve with experienceBy contrast our gold-standard EEG reviewers wereexperienced attending-level clinical EEGers to ensurevalidity of the gold standard
Our protocol relied on 2-hour CSA windowsWe chose to display 5 CSA panels (left and right lat-eral and parasagittal chains and hemispheric asym-metry spectrogram) Including additional CSApanels higher time resolution (eg 30-minute win-dows) and possibly other compressed-data formats(eg amplitude integrated EEG rhythmicity meas-ures) might have produced higher seizure detectionrates However increasing data volume might com-promise efficiency by producing cognitive overloadFurther research is necessary to determine whichquantitative EEG instruments alone and in combi-nation present the best cognitive match for humanEEG reviewers
Some have suggested that nurses EEG technolo-gists and residents can be trained to review CSA datato flag regions for direct review by physician ex-perts2021 These efforts are important because cEEGpatterns in the acutely ill are dynamic and requireprompt action However nonexpert CSA-basedscreening (without immediate visual confirmation)may yield more false alarms which might place addi-tional burdens on neurophysiologists charged withfollowing up on such alerts In the current studyconstant correlation of CSA patterns with the under-lying EEG was critical in achieving high sensitivityand efficiency and direct visual confirmation by atrained expert remains an essential step to determin-ing which cEEG patterns are significant rather thanartifactual or incidental
Our results are subject to several limitationsFirst our study is a single-center retrospectivereview and a larger multi-institutional prospectivetrial is needed to establish the validity and general-izability of our findings Second CSA cannot escapethe inherent limitations of scalp EEG including thefact that not all seizures may be detectable on scalpEEG For example exquisitely focal seizures maybe detectable only with invasive monitoring and
Figure 2 Time-savings group analysis
Comparison histograms of the time taken to review a given record with the assistance ofCSA (blue bars) and without (red) (A) All studies reviewed by readers AndashC using CSA guid-ance vs conventional review (B) All studies that contained seizures Studies were rankordered from the shortest to longest review time The average time to review 24 hours ofcEEG data when CSA was used was 8 (64) minutes whereas conventional review took 38(617) minutes on average (A) These were statistically different between the groups (p
0005) (B) If seizures were present time savings was more marked CSA review 10(64) minutes and conventional 44 (620) minutes (p 0005) The figure is truncated at60 minutes For 14 studies reading with conventional review took more than 60 minutesTimes to review for these outliers were 622 623 635 636 637 646 652 660 673716 724 750 958 and 1016 in chart A and 958 750 724 716 673 652 646636 635 623 and 622 in chart B Times to review were normalized to a standard dura-tion of 24 hours of cEEG ie all reported times are expressed as time spent per 24 hours ofEEG data cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 61
seizure activity of low amplitude frequency orduration or seizures in the presence of ldquomalig-nantrdquo-appearing background activity may be diffi-cult to discern even on careful inspection of the rawcEEG Third while our results suggest that patternsmeeting the strict definition of definite electro-graphic seizures24 can be identified readily border-zone rhythmic and periodic EEG patterns failing toqualify as definite electrographic seizures may nev-ertheless be symptomatic and require treatment insome cases Determination of the clinical signifi-cance of such cases is possible only by clinical cor-relation eg to determine whether the pattern inquestion reliably correlates with signssymptomsand whether the patient improves with treatmentIn such cases CSA-guided review may not signifi-cantly reduce the total time required for interpreta-tion Fourth it should be emphasized that ourestimate of approximately 75 time savings appliesonly to the part of EEG review after careful directconventional visual analysis of the initial 30 minutesof data As stated above there are reasons to believethat the familiarity with the cEEG provided by thisinitial review is critical to both time savings andsensitivity of subsequent CSA-guided screeningFifth not all centers have access to software or read-ing stations such as those used to view CSA in thisstudy However such centers may be less likely toperform large-scale cEEG and may thus be betterable to review their studies without relying on CSA-based screening Sixth some centers employ dedi-cated technicians to monitor and screen for seizures
allowing physicians to focus only on suspicious seg-ments perhaps obviating the advantage (for physi-cians) of CSA-guided review Seventh some centersemploy screening of CSA (andor other measures)by nurses and electroneurodiagnostic technologistsfollowed by page-by-page EEG review by a physi-cian in fellowship training or another electroneur-odiagnostic technician followed by complete ortargeted review by an attending-level neurophysiol-ogist This approach of triple EEG review whiletime-consuming and resource-intensive is arguablythe least likely to miss any significant findingsFurther outcome-oriented research is needed todetermine the optimal approach among these alter-natives Eighth it must be emphasized that theCSA-guided review protocol proposed here is notintended as a substitute for visual review by trainedexpert clinicians and indeed expert visual review ofprimary cEEG data is an indispensable componentof the present CSA-guided protocol Lastly the re-sults of the present study apply only in the criticalcare setting They have no obvious direct relevanceto diagnostic long-term video EEG monitoring forassessment of chronic epilepsy particularly for thepresurgical workup In such patients interictalspikes may be infrequent but very clinically impor-tant necessitating careful time-consuming visualsearch and patients may undergo days of cEEGrecording to detect even a small number of seizureson which neurosurgical decisions are based In thissetting missing one seizure can have significantclinical consequences
Figure 3 Sensitivity analysis for seizures and other abnormal patterns
The overall sensitivity of CSA-guided review and conventional review of reviewers AndashC is shown relative to the gold-standard findings of readers D and E seizures 873 (10411192) PDs 100 (4343) RDA 971 (3435) FS987 (7677) GS 100 (100100) and EDs 885 (6170) By definition the gold-standard conventional review groupdetected 100 of all seizures and common abnormal patterns CSA 5 compressed spectral array ED 5 epileptiformdischarge FS 5 focal slowing GS 5 generalized slowing PD 5 periodic epileptiform discharge RDA 5 rhythmic deltaactivity
62 Neurology 83 July 1 2014
Finally it remains to be determined whether thetime savings achievable by CSA-guided review ismeaningful in either clinical or cost-effectivenessterms In many cases initial identification of EEGevents represents only one part of providing criticalcare cEEG services Other responsibilities whichmay be even more time-consuming include clinicalcorrelation of EEG findings including bedside exam-ination as needed to determine their significanceevaluation of changes in medications frequent com-munication with clinical teams to report findingsand to make EEG-related management recommenda-tions and writing EEG reports Nevertheless if vali-dated our results may justify replacing at least thefront-line conventional page-by-page EEG reviewarguably the most time-sensitive stage of EEG analy-sis by the more efficient CSA-based screening proce-dure presented herein
Our results suggest that CSA-guided cEEG reviewcan enable significantly faster interpretation withoutsubstantial loss of sensitivity for critical findings in thevast majority of cases While intensive care unit out-come measures were not explored in this study thedemonstration that CSA-guided review enables rapid
and accurate evaluation of critical EEG findings (suchas the presence of seizures or nonconvulsive status epi-lepticus) suggests that this protocol may positively affectpatient care by allowing more timely management de-cisions in response to critical cEEG events
AUTHOR CONTRIBUTIONSLMVRM MMS and MBW conceptualized and designed the study
LMVRM (MGH clinical neurophysiology fellow) and MBW (faculty
with the MGH Epilepsy Service) completed the statistical analysis LMV
RM MMS and MBW drafted the original manuscript LMVRM
SP and MN contributed to the data production and collection SSC
AJC DBH MMS ESR and MBW reviewed and revised the
manuscript
STUDY FUNDINGNo targeted funding reported
DISCLOSUREL Moura reports no disclosures relevant to the manuscript M Shafi
received support from Harvard Catalyst KL2 MeRIT program M Ng
and S Pati report no disclosures relevant to the manuscript S Cash
A Cole and D Hoch received support from NIHNeurological Disor-
ders and Stroke NS062092 E Rosenthal reports no disclosures relevant
to the manuscript M Westover received support from the American
Brain Foundation Go to Neurologyorg for full disclosures
Received May 22 2013 Accepted in final form March 25 2014
Figure 4 CSA display obscured by artifact
Top screen Two-hour segments of CSA display as described in figure 3 Bottom screen Raw cEEG data as described infigure 3 cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 63
REFERENCES1 Vespa PM Nuwer MR Juhaacutesz C et al Early detection of
vasospasm after acute subarachnoid hemorrhage using con-
tinuous EEG ICU monitoring Electroencephalogr Clin
Neurophysiol 1997103607ndash615
2 Schreiber JM Zelleke T Gaillard WD et al Continuous
video EEG for patients with acute encephalopathy in a
pediatric intensive care unit Neurocrit Care 201217
31ndash38
3 Pandian JD Cascino GD So EL et al Digital video-
electroencephalographic monitoring in the neurological-
neurosurgical intensive care unit Arch Neurol 200461
1090ndash1094
4 Cloostermans MC Van Meulen FB Eertman CJ et al
Continuous electroencephalography monitoring for early
prediction of neurological outcome in postanoxic patients
after cardiac arrest a prospective cohort study Crit Care
Med 2012402867ndash2875
5 Rudin D Grize L Schindler C et al High prevalence of
nonconvulsive and subtle status epilepticus in an ICU of a
tertiary care center a three-year observational cohort
study Epilepsy Res 201196140ndash150
6 Young GB Doig GS Continuous EEG monitoring in
comatose intensive care patients epileptiform activity in
etiologically distinct groups Neurocrit Care 200525ndash10
7 Young GB Continuous EEG monitoring in the ICU
Acta Neurol Scand 200611467ndash68
8 Claassen J Mayer SA Kowalski RG et al Detection of
electrographic seizures with continuous EEG monitoring
in critically ill patients Neurology 2004621743ndash1748
9 Vespa PM Nuwer MR Nenov V et al Increased inci-
dence and impact of nonconvulsive and convulsive seizures
after traumatic brain injury as detected by continuous elec-
troencephalographic monitoring J Neurosurg 199991
750ndash760
10 Towne AR Waterhouse EJ Boggs JG et al Prevalence of
nonconvulsive status epilepticus in comatose patients
Neurology 200054340ndash345
11 Talwar D Torres F Continuous electrophysiologic mon-
itoring of cerebral function in the pediatric intensive care
unit Pediatr Neurol 19884137ndash147
12 Claassen J Hirsch LJ Kreiter KT et al Quantitative con-
tinuous EEG for detecting delayed cerebral ischemia in
patients with poor-grade subarachnoid hemorrhage Clin
Neurophysiol 20041152699ndash2710
13 Carrera E Claassen J Oddo M et al Continuous electroen-
cephalographic monitoring in critically ill patients with central
nervous system infections Arch Neurol 2008651612ndash1618
14 Sutter R Fuhr P Grize L et al Continuous video-EEG
monitoring increases detection rate of nonconvulsive status
epilepticus in the ICU Epilepsia 201152453ndash457
15 Claassen J Hirsch LJ Frontera JA et al Prognostic sig-
nificance of continuous EEG monitoring in patients with
poor-grade subarachnoid hemorrhage Neurocrit Care
20064103ndash112
16 Nuwer MR Quantitative EEG analysis in clinical settings
Brain Topogr 19968201ndash208
17 Nuwer M Assessment of digital EEG quantitative EEG
and EEG brain mapping report of the American Academy
of Neurology and the American Clinical Neurophysiology
Society Neurology 199749277ndash292
18 Shah AK Agarwal R Carhuapoma JR Loeb JA Com-
pressed EEG pattern analysis for critically ill
neurological-neurosurgical patients Neurocrit Care
20065124ndash133
19 Bricolo A Turazzi S Faccioli F et al Clinical application
of compressed spectral array in long-term EEG monitoring
of comatose patients Electroencephalogr Clin Neurophy-
siol 197845211ndash225
20 Stewart CP Otsubo H Ochi A et al Seizure identification in
the ICU using quantitative EEG displays Neurology 2010
751501ndash1508
21 Hirsch LJ LaRoche SM Gaspard N et al American Clin-
ical Neurophysiology Societyrsquos Standardized Critical Care
EEG Terminology 2012 version J Clin Neurophysiol
2013301ndash27
22 Abend NS Dlugos D Herman S Neonatal seizure detec-
tion using multichannel display of envelope trend Epilep-
sia 200849349ndash352
23 Williamson CA Wahlster S Shafi MM Westover MB
Sensitivity of compressed spectral arrays for detecting seiz-
ures in acutely ill adults Neurocrit Care 20142032ndash39
24 Young GB Jordan KG Doig GS An assessment of non-
convulsive seizures in the intensive care unit using contin-
uous EEG monitoring an investigation of variables
associated with mortality Neurology 19964783ndash89
Free Michael J Fox DVD Video on Parkinsonrsquos DiseaseThe AAN and the American Brain Foundation present actor and Parkinsonrsquos disease patientMichael J Fox hosting Parkinsonrsquos Disease A Guide for Patients and Families This new patienteducation video is now available free to members and the public either on DVD or online Thefree DVD can be ordered while supplies last by visiting AANcomviewPatientEducationVideos orcalling (800) 879-1960 The video can be viewed online at YouTubecomAANChannel with otherpatient education DVDs produced by the AAN
64 Neurology 83 July 1 2014
DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
ServicesUpdated Information amp
httpwwwneurologyorgcontent83156fullhtmlincluding high resolution figures can be found at
Supplementary Material
00000000537DC1htmlhttpwwwneurologyorgcontentsuppl20140629WNL00000Supplementary material can be found at
References
httpwwwneurologyorgcontent83156fullhtmlref-list-1at This article cites 24 articles 5 of which you can access for free
Subspecialty Collections
httpwwwneurologyorgcgicollectionhealth_care_reformHealth care reform
reshttpwwwneurologyorgcgicollectioneeg_see_epilepsy-seizuEEG see EpilepsySeizures
httpwwwneurologyorgcgicollectioncritical_careCritical carefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

seizure activity of low amplitude frequency orduration or seizures in the presence of ldquomalig-nantrdquo-appearing background activity may be diffi-cult to discern even on careful inspection of the rawcEEG Third while our results suggest that patternsmeeting the strict definition of definite electro-graphic seizures24 can be identified readily border-zone rhythmic and periodic EEG patterns failing toqualify as definite electrographic seizures may nev-ertheless be symptomatic and require treatment insome cases Determination of the clinical signifi-cance of such cases is possible only by clinical cor-relation eg to determine whether the pattern inquestion reliably correlates with signssymptomsand whether the patient improves with treatmentIn such cases CSA-guided review may not signifi-cantly reduce the total time required for interpreta-tion Fourth it should be emphasized that ourestimate of approximately 75 time savings appliesonly to the part of EEG review after careful directconventional visual analysis of the initial 30 minutesof data As stated above there are reasons to believethat the familiarity with the cEEG provided by thisinitial review is critical to both time savings andsensitivity of subsequent CSA-guided screeningFifth not all centers have access to software or read-ing stations such as those used to view CSA in thisstudy However such centers may be less likely toperform large-scale cEEG and may thus be betterable to review their studies without relying on CSA-based screening Sixth some centers employ dedi-cated technicians to monitor and screen for seizures
allowing physicians to focus only on suspicious seg-ments perhaps obviating the advantage (for physi-cians) of CSA-guided review Seventh some centersemploy screening of CSA (andor other measures)by nurses and electroneurodiagnostic technologistsfollowed by page-by-page EEG review by a physi-cian in fellowship training or another electroneur-odiagnostic technician followed by complete ortargeted review by an attending-level neurophysiol-ogist This approach of triple EEG review whiletime-consuming and resource-intensive is arguablythe least likely to miss any significant findingsFurther outcome-oriented research is needed todetermine the optimal approach among these alter-natives Eighth it must be emphasized that theCSA-guided review protocol proposed here is notintended as a substitute for visual review by trainedexpert clinicians and indeed expert visual review ofprimary cEEG data is an indispensable componentof the present CSA-guided protocol Lastly the re-sults of the present study apply only in the criticalcare setting They have no obvious direct relevanceto diagnostic long-term video EEG monitoring forassessment of chronic epilepsy particularly for thepresurgical workup In such patients interictalspikes may be infrequent but very clinically impor-tant necessitating careful time-consuming visualsearch and patients may undergo days of cEEGrecording to detect even a small number of seizureson which neurosurgical decisions are based In thissetting missing one seizure can have significantclinical consequences
Figure 3 Sensitivity analysis for seizures and other abnormal patterns
The overall sensitivity of CSA-guided review and conventional review of reviewers AndashC is shown relative to the gold-standard findings of readers D and E seizures 873 (10411192) PDs 100 (4343) RDA 971 (3435) FS987 (7677) GS 100 (100100) and EDs 885 (6170) By definition the gold-standard conventional review groupdetected 100 of all seizures and common abnormal patterns CSA 5 compressed spectral array ED 5 epileptiformdischarge FS 5 focal slowing GS 5 generalized slowing PD 5 periodic epileptiform discharge RDA 5 rhythmic deltaactivity
62 Neurology 83 July 1 2014
Finally it remains to be determined whether thetime savings achievable by CSA-guided review ismeaningful in either clinical or cost-effectivenessterms In many cases initial identification of EEGevents represents only one part of providing criticalcare cEEG services Other responsibilities whichmay be even more time-consuming include clinicalcorrelation of EEG findings including bedside exam-ination as needed to determine their significanceevaluation of changes in medications frequent com-munication with clinical teams to report findingsand to make EEG-related management recommenda-tions and writing EEG reports Nevertheless if vali-dated our results may justify replacing at least thefront-line conventional page-by-page EEG reviewarguably the most time-sensitive stage of EEG analy-sis by the more efficient CSA-based screening proce-dure presented herein
Our results suggest that CSA-guided cEEG reviewcan enable significantly faster interpretation withoutsubstantial loss of sensitivity for critical findings in thevast majority of cases While intensive care unit out-come measures were not explored in this study thedemonstration that CSA-guided review enables rapid
and accurate evaluation of critical EEG findings (suchas the presence of seizures or nonconvulsive status epi-lepticus) suggests that this protocol may positively affectpatient care by allowing more timely management de-cisions in response to critical cEEG events
AUTHOR CONTRIBUTIONSLMVRM MMS and MBW conceptualized and designed the study
LMVRM (MGH clinical neurophysiology fellow) and MBW (faculty
with the MGH Epilepsy Service) completed the statistical analysis LMV
RM MMS and MBW drafted the original manuscript LMVRM
SP and MN contributed to the data production and collection SSC
AJC DBH MMS ESR and MBW reviewed and revised the
manuscript
STUDY FUNDINGNo targeted funding reported
DISCLOSUREL Moura reports no disclosures relevant to the manuscript M Shafi
received support from Harvard Catalyst KL2 MeRIT program M Ng
and S Pati report no disclosures relevant to the manuscript S Cash
A Cole and D Hoch received support from NIHNeurological Disor-
ders and Stroke NS062092 E Rosenthal reports no disclosures relevant
to the manuscript M Westover received support from the American
Brain Foundation Go to Neurologyorg for full disclosures
Received May 22 2013 Accepted in final form March 25 2014
Figure 4 CSA display obscured by artifact
Top screen Two-hour segments of CSA display as described in figure 3 Bottom screen Raw cEEG data as described infigure 3 cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 63
REFERENCES1 Vespa PM Nuwer MR Juhaacutesz C et al Early detection of
vasospasm after acute subarachnoid hemorrhage using con-
tinuous EEG ICU monitoring Electroencephalogr Clin
Neurophysiol 1997103607ndash615
2 Schreiber JM Zelleke T Gaillard WD et al Continuous
video EEG for patients with acute encephalopathy in a
pediatric intensive care unit Neurocrit Care 201217
31ndash38
3 Pandian JD Cascino GD So EL et al Digital video-
electroencephalographic monitoring in the neurological-
neurosurgical intensive care unit Arch Neurol 200461
1090ndash1094
4 Cloostermans MC Van Meulen FB Eertman CJ et al
Continuous electroencephalography monitoring for early
prediction of neurological outcome in postanoxic patients
after cardiac arrest a prospective cohort study Crit Care
Med 2012402867ndash2875
5 Rudin D Grize L Schindler C et al High prevalence of
nonconvulsive and subtle status epilepticus in an ICU of a
tertiary care center a three-year observational cohort
study Epilepsy Res 201196140ndash150
6 Young GB Doig GS Continuous EEG monitoring in
comatose intensive care patients epileptiform activity in
etiologically distinct groups Neurocrit Care 200525ndash10
7 Young GB Continuous EEG monitoring in the ICU
Acta Neurol Scand 200611467ndash68
8 Claassen J Mayer SA Kowalski RG et al Detection of
electrographic seizures with continuous EEG monitoring
in critically ill patients Neurology 2004621743ndash1748
9 Vespa PM Nuwer MR Nenov V et al Increased inci-
dence and impact of nonconvulsive and convulsive seizures
after traumatic brain injury as detected by continuous elec-
troencephalographic monitoring J Neurosurg 199991
750ndash760
10 Towne AR Waterhouse EJ Boggs JG et al Prevalence of
nonconvulsive status epilepticus in comatose patients
Neurology 200054340ndash345
11 Talwar D Torres F Continuous electrophysiologic mon-
itoring of cerebral function in the pediatric intensive care
unit Pediatr Neurol 19884137ndash147
12 Claassen J Hirsch LJ Kreiter KT et al Quantitative con-
tinuous EEG for detecting delayed cerebral ischemia in
patients with poor-grade subarachnoid hemorrhage Clin
Neurophysiol 20041152699ndash2710
13 Carrera E Claassen J Oddo M et al Continuous electroen-
cephalographic monitoring in critically ill patients with central
nervous system infections Arch Neurol 2008651612ndash1618
14 Sutter R Fuhr P Grize L et al Continuous video-EEG
monitoring increases detection rate of nonconvulsive status
epilepticus in the ICU Epilepsia 201152453ndash457
15 Claassen J Hirsch LJ Frontera JA et al Prognostic sig-
nificance of continuous EEG monitoring in patients with
poor-grade subarachnoid hemorrhage Neurocrit Care
20064103ndash112
16 Nuwer MR Quantitative EEG analysis in clinical settings
Brain Topogr 19968201ndash208
17 Nuwer M Assessment of digital EEG quantitative EEG
and EEG brain mapping report of the American Academy
of Neurology and the American Clinical Neurophysiology
Society Neurology 199749277ndash292
18 Shah AK Agarwal R Carhuapoma JR Loeb JA Com-
pressed EEG pattern analysis for critically ill
neurological-neurosurgical patients Neurocrit Care
20065124ndash133
19 Bricolo A Turazzi S Faccioli F et al Clinical application
of compressed spectral array in long-term EEG monitoring
of comatose patients Electroencephalogr Clin Neurophy-
siol 197845211ndash225
20 Stewart CP Otsubo H Ochi A et al Seizure identification in
the ICU using quantitative EEG displays Neurology 2010
751501ndash1508
21 Hirsch LJ LaRoche SM Gaspard N et al American Clin-
ical Neurophysiology Societyrsquos Standardized Critical Care
EEG Terminology 2012 version J Clin Neurophysiol
2013301ndash27
22 Abend NS Dlugos D Herman S Neonatal seizure detec-
tion using multichannel display of envelope trend Epilep-
sia 200849349ndash352
23 Williamson CA Wahlster S Shafi MM Westover MB
Sensitivity of compressed spectral arrays for detecting seiz-
ures in acutely ill adults Neurocrit Care 20142032ndash39
24 Young GB Jordan KG Doig GS An assessment of non-
convulsive seizures in the intensive care unit using contin-
uous EEG monitoring an investigation of variables
associated with mortality Neurology 19964783ndash89
Free Michael J Fox DVD Video on Parkinsonrsquos DiseaseThe AAN and the American Brain Foundation present actor and Parkinsonrsquos disease patientMichael J Fox hosting Parkinsonrsquos Disease A Guide for Patients and Families This new patienteducation video is now available free to members and the public either on DVD or online Thefree DVD can be ordered while supplies last by visiting AANcomviewPatientEducationVideos orcalling (800) 879-1960 The video can be viewed online at YouTubecomAANChannel with otherpatient education DVDs produced by the AAN
64 Neurology 83 July 1 2014
DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
ServicesUpdated Information amp
httpwwwneurologyorgcontent83156fullhtmlincluding high resolution figures can be found at
Supplementary Material
00000000537DC1htmlhttpwwwneurologyorgcontentsuppl20140629WNL00000Supplementary material can be found at
References
httpwwwneurologyorgcontent83156fullhtmlref-list-1at This article cites 24 articles 5 of which you can access for free
Subspecialty Collections
httpwwwneurologyorgcgicollectionhealth_care_reformHealth care reform
reshttpwwwneurologyorgcgicollectioneeg_see_epilepsy-seizuEEG see EpilepsySeizures
httpwwwneurologyorgcgicollectioncritical_careCritical carefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

Finally it remains to be determined whether thetime savings achievable by CSA-guided review ismeaningful in either clinical or cost-effectivenessterms In many cases initial identification of EEGevents represents only one part of providing criticalcare cEEG services Other responsibilities whichmay be even more time-consuming include clinicalcorrelation of EEG findings including bedside exam-ination as needed to determine their significanceevaluation of changes in medications frequent com-munication with clinical teams to report findingsand to make EEG-related management recommenda-tions and writing EEG reports Nevertheless if vali-dated our results may justify replacing at least thefront-line conventional page-by-page EEG reviewarguably the most time-sensitive stage of EEG analy-sis by the more efficient CSA-based screening proce-dure presented herein
Our results suggest that CSA-guided cEEG reviewcan enable significantly faster interpretation withoutsubstantial loss of sensitivity for critical findings in thevast majority of cases While intensive care unit out-come measures were not explored in this study thedemonstration that CSA-guided review enables rapid
and accurate evaluation of critical EEG findings (suchas the presence of seizures or nonconvulsive status epi-lepticus) suggests that this protocol may positively affectpatient care by allowing more timely management de-cisions in response to critical cEEG events
AUTHOR CONTRIBUTIONSLMVRM MMS and MBW conceptualized and designed the study
LMVRM (MGH clinical neurophysiology fellow) and MBW (faculty
with the MGH Epilepsy Service) completed the statistical analysis LMV
RM MMS and MBW drafted the original manuscript LMVRM
SP and MN contributed to the data production and collection SSC
AJC DBH MMS ESR and MBW reviewed and revised the
manuscript
STUDY FUNDINGNo targeted funding reported
DISCLOSUREL Moura reports no disclosures relevant to the manuscript M Shafi
received support from Harvard Catalyst KL2 MeRIT program M Ng
and S Pati report no disclosures relevant to the manuscript S Cash
A Cole and D Hoch received support from NIHNeurological Disor-
ders and Stroke NS062092 E Rosenthal reports no disclosures relevant
to the manuscript M Westover received support from the American
Brain Foundation Go to Neurologyorg for full disclosures
Received May 22 2013 Accepted in final form March 25 2014
Figure 4 CSA display obscured by artifact
Top screen Two-hour segments of CSA display as described in figure 3 Bottom screen Raw cEEG data as described infigure 3 cEEG 5 continuous EEG CSA 5 compressed spectral array
Neurology 83 July 1 2014 63
REFERENCES1 Vespa PM Nuwer MR Juhaacutesz C et al Early detection of
vasospasm after acute subarachnoid hemorrhage using con-
tinuous EEG ICU monitoring Electroencephalogr Clin
Neurophysiol 1997103607ndash615
2 Schreiber JM Zelleke T Gaillard WD et al Continuous
video EEG for patients with acute encephalopathy in a
pediatric intensive care unit Neurocrit Care 201217
31ndash38
3 Pandian JD Cascino GD So EL et al Digital video-
electroencephalographic monitoring in the neurological-
neurosurgical intensive care unit Arch Neurol 200461
1090ndash1094
4 Cloostermans MC Van Meulen FB Eertman CJ et al
Continuous electroencephalography monitoring for early
prediction of neurological outcome in postanoxic patients
after cardiac arrest a prospective cohort study Crit Care
Med 2012402867ndash2875
5 Rudin D Grize L Schindler C et al High prevalence of
nonconvulsive and subtle status epilepticus in an ICU of a
tertiary care center a three-year observational cohort
study Epilepsy Res 201196140ndash150
6 Young GB Doig GS Continuous EEG monitoring in
comatose intensive care patients epileptiform activity in
etiologically distinct groups Neurocrit Care 200525ndash10
7 Young GB Continuous EEG monitoring in the ICU
Acta Neurol Scand 200611467ndash68
8 Claassen J Mayer SA Kowalski RG et al Detection of
electrographic seizures with continuous EEG monitoring
in critically ill patients Neurology 2004621743ndash1748
9 Vespa PM Nuwer MR Nenov V et al Increased inci-
dence and impact of nonconvulsive and convulsive seizures
after traumatic brain injury as detected by continuous elec-
troencephalographic monitoring J Neurosurg 199991
750ndash760
10 Towne AR Waterhouse EJ Boggs JG et al Prevalence of
nonconvulsive status epilepticus in comatose patients
Neurology 200054340ndash345
11 Talwar D Torres F Continuous electrophysiologic mon-
itoring of cerebral function in the pediatric intensive care
unit Pediatr Neurol 19884137ndash147
12 Claassen J Hirsch LJ Kreiter KT et al Quantitative con-
tinuous EEG for detecting delayed cerebral ischemia in
patients with poor-grade subarachnoid hemorrhage Clin
Neurophysiol 20041152699ndash2710
13 Carrera E Claassen J Oddo M et al Continuous electroen-
cephalographic monitoring in critically ill patients with central
nervous system infections Arch Neurol 2008651612ndash1618
14 Sutter R Fuhr P Grize L et al Continuous video-EEG
monitoring increases detection rate of nonconvulsive status
epilepticus in the ICU Epilepsia 201152453ndash457
15 Claassen J Hirsch LJ Frontera JA et al Prognostic sig-
nificance of continuous EEG monitoring in patients with
poor-grade subarachnoid hemorrhage Neurocrit Care
20064103ndash112
16 Nuwer MR Quantitative EEG analysis in clinical settings
Brain Topogr 19968201ndash208
17 Nuwer M Assessment of digital EEG quantitative EEG
and EEG brain mapping report of the American Academy
of Neurology and the American Clinical Neurophysiology
Society Neurology 199749277ndash292
18 Shah AK Agarwal R Carhuapoma JR Loeb JA Com-
pressed EEG pattern analysis for critically ill
neurological-neurosurgical patients Neurocrit Care
20065124ndash133
19 Bricolo A Turazzi S Faccioli F et al Clinical application
of compressed spectral array in long-term EEG monitoring
of comatose patients Electroencephalogr Clin Neurophy-
siol 197845211ndash225
20 Stewart CP Otsubo H Ochi A et al Seizure identification in
the ICU using quantitative EEG displays Neurology 2010
751501ndash1508
21 Hirsch LJ LaRoche SM Gaspard N et al American Clin-
ical Neurophysiology Societyrsquos Standardized Critical Care
EEG Terminology 2012 version J Clin Neurophysiol
2013301ndash27
22 Abend NS Dlugos D Herman S Neonatal seizure detec-
tion using multichannel display of envelope trend Epilep-
sia 200849349ndash352
23 Williamson CA Wahlster S Shafi MM Westover MB
Sensitivity of compressed spectral arrays for detecting seiz-
ures in acutely ill adults Neurocrit Care 20142032ndash39
24 Young GB Jordan KG Doig GS An assessment of non-
convulsive seizures in the intensive care unit using contin-
uous EEG monitoring an investigation of variables
associated with mortality Neurology 19964783ndash89
Free Michael J Fox DVD Video on Parkinsonrsquos DiseaseThe AAN and the American Brain Foundation present actor and Parkinsonrsquos disease patientMichael J Fox hosting Parkinsonrsquos Disease A Guide for Patients and Families This new patienteducation video is now available free to members and the public either on DVD or online Thefree DVD can be ordered while supplies last by visiting AANcomviewPatientEducationVideos orcalling (800) 879-1960 The video can be viewed online at YouTubecomAANChannel with otherpatient education DVDs produced by the AAN
64 Neurology 83 July 1 2014
DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
ServicesUpdated Information amp
httpwwwneurologyorgcontent83156fullhtmlincluding high resolution figures can be found at
Supplementary Material
00000000537DC1htmlhttpwwwneurologyorgcontentsuppl20140629WNL00000Supplementary material can be found at
References
httpwwwneurologyorgcontent83156fullhtmlref-list-1at This article cites 24 articles 5 of which you can access for free
Subspecialty Collections
httpwwwneurologyorgcgicollectionhealth_care_reformHealth care reform
reshttpwwwneurologyorgcgicollectioneeg_see_epilepsy-seizuEEG see EpilepsySeizures
httpwwwneurologyorgcgicollectioncritical_careCritical carefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

REFERENCES1 Vespa PM Nuwer MR Juhaacutesz C et al Early detection of
vasospasm after acute subarachnoid hemorrhage using con-
tinuous EEG ICU monitoring Electroencephalogr Clin
Neurophysiol 1997103607ndash615
2 Schreiber JM Zelleke T Gaillard WD et al Continuous
video EEG for patients with acute encephalopathy in a
pediatric intensive care unit Neurocrit Care 201217
31ndash38
3 Pandian JD Cascino GD So EL et al Digital video-
electroencephalographic monitoring in the neurological-
neurosurgical intensive care unit Arch Neurol 200461
1090ndash1094
4 Cloostermans MC Van Meulen FB Eertman CJ et al
Continuous electroencephalography monitoring for early
prediction of neurological outcome in postanoxic patients
after cardiac arrest a prospective cohort study Crit Care
Med 2012402867ndash2875
5 Rudin D Grize L Schindler C et al High prevalence of
nonconvulsive and subtle status epilepticus in an ICU of a
tertiary care center a three-year observational cohort
study Epilepsy Res 201196140ndash150
6 Young GB Doig GS Continuous EEG monitoring in
comatose intensive care patients epileptiform activity in
etiologically distinct groups Neurocrit Care 200525ndash10
7 Young GB Continuous EEG monitoring in the ICU
Acta Neurol Scand 200611467ndash68
8 Claassen J Mayer SA Kowalski RG et al Detection of
electrographic seizures with continuous EEG monitoring
in critically ill patients Neurology 2004621743ndash1748
9 Vespa PM Nuwer MR Nenov V et al Increased inci-
dence and impact of nonconvulsive and convulsive seizures
after traumatic brain injury as detected by continuous elec-
troencephalographic monitoring J Neurosurg 199991
750ndash760
10 Towne AR Waterhouse EJ Boggs JG et al Prevalence of
nonconvulsive status epilepticus in comatose patients
Neurology 200054340ndash345
11 Talwar D Torres F Continuous electrophysiologic mon-
itoring of cerebral function in the pediatric intensive care
unit Pediatr Neurol 19884137ndash147
12 Claassen J Hirsch LJ Kreiter KT et al Quantitative con-
tinuous EEG for detecting delayed cerebral ischemia in
patients with poor-grade subarachnoid hemorrhage Clin
Neurophysiol 20041152699ndash2710
13 Carrera E Claassen J Oddo M et al Continuous electroen-
cephalographic monitoring in critically ill patients with central
nervous system infections Arch Neurol 2008651612ndash1618
14 Sutter R Fuhr P Grize L et al Continuous video-EEG
monitoring increases detection rate of nonconvulsive status
epilepticus in the ICU Epilepsia 201152453ndash457
15 Claassen J Hirsch LJ Frontera JA et al Prognostic sig-
nificance of continuous EEG monitoring in patients with
poor-grade subarachnoid hemorrhage Neurocrit Care
20064103ndash112
16 Nuwer MR Quantitative EEG analysis in clinical settings
Brain Topogr 19968201ndash208
17 Nuwer M Assessment of digital EEG quantitative EEG
and EEG brain mapping report of the American Academy
of Neurology and the American Clinical Neurophysiology
Society Neurology 199749277ndash292
18 Shah AK Agarwal R Carhuapoma JR Loeb JA Com-
pressed EEG pattern analysis for critically ill
neurological-neurosurgical patients Neurocrit Care
20065124ndash133
19 Bricolo A Turazzi S Faccioli F et al Clinical application
of compressed spectral array in long-term EEG monitoring
of comatose patients Electroencephalogr Clin Neurophy-
siol 197845211ndash225
20 Stewart CP Otsubo H Ochi A et al Seizure identification in
the ICU using quantitative EEG displays Neurology 2010
751501ndash1508
21 Hirsch LJ LaRoche SM Gaspard N et al American Clin-
ical Neurophysiology Societyrsquos Standardized Critical Care
EEG Terminology 2012 version J Clin Neurophysiol
2013301ndash27
22 Abend NS Dlugos D Herman S Neonatal seizure detec-
tion using multichannel display of envelope trend Epilep-
sia 200849349ndash352
23 Williamson CA Wahlster S Shafi MM Westover MB
Sensitivity of compressed spectral arrays for detecting seiz-
ures in acutely ill adults Neurocrit Care 20142032ndash39
24 Young GB Jordan KG Doig GS An assessment of non-
convulsive seizures in the intensive care unit using contin-
uous EEG monitoring an investigation of variables
associated with mortality Neurology 19964783ndash89
Free Michael J Fox DVD Video on Parkinsonrsquos DiseaseThe AAN and the American Brain Foundation present actor and Parkinsonrsquos disease patientMichael J Fox hosting Parkinsonrsquos Disease A Guide for Patients and Families This new patienteducation video is now available free to members and the public either on DVD or online Thefree DVD can be ordered while supplies last by visiting AANcomviewPatientEducationVideos orcalling (800) 879-1960 The video can be viewed online at YouTubecomAANChannel with otherpatient education DVDs produced by the AAN
64 Neurology 83 July 1 2014
DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
ServicesUpdated Information amp
httpwwwneurologyorgcontent83156fullhtmlincluding high resolution figures can be found at
Supplementary Material
00000000537DC1htmlhttpwwwneurologyorgcontentsuppl20140629WNL00000Supplementary material can be found at
References
httpwwwneurologyorgcontent83156fullhtmlref-list-1at This article cites 24 articles 5 of which you can access for free
Subspecialty Collections
httpwwwneurologyorgcgicollectionhealth_care_reformHealth care reform
reshttpwwwneurologyorgcgicollectioneeg_see_epilepsy-seizuEEG see EpilepsySeizures
httpwwwneurologyorgcgicollectioncritical_careCritical carefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

DOI 101212WNL000000000000053720148356-64 Published Online before print May 23 2014Neurology
Lidia MVR Moura Mouhsin M Shafi Marcus Ng et al Spectrogram screening of adult EEGs is sensitive and efficient
This information is current as of May 23 2014
ServicesUpdated Information amp
httpwwwneurologyorgcontent83156fullhtmlincluding high resolution figures can be found at
Supplementary Material
00000000537DC1htmlhttpwwwneurologyorgcontentsuppl20140629WNL00000Supplementary material can be found at
References
httpwwwneurologyorgcontent83156fullhtmlref-list-1at This article cites 24 articles 5 of which you can access for free
Subspecialty Collections
httpwwwneurologyorgcgicollectionhealth_care_reformHealth care reform
reshttpwwwneurologyorgcgicollectioneeg_see_epilepsy-seizuEEG see EpilepsySeizures
httpwwwneurologyorgcgicollectioncritical_careCritical carefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online











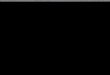



![Big Data Resources for EEGs: Enabling Deep Learning Research 1 · 2017. 12. 12. · Abnormal EEG Corpus [3] . It contains both normal and abnormal EEGs, with no patients overlapping](https://img.pdfslide.us/doc/110x75/61199806132e7f0dc63b51e3/big-data-resources-for-eegs-enabling-deep-learning-research-1-2017-12-12-abnormal.jpg)