Embed Size (px)
Citation preview

IN THIS ISSUE: REGULATORY ROUND UP Special features Good science: The newrole of Medical Affairs inan outcomes-focusedworldGreat innovation needsgreat leadershipBurn Out? … Not Me, I’mImmune!
JOURNAL OF THE BRITISHASSOCIATION OFPHARMACEUTICALPHYSICIANS
PHARMACEUTICAL PHYSICIAN
MAY 2017 VOLUME 27 | NO3
Resourcing Solutions for Medical Affairs, Pharmacovigilance and Clinical Development
Providing Pharmaceutical Physicians
www.axess.co.uk
This is just a selection of the current assignments with our pharmaceutical clients. For a confidential discussion please telephone Beth Thomas-Stonier at AXESS Limited on 020 8560 2300. To apply please send your CV to [email protected] quoting the reference number.Visit our website www.axess.co.uk to register for jobs by e-mail – new roles that match your criteria e-mailed to you on the same day that they are posted.
Permanent RolesDirector Medical Affairs Hepatitis C, EMEA Fast growing Global Biotech – Team of 5 W London PP 6866
EU Medical Director Oncology/ Haematology EMEA Global Pharma – Rich pipeline Surrey PP 6793
Medical Director UK Fast growing Specialty Pharma Central London PP 6855
Head of Medical Affairs UK/ Ire – General Medicine/ Fertility Global Biotech – leadership role W London PP 6862
Associate Medical Director Oncology EMEA Global Pharma – Significant launch activity Surrey PP 6879
Senior Medical Manager Oncology EMEA Fast growing Global Biotech W London PP 6874
Global Medical Manager – Neurology International Pharma – Parkinson’s Berkshire PP 6713
Global Medical Advisor – GI Specialty Pharma Middlesex PP 6696
Medical Manager UK Biologics Dermatology Global Pharma – launch and line management Berkshire PP 6748
Medical Manager UK Topical Dermatology UK/EU/Nordics Global Pharma – line management Berkshire PP 6810
Medical Advisor Ireland Biopharma Dublin PP 6875
Senior Medical Advisor UK – Hyperkalemia International Pharma Surrey PP 6801
Medical Advisor UK – Rare Diseases Biopharma – interesting portfolio Buckinghamshire PP 6864
Medical Director Clinical Development Global Biotech – Immuno-Oncology Germany PP 6861
Medical Director Clinical Research Research Organisation – Respiratory/ Infectious Diseases Central London PP 6882
Medical Director, Global Drug Safety Global Biopharma – Strategic focus Germany PP 6823
Senior Drug Safety Physicians – Oncology or Fertility Global Biopharma – Global remit and visibility Germany PP 6880 Interim PV Physician – 6m Global Pharma – Global Safety Lead – GI London PP 6780

PHARMACEUTICAL PHYSICIAN
Published 6 times per annum by BrAPPRoyal Station Court, Station RoadTwyford, Reading, Berkshire RG10 9NF. Telephone +44 (0)118 934 1943 Fax +44 (0)118 932 0981 Email [email protected] www.brapp.org
Call the BrAPP office for subscription information or to advertise in thejournal.
BrAPP grants editorial freedom to the editor of Pharmaceutical Physician.
The views expressed in the journal are those of the authors and may notcomply with the views of BrAPP or the authors' own companies.
© BrAPP ISSN 0960-6548
EDITOR: DR MADHU DAVIES
EDITORIAL BOARD: DR JANE BARRETT
DR HUGH BOARDMAN
DR DAVID FOWLER
LIZ LANGLEY [email protected]
DESIGN: DANA KIDSON
EDITORIAL 3
REGULATORY ROUND UP 4Anne Hetherington
SPECIAL FEATURE 6Good Science: the new role ofthe Medical Affairs in anoutcome-focused worldElizabeth Coulter, JamesCrowley and Benjamin Rhee
SPECIAL FEATURE 11Why life sciences innovatorsneed to build the right team– an opinion pieceTarquin Bennett-Coles
SPECIAL FEATURE 14Burn Out? .. not me I’mimmuneDr Catriona McMahon
SPECIAL FEATURE 18First medicDr Michael Atkins
RETRO FEATURE 22Pills, probabilities andprecaution –first publishedJan 2008Letter to Editor – publishedMarch 2008Professors Stephen Senn andSir Peter Lachmann
NEWS 28
Contents
MAY 2017 VOLUME 27 | NO3
CARDIFF UNIVERSITY/BRAPP
POSTGRADUATE COURSE IN PHARMACEUTICAL MEDICINEAn interactive course providing broad knowledge-based learning across the specialty of pharmaceuticalmedicine; run by BrAPP working closely with Cardiff University.
Sessions are mapped to the syllabus for the UK Diploma in Pharmaceutical Medicine exam.
Ten two-day, non-residential sessions run in central London from January 2018 to July 2019. (The exception isSession 1 which is held at Cardiff University.)
Expert teaching is provided by a wide spectrum of industry and academic experts and includes an IntegralRevision module and a Critical Appraisal workshop run by Dr Richard Kay.
Places are limited to 25 delegates.
For further information and to register please contact:[email protected] or visit www.brapp.org or call +44 (0) 118 934 1943
May 2017volume 27 | No 3PHARMACEUTICAL PHYSICIAN
3
THE “RETRO” FEATURE has provedvery popular with you: “Plus ca changemais plus ca meme chose”, perhaps? Itis fascinating re-reading opinion and‘state of the nation’ from some time agoand contrasting with today’s context.Lots to learn there. And thank you forthe constructive feedback. With thevarious reports on the Bial Phase I unitcrisis now freely available (and see aprevious issue of PP for a commentary)it seems appropriate to look back at theTGN issues and for each of us toconsider what we may have learned.
Your feedback also tells me thatRegulatory Round Up continues to saveyou time and effort bringing togetherthe key updates for the major agencies.Thank you to Anne Hetherington fortirelessly collating this for us. Change isthe order of the day.
I am thrilled to be able to bring you athought leader piece from the Accentureteam on the role of medical affairs in anoutcomes focused world. The world ofmedical affairs is changing rapidly tooand the role descriptions have evolvedvery considerably from those of perhapsonly 10 years ago. How are you future-proofing your career?
Continuing the leadership theme,Tarquin Bennett-Coles discusses the roleof great leadership in innovation,looking at various settings and askingsome key questions which may helpyou as you career plan.
Dovetailing well with that, MichaelAtkins, a hugely experiencedpharmaceutical physician who hasenjoyed a variety of senior leadershiproles in established pharma, considerswhat it takes to be the first medic in acompany. Recommended reading forthose of you contemplating thisinteresting environment.
Many of us try to be all things to allpeople- we like to make others ‘happy’.This carries a cost and CatrionaMcMahon, a former UK medicaldirector, discusses burn out and how we
might consciously avoid it. For those ofyou who are nicely defended againstthe idea that ‘it could be you’, it really isworth the read.
Enjoy the spring.
Dr Madhu Davies
EDITORIAL
Dr Madhu Davies
REGULATORY ROUND UP
By Anne Hetherington, Senior Regulatory Consultant, Envigo Ltd.
HERE IS THE LATEST ROUND UP OF REGULATORY NEWS FROM THE LEADING
AGENCIES, INCLUDING THE EUROPEAN MEDICINES AGENCY (EMA), THE MEDICINES
AND HEALTHCARE PRODUCTS REGULATORY AGENCY (MHRA) AND THE FOOD AND
DRUGS ADMINISTRATION (FDA). EMPHASIS IS PLACED ON THOSE NEW
REGULATIONS WHICH IMPACT ON CLINICAL AREAS.
PLEASE CLICK ON THE LINKS BELOW TO TAKE YOU TO THE RELEVANT ITEM.
WE HOPE THAT YOU WILL FIND THIS DIGEST OF INTEREST. IF YOU HAVE ANY
COMMENTS OR QUERIES PLEASE CONTACT US AT [email protected].
May 2017 volume 27 | No 3
4PHARMACEUTICAL PHYSICIAN
WORLD HEALTH ORGANISATION• WHO launches global effort to
halve medication-related errors in 5yearshttp://www.who.int/mediacentre/news/releases/2017/medication-related-errors/en/
EUROPEAN MEDICINES AGENCY (EMA)News and press releases• Medicine evaluation figures
http://www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/document_listing/document_listing_000256.jsp&mid=WC0b01ac0580099fbb
• Conditional marketingauthorisations give patients accessto important new medicines earlierhttp://www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2017/01/news_detail_002680.jsp&mid=WC0b01ac058004d5c1
• Human medicines: highlights of2016http://www.ema.europa.eu/ema/ind
ex.jsp?curl=pages/news_and_events/news/2017/01/news_detail_002678.jsp&mid=WC0b01ac058004d5c1
• First hormone replacement therapyfor parathyroid disorderhttp://www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2017/02/news_detail_002700.jsp&mid=WC0b01ac058004d5c1
• Multiplicity issues in clinical trialshttp://www.ema.europa.eu/ema/index.jsp?curl=pages/regulation/general/general_content_001220.jsp&mid=WC0b01ac05807d91a4
Updates• Post-orphan medicinal product
designation procedures: guidancefor sponsorshttp://www.ema.europa.eu/docs/en_GB/document_library/Regulatory_and_procedural_guideline/2015/11/WC500196994.pdf
• Report - Workshop on identifyingopportunities for ‘big data’ in
Anne Hetherington
ENVIGO.COM

medicines development andregulatory sciencehttp://www.ema.europa.eu/docs/en_GB/document_library/Report/2017/02/WC500221938.pdf
• Annual report on the use of thespecial contribution for orphanmedicinal productshttp://www.ema.europa.eu/docs/en_GB/document_library/Report/2017/02/WC500221159.pdf
• Scientific guideline: Concept paperon the need to revise Condition –Specific guidance, Appendix 4 tothe guideline on the evaluation ofanticancer medicinal products inmanhttp://www.ema.europa.eu/ema/doc_index.jsp?curl=pages/includes/document/document_detail.jsp?webContentId=WC500224997&murl=menus/document_library/document_library.jsp&mid=0b01ac058009a3dc
• Scientific guideline: Guideline onclinical development of fixedcombination medicinal products -Revision 2http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2017/03/WC500224836.pdf
• Regulatory and proceduralguideline: Guidance on the formatof the risk management plan (RMP)in the EU – in integrated format(Rev. 2), adoptedhttp://www.ema.europa.eu/docs/en_GB/document_library/Regulatory_and_procedural_guideline/2017/03/WC500224771.pdf
• Regulatory and procedural guideline:Guidelines on goodpharmacovigilance practices (GVP):Introductory cover note, last updatedwith revision 2 of module V on riskmanagement systems finalised post-public consultation, related revision2 of module XVI and revision 2 ofmodule II on PSMFhttp://www.ema.europa.eu/docs/en_GB/document_library/Regulatory_and
_procedural_guideline/2017/03/WC500224566.pdf
MEDICINES AND HEALTHCAREPRODUCTS REGULATORY AGENCY(MHRA)• New MedRegs blog
https://www.gov.uk/government/news/new-medregs-blog
FOOD AND DRUG ADMINISTRATION(FDA)Guidance for Industry• Considerations in Demonstrating
Interchangeability With a ReferenceProduct Guidance for Industryhttps://www.fda.gov/ucm/groups/fdagov-public/@fdagov-drugs-gen/documents/document/ucm537135.pdf
REGULATORY ROUND UP
May 2017 volume 27 | No 3PHARMACEUTICAL PHYSICIAN 5
SPECIAL FEATURE:Good science:The new role of Medical Affairs in an outcomes-focused world
By Elizabeth Coulton, James Crowley and Benjamin Rhee
FOR YEARS, PHARMACEUTICAL
COMPANIES HAVE DEPLOYED THEIR
MEDICAL AFFAIRS WORKFORCES TO
HELP PHYSICIANS IMPROVE PATIENT
CARE THROUGH THE SAFE AND
APPROPRIATE USE OF DRUGS. WHILE
THESE RESOURCES ARE CONSIDERED
VALUABLE, CUSTOMERS RARELY SEE
THEM AS CRITICAL TO IMPROVING
POPULATION HEALTH OUTCOMES.
THAT’S ABOUT TO CHANGE.
May 2017 volume 27 | No 3
6PHARMACEUTICAL PHYSICIAN
HEALTHCARE DISRUPTEDTHE HEALTHCARE INDUSTRY is in themidst of massive change. Two primarytrends are disrupting how scientific dataand drug information are used andhighlighting how the Medical Affairsworkforce can be more valuable tohealthcare delivery teams, fromsupporting administrators making policydecisions in boardrooms to supportingcare teams making treatment decisionsat the bedside.
Trend 1: Patient outcomes andpopulation healthThe healthcare industry is shifting itsfocus from volume to value. Thistransition is most evident in the move tomeasure and reimburse providers basedon the quality, not the quantity, of carethey deliver. Global healthcare reformsare accelerating this shift by introducingoutcomes-based payment models andnew care delivery models aimed ataddressing population health issues.Socialized medicine systems in Europe,Japan and China are taking a lead inthis regard, and are developing newapproaches to increasing healthcareeffectiveness and efficiency. In theUnited States, too, alternatives to thetraditional fee- for-service model are onthe rise.[1]
In this new environment, many moreparties—from population healthclinicians to pharmacists andadministrators—are joining physicians inmaking decisions aimed at improvinghealth outcomes. All of thesestakeholders need to know more aboutthe solutions, services and drugs (andthe science behind them) that areavailable. Pharmaceutical companies,through their Medical Affairs
workforces, are uniquely positioned tohelp.
Trend 2: Complexity of careScientific advances are making itpossible for providers, researchers,clinicians and administrators to define,understand and treat diseases at a moregranular level than ever before. Inaddition to making treatment paradigmsmore complex, these advances areproducing more data than thesestakeholders can effectively use.Information overload is likely to getmuch worse. Accenture research hasfound that more than 40 percent of lifesciences companies surveyed expect tosee their data volumes increase by atleast 50 percent in the coming year.[2]
This is particularly concerning becauseas the healthcare industry shifts more ofits attention and investments toimproving patient outcomes, playerswithin the industry are placing moreemphasis on the reliability, rigor andrelevance of the drug information thatunderpins so much of their decision-making. That information must beaccurate and trustworthy. It must bediscoverable. And it must be actionable.Often, it is none of the above. Thispresents a tremendous opportunity forMedical Affairs to serve as the source ofinformation and insight to improvehealth outcomes.
MEDICAL AFFAIRS: STEWARDSOF PATIENT OUTCOMESAgainst the backdrop of trends andchallenges that are now affecting allplayers in the healthcare ecosystem,pharmaceutical Medical Affairsorganizations have an unprecedentedopportunity to play a much more
Elizabeth Coulton James Crowley
Benjamin Rhee

strategic role in the delivery of patientoutcomes.
While regulatory restrictions willcontinue to define the nature of therelationships that Medical Affairs canhave with customers, pharmaceuticalcompanies can make those relationshipsbroader, deeper and much moremeaningful. To do so, Medical Affairswill need to re-imagine every aspect oftheir roles.
Who are the customers?Medical Affairs professionals willcontinue to be a vital source ofinformation for physicians looking toimprove the health outcomes of theirpatients. But they will also drivesolutions for a broader network ofdecision-makers and opinion leaders,including healthcare administrators andbusiness managers, as well as pharmacyand therapeutic committee members athospitals and health systems.Additionally, they will support otherstakeholders such as population healthmanagers, who work with hospitals andhealth systems to manage the healthcareoutcomes and costs of specific patientpopulations.
What services can be provided?Ensuring the safe and appropriate use ofdrugs has always been— and alwayswill be—the most important role forMedical Affairs personnel. But they nowhave the opportunity to serve as trustedexperts to their extended network ofstakeholders. Further, Medical Affairsprofessionals can act as credible curatorsand connectors of information to treatinformation overload and help themmake better decisions at the point ofcare. By helping capture, understandand use science from many sources,Medical Affairs can assume a prominent(and largely unfulfilled) role inminimizing complexity and improvingpatient outcomes and population health.
What skills will be needed?To achieve a broader reach and greaterimpact, the Medical Affairs workforcewill need deeper scientific knowledge in
areas such as population health. Otherskills will be equally critical.
• Collaboration skills will be importantbecause Medical Affairs fieldpersonnel will need to interact withcustomers, internal teams, andinternal and external experts in moreresponsive and personalized ways,connecting these healthcareecosystem participants to theinformation that will lead to betterhealth outcomes. They will need towork with experts inside and outsidetheir organizations to build theirknowledge of the complex sciencenow underpinning drug developmentand the patient journey. They willneed to engage with behavioralhealth researchers and healtheconomists to understand anddevelop valuable insights into issuesaffecting population health. And theywill need to interact with third-partyspecialists to understand how newtechnologies and solutions might beintegrated into a broader plan forimproving patient outcomes.
• Judgment skills will be increasinglyimportant in an environment that ispivoting from volume to value. Inmany disease areas, for example, thedefinition of value is not yet clear. Asthe link between the science ofmedicine and the business ofhealthcare delivery, Medical Affairsprofessionals can serve a strategic roleand help inform these valuediscussions by sharing the mostrelevant and trustworthy informationwith healthcare teams. Beyondcurating and prioritizing information,these professionals will apply theirjudgment to determine the best way tohelp their customers define outcomesand understand the science behind thepatient outcomes they seek.
STEWARDSHIP IN ACTIONOne of the ways Medical Affairsprofessionals can serve as stewards ofpatient outcomes is by helpinghealthcare teams tackle issues thatthreaten to derail achieving the desired
patient outcomes. Drug adherence is anexample.
Pharmaceutical customers can nowaccess mountains of information aboutwhy some patients fail to take theirmedications as prescribed. Similarly,digital technologies have produced ahost of potential tools to improveadherence.
Unfortunately providers don’t have thetime to sift through these tools andmaterials to determine the rightapproach for their patients.
The Medical Affairs workforce canhelp. First, they can collect, aggregate,and determine the relevance of onlineand offline information related toadherence. They can add additionalvalue by reviewing anecdotal evidencefrom their contacts in the field andscouring their own organizations’clinical trial data for insights andtechnical innovations that might informadherence strategies. Armed with themost useful and objective findings, theycan help their customers not onlyunderstand the barriers to patientadherence, but also devise solutions forovercoming them.
SPECIAL FEATURE:Good science:
The new role of Medical Affairs inan outcomes-focused world
May 2017 volume 27 | No 3PHARMACEUTICAL PHYSICIAN
Continues on page 8 ��
7
SPECIAL FEATURE:Good science:
The new role of Medical Affairs inan outcomes-focused world
PHARMACEUTICAL PHYSICIAN
How can we enable success forMedical Affairs?Technical and analytical skills willbecome more important. Accentureresearch found that 79 percent ofpharmaceutical companies intend toinvest in capabilities that will streamlineand automate some of their knowledgeworkers’ more time- consuming tasksover the next three years.[3] That’sencouraging. The challenge for leadersnow will be to balance the technologyinvestments made to support theMedical Affairs workforce withinvestments made for other workforces.
Technology investments for MedicalAffairs—both internal operationsgroups and field teams—should befocused on the things that will allowthese resources to deliver morepersonalized and more strategicservices. Such investments mightinclude solutions aimed at minimizingadministrative burdens, analyticscapabilities that reveal insights intocustomer needs and preferences, digitalmonitoring solutions that enable themining of new evidence sources, orsystems designed to help aggregateinsights and information for quickercustomer visit preparation.Pharmaceutical companies will need totrain internal and field personnel onhow to use these new technologies formaximum effect.
THE DIGITAL WORLD OFFERSNEW SOURCES OF EVIDENCEAccording to Accenture research, 57percent of US consumers accessed awebsite for medical information lastyear. One in five (21 percent) usedsocial media for that purpose. And 12percent turned to online communities.[4]
While the quality of informationretrieved from online sources is oftengeneral in nature and sometimesquestionable,[5] patients are using theirdigital findings to ask their doctors andproviders more specific questions. That,in turn, changes the types of informationpharmaceutical customers seek.
Pharmaceutical companies may want toinvest in digital monitoring solutionsthat allow Medical Affairs to uncovernew sources of evidence. Healthcareconsumers leave a digital footprint withtheir online queries and conversations,which means pharmaceutical companiescan analyze the behaviors, opinions andconcerns that patients demonstrateonline. By applying those insights, aswell as their judgment skills to identifythe trustworthiness and relevance ofsources, Medical Affairs
can better predict the types of questionspatients will ask of their physicians—and the types of questions thatpharmaceutical customers may ask ofMedical Affairs.
May 2017 volume 27 | No 3
�� Continues from page 7
8
In the workforce of the future, Medical Affairs must:
Determine the relevanceand trustworthiness ofonline and offlineinformation
Search for insights thatmight inform adherencestrategies
Compile data that helptheir customersunderstand patientadherence and devisesolutions
SHAPING THE FUTURE OFHEALTHWe believe the opportunity to refocusand enable the Medical Affairsworkforce is one of many that willemerge for Medical Affairs organizationsin the coming years. To ensure thatMedical Affairs continues to deliver theservices and solutions that meetcustomers’ growing expectations anddemands, pharmaceutical leadersshould:
should:Rally support across theorganization for a newMedical Affairs vision.
Constantly evaluate theirmedical strategies, as well asthe roles and resources theywill need in the future.
Invest in the skills,technologies and trainingthat will ultimately bringthat vision to life.
Measure the effectiveness ofMedical Affairs efforts sothat the services, channelsand tools that are availableto customers can becontinually refined andimproved.
Science does not stand still.Neither can pharmaceuticalmanufacturers’ Medical Affairsorganizations. It’s not too early forpharmaceutical leaders to start thinkingabout how they can position theirMedical Affairs organizations to have aneven greater impact on the healthcareecosystems they serve. Refining the roleof Medical Affairs from disease andproduct specialists to curators andconnectors of outcomes-focusedinformation is a first step in thatjourney.
The second step is equally important.It calls for leaders to honestly assesstheir workforce’s capacity to make thetransition. Do they have the rightnumber of customer-facing andoperational resources to deliver againstthe new Medical Affairs imperative? Dothey have the right talent and skill setsto address the growing B2B nature ofcustomer interactions? And how willMedical Affairs measure its success?
Join the conversation@AccentureStrat@AccentureLifSci@Accenture-Strategy
Contact the AuthorsElizabeth Coulton [email protected]
James Crowley [email protected]
Benjamin Rhee [email protected]
Additional ContributorsElizabeth Ferguson [email protected]
Cathy Xu [email protected]
About AccentureAccenture is a leading globalprofessional services company,providing a broad range of servicesand solutions in strategy, consulting,digital, technology and operations.Combining unmatched experience andspecialized skills across more than 40industries and all business functions—underpinned by the world’s largestdelivery network—Accenture works atthe intersection of business andtechnology to help clients improvetheir performance and createsustainable value for their stakeholders.With approximately 375,000 peopleserving clients in more than 120countries, Accenture drives innovationto improve the way the world works
SPECIAL FEATURE:Good science:
The new role of Medical Affairs inan outcomes-focused world
May 2017 volume 27 | No 3PHARMACEUTICAL PHYSICIAN
Continues on page 10 ��
9
Last year, US consumers went online for medical information:
57% Accessed a website 21% Used social media 12% Used onlinecommunities
SPECIAL FEATURE:Good science:
The new role of Medical Affairs inan outcomes-focused world
PHARMACEUTICAL PHYSICIAN
and lives. Visit us atwww.accenture.com
About Accenture StrategyAccenture Strategy operates at theintersection of business and technology.We bring together our capabilities inbusiness, technology, operations andfunction strategy to help our clientsenvision and execute industry-specificstrategies that support enterprise-widetransformation. Our focus on issuesrelated to digital disruption,competitiveness, global operatingmodels, talent and leadership helpsdrive both efficiencies and growth. Formore information, follow@AccentureStrat or visitwww.accenture.com/strategy
About Accenture Life SciencesAccenture’s Life Sciences group isdedicated to helping companies rethink,reshape or restructure their businessesto deliver better patient outcomes anddrive shareholder returns. We provideend-to-end business services as well asindividual strategy, consulting, digital,technology and operations projectsaround the globe in all strategic andfunctional areas—with a strong focus onR&D, Sales & Marketing and the SupplyChain. We have decades of experienceworking hand-in-hand with the world’smost successful companies to improvetheir performance across the entire LifeSciences value chain. Accenture’s LifeSciences group connects more than
13,000 skilled professionals in over 50countries who are personally committedto helping our clients achieve theirbusiness objectives and deliver betterhealth outcomes for people around theworld.
Accenture Life Sciences BlogAccenture experts share insights andopinions on opportunities andchallenges in the pharmaceutical andmedical technology industryww.accenture.com/lifesciencesblo.
Copyright © 2016 Accenture All rightsreserved.
May 2017 volume 27 | No 3
�� Continues from page 9
10
| REFERENCES1. Jeff Elton and Anne O’Riordan, Healthcare disrupted: Next generation business models
and strategies, Wiley, 2016, pp. 12-18.
2. Accenture Technology Vision Research for Life Sciences, 2015.
3. Ibid
4. Accenture Consumer Survey on Patient Engagement, US findings, 2016.
5. Eric Topol, The patient will see you now: The future of medicine is in your hands, BasicBooks, 2015, pp. 34-35.

May 2017 volume 27 | No 3PHARMACEUTICAL PHYSICIAN
SPECIAL FEATURE:Why life sciences innovators need
to build the right teamsAn opinion piece
By Tarquin Bennett-Coles, Principal Consultant in the Life Sciences Practice, Carmichael Fisher
11
GREAT INNOVATION NEEDSGREAT LEADERSHIP.THE LATE, GREAT Steve Jobs said:“Innovation distinguishes between aleader and a follower.”
So, when it comes to spottingopportunities in the exciting cross-overfields of life sciences, technology, andconsumer applications, the rightleadership team is vital.
Businesses may be set up with anoriginal goal in mind, such asdeveloping new tools for cancerscreening.
The potential applications for thetechnologies they innovate, however,could be far wider than the healthcarefield.
Tarquin Bennett-Coles, CarmichaelFisher’s Principal Consultant in LifeSciences Practice, says the need forsome members of leadership teams withbroader skills and experience is nowbeing widely recognised by companiesin this cross-over space.
The need for managerial agility inrecognising skills gaps and pluggingthem with the right people isparamount for a successful business.
“Original teams may well be veryfocused on the healthcare benefits oftheir potential projects and haveextensive experience in that field,” hesays.
“Their skills may be highly specialised.
“However, lucrative consumerapplications could transform the future
of a company. They could ensure itsviability and its ability to carry outfurther research and development inimportant areas of life sciences.
“Failure to capitalise on theseopportunities could have the oppositeeffect. Companies which fail to graspthem could be held back fromperforming important work.
“Leaders must be aware from the outsetthat there may be potential for theapplication of their technologies indifferent areas to those they initiallytarget, and they must be open to theopportunities which arise. They must beopen to changing direction.
“Then, people with the right kind ofskills at every level must be brought into develop these potentially lucrativeconsumer applications.
“As the project progresses, companiesmay need those with corporate skills orthose experienced in the use ofdifferent technologies.”
Many of the consumer markets whichmay use applications may be radicallydifferent to the field of life sciences.
“Leadership teams need people whounderstand these markets,” Mr Bennett-Coles says.
“They also need those with excellentcorporate skills. They will knowwhether companies need to be split andrun separately to maximise theopportunities.
“There are also differences intimescales. In life sciences, teams might
Tarquin Bennett-Coles

SPECIAL FEATURE:Why life sciences innovators needto build the right teams
An opinion piece
PHARMACEUTICAL PHYSICIAN
expect to see results after a five totwelve years development process.
“For those with experience of theconsumer markets, they would perhapsbe looking to develop a product or aservice within 18 months.
“This speed is necessary to ensure thetechnology isn’t overtaken or anotherteam moves more quickly to bringsomething to market.”
Two case studies show the importanceof that approach:
How technology developed as acancer diagnostic became a tool inthe war on terrorTeraView Ltd, based in Cambridge, wasoriginally set up as part of the Toshibaoverseas research laboratories in the1990s.
It began life as a way of researchingcancer diagnostic tools using Terahertzlight technology.
X-rays give us images of our bones.Terahertz T-rays allow us to seemolecular structures.
TeraView uses T-ray light, which sitsbetween microwaves and infrared, as atool to carry out tests and inspections.
The T-rays allow the creation of 3Dimages.
Though the technology was originallydeveloped as a tool in cancerdiagnostics, it soon became obvious that
it had several other applications whichneeded to be developed.
Alongside medical testing, TeraView’stechnology is used in thepharmaceutical, semi-conductor, andsolar industries.
It is also used to test for explosives,noxious gases, and non-metallicweapons.
Technology which began as a medicaldiagnostic is now an important tool insecurity screening.
TeraView’s CEO Don Arnone says:“These opportunities became apparentquite early on. We could see there waspotential in three or four differentmarkets and we pulled in people withexperience of operating in those markets.
“We knew we needed a team with theright technical skills and anentrepreneurial flair and professionalswith a good knowledge of thosemarkets to commercialise thetechnologies we were producing.
“Initially, we brought people in on aconsultancy basis, then on contract. Aswe moved forward, they stayed with us.
“We brought in people who understandmarkets in the USA and those who haveexperience in the automotive market.
“As the company grew and we faceddifferent challenges, we needed atechnological team which could help usdeliver solutions fairly rapidly.
May 2017 volume 27 | No 3
�� Continues from page 11
12
THE NEED FOR MANAGERIAL AGILITY IN RECOGNISING SKILLS GAPS
AND PLUGGING THEM WITH THE RIGHT PEOPLE IS PARAMOUNT FOR A
SUCCESSFUL BUSINESS.
“We also needed people who coulddevelop and maintain customerrelationships in our different markets.
“We’ve maintained a flat structure. Wedon’t have a bunch of expensiveexecutives or vice presidents, forexample.
“As we have grown, we have graspedopportunities and our team hasdeveloped knowledge and skill indifferent markets.
“We developed a product for theinspection of microchips in mobilephones for Intel in 2008/9.
“Since then, the team has developedcontacts and experience in the semi-conductor industry after working withIntel’s engineers for eight years.
“As we’ve grown, our team has adaptedto different markets and technologies,and there has been some convergence.
“However, there are still differences inmarkets which must be taken intoaccount. Someone in sales in the semi-conductor market would not beparticularly adaptable to selling in theautomotive market, for example.”
Understanding different markets ishelping one company expandoverseasFor innovative company Ieso DigitalHealth, building a team with anunderstanding of different healthcaremarketplaces has been a key buildingblock to success.
The Cambridgeshire company waslaunched in 2011. It delivers cognitivebehavioural therapy (CBT) to patientsthrough a ground-breaking onlinemethod.
Its Director Dr Andy Richards explains:“There’s a well-known inhibition whena patient sees a therapist face-to-face.Freud recognised this. It takes severalsessions to build a trust and honestdialogue.
“We deliver therapy online using awritten method which helps ourqualified therapists to develop trust withpatients much more quickly than if theywere physically seeing a therapist.
“Our system is highly secure and awritten record of all sessions is kept -something which is useful to therapistsand patients and allows improvedprotocols to be developed.”
“Patients can access treatment via ouronline method more quickly thanphysically seeing a therapist, and outtreatment has proved highly effective inmany cases.
“We took the decision in the UK towork within the NHS, rather thanprivately, so our patients are referred tous by NHS trusts.
However, there is a growing marketneed for this approach overseas, andthis is where the right leadership teamhas become an important element inIeso Digital Health’s growth.
Alongside skills in the commercial andtechnical fields, the company’s team hasneeded market-specific knowledge.
Dr Richards says: “If you take the UnitedStates, the ‘behavioural health’ market isvery underserved, but healthcare isdelivered in a very different way thanwithin the NHS including Medicaid andthe private healthcare segments. So, wehave needed senior people withexperience and skills in those markets,we have ‘aimed high’
“An additional key factor for us isregulation. It can be a complex area. Inthe USA, regulation varies from state tostate, and in Europe from country tocountry
“We need people with a deepunderstanding of what’s needed tooperate in these markets.
“Without the right people in place,companies will make a lot of mistakes.”
The opportunities in the cross-overspace between therapy and technologyare substantial.
With one in four of us likely to sufferfrom mental illness in our lives, and agrowing focus on preventative medicinefor mental health issues, world-widedemand for online therapy is only likelyto grow.
For Mr Bennett-Coles, the lessonslearned by companies like TeraViewand Ieso Digital Health are vital for anyforward-thinking business in the field oflife sciences.
Without the right skills and the rightentrepreneurial spirit, teams will fail totake advantage of opportunities forexperimentation and growth, he says.
Future success starts with the visionaryleadership to build those teams.
SPECIAL FEATURE:Why life sciences innovators need
to build the right teams
An opinion piece
May 2017 volume 27 | No 3PHARMACEUTICAL PHYSICIAN 13

SPECIAL FEATURE:Burn Out?… Not Me, I’m Immune!
By Dr Catriona McMahon
DR CATRIONA MCMAHON IS A
SEASONED PHARMACEUTICAL
PHYSICIAN, EX MEDICAL DIRECTOR OF
ASTRAZENECA UK LTD AND NOW AN
EXECUTIVE COACH, FOCUSING ON THE
NEEDS OF HEALTHCARE AND LIFE
SCIENCE PROFESSIONALS. SHE HAS A
SPECIALIST INTEREST IN WORKING
WITH PEOPLE RETURNING TO WORK
AFTER, OR REMAINING AT WORKING
DURING ILL-HEALTH. FOR MORE
INFORMATION, VISIT WWW.TE-ARACOACHING.CO.UK
May 2017 volume 27 | No 3
14PHARMACEUTICAL PHYSICIAN
AND SO I thought ... until 2012, when Iburnt out; acute on chronic stress,followed by clinical depression. Bothhad a significant impact on myperformance … and my outlook on life.I recovered, slowly, and in doing so,found out so much about myself that Ididn’t know. And I discovered what itfeels like to ask for help, to have thathelp refused and survive, and to receivegenuine, compassionate assistance –three experiences that now shape myapproach to my life and career.
As for many executives who experiencestress and burn-out, the causes weremany, originating from both my workand personal life. Some I couldn’t haveinfluenced, for example the severe painfrom a frozen shoulder and subsequentsurgery; but one that I might have, if Ihad been able to recognise it, was thedevelopment of workplace stress. Whilstit may not have been in my power tochange the business asks, I now seethat it was within my power to changehow I was managing those projects andtasks … if I had recognised the slipperyslope that I was on. I wonder now howmany of my friends and colleagues sawthe signs, how many of them tried totell me? Did they not try, or did I notlisten when they did? You’d think I’dremember…
If I were to ask you how confident youare that you are not in a state of sub-clinical stress, at risk of burn out, whatwould your answer be? Oh, no, notme, I thrive on this stuff (my oldresponse); I don’t know, I’m not surewhat to look out for; or no, I’m good asI feel in control of how I carry out myresponsibilities, have a great supportsystem and know how to listen to those
who care? I hope you fall into the lattercategory!
This article is an introduction toworkplace stress, to burn-out. It is not ascientific review of the topic, but apersonal reflection; and hopefully aconversation starter. We cannot managemental health issues in the workplaceby hiding them behind closed doors, nomatter how much we are tempted totry.
Stress is an important cause of ill healthin the workplace and can havesignificant impact on businessproductivity. But what is workplacestress, what is burn-out? The officialdefinition of workplace stress is “aharmful reaction that people have toundue pressures and demands placedon them at work and includes stress,depression or anxiety[1]”. Using thisdefinition, workplace stress has anincidence rate of 6.9 per 1,000 UKworkers in 2015/16, resulting in 11.7million working days lost, equating toan average of 23.9 days lost perindividual. In 2014/15, 35% of all workrelated ill health and 45% of all workingdays lost due to ill health were due toworkplace stress[2]. So, this is a bigproblem; and there is some evidencethat our training[3] and ways ofworking[4], [5], may place physicians atgreater risk than some otherprofessions. I wonder how relevantthese data, gathered from physicians inclinical practice, are to us, physicians inPharmaceutical Medicine? Subjectively,I recognise the discussion and they feelrelevant to me.
However, I find the above definitionchallenging as I struggle to define
Dr Catriona McMahon

‘undue’; none of my 2012 objectiveswere unreasonable; all were, in theory,achievable and I had the skills andcapability to deliver. Knight, in a recentHarvard Business Review article, definesburn out as “the mental and physicalexhaustion you experience when thedemands of your work consistentlyexceed the amount of energy you haveavailable[6]”. This description I do
recognise as relevant, reflecting thecomplexity of my own personal/worksituation and the importance of energy;it also reflects the conversations that Ihave with pre-stress or stressedcolleagues and clients.
In today’s increasingly tough and fast-paced work environments, workregularly invades our homes - via ourgranting of discretionary hours, and ourresponsiveness (some would argueaddiction) to remote and mobiletechnology. This in itself is not ‘bad’;indeed, many of us choose to work thisway. No, it is how we manage ourselveswithin our chosen patterns of work-lifethat has the greatest impact on our riskof stress; and for most of us, we get the
balance right enough to ensure that ourenergies remain sufficient to meet thedemands upon us, most of the time ...
So, how can we recognise when we arenot getting the balance ‘right enough’and/or we are failing to tick the ‘most ofthe time’ box? What should we bewatching out for that could signal thatour balance is at risk of going off
balance? Could I have detected mystress before it reached the tippingpoint?
We all know the risk factors forworkplace stress: lack of control withinrole, whether real or perceived; unclearrole/project expectations; dysfunctionalworkplace dynamics; a mismatch invalues; and frequent extremes of activity– from monotony to chaos. Similarly, weare aware of the importance of goodsocial support and healthy work/lifebalance. Like you, I knew all of this, yetI still slipped into the chasm of stress.So what did I miss? Honestly? Nothing.It wasn’t that I missed the signs; no, Isaw the issues, the risks, and decidedthat they didn’t apply to me; that I was
strong, that I could cope, that I couldmake these situations work for me - andas a business executive, I believed thatit was expected of me to manage the‘ambiguity’, the ‘challenges’ facing me,often alone. This fog of highexpectation very efficiently hid thechasm from my view.
So, I’d decided that the risk factors werenot relevant to me – I was already half-blind; how about my recognition of theearly signs? Lee, Medford and Halim[7]
characterise burn out as emotionalexhaustion, depersonalisation and areduced sense of professional efficacy,with the first being considered theearliest and most important sign(Table 1).
I can safely say that I experienced allthree signs. I was aware that I wasbecoming less engaged with my role,with the exception of my continuedpassion for team and individualdevelopment. Importantly, I was nolonger recognising many aspects of myrole as a potential source of growth anddevelopment and was becoming unsureas to where I could add new and/oradditional value. Looking back, I nowsee this perception resulted from a
SPECIAL FEATURE:Burn Out?
… Not Me, I’m Immune!
May 2017 volume 27 | No 3PHARMACEUTICAL PHYSICIAN
Continues on page 16 ��
IF I WERE TO ASK YOU HOW CONFIDENT YOU ARE THAT YOU ARE
NOT IN A STATE OF SUBCLINICAL STRESS, AT RISK OF BURN OUT, WHAT WOULD
YOUR ANSWER BE?
15
| TABLE 1: Adapted from Lee, Medford and Halim[5]
Features Explanation
Emotional exhaustion Emotional depletion from being overworked
Depersonalisation A sense of being unfeeling towards colleagues or peers;often negative, callous and detached responses
Professional efficacy A reduced sense of competence or achievement in one’swork
SPECIAL FEATURE:Burn Out?
… Not Me, I’m Immune!
PHARMACEUTICAL PHYSICIAN
combination of exhaustion,depersonalisation as I unconsciouslytried to reduce demand upon me, andsome, though initially limited, insightinto the short-term consequences of mystate. Unfortunately, it sometimes takesmoments of crisis for true awarenessdevelop – and this was the case for me.
So, with all of this in mind, how canyou avoid developing workplace stress?
First, be open to the risk factors in yourenvironment – I am sure that you dothis for your colleagues and teammembers; remember that you deservethe same care and attention and do thesame for yourself.
Listen carefully to the messages thatyour body/mind is sending you. Restassured, if you miss the early signs, thegentle shot across the bows that youwill experience, a stronger message willbe sent as your body/mind finds a wayto stop you! Hopefully it will only be a“cold” that takes a few weeks to shift …
Next, don’t just hear the comments ofcolleagues, listen carefully. If you feelyourself getting defensive, pause andask the question, why? Considerwhether it is possible that theircommentary is coming from a place ofconcern and caring, and not a place ofcriticism. Perhaps it is professionalfeedback; or perhaps they have moreinsight into your state than you have?
If you find yourself being impatient,short or sharp; if you find that yourthinking is slowing down; if you feelunusual self-doubt; or if you realise thatyou are struggling - don’t try andresolve these challenges by workingharder. Find a trusted colleague andspeak to them about what you arefeeling. In this way, you will share,which will reduce your burden and willstart to build a support system aroundyou.
And don’t manage a slippingperformance on your own – work withyour manager, a mentor or a coach;
someone who can explore yourexperiences with you, help you broadenyour perspective and identify how toregain and retain your balance.
Finally, consider professional(counselling or psychotherapeutic) helpif you realise that you are on the wrongside of the tipping point – I promiseyou, the feelings of embarrassment orshame that you may experience as youask will not remain, and, mostimportantly, do not define who you arein any way.
My journey to recovery is my own, andas my purpose for this article is to pre-empt burn-out, I will not go into furtherdetail here – I am happy to share ifanyone wants to contact me and askmore. But I do want to share what thisexperience has taught me. Whilst Iwould not wish burn-out on anyone, Ifind that I have a deep sense ofacceptance and, perversely perhaps, joythat it happened to me – I am nowaware of me and the world around mein a way that I was not before; andperhaps in a way that I wouldn’t havediscovered if life had stayed the same.
First, I now listen to my body/mind. Iknow that if I don’t listen and pay dueregard, it will find more impactful waysto slow me down!
Second, I appreciate that it is impossibleto compartmentalise my home, family,personal and work lives away fromeach other. I exist in each one; in fact,often in more than one at any time.Work stressors affect home and familypeace and vice versa. Now, rather thancompartmentalise, I integrate.
Next, I engage with and listen to thecouncil of others. I had an amazingcouncillor whilst I was at my lowest,and a great Executive Coach as I movedinto recovery. Now, as a member of the‘helping profession’ of ExecutiveCoaching, I work with a Supervisor whoco-creates with me an environment thatencourages and supports reflection onmy performance, whilst considering my
May 2017 volume 27 | No 3
�� Continues from page 15
16

associated physical and mental health. Irecognise that the supervisionrelationship is different from themanager-employee relationship, but I dobelieve that it is possible to develop areflective relationship with yourmanager or a trusted colleague; and ifnot, then with a formal coach ormentor.
Fourth, I have stopped hiding behind‘doing’, being busy all of the time, andnow dedicate time to ‘being’, includinghaving an active mindfulness practice.This has been a very challenging changefor me, as like many people, the ‘doingof stuff’ has taken priority over my‘being’ needs for a long time, andkeeping busy was an important defensemechanism – it’s much easier to keep
going, than to stop, accept, inquire …and change if need be.
And critically, I now embrace the factthat I’m not omnipotent – I am ashuman as the rest of us, and accept thatmy intelligence, position and seniority inan organisation neither protect me normake me immune to that simple,beautiful fact.
Workplace stress is not a sexy topic, butit is an all-pervading issue in today’shigh impact, fast pace corporatecultures; nobody is truly immune. Ourindividual health is critical to the healthyfunctioning of our organisations –whether they be our employers or ourhome/families. Look after yourself andstay well!
SPECIAL FEATURE:Burn Out?
… Not Me, I’m Immune!
May 2017 volume 27 | No 3PHARMACEUTICAL PHYSICIAN 17
| REFERENCES1. Work related Stress, Anxiety and Depression Statistics in Great Britain 2016. Available
from: http://www.hse.gov.uk/statistics/causdis/stress/stress.pdf. Accessed 28/3/17
2. Work related Stress, Anxiety and Depression Statistics in Great Britain 2016. Availablefrom: http://www.hse.gov.uk/statistics/causdis/stress/stress.pdf. Accessed 28/3/17
3. Montgomery, A. (2014). The inevitability of physician burnout: Implications forinterventions. Burnout Research 1 (2014) 50–56. Available from:doi.org/10.1016/j.burn.2014.04.002. Accessed 8/6/16
4. Ariely, D. & Lanier, W.L. (2015). Disturbing trends in physician burnout and satisfactionwith work-life balance; dealing with a malady among the nation’s healers. Mayo ClinicProceedings, 90 (12), 1593-1596.
5. Brooks, S.K., Gerada, C. and Chalder, T. (2011) Review of literature on the mental health ofdoctors: Are specialist services needed? Journal of Mental Health, Vol. 20 (2) 146-156.
6. Knight, R. (2015). Stress: How to overcome burnout and stay motivated. Harvard BusinessReview Online, April (reprint H01ZFC). Accessed 8/6/16
7. Lee, Y.Y., Medford, A.R.L. and Haim, A.S. (2015). Burnout in physicians. Journal of the RoyalCollege of Physicians, Edinburgh, 45: 104–7.
…NOW EMBRACE THE FACT THAT I’M NOT OMNIPOTENT – I AM AS
HUMAN AS THE REST OF US…
SPECIAL FEATURE:
First medic
By Dr Michael Atkins
SOME GUIDANCE FOR A MEDIC
AFFAIRS MEDIC ENTERING A COMPANY
THAT NEVER HAD ONE
May 2017 volume 27 | No 3
18PHARMACEUTICAL PHYSICIAN
I AM NOT talking about replacing anexisting medic or acting as a consultantor interim, I am talking about acompany that has NEVER had apharmaceutical physician before andnow needs one full time. It would beindiscreet to say from which companiesI am sharing my experiences butexperiences they were! Anyway, hereare some points to think about.
This article does not discuss the role ofthe medic in Phase I or other aspects ofR&D. It is likely (if needed) suchindividuals will already be in place.
• Is it for you? The first BIG question iswhether you are right for the job andthe job is right for you. The sort ofcompanies needing a medic are likelyto have been start-ups that have R&Dexperience and that’s all. They may ormay not have got as far as usingregulatory professionals to begin amarketing authorisation process. Thechances are that they have discoverednew words like “Medical Affairs”,marketing and sales.
In my opinion, you would be a very bigstep to be a “first medic” unless you area final ABPI Code signature and aMedical Director (or at that level). Ifnot, I believe you may struggle and beout of your depth and unhappy. Firstmedics are the brave and theentrepreneurial. It carries risks (andgreat potential benefits). This role is notjust a stepping stone on apharmaceutical physician’s path to otherthings. Immediate career prospects inthis company are zero.
• Due your “due diligence”. What hasthe company got and why do they
need a Medical Affairs medic? Whatare their expectations of you? Onecompany had the bizarre idea I couldschmooze a competent authority toaccept data I was lead to believe(before I joined) was “robust”. Itwasn’t and I didn’t.
It is likely the company will have fewemployees and even fewer whoinvolved (if any) in medical affairs. Meetas many as you can and ask their viewsof the company and its people.Remember, with few key employees, ifsomeone leaves or goes off sick ormaternity/paternity leave, who is goingto cover. You?
• The “package”. You may be offered alow salary and generous share options(“scare options”?). This could be at thestart of your billion dollar lifestyle butcompanies can falter and you mayfind you have taken a drop in salaryfrom your previous job with that“golden carrot” they promised goingmouldy after 2 years. Even moreconcerning (alarm bells) if you areasked to forgo a salary as part of thestart-up/buy-in. I walked away fromthat particular “opportunity”.
Don’t expect all the normal big pharmatrappings –car/car allowance, phone,computer, private health, holidays etc.Small companies may provide these butnot at the level you may have beenused to.
• Resources. Being the first andprobably the only medic you may endup a one person band. No longer theluxury of Medical Information tocheck references or an administratorto help with your diary and travel
Dr Michael Atkins

plans – you are on your own. For theright candidate, that will be excitingbut for others it is becomes a stressfuladditional workload on all the otherthings they expect you to do - PhaseIII trials, key opinion engagement andmanagement, setting up and runningadvisory boards, developing trainingslides on the Code and products…shall I go on? You cannot delegate.Who will cover for you on holidays?What about IT support?
Don’t expect to be trained – you musttake that in hand yourself to keep up todate for your own GMC status. That iswhy this role is unlike to suit anyonewho is still in higher medical training.Your managing director will want youfocussed on the tasks at hand – yourtraining is not on his/her radar.
Many functions may be contractedin/out rather than on head count. Thatcan pose challenges if such functionsare not on site in terms of just poppingto their office for a quick chat about adelicate issue.
Also, beware of promises that they wantyou to “build a medical department”. Itmay well be true and a hook to get youin. However, will it be on Day 1 youfind such plans are linked to revenueyet to come? Remember, most youngbiotech/pharma companies are on whatis called a “cash burn” – they arespending to fund the projects yet to becommercially viable. What you mightassume as a necessity, they see as aluxury.
Do they know what they don’t knowabout the ABPI Code? Be prepared forcreating Code compliant SOPs and foran uphill course when helping withsales force training versus the wide eyedwishes of the CEO to make moneyquickly. MSLs are not super reps togain KOL access and talk off-label andtheir objectives must not be based oncall rates. The CEO needs to understandand accept that. Hence, you must beboth Code expert and a compliancemanager - two hefty tasks. The battles Ihave had getting a dedicatedCompliance Manager into a growingorganisation are many. Want to see thescars?
• Travel. Not just in the UK, but whatwill be the requirements of seeinginvestigators/KOLs abroad andattending international conferences.You may be expected to manpromotional stands as the residentmedical expert. I was once asked todo just that in the first week of joininga small company as a first medic – inSingapore. Travel and workcommitments may take their toll onhome life and seeing your childrengrow. I got my British Airways Goldcard in one month and after 8000miles air travel. During that time, Ionce fell asleep in my own lecture.Travel can be tiring.
• Are you tough minded? Being theonly medic will mean you makingsome big decisions without a mentor.Can you stand your ground? Can younegotiate? You will need to engager
trust and respect and that is not doneby just being nice and saying yes allthe time.
• Is it a therapy are you know? – Ifyour background is ophthalmologyand a start-up company wants tolaunch a new product in glaucoma,this may be your chance to make areal impact. The company will wantyou to hit the ground running and thatmay include contact with your ownprecious KOL network.
• Map out your tenure. The CEO willwant to see your plans mapped outaccording to his requirements. Berealistic. Rome was not built in a day.
• Matrix management. All yourmanaging skills will be needed toguide the company along a MedicalAffairs journey. Some concepts will bealien to them or (worst still) they thinkthey know what is best. Explain yourintended actions rather than defendthem afterwards.
• Become a Mr/Ms fix-it. There is agreat opportunity to shape a growingorganisation as a medic. With yourprevious experience, you can show
SPECIAL FEATURE:First medic
May 2017 volume 27 | No 3PHARMACEUTICAL PHYSICIAN
Continues on page 20 ��
BEING THE ONLY MEDIC WILL MEAN YOU MAKING SOME BIG
DECISIONS WITHOUT A MENTOR
19

SPECIAL FEATURE:First medic
them how best to do it. They do nothave to invent square wheels andwaste time and resources in theprocess. However, you must notassume a mantle of infallibility. Withyour confidence, you can share areasof doubt and uncertainly whilst stillsuggesting options and the best courseto take – that shows you are incontrol.
• Things happen quickly. In one role Irecall suggesting to the ManagingDirector we should create a corporatebrochure – nothing fancy, but to setout our stall. He smiled and said “itwill be out of date in 6 weeks”. Badthings can also happen quickly.Following a Board Room coup, a newCEO was put in place – one of thetruly nastiest people I have ever hadthe misfortune to work under. I leftsoon afterwards.
• Keep commination short and clear • Talk to people: - Do you really
need to send that email to one
person and that person is sittingnext to you?
• Emails: - Short, relevant and few.Make sure you file them for easyretrieval.
• Meetings:-Short, relevant, and few.The agenda and minutes shouldoccupy just one page. Action points- clear, dated and named.
• Reports: - Short, relevant, and few.Send a one page monthly report toyour boss about what you havedone, and ongoing issues. This alsoforms part of your CPD/revalidationfile.
• Gut instinctsHaving taken all into consideration,what do your instincts tell you aboutthat job – are you excited or worried?For the right medic, being a first can bea life changing step. Go for it?
�� Continues from page 19
PHARMACEUTICAL PHYSICIAN CONTACT: Liz [email protected] 0118 934 1943
Advertise here or on the BrAPP website.
Reachyour target
market
Continuing delegates who have just completed YEAR 1 should re-register and taught modules recommence in October 2017.
New registrations for this academic year can be accepted at any time but places are limited to 25 attendees and taught moduleswill commence in January 2018.
The Course follows the syllabus for the Diploma in Pharmaceutical Medicine. Each session is of two working days’ duration.
Session 1 is conducted in Cardiff at the University but the remaining 9, including a tailored Revision session, are delivered inLondon in a modern purpose-designed, well-resourced training venue. The Course is not residential and many attendees living inand around London have found daily attendance easy and better for their own quality of life.
The course has undergone serious remodelling over the past two years to enhance delivery and ensure busy candidates andpharmaceutical physicians in training can learn constructively and proactively.
CARDIFF UNIVERSITY/BRAPP
POSTGRADUATE COURSE IN PHARMACEUTICAL MEDICINEAcademic year 2017/2018BrAPP is pleased to announce that we are now accepting registrations for thePostGraduate Course in Pharmaceutical Medicine (PGCPM).
For further details:please visit the BrAPP website www.brapp.org and use the PGCPM button
and to register, please call the BrAPP office on +44 (0) 118 934 1943and speak to Liz Langley. Email [email protected]
RETRO FEATURE: Pills, probabilities and precaution Reprinted from January 2008
Professor Stephen Senn.
Professor Senn
FIRST PUBLISHED IN PP IN JANUARY
2008, GIVEN RECENT EVENTS, ITBEARS RE-READING AND FURTHER
CONSIDERATION TODAY.
ALTHOUGH YOU DON’T NEED
STATISTICS TO TELL YOU THAT
SOMETHING IS WRONG WHEN FACED
WITH TERRIBLE OUTCOMES, YOU NEED
DATA, CALCULATION AND RISK
ASSESSMENT, IN SHORT STATISTICS, TO
HELP YOU PLAN SO THAT THINGS
DON’T GO WRONG AND YOU ALSO
NEED STATISTICS TO ANALYSE THE
DATA WHEN THEY GO RIGHT.
May 2017 volume 27 | No 3
22PHARMACEUTICAL PHYSICIAN
TRIALS AND TRIBULATIONSON 13 MARCH 2006 EIGHT HEALTHYyoung men entered a clinical trial ofTeGenero’s monoclonal antibodyTGN1412. Within 16 hours at the mostall six who had been given the activetreatment were in intensive care atnearby Northwick Park Hospital andbeing treated for the symptoms of asevere ‘cytokine storm’. These dramaticevents received extensive news mediacoverage around the world and haveprobably changed for ever our attitudeto running so-called ‘first in manstudies’.
The trial was planned to be a groupedescalation study with eight healthyvolunteers in each step, six of whomwere to be allocated the given dose ofTGN1412 and two of whom would begiven placebo. As it turned out, ofcourse, there was no escalation: the trialwas stopped at the first hurdle and inconsequence its results can besummarised as in Table 1 below.
Anyone with even an amateurknowledge of statistics, will recognisesuch a table as being a contingencytable and know that where thefrequencies are as low as this, acommon analysis is Fisher’s exact test.
Actually, Fisher’s exact test yields avery modest one-sided P-value of0.0357, which is not significant by theconventional standards of drug-development, which requires a one-sided P-value of no more than 0.025to declare significance in any giventrial.
Clearly this common formal analysisdoes not begin to do justice to theevidence. I am convinced that everyreader of Pharmaceutical Physician isconvinced with me that TGN1412caused the adverse events in this trial.What is the origin of our commonconviction?
One explanation is that such an analysistakes no account of backgroundknowledge that cytokine storms areextremely rare. The placebo group is avery small control group and if we baseour knowledge of the probability of anadverse reaction in the absence oftreatment on the results for the twosubjects given placebo alone, then theuncertainty in estimating thisbackground rate is so large that ittranslates into an uncertainty about theresults of the trial. This is illustrated byfigure 1, which shows the probability ofthe results of the trial as a function of a
| TABLE 1: Outcome of the TeGenero trial
CYTOKINE STORM?
Yes No Total
Treatment TGN1412 6 0 6
Placebo 0 2 2
Total 6 2 8
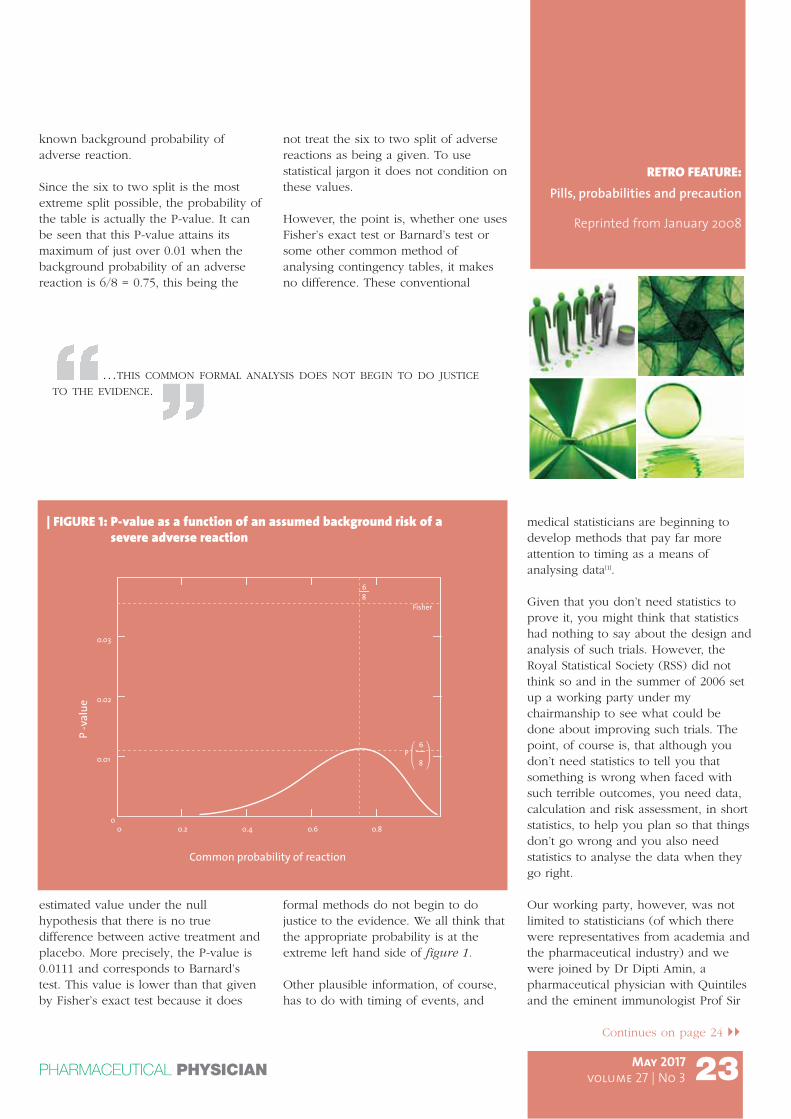
known background probability ofadverse reaction.
Since the six to two split is the mostextreme split possible, the probability ofthe table is actually the P-value. It canbe seen that this P-value attains itsmaximum of just over 0.01 when thebackground probability of an adversereaction is 6/8 = 0.75, this being the
estimated value under the nullhypothesis that there is no truedifference between active treatment andplacebo. More precisely, the P-value is0.0111 and corresponds to Barnard’stest. This value is lower than that givenby Fisher’s exact test because it does
not treat the six to two split of adversereactions as being a given. To usestatistical jargon it does not condition onthese values.
However, the point is, whether one usesFisher’s exact test or Barnard’s test orsome other common method ofanalysing contingency tables, it makesno difference. These conventional
formal methods do not begin to dojustice to the evidence. We all think thatthe appropriate probability is at theextreme left hand side of figure 1.
Other plausible information, of course,has to do with timing of events, and
medical statisticians are beginning todevelop methods that pay far moreattention to timing as a means ofanalysing data[1].
Given that you don’t need statistics toprove it, you might think that statisticshad nothing to say about the design andanalysis of such trials. However, theRoyal Statistical Society (RSS) did notthink so and in the summer of 2006 setup a working party under mychairmanship to see what could bedone about improving such trials. Thepoint, of course is, that although youdon’t need statistics to tell you thatsomething is wrong when faced withsuch terrible outcomes, you need data,calculation and risk assessment, in shortstatistics, to help you plan so that thingsdon’t go wrong and you also needstatistics to analyse the data when theygo right.
Our working party, however, was notlimited to statisticians (of which therewere representatives from academia andthe pharmaceutical industry) and wewere joined by Dr Dipti Amin, apharmaceutical physician with Quintilesand the eminent immunologist Prof Sir
RETRO FEATURE:Pills, probabilities and precaution
Reprinted from January 2008
May 2017 volume 27 | No 3PHARMACEUTICAL PHYSICIAN
Continues on page 24 ��
23
| FIGURE 1: P-value as a function of an assumed background risk of asevere adverse reaction
0 0.2 0.4 0.6 0.80
0.01
0.02
0.03
68
Common probability of reaction
P -v
alue
Fisher
P6
8
…THIS COMMON FORMAL ANALYSIS DOES NOT BEGIN TO DO JUSTICE
TO THE EVIDENCE.
RETRO FEATURE: Pills, probabilities and precaution
Reprinted from January 2008
PHARMACEUTICAL PHYSICIAN
Peter Lachmann, FRS, FMedSci, emeritusprofessor at Cambridge. We reported on13 March 2007, a year to the day afterthe trial of TGN1412, and our report isavailable from the RSS, in its journal[2]
and also on its website.
DATA DIFFICULTIESOne of our first tasks was to try toestablish what was known about therate at which severe adverse reactionsoccurred in first-in-man studies. To thisend we placed a freedom ofinformation act request with the MHRA.Initially this was refused but eventuallywith the kind help of Dr Martyn Wardof the MHRA we were provided withthe limited information that the MHRAhad.
Table 2 summarises the phase 1 trials bytype of investigational medicinalproduct (IMP), that is to say whether‘biological’ or ‘chemical’, and by type ofsubject, patient or healthy volunteer,that has been authorised by MHRAduring the period September 2004 toend of May 2006 inclusive.
Prior to the trial of TGN1412 thesestudies had yielded no adverse reactionsof similar severity but theses data onlyrepresent a fraction of those that wouldbe available had a policy of routinelylogging such information been in placemuch earlier. Of course one can alwaysregret that data were not routinelycollected earlier but InternationalConference on Harmonisation (ICH)guidelines instructing sponsorsregarding presentation of safety data
date back to the mid 1990s and these ofcourse reflect much earlier standardsfrom the three ICH regions so that it isdisappointing to find that more had notbeen undertaken by regulators.
Of course, hindsight is an exact science,and whatever the explanation of thedifficulty with which one can obtainstatistics on safety, a keyrecommendation of our report is thatdrug regulatory agencies shouldorganise themselves to collect data onadverse reactions in phase I trials. Thisis a field in which data need to bepooled between sponsors and thus itseems logical that regulators should takea lead.
ACCEPTABLE RISKSOf course, one wants not just to havereliable data on risk but to reduce thatrisk to an acceptable level. What isacceptable? Clearly to take the attitudethat only zero risk is acceptable wouldmean that no phase I trials could everbe carried out. We felt that two mattersneed to be considered: that which isacceptable to the individual and thatwhich is acceptable to society.
To understand the difference betweenthe two suppose that we decided thatno individual should run a risk of morethan 1 in 2000 of a severe adversereaction but that our best assessment ofthe risk for a given treatment was 1 in a1000. This is too high to study.However, suppose that healthyvolunteers are randomised with equalprobability to either placebo or
May 2017 volume 27 | No 3
�� Continues from page 23
24
| TABLE 2: Phase 1 trials authorized by the MHRA, September 2004 toend May 2006 by Investigational medicinal product (IMP)
TYPE OF SUBJECT
Type of IMP Patients Healthy Volunteers Total both type ofsubject
Biological 26 (28%) 66 (72%) 92 (100%)
Chemical 82 ( 9%) 842 (91%) 924 (100%)
Total both types IMP 108 (11%) 908 (89%) 1016 (100%)

treatment. The risk is now 1 in 2000.Does this make it acceptable? We thinknot and one way of arguing why not isto say that the expected number ofadverse reactions in a given trial is notreduced by adding subjects givenplacebo, although the risk to any subjectis reduced.
However, this line of argument can alsobe turned the other way around. Amuch criticised feature of the trial ofTGN1412 was that subjects were treatednearly simultaneously. Thus, aconsequence was that six sufferedadverse reactions rather than the onewho might have had a sufficient dosinginterval been observed. Such anapproach would have been morecautious and more acceptable in terms
of society’s risk. Indeed on of therecommendation of our report is that a‘proper interval’ for dosing subjectsshould be established for everytreatment and observed whenconducting first-in-man studies.However, even had this precaution beenobserved, somebody would still have tohave been first, so that the risk to thatindividual is also important.
DETERMINING RISKMany readers will no doubt say that thisis all very well but hopelessly academic.The risks can’t be determined and ifthey could, no-one could agree whatwas acceptable. We think this is toopessimistic. Individuals take risks all thetime and must make some sort ofassessment of them and unique eventsare also insurable. Several of ourrecommendations address this issue.
First we, recommend that a separatedocument expressing a formal riskassessment be produced prior to first-in-man studies. We believe that theexercise of having to commit to papercalculations of risk, however imperfect,will help improve risk assessment.
We also recommend that insurance forsuch studies should be mandatory andeffective. The TGN1412 study wasinsured but insurance has turned out tobe inadequate. One of the reasons isthat the design led to six simultaneousclaims rather than one. Clearlysomebody somewhere got thecalculations wrong. Had they beenavailable in a formal assessment itwould be easier to eliminate sucherrors.
We also think that there should be amore frank exchange of informationbetween all parties. The standard to beobserved is that of ‘open protocolhidden allocation’. That is to say alldetails of how the design will be run,including the allocation andrandomisation scheme to be employedshould be open to all, especially would-be subjects of the trial, and only whereblinding is required should the actualallocation be concealed.
It may seem again that this is a trivialand obvious point but first this standardis regularly violated in clinical trials inall phases of development employingplacebo run-ins[3, 4] and secondly theEuropean Medicines Agency’s (EMEA)own response to the TGN1412 story failsto address the issue of informedconsent[5].
DESIGNING BETTERFinally, it is perhaps worth mentioningthat since first-in-man studies are runwith the expectation, thank goodness,that severe adverse reaction will notoccur they also have to be designed todeliver good information when thingsdon’t go wrong. It is importanttherefore, that designs and plans foranalysis are good. This is precisely whyit is not an excuse to say, that for datasuch as those provided by the trial ofTGN1412 you don’t need statistics. Thepoint is that in embarking on such atrial you don’t expect that somethinglike that will happen but can neverexclude that it might so that the onlyjustification for such a risk being run isthat the data will be collected andanalysed in a way that is capable ofyielding useful information when thingsdon’t go wrong
Here we feel that the drug developerscould do much better. The protocol ofTGN1412 was extremely hazy aboutexactly how whatever information it wasdesigned to collect would be obtainedand analysed. In this respect it is nodifferent from scores of other trialsbeing run. We make a number ofrecommendations about approaches to
RETRO FEATURE:Pills, probabilities and precaution
Reprinted from January 2008
May 2017 volume 27 | No 3PHARMACEUTICAL PHYSICIAN
Continues on page 26 ��
THE RISK IS NOW 1 IN 2000. DOES THIS MAKE IT
ACCEPTABLE?
25
RETRO FEATURE: Pills, probabilities and precaution
Reprinted from January 2008
PHARMACEUTICAL PHYSICIAN
trial design and analysis depending onwhat effects can be assumed to bepresent or absent. Just to give a simpleexample, the fact that the allocationratio of six to two active to placebo wasproposed for dose escalation steps inthe TGN1412 study only makes sense ifplacebo results are to be pooled at theend of the trial but this in itself onlymakes sense if first, trend effects areassumed to be small and second one isconfident that the end of the trial willbe reached. But this latter step is farfrom guaranteed, even when theoutcome is not as catastrophic as wasthe case with this trial. We are notsuggesting that assumptions about trendeffects are not reasonable but we dofeel that they should be addressed inany protocol. In fact, we are feel that itis time that we took the business ofplanning and analysing phase one
studies as seriously as we do phasethree studies.
This is not to say that the sametechniques will be appropriate for phaseI as for phase III studies but it is to saythat the same degree of care andattention will be required.Unfortunately, it seems, whatever wehave learned from the tragic events ofMarch 2007, we are still in danger offalling short in the degree of scientificrespect we accord first-in-man studies.
ACKNOWLEDGEMENTI am extremely grateful to my colleagueson the working party for all their help inproducing our report. This article reflectsmy personal views.
Stephen Senn is Professor of Statistics,University of Glasgow
May 2017 volume 27 | No 3
�� Continues from page 25
| REFERENCES1. Farrington, CP, Whitaker, HJ. Semiparametric analysis of case series data (with discussion),
Journal of the Royal Statistical Society Series C-Applied Statistics 2006; 55: 1-28.
2. Senn, S, Amin, D, Bailey, RA, Bird, SM, Bogacka, B, Colman, P, Garrett, A, Grieve, A,Lachmann, P. Statistical issues in first-in-man studies, Journal of the Royal StatisticalSociety Series a-Statistics in Society 2007; 170: 517-579.
3. Senn, SJ. Are placebo run ins justified?, British Medical Journal 1997; 314: 1191-1193.
4. Senn, SJ. The Misunderstood Placebo, Applied Clinical Trials 2001; 10: 40-46.
5. O'Donnell, P. Not yet the last word on first-in-man, Applied Clinical Trials 2007.
26

May 2017 volume 27 | No 3PHARMACEUTICAL PHYSICIAN
LETTERS:
Reprinted from March 2008
FROM: PROFESSOR SIR PETER
LACHMANN
THURSDAY, 24 JAN 2008
SUBJECT: PILLS, PROBABILITIES AND
PRECAUTIONS. PROFESSOR SENN,PHARMACEUTICAL PHYSICIAN 2008;18:(5): P 6-10
27
“MADAM, I WOULD LIKE TO ADD just one point to Stephen Senn'sexcellent account of the TGN1412monoclonal antibody "first in man"study which went so badly wrong.
There are "obvious" uses of amonoclonal antibody where theanticipated effects result directly fromagonism or antagonism of the antibody'sligand; or from antibody-mediated cellkilling or phagocytosis. There are also"non-obvious" uses where the effectsare the result of more complicatedchains of events. These "non-obvious"applications are inherently morehazardous and they require moreintensive preclinical study and an evenmore cautious introduction into humanuse than is required for "obvious" uses
TGN1412 is a "superagonist" antibody toCD28, a stimulatory receptor widelydistributed on T-cells. The "obvious"function of this antibody wouldtherefore be to give rise to widespreadT-cell activation. The purpose for whichit was being developed was howeverthe selective activation of regulatory T-cells which inhibit effector T-cellactivation. The mechanism proposed bythe investigators for this selectivity isthat initial stimulation of all CD28+ve T-cells causes effector T-cells to secreteIL-2. This then binds CD25 (an IL-2receptor) on the regulatory T-cellswhich, together with the superagonistanti-CD28, gives them such a powerfulactivation stimulus that they can controlthe stimulated effector T-cells. This is anexcellent example of a "non-obvious"application.
This mechanism must depend on thebalance between the number of effector
T-cells on the one hand and thenumber of CD25-positive regulatory T-cells on the other so that the amount ofIL-2 produced is sufficient to stimulatethe regulatory cells but not so large asto cause systemic toxic reactions, andthat the number of regulatory T cells issufficient then to control the activity ofthe effector T-cells. It would not besurprising that this balance is favourablein one species and not in another; andin a single species such as humans, itmay be affected by age, sex, clinicalstatus, the presence of infection or of anacute phase state or other factors. Withhindsight it is clear enough that a moredetailed preclinical analysis would havebeen a good idea.
It would however be unfortunate if theunhappy experience with an"unobvious" application were to placeundue barriers in the way of developing"obvious" therapies with monoclonalantibodies and thereby delay theintroduction of valuable therapies.TGN1412 itself might still find a usefulrole as a therapy for reversing T-cellfailure in the elderly - which would bean "obvious" indication."
Sir Peter Lachmann, Sheila Joan SmithProfessor Emeritus of Immunology,University of Cambridge
NEW MHRA INSPECTORATEBLOGFrom: Medicines and Healthcareproducts Regulatory Agency
THE MHRA INSPECTORATE blog isaimed at those organisations that areinspected by MHRA and need to keepup to date with the latest thinking andguidelines. View the MHRA Inspectorate blog
It will give our inspectors a chance tospeak directly to the organisations theyinspect and get feedback from them ontopics they would like to hear moreabout. Areas the blog will coverinclude:• compliance management approaches• data integrity• preventing drug shortages• significant findings from our
inspections• supporting innovation and our work
with the MHRA Innovation Office • upcoming learning opportunities
The first article, from Mark Birse, GroupManager of the Inspectorate at MHRA,introduces the exciting new platform
and gives users an idea of what toexpect from the blog. Mark says:
A large part of our role in the MHRAInspectorate involves engaging with ourmany stakeholders. This new platformgives us an excellent opportunity to talkdirectly to those stakeholders in a lessformal way and help them maintaincompliance and engage with us onissues that are important to them.
It will also give stakeholders andopportunity to give us their thoughtsand comments and will encourage abeneficial two-way conversationbetween us at MHRA and those workingin industry and academia.
■
MHRA Inspectorate Group ManagerMark Birse speaking at an event
NEWS
From: Medicines and Healthcare products Regulatory Agency
May 2017 volume 27 | No 3
28PHARMACEUTICAL PHYSICIAN





























