Embed Size (px)
Citation preview

SPECIAL TOPIC
High- and Extra-High-Projection BreastImplants: Potential Consequences for Patients
John B. Tebbetts, M.D.Steven Teitelbaum, M.D.
Dallas, Texas; and Santa Monica,Calif.
Summary: All breast implants can potentially have deleterious effects on pa-tients’ tissues. Limiting negative tissue consequences and potential uncorrect-able deformities requires that surgeons be aware and educate patients regardingpotential consequences of various implant designs. High-profile implants havebeen available for decades, and during the current decade, extra-high-profileimplants have become available, but no valid peer-reviewed and publishedstudies have compared the potential tissue consequences of these designs tothose of other breast implant designs. Valid comparative studies are exceedinglydifficult to perform because of the number of variables that must be addressedto establish valid comparative cohorts. Nevertheless, the potential occurrence ofnegative tissue consequences from high- and extra-high-profile implants inprimary breast augmentation and breast augmentation reoperation cases is wellknown to experienced aesthetic breast surgeons. This article addresses potentialnegative effects on patients’ tissues of high- and extra-high-profile breast im-plants used for breast augmentation. This Special Topic article is not structuredor intended as a scientific article. It is written as a Special Topic and not anEditorial at the editor’s request. The cases presented are selected examples toillustrate potential clinical eventualities. The rate of occurrence of uncorrect-able tissue deformities relates directly to surgeon and patient awareness of thepotential consequences of implant selection decisions and requests. To mini-mize risks of negative tissue consequences for patients, surgeon awareness,patient education, and optimal implant selection decision processes areessential. (Plast. Reconstr. Surg. 126: 2150, 2010.)
All breast implants can potentially have del-eterious effects on patients’ tissues. The fre-quency and severity of these changes relate
directly to surgeons’ and patients’ willingness toprioritize preservation of tissues over arbitrary re-quests for breast projection or size.
Although many surgeons recognize that it isimportant for implant base width to not exceedthe base width of the patient’s parenchyma, tosatisfy a patient’s request for a specific size orvolume, those same surgeons may resort to ahigher projection implant with a narrower basewidth. High-profile and extra-high-profile im-plants have approximately one-third more vol-ume for a specific base width compared withmoderate-profile implants of the same basewidth. More volume and more projection causemore pressure on surrounding tissues, includ-
ing skin, subcutaneous tissue, breast paren-chyma, muscle, and bone.
In a recent article published elsewhere ana-lyzing 13 augmentation patients, the authors re-ported a small series of six primary and sevenrevision cases, and suggested that highly cohesive,extra-high-projection implants may be indicatedfor “large skin envelopes in breast augmentationpatients declining mastopexy, [and]...compli-cated implant exchanges....”1 Aside from the factthat no scientifically valid conclusions can be de-rived from a series this small, the conclusion of thisarticle and the popularity of extra-high-projectionimplants in some parts of the world for primarybreast augmentation should be a significant con-
From private practice.Received for publication September 22, 2009; revised April27, 2010.Copyright ©2010 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e3181f44564
Disclosure: No sources of funding are associatedwith the content of this article. Dr. Tebbetts has nofinancial interests that relate to the content of thisarticle. Dr. Teitelbaum is a consultant for Allerganand Lifecell.
www.PRSJournal.com2150

cern to patients and surgeons. Avoidance of per-manent or uncorrectable tissue deformities de-pends on the willingness of surgeons to prioritizescientifically valid and proven processes for assess-ing patients’ tissues above surgeon intuition, opin-ion, or any patient aesthetic requests.
These comments do not apply to the use oflarger or more highly projecting implants inbreast reconstruction, an environment in whichtissues have already been irreversibly compro-mised by disease. In primary breast augmentation,the tissue environment and the decision processesby patient and surgeon are very different com-pared with reconstruction. In reconstruction, tis-sues are, by definition, already compromised ordestroyed. In primary augmentation, a primaryobjective is to avoid tissue compromise, reopera-tion, and deformities resulting from a primary,medically unnecessary operation.
INDICATIONS FOR USE OF HIGH- ANDEXTRA-HIGH-PROJECTION IMPLANTS
Proposed indications for high- and extra-high-profile implants are based largely on sur-geon conjecture that these devices may be in-dicated for (1) “glandular ptotic” breasts, (2)“constricted lower pole” breasts, (3) “tuberousbreast” deformities, (4) avoiding mastopexies inpatient who do not want mastopexy scars, and(5) patients requesting more projection. Theseindications are based largely on subjective sur-geon speculation validated by no more than se-lected, often short-term, before-and-after pho-tographs. None is based on any publishedquantitative measurements or any scientificallyvalid long-term data confirming that high- andextra-high-profile implants are safe for tissues oraesthetically superior to less projecting im-plants.
This Special Topic article does not presentvalid, comparative, or quantitative scientific datato prove or disprove which implant devices may ormay not produce tissue compromises. To do sowould require (1) valid comparative cohorts thatcontrol for more than 50 variables, (2) possibleviolation of ethical and Helsinki guidelines byplacing different implant types and projectionson the two sides of a single patient, or (3) accessto detailed premarket approval data on eachspecific type of implant that manufacturersclaim is proprietary and have not released. Thisarticle presents issues and patient cases that ex-ist, and encourages further study with releaseand accumulation of scientifically valid data tofurther define patient safety issues.
CURRENT LITERATUREThe numbers of high- and extra-high-profile
implants in U.S. Food and Drug Administrationpremarket approval studies are too small for anyvalid conclusions about their safety and efficacy tobe drawn, and adverse outcomes are not catego-rized by device projection in any current premar-ket approval data. No other valid scientific series(of rigor and monitoring equal to U.S. Food andDrug Administration premarket approval data)documents the long-term safety and potential neg-ative or uncorrectable tissue consequences fromextra-high-projection implants in breast augmen-tation patients.
Handel2 succinctly described potential nega-tive tissue effects of breast implants when he wrote,“The long-term presence of implants typically re-sults in changes in breast anatomy and physiology,including parenchymal atrophy, tissue thinning,and diminished skin blood supply.” The potentialto limit these negative effects by specific tissue-based planning and implant selection processeshas been addressed in published studies that re-ported the lowest reported reoperation rates andthe absence of uncorrectable deformities with upto 7-year follow-up in series that limited implantsize to 350 cc and in which no high- or extra-high-projection implants were used.3–9 Outcomes datain these studies prove the safety and efficacy of low-and moderate-profile implants. Equivalent pub-lished data do not exist for high- and extra-high-profile implants.
SURGEON AND PATIENT OBJECTIVESAND DECISION PROCESSES
Satisfying patient requests and delivering vi-sually evident short-term results are important ob-jectives for aesthetic surgeons. Protecting patients’tissues requires that size and projection requestsare subordinate to a surgeon’s primary objectiveof protecting the patient’s tissues and preventinguncorrectable deformities or long-term tissuecompromises, especially when performing a med-ically unnecessary procedure. Fulfilling a patientrequest for volume or doing what may seem nec-essary to correct a specific condition (e.g., glan-dular ptosis or constricted lower pole breast)should be tempered by an acknowledgment thatthe very forces exerted by an implant to push thebreast envelope into a particular shape or dimen-sion are the same forces that can cause irrevers-ible, long-term tissue consequences and uncor-rectable tissue deformities. Patient (and surgeon)education are vitally important to optimize deci-
Volume 126, Number 6 • Extra-High-Projection Breast Implants
2151

sion processes and avoid a “cure” that is far worsethan the disease.
CHALLENGING QUESTIONS ANDCLINICAL OBSERVATIONS
Although surgeons’ opinions may promotethe use of these devices, no current scientificdata adequately define safe indications for use ofhigh- and extra-high-profile devices in breastaugmentation. Regardless of the size of pub-lished anecdotal series, absent quantified tissuemeasurements using clinical and imaging tech-niques and long-term follow-up comparable toU.S. Food and Drug Administration studies, thosestudies do not prove the safety of this type of devicefor primary breast augmentation.
Challenging questions remain unanswered byscience. How much of the additional projection ofa high-profile implant are lost to parenchymalatrophy or remodeling of the rib cage? When is theadditional level of correction or improvement inshape worth the potential negative long-term con-sequences to tissues? How do long-term resultscompare with short-term results? What scientificstudy designs can be structured and implementedto definitively define the effects of breast implantdesigns on patients’ tissues? What should deter-mine implant selection: long-term validated data,analysis of short-term photographs, or opinion notverified by data?
Surgeon opinion has established an unenvi-able track record of up to 25 percent reoperationrates in just 3 years after breast augmentation inU.S. Food and Drug Administration premarketapproval studies. Of much greater concern is thatsurgeon opinion and intuition, in the context ofpatient wishes, may risk uncorrectable tissue com-promises and deformities in breast augmentationpatients. Many of those uncorrectable problemsare caused by excessively large and excessively pro-jecting implants in augmentation, often with thejustification, “it’s what the patient wanted,” andwithout documentation that the patient was fullyeducated and understood the potential conse-quences of her requests on her tissues.
IMPLANT–SOFT-TISSUE DYNAMICS ANDTISSUE CONSEQUENCES
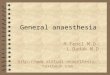
Figure 1 is an illustrated flowchart summariz-ing potential negative tissue consequences relatedto breast implant size and projection. Greater sizeand/or projection of breast implants have greaterpotential negative effects on patients’ tissues. Theweight and pressure of high- and extra-high-pro-jection implants potentially causes more stretch-
ing and thinning of the breast envelope (skinand subcutaneous tissue) and more parenchy-mal atrophy compared with smaller or less pro-jecting implants. Consequences to patients canbe disastrous and can produce uncorrectabledeformities and conditions that include paren-chymal thinning, skin stretch, inability to lac-tate, sensory compromise, implant edge or shellvisibility, visible traction rippling, and chest walldeformities. Regardless of what any patient re-quests, it is every physician’s first responsibilityto do no harm to the patient.
More than 50 variables must be analyzed incomparative augmentation cohorts to achieve sci-entific validity in comparative clinical studies ofvarious size and projection implants, making thesestudies virtually impossible to accomplish.3 Nev-ertheless, the management of many patients withhigh- and extra-high-profile implants has unequiv-ocally demonstrated specific patterns of tissuecompromises and uncorrectable deformities thatare not observed when implants have been se-lected by valid and published processes.3–9
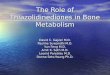
Capsular contracture provides surgeons anexcellent clinical model with which to observetissue effects of higher profile or projection im-plants, because a severe, spherical capsular con-tracture converts any low- or moderate-profileimplant to a high- or extra-high-profile shapeddevice. The tissue effects of capsular contrac-ture, especially more severe and longstandingcontractures, relate directly to the forces gener-ated by a dramatic increase in the projection (cre-ating more focal pressure) and decrease in basewidth (focusing the pressure on a smaller area)that affect adjacent and underlying tissues. Figure2 dramatically illustrates the disastrous conse-quences of a high-profile device with capsular con-tracture in an already thin patient. Surgeons can-not predictably control the wound-healingmechanisms that may produce capsular contrac-ture, but surgeons can certainly observe the tissueconsequences of more highly projecting implants,whether the implant was designed with additionalprojection or acquired the projection as the resultof capsular contracture. Those observations pro-vide insight and an opportunity to integrate theknowledge of potential tissue consequences intothe decision processes of implant selection forprimary augmentation.
Parenchymal atrophy and chest wall deformi-ties are most apparent when a high- or extra-high-profile implant is removed (Figs. 3 and 4). Thelarger or more projecting the implant, the tighterthe patient’s breast soft-tissue envelope; and the
Plastic and Reconstructive Surgery • December 2010
2152

Fig. 1. Illustrated flowchart summarizing potential negative tissue consequences related to breast implant sizeand projection.
Volume 126, Number 6 • Extra-High-Projection Breast Implants
2153

firmer the implant filler material, the greater thepressure that the implant focuses on adjacent tis-sues and the greater the risk of these deformities.
Temporary improvement occurs with high-and extra-high-profile implants in patients withglandular ptosis and other conditions. However,as surgeons observe these patients over time andinventory the tissue problems of high- and extra-high-profile patients seeking revision surgery,many surgeons recognize that higher profile im-plants almost invariably deliver one or more ofthe following:
1. Focused, maximal pressure where conse-quences are most dire, in the alreadystretched and thinned skin of the lowerpole, on overlying parenchyma, and on un-derlying chest wall.
2. Parenchymal pressure atrophy/thinningthat cannot be corrected, may compromiselactation and sensation, but for which pa-tients sometimes undergo reoperations witheven larger implants, site changes, or at-tempts at thickening the envelope with acel-lular dermal matrix grafts or fat injection.
3. Stretch of lower pole skin that produces (a)a more ptotic, “lower but larger” or “rock ina sock” breast; (b) a dramatic increase innipple-to–inframammary fold distance, (c)descent of the inframammary fold, or (d) acombination of (b) and (c) that produces a“bottomed-out” appearance.
4. Implant edge visibility and palpability.5. Visible traction rippling.6. Depression deformities of the rib cage,
which reduce projection, create deformity,and are essentially uncorrectable.
7. Compromised tissue vascularity from stretch,resulting in higher risks if later mastopexyis required.2
8. Disproportionate underfill of the upper poleas a result of a narrower implant dimension.
Some surgeons believe that ideal indicationsfor high- and extra-high-profile implants includeglandular ptosis and constricted lower polebreasts. A key question is whether these deformi-ties can be treated adequately and with less risk ofnegative tissue consequences with moderate-pro-file implants. Although anecdotal cases do notprovide scientifically valid answers, they may nev-ertheless provide insight. Figures 5 and 6 illustratechanges that occurred following treatment ofglandular ptosis with a larger and more projectingimplant. Figure 7 illustrates changes that occurredfollowing treatment of a constricted lower polebreast with a high-profile implant. These case ex-amples illustrate the inevitable tissue conse-quences of larger and higher profile breast im-plants, even in cases where logical indicationsseem to exist. Case examples such as these areinvaluable to help educate glandular ptosis pa-tients who want a large, projecting implant in lieuof a mastopexy, and a wide range of patients who
Fig. 2. A 30-year-old patient is shown 7 years after augmentation with a325-cc high-profile implant. The effects of capsular contracture have in-creased the projection of the breast implant, focused pressure on the overly-ing parenchyma and underlying chest wall, caused obliteration of overlyingparenchyma, caused dramatic skin envelope thinning, created radial-ori-ented stretch marks in the skin, and resulted in visible traction deformitiesto the thin overlying tissue. Similar tissue effects occur with breast implantsas implant projection or size increases, or with tighter tissues or more co-hesive filler materials.
Plastic and Reconstructive Surgery • December 2010
2154

request implants that are larger or more project-ing than their tissues can tolerate.
Patients who experience these effects oftensuffer severe emotional and self-esteem issues, andmany undergo multiple, additional operations inan attempt to correct problems that are often iat-rogenic and avoidable. The elective and medicallyunnecessary nature of breast augmentation makesnegative tissue compromises and uncorrectabledeformities all the more illogical and unnecessary.
Each of the negative consequences listed pre-viously is much greater in two specific groups ofpatients: (1) patients with a “tighter” skin enve-lope preoperatively, and (2) patients with a pre-
viously stretched and thinned envelope. Thegreatest risk to patients’ tissues from high- andextra-high-projection implants is using the im-plants in primary augmentation to force any pa-tient’s tissues to a preconceived or desired result.Figure 4 dramatically illustrates the potential tis-sue consequences for patients who may requesthigher projection and a high- or extra-high-pro-file implant. Surgeons should be fully aware thatthe firmer or more cohesive the silicone gelfiller of any implant, and/or the larger the im-plant, the greater the transmission of pressure totissues by the implant. The weight and pressureeffects of high- and extra-high-profile implants
Fig. 3. (Above) Severe thinning, stretch marks, and potential vas-cular compromise are evident intraoperatively, as minimal pres-sure from a retractor tip causes marked blanching of the skin en-velope in a 39-year-old patient 4 years postoperatively with high-profile 375-cc implants. (Below) Parenchymal atrophy, skinstretch, and skin thinning are seen in a 26-year-old patient afterexplantation of 400-cc high-projection implants just 4 years afterimplantation. The severe parenchymal atrophy and stretch thin-ning of the soft-tissue envelope are uncorrectable.
Fig. 4. Chest wall deformities, absence of parenchyma, andmarked lower pole skin stretch and thinning. Bilateral chest walldeformities and depressions are evident in a 24-year-old patientat explantation of high-profile, 425-cc implants, placed at her re-quest for increased projection, 5 years after primary augmenta-tion. Breast parenchyma is virtually nonexistent. The inframam-mary scar, placed 9 cm below the nipple in the inframammaryfold at the primary operation, is now located 13 cm below thenipple, quantifying the dramatic stretch of the lower pole skincaused by the implant.
Volume 126, Number 6 • Extra-High-Projection Breast Implants
2155

can be equally detrimental to tissues that are thinand stretched from pregnancy or from previous im-plants. Delivering the advantages of any implant de-sign with minimal compromises to patients’ tissuesrequires that surgeons understand implant–soft-tis-sue dynamics and carefully consider indications foruse of high- and extra-high-projection implants.
SUGGESTIONS FOR USE OF HIGH- ANDEXTRA-HIGH-PROFILE IMPLANTSTo avoid uncorrectable tissue compromises
and deformities for patients, surgeons should de-fine indications for implant selection using quan-tified, scientifically valid data, not intuition andsurgeon opinion. Requirements include measur-ing tissue characteristics including the thickness ofparenchyma and dimensions of skin, using provedimplant selection decision processes, and docu-menting changes in tissues over time that resultfrom extra-high-projection implants using clinicalmeasurements and breast imaging. This articledoes not define the level at which implant pro-jection or filler material may adversely or irrevers-ibly affect patients’ tissues. Specific indicationsbased on scientifically valid, comparative scientificdata are needed. Based on 45 years of combinedclinical experience, and prioritizing the safest out-
comes for augmentation and revision patientswith the least compromises, our current indica-tions for use of high- and extra-high-profile im-plants include the following:
1. High- or extra-high-projection implants arerarely indicated for primary breast augmenta-tion or revision. Published series indicate thata wide range of primary augmentation can beadequately treated with moderate projectiondevices that may have a lower risk of long-termtissue compromises. These series currentlydocument the lowest reoperation rates andrates of uncorrectable deformities in themedical literature for comparable series.3–9
In overly stretched envelopes and revisioncases, staged envelope reduction and sec-ondary placement of a smaller and less pro-jecting implant may be a much better optionfor preventing damage to patients’ tissues,and may incur less perioperative risks andprovide optimal predictability. The cost oftwo procedures is inconsequential com-pared with the cost of irreversible tissuecompromises and complications.
2. Highly cohesive, shaped implants are rarelyan ideal choice for reoperation or revisionbecause of the inability of surgeons to con-
Fig. 5. (Above) Result 6 years after treatment of glandular ptosis with high-profile, 500-cc implants and a periareolar “mastopexy.”The result illustrates a larger breast that is lower on the torso, with disproportionate lower breast fill, inadequate upper breast fill,a stepoff from chest wall to breast, and medial and lateral traction webbing at the junction of inframammary fold skin with the torso.(Below) Thepatient, despitecompromisedtissues, isbetterservedlong-termbyexplantationofthelarge, highlyprojectingimplantsto minimize further tissue consequences.
Plastic and Reconstructive Surgery • December 2010
2156

trol the tissue environment in already com-promised tissues. Previously stretched tissues(with or without vascular compromise) aremore prone to further stretch and to theinability to control pocket dimensions—acombination that increases risks of implantmalposition with shaped implants. If mini-mizing reoperations is the goal, round gelimplants may be a better alternative for re-operations compared with shaped implants.
3. Highly cohesive, shaped implants greaterthan 400-cc volume, even in wider breasts
with more lax skin envelopes,2,3 are rarelyindicated for primary or revision augmenta-tion because implant weight in these casesvirtually ensures more tissue stretch and lesspredictable implant position. Even if malpo-sition rates are low, they are not low forreoperation patients who require exchangeto a round implant when anatomical im-plant malposition occurs because of skinstretch around a shaped implant.
4. A highly cohesive, shaped implant, espe-cially with high or extra-high projection, is
Fig. 6. (Above) A 31-year-old patient with glandular ptosis who did not desire mastopexy and underwent augmentation withhigh-profile 375-cc implants (center), at 13 months postoperatively. The patient subsequently developed grade 3 capsular con-tracture (below) 23 months postoperatively, showing tissue thinning and webbing at the medial and lateral aspects of the infra-mammary fold skin. With relatively mild capsule contraction, implant edge visibility is present bilaterally in the upper medial aspectof the breasts because of skin thinning.
Volume 126, Number 6 • Extra-High-Projection Breast Implants
2157

never indicated for any primary breast aug-mentation patient’s tissues to force a pa-tient’s tissues to a desired result that exceedsan amount that can be substantiated to besafe by quantitative tissue measurementspreoperatively and peer-reviewed and pub-lished data.3–9 Peer-reviewed and publishedprocesses demonstrate unequivocally that byapplying tissue-based planning and implantselection, surgeons and patients can dramat-ically lower reoperation rates and exponen-tially reduce risks of uncorrectable tissuedeformities.3–9 These studies conclusivelydemonstrate that nearly any primary aug-mentation problem can be optimally treatedwithout using high- or extra-high-projection
breast implants while delivering the lowestreoperation rates and the most rapid recov-ery in the literature.
Although concerns and highly restricted indi-cations for use of high- and extra-high-projectionimplants may seem excessive to some colleagues,these indications have delivered scientifically ver-ified, peer-reviewed, and published patient out-comes that set benchmarks for dramatically im-proved patient recovery and reoperation rates anda low risk of permanent tissue compromise.3–9 Ex-ceeding the parameters of these studies usinglarge (�400 cc or �400 g) or high- and extra-high-projection implants requires that surgeonsdocument the safety and efficacy of high- and ex-
Fig. 7. An 18-year-old patient preoperatively (above, left), on the operating table (above, right) with 380-cc, high-profile,saline-filled implants filled to 440cc, and 2 years postoperatively (below, left). Six years later (below right), at age 24, followingthree additional operations, this patient had the potential for drastically negative tissue consequences even in young patientswith ideal tissues and with a deformity that seemingly provides logical indications for a high-profile or extra-high-profilebreast implant. The implant base width exceeds the base width of the atrophied parenchyma, inadequate soft-tissue coverageand tissue thinning have produced edge visibility, and the weight of the implant pulling on thin overlying tissues has pro-duced severe traction rippling. Mastopexy to improve the configuration of the stretched envelope has added additional tradeoffsof scars and potentially compromised sensation while questionably (and transiently) improving breast aesthetics.
Plastic and Reconstructive Surgery • December 2010
2158

tra-high-profile implants in comparable, scientif-ically valid studies.
POTENTIAL IMPROVEMENTS TOPROTECT PATIENTS’ TISSUES
Data currently exist that could be tremen-dously helpful to base the selection of high- andextra-high-profile implants on valid data. CurrentU.S. Food and Drug Administration premarketapproval data include serial magnetic resonanceimaging and device-specific adverse events data.These data could document types and degrees oftissue changes from a range of implant types andsizes. Unfortunately, to date, implant manufactur-ers have consistently used proprietary rights ex-planations to avoid providing these data for inde-pendent device- and size-specific review. Surgeonsand breast implant manufacturers who prioritizepatients’ tissues have an opportunity and a respon-sibility to take a closer and more scientific look athigh- and extra-high-profile breast implants andwork together to better define optimal, safe indi-cations and limitations for the use of these devices.
John B. Tebbetts, M.D.2801 Lemmon Avenue West, Suite 300
Dallas, Texas [email protected]
REFERENCES1. Mario AI, Molina AR, Malata CM. Indications for extra full
projection anatomical cohesive silicone gel implants in cos-metic and reconstructive breast surgery. Ann Plast Surg. 2008;61:607–612.
2. Handel N. Secondary mastopexy in the augmented patient: Arecipe for disaster. Plast Reconstr Surg. 2006;118:152S–163S;discussion 164S–165S, 166S–167S.
3. Tebbetts JB. A system for breast implant selection based onpatient tissue characteristics and implant-soft tissue dynamics.Plast Reconstr Surg. 2002;109:1396–1409; discussion 1410–1415.
4. Tebbetts JB, Adams WP. Five critical decisions in breast aug-mentation using five measurements in 5 minutes: The highfive decision support process. Plast Reconstr Surg. 2005;116:2005–2016.
5. Tebbetts JB. Patient acceptance of adequately filled breastimplants. Plast Reconstr Surg. 2000;106:139–147; discussion148–149.
6. Tebbetts JB. Dual plane (DP) breast augmentation: Optimiz-ing implant-soft tissue relationships in a wide range of breasttypes. Plast Reconstr Surg. 2001;107:1255–1272.
7. Tebbetts JB. Achieving a predictable 24-hour return to normalactivities after breast augmentation: Part I. Refining practicesusing motion and time study principles. Plast Reconstr Surg.2002;109:273–290; discussion 291–292.
8. Tebbetts JB. Achieving a predictable 24-hour return to normalactivities after breast augmentation: Part II. Patient prepara-tion, refined surgical techniques and instrumentation. PlastReconstr Surg. 2002;109:293–305; discussion 306–307.
9. Tebbetts JB. Achieving a zero percent reoperation rate at3 years in a 50-consecutive-case augmentation mamma-plasty premarket approval study. Plast Reconstr Surg. 2006;118:1453–1457.
Instructions for Authors: UpdateEthical Approval of Studies/Informed Consent
Authors of manuscripts that describe experimental studies on either humans or animals must supply to theEditor a statement that the study was approved by an institutional review committee or ethics committee andthat all human subjects gave informed consent. Such approval should be described in the Methods sectionof the manuscript. For studies conducted with human subjects, the method by which informed consent wasobtained from the participants (i.e., verbal or written) also needs to be stated in the Methods section.
In those situations where a formal institutional review board process is not available, the authors must indicatethat the principles outlined in the Declaration of Helsinki have been followed. More information regardingthe Declaration of Helsinki can be found at http://www.wma.net/e/policy/b3.htm.
Volume 126, Number 6 • Extra-High-Projection Breast Implants
2159





![2014FALL phys211a EELS ZihanXU A53044451courses.physics.ucsd.edu/2014/Fall/physics211a/specialtopic/eels2.pdf · Physics’211A’[2014FALL]’ElectronEnergy’Loss’Spectroscopy’](https://img.pdfslide.us/doc/110x75/5af423d17f8b9a92718d2046/2014fall-phys211a-eels-zihanxu-211a2014fallelectronenergylossspectroscopy.jpg)