Embed Size (px)
Citation preview

South East London Cancer Network
Management of cancers of
the colon, rectum and anus
06 November 2012
1
Document Control
Role
Organisation Name Date received
Consultant Surgeon GSTT Mr Mark George May / July 2012
CNS SLH Collette DeSilva June 2012
CNS Kings Stella Beazley July 2012
CNS GSTT Claire McGilly July 2012
Consultant Oncologist GSTT Dr Andrew Gaya August 2012
CNS Lewisham Claire Coughlan August 2012
CNS PRUH Collete De Silva September 2012
TWG sign off
September 2012
Contents
Preface 2
Network Hospitals & Staff 5
Colorectal Cancer Summary 13
Referral Form 15
Pathway 19
Colon Cancer 21
Rectal Cancer 23
Anal Cancer 29
Colorectal Surgery 31
Imaging 33
Histopathology 35
Emergency Presentation of Colorectal Cancer 41
Review After Persumed Curative Surgery 45
Metastatic Colorectal Cancer 47
Local Recurrence 49
Adjuvant Therapy 51
Family Cancer Screening 53
Colorectal Polyp Management 54
Audit & Research 55
Three year service delivery plan 58
Palliative Care 61
HPB Guidelines 65 Introduction 66
Referral guidelines 66
Imaging guidelines 66
Pre-operative evaluation 67
Surgical planning 67
Additional strategies to aid resectability 67
Radio-frequency ablation (RFA) 68
Synchronous liver lesions 68
Liver and pulmonary metastatic disease 68
Resection with (neo)-adjuvant chemotherapy 68
Guidelines for combined HPB and other surgical interventions 69
Pathology 69
Oncology (including clinical trials) 70
Follow-up 70
All HPB malignancies: inoperable/ palliative care 72

- 2 -
Preface
The aim of the colorectal teams in South East London is, quite clearly, to improve the outcome in patients with cancers of the colon, rectum and
anus. The role of the tumour working group is to establish that the practices required to achieve this occur throughout the group. The
integration of cancer services across the group will provide better local services for patients whilst ensuring access to specialist treatment when
required.
All patients should have access to all the treatment methods from which they may benefit. Therefore, we have to demonstrate that through the
group there is agreement on how the colorectal cancer service should be provided and provide evidence that what should happen does happen.
The exact service provision may vary between hospitals but the minimum requirement is described here.
The management of colorectal cancer will change as time goes by and this book will change to reflect this. The guidelines for the management
of colorectal cancer are based on various booklets produced over the last few years by the NHS executive1 and the Association of
Coloproctology of Great Britain and Ireland2. This book therefore is in three sections:
• operating policy for the multidisciplinary management of colorectal cancer
• annual report describing what has been achieved in 2010 and the three-year plan.
• summary of the 2007 peer review requirements highlighting those that have not been met
Terms of reference
Our specific aims are therefore to:
• review the NICE Improving Outcomes Guidance to improve patient care
• review the national guidelines
• develop local guidelines for patient care
• ensure compliance with guidelines
• establish the impact of guidelines on staff, access and equipment to identify gaps in the service
• prioritise targets and service improvements
• review quality measures and identify gaps and tackle these so that peer review is successful
• ensure compliance in data collection
• agree network-wide audits each year, ensure audits are completed, discussed and action required implemented across the network
• review new trials and encourage entry into trials
• review critical incidents and complaints reported to the network
• review attendance at team meetings
• select a ‘clinical champion’ for service improvement
• develop a network approach for patient information
• involve patients in service development
• develop a training and education programme for all members and disciplines
• contribute to the network annual report
1 Improving outcomes in colorectal cancer: The manual. Department of Health 1997. 2 Guidelines for the management of colorectal cancer. The Association of Coloproctology of Great Britain and Ireland. 2001.

Tumour working group membership
The members of the group that have attended the meetings of the group in the last two years are:
Cerena Barnett Nurse Specialist Queen Elizabeth Hospital
Stella Beazley Colorectal Nurse Specialist King’s College Hospital
Mr David Birch Colorectal surgeon Lewisham Healthcare Trust
Miss Clare Byrne Colorectal surgeon Lewisham Healthcare Trust
Dr Guy Chung-Faye Consultant Gastroenterologist Kings College Hospital
Claire Coughlan Nurse specialist University Hospital Lewisham
Roni Cummings Nurse Specialist Guy’s & St Thomas Hospital
Jacqueline Denton Nurse specialist Princess Royal University Hospital
Collette De Silva Nurse specialist Princess Royal University Hospital
Dr Neville Fernandez GP Lambeth PCT
Dr Andrew Gaya Clinical Oncologist Guy's & St Thomas' Hospitals
Mr Mark George Colorectal surgeon Guy’s & St Thomas’ Hospital
Mr Amyn Haji Colorectal surgeon Kings College Hospital
Mr Asif Haq Colorectal Surgeon King’s College Hospital
Prof Nigel Heaton HPB Surgeon King’s College Hospital
Lynne Higgins Colorectal Nurse Specialist King’s College Hospital
Dr Louise Izatt Geneticist Guy’s and St Thomas’s Hospital
Nikie Jervis HPB Nurse Specialist King’s College Hospital
Mr Hamid Khawaja Colorectal surgeon Queen Mary’s Hospital & Princess Royal University
Dr Martin Leslie Clinical oncologist Guy’s and St Thomas’s Hospital
Miss Jane Linsell Colorectal surgeon Lewisham Healthcare Trust
Gary Logue Nurse specialist Lewisham Healthcare Trust
Dr Nick Maisey Medical oncologist Guy’s and St Thomas’s Hospital
Claire McGilly Nurse Specialist Guy’s and St Thomas’s Hospital
Mr Savvas Papagrigoriadis Colorectal surgeon King’s College Hospital
Mr John Payne Colorectal surgeon Queen Mary’s Hospital
Mr Andreas Prachalias HPB Surgeon King’s College Hospital
Prof Mohamed Rela HPB Surgeon King’s College Hospital
Dr Paul Ross Medical oncologist Guy’s and St Thomas’s Hospital
Dr Nigel Sykes Consultant in Palliative Care St Christopher’s Hospice
Naomi Sheeter Service Manager (HPB & Colorectal) King’s College Hospital
Mr Frank Smedley Colorectal surgeon Princess Royal University Hospital
Emily Webster Business Manager, Specialist Medicine Lewisham Healthcare Trust
Melanie Welch Nurse specialist Queen Elizabeth hospital
Alastair Whittington Network Director SELCN
Mr Chui Yiu Colorectal surgeon Queen Elizabeth Hospital
These guidelines have been agreed by the group.
Mr Asif Haq
Chairman
- 3 -


5
The Network: Hospitals & staff
The South East London Cancer Network (SELCN) comprises six hospital trusts (in alphabetical order) :
• Guy’s and St Thomas’s Hospital
• King’s College Hospital
• Princess Royal University Hospital*
• Queen Elizabeth Hospital*
• Queen Mary’s Hospital*
*South London Healthcare NHS Trust
• Lewisham Healthcare Trust
The details of the core team members and the clinics held are in the following tables with one page for each of the six Trusts in the network.
Chair
The chair of the group is elected 2 yearly. The roles of the chairman include:
1 Management of the group
a. ensure the group fulfils the terms of reference
b. co-ordinate the work of the group with a clinical governance framework and an annual plan to achieve targets
c. oversee the agenda, minutes and meetings
d. represent the group on the Network Clinical Governance Group
e. attend relevant specialist network meetings
f. oversee the submission to the annual report
g. contribute to regular network updates
2 Strategic development
a. ensure the group reviews draft guidelines (such as NICE) working with the network management to influence development
of guidelines
b. ensure the groups reviews new guidance for service provision and develops options for service delivery with the group
c. ensure the group provides representation on the appraisal and implementation groups
d. co-ordinate the production of network-wide recommendations on implantation of appropriate national guidelines
e. co-ordinate the development of management pathways for patients and ensure the compliance of the group in this and
identifying inequalities in service provision
f. ensure that the implications of guidelines on staffing, education and resources are made available to the network
g. ensure the network is informed of deficiencies in the service against published quality measures and that action is taken to
address this
h. ensure the group contributes to network strategies for prevention, screening, diagnosis, treatment and palliative care
i. ensure the participation in network wide data collection
j. ensure the group has a plan of network-wide audits with dissemination of the results and action when required in terms of
service and education
k. ensure the group participates in network-wide clinical governance
l. ensure the group participates in CSC IP
m. ensure the group has a network wide approach to patient information
n. ensure the group supports the SE London cancer Research Network and entry of patients into trials
o. ensure the group develops mechanism for involving users in its work
3 Accountability
a. the chairman is accountable to the clinical director of the network and to inform the director on progress and any issues of
concern so that the network management team can provide support
Attendance at meetings
The attendance at the network meetings by each member of the group is recorded.
6
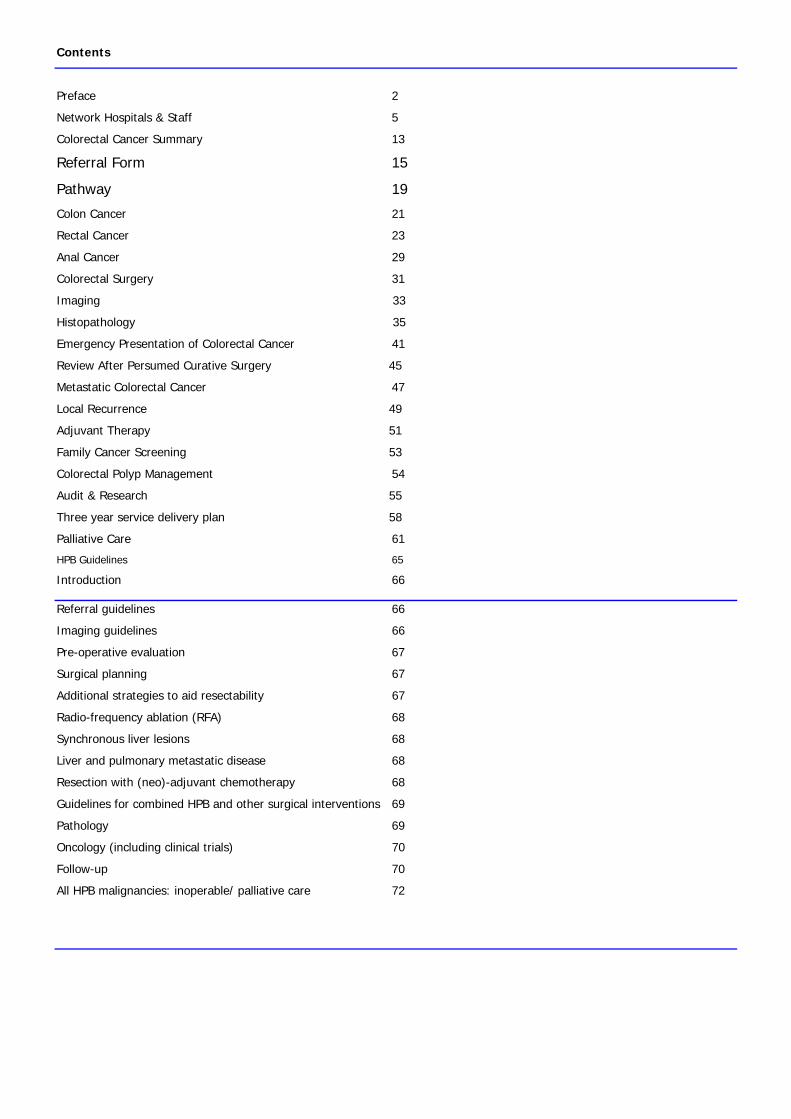
Guys and St Thomas’ Hospitals
Name Contact details
Mr Mark George (lead clinician) Tel: 020 7188 2569 [email protected]
Mr Viveck Datta TBA
Mr Andrew Williams Tel: 020 7188 2576 [email protected]
Mr Emin Carapeti Tel: 020 7188 2569 [email protected]
Mr Amir Darakhshan Tel:020 7188 2576 [email protected]
Surgery
Mr Alexis Schizas (Locum) Tel: 020 7188 2576 [email protected]
Dr Simon Anderson 020 7188 2496 [email protected] Gastroenterology
Dr Michelle McCarthy Tel: 020 7188 7627 [email protected]
Dr Paul Ross (Medical Oncologist)
Dr Nick Maisey
Tel: 020 7188 4249 [email protected]
Tel. 0207188 3761 [email protected]
Oncology
Dr Martin Leslie Clinical Oncologist)
Dr Andrew Gaya
Tel: 020 7188 4247 [email protected]
Imaging Dr Giles Rottenberg Tel: 0207 188 5558 [email protected]
Dr Hattie Deere Tel: 0207 188 2927 [email protected]
Dr Ula Mahadeva Tel: 020 7188 2934 [email protected]
Dr Fuju Chang Tel: 020 7188 2925 [email protected]
Pathology
Dr Simi George Tel: 020 7188 2917 [email protected]
Roni Cummings Tel: 020 7188 2564 [email protected] Colorectal nurse specialist
(responsible for user issues and
patient & carer information) Claire McGilly [email protected]
Margaret Northover Tel:020 7188 6469 [email protected] Stoma Therapists
Andrew Boddington Tel:020 7188 6469 [email protected]
Meeting co-ordinator Dawn Marshall Tel: 020 7188 2696 [email protected]
Clinic type Staff Day Location
Monday afternoon (alternate) St Thomas
Tuesday morning (alternate) Guy’s
Mr George
Wednesday afternoon Guy’s
Monday afternoon (alternate) St Thomas
Tuesday morning (alternate) Guy’s
Mr Williams
Wednesday afternoon St Thomas’ / Guy’s
Tuesday morning St Thomas’ Mr Carapeti
Wednesday afternoon (alternate) St Thomas’
Monday morning St Thomas’
Wednesday afternoon (alternate) Guy’s
Mr Datta
Thursday morning St Thomas’
Mr Darakhshan Monday and Tuesday (alternate)
Colorectal surgery
Mr Schizas Wednesday
Cancer Follow Up Roni Cummings Wednesday afternoon Guy’s
Oncology Dr Paul Ross, Dr Nick Maisey,,
Dr Martin Leslie & Dr Andrew Gaya
Tuesday morning St Thomas’
7
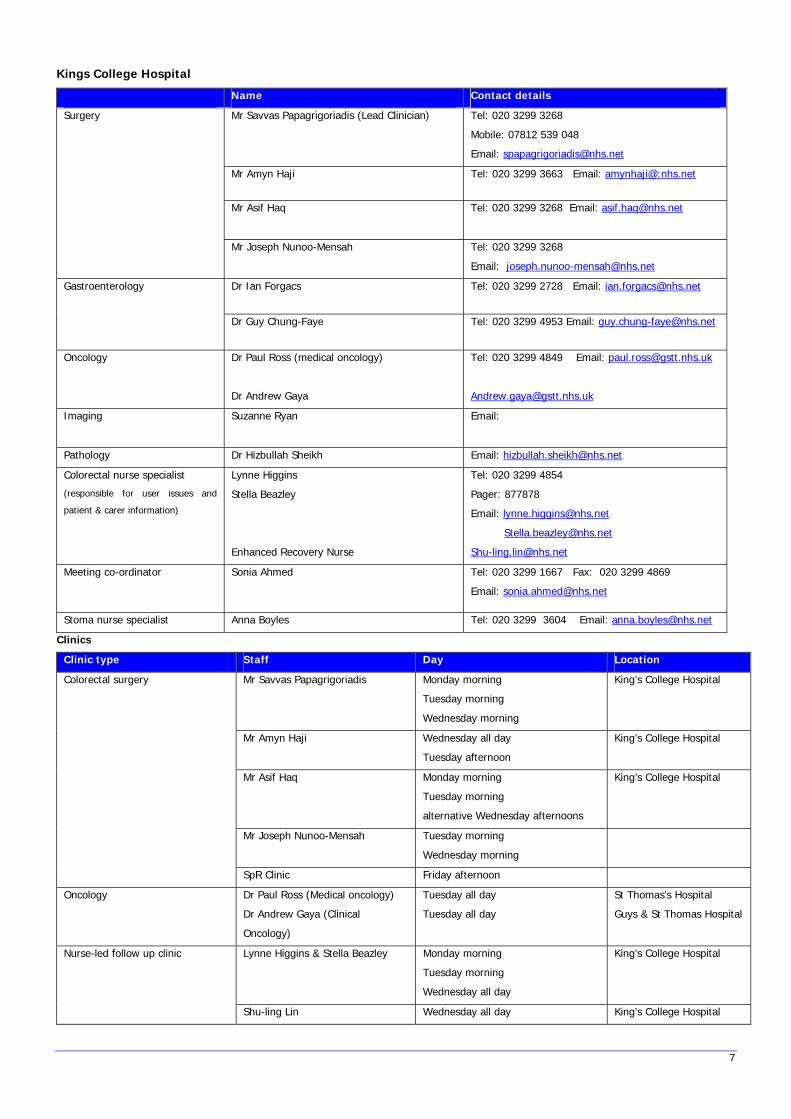
Kings College Hospital
Name Contact details
Mr Savvas Papagrigoriadis (Lead Clinician)
Tel: 020 3299 3268
Mobile: 07812 539 048
Email: [email protected]
Mr Amyn Haji Tel: 020 3299 3663 Email: amynhaji@:nhs.net
Mr Asif Haq
Tel: 020 3299 3268 Email: [email protected]
Surgery
Mr Joseph Nunoo-Mensah Tel: 020 3299 3268
Email: [email protected]
Dr Ian Forgacs Tel: 020 3299 2728 Email: [email protected] Gastroenterology
Dr Guy Chung-Faye Tel: 020 3299 4953 Email: [email protected]
Oncology Dr Paul Ross (medical oncology)
Dr Andrew Gaya
Tel: 020 3299 4849 Email: [email protected]
Imaging Suzanne Ryan Email:
Pathology Dr Hizbullah Sheikh Email: [email protected]
Colorectal nurse specialist
(responsible for user issues and
patient & carer information)
Lynne Higgins
Stella Beazley
Enhanced Recovery Nurse
Tel: 020 3299 4854
Pager: 877878
Email: [email protected]
Meeting co-ordinator Sonia Ahmed
Tel: 020 3299 1667 Fax: 020 3299 4869
Email: [email protected]
Stoma nurse specialist Anna Boyles Tel: 020 3299 3604 Email: [email protected]
Clinics
Clinic type Staff Day Location
Mr Savvas Papagrigoriadis Monday morning
Tuesday morning
Wednesday morning
King’s College Hospital
Mr Amyn Haji Wednesday all day
Tuesday afternoon
King’s College Hospital
Mr Asif Haq Monday morning
Tuesday morning
alternative Wednesday afternoons
King’s College Hospital
Mr Joseph Nunoo-Mensah Tuesday morning
Wednesday morning
Colorectal surgery
SpR Clinic Friday afternoon
Oncology Dr Paul Ross (Medical oncology)
Dr Andrew Gaya (Clinical
Oncology)
Tuesday all day
Tuesday all day
St Thomas’s Hospital
Guys & St Thomas Hospital
Lynne Higgins & Stella Beazley Monday morning
Tuesday morning
Wednesday all day
King’s College Hospital Nurse-led follow up clinic
Shu-ling Lin Wednesday all day King’s College Hospital
8
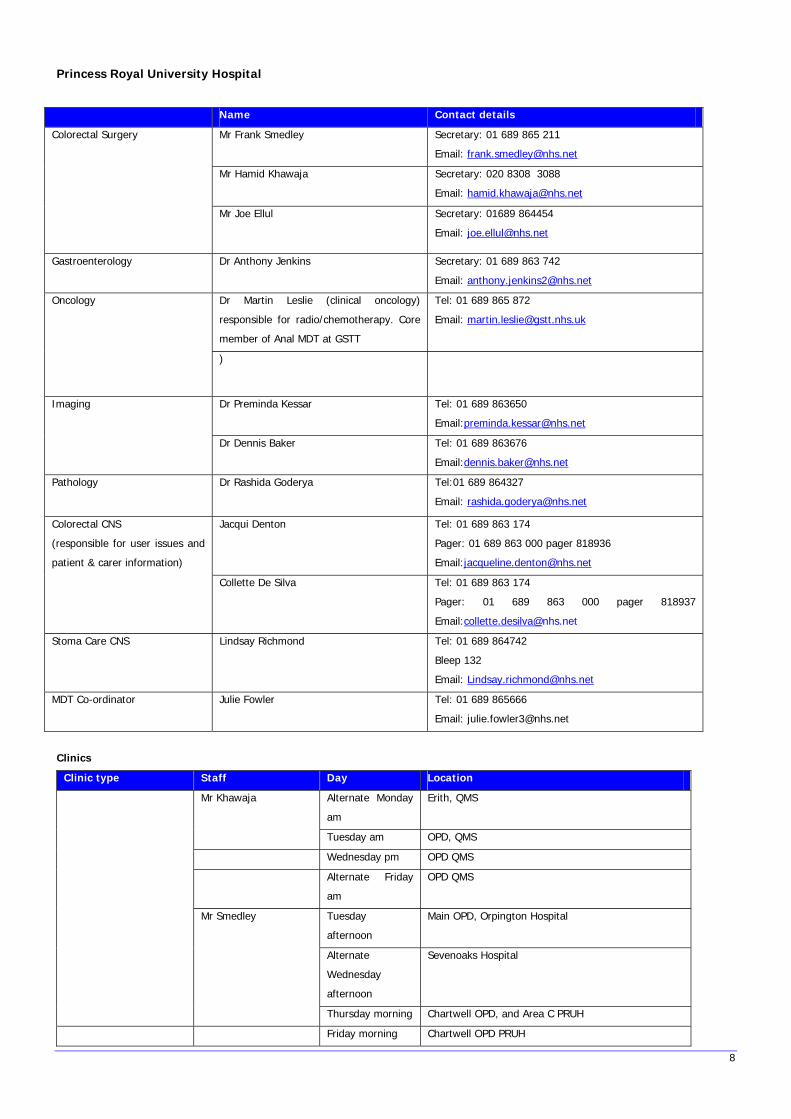
Princess Royal University Hospital
Name Contact details
Mr Frank Smedley
Secretary: 01 689 865 211
Email: [email protected]
Mr Hamid Khawaja Secretary: 020 8308 3088
Email: [email protected]
Colorectal Surgery
Mr Joe Ellul Secretary: 01689 864454
Email: [email protected]
Gastroenterology Dr Anthony Jenkins Secretary: 01 689 863 742
Email: [email protected]
Dr Martin Leslie (clinical oncology)
responsible for radio/chemotherapy. Core
member of Anal MDT at GSTT
Tel: 01 689 865 872
Email: [email protected]
Oncology
)
Dr Preminda Kessar Tel: 01 689 863650
Email:[email protected]
Imaging
Dr Dennis Baker Tel: 01 689 863676
Email:[email protected]
Pathology Dr Rashida Goderya Tel:01 689 864327
Email: [email protected]
Jacqui Denton Tel: 01 689 863 174
Pager: 01 689 863 000 pager 818936
Email:[email protected]
Colorectal CNS
(responsible for user issues and
patient & carer information)
Collette De Silva
Tel: 01 689 863 174
Pager: 01 689 863 000 pager 818937
Email:[email protected]
Stoma Care CNS Lindsay Richmond Tel: 01 689 864742
Bleep 132
Email: [email protected]
MDT Co-ordinator Julie Fowler Tel: 01 689 865666
Email: [email protected]
Clinics
Clinic type Staff Day Location
Alternate Monday
am
Erith, QMS Mr Khawaja
Tuesday am OPD, QMS
Wednesday pm OPD QMS
Alternate Friday
am
OPD QMS
Tuesday
afternoon
Main OPD, Orpington Hospital
Alternate
Wednesday
afternoon
Sevenoaks Hospital
Mr Smedley
Thursday morning Chartwell OPD, and Area C PRUH
Friday morning Chartwell OPD PRUH
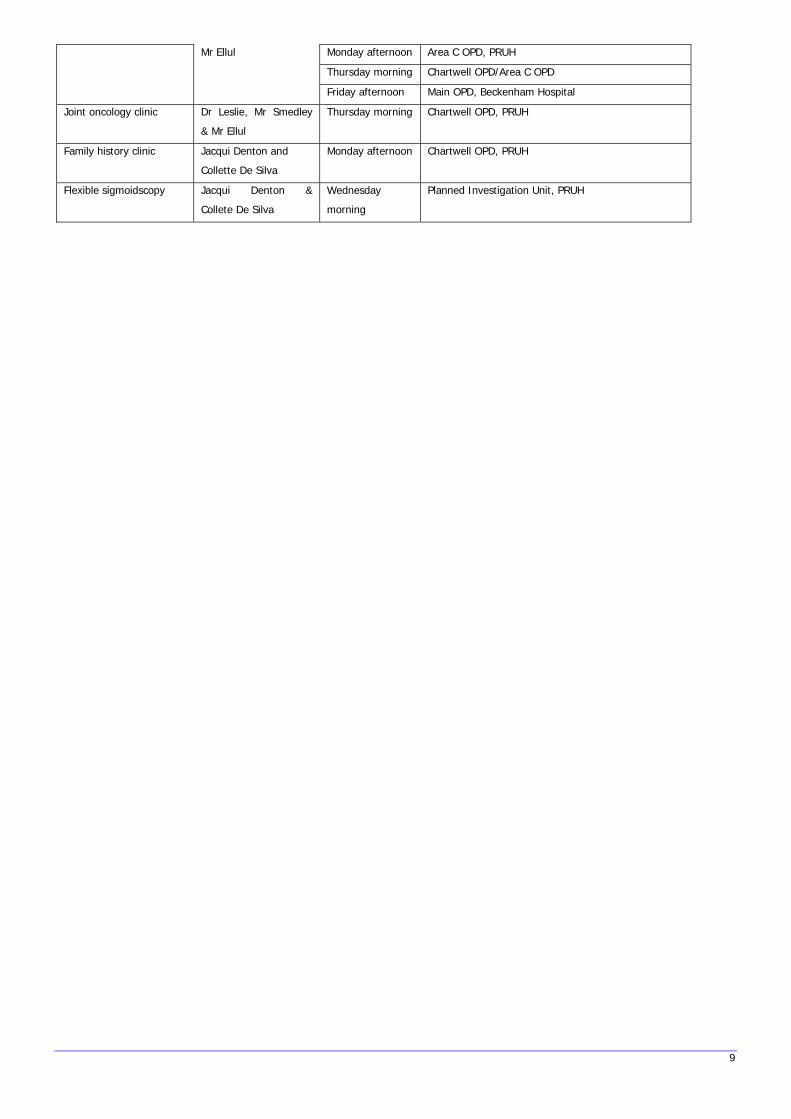
9
Monday afternoon Area C OPD, PRUH
Thursday morning Chartwell OPD/Area C OPD
Mr Ellul
Friday afternoon Main OPD, Beckenham Hospital
Joint oncology clinic
Dr Leslie, Mr Smedley
& Mr Ellul
Thursday morning Chartwell OPD, PRUH
Family history clinic
Jacqui Denton and
Collette De Silva
Monday afternoon Chartwell OPD, PRUH
Flexible sigmoidscopy Jacqui Denton &
Collete De Silva
Wednesday
morning
Planned Investigation Unit, PRUH
10
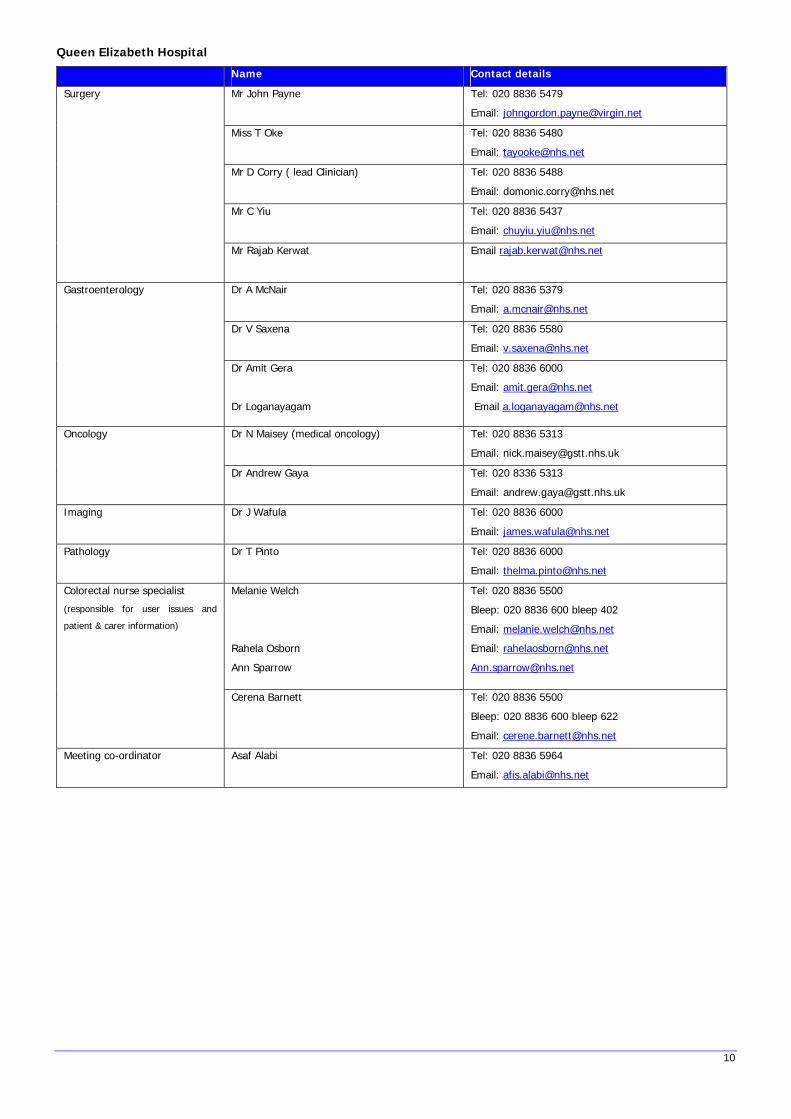
Queen Elizabeth Hospital
Name Contact details
Mr John Payne Tel: 020 8836 5479
Email: [email protected]
Miss T Oke Tel: 020 8836 5480
Email: [email protected]
Mr D Corry ( lead Clinician) Tel: 020 8836 5488
Email: [email protected]
Mr C Yiu Tel: 020 8836 5437
Email: [email protected]
Surgery
Mr Rajab Kerwat Email [email protected]
Dr A McNair Tel: 020 8836 5379
Email: [email protected]
Dr V Saxena Tel: 020 8836 5580
Email: [email protected]
Gastroenterology
Dr Amit Gera
Dr Loganayagam
Tel: 020 8836 6000
Email: [email protected]
Email [email protected]
Dr N Maisey (medical oncology) Tel: 020 8836 5313
Email: [email protected]
Oncology
Dr Andrew Gaya Tel: 020 8336 5313
Email: [email protected]
Imaging Dr J Wafula Tel: 020 8836 6000
Email: [email protected]
Pathology Dr T Pinto Tel: 020 8836 6000
Email: [email protected]
Melanie Welch
Rahela Osborn
Ann Sparrow
Tel: 020 8836 5500
Bleep: 020 8836 600 bleep 402
Email: [email protected]
Email: [email protected]
Colorectal nurse specialist
(responsible for user issues and
patient & carer information)
Cerena Barnett Tel: 020 8836 5500
Bleep: 020 8836 600 bleep 622
Email: [email protected]
Meeting co-ordinator Asaf Alabi Tel: 020 8836 5964
Email: [email protected]
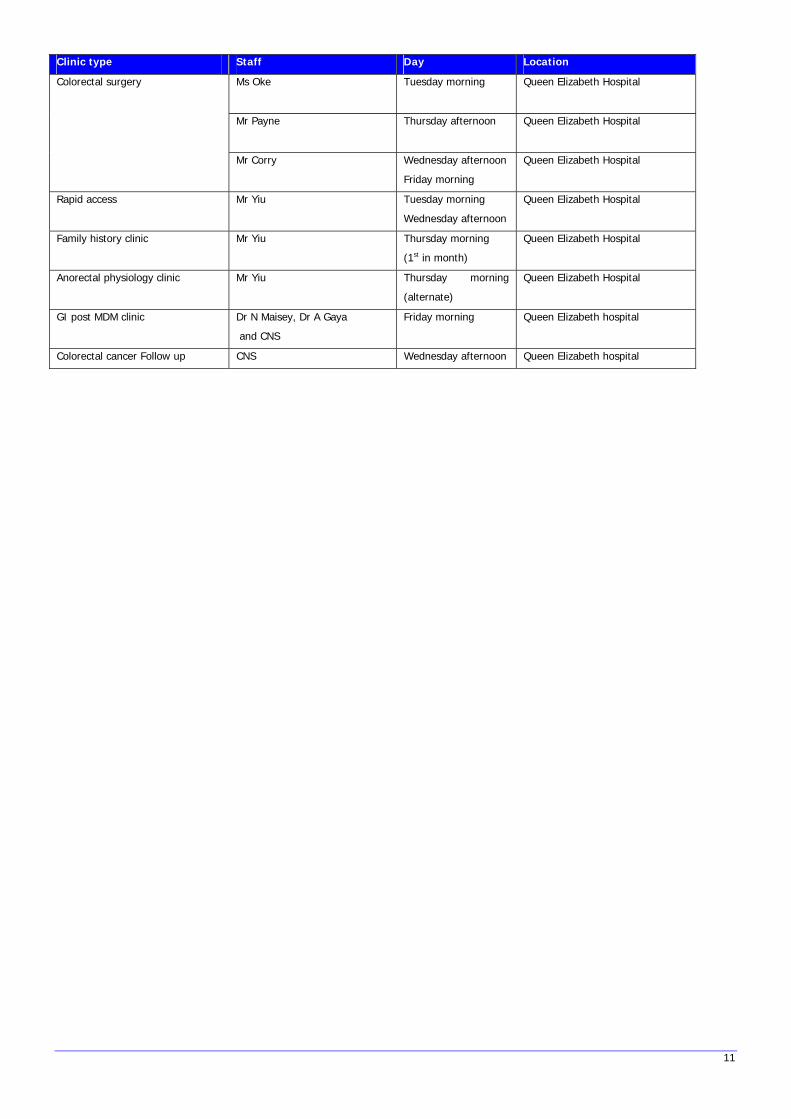
Clinic type Staff Day Location
Ms Oke Tuesday morning Queen Elizabeth Hospital
Mr Payne Thursday afternoon Queen Elizabeth Hospital
Colorectal surgery
Mr Corry Wednesday afternoon
Friday morning
Queen Elizabeth Hospital
Rapid access Mr Yiu Tuesday morning
Wednesday afternoon
Queen Elizabeth Hospital
Family history clinic
Mr Yiu Thursday morning
(1st in month)
Queen Elizabeth Hospital
Anorectal physiology clinic Mr Yiu Thursday morning
(alternate)
Queen Elizabeth Hospital
GI post MDM clinic Dr N Maisey, Dr A Gaya
and CNS
Friday morning Queen Elizabeth hospital
Colorectal cancer Follow up CNS Wednesday afternoon Queen Elizabeth hospital
11
12
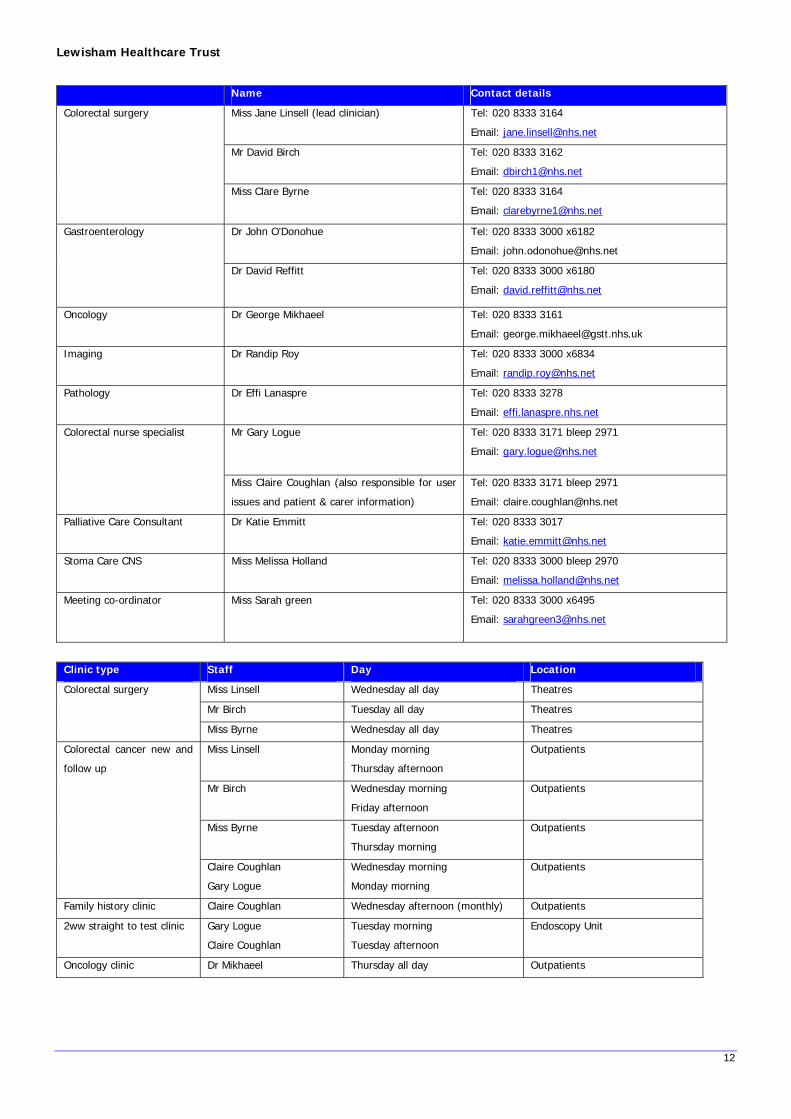
Lewisham Healthcare Trust
Name Contact details
Miss Jane Linsell (lead clinician) Tel: 020 8333 3164
Email: [email protected]
Mr David Birch Tel: 020 8333 3162
Email: [email protected]
Colorectal surgery
Miss Clare Byrne Tel: 020 8333 3164
Email: [email protected]
Dr John O’Donohue Tel: 020 8333 3000 x6182
Email: [email protected]
Gastroenterology
Dr David Reffitt Tel: 020 8333 3000 x6180
Email: [email protected]
Oncology Dr George Mikhaeel Tel: 020 8333 3161
Email: [email protected]
Imaging Dr Randip Roy Tel: 020 8333 3000 x6834
Email: [email protected]
Pathology Dr Effi Lanaspre Tel: 020 8333 3278
Email: effi.lanaspre.nhs.net
Mr Gary Logue Tel: 020 8333 3171 bleep 2971
Email: [email protected]
Colorectal nurse specialist
Miss Claire Coughlan (also responsible for user
issues and patient & carer information)
Tel: 020 8333 3171 bleep 2971
Email: [email protected]
Palliative Care Consultant Dr Katie Emmitt Tel: 020 8333 3017
Email: [email protected]
Stoma Care CNS Miss Melissa Holland Tel: 020 8333 3000 bleep 2970
Email: [email protected]
Meeting co-ordinator Miss Sarah green Tel: 020 8333 3000 x6495
Email: [email protected]
Clinic type Staff Day Location
Miss Linsell Wednesday all day Theatres
Mr Birch Tuesday all day Theatres
Colorectal surgery
Miss Byrne Wednesday all day Theatres
Miss Linsell Monday morning
Thursday afternoon
Outpatients
Mr Birch Wednesday morning
Friday afternoon
Outpatients
Miss Byrne Tuesday afternoon
Thursday morning
Outpatients
Colorectal cancer new and
follow up
Claire Coughlan
Gary Logue
Wednesday morning
Monday morning
Outpatients
Family history clinic Claire Coughlan Wednesday afternoon (monthly) Outpatients
2ww straight to test clinic Gary Logue
Claire Coughlan
Tuesday morning
Tuesday afternoon
Endoscopy Unit
Oncology clinic Dr Mikhaeel Thursday all day Outpatients

Colorectal cancer summary
Introduction
An overview of the patient journey is on the next page. More detailed descriptions of the policy for specific situations can be found in the
appropriate section.
Referral
Patients in whom a diagnosis of cancer is suspected are referred by their general practitioner by standard form via fax to a common number for
each hospital. An appointment in a colorectal clinic is given within two weeks. The national guidelines are in the table. The referral fax sheet for
general practitioners has been changed to reflect this to make it clear which patients should be referred. Referral should be on the basis of one
of the six following criteria3:
The form is on the next page. There is no specific requirement for investigations to be done before referral from general practice. If there is
concern that the patient may have large bowel cancer then the referral need not be delayed by waiting for faecal occult blood tests. General
practitioners are asked to send a letter by fax if the six criteria are not met but they remain concerned about the patient and fear that there
may be a sinister cause for the symptoms. The NICE guidelines do not mention abdominal pain. This network group agreed that abdominal pain
is likely to an important category for referral within the 2-week fax system.
Investigations in the outpatient clinic
In the outpatient clinic the routine investigation includes FBC, U&E, LFT and glucose as well as rigid sigmoidoscopy. The use of CEA is not
routine. Faecal occult blood testing should not delay referral for patients where the suspicion is that they have a colorectal cancer.
Referral from other teams
Other physicans, surgeons or radiologists can refer patients to the colorectal clinics.
Patients admitted under the care of non-colorectal team are taken over the next working day after admission or after a diagnosis is made.
Emergency treatment, when required, is arranged by the team admitting the patient.
Referral from other networks
The patient is referred by the consultant in charge of their care to an appropriate consultant in the receiving hospital. The referral will include
the relevant results and images (hard copy or on CDROM).
3 http://www.nice.org.uk/pdf/CSGCCfullguidance.pdf: Guidance for improving outcomes from colorectal cancer.
13

14
Secondary to tertiary referral policy.
When patients are diagnosed unexpectedly or incidentally with colorectal cancer, or known patients are diagnosed with recurrent or metastatic
disease by clinicians who are not members of the colorectal MDT, the CNS of the local MDT should be contacted with patients details. This
referral should be made by the end of the first complete working day after the diagnosis.
The method of communication is by direct contact to the CNS, whose contact details are with hospital switchboard. It is the responsibility of
the clinician who discovers the diagnosis to inform the CNS.
The CNS is then responsible for informing the patient of the referral by the other team and the diagnosis. This may be by telephone or in a
hospital environment.
The contact details of the colorectal nurse specialist should be distributed to all upper and lower surgeons, gynaecologists, gastroenterologists,
care of the elderly physicians and lead clinicians of cancer imaging.
Teenagers and Young Adults Tertiary Referral Protocol
There is also now a new network standard that all teenagers and young people in South Thames aged 19 to 24 will be discussed at local MDM
but also be referred through the Royal Marsden Teenage and Young Adults (TYA) MDT for discussion. Should any patients meet this criteria the
Colorectal CNS / mdt co-ordinator will fax the TYA network proforma to facilitate discussion at the TYA MDT. We are aware that GSTT is classed
as a designated hospital for TYA rather than a principal treatment centre but this service will be developing over the next 12-15 months. At
GSTT there is already a designated TYA Lead Cancer CNS – Gavin Maynard –Wyatt who we can liaise with for expert advice. Tel 0207 188
7188 ext 51449 Fax 020 7188 2728
Please see pages 65-67 for a copy of the leaflet.
Agreed policy for diagnosis and assessment
Whenever possible patients should have a tissue diagnosis of the tumour made before starting treatment. Therefore the preferred method of
diagnosing colorectal cancer is by colonoscopy or flexible sigmoidoscopy with biopsy. However it is recognised that CT colonography and
barium enema are performed in selected cases.
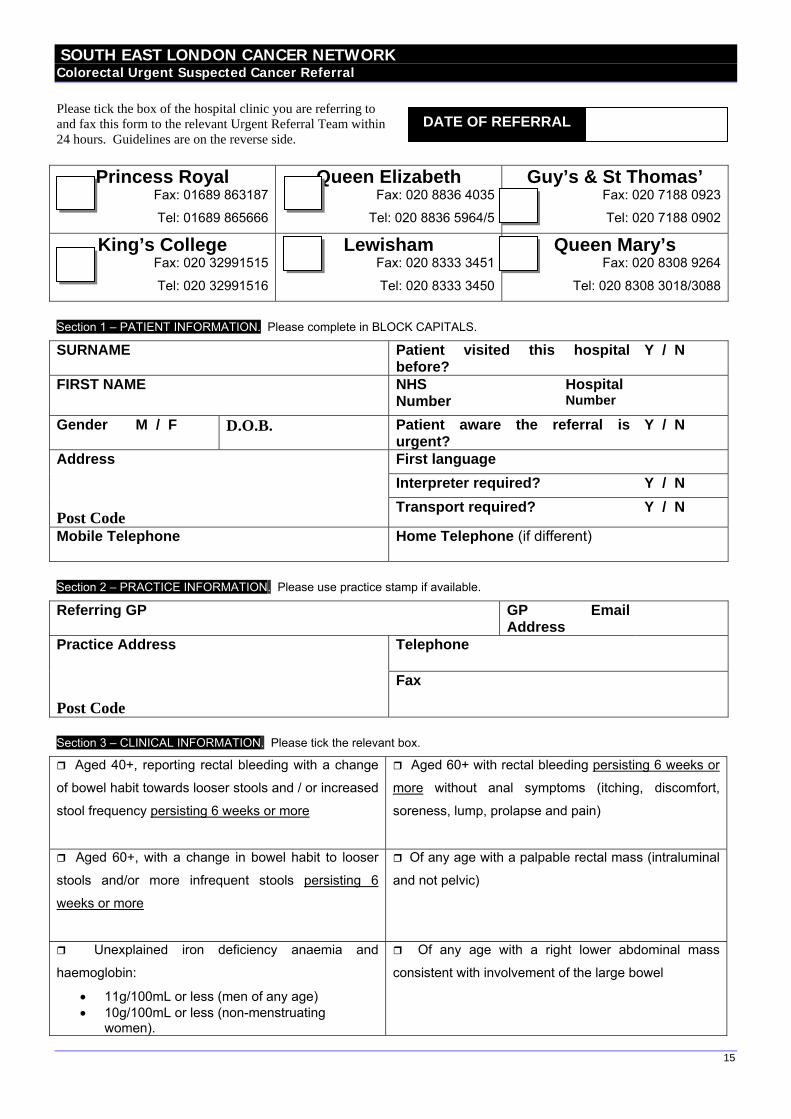
SOUTH EAST LONDON CANCER NETWORK Colorectal Urgent Suspected Cancer Referral
Please tick the box of the hospital clinic you are referring to and fax this form to the relevant Urgent Referral Team within 24 hours. Guidelines are on the reverse side.
15
Princess Royal Fax: 01689 863187
Tel: 01689 865666
Queen Elizabeth Fax: 020 8836 4035
Tel: 020 8836 5964/5
Guy’s & St Thomas’ Fax: 020 7188 0923
Tel: 020 7188 0902
King’s College Fax: 020 32991515
Tel: 020 32991516
Lewisham Fax: 020 8333 3451
Tel: 020 8333 3450
Queen Mary’s Fax: 020 8308 9264
Tel: 020 8308 3018/3088
DATE OF REFERRAL
Section 1 – PATIENT INFORMATION. Please complete in BLOCK CAPITALS.
SURNAME Patient visited this hospital before?
Y / N
FIRST NAME NHS Number
Hospital Number
Gender M / F D.O.B. Patient aware the referral is urgent?
Y / N
First language Interpreter required? Y / N
Address
Post Code
Transport required? Y / N
Mobile Telephone Home Telephone (if different)
Section 2 – PRACTICE INFORMATION. Please use practice stamp if available.
Referring GP
GP Email Address
Telephone Practice Address
Post Code
Fax
Section 3 – CLINICAL INFORMATION. Please tick the relevant box.
Aged 40+, reporting rectal bleeding with a change
of bowel habit towards looser stools and / or increased
stool frequency persisting 6 weeks or more
Aged 60+ with rectal bleeding persisting 6 weeks or
more without anal symptoms (itching, discomfort,
soreness, lump, prolapse and pain)
Aged 60+, with a change in bowel habit to looser
stools and/or more infrequent stools persisting 6
weeks or more
Of any age with a palpable rectal mass (intraluminal
and not pelvic)
Unexplained iron deficiency anaemia and
haemoglobin:
• 11g/100mL or less (men of any age) • 10g/100mL or less (non-menstruating
women).
Of any age with a right lower abdominal mass
consistent with involvement of the large bowel

16
Essential blood Results Hb: U + E’s/eGFR:
Ferritin:
Past Medical History - Attach patient computer record summary.
Medication: Please circle if patient is on any of these medications.
Hypoglycaemics Insulin, Warfarin, Clopidogrel, Dipyridamole Asprin

17
SOUTH EAST LONDON CANCER NETWORK Information to support Colorectal referrals Refer urgently patients:
• Aged 40+ reporting rectal bleeding with a change of bowel habit towards looser stools and / or increased stool frequency persisting 6 weeks or more.
• Aged 60+ with rectal bleeding persisting for 6 weeks or more without anal symptoms. • Aged 60+, with a change in bowel habit to looser stools and/or more infrequent stools persisting for
6 weeks or more. • Of any age with a right lower abdominal mass consistent with involvement of the large bowel. • Of any age with a palpable rectal mass (intraluminal and not pelvic). • With unexplained iron deficiency anaemia and a haemoglobin of 11g/100mL or below (men) and a
haemoglobin of 10g/100mL or below (non-menstruating women). Please check ferritin but do not delay referral.
Use this proforma to refer urgently (2 Week Wait)
Investigations in Primary Care:
• Always carry out a digital rectal examination in patients with unexplained symptoms related to the lower gastrointestinal tract.
• Where symptoms are equivocal a full blood count may help in identifying the possibility of colorectal cancer by demonstrating iron deficiency anaemia, which should then determine if a referral should be made and its urgency.
• When referring please ensure that the patient has a recent haemoglobin and U + E’s/eGFR as required by NPSA alert “Reducing risk of harm from oral bowel cleansing solutions”. For further information see: http://www.nrls.npsa.nhs.uk/resources/type/alerts/?entryid45=59869&p=2
• Faecal occult bloods and tumour markers (e.g. CEA) in symptomatic patients are of little diagnostic value.
Low risk symptoms:
It is recommended in patients having a normal abdominal and rectal examination and haemoglobin estimation that the following symptoms be used to identify patients at very low risk of bowel cancer: • Rectal bleeding with anal symptoms (itching, discomfort, soreness, lump, prolapse and pain). • Transient changes in bowel habit, particularly to harder stools and/or decreased frequency of
defaecation . • Abdominal pain as a single symptom without other high-risk symptoms and signs, an iron
deficiency anaemia, or intestinal obstruction. • Weight loss in the absence of higher risk symptoms unless rapid and profound. Patients with these symptoms can be initially safely managed in primary care by careful "treat, watch-and-wait" strategies and reviewed after 3 months. However, if symptoms persist or recur when off all treatment and • Remain low risk – refer routinely to clinic using Choose & Book or a letter. • Remain in the low risk category but are worrying / severe – refer to clinic using Choose & Book or
a letter, requesting an appointment as soon as possible. • Change to higher risk – refer urgently to clinic using this proforma.
18
Risk factors:
• Offer patients with ulcerative colitis a follow-up plan agreed with a specialist in an effort to detect colorectal cancer in this high-risk group
• There is insufficient evidence to suggest that a positive family history of colorectal cancer can be used to assist in the decision about referral of a symptomatic patient.
Version 2 June 2012
For comments, additional copies, or patient information resources for GPs to use contact the Network on Tel 020 7188 7090 /
Fax 020 7188 7120, or visit our website: www.selcn.nhs.uk.
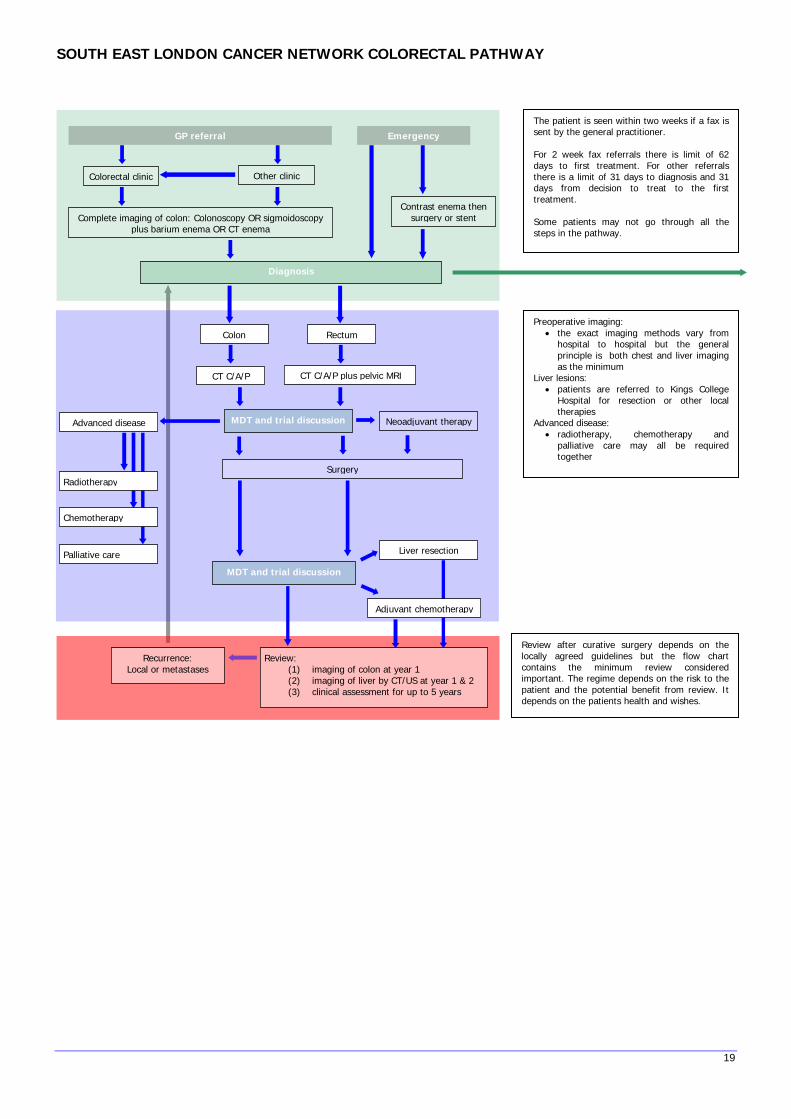
SOUTH EAST LONDON CANCER NETWORK COLORECTAL PATHWAY
GP referral Emergency
Colorectal clinic Other clinic
Complete imaging of colon: Colonoscopy OR sigmoidoscopy plus barium enema OR CT enema
Diagnosis
Contrast enema then surgery or stent
MDT and trial discussion
MDT and trial discussion
Neoadjuvant therapy
Surgery
Liver resection
Advanced disease
Chemotherapy
Radiotherapy
Palliative care
RectumColon
Recurrence: Local or metastases
Review: (1) imaging of colon at year 1 (2) imaging of liver by CT/US at year 1 & 2 (3) clinical assessment for up to 5 years
CT C/A/P CT C/A/P plus pelvic MRI
Adjuvant chemotherapy
Preoperative imaging: • the exact imaging methods vary from
hospital to hospital but the general principle is both chest and liver imaging as the minimum
Liver lesions: • patients are referred to Kings College
Hospital for resection or other local therapies
Advanced disease: • radiotherapy, chemotherapy and
palliative care may all be required together
Review after curative surgery depends on the locally agreed guidelines but the flow chart contains the minimum review considered important. The regime depends on the risk to the patient and the potential benefit from review. It depends on the patients health and wishes.
The patient is seen within two weeks if a fax is sent by the general practitioner. For 2 week fax referrals there is limit of 62 days to first treatment. For other referrals there is a limit of 31 days to diagnosis and 31 days from decision to treat to the first treatment. Some patients may not go through all the steps in the pathway.
19

Family history positive if one patient <50 at diagnosis and 1 first degree relative with colorectal cancer or HNPCC-related cancer. Amsterdam criteria for HNPCC - 3 relatives with CRC/HNPCC-rated cancer - 2 at least 2 successive generations - 1 diagnosed <50 Mr C Yiu on 020 8836 5437 (queries) Dr T Pinto on 020 8836 5656 for immunohistochemistry results Dr L Izatt on 020 7188 1378 or 020 7188 1364 for genetic referrals
Patients under 50 at time of diagnosis are considered for microsatellite instability analysis
FH –ve
IHC normal
FH –ve
IHC loss of staining
FH +ve
Normal review MLH1 lost MSH2 lost Genetic assessment
Colonoscopy every 3 years Colonosocpy every 2 years
If there is a family history of colorectal carcinoma and loss of MSH2 that is discovered before surgery then the patient may be offered a subtotal
colectomy.
Polyposis syndromes
The recommendations for screening are discussed in the family screening section.
Dataset
The Trusts in the group use the Association of Coloproctology database or a similar in keeping with the with minimum data set including waiting
times and cancer registry referral.
Waiting times
The waiting times that must be adhered4 to are:
• Urgent referral 62 days to first treatment
• Other referrals 31 days from decision to treat to first treatment
20
4 http://www.nocancerwaits.org/Clinician%27s%20ABC%20for%20Improving%20Cancer%20Waits.doc
Colon Cancer
Introduction
The diagnosis of colon cancer is usually made at colonoscopy or barium enema but is occasionally made on ultrasound, CT or CT colography.
Every attempt is made to obtain histological support for the diagnosis to avoid missing inflammatory bowel disease or lymphoma but this is not
an absolute requirement in every case and depends on the view of the team when the imaging is reviewed at the weekly meeting.
In addition, complete imaging of the large bowel is obtained to identify synchronous adenomas and carcinomas.
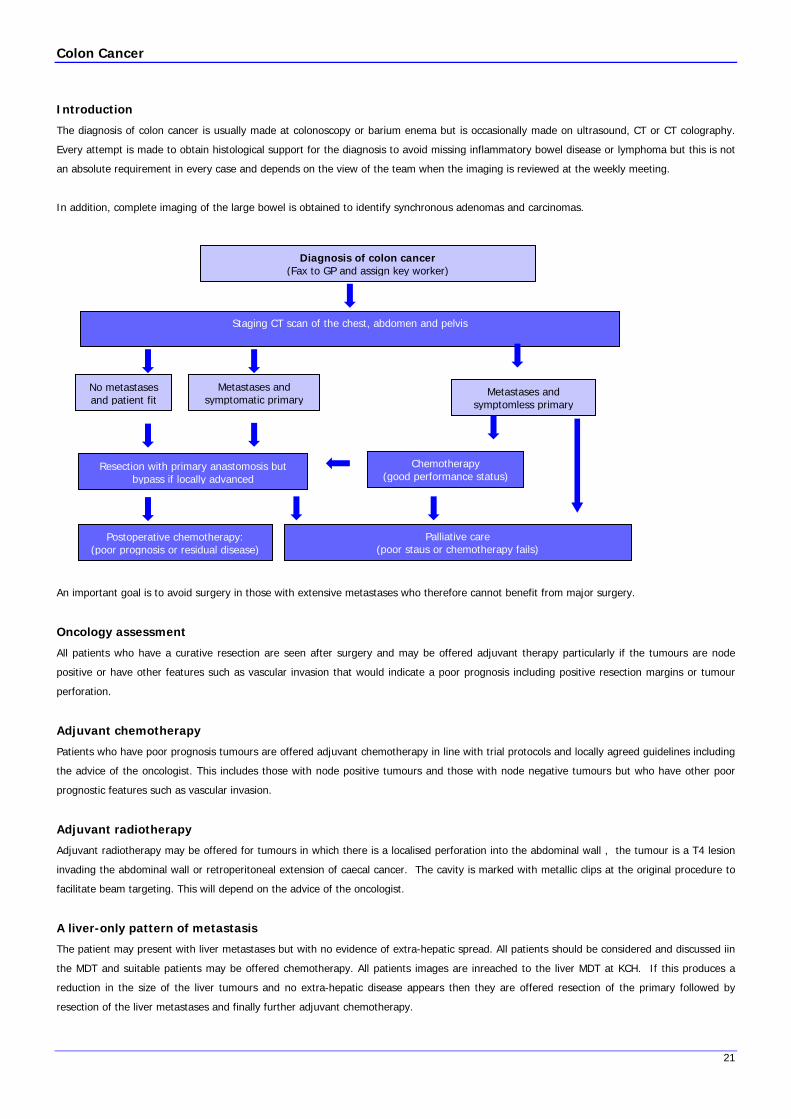
Diagnosis of colon cancer
(Fax to GP and assign key worker)
Staging CT scan of the chest, abdomen and pelvis
Metastases and symptomatic primary
No metastases and patient fit
Metastases and
symptomless primary
Chemotherapy (good performance status)
Resection with primary anastomosis but
bypass if locally advanced
Palliative care (poor staus or chemotherapy fails)
Postoperative chemotherapy: (poor prognosis or residual disease)
An important goal is to avoid surgery in those with extensive metastases who therefore cannot benefit from major surgery.
Oncology assessment
All patients who have a curative resection are seen after surgery and may be offered adjuvant therapy particularly if the tumours are node
positive or have other features such as vascular invasion that would indicate a poor prognosis including positive resection margins or tumour
perforation.
Adjuvant chemotherapy
Patients who have poor prognosis tumours are offered adjuvant chemotherapy in line with trial protocols and locally agreed guidelines including
the advice of the oncologist. This includes those with node positive tumours and those with node negative tumours but who have other poor
prognostic features such as vascular invasion.
Adjuvant radiotherapy
Adjuvant radiotherapy may be offered for tumours in which there is a localised perforation into the abdominal wall , the tumour is a T4 lesion
invading the abdominal wall or retroperitoneal extension of caecal cancer. The cavity is marked with metallic clips at the original procedure to
facilitate beam targeting. This will depend on the advice of the oncologist.
A liver-only pattern of metastasis
The patient may present with liver metastases but with no evidence of extra-hepatic spread. All patients should be considered and discussed iin
the MDT and suitable patients may be offered chemotherapy. All patients images are inreached to the liver MDT at KCH. If this produces a
reduction in the size of the liver tumours and no extra-hepatic disease appears then they are offered resection of the primary followed by
resection of the liver metastases and finally further adjuvant chemotherapy.
21

22
Key worker
As soon as after a diagnosis or large bowel malignancy is made the patient is assigned a key worker, given the hand-held record and asked if
they wish to receive copies of any correspondence regarding their condition.
The key worker (usually a nurse specialist) is responsible for the co-ordination of care with the colorectal multidisciplinary team and acts a link
between the patient and members of the team. Each Trust will determine locally how this is implemented.

Rectal cancer
Introduction
The diagnosis of rectal carcinoma is based on rectal examination, rigid sigmoidoscopy, flexible sigmoidoscopy and colonoscopy. Histological
confirmation is always obtained either sigmoidoscopically in the outpatient clinic or at flexible sigmoidoscopy or colonoscopy. Care is taken to
obtain large biopsies through the sigmoidoscopy to avoid delay arising from having to repeat a procedure in the event of inconclusive small cold
cup colonoscopic biopsies. The rectum is defined as being within 15cm of the anal margin.
Diagnosis of rectal cancer (Fax to GP and assign key worker)
Staging CT scan of the chest, abdomen and pelvis
MRI scan of the pelvis
Low small tumours in unfit patients
Low or zero volume metastases but primary with symptoms or that may obstruct
Extensive metastases
Palliative
careLow risk to circum-
ferential margin High risk to circum-
ferential margin Chemotherapy & radiotherapy
TEMTransanal excision
Neoadjuvant chemotherapy and radiotherapy
Neoadjuvant chemotherapy and radiotherapy are offered when the circumferential margin is at risk of involvement. This is usually the T3 and T4 middle third tumours and most of the lower third tumours.
Surgery with anterior resection to 5cm below tumour for upper third and TME to pelvic floor for lower two thirds with AP for very low tumours
Postoperative chemotherapy if poor prognosis or had neoadjuvant therapy and
postoperative radiotherapy for positive margins without pre-operative radiotherapy
Pre-operative one week high dose radiotherapy is no longer used now that a selective approach is used based on pelvic MRI. The patients at
greatest risk of circumferential margin positivity after resection are those with T3 and T4 middle third rectal cancer and all those with lower
third rectal cancers. All those that have neoadjuvant therapy should be considered for post-operative chemotherapy.
Local recurrence prevention
The outcome of treatment for local recurrence for rectal cancer is poor with salvage being successful in only 25% of patients at most.
Therefore, prevention is important. The factors involved are:
• selective use of pre-operative neoadjuvant therapy for more advanced tumours in the middle third and all lower third rectal cancers
• total mesorectal excision for middle and lower third rectal cancers
• rectal stump washout
• avoidance of intestinal perforation during resection5
5 The (http://www.fascrs.org/associations/1843/files/rectal_cancer_0605.pdf)
23

24
on.
The aim is to do a sphincter-saving resection in over 60% of cases of rectal cancer and to have a 30-day mortality rate of below 5.6%6 for
elective surgery and 20% for emergency surgery.
Neoadjuvant chemoradiotherapy
Neoadjuvant chemotherapy and radiotherapy is offered to those with T3 or T4 N0 or N1 middle third tumours and all lower third tumours. This
policy, based on selection on MRI T-staging, means that radiotherapy is selective and the one-week Scandinavian style radiotherapy is not
required7. For upper third tumours chemoradiation is determined on an individual basis after assessment of T & N stage, proximity to CRM,
and evidence of vascular invasi
Adjuvant chemotherapy
Patients who have poor prognosis tumours are offered adjuvant chemotherapy. This includes those with node positive tumours and those with
node negative tumours but who have other poor prognostic features such as vascular invasion. All those that have neoadjuvant therapy are
offered post-operative chemotherapy because of the results of down-staging.
Laparoscopic colorectal resection
There is an increasing role for laparoscopic surgery. At present the indications for considering the laparoscopic approach are patients who have
not had previous surgery, are not obese and who do not have a bulky pelvic tumour and depends on the NICE guidelines8.
Early Rectal Cancer
This is defined as T1 rectal cancers. In selected cases these may be suitable for local excision. The three techniques are transanal excision
(TAE), endoscopic mucosal resection (EMR) or transanal endoscopic microsurgery (TEMS). TEMS is only offered at Kings College Hospital and
the network therefore refers suitable patients there.
Protocol
Colonoscopy with biopsy
Histopathological confirmation of adenocarcinoma
CT scan chest, abdomen, pelvis for staging distant disease
MRI pelvis to stage local stage
Endorectal ultrasound to stage local disease
TAE and EMR can be offered locally at certain hospitals. Patients deemed suitable for TEMS are referred to Mr Papagrigoriadis at King’s College
Hospital. Patinets should be referred using the referral proforma (below).
6 ACPGBI colorectal cancer study 2002: Part B: Risk adjusted outcomes. The Association of Coloproctology of Great Britain and Ireland, 2001. 7 Perioperative radiotherapy for rectal cancer: the case for a selective pre-operative approach – the third way. A Crawshaw, T Hennigan, F Smedley, M D Leslie.
Colorectal Disease 2003; 5: 367-372. 8 http://www.nice.org.uk/pdf/guidancelapcolcanc.pdf

25
REFERRAL FOR TEMS (Transanal Endoscopic Micro Surgery)
New patient Response to treatment
Relapse Other
Please specify below*
Patient
Surname:
Forename:
Date of Birth:
NHS No:
Hospital No:
Address:
Postcode:
Tel. no:
GP
GP Practice Code:
Dr:
Address:
Post code:
Tel. no:
Fax no:
Email:
Date of initial referral letter:
Applies to initial referral from GP, A&E, screening or other consultant
Date 1st seen : seen by (Cons)
Priority type: 2ww Other (please state):
Is the rectal tumour known to be:
• Benign • Malignant • Uncertain
Has there been previous excision with TEMS/ TAR/ Colonoscopy?
• Yes • No
If the tumour is malignant what is the reason for
referral:
• Patient unfit for radical surgery • MDM decision because of T1 tumour • Patient choice (declines radical surgery) • Palliative
Is the patient considered fit for general anaesthesia?
• Yes • Uncertain
Note: If a patient is unfit for general anaesthesia TEMS
will not be possible
Please confirm that the patient has had MRI of rectum
in all cases:
• Yes • No
Please confirm the patient has had a full colonoscopy
in the last 12 months in all cases
• Yes
Has the patient had endorectal ultrasound?
• Yes • No
Please note: if endorectal ultrasound is available at your hospital
please perform prior to referral on all patients (benign & malignant).
If not available it will take place at King’s but warning us helps
improve the patient pathway.

26
• No
Please confirm the patients has had CT of the
abdomen and chest if tumour is malignant:
• Yes • No
Has the patient been discussed at your local MDM?
• Yes • No
Please note: Local MDM discussion required for all malignant
patients. We accept direct consultant referrals of benign adenomas
without MDM discussion.
Reason for referral: Advice only (MDM) MDM & consultation (OPD) Transfer (urgent)*
*if urgent pls contact SpR/Consultant on call via switchboard 020 3299 9000
Question(s) to be answered by multi-disciplinary team meeting:
Has patient been informed of diagnosis?
Provisional diagnosis:
Have pathology reports/slides been sent?
(please send to HPB Oncology Office)
Have imaging results been sent?
CD/ Image link (if CD, must be DICOM compatible)
Patient fitness to travel to centre:
Patient preference/concerns re treatment?
Referred by: at:
Contact details:
Tel: Fax:
Email:
Date: Day in patient pathway:
Additional information or attach referral letter :

27
Outcome : Centre use only
Patient listed for MDM : Y/N : If Y date
If N pls state why?
Outcome of discussion sent to referee? Y/N
If Y date If N pls state why?
Completed by : (name in capitals) (signature)


29
Anal cancer
Introduction
Squamous cell carcinoma of the anal canal or margin is an uncommon condition that used to be treated by abdominoperineal resection with
long term survival rates of only 40-70%. The use of radiotherapy alone with either external beam radiotherapy or brachytherapy increases cure
rates to 70-90%. The probability of cure decreases to 50% in node positive patients. Local control can be improved with the addition of
chemotherapy usually with 5FU and mitomycin. Primary treatment with chemotherapy and radiotherapy will cure most patients without the
need for major surgery and a permanent stoma.
Diagnosis and Staging
The diagnosis of carcinoma of the anus is based on histological confirmation on biopsies taken at examination under anaesthesia to distinguish
it from a low adenocarcinoma of the rectum. A staging CT of the chest and abdomen and a MRI scan of the pelvis are required. PET can be
extremely useful in determining nodal involvement and for planning of radiotherapy.
Treatment
In the absence of metastatic disease the patient is offered chemotherapy and radiotherapy, as part of a clinical trial if possible. If the treatment
fails to control the disease then the patient is offered abdominal-perineal resection, with the use of flaps to aid perineal healing. The usual
regime would be 50.4Gy in 28 fractions along with 5FU and mitomycin C. Boosts up to 60Gy are widely used if residual or bulky disease was
present. Selected patients with node positive disease will be offered Intensity Modulated Radiotherapy which significantly improves the
morbidity of treatment.
If inguinal lymphadenopathy persists after the initial treatment then a needle biopsy is performed with a view to block dissection of the groin.
Distant metastases may be treated palliatively with chemotherapy and radiotherapy is offered for bone metastases depending on the advice of
the oncologist.
Currently there are no clinical trial open for anal cancer patients. ACT III is awaited.
Review
The risk of recurrence is greatest in the first two years. The patients are seen every three months for two years with biopsy of possible
recurrences. They are then seen every 6 months to 5 years then discharged. Searching for metastases is of no help and therefore routine
surveillance imaging is not required unless there is the suspicion of malignancy.
Referral Guidelines
All anal cancers are referred to Dr Martin Leslie or Dr Andrew Gaya. These patients are discussed at the MDM held at St Thomas’. Referrals are
made by direct communication with the CNS at GSTT. Treatment with chemoradiotherapy or chemotherapy may then be offered by Dr Leslie
or Dr Gaya.
In patients who do not have a complete response or recurrent disease then salvage abdominoperineal excision possibly with a myocutaneous
flap may be offered. These patients require histological confirmation of recurrence and complete restaging with CT, MRI and PET scans. This
is undertaken by Mr Mark George at GSTT and will use flaps to heal the perineum.
Patients would be presented initially at their local MDT and then referred to the anal MDT. Subsequent management decisions are made by the
anal MDT. Follow up can be done locally or at the anal cancer centre depending on patient preference.

31
Colorectal surgery
Preparation for surgery
The preparation for surgery includes:
• pre-assessment clinic
• informed consent with the consent form done in advance
• pre-operative assessment by stoma nurse if required
• cross match blood when required although the current recommendations are that this is not required for elective colorectal resection
unless significant blood loss is anticipated
• bowel preparation (where no obstruction is present) depending on local guidelines
• thromboembolism prophylaxis with low molecular weight heparin combined with anti-embolic stockings with intermittent calf-
compression in theatre being considered
• antibiotic proplylaxis with the exact regime depending on local guidelines
• correction of iron deficiency anaemia to avoid transfusion requirement
• MRSA swab
• access to HDU and ITU depending on the pre-operative assessment
Laparoscopic Policy All appropriate patients must be offered the choice of laparoscopic surgery for colorectal cancer. All laparoscopic colorectal operations should be
performed by surgeons properly trained in colorectal surgery and identified as named laparoscopic surgeons on the network list found in the
constitution document. These surgeons should also have undergone preceptorship laparoscopic training, particularly in rectal procedures. Their
results should be carefully audited in the local hospital multidisciplinary setting and should also be submitted to the Association of
Coloproctology of Great Britain and Ireland colorectal cancer database.
Detailed referral criteria for laparoscopic surgery are being worked on, but the minimum criteria for offering patients laparoscopic surgery are:
The criteria for offering patients laparoscopic surgery are:
BMI less than 30
No previous major abdominal surgery
Avoiding obvious T4 cancers on pre-operative staging
No clinical or radiological signs of obstruction
Adherence to NICE / LAPCO guidelines.
All cases will be considered for laparoscopic surgery within the MDT, and those cases deemed outside the capabilities of the local team will be
offered referral elsewhere. to ensure appropriate availability of appropriate surgical procedure.
Preparation for stoma formation
If the patient may require a stoma then the discussion for consent must include this. The patient should see the stoma nurse at the earliest
opportunity for adequate preparation. The patient should be seen by a stoma nurse before surgery whenever possible. In an emergency the
stoma site should be marked by an experienced surgeon.
Operation record
The operation note should include:
• patient’s name, date of birth and hospital number
• date and time of procedure
• name of surgeon, assistants and anaesthetist
• name of procedure
• ASA grade and estimated blood loss
• details of the tumour site and extent of spread
• details of the procedure
• presence or absence of tumour spread
32
• conclusion as to whether the procedure was curative or palliative
• marking of areas of residual disease with metallic clips to direct radiotherapy
• post-operative instructions about fluid balance and antibiotic and DVT prophylaxis
Colonoscopy
Colonoscopy reports should include:
• name of endoscopist
• the instrument used and serial number
• the quality of the preparation
• the point to which examination was possible
• reason for not being able to reach the caecum or terminal ileum
• how the caecum was identified
• which biopsies were obtained
• any therapeutic procedure performed
The goal is to achieve a completion rate of 90% with appropriate audit9.
9 Recommendations for training in gastrointestinal endoscopy 1999. Joint advisory group on Gastrointestinal Endoscopy. London JCHMT 1999.
33
Imaging reporting standard
Introduction
The exact guidelines such as CT slice thickness have not been set as the imaging machines vary between the hospitals within the network but
all the Trusts in the network are working towards the national guidelines.
Colon cancer
The colon cancer reporting standard includes
• method of scan
• site of tumour
• radiological assessment of resectability
• local invasion of organs
• nodal changes including size of largest
• liver metastases (size, segment and number)
• synchronous colon lesions
• other incidental features
• the TNM staging is desirable.
Rectal cancer
The rectal cancer reporting standard includes
• method of scan
• site of tumour (distance from anal margin)
• mesorectal involvement including, if possible, the shortest distance to the mesorectal fascia
• resectability
• local invasion of organs
• synchronous colon lesions
• nodal changes including size of largest
• liver metastases (size, segment and number)
• other incidental features
• the TNM staging is desirable.
Anal cancer
The anal cancer reporting standard includes
• method of scan
• size of tumour
• perirectal fat involvement
• resectability
• local invasion of levator ani or pelvic side walls
• liver metastases (size, segment and number)
• other incidental features
• the TNM staging is desirable.


35
Histopathology
The histopathology national minimum data set is available online from the Royal College of Pathologists10. The rationale behind the uniform method of
reporting pathological specimens in large bowel cancer are:
• to identify those that may benefit form adjuvant chemotherapy
• to identify the patients with rectal cancer who may be at high risk of local recurrence and therefore who may benefit from neoadjuvant
chemotherapy and radiotherapy or post operative radiotherapy possibly combined with chemotherapy
• to allow estimation of prognosis
• to allow comparison between different departments
The laboratory procedures including histological and histochemical investigations are performed as in the minimum dataset from the Royal College of
pathologists. Further histochemical staining may be required to identify the type of tumour and site of origin of material obtained by biopsy when the
diagnosis is uncertain and there is doubt about the tumour type or its originating site. These are discussed the team meetings.
Staging classification
TNM
The TNM classification is to be preferred and the records, imaging reports and histopathology reports should be reported this way if possible.
T primary tumour
Tx primary cannot be assessed
T0 no evidence of primary tumour
Tis carcinoma in situ
T1 tumour invaded submucosa
T2 tumour invades muscularis propria
T3 tumour invade through muscularis propria
T4 tumour penetrates the visceral peritoneum or directly into other organs of structures
N regional lymph node state
Nx regional lymph nodes cannot be assessed
N0 no regional lymph node metastasis
N1 metastasis in 1-3 pericolic or perirectal lymph nodes
N2 metastases in 4 or more pericolic or perirectal lymph nodes
M distant metastasis
Mx metastatic disease cannot be assessed
M0 no distant metastasis
M1 distant metastasis
The addition of the prefix of a small ‘p’ denoted staging based on histological assessment.
Dukes’
A invasive carcinoma not breaching the muscularis propria
B invasive carcinoma breaching the muscularis propria but with no nodal involvement
C1 lymph node involvement not affecting the apical node
C2 lymph node involvement affecting the apical node
10 http://www.rcpath.org/resources/pdf/colorectalcancer.pdf
36
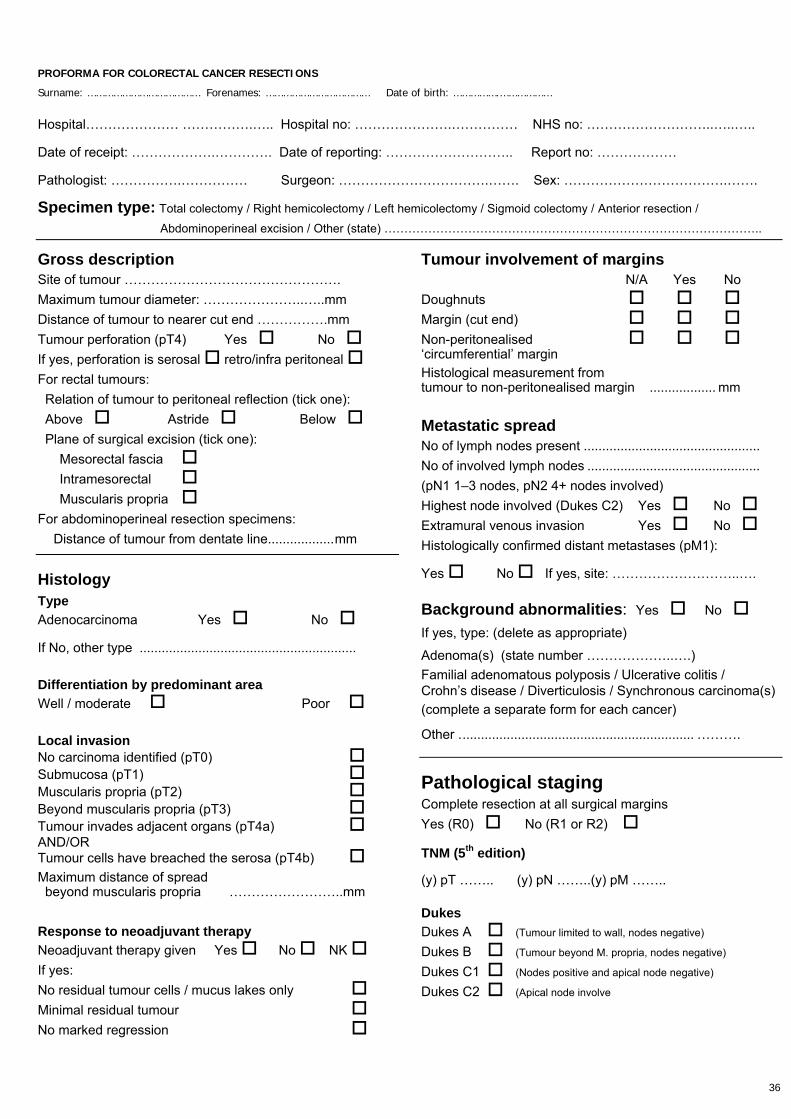
PROFORMA FOR COLORECTAL CANCER RESECTIONS
Surname: ………………………………… Forenames: ……………………………… Date of birth: …………….………………
Hospital………………… …………….….. Hospital no: ………………….…………… NHS no: ………………………..…..…..
Date of receipt: ……………….…………. Date of reporting: ……………………….. Report no: ………………
Pathologist: …………….…………… Surgeon: …………………………….……. Sex: ……………………………….…….
Specimen type: Total colectomy / Right hemicolectomy / Left hemicolectomy / Sigmoid colectomy / Anterior resection /
Abdominoperineal excision / Other (state) …………………………………………………………………………………..
Gross description Site of tumour …………………………………………. Maximum tumour diameter: …………………..…..mm Distance of tumour to nearer cut end …………….mm Tumour perforation (pT4) Yes No If yes, perforation is serosal retro/infra peritoneal For rectal tumours: Relation of tumour to peritoneal reflection (tick one): Above Astride Below Plane of surgical excision (tick one):
Mesorectal fascia Intramesorectal Muscularis propria
For abdominoperineal resection specimens: Distance of tumour from dentate line..................mm
Histology Type Adenocarcinoma Yes No
If No, other type ...........................................................
Differentiation by predominant area Well / moderate Poor
Local invasion No carcinoma identified (pT0) Submucosa (pT1) Muscularis propria (pT2) Beyond muscularis propria (pT3) Tumour invades adjacent organs (pT4a) AND/OR Tumour cells have breached the serosa (pT4b) Maximum distance of spread beyond muscularis propria ……………………..mm
Response to neoadjuvant therapy Neoadjuvant therapy given Yes No NK If yes: No residual tumour cells / mucus lakes only Minimal residual tumour No marked regression
Tumour involvement of margins N/A Yes No Doughnuts Margin (cut end) Non-peritonealised ‘circumferential’ margin Histological measurement from tumour to non-peritonealised margin .................. mm
Metastatic spread No of lymph nodes present ................................................ No of involved lymph nodes ............................................... (pN1 1–3 nodes, pN2 4+ nodes involved) Highest node involved (Dukes C2) Yes No Extramural venous invasion Yes No Histologically confirmed distant metastases (pM1):
Yes No If yes, site: ………………………..….
Background abnormalities: Yes No
If yes, type: (delete as appropriate)
Adenoma(s) (state number ………………..….) Familial adenomatous polyposis / Ulcerative colitis / Crohn’s disease / Diverticulosis / Synchronous carcinoma(s) (complete a separate form for each cancer)
Other ................................................................ ……….
Pathological staging Complete resection at all surgical margins Yes (R0) No (R1 or R2)
TNM (5th edition)
(y) pT …….. (y) pN ……..(y) pM ……..
Dukes Dukes A (Tumour limited to wall, nodes negative) Dukes B (Tumour beyond M. propria, nodes negative) Dukes C1 (Nodes positive and apical node negative) Dukes C2 (Apical node involve
37
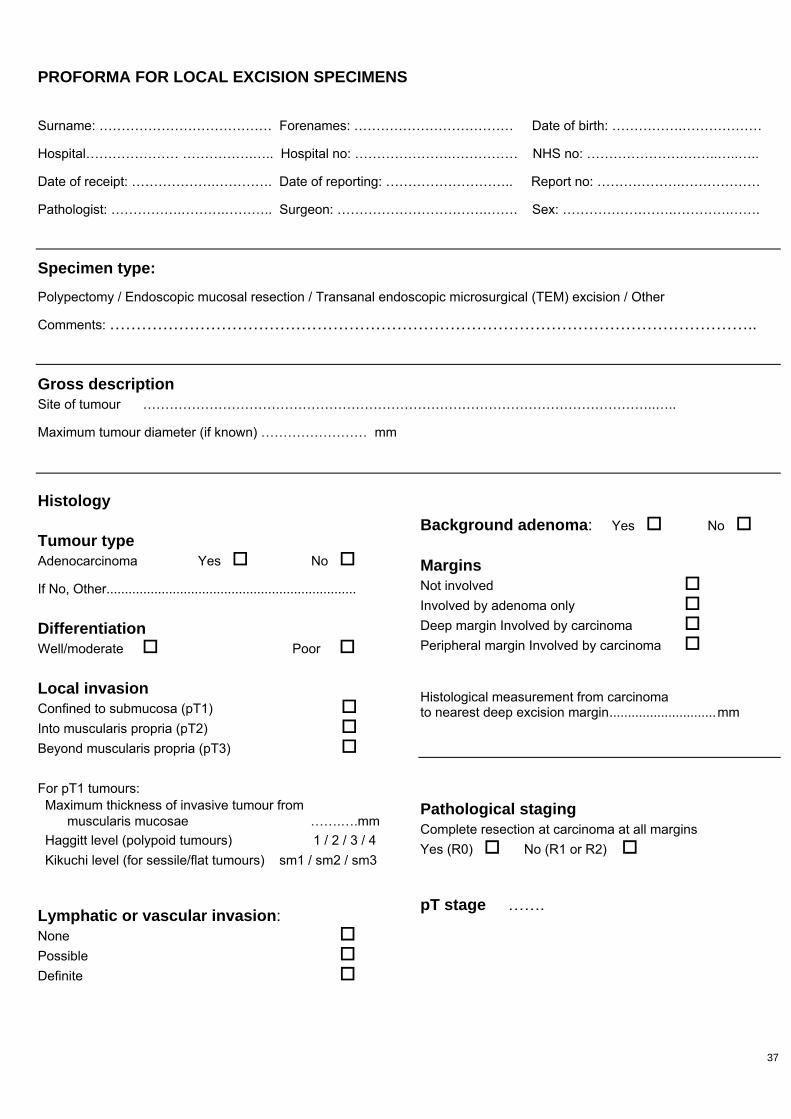
PROFORMA FOR LOCAL EXCISION SPECIMENS
Surname: ………………………………… Forenames: ……………………………… Date of birth: …………….………………
Hospital………………… …………….….. Hospital no: ………………….…………… NHS no: ………………….……..…..…..
Date of receipt: ……………….…………. Date of reporting: ……………………….. Report no: ……………….………………
Pathologist: …………….……….……….. Surgeon: …………………………….……. Sex: …………………….………….…….
Specimen type:
Polypectomy / Endoscopic mucosal resection / Transanal endoscopic microsurgical (TEM) excision / Other
Comments: …………………………………………………………………………………………………………..
Gross description Site of tumour ……………………………………………………………………………………………………..…..
Maximum tumour diameter (if known) …………………… mm
Histology Tumour type Adenocarcinoma Yes No
If No, Other....................................................................
Differentiation Well/moderate Poor
Local invasion Confined to submucosa (pT1) Into muscularis propria (pT2) Beyond muscularis propria (pT3) For pT1 tumours: Maximum thickness of invasive tumour from muscularis mucosae …….….mm Haggitt level (polypoid tumours) 1 / 2 / 3 / 4 Kikuchi level (for sessile/flat tumours) sm1 / sm2 / sm3
Lymphatic or vascular invasion: None Possible Definite
Background adenoma: Yes No
Margins Not involved Involved by adenoma only Deep margin Involved by carcinoma Peripheral margin Involved by carcinoma Histological measurement from carcinoma to nearest deep excision margin.............................mm
Pathological staging Complete resection at carcinoma at all margins Yes (R0) No (R1 or R2)
pT stage …….


39

41
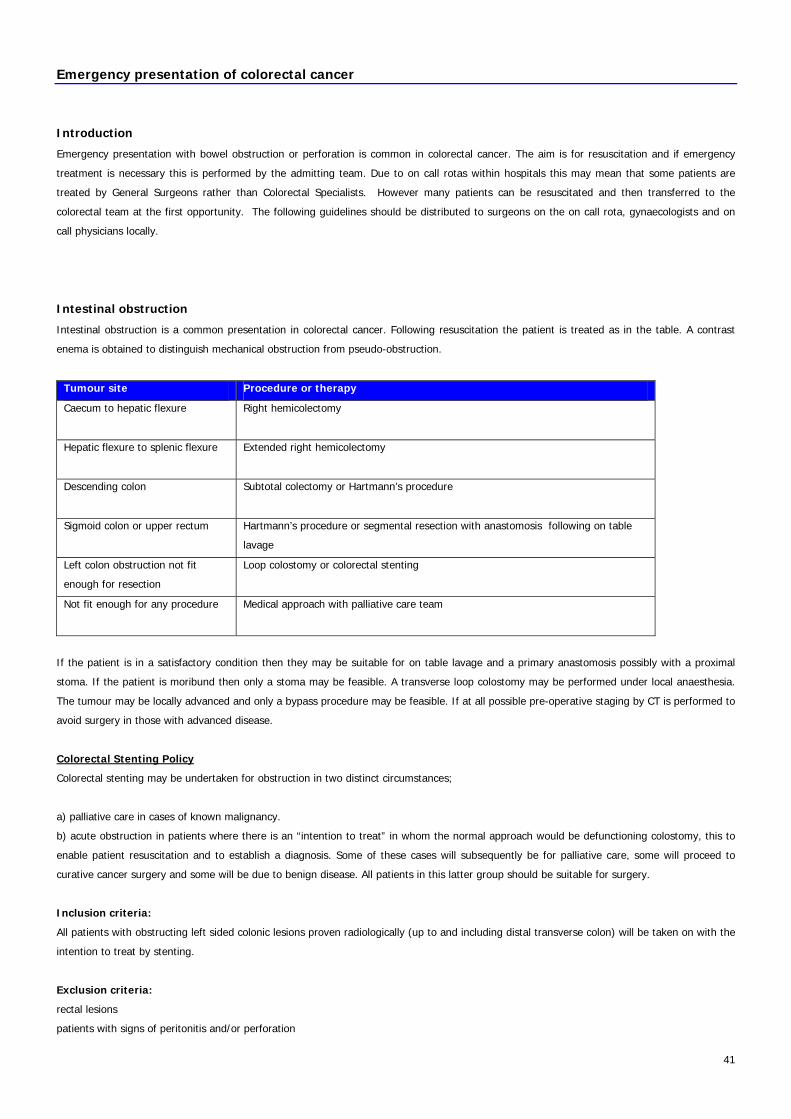
Emergency presentation of colorectal cancer
Introduction
Emergency presentation with bowel obstruction or perforation is common in colorectal cancer. The aim is for resuscitation and if emergency
treatment is necessary this is performed by the admitting team. Due to on call rotas within hospitals this may mean that some patients are
treated by General Surgeons rather than Colorectal Specialists. However many patients can be resuscitated and then transferred to the
colorectal team at the first opportunity. The following guidelines should be distributed to surgeons on the on call rota, gynaecologists and on
call physicians locally.
Intestinal obstruction
Intestinal obstruction is a common presentation in colorectal cancer. Following resuscitation the patient is treated as in the table. A contrast
enema is obtained to distinguish mechanical obstruction from pseudo-obstruction.
Tumour site Procedure or therapy
Caecum to hepatic flexure
Right hemicolectomy
Hepatic flexure to splenic flexure
Extended right hemicolectomy
Descending colon
Subtotal colectomy or Hartmann’s procedure
Sigmoid colon or upper rectum Hartmann’s procedure or segmental resection with anastomosis following on table
lavage
Left colon obstruction not fit
enough for resection
Loop colostomy or colorectal stenting
Not fit enough for any procedure
Medical approach with palliative care team
If the patient is in a satisfactory condition then they may be suitable for on table lavage and a primary anastomosis possibly with a proximal
stoma. If the patient is moribund then only a stoma may be feasible. A transverse loop colostomy may be performed under local anaesthesia.
The tumour may be locally advanced and only a bypass procedure may be feasible. If at all possible pre-operative staging by CT is performed to
avoid surgery in those with advanced disease.
Colorectal Stenting Policy
Colorectal stenting may be undertaken for obstruction in two distinct circumstances;
a) palliative care in cases of known malignancy.
b) acute obstruction in patients where there is an “intention to treat” in whom the normal approach would be defunctioning colostomy, this to
enable patient resuscitation and to establish a diagnosis. Some of these cases will subsequently be for palliative care, some will proceed to
curative cancer surgery and some will be due to benign disease. All patients in this latter group should be suitable for surgery.
Inclusion criteria:
All patients with obstructing left sided colonic lesions proven radiologically (up to and including distal transverse colon) will be taken on with the
intention to treat by stenting.
Exclusion criteria:
rectal lesions
patients with signs of peritonitis and/or perforation

42
patients with closed loop obstruction and right iliac fossa tenderness
Palliative care
Patients with known malignancy who are classified for palliative care will be considered for stenting.
Stenting for these patients should be available within 5 working days unless there is evidence to suggest impending obstruction. In cases of
impending obstruction the service should be available on a next day basis.
Initial access to the tumour will usually be via endoscopy to enable wire access across the lesion. High quality fluoroscopy with a c-arm
screening unit is necessary to enable accurate stent placement. In cases where the lesion is non-obstructing departments may place the stent
with fluoroscopic guidance alone but there must be easy access to back up endoscopy.
Intention to treat
All patients should have a water soluble contrast enema to establish and locate the level of obstruction and to define evidence of a closed loop
obstruction.
Access to stenting should be within 24 hours, this will necessitate a weekend/bank holiday on call availability of personnel.
It is recognised that this will not always be available due to personnel shortages, in these case patients may be treated by conventional surgical
approach. Trusts should look to develop a service rota to accommodate 24/7cover for stenting access.
Personnel
The practice will be led by a named radiologist and surgeon from each hospital trust.
It will usually be undertaken as a combined procedure with an endoscopist and a radiologist. Where either have the necessary cross cover skills
then they may undertake the procedures with the necessary nursing, radiographic and ancillary staff. Each trust will agree and record who is
considered competent, this will be ratified by the SCN colorectal tumour group.
Stents
There are several stent systems available. The ideal stent will be large enough to relieve obstruction, compliant with the bowel wall whilst
having a good radial force and have a low migration rate. Stainless stents such as the Wallstent are “old” technology, these are non compliant
and have a high migration rate. Nitonol stents should be used. Sizing should be 30mm or larger (“through ‘scope” systems only get up to 28mm
and are therefore not ideal).
The following clinicians are involved in colorectal stenting
GSTT Dr Tarun Sabhawal
Lewisham Dr Dewar, Dr Leslie
QEW Dr Vishal Saxena, Dr Suren Surenthrian, Miss Tayo Oke, Dr Alistair Mcnair, Dr Amit Gera
King’s Dr Guy Chung Faye
Sidcup Mr Rajab Kerwat
PRUH Dr Viktor Serafimov, Dr Ajay Arora, Mr Joe Ellul, Mr Tarun Signhal, Mr W Katugampola,
Mr Mofta El Buzidi
Intestinal perforation
Intestinal perforation is less common but carries a poorer prognosis. The treatment is as in the table above but it is seldom appropriate to
consider a primary anastomosis in the face of faecal peritonitis.

43
Intestinal haemorrhage
Haemorrhage is uncommon and rarely requires emergency treatment. The condition is treated in the same way as elective cases once the
haemorrhage has stopped.
Subsequent management
After treatment of the emergency the patient is discussed in the local MDT. Subsequent management may include postoperative
chemotherapy and radiotherapy. Follow up in colorectal surgical clinic is arranged to discuss stoma closure and on going cancer follow up.


45
Review after presumed curative surgery
Introduction
Those who have had a potentially curative resection are reviewed regularly to identify recurrence in the belief that early treatment may confer a
survival advantage11. The exact regime is a matter of considerable debate12.
Patients are routinely referred for an oncology opinion after surgery depending on the view of the team at the weekly meeting.
Clinical review
The patients are seen regularly in the outpatient clinic for the first two years. Thereafter they are seen once a year. Patients are discharged
after five years although this may be sooner if the patient has other severe intercurrent medical problems.
Colonic imaging
If the whole colon was not seen before surgery then a colonoscopy is done in the first three months after completion of treatment. Otherwise it
is done at the end of year one after resection. A second one may be done in the next 3-4 years.
After that, the colonoscopy is repeated every three years. After three normal colonoscopies no further ones are arranged. This is in keeping
with the ACPGBI evidence based practice guidelines. The age at cessation of review depends on the general condition of the patient and not
age. One must consider the amount of ‘life left’ and therefore will be influenced by the general condition of the patient and the patient’s wishes.
Cross-sectional imaging
A CT of the abdomen and pelvis is done at the end of year one and year two after resection.
Tumour markers
The requirement for CEA measurements varies from hospital to hospital. It is not routinely done as there is still no evidence that the lead time
provided by CEA monitoring provides a survival advantage13.
However, in some high risk patients and those undergoing chemotherapy it may be appropriate and the patient may require CEA measurement
every 3 months for the first year, every 6 months for the second year and then annually to 5 years. However, this will depend on the prognosis
of the tumour and the treatment offered. In addition, one must consider whether the patient’s general condition would allow any disease
identified to be treated.
Clinical nurse specialist review
All the hospitals in the network are working toward implementing review by colorectal nurse specialist. The aims of the clinic would be to:
• arrange review investigations to identify local recurrence and metastases
• provide standardised approach to colorectal cancer review across the network
• psychological support
• symptom control
• support audit
• plan care and complete end of treatment summary
• undertake holistic needs assessment
It is envisaged that the minimum recommendations from the Association of Coloproctology of Great Britain and Ireland will be consider
appropriate in all the hospitals in the network. The patients will still be seen by the surgeon and oncologist as appropriate after surgery. Those
who hae a presumed curative resection will then be reviewed by the nurse specialist. Those with metastases will be seen by the oncologist,
11 Cost effectiveness analysis of intensive versus conventional follow up after curative resection for colorectal cancer. AG Reneham, ST O’Dwyer, DK Whynes. BMJ
2004; 328: 81-84. 12 Guidelines for follow up after resection of colorectal cancer. J H Scolefield, R J Steele. Gut 2002; 51 (Suppl V): v3-v5. 13 S Cairns, J H Scolefield (ed). Guidelines for colorectal screening in high risk groups. Gut 2002; 51 (Suppl V): v14.

46
surgeon or palliative care team depending on the extent and nature of the disease. The clinics will run alongside a consultant surgeon’s clinic
should further advice or assessment be required.
The review will include a form-based assessment including:
• history
• abdominal examination
• rectal examination
• sigmoidoscopy
• arrangement of the appropriate imaging
47
Metastatic colorectal cancer
Introduction
The chemotherapy regimes are under review at present and will change in the second half of 2005 depending on the NICE guidelines.
Liver metastases
Liver metastases are very common and will develop at some time in about half of those with colorectal carcinoma. The management plan
depends on the time of presentation, the extent of the spread, the performance status and the symptoms from the primary. Any patient with
liver metastases that may benefit from specialist care is referred to Kings College Hospital. In the first instance the patients details and the
images can be sent by email or on CD-ROM for consideration for specialist treatment such as surgery. SEE Liver resection guideleines
In general if the metastases are identified at the time of the detection of the primary (synchronous) then the patient is offered chemotherapy in
the first instance (possibly before resection of the primary tumour) and surgery offered if, at review, the disease is deemed operable. If the liver
metastases are detected more than 6 months after resection of the primary (metachronous) then the patient is offered liver surgery if
operable. The patients with non-operable lesions may be offered further chemotherapy or radiofrequency ablation. Some may only be suitable
palliative care.
Lung metastases
Lung metastases may occur in the absence of liver deposits especially with low rectal cancers. Patients with lung metastases are offered
chemotherapy and lung resection may be appropriate. The patients are referred for palliative care if lung resection is not feasible.
The criteria for diagnosis of lung metastases are:
• new single or multiple lesion seen on chest CT with previous examinations for comparison
• biopsy is not required
Brain
Brain metastases are uncommon but may occur especially in rectal carcinoma. Palliative radiotherapy may be of value. The patients are referred
for palliative care.
Ovarian ‘Krukenberg’ metastases
Spread to the ovaries is uncommon. If the ovaries are abnormal at the time of initial surgery then bilateral oophorectomy is required. If the
ovaries appear to be abnormal on subsequent imaging then the patient may be offered oophorectomy. Patients may be offered chemotherapy
or palliative care if no anti-tumour treatment is feasible.
Peritoneal seedlings
Peritoneal seedlings occur uncommonly in isolation but often follow colonic or rectal perforation. Chemotherapy is associated with a poor
response rate and few survive more than a year. The patients are referred for palliative care.
Bone metastases
Bone metastases are uncommon in colorectal cancer. Chemotherapy is of limited value but radiotherapy may be appropriate for bone pain. The
patients are referred for palliative care. Orthopaedic – cord compression / unstable pathological fractures.


49
Local recurrence
Colon cancer
Local recurrence is uncommon in colon cancer except after localised perforation occurring at presentation. Occasionally it is amenable to further
resection although it is usually too far advanced by the time that it is detected. Radiotherapy and chemotherapy may be of value but it is often
the case that the only practical treatment is palliative care.
The patient should imaging of the colon (barium enema, colonoscopy or CT enema) and cross-sectional imaging usually by CT of the chest,
abdomen and pelvis.
Rectal cancer
Local recurrence after resection for rectal cancer is identified by:
1 examination
2 sigmoidoscopy
3 colonoscopy
4 CT or MRI
5 PET scan may be useful after radiotherapy when it may be difficult to distinguish between fibrosis and tumour
It is confirmed histologically either by luminal biopsy at sigmoidoscopy or colonoscopy or percutaneous biopsy under CT control. The treatment
options are:
1 transanal excision of a small suture line recurrence
2 further radical resection by anterior resection, abdominoperineal resection, abdominoscaral resection or pelvic exenteration
3 proximal stoma if there are intractable rectal symptoms
4 radiotherapy possibly combined with chemotherapy
5 chemotherapy alone if previous treatment with radiotherapy
6 palliative care
7 laser ablation
8 stenting if high enough to have the stent lower margin away from the anal sphincter
9 Stereotactic body radiotherapy


51
Adjuvant therapy
Chemotherapy
Adjuvant chemotherapy is offered in several situations:
1 patients with poor prognosis colon and rectal cancers that are either node positive or they are node negative but have other poor
prognostic features such as extramural vascular invasion
2 patients with poor prognosis rectal cancers who have had pre-operative neoadjuvant therapy and in whom the histological staging
based on the resection specimen is inadequate because of down-staging by pre-operative treatment
Radiotherapy
Adjuvant radiotherapy is less commonly used but may be offered when:
1 there is a positive circumferential margin after TME for rectal cancer and no pre-operative treatment has been given
2 there a locally advanced or locally perforated colon cancer and therefore doubt about the completeness of the resection
3 retroperitoneal extension of caecal cancer
Neoadjuvant therapy
Patients with carcinoma of the rectum affecting the lower two thirds are offered neoadjuvant therapy (see flow chart in the section on rectal
cancer). Selection is based on the findings at MRI.

53
Family cancer screening
Introduction
Colorectal cancer is, at least in part, inherited. The risk to an individual depends on the number of relatives and the age at which they
developed colorectal cancer. This is for patients who have not had colorectal cancer themselves. Below is a brief summary of current guidelines.
Number affected Relatives affected Screening offered
1 One FDR <50 Colonoscopy once at 55y
Local family history +/- genetic clinic referral
1 FDR and 1FDR/ SDR (same side of family)
<60
Colonoscopy at 5 yearly 50-75
Local family history +/- genetic clinic referral
2
2 FDR (ave >59)
Colonoscopy at 55y
Local family history clinic referral
3 3 FDR/SDR but Amsterdam negative Colonoscopy every 5y 50 - 75y and Genetic referral
More than 3 Lynch Syndrome by Amsterdam criteria or
multiple colorectal polyps
Colonoscopy at 25y then every 2y until 75y.
Genetic referral
Polyposis (FAP)
Family history of familial adenomatous
polyposis
Genetic referral and also to St Mark’s Hospital.
All patients are referred to a family cancer clinic in line with the Regional Genetic Service Guidelines.
FDR= first degree relative.
SDR= second degree relative
LSRC=Lynch Syndrome related cancer (endometrial, ovarian, stomach, small bowel, brain, ureter, renal pelvis)
Dr L Izatt, Consultant
Clinical Genetics
7th Floor New Guy’s House
Guy’s Hospital
St Thomas Street
London SE1 9RT
Tel: 020 7188 1364 Secretary: 020 7188 1378 Fax: 020 7188 1369 Email: [email protected]

54
Colorectal polyp management
The recommended guidelines for screening and treatment of patients with familial hereditary non-polyposis colorectal cancer, juvenile polyposis and Peutz-Jegher’s syndrome are described in further detail elsewhere14.
Introduction
The management plan depends on the polyp histology. Many are incidental findings when the patient is being investigated for intestinal
symptoms. Some are identified on screening for familial colorectal cancer.
Adenocarcinoma in a polyp
A malignant polyp is treated as for the normal malignant tumour as described above. The problem decision arises when a pedunculated polyp
contains foci of carcinoma but it appears to be completely excised. The decision to do a large bowel resection when no further mural or nodal
disease is present may be difficult especially in the unfit patient.
Adenomas
The surveiilance guidelines after removal of colorectal adenomas depends on the risk of development of a carcinoma. Colon cancer is believed
to have a pre-malignant phase of adenoma formation and therefore adenoma eradication may reduce the risks of subsequently developing
colorectal carcinoma. The risk can be assessed on the size and number of adenomas15.
Initial colonoscopy and polypectomy
LOW RISK
1 or 2 adenomas
and
all < 1cm
INTERMEDIATE RISK
3 or 4 adenomas
or
one >1cm
HIGH RISK
5 or more small adenomas
or
3 or more< with one >1cm
Colonoscopy after 3 years Colonoscopy after 1 yearColonoscopy after 5 years
or no surveillance
1 clear colonoscopy: repeat after 3y
2 clear colonoscopies: cease review
Low/intermediate risk: repeat 3y
High risk: repeat 1y
Normal colonoscopy repeat 3y
Low/intermediate risk: repeat 3y
High risk: repeat 1y
No adenoma: cease review
Low risk: repeat after 5 y
Intermediate: repeat after 3y
High risk: repeat after 1y
The decision regarding the colonoscopic review also takes into account the completeness of the colonoscopy, intercurrent medical illness and
family history of colorectal carcinoma. The findings at colonoscopy then determine which group (low, medium or high risk) to which the patient
transfers until no further surveillance is required.
Metaplastic polyps
If the polyps are small in number no review is necessary. If they are serrated adenomas they are treated like adenomas as above. If there are a
large number of polyps they are referred to St Mark’s Hospital.
14 Guidance on gastrointestinal surveillance for hereditary non-polyposis colorectal cancer, familial adenomatous polyposis, juvenile polyposis and Peutz-Jeghers
syndrome. Gut 2002; 51 (Suppl V): v21-v27. 15 Surveillance guidelines after removal of colorectal adenomatous polyps. W S Atkins, B P Saunders. Gut 2002; 51 (Suppl V): v6-v9.
55
Audit and clinical research
Current clinical trials
The current clinical trials are described in the next section.
Completed audit projects
The completed network-wide audit projects are in the table.
Title Results Discussion Action
1 Anastomotic leak
Leaks occurring in 2002.
The leak rates were:
PRUH = 2/105= 2%
QMS = 2/80 = 2%
UHL = 0/35 = 0%
GSST = 3/98 = 3%
QEW = 5/104 = 4.8%
KCL = 4/84 = 4%
The anastomotic leak rate in all hospitals is
in keeping with the national figures.
No action required.
2 Quality of two-week
wait referrals
Fax referral from in April, May
and June 2003.
The number with colorectal
cancer were:
PRUH= 9/85 = 10.5%
QMS = 4/43 = 9.3%
UHL = 12/109 = 11%
GSST = 4/87 = 5%
QEW = 7/74 =9.45%
KCL = 7/97 = 7.2%
The figures are in line with what is found
nationally but it may be possible to improve
this by making the criteria for referral
clearer.
New fax referral form
developed.
3 Appropriateness of 2
week wait referrals
Fax referral from January,
February and March 2004.
The number considered
appropriate were:
PRUH (no data)
QMS = 53/63 = 81.5%
UHL = 95/113 = 84%
GSST = 50/77 = 64.9%
QEW = 96/110 = 87.2%
KCL = 65/65 = 100%
The figures are in line with what is found
nationally but it may be possible to improve
this by making the criteria for referral
clearer to reduce the inappropriate referrals.
New fax referral form
developed.
Current audit projects
The current network-wide audit projects are:
1. the outcome in patients not offered surgery (data collected for 2005 and survival is being reviewed at 3 and 5 years) . 2. the outcome in recurrent rectal cancer
Patient-held records
The booklets are now available for use in each Trust.
Integrating service improvement
The individual responsible for integrating service improvement is to be decided locally within each Trust. For the tumour working group, it has
been decided that the current chairman will assume this role.

57
Colorectal Trials
Non-Commercial Colorectal Studies
CD-16 Investigation of CD16+ cell number and function in patients with
advanced colorectal carcinoma before treatment and after two lines of standard treatment
Recruiting at: GSTFT
COIN-B A two-arm phase II randomised trial of intermittent chemotherapyplus continuous cetuximab and of intermittent chemotherapy plusintermittent cetuximab in first line treatment of patients with K-ras-normal (wild-type) metastatic colorectal cancer
GSTFT
NewEPOC A prospective randomised open label trial of oxaliplatin /
irinotecan plus fluoropyrimidine versus oxaliplatin / irinotecan plus fluoropyrimidine and cetuximab pre and post operatively in patients with resectable colorectal liver metastases requiring chemotherapy
GSTFT
NSCCG National Study of Colorectal Cancer Genetics GSTFT PRUH QEW QMS UHL
PICCOLO A randomised clinical trial of treatment for fluorouracil-resistant advanced colorectal cancer comparing standard single-agent irinotecan versus irinotecan plus panitumumab and versus irinotecan plus ciclosporin
GSTFT QEW
QUASAR II Multicentre international study capecitabine +/- bevacizumab as adjuvant treatment of colorectal cancer
GSTFT QEW UHL
SCOT Short Course Oncology Therapy - A study of Adjuvant Chemotherapy in colorectal cancer by the CACTUS & QUASAR 3 Groups
GSTFT QEW UHL
ARISTOTLE A phase III trial comparing standard versus novel CRT as preoperative treatment for MRI defined locally advanced rectal cancer GSTT FIREARC Functional Imaging and Early Response Evaluation In Rectal Cancer GSTT Commercial Colorectal Studies VELOUR GSTFT
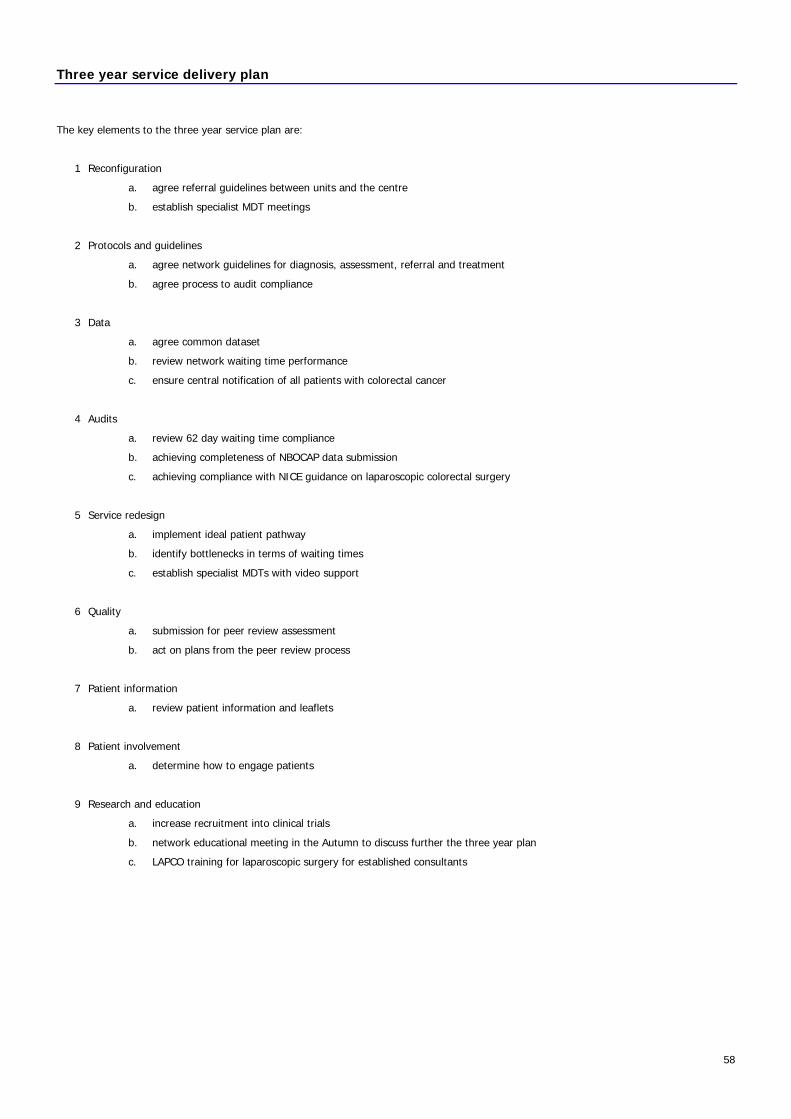
58
Three year service delivery plan
The key elements to the three year service plan are:
1 Reconfiguration
a. agree referral guidelines between units and the centre
b. establish specialist MDT meetings
2 Protocols and guidelines
a. agree network guidelines for diagnosis, assessment, referral and treatment
b. agree process to audit compliance
3 Data
a. agree common dataset
b. review network waiting time performance
c. ensure central notification of all patients with colorectal cancer
4 Audits
a. review 62 day waiting time compliance
b. achieving completeness of NBOCAP data submission
c. achieving compliance with NICE guidance on laparoscopic colorectal surgery
5 Service redesign
a. implement ideal patient pathway
b. identify bottlenecks in terms of waiting times
c. establish specialist MDTs with video support
6 Quality
a. submission for peer review assessment
b. act on plans from the peer review process
7 Patient information
a. review patient information and leaflets
8 Patient involvement
a. determine how to engage patients
9 Research and education
a. increase recruitment into clinical trials
b. network educational meeting in the Autumn to discuss further the three year plan
c. LAPCO training for laparoscopic surgery for established consultants

59
Index
2 week referral fax ............................................................ 15, 17
Adenomas .............................................................................. 47
serrated .............................................................................. 47
Adjuvant chemotherapy................................................21, 24, 43
Adjuvant radiotherapy ....................................................... 21, 43
Anal cancer....................................................................... 25, 29
Anterior resection.................................................................... 23
Antibiotic prophylaxis............................................................... 27
AP resection............................................................................ 23
Attendance at meetings ............................................................. 8
Bone metastases..................................................................... 39
Bowel preparation ................................................................... 27
Brain metastases..................................................................... 39
CEA........................................................................................ 37
Chairman’s roles........................................................................ 7
Chemotherapy ........................................................................ 21
Colon cancer ..................................................................... 21, 29
Colonic polyps......................................................................... 47
Colonoscopy ........................................................................... 27
Colorectal stenting .................................................................. 35
Consent .................................................................................. 27
Current audit projects.............................................................. 49
Current trials........................................................................... 49
DVT prophylaxis ...................................................................... 27
Emergency presentation .......................................................... 35
Family cancer screening........................................................... 45
FAP ........................................................................................ 45
Follow up plan ........................................................................ 18
Guy’s and St Thomas’s Hospital.............................................. 7, 9
HDU ....................................................................................... 27
HNPCC ................................................................................... 45
Hospitals
Guy’s and St Thomas’s ....................................................... 7, 9
Kings College................................................................... 7, 10
Princess Royal University Hospital ..................................... 7, 11
Queen Elizabeth Hospital .................................................. 7, 12
Queen Mary Hospital ........................................................ 7, 13
University Hospital Lewisham............................................ 7, 14
Intestinal haemorrhage ........................................................... 35
Intestinal obstruction............................................................... 35
Intestinal perforation............................................................... 35
ITU ........................................................................................ 27
Key worker ............................................................................. 22
Kings College Hospital ......................................................... 7, 10
Krukenberg metastases ........................................................... 39
Laparoscopic colorectal resection ............................................. 24
Liver metastases ............................................................... 21, 39
metachronous...................................................................... 39
synchronous ........................................................................ 39
Local recurrence................................................................ 18, 41
colon cancer ........................................................................ 41
prevention ........................................................................... 23
rectal cancer ........................................................................ 41
Lung metastases ..................................................................... 39
Membership of the group...........................................................3
Metaplastic polyps ................................................................... 47
Metastases.............................................................................. 39
bone ................................................................................... 39
brain ................................................................................... 39
liver..................................................................................... 39
lung .................................................................................... 39
ovarian................................................................................ 39
peritoneum.......................................................................... 39
Microsatellite instability ............................................................ 19
MLH1...................................................................................... 19
MSH2 ..................................................................................... 19
Neoadjuvant chemoradiotherapy .............................................. 24
Neoadjuvant radiotherapy........................................................ 43
Neoadjuvant therapy ......................................................... 18, 23
Nurse specialist review............................................................. 37
Oncology assessment .............................................................. 21
Operation records.................................................................... 27
Ovarian metastases ................................................................. 39
Palliative care.................................... 18, 21, 23, 35, 59, 60,61,62
Patient held records................................................................. 49
Peritoneal seedlings................................................................. 39
Polyposis................................................................................. 45
Pre-assessment clinic............................................................... 27
Preparation for surgery ............................................................ 27
Princess Royal University Hospital......................................... 7, 11
Proposed audit projects ........................................................... 51
Proposed trials ........................................................................ 51
Queen Elizabeth Hospital ..................................................... 7, 12
Queen Mary Hospital ........................................................... 7, 13
Rectal cancer .................................................................... 23, 29
Rectal stump washout ............................................................. 23
Referral ..................................................................................18
Referral from other teams........................................................ 15
Referral guidelines................................................................... 15
Referral to and from networks.................................................. 15
Referral to specialist team........................................................ 35
Review after curative surgery................................................... 37
SELCN
Hospitals in the group ............................................................7
TWG membership ..................................................................3
Serrated adenomas ................................................................. 47
60
Service improvement............................................................... 49
Short course radiotherapy........................................................ 23
Staging............................................................................. 18, 31
Dukes ................................................................................. 31
TNM.................................................................................... 31
Stenting.................................................................................. 35
Stents..................................................................................... 35
Stoma formation ..................................................................... 27
Stoma nurse assessment ......................................................... 27
Surveillance after surgery ........................................................ 37
TEM ....................................................................................... 23
Terms of reference.................................................................... 3
Three-year plan ...................................................................... 53
Total mesorectal excision......................................................... 23
Trananal excision .................................................................... 23
Transanal endoscopic microsurgery .................................... 23, 24
Transanal excision ................................................................... 24
Trials
ACT II ................................................................................. 51
CLOCC................................................................................. 51
COIN................................................................................... 51
EPIC.................................................................................... 51
EXPERT-C ............................................................................ 51
EXTRA................................................................................. 51
NSCCG ................................................................................ 51
Tumour markers...................................................................... 37
Tumour working group membership ...........................................3
University Hospital Lewisham ............................................... 7, 14
Waiting times .......................................................................... 19
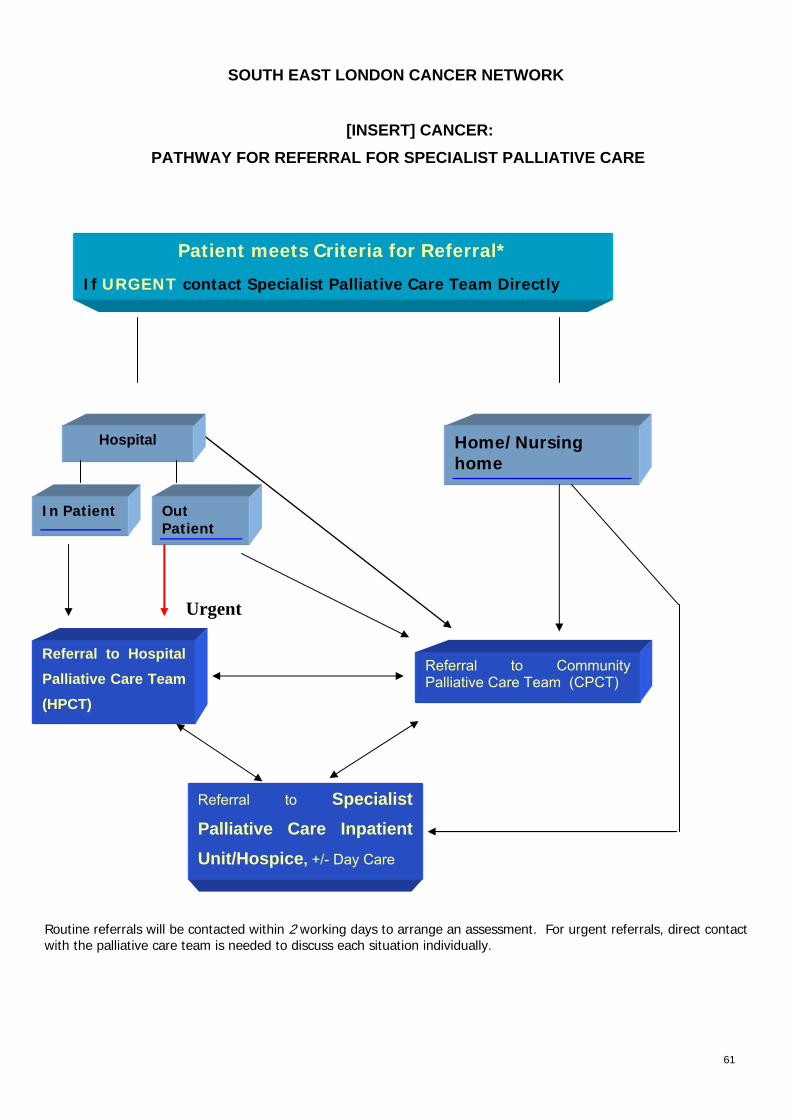
61
SOUTH EAST LONDON CANCER NETWORK
[INSERT] CANCER: PATHWAY FOR REFERRAL FOR SPECIALIST PALLIATIVE CARE
Patient meets Criteria for Referral*
If URGENT contact Specialist Palliative Care Team Directly
Routine referrals will be contacted within 2 working days to arrange an assessment. For urgent referrals, direct contact with the palliative care team is needed to discuss each situation individually.
Home/Nursing home
In Patient Out Patient
Referral to Hospital Palliative Care Team (HPCT)
Referral to Community Palliative Care Team (CPCT)
Hospital
Urgent
Referral to Specialist Palliative Care Inpatient Unit/Hospice, +/- Day Care

62
Criteria for Referral∗
Most patients will have an advanced, progressive disease, where the focus of care will have changed from curative to palliative and the prognosis is limited. Some patients, who have complex specialist needs, can be referred at an earlier stage, from diagnosis onwards. Patients may be discharged if their condition stabilises. A demonstrable need for specialist palliative care services must be established. Appropriate reasons for referral may include potential / existing difficulties with the following:
Pain and Symptom management
Meeting the psycho-social needs of the patient & their family, and/or significant others
Terminal Care/Dying
• Where possible, the patient, and if not, the carer, should be informed and in agreement with the referral
• Any Health Care Professional can refer to the Specialist Palliative Care Team, but acceptance must be
with the agreement of the GP or inpatient Consultant
Criteria for Urgent Referral: needing advice/assessment within 1-2 working days.
• Difficult psychological/physical symptoms causing distress and not responding to current management
• Rapidly deteriorating condition
Mechanisms of Referral Hospital Palliative Care Teams
Hospital Contact Details Method of Referral
King's College Hospital Telephone 020 3299 4060
Fax 020 3299 4713
Telephone
GSTT St Thomas':
020 7188 4755
Fax 020 7188 4720
Guy's
020 7188 4754
Fax 020 7188 4748
Referral form
Queen Elizabeth Hospital,
Woolwich
020 8836 5442
Fax 020 8836 5428
Telephone
Queen Mary's Hospital,
Sidcup
020 8308 3295
Fax 020 8308 3168
Telephone
Princess Royal University
Hospital
01689 825755
Fax 01689 892999
PRUH hospital Bleep 745/629
Telephone
Lewisham Hospital 020 8333 3017
Fax 020 8333 3270
Referral form
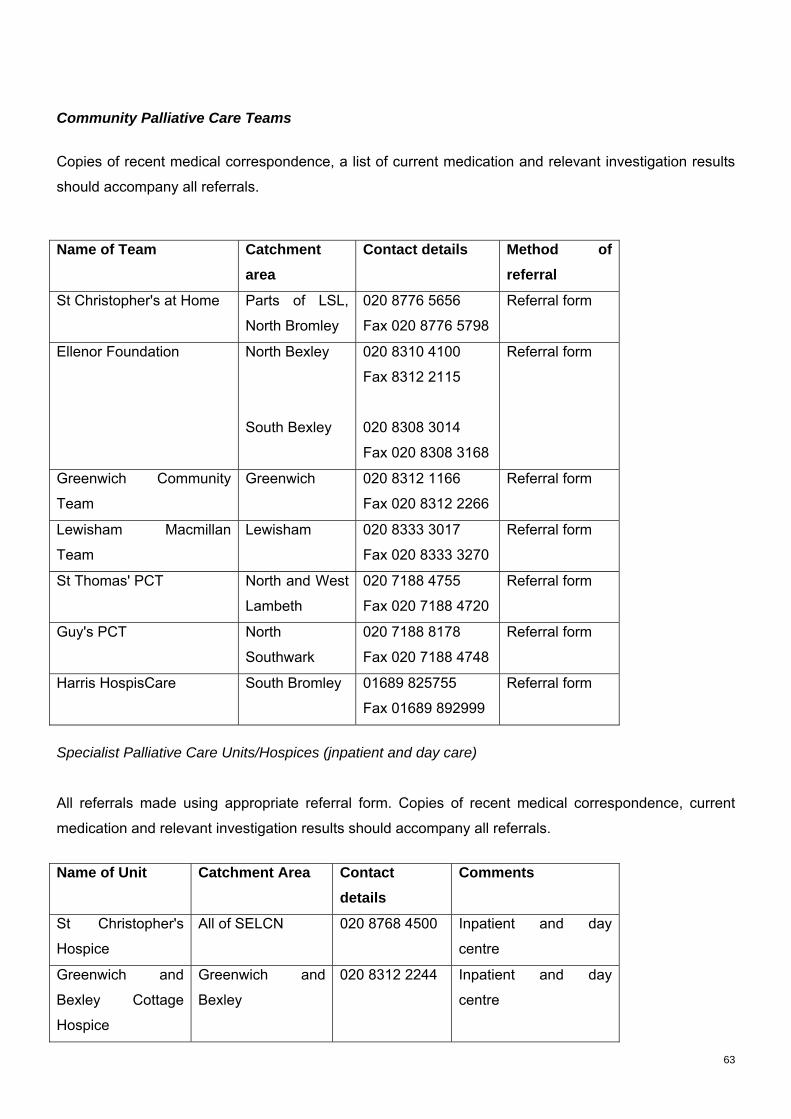
63
Community Palliative Care Teams
Copies of recent medical correspondence, a list of current medication and relevant investigation results
should accompany all referrals.
Name of Team Catchment area
Contact details Method of referral
St Christopher's at Home Parts of LSL,
North Bromley
020 8776 5656
Fax 020 8776 5798
Referral form
Ellenor Foundation North Bexley
South Bexley
020 8310 4100
Fax 8312 2115
020 8308 3014
Fax 020 8308 3168
Referral form
Greenwich Community
Team
Greenwich 020 8312 1166
Fax 020 8312 2266
Referral form
Lewisham Macmillan
Team
Lewisham 020 8333 3017
Fax 020 8333 3270
Referral form
St Thomas' PCT North and West
Lambeth
020 7188 4755
Fax 020 7188 4720
Referral form
Guy's PCT North
Southwark
020 7188 8178
Fax 020 7188 4748
Referral form
Harris HospisCare South Bromley 01689 825755
Fax 01689 892999
Referral form
Specialist Palliative Care Units/Hospices (jnpatient and day care)
All referrals made using appropriate referral form. Copies of recent medical correspondence, current
medication and relevant investigation results should accompany all referrals.
Name of Unit Catchment Area Contact details
Comments
St Christopher's
Hospice
All of SELCN 020 8768 4500 Inpatient and day
centre
Greenwich and
Bexley Cottage
Hospice
Greenwich and
Bexley
020 8312 2244 Inpatient and day
centre
64
Trinity Hospice LSL 020 7787 1000 Inpatient and day
centre
Harris HospisCare South Bromley
01689 605300
Fax 01689
605303
Day centre
Richard Dimbleby
Cancer Information
and Support
Service
All of SELCN 020 7188 5918 Information centre and
psychological support
service
Symptom Control Guidelines South East London Cancer Network Palliative Care Coordinating Group have developed guidelines for
management of common symptoms within the hospital or community setting. These guidelines are
available from your local Specialist Palliative Care Team or by contacting SELCN on 020 7188 7090
65
66
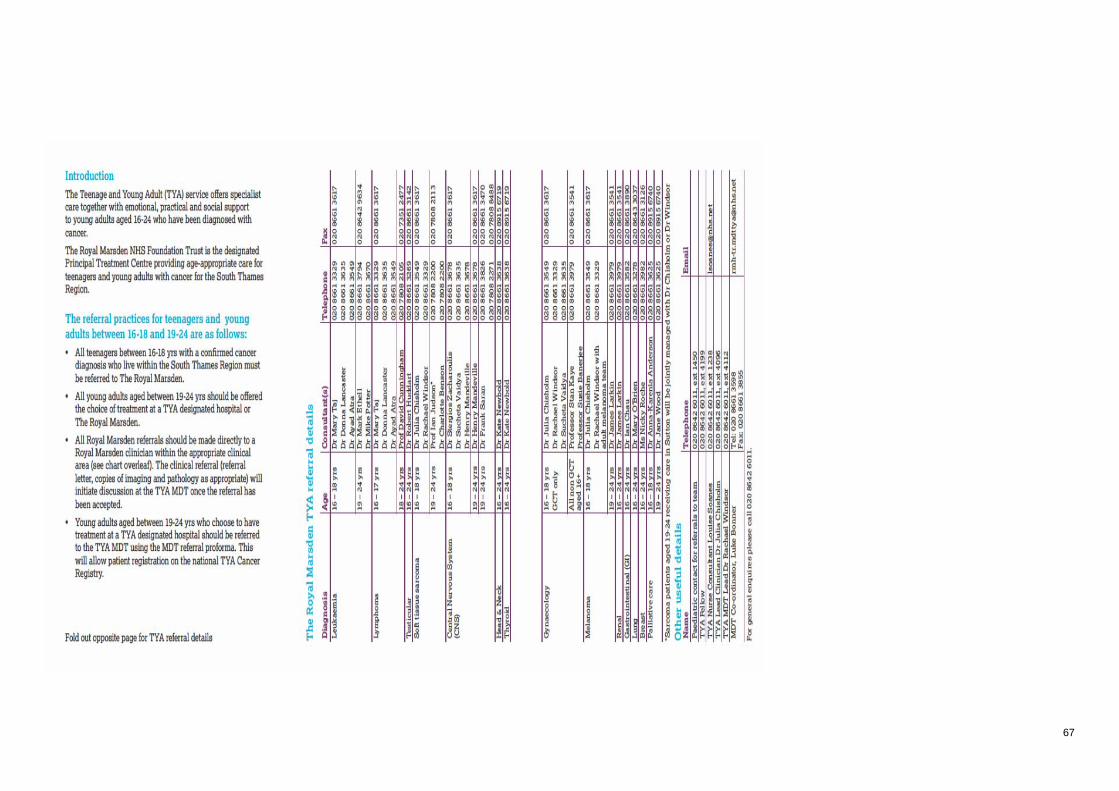
67
68
King’s College Hospital NHS Foundation Trust Hepato-biliary and Pancreatic Service
CLINICAL GUIDELINES FOR THE MANGEMENT OF PATIENTS WITH COLORECTAL LIVER METASTASES
as included in the Operational Policy for the care of patients with suspected hepato-biliary and pancreatic malignancies (HPB)
South East London Cancer Network
Kent & Medway Cancer Network

69
70
Introduction In September 2006 King’s was designated as the specialist centre for all patients with colorectal liver metastatic disease from both the SE London and Kent and Medway Cancer Networks. King’s had a successful Peer Review as a Liver Resection MDT for patients with colorectal liver metastases in October 2007.
Recent advances in liver surgery and new chemotherapeutic agents have altered the approach to colorectal liver metastases (CLM)
dramatically. Of the almost 50-60% of patients with colorectal cancer who develop liver metastases, it is expected that up to 40% will be
amenable to resection, more than doubling the historic resection rate of 10-15%, and more than 40% of these patients will be alive and disease
free at 5 years post-resection (compared to an untreated 5 year survival rate of less than 1%).
Therefore, it is recommended that the majority of patients with CLM are assessed by a specialist HPB MDT, for resection of their disease. In
fact, most authorities agree that the only independent limiting factor (out with co-morbidity preclusion) for resecting CLM is the volume of the
remaining functional liver.
Referral guidelines Patients with synchronous liver metastases, with treatment for their primary disease planned/underway, should be referred to King’s, following
discussion at an outreach MDM, with a copy of the outreach MDM outcome and proforma for tracking purposes and to enable the advice given
by the King’s HPB surgeon to be logged. These patients will not be required to attend for King’s outpatient review unless subsequent outreach
MDM review decides this is appropriate at a later date.
Patients who have developed liver metastases subsequent to treatment of their primary, where resection of their liver disease is considered
possible if downstaged, at outreach MDM, and who are awaiting/undergoing second-line chemotherapy should be referred to King’s with MDM
outcome and completed proforma, again for tracking purposes and to enable advice given by King’s surgeon to be logged. We recognise that
there may be a subsequent c.3-6 month wait while the patient completes chemotherapy.
Patients whose liver disease is deemed immediately resectable at an outreach MDM should be referred up with MDM outcome, proforma and all
imaging for review at the King’s liver resection MDM and review in HPB outpatients’ clinic. These patients will need pre-assessing at King’s.
Imaging guidelines The patient referred to King’s for management of colorectal liver metastases is likely to have had previous investigations including staging CT at
the time of their original diagnosis of colorectal cancer and subsequent follow or restaging scan series. The patient may have had a PET, CT
PET or MRI scan for further staging.
It is very important that when the patient is initially referred to King’s for collaborative management of their hepatic metastatic disease their
imaging is included in the referral. Ideally, a CD of all of their scans to date should be forwarded with the referral. Contrast enhanced CT of
chest, abdomen and pelvis remains the gold standard in imaging patients with CLM and patients should be referred when this CT has been
obtained. Baseline LFTs and CEA should also be part of the initial investigations
Subsequent imaging may not be required, but if it is then the following will be considered:
o Ultrasound o CT o MRI o PET scan o Imaging guided biopsy [CT or USS] o Portal Vein Embolisation [for liver volume modulation prior to resection]
Details of techniques used are included in the Network Imaging Group protocol.
At the time of treatment for CLM, the latest axial staging imaging must not be more than 6 weeks old.
Further axial imaging in the form of MRI will occasionally be used after review of the initial CT at King’s HPB MDM in cases where diagnosis is
uncertain or additional information is required prior to planning surgery (i.e. vascular and/or biliary anatomy considerations).
71
The role of PET scanning is under evaluation worldwide and definitive results are awaited. Its use for patients evaluated at King’s HPB MDM is
for discussion on a case by case basis and would usually only be indicated in the setting of excluding the presence of extra-hepatic disease
when liver resection is planned in the presence of unfavourable history i.e. ruptured primary, or primary tumour histology, e.g. pT4 and/or N2, or
where there is suspicion of pulmonary spread.
Other investigative measures such as EUS, image guided biopsy and laparoscopic biopsy can also be used when there are specific clinical
needs.
Intra-luminal staging remains within the spectrum of responsibilities of the colorectal team treating or who have treated the primary tumour.
Pre-operative evaluation Any liver resection irrespective of the extent or the mode (laparoscopic or open) should be considered as major surgery. In addition, the majority
of these patients would have undergone various periods of systemic chemotherapy. Therefore, appropriate cardiovascular, respiratory and
nutritional assessment is mandatory.
These patients should be assessed by an anaesthetist at King’s prior to their admission for surgery and based on this evaluation of peri-
operative risk additional investigations may be requested.
Every patient coming in for a liver resection should have the following baseline investigations done:
FBC, U&Es, clotting profile, LFTs, tumour markers (CEA and CA19.9), chest x-ray, ECG, cross-match of appropriate amount of blood, screen
for nosocomial pathogens and the first stage of consent taken by a member of the surgical team.
Surgical planning The exact type of liver resection should have been discussed and decided at King’s HPB MDM prior to surgery. Operative strategies can and
should change according to intra-operative findings. However, the following principles should be observed:
I. Complete tumour clearance with clear resection margins; when anatomically feasible the rule of 1cm should be observed II. Full evaluation of the liver with intra-operative USS, as this can add to intra-operative resection planning and uncover previously
undetected lesions. With the role of laparoscopic staging rapidly evolving it is anticipated that this modality will also be part of the final evaluation prior to resection.
III. Planning for resection should (if possible) take into account the ¨mapping¨ of the disease at the time of presentation, as there is growing evidence that even lesions with complete radiological response to chemotherapy can re-grow if no definitive treatment is applied. When this is not possible (due to remnant functional liver mass) alternative strategies should be adopted (e.g. RFA or closer post-operative surveillance).
IV. Contraindications for liver resection at the time of the final assessment remain the presence of peritoneal spread and porta-hepatis nodal involvement
V. Where the liver resection is following a course of chemotherapy provisions should be made for a ¨wash-out¨ period of 4-6 weeks between the completion of chemotherapy and surgery.
Additional strategies to increase resectability:
Portal vein embolisation (PVE)
When, on CT volumetric studies, the expected remnant functional liver mass after the proposed hepatectomy would be marginal, or inadequate,
percutaneous right portal vein embolisation should be explored as a mode to induce compensatory hypertrophy of the unaffected part of the
liver, thus facilitating an extended right hepatectomy. If satisfactory response is achieved then resection is scheduled no later than 6-8 weeks
after the PVE.
Two-stage hepatectomy
For patients with bi-lobar multi-nodular disease when complete removal of all tumours is thought not possible with a single procedure a two-
stage approach can be adopted by first resecting the most tumour laden lobe. Allowing for a period of 6 weeks for regeneration of the remnant
72
liver, resection is then completed with removal of part of the remaining liver lobe. This approach can be combined with PVE prior to the first
stage and/or RFA of the remnant tumours at either stage.
Laparoscopic liver resection
In recent years there has been a very dynamic expansion in the application of laparoscopic techniques in HPB surgery. There is now enough
data to support its role in the treatment of patients with CLM. Although almost any type of liver resection can be performed laparoscopically
there is not wider consensus for a blanket application of the method, owing predominantly to the lack of long-term survival data.
At King’s every patient with CLM who requires resection of up to 2 liver segments in anatomically favourable sites is considered for laparoscopic
liver resection. It is envisaged that as experience and data accumulate, the spectrum of this mode will increase.
Radio-Frequency Ablation (RFA) Although resection remains the gold standard for treatment of CLM the availability of RFA can significantly add to the treatment options
particularly for patients who:
I. Are not candidates for liver resection due to poor performance status
II. Have multi-focal disease that cannot be resected (even after the implementation of the previously discussed pre-operative strategies)
III. Have recurrent disease in their liver remnant that will not tolerate further resection
IV. Are not willing to undergo liver resection, but would accept a less invasive mode of treatment
V. Require consideration of RFA in combination with liver resection when parenchyma sparing is required as means of control of otherwise irresectable disease
VI. Finally, as a part of a two-stage hepatectomy, as outlined above
RFA will be delivered either percutaneously or intra-operatively (laparoscopic or open) based on individual patient needs.
Synchronous liver lesions There is sufficient evidence to support the simultaneous treatment of the primary colorectal tumour and the CLM. Emerging evidence may
support dual surgical approach in low volume/solitary CLM. However, most centres avoid combining a major liver resection (more than 3 liver
segments) with left-sided or pelvic colectomies due to increased risk for post-operative liver failure and/or septic complications from anastomotic
leaks (see guidelines below).
It is pertinent to note however that the long-term prognosis is not influenced by simultaneous surgery and the vast majority of data reflect results
from the staggered approach.
In the same context major liver resections should not be combined with other major GI tract procedures (i.e. reversal of covering stomas).
Liver and pulmonary metastatic disease The simultaneous presence of liver and lung colorectal metastases does not preclude the surgical treatment of both sites. If by thoracic criteria
the pulmonary disease is resectable then the CLM should be assessed for treatment and this should be completed prior to the lung resection(s).
The advent of RFA for pulmonary metastases can further enhance the therapeutic options for this group of patients.
Resection with (neo-) adjuvant chemotherapy As much as chemotherapy has transformed the treatment of CLM and has been the key factor in the increase in the resectability rate, the ideal
protocol is yet to be defined. The length and the agents will depend on:
I. the presentation (synchronous vs. metachronous) II. any previous chemotherapy treatment and observed response rate III. any previous liver resection
73
IV. the disease free interval
Current evidence suggests that a staggered approach (chemotherapy-surgery-chemotherapy) may offer the best results for patients treated for
their CLM for the first time.
Guidelines for combined HPB and other surgical interventions We have agreed guidelines for the management of patients who require a HPB surgical intervention in combination with other surgery:
Surgeon from another Trust operating at King’s
The patient is admitted under the King’s HPB consultant who takes full responsibility for the care of that patient, even if the HPB part of the
operation is the more minor.
King’s HPB surgeon operating at another Trust
The patient is admitted under the local Trust consultant who takes full responsibility for the care of that patient. If the HPB part of the operation
is the more major then that surgery should not be taking place off site.
No pancreatic resections or liver resections for colorectal liver metastases can be undertaken off site as this would contravene the IOG.
Surgeon from within King’s operating with King’s HPB team
The surgeon performing the more major part of the operation should agree to admit the patient under their name, to one of their wards and take
overall responsibility for the operation.
Combined liver and other organ resection when consultants from other specialties are involved:
Liver surgery and colonic resection
As a rule, when the liver resection is of >2 segments, or is 2 liver segments but is combined with RFA, the index consultant will be the HPB
surgeon.
When the colonic resection is left sided or a pelvic resection the liver resection is commonly ≤ 2 liver segments and the index surgeon is the
colorectal surgeon.
When only operative RFA ≤3 lesions, is performed then the colorectal surgeon is the index surgeon.
If the RFA is to <3 lesions then the index surgeon is the HPB surgeon.
N.B. these are general guidelines that it is hoped will help clinicians in decision making. When the clinical situation indicates a need for
deviation it is expected that appropriate discussions will take place between the clinicians involved, confirmed in MDM(s) if necessary.
It is important to stress however, that one clinician will always be identified as the index surgeon.
Pathology Description and sampling of the tumour are carried out in compliance with the guidelines issued by the Royal College of Pathologists (RCPath)
in 2007 (minimum dataset for histopathological reporting of primary and metastatic carcinoma). The specimen is measured and weighed.
Location and size of the tumour are noted. When relevant specimens are photographed. The relationship between tumour and resection margin
is noted and the distance of the tumour from the resection margin is measured macroscopically. The margin usually considered during
macroscopic examination, sampled and assessed microscopically is the hepatic transection margin unless indicated otherwise by the surgeon.
Tumours are graded into well, moderately and poorly differentiated. The presence of necrosis, invasion of vascular/biliary structures, liver
capsule and peri-hepatic tissue is noted.
74
The possibility of integrating electronic templates into the histopathology reporting system is being considered for the update of the system,
which should take place in 2009.
All resection specimens are discussed at the weekly MDT meeting.
Oncology (10-2D-216) Patients with potentially resectable colorectal liver metastases are considered for peri-operative chemotherapy with an oxaliplatin containing
regimen.
Cape-Ox Capecitabine 1000 mg/m2 twice daily for 14 days
Oxaliplatin 130 mg/m2 day 1
Repeated every 21 days
Oxaliplatin modified deGramont schedule:
Oxaliplatin 85 mg/m2 day 1
Leucovorin 200 mg/m2 day 1
5FU bolus 400 mg/m2 day 1
5FU infusion 2400 mg/m2 over 46 hours
Repeated every 14 days
Chemotherapy for patients given as a combination treatment with metastatectomy is managed by either the core oncology member of the liver
resection MDT, or by an oncologist from the referring colorectal MDT following discussion and treatment planning in the liver resection MDT.
Clinical Trials
Resectable liver metastases
NEW EPOC- A prospective randomised open label trial of oxaliplatin/irinotecan plus fluoropyrimidine versus oxaliplatin/irinotecan plus
fluoropyrimidine and cetuximab pre and post operatively in patients with resectable colorectal liver metastases requiring chemotherapy
Irresectable liver metastases
BOXER – a phase II trial of capecitabine, oxaliplatin and bevacizumab in patients with non-resectable liver metastases from colorectal cancer
FOXFIRE
Due to start 2010 – a trial of SIR-spheres +/- chemotherapy for patients with irresectable liver metastases form colorectal cancer.
Follow-up Following a liver resection for CLM at King’s patients will be seen in King’s HPB outpatient clinic 2-3 weeks post-discharge. By then plans for
further treatment should be in place with their local oncologist. If there are no active surgical/ hepatological issues the patients can be
discharged from further HPB follow-up. Referral back to the specialist liver MDT would be triggered by evidence of disease of recurrence within
the remaining liver on surveillance CT scans.
In cases where further surgery (i.e. a staged hepatectomy) or other interventional procedures (i.e. RFA) or in cases where there is known
residual disease within the liver, these patients will continue to attend King’s HPB outpatient clinics until all active issues are resolved.
Although the issue of post-liver resection baseline CT scan is still a matter for debate it is appropriate for these patients to have a CT scan
locally 4-6 weeks after their resection when post-operative changes have diminished and regeneration would be expected to have mostly
completed. It would also roughly match the initiation of their adjuvant chemotherapy (when appropriate).

75
The CT surveillance should follow a 6 monthly pattern for the first 3 years following liver resection, as the bulk of recurrences are observed
during that timeframe and a12 monthly pattern thereafter until 5 years post-resection. These surveillance CTs should be promptly sent for
review at King’s MDM.
Clinical examination, LFTs and tumour markers should complete the surveillance protocol. It is hoped that the above will be facilitated locally.

76
All HPB malignancies:
Inoperable disease: Patients who are not candidates for any type of surgery due to disease extent should have their endoscopic palliation + chemotherapy and,
when the need arises, palliative care locally. This should be organised in a manner that saves further centre outpatient visits unless the
required procedures/treatments cannot be offered locally. Follow up should be provided by local oncologists (when appropriate), referring
physicians and general practitioner.
Unfit for surgery: Medically unfit patients should receive whatever care is appropriate (chemotherapy, palliative care) locally without further coming to the centre
outpatients. Referring physicians/oncologist/general practitioner should provide their follow up.
Palliative Care: For patients who would benefit from palliative care team only, this should be provided locally. Efforts should be made for these patients to avoid
centre outpatients – even at the referral stage – and their palliative care should be organised following initial MDM discussion.
It is important to note that survival data (disease recurrence, mode of disease progression) obtained during the follow up of patients with pancreatic cancer assessed and /or treated at King’s College Hospital, should be communicated back to King’s College Hospital for appropriate completion of patient records.
• Patients will initially be presented at their local MDT. Patients for a liver resection opinion are referred to Kings. A referral letter with the patient’s clinical details, serial CEA levels and TNM staging of the primary tumour should be faxed prior to discussion at the MDM.
The patient is the responsibility of the colorectal MDT until the opinion for the liver resection MDT. After the liver resection MDT the patient will then remain under the liver team if resection is offered or be referred back to the colorectal MDT if liver resection is not offered.

77
TO : HPB Team A/o CONSULTANT NAME : (If applicable)
New patient Response to treatment
Relapse Other
Please specify below*
Patient:
Surname:
Forename:
Date of Birth:
NHS No:
Hospital No:
Address:
Postcode:
Tel.no:
GP:
GP Practice Code:
Dr:
Address:
Post code:
Tel.no:
Fax no:
Email:
Primary diagnosis :
Date of primary diagnosis :
Primary Treated : Y N If not yet but planned – date :
How Treated : Neo-adjuvant therapy Surgery Adjuvant therapy
Date treated :
If Surgery was this an Elective / Emergency procedure (delete as applicable)
Metastatic disease suspected : At primary diagnosis / Metachronously
Details of neo-adjuvant therapy : (if applicable)
Type :
Start date :
Completion date :
Overall response :
Surgical details : eg Operation type
Staging :
Has patient had adjuvant chemotherapy? Y / N
If Y – please state regime :
Date completed :
OR

78
Date started :
Date due to complete :
Imaging Pre chemo Post chemo
USS
CT
MRI
PET
Please send available imaging
Pre op CEA : Date :
Post op CEA : Date :
Current CEA : Date :
Reason for referral : *if urgent pls contact SpR/Consultant on call via switchboard 020 7737 4000
Advice Only Assessment for surgery Assessment for RFA
Other : pls state :
Question(s) to be answered by multi-disciplinary team meeting :
Has patient been informed of referral?
Provisional diagnosis :
Have pathology reports/slides been sent? Y/N
To :
Have imaging results been sent ? Y/N
Hard copy / CD
Patient fitness to travel to centre: Y / N – may require transport
Patient preference/concerns re treatment?
Referred by: at :
Contact details:
Fax no. please (ESSENTIAL for rapid feedback):
Date: CNS Name :
Additional information or attach referral letter : pls include any relevant PMHx.

79
Outcome : MDM Centre use only
Patient listed for mdm : Y/N : If Y date
If N pls state why ?
Outcome of discussion sent to referee ? Y / N
If Y date If N pls state why ?
Completed by : (name in capitals) (signature)
FOR MDM DISCUSSION ALL IMAGING AND HISTOLOGY MUST BE PROVIDED Fax this form to 020 3299 1778 HPB MDT Administrator, KH1453, Institute of Liver Studies, KCH, Denmark Hill, London, SE5 9RS
HPB Service central email address: [email protected] Telephone: 020 3299 5188