Embed Size (px)
Citation preview

Leukemia Research Vol. 13, No, 5, pp. 367-376, 1989. 0145-2126/89 $3.00 + .00 Printed in Great Britain. Pergamon Press plc
SPECIFIC CHROMOSOME CHANGES AND NON- OCCUPATIONAL EXPOSURE TO POTENTIALLY
CARCINOGENIC AGENTS IN ACUTE LEUKEMIA IN CHINA
YoU-SHENG LI, YU-LAN ZHAO, QI-Po JIANG and CONG-LI YANG
Institute of Hematology, Chinese Academy of Medical Sciences, Tianjin, People's Republic of China
(Received 13 October 1988. Accepted 19 November 1988)
Abstract---Cytogenetic studies were performed on 44 Chinese patients with acute leukemia. A high percentage of patients (37.5%) with t(8;21), t(15;17) or 17q- (in poorly banded preparations), and abnormalities involving 11q23 were noted in 32 unselected patients with ANLL. A similar high percentage was previously reported in Japan and in South Africa but not in westem countries. Data on casual or other non-occupational exposure to potentially carcinogenic agents were obtained by interview with the patients at their first presentation. Most patients with these three major chromo- somal changes had a history of exposure, whereas most other patients did not (p = 0.01). Patients with ANLL-M3 were more often exposed than were the other patients (4/6 vs 8/38, p = 0.03). The only common exposure was to organophosphate insecticides. Twenty seven cases of therapy-related leukemia were collected from the Chinese medical literature, and 12 out of 22 (55%) cases in which subtypes were specified were ANLL-M3. This was significantly higher than the percentage of M3 in de novo ANLL in China and also higher than that of therapy-related leukemia from western countries. Two patients had siblings who died of leukemia at a similar age. The two patients showed inv(16) and del(6q) respectively.
Key words: Chromosomes, exposure to carcinogens, therapy-related leukemia, leukemia.
THE DEVELOPMENT of leukemia may depend on the action of environmental carcinogenic agents against the genetic background of the patients. The incidence of leukemia is expected to vary in different parts of the world. However , the reasons for the variation in the incidence of subtypes of acute leukemia in different countries remain obscure because the sub- classification is still based on morphological criteria. These differences are particularly notable in ANLL, where the rate of disagreements among different hematologists is often high. Cytogenetic studies have revealed many specific chromosomal changes which are uniquely associated with specific types of cancer. Molecular analysis has indicated that alterations in the level of expression of the involved genes or in the properties of the encoded proteins resulting from these specific chromosomal changes play an integral role in the process of malignant transformation [1, 2].
Abbreviations: ALL, acute lymphocytic leukemia; ANLL, acute non-lymphocytic leukemia; BrdU, bromodeoxyuridine; CML, chronic myeloid leukemia; FrdU, fluorodeoxyuridine; ICRF-154, 1,2-bL~(3,5-deoxo- piperazin-l-yl) ethane; PHA, phytohemagglutinin.
Correspondence to: Dr Cong-Li Yang, Institute of Hematology, 288 Nanjing Road, Tianjin, People's Repub- lic of China.
367
The Fourth International Workshop on Chromo- somes in Leukemias compiled 716 cases of ANLL from all over the world and found a high incidence of three major specific chromosomal changes, t(8;21)(q22;q22), t(15;17)(q22;q21) and rearrange- ments involving chromosome l l q in Japan and in South Africa [3]. Some chromosomal changes have been found to be associated with patients' previous occupational exposure [3-5]. However , no time consequent events could be documented and appar- ent contradictory results appeared [6] because of difficulties in ascertainment of exposure as well as whether an agent is carcinogenic/mutagenic or not. In an attempt to determine the frequency of these three major chromosomal changes in China and their possible cause, we found that they are also very common in China and they were linked with non- occupational exposure to carcinogenic agents.
M A T E R I A L S AND M E T H O D S
1. Patients From January 1985 to December 1986, a total of 44
patients with acute leukemia were karyotyped. Thirty-two of the patients with ANLL were unselected, i.e. cytogenetic studies were performed when the patients were first seen and suspected to have leukemia and a bone marrow aspir-
368 You-StroNG LI et al.
ation was requested. All patients were Chinese from Tian- jin or other areas of northern China.
The classification of acute leukemia was based on the proposals by the FAB Cooperative Group [7, 8].
2. Patients' exposure to potentially carcinogenic agents Thirty-one of our patients were from rural areas and the
majority of them were peasants. The peasants in China are not exactly the same as farmers in western countries, and the majority of Chinese peasants do not have direct contact with insecticides and they live in a relatively less polluted environment. They usually drink water from wells and their foods are from their own lands. Thus our data on patients' exposure were obtained from direct interview with patients by clinicians before the diagnosis of leukemia was made and before the cytogenetic studies were per- formed. The patients were asked if they had been exposed to radiation or any chemicals. The recorded exposures as shown in Table 2 may well not be carcinogenic or mutagenic, e.g. exposures to fluorine, urea, ammonium nitrate, polyvinyl chloride, but no change was made in order to avoid subjective bias. The possible occupational exposure was determined by the first author of this paper based on relevant medical records.
3. Cytogenetic studies Conventional techniques were applied for cell culture,
harvesting, and chromosome banding [9, 10]. Limited by equipments and chemicals available, all kary-
otypic analysis was done under the microscope and no further analysis was attempted for complex karyotypes. Even though emphasis was put on the ascertainment of the three major chromosomal changes, t(8;21), t(15;17), and rearrangements involving l lq in order to determine their frequency in China, the subtle alteration of the 11q23 might be missed in poorly banded preparations.
RESULTS
1. Karyotypes
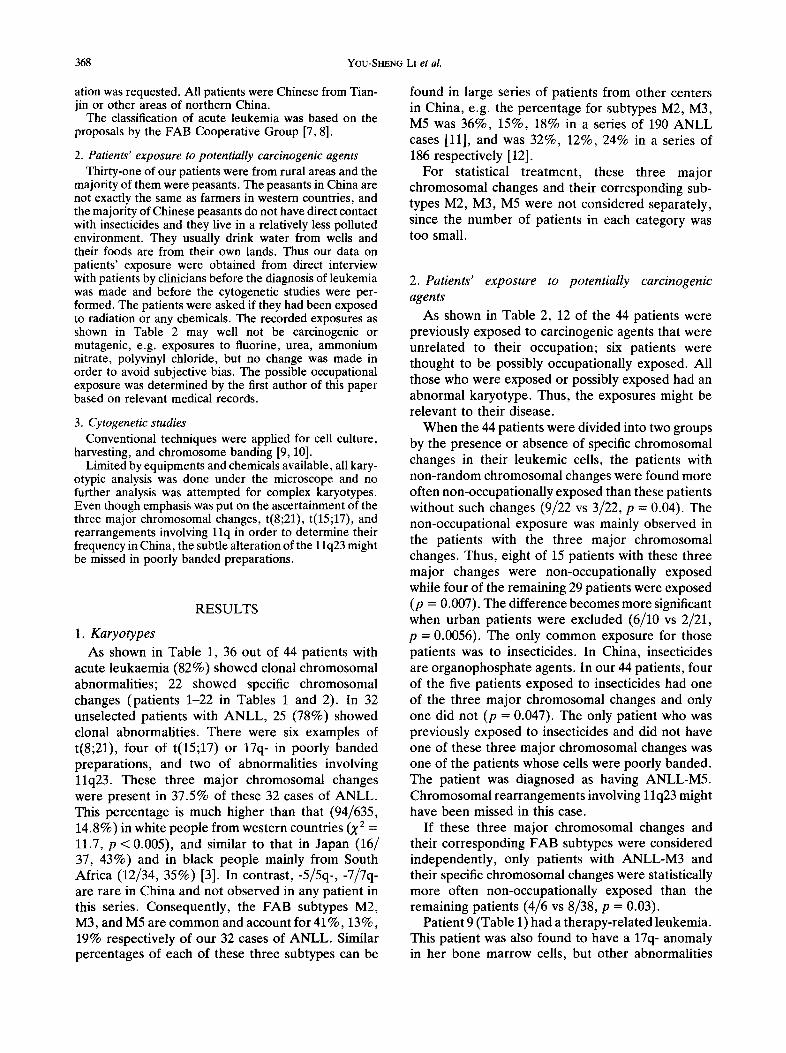
As shown in Table 1, 36 out of 44 patients with acute leukaemia (82%) showed clonal chromosomal abnormalities; 22 showed specific chromosomal changes (patients 1-22 in Tables 1 and 2). In 32 unselected patients with ANLL, 25 (78%) showed clonal abnormalities. There were six examples of t(8;21), four of t(15;17) or 17q- in poorly banded preparations, and two of abnormalities involving 11q23. These three major chromosomal changes were present in 37.5% of these 32 cases of ANLL. This percentage is much higher than that (94/635, 14.8%) in white people from western countries (X 2 = 11.7, p < 0.005), and similar to that in Japan (16/ 37, 43%) and in black people mainly from South Africa (12/34, 35%) [3]. In contrast , -5/5q- , -7/7q- are rare in China and not observed in any patient in this series. Consequently, the FAB subtypes M2, M3, and M5 are common and account for 41%, 13%, 19% respectively of our 32 cases of ANLL. Similar percentages of each of these three subtypes can be
found in large series of patients from other centers in China, e.g. the percentage for subtypes M2, M3, M5 was 36%, 15%, 18% in a series of 190 ANLL cases [11], and was 32%, 12%, 24% in a series of 186 respectively [12].
For statistical treatment, these three major chromosomal changes and their corresponding sub- types M2, M3, M5 were not considered separately, since the number of patients in each category was too small.
2. Patients' exposure to potentially carcinogenic agents
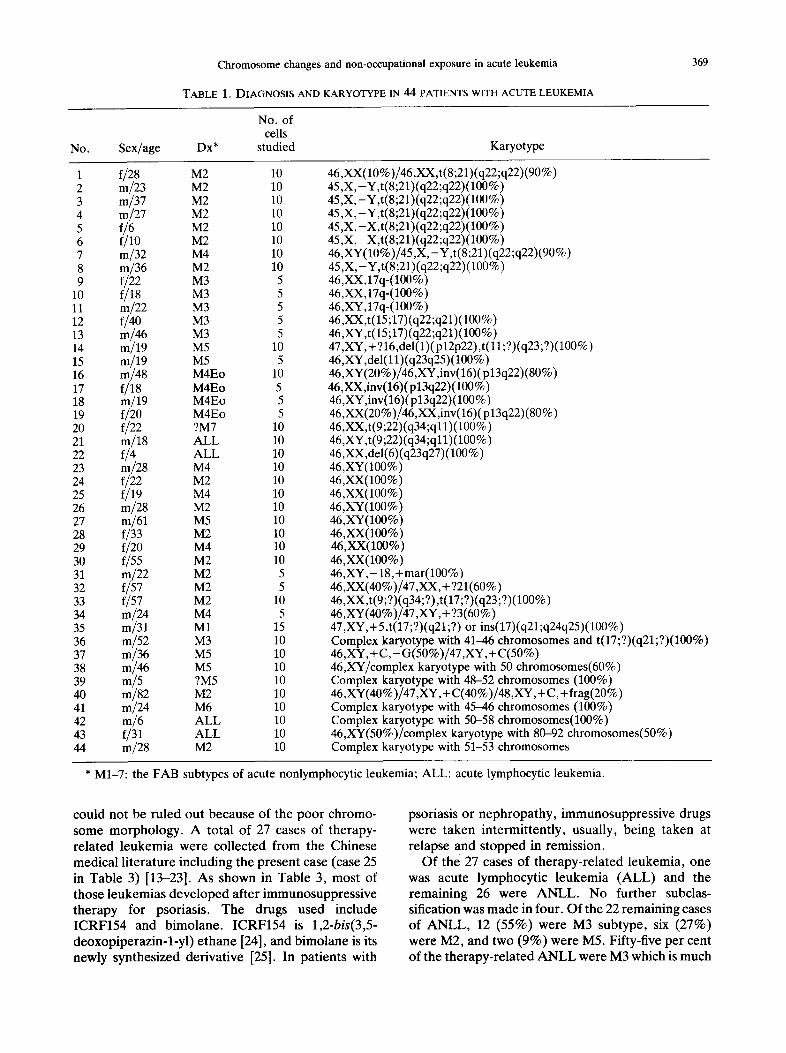
As shown in Table 2, 12 of the 44 patients were previously exposed to carcinogenic agents that were unrelated to their occupation; six patients were thought to be possibly occupationally exposed. All those who were exposed or possibly exposed had an abnormal karyotype. Thus, the exposures might be relevant to their disease.
When the 44 patients were divided into two groups by the presence or absence of specific chromosomal changes in their leukemic cells, the patients with non-random chromosomal changes were found more often non-occupationally exposed than these patients without such changes (9/22 vs 3/22, p = 0.04). The non-occupational exposure was mainly observed in the patients with the three major chromosomal changes. Thus, eight of 15 patients with these three major changes were non-occupationally exposed while four of the remaining 29 patients were exposed (p = 0.007). The difference becomes more significant when urban patients were excluded (6/10 vs 2/21, p = 0.0056). The only common exposure for those patients was to insecticides. In China, insecticides are organophosphate agents. In our 44 patients, four of the five patients exposed to insecticides had one of the three major chromosomal changes and only one did not (p = 0.047). The only patient who was previously exposed to insecticides and did not have one of these three major chromosomal changes was one of the patients whose cells were poorly banded. The patient was diagnosed as having ANLL-M5. Chromosomal rearrangements involving 1 lq23 might have been missed in this case.
If these three major chromosomal changes and their corresponding FAB subtypes were considered independently, only patients with ANLL-M3 and their specific chromosomal changes were statistically more often non-occupationally exposed than the remaining patients (4/6 vs 8/38, p = 0.03).
Patient 9 (Table 1) had a therapy-related leukemia. This patient was also found to have a 17q- anomaly in her bone marrow cells, but other abnormalities
Chromosome changes and non-occupational exposure in acute leukemia
TABLE 1. DIAGNOSIS AND KARYOTYPE IN 44 PATIENTS WITH ACUTE LEUKEMIA
369
No.
No. of cells
Sex/age Dx* studied Karyotype
1 f/28 M2 10 2 m/23 M2 10 3 m/37 M2 10 4 m/27 M2 10 5 f/6 M2 10 6 f/lO M2 10 7 m/32 M4 10 8 m/36 M2 10 9 f/22 M3 5
10 f/18 M3 5 11 m/22 M3 5 12 f/40 M3 5 13 m/46 M3 5 14 m/19 M5 10 15 m/19 M5 5 16 m/48 M4Eo 10 17 f/18 M4Eo 5 18 m/19 M4Eo 5 19 f/20 M4Eo 5 20 f/22 ?M7 10 21 m/18 ALL 10 22 f/4 ALL 10 23 m/28 M4 10 24 f/22 M2 10 25 f/19 M4 10 26 m/28 M2 10 27 rn/61 M5 10 28 f/33 M2 10 29 f/20 M4 10 30 f/55 M2 10 31 m/22 M2 5 32 f/57 M2 5 33 f/57 M2 10 34 m/24 M4 5 35 m/31 M1 15 36 m/52 M3 10 37 m/36 M5 10 38 m/46 M5 10 39 m/5 ?M5 10 40 m/82 M2 10 41 m/24 M6 10 42 m/6 ALL 10 43 f/31 ALL 10 44 m/28 M2 10
46,XX(lO%)/46,XX,t(8;21)(q22;q22)(90%) 45,X,-V,t(8;21)(q22;q22)(lO0%) 45,X,-Y,t(8;21)(qZ2;qZ2)(100%) 45,X,-Y,t(8;21)(qZZ;qZ2)(100%) 45,X,-X,t(8;Zl)(q22;qZ2)(100%) 45,X,-X,t(S;Zl)(qZZ;qZ2)(100%) 46,XY(lO%)/45,X,-Y,t(8;Z1)(qZ2;q22)(90%) 45,X,-Y,t(8;Zl)(qZZ;qZ2)(lO0%) 46,XX,lYq-(100%) 46,XX,17q-(100%) 46,XY,17q-(100%) 46,XX,t(15;17)(q22;q21)(100%) 46,XY,t(15;17)(q22;q21)(100%) 47,XY,+ ?16,del(1)(plEp22),t(11;?)(q23;?)(100%) 46,XY,del(l 1)(q23q25) (100%) 46,XY(20%)/46,XY,inv(16)(p13q22)(80%) 46,XX,inv(16)(plaq22)(100%) 46,XY,inv(16)(plaq22)(100%) 46,XX(20%)/46,XX,inv(16)(p13q22)(80%) 46,XX,t(9;E2)(qa4;q11)(100%) 46,XY,t(9;22)(q34;ql 1)(100%) 46 ,XX,del(6)(q23q27) (100%) 46,XY(100%) 46,XX(100%) 46,XX(100%) 46,XY(100%) 46,XY(100%) 46,XX(100%) 46,XX(100%) 46,XX(100%) 46,XY,- 18,+mar(100%) 46,XX(40%)/47,XX, + 721(60%) 46,XX,t(9;?)(qa4;?),t(17;?)(q23;?)(100%) 46,XY(40%)/47,XY, + ?3(60%) 47,XY,+5,t(17;?)(q21;?) or ins(17)(q21;q24q25)(100%) Complex karyotype with 41-46 chromosomes and t(17;?)(q21;?)(100%) 46,XY, + C,- G(50%)/47 ,XY, + C(50%) 46,XY/complex karyotype with 50 chromosomes(60%) Complex karyotype with 48-52 chromosomes (100%) 46,XY(40%)/47,XY,+C(40%)/48,XY,+C,+frag(20%) Complex karyotype with 45-46 chromosomes (100%) Complex karyotype with 50-58 chromosomes(100%) 46,XY(50%)/complex karyotype with 80-92 chromosomes(50%) Complex karyotype with 51-53 chromosomes
* M1-7: the FAB subtypes of acute nonlymphocytic leukemia; ALL: acute lymphocytic leukemia.
could not be ruled out because of the poor chromo- some morphology. A total of 27 cases of therapy- related leukemia were collected from the Chinese medical literature including the present case (case 25 in Table 3) [13-23]. As shown in Table 3, most of those leukemias developed after immunosuppressive therapy for psoriasis. The drugs used include ICRF154 and bimolane. ICRF154 is 1,2-bis(3,5- deoxopiperazin-l-yl) ethane [24], and bimolane is its newly synthesized derivative [25]. In patients with
psoriasis or nephropathy, immunosuppressive drugs were taken intermittently, usually, being taken at relapse and stopped in remission.
Of the 27 cases of therapy-related leukemia, one was acute lymphocytic leukemia (ALL) and the remaining 26 were ANLL. No further subclas- sification was made in four. Of the 22 remaining cases of ANLL, 12 (55%) were M3 subtype, six (27%) were M2, and two (9%) were M5. Fifty-five per cent of the therapy-related ANLL were M3 which is much
370 You-SHENG LI et al.
TABLE 2. CARCINOGENIC EXPOSURE IN 44 PATIENTS WITH ACUTE LEUKEMIA
Non-occupational Possible occupational No. Residence exposure Occupation exposure
1 Rural Insecticides Peasant 2 Rural Isoniazid Student 3 Rural Mechanic Petrol products 4 Urban Worker 5 Rural Child 6 Rural Student 7 Rural Fluorine Cadre 8 Urban Machinist Petrol products 9 Urban ICRF154 Worker
10 Urban Worker 11 Urban Benzene, solvent Student 12 Rural Insecticides Worker 13 Rural Insecticides Peasant 14 Rural Insecticides Peasant 15 Rural Student Petrol products
(living in oil field) 16 Urban Teacher 17 Urban Student 18 Rural Student 19 Rural Peasant 20 Urban Electric welder 21 Rural Urea, ammonium Peasant
nitrate 22 Rural Child 23 Rural Office worker 24 Rural Peasant 25 Rural Peasant 26 Rural Worker 27 Rural Cadre 28 Urban Cadre 29 Rural Worker 30 Rural Peasant 31 Rural Peasant 32 Rural Housewife 33 Rural Peasant 34 Urban Polyvinyl chloride Worker 35 Rural Cadre
36 Rural Worker 37 Rural Insecticides Peasant 38 Rural Peasant 39 Rural Child 40 Urban Worker 41 Urban Little X ray Electric welder 42 Rural Child 43 Urban Teacher 44 Rural Peasant
Metal, electrical magnetic field
Chemicals (worked in a small chemical factory)
Metal, electrical magnetic field
higher than the percentage of patients with M3 in de
n o v o A N L L in China (10-15%), and is also much higher than that in the present 32 unselected patients with A N L L (Z 2 = 11, p < 0.005). This suggests that the immunosuppressive therapy received for the patients ' pr imary disorders was relevant to the sub- sequent development of leukemia. The interval t ime from the beginning of chemotherapy to the diagnosis
of leukemia was f rom 0.8 to 22 yr with a mean of 5 yr and a median t ime of 4 yr.
Rosner and Griinward [26] collected 615 cases of therapy-related A N L L from the literature including 93 secondary to a therapy for non-neoplastic disorders. Of those 615 cases, 12 (3%) were M3, 23 (4%) were M5, and 335 (54%) were myeloblastic (M1 or M2). No obvious difference was present
Chromosome changes and non-occupational exposure in acute leukemia
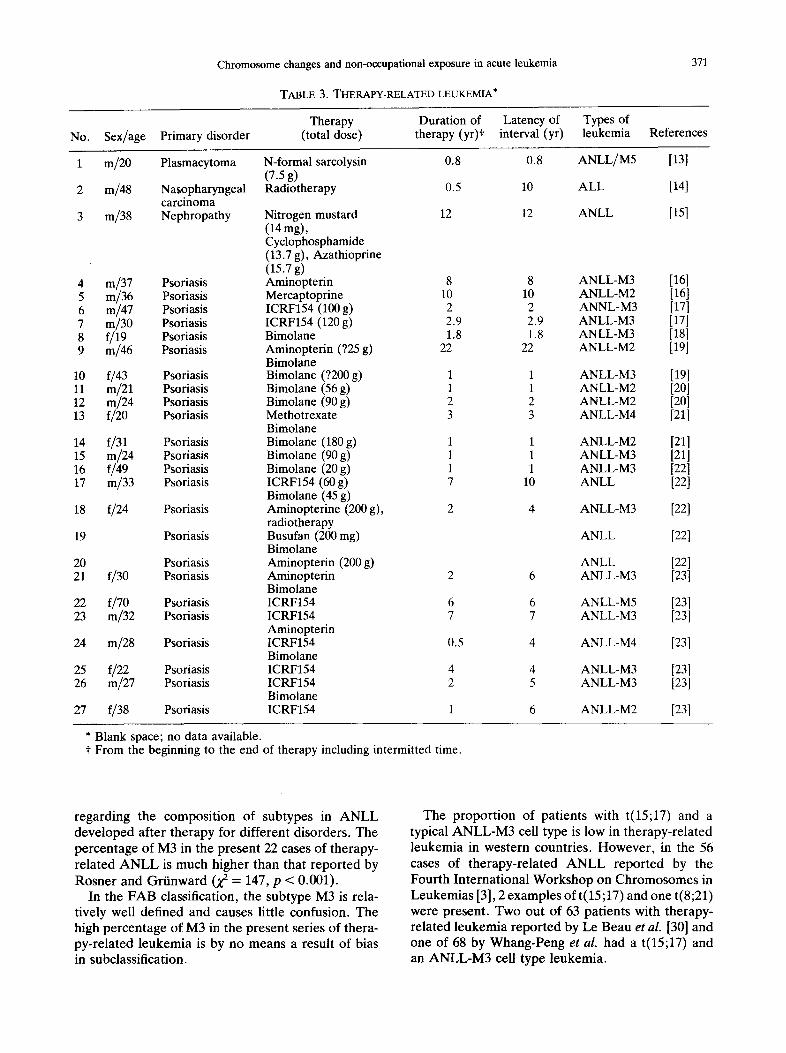
TABLE 3. THERAPY-RELATED LEUKEMIA*
371
Therapy Duration of Latency of Types of No. Sex/age Primary disorder (total dose) therapy (yr)t interval (yr) leukemia References
1 m/20 Plasmacytoma N-formal sarcolysin 0.8 0.8 (7.5 g)
2 m/48 Nasopharyngeal Radiotherapy 0.5 10 carcinoma
3 m/38 Nephropathy Nitrogen mustard 12 12 (14 mg), Cyclophosphamide (13.7 g), Azathioprine (15.7 g)
4 m/37 Psoriasis Aminopterin 8 8 5 m/36 Psoriasis Mercaptoprine 10 10 6 m/47 Psoriasis ICRF154 (100 g) 2 2 7 m/30 Psoriasis ICRF154 (120 g) 2.9 2.9 8 f/19 Psoriasis Bimolane 1.8 1.8 9 m/46 Psoriasis Aminopterin (?25 g) 22 22
Bimolane 10 f/43 Psoriasis Bimolane (?200 g) 1 1 11 m/21 Psoriasis Bimolane (56 g) 1 1 12 m/24 Psoriasis Bimolane (90 g) 2 2 13 f/20 Psoriasis Methotrexate 3 3
Bimolane 14 f/31 Psoriasis Bimolane (180 g) 1 1 15 m/24 Psoriasis Bimolane (90 g) 1 1 16 f/49 Psoriasis Bimolane (20 g) 1 1 17 m/33 Psoriasis ICRF154 (60 g) 7 10
Bimolane (45 g) 18 f/24 Psoriasis Aminopterine (200 g), 2 4
radiotherapy 19 Psoriasis Busufan (200 mg)
Bimolane 20 Psoriasis Aminopterin (200 g) 21 f/30 Psoriasis Aminopterin 2 6
Bimolane 22 f/70 Psoriasis ICRF154 6 6 23 m/32 Psoriasis ICRF154 7 7
Aminopterin 24 m/28 Psoriasis ICRF154 0.5 4
Bimolane 25 f/22 Psoriasis ICRF154 4 4 26 m/27 Psoriasis ICRF154 2 5
Bimolane 27 f/38 Psoriasis ICRF154 1 6
ANLL/M5 [13]
ALL [141
ANLL [15]
ANLL-M3 [16] ANLL-M2 [16] ANNL-M3 [17] ANLL-M3 [17] ANLL-M3 [181 ANLL-M2 [19]
ANLL-M3 [19] ANLL-M2 [201 ANLL-M2 [201 ANLL-M4 [211
ANLL-M2 1211 ANLL-M3 1211 ANLL-M3 [22] ANLL [221
ANLL-M3 [221
ANLL [22]
ANLL [22] ANLL-M3 [23 t
ANLL-M5 [23] ANLL-M3 [231
ANLL-M4 1231
ANLL-M3 [23] ANLL-M3 [231
ANLL-M2 [23]
* Blank space; no data available. f From the beginning to the end of therapy including intermitted time.
regarding the composition of subtypes in ANLL developed after therapy for different disorders. The percentage of M3 in the present 22 cases of therapy- related A N L L is much higher than that reported by Rosner and Griinward (Z 2 = 147, p < 0.001).
In the FAB classification, the subtype M3 is rela- tively well defined and causes little confusion. The high percentage of M3 in the present series of thera- py-related leukemia is by no means a result of bias in subclassification.
The proportion of patients with t(15;17) and a typical ANLL-M3 cell type is low in therapy-related leukemia in western countries. However, in the 56 cases of therapy-related A N L L reported by the Fourth International Workshop on Chromosomes in Leukemias [3], 2 examples of t(15 ;17) and one t(8;21) were present. Two out of 63 patients with therapy- related leukemia reported by Le Beau et al. [30] and one of 68 by Whang-Peng et al. had a t(15;17) and an ANLL-M3 cell type leukemia.
372 You-SHENG LI et al.
3. Familial leukemia
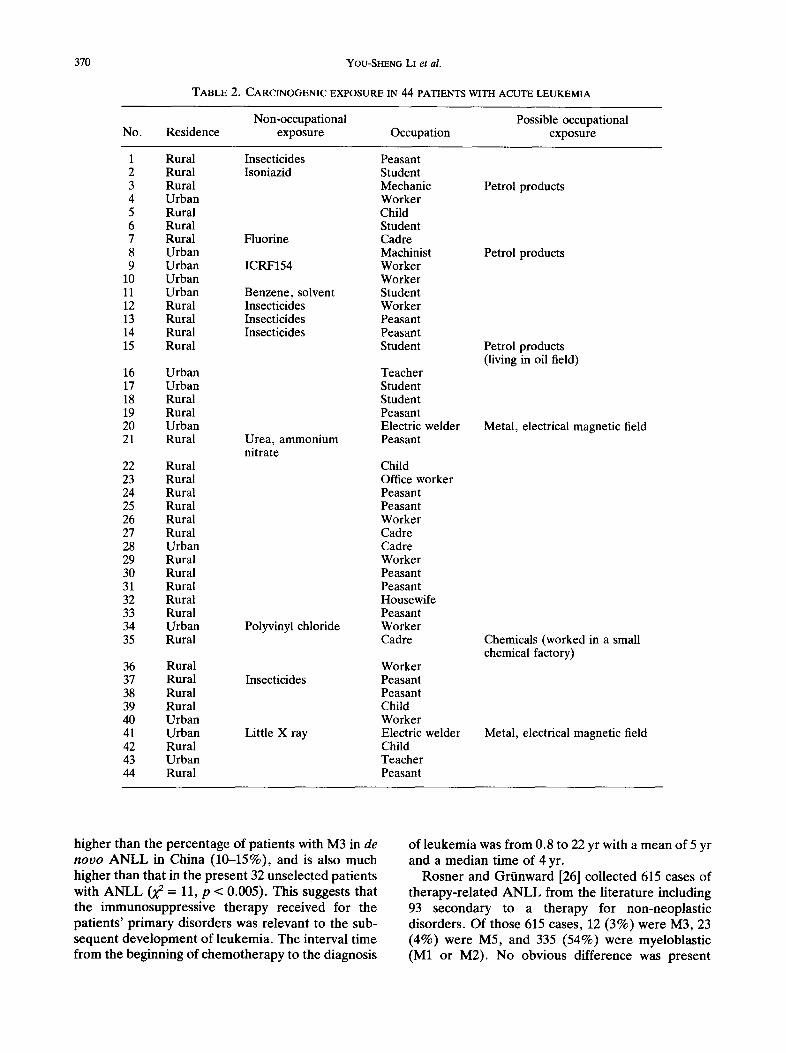
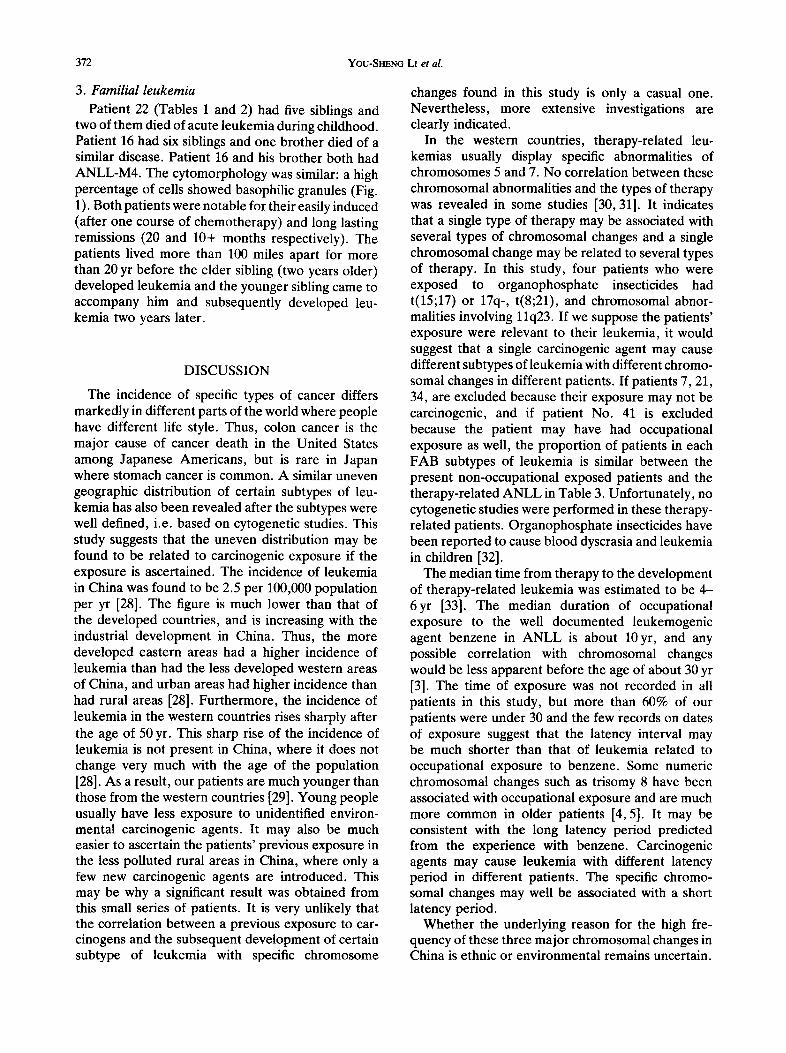
Patient 22 (Tables 1 and 2) had five siblings and two of them died of acute leukemia during childhood. Patient 16 had six siblings and one brother died of a similar disease. Patient 16 and his brother both had ANLL-M4. The cytomorphology was similar: a high percentage of cells showed basophilic granules (Fig. 1). Both patients were notable for their easily induced (after one course of chemotherapy) and long lasting remissions (20 and 10+ months respectively). The patients lived more than 100 miles apart for more than 20 yr before the elder sibling (two years older) developed leukemia and the younger sibling came to accompany him and subsequently developed leu- kemia two years later.
DISCUSSION
The incidence of specific types of cancer differs markedly in different parts of the world where people have different life style. Thus, colon cancer is the major cause of cancer death in the United States among Japanese Americans, but is rare in Japan where stomach cancer is common. A similar uneven geographic distribution of certain subtypes of leu- kemia has also been revealed after the subtypes were well defined, i.e. based on cytogenetic studies. This study suggests that the uneven distribution may be found to be related to carcinogenic exposure if the exposure is ascertained. The incidence of leukemia in China was found to be 2.5 per 100,000 population per yr [28]. The figure is much lower than that of the developed countries, and is increasing with the industrial development in China. Thus, the more developed eastern areas had a higher incidence of leukemia than had the less developed western areas of China, and urban areas had higher incidence than had rural areas [28]. Furthermore, the incidence of leukemia in the western countries rises sharply after the age of 50 yr. This sharp rise of the incidence of leukemia is not present in China, where it does not change very much with the age of the population [28]. As a result, our patients are much younger than those from the western countries [29]. Young people usually have less exposure to unidentified environ- mental carcinogenic agents. It may also be much easier to ascertain the patients' previous exposure in the less polluted rural areas in China, where only a few new carcinogenic agents are introduced. This may be why a significant result was obtained from this small series of patients. It is very unlikely that the correlation between a previous exposure to car- cinogens and the subsequent development of certain subtype of leukemia with specific chromosome
changes found in this study is only a casual one. Nevertheless, more extensive investigations are clearly indicated.
In the western countries, therapy-related leu- kemias usually display specific abnormalities of chromosomes 5 and 7. No correlation between these chromosomal abnormalities and the types of therapy was revealed in some studies [30, 31]. It indicates that a single type of therapy may be associated with several types of chromosomal changes and a single chromosomal change may be related to several types of therapy. In this study, four patients who were exposed to organophosphate insecticides had t(15;17) or 17q-, t(8;21), and chromosomal abnor- malities involving 11q23. If we suppose the patients' exposure were relevant to their leukemia, it would suggest that a single carcinogenic agent may cause different subtypes of leukemia with different chromo- somal changes in different patients. If patients 7, 21, 34, are excluded because their exposure may not be carcinogenic, and if patient No. 41 is excluded because the patient may have had occupational exposure as well, the proportion of patients in each FAB subtypes of leukemia is similar between the present non-occupational exposed patients and the therapy-related ANLL in Table 3. Unfortunately, no cytogenetic studies were performed in these therapy- related patients. Organophosphate insecticides have been reported to cause blood dyscrasia and leukemia in children [32].
The median time from therapy to the development of therapy-related leukemia was estimated to be 4- 6yr [33]. The median duration of occupational exposure to the well documented leukemogenic agent benzene in ANLL is about 10 yr, and any possible correlation with chromosomal changes would be less apparent before the age of about 30 yr [3]. The time of exposure was not recorded in all patients in this study, but more than 60% of our patients were under 30 and the few records on dates of exposure suggest that the latency interval may be much shorter than that of leukemia related to occupational exposure to benzene. Some numeric chromosomal changes such as trisomy 8 have been associated with occupational exposure and are much more common in older patients [4, 5]. It may be consistent with the long latency period predicted from the experience with benzene. Carcinogenic agents may cause leukemia with different latency period in different patients. The specific chromo- somal changes may well be associated with a short latency period.
Whether the underlying reason for the high fre- quency of these three major chromosomal changes in China is ethnic or environmental remains uncertain.
o B
o
yL,{~
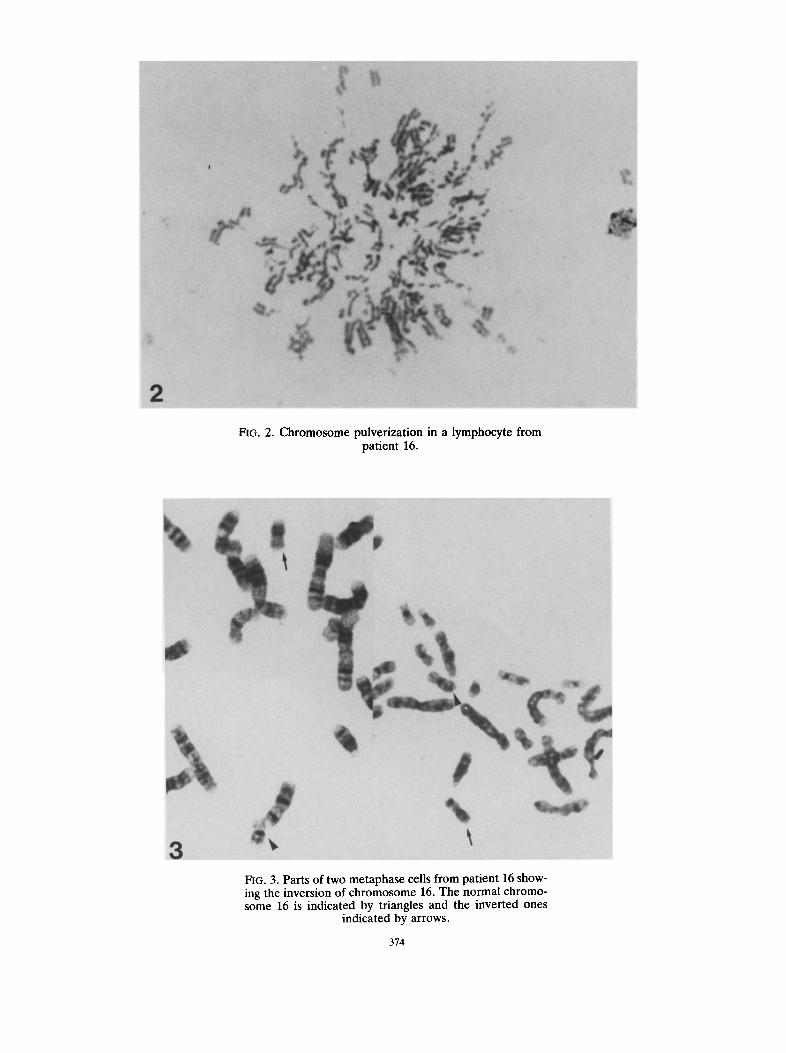
s~oaJ~ Aq p~J!pu! ~atlO palJaAU! aql pue Sal~Ue.Ul £q pale0!pu! s! 9I auios -ouio.tq3 Ieui.tOU aqz "91 auiosouio./qa ~o UO!SaaAU! aql gm -,~oqs 9I lua!led UlOaj SIlOO aseqdelaui OrAl Jo slzed "g "Did
%
i
1:;
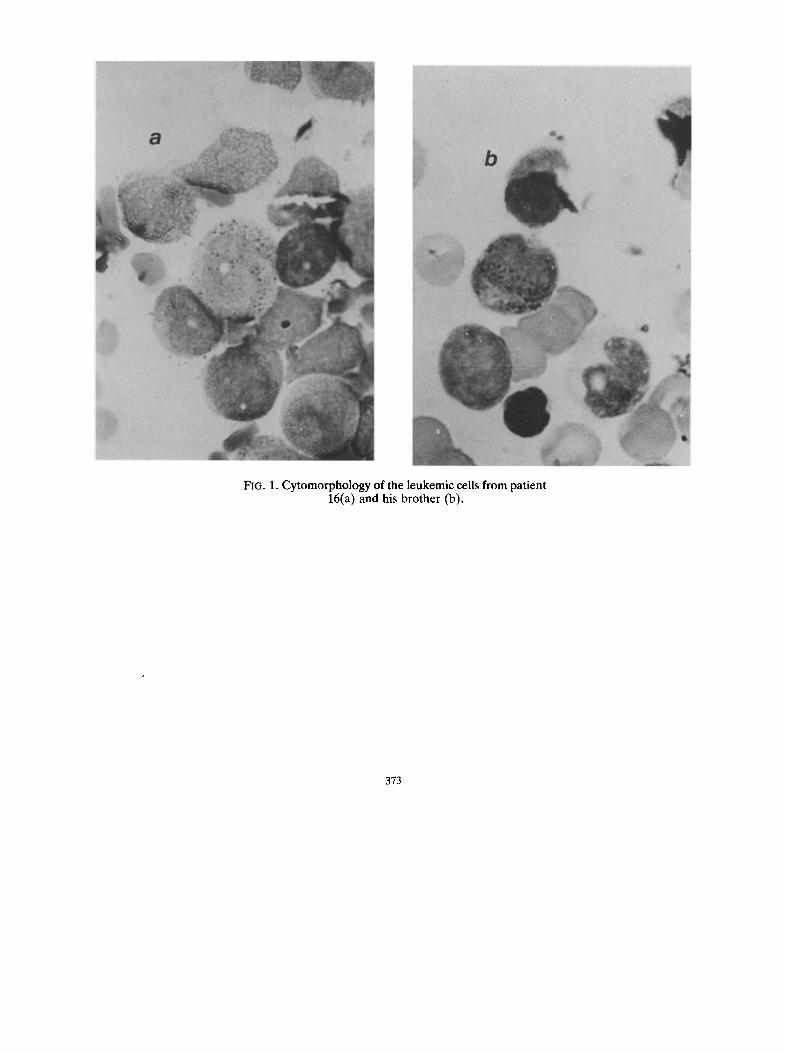
-9 L ~u~!J,~u moa:t a~.~aoqdui~(l ~ u! uop, ez.ua^lnd amosomoaqD "~ "oL4
Chromosome changes and non-occupational exposure in acute leukemia 375
Although they were found to be associated with carcinogenic exposure in this study, it may well be a different ethnic response to a similar industrial pollution. A high percentage of patients with t(8;21) was also reported in Russia [34].
In this study two patients who showed inv(16) and del(6q) had siblings who died of leukemia. In patient 16, peripheral blood cells obtained during remission were stimulated by PHA and cultured with caffeine, FrdU [27], or with BrdU to study fragile sites. An increase in the frequency of chromosomal aber- rations was noted (data not shown), and chromo- somes were pulverized in some cells cultured with caffeine (Fig. 2). Breaks were occasionally seen at 16q22, but were thought to be part of the results of chromosomal fragility in this patient. These siblings had leukemia at a similar age. An explanation is that a common transient environmental agent and inherited susceptibility might have been the cause of their leukemia. Interestingly, a childhood cluster of acute promyelocytic leukemia (M3) has been reported recently in South Africa [35]. Four of their nine patients who were studied cytogenetically, each showed the t(15;17). The authors pointed out that an environmental factor might offer a more likely explanation for the apparent temporal and spatial clustering of these cases. The best known specific chromosomal change t(9;22)(q34;q11) was supposed to superimpose upon a pre-existing monoclonal cell proliferation [36]. Furthermore, the occurrence of t(15;17) in Ph' chromosome positive chronic myeloid leukemia (CML) is associated with blastic trans- formation in promyelocytic cell type [37]. Conceiv- ably, chromosomal fragility, acquired or inherited, and exposure to carcinogenic agents that cause chromosomal aberration may predispose to the emergence of a clone with specific chromosomal changes in such patients. The cell type of the leu- kemia which so develops is decided by the cell type of pre-existing monoclonal proliferation but may also be decided by the type of specific chromosome changes or by both.
In the light of this study as well as of others [31, 38], highly specific chromosomal changes may well occur in therapy-related or carcinogenic-exposure-related leukemia. The majority of human cancers are caused by exposure to known or unknown carcinogenic agents. It may require the collaborative efforts of epidemiologists and cytogeneticists to identify those unknown environmental carcinogenic agents.
Acknowledgements--The authors wish to thank Dr Michelle M. Le Beau, Department of Medicine, University of Chicago, Chicago, for her careful reading and con- structive criticism of the manuscript, Dr Shi-Rong Xu,
Hebei Medical College, China, for supplying some clinical data.
REFERENCES
1. Rowley J. D. (1984) Biological implications of con- sistent chromosome rearrangements in leukemia and lymphoma. Cancer Res. 44, 3159.
2. Le Beau M. M. & Rowley J. D. (1986) Chromosomal abnormalities in leukemia and lymphoma: clinical and biological significance. In Advances in Human Genetics (Harris H. & Hirchhord K., Eds), p. 1. Plenum Press, New York and London.
3. Fourth International Workshop on Chromosomes in Leukemias (1984) A prospective study of acute nonlymphocytic leukemia, Chicago, Illinois, U.S.A., September 2-7, 1982. Cancer Genet. Cytogenet. 11, 251.
4. Mitelman F., Brandt L. & Nilsson P. G. (1978) Relation among occupational exposure to potential mutagenic/carcinogenic agents, clinical findings, and bone marrow chromosomes in acute non-lymphocytic leukemia. Blood 52, 1229.
5. Golomb H. M., Alimena G., Rowley J. D., Vardiman J. W., Testa J. R. & Sovik C. (1982) Correlation of occupation and karyotype in adults with acute nonlymphocytic leukemia. Blood 60, 404.
6. Lawler S. D., Summersgill B. M., Clink H. McD. & McElwain T. Y. (1979) Chromosomes, leukemia, and occupational exposure to leukemogenic agents. Lancet 2, 853.
7. Bennett J. M., Catovsky D., Daniel M-T., Flandrin G., Galton D. A. G., Gralnick H. R. & Sultan C. (1976) The French-American-British (FAB) Coop- erative Group: proposals for the classification of the acute leukemias. Br. J. Haemat. 33, 451.
8. Bennet J. M., Catovsky D., Daniel M-T., Flandrin G., Galton D. A. G., Gralnick H. R. & Sultan C. (1985) Proposed revised criteria for the classification of acute myeloid leukemia: a report of the French-American- British Cooperative Group. Ann. Intern. Med. 103, 620.
9. Li Y. S. & Hayhoe F. G. J. (1982) Cytogenetic study in acute myeloid leukemia using peripheral blood samples sent by post. J. clin. Path. 35, 861.
10. Li Y. S. (1985) Correlation of karyotype with patient sex and age in acute myeloid leukemia. Cancer Genet. Cytogenet. 14, 73.
11. Lin S-P., Huang Z-Z., Liu M-H. & Ou Y-H. (1987) Cytochemistry in 312 cases of acute leukemia. Chinese J. Hemat. 8, 33. (In Chinese.)
12. Yang A-Y. & Zhao R. (1987) Phagocytosis in malig- nant hematological disorders. Chinese J. Hemat. 8, 32. (In Chinese.)
13. Yang R-F., Chen Z-S., Wong S-R., Lu Q-Y. & Peng H- H. (1986) Acute monocytic leukemia developed after plasmacytomas. Chinese J. Hemat. 7, 603. (In Chinese.)
14. Li Z-C., Huang Y-W. & Yu S-L. (1986) Acute lympho- cytic leukemia after radiotherapy for nasopharyngeal carcinoma. Chinese J. Hemat. 7, 668. (In Chinese.)
15. Han D-Y. (1980) Immunosuppressive therapy and acute myeloid leukemia. Chinese J. Hemat. 1, 153 (In Chinese.)
16. Xu S-R. & Wu Z-Q. (1986) Cytotoxic drugs and acute leukemia. Chinese J. Med. 25, 490. (In Chinese.)
376 You-SHENG LI et al.
17. Huang W-X., Li H-Z. & Chang A. (1985) Acute promyelocytic leukemia after ICRF154 therapy for psoriasis. Chinese J. Derm. 18, 39. (In Chinese.)
18. Zhou Y-H. (1986) Acute promyelocytic leukemia after treatment with bimolane for psoriasis. Chinese J. Derm. 19, 56. (In Chinese.)
19. Liu J-L. (1987) Acute leukemia developed after treat- ment with bimolane. Chinese J. Hemat. 8, 60. (In Chinese.)
20. Li C-L. & Gao L-S. (1987) Bimolane-therapy-related leukemia. Chinese J. Hemat. 8, 57. (In Chinese.)
21. Shao J-Z. & Zhang G-R. (1987) Leukemia developed after treatment with bimolane for psoriasis. Chinese J. Hemat. 8, 30. (In Chinese.)
22. Huang Z-Z., Hua Z. & Xiong S-M. (1987) Leukemia after immunosuppressive therapy for psoriasis. Chinese J. Hemat. 8, 29. (In Chinese.)
23. Qian L-S., Yang B-Q. & Xue Y-P. (1987) Acute nonlymphocytic leukemia after treatment for psoriasis. Chinese J. Hemat. 8, 27. (In Chinese.)
24. Creighton A. M., Hellmann K. & Whitecross S. (1969) Antitumor activity in a series of bisdiketopiperazines. Nature, Lond. 222, 384.
25. Ren Y-F., Shu H-L., Zhang T-M., Chen Z-Y. & Lin C. (1980) Studies on a new antitumor drug bimolane (AT-1727). Sci. Bull. 25, 189. (In Chinese.)
26. Rosner F. & Griinward H. W. (1980) Cytotoxic drugs and leukemogenesis. Clinics Haemat. 9, 663.
27. Yunis J. J. & Soreng A. L. (1984) Constitutive fragile sites and cancer. Science, N.Y. 226, 1199.
28. Chou J. L. & Pan S. P. (1985) Epidemiology of leu- kemias in the People's Republic of China. Leukemia Res. 9, 777.
29. Li Y. S. & Yang C-L. (1987) Consistent chromosomal changes in Chinese patients with acute nonlymphocytic leukemia. Cancer Genet. Cytogenet. 26, 379.
30. Le Beau M. M., Albain K. S., Larson R. A., Vardiman J. W., Davis E. M., Blough R. R., Golomb H. M. &
Rowley J. D. (1986) Clinical and cytogenetic cor- relations in 63 patients with therapy-related myelo- dysplastic syndromes and acute nonlymphocytic leukemia: further evidence for characteristic abnor- malities of chromosomes Nos 5 and 7. J. clin. Onc. 4, 325.
31. Whang-Peng J., Young R. C., Lee E. C., Longo D. L., Schechter G. P. & DeVita V. T. (1988) Cytogenetic studies in patients with secondary leukemia/dysmyelo- poietic syndrome after different treatment modalities. Blood 71, 403.
32. Reeves J. D. (1982) Household insecticide-associated blood dyscrasias in children. Am. J. Ped. Hemat. Oncol. 4, 438.
33. Levine E. G. & Bloomfield C. D. (1986) Secondary myelodysplastic syndromes and leukaemias. Clin. Haemat. 15, 1037.
34. Prigogina E. L., Fleischman E. W., Puchkova G. P., Mayakova S. A., Volkova M. A., Protasova A. K. & Frenkel M. A. (1986) Chromosomes in acute nonly'mphocytic leukemia. Hum. Genet. 73, 137.
35. Gilbert R. D., Kavabus C. D. & Mills A. E. (1987) Acute promyelocytic leukemia: a childhood cluster. Cancer 59, 933.
36. Fialkow P. J., Martin P. J., Najfield V., Penfold G. K., Jacobson R. J. & Hansen J. A. (1981) Evidence for multi-step pathogenesis of chronic myelogenous leukemia. Blood 58, 158.
37. Louwagie A. L., Meccuci C., Criel A., Hoof A. H. & Berghe H. van den. (1987) Variant translocation t(15q;17q) accompanying a promyelocytic accelerated phase of Ph'-positive chronic myeloid leukemia. Can- cer Genet. Cytogenet. 28, 349.
38. Archimaud E., Charrin C., Guyotat D., Magaud J- P. & Gentilhomme O. (1988) Acute leukaemia with t(4;ll) in patients previously exposed to carcinogens. Br. J. Haemat. 69, 467.