Embed Size (px)
Citation preview

Specificities of anti-platelet antibodies in multitransfusedpatients with haemato-oncological disorders
MARTIN KURZ, HIL DE GARD GRE INIX,* PAUL HOC KER, PE TER KALHS,* PAUL KNOBL,* WOLFGANG RICHARD MAYR,MIC HAEL POBE R
† SIMO N PANZER Clinic for Blood Group Serology and Transfusion Medicine, *First Medical Department,Bone Marrow Transplatation Unit, University of Vienna, †First Medical Department, Wilhelminenspital, Austria
Received 13 March 1996; accepted for publication 19 August 1996
Summary. The clinical condition and the formation ofplatelet-reactive antibodies influence the post-transfusionplatelet increment. We analysed the specificities of platelet-reactive antibodies in 81 multitransfused patients withhaemato-oncological diseases refractory to platelet trans-fusions, or prior to a scheduled stem cell transplantation.In 17 additional patients we prospectively determined thedevelopment of platelet-reactive antibodies at the time ofchemotherapy in weekly intervals. Sera were tested by themonoclonal antibody-specific immobilization of plateletantigens (MAIPA)-technique for antiplatelet antibodiesagainst HLA class I antigens, the human platelet-specificalloantigens (HPA)-1, -2, -3, -5, and the platelet membraneglycoproteins (GP) Ia/IIa, Ib/IX, IIb/IIIa (panreactive).
Platelet reactive antibodies were found in 54% of bloodsamples. They were frequent in patients with a history ofpossible previous immunization, particularly if patientswere refractory to platelet transfusions. Platelet-reactiveHLA antibodies were the most common antibodies. Evenpatients without a known risk of primary immunizationwho received exclusively leucocyte-depleted blood productsformed antibodies. By the MAIPA technique, even LCT-negative sera were found to contain platelet-reactiveantibodies.
Keywords: platelet transfusion, refractoriness, immunizationantiplatelet antibodies specificities.
During the last three decades, therapeutic regimens forhaemato-oncological diseases have become more aggressiveand long-lasting, and therefore require frequent use of bloodproducts, especially platelet concentrates, to sustain haemo-static competence. However, platelet transfusions may fail toresult in the expected increase in platelet counts. The mainreasons are either clinical causes, e.g. septicaemia, hepato-splenomegaly, severe haemorrhage, drugs (vancomycin,amphotericin B) and disseminated intravascular coagulation(Bishop et al, 1988; Friedberg et al, 1993; Doughty et al,1994), or immunomediated destruction of platelet mem-brane structures. So far, in the majority of studies, thepresence of antiplatelet antibodies has been evaluated inpatients refractory to platelet transfusions (Pegels et al,1982; Brand et al, 1986; Heal et al, 1987; Murphy et al,1987; O’Connell et al, 1988; Pamphilon et al, 1989; Kickleret al, 1990). In most of these studies, alloantibodies againsthuman leucocyte antigen (HLA) class I determinants
were found. Alloimmunization against human plateletantigens (HPA) and panreactive anti-platelet (iso)antibodies(McGrath et al, 1988; Kickler et al, 1990; Godeau et al, 1992)may prevent the post-transfusion platelet increment. It isexpected that, as a result from a secondary immune responseafter primary immunization during a previous pregnancy,women are more likely to form antiplatelet antibodies(predominantly anti-HLA antibodies) than men (Howard &Perkins, 1978; Andreu & Dewailly, 1994; Sintnicolaas et al,1995).
Although the identification of antiplatelet antibodies hasimproved within the last 15 years, few data on the incidenceand specificities of platelet reactive antibodies – other thananti-HLA antibodies – in multitransfused patients have beenreported (Kickler et al, 1990). The sensitivity and power todetect specificities of platelet-reactive antibodies are impor-tant factors in the elucidation of their nature. Further,platelet-reactive anti-HLA antibodies should be determinedby their reactivity with platelets, rather than inferring fromlymphocytotoxicity (Murphy & Waters, 1985; Godeau et al,1992). Therefore we analysed sera from patients withhaemato-oncological diseases for their specificities against
British Journal of Haematology, 1996, 95, 564–569
564 # 1996 Blackwell Science Ltd
Correspondence: Dr Simon Panzer, Clinical Department for BloodGroup Serology, University of Vienna, Wahringer Gurtel 18–20,A-1090 Vienna, Austria.

565Anti-platelet Antibodies in Multitransfused Patients
# 1996 Blackwell Science Ltd, British Journal of Haematology 95: 564–569
platelets and evaluated their influence on platelet trans-fusion response.
PATIENTS
Blood samples were drawn from 81 patients (f=m � 36/45),including 11 children. The median age of this patientpopulation was 37 years, range 1–79 years; the medianage of the adult group (>17 years old) was 41 years, range18–79 years. All patients were receiving therapy forhaemato-oncological diseases (32 AML, 13 ALL, 21 lympho-mas including NHL, multiple myeloma, Hodgkin’s diseaseand CLL, two severe aplastic anaemias, seven solid tumours,and six other malignancies). 26 adult female patients hadbeen exposed to possible previous immunization due topregnancy (23 patients) and/or non-leucocyte-depletedtransfusions. Eight adult male patients had received non-leucocyte-depleted transfusions. None of the children havebeen previously immunized. Accordingly, patients weregrouped into those with a history of possible previousimmunization (34 patients) and those without such ahistory (47 patients). Only packed red cells and plateletconcentrates filtered with a third-generation leucocyte filter(Leucozytenfiltersystem BPF4 BS-A, Geratezentrale furBluttransfusion des Osterreichischen Roten Kreuzes, Eugen-dorf, Austria; Leucozytenfiltersystem LRB6/PL50, Gerate-zentrale fur Bluttransfusion des Osterreichischen RotenKreuzes, Eugendorf, Austria, respectively) were consideredas leucocyte-depleted. Refractoriness was defined by acorrected count increment (CCI), 16–20 h post transfusion,of <5� 109/l (Panzer et al, 1987; Bishop et al, 1992),irrespective of the concurrence of any clinical conditionsknown to adversely affect the CCI.
In addition, we prospectively determined the developmentof platelet-reactive antibodies at the time of chemotherapy ina further 17 patients (f/m 8/9, median age 48, range 25–81).These patients received exclusively leucocyte-depleted bloodproducts. Samples were drawn at weekly intervals for at least4 consecutive weeks (range 4–15 weeks). 13 patients weretreated for AML, two for ALL and two for NHL. In eightpatients (five AML, two NHL, one ALL) chemotherapy waspart of the pretransplantation conditioning. Three femaleand five male patients had no history of previous immunization.
METHODS
Patients’ sera were tested for their reactivity against apanel of platelets from blood group O donors homozygous forHPA-1a, -1b, -2a, -2b, -3a, -3b, -5a, -5b by the monoclonalantibody-specific immobilization of platelet antigens assay(MAIPA) (Kiefel et al, 1987; Benda et al, 1989) using thefollowing monoclonal antibodies (mAb): clone FMC-25(anti-CD42a, GPIb/IX, Serotec Ltd, Oxford, U.K.), clone P2(anti-CD41a, anti-GPIIb/IIIa; Immunotech-Dianova, Hamburg,Germany) and clone Gi9 (Immunotech-Dianova). Serareactive with all panel platelets, irrespective of the alloantigenmake-up, were termed panreactive, inferring autoreactivity.In vivo coating of platelets with IgG antibodies was evaluatedby testing the patient’s autologous platelets if the platelet
count was high enough for their separation (direct MAIPA, forGPIa/IIa, Ib/IX and IIb/IIIa). Also, platelets from at least 60blood group O donors were pooled to obtain the expression of>90% of all HLA class I determinants detectable by theMAIPA technique with any antisera after immunoprecipita-tion with clone B1G6 (anti-�2 microglobulin, Immunotech).Serum samples with detectable HLA class I antibodies werealso tested by the standard NIH-microlymphocytotoxicity test(LCT) against 30 random HLA-typed donors. In addition, theplatelet aggregation test using fresh platelets from blood groupO donors homozygous for HPA-2a and -2b, was appliedto determine anti-HPA-2 antibodies (Panzer et al, 1995).Leupeptin (Sigma, St Louis, Mo.) was added to avoidproteolysis of the GPIb/IX complex. Sequentially drawnsamples from individual patients were tested within thesame MAIPA assay.
To further substantiate the alloreaction, patients withplatelet-specific antibodies were genotyped for HPA-1 to -5.Genomic DNA was isolated by the salting-out procedure fromwhole blood anticoagulated with K-EDTA and used forgenotyping for HPA-1, -2, -3 and -5, as described previously(Simsek et al, 1993; Holensteiner et al, 1995).
Statistical analysis. All data were evaluated by contingencytables and chi-square tests and, if necessary, substituted bythe two-sided Fisher’s exact test. A P-value <0.05 wasnecessary for the rejection of the H0 hypothesis.
RESULTS
The presence of platelet-reactive antibodies was evaluated in35 patients screened prior to stem cell transplantation(f=m � 17/18) and in 46 patients who were refractory toplatelet transfusion therapy (f=m � 19/27). Among thelatter, 32 cases had a clinical condition or drug therapyknown to adversely affect the CCI. Refractoriness wasassociated with infection in 24 patients and in a furthereight patients with other adverse clinical conditions.
A compilation of detectable antibody specificities in the 47patients without, and 34 patients with, a history of possibleprevious immunization is shown in Table I. Platelet reactiveantibodies were detectable in 44 patients (54%). Theincidence of antibodies was significantly higher in patientswith a history of previous immunization as compared tothose without (�2
� 6.17, P � 0.013). In both patientpopulations, refractory patients had a significantly higherincidence of antibodies than patients evaluated as apretransplant measure (�2
� 9.8, P � 0.002). Antibodieswere more common in transfusion refractory patients, ifpreviously immunized (�2
� 7:51, P � 0.006); no suchdifference was noted in patients screened prior to transplan-tation (�2
� 2.33, P > 0.05).In line with previous reports (Slichter, 1990), HLA class I
antibodies (n � 32, 40%) were the most common antiplate-let antibodies. 26% (n � 21) of the samples containedpanreactive antiplatelet antibodies, whereas antiplatelet-specific alloantibodies were rare (n � 14, 17%). In 20%(n � 16) of the cases, panreactive antibodies were associatedwith HLA antibodies. Panreactive antibodies against GPIb/IXwere similar in frequency to those against GPIIb/IIIa. Five

samples contained anti-GPIa/IIa antibodies, which were seenonly in combination with anti-GP Ib/IX and IIb/IIIa. MostHPA antibodies were directed against HPA-1b and -5b. Thefrequency of HLA antibodies was higher in patients refractoryto platelet transfusions than in those screened prior totransplantation (�2
� 9.7, P � 0.002). Alloantibodies (HLAand HPA antibodies) were more frequent in patients with apossible previous immunization than in those without(P < 0.05).
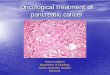
A close evaluation of the formation of platelet-reactiveantibodies was possible in 17 repeatedly examinedpatients. Only one patient already had HLA antibodiesat the start of chemotherapy, and these persisted. HLAantibodies were formed during the observation period ineight individuals. They were transient in five (two of thempreimmunized), but remained in the other three (allpreimmunized) patients. Figs 1 and 2 illustrate thedevelopment of HLA antibody reactivity in two female
# 1996 Blackwell Science Ltd, British Journal of Haematology 95: 564–569
566 Martin Kurz et alTable I. Platelet-reactive antibodies in 81 retrospectively compiled multitransfused haemato-oncological patients.
Previously not immunized Previously immunized*(n � 47) (n � 34)
Refractory Screening Refractory ScreeningTarget antigen (n � 29) (n � 18) (n � 17) (n � 17)
HLA 4 0 7 1HPA 1 1 3 2Panreactive 2 0 1 2HLA�panreactive 7 3 2 1HLA�HPA 2 0 1 1HLA�HPA + panreactive 0 0 2 1
Ib/IX 2 1 1 2IIb/IIIa 1 2 1 1Ib/IX� IIb/IIIa 3 0 2 0Ia/IIa� Ib/IX + IIb/IIIa 3 0 1 1
HPA-1 2 0 1 1HPA-2 0 0 1 0HPA-3 0 0 1 1HPA-5 0 1 3 1HPA-1�HPA-3 0 0 0 1HPA-1�HPA-5 1 0 0 0
* Patients with a history of a previous pregnancy and/or transfusions of non-leucocyte-depletedblood products.
Fig 1. Development of HLA antibodies in apatient who has been pregnant and receivednon-leucocyte-depleted blood products whentreated for AML. The arrow indicates the startof conditioning treatment (CT) fortransplantation, for which she receivedexclusively leucocyte-depleted blood products.The HLA antibody became detectable byMAIPA assay at the time of infection (solidline). Closed circles indicate that the LCT wasalso positive. The dashed line is for the CCI.

567Anti-platelet Antibodies in Multitransfused Patients
# 1996 Blackwell Science Ltd, British Journal of Haematology 95: 564–569
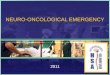
patients. In Fig 1 the patient has had two successfulpregnancies and had previously received non-leucocyte-depleted transfusions, when undergoing intensive chemo-therapy. At the time of this investigation she wasundergoing allogeneic bone marrow transplantation. Theantibody was first detectable by the MAIPA assay aloneand the following samples were also complement fixing.An effect on transfusion response could not be evaluatedbecause no further transfusions were necessary. The otherpatient (Fig 2) had never been pregnant and receivedexclusively leucocyte-depleted transfusions when under-going induction chemotherapy for AML. The pre-existingMAIPA-reactive HLA antibody disappeared shortly afterconditioning for marrow transplantation but reappearedduring a period of infection. At this time, platelettransfusion was not followed by a platelet increment.Again, the MAIPA assay was more sensitive for the detectionof the antibody than the LCT.
In these 17 prospectively studied cases, panreactiveantibodies were present only in preimmunized patients.They were transient in two and remained throughout theobservation period in one patient, respectively. One indivi-dual with a previous history of non-leucocyte-depletedtransfusions formed transient anti-HPA-1b and -5b. Anti-bodies appeared at the time of fever in nine subjects. At thesame time a low CCI indicated non-responsiveness totransfusion therapy in six patients.
DISCUSSION
We have shown that about 50% of blood samples fromhaemato-oncological patients contain platelet-reactive anti-bodies. These antibodies are most frequent in patients witha history of possible immunization (i.e. previous non-leucocyte-depleted transfusions and/or pregnancies), par-ticularly if patients are refractory to platelet therapy. Serumsamples from the refractory patients frequently containedHLA antibodies, even when these patients had no history of
primary immunization and received exclusively leucocyte-depleted blood products.
In a previous study, Novotny et al (1995) showed that 19%of their haemato-oncological patients have HLA antibodies,but only 2.7% of patients with no history of priorimmunization, develop HLA antibodies if transfused withleucocyte-depleted blood products. HLA antibodies can bedetected in 25–70% of patients, who have received non-leucocyte-depleted blood products (Dutcher et al, 1981;Brubaker & Romine, 1987; Slichter, 1990). In all theseinvestigations the presence of HLA antibodies was deter-mined by the reactivity of sera against leucocyte antigensinferring their reactivity against platelets. The need to testfor HLA antibodies, reactive with platelets rather than withlymphocytes, has been emphasized previously (Brand et al,1978). We therefore used the MAIPA technique in all ourpatients to specifically determine the serum reactivity againsthuman �2-microglobulins associated with HLA class I mol-ecules on platelets. Thus, not only cytotoxic (complementactivating) HLA antibodies, but also non-cytotoxic platelet-reactive HLA antibodies were detectable. The higher sensitivityfor the detection of platelet reactive HLA antibodies isillustrated in Figs 1 and 2; serum samples from these patientscontained HLA antibodies, which were reactive by MAIPAbefore becoming positive by the LCT. Similarly, we can assumethat some HLA antibodies were detected by the MAIPA assaywhich could have been missed by the LCT. These maycontribute to the high incidence of HLA antibodies in ourpatients, even if they had no history of a possible previousimmunization. Preimmunized refractory patients had ahigher incidence of HLA antibodies than those thatwere refractory but not preimmunized. In the presence ofMAIPA-positive, LCT-negative HLA antibodies, a reducedresponse to platelet therapy was observed, suggesting abiological effect of these antibodies (Figs 1 and 2). Thisremains to be confirmed in a larger patient population.
In addition to HLA antibodies, a high incidence in ourpatients of panreactive platelet antibodies was seen using the
Fig 2. Transient disappearance of HLAantibodies in a patient who underwent BMTafter a previous treatment for AML. Thepatient has never been pregnant and hasreceived exclusively leucocyte-depleted bloodproducts. The antibody reappeared at the timeof infection, when the patient was refractory toplatelet transfusion therapy. Experimentaldesign as in Fig 1.

MAIPA technique. These findings are similar to those fromprevious studies which applied a platelet immunofluorescencetest (Pegels et al, 1982; McGrath et al, 1988; Doughty et al,1994). We cannot exclude that some of these antibodies wereactually antiplatelet alloantibodies formed due to a patient’srare allotype. These antibodies reacted equally with allplatelets from our panel, which included platelets homo-zygous for HPA-1a/b, -2a/b, -3a/b and -5a/b. In particular,antiplatelet GP IIIa-reactive antibodies may have containedallospecifities, as this GP carries most platelet-specificalloantigens (Newman, 1994). The alloantigens used in thisstudy for the detection of antibodies, however, are consideredthe clinically most relevant platelet antigens in Caucasoidsand it is therefore unlikely that we have missed a significantnumber of alloantibodies to platelet-specific antigens.
Similarly to patients with autoimmune thrombocyto-penia, panreactive antiplatelet antibodies directed againstGP IIb/IIIa were as common as antibodies against GP Ib/IX(Kiefel et al, 1991). Moreover, anti-GP Ia/IIa antibodieswere only detectable in sera that contained also anti-GPIIb/IIIa and anti-GP Ib/IX antibodies (Mueller-Eckhardt,1990).
Anti-HPA antibodies were a rare finding in our patients.50% of the sera which contained anti-HPA antibodies werealso reactive against HLA antigens. As previously reported(Gruber & O’Neill, 1992; Schnaidt et al, 1996), the mostcommon allospecificities were anti-HPA-1b and anti-HPA-5b.Of note, the latter are the most common platelet-specificantibodies induced by pregnancy (Panzer et al, 1995).Therefore it is more likely that these antibodies are presentin females with a prior pregnancy without receiving anytransfusions, or develop as a secondary immune response. Themajority of our preimmunized patients were female and anti-HPA-5b was found in five of them. All combinations of anti-HPA antibodies included immunization against HPA-1, whichfurther emphasizes the immunogenicity of this antigen. Asonly 17% of patients formed HPA antibodies, their influenceon platelet transfusion could not be estimated.
McGrath et al (1988) have indicated that panreactive andHLA antibodies frequently develop only during an episode ofinfection and disappear at varying times after recovery(McGrath et al, 1988). In line with this data, HLA antibodies,panreactive antibodies, and even HPA antibodies weretransiently present in some of our prospectively studiedpatients. Their number is too small for the evaluation of thebiological significance of these antibodies.
ACKNOWLEDGMENTS
The authors are grateful to Mrs A. Neumeister andB. Eichelberger for excellent technical assistance. Thisstudy was supported in part by grant 958 from theMedizinisch-Wissenschaftlicher Fonds des Burgermeistersder Stadt Wien.
REFERENCES
Andreu, G. & Dewailly, J. (1994) Prevention of HLA Alloimmunizationby using leukocyte-depleted components. Leukocyte-Depleted Blood
Products (ed. by T. A. Lane and G. Myllyla), pp. 29–40, Karger,Basel.
Benda, H., Panzer, S., Kiefel, V., Mannhalter, C., Hinterberger, W.,Lechner, K. & Mueller-Eckhardt, C. (1989) Identification of thetarget platelet glycoprotein in autoimmune thrombocytopeniaoccurring after allogeneic bone marrow transplantation. Blut, 58,151–153.
Bishop, J.F., Matthews, J.P., Yuen, K., McGrath, K., Wolf, M.M. &Szer, J. (1992) The definition of refractoriness to platelettransfusions. Transfusion Medicine, 2, 35–41.
Bishop, J.F., McGrath, K., Wolf, M.M., Matthews, J.P., DeLuise, T.,Holdsworth, R., Yuen K., Veale, M., Whiteside, M.G., Cooper, I.A. &Szer, J. (1988) Clinical factors influencing the efficacy of pooledplatelet transfusions. Blood, 71, 383–387.
Brand, A., Sintnicolaas, K., Claas, F.H.J. & Eernisse, J.G. (1986) ABHantibodies causing platelet transfusion refractoriness. Transfusion,26, 463–466.
Brand, A., van Leeuwen, A., Eernisse, J.G. & Van Rood, J.J. (1978)Platelet transfusion therapy: optimal donor selection with acombination of lymphocytotoxicity and platelet fluorescence tests.Blood, 51, 781–788.
Brubaker, D.B. & Romine, M. (1987) Relationship of HLA andplatelet-reactive antibodies in alloimmunized patients refractoryto platelet therapy. American Journal of Hematology, 26, 341–352.
Doughty, H.A., Murphy, M.F., Metcalfe, P., Rohatiner, A.Z.S., Lister, T.A.& Waters, A.H. (1994) Relative importance of immune and non-immune causes of platelet refractoriness. Vox Sanguinis, 66, 200–205.
Dutcher, J.P., Schiffer, C.A., Aisner, J. & Wiernik, P.H. (1981) Long-term follow-up of patients with leukemia receiving platelettransfusions: identification of a large group of patients who donot become alloimmunized. Blood, 58, 1007–1011.
Friedberg, R.C., Donnelly, S.F., Boyd, J.C., Gray, L.S. & Mintz, P.D.(1993) Clinical and blood bank factors in the management ofplatelet refractoriness and alloimmunization. Blood, 81, 3428–3434.
Godeau, B., Fromont, P., Seror, T., Duedari, N. & Bierling, P. (1992)Platelet alloimminization after multiple transfusions: a prospectivestudy of 50 patients. British Journal of Haematology, 81, 395–400.
Gruber, J.A. & O’Neill, G.J. (1992) Frequency of alloimmunization toplatelet-specific antigens in multitransfused thrombocytopenicpatients. Blood, 80, (Suppl.), 218a.
Heal, J.M., Blumberg, N. & Masel, D. (1987) An evaluation ofcrossmatching, HLA, and ABO matching for platelet transfusionsto refractory patients. Blood 70, 23–30.
Holensteiner, A., Walchshofer, S., Adler, A., Kittl, E.M., Mayr, W.R. &Panzer, S. (1995) Human platelet antigen gene frequencies in theAustrian population. Haemostasis, 25, 133–136.
Howard, J.E. & Perkins, H.A. (1978) The natural history ofalloimmunization to platelets. Transfusion, 18, 496–503.
Kickler, T., Kennedy, S.D. & Braine, H.G. (1990) Alloimmunization toplatelet-specific antigens on glycoproteins IIb/IIIa and Ib/IX inmultiply transfused thrombocytopenic patients. Transfusion, 30,622–625.
Kiefel, V., Santoso, S., Kaufmann, E. & Mueller-Eckhardt, C. (1991)Autoantibodies against platelet glycoprotein Ib/IX: a frequentfinding in autoimmune thrombocytopenic purpura. British Journalof Haematology, 79, 256–262.
Kiefel, V., Santoso, S., Weisheit, M. & Mueller-Eckhardt, C. (1987)Monoclonal antibody-specific immobilization of platelet antigens(MAIPA): a new tool for the identification of platelet reactiveantibodies. Blood, 70, 1722–1726.
McGrath, K., Wolf, M., Bishop, J., Veale, M., Ayberk, H., Szer, J.,Cooper, I. & Whiteside, M. (1988) Transient platelet and HLA
# 1996 Blackwell Science Ltd, British Journal of Haematology 95: 564–569
568 Martin Kurz et al

569Anti-platelet Antibodies in Multitransfused Patients
# 1996 Blackwell Science Ltd, British Journal of Haematology 95: 564–569
antibody formation in multitransfused patients with malignancy.British Journal of Haematology, 68, 345–350.
Mueller-Eckhardt, C. (1990) Platelet allo- and autoantigens andtheir clinical implications. Transfusion Medicine in the 1990s (ed. byS. T. Nance), pp. 63–93. American Association of Blood Banks,Arlington, Va.
Murphy, M.F., Metcalfe, P., Ord, J., Lister, T.A. & Waters, A.H. (1987)Disappearance of HLA and platelet-specific antibodies in acuteleukaemia patients alloimmunized by multiple transfusions.British Journal of Haematology, 67, 255–260.
Murphy, M.F. & Waters, A.H. (1985) Immunological aspects ofplatelet transfusion. British Journal of Haematology, 60, 409–414.
Newman P.J. (1994) Nomenclature of human platelet alloantigens: aproblem with the HPA system? Blood, 83, 1447–1451.
Novotny, V.M., van Doorn, R., Witvliet, M.D., Claas, F.H. & Brand, A.(1995) Occurrence of allogeneic HLA and non-HLA antibodiesafter transfusion of prestorage filtered platelets and red blood cells:a prospective study. Blood, 85, 1736–1741.
O’Connell, B., Lee, E.J. & Schiffer, C.A. (1988) The value of 10-minute posttransfusion platelet counts. Transfusion, 28, 66–67.
Pamphilon, D.H., Farrell, D.H., Donaldson, C., Raymond, P.A.,Brady, C.A. & Bradley, P.A. (1989) Development of lymphocyto-toxic and platelet reactive antibodies: a prospective study inpatients with acute leukemia. Vox Sanguinis, 57, 177–81.
Panzer, S., Auerbach, L., Fischer, G., Holensteiner, A., Kittl, E.M.,Mayr, W.R., Putz, M., Wagenbichler, P. & Walchshofer, S. (1995)Maternal alloimmunization against fetal platelet antigens: a
prospective study. British Journal of Haematology, 90, 655–660.Panzer, S., Maier, F., Hocker, P., Mayr, W.R. & Hinterberger, W.
(1987) Platelet transfusion: influence of clinical and immuno-logical conditions. Infusionstherapie und Klinische Ernahrung, 14,(Suppl. 2), 10–14.
Pegels, J.G., Bruynes, E.C.E., Engelfriet, C.P. & von dem Borne, A.E.G.Kr.(1982) Serological studies in patients on platelet- and granulo-cyte-substitution therapy. British Journal of Haematology, 52, 59–68.
Schnaidt, M., Northoff, H. & Wernet, D. (1996) Frequency andspecificity of platelet-specific alloantibodies in HLA-immunizedhaemato-oncologic patients. Transfusion Medicine, 6, 111–114.
Simsek, S., Faber, N.M., Bleeker, P.M., Vlekke, A.B.J., Huiskes, E.,Goldschmeding, R. & von dem Borne, A.E.G.Kr. (1993) Deter-mination of human platelet antigen frequencies in the Dutchpopulation by immunophenotyping and DNA (allele-specificrestriction enzyme) analysis. Blood, 81, 835–840.
Sintnicolaas, K., van Marwijk Kooij, M., van Prooijen, H.C.,van Dijk, B.A., van Putten, W.L.J., Claas, F.H.J., Novotny, V.J.M. &Brand, A. (1995) Leukocyte depletion of random single-donorplatelet transfusions does not prevent secondary human leukocyteantigen-alloimmunization and refractoriness: a randomizedprospective study. Blood, 85, 824–828.
Slichter, S.J. (1990) Mechanisms and management of plateletrefractoriness. Transfusion Medicine in the 1990s (ed. by S. T.Nance), pp. 95–179. American Association of Blood Banks,Arlington, Va.