Embed Size (px)
Citation preview

© 2016 by the American Pharmacists Association. All rights reserved.
2
Specialty medications: Implications for pharmacy
practice, patients and research
Patrick Gleason, PharmD, FCCP, BCPS Director, Health Outcomes, Prime Therapeutics
Adjunct Professor, University of Minnesota, College of Pharmacy
3
Disclosures• Patrick Gleason declares he is employed by a pharmacy
benefit manager, Prime Therapeutics.
• He has no other conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
4
• Target Audience: Pharmacists
• ACPE#: 0202-0000-16-074-L01-P
• Activity Type: Knowledge-based
5
Learning Objectives
• State a working definition of the term “specialty drug.”
• Describe at least five factors that influence whether a drug product is considered a “specialty drug.”
• Explain differences in the coverage of specialty drugs in the pharmacy benefit versus the medical benefit of an insured or prepaid health program.
• List new channels of distribution emerging for specialty drugs.
• Identify the relative role of traditional drugs and specialty drugs in total spending by U.S. health insurance plans.
6
Prime Therapeutics• 13 Blue Plan owners
• 19 Blue Plan clients
• 25.6 million members
• $22.5 billion drug spend managed
• 337 million annual claim volume (weighted)
• 67,000+retail pharmacies in network
• 7.2 million Prescriptions shipped via PrimeMail®
• $4.4 billion revenue in 2014
• 3,900 employees

© 2016 by the American Pharmacists Association. All rights reserved.
7
Drugs now comprise more than 25 percent of all employer health insurance expenditures.
• True
• False
8
Specialty drugs are currently over 40 percent of all employer drug expenditures.
• True
• False
9
The specialty drug member cost share where there begins to be a statistically significant increase in new start abandonment was:
A.$50
B.$100
C.$150
D.$250
E.$500
10
The most common specialty benefit cost share is:
A. $50
B. $100
C.20 percent coinsurance
D.50 percent coinsurance
E. Co-insurance with minimum and maximum
11
The leading employer specialty management strategy is:
A. Narrow specialty network
B. Medical benefit drug coverage changes to influence site of care
C.Formulary exclusion with limited brand coverage across therapeutic categories
D.Utilization management (e.g., prior authorization, step-therapy, quantity limits)
12
Prescription drugs’ sizable share of health spending
• 19 percent of employer health care expenditures is retail (Rx benefit) drugs
• 23 percent of employer health care expenditures is hospital care
• Combined Rx benefit + medical benefit drug > 25 percent of total health care expenditures
Sourced: Prescription Drugs’ Sizable Share of Health Spending. by Drew Altman December 13, 2105. http://blogs.wsj.com/washwire/2015/12/13/prescription-drugs-sizable-share-of-health-spending/tab/print/

© 2016 by the American Pharmacists Association. All rights reserved.
13
Prime Therapeutics: Commercial book of business
Over 15 million members during 2014
Pharmacy benefit• $24.78 per member per month (PMPM) specialty drug expenditures• 31 percent of all drug expenditures was specialty drug expense
Medical benefit• $18.06 PMPM spent on drugs
Medical + pharmacy benefit specialty drugs• 43 percent of all drug expenditures in 2014
Source: Prime Therapeutics LLC, 2014 internal data
14
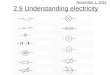
Distribution of spending across medical and pharmacy benefits varies by drug class
$300 $600 $900 $1,200 $1,500
AUTOIMMUNEINJECTABLE CANCER
MULTIPLE SCLEROSISHEPATITIS C
ORAL CANCERHIV & IMMUNOSUPPRESSANTS
BLOOD MODIFIERSIMMUNE GLOBULINS
HEMOPHILIAENZYME DEFICIENCIES
NAUSEA & VOMITINGGROWTH HORMONES
ANTICOAGULANTSCYSTIC FIBROSIS
LUNG DISORDERSINFERTILITY
PULMONARY HYPERTENSIONVISCO SUPPLEMENTS
MillionsSpecialty drug spend by category and benefit coverage
TOTAL MEDICAL TOTAL PHARMACY
Source: Prime Therapeutics LLC, 2014 internal data
15
The importance of a comprehensive picture: 15 million commercially insured members
Top Pharmacy benefitspecialty drugs*
Class% of Rx
specialty spend
Humira Autoimmune 13.1
Sovaldi Hepatitis C 9.2
Enbrel MS 8.0
Copaxone MS 4.3
Rebif/Avonex(interferon beta-1a)
MS 4.0
Tecfidera MS 3.2
Atripla HIV 2.9
SomatropinGrowth hormone
2.9
Gleevec Cancer 2.1
Olysio Hepatitis C 1.9
Top Medical benefitspecialty drugs*
Class% of Medical
specialty spend
Remicade Autoimmune 11.4
Neulasta Blood modifier 8.9
Avastin Cancer 7.0
Herceptin Cancer 5.9
RituxanAutoimmune/ cancer
5.5
Tysarbri MS 2.9
EpoetinEnd stage renal disease
2.6
Alimata Cancer 2.1
Gammunex-C /Gammagard
Immune globulin 2.1
Doxetaxel Cancer 2.0
Source: Prime Therapeutics LLC, 2014 internal data* All brand names are the property of their respective owner
16
Specialty drugs: Inflationary and utilization (2012-2014)
• 15 million commercially insured members
• Average age 35 years
• 50 percent women
Source: Prime Therapeutics LLC, 2012 – 2014 internal data
5 per 1,000
$4,700
17
Tools to manage specialty spend
Patient cost share & formulary (drug list) management
Utilization management
Contracting management
Care /casemanagement
Channel management
• Prior authorization
• Step therapy
• Quantity limit maximums per prescription fill
• Rebates
• Fee schedules
• Patient counseling to ensure safe & effective drug use
• Patient services to ensure use of preferred care network and specialist
• Coordination of care
• Specialty pharmacy network
• Drug purchasing discounts
• Optimize site of care
• Patient financial assistance (coupons) for preferred formulary tier drugs
Source: Health Affairs 2014;33(10):1761-1769
18
Pharmacy Benefit Management Institute: 2015 Specialty Drug Benefit Report Employer Survey
Source: PBMI https://www.pbmi.com/shop/reports/2015-specialty-drug-benefit-report/

© 2016 by the American Pharmacists Association. All rights reserved.
19
Multiple sclerosis (MS) specialty drug costs
• ~13 percent increase in MS drug cost year over year
• If 20 percent coinsurance, $960 monthly member contribution
– Yearly member contribution $11,520
Source: Prime commercial book of business, 2011-2014
$4,800
20
Prime health insurance marketplace: Enrollment and deductibles
Source: Prime HIM data, 2015-2016
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$8,000
2015 Bronze 2016 2015 Silver 2016 2015 Gold 2016 2015 Platinum 2016
Range $1,000 $850 $500 $1,500 $400 $1,250 0 0
Low $5,000 $6,000 $1,500 $1,500 $1,000 $500 $1,000 $200
Individual deductible by metallic level2015 and 2016
$6,000
$6,850
$2,000
$3,000
$1,400$1,750
$1,000
$200
21
2015 – 20th annual Towers Watson/National Business Group on Health Best Practices in Health Care Employer Survey
Source: 2015 Towers Watson/National Business Group on Health (NBGH) Best Practices in Health Care Survey, Dec. 15, 2015
22
Hepatitis C drugs utilization management impact
• In the first half of 2015, plans using Metavir score-based prior authorization had:
• 36 percent lower utilization
• 200 fewer new starts
• Cost neutrality of treating hepatitis C in people with Metavir score < 2 has not been demonstrated.1,2
Source: charts – Prime Therapeutics LLC, internal data 2013 - 2015
1. Ann Intern Med. 2015;162(6):397-406.
2. JAMA Internal Med. 2015 Nov 23:1-9. doi: 10.1001/jamainternmed.2015.6011. [Epub ahead of print]
23
Specialty pharmacy
Source: Health Affairs 2014;33(10):1761-1769
24
Tools to manage specialty spend
Patient cost share & formulary (drug list) management
Utilization management
Contracting management
Care /casemanagement
Channel management
• Prior authorization
• Step therapy
• Quantity limit maximums per prescription fill
• Rebates
• Fee schedules
• Patient counseling to ensure safe & effective drug use
• Patient services to ensure use of preferred care network and specialist
• Coordination of care
• Specialty pharmacy network
• Drug purchasing discounts
• Optimize site of care
• Patient financial assistance (coupons) for preferred formulary tier drugs
Source: Health Affairs 2014;33(10):1761-1769

© 2016 by the American Pharmacists Association. All rights reserved.
25
Pharmaceutical companies coupons
Program provides up to $8,000 of assistance per patient for each 12-month period to cover out of pocket costs for ENBREL®,
including copayments, coinsurance and prescription deductible. -See more at: https://www.enbrel.com/support/financial-
assistance/#sthash.VuCMhqkL.dpuf
Source: Health Affairs 2014;33(10):1761-1769
26
Specialty drug coupons patient pay impact at Prime Therapeutics Specialty PharmacyTM
117,330 prescriptions with a coupon
57%
3%
Patient cost share greater than $50
12%
1%
Patient cost share greater than $250
Patient pay beforecopay coupon
After coupon
Source: Health Affairs 2014;33(10):1761-1769
27
Cost share (patient pay) impact on primary non-adherence
Unadjusted abandonment rates of specialty drugs by 15,937 patients newly initiating or restarting use
Source: Health Affairs 2014;33(10):1761-1769; authors Catherine I. Starner, G. Caleb Alexander, Kevin Bowen, Yang Qiu, Peter J. Wickersham and Patrick P. Gleason6
28
Prime Therapeutics Specialty Pharmacy prescriptions dispensed by condition/drug class
Core Category Claims Patients Patient Paid Plan Paid Total Paid
Biologic Anti-Inflammatory 184,347 27,457 $28,692,572 $554,197,794 $582,890,366
Multiple Sclerosis 99,842 12,174 $19,350,996 $464,245,066 $483,596,062
Hepatitis C 16,059 2,607 $3,873,329 $224,852,337 $228,725,666
Cancer – Oral drugs 24,575 4,368 $3,195,650 $154,771,380 $157,967,030
Growth Hormones 20,389 2,803 $3,257,027 $71,486,463 $74,743,490
Cystic Fibrosis 5,399 877 $577,770 $25,774,986 $26,352,757
Infertility 18,334 3,867 $1,814,340 $31,108,127 $32,922,467
Hemophilia 1,423 216 $188,499 $35,711,939 $35,900,438
Others* 26,498 6,756 $2,913,468 $69,544,976 $72,458,444
Overall 396,866 59,170 $63,863,651 $1,631,693,068 $1,695,556,719
*Others include primarily pulmonary hypertension, lung disorders, immune globulins, enzyme deficiencies, human immunodeficiency virus, cancer-injectable, and anticoagulants.
† Members column does not sum due to some members using drugs in multiple core categories.
• $1.695 billion in specialty drug claims
• 63 percent of all specialty drug costs are in the first two rows
Specialty pharmacy claims by core category during 2014 among 15 million commercially insured members
Source: Prime Therapeutics LLC, 2014 internal data
29
• Saved members more than $41.7 million in 2014
• 35,230 members (60 percent) received a copay offset
• $1,185 average savings per member who received any copay offset
Specialty pharmacy claims by core category during 2014 among 15 million commercially insured members
Copay coupons/Patient assistance programs (PAP)
Core CategoryCoupon/PAP
Claims Coupon/PAP Members Coupon/PAP Amount% of Member Cost Share Offset by Coupons/PAP
Biologic Anti-Inflammatory 120,466 21,856 $23,029,214 80.3
Multiple Sclerosis 53,706 8,714 $12,669,452 65.5
Hepatitis C 6,290 1,547 $2,937,912 75.8
Cancer – Oral drugs 2,185 614 $1,245,836 39.0
Growth Hormones 5,139 1,024 $687,064 21.1
Cystic Fibrosis 1,252 315 $252,862 43.8
Infertility 149 77 $25,187 1.4
Hemophilia 86 18 $21,440 11.4
Others* 5,016 1,138 $880,328 30.2/Ranges 1.4-71.0
Overall 194,289 35,230 $41,749,295 65.4/Ranges 1.4-80.3
*Others include primarily pulmonary hypertension, lung disorders, immune globulins, enzyme deficiencies, human immunodeficiency virus, cancer-injectable, and anticoagulants.† Members column does not sum due to some members using drugs in multiple core categories.
Source: Prime Therapeutics LLC, 2014 internal data
30
Prime Therapeutics research implications
• As patient cost shares go beyond $250 per month, more patients abandon their initial multiple sclerosis or biologic anti-inflammatory prescription
• A patient’s cost share for preferred tier specialty drugs on the formulary (drug list) should be $250 or less per month
• When coupons were applied, they reduced patient cost share to less than $250 and saved patients $6 of every $10 they are asked to pay out of pocket
• Unless used on preferred specialty drugs, coupons undermine insurer’s ability to manage costs, risking increases to premiums
• Laws banning specialty drug tiers and/or capping cost shares will likely increase costs and result in more limit drug access due to expanded formulary exclusion lists

© 2016 by the American Pharmacists Association. All rights reserved.
31
Network
Formulary/Rebates Utilization
Mgmt
Benefitdesign
Care Management
Coupons/PAPs
Research needs
Clinical outcomesPractice implications
32
Key Points• Specialty drug expenses will soon be half of all drug expenditures,
with substantial expense through the medical benefit
• Insurers are implementing more limited formularies, utilization management and cost sharing to address rising specialty expenditures
• Pharmaceutical manufacturer coupons are frequently used to eliminate member cost sharing, negating the formulary cost share tiering
• More research is needed to understand the pharmacy benefit management tools impact on practice, clinical outcomes and costs
33
Drugs now comprise more than 25 percent of all employer health insurance expenditures.
• True
• False
34
Specialty drugs are currently over 40 percent of all employer drug expenditures.
• True
• False
35
The specialty drug member cost share where there begins to be a statistically significant increase in new start abandonment was:
A.$50
B.$100
C.$150
D.$250
E.$500
36
The most common specialty benefit cost share is:
A. $50
B. $100
C.20 percent coinsurance
D.50 percent coinsurance
E. Co-insurance with minimum and maximum

© 2016 by the American Pharmacists Association. All rights reserved.
37
The leading employer specialty management strategy is:
A. Narrow specialty network
B. Medical benefit drug coverage changes to influence site of care
C.Formulary exclusion with limited brand coverage across therapeutic categories
D.Utilization management (e.g., prior authorization, step-therapy, quantity limits)
38
Specialty Drugs:How Did That Iceberg Get Here?
New Channels & Framework for Drugs
Stephen W. Schondelmeyer, PharmD, PhD, FAPhA
CMC Endowed Chair in Pharmaceutical Management & Economics
Professor & Director, PRIME Institute
College of Pharmacy, University of Minnesota
39
DisclosuresStephen W. Schondelmeyer declares that: • He is employed by the University of Minnesota and conducts drug
benefit management for the University’s health benefit program (UPlan).
• He has grants from the Minnesota Department of Health and the AARP Public Policy Institute.
• He serves on the Editorial Advisory Board of Drug Topics and First Report Managed Care.
• He has no other grants, employment, gifts, stock holdings, and honoraria.
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
40
Learning Objectives
• State a working definition of the term “specialty drug.”
• Describe at least five factors that influence whether a drug product is considered a “specialty drug.”
• Explain differences in the coverage of specialty drugs in the pharmacy benefit versus the medical benefit of an insured or prepaid health program.
• List new channels of distribution emerging for specialty drugs.
• Identify the relative role of traditional drugs and specialty drugs in total spending by U.S. health insurance plans.
41
DisclosuresStephen W. Schondelmeyer declares that: • He is employed by the University of Minnesota and conducts drug
benefit management for the University’s health benefit program (UPlan).
• He has grants from the Minnesota Department of Health and the AARP Public Policy Institute.
• He serves on the Editorial Advisory Board of Drug Topics and First Report Managed Care.
• He has no other grants, employment, gifts, stock holdings, and honoraria.
The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
42
Which of the following is NOT a common factor used to define specialty drugs?
A. Complex, chronic conditions
B. Administration by injection or inhalation
C. High cost drug
D. Oral route of administration

© 2016 by the American Pharmacists Association. All rights reserved.
43
What percent of total healthcare spending by commercial insurers in the U.S. in 2016 is expected to be spent on drug therapy?
A. 7% to 8%
B. 9% to 10%
C. 12% to 15%
D. 29% to 34%
44
Which of the following channels of distribution is showing the least growth due to specialty drugs?
A. Hospital Outpatient
B. Mail Order Pharmacies
C. Limited Distribution Pharmacies
D. Physician’s Offices
45
Which of the following is NOT true regarding drug expenditures for a commercially insured population in 2016?A. Drug spending is a small part of health expenditures at
about 10%.
B. Drug spending exceeds spending on physicians.
C. Drug spending exceeds total hospital inpatient
spending.
D. Specialty drug spending in all settings accounts for
about 40% of total drug spending.
46
Specialty Drugs: Overview• Defining a “Specialty Drug”
• Channels of Distribution for Specialty Drugs
• Coverage of Specialty Drugs
• Monitoring Specialty Drug Spend & Trend
• Impact of Specialty Drug Patterns on Pharmacy Practice
• Impact of Specialty Drug Patterns on Research
47
Factors Considered in Defining a Specialty Drug
• Special or complex handling & distribution requirements, or
• Route of administration such as injection, infusion, inhalation, implantation, or instillation (“the 5 I’s”), or
• Patient management, monitoring or disease support system before, or after, drug administration, or
• Special patient training & education needed for safe & effective use or for self-administration, or
• FDA approval by a BLA versus an NDA, or
• FDA designation as an Orphan Indication for the drug, or
• FDA approved Risk Evaluation & Mitigation (REMS) program, or
• Chronic or high risk disease or certain therapeutic categories, or
• Drugs with Limited Distribution (voluntary or required), and
48
Does High Cost Define Specialty Drugs?
• High cost is the most common element listed.(1)
• High cost is “always noted but not always included in the formal definition.”(2)
• Level for “high cost” varies – Ranges from costs that exceed $500 to $2,500 per month(3).
• High cost alone is not sufficient to define a specialty drugsince this factor alone would place many high cost, traditional brand name drugs on the specialty list.(1)
– For example, Abilify 10 mg tabs #30 costs $910, or Cialis 10 mg tabs #12 costs $577
(2) AMCP, The AMCP Format for Formulary Submission, Version 3.1, Dec. 12, 2012, Specialty Pharmaceuticals Addendum, pp. 34-39.(1) Blaser DA, Lewtas AJ, et al. How to define specialty pharmaceuticals – a systematic review. Am J Pharm Benefits. 2010;2(6):371-380.
(3) EMD Serono Specialty Digest, 8th Edition, Managed Care Strategies for Specialty Pharmaceuticals, 2012, p. 20.

© 2016 by the American Pharmacists Association. All rights reserved.
49
Impact of High Cost Limit forSpecialty Drugs
* Prescription claims & dollars from self-insured population for calendar year 2015, compiled by PRIME Institute, University of Minnesota.
$ 600: 3.9% of claims & 49.8% of spend
$1,000: 2.2% of claims & 41.8% of spend
$2,500: 1.3% of claims & 32.8% of spend
$5,000: 0.7% of claims & 20.8% of spend
50
A Working Definition for aSpecialty Drug
• A drug that “requires a difficult or unusual process of delivery to the patient (preparation, handling, storage, inventory, distribution, Risk Evaluation & Mitigation (REMS) program, data collection, or administration”(1) or
• “Patient management prior to, or following, administration (monitoring, disease or therapeutic support systems).”(1)
• High cost (always noted, but may vary by plan).
(1) AMCP, The AMCP Format for Formulary Submission, Version 3.1, Dec. 12, 2012, Specialty Pharmaceuticals Addendum, pp. 34-39.
51
Who Determines Specialty Drug Definition?
• Medicare Part D - $600 per claim (unchanged since 2006)
• Medicare Part A & B – Drugs given in physician’s office
• Medicaid - State determines list & cost limit
• Self-Insured Employer (or Union) – determines list & cost limit
• Managed Care Plan – determines list & cost limit
• PBM – determines list & cost limit
• Specialty Pharmacy – determines list & cost limit
52
Coverage of Specialty Drugs
• Manufacturer gets FDA Approval for drug
• Medicare & Medicaid have to cover the drug
• Private & Commercial have pressure to cover the drug– Civil lawsuit for inadequate treatment if not covered
• FDA approval without utilization management tools is like writing a Blank Check to the manufacturer.
• Covered under:– Medical benefit (Commercial Medical or Medicare Parts A & B)
– Pharmacy benefit (Commercial Pharmacy or Medicare Part D)
53
Specialty Drugs: CoveragePharmacy BenefitMedical Benefit
• Prescriptions• Transaction Record• Drugs Identified• Drug Cost• Drug volume• Hidden incentives• Timely Claims• Utilization mgmt• Case Management• Drug Use Data• Drug Cost
Not always writtenBundled in office visit claimsHCPCS (J Codes) usedDrug cost part of total visitDrug mfg & dose uncertainProvider discount unknownClaims processed (days-months)
Retrospective DUR (at best)
Poor info. access, not easyNot available, not included 20%-100% > Pharmacy benefit
Based on prescriptionsClaim for each prescriptionNDC # for each drugDrug cost is knownDrug mfg & dose knownPharmacy price knownClaims processed (real time)
Concurrent DUR, PAGood info., easily doneReadily availableCosts less than medical benefit
Coverage Issue
54
Specialty Drug Distribution Channels
• How and where specialty drugs are distributed is
a choice and is influenced by:– Drug Manufacturer
– FDA
– Wholesalers & Specialty Wholesalers
– Plan Sponsors (private & public)
– PBMs
– Specialty pharmacies & limited distribution pharmacies
• “Specialty pharmaceuticals may also be dispensed by retail, hospital, or infusion pharmacies, which may provide some (or all) of the services that specialty pharmacies provide.”(1)
(1) AMCP, The AMCP Format for Formulary Submission, Version 3.1, Dec. 12, 2012, Specialty Pharmaceuticals Addendum, p. 35.

© 2016 by the American Pharmacists Association. All rights reserved.
55
Specialty Drug Channels
• Growth in new drug $’s is in specialty drugs
• Growth in Pharmacy Benefit is in:– Specialty pharmacies (PBM-owned or stand alone)
– Limited distribution pharmacies (manufacturer chosen)
• Growth in Medical Benefit is in:– Physician’s offices & clinics (manufacturer & provider driven)
– Hospital outpatient (manufacturer & hospital driven)
– Home infusion providers (provider & patient driven)
56
Changing Channels of Distribution for Drugs
ChainPharmacy
Mass MerchantPharmacy
Food & DrugPharmacy
IndependentPharmacy
Mail OrderPharmacy
Health PlanPharmacy
Clinic &Drs’ Office
Long TermCare
PharmacyHospital
GovernmentFacilities &
Other
Chain Warehouse
RegionalWholesalers National Wholesalers
Drug Manufacturers & Marketers
Source: Prepared by PRIME Institute, University of Minnesota.
Bulk Sales
Bulk Sales
Manufacturer Direct Sales
Generics & aFew Old Brands
Specialty& Bio Therapies
SpecialtyPharmacy
Limited Distr.Pharmacy
$
+
+ +
Revenue Shifting fromLeft to Right
HospitalOutpatient+
57
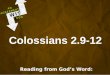
Drug Claims by Distribution Channel: 2014 (Traditional Pharmacy & Medical Channels)
Source: U of M UPlan Health Benefit, 2014 (with estimates for Medical Drug Expenditures).
% of Total Drug $
58.6% 41.4%Traditional Pharmacy Specialty Pharmacy & Medical
$ Annual Growth Rate~ -2% to +3%
$ Annual Growth Rate~ +10% to +25%
58
Physicianor Clinic
Specialty Drugs Distribution
Patient
SpecialtyWholesaler
Manufacturer
Physicianor Clinic
Buy & Bill
59
Physicianor Clinic
Specialty Drugs Distribution
Patient
Pharmacy
Wholesaler
Manufacturer
PharmacyNetwork
White Bag
Brown Bag
60
Physicianor Clinic
Specialty Drugs Distribution
Patient
PBM
Mail OrderPharmacy
Manufacturer
SpecialtyPharmacy
SpecialtyPharmacy

© 2016 by the American Pharmacists Association. All rights reserved.
61
Physicianor Clinic
Specialty Drugs Distribution
Patient
SpecialtyWholesaler
Manufacturer
PBM
Mail OrderPharmacy
SpecialtyPharmacy
Pharmacy
Wholesaler
Physicianor Clinic
PharmacyNetwork
SpecialtyPharmacy
62
New Specialty Drugs: 2009-2014(New Biotechnology Drugs, Vaccines, & Indications)
Source: IMS Health & Express Scripts
SpecialtyDrugs
96
TraditionalDrugs
49
New Molecular Entities 145
2/3 of New Approvals Were Specialty Drugs
63
What is the Spend & Trend of Pharmaceuticals &Specialty Drugs?
Are drugs a small part of the health care dollar?
64
Hospital Care,31.4%
PhysicianServices,
20.0%
Dental Services, 3.8%
Home Health Care 2.8%
Nursing Homes, 5.3%
Prescription Drugs, 9.6%
Durable Med Equip, 1.4%
Govt. Adm.,1.2%
Health Insur. Admin., 6.6%
Public Health, 2.6%
Capital Costs 5%
Research, 1.4%Other, 10.0%
The Nation’s Health Dollar: 2015Where Did It Go?
*
*
**
**
* *
*Other sectors thatinclude Rx drugs.
> 17.5% in 2016Rx Drugs in All Settings
Are Drugs Used in Other Sectors?
YES!
*
What Role Did Drugs Play?
*
65
Projected Healthcare Expenditures forCommercial Insured Population: 2016
Source: Milliman, Inc., Commercial Specialty Medication Research: 2016 Benchmark Projections, Dec. 1, 2015.Projections for 2016 using Truven’s MarketScan data for commercially insured population from 2012 & 2013.
$ PMPM
Non-Drug Service
Traditional Drugs
$421
$120
$541
20.5%
14.2%
Specialty Drugs
34.7%All Drugs
Specialty Drugs
Traditional Drugs * 29.0% w/o HospitalInpatient Drugs
66
Projected Healthcare Expenditures forCommercial Insured Population: 2016$ PMPM
Non-Drug Service
Drugs Only
$119
$138
$11
$111
$42
$120
Source: Milliman, Inc., Commercial Specialty Medication Research: 2016 Benchmark Projections, Dec. 1, 2015.Projections for 2016 using Truven’s MarketScan data for commercially insured population from 2012 & 2013.

© 2016 by the American Pharmacists Association. All rights reserved.
67
Projected Healthcare Expenditures forCommercial Insured Population: 2016$ PMPM
Non-Drug Service
Drugs Only
$119
$138
$11
$111
$42
$120
Specialty Drugs $188* Pharmacy Benefit Spending > Hospital Inpatient Spending* Pharmacy Benefit Spending = Hospital Inpatient Spending - Drugs
* Pharmacy Benefit Spending > Physician Office Spending
* All Drugs All Settings w/o Hospital Inpatient = 29.0% of Total Healthcare Spending* All Drugs All Settings w/Hospital Inpatient = 34.7% of Total Healthcare Spending
Source: Milliman, Inc., Commercial Specialty Medication Research: 2016 Benchmark Projections, Dec. 1, 2015.Projections for 2016 using Truven’s MarketScan data for commercially insured population from 2012 & 2013.
68
Where is the Spending Growth & Trend for Pharmaceuticals &
Specialty Drugs?
Are drugs growing slower than the U.S. economy?
69
Avg Cost per Drug Claim in Self-Insured Employer Plan (UPlan): 2004-2015 (Feb.)
$0$25$50$75
$100$125$150$175$200$225$250$275$300$325$350$375$400$425$450$475$500$525
Jan
-04
Ap
r-04
Jul-
04
Oct
-04
Jan
-05
Ap
r-05
Jul-
05
Oct
-05
Jan
-06
Ap
r-06
Jul-
06
Oct
-06
Jan
-07
Ap
r-07
Jul-
07
Oct
-07
Jan
-08
Ap
r-08
Jul-
08
Oct
-08
Jan
-09
Ap
r-09
Jul-
09
Oct
-09
Jan
-10
Ap
r-10
Jul-
10
Oct
-10
Jan
-11
Ap
r-11
Jul-
11
Oct
-11
Jan
-12
Ap
r-12
Jul-
12
Oct
-12
Jan
-13
Ap
r-13
Jul-
13
Oct
-13
Jan
-14
Ap
r-14
Jul-
14
Oct
-14
Jan
-15
$ / Claim
Average Drug Claim
Patented Brand(SS-Rx)
Generic (Gen-Rx)
$474
$ 41
$135
Brand Prices Increased > 13% in 2014
OTCs as Rx $ 39
Source: Based on data from Univ. of Minnesota self-insured drug benefit (UPlan) 2004 to 2015 & compiled by PRIME Institute, University of Minnesota.
70
Avg Cost per Drug Claim in Self-Insured Employer Plan (UPlan): 2004-2015 (Feb.)
$0
$500
$1,000
$1,500
$2,000
$2,500
$3,000
$3,500
$4,000
$4,500
$5,000
Jan-
04A
pr-
04Ju
l-04
Oct
-04
Jan-
05A
pr-
05Ju
l-05
Oct
-05
Jan-
06A
pr-
06Ju
l-06
Oct
-06
Jan-
07A
pr-
07Ju
l-07
Oct
-07
Jan-
08A
pr-
08Ju
l-08
Oct
-08
Jan-
09A
pr-
09Ju
l-09
Oct
-09
Jan-
10A
pr-
10Ju
l-10
Oct
-10
Jan-
11A
pr-
11Ju
l-11
Oct
-11
Jan-
12A
pr-
12Ju
l-12
Oct
-12
Jan-
13A
pr-
13Ju
l-13
Oct
-13
Jan-
14A
pr-
14Ju
l-14
Oct
-14
Jan-
15
Source: Based on data from Univ. of Minnesota self-insured drug benefit (UPlan) 2004 to 2015 & compiled by PRIME Institute, University of Minnesota.
$ / Claim
Generic
Patented Brand
$4,055
$4,791
$ 41
$474
[$4,055/Month or $48,660/Year]Specialty Drug Claims
Brand to Generic 11 : 1
Specialty to Brand 10 : 1
Specialty to Generic 100 : 1
71
What is the cost of specialty drugs?
Specialty Drugs & Costs
• Oncology
• Hepatitis C
• Growth Hormone
• Transplant Drugs
• Arthritis Drugs
• Hemophiliac Drugs
• Antiretrovirals (HIV)
• Multiple Sclerosis
• Coagulation Drugs
• Gaucher’s Disease
• Anemia Drugs
• Other Specialty
Xeloda, Afinitor, Gleevec, Tasigna, Nexavar $40,000 to $130,000
Sovaldi, Olysio, Harvoni, Infergen $84,000 to $150,000
Norditropin,somatropin (generic),Omnitrope $10,000 to $120,000
Cellcept, Rapamune, Prograf, Myfortic $ 1,000 to $25,000
Enbrel, Humira, Remicade, Kineret $25,000 to $85,000
Kogenate FS, Benefix, Recombinate $100,000 to $250,000
Truvada, Atripla, Reyataz, Emtriva $ 6,000 to $30,000
Avonex, Copaxone, Rebif, Tysarbi $30,000 to $75,000
Lovenox, Arixtra, Innohep, Fragmin $15,000 to $60,000Ceredase, Cerezyme $80,000 to $150,000Procrit, Neupogen, Epogen, Neulasta, Aranesp $15,000 to $100,000Soliris $40,000 to $500,000
Annual Cost of Therapy
2013 Median Annual Household Income in U.S. ~ $ 53,657 72
U.S. Annual Income: 2014
U.S. Bureau of the Census, 2015; AARP Report, 2015
$ / YearIncome per Family / Household
Specialty $53,364
Brand $ 2,960
Generic $ 283
Income per Person
Are Specialty Drugs Affordable---Even at the Societal Level?

© 2016 by the American Pharmacists Association. All rights reserved.
73
Specialty Drugs: Utilization
Annual Plan Cost
$2.08 million
Cost of Drug Therapy
$52,000Per Person
40 with MSWill Seek
Treatment (67%)
60 personsWith
Multiple Sclerosis(0.18%)
Covered Population
of
40,093
Multiple Sclerosis & Plan Cost: 2013
Annual Plan Cost of
Drug Therapy$51.88 PMPY
5.4% ofTotal PMPY
74
Specialty Drugs: Utilization
Annual Plan Cost
$1.53 million
Cost of Drug Therapy
$102,000Per Person
15 with Hep CWill Seek
Treatment (1.5%)
1,000 personsWith
Hepatitis C(2.5%)
Covered Population
of
40,093
Hepatitis C (Sovaldi & Olysio) & Plan Cost: 2013
Annual Plan Cost of
Drug Therapy $38.16 PMPY
4.0% ofTotal PMPY
75
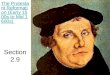
Humulin U-500: Average $/Monthfor Commercial Insurance: 2005-2013
$187
$247
$431
$864
$0
$100
$200
$300
$400
$500
$600
$700
$800
$900
$1,000
Jan
-06
Ap
r-06
Jul-
06
Oct
-06
Jan
-07
Ap
r-07
Jul-
07
Oct
-07
Jan
-08
Ap
r-08
Jul-
08
Oct
-08
Jan
-09
Ap
r-09
Jul-
09
Oct
-09
Jan
-10
Ap
r-10
Jul-
10
Oct
-10
Jan
-11
Ap
r-11
Jul-
11
Oct
-11
Jan
-12
Ap
r-12
Jul-
12
Oct
-12
Jan
-13
Ap
r-13
Jul-
13
Oct
-13
Jan
-14
Based on data from self-insured drug benefit 2004 to 2013 & compiled by PRIME Institute, University of Minnesota.
$ / Month
$ 5,172/Year
* 461% Increase In 8 Years
$ 2,248/Year
$ 10,375/Year
$ 2,954/Year
13% IncreaseIn 4 Years: 2006 to 2010
75% IncreaseIn 2 Years: 2010 to 2012
200% IncreaseIn 2 Years: 2012 to 2014
76
When insulin has a200% increase in price
does the patient’s
NO ! ! !Are We Getting Our Money’s Worth
When Drug Prices Go Up 200%?
diabetes get 200% better?
When a Drug Price Goes Up 200%?What Happens to the Cost-Effectiveness?
77
What Does the Future Hold?
78
What Is the Impact of Specialty Drugs Trends for Pharmacy Practice?
• Drug spend is shifting to non-retail channels!
• The money is in care management not drug distribution.
• Pharmacists must become familiar with how to assess affordability of drug therapy.
• Pharmacists will be needed in unique practice settings.
• Pharmacists will be needed to manage biosimilars.
• Pharmacists have a role in pharmocogenomics.
• Pharmacists need to know the “value” of drugs.

© 2016 by the American Pharmacists Association. All rights reserved.
79
What Is the Impact of Specialty Drug Trends for Research?
• Pharmacists need to know the “value” of drugs.
• Price changes must be taken into account in applying economic analyses.
• Cost and price changes need to be taken into account in prescribing & formulary decisions.
• Need to understand and study the issue of affordability of drug therapy.
• Need to re-evaluate the threshold level for QALYs.
• Need to develop means to express price feedback without blocking access to needed drug therapy.
80
Need for More R & DWe need more R & D ?
R
DIncreased R & D Will Result in
Improved Health Value
&
81
Traditional Prescriptions(>85% of Rxs Are Generic)
Specialty Prescription Drugs Are About
1% of Rxs &>50% of Rx $
How Did That Iceberg Get Here?
Specialty Prescriptions in Health Benefit ProgramsAccount for 30% to 50% of
Total Drug Spend
2/3 of New Drug Approvals Are for Specialty
Drugs
Specialty Drug Spending is Growing10% to 25% per Year.
82
Which of the following is NOT a common factor used to define specialty drugs?
A. Complex, chronic conditions
B. Administration by injection or inhalation
C. High cost drug
D. Oral route of administration
83
What percent of total healthcare spending by commercial insurers in the U.S. in 2016 is expected to be spent on drug therapy?
A. 7% to 8%
B. 9% to 10%
C. 12% to 15%
D. 29% to 34%
84
Which of the following channels of distribution is showing the least growth due to specialty drugs?
A. Hospital Outpatient
B. Mail Order Pharmacies
C. Limited Distribution Pharmacies
D. Physician’s Offices

© 2016 by the American Pharmacists Association. All rights reserved.
85
Which of the following is NOT true regarding drug expenditures for a commercially insured population in 2016?A. Drug spending is a small part of health expenditures at
about 10%.
B. Drug spending exceeds spending on physicians.
C. Drug spending exceeds total hospital inpatient
spending.
D. Specialty drug spending in all settings accounts for
about 40% of total drug spending.