Embed Size (px)
Citation preview

December 2015
Specialized Skills Training Workbook
1
Texas Department of Assistive and Rehabilitative Services
Division of Early Childhood Intervention Services

December 2015
Table of ContentsWhat is the SST Workbook?.........................................................................................................4
Section 1 – Brain Development, Cognitive Processes and Executive Functioning......................6
Child Development - Review.....................................................................................................6
Basics of Infant and Toddler Brain Development......................................................................6
Nutrition matters....................................................................................................................7
Positive relationships with primary caregivers are essential..................................................7
Experiences influence the brain – both positively and negatively.........................................7
Myelination and Response Time...........................................................................................8
Cognitive Processes and Executive Function...........................................................................8
Executive Function – A Lifelong Skill.......................................................................................10
The Impact of Cognitive Skills on Overall Development..........................................................11
Executive Function – Extension...............................................................................................12
Section 2 – Scaffolding................................................................................................................13
Scaffolding – Extension...........................................................................................................14
The ASD Toddler Initiative has developed two modules about effectively using and then fading prompts. Although the focus of these modules is on infants and toddler with ASD, the strategies outlined in the modules can be used with all children in ECI..................................14
Module 1 – Least to Most Prompting: http://asdtoddler.fpg.unc.edu/prompting/steps-implementing/least-most-steps-implementing.........................................................................14
Module 2 – Graduated Guidance Prompting: http://asdtoddler.fpg.unc.edu/table-contents/steps-implementing/graduated-guidance-steps-implementing...........................................................................................................................14
Section 3 – What Does an SST Visit Look Like?.........................................................................15
Extension – Coaching Practices..............................................................................................17
Section 4 – Behavior and Social Emotional Skills.......................................................................18
Challenging Behavior...............................................................................................................18
Why do toddlers tantrum as frequently as they do?................................................................23
Now You Try........................................................................................................................24
Toileting...................................................................................................................................26
Challenging Behavior and Social Emotional Skills – Extension..............................................27
Section 5 – Developmental Strategies and Activities..................................................................29
2

December 2015
Responsive Caregiving............................................................................................................29
Routines, Natural Environments and Familiar Adults..............................................................32
Now You Try:.......................................................................................................................34
Development and Learning......................................................................................................36
Activity Analysis...................................................................................................................36
Cognitive and Social-Emotional Development and Activities..................................................38
Cognitive/Social-Emotional Activity Table...........................................................................39
Activity Suggestions.............................................................................................................41
Activity Suggestions.............................................................................................................42
Activity Suggestions.............................................................................................................43
Activity Suggestions.............................................................................................................44
What are your activity ideas?...............................................................................................44
Now You Try:.......................................................................................................................45
Activity Suggestions.............................................................................................................49
Activity Suggestions.............................................................................................................50
Activity Suggestions.............................................................................................................51
What are your activity ideas?...............................................................................................51
Now You Try:.......................................................................................................................52
Activity Suggestions.............................................................................................................56
What are your activity ideas? ..............................................................................................57
Now You Try:.......................................................................................................................58
Activity Suggestions.............................................................................................................62
What are your activity ideas? ..............................................................................................62
Now You Try:.......................................................................................................................63
Activity Suggestions.............................................................................................................67
What are your activity ideas? ..............................................................................................68
Now You Try:.......................................................................................................................69
Activity Suggestions.............................................................................................................73
What are your activity ideas? ..............................................................................................73
Now You Try:.......................................................................................................................74
Developmental Activities – Extension......................................................................................78
Section 6 – Global Child Outcomes and Family Outcomes.........................................................81
3

December 2015
Global Child Outcomes............................................................................................................81
Family Outcomes.....................................................................................................................83
Child Outcomes – Extension...................................................................................................83
Section 7 – Transition and School Readiness.............................................................................84
Section 8 – Documentation of SST.............................................................................................85
Why is documentation important?...........................................................................................85
Exercise #1 - Getting to know the readers...........................................................................87
Minimum Requirements.......................................................................................................88
Exercise #2 - Getting to know the rules...............................................................................89
Exercise #3 - Getting to know the required elements..........................................................90
What should progress notes look like?................................................................................93
Exercise #4 – Getting to know the contents of a progress note..........................................96
Exercise #5 – Getting to know when there’s room for improvement.................................106
What are some routine checks?........................................................................................115
Check Your Answers for the Documentation Exercises........................................................117
Getting to Know the Readers (page 83)............................................................................117
Getting to Know the Rules (page 85).................................................................................117
Getting to Know the Required Elements (page 86-88)......................................................117
Getting to Know the Contents of a Progress Note (page 92-93).......................................118
Getting to know when there’s room for improvement (page 102-110)..............................118
What is the SST Workbook?This workbook, developed in conjunction with the Specialized Skills Training (SST) document, is intended to be used by Early Intervention Specialists to enhance their knowledge of Specialized Skills Training. Specialized Skills Training is a service that is exclusively provided by Early Intervention Specialists employed by ECI programs (programs who contract with the Texas Department of Assistive and Rehabilitative Services to provide Part C services). It provides information essential to delivering effective Specialized Skills Training, and extends the EIS’s knowledge of developmentally appropriate activities for infants and toddlers. Additionally, the workbook provides several opportunities for the EIS to practice implementing the skills he/she has learned.
4

December 2015
Early intervention Specialists can earn continuing professional education (CPE) credits for completing portions of, or the entire workbook. The amount of CPE is determined by the amount of time spent reviewing the information and completing the activities, up to 10 hours per year. Use the CPE Documentation Log to determine how many hours of CPE should be awarded. The EIS’s supervisor will need to fill in the number of hours and sign the certificate. (https://admin.abcsignup.com/files/{07D0901F-86B6-4CD0-B7A2-908BF5F49EB0}_59/36992/SSTcertificate.pdf)
5

December 2015
Section 1 – Brain Development, Cognitive Processes and Executive Functioning
Child Development - Review This section provides information about brain development and the building blocks of cognitive processes in infants and toddlers. If you need a review of general infant and toddler development, complete the Children’s Medical Services Infant and Toddler Development Module - http://www.cms-kids.com/providers/early_steps/training/itds/module1/module1.html
Basics of Infant and Toddler Brain Development Providers of any early intervention service must understand the basics of infant and toddler brain development. Brain development research answers the basic question of why early intervention is so important and why a child should not wait until he/she goes to school to receive services. Research demonstrates the brain is the most malleable or “plastic” during the infant and toddler years.
The brain is much more sensitive to experience in the first few years of life than in later years.(Tierney & NELSON III, 2009)
Providing early intervention services is both an exciting opportunity, because of the potential for rapid change and improvement, and a great responsibility, because the intervention, or lack of appropriate intervention, can have a life-long effect on the child.
During the infant and toddler period, the brain undergoes tremendous growth and development. A newborn’s brain is only 25% of the size of an adult’s brain. In contrast, a three year old’s brain is 80% of the size of an adult’s. During the first three years of life, the brain develops millions of connections, or synapses, between the existing neurons. At its peak, the cerebral cortex creates an astonishing two million new synapses every second (Zero to Three). These connections are strengthened or “pruned” depending on use.
The Zero to Three website has a “brain map” that provides information about brain development at different ages. Link to the Zero to Three brain map: http://www.zerotothree.org/child-development/brain-development/baby-brain-map.html
The key points about brain development addressed below are the basis for many of the early intervention evidence based practices. EISs should incorporate these principles
6

December 2015
into their SST visits and can use brain development research to explain why the strategies based on these principles are effective.
Nutrition mattersHave you ever wondered why IDEA requires that we assess the nutritional needs of eligible children? A baby must have adequate nutrition in order to produce new brain cells. Children who are malnourished have brains that are smaller than normal, because of reduced dendritic growth, reduced myelination, and the production of fewer glia (supporting cells in the brain which continue to form after birth and are responsible for producing myelin). Inadequate brain growth explains why children who were malnourished as fetuses and infants often suffer lasting behavioral and cognitive deficits, including slower language and fine motor development, lower IQ, and poorer school performance (Zero to Three). Early intervention services will not be very effective if the child is not receiving adequate nutrition.
Positive relationships with primary caregivers are essentialInfants prefer human stimuli over everything else. They innately orient to people's faces and would rather listen to speech or singing than any other kind of sound. Scientists have not discovered any special tricks for enhancing the natural wiring phase in children's brain development. Normal, loving, responsive caregiving seems to provide babies with the ideal environment for encouraging their own exploration, which is always the best route to learning (Zero to Three).
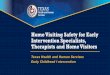
Experiences influence the brain – both positively and negativelyResearchers use the term plasticity to describe the brain's ability to change in response to repeated stimulation. Our brains prepare us to expect certain experiences by forming the pathways needed to respond to those experiences. For example, our brains are "wired" to respond to the sound of speech; when babies hear people speaking, the neural systems in their brains responsible for speech and language receive the necessary stimulation to organize and function (Perry, 2006). The more babies
7
This graphic demonstrates how brain synapses increase as the child grows. It also demonstrates how certain synapses are strengthened (darker/bolder lines) through consistent use. Source: Corel, JL. The postnatal development of the human cerebral cortex. Cambridge, MA: Harvard University Press; 1975.
December 2015
are exposed to people speaking, the stronger their related synapses become. If the appropriate exposure does not happen, the pathways developed in anticipation may be discarded or “pruned”. It is through these processes of creating, strengthening, and discarding synapses that our brains adapt to our unique environment. Because the brain adapts to its environment, it will adapt to a negative environment just as readily as it will adapt to a positive one (Child Welfare Information Gateway).
Myelination and Response TimeAlthough all of the neurons in the cortex are produced before birth, they are poorly connected. Newborns' brains contain very little myelin, the dense impermeable substance that covers the length of mature brain cells and is necessary for clear, efficient electrical transmission. This lack of myelin is the main reason why babies and young children process information so much more slowly than adults. It explains why it might take a toddler a minute or more to begin responding to a request such as "Joey, bring Mommy the teddy bear." Myelination of the cerebral cortex begins in the primary motor and sensory areas, regions receiving the first input from the eyes, ears, nose, skin, and mouth. It then progresses to "higher-order," or association regions controlling the more complex integration of perception, thoughts, memories, and feelings. Myelination is an extended process: although most areas of the brain begin adding this critical insulation within the first two years of life, some of the more complex areas in the frontal and temporal lobes continue the process throughout childhood and perhaps well into a person's 20s (Zero to Three).
In review, watch the one minute video clip from the Discovery Channel about brain development: http://health.howstuffworks.com/human-body/398-understanding-the-brain-development-video.htm
Cognitive Processes and Executive Function Cognitive processes are a major focus of Specialized Skills Training. As stated in the SST document, EISs are credentialed specialists in:
Infant and toddler development, both typical and atypical patterns Early childhood cognition, motivation and how infants and toddlers learn Typical infant and toddler behavior and challenging behaviors (biting, tantrums,
picky eating, sleep issues) Infant and toddler social interactions Understanding how developmental areas are interconnected
8

December 2015
Additionally, IDEA includes the following information in the definition of Special Instruction (SST):
the design of learning environments and activities that promote the child’s acquisition of skills in a variety of developmental areas, including cognitive processes and social interaction.
The cognitive development domain includes four components describing how young children develop and demonstrate abilities: exploring the world around them, solving problems, remembering and retaining information, and pretending and using their imagination. Cognitive development is growth in children’s thinking, reasoning, and understanding. Positive early experiences supporting cognitive development contribute to lifelong traits, such as curiosity and persistence.
The four components of the cognitive domain are part of a cognitive process called Executive Function. Executive function “refers to a group of skills that helps us to focus on multiple streams of information at the same time, monitor errors, make decisions in light of available information, revise plans as necessary, and resist the urge to let frustration lead to hasty actions” (The Center on the Developing Child at Harvard University, Working Paper 11).
The building blocks to executive function are skills developed over time, starting as early as the first year of life. SST is an appropriate service to help parents learn how to support their child’s development of executive function skills. Three building blocks for executive function are:
i. Working memory - which includes the ability to following multiple-step instructions and taking turns in group activities;
ii. Inhibitory control - which makes the following possible: selective, focused, and sustained attention. It also includes joint attention, and the ability to take turns; and
iii. Cognitive flexibility - which includes the ability to switch gears and adjust to changed demands.
Watch the 5 minute video for an explanation of the building blocks of executive function and how they work together: Executive Function: Skills for Life and Learning (2012)
Let’s look at how the skills of executive function relate to the cognitive process of problem solving.
9

December 2015
Problem solving requires 4 steps:
1. Assessing the problem2. Developing a plan to address the problem3. Executing the plan4. Evaluating the effectiveness of the plan
Skills needed to assess the problem include working memory of the issues related to the problem and the ability to focus (inhibitory control) on the problem. Skills to develop a plan include working memory of the available options and inhibitory control to arrive at the best plan. Execution of the plan requires inhibitory control and cognitive flexibility, as seen in the ability to change priorities or fix mistakes. Evaluation of the plan requires the use of all 3 skills: working memory, inhibitory control, and cognitive flexibility.
Executive function includes both cognitive processes and social interaction. As noted above, the building block, inhibitory control, includes joint attention and turn taking. Joint attention and turn taking are also foundational social skills. Behavior issues may impact a child’s ability to benefit from intervention for delays in other domains.
So much of a toddler’s learning involves social interaction. As a result, an early intervention program that promotes attention to people and social cues may pay dividends in promoting the normal development of brain and behavior.-Dr. Geraldine Dawson, a professor at the University of North Carolina, Chapel Hill.
Executive Function – A Lifelong Skill A new evidence base has identified executive function skills as being essential for school achievement, success in work, and healthy lives. The Center on the Developing Child at Harvard University has published a new two-page summary, InBrief: Executive Function: Essential Skills for Life and Learning (2012), outlining how these skills develop, what can disrupt their development, and how supporting them pays off in school and life.
10

December 2015
The Impact of Cognitive Skills on Overall Development EISs are the child development experts on the IFSP team. As such, it is important to identify how the intervention provided to address cognitive and/or social-emotional delays will impact the development of a child in the other developmental domains. The BDI Summary Sheet example below demonstrates this connection for a child with a motor delay. In this example, we can see that Angelita’s motor delay might be impacting her performance in other domains that require motor skills. This same concept will hold true for children with cognitive or social-emotional delays. Young children’ development is interconnected. A delay in one area will more than likely affect the other developmental areas. In the next section, you will have opportunities to practice making those connections yourself by doing an activity analysis.
11

December 2015
Executive Function – Extension 1) After you have had an opportunity to practice some of the exercises in your workbook, you will benefit from additional training on Executive Function. The Harvard Center on the Developing Child has a new online training module to help early care and education providers better understand and support the development of executive function skills. The modules were produced by the Washington State Department of Early Learning, in collaboration with the Center's Frontiers of Innovation initiative.
2) You will need to be able to talk about SST as a service to families, and as part of your program’s public awareness activities. Neuroscientific research on the early brain is a critical part of the evidence base for early childhood. Yet it can be difficult to understand and convey this information. ReadyNation, in collaboration with the Center on the Developing Child at Harvard University, has developed and compiled an array of tools enabling individuals without a science background to understand and present this evidence to diverse audiences. The following are a few tools available on the ReadyNation website. http://www.readynation.org/advocacy-toolkit/).
Heavily annotated PowerPoint presentation that can be delivered in 12-15 minutes.
Four short (3 to 9 minute) videos from the Center on the Developing Child or Invest in US, a project of the First Five Years Fund.
Talking points to accompany any of these videos. They can be used on their own, or embedded in a larger presentation.
Briefs from the Center on the Developing Child which detail the foundations of lifelong health, the science of early childhood development, the impact of early adversity on children’s development, and early childhood program effectiveness.
3) The Harvard Center for the Developing Child has developed a guide which describes a variety of activities and games that represent age-appropriate ways to support and strengthen various components of Executive Function and Self-Regulation in children. http://developingchild.harvard.edu/resources/tools_and_guides/enhancing_and_practicing_executive_function_skills_with_children/
12

December 2015
Section 2 – Scaffolding In addition to their strong knowledge base in infant and toddler development, EISs must also have a thorough grasp on how infants and toddlers learn. The phases of the learning process are:
• acquisition - learning how to do the skill• fluency- learning to do the skill smoothly and at natural rates• maintenance - learning to do the skill after instruction has stopped• generalization- learning to apply the skill whenever and wherever it is needed.
One of the most frequently used models in early intervention to support children’s learning throughout the different phases is “scaffolding”. The term scaffolding was coined by researchers David Wood, Jerome Bruner and Gail Ross based on Len Vygotsky’s theory of the Zone of Proximal Development.
The zone of proximal development (ZPD) has been defined as "the distance between the actual developmental level as determined by independent problem solving and the level of potential development as determined through problem solving under adult guidance, or in collaboration with more capable peers" (Vygotsky, 1978, p86)
Wood, Bruner and Ross proposed once the child, with the benefit of scaffolding, masters the task, the scaffolding can then be removed and the student (child) will then be able to complete the task again on his own. In early intervention, much of the scaffolding or support you will provide is through prompts. The ASD Toddler Initiative describes and provides video examples of commonly used prompts in early intervention: http://asdtoddler.fpg.unc.edu/prompting-module/overview-prompting/what-prompting/types-prompts (Types of Prompts page only)
The Center for Medical Services provides more information about scaffolding in early intervention. http://www.cms-kids.com/providers/early_steps/training/itds/module4/lesson2_6.html(Note that this link will take you to the middle of the larger training module. Information about scaffolding can be found in the middle of the page and continues until the next page – the end of the module.)
13

December 2015
Scaffolding – Extension The ASD Toddler Initiative has developed two modules about effectively using and then fading prompts. Although the focus of these modules is on infants and toddler with ASD, the strategies outlined in the modules can be used with all children in ECI.
Module 1 – Least to Most Prompting: http://asdtoddler.fpg.unc.edu/prompting/steps-implementing/least-most-steps-implementing
Module 2 – Graduated Guidance Prompting: http://asdtoddler.fpg.unc.edu/table-contents/steps-implementing/graduated-guidance-steps-implementing
14

December 2015
Section 3 – What Does an SST Visit Look Like?Do you have a thorough understanding of what an early intervention visit should look like? Click on the link to access a short video from Virginia’s Part C Integrated Training Collaborative, about Coaching in Early Intervention: http://www.youtube.com/watch?v=sL_WOCu3Ptg
The Making It Work Service Delivery module introduces the basic structure of early childhood intervention visits using the early intervention coaching model as developed by M’Lisa Shelden and Dathan Rush. As a review, a service delivery visit should consist of the following five steps:
Joint Planning Observation Action/Practice Feedback Reflection
The specialization and individualization of the service occurs during these five steps. Every child and family will have different discussions during joint planning, different activities will be observed, and different strategies will be used during the action and practice phase. Additionally, feedback will be individualized to the family and will be based on the strategy being taught and practiced. Likewise, the reflection phase will be individualized to the needs of the child and family.
The activities used during the action and practice phase for Specialized Skills Training visit should:
Assist the parent in supporting their child’s development across domains with an emphasis on strengthening cognitive skills, positive behaviors and social interactions, and
Promote the parent’s confidence and competence in addressing their child’s development.
Furthermore, according to Texas Rule, SST visits should “…include skills training and anticipatory guidance for family members, or other significant caregivers to ensure effective treatment and to enhance the child's development.” By definition anticipatory guidance is “guidance provided by an expert or knowledgeable group to those with a particular interest (e.g., parents), anticipating likely upcoming concerns.” (Medical Dictionary) When provided with practical developmental information prior to significant physical, emotional and psychological milestones, parents are better able to anticipate
15

December 2015
impending changes, maximize their child's developmental potential and identify their child's special needs.
There are numerous examples of the types of activities that can be used during SST visits in this workbook. Remember, each SST visit will be individualized to the needs of the child and family. Even SST visits for the same child should not look exactly the same from week to week. Each of the five phases of the SST visit should evolve and change based on the child’s progress.
No matter which strategies are being used, parent or caregiver engagement during SST is crucial for the coaching process to be effective. You can ensure parent engagement by including “return demonstration” as part of the action/practice portion of the visit. Return demonstration allows the EIS to ensure that the parent understands how to use the strategy or activity the EIS has taught. Return demonstration occurs in an SST visit when:
The parent immediately practices an activity the EIS taught. The parent shows the EIS a videotaped example of using a previously taught
activity with the child. The parent demonstrates how she has used the strategy during a routine and
discusses the success or challenges.
Different parents will have varying degrees of ease demonstrating their understanding of a concept. It is important to help all parents feel comfortable with this process. If parent learning is emphasized throughout the pre-enrollment and IFSP process, parents will be prepared for the approach, and you will be able to move toward complete implementation of this valuable technique.
Documenting your service is an important and necessary part of your work. You can use your documentation as a tool to support the coaching process. You reflect with the parent about what was planned for the family to do since your last visit, and how well the plan was implemented; what worked and what didn’t work. You discuss and document your observations of the parent’s demonstration of the planned activities. This gives you an opportunity to give positive feedback to the parent, tweak the activity in some way if needed, and demonstrate your suggestions for changes or next steps. You then document your feedback to the parent, and together, you plan what the family will do until the next visit. Documenting all of this information will provide the family reminders of everything that was discussed and things to do until your next visit. Documenting all of these things takes time, so be sure to include this time when you plan for the visits on the IFSP. Depending on the needs of the family, you can
16

December 2015
document as you go, or at the end of the visit. More information about documentation of SST visits can be found in Chapter 8.
Extension – Coaching Practices Coaching Quick Reference Guide by Dathan Rush and M’Lisa Shelden: http://fipp.org/static/media/uploads/briefcase/briefcase_vol1_no1.pdf
Tips and Techniques for Effective Coaching Interactions by Dathan Rush and M’Lisa Shelden: http://fipp.org/static/media/uploads/casecollections/briefcase_vol1_no2.pdf
Common Misconceptions about Coaching in Early Intervention by Dathan Rush and M’Lisa Shelden: http://fipp.org/static/media/uploads/casecollections/caseinpoint_vol4_no1.pdf
17

December 2015
Section 4 – Behavior and Social Emotional Skills
Challenging Behavior During your work as an SST provider, you’re likely to encounter defiance, aggression and other challenging behavior from the children you see. Toddlerhood in particular is a time for children to learn the bounds of acceptable behavior. This is demanding for early intervention providers, because the criteria for what is acceptable vary across cultures and families. Even within a single family, it’s common for caregivers to disagree about which behaviors are appropriate, and to have different ideas about the best way to manage challenging behavior. As an EIS, you may be asked to help families deal with typical toddler behavior problems. In other situations, you may recognize behavior challenges, such as frequent or prolonged tantrums, are getting in the way of working on and meeting IFSP outcomes.
All children benefit from having their social-emotional development supported through positive and responsive relationships with their parents and primary caregivers. Therefore, the foundation for all ECI services, including SST, is responsive and supportive caregiving practices. However, as demonstrated in this graphic, some children need intervention that is beyond positive relationships and supportive environments to address their delayed or atypical social-emotional skills. This chapter offers some strategies for working with parents and caregivers to address these challenging behaviors.
18

December 2015
Causes of Challenging Behavior and Strategies for Managing Them
Issue Related to Challenging Behavior
Why It May Lead to Behavior Problems Behaviors You Might See Strategies To Try
Typical Development Emotional and neurological response to learning new skills (“Touchpoints”)
Testing increased autonomy Anxiety about new experiences
Refusing to comply with instructions
Tantrums or crying for no apparent reason
Waking during the night (after sleep patterns have been established)
Saying “No” to every offer, even those he or she wants
Mild aggression toward other children and familiar adults
Consolable fear of situations or people that did not bother the child before
Provide anticipatory guidance to parents (See the Touchpoints series by Brazelton for more information)
Help parents reframe challenging behavior as a typical response to new skill development
Help parents recognize positive behaviors to reward
Model and encourage parents to ignore tantrums
Help parents identify age-appropriate consequences for aggression
Environmental Triggers Too many choices leading to overstimulation or distraction
Lack of opportunities for age-appropriate exploration
Sensitivity to:o Noise levelso Particular noises (e.g. vacuum
cleaner)o Temperatureo Crowdso Itchy clothingo Visually “busy” environments
Tantrums for no discernible reason
Screaming or crying for no other reason
Inattention to other people Acting without regard to
personal safety Withdrawing to another
environment Hyperactivity
Help parents identify environmental factors that might cause discomfort
Introduce potential triggers gradually and pair with something the child enjoys
If problems are severe or persistent, consult with OT to see if sensory strategies might be appropriate
19
December 2015
Issue Related to Challenging Behavior
Why It May Lead to Behavior Problems Behaviors You Might See Strategies To Try
Developmental Delays Frustration due to the child’s inability to use skills (such as words to indicate wants, or to move across the room to get a toy)
Parent’s inability to read the child’s nonverbal cues, which may differ from those of typical children
Parental expectations for the child to have the skills of a typically-developing child
Tantrums Aggression
Help parents understand the roots of the child’s frustration
Help the parents teach the child compensatory skills (e.g. signs if the child’s words are unintelligible)
Identify and alert the parents to cues the child is becoming frustrated, is hungry, etc. to prevent the undesirable behavior
Trauma Overly sensitive neurological response to even minor stressors sets off “fight or flight” behavior
Heightened wariness of danger Sense of uncertainty, helplessness and
lack of control Attachment problems, if abuse or
neglect occurred
Tantrums Aggression Sleeplessness Changes in appetite Physical and emotional
withdrawal Nightmares Overly friendly and
affectionate to strangers Ritualized self-calming
behaviors Anxiety or fearfulness Hypervigilance
If you suspect a child’s challenging behavior is a result of trauma, refer to a professional with social-emotional expertise (e.g. LMSW, LPC, Psychologist) with expertise in very young children
Executive Functioning Problems
Reduced ability to connect consequences with behaviors
Difficulty focusing Difficulty transitioning from one activity
to another Reduced ability to interpret social cues Difficulty adapting to new environments
or changes in familiar ones Difficulty with delayed gratification Difficulty with listening attention and
Inattention Doesn’t follow rules Doesn’t seem to learn from
consequences Lack of awareness of safety
issues Aggression Hyperactivity Impulsivity Difficulty socializing with
Teach caregivers to make sure they have the child’s attention before they speak to him
Help the family find outlets for the child’s high activity level
For older children, play games that reinforce paying attention and not acting on impulse (e.g. Mother May I, Simon Says, Red Light/Green Light, Ring Around
20

December 2015
Issue Related to Challenging Behavior
Why It May Lead to Behavior Problems Behaviors You Might See Strategies To Try
processing auditory information other children the Rosey) Pair spoken information or
instructions with visual cues Make sure consequences are
immediate and of a short duration
Consult OT, SLP and/or licensed professional with expertise in social-emotional development (e.g. LPC, LMSW) if strategies are unsuccessful
Medical/Physical Issues Physical pain or discomfort decrease ability to focus and learn
Invasive or painful procedures may result in trauma
Side effects of medication can include:o Increased activity levelo Gastric problemso Increased aggressiono Drowsinesso Sleeplessness
Inattention/lack of focus Frequent, inconsolable
crying or screaming Withdrawal Hyperactivity Aggression
Help parents find the best times of day for different activities
Teach parents to use activities the child finds calming or stimulating depending on what the child needs
Accompany parents to medical appointments to help them explain any problematic side effects
Help parents establish calming bed time routines if sleep is a problem
Consult RN, dietitian, OT or licensed professional with expertise in social-emotional development (e.g. LCSW, LPC) if strategies are unsuccessful
Parenting Issues Lack of consistency Expectations for the child to progress
and learn like typically-developing children
Tantrums Aggression Withdrawal Doesn’t follow rules
Help parents develop age-appropriate consequences for problem behaviors
Provide anticipatory guidance
21

December 2015
Issue Related to Challenging Behavior
Why It May Lead to Behavior Problems Behaviors You Might See Strategies To Try
Ineffective or overly-harsh consequences
Lack of child development knowledge
Anxiety and other information on both typical and delayed child development
Help parents identify when they are not being consistent
If concerns persist, consult a licensed professional with expertise in family relationships (e.g. LPC, LCSW)
22

December 2015
Why do toddlers tantrum as frequently as they do?
Toddlers are known for their ability to go-go-go! Their high energy level, along with increasing physical motor development, allows them to explore their curiosity and test limits as their world expands. Because they are still developing executive function, this can often lead to tantrums and behavior issues.
23
Tantrum
Independence
Impulsivity
Curiosity
High Energy Levels
Frustration

December 2015
The following table provides a list of comments parents might make during a visit. There are several blanks at the end of the table to add in comments that you have heard. This activity will help you develop a repertoire of developmentally appropriate suggestions that can address parents’ concerns about their child’s behavior.
Consider what a more developmentally appropriate expectation would be, how you would respond, and what strategies you would recommend when discussing behavior concerns with a parent or caregiver. Fill in the blanks with your answers. Check with your supervisor or an experienced EIS to see if he/she agrees with your responses and suggested strategies.
What a parent might say…
Developmentally appropriate expectation…
How you would respond…
Strategies…
Clara does not like books—she will flip through pages quickly while I try to read to her.
Being able to focus for a shorter period of time, like pointing and naming 1-2 pictures a page.
Toddlers have shorter attention spans and sometimes have to build up their attention span
Start by sitting and naming 1-2 pictures a page, instead of reading. Look at books just after snack time (if child is sitting in a high chair)
Now You TryGracie is hyper—she will not sit still to watch a movie with us.
Ryan makes a mess when he feeds himself, but he insists on doing it alone and spills half of his food on the floor.
Ethan is impatient—he throws a tantrum at the grocery store while I’m doing the weekly shopping.
Joaquin gets angry when I don’t
24

December 2015
What a parent might say…
Developmentally appropriate expectation…
How you would respond…
Strategies…
understand what he wants. He will cry and scream when I ask him to tell me what he wants.Omar cries when it’s time to leave the park even when I’ve told him we can only stay for 30 minutes.
Elena does not like to share her toys. She will snatch them away and say “mine!”
25

December 2015
Toileting Even parents of typically-developing toddlers may view toilet-training as a particularly stressful task. The problems with toilet-training can be compounded with children with disabilities or delayed development. Here are some tips to help parents and other caregivers with toilet-training.
1. Make sure the child has the necessary skills to successfully learn to use the toilet independently. These include:
Feels discomfort when diaper is wet or dirty. Can effectively communicate needs. Can get to the bathroom independently. Can pull pants down independently.
If the child doesn’t have these skills, he/she may not be ready for toilet-training.2. Help the parent identify effective reinforcers for the child that can be given quickly
after the desired behavior (sitting on the toilet for 3 minutes, urinating in the toilet, etc.).
3. Start slow. See how long the child can sit on the toilet without getting up and build from there.
4. Remind families to reinforce even small improvements. For example, if the child was able to sit on the toilet for only 30 seconds before getting up, but is now able to stay there for two minutes, he/she should be rewarded with praise or some other reinforcer.
5. Make sure the child is getting plenty of fluid during the morning and early afternoon.
6. Help families identify the best time to toilet-train in relation to meals and snacks (for example, 30 minutes after eating).
7. Start toilet-training during a time when the family will be spending most of their time at home, not when lots of appointments outside the home are scheduled.
8. Remind parents toilet-training is a time-consuming process. It should not be started if caregivers don’t have much time to devote to the task.
9. Help the parent find ways to entertain the child while he/she sits on the toilet.10.Remind parents toileting accidents are common in young children, and a child
should never be punished for these.
For additional tips on toilet training, visit: http://www.aota.org/-/media/Corporate/Files/AboutOT/consumers/Youth/Establishing-Toileting-Routines-for-Children-Tip-Sheet.pdf
Notes:
26

December 2015
27

December 2015
Challenging Behavior and Social Emotional Skills – Extension The Backpack Connection Series was created by Technical Assistance Center on Social Emotional Intervention (TACSEI) to provide a way for teachers, early interventionists and parents/caregivers to work together to help young children develop social emotional skills and reduce challenging behaviorhttp://www.challengingbehavior.org//do/resources/backpack.html
TACSEI's "Making Life Easier" series is designed specifically for parents and caregivers. This series of tip sheets contains valuable information on how to make often challenging events easier to navigate, and even enjoyable, for both caregivers and children.http://www.challengingbehavior.org/do/resources/making_life_easier.html
The Center on the Social Emotional Foundations for Early Learning has designed learning modules that provides guidance on infant and toddler social-emotional development and responsive routines, environments and strategies to support an infant or toddler’s social emotional development. The modules can be accessed at this link: http://csefel.vanderbilt.edu/resources/training_infant.html. Participants should view the PowerPoint, read the PowerPoint notes, review the video clips and complete the activities.
The Center on the Social Emotional Foundations for Early Learning has also developed a video about promoting social emotional competence. The video is 30 minutes long.http://csefel.vanderbilt.edu/resources/social_emotional_competence.html
This guide from the Center on the Social Emotional Foundations for Early Learning addresses biting: http://csefel.vanderbilt.edu/documents/biting-parenting_tool.pdf
The Center on the Social Emotional Foundations for Early Learning has also developed a “What Works” series. These tip sheets are available in English and Spanish.http://csefel.vanderbilt.edu/resources/what_works.html
Beyond Use Your Words: How Babies Begin to Develop Self –Control in the First Three Years (Podcast – 24 minutes): https://s3.amazonaws.com/zttpodcastseries/podcast/Brenda%20Jones%20FINAL.mp3?s_src=podcast&s_subsrc=self_control
28

December 2015
Early Experiences Count: How Emotional Development Unfolds Starting at Birth (Podcast – 23 minutes): https://s3.amazonaws.com/zttpodcastseries/podcast/Ross%20Thompson%20FINALvs.mp3
Shh, Shh, It’s Okay: Coping With Crying in Babies and Toddlers (Podcast – 23 minutes): https://s3.amazonaws.com/zttpodcastseries/podcast/Pam%20High.mp3?s_src=podcast&s_subsrc=crying
Establishing Bath Time Routines for Children (Two page tip sheet)http://www.aota.org/-/media/Corporate/Files/AboutOT/consumers/Youth/BathTimeTipSheet.PDF
29

December 2015
Section 5 – Developmental Strategies and ActivitiesNormal, loving, responsive caregiving seems to provide babies with the ideal environment for encouraging their own exploration, which is always the best route to learning (Zero to Three).
This section will review the following: Ideas to support the family to help their child’s
development Strategies that fit into infant/toddler and family routines Developmentally appropriate activities
Watch the Serve and Return video from the Harvard University Center on the Developing Child for more information about how interactions from caregivers influence the architecture of a child’s brain:
http://developingchild.harvard.edu/resources/multimedia/videos/three_core_concepts/serve_and_return/
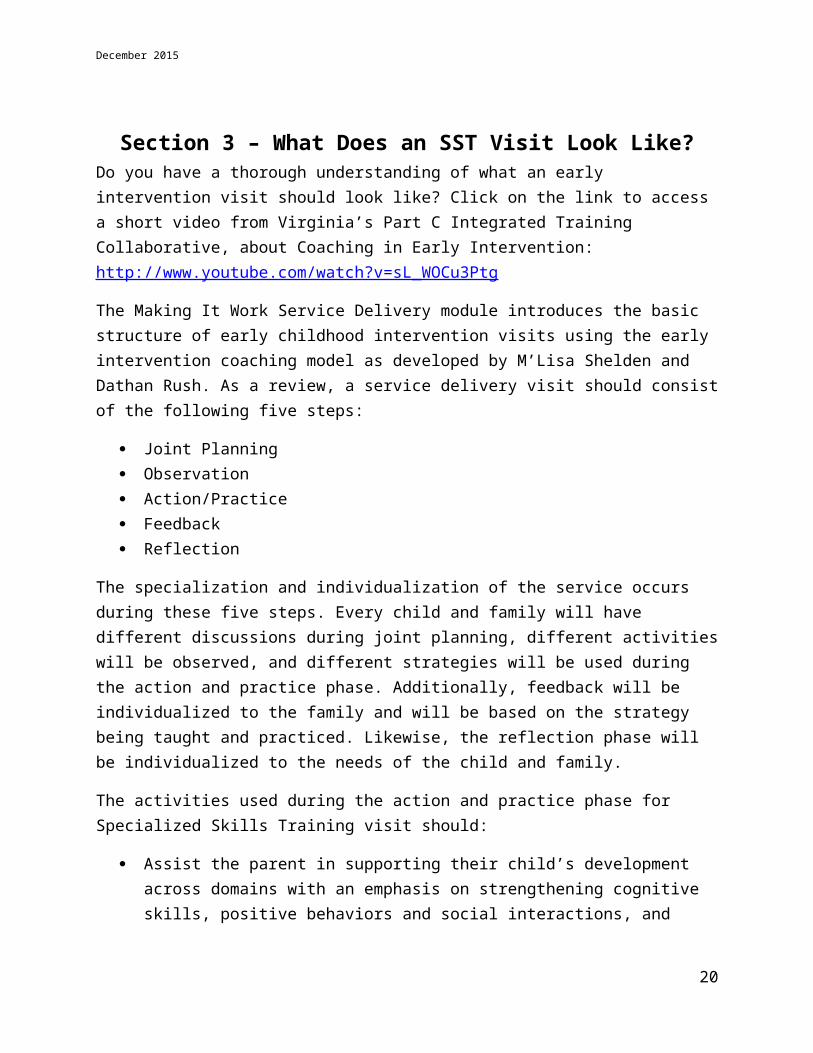
Responsive Caregiving
30
What is it? Responsive caregiving is a style of interaction in which caregivers take the time to pay attention to what a child is signaling, and then provide a response meeting the child’s needs in a loving way.
How can parents be responsive?
There are many kinds of behaviors caregivers can
use to be responsive; such as, voice tone, facial
expression, affection, and talking about the child's
interest and ideas.
Why is it important to Early Intervention Specialists? An EIS's knowledge of Responsive Caregiving can support the parents in promoting their child's development in all domains.

December 2015
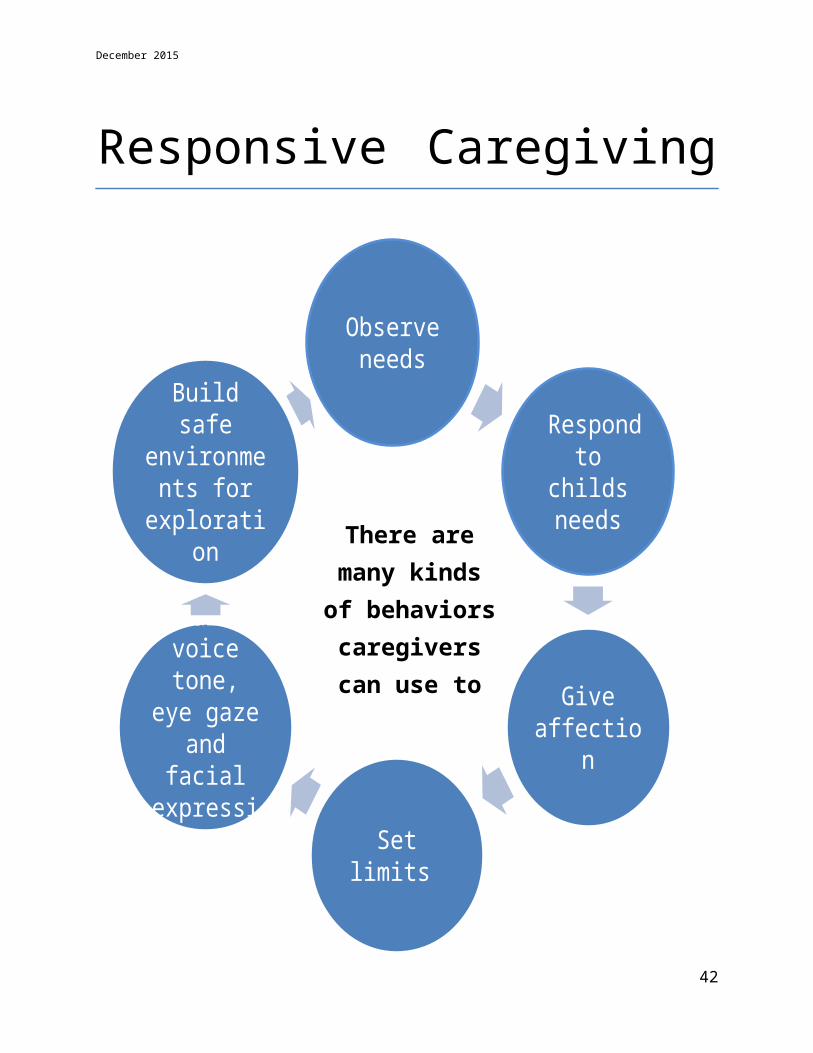
Responsive Caregiving
Responsive Caregiving
31
The first three years of life are the most
important years.
During this period, brain development
occurs at a very rapid rate in
response to each child’s early experiences
The quality of these early learning experiences is shaped by three factors: the caregiver with whom
the child spends his or her time, the child’s nutrition, and the child’s environment.
Research is clear that Responsive
Caregiving is critical to a child’s early
development.
There are many kinds of
behaviors caregivers can
use to be responsive.
Observe needs
Respond to childs needs
Give affection
Set limits
Modulate voice tone,
eye gaze and facial
expression
Build safe environments
for exploration

December 2015
Routines, Natural Environments and Familiar Adults
Responsive Feeding Practices
When therapeutic activities are embedded into the child’s and family’s daily routine – the environment becomes therapeutic.
Embed every activity into the child and family’s daily routines.
32
Feed infants directly and assist older children when
they feed themselves
Feed slowly and patiently, and encourage children to eat, but do not force them
If children refuse many foods, experiment with
different food combinations, tastes, textures, and
methods of encouragement
Feeding times are periods of learning and love – talk to
children during feeding, with eye to eye contact.
Minimize distractions during meals

December 2015
Daily routines are meaningful contexts for young children to learn new skills because they are predictable, functional, and occur numerous times throughout the day. Interventions can be integrated into play, caregiving, and other activity based routines. The following table gives examples of how activities can be built into the daily life of the child. These examples are only a few ideas in which routines and activities can be used.
IFSP Outcomes
Daily Home Routines
Ashley will say juice or water to ask for something to drink at meal time or snack time at least twice a day for three weeks.
Ashley will walk without having her hand held to the car from the house in the morning and from the car to the house in the evening daily for two weeks.
Ashley will point to at least three pictures when named during her bedtime story every night for a week.
Waking Routine Greet her when she wakes and cue her to either put her hands up or vocalize/verbalize a request for assistance out of her bed.
N/A N/A
Breakfast Give her options between two food items and/or drink items (e.g. Do you want the Cheerio’s or the yogurt?). Have Ashley verbalize a choice. Model the words for her to imitate.
Point to the eating area, and ask her to walk pushing her walker to the breakfast area.
Show a picture book. Talk or sing about the pictures in the book. Point to each picture when you talk about it.
Bathing/Toileting or Dressing
Ask her if she needs her diaper changed, encouraging her to imitate “yes” or “no”.
Offer hand to walk her to changing area.
Read picture books which discuss toileting.
Snack Time Give a small amount of Point to high chair N/A
33

December 2015
food or drink and ask if she wants more, asking her to sign or verbalize “more”.
and ask her to walk to it. Provide support if needed.
Play Time Give her options between two toys or play objects. Model the words she needs to use to express her choice.
Assist her to play ball (throw and catch) while she is standing.
Make a book with photographs of family members and pets. Encourage her to point to each family member when named. Assist her in turning the pages.
Now You Try:This exercise will help you develop a collection of activity strategies that can be used to work on a variety of IFSP outcomes. Pick three outcomes from a recent IFSP you developed. Fill in the outcomes at the top of the table and add in activity ideas for each of the applicable routines. You may also add in different routines at the end of the “daily home routines” column.
IFSP Outcomes
Daily Home Routines
Waking Routine
34

December 2015
Breakfast
Bathing/Toileting or Dressing
Snack Time
Play Time .
Notes:
35

December 2015
Development and Learning The development of a child into a highly complex being occurs synchronously across all domains of development. Skills in the Gross/Fine Motor, Cognitive, Social/Emotional, Speech, Language, Communication and Self Help/Adaptive domains develop together in a continuous spiral with lower level skills laying the foundation for the emergence of the next higher level skill.
Since the child is a holistic being and cannot be compartmentalized into any one domain, it is the engagement of the whole being in various activities that leads to the development of skills and learning. Learning occurs when the child actively engages in and frequently practices skills, receives timely and appropriate motivation and feedback, and when the activity occurs in an enjoyable setting involving personal interactions and a considerable level of personal support with familiar adults.
Activity AnalysisMany of the enjoyable activities children engage in everyday cross developmental domains. Activity analysis serves as a frame of reference when activities are identified to address outcomes and developmental needs, and can show the connection of why you using a particular activity.
Sample questions to ask (age ranges and activity are specific to this example):
How many developmental domains does this everyday play activity for children in the age group of 30-36 months impact?
What skills are needed for a 30 month old child to engage in ball play for 5 minutes?
How can this activity be modified/graded/individualized for this child?
Activity Gross Motor
Fine Motor Cognitive Social/
Emotional
Self Help Speech/ Language/ Communication
Ball throw and catch with familiar adult
Yes –sitting, transitions, standing, crawling, walking
Yes-midline orientation, bilateral coordination, eye-hand coordination
Yes -attention, working memory, inhibitory control, problem solving
Yes-meaningful interaction with significant adult
Yes - Balance, following directions, bilateral coordination
Yes – turn-taking, following directions, verbalizations during interaction, requesting
36

December 2015
More examples:
Activity Gross Motor Fine Motor Cognitive Social/Emotional
Self Help Speech/ Language/ Communication
Points to and labels pictures; answers simple questions; listens to stories read aloud
Yes- positioning(prone/sitting/tall kneel/ standing)
Yes – follow with finger/finger isolation/ visual tracking/ localization
Yes- attention, memory, processing
Yes – bonding/ meaningful interaction
N/A Yes – receptive and expressive naming (nouns, verbs, adjectives, etc.), wh-questions, auditory attention
Activity Gross Motor Fine Motor Cognitive Social/Emotional
Self Help Speech/ Language/ Communication
Kicking ball
Yes –standing, balance, maintenance of balance on one foot while kicking
No Yes -attention, working memory, inhibitory control, problem solving
Yes-meaningful interaction with significant adult
Yes - balance, following directions, bilateral coordination
Yes – turn-taking, following directions, verbalizations during interaction, requesting
37

December 2015
Cognitive and Social-Emotional Development and Activities The root skills needed to develop higher level cognitive processes, such as executive function, develop during the infant and toddler period. These skills include working memory, which is the ability to retain and work with information in the brain (WM); inhibitory control, which is the ability to focus attention and filter distractions (IC); and cognitive flexibility, which is the ability to switch mental or cognitive gears (CF). Executive function includes both cognitive processes and social interaction.
Social and emotional development is a broad domain which encompasses many skills forming the foundation all children need to become healthy, happy, and successful adults. Social/emotional skills include attachment/separation/autonomy (ASA), development of self (recognizing others are there) (DS), and learning rules and expectations- social interaction and play (RSI).
38
Cognitive
Inhibitory Control (IC)
Working Memory (WM)
Cognitive Flexibility (CF)
Social Emotional
Attachment/Seperation/
Autonomy (ASA)
Development of Self(DS)
Learning Rules and expectations- social interaction and play
(RSI)

Cognitive/Social-Emotional Activity TableThe following table explains how activities address the various components of cognitive and social-emotional domains.
June 2015 39

Age in months
Activity WM IC CF ASA DS RSI
0-6 Sing lullabies and tell the baby nursery rhymes. Use a soft and gentle voice when talking to baby.
Baby remembers familiar voices
Soothing voices help baby resist crying
Understands different voices may sing same song
Becomes attached to soothing voices
Identifies preferred voices or songs
Response to songs or rhymes promotes social development
6-12 Hide toy under cloth within child’s reach, remove cloth, instruct child not to touch, hide toy slightly out of reach, remove cloth
Object permanence
Not to touch Seek other methods of retrieval
Autonomy Not to touch
Learns rules
12-18 Take turns rolling a ball back and forth.
Child has to remember what he/she is supposed to be doing when it’s his/her turn again
Joint attention; child has to be able to release the ball and give the adult a turn
Understand adjustments may be made in the way the partner rolls the ball (e.g. different direction/to a different partner)
Autonomy Identifies the turn-taking partner(s)
Learn expectation of returning the ball once it is received—promotes turn-taking skills
18-24 Story time-let the child choose books to read and help turn
Child remembers familiar objects, actions
Wait to turn the page
Understanding books come in different sizes and shapes, and may have
Becomes attached to reading partner
Feels like he/she is in control of the reading
Learns rules of turn taking and reading (right side up, turn page by page)
June 2015 40

June 2015 41
Activity Suggestions
0-2 Months
June 2015 42
Anticipate child’s needs. Keep
diapers and bottle ready.
Call name when approaching to encourage head
turning from side to side in supine.
Hold child firmly, talk to the child and rock
gently.
Use bright mobiles, rattles, or
squeaky toys within 8-12 inches of
child's eyes.Encourage head
lifting in prone/supine,
support at shoulders while handling during daily routines.
Play in front of mirror, label body parts,
repeat child's name , wait for eye contact and response, and reward child with
smile.
Play Peek –a- Boo, sing nursery
rhymes, tell stories while holding child
in prone over mothers tummy.

Activity Suggestions
0-2 Months
June 2015 43
Alternate position of toys, light source and mobiles so child will turn to look
at different sides.
Move toys across midline,
encourage turning, talk and
sing to child while looking into eyes.
Lay child on stomach with
pillow under chest to encourage head
lifting.
Touch child’s hand with object
then move it away to encourage eye
tracking and reaching with
hands.
Lay child on side with toys in front
to encourage turning to side.
Encourage rolling supine to prone,
propping on arms and hold in
supported sitting while talking and singing to child.

Activity Suggestions
2–6 Months
June 2015 44
Caring for young children with
disabilities or special needs is the same as caring for all young
children. All children need love, good nutrition, safety,
guidance, and positive stimulation.
At bedtime use soothing voice to
calm; a music box to lull baby to sleep; sing
lullabies .Respond
quickly when infants are hungry by feeding,
holding, and cuddling them.
Talk with infants about what is
happening when bathing, diapering,
and dressing. (“Now I am
washing your arms.”)
Show enthusiasm for sounds made
through facial and vocal expression e.g. "Did you hear
that? A bell ringing!"
Bring child’s attention to
hands and feet, toes and fingers.
Tie soft colorful ribbons around
ankles and wrists when the baby
will have constant
supervision.
Repeat and emphasize
child's name and names of other family member
when you talk to child.

Activity Suggestions
2-6 Months Listen to and sing with infants often, especially during daily routines,
such as feeding and diaper changes. Give infants safe toys that produce interesting results or movements
in response to their actions (cause and effect toys). Hold, cuddle, hug, smile, and laugh with infants. Hold during bottle feeding times, and talk with them in a calm and
soothing tone. Use the child’s name often during your conversations throughout the day.
Notice, understand, and follow the signals of infants, such as cries for hunger or pain, turning away when full, or when ready to stop interacting.
Notice infants’ reaction when new people enter the room and introduce new people by name to the infant.
Create surroundings without a lot of loud noises and distractions. Place objects with different shapes, sizes, textures, and sounds within infants'
reach (make sure the objects are safe to mouth). Name and describe objects infants are exploring and encourage them to
continue to play with the objects by telling them you like their “music” or banging. Play “sound localization” games. Select a few sound makers – jingle bells,
rattles, crumpling paper, squeaky toys – make sounds 2 to 3 times, 5 to 7 inches from babies face and wait for response. Repeat the activity from a different direction and each time wait for baby to make eye contact with the sound maker.
What are your activity ideas?
June 2015 45

Now You Try:Activity analysis will allow you to determine which developmental areas are addressed when using a specific activity. Knowing this information is critical when documenting how your SST service helps the child meet his/her developmental outcomes and when explaining to parents and caregivers why you are suggesting certain strategies. Pick some of the
activities from pages 40 – 44 and analyze them as demonstrated on pages 36-37. You can review your analysis with your supervisor or another experienced EIS.
Activity Gross Motor Fine Motor Cognitive Social/Emotional
Self Help Speech/ Language/ Communication
June 2015 46

Analyze these activities even further by identifying some of the activities from the previous table addressing cognitive and social/emotional development and determine if
June 2015 47

they address the individual components of social/emotional and cognitive development. Examples of this analysis can be found on pages 38-40. You can review your analysis with your supervisor or another experienced EIS.
June 2015 48

Cognitive/Social-Emotional Activity Table
Activity WM IC CF ASA DS RSI
June 2015 49

Notes:
June 2015 50

Activity Suggestions
6-12 months
• Share books with older infants. Show them books with interesting colors, patterns, pictures, and textures.
• Notice when older infants drop items and pick them up, and allow them to repeat the dropping action.
• Allow older infants to touch your face, skin, or hair and name body parts (“That’s my nose. Here’s your nose.”).
• Provide toys and objects that make noise, and create opportunities to make and listen to different sounds together (crunch leaves or bang on pots and pans).
• Notice and respond positively to older infants’ desire to play games over and over again.
• Create an environment that encourages discovery, and give uninterrupted playtime.
• Give older infants safe toys to repeat motions, such as rocking, sliding, or balancing.
• Engage and play alongside older infants.
• Celebrate when older infants learn how to use a toy or object.
• Recognize toddlers' interest in the natural world and help describe what they see, hear, and experience.
• Explore surroundings and talk about how things are similar and different.
• Keep toys around that respond to older infants’ actions, such as pop-up boxes, squeaky toys, and musical instrument toys.
• Create a variety of safe spaces and objects for older infants to crawl over, around, and through.
• Give older infants similar toys of different sizes they can nest (bowls, measuring cups, nesting cups).
• Show excitement when older infants discover new uses for things (putting blocks in a box or pot).
• Keep containers filled with objects around and encourage filling and emptying the containers.
• Watch for and encourage older infants’ use of words, signs, and gestures, such as pointing and reaching to signal what they want.
June 2015 51

• Play hide-and-find games by placing a toy under a cloth or other cover for older infants to find.
Activity Suggestions
6-12 months
• Talk about familiar caregivers when they are not present.
• Recognize older infants' favorite books and read with them over and over again.
• Comment when older infants remember something belongs to you or someone else (“Yes, those are Luna’s shoes.”).
• Notice and be responsive to older infants’ words, gestures, laughs, gazes, and cries.
• Stay close by as older infants explore.
• Reassure older infants you will return when you need to leave, explaining where you are going and when you will be back.
• Introduce older infants to new people and allow them time to become comfortable.
• Respond quickly and sensitively to toddlers’ emotional and physical needs.
• Encourage sitting. Seat child between parents’ legs with hands bearing weight and engage child with talking, singing, toys. Encourage and support transitions from prone to all fours to sitting. Encourage crawling.
• Encourage child to lift hips during diaper change. Facilitate by holding thighs and bounce up and down.
• Hold child in standing and bounce to music.
• Encourage activities like going to a playground where the child can swing, slide, play in a sand box and water play.
• Place child in side sitting with picture book/toys in front to encourage weight bearing on one side while engaging other hand in activity.
• Stand the child between parents’ legs while parent is seated on a chair to encourage supported standing. Parent can sing songs, rhymes, and talk with the child.
• Arrange furniture to encourage pull to stand and cruising along furniture.
• Draw happy face on feet/ hands to encourage playing with hands, feet, fingers, and toes.
June 2015 52

• Pause during rhythmic bouncing or rocking game, wait for child to indicate for more, or ask “do you want more?” - then say “OK’ and resume game.
June 2015 53

Activity Suggestions
6-12 months
• Demonstrate action of toys, e.g.: banging blocks, spinning a top, winding a toy, and turning on a radio. Wait to see if child follows. Give plenty of time for the child to explore own methods. Express delight when child can imitate action. During playtime, offer second toy. Wait for child to reach with other hand.
• Play lots of social interaction games (peekaboo, pat-a-cake, I’m-going-to-get-you, etc.).
• Use a variety of facial expressions during interaction and to communicate feelings.
• Encourage visual tracking by using brightly colored and shiny toys, bringing them close to child’s face (8 inches away), and moving them side to side and up and down.
• Present in sitting, prone or on all fours objects like large knobbed puzzles, small cones, rice/bean bins, musical instruments, blocks, books, and differently textured toys. Play with noisy materials.
• Play with small edible objects, like cheerios, rice crispies, food-bananas, and soft macaroni.
What are your activity ideas?
June 2015 54

Now You Try:Activity analysis will allow you to determine which developmental areas are addressed when using a specific activity. Knowing this information is critical when explaining to parents and caregivers why you are suggesting certain strategies. Pick some of the activities from pages 49-51 and analyze them as demonstrated on pages 36-37. You can review your
analysis with your supervisor or another experienced EIS.
Activity Gross Motor
Fine Motor
Cognitive Social/Emotional Self Help Speech/ Language/ Communication
June 2015 55

June 2015 56

Analyze these activities even further by identifying some of the activities from the previous table addressing cognitive and social/emotional development and determine if they address the individual components of social/emotional and cognitive development. Examples of this analysis can be found on pages 38-40. You can review your analysis with your supervisor or another experienced EIS.
June 2015 57
Cognitive/Social-Emotional Activity Table
Activity WM IC CF ASA DS RSI
June 2015 58

Notes:
June 2015 59

Activity Suggestions
12-18 months
• Describe in simple language (to the toddler) how toddlers can use their bodies to make things move or change.
• Model how toddlers can do different activities with toys (throw a ball into a basket).
• Provide toys that require pushing, pulling, pouring, sorting, and matching.
• Accept knowing toddlers will need comfort items (blanket, favorite toy, pacifier, etc.) to bring with them on trips or visits to new places.
• Connect with toddlers at naptime or bath time.
• Respond with affection and care when approached by upset or hurt toddlers.
• Games: Creep through a maze of boxes; a cloth tunnel, on uneven surfaces (soft mattress on bed).
• Stand child with back support by a corner, let child hold large toy which requires 2 hands, like ball play.
• Practice independent standing –hold from behind and briefly let go; place child in standing with a low stool/coffee table in front and encourage activities with both hands (crumpling paper).
• Place child in kneeling with a low coffee table/stool in front of him/her and encourage bilateral activities such as making bubbles with an eggbeater in a bowl of soap solution.
June 2015 60

• Place child in half kneel in front of a coffee table and engage in two handed activities like putting coins through a small opening in a milk carton or piggy bank.
• Stoop and recover activities- Have child sit on a stool. Encourage him/her to lean down and pick up toys; repeat in kneel, half kneel and supported standing in front of furniture.
• Walk with bilateral support.
• Walk with unilateral support/independent walking.
• Utilize toys within a home; stacking toys, cups for pouring/ drinking, seriate baskets, spinning toys, push/pull toys, musical instruments, nesting baskets, in-set puzzles, piggy bank games.
• Find a toy when it’s being moved/hidden. Hide toy under napkin and say “look under your napkin!”
• Finger paints.
• Wind-up toys.
• Picture books with shapes, colors, objects, sizes and animals.
• Pointing games – pointing to communicate – picture books ask “where is the ____”, wait for child to point to the correct named picture.
• Play pointing games with friends, extended family and pets.
• Teach child to interpret pointing (“you are pointing to the juice – do you want to drink?”).
• Squeaking books.
• Give simple directions to encourage listening and following – include two objects (“Give me cup and spoon” and “Thank you for the napkin and cup”). Repeat request if child doesn’t follow immediately.
• Identify simple body parts (heads, knees, toes, tummy, etc.).
June 2015 61

What are your activity ideas?
June 2015 62

Now You Try:Activity analysis will allow you to determine which developmental areas are addressed when using a specific activity. Knowing this information is critical when explaining to parents and caregivers why you are suggesting certain strategies. Pick some of the activities from pages 56-57 and analyze them as demonstrated on pages 36-37. You can review your
analysis with your supervisor or another experienced EIS.
Activity Gross Motor
Fine Motor Cognitive Social/Emotional Self Help Speech/ Language/ Communication
June 2015 63

Analyze these activities even further by identifying some of the activities from the previous table addressing cognitive and social/emotional development and determine if they address the different components of social/emotional and cognitive development. Examples of this analysis can be found on pages 38-40. You can review your analysis with your supervisor or another experienced EIS.
June 2015 64
Cognitive/Social-Emotional Activity Table
Activity WM IC CF ASA DS RSI
June 2015 65

Notes:
June 2015 66

Activity Suggestions
18-24 months
• Use the terms girl, boy, man, woman as opportunities arise during daily activities. Gender discrimination at this age is based on clothing, hair, and name.
• Identify gender of characters in picture books. Ask “which child is the girl? Where is the boy?”
• Match identical pictures by using family members to match pictures.
• During story time, choose story books with large, colorful, uncomplicated pictures, few words on each page, simple plot and sequence of events, topics relevant to young children, and essential phrases repeated throughout the story (e.g. Brown Bear, Brown Bear).
• Describe the function of body parts when they are named during daily activity (Nose to smell flowers, eyes to see colors, ears to hear music).
• Identify objects by their functions. “The dog wants to play. What can he play with?” “What do we ______ with?” Questions to ask include “what do we write with? What do we make our hair with? What do we open a lock with?”
• Play sorting games by sorting fruits from clothes, or books from toys.
• Identify body parts in pictures.
• Play house.
• Label objects in the environment in writing.
• At appropriate points during daily activities, teach the child what is safe and what is unsafe.
• Provide child with a dirt or sand and water area with tools, such as cups, scoops, buckets, shovels, or sifters.
What are your activity ideas?
June 2015 67

Now You Try:Activity analysis will allow you to determine which developmental areas are addressed when using a specific activity. Knowing this information is critical when explaining to parents and caregivers why you are suggesting certain strategies. Pick some of the activities from page 62 and analyze them as demonstrated on pages 36-37. You can review your analysis with
your supervisor or another experienced EIS.
Activity Gross Motor
Fine Motor Cognitive Social/Emotional Self Help Speech/ Language/ Communication
June 2015 68

Analyze these activities even further by identifying some of the activities from the previous table addressing cognitive and social/emotional development and determine if they address the different components of social/emotional and cognitive development. Examples of this analysis can be found on pages 38-40. You can review your analysis with your supervisor or another experienced EIS.
June 2015 69

Cognitive/Social-Emotional Activity Table
Activity WM IC CF ASA DS RSI
June 2015 70

Notes:
June 2015 71

Activity Suggestions
24-30 monthsStay close by while toddlers begin to explore their surroundings and people, and as they begin to play or pretend play
• Ball games - roll back and forth, throw and catch, throw at a target, kick ball.
• Activities with bubbles providing the child with opportunities to blow bubbles.
• Create sculptures through play dough activities. Have child name creation.
• Read picture books with child pointing out specific letters and sounds.
• Interlock puzzles.
• Ride a tricycle.
• Walk up and down stairs providing support as needed.
• Use different media to provide opportunities for scribbling activities.
• Stack blocks.
• Build a tower and then let child knock down the tower.
• Make a train of animals or other objects within the house.
• Build a bridge/tunnel with couch cushions.
• Peg Board activities.
• Activities to encourage finger pointing like asking the child where objects are located from a distance.
• Encourage self-feeding.
• Allow child to help with easy household chores.
• Work on following more complex directions by giving the child 2-3 unrelated tasks.
• Provide opportunities for child to work on undressing.
• Toilet training (see pg. 20 for ideas).
• Open and close zippers and large buttons.
• Teach child how to cope with fears.
• Encourage child to feel proud of self and the work the child does.
June 2015 72

• Begin to label feelings.
• Engage in pretend play.
• Encourage using 4-5 word sentences.
• Include the pronouns me, mine, you etc. during communication with child.
• Provide consistent choices for child to make decisions.
• Add song and sorting to clean-up activities.
• Categorization – shape, color, size, animals.
• Create a sensory bin for sand and water play.
• Label names of rooms of the house.
• Match shapes and identify shapes.
• Increase attention while playing.
• Encourage asking simple questions.
• Answer all “what” and “why” questions asked by child.
• Encourage problem solving with tools with switches, buttons, knobs, and keys.
• Encourage sticking and pasting activities
• Provide opportunities to sort more complex (3-4) items
• String beads.
• Fold paper.
• Help create self-concept and identity through mirror play.
What are your activity ideas?
June 2015 73

Now You Try:Activity analysis will allow you to determine which developmental areas are addressed when using a specific activity. Knowing this information is critical when explaining to parents and caregivers why you are suggesting certain strategies. Pick some of the activities from pages 67-68 and analyze them as demonstrated on pages 36-37. You can review your
analysis with your supervisor or another experienced EIS.
Activity Gross Motor
Fine Motor Cognitive Social/Emotional Self Help Speech/ Language/ Communication
June 2015 74

Analyze these activities even further by identifying some of the activities from the previous table addressing cognitive and social/emotional development and determine if they address the different components of social/emotional and cognitive development. Examples of this analysis can be found on pages 38-40. You can review your analysis with your supervisor or another experienced EIS.
June 2015 75

Cognitive/Social-Emotional Activity Table
Activity WM IC CF ASA DS RSI
June 2015 76

Notes:
June 2015 77

Activity Suggestions
30-36 months
• Encourage increased use of verbs, adjectives and adverbs “bring me the blue and green balls,” “put the wet towel on the chair,” “roll the play dough to make it flat and round.”
• Sort by color.
• Sort by size “Big, bigger, biggest,” “long, longer, longest.”
• Ask what/where/why/who questions and wait for child’s answer.
• Help child learn the meaning of “No.”
• Set limits.
• Provide opportunities for child to make simple choices.• Understand the difference of one and many.
• Use describing words for size and attributes of objects (Is your shirt longer than mine or is it shorter?).
• Encourage labeling of and words for more complex emotions and feelings.
• Prompt various expressions.
• Interact with the child by reciting nursery rhymes and participating in storytelling together.
• Practice having child imitate five word sentences and learning opposites (the stove is hot, the ice is ____?).
• Involve child in activities which require hopping, jumping, climbing, running, riding a tricycle, using a playground, jungle gym and obstacle course regularly.
• Continue to encourage scribbling, copying simple shapes, puzzles, blocks, picture books, sand and water play.
• Provide household items for toddlers to sort into groups of similar colors, types, or shapes (socks, cups, plastic lids).
• Help toddlers mix colored water or finger paints and talk about the experience.
• Provide encouragement for trying activities and playing with or meeting new people.
What are your activity ideas?
June 2015 78

Now You Try:Activity analysis will allow you to determine which developmental areas are addressed when using a specific activity. Knowing this information is critical when explaining to parents and caregivers why you are suggesting certain strategies. Pick some of the activities from page 73 and analyze them as demonstrated on pages 36-37. You can review your analysis with
your supervisor or another experienced EIS.
Activity Gross Motor
Fine Motor Cognitive Social/Emotional Self Help Speech/ Language/ Communication
June 2015 79

Analyze these activities even further by identifying some of the activities from the previous table addressing cognitive and social/emotional development and determine if they address the different components of social/emotional and cognitive development. Examples of this analysis can be found on pages 38-40. You can review your analysis with your supervisor or another experienced EIS.
June 2015 80

Cognitive/Social-Emotional Activity Table
Activity WM IC CF ASA DS RSI
June 2015 81

Notes:
June 2015 82

Developmental Activities – Extension Do you need more resources about incorporating learning activities into daily routines? These extension activities provide more ideas for activities and strategies, offer information about providing routines based intervention and suggest tips for involving caregivers in the early intervention visit.
Resource Name
Link Activity Ideas/Strategies
Routines Based Intervention
Involving Caregiver
Early Learning Guidelines
http://earlylearningtexas.org/itelg.aspx
X X
Children’s Medical Services Training – Module 4, Lessons 2 (social emotional support)
http://www.cms-kids.com/providers/early_steps/training/itds/module4/lesson2_1.html
(Note that this is training for Florida’s Part C program. However, this information can be applied to the ECI program in Texas. You do not need to complete any of the activities that require you to fill out the Florida Part C forms.)
X X X
Children’s Medical Services Training – Module 4, Lesson 3 (motor focused activities)
http://www.cms-kids.com/providers/early_steps/training/itds/module4/lesson3_1.html
(Note that this is training for Florida’s Part C program. However, this information can be applied to the ECI program in Texas. You do not need to complete any of the activities that require you to fill out the Florida Part C forms.)
X X X
Children’s Medical Services Training – Module 4, Lesson 4 (language focused activities)
http://www.cms-kids.com/providers/early_steps/training/itds/module4/lesson4_1.html
(Note that this is training for Florida’s Part C program. However, this information can be applied to the ECI program in Texas. You do not need to complete any of the activities that require you to fill out the
X X X
June 2015 83

Florida Part C forms.)Children’s Medical Services Training - Module 4, Lesson 5 (cognitive focused activities)
http://www.cms-kids.com/providers/early_steps/training/itds/module4/lesson5_1.html
(Note that this is training for Florida’s Part C program. However, this information can be applied to the ECI program in Texas. You do not need to complete any of the activities that require you to fill out the Florida Part C forms.)
X X X
Delaware Early Learning Foundations
http://www.dhss.delaware.gov/dms/epqc/birth3/files/deinfant_0211.pdf
X X
Thinking Differently about Therapy Materials
http://tactics.fsu.edu/MIH/handouts/steps/training10s/set1/TherapyMaterials.pdf
X X
TaCTICS – Using Routines as Context for Intervention
http://tactics.fsu.edu/modules/modThree.html
X X X
TaCTICS – Involving Careprovider in Teaching and Learning
http://tactics.fsu.edu/modules/modFour.html
X X
FACETS – Identifying Family Activities and Routines – Conversation Starters
http://facets.lsi.ku.edu/sites/facets.drupal.ku.edu/files/docs/Module2/Identifyingfmilyroutines.pdf
X X X
FACETS – Identifying Child Care/Classroom Activities and Routines – Conversation Starters
http://facets.lsi.ku.edu/sites/facets.drupal.ku.edu/files/docs/Module2/Identifyingchildcarerout.pdf
X X X
More than Baby Talk: 10 Ways to Promote the
http://fpg.unc.edu/sites/fpg.unc.edu/files/
X
June 2015 84

Language and Communication Skills of Infants and Toddlers
resources/reports-and-policy-briefs/BabyTalk_WEB_2015.pdf
June 2015 85

HELP Activity Guide
This is available from the DSHS Audiovisual Library if you don’t have a copy at your program.http://www.dars.state.tx.us/ecis/resources/library.shtml
X X X
HELP at HomeActivity Sheets for Parents
This is available from the DSHS Audiovisual Library if you don’t have a copy at your program.http://www.dars.state.tx.us/ecis/resources/library.shtml
X X X
Teaching Your Child to Become Independent with Daily Routines
http://csefel.vanderbilt.edu/documents/teaching_routines.pdf
X X
Tips for Early Care and Education Providers - Tips and concepts to help you work with young children with Autism Spectrum Disorder
https://www.acf.hhs.gov/sites/default/files/ecd/508_tips_for_early_care_and_education_providers_april_2013.pdf
X X X
Young Children Develop in an Environment of Relationships(Responsive Caregiving)
http://developingchild.harvard.edu/index.php/resources/reports_and_working_papers/working_papers/wp1/
X
Making the MOST of Creativity in Activities for Young Children with Disabilities
http://www.naeyc.org/files/tyc/file/MitchellVol2No2NEXT.pdf
X
June 2015 86

Section 6 – Global Child Outcomes and Family Outcomes
Global Child Outcomes In Texas ECI, we use the term “outcomes” in two different ways. The most common use is in referring to individual IFSP outcomes. Those are the individualized goals an IFSP team creates for each child based on the developmental needs of the child and the priorities of the family. Developing individual IFSP outcomes is a team activity that is not discipline-specific. You can find more information on developing individual child outcomes in Making It Work, in the “IFSP Outcomes in a Box” training and the third webinar from the Quality Services Series, Comprehensive Needs Assessment and Developing Outcomes.
“Outcomes” is also used to refer to the three Global Child Outcomes. As an IFSP team member, you may have been involved in determining ratings for a child related to his/her developmental skills in three general skill areas or outcomes. Since 2009, each state receiving federal funding for early intervention services has been required to collect and report outcomes data to the Office of Special Education Programs (OSEP) at the US Department of Education.
But the Global Child Outcomes are not just about collecting data. They articulate meaningful, functional goals all parents have for their children, regardless of age or ability. An overarching purpose for all ECI services is helping children achieve the Global Child Outcomes.
The Three Global Child Outcomes are:1) Children will have positive social-emotional skills (including positive social
relationships).2) Children acquire and use knowledge and skills (including language and
communication skills).3) Children take appropriate action to meet their needs.
Examples of Outcome 1 (positive social-emotional skills) Kassidy (22 months) and Landon (24 months) sit next to each other and stack
blocks to build towers. Jonathan (2 months) calms down when his mother picks him up when he is
fussy. Lara (31 months) plays group games, like London Bridge, at child care.
Examples of Outcome 2 (acquiring and using knowledge and skills) Carter (7 months) babbles when his dad talks to him. Marisa (11 months) likes to drop snacks from her high chair and watch them fall.
June 2015 87

Jesse (30 months) can identify most body parts when you point to them.
Examples of Outcome 3 (acting appropriately to meet needs) Sophia (9 months) picks up and eats Cheerios independently. Connor (22 months) runs without falling. Aiden (27 months) tells his mom “poopy” when he needs a diaper change.
You probably noticed many of these skills cross domains. For instance, for Sophia to finger-feed independently, she is using skills in both the self-help and motor domains. When Carter babbles in response to his dad talking to him, he’s using both social and communication skills.
Regardless of the individual IFSP outcomes you’re working on with a child, they usually fall under one or more of the Three Global Child Outcomes. As a provider of SST, you are uniquely situated to help parents enhance a child’s abilities in all three of the Global Child Outcomes. As an EIS, you can use your knowledge of child development across domains to help the IFSP team assign accurate outcomes ratings, and to help other team members build activities that cross domains into the strategies they teach families. This workbook has provided numerous examples of working across domains to help children develop the functional skills they need.
June 2015 88
Family Outcomes Although most Early Intervention Specialists are aware of the Global Child Outcomes, they may not be as familiar with the Family Indicator, also known as Family Outcomes. Like the Global Child Outcomes, ratings on the Family Indicator for the State of Texas are reported annually to OSEP. The Indicator refers to the percentage of families who report ECI has helped them:
1) Know their rights.2) Effectively communicate their children’s needs.3) Help their children develop and grow.
In Texas, a sample of families who’ve been enrolled in ECI for at least six months receive a survey with 47 questions related to the three family outcomes. All members of a family’s ECI team, not just the assigned Service Coordinator, are responsible for helping the family achieve the three outcomes included in the Indicator. SST is a critical service for addressing the outcome, “Families help their child develop and learn.” As an EIS, one of your primary roles is showing families how they can incorporate activities that will enhance their child’s development into their daily lives. SST is more than teaching the child new skills; its true purpose is helping parents learn how to improve their child’s developmental trajectory.
Child Outcomes – Extension There is specific training about the global child outcomes located on the DARS ECI website: http://www.dars.state.tx.us/ecis/childoutcomes.shtml
June 2015 89

Section 7 – Transition and School ReadinessTransition planning not only includes an assessment of services a child might need when he/she turns 3, but also includes an assessment of the skills the child needs to be successful in the next service settings. The IFSP meeting which includes transition planning could also include developing new outcomes to address these skills.
Review this infographic about skills all children need to be “school ready”: http://www.zerotothree.org/public-policy/school-readiness-infographic.html . As you can see, many of the skills and strategies experts recommend for school readiness are embedded in all ECI services (relationships, everyday experiences, play).
Although all developmental areas need to be considered during transition planning, more and more experts are emphasizing the importance of social-emotional skills as a component of school readiness.
Social and behavioral competence in young children predicts their academic performance in the first grade over and above their cognitive skills and family backgrounds (Raver & Knitzer, 2002) (Read the full article at this link: http://csefel.vanderbilt.edu/resources/inftodd/mod4/4.3.pdf)
As a specialist in cognitive skills, social skills and challenging behavior, EISs are uniquely qualified to help prepare a child to be successful in school and other group settings. Many of the developmental activities addressed in previous chapters will support a child’s “school readiness”. In addition, the resources listed below provide guidance on addressing specific skills a child will need to thrive in his/her future settings.
Transitioning Between Activities: http://csefel.vanderbilt.edu/briefs/wwb4.pdfHandout: http://csefel.vanderbilt.edu/briefs/handout4.pdf
Helping Children Understand Classroom Routines and Schedules: http://csefel.vanderbilt.edu/briefs/wwb3.pdfHandout: http://csefel.vanderbilt.edu/briefs/wwb4.pdf
Helping Children Manage Their Own Behavior: http://csefel.vanderbilt.edu/briefs/wwb7.pdfHandout: http://csefel.vanderbilt.edu/briefs/handout7.pdf
Key Math Skills for School: http://www.zerotothree.org/child-development/early-development/supporting-early-math-skills.html#key
June 2015 90

Building Literacy Skills (24 – 36 months): http://main.zerotothree.org/site/PageServer?pagename=ter_par_2436_language_what
Section 8 – Documentation of SSTMost helping professionals, including Early Intervention Specialists, value their time spent providing services above all other work related activities. On the list of work related activities we don’t enjoy, documentation is frequently at the top of the list. It is not unusual to view documentation as a necessary evil and overlook the importance of having an accurate record of intervention. But, consider how important documentation is to you outside of ECI. If you are visiting a medical specialist, wouldn’t you want the medical record from your primary care physician to be complete, accurate and thorough? When purchasing a home, wouldn’t you want the inspection report, any disclosures about the home and the mortgage information to be thoroughly documented?
In this chapter, we will consider the importance of documentation, review documentation requirements, look at some routine quality checks, and complete practice exercises to help strengthen the documentation of the services you provide.
Why is documentation important? Let’s consider the varied reasons for record keeping. It can help to remember all of the potential readers of our documentation. Potential readers include the child’s primary care provider, other service providers, other team members, our supervisor, regulatory agencies, third party payers, and the child’s parents. Each of these readers expects a complete record adequately conveying the child’s functioning and what we did to address the child’s needs.
The various readers have different reasons for reading our documentation. Here’s a non-exhaustive list of some of the reasons we need to competently document what happened in the service event:
1. Continuity of care within ECI – After the child is enrolled in ECI, we have an obligation to provide services in a timely and efficient manner. This includes providing services as planned in the IFSP. To meet this responsibility it is critical for each of us to record what we did and what still needs to be done so a peer can step in should we be unable to perform services as planned.
2. Inform other service providers – Most of the children enrolled in ECI receive services from other providers. This includes the primary care
June 2015 91

physician or service agency making the referral as well as service providers who will be helping the child and family after they leave ECI. We have an ethical responsibility to provide a competent and professional description of the child’s functioning and the interventions we provide.
3. Inform program and agency management and supervision – Review of service documentation is one of the ways our work is supervised. Every progress note contains a wealth of information about the service provider. The documentation can reflect strengths as well as weaknesses in the professional’s ability to perform his/her job duties and to address the child’s and family’s needs.
4. Parents’ right to know and informed consent – Parents have the right to review records at any time. They have the right to know what we are doing and why. They have a right to know if progress is being made or if they are wasting their time and money.
5. Formal record of child’s functioning and response to services – Parents’ rights extend to having a complete record of service delivery and their child’s response to those services. In some cases our documentation may be used to verify the need for additional services and aid in service planning.
6. Formal record of performance of duty - In rare situations our documentation can be subpoenaed into a court of law. In these situations our documentation will stand as evidence we performed our duty competently and ethically.
7. Data collection and contract compliance – The agency that employs you receives federal and state money for the work you do. The ECI program must be able to present evidence the money was spent for its designed purpose. Usually this obligation includes being able to prove the services had the desired positive effect for the child and family.
8. Reimbursement – Third party payers (i.e. private and public insurance) pay for only those services which were provided. In addition, payment is made for only needed services when the documentation indicates the service is likely to obtain the desired positive effect for the child.
9. Professional pride and reputation – As stated in #3, every progress note contains information about the service provider as well as the child. The description of the service event and the completeness of the note
June 2015 92
convey your knowledge and skill as a provider, and your regard for the child and family. The professionalism of the note also conveys the value you place on your role in the child’s life.
June 2015 93

Exercise #1 - Getting to know the readers
Each of these readers may review documentation for different purposes. Select the best and primary reason from the column on the right that describes what a reader is looking for in a review:
Reader Answer Reviews documentation to1. Co-workers a. provide guidance and
feedback to improve the provider’s ability to perform his/her job duties.
2. Other current service providers
b. verify the ECI program and their employees and contractors have been good stewards of the public tax dollar by delivering effective, needed services.
3. Supervisor c. make sure you have done an adequate job in providing the service and accurately documented the service event.
4. Parent d. understand the child’s progress to date and develop appropriate services after the child leaves ECI.
5. Future service providers
e. ensure their provision of service is consistent with what has been done to date.
6. Lawyer/Judge/Jury f. verify the service provided was necessary.
7. State and federal governments
g. prove your role in an alleged illegal or unethical activity.
8. Third party payers h. ensure their involvement with the child and family neither duplicates nor contradicts the services provided by ECI.
9. Yourself i. understand what is happening to his/her child and make sure there is a
June 2015 94
benefit to the child.
June 2015 95

Our responsibilities as ethical and competent professionals include providing adequate documentation that can be used for all the purposes listed above, and the importance of documentation can’t be overemphasized. It is impossible to predict which reader and to what purpose the reader will request access to our documentation. Fortunately, a well written progress note will satisfy most readers and most purposes.
Minimum RequirementsValid documentation of the provision of SST must contain some minimum elements. The minimum elements for every ECI progress note are identified in state rule: Texas Administrative Code, Title 40 (40 TAC), Part 2, Chapter 108, Subchapter K, Rule §108.1111 (See 40 TAC §108.1111). Additionally, the minimum elements for every SST progress note are identified in state rule: 40 TAC, Part 2, Chapter 108, Subchapter E, Rule §108.501(f) (See 40 TAC §108.501).
Incomplete documentation can result in your agency having to return payment for a service; this is known as recoupment. It can also create the impression the provider is not qualified to provide the service or not adequately trained. Incomplete documentation can also result in the judgment the service was not provided according to state regulations or SST was not provided at all.
June 2015 96

Exercise #2 - Getting to know the rules
It’s critical to know the requirements for documentation. This exercise helps you learn the ECI rule. Go to the state rule (40 TAC §108.501) to complete this exercise.
1. Which three names must be documented?
2. Date of service and start time are required. Is the end or stop time required?
3. What does “method” refer to?
4. What are three techniques of engaging the parent or caregiver are spelled out in the rule?
5. What piece of information from the IFSP must be carried over into the progress note?
6. What about the child must be documented?
7. What about the service provider must be documented?
June 2015 97

Exercise #3 - Getting to know the required elementsIt may seem silly to worry about each of the individual required elements. The next exercise will help explain why each element is required. Use the following phrases (a through m) to fill in the blanks in the numbered paragraphs below.
a. Child’s nameb. ECI program namec. EIS’s named. Date and time of servicee. Length of timef. Place of serviceg. Method of service deliveryh. How we engaged the parent or caregiveri. IFSP outcome j. Child’s progress k. Other relevant information l. EIS’s signaturem. Credential as an EIS
1. The documented can be used to verify a service was actually provided. On a day to day basis this information enables the reader to organize the content of the record into a chronological history of the child’s development and services provided.
2. From a therapeutic perspective, there is a significant difference between services being provided individually or in a group format. Therefore the provision of group services requires additional justification and permissions to be documented in the child’s record. Reimbursement for group services is usually less per child than individual one-on-one services. Including the tells the reader whether individual or group services were provided.
3. The primary purpose of intervention is to assist the family as they help their child meet his or her developmental outcomes. Our sessions are planned, modified and delivered in response to child change (or lack of change), therefore the must be documented. Information about how the child is responding to intervention is necessary for services to continue to be effective. Additionally, funding sources expect to see documentation of the effect of services on the child’s development.
June 2015 98

4. Including the in the progress notes tells the reader the purpose of the service event. Without this information it can be impossible for the reader to determine the need for the service event. If there is no need for the service event then a third party payers has no reason to pay for the service. Similarly, if there is no need for the service, parents have no reason to incorporate the intervention into their daily routines or keep their child enrolled in services.
5. The reader of the child’s record may not have access to the entire record but may instead see single pieces of the record such as an isolated progress note. Because the progress note is separated from the rest of the chart the must be on each progress note.
6. The state rules restrict the provision of SST to individuals who have completed required training which establishes them as an expert in early childhood development. Proof that an adequately trained professional provided the service is shown when we include the in the progress note. Without this information it can be argued the person providing the service was incompetent.
7. Including the lets the reader know who is ultimately responsible for the service. This information lets parents know who to contact if they have any concerns. After the child leaves ECI, this information will help the family and future service providers know who to contact to obtain information about the child’s functioning, progress, and interventions used while in ECI.
8. The on the progress note serves the same function as a signature does on any document: The person signing is verifying the content of the document is true and accurate. When reimbursement for services is involved, the person signing is confirming they provided the service as described at the date and time indicated.
9. A distinguishing characteristic of ECI services is the majority of services are provided in the child’s natural environment. Identifying the lets the reader know the services were provided in accordance with the ECI model. This information is also entered into TKIDS as the DARS ECI contract requires 98% of delivered services to occur in the natural environment. The payment of some services may vary by service location as well. For example the reimbursement for services in the home may be higher than services provided in a clinic.
June 2015 99

10.The ECI approach to service delivery is holistic. This means the assessment of the child’s and family’s needs and the interventions provided address all aspects of the child’s functioning and life. The ECI approach also uses an interdisciplinary team. This means individual service providers work together to address all aspects of the child’s functioning and life. Documentation of proves we are addressing the whole child and are making effort to share this information with the rest of the team.
11.ECI programs must be able to justify the time billed to third party payers and be able to demonstrate efficient use of contract funds. For these reasons we include the in the progress note. Information about the time spent providing SST is also used by the state to determine the rate of reimbursement for SST. Duration of service provision may also be used to determine caseloads and inform supervision.
12.The component that differentiates ECI from other services is the instruction to the parent and caregivers. Describing tells the reader we did provide the services according to the ECI model and rules. Failure to include this information may result in the recoupment of payment as it may be judged an ECI service was not provided. In addition, the omission of this information conveys to the parent their involvement is unimportant.
13.Documenting the tells the reader who provided the service. This information is necessary to verify the service was actually provided. This information also tells the reader who is responsible for all of the required elements and content of the progress note.
June 2015 100

What should progress notes look like? After reviewing all of the preceding material, you might be thinking there’s not enough time to document completely or to include all these requirements in every note you write. None of the requirements can be ignored, so we have to find a way to include everything.
Straightforward requirements - Many of the requirements can be pre-printed on the form, or filled in prior to your visit, including the date and place of service, the method, child’s name, and the ECI program name. The IFSP outcome you will be working on is included, but does not have to be exact – an accurate abbreviation will work.
Engagement of the Caregiver - Your engagement of the parent or caregiver is the most important component of a SST session, and should be documented as such. Parent training and instruction is what sets ECI apart from other providers, and it is the reason funding sources pay for ECI services as separate and distinct from other therapeutic services to children. The definition of SST specifically includes training and guidance of caregivers, so without good documentation of this component, SST is incomplete. There are several things to consider as we document our work with parents:
Caregiver as learner - The primary learner during an ECI visit is the caregiver, and this should be reflected in your progress note. What did you teach? What feedback did you provide? What questions did you answer? How did you coach?
Service delivery triad – The focus of each SST session is on ways the caregiver can interact with the child to support the child’s development and achievement of outcomes. The EIS works, not with the child, but with the child and caregiver together.
Materials in home – Critical to the success of ECI services is the caregiver’s ability to implement interventions when you are not there. Therefore the interventions you demonstrate need to use materials that exist in the natural environment. How did you assist the family to use the objects, materials and toys to which they have ready access, either in their home or in the community?
Familiar routines for every day learning – Because the caregiver will implement the strategies you are teaching in the child’s daily life, document how you discussed applicable routines with the parent.
June 2015 101

Child responses and progress - The engagement of the caregiver is how we ensure maximum learning and development for children enrolled in ECI. Infants and toddlers learn best through everyday experiences and interactions with familiar people in familiar contexts. The enrolled child is the target of intervention, and so we must also document the child’s responses and progress. This means documenting:
the child’s response to the strategies and techniques being used (not the child’s response to you as a provider.);
your expert observations of any progress, or lack of progress toward the stated outcome;
parent reports about how the child has been responding to the intervention in daily routines and activities (when you are not there); and
how you adjust strategies and techniques based on the child’s response and progress or lack of progress.
Delivery of a skilled, professional service - Early intervention providers understand play is the work of children, and play can be a therapeutic activity for a child. Your documentation needs to reflect this understanding by describing:
the purpose, as related to the stated outcome, of play activities; how you applied your professional knowledge, expertise and skill; and what you did during the session.
June 2015 102

Since every reader of the child’s record is not an early intervention provider, the responsibility falls on you to provide evidence of your application of skilled professional knowledge and expertise in early childhood development. Words like, “observed,” and “encouraged,” have little meaning unless you provide a description of how your observations and encouragement relate to the child’s outcomes. The following table is a collection of examples to help illustrate the difference between unskilled and skilled activities.
Unskilled activities Skilled activitiesObserving child and parent/caregiver’s actions without feedback
Continuously assessing the child’s and parent/caregiver’s performance
Making vague or relative comments about performance
Providing objective data to show progress such as accuracy, speed, frequency, and independence
Practicing actions that do not vary in complexity or level of cueing
Adjusting interventions to help the child and family achieve outcomes
Playing without explaining the therapeutic value of the play
Providing rationale for how the activity relates to the outcome
Encouraging without including a description of the technique used
Using expertise in child development and behavior to increase the child’s motivation and success
Reminding without assessing or addressing the possible barriers to implementation
Sharing expertise in child development and behavior with parent/caregiver to increase the parent/caregiver’s motivation and success
June 2015 103
Exercise #4 – Getting to know the contents of a progress noteIt’s important to both know the required elements, and to know how to functionally document them in a progress note. This activity will provide examples of how to document the required elements. The following are examples of the above mentioned elements of a good progress note. Which activity (1-11) matches which element (a-k)
Activity Your Answer Element1. I showed Mattie how to use a rolled up bath towel to support Trevor’s back.
a. Caregiver as learner
2. Worked with Binh on better positioning for Nguyen in his highchair. Helped her choose a large book that she wrapped in a towel to put in the seat to elevate him for better hand use. With the towel roll placed around his hips, he was able to grasp objects with both hands.
b. Service delivery triad
3. Kayla agreed diaper changing time would be the best opportunity to work on the leg stretches the OT showed her.
c. Materials in home
4. Aston played with his blocks, placing them as directed by Ashley, followed by applause and praise from Ashley when he did as requested.
d. Familiar routines for everyday learning
5. I noticed Lela was placing Carlos’s toys too far out for him to be interested in crawling toward the toy. I demonstrated how to gauge how close to
e. Return demonstration
June 2015 104

Activity Your Answer Elementplace the toy by watching Carlos’s expression.
6. Texemma stated the older children are answering her questions to Dylan so she’s having a difficult time figuring out if he’s hearing her let alone understanding and responding to her questions.
f. Child’s response to intervention
7. I demonstrated how to drop objects into a container to make a “bang.” Nina tried it several times with Pia and agreed that approach increased Pia’s interest in releasing objects on command.
g. Parent’s report of how child is responding to interventions
8. Kelly responded more rapidly to tapping the picture in the book than to verbal prompts.
h. Observations of any progress or lack of progress
9. While Charlie is demonstrating more effective grasping and releasing, he is now throwing things rather than placing them.
i. Adjustment of interventions in response to progress or lack of progress
10. I demonstrated blocking Deon’s upward arm movement at the same time I asked him to give me his toy car to reduce his ability to throw instead of give.
j. Purpose of play
11. Kim loves it when Loc sings to her. Coached Loc to
k. Delivery of a skilled service
June 2015 105

Activity Your Answer Elementpause for a few seconds when singing “Old MacDonald” to see if Kim would make the animal sound. Loc tried it, but his pause was a little too short. He tried again with a longer pause, and Kim said, “mmm” for the cow.
June 2015 106

SST documentation should contain the following five components:
1. Coaching and instructions to the family or caregiver,2. Attention to how activities apply to child and family routines,3. Modeling intervention techniques within everyday learning opportunities,4. Evidence of a skilled professional service, and 5. The child’s response and progress.
The following sample of an SST progress note demonstrates how these five pieces of information can come together in a single progress note. The sample note is separated line by line, but would be written as a continuous narrative. You can see this note contains the discussed components but is still fairly short. The documentation clearly shows the EIS is always thinking about, and helping the parent understand, the therapeutic purposes of the activities.
Codes for note:
coaching and instructions to the family or caregiver
attention to how activities apply to child and family routines
modeling intervention techniques within everyday learning opportunities
skilled, professional service
child’s response and progress
June 2015 107

SST Session
Date 5/30/13
Name Rocky
Current Status; Changes since last visit
Pointing and gesturing more to try to tell them what he wants, but hasn’t used any sign or words. Pointed toward toy area and vocalized when I arrived to indicate his desire to play. Rpt - tantrums when they didn’t understand him, 5-6 last weeks.
IFSP Outcomes worked on
use 5 single words to tell us what he wants instead of tantrums
Activities with caregiver to address outcomes
Arrived during afternoon playtime.Dad and Mom present
I reviewed benefits of signing to encourage communication and words.
Dad and Rocky selected nesting cups from their toys.
Taught Dad sign for “cup”.
Demonstrated for Dad then he assisted Rocky hand-over-hand to sign “cup” while Mom held the cups.
After three turns, Rocky signed and said “up” to ask for a cup.
Switched to Rocky’s favorite puzzle. Dad held puzzle pieces, Mom physically assisted Rocky to sign “more”. Explained reducing assistance to prompts/modeling, and taught signs for puzzle pieces fish, dog, cat and bird which they then practiced while playing. Suggested use signs often to refer to family dog and cat.
Emphasized importance of always saying the word clearly with sign.
Rocky completed puzzles, signed “more” with decreased physical prompts.
Tantrums this week were usually at meal or snack time.
Reminded Dad - provide choices for snacks
You can encourage him to indicate choice by using sign or gesture; but don’t withhold choices to point of frustration.
Reviewed and demonstrated the signs for eat, drink, cracker, and apple. Agreed I will come during snack time next week and we will work on that routine.
Reminders; things to practice till our next visit
1) Use signs while playing with cups and puzzles.2) Offer choices at snack time, and model the signs eat, drink, cracker and apple.3) Frequent use of signs “dog” and “cat”. Always say the word, and encourage imitation.
June 2015 108

Another example of an SST progress noteSST Session
Date 5/30/13
Name Ryan
Current Status; Changes since last visit
Phyllis worked on attention span with books, but he’s uninterested. Sister tried rolling car – he picks up, spins wheels won’t give it back. Hasn’t said “mama” but “aa-aa-aa” noises to get attention, instead of grabbing or screaming. Screaming still main way of getting attention.
IFSP Outcomes worked on
Turn-taking; increase attention span and joint attention; say “Mama” to get Mom’s (Phyllis) attention.
Activities with caregiver to address outcomes
Phyllis borrowed library books with the word “mama” that SLP recommended. She read to Ryan. I showed how to draw attention back to a picture with exaggerated/ excited speech and using gestures and movements. Suggested books with interactivity, like flaps or tabs, to help hold attention. She practiced with Lift the Flap book and he attended for about a minute.
Tried ball instead of a car for turn-taking. Demonstrated hand-over-hand assistance to roll the ball back for turn-taking. We switched places and she used the hand-over-hand technique. Also demonstrated taking turns dropping the ball into a laundry basket. Will practice reciprocal ball play in the afternoon with sister.
I reminded Mom saying “aa-aa-aa” can be interpreted as purposeful communication. When he makes the sound, she can say, “You want mama? Here I am” and give him some attention. Reminded Mom ignoring screaming and rewarding purposeful sounds will reinforce appropriate sound development.
Suggested 1) move most toys into closet to decrease distraction 2) move other toys to shelf out of reach to stimulate request with sounds or gestures. Discussed not using cars as a reward, but instead can use physical play he enjoys, like bouncing on knee facing her.
Reminders; things to practice till our next visit
Continue with book techniques practiced today. Rearrange toys as discussed. Ball play with sister in afternoons.
There is no required format for service documentation and the ECI contractor may use any format that works best for their staff. The world’s best format will not work, however, if we don’t use the prompts provided on the form.
June 2015 109

What sort of things should l avoid in my documentation?
A. Play with no purpose – Professionals in the field of early intervention know the value of play. Bubble blowing, reading books, playing in sand – you could probably list a hundred fun, toddler activities that support development. Remember play is a means to an end, and has a developmental or therapeutic purpose in SST. The purpose needs to be clearly indicated in your notes.
Poorly documented Well documented
Jack enjoyed looking at Spot lift-the-flap-book.
Explained and demonstrated to Inez (mom) how to use single words when looking at a book with Jack. She practiced with their Spot lift-the-flap book.
B. Use of the term “encouraged” - The word “encourage” means to inspire or cheer. It can indicate a child is developmentally able to do something, but just needs to be coaxed to do it. You may be teaching a parent to provide positive reinforcement, or teaching how to provide learning opportunities. Use of the term “encouraged” alone does not convey a needed service was provided. An acceptable use of the term is related to a technique to encourage a behavior in the child.
Poorly documented Well documented
Encouraged Jack to pull up on the sofa. Prompted Terrell (dad) to remove sofa cushions for a lower surface, and to place favorite toy on sofa to encourage Jack to
June 2015 110
Question:I was told Medicaid prohibits two different services (e.g., Case Management and Skills Training) being documented in the same progress note even though there is a separate billing line for each service, clear demarcation in the narrative separating the services, and each service met documentation guidelines.
DARS Response:There is no prohibition to having two services documented on one sheet of paper. The documentation of each service event must include all of the required elements per applicable state and federal laws and regulations, including signature with the credentials required for each service (e.g., “Service Coordinator” for the case management and “EIS” for the SST). The content of each progress note should clearly identify the service provided and therefore make it easy to determine which line on the billing strip applies to that section of the document. Two services combined in one narrative make it difficult for the auditor to verify all of the required elements per service are present and the correct amount of time per service was billed. This inherent difficulty is amplified when the two services are poorly documented (e.g., it is impossible to discern the case management activity from the SST activity).

pull to stand. C. Use of the generic “we” – It’s important your progress notes describe what you did,
as a professional, during the session. It is equally important you reflect what the parent practiced or demonstrated.
Poorly documented Well documented
We named farm animals while Emma put them in a puzzle.
I explained and modeled naming pieces as Emma placed them in puzzle. Tanis (mom) then practiced in play with another favorite puzzle.
D. SST as “mini-therapy” – EISs are not therapy assistants. SST is a separate and distinct service from any therapy that may be provided, and it is important SST progress notes reflect this distinction.
Outcome Therapy note SST
Walking all over the house PT teaches the parent exercises to strengthen legs and core muscles (details of teaching and demonstrating listed).
Suggested to Laswayn (mom) ways to modify living room to allow child to move around freely, and to encourage cruising. (appropriate use of term “encourage”)
Self-Feeding of finger foods OT teaches the parent techniques for playing with play dough to strengthen hands and fingers, and improve eye-hand coordination.
Brainstorms with parent to identify favorite foods appropriate for finger feeding. Assists parent with positioning and presentation of foods in high chair.
Use of words to communicate
SLP teaches parent how to isolate and emphasize specific early developing speech sounds when looking at books with the child.
Coaches parent on naming objects in the child’s immediate environment using single words, clear speech, and drawing child’s attention to the object.
June 2015 111

E. Only strengths – It is important to build on a child’s strengths, and to help parents identify and value the strengths of their child. Your progress notes must also describe increments of child progress, and the steps you are taking to build on strengths to correct deficits and address needs.
Poorly documented Well documented
Trig can sit up on his own. Will continue working on trunk strength.
Trig can sit up on his own but has difficulty staying upright for more than a few seconds. Showed mom how to use cushions from the sofa for added support as we work toward strengthening his back muscles.
F. Narrative reflects only what the child did – Child progress and the child’s responses to intervention are an important component of documenting services. Too often, however, progress notes consist only of a description of what the child did during a session, leaving out the coaching and instructions to the family or caregiver, attention to family routines and the skilled, professional service.
Poorly documented Well documented
Bella did a good job pasting flowers. Robin (mom) practiced holding the pieces of flower (petal, stem, leaf) next to her mouth as she said the word three times before handing the piece to Bella for pasting.
Bella joined in singing The Farmer in the Dell. She really enjoyed making the animal sounds.
I suggested Robin wait to see if Bella would offer an animal or initiate the sound when singing the Farmer in the Dell. I demonstrated starting the animal sound but letting Bella finish it before joining back in. Bella really seemed to enjoy trying to make the animal noise before Robin did.
G. Instructions to caregiver appear only in “Things to do till our next visit” section - Instructions, coaching, discussion and problem solving with caregivers are the most important components of SST (and all ECI services). Your progress notes should reflect this emphasis throughout the session.
H. Wrong credential - remember; only an EIS is a qualified, authorized provider of SST. If you sign your progress note as Service Coordinator, or Teacher, or Social Worker or any other title, the service has been provided by someone who is not qualified to provide the service.
June 2015 112

I. Illegible – An illegible entry is the same as no entry at all. Illegible notes are very frustrating for all readers, be they a co-worker, supervisor, or parent. An auditor reads service documentation to verify services were provided as billed and/or in compliance with rule. If the note is illegible the auditor will not be able to affirm the appropriateness of the services. This can result in a variety of different consequences including recoupment of funds. If your handwriting is illegible to most readers and beyond your control to correct, please ask your supervisor about the possibility of using an accommodation such as transcription services or access to a computer. Some options include:
Dragon Dictation (Android, Blackberry, iPhone)http://www.nuancemobilelife.com/apps/dragon-dictation
Vlingo (Android)http://www.vlingo.com/apps/android
Quick Voice to Text (iPhone)https://itunes.apple.com/us/app/quickvoice2text-email-pro/id285877935
Please remember text and email are not secured transmissions. Never text or email a child or family’s name or other identifying information.
June 2015 113

Exercise #5 – Getting to know when there’s room for improvementThis activity will help you become a documentation expert by providing practice with both reviewing and correcting progress notes. The following are real-life progress notes (names have been changed). Identify problems with each note by answering these questions:
1. Does the note address an identified need and outcome?2. Does the note follow the adult learner and service delivery triad?3. Does the note provide documentation that the service provider is using
daily routines and materials in the home?4. Does the note provide documentation of the child’s response to
intervention?5. Is the application of professional knowledge clear?
Then try your hand at improving the progress note.
Note #1Toby was seen today at home with mom and brother for scheduled SST session. Toby is doing very well. Mom reports Toby is trying harder to say what he wants. In the session I heard him say: baby, hi, puppy. Mom encourages him to repeat sounds and single words. While playing we worked on:
- Imitation of sounds, movements, single words, and simple phrases.- Encourage her to repeat what we would do.- Looked at books and pointing and naming pictures.- Finger plays and Toby would try to do movements.
Toby did great! Toby had a good session. Now You Try
June 2015 114
Note #21. IFSP Outcomes (specify) Addressed:Reduce tantrums, use signs, verbalize2. What has happened since last visit?Nadir has continued to respond to sounds over the last week and is recognizing signs as well3. What did we observe/try today? (specify actions/engagement of all participants in visit)Nadir and class are on their way to the gym to play. Nadir holds Alberta’s hand and she reports he has been giving her a lot of hugs this week after seeming mad at her last week. She looks at him while she talks to EIS and he smiles at her and wants to be picked up. Once In the gym he is ready to run and has to be told and signed to sit back down while the teachers get the toys out. He goes on his own to sit back down 3 times when he is told and shown the sign to sit. Once able to play EIS and teacher work on the sign for ball, good, thank you, please, and sorry. He is paying more attention when shown signs and when his back was towards me, EIS called his name loudly and he turned. Teacher continues to struggle to keep his cochlear on at times since it is so easy for him to grab it and pull it off, but she consistently puts it back on correctly so he can benefit from it. In the classroom she continues to work on signs with him and the other children as they look at books.4. What might we do different/continue? What will occur between visits?Continue to sign to him and speak to him where he can dearly see your face and lips. Make sure his cochlear is on throughout the day and tell him "no" when he grabs it. If he has a tantrum, redirect him to an appropriate activity or ignore it.Now You Try
June 2015 115

Note #3Outcomes addressed:Following directions (goal #9)What’s happened since last visit (progress reported by family, concerns):Salme is very inconsistent with following directions.Summary of activities worked on today (include how those present participated and specific progress noted by provider):Met at daycare for scheduled SST visit with staff. Salme and other children present. Staff watched provider as I played with Salme, giving her simple directions paired with verbal and visual cues. Discussed with staff how this helps cue Salme to what you are asking her to do. Modeled for staff how to use hand over hand assistance to guide Salme through direction. Staff then practiced above techniques with Salme while this worker observed and coached. Activities to work on before the next visit:*Give Salme verbal and visual cues when giving her directions. *Use hand over hand assistance to guide Salme through the direction. Now You Try
June 2015 116

Note #4Others present:Teachers, kidsSince our last visit:Su-bin’s attention to task is improvingGoal(s) worked on today:Gross motor, speechActivities:Met with Su-bin at Head Start, class was outside playing in the leaves! Teacher was grabbing bunches and throwing them up in the air and kids were imitating. Su-bin threw his just above his shoulders so I helped him reach higher to extend range. Encouraged him to stay involved in class activity. We ran through leaves and all kids participated (class of 3 today!). Encouraged Su-bin to run and try to keep up – he was last but was enjoying activity. Then he walked to nearby fence and stooped and picked up leaves and poked them through the chain links. He repeated “whee” and “whoa” when throwing leaves. How can this be a part of your family’s daily weekly activities? Encourage Su-bin to repeat words to describe activity.Now You Try
June 2015 117

Note #5Changes since last visit:Grandmother reports he is starting to take 1-2 steps on his own now.Worked toward IFSP outcome(s) of:To eat table foods.Today’s activities/observations and parent/caregiver participation:Today Trevor participated in meal time. Observed Trevor kept calling out “mama” and attempted to imitate some words “papa.” Discussed using signs to meal time to help Trevor communicate “papa, more, drink, and finished.” Trevor began to wave when he heard EIS say “bye bye” as she took turns having a conversation in hi language. Trevor practiced bringing spoon to his mouth on his own. Discussed always giving him a spoon at meal times to continue practice bringing spoon to his mouth.Child’s progress and recommended activities:1. Use signs to help Trevor communicate what he wants (more, food, drink,
and finished)2. Give him an extra spoon while feeding him to practice bringing his spoon
to his mouth.3. Name food items as you offer choices for Trevor to pick and recognize by
name.Now You Try
June 2015 118

Note #6IFSP Outcomes (specify) Addressed:For Mica to become comfortable with EIS being in Mica’s home so EIS can instruct Mom on strategies to use to increase Mica’s attention span. Mom wants Mica’s attention span and joint attention to increase so he will be able to stay focused on one activity for at least 10 to 15 minutes during playtime. Mica will request his want/needs with words/word approximations during snack time and play time 5 times a day or 7 consecutive days. What has happened since last visit?Mom reports Mica is interested in playing with her when others (strangers) are not around. However, he continued to cling to her when ST came for therapy. Mom reported Mica did a first this week. He and Mom went to a playground at the mall. Mom said Mica played with the other children some but mostly ran around doing his own thing. However, Mom did report she saw Mica play “Duck Duck” at daycare this week. This was interacting with other children. What did we observe/try today? (specify actions/engagement of all participants in visit)Today EIS instructed Mom we would sit on the floor with Mica. Mom presented Mica with puzzles. At first Mica would identify some of the puzzle pieces and try to put them in the correct opening. Mica even brought a puzzle over to EIS. This was the first time he approached EIS. Some of the time Mica wanted to throw the puzzle pieces. However, after using some distraction, Mica started playing with the puzzle pieces in a different way. He turned them face down and moved them around the room. He had his own plan. We made progress today because the second half of the visit Mica seemed to be OK that EIS was there. What might we do different/continue? What will occur between visits?When playing with Mica, help him recognize when a picture is upside down. Help Mica understand the concept of “upside down” with objects before trying pictures. Left a handout for family: Right Side Up.”Now You Try
June 2015 119

Note #7Outcome: Sign needs/wants Arrived at childcare center for snack time. I sat beside Hector at the table with Sally (tchr) and 4 other kids. Sally has started giving the children small portions of snack foods instead of the whole thing at once as we discussed last week. Demonstrated pausing to allow Hector time to request. I assisted Hector (hand over hand) to sign “cookie” for another piece, and to sign “drink” for more juice. He enjoyed the signs, and by the end of snack, he required only minimal prompt for “drink”. Use of signs may help decrease Hector’s frustration about communication and help decrease tantrums. Class had “free play” time during diaper changes. I modeled using single words and two signs (truck and baby) to describe Hector’s play. Modeled pausing to allow Hector time to imitate. Explained to Sally these techniques allow Hector to learn more vocabulary, and is a start for reciprocal communication that will decrease tantrums. Now You Try
June 2015 120

Note #8Current Status and changes since last visit: Pointing and gesturing more to try to tell them what he wants. Had a few tantrums when they didn’t understand him. IFSP Outcome worked on: To say words and have fewer tantrumsActivities with caregiver to address outcomesArrived during afternoon playtime. Dad and Mom present, reviewed benefits of signing to encourage communication and words. Dad and Alex selected nesting cups from their toys. Showed Dad how to sign “cup.” He assisted Alex hand-over-hand to sign “cup” while Mom held the cups. After three turns, Alex signed and said “up” to ask for a cup! Switched to Alex’s favorite puzzle. Dad held puzzle pieces; Mom physically assisted Alex to sign “more.” Explained reducing assistance to prompts/modeling, and taught them signs for puzzle pieces fish, dog, cat and bird. Suggested use signs often to refer to pet dog and cat. Emphasized importance of always saying the word clearly with sign.Tantrums this week usually at meal or snack time. Suggested providing choices for snacks, encourage him to indicate choice by using sign or gesture. Discussed some specifics, reviewed the signs for eat, drink, cracker, and apple. Agreed I will come during snack time next week and we will work on that routine.Reminders about what to practice:
1. Use signs while playing with cups and puzzles. 2. Offer choices at snack time, and model the signs eat, drink, cracker and
apple. 3. Frequent use of signs “dog” and “cat.” Always say the word, and
encourage imitation. Now You Try
June 2015 121
Note #9Outcome:To crawl Kim was in her high chair when EIS arrived. She was happy and smiling. We played peek-a-boo for a short time to get her comfortable with EIS. Suong put a blanket down and EIS pulled over the cube toy to play with. Suong set her on her bottom and EIS placed the toys around her. She reached out for the blocks and pivoted on her tummy. When she reached out for the cube which was placed quite aways away she tried to go to her tummy but her leg got caught up under her so EIS showed Suong how to gently pull her leg just a little bit under her and then Kim did the rest of the work and she went to all fours. She immediately went down on her tummy but the work on her arms was there. She reached for the blocks and mom helped her place them where they go and turned on some music. She got very excited and started to dance. When EIS attempted to fold her legs under her to show mom how to help her stay that way, Kim got upset. Suong calmed her down and we tried floor time again after a little bit. Now You Try
June 2015 122

As seen in some of these examples, it is not possible to adequately document a service with a few sentences hurriedly written. Your job duties include taking the time necessary to adequately document what you have done.
A parent can refer to a well written progress note to guide their intervention with the child in routines. In the days following a session, the note can remind the parent of how to implement strategies and activities. It can help the parent remember what to look for in the child’s responses, and the reasons for the activities.
Auditors use the content of a progress note to make a judgment about how much should have been billed for a service. It seems clear that for an hour of service provision you will need to write more than five or six lines. Descriptions not related to service provision such as, “Kim was in her high chair when EIS arrived. She was happy and smiling,” or are vague such as, “Toby did great! Toby had a good session,” do not describe the service provided nor the effectiveness of the service provided.
Another truth that becomes self-evident in these examples is how important it is to have quality SMART outcomes. If the outcome is not measurable it is not possible to document what interventions are or are not effective over time. It is difficult to determine how SST can be of assistance with vague outcomes such as “eat table foods.” The first step you can take to ensuring the quality of your service documentation is to assist the IFSP team in writing quality outcomes.
What are some routine checks?As indicated earlier in this chapter, there are a number of oversight entities who may review your documentation. To avoid negative findings in a review or audit you should routinely double check your documentation to make sure your documentation is adequate. The following is a non-exhaustive list of things you should be checking.
1. Service is on the IFSP.2. The note is legible to the average person.3. All required documentation elements are present.4. Signature includes the credential of EIS.5. IFSP outcome is referenced and content of note addresses the identified
outcome.6. Content of note addresses coaching, training, modeling, and instructing of
caregiver.7. Content of note indicates application of provider’s professional expertise in
early childhood intervention.8. Language used is understandable to the layperson (if technical language
is used, a non-jargon explanation is included).
June 2015 123

Using the information in this section of the workbook, create a checklist to use on your progress notes. Reviewing documentation you’ve already completed will help you identify areas needing improvement. You may want to get together with your supervisor and see if your supervisor has identified areas you may want to strengthen in your documentation. Tailoring your checklist to address areas for your professional development will create a more valuable tool to you.
For example, if you’re good at describing the instruction provided to the caregiver but sometimes you forget to ask the caregiver how they did with the interventions when you weren’t there, you’ll probably want to be sure to include something like, “Content includes caregiver report on using intervention” on your checklist. Another example would be, “Content includes needs” to help remind you to address the child’s strengths and needs.
June 2015 124

Check Your Answers for the Documentation Exercises
Getting to Know the Readers (page 83)1. e2. h3. a4. i5. d6. g7. b8. f9. c
Getting to Know the Rules (page 85)1. Child, ECI contractor, EIS2. No. Length of time is required. The ECI program can choose to use start and stop
time together to convey length of time. 3. Individual or group. 4. Coaching, discussing, and modeling.5. The outcome goal that is being addressed6. The child’s progress toward the IFSP outcome and any relevant new information.7. Name, title as EIS, signature.
Getting to Know the Required Elements (page 86-88)1. d2. g3. j4. i5. a6. m7. b8. l9. f10. k11. e12. h13. c
June 2015 125

Getting to Know the Contents of a Progress Note (page 92-93)1. c2. b3. d4. j5. a6. g7. e8. f9. h10. k11. i
Getting to know when there’s room for improvement (page 102-110)
Note #1Addresses an identified need and outcome? There is no indication of the intent of this
session. There is no identified need for this service event.
Adult learner and service delivery triad? There is no evidence of the EIS coaching or modeling. “Mom encourages him” does not convey whether or not the mother is using the techniques demonstrated to her. We do not know if the techniques used by the mother were effective or if they need to be modified.
Daily routines and materials in home? While the note mentions things that probably existed in the home (books, finger puppets) there is no indication interventions are being incorporated into daily routines. While the brother is mentioned as being in attendance, there is no indication the brother was incorporated into the session.
Child response to intervention? Comments the child did well or had a good session do not convey any information. The note indicates words Toby said but there is no indication if they spontaneously occurred or were the direct responses to the interventions being used.
Application of professional knowledge? We do not know what techniques the EIS demonstrated to facilitate Toby’s imitation of sounds, movements, single words, and simple phrases. The EIS did not provide techniques that will encourage Toby to describe what his mom or brother are doing. We did not know who did the looking,
June 2015 126

pointing, and naming. We do not know the intent of looking at books and pointing and naming pictures. Similarly we do not know what was done with “finger plays” nor why this will help Toby’s development.
June 2015 127

POSSIBLE IMPROVEMENT:Today’s session included Toby, Milee (mom), and Toby’s older brother. Goal – saying words in response to cue. Milee reported they use drive time to practice words. Brother holds up object, brother and mom state the word, 3 times, then complete it if Toby doesn’t. Milee says Toby always gives it a real good try – at the very least saying the starting sound. Milee, brother, and Toby demonstrated. I recommended adding movement to facilitate learning. Since Milee will be driving, this task falls to big brother (he was thrilled). We practiced - brother selected the item and the movement – rocking left right, bouncing in seat, etc. Lots of laughter. Toby tried every time. He completed the words, “puppy” and “baby.” Much applause and hug from brother. I asked how running narrative technique was going. Milee indicated she felt odd telling a two year old how to make meatloaf. Reminded Milee speech depended upon hearing and seeing others speak. Much discussion. Milee agreed to try bath time, telling Toby how to bathe, to see if that felt more natural.
Note #2Addresses an identified need and outcome? Neither “reduce tantrums” or “verbalize”
are addressed in what was done today (#3) section.
Adult learner and service delivery triad? In the description of what was done today (#3), there is no indication of the EIS coaching or providing instruction to Alberta. We do not know what “work on sign for…” means. The reader is left to assume the EIS is teaching Alberta the signs for these words. If this is the case, professional knowledge in child development is not needed here.
Daily routines and materials in home? This narrative indicates a failure to use the naturally occurring routine of playing in the gym. Instead the child is required to attend to the EIS and Alberta while his classmates are off playing without him.
Child response to intervention? The response to the “since last visit” prompt creates the impression Nadir’s functioning has improved spontaneously and is not related to the implementation of interventions. Comments about Nadir’s relationship with Alberta are irrelevant, unless it has been negatively impacting Nadir’s development. If the relationship has been negatively impacting development, the observations should include mention as to why this information is important. Similarly we do not know why stating he is paying more attention is important. Given there is no outcome related to attention, no indication the EIS or Alberta are doing something to increase attention or have discovered a technique that helps Nadir to be more attentive, this information is also irrelevant. Similarly we do not
June 2015 128

know the significance of him responding to his name. We do not know what the EIS is trying to prove or document with this comment.
Application of professional knowledge? The instruction provided by the EIS (#4) does not require expertise in child development. Given the last two sentences in #3, Alberta is doing what is expected of her, the EIS is not offering any refinements, so no additional services are needed from the EIS.
POSSIBLE IMPROVEMENT:1. IFSP Outcomes (specify) Addressed:Respond to sign 5 times in a row, produce signs w/prompt 3 times in a row, and reduce tantrums to once a week.
2. What has happened since last visit?Alberta (teacher) stated Nadir is picking up some of the signs but not met criteria. Already been one tantrum this week. Redirecting works better than ignoring. Nadir responding to sounds - cochlear is going to work!
3. What did we observe/try today? (specify actions/engagement of all participants in visit)Gym time with his class. Nadir high tailed it to the balls. Demonstrated how to step into kids’ play to introduce signs (ball, please, thank you, sorry) with minimal disruption to play. Alberta tried. Noticed she wasn’t making sure she had his attention before signing. Recommended moving the signing of the word up to her lips so Nadir doesn’t have to look two places to get the message. Alberta tried, Nadir did respond to “please” 3 times in a row. Still not producing w/o prompt. Interruption irritated Nadir but no tantruming! Agreed with Alberta that play may be too distracting for production of sign. Alberta stated problems with Nadir taking off cochlear – saying no isn’t enough. Discussed possible options. No skin irritation. Alberta will try blocking the grab and putting something else in his hand.
4. What might we do different/continue? What will occur between visits?1) Get Nadir’s attention and sign near mouth.
2) Request Nadir to sign during story time (less active)
3) Continue with redirection on tantrums
4) Block and redirect for cochlear
June 2015 129

Note #3Addresses an identified need and outcome? Yes
Adult learner and service delivery triad? Yes
Daily routines and materials in home? There is no mention of routine or materials used.
Child response to intervention? There is no indication of the effectiveness of the techniques being demonstrated to the daycare worker.
Application of professional knowledge? Yes
POSSIBLE IMPROVEMENT:Outcomes addressed:Following directions (goal #9)
What’s happened since last visit (progress reported by family, concerns):Daycare staff reported they tried using the verbal cues as recommended but it does not seem to be helping.
Summary of activities worked on today (include how those present participated and specific progress noted by provider):Staff watched as Salme and I played with some blocks - giving her simple directions paired with verbal and visual cues. Discussed with staff how this helps cue Salme to what you are asking her to do. Modeled for staff how to use hand over hand assistance to guide Salme through direction. Staff then practiced above techniques with Salme while EIS observed and coached. When Salme tired of blocks we moved to play dough. Adding visual cues appears to be very helpful as Salme complied with most requests, until she tired of blocks. Salme accepted hand over hand unless EIS moved too quickly. Discussed how technique could be used throughout the day. Toughest time is when Salme first gets there. Scheduled next week’s visit to Salme’s arrival time on Wednesday.
Activities to work on before the next visit:*Give Salme verbal and visual cues when giving her directions. *Use hand over hand assistance to guide Salme through the direction, slowly.
June 2015 130

Note #4Addresses an identified need and outcome? Gross motor yes, but not speech.
Adult learner and service delivery triad? No. There is no indication the EIS interacted with the teacher.
Daily routines and materials in home? EIS is taking advantage of a spontaneously occurring event. In spite of the form’s prompt to talk specifically about the family’s routines, there is no indication the EIS has helped the teacher identify the best time to incorporate the interventions. The prompt on the form itself conveys the “Activities” of today’s service event are not expected to be a part of the family’s routines.
Child response to intervention? There is no description of SST intervention. We do not know what “helped him reach” and “encouraged” mean. We do not know if those actions were effective.
Application of professional knowledge? No. There is no indication SST was provided.
POSSIBLE IMPROVEMENT:Others present:Teacher (Carla), kids
Since our last visit:Carla stated the techniques we practiced last week are helping Su-bin’s attention to task. No modification needed at this time.
Goal(s) worked on today:Gross motor, speech
Activities:At Head Start, class was outside playing in the leaves. Grabbing bunches and throwing in the air. Pointed out to Carla this would be a good time to incorporate what PT showed her last week to improve arm extension. Reminded Carla she doesn’t have to help every time (and ignore other children). With Carla’s assistance Su-bin did better (got above shoulders), quickly faded till Carla assisted again. Noticed he was repeating Carla’s “whee”s and “whoa”s without prompting. Then running through leaves. I started saying, “Run, run” and asking him what he was doing to prompt Carla. She picked up the hint and incorporated into rest of outdoor activity. Questions to Su-bin got more whees and whoas. Su-bin then turned to picking up leaves and poking them through the fence. I pointed this out to Carla as another opportunity for extensions. Discussed if
June 2015 131

brief focused time at set time in day would work better for her. She said no, just needs to remember to look for opportunities.
What might we do different/continue? What will occur between visits?Look for arm extension opportunities - “outside time” may be most likely. Need to identify the best opportunities for repeating words – outside with other children may be too distracting.
Note #5Addresses an identified need and outcome? No. It is not clear how saying or signing
words, waving goodbye, or using a spoon addresses the goal of eating table foods.
Adult learner and service delivery triad? There are two documented recommendations (use sign and give Trevor a spoon). There is no indication of modeling, coaching, or instruction.
Daily routines and materials in home? Yes, routine of eating.
Child response to intervention? We have observations of Trevor’s behaviors but they are not connected to an intervention.
Application of professional knowledge? No. The outcome itself, as stated, is a poor match for SST. Review of the IFSP and needs assessment indicates Lela (mother) would like Trevor to “eat finger food solid food.” There is no indication of a behavioral issue related to eating. Other outcomes include “identifying common things.”
POSSIBLE IMPROVEMENT:Changes since last visit:Grandmother (Dulcea) reports interventions are working – he is starting to take 1-2 steps on his own now.
Worked toward IFSP outcome(s) of:Self-feeding finger foods. Identify common items.
Today’s activities/observations and parent/caregiver participation:Arrived at meal time. Dulcea offered pieces of toast, carrots, and fish sticks. Trevor ignored/refused and stared at jar of baby food (carrots) on table. Recommended hiding jar behind napkins and use as reward for finger feeding. Demonstrated. Dulcea picked up quickly – one prompt to not come in too quickly with reward (too much in mouth). Also good time to identify food items. Demoed: Ask Trevor which finger food he wants, name food when offered, name food accepted. Trevor did not name food but repeatedly
June 2015 132

said “mama” and perhaps “papa.” After meal, demoed use of pictures to connect spontaneous speech to correct items. Dulcea implemented w/o assistance. No evidence of effectiveness – will tell over time.
Child’s progress and recommended activities:1. Hiding baby food jar makes finger food more desirable. 2. Using jarred food as reward encourages him to eat finger food.3. Naming items when offered and accepted helps Trevor to identify items.4. Asking Trevor what he wants to eat encourages him to say what he wants.
Note #6Addresses an identified need and outcome? No. There is no indication the EIS
addressed either the attention span or expressing needs outcomes. Referring back to the IFSP and needs assessment, there is no documented need in the personal-social domain. There is no outcome for Mica to be comfortable with the EIS.
Adult learner and service delivery triad? No. There is no indication of the EIS modeling, coaching, or providing instruction.
Daily routines and materials in home? Yes.
Child response to intervention? One reference to an intervention “after using some distraction” does appear to be successful. “Using distraction” was neither explained nor taught to the parent.
Application of professional knowledge? No. There is no indication of SST being provided in the “what did we try” section. The recommendations in the “What will Occur between visits” section is unrelated to the stated outcomes and does not tell the parent how they are to do what is being requested of them.
POSSIBLE IMPROVEMENT:IFSP Outcomes (specify) Addressed:Mom (Michele) wants Mica’s attention span and joint attention to increase so he will be able to stay focused on one activity for at least 10 to 15 minutes during playtime. Mica will request his wants/needs with words/word approximations during snack time and play time 5 times a day or 7 consecutive days.
What has happened since last visit?Michele reported the effectiveness of first ST session was limited – Mica clung to her. Seems to be handling other social situations well, even their first trip to the playground at the mall.
June 2015 133
What did we observe/try today? (specify actions/engagement of all participants in visit)Given it was my first visit with Mica, spent a few minutes playing with a puzzle – I slowly increased proximity and involvement. At same time I talked with Michele about things that keep Mica’s interest, how to incorporate that into activities. We agreed to try car sounds when driving puzzle pieces over to him. (No demo from me – Mica still cautious) At first car sounds distracted from next step - identifying the piece. Michele was very good at patiently prompting until Mica identified the piece with approximation. Sometimes Mica would lose focus. Recommended different car sounds to get his attention back. Beep beep seems to work very well, makes him laugh. After about fifteen minutes suggested to mom to ask Mica what he wanted to play with next. Mica gestured for his cars. Had to stop Michele from responding before Mica said “ca.” Suggested she use each car as a separate learning opportunity – “Do you want the blue car? Say blue.” Michele used beep beep to refocus w/o my prompting. Worked well here as well.
What might we do different/continue? What will occur between visits?Continue to use car sounds to help Mica focus during play time. Resist urge to respond to Mica’s gestures during play and snack time.
Note #7Addresses an identified need and outcome? Yes
Adult learner and service delivery triad? Yes
Daily routines and materials in home? Yes
Child response to intervention? Yes
Application of professional knowledge? Yes
POSSIBLE IMPROVEMENT:Outcome:Sign needs/wants
Arrived at childcare center for snack time. I sat beside Hector at the table with Sally (tchr) and 4 other kids. Sally has started giving the children small portions of snack foods instead of the whole thing at once as we discussed last week. Demonstrated pausing to allow Hector time to request. Sally adjusted easily. I assisted Hector (hand over hand) to sign “cookie” for another piece, and to sign “drink” for more juice. Sally practiced assisting hand over hand. He enjoyed the signs, and by the end of snack, he required only minimal prompt for “drink.” Use of signs may help decrease Hector’s
June 2015 134

frustration about communication and help decrease tantrums. Class had “free play” time during diaper changes. I modeled using single words and two signs (truck and baby) to describe Hector’s play. Modeled pausing to allow Hector time to imitate. Explained to Sally these techniques allow Hector to learn more vocabulary, and it’s a start for reciprocal communication that will decrease tantrums. Taught Sally signs for ball, block, and paint. Sally practiced with me, will use with Hector at first opportunity.
Note #8Addresses an identified need and outcome? Yes
Adult learner and service delivery triad? Yes
Daily routines and materials in home? Yes
Child response to intervention? Yes
Application of professional knowledge? Yes
POSSIBLE IMPROVEMENT:Absolutely nothing.
Note #9Addresses an identified need and outcome? Yes
Adult learner and service delivery triad? Yes
Daily routines and materials in home? Yes
Child response to intervention? Yes
Application of professional knowledge? Yes
POSSIBLE IMPROVEMENT:Outcome:To crawl
Suong (Mom) set Kim on her bottom on floor, EIS placed the toys around her. She reached out for the blocks and pivoted on her tummy. When she reached out for the cube which was placed quite aways, she tried to go to her tummy but her leg got caught up under her so EIS showed Suong how to gently pull her leg just a little bit under her and then Kim did the rest of the work and she went to all fours. She immediately went down on her tummy but the work on her arms was there. She reached for the blocks
June 2015 135

and mom helped her place them where they go and turned on some music. She got very excited and started to dance. When EIS attempted to fold her legs under her to show mom how to help her stay that way, Kim got upset. Suong calmed her down and we tried floor time again after a little bit, dancing while reaching for toys and Suong assisting Kim in going to all fours.
June 2015 136


















![Case Management for Children and Pregnant Women07D0901F-86B6-4CD0-B7A2... · 2016-10-14 · Case Management for Children and Pregnant Women [graphic image] [DSHS and THSteps logos]](https://img.pdfslide.us/doc/110x75/5e6fa2cfb08c127db03f2375/case-management-for-children-and-pregnant-women-07d0901f-86b6-4cd0-b7a2-2016-10-14.jpg)