Embed Size (px)
Citation preview

Downloaded from UvA-DARE, the institutional repository of the University of Amsterdam (UvA)http://hdl.handle.net/11245/2.55900
File ID uvapub:55900Filename ThesisVersion unknown
SOURCE (OR PART OF THE FOLLOWING SOURCE):Type PhD thesisTitle Primary hyperoxaluria type 1 : clinical, genetic and biochemical studiesAuthor(s) C.S. van WoerdenFaculty AMC-UvAYear 2008
FULL BIBLIOGRAPHIC DETAILS: http://hdl.handle.net/11245/1.385455
Copyright It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/orcopyright holder(s), other than for strictly personal, individual use, unless the work is under an open content licence (likeCreative Commons). UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)(pagedate: 2014-11-23)

PRIMARY HYPEROXALURIA TYPE 1:
clinical, genetic and biochemical studies
PR
IMA
RY
HY
PE
RO
XA
LU
RIA
TY
PE
1: c
linic
al, g
en
etic
an
d b
ioch
em
ica
l stu
die
sC
HR
IST
IAA
N V
AN
WO
ER
DE
N
Christiaan
van Woerden
01.6
01.10 01.7
01.2
01.3 01.5
FIGURES CHAPTER 01

Primary hyperoxaluria type 1:
clinical, genetic and biochemical studies
Christiaan van Woerden
VAN WOERDEN 5/19/08 8:53 AM Pagina 1

Primary hyperoxaluria type 1: clinical, genetic and biochemical studies.
Thesis, Academic Medical Center - University of Amsterdam, The Netherlands. With summary in Dutch.
ISBN 978-90-9023208-9
© 2008 Christiaan van Woerden, Amsterdam, The Netherlands
Lies KindtLies KindtHanna HirschChristiaan van WoerdenGildeprint Drukkerijen B.V., Enschede
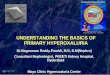
Birefringent calcium oxalate crystals in a kidney biopsy specimen visualized by polarized light microscopy
This work has been supported by grants of the Stichting MetaboleZiekten and de Stichting tot Steun Emma Kinderziekenhuis.
Financial support for the printing of this thesis was kindly provided by OxThera, Altus Pharmaceuticals, Ferring BV Hoofddorp,Stichting Metabole Ziekten, Actelion Pharmaceuticals Nederland BV,Novo Nordisk BV, Baxter BV.
Lay-out
Cover design
Portrait author
Cover photograph
Printed by
Cover photo:
VAN WOERDEN 5/19/08 8:53 AM Pagina 2

PRIMARY HYPEROXALURIA TYPE 1:clinical, genetic and biochemical studies
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctoraan de Universiteit van Amsterdamop gezag van de Rector Magnificus
prof. dr. D.C. van den Boomten overstaan van een door het college voor promoties
ingestelde commissie,in het openbaar te verdedigen in de Agnietenkapel
op dinsdag 1 juli 2008, te 12:00 uur
door
Christiaan Simon van Woerdengeboren te Gouda
VAN WOERDEN 5/19/08 8:53 AM Pagina 3

PROMOTIECOMMISSIE
Promotores:
Prof. dr. F.A. WijburgProf. dr. R.J.A. Wanders
Co-promotores:
Dr. J.W. GroothoffDr. M. Duran
Overige Leden:
Prof. dr. J.M.F.G. Aertsdr. S. FerdinandusseProf. dr. A.J. van der HeijdenProf. dr. H.S.A. HeymansProf. dr. B. HoppeProf. dr. R.T. Krediet
Faculteit der Geneeskunde
VAN WOERDEN 5/19/08 8:53 AM Pagina 4

PRIMARY HYPEROXALURIA TYPE 1:
clinical, genetic and biochemical studies
Christiaan
van Woerden
VAN WOERDEN 5/19/08 8:53 AM Pagina 5

ABBREVIATIONS
alanine:glyoxylate aminotransferasegene encoding AGTAGT deficient mousecompound developmental scoreconfidence intervalcross reactive materialD-amino acid oxidaseenzymeendogenous oxalate productionend-stage renal diseasegas chromatography - mass spectrometryglomerular filtration rateglutamate:glyoxylate aminotransferaseglycolate oxidaseglyoxylate reductase/ hydroxypyruvate reductasehyaluronanhemodialysishigh-performance liquid chromatographylactate dehydrogenaseosteopontinperoxisomal biogenesis disorderspolymerase chain reactionperitoneal dialysisprimary hyperoxaluria type 1primary hyperoxaluria type 2rate of appearancerate of disappearanceREgistratie NIerfunctievervanging NEderlandstandard deviationstandard errorradiographZellweger spectrum disorders
AGTAGXT
AGXT -/- mouseCDS
CICRMDAOENZEOP
ESRDGC-MS
GFRGGT
GOGR/HPR
HAHD
HPLCLDHOPN
PBDsPCRPD
PH1PH2
RaRd
RENINESDSE
X-rayZSDs
VAN WOERDEN 5/19/08 8:53 AM Pagina 6

INHOUD
CHAPTER 01 General introduction
CHAPTER 02 Postponing urine acidification for 24 h does not change the oxalate concentration
CHAPTER 03 Primary hyperoxaluria type 1 in The Netherlands: prevalence and outcome
CHAPTER 04 Clinical implications of mutation analysis in primary hyperoxaluria type 1
CHAPTER 05 Primary hyperoxaluria remains undiagnosed inpatients with hyperoxaluria and recurrent urolithiasis
CHAPTER 06 High incidence of hyperoxaluria in generalized peroxisomal disorders
CHAPTER 07 Quantification of endogenous oxalate production inpatients with primary hyperoxaluria type 1: a stableisotope method
CHAPTER 08 Oxalate production in Agxt -/- mice hepatocytes during incubation with potential sources of glyoxylatemetabolism suggests additional routes for glyoxylatedetoxification
CHAPTER 09 General discussion
CHAPTER 10 Summary
CHAPTER 11 Nederlandse samenvatting(Summary in Dutch)
APPENDIX 01Reports of Oxalosis
APPENDIX 02reference values for diagnostic studies
Dankwoord
Stellingen
PAGE
9
49
53
65
80
83
93
103
115
137
141
153
159
170
175
VAN WOERDEN 5/19/08 8:53 AM Pagina 7

Index of CHAPTER 01
HISTORY OF PH1 10GENERAL CONCEPT AND
CLASSIFICATION OF PRIMARY HYPEROXALURIA 11PH1 11PH2 12Unclassified PH 12PRIMARY HYPEROXALURIA: THE ORIGIN OF OXALATE 13Main precursors. 13Glyoxylate: its transamination, oxidation and reduction 13Glycine and Glycolate, precursors of Glyoxylate in peroxisomes 14 Hydroxyproline: a precursor of glyoxylate in mitochondria 15ALANINE: GLYOXYLATE AMINOTRANSFERASE (AGT) 16AGT deficiency in human PH1 16AGT crystal structure 17Species differences in AGT intracellular localization 17THE AGXT GENE 17Cloning and mapping 17Polymorphic variants 18Genetic basis of mitochondrial mistargeting of AGT 18Co-segregation of the minor allele with other AGXT mutations 18PATHOPHYSIOLOGY OF RENAL DISEASE
IN PRIMARY HYPEROXALURIA 19 CLINICAL PRESENTATION AND CLINICAL STUDIES IN
PRIMARY HYPEROXALURIA TYPE 1 20DIAGNOSTIC APPROACH TO PRIMARY HYPEROXALURIA TYPE 1 22Clinical diagnosis 22Metabolic studies 23Urine 23 Plasma 24Peritoneal fluid 26Genetic diagnosis 26Enzymatic diagnosis 27Prenatal diagnosis 27 THERAPEUTIC APPROACH TO PRIMARY HYPEROXALURIA TYPE 1 27Conservative treatment 27Transplantation: Kidney transplantation, Liver transplantation or Combined liver-kidney transplantation 29ZELLWEGER SPECTRUM DISORDERS 30 SECONDARY HYPEROXALURIA 30 AIM OF THE STUDY 31REFERENCES 33
01.0101.02
01.02.01 01.02.02 01.02.0301.0301.03.0101.03.0201.03.0301.03.0401.0401.04.0101.04.0201.04.0301.0501.05.0101.05.0201.05.0301.05.0401.06
01.07
01.0801.08.0101.08.0201.08.02.01
01.08.02.02
01.08.02.03
01.08.0301.08.0401.08.0501.09 01.09.0101.09.02
01.1001.1101.12
VAN WOERDEN 5/19/08 8:53 AM Pagina 8

CHAPTER 01 GENERAL INTRODUCTION
Parts of this chapter have been published in
Nederlands Tijdschrift voor Geneeskunde 2006;150:1669-72
This thesis focuses on a single metabolic disorder of the liver, called primary hyperoxaluria type 1 (PH1; MIM 259900). It is characterisedby an overproduction of oxalate because of a deficiency of the peroxiso-mal enzyme alanine:glyoxylate aminotransferase. The clinical expres-sion and the molecular-biochemical characteristics of PH1 are extreme-ly heterogeneous. Patients may be asymptomatic, suffer from stone dise-ase, or develop end-stage renal disease and systemic oxalosis with multi-organ disease. Presentation occurs at any age. Until recently, severalimportant questions about PH1 were still unanswered:● Which patients are at risk for a severe course of the disease? ● What is the optimal therapeutic strategy in any particular patient? ● What is the exact source of glyoxylate, the direct precursor of oxalate? Aiming to find answers to these questions, we investigated the epidemi-ology of PH1 in The Netherlands. We also looked for associations betweenclinical characteristics and genetic and biochemical features in patients,in order to develop parameters that may facilitate the diagnostic proce-dures and decision-making in the treatment of patients with PH1. Inaddition, we investigated the incidence of hyperoxaluria in the Zellwegerspectrum disorders, which comprise a group of patients with a genera-lized loss of peroxisomal functions. Finally, we aimed to measure therate of appearance of oxalate in plasma in humans, and to unravel theexact sources of glyoxylate in order to find clues for new therapeuticapproaches.
This chapter presents an overview of primary hyperoxaluria type 1:01.01 the history of research in the twentieth century01.02 its classification01.03, 01.04
and 01.05 its metabolic and molecular basis 01.06 the pathophysiology and mechanisms leading to renal
involvement and symptoms01.07 a description of the clinical characteristics and outcome01.08
and 01.09 an overview of diagnosis and treatment01.10 an introduction to the Zellweger spectrum disorders01.11 a short description of secondary hyperoxaluria01.12 an outline of the research questions that we address in
this project.
The colour illustrations of Chapter 01 can be found on the cover.CHAPTER 01
page 9
VAN WOERDEN 5/19/08 8:53 AM Pagina 9

01.01
CHAPTER 01
page 10
HISTORY OF PH1Renal calculi are one of the oldest reported medical problems inhumans, as demonstrated by archaeological studies and descriptionsby Hippocrates, Celsus, Galen and Morgagni (68). Oxalate was recogni-zed as a natural product in the eighteenth century. Already in the early19th century, it had become possible to analyse urine crystals, and cal-cium oxalate was recognised as a frequent element of kidney stones, asreviewed by Hockaday and associates in 1839 (73). A four-and-a-halfyear old boy with “infiltration of renal parenchyma with crystallinedepositions” was described in 1925 by Lepoutre (108), later marked asthe first published case with primary hyperoxaluria. Urinary oxalatecould not be measured at that time, but Lepoutre stated that this wasa human presentation of renal oxalate calcification. He compared hisfindings with the animal studies of Ebstein and Nicolaier in 1897 (53).These investigators were able to induce the formation of calcium oxa-late kidney stones in rabbits and dogs, following the administration ofoxalate and oxamid in drinking water. Until the 2nd half of the 20thcentury, sporadic cases of the same type of kidney crystal depositionwere published. One of the striking clinical stories tells about a boy, 11years of age in 1942, who received a physical examination and a urineexamination at the request of his mother, because of nocturia and poly-dypsia. It revealed extensive calcification of the renal parenchyma ofboth kidneys, called nephrocalcinosis, which appeared to involve themedullary pyramids predominantly, with some ureteral dilatation(212). In the early 1950s, two detailed reports appeared of childrenwho died at 7 and 12 years of age of renal insufficiency with systemicoxalate depositions in multiple tissues and organs. This was the firstclinical and pathological report of the most severe clinical form of pri-mary hyperoxaluria, called oxalosis (26,50). Adult patients with hyper-oxaluria and kidney stones were described as well. By 1960, Antoineand colleagues retrieved 36 cases in whom kidney parenchymal oxala-te depositions had been found (4,30). They reviewed all cases, andfound that presentation could be as early as 3 months of age up to aslate as 57 years of age. An inherited defect was suspected, on the basisof the reports of affected relatives and identical twins (5). The combi-nation of elevated levels of urinary oxalate with this clinical picture ofnephrocalcinosis was identified in 1953 and in 1957 (6). Followingurine analyses of patients, parents and controls using isotope-dilutiontechniques, elevated glycolate levels were demonstrated for the firsttime by Frederick et al. in 1963 (56). A second inherited form of hyper-oxaluria was recognized in 1968, with the coincidence of elevated uri-nary oxalate and L-glycerate instead of glycolate (208). Subsequent stu-dies led to the identification of the enzyme defect in PH2 at the levelof D-glycerate dehydrogenase, which also displays glyoxylate reducta-se activity. Speculations about the metabolism leading to the genera-tion of oxalate were already going on since the early 1950’s. Glyoxylate
VAN WOERDEN 5/19/08 8:53 AM Pagina 10

became recognized as the direct precursor of oxalate and experimentsin the early 1960’s pointed towards a defect in the glyoxylate to glycineinterconversion in primary hyperoxaluria type 1 (56). However, it wouldtake more than 20 years until Danpure and co-workers were the first toidentify a deficient activity of the liver specific enzyme AGT(alanine:glyoxylate aminotransferase) in PH1 patients (47). Since then, anumber of case reports and some comprehensive epidemiologic studieshave been published (27, 72, 112). Insight into the origins of PH1 wasfurther advanced when the gene mutated in PH1 was identified in 1991which made DNA diagnosis possible (161). The biochemical and geneticcauses of PH2 were unravelled later (39, 174) and patients were descri-bed, although at a much lower frequency compared to PH1 (95, 207).
GENERAL CONCEPT AND CLASSIFICATION OF PRIMARY HYPEROXALURIAHyperoxaluria can be the result of a genetic metabolic defect, as in primary hyperoxaluria type 1 or type 2, leading to an excessive endo-genous oxalate production or can be caused by increased intestinaloxalate absorption, or decreased excretion, called secondary hyperoxa-luria (FIGURE 01.1). Urinary oxalate levels are generally higher in pri-mary hyperoxaluria, but the secondary form can lead to severe morbi-dity as well. Because of the clinical impact of hyperoxaluria in patientswith other disorders (e.g. disorders of the gastro-intestinal tract), anoverview of secondary hyperoxaluria is given at the end of this chapter.
Classification of hyperoxaluria. Two genetic metabolic types of primaryhyperoxaluria are known, and three ways of developing secondaryhyperoxaluria are distinguished
PH1Primary hyperoxaluria type 1 (PH1) is an autosomal recessive inheriteddisorder of glyoxylate metabolism due to deficiency of a peroxisomalenzyme, named alanine:glyoxylate aminotransferase, AGT (47). Due to
01.02
FIGURE 01.1
01.02.01
CHAPTER 01
page 11
VAN WOERDEN 5/19/08 8:53 AM Pagina 11

this deficiency, peroxisomal glyoxylate cannot be transaminated intoglycine, but is oxidized into oxalate and reduced into glycolate. A singlemutated gene, called the AGXT gene, mapped at chromosome 2q37.3, con-stitutes the molecular basis of the AGT enzyme deficiency (161).
In humans, oxalate is an end product of glyoxylate metabolism. Anyexcess of oxalate, either produced endogenously or by ingestion oflarge amounts of oxalate, is transported via the blood stream to thekidneys and subsequently excreted into the urine. Due to the very lowsolubility of the calcium salt of oxalate, the concentration process ofthe urine may lead to crystal formation in the urinary tract as well asin the renal parenchyma (FIGURE 01.2 and 01.3). Crystals are demon-strated by light microscopy in a kidney biopsy specimen, and can bemade visible especially using polarized light microscopy (FIGURE 01.4)or after von Kossa staining (FIGURE 01.5). Calcium oxalate cystallizationmay become visible as nephrocalcinosis or renal stones on ultrasoundor abdominal X-ray (FIGURES 01.6 and 01.7). The striking feature ofnephrocalcinosis is a diffusely increased echogenicity of the renalparenchyma at normal to low gain settings (116, 210). This abnormalpattern is evident when comparing the kidneys with adjacent liver tis-sue, which usually contains more internal echoes than the renal paren-chyma. More invasive diagnostic procedures may reveal calcium oxala-te crystals attached to tubular epithelium of nephrons (FIGURE 01.5).Calcifications can result in interstitial nephritis and fibrosis, eventual-ly leading to renal insufficiency and end-stage renal disease (ESRD).When renal insufficiency develops, calcium oxalate depositions notonly accumulate in renal parenchyma but also in other tissues. Theseextrarenal sequelae are called oxalosis or systemic oxalosis (21).
PH2Primary hyperoxaluria type 2 (PH2) is a disorder of glyoxylate but alsoof hydroxypyruvate metabolism (208). Mutations in the glyoxylatereductase/ hydroxypyruvate reductase gene, the GRHPR gene, result ina deficiency of the bifunctional enzyme glyoxylate reductase/ hydro-xypyruvate reductase, GR/HPR, with development of hyperoxaluria andhyper-L-glyceric aciduria (174) (FIGURE 01.8 presents the metabolicscheme). Excess oxalate gives rise to the same phenotype as found inPH1 albeit less severe, and with much less patients recognized so far.A further description of PH2 is beyond the scope of this thesis.
Unclassified PHIn six reports, a total number of 13 patients, some of them being sibpairs, with atypical PH leading to renal involvement (urolithiasis andnephrocalcinosis, declining renal function) have been described (38,98, 132, 134, 140, 193). Common to all patients, AGT and GR/HPR acti-vities were normal, AGT was normally localized in peroxisomes and
01.02.02
01.02.03
CHAPTER 01
page 12
VAN WOERDEN 5/19/08 8:53 AM Pagina 12

DNA analysis of AGXT or GRHPR genes was unremarkable. Urine samp-les showed hyperoxaluria (six patients, of which one sib pair), hyper-glycolic aciduria (three patients of which one sib pair), or a combina-tion of the two (four patients). One report described a decline of uri-nary glycolate levels upon pyridoxine administration (98). It is sug-gested that glycolate oxidase (GO) may be involved in this disorder (seebelow) (134), but the exact nature of this type of primary hyperoxalu-ria has not been found yet.
PRIMARY HYPEROXALURIA: THE ORIGIN OF OXALATE Main precursors Oxalate, excreted in urine, is derived from both dietary sources andfrom endogenous synthesis. The dietary contribution used to be esti-mated at 10% of total urinary oxalate (7), but recent investigations haveshown that oxalate may be derived in approximately equal parts fromthe diet and endogenous liver metabolism. The dietary oxalate contri-bution may vary since oxalate absorption depends on calcium intake(76). Precursors of endogenous oxalate synthesis are sugars and aminoacids (171) of which glycine is the most closely related to oxalate (41).The only studies which investigated the biochemical pathways leadingto oxalate production report a 40% contribution of glycine to oxalatesynthesis (11, 41). Glyoxylate plays a pivotal role in the endogenousoxalate generation (169). Ascorbate is probably the only non-enzymiccontributor to the oxalate production, but its role seems insignificantin PH1 patients (11, 12, 14, 42), as studies that suggested an importantcontribution of ascorbate to urinary oxalate production may have beenbiased by the use of imprecise, analytical procedures for oxalate detec-tion. Moreover, ascorbic acid may be converted to oxalate after voidingof urine, thus overestimating endogenous oxalate synthesis.
Glyoxylate: its transamination, oxidation and reductionGlyoxylate can be transaminated into glycine (FIGURE 01.8). This con-version detoxifies the cell from the reactive aldehyde glyoxylate. It isonly this single conversion, which is catalyzed by the AGT enzyme,which deficiency leads to the appearance of primary hyperoxaluriatype 1. Apart from AGT, however, the more widely dispersed glutama-te:glyoxylate aminotransferase (GGT) has the same function, althoughlocalized in the cytosol. However, for human glyoxylate metabolism,which is mainly localized in liver peroxisomes, AGT is the most impor-tant enzyme (145). As common to many aminotransferases, pyridoxalphosphate is the cofactor of this enzyme (60, 188). Pyridoxal phospha-te is synthesized from pyridoxine, vitamin B6, and depletion of pyri-doxine has been associated with a rise in urinary oxalate excretion inanimal experiments (61). A human patient with hyperoxaluria due topyridoxine deficiency has never been observed, though. Apart fromtransamination, glyoxylate can also be oxidized to oxalate, or reduced
01.0301.03.01
01.03.02
CHAPTER 01
page 13
VAN WOERDEN 5/19/08 8:53 AM Pagina 13

to glycolate. Glycolate oxidase (GO) and lactate dehydrogenase (LDH)both catalyze glyoxylate oxidation (164). Of these enzymes, glycolateoxidase is exclusively expressed in peroxisomes, catalyzing the con-version of glyoxylate into oxalate. However, when abundant glyoxylateis present, LDH may catalyze the same reaction in the cytosol, onceexcess glyoxylate has passed into the cytosol (8). The cytosolic enzy-mes glyoxylate reductase (GR) (180, 208) and lactate dehydrogenase(LDH) reduce glyoxylate to glycolate (FIGURE 01.8) (180). In PH1, thesum of biochemical pathways involving glyoxylate metabolism yieldoxalate and glycolate, that are excreted in urine.
Biochemical pathways in primary hyperoxaluria type 1 and type 2. AGT; alanine:glyoxylate aminotransferase, GO; glycolate oxidase, DAO;D-amino acid oxidase, LDH; lactate dehydrogenase, GR/HPR; glyoxylatereductase/ hydroxypyruvate reductase
Glycine and Glycolate, precursors of Glyoxylate in peroxisomesTwo direct precursors of glyoxylate are glycine and glycolate. In liverperoxisomes, D-amino acid oxidase (DAO) catalyzes the conversion ofglycine to glyoxylate (FIGURE 01.8). Glycolate is oxidized by glycolateoxidase (GO) (219). Both DAO and GO are peroxisomal enzymes. A by-product in the oxidation reaction is H2O2, which is degraded in peroxis-omes by catalase.In contrast to the metabolism of glycine, which is well established, themetabolic origin of glycolate is much more obscure. At least underexperimental conditions, the following substrates have been proposedas precursors of glycolate: glycolaldehyde and ethylene glycol (32),
FIGURE 01.8.
01.03.03
CHAPTER 01
page 14
VAN WOERDEN 5/19/08 8:53 AM Pagina 14

xylitol (58, 92), hydroxypyruvate, ethanolamine (170) and fructose (91,142, 171). Their exact contribution to glycolate and oxalate synthesisin humans is unknown. However, [14C1]hydroxypyruvate and[14C1]ethanolamine were studied and appear not to be effective pre-cursors of [14C]oxalate (59). For hydroxypyruvate, reduction to D-gly-cerate by glyoxylate/ hydroxypyruvate reductase, GR/HPR, is obser-ved, hence preventing glycolate generation in the cytosol (FIGURE 01.8).The importance of this reaction is illustrated by PH2, in which GR/HPRdeficiency results in the conversion of hydroxypyruvate into L-glyce-rate and oxalate (FIGURE 01.8). Clinical studies gave evidence for therole of ethylene glycol, xylitol and fructose as oxalate precursorsbecause patients who were intoxicated with these compounds devel-oped calcium oxalate kidney stones as well as renal insufficiency (66,90, 109, 126, 142, 222). Another pathway was proposed, in which gly-colate dehydrogenase converts glycolate directly to oxalate. This reac-tion was thought to bypass glyoxylate (FIGURE 01.9). However, no fur-ther evidence for such a route was found after analysis of rat liver frac-tions and human urine samples of LDH subunit deficient patients (217).
Xylitol, fructose, glycolate and glyoxylate metabolism, adapted from James et al (172), 3; aldehyde dehydrogenase, 4; glycolateoxidase, 5; glycolate oxidase and lactate dehydrogenase, 6; glycolatedehydrogenase, 7; hydroxypyruvate decarboxylase, 8; alanine:glyoxylateaminotransferase (synonym: serine:pyruvate aminotransferase).Note: Hypothetical conversion, is not widly believed to occur.
Hydroxyproline: a precursor of Glyoxylate in mitochondriaHydroxyproline, a break down product of collagen (153), is anothersource for glyoxylate formation. Its importance has been suggestedrecently (99, 100). Hydroxyproline is metabolized mainly in mitochon-
FIGURE 01.9
01.03.04
CHAPTER 01
page 15
VAN WOERDEN 5/19/08 8:53 AM Pagina 15

dria of hepatocytes and renal proximal tubule cells. Its metabolic con-version results in the formation of equal amounts of pyruvate and gly-oxylate (99). Daily collagen turnover in humans, which is estimated at2-3g/day (153), leads to the generation of 240-420mg of hydroxyproli-ne and of 140-240mg of glyoxylate. Another source of hydroxyprolineis dietary consumption, especially by ingestion of collagen-containingmeat products and gelatine-containing foods. Human experimentsdemonstrating a rise in oxalate and glycolate excretion upon gelatineconsumption, support this notion (100).
ALANINE:GLYOXYLATE AMINOTRANSFERASE (AGT)AGT deficiency in human PH1The enzyme alanine:glyoxylate aminotransferase (AGT) is a liver speci-fic, peroxisomal enzyme which is deficient in PH1 patients, as firstdemonstrated by Danpure and colleagues (47). The immunocytochemi-cal localization was studied by Cooper et al. using protein A-goldimmunocytochemistry (33). AGT consists of 392 amino acid residuesand is encoded by a single gene, the AGXT gene. In PH1 patients AGT isdeficient in its activity, although in many patients a significant residu-al AGT activity, up to more than 50% of normal value, can be detected(33, 47). Different levels of immunoreactivity of the AGT protein werefound as well. No correlation between levels of residual activity on theone hand, and the severity of clinical signs and symptoms on the otherhand, could be detected (43, 48).
After its synthesis on free polyribosomes, AGT normally dimerizes andis imported into liver peroxisomes in humans. Dimerization is not aprerequisite per se for peroxisomal routing, but it prevents mitochon-drial import (137, 221). The peroxisomal import is facilitated by aperoxisomal targeting sequence Lys-Lys-Leu (KKL), localized at the C-terminus of the polypeptide (137). The KKL-sequence differs from theprototypical, well conserved PTS1 sequence Ser-Lys-Leu (SKL) which isusually found in peroxisomal enzymes. A specific region of humanAGT, called PTS1A, probably contains additional peroxisomal targetinginformation (86). Although the exact mechanism leading to a stableperoxisomal targeting signal is unclear, the PTS1A and PTS1 regioninteract closely in the three-dimensional crystal structure of AGT.Normally, human AGT is found exclusively in peroxisomes, but sur-prisingly, based on genetic evidence, 4 % of healthy humans is predic-ted to have a combination of 5% of mitochondrion targeted AGT and95% peroxisome targeted AGT in liver cells (162). This results from thecreation of a mitochondrial targeting signal at the N-terminus thatoverrules the peroxisomal targeting information.
These peculiarities in combination with their genetic background aredescribed below in the paragraph THE AGXT GENE.
01.0401.04.01
CHAPTER 01
page 16
VAN WOERDEN 5/19/08 8:53 AM Pagina 16

AGT crystal structureThe crystal structure of AGT has been unravelled recently, facilitatingpredictions regarding genotype and enzymatic phenotype (221). AGT isa homodimer, built from two identical subunits. Each monomer con-sists of a large N-terminal domain and a smaller C-terminal domain.The core of the dimerization interface is formed by two helices and fiveconnecting loops. This results in a surface, which is in close contactwith the same area of the other monomer. The pyridoxal phosphate co-factor binds in a pocket at the dimer interface, and facilitates the cata-lytic and enzymatic function of AGT.
Species differences in AGT intracellular localization In most humans, the localization of AGT is restricted to the peroxis-omes. Yet, in other vertebrates, like cats and dogs, AGT is predomi-nantly localized in mitochondria and only in a small proportion inperoxisomes. In other mammals, AGT is evenly distributed betweenboth peroxisomes and mitochondria, like in rats or marmosets. The subcellular localization of AGT is thought to have changed during evolu-tion, depending on the dietary contribution of oxalate in different spe-cies (45). For example, a vegetable diet, containing relatively highamounts of glycolate or oxalate, requires adequate break down of oxa-late precursors to obtain a minimal endogenous production of oxalate.For this reason it is thought that the AGT enzyme is localized inperoxisomes in herbivores such as sheep (45, 75). On the other hand,carnivores have a high intake of collagen, which is also a precursor ofoxalate via conversion into hydroxypyruvate and glyoxylate.Therefore, they require an adequate breakdown of collagen compo-nents. Since hydroxyproline metabolism has been localized in mito-chondria (99), the AGT localized in mitochondria is likely to detoxifyglyoxylate in this compartment. For humans, the expression of so cal-led polymorphic mitochondrion targeted AGT (paragraph THE AGXT
GENE) occurs more frequently in areas where meat is an important die-tary component in contrast to areas where vegetables are the mostcommon dietary component .
THE AGXT GENECloning and mappingThe AGXT gene encoding the AGT enzyme (161), consists of 11 exons,ranging from 64 to 407 base pairs, and spans about 10 kb at the telom-eric end of the long arm of chromosome 2, 2q37.3. It is composed of 11exons. The open reading frame encodes a polypeptide of 392 aminoacids. Soon after its cloning and mapping, a number of mutations andpolymorphisms related to PH1 have been sequenced. As of the beginningof the 21st century, the number of sequence variants reported in theHuman Gene Mutation Database (www.hgmd.cf.ac.uk) reaches over 50(34, 35, 57, 218).
01.04.02
01.04.03
01.0501.05.01
CHAPTER 01
page 17
VAN WOERDEN 5/19/08 8:53 AM Pagina 17

Polymorphic variantsTwo different haplotypes or polymorphic variants are recognized witha high frequency in European and North American populations: the‘major’ allele (frequency ~80%) and the ‘minor’ allele (frequency ~20%)(162). The frequency of the minor allele is ~3% in South Africans and~2% in the Japanese population (37, 46). The minor allele is characteri-zed by a 32C>T point mutation resulting in a substitution of the aminoacids proline11➔leucine (Pro11Leu). This minor allele is frequentlyassociated with a 74bp-duplication in the first intron, a 1020A>G pointmutation leading to an isoleucine340➔methionine (Ile340Met) substi-tution (159), and an Epstein-Barr-virus-like VNTR in the fourth intron(46). In the (South) African population, another polymorphic variantwith a c.976G>A point mutation, yielding a Val326Ile polymorphism isfound in ~12% (37).
Genetic basis of mitochondrial mistargeting of AGTThe minor allele alone does not cause PH1, but some interesting bio-chemical consequences have been observed in homozygous individu-als. The most intriguing is the so called mistargeting of a small pro-portion (5%) of the AGT enzyme to mitochondria instead of peroxisom-es (162). In other words, a proportion of AGT, which is normally locali-zed in the peroxisomal matrix, is imported into mitochondria. Themechanism behind this biochemical phenotype is considered to be achange in AGT protein folding. Normal AGT dimerizes after its synthe-sis. In this state, it can be imported in peroxisomes, but not in mito-chondria (106). In vitro studies have shown that the Pro11Leu poly-morphism creates a weak mitochondrial targeting sequence at the N-terminus of AGT (115, 158), which could create an alfa-helix at this siteof AGT. This in its turn prevents normal dimerization and 5% of AGT isimported in mitochondria in vivo (106, 137). Affinity for mitochondri-al import is increased by the additional occurrence of the c.508G>Amutation yielding a Gly170Arg substitution, which is the most commonmutation in PH1 found so far (106, 114, 115, 137, 158, 162).Mistargeting of AGT to liver mitochondria is then enhanced, resultingin about 90% of AGT routed to the mitochondria and only 10% toperoxisomes (162). The Pro11Leu polymorphism induces two otherchanges in the AGT enzyme: it decreases the catalytic activity by 70%and, at elevated temperatures, it decreases the efficiency of dimeriza-tion of AGT translated in vitro (114). Furthermore, it sensitizes AGT tothe deleterious effects of other mutations that probably would havebeen innocuous if they had occurred alone (137).
Co-segregation of the minor allele with other AGXT mutationsApart from the specific enzymic mistargeting phenotype, the minorallele also predisposes AGXT to the pathogenic effects of the three othercommonest sequence changes Ile244Thr, Phe152Ile, and Gly41Arg
01.05.02
01.05.03
01.05.04
CHAPTER 01
page 18
VAN WOERDEN 5/19/08 8:53 AM Pagina 18

(114), resulting in aggregation of the AGT protein, as reviewed in theAPPENDIX 02. For example, the Ile244Thr mutation, which is the secondmost common mutation in patient groups studied so far, also segrega-tes with Pro11Leu. Its frequency is 9% in European and North Americanpopulations (201). AGT activity is low, and the phenomenon of mito-chondrial mistargeting is not seen in this genotype. Santana and asso-ciates demonstrated that Ile244Thr AGT forms aggregates in vitro (178).Proteolytic disposal in vivo could explain low AGT levels found in liverbiopsies of these patients. The Gly82Glu occurs on the background ofthe major allele and results in loss of AGT catalytic activity, possiblydue to failure of binding the co-factor (114, 160). For the Gly41Argmutation, segregation with the Pro11Leu polymorphism leads to aggre-gation into core-like structures in the peroxisomal matrix (49). WithoutPro11Leu (155), the specific AGT activity is only reduced in patients(114). Ser205Pro is only observed in Japanese PH1 patients on the majorallele. It renders AGT highly unstable and AGT is degraded subsequent-ly (144). A small insertion at codon 11 was found by an Italian group,c.33_34insC (155). A heterogenic picture was seen in these patients butno expression studies were carried out (3, 154). Apart from these speci-fic AGXT gene mutations, a large number of other AGXT mutations havebeen reported (2, 16, 34, 36, 37, 46, 49, 57, 113, 131, 135, 143, 160,165, 199, 200, 201, 218). An overview can be found at the website of theHuman Gene Mutation Database (http://www.hgmd.cf.ac.uk/ac).
In summary, after the characterization of the AGXT gene and the firstPH1-related mutations in 1990 by Purdue et al. (161) a few cross-secti-onal studies had been reported on the prevalence of AGXT gene muta-tions (46, 77, 113, 199, 200, 201). Some genetic AGXT mutations hadbeen linked to specific defects of the AGT enzyme, such as intrape-roxisomal aggregation, loss of the pyridoxal phosphate binding siteand, most fascinatingly, a conformational change of the enzyme lea-ding to a predominantly mitochondrial instead of a solely peroxisomallocalized AGT enzyme (44, 105, 106, 158, 160, 162). However, theseinvestigations could not reveal the relationship between genetic cha-racteristics on the one hand and clinical characteristics and outcomeon the other hand.
PATHOPHYSIOLOGY OF RENAL DISEASE IN PRIMARY HYPEROXALURIAThe concentration process of urine in the kidneys results in increasingconcentrations of both oxalate and calcium. Since the solubility coeffi-cient of calcium and oxalate is low, they easily precipitate as calciumoxalate crystals. Urine is easily supersaturated with stone forming ions(166) but under normal conditions crystallization is prevented by thepresence of crystallization inhibitors such as citrate and magnesium.However, the high output of urinary oxalate in PH1 increases the pre-
01.06
CHAPTER 01
page 19
VAN WOERDEN 5/19/08 8:53 AM Pagina 19

cipitation risk. This has already been investigated in animal models in1926 by Dunn and colleagues and in 1960 by Largiader, as reviewed byHockaday et al. (1964) (73). In the patient, these calcium oxalate cry-stals are considered to be the basis for stone formation. Although cry-stallization of oxalate with calcium was generally presumed to occur inthe renal parenchyma or medullary interstitium, the exact nature andextent of crystal deposition and its consequences for renal damage arenot known. Massive crystalluria in patients with a severe form ofhyperoxaluria could lead to early development of urolithiasis, nephro-calcinosis, and renal insufficiency due to insoluble and obstructiveproperties of calcium oxalate. Contrary to previous hypotheses, oxala-te itself is only toxic at extremely high concentrations (181) and is pre-dicted not to lead to changes in tubular epithelial functioning or dama-ge in vivo. However, the presence of crystalluria has been demonstra-ted in recurrent renal-stone formers, and appeared to be increasedafter oral sodium oxalate loading (167). In recent years, another mecha-nism has become the focus of stone research, namely binding of cry-stals to the tubular epithelium, which may be mediated by the expres-sion of the receptor CD44 and its ligands hyaluronan (HA) and osteop-ontin (OPN) (9, 101, 195-197). Asselman et al. have shown that theexpression of HA precedes crystal retention in experimental modelsand, together with OPN, it is also associated with nephrocalcinosis inkidneys of preterm infants and renal transplants (9, 195). Observationsin monolayer cell cultures show that HA expression can be inducedafter creation of an artificial wound in the monolayer. In these circum-stances, CD44, which is normally present basolaterally, is expressed atthe apical cell surface, as well as HA. They are visible until wound hea-ling is completed. In human renal epithelial cells, the expression ofCD44, HA and OPN could well follow damage due to passage of calciumoxalate crystals. Consequently, crystals may attach to these expressedmolecules, causing nephrocalcinosis. Hyaluronan has been shown tobind crystals in cell culture experiments of Verkoelen et al., in which itmay serve as a stone binding glue (197). The presence of these mole-cules for PH1 and their implications for clinical management are cur-rently unknown and warrant further investigation.
CLINICAL PRESENTATION AND CLINICAL STUDIES INPRIMARY HYPEROXALURIA TYPE 1After the description of some case reports in the second half of the pre-vious century, the first large patient cohort was described in Sweden,comprising 17 patients of Scandinavian origin (72). At that time, theenzyme deficiency had not yet been discovered and a complete dia-gnostic work up was therefore not possible for all patients. Upon thediscovery of AGT deficiency as the cause of PH1, many patients withsuspected PH1 were analyzed and published. In 2000, at the start of theproject leading to this thesis, a French cohort had been published
01.07
CHAPTER 01
page 20
VAN WOERDEN 5/19/08 8:53 AM Pagina 20

(Cochat et al., 1995) (27), a Swiss cohort focused on the infantile pre-sentation (Leumann et al., 1987) (112) and an overview of 330 cases(Latta et al., 1990) (103). One phenomenon was recognized in all ofthese studies: PH1 is a very heterogeneous disease with respect to ageat presentation, outcome of renal function, and biochemical characte-ristics. The first symptoms in patients with primary hyperoxaluriawere usually related to renal stone disease, such as colic pain, hema-turia and/or recurrent urinary tract infection (103). However, nephro-calcinosis may also develop without any of these signs and symptoms.Some patients only become clinically symptomatic at the time end-stage renal disease has already developed. Systemic deposition of cal-cium oxalate may occur throughout the body when plasma oxalate con-centration rises above 20 µM and glomerular filtration rate falls below60ml/min/1.73m2 (136). The chemical composition of these systemicdepositions was also calcium oxalate (26, 70). The risk for systemicoxalosis increases sharply when the GFR comes down to 20ml/min/1.73m2 (136). When dialysis is started (GFR<10ml/min/1.73m2),further development of oxalosis cannot be prevented. Despite intensi-ve dialysis schedules, patients develop the most severe complicationsof primary hyperoxaluria due to systemic oxalate depositions, whichcan occur in many organs and tissues, like bones, muscle fibres andconnective tissues (18, 21, 194), and the nervous system, particularlythe interstitium of peripheral nerves (69). Other tissues are involved,such as the vascular system, the heart (21, 26, 194), myocardiac musclefibers (21, 194), tracheal cartilage (21), lungs (69), prostate (21), brains,meninges and in walls of congested meningeal vessels (70), choroidplexus, pineal gland, ovaries, fallopian tubes, uterus, thymus, salivaryglands, pancreas, bladder (52) and in joints (125). Consequences ofoxalosis range from frequent bone fractures and loss of visual acuity,to advanced neural damage, cardiac conductivity blocks, and arterialvessel obstruction with necrosis and gangrene, eventually leading toearly mortality (65, 69, 70, 119). Although the liver is the primary sitefor oxalate production, liver oxalate depositions have only been obser-ved infrequently (1, 69). The most striking features of systemic oxalo-sis are presented in APPENDIX 01.
The clinical pattern emerging from the initially published patientcohorts showed that infantile patients often presented with end-stagerenal disease, failure to thrive, metabolic acidosis, vomiting, anorexiaor anemia, generally preceding rapid progression of renal insufficien-cy. Although most patients presented within the first decade of lifewith renal involvement, presentation in adulthood was also frequentlyobserved. These observations resulted in a clinical classification of primary hyperoxaluria type 1 into three groups (29):1. a severe, neonatal or infantile form, with urolithiasis, nephrocal-
cinosis, or end-stage renal disease before the first birthday.CHAPTER 01
page 21
VAN WOERDEN 5/19/08 8:53 AM Pagina 21

Outcome, regarding preservation of kidney function or patientsurvival, was assumed to be poor in this group;
2. a mild form, with onset of symptoms in late adulthood, and afavourable prognosis of kidney function;
3. an intermediate group, comprising patients presenting in child-hood, with a slow decline of renal function over years and deve-lopment of ESRD in more that half of them.
Not all these observations were based on comprehensive epidemiolo-gical studies. Several case reports of patients with adult onset of symp-toms, who presented in end-stage renal disease (102) and reports ofpatients with neonatal PH1 with a relatively mild course argumentedagainst this classification (129, 203).
DIAGNOSTIC APPROACH TO PRIMARY HYPEROXALURIA TYPE 1Diagnosis of primary hyperoxaluria type 1 is based on clinical, meta-bolic, genetic and enzymatic studies. The gold standard of diagnosis isthe demonstration of absence, or decrease in peroxisomal AGT enzymeactivity. As human AGT is almost exclusively expressed in liver, thisrequires an invasive liver biopsy. Therefore, other less invasivemethods are currently regarded as the first choice in the diagnosticwork up. In this overview, the approach to diagnosis of primary hyper-oxaluria type 1 will be discussed. The appendix provides a table withreference values for relevant diagnostic tests.
Clinical diagnosisThe clinical presentation of PH1 is extremely heterogeneous. Patientsmay present with symptoms between 0 and at least 60 years of age.Symptoms vary from single urinary stones, recurrent urinary tractinfection and hematuria to all stigmata of end-stage renal disease. Inchildren, non-specific symptoms as failure to thrive, feeding problemsand vomiting may be the first findings. Weight gain and edema, loss ofappetite and fatigue may indicate renal insufficiency at any age. Sincecalcium oxalate is also deposited at other sites in the body apart fromthe kidneys, the longer the period of renal insufficiency exists, the morecalcium oxalate depositions can be found elsewhere in the body. Typicalbone lesions on X-ray and brown retinal maculae on fundoscopia (FIGURE
01.10) characterize systemic oxalosis in patients with severe renal fai-lure. Renal stones, nephrocalcinosis, and in the case of severe renal fai-lure a highly echo dense appearance of the kidney with loss of cortico-medullary differentiation are the most common abnormalities found byultrasound (FIGURE 01.7). Renal biopsy may reveal typical fan-shapedoxalate crystals (FIGURE 01.4) and signs of interstitial nephritis (27, 79,80, 103, 112, 130). In summary, symptoms of renal calcification, butalso signs of renal failure and of bone disease and visual impairmentmay be the first clues to initiate a diagnostic work up for PH1. In gene-
01.08
01.08.01
CHAPTER 01
page 22
VAN WOERDEN 5/19/08 8:53 AM Pagina 22

ral, oxalate crystals can originate either from endogenous oxalate pro-duction in patients with primary hyperoxaluria, or excessive oxalateintake due to high dietary oxalate loads, or enhanced oxalate absorptionin patients with malabsorption syndromes or inflammatory bowel dis-orders, or decreased oxalate excretion in patients with end-stage renaldisease on dialysis. However, none of the clinical signs and symptomsis pathognomonic for a diagnosis of PH1. Therefore, any patient pre-senting with these clinical signs and symptoms should be furtherinvestigated for PH1
Metabolic studiesAssessment of patients for a diagnosis of primary hyperoxaluria canstart with metabolic analysis for elevated levels of oxalate in urine, plas-ma or peritoneal fluid.
UrineThe use of urinary metabolites in the diagnosis of PH1 is restricted topatients with a preserved renal function, since false negative resultsmay be obtained when renal function declines. In case of renal insuffi-ciency, one should proceed to analysis of plasma metabolites. Twomechanisms interfere with reliable determination of oxalate: crystalli-zation and ascorbate interference. For these confounders, urine is col-lected in acidified containers. If urine is kept at a pH<2, oxalateremains solved and does not crystallize with calcium ions. Meanwhile,the enzymatic conversion of ascorbate to oxalate in vitro is reduced,though it will take place during storage with time, even at low storagetemperatures (211). This may result in false positive values.
Assessment of urinary levels of oxalate and glycolate has always beenthe first line in the diagnostic assessment of PH1. Due to potential cir-cadian variation in urinary oxalate excretion (148), which parallels vari-ations in creatinine excretion, it is generally advised to study 24-hoursamples (128, 152). However, by calculation of the ratio of urinary oxa-late to creatinine [mmol/mol] and glycolate to creatinine in spontane-ously voided urine samples potential misinterpretation because ofsampling errors is avoided. Therefore, analysis of spot-urines producescomparable results to 24-hour urinary collections (88) making urinaly-sis in young children easier. For children, creatinine and oxalate excre-tion is higher at younger age. Therefore, age-related reference valueshave been obtained in a number of studies (15, 62, 111, 163, 198).Results of urinary oxalate excretion between adults and children mayalso be compared if expressed as mmol per 1.73m2 body surface areaper day (62, 128). For PH1, levels usually exceed 1 mmol per 1.73m2
body surface area. An elegant technique assessing urinary oxalate andglycolate from dried urine filter spots in a pediatric population wasdeveloped by Blau et al. (20).
01.08.02
01.08.02.01
CHAPTER 01
page 23
VAN WOERDEN 5/19/08 8:53 AM Pagina 23

Values of urinary glycolate concentration in control subjects have beenreported in 13 studies, and range from 1 to 99.6 mg/24 hr, which isequal to 1 to 135 mmol/mol creatinine/24 hr (206). Urinary glycolateas assessed by gas chromatography produces valid and accurateresults (111). Using tetrahydrofuran, the extraction procedure for ana-lysis with gas chromatography was improved by Dietzen et al. (51). Therange of normal glycolate values reflects a considerable daily variabili-ty of urinary glycolate levels (206). Most reliable results are obtainedby expressing the results as the glycolate/creatinine ratio. Whether gly-colate levels in PH1 patients also vary to a great extent has not beeninvestigated. If so, it may contribute to the observation of normal uri-nary glycolate levels in 25% of PH1 patients, which is a major pitfall inthe diagnosis of PH1 based on urinalysis.
PlasmaIn patients with PH1, plasma levels of oxalate and glycolate not onlyrise in renal insufficiency, but may also be elevated in patients with apreserved renal function. Therefore, assessment of these metabolitesin plasma is of value for diagnosis in all patients with suspected PH1.However, in patients with preserved renal function, normal levels donot exclude PH1.
Elevated plasma oxalate concentration is a common observation inpatients with renal insufficiency not due to PH1. However, oxalatelevels in non-PH patients with renal insufficiency rarely exceed 50-60µmol/l (10 times upper range of reference values), in contrast to PH1patients in whom levels may rise to 200-300 µmol/l. Nevertheless, theisolated determination of plasma oxalate cannot always discriminatebetween primary hyperoxaluria or high levels of plasma oxalate due torenal insufficiency. Wolthers et al suggested that a plasma oxalate:cre-atinine ratio exceeding 0.1 and a calculated total quantity of oxalateremoved by dialysis exceeding 2 mmol to be supportive of a diagnosisof hyperoxaluria (214). Other causes of secondary hyperoxaluria, resul-ting in elevated plasma oxalate levels, may include intake of highamounts of vitamin C, and hyperoxaluria caused by inflammatorybowel disease or short bowel syndrome (31, 136, 150). The issue ofsecondary hyperoxaluria due to high amounts of vitamin C intakeremains controversial. Some clinical reports found a significant rise ofurinary oxalate excretion upon oral ascorbate loading (17, 71, 191).Two case reports found the occurrence of acute renal failure in other-wise healthy persons due to vitamin C supplementation of 2.5 g – 4 gper day (121, 139). The effect of ascorbic acid supplementation wasstudied in some controlled studies, using healthy volunteers and stoneformers (up to 10 grams per day) (25, 123, 182). Although the conver-sion rate of ascorbic acid into oxalate was 1-2%, it may become a clini-cally significant increase in patients with primary hyperoxaluria since
01.08.02.02
CHAPTER 01
page 24
VAN WOERDEN 5/19/08 8:53 AM Pagina 24

the solubility of calcium oxalate in urine is very limited. However,others could not demonstrate this relationship (23, 192, 205, 211). Astudy assessing the fate of oral suppletion of isotopic ascorbic acid fee-dings found that ascorbic acid is only a minor contributor to oxalateexcretion in primary hyperoxaluria (10). No other studies assessed thein vivo ascorbate conversion in patients with biochemically or geneti-cally determined PH1.
Determination of glycolate concentration in plasma in addition to plas-ma oxalate has been suggested to allow discrimination of PH1 patientsfrom patients with other causes of renal insufficiency (87, 117, 118).However, since little studies in patients with PH1 having end-stage renaldisease have been performed, the sensitivity of plasma glycolate testingis not known. On the other hand, the specificity seems to be high sincestudies in patients who have received a curative liver transplantationshow a decline of glycolate up to normal values within days (87).
Collection procedure and preparationAs vitamine C in plasma and other potential sources of glyoxylate maycause in vitro oxalate synthesis after collection of a blood sample,resulting in false positively elevated levels of plasma oxalate, plasmashould be deproteinized quickly after it has been drawn in pre-cooledheparine vacutainers and stored at - 20 ºC and storage time should beas short as possible (149, 151, 213). Interference of ascorbate with themeasurement of plasma oxalate is prevented by acidification, prior toanalysis, since alkaline pH could lead to generation of oxalate fromascorbate (141, 151).
Analytical methodsPlasma oxalate analysis by means of in vivo dilution, a radiochemicaltechnique using labeled [14C]oxalate, has by far provided the mostaccurate measurement of plasma oxalate concentration. The referencevalue has been determined by this method as 1.39 (range 1.04 to 1.78)(31, 74, 157). As this assay is impracticable as it uses a radioactivelabel, other assays have been developed. Enzymatic measurementsusing oxalate oxidase reactions are most prone to false results byascorbate interconversion (40, 96, 107). For ion chromatography(HPLC), the main problem is in-column conversion of endogenousascorbate to oxalate, which can be avoided either by ascorbate oxida-tion with iron(III)ions (97) or by means of boric acid dilution (216). Gaschromatography-mass spectrometry (GC-MS) is probably the mostaccurate technique though more laborious than ion chromatography.Its reliability is very high because of the use of stable isotope labeledinternal standards (87). Plasma oxalate levels in healthy persons have been measured withthese different techniques. Levels range from 0.4-6.0 µM, depending on
CHAPTER 01
page 25
VAN WOERDEN 5/19/08 8:53 AM Pagina 25

the method of analysis (152). For PH1 patients with preserved renalfunction, plasma oxalate levels may be within the normal range. Levelsgradually exceed 10 µM when renal function declines from 80 to 40ml/min/1.73m2, however, plasma oxalate levels rise progressivelyabove 30 µM when the glomerular filtration rate falls below 40ml/min/1.73m2 (136).
Plasma glycolate measurements by HPLC and GC-MS methods haverevealed glycolate levels of 7.5 ± 2.4 µM in healthy persons (87).Another sensitive HPLC procedure was developed by Hagen et al. (67).Plasma glycolate levels of PH1 patients with preserved renal functioncan exceed 20 times the upper limit of the normal reference range andare therefore highly discriminative in the diagnosis of PH1 (118). InPH1 patients on hemodialysis or peritoneal dialysis, plasma glycolatelevels may even rise up to 150 times the normal range (117), whereasglycolate remains normal in primary hyperoxaluria-unrelated end-stage renal disease.
Peritoneal fluidOxalateThe use of dialysate in the diagnosis of PH1 in patients on peritonealdialysis (PD) has been investigated in one case-control study: four PH1patients on PD and four controls. This study revealed an oxalate/ cre-atinine ratio of 512 (range 265-638) mg/g in four PH1 patients on PD ascompared to 130 (range 64-191) mg/g in PD patients with other under-lying diseases (124).
GycolateOne study has been published on glycolate levels in the dialysate of aPH1 patient in comparison with five non-PH PD patients, which showedsignificantly elevated levels of glycolate in the PH patient: 48.3µmol/day in the PH1 patient versus 19.6 (range 15.1-27.5) µmol/day inthe non-PH PD patients (215). The analysis was performed by means ofstandard organic acid analysis using gas chromatography without anisotopic internal standard as control.
Though analysis of oxalate and glycolate in dialysate fluid is not wide-ly practiced, it seems of additional diagnostic value.
Genetic diagnosisAfter characterization of the AGXT gene as described above, expressionstudies showed the pathogenicity of the most common mutations,including the amino acid substitutions Gly170Arg, Gly82Glu andGly41Arg (114).
01.08.02.03
01.08.03
CHAPTER 01
page 26
VAN WOERDEN 5/19/08 8:53 AM Pagina 26

Enzymatic diagnosisFor patients in whom the diagnosis remains uncertain after urinary andgenetic analyses, assessment of the AGT enzyme activity in a liver bio-psy specimen may be the ultimate diagnostic procedure. The analysis ofthe AGT enzyme was first performed in 1972 (138, 172). The analysis waslater performed using a Cobas Fara centrifugal analyzer (83, 84), or ana-logous procedures and can be performed in a semi-automated way (175). The AGT enzyme has a considerable range in residual in vitro activity fordifferent genotypes in PH1. Three main forms of AGT deficiency arerecognized (48):
1. absence of both immunoreactive and catalytically active AGT(CRM-/ENZ-); the AGT activity may be below the detection level;
2. presence of immunoreactive AGT but absence of catalytically acti-ve AGT (CRM+/ENZ-);
3. presence of both immunoreactive and catalytically active AGT(CRM+ /ENZ+): the residual in vitro activity ranges from 15% up to50% of normal activity. The inconsistency of the apparent in vitroactivity and lack of in vivo activity of the enzyme in the latter situ-ation is due to mitochondrial mistargeting of AGT. In all these 3situations, the diagnosis of PH1 is confirmed, though heterozygo-te carriers may also be detected with 50% residual enzyme activi-ty. However, no reports have demonstrated hyperoxaluria in car-riers. Therefore, it is probably without clinical significance. Incase of doubt when high residual activity of AGT is found, AGTmistargeting to mitochondria can be assessed by immunocyto-chemical localization studies of the enzyme (33), though the mito-chondrial mistargeting phenotype should have been traced bygenetic sequencing at this stage, revealing the Gly170Arg – or pos-sibly Phe152Ile – genotype (158).
Prenatal diagnosisMolecular genetics is the method of choice for prenatal diagnosis, usingmutation analysis (173). It can be used in the first trimester of pregnancy.
THERAPEUTIC APPROACH TO PRIMARY HYPEROXALURIA TYPE 1Treatment of patients with PH1 is mainly centered on influencing themetabolism of oxalate and glyoxylate, prevention of renal sequelae,treatment of urolithiasis and, in case of end-stage renal disease, insti-tution of renal replacement therapy.
Conservative treatmentAs with renal stone disease in general, conservative management con-sists of increasing fluid intake to dilute urine if renal function permits,dietary modifications, and the administration of pharmacologic agentsthat minimize the risk of supersaturation by increasing the urinary
01.08.04
01.08.05
01.09
01.09.01
CHAPTER 01
page 27
VAN WOERDEN 5/19/08 8:53 AM Pagina 27

concentration of inhibitory substances (81). Maintaining a good hydrationis especially important in patients at risk for dehydration, for example incase of diarrhoea. In children, who are at risk for rapid dehydration, earlyinstitution of naso-gastric tube hydration or intravenous fluid admi-nistration is mandatory. Continuous naso-gastric tube hydration duringnighttime should be considered in small children or patients with alreadysevere nephrocalcinosis and renal damage. For dietary measures, a suffi-cient calcium intake is advised in order to bind any dietary oxalate in thedigestive tract before it can be absorbed and excreted by the kidneys.Although excessive ingestion of dietary oxalate should be avoided, abso-lute elimination of oxalate containing food is probably less importantsince the ingested amount of oxalate is relatively small compared to endo-genously produced oxalate. Citrate, 0.15 g/kg, is considered to be apotent chelator of calcium in urine but under normal conditions it is notsufficient to chelate more than a fraction of the calcium present (85).However, its use in humans strongly inhibits calcium oxalate nucleationand aggregation (89, 110, 179, 186). Potassium citrate is preferred to sodi-um citrate since it prevents high sodium intake and secondary hypercal-ciuria due to high sodium intake. In addition, citrate acts as an alkalini-zing agent, further reducing the risk of crystallization (168, 220).
Magnesium salts are sometimes used as modifiers of nucleating agentsbut magnesium may only be added to potassium citrate therapy to fur-ther inhibit calcium oxalate crystallization (122, 220). An adverseaffect of magnesium administration is the potential occurrence ofdiarrhoea which may lead to dehydration, greatly enhancing the riskfor crystallization of calcium oxalate in the kidney.
The best evidence for successful pharmacological intervention inpatients with PH1 comes from studies assessing the use of pyridoxineand orthophosphate. Animal studies had already studied the effects ofpyridoxine on oxalate metabolism (60). Pyridoxine was first describedfor treatment of patients with PH1 in 1967 (185) but the effects wereconflicting (63). Orthophosphate alone was known for its inhibitoryeffect on crystal formation, though the exact mechanism of this phe-nomenon was not clear (85). A long-term follow-up study in PH1patients evaluated the use of pyridoxine and orthophosphate andfound a decreased urinary calcium oxalate crystallization and preser-vation of renal function (129). An intake of more than 1000mg per daymay lead to reversible, peripheral neuropathy (190). For pyridoxine, aninitial dose of 5 mg/kg is usually prescribed. The potential decline ofurinary oxalate should be awaited for 2-3 months after which the dosa-ge is optimized under control of urinary oxalate excretion. Usually,either citrate or orthophosphate is added to the treatment regimen. Fororthophosphate no further studies are available as to assess its effec-tiveness.
CHAPTER 01
page 28
VAN WOERDEN 5/19/08 8:53 AM Pagina 28

Transplantation:
Kidney transplantation, Liver transplantation or Combined liver-kidney transplantation
Currently, a definitive cure of the metabolic enzyme deficiency in PH1is only feasible through liver transplantation. This was initially perfor-med at the time end-stage renal disease had ensued under carefullyoptimized conditions (104), but later on, pre-emptive liver transplan-tations were introduced to prevent development of end-stage renaldisease. Combined liver-kidney transplantations were also performedto correct both the enzymatic defect and the renal insufficiency.
For patients with PH1, four transplantation procedures are known: (1) sole kidney transplantation; (2) pre-emptive liver transplantation,(3) combined liver-kidney transplantation, or (4) sequential liver-kid-ney transplantation, in which the kidney transplantation is plannedafter reduction of plasma oxalate levels, in order to reduce oxalate bur-den for the kidney transplant. For each of these options, systematic cli-nical evidence is collected in different cohorts, and adverse effects areconsiderable: option (1) was thought to be prone for early graft failuredue to recurrence of oxalate depositions; option (2) would be reservedto patients who do not respond to conservative treatment, but nopatient characteristics could determine this; option (3) needed carefulorgan selection and operative care; and for option (4), immunizationproblems were expected since organs from different donors were goingto be transplanted. A European cohort study that collected data byquestionnaires, found that the outcome of kidney function was inver-sely related to the time between onset of dialysis treatment and trans-plantation. They found excellent results with combined liver-kidneytransplantations (28, 93, 94) which was confirmed by a single centerexperience (133). However, incompleteness of data might have resultedin bias towards positive outcome. In a United States follow-up survey,renal allograft survival was equal in patients who had undergone a soli-tary kidney, as compared to those who had received a combined liver-kidney transplantation; at the same time, the patient survival was betterfor kidney transplanted recipients (176). A high morbidity and mortali-ty rate was observed in infants and young children undergoing comb-ined liver-kidney transplantation which suggested a pre-emptive livertransplantation or a combined liver-kidney transplantation before rea-ching end-stage renal disease (54). Few reports have reported the suc-cessful use of pre-emptive liver transplantation in order to prevent dia-lysis-induced oxalosis (146). A better prediction of outcome of patientswas needed for appropriate choice of transplantation.
01.09.02
CHAPTER 01
page 29
VAN WOERDEN 5/19/08 8:53 AM Pagina 29

ZELLWEGER SPECTRUM DISORDERSThe Zellweger spectrum disorders (ZSDs) belong to the group of peroxi-some biogenesis disorders (PBDs), that are characterized by a defect inperoxisomal assembly (202). The failure to assemble peroxisomes inthe cells of these patients, results in a failure to import peroxisomalenzymes into the peroxisomal matrix. Subsequently, most of theseenzymes, after their synthesis in the cytosol, are rapidly degraded, andmultiple peroxisomal functions are lost. However, the AGT enzyme wasreported to be stable in the cytosol just like a few other peroxisomalenzymes including catalase (204). We studied the clinical picture ofpatients with ZSDs, to observe potential effects of cytosolic localizedAGT on glyoxylate metabolism. The prototype of PBDs are Zellwegersyndrome patients, with an early lethal course, but other patients havemilder phenotypes. Still, many have a severe physical and mental retar-dation, although to different extents, and mild cases survive into adult-hood, and are socially and intellectually educable (156). Clinical featu-res include neurodevelopmental impairment, retinopathy, perceptivedeafness, and hepatic dysfunction (202). Renal involvement with uroli-thiasis, nephrocalcinosis and hyperoxaluria was observed in threepatients, despite normal AGT activity. The incidence of hyperoxaluriain ZSD patients and its clinical implications was, however, unknown.
SECONDARY HYPEROXALURIAAs previously stated, dietary absorption of oxalate is estimated toaccount for approximately 10-50% of the total daily oxalate excretion(76, 209). Secondary hyperoxaluria has four pathophysiological ori-gins: 1. an increased ingestion of oxalate from dietary sources such asrhubarb, spinach, cocoa, tea, parsley, pepper, peanuts, beets; 2. anincreased absorption due to bowel disorders (187) such as cystic fibro-sis (64, 78, 82, 183), inflammatory bowel disease, ileal resection; 3. adecreased clearance of oxalate due to renal insufficiency (214); or 4. asa consequence of long term parenteral nutrition in preterm infants(22). Even without specific disorders of the gastrointestinal tract, theremay be a higher oxalate uptake from the diet by recurrent renal-stoneformers (167). All these mechanisms can lead to elevated levels of uri-nary oxalate which may become as high as in primary hyperoxaluria,although levels are generally lower (82, 184). Plasma oxalate may alsobe increased (64, 78, 82, 183, 187). Contrary to what is observed in pri-mary hyperoxaluria, levels of glycolate and L-glycerate are normal inthese patients. Secondary hyperoxaluria may lead to severe morbiditywith urolithiasis or nephrocalcinosis as observed especially in patientswith malabsorptive syndromes, and eventually renal insufficiency(150, 184) or even ESRD (19). However, large cohorts have never beendescribed. In dialysis-related secondary hyperoxaluria, extra renaldepositions of calcium oxalate are rare and do not follow the relentlesspattern of PH1 (119).
01.10
01.11
CHAPTER 01
page 30
VAN WOERDEN 5/19/08 8:53 AM Pagina 30

The mechanism leading to hyperoxaluria in these disorders is not alwa-ys clear. However, for malabsorptive diseases, several hypotheses existby which hyperoxaluria is generated. Three mechanisms are mainlysuggested to give rise to absorptive hyperoxaluria: first, calcium bindsto fatty acids, in steatorrhoea, which is present in patients with malab-sorption. Because of this, less calcium is available to bind oxalate andmore oxalate is available for uptake in the colon. A higher fat intake perse, however, does not necessarily contribute to higher excretion of uri-nary oxalate (13, 120). Secondly, as a consequence of elevated fattyacid concentration in the colon, the permeability of the colon for oxa-late absorption increases, resulting in more oxalate uptake. Thirdly, adepletion of the oxalate degrading bacteria is seen in some patientswith cystic fibrosis, possibly due to frequent use of antibiotics. Thisalso leads to higher oxalate concentrations in the gut, with elevatedoxalate uptake (183). Dietary restrictions of oxalate containing pro-ducts can sometimes prevent or decrease the severity of secondaryhyperoxaluria. However, it can be a persistent clinical problem inmalabsorptive diseases. For patients on dialysis, hyperoxaluria andhyperoxalemia are caused by the inability of dialysis techniques toremove oxalate sufficiently, and oxalate accumulation occurs. Plasmalevels can rise up to 116 µmol/l and systemic oxalosis with organinvolvement has been reported frequently (19, 55, 127, 147, 189).
AIM OF THE STUDYResearch has elucidated parts of the complicated genetic and metabo-lic changes that constitute the basis of primary hyperoxaluria type 1.However, a number of questions remain to be answered.
One of the most difficult issues in primary hyperoxaluria type 1 (PH1)is the heterogeneity of the disease, at the genetic, biochemical and cli-nical level. This heterogeneity prevents a clear prediction of diseaseseverity or of outcome of patients based on patient characteristics. Themain aim of this study is to unravel this heterogeneity. For this, a nati-onwide cohort will be recruited, and patient characteristics will be des-cribed, at the genetic, biochemical and clinical level. This facilitates thecalculation of the prevalence of PH1 in The Netherlands, and may leadto a correlation between genetic and biochemical studies on the onehand, and clinical outcome of patients on the other hand. Differentoptions for treatment will also be assessed in the patient cohort, inclu-ding conservative treatment with pyridoxine, and transplantations.Concerning the issue of transplantation, either a (1) kidney, (2) pre-emptive liver, (3) combined liver-kidney, or (4) sequential liver-kidneytransplantation is available. For each of these options, systematic cli-nical evidence is lacking and adverse effects are considerable. At thetime of onset of this study, data on the outcomes of the different trans-plantation policies were too conflicting to draw definite conclusions
01.12
CHAPTER 01
page 31
VAN WOERDEN 5/19/08 8:53 AM Pagina 31

for therapeutic strategies. To address this issue, we decided to analyzeall transplanted patients in our cohort and we designed a strategy fortype and timing of transplantations, based on the clinical, biochemicaland genetic experience in our national cohort.
Diagnostic studies include the use of mutation analysis of the AGXTgene. The applicability of DNA diagnosis for patients with primaryhyperoxaluria was not known in The Netherlands. Furthermore, therelationship between AGXT gene mutations and the clinical phenotypeof patients with PH1 was unclear. We aim to assess the spectrum ofAGXT gene mutations in Dutch patients with PH1 and evaluate the useof DNA diagnosis in PH1, as a rapid, non-invasive tool in diagnosticscreening. Using the clinical information of the Dutch patient cohort,we will try to relate the clinical phenotype to AXGT gene mutations.
Another issue concerning screening for PH1 is the collection of urinefor oxalate and glycolate measurements. This is usually performed inacidified containers, which exposes patients to the hazards of hydro-chloric acid. No systematic studies have addressed its use in PH1 andwe investigate whether hydrochloric acid should still be applied, or itcould be added to the urine collection after arrival of the urine speci-men at the laboratory.
Regarding the occurrence of hyperoxaluria and renal involvement insome patients with Zellweger spectrum disorders, our aim is to studya cohort of these patients to assess the incidence of hyperoxaluria inthem, and the potential implications for renal involvement.Biochemically, patients with Zellweger spectrum disorders lackperoxisomes and therefore, the in vivo results of cytosolically localizedAGT enzyme becomes apparent. The correlation between the clinicalseverity of this neurological disease and the incidence of renal invol-vement and hyperoxaluria will be studied.
Finally, we initiate research to evaluate potential new treatment in PH1and to investigate a biochemical model that facilitates studies of thebiochemical origin of oxalate. For patients with a preserved renal func-tion, urinary excretion of oxalate is regarded to reflect endogenousoxalate production, unless renal insufficiency occurs. New treatmentcould be targeted to try to reduce endogenous oxalate synthesis.Evaluation of its efficacy is only possible if a careful estimation ofendogenous oxalate synthesis is available. Since endogenous oxalate isproduced by the liver, the rate of appearance of oxalate in plasmawould accommodate this need. We use an in vivo isotope dilutionmethod to calculate the rate of appearance of oxalate in plasma inpatients and control subjects. CHAPTER 01
page 32
VAN WOERDEN 5/19/08 8:53 AM Pagina 32

The Agxt -/- mouse, an animal model for primary hyperoxaluria type 1,was recently developed by Salido et al. (177). The Agxt -/- mouse is defi-cient for the AGT enzyme, and displays high levels of urinary oxalate.Development of rational therapies that interfere with endogenous oxa-late synthesis is hampered by the lack of knowledge on the exact sour-ces of oxalate, apart from its direct precursor glyoxylate. Therefore, wewill isolate hepatocytes from the Agxt -/- mouse to study the contribu-tion of potential precursors of oxalate synthesis.
REFERENCES
CHAPTER 01
page 33
1. Akhan O, Ozmen MN,
Coskun M, Ozen S, Akata D, Saatci U.
Systemic oxalosis: pathognomonic
renal and specific extrarenal findings
on US and CT.
Pediatr Radiol 1995;25:15-16.
2. Amoroso A, Pirulli D, Florian F,
Puzzer D, Boniotto M, Crovella S et al.
AGXT gene mutations and their
influence on clinical heterogeneity of
type 1 primary hyperoxaluria.
J Am Soc Nephrol 2001;12:2072-79.
3. Amoroso A, Pirulli D, Puzzer D,
Ferri L, Crovella S, Ferrettini C et al.
Gene symbol: AGXT. Disease: primary
hyperoxaluria type I. Hum Genet
1999;104:441.
4. Antoine B, Slama R, Josso F,
de M, Habib R, Richet G.
The destruction of the renal
parenchyma by invasion by calcium
oxalate crystals. 2 New cases of
‘renal oxalosis’.
Presse Med 1960;68:803-6.
5. Aponte GE, Fetter TR. Familial
idiopathic oxalate nephrocalcinosis.
Am J Clin Pathol 1954;24:1363-73.
6. Archer HE, Dormer AE, Scowen
EF, Watts RW. Primary hyperoxaluria.
Lancet 1957;273:320-22.
7. Archer HE, Dormer AE, Scowen
EF, Watts RW. Studies on the urinary
excretion of oxalate by normal subjects.
Clin Sci 1957;16:405-11.
8. Asker H, Davies D. Purification
of rat liver enzymes involved in the
oxidation of glyoxylate. Biochim
Biophys Acta 1983;761:103-8.
9. Asselman M, Verhulst A, De
Broe ME, Verkoelen CF. Calcium
oxalate crystal adherence to
hyaluronan-, osteopontin-, and CD44-
expressing injured/regenerating
tubular epithelial cells in rat kidneys.
J Am Soc Nephrol 2003;14:3155-66.
10. Atkins GL, Dean BM, Griffin WJ,
Scowen EF, Watts RW. Quantitative
aspects of ascorbic acid metabolism in
patients with primary hyperoxaluria.
Clin Sci 1965;29:305-14.
11. Atkins GL, Dean BM, Griffin WJ,
Scowen EF, Watts RW. Primary hyper-
oxaluria. The relation between ascorbic
acid and the increased urinary excretion
of oxalate. Lancet 1963;12:1096-97.
12. Auer BL, Auer D, Rodgers AL.
Relative hyperoxaluria, crystalluria
and haematuria after megadose
ingestion of vitamin C. Eur J Clin
Invest 1998;28:695-700.
VAN WOERDEN 5/19/08 8:53 AM Pagina 33

CHAPTER 01
page 34
13. Bailly GG, Norman RW,
Thompson C. Effects of dietary fat on
the urinary risk factors of calcium
stone disease. Urology 2000;56:40-44.
14. Baker EM, Saari JC, Tolbert BM.
Ascorbic acid metabolism in man.
Am J Clin Nutr 1966;19:371-78.
15. Barratt TM, Kasidas GP,
Murdoch I, Rose GA. Urinary oxalate
and glycolate excretion and plasma
oxalate concentration.
Arch Dis Child 1991;66:501-3.
16. Basmaison O, Rolland MO,
Cochat P, Bozon D. Identification of 5
novel mutations in the AGXT gene.
Hum Mutat 2000;15:577.
17. Baxmann AC, De OGM, Heilberg IP.
Effect of vitamin C supplements on
urinary oxalate and pH in calcium
stone-forming patients.
Kidney Int 2003;63:1066-71.
18. Benhamou CL, Bardin T,
Tourliere D, Voisin L, Audran M,
Edouard C et al. Bone involvement in
primary oxalosis. Study of 20 cases.
Rev Rhum Mal Osteoartic 1991;58:763-69.
19. Bernhardt WM, Schefold JC,
Weichert W, Rudolph B, Frei U,
Groneberg DA, Schindler R.
Amelioration of anemia after kidney
transplantation in severe secondary
oxalosis. Clin Nephrol 2006;65:216-21.
20. Blau N, Matasovic A,
Lukasiewicz-Wedlechowicz A, Heiz-
mann CW, Leumann E. Simultaneous
determination of oxalate, glycolate,
citrate, and sulfate from dried urine
filter paper spots in a pediatric popu-
lation. Clin Chem 1998;44:1554-56.
21. Boquist L, Lindqvist B, Ostberg
Y, Steen L. Primary oxalosis.
Am J Med 1973;54:673-81.
22. Buchman AL, Moukarzel AA,
Ament ME. Excessive urinary oxalate
excretion occurs in long-term TPN
patients both with and without ileo-
stomies. J Am Coll Nutr 1995;14:24-28.
23. Butz M, Hoffmann H, Kohlbecker G.
Dietary influence on serum and urinary
oxalate in healthy subjects and oxalate
stone formers. Urol Int 1980;35:309-15.
24. Caldwell EF, Mayor LR, Thomas
MG, Danpure CJ. Diet and the
frequency of the alanine:glyoxylate
aminotransferase Pro11Leu polymor-
phism in different human populations.
Hum Genet 2004;115:504-9.
25. Chai W, Liebman M, Kynast-
Gales S, Massey L. Oxalate absorption
and endogenous oxalate synthesis
from ascorbate in calcium oxalate
stone formers and non-stone formers.
Am J Kidney Dis 2004;44:1060-69.
26. Chou LY, Donohue WL. Oxalosis;
possible inborn error of metabolism
with nephrolithiasis and nephrocalci-
nosis due to calcium oxalate as the
predominating features. Pediatrics
1952;10:660-66.
27. Cochat P, Deloraine A, Rotily M,
Olive F, Liponski I, Deries N.
Epidemi-ology of primary hyper-
oxaluria type 1. Société de Néphrologie
and the Société de Néphrologie
Pédiatrique. Nephrol Dial Transplant
1995;10 Suppl 8:3-7.
28. Cochat P, Gaulier JM, Koch
Nogueira PC, Feber J, Jamieson NV,
VAN WOERDEN 5/19/08 8:53 AM Pagina 34

Rolland MO et al. Combined liver-
kidney transplantation in primary
hyperoxaluria type 1. Eur J Pediatr
1999;158 Suppl 2:S75-S80.
29. Cochat P, Rolland MO.
Primary hyperoxalurias. In: Fernandes
J, Saudubray JM, van den Berghe G,
eds. Inborn metabolic diseases and
treatment. Heidelberg: Springer
Verlag, 2000:441-46.
30. Cochran M, Hofhkinson A,
Zarembski PM, Anderson CK.
Hyperoxaluria in adults. Br J Surg
1968; 55:121-28.
31. Constable AR, Joekes AM,
Kasidas GP, O'Regan P, Rose GA.
Plasma level and renal clearance of
oxalate in normal subjects and in
patients with primary hyperoxaluria
or chronic renal failure or both.
Clin Sci 1979;56:299-304.
32. Conyers RA, Bais R, Rofe AM.
The relation of clinical catastrophes,
endogenous oxalate production, and
urolithiasis.Clin Chem 1990;36:1717-30.
33. Cooper PJ, Danpure CJ,
Wise PJ, Guttridge KM.
Immunocytochemical localization of
human hepatic alanine: glyoxylate
aminotransferase in control subjects
and patients with primary hyper-
oxaluria type 1. J Histochem
Cytochem 1988;36:1285-94.
34. Coulter-Mackie MB, Lian Q,
Applegarth D, Toone J. The major
allele of the alanine:glyoxylate amino-
transferase gene: Nine novel mutations
and polymorphisms associated with
primary hyperoxaluria type 1.
Mol Genet Metab 2005;86:172-78.
35. Coulter-Mackie MB, Rumsby G.
Genetic heterogeneity in primary hyper-
oxaluria type 1: impact on diagnosis.
Mol Genet Metab 2004;83:38-46.
36. Coulter-Mackie MB, Rumsby G,
Applegarth DA, Toone JR. Three novel
deletions in the alanine:glyoxylate ami-
notransferase gene of three patients
with type 1 hyperoxaluria.
Mol Genet Metab 2001;74:314-21.
37. Coulter-Mackie MB, Tung A,
Henderson HE, Toone JR, Applegarth
DA. The AGT gene in Africa: a distinctive
minor allele haplotype, a polymorphism
(V326I), and a novel PH1 mutation
(A112D) in Black Africans.
Mol Genet Metab 2003;78:44-50.
38. Craigen WJ. Persistent glycolic
aciduria in a healthy child with normal
alanine-glyoxylate aminotransferase
activity. J Inherit Metab Dis 1996;
19:793-94.
39. Cramer SD, Ferree PM, Lin K,
Milliner DS, Holmes RP. The gene
encoding hydroxypyruvate reductase
(GRHPR) is mutated in patients with
primary hyperoxaluria type II.
Hum Mol Genet 1999;8:2063-69.
40. Crawford GA, Mahony JF,
Gyory AZ. Measurement of urinary
oxalate in the presence of ascorbic acid.
Clin Chim Acta 1985;147:51-57.
41. Crawhall JC, Scowen EF, Watts RW.
Conversion of glycine to oxalate in
primary hyperoxaluria. Lancet
1959;2:806-9.
42. Curhan GC, Willett WC, Rimm
EB, Stampfer MJ. A prospective study of
the intake of vitamins C and B6, and
CHAPTER 01
page 35
VAN WOERDEN 5/19/08 8:53 AM Pagina 35

the risk of kidney stones in men.
J Urol 1996;155:1847-51.
43. Danpure CJ. Molecular and
clinical heterogeneity in primary
hyperoxaluria type 1.
Am J Kidney Dis 1991;17:366-69.
44. Danpure CJ. The molecular
basis of alanine: glyoxylate amino-
transferase mistargeting: the most
common single cause of primary
hyperoxaluria type 1.
J Nephrol 1998;11 Suppl 1:8-12.
45. Danpure CJ. Variable peroxiso-
mal and mitochondrial targeting of
alanine: glyoxylate aminotransferase
in mammalian evolution and disease.
Bioessays 1997;19:317-26.
46. Danpure CJ, Birdsey GM,
Rumsby G, Lumb MJ, Purdue PE,
Allsop J. Molecular characterization
and clinical use of a polymorphic tan-
dem repeat in an intron of the human
alanine:glyoxylate aminotransferase
gene. Hum Genet 1994;94:55-64.
47. Danpure CJ, Jennings PR.
Peroxisomal alanine:glyoxylate amino-
transferase deficiency in primary
hyperoxaluria type I.
FEBS Lett 1986;201:20-24.
48. Danpure CJ, Jennings PR,
Fryer P, Purdue PE, Allsop J. Primary
hyperoxaluria type 1: genotypic and
phenotypic heterogeneity.
J Inherit Metab Dis 1994;17:487-99.
49. Danpure CJ, Purdue PE, Fryer P,
Griffiths S, Allsop J, Lumb MJ et al.
Enzymological and mutational
analysis of a complex primary
hyperoxaluria type 1 phenotype
involving alanine:glyoxylate amino-
transferase peroxisome-to-mitochon-
drion mistargeting and intra-
peroxisomal aggregation.
Am J Hum Genet 1993;53:417-32.
50. Davis JS, Klingberg WG, Stowell RE.
Nephrolithiasis and nephrocalcinosis
with calcium oxalate crystals in kidneys
and bones. J Pediatr 1950;36:323-34.
51. Dietzen DJ, Wilhite TR, Kenagy
DN, Milliner DS, Smith CH, Landt M.
Extraction of glyceric and glycolic
acids from urine with tetrahydrofuran:
utility in detection of primary hyper-
oxaluria. Clin Chem 1997;43:1315-20.
52. Doganavsargil B, Akil I, Sen S,
Mir S, Basdemir G. Autopsy findings
of a case with oxalosis.
Pediatr Dev Pathol 2007;14:1.
53. Ebstein W, Nicolaier A. Über die
Wirkung der Oxalsäure und einiger
ihrer Derivate auf die Nieren.
Virchows Archiv 1897;148:366-88.
54. Ellis SR, Hulton SA, McKiernan
PJ, de Ville de GJ, Kelly DA. Combined
liver-kidney transplantation for primary
hyperoxaluria type 1 in young children.
Nephrol Dial Transplant 2001;16:348-54.
55. Fayemi AO, Ali M, Braun EV.
Oxalosis in hemodialysis patients: a
pathologic study of 80 cases. Arch
Pathol Lab Med 1979;103:58-62.
56. Frederick EW, Rabkin MT,
Richie RH, Jr., Smith LH, Jr. Studies
on primary hyperoxaluria. I. In vivo
demonstration of a defect in
glyoxylate metabolism. N Engl J Med
1963;269:821-29.CHAPTER 01
page 36
VAN WOERDEN 5/19/08 8:53 AM Pagina 36

57. Frishberg Y, Rinat C, Shalata A,
Khatib I, Feinstein S, Becker-Cohen R
et al. Intra-familial clinical heteroge-
neity: absence of genotype-phenotype
correlation in primary hyperoxaluria
type 1 in Israel. Am J Nephrol
2005;25:269-75.
58. Gambardella RL, Richardson KE.
The pathways of oxalate formation
from phenylalanine, tyrosine, tryptop-
han and ascorbic acid in the rat.
Biochim Biophys Acta 1977;499:156-68.
59. Gambardella RL, Richardson KE.
The formation of oxalate from hydro-
xypyruvate, serine, glycolate and
glyoxylate in the rat. Biochim
Biophys Acta 1978;544:315-28.
60. Gershoff SN, Vitamin B6
and oxalate metabolism.
Vitam Horm 1964;22:581-89.
61. Gershoff SN, Faragalla FF.
Endogenous oxalate synthesis and gly-
cine, serine, deoxypyridoxine inter-
relationships in vitamin B6-deficient
rats. J Biol Chem 1959;234:2391-93.
62. Gibbs DA, Watts RW. The varia-
tion of urinary oxalate excretion with
age. J Lab Clin Med 1969;73:901-8.
63. Gibbs DA, Watts RW. Biochemical
studies on the treatment of primary
hyperoxaluria. Arch Dis Child
1967;42:505-8.
64. Gibney EM, Goldfarb DS. The
association of nephrolithiasis with
cystic fibrosis. Am J Kidney Dis
2003;42:1-11.
65. Gottlieb RP, Ritter JA. ‘Flecked
retina’ - an association with primary
hyperoxaluria. J Pediatr 1977;90:939-42.
66. Guo C, McMartin KE. The cyto-
toxicity of oxalate, metabolite of ethyle-
ne glycol, is due to calcium oxalate
monohydrate formation. Toxicology
2005;208:347-55.
67. Hagen L, Walker VR, Sutton RA.
Plasma and urinary oxalate and glyco-
late in healthy subjects. Clin Chem
1993;39:134-38.
68. Hagler L, Herman RH. Oxalate
metabolism. I. Am J Clin Nutr
1973;26:758-65.
69. Hall BM, Walsh JC, Horvath JS,
Lytton DG. Peripheral neuropathy com-
plicating primary hyperoxaluria.
J Neurol Sci 1976;29:343-49.
70. Haqqani MT, Crystals in brain
and meninges in primary hyperoxalu-
ria and oxalosis. J Clin Pathol
1977;30:16-18.
71. Hatch M, Mulgrew S, Bourke E,
Keogh B, Costello J. Effect of mega-
doses of ascorbic acid on serum and
urinary oxalate. Eur Urol 1980;6:166-69.
72. Helin I. Primary hyperoxaluria.
An analysis of 17 Scandinavian
patients. Scand J Urol Nephrol
1980;14:61-64.
73. Hockaday TD, Clayton JE,
Frederick EW, Smith LH, Jr. Primary
hyperoxaluria. Medicine 1964;43:315-45.
74. Hodgkinson A, Wilkinson R.
Plasma oxalate concentration and
renal excretion of oxalate in man.
Clin Sci Mol Med 1974;46:61-73.
75. Holbrook JD, Birdsey GM, Yang Z,
CHAPTER 01
page 37
VAN WOERDEN 5/19/08 8:53 AM Pagina 37

Bruford MW, Danpure CJ. Molecular
adaptation of alanine:glyoxylate
amino-transferase targeting i
n primates. Mol Biol Evol 2000;
17:387-400.
76. Holmes RP, Goodman HO,
Assimos DG. Contribution of dietary
oxalate to urinary oxalate excretion.
Kidney Int 2001;59:270-76.
77. Hoppe B, Danpure CJ, Rumsby
G, Fryer P, Jennings PR, Blau N et al.
A vertical (pseudodominant) pattern of
inheritance in the autosomal recessive
disease primary hyperoxaluria type 1:
lack of relationship between genotype,
enzymic phenotype, and disease severity.
Am J Kidney Dis 1997;29:36-44.
78. Hoppe B, Hesse A, Bromme S,
Rietschel E, Michalk D. Urinary
excretion substances in patients with
cystic fibrosis: risk of urolithiasis?
Pediatr Nephrol 1998;12:275-79.
79. Hoppe B, Langman CB. A United
States survey on diagnosis, treatment,
and outcome of primary hyperoxaluria.
Pediatr Nephrol 2003;18:986-91.
80. Hoppe B, Latta K, von
Schnakenburg C, Kemper MJ. Primary
hyperoxaluria-the German experience.
Am J Nephrol 2005;25:276-81.
81. Hoppe B, Leumann E, von UG,
Laube N, Hesse A. Diagnostic and
therapeutic approaches in patients
with secondary hyperoxaluria.
Front Biosci 2003;8:437-443.
82. Hoppe B, von Unruh GE,
Blank G, Rietschel E, Sidhu H,
Laube N, Hesse A. Absorptive hyper-
oxaluria leads to an increased risk
for urolithiasis or nephrocalcinosis
in cystic fibrosis.
Am J Kidney Dis 2005;46:440-45.
83. Horvath VA, Wanders RJ. Rapid
identification of primary hyperoxaluria
type I patients using a novel, fully
automated method for measurement of
hepatic alanine: glyoxylate amino-
transferase. J Inherit Metab Dis
1994;17:336-38.
84. Horvath VA, Wanders RJ.
Re-evaluation of conditions required
for measurement of true alanine:
glyoxylate aminotransferase activity
in human liver: implications for the
diagnosis of hyperoxaluria type I.
Ann Clin Biochem 1994;31:361-66.
85. Howard JE, Thomas WC, Jr.
Control of crystallization in urine.
Am J Med 1968;45:693-99.
86. Huber PA, Birdsey GM, Lumb
MJ, Prowse DT, Perkins TJ, Knight DR,
Danpure CJ. Peroxisomal import of
human alanine:glyoxylate aminotrans-
ferase requires ancillary targeting
information remote from its C terminus.
J Biol Chem 2005;280:27111-20.
87. Inoue Y, Masuyama H, Ikawa H,
Mitsubuchi H, Kuhara T. Monitoring
method for pre- and post-liver trans-
plantation in patients with primary
hyperoxaluria type I. J Chromatogr B
Analyt Technol Biomed Life Sci 2003;
792:89-97.
88. Itami N, Yasoshima K, Akutsu Y,
Nonomura K. Spot-urine screening for
primary hyperoxaluria.
Nephron 1990;56:337-38.
89. Ito H, Suzuki F, Yamaguchi K,
CHAPTER 01
page 38
VAN WOERDEN 5/19/08 8:53 AM Pagina 38

Nishikawa Y, Kotake T. Reduction of
urinary oxalate by combined calcium
and citrate administration without
increase in urinary calcium oxalate
stone formers. Clin Nephrol 1992;
37:14-18.
90. Jacobsen D, Ovrebo S, Ostborg J,
Sejersted OM. Glycolate causes the aci-
dosis in ethylene glycol poisoning and
is effectively removed by hemodialysis.
Acta Med Scand 1984;216:409-16.
91. James HM, Bais R, Edwards JB,
Rofe AM, Conyers AJ. Models for the
metabolic production of oxalate from
xylitol in humans: a role for fructo-
kinase and aldolase. Aust J Exp Biol
Med Sci 1982;60:117-22.
92. James HM, Williams SG, Bais R,
Rofe AM, Edwards JB, Conyers RA.
The metabolic production of oxalate
from xylitol: activities of transketolase,
transaldolase, fructokinase and aldola-
se in liver, kidney, brain, heart and
muscle in the rat, mouse, guinea pig,
rabbit and human. Int J Vitam Nutr
Res Suppl 1985;28:29-46.
93. Jamieson NV. The European
primary hyperoxaluria Type 1
Transplant Registry report on the
results of combined liver/kidney trans-
plantation for primary hyperoxaluria
1984-1994. European PH1 Transplan-
tation Study Group. Nephrol Dial
Transplant 1995;10 Suppl 8:33-37.
94. Jamieson NV. The results of
combined liver/kidney transplantation
for primary hyperoxaluria (PH1) 1984-
1997. The European PH1 transplant
registry report. European PH1
Transplantation Study Group.
J Nephrol 1998;11 Suppl 1:36-41.
95. Johnson SA, Rumsby G,
Cregeen D, Hulton SA. Primary
hyperoxaluria type 2 in children.
Pediatr Nephrol 2002;17:597-601.
96. Kasidas GP, Rose GA.
Measurement of plasma oxalate in
healthy subjects and in patients with
chronic renal failure using immobilised
oxalate oxidase. Clin Chim Acta
1986;154:49-58.
97. Kasidas GP, Rose GA.
Spontaneous in vitro generation of oxa-
late from L-ascorbate in some assays
for urinary oxalate and its prevention.
In: Schwille PO, Smith LH, Robertson
WG, eds. Urolithiasis and related clini-
cal research. New York: Plenum Press,
1985:653-56.
98. Kist-van Holthe JE, Onkenhout
W, van der Heijden AJ. Pyridoxine-res-
ponsive nephrocalcinosis and glycolic
aciduria in two siblings without hyper-
oxaluria and with normal alanine:
glyoxalate aminotransferase activity.
J Inherit Metab Dis 2000;23:91-92.
99. Knight J, Holmes RP.
Mitochondrial hydroxyproline metabo-
lism: implications for primary hyper-
oxaluria. Am J Nephrol 2005;25:171-75.
100. Knight J, Jiang J, Assimos DG,
Holmes RP. Hydroxyproline ingestion
and urinary oxalate and glycolate
excretion. Kidney Int 2006;70:1929-34.
101. Knoflach A, Azuma H, Magee C,
Denton M, Murphy B, Iyengar A et al.
Immunomodulatory functions of low-
molecular weight hyaluronate in an
acute rat renal allograft rejection
model. J Am Soc Nephrol
1999;10:1059-66.
CHAPTER 01
page 39
VAN WOERDEN 5/19/08 8:53 AM Pagina 39

102. Knols G, Leunissen KM, Spaapen
LJ, Bosman FT, vd Wiel TW, Kootstra G,
van Hooff JP. Recurrence of nephro-
calcinosis after renal transplantation
in an adult patient with primary
hyperoxaluria type I. Nephrol Dial
Transplant 1989;4:137-39.
103. Latta K, Brodehl J. Primary
hyperoxaluria type I.
Eur J Pediatr 1990;149:518-22.
104. Latta K, Jamieson NV,
Scheinman JI, Scharer K, Bensman A,
Cochat P et al. Selection of transplan-
tation procedures and perioperative
management in primary hyperoxaluria
type 1. Nephrol Dial Transplant
1995;10 Suppl 8:53-57.
105. Leiper JM, Danpure CJ.
A unique molecular basis for enzyme
mistargeting in primary hyper-
oxaluria type 1. Clin Chim Acta
1997;266:39-50.
106. Leiper JM, Oatey PB, Danpure
CJ. Inhibition of alanine:glyoxylate
aminotransferase 1 dimerization is a
prerequisite for its peroxisome-to-mito-
chondrion mistargeting in primary
hyperoxaluria type 1.
J Cell Biol 1996;135:939-51.
107. Lemann J, Jr., Hornick LJ,
Pleuss JA, Gray RW. Oxalate is over-
estimated in alkaline urines collected
during administration of bicarbonate
with no specimen pH adjustment.
Clin Chem 1989;35:2107-10.
108. Lepoutre C. Calculs multiples
chez un enfant: Infiltration du paren-
chyme renal par des depots cristallins.
J Urol 1925;20:424.
109. Leth PM, Gregersen M.
Ethylene glycol poisoning.
Forensic Sci Int 2005;155:179-84.
110. Leumann E, Hoppe B, Neuhaus T.
Management of primary hyperoxaluria:
efficacy of oral citrate administration.
Pediatr Nephrol 1993;7:207-11.
111. Leumann EP, Dietl A, Matasovic
A. Urinary oxalate and glycolate excre-
tion in healthy infants and children.
Pediatr Nephrol 1990;4:493-97.
112. Leumann EP, Niederwieser A,
Fanconi A. New aspects of infantile oxa-
losis. Pediatr Nephrol 1987;1:531-35.
113. Lhotta K, Rumsby G, Vogel W,
Pernthaler H, Feichtinger H, Konig P.
Primary hyperoxaluria type 1 caused
by peroxisome-to-mitochondrion
mistargeting of alanine: glyoxylate
aminotransferase. Nephrol Dial
Transplant 1996;11:2296-98.
114. Lumb MJ, Danpure CJ.
Functional synergism between the
most common polymorphism in
human alanine:glyoxylate amino-
transferase and four of the most
common disease-causing mutations.
J Biol Chem 2000;275:36415-22.
115. Lumb MJ, Drake AF,
Danpure CJ. Effect of N-terminal
alpha-helix formation on the
dimerization and intra-cellular
targeting of alanine:glyoxylate
aminotransferase.
J Biol Chem 1999;274:20587-96.
116. Malek RS, Kelalis PP. Nephro-
calcinosis in infancy and childhood.
J Urol 1975;114:441-43.CHAPTER 01
page 40
VAN WOERDEN 5/19/08 8:53 AM Pagina 40

117. Marangella M, Petrarulo M,
Bianco O, Vitale C, Finocchiaro P,
Linari F. Glycolate determination
detects type I primary hyperoxaluria
in dialysis patients. Kidney Int
1991;39:149-54.
118. Marangella M, Petrarulo M,
Vitale C, Cosseddu D, Linari F. Plasma
and urine glycolate assays for differen-
tiating the hyperoxaluria syndromes.
J Urol 1992;148:986-89.
119. Marangella M, Vitale C,
Petrarulo M, Tricerri A, Cerelli E,
Cadario A et al. Bony content of
oxalate in patients with primary
hyperoxaluria or oxalosis-unrelated
renal failure. Kidney Int 1995;
48:182-87.
120. Masai M, Ito H, Kotake T. Effect
of dietary intake on urinary oxalate
excretion in calcium renal stone formers.
Br J Urol 1995;76:692-96.
121. Mashour S, Turner JF, Jr.,
Merrell R. Acute renal failure, oxalosis,
and vitamin C supplementation: a case
report and review of the literature.
Chest 2000;118:561-63.
122. Massey L. Magnesium therapy
for nephrolithiasis.
Magnes Res 2005;18:123-26.
123. Massey LK, Liebman M, Kynast-
Gales SA. Ascorbate increases human
oxaluria and kidney stone risk.
J Nutr 2005;135:1673-77.
124. Mattoo TK, Katawee Y. Oxalate
creatinine ratio in the peritoneal fluid
of patients with primary hyperoxaluria.
Nephron 1992;60:496-97.
125. Mclaurin AW, Beisel WR,
Mccormick GJ, Scalettar R, Herman RH.
Primary hyperoxaluria.
Ann Intern Med 1961;55:70-80.
126. Meier M, Nitschke M, Perras B,
Steinhoff J. Ethylene glycol intoxication
and xylitol infusion--metabolic steps of
oxalate-induced acute renal failure.
Clin Nephrol 2005;63:225-28.
127. Milgram JW, Salyer WR.
Secondary oxalosis of bone in
chronic renal failure.
A histopathological study of
three cases. J Bone Joint Surg
Am 1974;56:387-95.
128. Milliner DS. The primary hyper-
oxalurias: an algorithm for diagnosis.
Am J Nephrol 2005;25:154-60.
129. Milliner DS, Eickholt JT,
Bergstralh EJ, Wilson DM, Smith LH.
Results of long-term treatment with
orthophosphate and pyridoxine in
patients with primary hyperoxaluria.
N Engl J Med 1994;331:1553-58.
130. Milliner DS, Wilson DM,
Smith LH. Phenotypic expression of
primary hyperoxaluria: Comparative
features of types I and II. Kidney
International 2001;59:31-36.
131. Minatogawa Y, Tone S, Allsop J,
Purdue PE, Takada Y, Danpure CJ, Kido R.
A serine-to-phenylalanine substitution
leads to loss of alanine:glyoxylate
aminotransferase catalytic activity
and immunoreactivity in a patient
with primary hyperoxaluria type 1.
Hum Mol Genet 1992;1:643-44.
132. Monico CG, Milliner DS.
Hyperoxaluria and urolithiasis in young
CHAPTER 01
page 41
VAN WOERDEN 5/19/08 8:53 AM Pagina 41

children: an atypical presentation.
J Endourol 1999;13:633-36.
133. Monico CG, Milliner DS.
Combined liver-kidney and kidney-
alone transplantation in primary
hyperoxaluria.
Liver Transpl 2001;7:954-63.
134. Monico CG, Persson M, Ford GC,
Rumsby G, Milliner DS. Potential
mechanisms of marked hyperoxaluria
not due to primary hyperoxaluria I or II.
Kidney Int 2002;62:392-400.
135. Monico CG, Rossetti S, Olson JB,
Milliner DS. Pyridoxine effect in type I
primary hyperoxaluria is associated
with the most common mutant allele.
Kidney Int 2005;67:1704-09.
136. Morgan SH, Purkiss P, Watts RW,
Mansell MA. Oxalate dynamics in chronic
renal failure. Comparison with normal
subjects and patients with primary
hyperoxaluria. Nephron 1987;46:253-57.
137. Motley A, Lumb MJ,
Oatey PB, Jennings PR, De Zoysa PA,
Wanders RJ et al. Mammalian
alanine/glyoxylate aminotransferase 1
is imported into peroxisomes via the
PTS1 translocation pathway. Increased
degeneracy and context specificity of
the mammalian PTS1 motif and impli-
cations for the peroxisome-to-mito-
chondrion mistargeting of AGT in
primary hyperoxaluria type
1. J Cell Biol 1995;131:95-109.
138. Nakatani T, Kawasaki Y,
Minatogawa Y, Okuno E, Kido R.
Peroxisome localized human hepatic
alanine-glyoxylate aminotransferase
and its application to clinical diagnosis.
Clin Biochem 1985;18:311-16.
139. Nasr SH, Kashtanova Y, Levchuk
V, Markowitz GS. Secondary oxalosis
due to excess vitamin C intake.
Kidney Int 2006;70:1672.
140. Neuhaus TJ, Belzer T, Blau N,
Hoppe B, Sidhu H, Leumann E. Urinary
oxalate excretion in urolithiasis and
nephrocalcinosis. Arch Dis Child
2000;82:322-26.
141. Ng RH, Menon M, Ladenson JH.
Collection and handling of 24-hour
urine specimens for measurement of
analytes related to renal calculi.
Clin Chem 1984;30:467-71.
142. Nguyen NU, Dumoulin G,
Henriet MT, Regnard J. Increase in uri-
nary calcium and oxalate after fructo-
se infusion. Horm Metab Res
1995;27:155-58.
143. Nishiyama K, Funai T, Katafuchi
R, Hattori F, Onoyama K, Ichiyama A.
Primary hyperoxaluria type I due to a
point mutation of T to C in the coding
region of the serine:pyruvate amino-
transferase gene. Biochem Biophys Res
Commun 1991;176:1093-99.
144. Nishiyama K, Funai T, Yokota S,
Ichiyama A. ATP-dependent degrada-
tion of a mutant serine: pyruvate/
alanine:glyoxylate aminotransferase in
a primary hyperoxaluria type 1 case.
J Cell Biol 1993;123:1237-48.
145. Noguchi T, Takada Y.
Peroxisomal localization of serine:
pyruvate aminotransferase in human
liver. J Biol Chem 1978;253:7598-600.
146. Nolkemper D, Kemper MJ,
Burdelski M, Vaismann I, Rogiers X,
Broelsch CE et al. Long-term results
CHAPTER 01
page 42
VAN WOERDEN 5/19/08 8:53 AM Pagina 42

of pre-emptive liver transplantation in
primary hyperoxaluria type 1.
Pediatr Transplant 2000;4:177-81.
147. op de Hoek CT, Diderich PP,
Gratama S, von Hofwegen EJ. Oxalosis
in chronic renal failure. Proc Eur Dial
Transplant Assoc 1980;17:730-35.
148. Osther PJ. Hyperoxaluria in
idiopathic calcium nephrolithiasis--
what are the limits? Scand J Urol
Nephrol 1999;33:368-71.
149. Parkinson IS, Channon SM,
Tomson CR, Adonai LR, Ward MK,
Laker MF. The determination of plasma
oxalate concentrations using an enzy-
me/bioluminescent assay. 2. Co-immo-
bilisation of bioluminescent enzymes
and studies of in vitro oxalogenesis.
Clin Chim Acta 1989;179:97-108.
150. Parks JH, Worcester EM,
O'connor RC, Coe FL. Urine stone risk
factors in nephrolithiasis patients with
and without bowel disease.
Kidney Int 2003;63:255-65.
151. Petrarulo M, Bianco O,
Marangella M, Pellegrino S, Linari F,
Mentasti E. Ion chromatographic deter-
mination of plasma oxalate in healthy
subjects, in patients with chronic renal
failure and in cases of hyperoxaluric
syndromes. J Chromatogr 1990;
511:223-31.
152. Petrarulo M, Vitale C, Facchini
P, Marangella M. Biochemical approach
to diagnosis and differentiation of
primary hyperoxalurias: an update.
J Nephrol 1998;11 Suppl 1:23-28.
153. Phang JM, Hu CA, Valle D.
Disorders of proline and hydroxyproline
metabolism. In: Scriver CR, Beaudet AL,
Sly WS, Valle D, Childs B, Kinzler KW,
Vogelstein B, eds. The Metabolic and
Molecular Basis Of Inherited Disease.
New York: McGraw-Hill, 2001:1821-38.
154. Pirulli D, Marangella M,
Amoroso A. Primary hyperoxaluria:
genotype-phenotype correlation.
J Nephrol 2003;16:297-309.
155. Pirulli D, Puzzer D, Ferri L,
Crovella S, Amoroso A, Ferrettini C
et al. Molecular analysis of hyperoxalu-
ria type 1 in Italian patients reveals
eight new mutations in the alanine:
glyoxylate aminotransferase gene.
Hum Genet 1999;104:523-25.
156. Poll-The BT, Gootjes J, Duran M,
De Klerk JB, Wenniger-Prick LJ,
Admiraal RJ et al. Peroxisome biogene-
sis disorders with prolonged survival:
phenotypic expression in a cohort of
31 patients. Am J Med Genet A 2004;
126:333-38.
157. Prenen JA, Boer P, Mees EJ,
Endeman HJ, Spoor SM, Oei HY.
Renal clearance of [14C]oxalate:
comparison of constant-infusion
with single-injection techniques.
Clin Sci 1982;63:47-51.
158. Purdue PE, Allsop J, Isaya G,
Rosenberg LE, Danpure CJ.
Mistargeting of peroxisomal L-alanine:
glyoxylate aminotransferase to mito-
chondria in primary hyperoxaluria
patients depends upon activation of
a cryptic mitochondrial targeting
sequence by a point mutation. Proc
Natl Acad Sci U S A 1991;88:10900-04.
159. Purdue PE, Lumb MJ, Allsop J,
Danpure CJ. An intronic duplication
CHAPTER 01
page 43
VAN WOERDEN 5/19/08 8:53 AM Pagina 43

in the alanine: glyoxylate aminotrans-
ferase gene facilitates identification of
mutations in compound heterozygote
patients with primary hyperoxaluria
type 1. Hum Genet 1991;87:394-96.
160. Purdue PE, Lumb MJ, Allsop J,
Minatogawa Y, Danpure CJ. A glycine-
to-glutamate substitution abolishes
alanine:glyoxylate aminotransferase
catalytic activity in a subset of patients
with primary hyperoxaluria type 1.
Genomics 1992;13:215-18.
161. Purdue PE, Lumb MJ, Fox M,
Griffo G, Hamon-Benais C, Povey S,
Danpure CJ. Characterization and
chromosomal mapping of a genomic
clone encoding human alanine:
glyoxylate aminotransferase.
Genomics 1991;10:34-42.
162. Purdue PE, Takada Y,
Danpure CJ. Identification of mutations
associated with peroxisome-to-mito-
chondrion mistargeting of alanine/gly-
oxylate aminotransferase in primary
hyperoxaluria type 1. J Cell Biol
1990;111:2341-51.
163. Reusz GS, Dobos M, Byrd D,
Sallay P, Miltenyi M, Tulassay T. Urinary
calcium and oxalate excretion in
children. Pediatr Nephrol 1995;9:39-44.
164. Richardson KE, Tolbert NE.
Oxidation of glyoxylic acid to oxalic
acid by glycolic acid oxidase. J Biol
Chem 1961;236:1280-84.
165. Rinat C, Wanders RJ, Drukker A,
Halle D, Frishberg Y. Primary hyper-
oxaluria type I: a model for multiple
mutations in a monogenic disease
within a distinct ethnic group.
J Am Soc Nephrol 1999;10:2352-58.
166. Robertson WG, Peacock M,
Nordin BE. Activity products in stone-
forming and non-stone-forming urine.
Clin Sci 1968;34:579-94.
167. Robertson WG, Peacock M,
Nordin BE. Calcium crystalluria in
recurrent renal-stone formers.
Lancet 1969;2:21-24.
168. Rodgers A, lie-Hamdulay S,
Jackson G. Therapeutic action of
citrate in urolithiasis explained by
chemical speciation: increase in pH is
the determinant factor. Nephrol Dial
Transplant 2006;21:361-69.
169. Rofe AM, Chalmers AH, Edwards
JB. [14C]oxalate synthesis from [U-
14C]glyoxylate and [1-14C]glycollate in
isolated rat hepatocytes. Biochem Med
1976;16:277-83.
170. Rofe AM, James HM, Bais R,
Conyers RA. Hepatic oxalate production:
the role of hydroxypyruvate. Biochem
Med Metab Biol 1986;36:141-50.
171. Rofe AM, James HM, Bais R,
Edwards JB, Conyers RA.The production
of (14C) oxalate during the metabolism
of (14C) carbohydrates in isolated rat
hepatocytes. Aust J Exp Biol Med Sci
1980;58:103-16.
172. Rowsell EV, Al-Tai AH, Carnie
JA. Liver L-serine-pyruvate aminotrans-
ferase activity in different animal spe-
cies. Biochem J 1972;127:27P.
173. Rumsby G. Experience in prenatal
diagnosis of primary hyperoxaluria type
1. J Nephrol 1998;11 Suppl 1:13-14.
174. Rumsby G, Cregeen DP.
Identification and expression of a cDNA
CHAPTER 01
page 44
VAN WOERDEN 5/19/08 8:53 AM Pagina 44

for human hydroxypyruvate/glyoxylate
reductase. Biochim Biophys Acta
1999;1446:383-88.
175. Rumsby G, Weir T, Samuell CT.
A semiautomated alanine:glyoxylate
aminotransferase assay for the tissue
diagnosis of primary hyperoxaluria
type 1. Ann Clin Biochem 1997;
34:400-04.
176. Saborio P, Scheinman JI.
Transplantation for primary hyperoxa-
luria in the United States. Kidney Int
1999;56:1094-100.
177. Salido EC, Li XM, Lu Y, Wang X,
Santana A, Roy-Chowdhury N et al.
Alanine-glyoxylate aminotransferase-
deficient mice, a model for primary
hyperoxaluria that responds to adeno-
viral gene transfer. Proc Natl Acad Sci
USA 2006;103:18249-53.
178. Santana A, Salido E, Torres A,
Shapiro LJ. Primary hyperoxaluria type
1 in the Canary Islands: A conforma-
tional disease due to I244T mutation in
the P11L-containing alanine:glyoxylate
aminotransferase. Proc Natl Acad Sci
USA 2003;7277-82.
179. Sarica K, Erturhan S, Yurtseven
C, Yagci F. Effect of potassium citrate
therapy on stone recurrence and
regrowth after extracorporeal shoc-
kwave lithotripsy in children.
J Endourol 2006;20:875-79.
180. Sawaki S, Yamada K. Glyoxylate
reductase activity of lactate dehydro-
genase. J Vitaminol (Kyoto) 1965;
11:294-96.
181. Schepers MS, Van Ballegooijen
ES, Bangma CH, Verkoelen CF. Oxalate
is toxic to renal tubular cells only at
supraphysiologic concentrations.
Kidney Int 2005;68:1660-69.
182. Schmidt KH, Hagmaier V, Hornig
DH, Vuilleumier JP, Rutishauser G.
Urinary oxalate excretion after large
intakes of ascorbic acid in man.
Am J Clin Nutr 1981;34:305-11.
183. Sidhu H, Hoppe B, Hesse A,
Tenbrock K, Bromme S, Rietschel E,
Peck AB. Absence of Oxalobacter formi-
genes in cystic fibrosis patients: a risk
factor for hyperoxaluria.
Lancet 1998;352:1026-29.
184. Smith LH, Fromm H, Hofmann
AF. Acquired hyperoxaluria, nephro-
lithiasis, and intestinal disease.
Description of a syndrome. N Engl J
Med 1972;286:1371-75.
185. Smith LH, Jr., Williams HE.
Treatment of primary hyperoxaluria.
Mod Treat 1967;4:522-30.
186. Soygur T, Akbay A, Kupeli S.
Effect of potassium citrate therapy
on stone recurrence and residual frag-
ments after shockwave lithotripsy in
lower caliceal calcium oxalate uro-lithi-
asis: a randomized controlled trial.
J Endourol 2002;16:149-52.
187. Stauffer JQ, Humphreys MH,
Weir GJ. Acquired hyperoxaluria with
regional enteritis after ileal resection.
Role of dietary oxalate.
Ann Intern Med 1973;79:383-91.
188. Thompson JS, Richardson KE.
Isolation and characterization of an L-
alanine: glyoxylate aminotransferase
from human liver. J Biol Chem
1967;242:3614-19.
CHAPTER 01
page 45
VAN WOERDEN 5/19/08 8:53 AM Pagina 45

189. Tomson CR, Channon SM,
Parkinson IS, Morley AR, Lennard TW,
Parrott NR, Laker MF. Plasma oxalate
concentration and secondary oxalosis
in patients with chronic renal failure.
J Clin Pathol 1988;41:1107-13.
190. Toussaint C. Pyridoxine-respon-
sive PH1: treatment. J Nephrol
1998;11 Suppl 1:49-50.
191. Traxer O, Huet B, Poindexter J,
Pak CY, Pearle MS. Effect of ascorbic
acid consumption on urinary stone risk
factors. J Urol 2003;170:397-401.
192. Tsao CS, Salimi SL. Effect of
large intake of ascorbic acid on urina-
ry and plasma oxalic acid levels.
Int J Vitam Nutr Res 1984;54:245-49.
193. Van Acker KJ, Eyskens FJ,
Espeel MF, Wanders RJ, Dekker C,
Kerckaert IO, Roels F. Hyperoxaluria
with hyperglycoluria not due to
alanine:glyoxylate aminotransferase
defect: a novel type of primary hyper-
oxaluria. Kidney Int 1996;50:1747-52.
194. van Gastel C, Dorhout Mees EJ,
Koten JW, de Minjer A. 2 patients with
primary oxalosis. Ned Tijdschr
Geneeskd 1965;109:832-33.
195. Verhulst A, Asselman M, Persy
VP, Schepers MS, Helbert MF, Verkoelen
CF, De Broe ME. Crystal retention capa-
city of cells in the human nephron: invol-
vement of CD44 and its ligands hyaluro-
nic acid and osteopontin in the transition
of a crystal binding- into a nonadherent
epithelium. J Am Soc Nephrol 2003;
14:107-15.
196. Verkoelen CF, Van Der Boom
BG, Houtsmuller AB, Schroder FH,
Romijn JC. Increased calcium oxalate
monohydrate crystal binding to injured
renal tubular epithelial cells in culture.
Am J Physiol 1998;274:F958-F965.
197. Verkoelen CF, Van Der Boom
BG, Romijn JC. Identification of hyalu-
ronan as a crystal-binding molecule at
the surface of migrating and prolifera-
ting MDCK cells. Kidney Int
2000;58:1045-54.
198. von Schnakenburg C, Byrd DJ,
Latta K, Reusz GS, Graf D, Brodehl J.
Determination of oxalate excretion in
spot urines of healthy children by ion
chromatography. Eur J Clin Chem Clin
Biochem 1994;32:27-29.
199. von Schnakenburg C, Hulton
SA, Milford DV, Roper HP, Rumsby G.
Variable presentation of primary
hyperoxaluria type 1 in 2 patients
homozygous for a novel combined
deletion and insertion mutation in
exon 8 of the AGXT gene. Nephron
1998;78:485-88.
200. von Schnakenburg C, Rumsby G.
Identification of new mutations in
primary hyperoxaluria type 1 (PH1).
J Nephrol 1998;11 Suppl 1:15-7.
201. von Schnakenburg C, Rumsby G.
Primary hyperoxaluria type 1: a
cluster of new mutations in exon 7
of the AGXT gene. J Med Genet 1997;
34:489-92.
202. Wanders RJ. Metabolic and
molecular basis of peroxisomal
disorders: a review. Am J Med Genet
A 2004;126:355-75.
203. Wanders RJ, van Roermund CW,
Jurriaans S, Schutgens RB, Tager JM,
CHAPTER 01
page 46
VAN WOERDEN 5/19/08 8:53 AM Pagina 46

van den BH et al. Diversity in residual
alanine glyoxylate aminotransferase
activity in hyperoxaluria type I: corre-
lation with pyridoxine responsiveness.
J Inherit Metab Dis 1988;
11 Suppl 2:208-11.
204. Wanders RJ, van Roermund CW,
Westra R, Schutgens RB, van der Ende
MA, Tager JM et al. Alanine glyoxylate
aminotransferase and the urinary
excretion of oxalate and glycollate in
hyperoxaluria type I and the Zellweger
syndrome. Clin Chim Acta 1987;
165:311-19.
205. Wandzilak TR, D'Andre SD,
Davis PA, Williams HE. Effect of high
dose vitamin C on urinary oxalate
levels. J Urol 1994;151:834-37.
206. Wandzilak TR, Hagen LE,
Hughes H, Sutton RA, Smith LH,
Williams HE. Quantitation of glycolate
in urine by ion-chromatography.
Kidney Int 1991;39:765-70.
207. Webster KE, Ferree PM, Holmes
RP, Cramer SD. Identification of mis-
sense, nonsense, and deletion muta-
tions in the GRHPR gene in patients
with primary hyperoxaluria type II
(PH2). Hum Genet 2000;107:176-85.
208. Williams HE, Smith LH, Jr.
L-glyceric aciduria. A new genetic
variant of primary hyperoxaluria.
N Engl J Med 1968;278:233-38.
209. Williams HE, Wandzilak TR.
Oxalate synthesis, transport and the
hyperoxaluric syndromes.
J Urol 1989;141:742-49.
210. Wilson DA, Wenzl JE, Altshuler
GP. Ultrasound demonstration of dif-
fuse cortical nephrocalcinosis in a case
of primary hyperoxaluria. AJR Am J
Roentgenol 1979;132:659-61.
211. Wilson DM, Liedtke RR.
Modified enzyme-based colorimetric
assay of urinary and plasma oxalate
with improved sensitivity and no
ascorbate interference: reference
values and sample handling procedures.
Clin Chem 1991;37:1229-35.
212. Wohl H. Nephrocalcinosis.
J Pediatr 1942;21:382-85.
213. Wolthers BG, Hayer M. The
determination of oxalic acid in plasma
and urine by means of capillary gas
chromatography. Clin Chim Acta
1982;120:87-102.
214. Wolthers BG, Meijer S, Tepper T,
Hayer M, Elzinga H. The determination
of oxalate in haemodialysate and
plasma: a means to detect and study
'hyperoxaluria' in haemodialysed
patients. Clin Sci 1986;71:41-47.
215. Wong PN, Law EL, Tong GM,
Mak SK, Lo KY, Wong AK. Diagnosis
of primary hyperoxaluria type 1 by
determination of peritoneal dialysate
glycolic acid using standard organic-
acids analysis method.
Perit Dial Int 2003;23:S210-S213.
216. Worcester EM, Nakagawa Y,
Bushinsky DA, Coe FL. Evidence that
serum calcium oxalate supersaturation
is a consequence of oxalate retention in
patients with chronic renal failure.
J Clin Invest 1986;77:1888-96.
217. Yanagawa M, Maeda-Nakai E,
Yamakawa K, Yamamoto I, Kawamura
J, Tada S, Ichiyama A. The formation
CHAPTER 01
page 47
VAN WOERDEN 5/19/08 8:53 AM Pagina 47

of oxalate from glycolate in rat and
human liver. Biochim Biophys Acta
1990;1036:24-33.
218. Yuen YP, Lai CK, Tong GM,
Wong PN, Wong FK, Mak SK et al.
Novel mutations of the AGXT gene
causing primary hyperoxaluria
type 1. J Nephrol 2004;17:436-40.
219. Zeltich I, Ochoa S. Oxidation
and reduction of glycolic and
glyoxylic acids in plants. I.
Glycolic and oxidase.
J Biol Chem 1953;201:707-18.
220. Zerwekh JE, Odvina CV,
Wuermser LA, Pak CY. Reduction of
renal stone risk by potassium-
magnesium citrate during 5 weeks of
bed rest. J Urol 2007;177:2179-84.
221. Zhang X, Roe SM, Hou Y,
Bartlam M, Rao Z, Pearl LH,
Danpure CJ. Crystal structure
of alanine:glyoxylate amino-
transferase and the relationship bet-
ween genotype and enzymatic
phenotype in primary hyperoxaluria
type 1. J Mol Biol 2003;331:643-52.
222. Zwaveling JH, Sangster B, van
DA. Ethylene glycol poisoning. Ned
Tijdschr Geneeskd 1988;132:485-89.
CHAPTER 01
page 48
VAN WOERDEN 5/19/08 8:53 AM Pagina 48

CHAPTER 02 Postponing urine acidification for 24 hours doesnot change the oxalate concentration
Christiaan S van Woerden, Hidde H Huidekoper, Jaap W Groothoff, Frits A Wijburg and Marinus Duran
Clinica Chimica Acta 2007;
384:184-185
INTRODUCTION
Oxalate is produced in excess in patients with primary hyperoxaluriaand excreted into the urine. An accurate determination of urinary oxa-late is indispensable for the diagnosis and therapeutic follow-up ofpatients with primary hyperoxaluria (1). For this purpose, urine collecti-on is usually performed in acidified containers, to avoid false negativeresults due to potential precipitation of calcium oxalate. Although theeffect of long-term urine storage at different conditions on oxalate con-centration has been studied (2,3), no studies have addressed the need foracidification at voiding for the initial diagnosis of hyperoxaluria.Reliable results might also be obtained by urine acidification upon arri-val in the laboratory. Such a procedure will abolish the risk of acid burnsby accidental spilling or vapour inhalation of concentrated hydrochloricacid for patients or their caretakers.
METHODS
In the present study we investigated the effects of delayed acidificationof urine upon its collection on the analysis of urinary oxalate. The studywas conducted in four patients with primary hyperoxaluria type 1, ofwhom one received hemodialysis (PH1 dial), and in three control sub-jects, of whom one received peritoneal dialysis (Non-PH1 dial). All main-tained a low oxalate diet starting three days prior to the first urine col-lection. The subjects collected morning urine samples after overnightfasting on four to eight non-consecutive days. Immediately after voi-ding, the urine was split into two aliquots. One-half was put in a drycontainer and the other half in a container containing 15 ml 25% hydro-chloric acid and gently shaken. Both containers were taken to the labo-ratory within 4 hours after urine collection. The non-acidified urine wasagain divided into two portions. One was acidified to pH1 and the otherwas acidified to pH1 only after a storage period of 24 hours at 4ºC.
Following acidification and prior to analysis, the urine samples wereshaken at room temperature. Urinary oxalate concentration wasdetermined by ion chromatography (Dionex-DX 300). Calcium, magne-
CHAPTER 02
page 49
VAN WOERDEN 5/19/08 8:53 AM Pagina 49

sium and citrate concentrations were measured at the same time (spec-trophotometric, colorimetric) for calculation of the urine super satura-tion, in order to observe stability of ion concentrations over time (4).
RESULTS
The Wilcoxon signed-ranks test assessed differences in sample concen-trations. Statistical significance was set at P < 0.05 for all comparisons. The results showed that urinary oxalate concentrations, expressed asmmol/mmol creatinine, were not significantly different between theurine samples acidified immediately after voiding and the urine samp-les acidified after either 4 or 24 hours (Wilcoxon rank test, p = 0.609for 4 hours and p = 0.334 for 24 hours, FIGURE 02.1). Urinary calciumconcentration was below the upper range of reference value in all sub-jects. Calculated median urine super saturation was 16 (range (6-36)mmol/l for patients and 3 (range 2-5) mmol/l for controls.
DISCUSSION
Postponed acidification of urine samples did not change the calculatedsuper saturation. Apparently, there is a higher concentration of ions inthe urine of patients with hyperoxaluria, which poses them at risk forurinary stone formation. However, this did not influence the determi-nation of urinary oxalate, even if acidification was delayed for 24 hours.These results support postponed urine acidification at the laboratory.
Urinary oxalate (mean ± SD) in all subjects with immediate acidification, acidification 4 hours after collection and acidification 24 hours after collection.
FIGURE 02.1
CHAPTER 02
page 50
VAN WOERDEN 5/19/08 8:53 AM Pagina 50

No significant intra-individual day-to-day variation in urinary oxalateconcentration, corrected for creatinine concentration, was measured inthe urine of PH1 patients A and B, nor in the control subjects (non-PH1dial, control A and B). This is in agreement with observations made byZarembski et al. (5). However, a considerable intra-individual variationwas observed for the urine samples of the PH1 patient on hemodialy-sis and in patient C (FIGURE 02.1). The variation in the PH1 patient ondialysis may be explained by oxalate mobilization from the extensiveaccumulation of oxalate in tissues, which may vary depending on thetime intervals between the dialysis sessions. The variation of oxalateexcretion in patient C may be the result of varying dietary intake.Nevertheless, the observed variations would not jeopardize the dia-gnosis of PH1, as even the lowest level of oxalate excretion in this sub-ject was twice the upper limit of reference range. However, these vari-ations may obscure the response to therapeutic interventions aimed atreducing oxalate production. More sensitive methods to detect changesin endogenous oxalate production are therefore warranted. In conclu-sion, we demonstrated that collected urine could be stored at 4ºC in ahome setting without acidification for a period up to at least 24 hours,without resulting in variations in oxalate concentration that wouldcumber a diagnostic screening of primary hyperoxaluria.
REFERENCES
CHAPTER 02
page 51
1. Danpure CJ. Primary
Hyperoxaluria. In: Scriver CR,
Beaudet AL, Sly WS, Valle D, eds.
The Metabolic and Molecular Bases
of Inherited Disease. New York:
McGraw-Hill, 2001:3323-67.
2. Mazzachi BC, Teubner JK,
Ryall RL. Factors affecting
measurement of urinary oxalate.
Clin Chem 1984;30:1339-43.
3. Ng RH, Menon M, Ladenson JH.
Collection and handling of
24-hour urine specimens for
measurement of analytes
related to renal calculi.
Clin Chem 1984;30:467-71.
4. Ogawa Y, Machida N, Ogawa T,
Oda M, Hokama S, Chinen Y et al.
Calcium oxalate saturation in dialysis
patients with and without primary
hyperoxaluria. Urol Res 2006;34:12-16.
5. Zarembski PM,
Hodgkinson A. Some factors
influencing the urinary excretion
of oxalic acid in man.
Clin Chim Acta 1969;25:1-10.
VAN WOERDEN 5/19/08 8:53 AM Pagina 51

CHAPTER 02
page 52
VAN WOERDEN 5/19/08 8:53 AM Pagina 52

CHAPTER 03 Primary hyperoxaluria type 1 in The Netherlands: prevalence and outcome
Christiaan S van Woerden, Jaap W Groothoff, Ronald JA Wanders, Jean-Claude Davin and Frits A Wijburg
Nephrology Dialysis Transplantation 2003;
18: 273-279
Background. Primary hyperoxaluria type 1 (PH1) is a phenotypicallyheterogeneous disease. To date the relationship between biochemicalparameters and outcome is unclear. We therefore undertook a nationalcohort study on biochemical and clinical parameters and outcome inPH1.
Methods. Review of medical charts of all Dutch PH1 patients, whowere identified by sending questionnaires to all Dutch nephrologistsfor children and adults.
Results. Fifty-seven patients were identified. The prevalence andincidence rates were 2.9/106 and 0.15/106/year, respectively. Medianage at diagnosis was 7.3 years (range 0-57). Seventeen (30%) patientswere older than 18 years at time of diagnosis, of whom 10 (59%) presented with end-stage renal disease (ESRD), in contrast to only nine(23%) of those aged under 18 years. Median age at initial symptoms was6.0 years (range 0-50). In four of nine patients with infantile PH1, normalrenal function was preserved after a median follow-up of 7.7 years(range 0.1-16). Progression to renal insufficiency was associated withthe presence of nephrocalcinosis, as assessed by ultrasound (relativerisk=1.8; 95% CI, 1.0-3.4) and with pyridoxine-unresponsiveness (relative risk 2.2; 95% CI, 1.1-4.2) but not with age at presentation, theextent of hyperoxaluria, or AGT activity. No apparent nephrocalcinosiswas found in five of the 19 patients who presented with ESRD.
Conclusions. Although more than one-half of the PH1 patients havesymptoms under the age of 10 years, PH1 can present at any age. In adults, PH1 presents predominantly with ESRD, which may be due tomisinterpretation of early symptoms. Although nephrocalcinosis iscorrelated with development of renal insufficiency, the latter can occureven in the absence of nephrocalcinosis. Pyridoxine sensitivity is asso-ciated with better outcome in PH1.
ABSTRACT
CHAPTER 03
page 53
VAN WOERDEN 5/19/08 8:53 AM Pagina 53

INTRODUCTION
Primary hyperoxaluria type 1 (PH1) is a rare autosomal recessive inbornerror of glyoxylate metabolism. It is characterized by a functional defectof the liver specific enzyme alanine:glyoxylate aminotransferase (AGT)which is localized in peroxisomes (1). PH1 is caused either by deficientAGT activity or by mistargeting of the enzyme to mitochondria insteadof peroxisomes. AGT detoxifies the metabolite glyoxylate to glycine,using pyridoxal-5-phosphate as a coenzyme. In the absence of functionalAGT, oxalate and glycolate are produced in excess, leading to hyper-oxaluria and hyperglycolic aciduria. The marked excess of oxalate leadsto the formation of insoluble calcium oxalate, resulting in crystalluria,renal stone formation and nephrocalcinosis. In addition to PH1, twoother types of primary hyperoxaluria have been described: primaryhyperoxaluria type 2 (PH2), which is caused by deficient glyoxylatereductase/D-glycerate dehydrogenase activity, leading to elevated levelsof oxalate and L-glycerate in the urine (2) and a type of primary hyper-oxaluria that has not been unravelled in terms of biochemical or molecularmechanism: unclassified or atypical PH (3). These other types exhibit thesame symptoms as in PH1, albeit somewhat less severe. PH1 shows considerable phenotypic, enzymatic and genotypic heterogeneity (4-7).
Some patients have no symptoms at all or suffer only from recurrenturolithiasis. Other patients develop a chronic renal insufficiency withsystemic oxalosis, characterized by oxalate depositions in multiple tissues, such as bone, retina and nerve tissue (8). Even in patients withapparent nephrocalcinosis, conservative treatment with hyper-hydration,citrate and pyridoxine can be successful (9,10).
Unfortunately, the outcome is poor in most patients. Approximately 50%of them have been reported to reach end-stage renal disease (ESRD) atthe age of 25 years (4,5,7). Patients with ESRD require intensive dialysissessions in order to delay systemic oxalate deposition (11). Renal graftsmay fail even after a combined liver-kidney transplantation, due tosystemic oxalosis (12).
Currently, three clinical subgroups are distinguished within PH1. First,a rare infantile form with early renal insufficiency. Secondly, a rare late-onset form with occasional stone passage in late adulthood and with agood prognosis with respect to renal function. Thirdly, the most commonform, with recurrent urolithiasis or nephrocalcinosis and often progressive renal insufficiency (13). However, the relationship betweenbiochemical and clinical parameters on the one hand and outcome onthe other remains unclear. Therefore we undertook a multi-centreretrospective study on Dutch PH1 patients to delineate the clinical andbiochemical spectrum of PH1, its therapy and its outcome.
CHAPTER 03
page 54
VAN WOERDEN 5/19/08 8:53 AM Pagina 54

SUBJECTS AND METHODS
The cohort formation was based on two sources. The database of thenational Dutch Registry of patients on renal replacement therapy (RENINE,Rotterdam, The Netherlands). The registry was founded in 1985. Allpatients on dialysis are included in this database, as registration isobligatory for reimbursement of renal replacement therapy. All physicians of the Dutch Society of Paediatric Nephrology and theDutch Society of Nephrology received a questionnaire and were personallyapproached by CSvW or JWG if they did not respond.
The questionnaires provided individual data about the patients: age,sex, age at first symptoms, age at biochemical diagnosis, symptoms atdiagnosis, diagnostic procedures, duration of follow-up, therapeuticstrategies and outcome.
All known Dutch PH1 patients who were investigated and/or treated bya nephrologist were included. Prevalence rate was calculated for themost recent follow-up.
Patients were diagnosed as type 1 PH if either deficient AGT activity orthe combination of hyperoxaluria and hyperglycolic aciduria wasdemonstrated (ratios in a 24 hour collection of urine exceeding 54mmol/mol creatinine for oxalate and 140 mmol/mol creatinine for gly-colate, as determined in our laboratory). Urinary oxalate and glycolatereference values for small children were derived from data of Reusz etal. (14). For patients in whom urinary oxalate could not be measuredbecause of anuria, highly elevated plasma oxalate levels of more than20 times the upper limit of the reference range were considered to becaused by PH1 and not by renal insufficiency itself (15). Patients in whomonly hyperoxaluria was measured were considered to have PH1 if thiswas demonstrated in other family members. If these firm diagnosticgrounds were not present, we decided to include patients with the fol-lowing highly suspicious circumstantial evidence for PH1: (i) signifi-cant response to pyridoxine therapy (dosage 400-1200 mg/day), defin-ed by a decline of urinary or plasma oxalate levels of more than 30%upon pyridoxine therapy (16); (ii) severe systemic oxalosis. Primaryhyperoxaluria type 2 was diagnosed on the bases of elevated urinary levels of oxalate and L-glycerate as well as deficientactivities of D-glycerate dehydrogenase and glyoxylate reductase (2).Hyperoxaluric patients who did not fit in any of these categories weregrouped as the atypical type of PH (3). Nephrocalcinosis was clinicallyassessed, based on sonographic or radiological examination. Prevalenceand incidence rates were calculated using national demographic dataprovided by the Health and Welfare Department of StatisticsNetherlands. Infantile PH1 was defined as PH1 becoming symptomatic
Sources
Questionnaire
Population
Analysis
CHAPTER 03
page 55
VAN WOERDEN 5/19/08 8:53 AM Pagina 55

before the age of 1 year. Follow-up was defined as the period betweenpresentation of initial symptoms or date of diagnosis if no symptomswere present and the date of investigation or date of death of a patient.Renal function was estimated by the Cockroft formula in adults, andthe Schwartz formula in children using plasma creatinine values(17,18). Renal insufficiency was defined as a creatinine-clearance ofless than 60 ml/min/1.73 m2. End-stage renal disease (ESRD) was defined as a creatinine-clearance of less than 10 ml/min/1.73 m2.
Five different parameters in relation to outcome were investigated: age at initial symptoms, nephrocalcinosis at diagnosis, level of urinary oxalate at the time of diagnosis, AGT activity and pyridoxine responsive-ness (19). For analysis, dichotomous variables were composed according to supposed clinical relevance and related to outcome. For urinary oxalate excretion, the median level of the entire cohort was calculated using all urinary oxalate excretion levels in individualpatients measured at the time of diagnosis. Patients with oxalate levelsexceeding the median level were compared to those with urinary oxalate levels below the median level with respect to outcome. In thesame way, patients with AGT activity lower than 15% of reference activity (normal range 72-166, median 97 nmol/min.mg) were comparedto those with AGT activity above 15% (20). Calculation of reference activity was based on measurements of AGT activities in control liversin our own laboratory. We considered pyridoxine therapy successful ifurinary oxalate persistently declined by more than 30% (16). Outcomewas dichotomized, creating a group of patients with renal insufficiency,and a group without renal insufficiency. Relative risks were calculatedfor potential prognostic factors. The overall renal survival was estimated as a function of age by theKaplan-Meier method, with patient follow-up censored at renal insuf-ficiency. Statistical package used was SPSS 8.0, 1998 and CIA Version 1.0.
RESULTS
We obtained a 100% response from all 189 physicians. Fifty-seven PH1patients from 44 families were identified of whom 15 had been diagnosed by family screening. Consanguinity was reported in fivefamilies. Twenty-one of 57 patients had a positive family history forrecurrent urolithiasis. Male/female ratio was 27/30. The calculated pre-valence rate was 2.9/106 inhabitants and the incidence rate was0.15/106 per year. The median follow-up time was 12.6 years (range 1-26)in the 15 patients (26%) who were found by family screening, and 11.3years (range 0-60) in the other 42 patients. Five patients had a different type of primary hyperoxaluria. One patient was diagnosedwith PH2 and four presented with an atypical disorder in oxalate metabolism resulting in primary hyperoxaluria that could not be
The cohort
CHAPTER 03
page 56
VAN WOERDEN 5/19/08 8:53 AM Pagina 56

classified as either PH1 or PH2. As the majority presented with PH1, wedecided to analyse only the results of the PH1 patients in our study.
The median age at diagnosis was 7.3 years (range 0-57). Of 57 patients,17 (30%) were diagnosed after the age of 18. The diagnosis was established on firm grounds in 49. In 44 patients,the diagnosis was based on either AGT deficiency (29 patients), orhyperglycolic hyperoxaluria (15 patients). In four patients it was basedon elevated urinary oxalate levels and PH1 in their families and in onepatient on the basis of highly elevated plasma oxalate. In addition, another eight patients were included, two of them on the basis of pyridoxine responsive hyperoxaluria and six on severe systemic oxalosis.
Median age at initial symptoms was 6.0 years (range 0-50). In 10patients (18%), the onset of symptoms was at adult age. Symptoms andfindings at diagnosis are given in TABLE 03.1. Of the 15 patients foundby family screening, five were asymptomatic at the time of diagnosis.All other patients had renal symptoms at the time of diagnosis. ESRDwas present in 10 out of 17 (59%) patients of those diagnosed at adultage versus 9 out of 40 (23%) of the pediatric patients. Of all 10 adultpatients with ESRD at diagnosis, four presented without evident nephro-calcinosis. Renal biopsies in these four patients showed interstitialnephritis with calcium oxalate crystals in destroyed tubules.Nephrocalcinosis was present in eight of nine paediatric patients withESRD at onset. In retrospect, of the patients in whom PH1 was diagnosedonly at the time of ESRD, all nine paediatric patients had suffered fromurolithiasis or failure to thrive for 0.2 years (range 0.0-10.7) and eightadult patients diagnosed had reported urolithiasis for 2.5 years (range0.0-35.8). Two adult patients had neither urolithiasis nor any othersymptoms that could be related to PH1 at the time they developedESRD.
Diagnosis
Initial symptoms
CHAPTER 03
page 57
VAN WOERDEN 5/19/08 8:53 AM Pagina 57

Symptoms and findings of PH1 patients at diagnosis
No. of patients (%) Median age, years (range)
57 (100) 7.3 (0.1-57.3)
Renal insufficiency 27/57 (47) 10.0 (0.1-50.8)
● without nephrocalcinosis 3/27 (11) 28.0 (0.1-50.8)
or urolithiasis
● with nephrocalcinosis only 9/27 (33) 0.4 (0.1-10.0)
● with urolithiasis only 4/27 (15) 23.7 (12.0-40.7)
● with both nephrocalcinosis 11/27 (41) 18.0 (3.0-48.8)
and urolithiasis
● ESRD 19/27 (70) 18.0 (0.3-50.8)
Preserved renal function 30/57 (53) 7.0 (0.2-57.3)
● no symptoms 5/30 (17) 2.0 (0.2-57.3)
● with nephrocalcinosis 5/30 (17) 7.0 (4.0-11.8)
● with urolithiasis 12/30 (40) 6.9 (0.5-38.0)
● with both nephrocalcinosis 8/30 (26) 7.6 (5.0-30.0)
and urolithiasis
Systemic symptoms
● Bone disease 12/57 (21)
● Retinopathy 5/57 (9)
● Failure to thrive 6/57 (11)
Other symptoms (neuropathy, 20/57 (35)
malaise, chronic diarrhoea)
Nine patients (16%) were symptomatic during infancy. Five patients hadsymptoms due to renal insufficiency (failure to thrive) and one hadurolithiasis. Three patients were found by family screening. Two ofthem had a reduced renal function and were diagnosed shortly afterbirth by screening, because PH1 had been found in an older sibling whodied of PH1. The third patient found by screening had been known tohave haematuria and nephrocalcinosis since 3 months of age.
Time between initial symptoms and renal insufficiencyThere was no relationship between age at onset of symptoms and ageat start of dialysis.
Of the 27 patients with renal insufficiency at presentation, 19 hadESRD. Of the other eight patients with renal insufficiency, four developedESRD. In two patients, renal function has remained stable throughoutthe follow-up period, being 4 years. In two patients, who were followedup for 7.5 and 13 years, respectively, renal function improved to normal values. Of 30 patients with a normal renal function at first examination, eight developed renal insufficiency leading to ESRD infive. Overall, 33 of 57 patients developed renal insufficiency, of whom
TABLE 03.1
Infantile PH1
Outcome
CHAPTER 03
page 58
VAN WOERDEN 5/19/08 8:53 AM Pagina 58

28 had ESRD at the end of the study. Of these 33 with renal insufficiency,24 (73%) demonstrated nephrocalcinosis at diagnosis (TABLE 03.2).FIGURE 03.1 shows the Kaplan-Meier survival curve of renal function inrelation to age, with end-point at renal insufficiency. Fifty per cent ofthe patients had reached renal insufficiency at a median age of 30.0years (range 22.2-37.7). Eleven patients (19%) died as a consequence ofPH1 or its therapy at a median age of 18.0 years (range 0-55). Renalinsufficiency occurred in four (27%) of the 15 patients found by familyscreening. Of 17 isolated kidney transplantations, performed at a medianage of 31.2 years (range 11.1-55.4), eight were successful. The mediansurvival of the kidney grafts was 2.7 years (range 0-26). Transplant failure was always caused by deposition of calcium oxalate. The onlypatient who received a liver transplant without a renal graft died fromcomplications of the liver graft. Of three combined liver/kidney trans-plantations, performed at the ages of 1.7, 3.9 and 16.6 years, respectively,one was successful, one needed a second liver graft and one a secondrenal graft.
Outcome in relation to initial symptoms (%)
Initial No. of Renal ESRD Death
symptoms patients insufficiency
● Nephrocalcinosis 14 (25) 9/14 (64) 7/14 (50) 4/14 (29)
● Nephrocalcinosis 19 (33) 15/19 (79) 13/19 (68) 5/19 (26)
with urolithiasis
● Urolithiasis 16 (28) 6/16 (38) 6/16 (38) 1/16 (6)
● No nephrocalcinosis, 8 (14) 3/8 (38) 2/8 (25) 1/8 (13)
no urolithiasis
Total number (%) 57 (100) 33 (58) 28 (49) 11 (19)
TABLE 03.2
FIGURE 03.1
Cumulative
survival of renal
function in
relation to age
with patient
follow-up
censored at renal
insufficiency
(creatinine
clearance less
than 60 ml/min/
1.73 m2).
Age years
VAN WOERDEN 5/19/08 8:53 AM Pagina 59

Median follow-up was 7.7 years (range 0.1-16) in nine patients. Fivedeveloped ESRD. The three patients who were found by screening showedcomplete recovery from initial symptoms, improvement of renal functionand/or decrease of nephrocalcinosis upon conservative treatment. Allthree were sensitive to pyridoxine therapy. The two index patients haddeveloped ESRD and died before the age of 6 months. One other patientwith a follow-up of 10 months, presenting with infections and urolithi-asis, was pyridoxine sensitive and preserved renal function.
Relative risks were calculated for different parameters (TABLE 03.3).One patient had a full response on pyridoxine therapy (i.e. normaliza-tion of urinary oxalate levels) and three patients had a urinary oxalate reduction of more than 80%. Eight of 24 (33%) patients who were res-ponsive to pyridoxine developed renal insufficiency, resulting in ESRDin five of them. Of the 11 patients who were pyridoxine-resistant, eight(73%) developed renal insufficiency, resulting in ESRD in six of them.
Calculated relative risks for different parameters
Parameter No. of patientsa Relative risk for (95% CI)b
renal insufficiency
● Urinary oxalate above 18/37 1.1 (0.5-2.2)
the median level
● AGT < 15% of reference value 19/29 0.45 (0.3-1.8)
● Pyridoxine non-responsive 11/35 2.2 (1.1-4.2)
● Nephrocalcinosis 33/57 1.8 (1.0-3.4)
a Number of patients/number of patients for whom information
could be obtainedb 95% CI = 95% confidence interval
DISCUSSION
In this study we performed a thorough search in The Netherlands forall PH1 patients by using data from multiple sources, includingpatients on renal replacement therapy as well as patients with preservedrenal function. Despite the limitations of such a retrospective study, wefeel that we acquired a complete overview of Dutch PH1 patients: wewere able to contact all nephrologists nationwide who are in charge oftreatment of PH1 patients. Probably due to the methods used forpatient retrieval, the prevalence rate we found for PH1 in TheNetherlands (2.9 per 106) is higher than those reported by Cochat et al.(1995) (5) in France (1.05 per 106) and by Kopp and Leumann (1995) inSwitzerland (2 per 106) (21). Since the calculated incidence for PH1 in
Outcome ofinfantile PH1
Determinantsof outcome
TABLE 03.3
CHAPTER 03
page 60
VAN WOERDEN 5/19/08 8:53 AM Pagina 60

The Netherlands was not higher than reported in those other Europeancountries, the higher prevalence has to be explained by the longer periodfor patient retrieval we used. Nevertheless, we believe that the obser-ved prevalence rate is still an underestimation of the true prevalence,since the heterogeneous phenotype and the vague initial symptomscan easily result in a delay of screening for PH1 or no screening at all.For instance, 26% of the patients in our study were found by screeningin families with one or more known PH1 patients, and 66% of them already had renal symptoms that were at that time not linked to PH1:urolithiasis, haematuria and recurrent urinary-tract infections. The lowprevalence of PH2 as observed in our study may also be explained bythe mild symptoms in this disorder, resulting in a failure to diagnosethe underlying metabolic disease.
Symptoms in the Dutch PH1 patients, whether presenting at infantile,pediatric or adult ages, are comparable to those described in previousstudies (4,5,7,21,22). While most infantile patients present with a-specific symptoms such as failure to thrive, older patients have symp-toms that are often related to the urinary tract. In our study, ESRD waspresent in 10 (59%) of 17 patients diagnosed at adult age versus in nine(23%) of 40 patients presenting at pediatric age. The high prevalence ofESRD in adults, and the fact that in this study ESRD is reported to occureven in the absence of a history of urinary stones is remarkable. Thisseems to contrast with the presumption that in adults PH1 presents predominantly with a mild phenotype. However, it may wellbe that in these patients mild signs and symptoms prior to the deve-lopment of ESRD were not adequately understood, and that thereforethe opportunity for a timely diagnosis was missed. This stresses theimportance of a search for hyperoxaluria in all patients with otherwiseunexplained mild renal symptoms. In view of our finding that ESRDmay occur as the first presenting sign of PH1, even in the absence ofreported previous symptoms like urolithiasis, we believe that screeningfor PH1 should be performed in all patients with ESRD of unknown origin.
In our study, progression to renal insufficiency was not statisticallyassociated with the level of urinary oxalate or with AGT activity (TABLE
03.3), which is in agreement with other observations (6). Apparently,the in vitro activity of the AGT enzyme does not adequately predict the in vivo metabolism of glyoxylate. In contrast, progression to renalinsufficiency was statistically associated with the presence of nephrocal-cinosis, detected by ultrasound, and with non-responsiveness to pyri-doxine (TABLE 03.3). In this study, we assessed the effectiveness of pyridoxine on the reduction of urinary oxalate levels in PH1. Accordingto the suggestion of Latta to define pyridoxine responsiveness by a 30%reduction in urinary oxalate levels (16,23), 69% of the Dutch PH1 cohortis responsive to pyridoxine treatment. Our results demonstrate that
CHAPTER 03
page 61
VAN WOERDEN 5/19/08 8:53 AM Pagina 61

response to pyridoxine therapy predicts outcome of renal function(TABLE 03.3). Therefore, a 30% decrease of urinary oxalate upon pyridoxi-ne administration is a clinically relevant value to evaluate this therapyin individual PH1 patients. Furthermore, early recognition of PH1 asthe cause of renal insufficiency is of the utmost importance because pyridoxine may reverse the course of the renal disease, as demonstratedby our study. Good outcomes can be achieved by pyridoxine treatment,even in infantile cases. Three of nine infantile patients in our studyrecovered from severe symptoms present at the time of diagnosis afterthe start of pyridoxine and one other infantile patient preserved renalfunction upon pyridoxine administration. This effect of pyridoxine onthe course of renal insufficiency in infantile PH1 patients has only beenreported so far in exceptional cases (23).
Although progression to renal insufficiency was statistically associatedwith the presence of nephrocalcinosis, nephrocalcinosis was not foundby renal ultrasound in five of 19 patients presenting with ESRD.Interestingly, in four of those five patients, calcium oxalate depositionswere visible on kidney biopsy specimens. In one of these five patients,renal biopsy was not performed.
It is unlikely that in these patients nephrocalcinosis was missed onultrasound, as sonography appears to be a sensitive and reliablemethod for the detection of nephrocalcinosis (24). Apparently, calciumoxalate deposition as seen on renal biopsy can occur without nephro-calcinosis as detected by ultrasound. The role of oxalate in the destructionof renal parenchyma is uncertain. It has been generally assumed thatthe destruction of the renal parenchyma in PH1 is caused by the diffusedeposition of calcium oxalate in the kidneys, visible as nephro- calcinosis on ultrasound studies (25). Alternatively, it has been sug-gested that a high oxalate concentration can be toxic by enhancing theproduction of free radicals, thereby destroying renal tubular cells,resulting in renal insufficiency (26). Whatever the precise mechanismof renal destruction in PH1 may be, these findings clearly demonstratethat the absence of nephrocalcinosis as detected on renal ultrasoundstudies does not exclude PH1 and evolution to ESRD. Since the combination of nephrocalcinosis and urolithiasis in children is highlysuspicious for PH1 (27), we therefore recommend a diagnostic work upfor hyperoxaluria in all patients with unexplained chronic renal insufficiency or recurrent urinary tract symptoms at all ages.
One-third of the patients in this Dutch PH1-cohort had already developedESRD before PH1 was diagnosed. There are several explanations for thislate detection. First, metabolic assessment is not a routine procedure in patients with recurrent urinary tract symptoms. Secondly,the diagnostic procedure of PH1 can be cumbersome; even small
CHAPTER 03
page 62
VAN WOERDEN 5/19/08 8:53 AM Pagina 62

violations of the protocol of urine collection for oxalate measurementcan cause false-negative results and, as we have demonstrated in thispaper, progression to ESRD is possible without apparent nephro-calcinosis on renal ultrasound. Extensive family screening of patientswith demonstrated PH1 may reveal asymptomatic patients as well aspatients with renal disease not yet attributed to PH1. If adequate metabolic screening strategies are applied, early treatment of thesepatients is possible, which may prevent (further) loss of renal function.
We thank all the physicians nation-wide who agreed to provide detailedinformation on PH1 patients.
REFERENCES
CHAPTER 03
page 63
1. Danpure CJ, Jennings PR.
Peroxisomal alanine:glyoxylate amino-
transferase deficiency in primary
hyperoxaluria type I. FEBS Lett
1986;201:20-24.
2. Giafi CF, Rumsby G. Kinetic
analysis and tissue distribution of
human D-glycerate dehydrogenase/
glyoxylate reductase and its relevance
to the diagnosis of primary hyper-
oxaluria type 2. Ann Clin Biochem
1998;35:104-109.
3. Neuhaus TJ, Belzer T, Blau N,
Hoppe B, Sidhu H, Leumann E. Urinary
oxalate excretion in urolithiasis and
nephrocalcinosis. Arch Dis Child
2000;82:322-26.
4. Latta K, Brodehl J. Primary
hyperoxaluria type I. Eur J Pediatr
1990;149:518-22.
5. Cochat P, Deloraine A, Rotily M,
Olive F, Liponski I, Deries N.
Epidemiology of primary hyperoxaluria
type 1. Société de Néphrologie and the
Société de Néphrologie Pédiatrique.
Nephrol Dial Transplant 1995;10
Suppl 3-7.
6. Danpure CJ. Molecular and
clinical heterogeneity in primary
hyperoxaluria type 1. Am J Kidney
Dis 1991;17:366-69.
7. Milliner DS, Wilson DM,
Smith LH. Phenotypic expression
of primary hyperoxaluria:
Comparative features of types I
and II. Kidney International
2001;59:31-36.
8. Danpure CJ. Primary Hyper-
oxaluria. In: Scriver CR, Beaudet AL,
Sly WS, Valle D, eds.
The Metabolic and Molecular Bases
of Inherited Disease. New York:
McGraw-Hill, 2001:3326.
9. Milliner DS, Eickholt JT,
Bergstralh EJ, Wilson DM, Smith LH.
Results of long-term treatment with
orthophosphate and pyridoxine in
patients with primary hyperoxaluria.
N Engl J Med 1994;331:1553-58.
10. Leumann E, Hoppe B, Neuhaus
T, Blau N. Efficacy of oral citrate
administration in primary hyperoxaluria.
Nephrol Dial Transplant 1995;10
Suppl 8:14-16.
VAN WOERDEN 5/19/08 8:53 AM Pagina 63

11. Broyer M, Jouvet P, Niaudet P,
Daudon M, Revillon Y. Management of
oxalosis. Kidney Int Suppl 1996;53:93-98.
12. Cochat P, Gaulier JM, Koch
Nogueira PC, Feber J, Jamieson NV,
Rolland MO et al. Combined liver-kidney
transplantation in primary hyper-
oxaluria type 1. Eur J Pediatr 1999;158
Suppl 2:S75-S80.
13. Cochat P, Basmaison O. Current
approaches to the management of
primary hyperoxaluria. Arch Dis Child
2000;82:470-73.
14. Reusz GS, Dobos M, Byrd D,
Sallay P, Miltenyi M, Tulassay T.
Urinary calcium and oxalate excretion
in children. Pediatr Nephrol 1995;9:39-44.
15. Wolthers BG, Meijer S, Tepper T,
Hayer M, Elzinga H. The determination
of oxalate in haemodialysate and
plasma: a means to detect and study
'hyperoxaluria' in haemodialysed
patients. Clin Sci 1986;71:41-47.
16. Leumann E, Hoppe B. What is
new in primary hyperoxaluria? Nephrol
Dial Transplant 1999;14:2556-58.
17. Cockcroft DW, Gault MH.
Prediction of creatinine clearance
from serum creatinine.
Nephron 1976;16:31-41.
18. Schwartz GJ, Haycock GB,
Edelmann CM, Jr., Spitzer A. A simple
estimate of glomerular filtration rate in
children derived from body length and
plasma creatinine. Pediatrics
1976;58:259-63.
19. Horvath VAP, Wanders RJA.
Aminooxy acetic acid: a selective
inhibitor of alanine:glyoxylate amino-
transferase and its use in the diagnosis
of primary hypero-xaluria type I. Clin
Chim Acta 1995; 243:105-114.
20. Danpure CJ. Primary
Hyperoxa-luria. In: Scriver CR, Beaudet
AL, Sly WS, Valle D, eds. The Metabolic
and Molecular Bases of Inherited
Disease. New York: McGraw-Hill,
2001:3323-67.
21. Kopp N, Leumann E. Changing
pattern of primary hyperoxaluria in
Switzerland. Nephrol Dial Transplant
1995;10:2224-27.
22. Cochat P, Koch Nogueira PC,
Mahmoud MA, Jamieson NV, Scheinman
JI, Rolland MO. Primary hyperoxaluria
in infants: medical, ethical, and econ-
omic issues. J Pediatr 1999;135:746-50.
23. Toussaint C. Pyridoxine-responsi-
ve PH1: treatment. J Nephrol 1998;
11 Suppl 1:49-50.
24. Dick PT, Shuckett BM, Tang B,
Daneman A, Kooh SW. Observer
reliability in grading nephrocalcinosis on
ultrasound examinations in children.
Pediatr Radiol 1999;29:68-72.
25. van Buren M. A stony history.
Nephrol Dial Transplant
2000;15:551-53.
26. Scheid C, Koul H, Hill WA, Luber-
Narod J, Kennington L, Honeyman T et al.
Oxalate toxicity in LLC-PK1 cells: role of
free radicals. Kidney Int 1996;49:413-19.
27. Singh DR, Sagade SN,
Kamat MH, Deshpande RB, Shah BV.
Oxalosis with nephrocalcinosis. Nephrol
Dial Transplant 2000;15:124-25
CHAPTER 03
page 64
VAN WOERDEN 5/19/08 8:53 AM Pagina 64

CHAPTER 04 Clinical implications of mutation analysis in primary hyperoxaluria type 1
Christiaan S van Woerden, Jaap W Groothoff, Frits A Wijburg, Carla Annink, Ronald JA Wanders and Hans R Waterham
Kidney International 2004;
66:746-752
Background. Primary hyperoxaluria type 1 (PH1) is an inborn error ofglyoxylate metabolism with an extensive clinical and genetic heteroge-neity. Although over 50 disease-causing mutations have been identi-fied, the relationship between genotype and clinical outcome remainsunclear. The aim of this study was to determine this association inorder to find clues for improvement of patient care.
Methods. AGXT mutation analysis and assessment of biochemicalcharacteristics and clinical outcome were performed on patients froma Dutch PH1 cohort.
Results. Thirty-three of a cohort of 57 PH1 patients, identified inThe Netherlands over a period of 30 years, were analyzed. Nine differentmutations were found. The most common mutations were the Gly170Arg,Phe152Ile, and the c.33_34insC mutations, with an allele frequency of44%, 19%, and 15%, respectively. Homozygous Gly170Arg and Phe152Ile mutations were associated with pyridoxine responsiveness and a preser-ved renal function over time when treatment was timely initiated. All patients homozygous for the c.33_34insC mutation had end-stagerenal disease (ESRD) before the first year of age. In two unrelated patients,a new Val336Asp mutation was found coupled with the Gly170Arg muta-tion on the minor allele. We also found 3 patients homozygous for a novelGly82Arg mutation with adverse outcome in 2 of them.
Conclusion. Early detection of Gly170Arg and Phe152Ile mutations inPH1 has important clinical implications because of their associationwith pyridoxine responsiveness and clinical outcome. The associationof a homozygous c.33_34insC mutation with severe infantile ESRD,resulting in early deaths in 2 out of 3 cases, warrants a choice for earlyliver transplantation in patients and prenatal diagnostics in affectedfamilies.
ABSTRACT
CHAPTER 04
page 65
VAN WOERDEN 5/19/08 8:53 AM Pagina 65

INTRODUCTION
Primary hyperoxaluria type 1 (PH 1) is a rare autosomal-recessiveinborn error of glyoxylate metabolism caused by a functional deficiencyof the peroxisomal liver-specific enzyme alanine:glyoxylate aminotrans-ferase (AGT). This enzyme deficiency leads to an overproduction of oxa-late and, in most cases, of glycolate. The accumulation of oxalate causesinsoluble calcium oxalate depositions in renal tissue and, in case of renalinsufficiency, systemic tissue damage caused by oxalate storage.Clinically, symptoms can vary from infrequently occurring renal stonesto early onset nephrocalcinosis and end-stage renal disease (ESRD) withsevere systemic disease. Administration of pyridoxine (vitamin B6) inpharmacological dosages (5-15 mg/kg/day) results in a reduction of uri-nary oxalate excretion in about 30% of patients with PH1.
PH1 is caused by mutations in the AGXT gene encoding AGT. The AGXTgene is located at 2q37.3 and consists of 11 exons, ranging from 65 bpto 407 bp (1). To date, 7 polymorphisms and more than 50 differentmutations have been found in the AGXT gene. Two different haplotypeshave been identified based on the presence or absence of three specificpolymorphic variants: the major (frequency 80%) and the minor haplo-type (frequency 20%). The latter is defined by a 74-bp duplication withinthe first intron, and by 32C>T and 1020A>G point mutations, which leadto Pro11Leu and Ile340Met amino acid substitutions.
In healthy individuals who are homozygous for the minor haplotype(frequency of 4% in the Caucasian population), 5% of AGT is mistargetedto mitochondria instead of to peroxisomes. In combination with aGly170Arg substitution, however, this minor haplotype leads to mis-tar-getting to the mitochondria of 90% of AGT. This not only causes a signi-ficant reduction of its activity in vivo, but also has consequences for itsfunctioning in glyoxylate metabolism. Several other mutations causingamino acid substitutions have shown to be associated with specific AGTphenotypes: the Gly82Glu substitution abolishes AGT catalytic activity,and the Gly41Arg substitution and Ile244Thr substitution both lead toprotein destabilization and aggregation into inclusion bodies (2).
Although several studies have established a relation between genotypeand in vitro AGT functioning, the association between genotype andbiochemical characteristics in vivo is less evident. One of the mostimportant unanswered questions is the relationship between clinicaloutcome and genotype. In order to investigate this relationship, wereviewed the biochemical characteristics, as well as the clinical outco-me, in 33 patients of a Dutch cohort of all known PH1 patients over aperiod of 30 years in whom we were able to obtain DNA.CHAPTER 04
page 66
VAN WOERDEN 5/19/08 8:53 AM Pagina 66

METHODS
Recently, we described a cohort of 57 patients with PH1 diagnosed bet-ween 1970 and 2000 in The Netherlands (3). From this cohort, weapproached all living patients and/or their parents to participate inthis study. Furthermore, we isolated DNA from liver biopsy tissue of 2deceased PH1 patients. Patients who were diagnosed after the year2000 were also approached, and, after informed consent was received,information on their clinical status was obtained.Diagnosis of PH1 was made if either deficient AGT activity in the liversamples or the combination of hyperoxaluria and hyperglycolic acidu-ria (24-hour urine excretion exceeding 0.5 mmol/L oxalate or 0.054mmol oxalate/mmol creatinine and 0.14 mmol glycolate/mmol creati-nine) was demonstrated. Renal function was estimated by the Cockroftformula in adults and the Schwartz formula in children using plasmacreatinine values (4,5). For patients in whom urinary oxalate could notbe measured because of anuria, highly elevated plasma oxalate levelsof more than 20 times the upper limit of the reference range (less than5 molµ/L) were considered to be caused by PH1 and not by renal insuf-ficiency itself (6). Patients in whom only hyperoxaluria was establishedwere considered to have PH1 if measurements in liver biopsies demon-strated deficient AGT activities in other family members. When thesefirm grounds were not present, we decided to include only patientswith the following highly suspicious circumstantial evidence for PH1:(1) significant response to pyridoxine therapy; and (2) severe systemicoxalosis. Renal insufficiency was defined as a creatinine clearance ofless than 60 mL/min/1.73 m2. ESRD was defined as a creatinine-clea-rance of less than 10 mL/min/1.73 m2 body surface area (BSA).Mutations in the AGXT gene were investigated in relation to pyridoxineresponsiveness and outcome. Pyridoxine responsiveness was definedby a decline of urinary or plasma oxalate levels of more than 30% in atleast two urine samples upon pyridoxine therapy (7). We calculated theprescribed dosages of pyridoxine per kg body weight in patients inwhich response of pyridoxine on oxalate excretion was measured. AGTenzyme activities were determined in liver samples as described, andare expressed as percentages of the mean AGT activity determined incontrol liver samples (8).
Genomic DNA was extracted from lymphocytes using the Wizard GenomicDNA purification kit according to the instructions of the supplier(Promega, Madison, WI, USA). Six sets of AGXT-specific primers with -21M13 or M13rev extensions were used for the amplification of theentire AGXT coding region encoded by exon 1 to 11 (TABLE 04.1) Eachpolymerase chain reaction (PCR) contained 0.4 µmol/L of each primer(synthesized by Pharmacia, Uppsala, Sweden), 10 mmol/L Tris/HCl pH8.4, 50 mmol/L KCl, 1.5 or 2 mmol/L MgCl2, 0.01% w/v bovine serum
Patients
Mutation analysis
CHAPTER 04
page 67
VAN WOERDEN 5/19/08 8:53 AM Pagina 67

albumin (BSA), 0.2 mmol/L dNTP (Pharmacia), and 0.5 µL Taq DNA poly-merase (Promega). Two different PCR programs were used to amplifythe exons. For exons 1, 2, 3, 4, and 11, the amplification started with 2minutes of denaturation at 96ºC, followed by 5 cycles of 30 seconds at96ºC, 30 seconds at 55ºC, and 1 minute at 72ºC, and 25 cycles of 30seconds at 94ºC, 30 seconds at 55ºC, and 1 minute at 72ºC, with a finalextension step of 7 minutes at 72ºC. For exons 5 to 10, the amplifica-tion started with 2 minutes of denaturation at 96ºC, followed by 5cycles of 30 seconds at 96ºC, 30 seconds at 55ºC, and 2 minutes at72ºC, and 25 cycles of 30 seconds at 94ºC, 30 seconds at 55ºC, and 2minutes at 72ºC, with a final extension step of 7 minutes at 72ºC. ThePCR fragments were analyzed by direct sequencing using the Big DyeTerminator Cycle Sequencing Kit or the Big Dye Primer Cycle sequen-cing kit (Applied Biosystems, Foster City, CA, USA) on an ABI 3100automated DNA sequencer according to the manufacturer's protocol(Applied Biosystems). Mutation analysis was performed with DNA ofthe probands and, when available, with DNA of the parents in order toestablish the zygosity of the probands.
The study design was approved by the Medical Ethics Committee of theAcademic Medical Center, and informed consent was obtained from the participants or their parents.
AGXT-specific primers used for mutation analysis of PH1 patients
5' Primer 3' Primer
[-21M13]-AAG CAC AGA TAA GCC TCA GG [M13-Rev]-GAT GGA TCC AGG GCC ATC CC
[-21M13]-GAC ACT CAC GGC CCA CTC TG [M13-Rev]-GAG CTG TGC TCC AGT CCA CC
[-21M13]-TCA CCT GCT GCC CTC CAT TC [M13-Rev]-TGC ACA GAG GTG AGG GTC TG
[-21M13]-ACT GAG AGG CTG GTG CTC AG [M13-Rev]-AGT GCG CCT GTC TCC TCC TG
[-21M13]-CAC CCA TGT CAC TGC CCA CC [M13-Rev]-CAC CTG GTG CAC AGT CCT GC
[-21M13]-AGG CGG GAG GCT GAC GTC AG [M13-Rev]-CTC CTC TCA CTC TTT CAC AG
[-21M13]:5'-TGTAAAACGACGGCCAGT-3'. [M13-Rev]: 5'-CAGGAAACAGCTATGACC-3'.
RESULTS
We identified 57 PH1 patients in The Netherlands over a period of 30years (3). For the present study we obtained material for DNA analysisof 33 of these 57 patients, two of whom had died at the time of investi-gation. These 33 patients were the offspring of 26 families. Patient cha-racteristics are given in TABLE 04.2; mutational data, biochemical phe-notype, and clinical outcome of all patients are presented in TABLE
04.3. Consanguinity was reported in one family (family 5, TABLE 04.3).The ethnic origin varied: Dutch (23), Turkish (2), Surinam (3), Albanian
TABLE 04.1
Exon
1 and 2
3 and 4
5 and 6
7 and 8
9 and 10
11
Clinical data
CHAPTER 04
page 68
VAN WOERDEN 5/19/08 8:53 AM Pagina 68

(4), and mixed Dutch-Turkish (1). The median age at diagnosis was 6.6(range 0 to 57) years. Twenty (59%) patients were diagnosed under theage of 18, and six (18%) in the first year of life. At the time of diagno-sis, 15 patients (44%) had renal insufficiency, 14 of whom had alreadydeveloped ESRD. No differences in time of follow-up were found bet-ween the patients with a stable renal function and those who develop-ed renal insufficiency [median (range) follow-up: 13.1 (0 to 47) and 7.7(0 to 46) years, respectively]. AGT activity was measured in the liversamples of 21 patients. The median AGT activity was 9.5% of controlvalues (range 1% to 47%). Pyridoxine therapy was initially started in 16patients. In 13 of these 16 patients, pyridoxine therapy induced a sig-nificant decrease of urinary oxalate excretion. In two additionalpatients, pyridoxine was successfully prescribed after isolated kidneytransplantation (patients 8 and 18, TABLE 04.3).
Kidney transplantation was primary performed in nine and combinedliver-kidney transplantation in six patients. Two patients received asecond isolated renal graft, eight and six years, respectively, after theirfirst transplantation, and in one patient combined liver kidney trans-plantation was performed 7 years after the first isolated kidney trans-plantation. In one patient, isolated kidney transplantation was perfor-med after combined liver kidney transplantation. Renal graft functionswere preserved in five patients with isolated kidney transplantation for2, 3, 3, 9, and 14.5 years, respectively (TABLE 04.3). Of all six patientswith combined liver-kidney transplantation, one patient died as a con-sequence of liver failure, and one patient developed severe cirrhosis.One patient showed a deterioration of the renal function; the otherthree patients had a preserved renal and liver function after a follow-up of 1, 4, and 7 years, respectively.
Patient characteristics Abbreviation:ESRD, end-stage renal disease.
Total number of patients 33
Male/female 15/18
Median age at time of investigation (years) 27 (3-63)
Median age at time of diagnosis (years) 6.6 (0-50)
Infantile onset of symptoms 8
Urolithiasis 19
Nephrocalcinosis 17
Pyridoxine responsiveness 15
Renal insufficiency at the time of diagnosis 15
ESRD at the time of diagnosis 14
ESRD or renal insufficiency at follow-up 21
Kidney transplantation 12 in 10 patients
Combined liver-kidney transplantation 6
Deceased 2
TABLE 04.2
CHAPTER 04
page 69
VAN WOERDEN 5/19/08 8:53 AM Pagina 69

Mutations and clinical characteristics of all patients
Mutation Age of Age of Renal function
(allele) symptoms/ follow-up of diagnosis
diagnosis years
years
Gly170Arg (m) Gly170Arg (m) 5/5 13 Normal
Gly170Arg (m) Gly170Arg (m) 42/42 53 ESRD
Gly170Arg (m) Gly170Arg (m) 35/35 49 Normal
Gly170Arg (m) Gly170Arg (m) 6/6 55 Normal
Gly170Arg (m) Gly170Arg (m) 48/48 53 ESRD
Gly170Arg (m) Gly170Arg (m) 10/16 36 ESRD
Gly170Arg (m) Gly170Arg (m) 7/7 34 Normal
Gly170Arg (m) Gly170Arg (m) 25/25 38 Normal
Gly170Arg (m) Gly170Arg (m) 0.5/3.5 17.8 ESRD
Gly170Arg (m) Gly170Arg (m) 50/50 58 ESRD
Gly170Arg (m) Gly170Arg (m) 57/57 61 Normal
Gly170Arg (m) Xo (M) 0.4/0.4 11 ESRD
Gly170Arg (m) Xo (M) 0.3/0.3 15 Normal
Gly170Arg (m) Xo (m) 0.5/0.5 3 Normal
Gly170Arg - Val336Asp (m) 5/5 8 Decreased
Gly170Arg - Val336Asp (m)
Gly170Arg (m) Leu153Val (M) 27/27 39 ESRD
Phe152Ile (m) Phe152Ile (m) 2/2 31 Normal
Phe152Ile (m) Phe152Ile (m) 25/30 59 ESRD
Phe152Ile (m) Phe152Ile (m) 31/31 37 ESRD
Phe152Ile (m) Phe152Ile (m) 22/22 26 Normal
Phe152Ile (m) Gly170Arg (m) 1/1 10 Normal
Phe152Ile (m) Gly170Arg-Val336Asp(m) 4/4 20 Normal
Phe152Ile (m) Xo (m) 40/40 44 ESRD
Phe152Ile (m) 33delC (M) 2/2 27 Normal
c.33_34insC (M) c.33_34insC (M) 0.1/0.1 8 ESRD
c.33_34insC (M) c.33_34insC (M) 0.5/0.5 0.6 ESRD
c.33_34insC (M) c.33_34insC (M) 0.6/0.6 1.3 ESRD
c.33_34insC (M) Gly170Arg (m) 4/14 23 ESRD
c.33_34insC (M) Gly170Arg (m) 6/6 29 Normal
Gly82Arg (m) Gly82Arg (m) 0.6/0.6 16 Normal
Gly82Arg (m) Gly82Arg (m) 6/6 19 Normal
Gly82Arg (m) Gly82Arg (m) 7/7 21 Normal
C173X (M) IVS1-1G>A (M) 0.2/0.2 14 ESRD
TABLE 04.3
Patient
(family)
1 (1)
2 (2)
3 (3)
4 (3)
5 (3)
6 (4)
7 (5)
8 (5)
9 (6)
10 (7)
11 (7)
12 (8)
13 (8)
14 (9)
15 (10)
16 (11)
17 (12)
18 (13)
19 (14)
20 (14)
21 (15)
22 (16)
23 (17)
24 (18)
25 (19)
26 (20)
27 (21)
28 (22)
29 (23)
30 (24)
31 (25)
32 (25)
33 (26)
Abbreviations :
m, minor allele; M, major allele; PyrR, pyridoxine responsiveness defined by more than
30% reduction of urinary-oxalate upon pyridoxine; treatment Pyr D, pyridoxine dosage
in mg/kg/day: minimal dosage with more than 30%
response of urinary oxalate or maximum prescribed dosage in case of no response
VAN WOERDEN 5/19/08 8:53 AM Pagina 70

Renal function/ Tx PyrR Pyr D AGT %
outcome of age, mg/kg
follow-up years
age, years
Preserved + 2.5 47.4
Tx preserveda K (44) ND ND
Preserved + 14.2 46.9
ESRD (51)/Tx preserveda K (52) +b 11.4 14.9
ESRD ND ND
Tx preserveda K (22) ND ND
Preserved + 7.1 34.0
ESRD (34)/Tx preserveda K (36) +b 14.2 ND
Tx decreaseda K (9, 17) ND 30.0
Tx decreaseda K (50, 56) ND 37.1
Preserved + 6.6 ND
ESRD (4)/Tx preserveda LK (4), K (6) ND ND
Preserved + 13.6 5.2
Preserved + 30 6.2
Decreasing - 4.0 4.5
ESRD/Tx-preserveda K (31), LK (38) ND 16.4
Preserved + 12.5 12.9
Tx decreasing slowlya K (31) +b 14.3 ND
ESRD ND ND ND
Preserved + 2.9 10.0
Preserved + 7.5 10.0
Decreased + 6.0 10.2
ESRD ND 16.6
Preserved + 6.0 5.9
Tx preserveda LK (1.7) ND 5.2
Died + 15 1.1
Died (liver failure) LK (1.3) ND 5.0
Tx preserveda/liver failure LK (16.5) ND ND
Preserved + 8.0 16.3
Preserved ND ND
ESRD (18)/Tx decreasinga LK (19) - 5.7 3.6
Decreased - 20.0 ND
Tx preserveda K (11) ND 4.1
on oxalate excretion; AGT %, percentage AGT-activity in vitro related to AGT-
activity in vitro of control tissue; K, kidney transplantation; LK, combined liver-kidney
transplantation; ESRD, end-stage renal disease; ND, not determined; Tx, transplantation.a Renal graft function; b Determined after transplantation.
VAN WOERDEN 5/19/08 8:53 AM Pagina 71

Nine different mutations were found in 26 unrelated probands (TABLE
04.4). We found the Gly170Arg mutation in 20 patients (60.6%), 15 ofwhom were unrelated. The allele frequency was 44%. Seven patientswere compound heterozygous, and eight were homozygous for thismutation. The minor allele, consisting of the Pro11Leu polymorphismand the 74-bp insertion in the first intron, always co-segregated withthis mutation.
Eight patients, seven of whom were unrelated, carried the Phe152Ilemutation (allele frequency 19%).
The c.33_34insC mutation was found in five patients (allele frequency15%). In two patients (patients 15 and 22, TABLE 04.3), a novel mutationwas identified on the Gly170Arg allele: an amino acid changeVal336Asp (1007T>A mutation). In four cases (patients 12, 13, 14, 23,TABLE 04.3), only 1 heterozygous mutation was found. Of six probands,another seven siblings were diagnosed by screening (TABLE 04.3).Sequencing revealed the same mutations in each affected family. Inthree patients of two unrelated families, we found homozygosity for apreviously unrecognized 121G>A (244G>A) mutation, resulting in aGly82Arg substitution.
Mutations in the AGXT gene in Dutch PH1 patients
Mutationa Exonb Allelec Coding effect
IVS1-1G>A Intron 1 Major Splicing defect
c.33_34insC (156insC) 1 Major Frame shift
33delC (156delC) 1 Major Frame shift
244G>C (336G>C) 2 Minor Gly82Arg
454T>A (576T>A) 4 Minor Phe152Ile
457T>G (579T>G) 4 Major Leu153Val
508G>A (630G>A) 4 Minor Gly170Arg
519C>A (641C>A) 5 Major Cys173STOP
1007T>A 6 Minor Val336Asp
a Nucleotide numbering starts from the first AUG (position 123) according to cDNA
sequence of GenBank Accession number NM_000030. Between brackets the nota-
tion according to the previously introduced numbering system which starts at the
first nucleotide of this cDNA sequence.b Exon-intron numbering according to Purdue (9).
Gene mutations
TABLE 04.4
CHAPTER 04
page 72
VAN WOERDEN 5/19/08 8:53 AM Pagina 72

The Gly170Arg and Val336Asp substitutionsOf the 12 patients who were homozygous for the Gly170Arg substitu-tion (patients 1 to 11 and 15, TABLE 04.3), five had developed ESRD attime of diagnosis. Pyridoxine responsiveness was observed in six of allseven patients in whom pyridoxine responsiveness was measured. Inone additional patient with ESRD at time of diagnosis, pyridoxine res-ponsiveness was established after kidney transplantation. The onlypatient without response upon pyridoxine administration developedrenal insufficiency. Remarkably, this patient was also homozygous fora second, previously unrecognized mutation: the Val336Asp mutation.This novel mutation, in association with the Gly170Arg allele, was alsoidentified heterozygous in another patient who was initially pyridoxi-ne responsive, but showed nevertheless a decline of renal function atfollow-up. Levels of urinary oxalate remained above 0,1 mmol/mmolcreatinine despite a decline from the levels at time of diagnosis. All buttwo homozygous Gly170Arg patients with a normal renal function attime of diagnosis (and without the additional Val336Asp mutation) pre-served their renal function over time. The two patients that developedESRD over time were unfortunately both lost to follow-up in the periodbetween diagnosis and onset of dialysis; both patients had not beentreated with pyridoxine, potassium citrate, or high fluid intake. Afterkidney transplantation, both patients were responsive to pyridoxinetherapy and preserved their renal function to date with a graft survivalof 3 and 14.5 years, respectively (patients 4 and 8, TABLE 04.3).Four out of six homozygous Gly170Arg patients who received a renalgraft were able to preserve their renal functions after a mean follow-upof 8 (range 3 to 14.5) years.
The Phe152Ile substitutionIn two out of all four homozygous Phe152Ile patients (patients 17 and20, TABLE 04.3), pyridoxine therapy was used successfully in reducingurinary oxalate excretion. Both patients preserved their renal functionover time, with a follow-up of 4 and 29 years, respectively. The twoother patients had ESRD at time of diagnosis. In one of them (patient 18,TABLE 04.3), pyridoxine therapy was initiated at the onset of hemodialy-sis treatment, resulting in a significant fall in plasma oxalate, whichcontinued to decrease after isolated kidney transplantation. However,renal function slowly decreased throughout the follow-up period due toa chronic vascular rejection (10). Of the four heterozygous Phe152Ilepatients, one had ESRD at time of diagnosis (patient 23, TABLE 04.3). Allother three patients were pyridoxine responsive; two of them preservedtheir renal function over time with a follow-up period of 9 and 25 years,respectively (patients 21 and 24, TABLE 04.3). The only pyridoxine-res-ponsive patient with a decrease in renal function over time under treat-ment was compound heterozygous for the Phe152Ile allele and theGly170Arg+Val336Asp allele (patient 22, TABLE 04.3).
Associationsbetween
genotype andphenotype
CHAPTER 04
page 73
VAN WOERDEN 5/19/08 8:53 AM Pagina 73

The c.33_34insC mutationAll 3 patients who were homozygous for the c.33_34insC mutationdeveloped ESRD within their first year of life. Diagnosis was made atthe same time. Two of these patients died within one year after the diagnosis was established (patients 25 to 27, TABLE 04.3).
The Gly82Arg substitutionPyridoxine responsiveness was measured in two of three homozygousGly82Arg patients (patients 31 and 32, TABLE 04.3) and found negativein both. One of these two patients had ESRD at the time of diagnosisand received a combined liver and renal graft (patient 31, TABLE 04.3).The other patient showed a decline in renal function over time. In theonly patient that preserved renal function over time, pyridoxine responsiveness was not measured (patient 30, TABLE 04.3).
Single and double (compound) heterozygous mutationsWe found compound heterozygous mutations in seven patients, threeof whom had ESRD at the time of diagnosis (patients 16, 28, and 33,TABLE 04.3). The course of renal function over time showed a great vari-ation. Two out of four patients who were only heterozygous for onemutation also had ESRD at time of diagnosis (patients 12 and 23, TABLE
04.3).
DISCUSSION
We collected data on both the clinical characteristics and genotypes ina large cohort of PH1 patients in The Netherlands. The majority of thedetected mutations have previously been found in association withPH1. This makes the AGXT mutation screening a useful tool in the dia-gnostic work-up of PH1 patients in The Netherlands.
In our cohort of Dutch PH1 patients, the Gly170Arg mutation was themost common mutation. Our finding that this mutation was associatedwith pyridoxine responsiveness is consistent with other reports(11,12). Previously, Motley et al. have described the molecular basis forthe combination of severe hyperoxaluria and hyperglycoluria with thepresence of a considerable AGT activity in vitro and pyridoxine res-ponsiveness in these patients (13). They showed that the Gly170Argmutation, which is always located on the minor allele, results in incre-ased mistargeting of AGT to the mitochondria instead of peroxisomes,which leads to inactivation of the enzyme in vivo. This mitochondrialmistargeting of AGT already occurs to a small extent ( 5%) with AGTencoded by the minor allele because of the presence of a Pro11Leumutation (14). This mutation creates a weak mitochondrial targetingsequence in the amino terminus of the encoded AGT. The Gly170Argmutation increases the efficiency of the mitochondrial targeting
Gly170Arg
CHAPTER 04
page 74
VAN WOERDEN 5/19/08 8:53 AM Pagina 74

sequence by delaying the dimerization of AGT and consequently bypreventing the folding of the protein (2,15). As a result of this, theamino terminus remains accessible for mitochondrial import.Pyridoxine increases the residual activity of the 10% peroxisomal-loca-ted AGT. Previously, there has been discussion whether this relativelyfavorable biological background (i.e., the pyridoxine responsiveness) isin line with the clinical outcome of patients with this mutation. Allhomozygous Gly170Arg cohort patients who had a preserved renalfunction at the time of diagnosis and who were treated accordinglywith pyridoxine, a high fluid intake, and potassium citrate were able topreserve renal function throughout the follow-up period. However, fivehomozygous patients had already developed ESRD at the time of dia-gnosis. Therefore, renal function can be preserved in patients with aGly170Arg mutation (but without a Val336Asp mutation, as discussedbelow) after a timely diagnosis and treatment with pyridoxine. This issupported by the course of isolated renal transplantations inGly170Arg-positive patients in our cohort. In contrast to what might beexpected in PH1 patients with isolated kidney transplantation, renalfunction was preserved in four out of six of these patients after a medi-an follow-up of more than seven years, most likely as a consequence ofpyridoxine therapy.
A novel mutation, 1007T>A (1129T>A), was found in two patients andtheir relatives, which results in the amino acid replacement Val336Asp.The mutation was present on the minor allele and in combination withthe frequent Gly170Arg mutation. While Gly170Arg is correlated withpyridoxine responsiveness, the Val336Asp mutation appears to inter-fere in a negative way with the effect of pyridoxine, and in fact, pre-disposes to the development of renal insufficiency, at least in homo-zygous patients.
We found a relatively high number of patients carrying the Phe152Ilemutation. This mutation has previously been described in six patients(1,11,16). However, this is the first time that homozygous patients forthis mutation are reported. The high prevalence of Phe152Ile in ourstudy, when compared to others, suggests a founder effect. The bene-ficial effect of pyridoxine in these patients is in line with observationspreviously made (1).
The c.33_34insC mutation is the third most common mutation found inour study. Patients affected by this mutation in a homozygous condi-tion all suffered from the most severe form of infantile PH1, with ESRDbefore the first birthday. In the two patients who were compoundheterozygous for the c.33_34insC mutation, the onset of symptomsand development of ESRD was much later, and the level of AGT activi-ty was higher than in the homozygous patients. In previous studies,
Val336Asp
Phe152Ile
c.33_34insC
CHAPTER 04
page 75
VAN WOERDEN 5/19/08 8:53 AM Pagina 75

the c.33_34insC mutation has also been found (11,17). The results ofthe study by Milosevic et al. are in line with our findings (17).Remarkably, a study by Amoroso et al. revealed the opposite effect ofthe homozygous and heterozygous c.33_34insC mutation: the worstoutcome was shown by the heterozygous patient (no pyridoxine res-ponsiveness, no residual AGT activity), in contrast to a milder pheno-type in two homozygous patients who both appeared to be pyridoxineresponsive, and only one of whom developed ESRD (11). This seemshard to explain because the insertion of a nucleotide at residue 33(156) will result in a reading frame shift and introduces a terminationcodon at residue 44 (167). The resulting truncated protein would notbe predicted to have any enzyme activity, if synthesized at all. The factthat a heterozygous patient for this mutation was responsive to pyri-doxine therapy can be explained by the presence of the Gly170Argmutation.
Although all three Gly82Arg homozygous patients had a normal renalfunction at the time of diagnosis, two of them suffered from progres-sive renal insufficiency over time. Both patients were not responsive topyridoxine. As far as we know, these two families are the first ever des-cribed with this mutation. This mutation parallels the previously repor-ted Gly82Glu mutation with respect to the pyridoxine unresponsive-ness (2). Zhang et al. showed that binding of pyridoxine to AGT hasbecome impossible under influence of the Gly82Glu mutation as aresult of a change in the crystal structure of AGT (18). It seems likelythat the same occurs in the Gly82Arg mutation.
In four patients, only one heterozygous mutation could be found.Purdue et al. and Milosevic et al. already showed that in patients whowere heterozygous for the Gly170Arg allele and homozygous for theminor allele, only the mutant allele was expressed, indicating that theother allele contained a mutation affecting its transcription or proteinstability (14,17). However, of the three patients heterozygous for theGly170Arg allele, only one was homozygous for the minor allele, sug-gesting that there may be more alleles that are not expressed. No liversamples were available to test at the transcription level.
Like the true heterozygous patients, all compound heterozygouspatients showed a great variation in clinical outcome.
CLINICAL IMPLICATIONS
This study shows a clear association between homozygosity forGly170Arg and Phe152Ile mutation on one side, and pyridoxine res-ponsiveness on the other side. The clinical course of these patientssuggests that early treatment preserves renal function. Therefore, we
Gly82Arg
Heterozygousand
compoundheterozygous
mutations
CHAPTER 04
page 76
VAN WOERDEN 5/19/08 8:53 AM Pagina 76

believe that the combination of these particular mutations, hyperoxa-luria, hyperglycolic aciduria, and pyridoxine responsiveness abolishesthe need for AGT assessment because this will not reveal anything thatmight influence the treatment policy. The same counts for homozy-gous c.33_34insC patients with neonatal onset of disease who do notrespond to pyridoxine. In all other cases, AGT assessment remains anecessary tool in the diagnostic work up of PH1.
Mutation analysis might also play a role in the prevention of disease inthe relatives of PH1 patients. Family members who are also affectedbut not yet diagnosed may benefit from an early conservative treat-ment with pyridoxine. Our study showed that affected siblings whowere found by screening had a better outcome compared with the pro-band, despite the fact that they inherited the same mutation.
Finally, mutation analysis in ESRD PH1 patients might be useful in thedecision whether to perform combined liver-kidney or isolated kidneytransplantation. Therefore, we believe that even in those PH1 patientswho already have developed an ESRD, AGXT mutation analysis can bevery useful. It seems defensible only to perform isolated kidney trans-plantation in homozygous Gly170Arg or Phe152Ile patients. On theother hand, the adverse outcome of the pyridoxine negativec.33_34insC and Gly82Arg mutations gives more argument for a comb-ined liver-kidney, or a timely planned liver transplantation in thesepatients. Prenatal diagnostics may be applied in affected families. Wetherefore believe that mutation analysis should be an integral part ofthe diagnostic work-up of patients.
We tried to make a complete overview of PH1 mutations in a recentlyset up cohort of PH1 patients, comprising the entire spectrum of thedisease. Some patients, however, have been lost to follow-up (death,refusal to participate), resulting in a smaller cohort than clinically des-cribed before. Other factors like diet and levels of citrate, pH in theurine, may also interplay in the process of renal tissue damage. As cli-nical data were obtained retrospectively, these factors have not beenassessed in our study.
CONCLUSION
Mutation analysis in patients with PH1 has shown to be an importantdiagnostic tool in PH1 and should be applied in all patients with seve-re hyperoxaluria. Assessment of a well-known mutation in a patientwith severe hyperoxaluria might abolish the need for the invasive liverbiopsy in establishing the diagnosis PH1. Moreover, our data haveshown that in certain PH1 patients, mutation analysis can also be usedas a guide in the therapeutic approach of these patients.
Limitations of the study
CHAPTER 04
page 77
VAN WOERDEN 5/19/08 8:53 AM Pagina 77

1. Danpure CJ, Purdue PE,
Fryer P, Griffiths S, Allsop J,
Lumb MJ et al. Enzymological and
mutational analysis of a complex
primary hyperoxaluria type 1 pheno-
type involving alanine:glyoxylate
aminotrans-ferase peroxisome-to-mito-
chondrion mistargeting and intra-
peroxisomal aggregation. Am J Hum
Genet 1993;53:417-32.
2. Lumb MJ, Danpure CJ.
Functional synergism between
the most common polymorphism
in human alanine:glyoxylate
aminotransferase and four of
the most common disease-
causing mutations. J Biol
Chem 2000;275:36415-22.
3. van Woerden CS,
Groothoff JW, Wanders RJ,
Davin JC, Wijburg FA. Primary hyper-
oxaluria type 1 in The Netherlands:
prevalence and outcome. Nephrol
DialTransplant 2003;18:273-79.
4. Cockcroft DW, Gault MH.
Prediction of creatinine clearance
from serum creatinine.
Nephron 1976;16:31-41.
5. Schwartz GJ, Haycock GB,
Edelmann CM, Jr., Spitzer A. A simple
estimate of glomerular filtration rate
in children derived from body length
and plasma creatinine.
Pediatrics 1976;58:259-63.
6. Wolthers BG, Meijer S,
Tepper T, Hayer M, Elzinga H.
The determination of oxalate in
haemodialysate and plasma: a means
to detect and study 'hyperoxaluria' in
haemodialysed patients.
Clin Sci 1986;71:41-47.
7. Leumann E, Hoppe B. What is
new in primary hyperoxaluria? Nephrol
Dial Transplant 1999;14:2556-58.
8. Wanders RJ, Ruiter J, van
Roermund CW, Schutgens RB, Ofman
R, Jurriaans S, Tager JM. Human liver
L-alanine-glyoxylate aminotransferase:
characteristics and activity in controls
and hyperoxaluria type I patients using
a simple spectrophotometric method.
Clin Chim Acta 1990;189:139-44.
9. Purdue PE, Lumb MJ, Fox M,
Griffo G, Hamon-Benais C, Povey S,
Danpure CJ. Characterization and
chromosomal mapping of a genomic
clone encoding human alanine:glyoxy-
late aminotrans-ferase.
Genomics 1991;10:34-42.
10. Rosier JG, Baadenhuijsen H,
Koene RA. Long-term survival of
a renal allograft in a patient with pri-
mary hyperoxaluria (type I). Neth J
Med 1981;24:179-84.
11. Amoroso A, Pirulli D, Florian F,
Puzzer D, Boniotto M, Crovella S et al.
AGXT gene mutations and their influence
on clinical heterogeneity of type 1
primary hyperoxaluria. J Am Soc
Nephrol 2001;12:2072-79.
12. Hoppe B, Danpure CJ, Rumsby
G, Fryer P, Jennings PR, Blau N et al.
A vertical (pseudodominant) pattern of
inheritance in the autosomal recessive
disease primary hyperoxaluria type 1:
lack of relationship between genotype,
enzymic phenotype, and disease severity.
Am J Kidney Dis 1997;29:36-44.
13. Motley A, Lumb MJ, Oatey PB,
Jennings PR, De Zoysa PA, Wanders RJ
et al. Mammalian alanine/glyoxylate
REFERENCES
CHAPTER 04
page 78
VAN WOERDEN 5/19/08 8:53 AM Pagina 78

aminotrans-ferase 1 is imported
into peroxisomes via the PTS1 trans-
location pathway. Increased degeneracy
and context specificity of the mammalian
PTS1 motif and implications for the
peroxisome-to-mitochondrion mistargeting
of AGT in primary hyperoxaluria type
1. J Cell Biol 1995;131:95-109.
14. Purdue PE, Takada Y, Danpure CJ.
Identification of mutations associated
with peroxisome-to-mitochondrion
mistargeting of alanine/glyoxylate
aminotransferase in primary hyper-
oxaluria type 1. J Cell Biol 1990;
111:2341-51.
15. Leiper JM, Oatey PB, Danpure CJ.
Inhibition of alanine:glyoxylate amino-
transferase 1 dimerization is a pre-
requisite for its peroxisome-to-mito-
chondrion mistargeting in primary
hyper-oxaluria type 1. J Cell Biol
1996;135:939-51.
16. Coulter-Mackie MB, Rumsby G,
Applegarth DA, Toone JR. Three novel
deletions in the alanine:glyoxylate ami-
notrans-ferase gene of three patients
with type 1 hyperoxaluria. Mol Genet
Metab 2001;74:314-21.
17. Milosevic D, Rinat C, Batinic D,
Frishberg Y. Genetic analysis- a dia-
gnostic tool for primary hyperoxaluria
type 1. Pediatr Nephrol 2002;17:896-98.
18. Zhang X, Roe SM, Hou Y, Bartlam
M, Rao Z, Pearl LH, Danpure CJ. Crystal
structure of alanine:glyoxylate amino-
transferase and the relationship between
genotype and enzymatic phenotype in
primary hyperoxaluria type 1.
J Mol Biol 2003;331:643-52.
CHAPTER 04
page 79
VAN WOERDEN 5/19/08 8:53 AM Pagina 79

CHAPTER 05 Primary hyperoxaluria remains undiagnosed in patients with hyperoxaluria and recurrent urolithiasis
Christiaan S van Woerden, Jaap W Groothoff, Frits A Wijburg, Hans R Waterham, Ronald JA Wanders, Marcel JW Janssen and Marinus Duran
Clinical Chemistry 2007;
53:1553-1554
Primary hyperoxaluria (PH) is a metabolic disorder caused by deficiencyof either the liver-specific enzyme alanine:glyoxylate aminotransferase(AGT) for PH type 1 (PH1) or glyoxylate reductase/hydroxypyruvatedehydrogenase (GR/HPR) for PH type 2 (PH2). PH increases endogenousoxalate production, leading to the development of renal stones andnephrocalcinosis, which may result in end-stage renal disease (ESRD) (1).The first step in the diagnostic process involves measurement of urinary oxalate, glycolate, and L-glycerate, followed by enzymatic ana-lysis of AGT (in liver) or GR/HPR (in lymphocytes), or genetic testing ofthe AGXT gene for PH1 or the GRHPR gene for PH2. Extensive metabolicscreening is rarely performed in adults who present with stone diseasebecause PH disease presentation usually occurs in childhood, not inadulthood. Nevertheless, more than one-third of PH1 is diagnosed inadult patients in ESRD (2). Early diagnosis and treatment is of utmostimportance in PH, because conservative therapy can prevent renal insuf-ficiency (2), particularly pyridoxine therapy in PH1 (3). If treatment is not initiated in a timely manner, ESRD will ensue in thesepatients. Therefore, adequate diagnostic measures should be taken afterthe first clinical signs and symptoms have evolved.
We performed a comprehensive search among all nephrologists in TheNetherlands (2) and discovered a relatively high prevalence of PH inThe Netherlands. The high number of adult patients who were diagno-sed only after the development of ESRD (59% for adults) indicates thatour search method may have missed patients with PH and prompted usto design a strategy to identify more patients with PH. During a periodof 8 years, in one routine academic hospital laboratory, we traced allpatients with hyperoxaluria and performed further metabolic and gene-tic investigations to diagnose or exclude PH.
Since 1995, urinary oxalate has been measured at the Laboratory forGeneral Clinical Chemistry at the Department of Clinical Chemistry inthe Academic Medical Center. Until 2003, results of urinary oxalatescreening revealed hyperoxaluria in 32 of 150 patients, according tothe reference interval we determined with a 24-h urine collection study
CHAPTER 05
page 80
VAN WOERDEN 5/19/08 8:53 AM Pagina 80

performed in this laboratory. In 25 of these 32 patients (those we wereable to contact) we performed analyses of urinary oxalate, glycolate,and L-glycerate in fresh 24-h urine by ion chromatography (Dionex)and gas chromatography. Hyperoxaluria was detected in six patients(clinical characteristics as listed in TABLE 05.1). One patient had PH1,confirmed by detection of a C.508G>A mutation on the so-called minorallele of the AGXT gene, leadin g to a Gly170Arg amino acid substitu-tion in the AGT enzyme. The urinary oxalate excretion rate was onlymildly increased because this patient used pyridoxine at the time ofurinalysis. The other five patients had urinary glycolate and L-glycera-te excretion rates that were within the reference intervals and therefo-re in these five patients the diagnosis of PH was rejected and no fur-ther testing was performed. Four of these five patients had developedurinary tract symptoms after the onset of intestinal disease, diagnosedas secondary hyperoxaluria related to malabsorption. The fifth patientdid not have evidence of PH or secondary hyperoxaluria and thereforethis case was classified as idiopathic hyperoxaluria.
Characteristics of patients with hyperoxaluriaReference value: 0-54 mmol/mol creatinine
Patient Age Age at Symptoms Urinary Co- Diagnosis
years first oxalate morbidity
symptoms mmol/mol
years creatinine
1 59 2 UNI 60 PH1
2 85 34 U 80 IH
3 55 51 UNR 70 Sb SH
4 40 31 UNR 200 Cd SH
5 63 48 UI 130 Sb,Cd SH
6 69 50 UE 100 Sb SH
Abbreviations
Symptoms: U; urolithiasis, N; nephrocalcinosis, R; renal insufficiency,
E; end-stage renal disease
Co-morbifity: Sb; short bowel after intestinal resections, Cd; Crohn's disease
In this study, we searched for PH in a specific patient group in whichwe suspected that PH may have been underdiagnosed (2). Apparently,our strategy led to the discovery of a patient with previously undiagnosedPH. In view of the very low prevalence of PH in populations studied sofar, the finding of a new PH patient in a cohort of 150 patients is remar-kable and confirms that PH remains undiagnosed in some adultpatients, and that the prevalence of this disease may be higher than
TABLE 05.1
CHAPTER 05
page 81
VAN WOERDEN 5/19/08 8:53 AM Pagina 81

previously estimated (2). The cases we describe in this report showthat PH can be diagnosed only with an immediate and complete diagnostic work-up, a procedure that provides the best opportunity toprevent further renal damage. Therefore, episodes of urolithiasis,nephrocalcinosis, recurrent urinary tract infections, or unexplaineddecline of renal function require assessment of urinary oxalate toexclude PH. We strongly suggest that performing the same screeningstrategy in other hospital laboratories will detect more PH patients whomay benefit from early recognition and treatment.
As previously reported, hyperoxaluria, dehydration, and other co-morbidities may lead to renal involvement (4). Citrate administrationdecreases the risk of stone formation (5), but this treatment was notused in three of the cases we investigated, an omission that may haveplaced them at higher risk for renal involvement. Therefore, all availa-ble conservative measures to decrease the risk of stone formationshould be taken in patients with any type of hyperoxaluria.
REFERENCES
CHAPTER 05
page 82
1. Danpure CJ. Primary hyper-
oxaluria. In: Scriver CR, Beaudet AL,
Sly WS, Valle D, eds. The Metabolic and
Molecular Bases of Inherited Disease.
New York: McGraw-Hill, 2001:3323-67.
2. van Woerden CS, Groothoff JW,
Wanders RJ, Davin JC, Wijburg FA.
Primary hyperoxaluria type 1 in The
Netherlands: prevalence and outcome.
Nephrol Dial Transplant 2003;
18:273-79.
3. van Woerden CS,
Groothoff JW, Wijburg FA, Annink C,
Wanders RJ, Waterham HR. Clinical
implications of mutation analysis in
primary hyperoxaluria type 1. Kidney
Int 2004;66:746-52.
4. Parks JH, Worcester EM,
O’Connor RC, Coe FL. Urine stone risk
factors in nephrolithiasis patients with
and without bowel disease. Kidney Int
2003;63:255-65.
5. Soygur T, Akbay A, Kupeli S.
Effect of potassium citrate therapy
on stone recurrence and residual
fragments after shockwave lithotripsy
in lower caliceal calcium oxalate
urolithiasis: a randomized controlled
trial. J Endourol 2002;16:149-52.
VAN WOERDEN 5/19/08 8:53 AM Pagina 82

CHAPTER 06 High incidence of hyperoxaluria in generalized peroxisomal disorders
Christiaan S van Woerden, Jaap W Groothoff, Frits A Wijburg, Marinus Duran, Ronald JA Wanders, Peter G Barth and Bwee Tien Poll-The
Molecular Genetics and Metabolism 2006
88:346-50
The Zellweger spectrum disorders (ZSDs) are characterized by a gene-ralized loss of peroxisomal functions caused by deficient peroxisomalassembly. Clinical presentation and survival are heterogeneous.Although most peroxisomal enzymes are unstable in the cytosol ofperoxisome-deficient cells of ZSD patients, a few enzymes remain sta-ble among which alanine:glyoxylate aminotransferase (AGT). Its defi-ciency causes primary hyperoxaluria type 1 (PH1, MIM 259900), aninborn error of glyoxylate metabolism characterized by hyperoxaluria,nephrocalcinosis, and renal insufficiency. Despite the normal level ofAGT activity in ZSD patients, hyperoxaluria has been reported in seve-ral ZSD patients. We observed the unexpected occurrence of renal sto-nes in a cohort of ZSD patients. This led us to perform a study in thiscohort to determine the prevalence of hyperoxaluria in ZSDs and tofind clinically relevant clues that correlate with the urinary oxalateload. We reviewed medical charts of 31 Dutch ZSD patients with pro-longed survival (more than 1 year). Urinary oxalate excretion wasassessed in 23 and glycolate in 22 patients. Hyperoxaluria was presentin 19 (83%), and hyperglycolic aciduria in 14 (64%). Pyridoxine treat-ment in six patients did not reduce the oxalate excretion as in somePH1 patients. Renal involvement with urolithiasis and nephrocalcinosiswas present in five of which one developed end-stage renal disease.The presence of hyperoxaluria, potentially leading to severe renalinvolvement, was statistically significant correlated with the severityof neurological dysfunction. ZSD patients should be screened by uri-nalysis for hyperoxaluria and renal ultrasound for nephrocalcinosis inorder to take timely measures to prevent renal insufficiency.
ABSTRACT
CHAPTER 06
page 83
VAN WOERDEN 5/19/08 8:53 AM Pagina 83

INTRODUCTION
The Zellweger spectrum disorders (ZSDs) include the severe classicZellweger syndrome with an early lethal course, and much milder phe-notypes with prolonged survival known as neonatal adrenoleukodystro-phy and infantile Refsum disease. Most common clinical features areneurodevelopmental impairment, retinopathy, perceptive deafness, andhepatic dysfunction (1). The extent of the neurodevelopmental impair-ment is highly variable. Some patients reach adolescence and are soci-ally and intellectually educable, underscoring the need for proper medi-cal attendance. Although renal involvement is known from pathologicalstudies (e.g., renal cysts), functional renal impairment is uncommon. Peroxisome biogenesis is impaired in ZSDs, resulting in a loss of peroxi-somal functions, including the deficient ß-oxidation of certain fattyacids, notably hexacosanoic acid (C26:0) and pristanic acid as well asthe impaired formation of polyunsaturated fatty acids and plasmalo-gens (1). Survival is best predicted biochemically by the dihydroxyaceto-nephosphate acyltransferase (DHAPAT) activity and C26:0 ß-oxidationactivity as measured in fibroblasts (2). The genetic basis is heterogene-ous with 12 mutant PEX genes identified so far (3). The most commonc.2528 G>A mutation, which leads to an amino acid substitution at posi-tion 843 of the PEX1 protein (G843D), is generally associated with a mildphenotype (4-8). At the other end of the clinical spectrum, thec.2097_2098insT (null) mutation gives rise to a truncated PEX1 proteinand is associated with the classical Zellweger syndrome phenotype(9,10). Most peroxisomal enzymes are unstable in the cytosol which explains thefunctional deficiency of most peroxisomal enzymes in ZSD. A few enzy-mes, however, remain stable, among which alanine:glyoxylate amino-transferase (AGT; EC 2.6.1.44). This enzyme catalyzes the conversion ofglyoxylate to glycine. Mutations in the AGXT gene, occurring in the inhe-rited disorder of glyoxylate metabolism primary hyperoxaluria type 1(PH1), render the enzyme inactive, either by inactivating AGT directly orby mistargeting of AGT to mitochondria (11). The resulting excess gly-oxylate is either oxidized to oxalate or reduced to glycolate and excretedinto the urine. The resulting excess oxalate easily precipitates as calciumoxalate leading to the formation of urolithiasis, nephrocalcinosis, andrenal insufficiency (12,13). Pyridoxine administration reduces the uri-nary oxalate load in approximately 30% of the patients (14).
Over the past decade, several ZSD patients have been described withhyperoxaluria (6,15,16). To date, a systematic survey on the occurren-ce of hyperoxaluria in ZSDs has not been performed. Therefore, weundertook a cohort study in order to delineate the prevalence ofhyperoxaluria in patients with ZSDs and to find clinically relevant vari-ables that correlate with the severity of urinary oxalate excretion.
CHAPTER 06
page 84
VAN WOERDEN 5/19/08 8:53 AM Pagina 84

MATERIALS AND METHODS
Patient data were retrieved from a recently collected cohort of patientsdiagnosed between 1975 and 2002, comprising 31 Dutch ZSD patientswith survival beyond the first year of life (6). Clinical data were revie-wed, including data on renal ultrasounds and radiographies. The dia-gnosis was confirmed by appropriate studies in plasma (very-long-chain fatty acids, bile acid intermediates, pipecolic acid, phytanic acid,pristanic acid, and docosahexaenoic acid), erythrocytes (plasmalogenlevels), and fibroblasts (de novo plasmalogens biosynthesis, activity ofdihydroxyacetonephosphate acyltransferase (DHAPAT), oxidation ratesof C26:0, pristanic acid, and phytanic acid, immunoblot analysis ofacyl-CoA oxidase and peroxisomal thiolase, and immunofluorescencemicroscopy analysis of catalase), followed by complementation studiesand molecular analysis of the relevant PEX gene in most cases.Neurological development was assessed by using the compound deve-lopmental score (CDS) as designed and published previously (6). Thisscore is a measure of the development of statural motor control, handcontrol, verbal development, and visual development. A maximum of10 points may be given to patients with appropriate development onall aspects of the score. For patients under the age of four, a generalassessment of neurological development was made, as the CDS canonly be used for patients over four years of age.
Urinary oxalate levels were assayed by ion chromatography and urina-ry glycolate levels by gas chromatography. Urinary levels exceeding 54mmol oxalate/mol creatinine and 140 mmol glycolate/mol creatinine,respectively, were considered as elevated. Age related reference valueswere used as determined by Reusz et al. (17). For patients with prima-ry hyperoxaluria the median urinary oxalate level is 185 (range 60-600)mmol/mol creatinine and the median urinary glycolate level is 345(range 180-1740) mmol/mol creatinine as detected in our laboratory.The DHAPAT activity and C26:0 ß-oxidation in fibroblasts and plasmalevels of C26:0 were investigated for potential predictive value withrespect to neurological development as expressed by the compounddevelopmental score. Mutations in the PEX genes were investigated fortheir association with neurological development and hyperoxaluria.
For analysis, patients were categorized with respect to developmentaloutcome into a group of poor (CDS!5) and favorable (CDS>5) outcome.The correlation of the different biochemical markers and the neurologi-cal development between the two groups was evaluated using the Mann-Whitney U test. Additionally, dichotomous variables were composedregarding presence or absence of hyperoxaluria. The Fischer’s Exact Testwas used to analyze the association between neurological developmentand hyperoxaluria. Statistical package used was SPSS 11.5.1 Statistics UK.
Patients
Biochemicaland genetic
analysis
Statistical analysis
CHAPTER 06
page 85
VAN WOERDEN 5/19/08 8:53 AM Pagina 85

RESULTS
Urinary tract symptoms were recorded in five patients and consisted ofcolic pains, hematuria, and recurrent urinary tract infections (TABLE
06.1). Renal ultrasound was performed in 15 out of the 19 patients withhyperoxaluria. Urolithiasis or nephrocalcinosis were found in fivepatients. One of them (nr 1) underwent lithotripsy and another (nr 2)underwent surgical removal of kidney stones. In this patient, a hugeobstructing renal stone, causing extensive hydronephrosis withoutsigns of colic pains, was found by chance on an abdominal X-ray thatwas made in order to assess a scoliosis. In retrospect, hematuria hadalready been present in this patient. Renal function was preserved inall but one patient. This child (nr 1) died at 15 years of age due to theconsequences of end-stage renal disease. Four patients (nrs 2, 3 as wellas two others) suffered from recurrent episodes of diarrhea. Patient nr3 also suffered from steatorrhea.
a Plasma C26:0, reference range: 0.45-1.32 µM, C26:0/C22:0,
reference range: 0.0-0.02.
b NQ, not quantified.
c Reference range for oxalate < 54 mmol/mol creatinine
d Reference range for glycolate < 174 mmol/mol creatinine
e G843D genotype: (++) homozygous G843D; (+/-) heterozygous G843D.
f This patient is mutated in the PEX5 gene.CHAPTER 06
page 86
VAN WOERDEN 5/19/08 8:53 AM Pagina 86

Clinical, biochemical, and genetic characteristics of the five ZSD patientswith renal involvement
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5
15 11 2.8 1.3 4.3
+ - + + +
+ - + - +
- - - + -
+ + - - -
+ + + - -
+ + + - -
+ + + + +
+ + + + +
+ + + + +
+ - + + +
- + + + +
+ - + - +
+ - - - +
+ + + + +
- + + + -
+ + - - -
+ - - - -
3 5 Poor Poor 2
4.73 5.24 NQb 5.08 3.96
0.28 0.36 0.19 0.24 0.26
100 (90;110) 260 (30;540) 200 (200) 480 (310;740) 275 (230;390)
NQ 98 (5;353) 94 (94) 63 (37;134) 26 (15;41)
++ +/- --f ++ +/-
TABLE 06.1
Age at last
follow-up (years)
Death
Neonatal period
● Poor feeding
● Failure to thrive
Motor milestones
● Walks
● Stands with support
● Sits
Retinopathy
Extinguished ERG
Profound hearing
impairment
Epilepsy
Feeding problems
Urinary tract
complications
● Hematuria
● Urinary tract
infections
● Urolithiasis
● Nephrocalcinosis
● Hydronephrosis
● End-stage renal
disease
Compound
developmental score
Plasma very-long-
chain fatty acidsa
● C26:0
● C26:0/C22:0
Oxalate levels mean
(range) mmol/mol
creatininec
Glycolate levels mean
(range) mmol/mol
creatinined
Genotype
G843De
VAN WOERDEN 5/19/08 8:53 AM Pagina 87

Urinalysis was performed in 23 (74%) of the 31 patients. The remainingeight patients had died. In 19 (83%) of these 23 patients hyperoxaluriawas detected at least once, with hyperglycolic aciduria in 12. Sixpatients had isolated hyperoxaluria and two had isolated hyperglycolicaciduria. Two patients had completely normal oxalate and glycolatelevels. Glycolic acid was not measured in one patient with hyperoxalu-ria. Urinary oxalate and glycolate levels did not change consistentlywith progression of the disease over time. All 11 patients with a poorneurological development had hyperoxaluria. A representation of oxa-late and glycolate measurements as compared to the degree of neuro-logical dysfunction is shown in FIGURE 06.1. A poor neurological deve-lopment was statistically significant correlated with elevated levels ofurinary oxalate (Kendall’s tau-b coefficient = 0.44, p = 0.015). The acti-vity of hepatic AGT was assessed in one patient (nr 2) and was foundto be normal. For peroxisomal C26:0 ß-oxidation and plasma levels ofC26:0 a correlation was found with the degree of neurological deve-lopment (p = 0.02 and p = 0.01, respectively) but not for DHAPAT acti-vity and neurological development (p = 0.438).
Representation of urinary oxalate and glycolate for all ZSD patients,categorized for the degree of neurological dysfunction. Patients with a mild degree of neurological development are shown on the left part of the X-axis and patients with a severe degree of neurological development on the right side. ( - - - - - - - - ) Upper level of reference values for urinary oxalate. ( _______ ) Upper level of reference values for urinary glycolate. Dots (●) represent urinary oxalate.Diamonds (◆) represent urinary glycolate.
FIGURE 06.1
CHAPTER 06
page 88
VAN WOERDEN 5/19/08 8:53 AM Pagina 88

Genetic analysis revealed that the mild c.2528 G>A mutation in thePEX1 gene was present in 13 out of 23 patients: seven in the group witha favorable neurological development and six in the group with a poorneurological development. The other patients had other, less commonmutations.
Pyridoxine was administered to six of the 19 ZSD patients with hyper-oxaluria but did not result in a decline of oxalate excretion. None of thepatients received vitamin C supplementations at the time of oxalatemeasurements. Detection of hyperoxaluria was irrespective of diarrheaepisodes.
DISCUSSION
This is the first systematic survey on the prevalence of hyperoxaluriain a cohort of patients with Zellweger spectrum disorders. Our resultsshow that hyperoxaluria is a common finding in ZSD patients. The hig-hest levels of urinary oxalate in the ZSD patients as described in thispaper equal the levels found in patients with primary hyperoxaluriatype 1. In addition, levels of urinary glycolate are mostly raised albeitto a lesser extent as compared to patients with primary hyperoxaluria.In addition, urinary tract involvement was always accompanied byhyperoxaluria. Hyperoxaluria in patients with ZSD resulted in signifi-cant clinical morbidity and even mortality. Lithotripsy was mandatoryin one patient and one patient required surgical intervention for stoneremoval. End-stage renal disease, most probably caused by hyperoxa-luria, developed in another patient.
In four patients, intermittent diarrhea was seen in combination withhyperoxaluria. Patients with malabsorption syndromes can displayhyperoxaluria due to elevated enteric oxalate uptake (18. We excludedthis pathophysiological mechanism in our cohort, as oxalate excretiondid not vary with stool pattern. A high intake of vitamin C may alsoresult in a high urinary oxalate excretion (19). However, as none of thepatients received vitamin C supplementations during our study, we canexclude this as a confounding factor.In most of the patients with ZSD and hyperoxaluria, glycolic acid wasalso raised up to levels seen in PH1. As detected in one of our patientsand reported before in others, AGT activity is normal at least whenmeasured in total liver homogenates of ZSD patients (15,20).Apparently, the absence of normal compartmentalization of AGT inperoxisomes as a result of the defective import machinery leads to animpairment in glyoxylate metabolism. In ZSD patients with hyperoxa-luria, at least part of the produced glyoxylate was not converted intoglycine by AGT but appeared to be converted into oxalate probably bythe cytosolic enzyme lactate dehydrogenase (FIGURE 06.2).
CHAPTER 06
page 89
VAN WOERDEN 5/19/08 8:53 AM Pagina 89

Reactions involved in oxalate synthesis in man. In controls, AGT converts glyoxylate into glycine. In ZSD patients, peroxisomes areabsent and AGT is localized in the cytosol. AGT, alanine:glyoxylate aminotransferase; DAO, D-amino acid oxidase; GO, glycolate oxidase;GR/HPR, glyoxylate reductase/hydroxypyruvate reductase; LDH, lactate dehydrogenase.
We found a statistically significant positive relation between the sever-ity of the disease, as expressed by the compound developmental score,on the one hand, and the presence of hyperoxaluria on the other hand.Apparently there is a relative preservation of both neurological functi-ons as well as of functional AGT activity in some patients suggesting acommon mechanism. This could be due to functional AGT activity out-side the peroxisome or some residual AGT import in peroxisomes inmildly affected patients. Other, yet unknown, genetic or environmentalfactors may influence the functional activity of some of the peroxiso-mal enzymes when localized in the cytosol. Further studies are neces-sary to address these hypothetical mechanisms. The identification ofC26:0 ß-oxidation in fibroblasts and levels of C26:0 in plasma as aprognostic marker for neurological development further supports thehypothesis that a variable degree of cellular dysfunction underliesboth the clinical heterogeneity and the heterogeneity with respect tourinary oxalate levels.
The equal presence of the mild c.2528 G>A mutation in both the mildand the severe patient groups shows that the genotype in patients withZSD cannot predict outcome, either clinically as expressed by the levelof neurological dysfunction, or biochemically as expressed by the levelof urinary oxalate. The frequencies of the genotypes of the otherpatients were too low to draw conclusions.
FIGURE 06.2
CHAPTER 06
page 90
VAN WOERDEN 5/19/08 8:53 AM Pagina 90

Our results strongly indicate the need for periodic urinalysis in allpatients with ZSDs immediately after diagnosis has been made. As col-lection of a 24-h sample of urine can be difficult in patients with seve-re developmental delay and poor bladder control, one should be awareof potential sample errors if only small collections of urines are used(21). Therefore, repeated tests may be necessary. If hyperoxaluria isdetected, sufficient fluid intake in combination with oral citrate aremandatory in order to try to prevent formation of calcium oxalate andthus of renal stones and nephrocalcinosis. In addition, it is importantto search for urolithiasis or nephrocalcinosis in ZSD patients by meansof abdominal ultrasound, in order to initiate appropriate therapy asearly as possible trying to prevent further renal damage.
REFERENCES
CHAPTER 06
page 91
1. Wanders RJ. Metabolic and
molecular basis of peroxisomal disor-
ders: a review. Am J Med Genet A
2004;126:355-75.
2. Gootjes J, Mooijer PA, Dekker C,
Barth PG, Poll-The BT, Waterham HR,
Wanders RJ. Biochemical markers
predicting survival in peroxisome
biogenesis disorders. Adv Exp Med
Biol 2003;544:67-68.
3. Shimozawa N, Tsukamoto T,
Nagase T, Takemoto Y, Koyama N,
Suzuki Y et al. Identification of a new
complementation group of the peroxi-
some biogenesis disorders and PEX14
as the mutated gene. Hum Mutat
2004;23:552-58.
4. Gartner J, Preuss N, Brosius U,
Biermanns M. Mutations in PEX1 in
peroxisome biogenesis disorders:
G843D and a mild clinical phenotype.
J Inherit Metab Dis 1999;22:311-13.
5. Geisbrecht BV, Collins CS,
Reuber BE, Gould SJ. Disruption of a
PEX1-PEX6 interaction is the most
common cause of the neurologic
disorders Zellweger syndrome, neo-
natal adrenoleukodystrophy, and
infantile Refsum disease. Proc Natl
Acad Sci USA 1998;95:8630-35.
6. Poll-The BT, Gootjes J, Duran M,
De Klerk JB, Wenniger-Prick LJ,
Admiraal RJ et al. Peroxisome bio-
genesis disorders with prolonged
survival: phenotypic expression in
a cohort of 31 patients. Am J Med
Genet A 2004;126:333-38.
7. Reuber BE, Germain-Lee E,
Collins CS, Morrell JC, Ameritunga R,
Moser HW et al. Mutations in PEX1 are
the most common cause of peroxisome
biogenesis disorders. Nat Genet
1997;17:445-48.
8. Walter C, Gootjes J, Mooijer PA,
VAN WOERDEN 5/19/08 8:53 AM Pagina 91

Portsteffen H, Klein C, Waterham HR et al.
Disorders of peroxisome biogenesis
due to mutations in PEX1: phenotypes
and PEX1 protein levels.
Am J Hum Genet 2001;69:35-48.
9. Collins CS, Gould SJ.
Identification of a common PEX1
mutation in Zellweger syndrome.
Hum Mutat 1999;14:45-53.
10. Maxwell MA, Nelson PV,
Chin SJ, Paton BC, Carey WF,
Crane DI. A common PEX1 frameshift
mutation in patients with disorders
of peroxisome biogenesis correlates
with the severe Zellweger syndrome
phenotype.
Hum Genet 1999;105:38-44.
11. Danpure CJ, Rumsby G.
Molecular aetiology of primary
hyperoxaluria and its implications
for clinical management.
Expert Rev Mol Med 2004;6:1-16.
12. Cochat P, Deloraine A, Rotily M,
Olive F, Liponski I, Deries N.
Epidemi-ology of primary hyper-
oxaluria type 1. Société de Néphro-
logie and the Société de Néphrologie
Pédiatrique. Nephrol Dial Transplant
1995;10 Suppl 8:3-7.
13. van Woerden CS, Groothoff JW,
Wanders RJ, Davin JC, Wijburg FA.
Primary hyperoxaluria type 1 in The
Netherlands: prevalence and outcome.
Nephrol Dial Transplant 2003;18:273-79.
14. van Woerden CS, Groothoff JW,
Wijburg FA, Annink C, Wanders RJ,
Waterham HR. Clinical implications of
mutation analysis in primary
hyperoxaluria type 1. Kidney Int
2004;66:746-52.
15. Danpure CJ, Fryer P,
Griffiths S, Guttridge KM, Jennings PR,
Allsop J et al. Cytosolic compart-
mentalization of hepatic alanine:
glyoxylate aminotransferase in
patients with aberrant peroxisomal
biogenesis and its effect on oxalate
metabolism.
J Inherit Metab Dis 1994;17:27-40.
16. Barth PG, Gootjes J, Bode H,
Vreken P, Majoie CB, Wanders RJ.
Late onset white matter disease in
peroxisome biogenesis disorder.
Neurology 2001;57:1949-55.
17. Reusz GS, Dobos M, Byrd D,
Sallay P, Miltenyi M, Tulassay T.
Urinary calcium and oxalate excretion
in children. Pediatr Nephrol 1995;9:39-44.
18. Emmett M, Guirl MJ, Santa
Ana CA, Porter JL, Neimark S,
Hofmann AF, Fordtran JS. Conjugated
bile acid replacement therapy reduces
urinary oxalate excretion in short
bowel syndrome. Am J Kidney Dis
2003;41:230-37.
19. Traxer O, Huet B, Poindexter J,
Pak CY, Pearle MS. Effect of ascorbic
acid consumption on urinary stone risk
factors. J Urol 2003;170:397-401.
20. Wanders RJ, van Roermund CW,
Westra R, Schutgens RB, van der Ende
MA, Tager JM et al. Alanine glyoxylate
aminotransferase and the urinary
excretion of oxalate and glycollate in
hyperoxaluria type I and the Zellweger
syndrome. Clin Chim Acta
1987;165:311-19.
21. Hargreave TB, Sali A, Mackay C,
Sullivan M. Diurnal variation in urinary
oxalate. Br J Urol 1977;49:597-600.
CHAPTER 06
page 92
VAN WOERDEN 5/19/08 8:53 AM Pagina 92

CHAPTER 07 Quantification of endogenous oxalate production in patients with primary hyperoxalu-ria type 1: a stable isotope method
Hidde H Huidekoper, Christiaan S van Woerden, Jaap W Groothoff,Marinus Duran, An FC Ruiter, Mariëtte T Ackermans, Hans P Sauerweinand Frits A Wijburg
Background Plasma oxalate concentration and urinary oxalate excre-tion have been shown inaccurate parameters to monitor endogenousoxalate production (EOP) in patients with primary hyperoxaluria type 1(PH1) and renal insufficiency. A reliable parameter is needed in thesepatients to evaluate the efficacy of therapeutic interventions.Therefore, we devised a stable isotope oxalate tracer method to quan-tify the rate of appearance of oxalate (Ra oxalate).
Methods Three adult patients with PH1 and three adult controlsubjects, all with a preserved renal function, were given a primed con-tinuous infusion of [1,2-13C]sodium-oxalate lasting eight hrs. Everyhour a blood sample was drawn and acidified to determine plasma [1,2-13C]oxalate enrichment. During tracer infusion all urine of the subjectswas collected to determine urinary oxalate excretion. Isotopic equili-brium was reached after 360 min of tracer infusion in the patients andafter 120 min in the control subjects.
Results Ra oxalate calculated from plasma [1,2-13C]oxalate enrich-ment at isotopic equilibrium was 0.031, 0.029 and 0.024 µmol/kg·min inpatients 1, 2 and 3, and 0.015, 0.017 and 0.016 µmol/kg·min in controlsubjects 1, 2 and 3, respectively. Urinary oxalate excretion was wellreflected by Ra oxalate in all three patients, but was lower than Ra oxala-te in controls. This suggests overestimation of Ra oxalate in control sub-jects, possibly due to in vitro oxalogenesis despite adequate plasma acidification.
Conclusion Ra oxalate is accurately determined in patients with PH1using our stable isotope method and may be used to monitor thera-peutic interventions in patients with PH1 and renal insufficiency.
ABSTRACT
CHAPTER 07
page 93
VAN WOERDEN 5/19/08 8:53 AM Pagina 93

INTRODUCTION
In primary hyperoxaluria type 1 (PH1) the liver specific peroxisomalenzyme alanine:glyoxylate aminotransferase (AGT; EC 2.6.1.44), whichcatalyzes the transamination of glyoxylate to glycine, is either deficientor mistargeted to mitochondria instead of peroxisomes (1). Alternatively,glyoxylate can be oxidized to oxalate, a non-functional end metabolite ofthe glycine oxidative pathway, which is then excreted in urine.Therefore, the deficiency or mistargeting of AGT causes an excess pro-duction of oxalate in patients with PH1, which may result in the forma-tion of a highly insoluble calcium-oxalate salt (2). This causes crystallu-ria, renal stone formation and nephrocalcinosis with a high risk forrenal insufficiency and eventually end-stage renal disease (3,4). As aconsequence of renal insufficiency calcium-oxalate accumulates in othertissues and organs, resulting in systemic oxalosis, which may finallyseverely damage organs such as heart, eyes, bone and skin (5). The pro-cess of systemic oxalosis starts when glomerular filtration rate (GFR)falls below 60 ml/min·1.73 m2 (6).
Only patients with specific gene mutations leading to Gly170Arg orPhe152Ile substitution in the AGXT gene encoding AGT have been shownto respond to pyridoxine supplementation with a decrease of urinaryoxalate excretion, probably because pyridoxal-5-phosphate is an essenti-al co-factor for AGT (7,8). Currently, the only therapeutic option for theother patients with PH1 is a liver transplantation in order to eliminatethe enzymatic defect of AGT, often combined with a kidney transplanta-tion to restore renal function. However, this procedure has significantmorbidity and mortality (9). Therefore, new therapeutic strategies areneeded aimed at reducing endogenous oxalate production (EOP) inpatients with PH1. Directions of interest include pharmacological inter-ventions in the glyoxylate pathway, hepatocyte cell transplantation,recombinant gene therapy and colonic degradation of endogenous oxa-late by Oxalobacter formigenes (10,11).
In order to evaluate therapy efficacy an appropriate marker is needed.It has been shown that plasma oxalate concentration may remain ele-vated up to years after liver transplantation, due to the wash-out ofaccumulated oxalate in tissues (9,12). Therefore, plasma oxalate con-centration is not a reliable marker for EOP in PH1, as is urinary oxalateexcretion in patients with renal insufficiency. Even in patients with PH1and a preserved renal function, elevated levels of plasma oxalate maymask the efficacy of treatment due to sustained hyperoxaluria. This isemphasized by a recent study in which no effect of OTZ, a potentialglyoxylate lowering agent, on urinary oxalate excretion could be detec-ted in two patients with PH1 (13), whereas this effect was demonstra-ted in healthy individuals (14).
CHAPTER 07
page 94
VAN WOERDEN 5/19/08 8:53 AM Pagina 94

The determination of the rate of appearance of oxalate (Ra oxalate) inplasma, reflecting both EOP and oxalate wash-out from tissues, shouldbe a more accurate parameter to evaluate therapy efficacy in patientswith PH1 and renal insufficiency. Several studies have quantified oxa-late production in patients with PH1 using 14C labeled oxalate (15-18),but this method is ethically not applicable in clinical practice becauseof the obvious disadvantage of using a radioactive tracer in vivo.Therefore, we developed a stable isotope dilution method to quantifyRa oxalate. In the present chapter this method is described.
MATERIALS AND METHODS
Three adult patients with PH1 were included in this study. Patients 2and 3 are siblings. AGT deficiency was established either by measure-ment of AGT activity in a liver biopsy specimen (19) or by mutationanalysis of the AGXT gene (7). The patients were compared with threehealthy adults. Renal function as assessed by GFR estimated fromserum creatinine (20) was lower in patients with PH1 than in controlsubjects, but still above the threshold at which systemic oxalosis progressively occurs (6). Patient 1 was pyridoxine responsive, whereaspatients 2 and 3 were not. Patient 2 was treated with hyperhydrationand supportive medication (magnesiumhydroxide and dihydro-tachysterol), whereas patient 3 was only treated with supportive medication.All studies were approved by the Institutional Review Board. All subjects gave informed consent prior to the studies.
Three days prior to the study all subjects maintained a low-oxalate dietto eliminate dietary influences during studies. All subjects startedfasting 12 hrs before the start of the study and remained fasted throug-hout the whole study. They were allowed to drink water ad libitum. Twointravenous catheters were inserted into an antecubital vein of eacharm. One catheter was used for administration of [1,2-13C]sodium-oxa-late (99% pure; Cambridge Isotope Laboratories, Cambridge, MA) andthe other for blood sampling. After collection of a baseline blood sam-ple to determine the background enrichment of [1,2-13C]oxalate inplasma, a primed continuous infusion of [1,2-13C]sodium-oxalate wasstarted. The priming bolus of [1,2-13C]sodium-oxalate was 0.11µmol/kg in patients and 0.011 µmol/kg in control subjects, and thecontinuous infusion rate of [1,2-13C]sodium-oxalate was 1.25nmol/kg·min in patients and 0.125 nmol/kg·min in control subjects.These infusion protocols were designed in order to reach a plasma [1,2-13C]oxalate enrichment of approximately 5%, based on previouslypublished data on urinary oxalate excretion (15, 17, 21). Infusion of[1,2-13C]sodium-oxalate was continued for 8 hrs in all subjects. Every hour a blood sample was drawn in order to determine
Study subjects
Study protocol
CHAPTER 07
page 95
VAN WOERDEN 5/19/08 8:53 AM Pagina 95

[1,2-13C]oxalate enrichment in plasma. Blood samples were collected inheparin Microtainers (Becton–Dickinson, Franklin Lakes, NJ, USA),which were immediately centrifuged at 3000 rpm for 10 min. Exactly 1ml of plasma was transferred into a glass tube containing 0.4 g sodiumchloride (in quadruple). Plasma was acidified with 37% hydrochloricacid in order to precipitate protein and in order to eliminate any pos-sible oxalate formation from ascorbate (22). Hereafter, the acidifiedplasma was stored at -20ºC until analysis.
Prior to initiation of [1,2-13C]sodium-oxalate infusion all subjects wereasked to void in order to empty their bladder. Hereafter, all urine wascollected from the subjects until the end of [1,2-13C]sodium-oxalateinfusion in order to calculate urinary oxalate excretion during studies.Urine was acidified immediately after collection and was stored at -20ºC until analysis.
Plasma oxalate concentration and [1,2-13C]oxalate enrichment:Plasma oxalate concentration and [1,2-13C]oxalate enrichment weredetermined in separate runs. Briefly, the acidified plasma was extrac-ted twice with 4 ml ethylacetate and dried under a stream of nitrogen.The O-t-butyldimethylsilyl-quinoxalinol derivative of oxalate was for-med with o-phenylenediamine and MTBSTFA/pyridine. An aliquot wasinjected into a GC/MS system (HP 6890 series GC system and 5973Mass Selective Detector, Agilent Technologies, Palo Alto, CA, USA).Separation was achieved on a CP-SIL 19CB capillary column (30 m x0.25 mm x 0.15 µm, Varian, Middelburg, The Netherlands). Selected ionmonitoring (EI), data acquisition and quantitative calculations wereperformed using the Agilent Technologies Chemstation software. Theoxalate derivative was monitored at m/z 333 for oxalate and m/z 335
TABLE 07.1
Analyticalmethods
CHAPTER 07
page 96
Subject characteristics
Subjects Sex Age Height Weight
y m kg
Patient 1 M 28.2 1.82 67.6
Patient 2 F 20.0 1.65 52.7
Patient 3 F 23.2 1.78 70.6
Control 1 M 30.6 1.79 63.0
Control 2 M 30.6 1.94 91.2
Control 3 F 22.3 1.75 68.0
VAN WOERDEN 5/19/08 8:53 AM Pagina 96

for [1,2-13C]oxalate. For quantification of the enrichment a standardcurve with known enrichments of [1,2-13C]oxalate was derivatized asdescribed before. Oxalate tracer/tracee ratio’s were calculated as des-cribed by B.W. Patterson et al (24). In order to measure plasma oxalate concentration, [1,2-13C]oxalate wasadded to the acidified plasma as an internal standard. A correction wasmade for the contribution of the tracer to the internal standard peak.Oxalate concentration in the plasma samples was then calculated froma standard curve with known concentrations of oxalate.Urinary oxalate and creatinine concentration: urinary oxalate concentration was determined by ion chromatography(Dionex-DX 300) (25). Urinary creatinine concentration was determinedusing spectrophotometry according to the Jaffé method.
Rates of oxalate appearance (Ra oxalate) and disappearance (Rd oxalate):Ra oxalate was calculated with Steele’s steady-state equation (26). In thepresence of isotopic steady-state Ra oxalate equals Rd oxalate and the-refore also reflects the rate of oxalate clearance from plasma.Rate of urinary oxalate and creatinine excretion: the rate of urinary oxa-late excretion (µmol/kg·min) was calculated by multiplying urinaryoxalate concentration (µmol/L) by total urinary volume (L), which wasthen divided by the collection time (min) and by bodyweight (kg) inorder to calculate the rate of urinary oxalate excretion in all subjects.The rate of urinary creatinine excretion (µmol/kg·min) was calculatedin the same way in all subjects.
Calculations
CHAPTER 07
page 97
Enzyme activity Mutation Plasma GFR†
(normal range)* analysis‡ creatinine
nmol/min·mg allele 1/allele 2 µmol/L ml/min
protein 1.73 m2
9.8 (135 – 179) ND 74 102.0
ND c.33_34insC / c.33_34insC 107 63.1
ND c.33_34insC / c.33_34insC 83 68.2
ND ND 56 144.5
ND ND 53 123.
ND ND 58 106.9
* Horvath et al Clin Chim Acta 1995;243(2):105-114
† van Woerden et al Kidney Int 2004;66(2): 746-752
‡ estimated from serum creatinine; Levey et al Clin Chem 2007;53(4): 766-772
ND = not determined
VAN WOERDEN 5/19/08 8:53 AM Pagina 97

RESULTS
Plasma enrichment of [1,2-13C]oxalate expressed as TTR (%) in all sub-jects is shown in FIGURE 07.1. An increase in TTR during studies wasobserved in all three patients until approximately 360 min of [1,2-13C]sodium-oxalate infusion. Hereafter, TTR reached a plateau in allthree patients. In the control subjects, TTR remained constant after120 min of [1,2-13C]sodium-oxalate infusion.
In all subjects, Ra oxalate was calculated using the mean TTR in theblood samples at t=360, t= 420 and t= 480 min. Ra oxalate was 0.031,0.029 and 0.024 µmol/kg·min in patients 1, 2 and 3, respectively. Incontrol subjects 1, 2 and 3 Ra oxalate was 0.015, 0.017 and 0.016µmol/kg·min, respectively.
Median (range) plasma oxalate concentration at isotopic equilibriumwas 8.6 (8.6-9.6), 11.3 (11.1-11.8) and 10.1 (9.8-10.7) µM in patients 1,2 and 3, and 3.2 (2.6-4.1), 3.7 (3.3-5.1) and 3.7 (3.4-4.2) µM in controlsubjects 1, 2 and 3, respectively.
Urinary oxalate excretion during [1,2-13C]sodium-oxalate infusion was0.035, 0.031 and 0.035 µmol/kg·min in patients 1, 2 and 3, and 0.002,0.005 and 0.004 µmol/kg·min in control subjects 1, 2 and 3, respective-ly. Urinary creatinine excretion during [1,2-13C]sodium-oxalate infusionwas 0.15, 0.16 and 0.14 µmol/kg·min in patients 1, 2 and 3, and 0.14,0.15 and 0.13 µmol/kg·min in control subjects 1, 2 and 3, respectively.
DISCUSSIONIn this paper a novel stable isotope dilution method is described inorder to quantify oxalate kinetics in plasma. This method may be usedas a parameter to evaluate the efficacy of therapeutic interventions inpatients with PH1 and renal insufficiency, since plasma oxalate con-centration and urinary oxalate excretion are not reliable parameters for
FIGURE 07.1
Plasma enrichment of[1,2-13C]oxalate
and Ra oxalate
Plasma oxalateconcentration
Urinary oxalate andcreatinineexcretion
CHAPTER 07
page 98
Plasma [1,2-13C]oxalate
enrichment expressed as
TTR (%) in patients with
PH1 (closed symbols) and
control subjects (open
symbols) during 8 hrs of
a primed continuous
[1,2-13C]sodium-oxalate
infusion.
INFUSION TIME (MIN)
TT
R
(%)
VAN WOERDEN 5/19/08 8:53 AM Pagina 98

endogenous oxalate production (EOP) in these patients.We used a primed continuous infusion of [1,2-13C]sodium-oxalate inorder to quantify Ra oxalate in both patients with PH1 and age matchedhealthy control subjects. Renal function was comparable in all subjectsas their urinary creatinine excretion rate was approximately similar.Previously, a single injection stable isotope method with [1,2-13C]sodi-um-oxalate has been described to quantify oxalate turn-over (27).However, single injection [14C]oxalate methods have been shown tooverestimate oxalate turn-over when compared to constant [14C]oxala-te infusion methods as with the former a non-negligible amount of tra-cer will already be excreted in urine prior to homogenous distributionof the tracer throughout the pool, causing an erroneously high calcula-ted rate of oxalate turn-over (15). In addition, numerous blood samplesare generally required to accurately calculate substrate turn-over inplasma from the decay in isotopic enrichment of single injection of asubstrate tracer. Therefore, we choose to device a primed continuousoxalate tracer method as this would be a more clinically applicablemethod to quantify Ra oxalate.After approximately 360 min of a primed continuous infusion of [1,2-13C]sodium-oxalate a steady-state in plasma isotopic enrichment wasreached in the patients with PH1. In control subjects, a steady-state inisotopic enrichment was already present after only 120 min of [1,2-13C]sodium-oxalate infusion. The latter is consistent with a previ-ous study using a primed continuous infusion of [14C]oxalate in heal-thy subjects (15). This difference in equilibration period betweenpatients and control subjects is caused by the higher metabolic pool ofoxalate (the product of plasma oxalate concentration and of oxalatedistribution volume) in patients with PH1 as compared to healthy sub-jects (6,17,18), as a steady-state in plasma [1,2-13C]-oxalate enrichmentcan only be achieved when the oxalate tracer has been evenly disper-sed throughout the whole metabolic pool. This also implicates that alonger equilibration period or a higher priming bolus of [1,2-13C]sodi-um-oxalate is needed in patients with PH1 and renal insufficiency.Ra oxalate calculated at isotopic equilibrium was in the same range inall three patients and closely resembled urinary oxalate excretion.Since GFR in the patients was above the threshold at which systemicoxalosis is suggested to occur (6), and almost all oxalate is cleared fromplasma by renal clearance (28), Ra oxalate was expected to equal urina-ry oxalate excretion. This is indeed reflected by our data. Furthermore,our data suggest that daily oxalate production in patients with PH1would amount to 2.55 mmol per day. This is in concordance with a pre-vious estimate of daily oxalate production in patients with PH1 (15).Finally, although a high variation in plasma oxalate concentration hasbeen reported in the patients with PH1, plasma oxalate concentrationin our patients as quantified with our method was consistent withreported data on plasma oxalate concentration in patients with PH1
CHAPTER 07
page 99
VAN WOERDEN 5/19/08 8:53 AM Pagina 99

with a preserved renal function (6,15,17). Therefore, Ra oxalate may beaccurately quantified in patients with PH1 after a primed continuousinfusion of [1,2-13C]sodium-oxalate lasting at least 360 min as descri-bed in the present chapter.In healthy control subjects, however, Ra oxalate was higher than expec-ted as it exceeded urinary oxalate excretion several fold. Daily oxalateproduction in healthy subjects would amount to 1.72 mmol per daybased on the Ra oxalate data and to 0.41 mmol per day based on theurinary excretion data. The latter is in good agreement with previousdata on daily urinary oxalate excretion in control subjects (15,17, 28).This suggests that Ra oxalate as determined by our method is overesti-mated. Furthermore, although a large variation has been reported inplasma oxalate concentration in healthy subjects, as summarized in arecent study describing a stable isotope dilution method to quantifyplasma oxalate and glycolate concentration in vitro (29), plasma oxala-te concentration as determined in our control subjects was in the hig-her reported range. The same dilemma was encountered in the studyof France et al who described a single injection [1,2-13C]sodium-oxala-te method to quantify Ra oxalate and found a daily oxalate productionrate of 1.89 mmol in a healthy subject (27). These authors contributedthis high production rate of oxalate to in vitro oxalogenesis from ascor-bate despite acidification of the plasma samples after collection. Wecannot rule out that some in vitro oxalogenesis from ascorbate occur-red before analysis of the samples as this has been shown to occur inacidified frozen urine during prolonged storage (23). If so, this willhave caused an overestimation of plasma oxalate concentration and ofRa oxalate in control subjects. Alternatively, urinary oxalate excretioncould have been underestimated in control subjects due to precipita-tion of oxalate with calcium in vitro. This seems less likely, however, asurinary super saturation is low in control subjects (30) and urinary aci-dification has been shown effective in preventing calcium-oxalate pre-cipitation (23). Since both Ra oxalate and plasma oxalate concentrationare higher in patients with PH1, the relative contribution of in vitro oxa-logenesis to total oxalate concentration in the plasma samples and Raoxalate is smaller in patients than in control subjects and is probablynegligible in patients with renal insufficiency exhibiting a much higherplasma oxalate concentration. To limit the influence of possible in vitrooxalogenesis on the determination of Ra oxalate and plasma oxalateconcentration, plasma samples should be immediately acidified andanalyzed as soon as possible after their collection.In conclusion, the reported stable isotope method to quantify Ra oxa-late seems accurate in patients with PH1, but not in control subjects.This method may be used to monitor therapeutic interventions inhyperoxaluric patients with renal insufficiency as plasma oxalate con-centration and urinary oxalate excretion are inaccurate parameters ofEOP in these patients.
CHAPTER 07
page 100
VAN WOERDEN 5/19/08 8:53 AM Pagina 100

REFERENCES
CHAPTER 07
page 101
1. Danpure CJ. Primary
Hyperoxa-luria. In: Scriver CR,
Beaudet AL, Sly WS, Valle D, eds. The
Metabolic and Molecular Bases of
Inherited Disease. New York:
McGraw-Hill, 2001:3323-67.
2. Zarembski PM, Hodgkinson A.
Plasma oxalic acid and calcium levels
in oxalate poisoning. J Clin Pathol
1967;20:283-85.
3. Milliner DS, Wilson DM, Smith LH.
Phenotypic expression of primary
hyperoxaluria: Comparative features
of types I and II. Kidney International
2001;31-36.
4. van Woerden CS, Groothoff JW,
Wanders RJ, Davin JC, Wijburg FA.
Primary hyperoxaluria type 1 in The
Netherlands: prevalence and outcome.
Nephrol Dial Transplant 2003;18:273-79.
5. Chaplin AJ. Histopathological
occurrence and characterisation of cal-
cium oxalate: a review. J Clin Pathol
1977;30:800-11.
6. Morgan SH, Purkiss P, Watts RW,
Mansell MA. Oxalate dynamics in chronic
renal failure. Comparison with normal
subjects and patients with primary
hyperoxaluria. Nephron 1987;46:253-57.
7. van Woerden CS, Groothoff JW,
Wijburg FA, Annink C, Wanders RJ,
Waterham HR. Clinical implications of
mutation analysis in primary hyperoxa-
luria type 1. Kidney Int 2004;66:746-52.
8. Monico CG, Rossetti S, Olson JB,
Milliner DS. Pyridoxine effect in type I
primary hyperoxaluria is associated
with the most common mutant allele.
Kidney Int 2005;67:1704-09.
9. Jamieson NV. A 20-year expe-
rience of combined liver/kidney trans-
plantation for primary hyperoxaluria
(PH1): the European PH1 transplant
registry experience 1984-2004.
Am J Nephrol 2005;25:282-89.
10. Bobrowski AE, Langman CB.
Hyperoxaluria and systemic oxalosis:
current therapy and future directions.
Expert Opin Pharmacother
2006;7:1887-96.
11. Hoppe B, Beck B, Gatter N, von
UG, Tischer A, Hesse A et al.
Oxalobacter formigenes: a potential
tool for the treatment of primary
hyperoxaluria type 1. Kidney Int
2006;70:1305-11
12. Monico CG, Milliner DS.
Combined liver-kidney and kidney-alone
transplantation in primary hyperoxaluria.
Liver Transpl 2001;7:954-63.
13. Holmes RP, Assimos DG, Wilson
DM, Milliner DS. (L)-2-oxothiazolidine-
4-carboxylate in the treatment of pri-
mary hyperoxaluria type 1. BJU Int
2001;88:858-62.
14. Holmes RP, Assimos DG, Leaf
CD, Whalen JJ. The effects of (L)-2-oxo-
thiazolidine-4-carboxylate on urinary
oxalate excretion. J Urol 1997;158:34-37.
15. Prenen JA, Boer P, Mees EJ,
Endeman HJ, Spoor SM, Oei HY. Renal
clearance of [14C]oxalate: comparison
of constant-infusion with single-injection
techniques. Clin Sci (Lond) 1982;63:47-51.
16. Prenen JA, Dorhout Mees EJ,
Boer P. Plasma oxalate concentration
and oxalate distribution volume in
patients with normal and decreased
VAN WOERDEN 5/19/08 8:53 AM Pagina 101

CHAPTER 07
page 102
renal function. Eur J Clin Invest
1985;15:45-49.
17. Watts RW, Veall N, Purkiss P.
Sequential studies of oxalate dynamics
in primary hyperoxaluria. Clin Sci
(Lond) 1983;65:627-33.
18. Watts RW, Veall N, Purkiss P.
Oxalate dynamics and removal rates
during haemodialysis and peritoneal
dialysis in patients with primary
hyperoxaluria and severe renal failure.
Clin Sci (Lond) 1984;66:591-97.
19. Horvath VAP, Wanders RJA.
Aminooxy acetic acid: A selective inhi-
bitor of alanine:glyoxylate aminotrans-
ferase and its use in the diagnosis of
primary hyperoxaluria type I. Clin
Chim Acta 1995;243;105-14
20. Levey AS, Coresh J, Greene T,
Marsh J, Stevens LA, Kusek JW, Van LF.
Expressing the Modification of Diet in
Renal Disease Study equation for esti-
mating glomerular filtration rate with
standardized serum creatinine values.
Clin Chem 2007;53:766-72.
21. Prenen JA, Boer P, van LL,
Oldenburg SJ, Endeman HJ. Urinary
oxalate excretion, as determined by iso-
tope dilution and indirect colorimetry.
Clin Chim Acta 1983;127:251-61.
22. Wilson DM, Liedtke RR. Modified
enzyme-based colorimetric assay of
urinary and plasma oxalate with
improved sensitivity and no ascorbate
interference: reference values and
sample handling procedures.
Clin Chem 1991;37:1229-35.
23. Mazzachi BC, Teubner JK,
Ryall RL. Factors affecting measure-
ment of urinary oxalate. Clin Chem
1984;30:1339-43.
24. Patterson BW, Zhao G, Klein S.
Improved accuracy and precision of gas
chromatography/mass spectrometry
measurements for metabolic tracers.
Metabolism 1998;47:706-12.
25. Blau N, Matasovic A, Lukasiewicz-
Wedlechowicz A, Heizmann CW,
Leumann E. Simultaneous determina-
tion of oxalate, glycolate, citrate, and
sulfate from dried urine filter paper
spots in a pediatric population.
Clin Chem 1998;44:1554-56.
26. Steele R. Influences of glucose
loading and of injected insulin on
hepatic glucose output. Ann N Y Acad
Sci 1959;82:420-30.
27. France NC, Holland PT, Wallace
MR. Contribution of dialysis to endoge-
nous oxalate production in patients
with chronic renal failure. Clin Chem
1994;40:1544-48.
28. Elder TD, Wyngaarden JB. The
biosynthesis and turnover of oxalate in
normal and hyperoxaluric subjects.
J Clin Invest 1960;39:1337-44.
29. Inoue Y, Masuyama H, Ikawa H,
Mitsubuchi H, Kuhara T. Monitoring
method for pre- and post-liver trans-
plantation in patients with primary
hyperoxaluria type I. J Chromatogr B
Analyt Technol Biomed Life Sci
2003;792:89-97.
30. van Woerden CS, Huidekoper
HH, Groothoff JW, Wijburg FA, Duran M.
Postponing urine acidification for 24 h
does not change the oxalate concentra-
tion. Clin Chim Acta 2007;384:184-85.
VAN WOERDEN 5/19/08 8:53 AM Pagina 102

CHAPTER 08. Oxalate production in Agxt -/- mice Hepatocytesduring incubation with potential sources of glyoxy-late metabolism suggests additional routes for glyoxylate detoxification
Christiaan S van Woerden, Jos P Ruiter, Lia EM van Lint, Jaap W Groothoff,Frits A Wijburg, Marinus Duran, Ronald JA Wanders, Eduardo C Salido
Introduction. Excess oxalate production results in renal sequelae inpatients with primary hyperoxaluria type 1 (PH1), due to deficiency ofthe liver-specific peroxisomal enzyme alanine:glyoxylate aminotrans-ferase (AGT). Oxalate is produced from glyoxylate. To date, the absolu-te contribution of potential precursors of glyoxylate has been investi-gated in various models, among which HepG2 cells and wild type ani-mal hepatocytes but not in an in vitro model for PH1. Recently, a mousemodel, deficient in peroxisomal AGT activity, has been generated. It isbiochemically comparable to human PH1, exhibiting elevated urineoxalate excretion. We used this model to investigate the in vitro oxala-te production upon incubation with different potential precursors.Methods. Metabolic incubation studies were performed in isolatedhepatocytes of Agxt -/- and wild type mice. Experiments were perfor-med in alanine depleted and alanine enriched media (10mM). Seven dif-ferent potential precursors were used, including glyoxylate, glycolate,glycine, L-serine, hydroxyproline, xylitol and fructose. Production ofoxalate and glycolate was measured by gas chromatography-massspectrometry (GC-MS) and glycine production by high-pressure liquidchromatography (HPLC).Results. Incubation of wild type hepatocytes with glyoxylateresulted in a production of 4% oxalate and 8% glycolate. Incubation ofAgxt -/- hepatocytes with glyoxylate resulted in a production of 2% oxa-late and 4 % glycolate of the initial total amount of the precursor. Noneof the other precursors resulted in the formation of oxalate or glycola-te. Production rate was decreased in wild type cells upon addition of10mM alanine but not in Agxt -/- cells. In alanine-enriched media, gly-cine synthesis was lower in Agxt -/- cells compared to wild type cells,but not zero. Depletion of alanine resulted in complete inhibition ofglycine synthesis in both cell types.Conclusion. Except for glyoxylate and glycolate, none of the propo-sed glyoxylate precursors contributes to in vitro oxalate production.Incubation studies in Agxt -/- hepatocytes show modest fluxes throughthe glyoxylate pathway. In view of sustained glycine synthesis uponalanine addition and moderate oxalate excretion, our studies support apotential role for a second, potentially mitochondrial, AGT mediatedglyoxylate metabolism, at least in mice.
ABSTRACT
CHAPTER 08
page 103
VAN WOERDEN 5/19/08 8:53 AM Pagina 103

INTRODUCTION
Oxalate overproduction is the biochemical hallmark of primary hyper-oxalurias. Oxalic acid complexes with calcium ions, resulting in thedeposition of insoluble calcium oxalate crystals, notably in the kidneys.Primary hyperoxaluria type 1 (PH1) results from the deficiency of alani-ne:glyoxylate aminotransferase, AGT (FIGURE 08.1). The liver specificperoxisomal enzyme alanine:glyoxylate aminotransferase (AGT) nor-mally converts toxic glyoxylate into glycine. Mutations in the AGXT genecause AGT deficiency in PH1 after which glyoxylate is diverted in twoways: (1) the peroxisomal enzyme glycolate oxidase (GO, Km 0,2 mM. asstudied by Schwam et al (1) oxidizes glyoxylate into oxalate as does thecytosolic enzyme lactate dehydrogenase (LDH) and (2) glyoxylate reduc-tase (GR) reduces glyoxylate into glycolate. For a genetically specifiedsubgroup of patients with primary hyperoxaluria type 1, a reduction ofurinary oxalate by suppletion of pharmacological doses of pyridoxine,which is a co-factor of AGT, results in a decreased urinary excretion ofoxalate and a clinically relevant longer preservation of kidney function(2). Unfortunately, pyridoxine responsiveness is only observed in 35-40%of the patients. Correction of the enzymatic defect is otherwise onlyachieved by a liver transplantation, subject to compatible organ supply,with its major drawback of life long requirement of immunosuppressivetherapy that causes transplantation related morbidity. Therefore, thereis an urgent need for better therapy.
One of the potential therapeutic approaches might be by dietary modi-fications or pharmacological interventions that divert or alter metabo-lic pathways. Ideally, these interventions will decrease availability ofsubstrates that result in the formation of disease-causing metabolites.For the primary hyperoxalurias however, the pathways leading to oxa-late synthesis are only partly understood. A clear understanding ofthese metabolic pathways is a prerequisite for the design of alternati-ve therapies. Studies providing insight into the biochemistry of oxala-te metabolism are limited especially because oxalate metabolism onlyoccurs in hepatocytes, and hepatocytes cell lines of patients with pri-mary hyperoxaluria are not available for research. Recently, an Agxt -/-
mouse, deficient for the peroxisomal AGT enzyme, has been developed.We initiated the current research project to investigate the contributionof potential precursors to oxalate production by means of incubationstudies in isolated hepatocytes of Agxt -/- mice.
Fluxes through the glyoxylate pathway with its relevant enzymes.FIGURE 08.1
VAN WOERDEN 5/19/08 8:53 AM Pagina 104

MATERIALS AND METHODS
Agxt -/- mice were generated as described previously (3). Genetic ana-lysis of the AGXT gene was performed prior to the experiments toascertain the desired genotype was obtained.
Mice were anaesthetized using pentobarbital, and subjected to laparot-omy. A 24 Gauge canula was inserted in the portal vein, and the liver wasfirst perfused with Hepes buffer at pH 7,4 and afterwards with collage-nase (50mg/100ml) in Hepes buffer. Liver cells were harvested inWilliams medium and washed for three consecutive times. After eachwash step, cells were spun for five minutes at 300 rpm and the pellet wasresuspended in 50 ml Williams medium. After the last washing step, cellnumbers were calculated manually and using a Coulter Counter(Beckman Coulter, Inc. 2007). Viable cells were resuspended in Krebssolution and enough buffer was added to generate a concentration of onemillion cells per milliliter prior to the start of the incubation studies.
Experiments were performed in Eppendorf tubes (2 ml) at 0ºC untiladdition of the precursors. Incubation of the samples was performedfor one hour at 37ºC, and gently shaken during incubation. The incu-bations were stopped by adding 20 µl of HCl 30%. Samples were storedat -20ºC until analysis.
For every precursor, an extra sample was taken separately and acidifiedimmediately upon its preparation, to measure background levels ofoxalate, glycolate and glycine. In the same way, two separate samples,one containing Agxt -/- and one containing wild type hepatocytes wereacidified before incubation to measure background activity. Sevenpotential precursors were chosen and prepared in five different con-centrations (0.25, 0.5, 1.0, 5.0 and 10.0 mM) for incubation, includingglyoxylate, glycolate, glycine, L-serine, hydroxyproline, xylitol andfructose. Experiments were performed in alanine depleted and alanineenriched (10mM) media.
Hepatocytes
CHAPTER 08
page 105
VAN WOERDEN 5/19/08 8:53 AM Pagina 105

Oxalate, glycolate
Concentrations of oxalate and glycolate were measured by gas chro-matography-mass spectrometry (GC-MS) in one run.Chemicals[1,2-13C]oxalate and D2-glycolate were from Cambridge IsotopeLaboratories. MTBSTFA and ethyl acetate were from Sigma Aldrich.
Preparation and GC-MS analysis
All samples were thawed and centrifuged at 4ºC for five minutes at14000 rpm. With slight modifications of the procedure, solvent extrac-tion with ethyl acetate and trimethylsilylation was performed as des-cribed previously (4). For derivatization, 50 µl sample was used. Of asaturated solution of NaCl 50 µl was added to enhance extraction.Internal standards for oxalate and glycolate determination were comb-ined in 100 µl distilled water and added to the medium. Extraction wasperformed two times using 2.5 ml ethyl acetate. The pooled ethyl ace-tate fractions were evaporated under N2 at room temperature.Derivatization was performed using 80 µl MTBSTFA at 80ºC for 30minutes. After cooling, 1 µl of sample was injected into the gas chro-matograph (Hewlett Packard). Runtime was 30 minutes.
Gas chromatography-Mass spectrometry
A MSD 5973N mass spectrometer, coupled to a GC6890N gas chroma-tograph (Hewlett Packard) was used according to the manufacturer’sprotocol. A CPsil-19CB column, (25mtr*0.25mm*0.20µm) was used.
The gas chromatographic conditions were as follows: carrier gas heli-um, injection temperature: 300 °C, split ratio 1:10 column flow rate: 1.8ml/min. Oven program: 80 °C for 1.5 min, followed by 10°C/min until200 °C is reached. Then 30 °C/min until 250°C for five minutes.Quantization was performed by SIM. The ions at m/z 261 and 263 wereused for oxalate and its internal standard, and the ions at m/z 247 andm/z 249 were used for glycolate and its internal standard. A correcti-on of 10% was made for the quantitation of oxalate and glycolate,because endogenous and labelled compounds both contribute signifi-cantly to the other ions.
For validation, the same sample was measured 10 consecutive times,yielding a standard deviation of 0.05 µM for oxalate and 0.14 µM forglycolate. Variation coefficients were 1.02% for oxalate and 1.32% forglycolate. Linearity was observed at least until a spiked concentrationof 100 µM for oxalate and glycolate (R2 = 1). Recovery was 113% foroxalate and 91% for glycolate.
Product analysis
CHAPTER 08
page 106
VAN WOERDEN 5/19/08 8:53 AM Pagina 106

Glycine
Glycine was analyzed by derivatization using a HPLC procedure, asdescribed previously. Samples were thawed and centrifuged at 4ºC forfive minutes at 14000 rpm. 25 µl of supernatans was diluted with 140µl of distilled water and neutralized with 10 µl 2M KOH/ 0.6 M MOPS.This sample was used for HPLC analysis.
RESULTS
We were able to detect low amounts of oxalate, with a detection limitof 0.5 µM by using GC-MS. Background levels of oxalate and glycolatein wild type and Agxt -/- cells were similar. For glycine measurements,the established HPLC procedure was used and proved highly reliableunder the current conditions, with excellent calibration curves.
Up to 8% of added glyoxylate was converted into glycolate and 4% intooxalate for wild type isolated hepatocytes, whereas the production ofglycolate and oxalate was reduced in Agxt -/- knockout hepatocyteswith 3% (glycolate) and 2% (oxalate) produced from glyoxylate. Additionof alanine resulted in a decreased production of oxalate and glycolatein both wild-type and AGT deficient hepatocytes, though reduction wasmore pronounced in the wild type hepatocytes (FIGURE 08.2 and 08.3).Glycine was formed in wild type hepatocytes and to a lesser extent inAgxt -/- hepatocytes. Addition of alanine strongly enhanced glycine pro-duction in both cell types (FIGURE 08.4).
Oxalate production during incubation of wild type and Agxt -/-
hepatocytes with glyoxylate.
Highest glycolate concentration for wild type cells is 398 µM
and for Agxt -/- cells is 227 µM.
Open bars: wild type hepatocytes
Dashed bars: Agxt -/- hepatocytes
Glyoxylateincubation
FIGURE 08.2
CHAPTER 08
page 107
VAN WOERDEN 5/19/08 8:53 AM Pagina 107

Glycolate production during incubation of wild type and Agxt -/- hepatocytes with glyoxylate.
Highest glycolate concentration for wild type cells is 791 µM and for Agxt -/- cells
is 292 µM. Open bars: wild type hepatocytes Dashed bars: Agxt -/- hepatocytes
Glycine production during incubation of wild type and Agxt -/- hepato-cytes with glyoxylate, in alanine depleted and alanine enriched media.
Open bars: wild type hepatocytes
Dashed bars: Agxt -/- hepatocytes
Glycine production during incubation with different precursors. The first bar in each category represents experiments with 10 mM alanine, and the second bar during alanine depletion.
FIGURE 08.3
FIGURE 08.4
FIGURE 08.5
CHAPTER 08
page 108
VAN WOERDEN 5/19/08 8:53 AM Pagina 108

A low amount of oxalate was produced during glycolate and 4-hydro-xyproline incubation. Only for wild type cells, the amount was lowerafter addition of alanine, but not for Agxt -/- cells. Glycolate producti-on was also raised upon loading with 4-hydroxyproline. Comparableamounts of glycine were formed in glycolate incubated cells, and ala-nine increased its synthesis to the same extent (concentrations 25 µMin alanine depleted and 45 µM in alanine enriched experiments). For 4-hydroxyproline loading, elevated concentrations of glycine were obser-ved in wild type cells, that did only slightly respond to alanine addi-tion (61 and 70 µM, respectively). A low concentration of glycine wasobserved in Agxt -/- cells without any influence of alanine (15 µM).
For the other compounds, slightly raised glycolate production wasobserved, but not at all for oxalate. For glycine and fructose incuba-tion, addition of alanine resulted in lower glycolate concentrations inwild type cells but not in Agxt -/- cells. For L-serine, glycolate producti-on was higher in wild type cells that were stimulated with alanine. Forxylitol incubations, addition of alanine resulted in higher glycolateconcentrations in both types of cells. Lowest concentrations of glycinewere seen in wild type cells upon incubation with xylitol and fructose.Agxt -/- cells did not show glycine production with any of these two pre-cursors. Serine incubation resulted in the second highest glycine con-centration (112 µM for wild type and 79 µM for Agxt -/- cells) with onlysmall change after alanine addition (123 µM for wild type and 55 µMfor Agxt -/- cells).
DISCUSSION
We investigated the production of oxalate, glycolate and glycine inhepatocytes of wild type mice and compared them with their producti-on in Agxt -/- mice, a recently developed genetically modified animalmodel for primary hyperoxaluria type 1, during incubation with vari-ous naturally occurring potential precursors of glyoxylate, oxalate andglycolate. Because oxalate and glycolate are both end products of gly-oxylate metabolism, which is defective in primary hyperoxaluria type1, the measurement of oxalate and glycolate serves as an indicator ofglyoxylate metabolism. The quantification of glycine was performed toanalyze any persistent normal flux through the glyoxylate pathway.
Concerning the detection of oxalate and glycolate, we were able to mea-sure small concentrations by means of gas chromatography-mass spec-trometry in the same run. Stable isotopes of oxalate and glycolate wereused as internal standards, which makes the procedure very specificand accurate. Linearity was excellent (R2 = 0.99), Recovery for oxalatewas 133%, variation coefficient 5.2%, and recovery for glycolate was90%, with a variation coefficient of 3.2%. Limit of detection was 0.5 µM
Glycolate and4-hydroxy-
proline incubation
Glycine, L-serine,
xylitol, fructose
CHAPTER 08
page 109
VAN WOERDEN 5/19/08 8:53 AM Pagina 109

for oxalate and 1.5 µM for glycolate. In patients with primary hyper-oxaluria type 1, plasma concentrations of oxalate and glycolate areusually in the same range (5) . With the current method we were able todiscriminate between low variations in oxalate and glycolate producti-on rates.
In Agxt -/- mice and in human primary hyperoxaluria type 1, levels ofurinary oxalate excretion are three to four times the upper limit of thereference range (3). Surprisingly, only a modest production of oxalatewas observed in hepatocytes of Agxt -/- mice after exposure with any ofthe precursors. Even wild type hepatocytes produced more oxalate andespecially more glycolate, if depleted for the co-substrate alanine. Thisdifference between wild type cells and Agxt -/- hepatocytes might bedue to differences in viability of the cells. However, in previous expe-riments with wild type mice hepatocytes, we assessed viability of thecells prior to our experiments (results not shown). Since our procedu-res always resulted in good viability of the cells, we did not test for via-bility in the knockout mice hepatocytes, in order not to lose any cells.Before proceeding to the metabolic studies, we analyzed the cellsunder the microscope for manual counting. During this procedure, there was no evidence of potential loss of via-bility of cells. Moreover, addition of alanine during the incubation,which is the co-substrate of the enzyme alanine:glyoxylate amino-transferase (AGT), resulted in a change in production of metabolites,suggesting that viability was not decreased.
Upon addition of alanine a pronounced decrease of oxalate and glycolate production was seen in wild type cells, but to a much lessextent in Agxt -/- cells. On the other hand, depletion of alanine resultedin almost absent glycine production. The strong influence of alanine inthese experiments points towards the existence of residual AGT activity in the livers of Agxt -/- mice. As demonstrated before, no AGTactivity is present in peroxisomal fractions of these mice (3). However,additional AGT2 activity in mitochondria of the mice may be found,like in HepG2 cells (6). Therefore, the absence of excess oxalate andglycolate production in Agxt -/- hepatocytes, and the sustained glycinesynthesis upon addition of its co-substrate alanine, would suggest thatmitochondrial AGT2 contributes significantly and is capable of detoxi-ficating precursors of glyoxylate metabolism, at least in the experi-mental system used in this study. These precursors may not have reached the peroxisomal matrix, therefore not leading to oxalate pro-duction. The biochemical phenotype of primary hyperoxaluria withexcess production of oxalate, results from exclusively peroxisomal oxalate generation, and any precursor of glycolate, glyoxylate or oxalate must be imported or synthesized in the peroxisomal compart-ment to contribute to this biochemical phenotype.
CHAPTER 08
page 110
VAN WOERDEN 5/19/08 8:53 AM Pagina 110

Whether the addition of alanine also results in decreased oxalate production in vivo may be addressed by adding alanine tot the diet ofAgxt -/- mice. We did not yet perform such experiments.
Glycolate production was much higher in wild type cells. Since glyoxy-late is reduced to glycolate by the enzyme glycolate reductase, the pro-duction of glycolate in wild type cells was not expected to be higherthan in Agxt -/- hepatocytes. Alternatively, the cytosolic enzyme gluta-mate:glyoxylate aminotransferase (GGT) may also catalyze the conver-sion of glyoxylate into glycine. However, a clear response upon alaninewas found, suggesting that this enzyme did not contribute to the pro-duction of glycine or decreased oxalate formation.
If mitochondria significantly contribute to glyoxylate detoxification,this may also explain the high amount of glycine as was found in Agxt -/-
hepatocytes, almost equaling glycine production in wild type hepatocy-tes. Wild type cells metabolized approximately 140% of glycine found inAgxt -/- hepatocytes. This likely reflects the synthesis of glycine in bothmitochondria as well as peroxisomes, whereas Agxt -/- hepatocytes onlymetabolize glyoxylate via mitochondria. The clinical importance of this pathway has been discussed by Baker etal, who proposed an important role for mitochondrial glyoxylate meta-bolism regarding the breakdown of collagen during the turnover of vari-ous tissues (6). The results of our experiments are in line with thishypothesis.
During incubation with L-serine, knockout hepatocytes showed a glyci-ne production which was 50% of glycine synthesis in wild type cells.This may be the result of absence of peroxisomal AGT activity. Apartfrom glyoxylate detoxification, the AGT enzyme has a dual function asit also demonstrates serine:pyruvate transaminase (SPT) activity. As anSPT, the enzyme converts serine into hydroxypyruvate in peroxisomesand mitochondria (7). This could lead to glycine production (FIGURE.08.6), as proposed by Holmes and Assimos (8). In the absence ofperoxisomal AGT/ SPT activity, serine can only be metabolized viamitochondrial AGT/SPT mediated pathways. Therefore, wild type cellsproduce more glycine, as was demonstrated in our experiments. On theother hand, there is also a higher production of oxalate and glycolatein cells that were exposed to L-serine. This implies that the fluxthrough this AGT/SPT mediated pathway is high enough to generateglycine, glycolate and oxalate. The low oxalate and glycolate concen-trations in Agxt -/- hepatocytes illustrates a generally lower flux of seri-ne metabolism, since the peroxisomal route is not functional. For glycine as a precursor, the absence of oxalate production in wildtype and knockout hepatocytes is in line with the reported lack ofD/amino acid oxidase expression in the mouse liver (9).
CHAPTER 08
page 111
VAN WOERDEN 5/19/08 8:53 AM Pagina 111

With the current experiments, we observed only small fluxes in gly-oxylate metabolism in cells if they were abundantly fed with variousprecursors of oxalate synthesis. Whether these low fluxes are sufficientto generate the high urinary excretion of oxalate in Agxt -/--mice or inpatients with primary hyperoxaluria type 1, remains to be established.An estimation of the internal flux in the glyoxylate metabolism shouldtherefore be performed by other studies, such as isotope dilution tech-niques in patients.
The limitations of this study concern the difficulty to establish thepoint of entry of the applied metabolic precursors of glyoxylate. Sinceintact hepatocytes have been used and not separated organelles, theobserved product synthesis can only reflect what occurs in the entirehepatocytic metabolome. Furthermore, extrapolation of results fromanimal studies to the human analogue should be undertaken with cau-tion, especially since additional enzymes such as glycolate oxidase,glyoxylate reductase/hydroxypyruvate reductase can modulate oxalatemetabolism in a critical way. Regardless of this drawback, this is thefirst time a knockout model has been used in the metabolic studies ofprimary hyperoxaluria. Previously, incubations have been carried outin different models, including in humans in vivo, rats in vivo, perfusedrat livers, isolated hepatocytes, subcellular fractions of liver tissue (asdiscussed in Chapter 01). Other studies have drawn conclusions fromextrapolations from the properties of isolated enzymes. Therefore, thetype of research presented here may be of value since it creates newways to study oxalate metabolism, more closely related to human pri-mary hyperoxaluria than before. Further experiments may investigateif a change in the permeability of peroxisomes results in different ratesof oxalate and glycolate production, in order to assess if transport ofsubstrates across the peroxisomal membrane limits glyoxylate synthe-sis. Alternatively, isolated peroxisomes may be used for this purpose.For research aiming to identify potential sources of glyoxylate, inter-mediate metabolites, notably alfa-keto-gamma-hydroxyglutarate (pro-duced in the catablolism of hydroxyproline), and indolepyruvate (pro-duced in the catabolism of tryptophan) may be studied (10).Furthermore, an additional knockout mouse model in which both mito-chondrial and peroxisomal AGT activities are absent might be con-structed. This model should demonstrate strongly decreased glycinesynthesis and increased oxalate and glycolate production, if mitochon-dria or other compartments have indeed an important role in thedetoxification of glyoxylate. Eventually, elucidation of oxalate metabo-lism, its involved precursors and enzymes, may facilitate developmentof rational therapies, such as substrate deprivation, metabolic routeblockade via enzyme modification, or pathway diversion through enzy-me induction (with GR/HPR, or LDH FIGURE 08.1). This might be animportant step in studying potential therapeutic goals for PH1.
Clinical relevance
Limitations of the study
CHAPTER 08
page 112
VAN WOERDEN 5/19/08 8:53 AM Pagina 112

FIGURE 08.6
The glyoxylatepathway, as proposed byHolmes andAssimos (8).
REFERENCES
CHAPTER 08
page 113
1. Schwam H, Michelson S,
Randall WC, Sondey JM,
Hirschmann R. Purification and cha-
racterization of human liver glycolate
oxidase. Molecular weight, subunit,
and kinetic properties. Biochemistry
1979;18:2828-33.
2. van Woerden CS, Groothoff JW,
Wijburg FA, Annink C, Wanders RJ,
Waterham HR. Clinical implications
of mutation analysis in primary
hyperoxaluria type 1.
Kidney Int 2004;66:746-52.
3. Salido EC, Li XM, Lu Y, Wang X,
Santana A, Roy-Chowdhury N et al.
Alanine-glyoxylate aminotransferase-
deficient mice, a model for primary
hyperoxaluria that responds to
adenoviral gene transfer. Proc Natl
Acad Sci USA 2006;103:8249-54.
4. Wolthers BG, Hayer M.
The determination of oxalic acid in
plasma and urine by means of
capillary gas chromatography.
Clin Chim Acta 1982;120:87-102.
5. Inoue Y, Masuyama H, Ikawa
H, Mitsubuchi H, Kuhara T.
Monitoring method for pre- and post-
liver transplantation in patients with
primary hyperoxaluria type I. J
Chromatogr B Analyt Technol Biomed
Life Sci 2003;792:89-97.
6. Baker PR, Cramer SD, Kennedy
M, Assimos DG, Holmes RP.
Glycolate and glyoxylate metabolism in
HepG2 cells. Am J Physiol Cell Physiol
2004;287:C1359-C1365.
7. Ichiyama A, Xue HH, Oda T,
Uchida C, Sugiyama T, Maeda-
Nakai E et al. Oxalate synthesis in
mammals: properties and subcellular
distribution of serine:pyruvate/
alanine:glyoxylate aminotransferase
in the liver. Mol Urol 2000;4:333-40.
8. Holmes RP, Assimos DG.
Glyoxylate synthesis, and its modula-
tion and influence on oxalate synthesis.
J Urol 1998;160:1617-24.
9. Konno R, Sasaki M, Asakura S,
Fukui K, Enami J, Niwa A.
D-amino-acid oxidase is not present in
the mouse liver. Biochim Biophys
Acta 1997;1335:173-81.
10. Poore RE, Hurst CH, Assimos
DG, Holmes RP. Pathways of hepatic
oxalate synthesis and their regulation.
Am J Physiol 1997;272:C289-C294.
VAN WOERDEN 5/19/08 8:53 AM Pagina 113

CHAPTER 08
page 114
VAN WOERDEN 5/19/08 8:53 AM Pagina 114

CHAPTER 09 General discussion
The work presented in this thesis was carried out to explore a numberof clinical and biochemical concepts regarding primary hyperoxaluriatype 1 (PH1). The studied concepts comprised the following:
1. Epidemiology of hyperoxaluria: Description of the clinical phenotype of patients with PH1 in The Netherlandsincluding the age at presentation, symptoms and clinical outcome of patients.The incidence of PH1 in a cohort of routinely screened patients withurolithiasis.The occurrence of hyperoxaluria in patients with generalized peroxiso-somal disorders, i.e. Zellweger spectrum disorders. 2. The association between genetic, biochemical and clinical para-meters with respect to outcome of kidney function in PH1. 3. Additional biochemical studies in PH including in vitro and in vivostudies concerning oxalate synthesis and studies on the appropriatecollection of urine for diagnostic investigations.
EPIDEMIOLOGY OF HYPEROXALURIA
Most important conclusions:1. The prevalence and incidence of PH1 found in the Dutch cohort studyis three times higher than expected on the basis of previous data.2. PH1 is often undetected, especially in adults. This is an importantfactor in the development of renal failure in PH1.3. Over 80% of patients with Zellweger spectrum disorders have hyper-oxaluria. Clinically important hyperoxaluria occurs pre-dominantly in patients with severe neurological impairment.
At onset of the study, reliable epidemiological data on PH1 were lac-king. We therefore decided to study its prevalence and clinical spec-trum in a nationwide survey. We recruited the Dutch cohort of PH1patients by interviewing all nephrology centers in The Netherlands.Due to outstanding contacts of the Dutch Society of Nephrology withher members, we could approach nephrologists, both for pediatric aswell as for adult medicine. This resulted in a relatively high number ofPH1 patients retrieved in The Netherlands, compared to studies inother countries: 2.9 per million, which is three times higher than pre-viously observed (1). This high number is most probably a reflection ofour thorough search strategy. However, we believe that the observedprevalence is still an underestimation of the true prevalence for thefollowing reasons:1. Our methods of patient retrieval were limited to nephrologists. It islikely that other specialists are also involved in the diagnosis and treat-
09.01
CHAPTER 09
page 115
VAN WOERDEN 5/19/08 8:53 AM Pagina 115

ment of these patients, such as general practitioners, internists, or urolo-gists and may be the primary physicians involved in their follow-up.Approaching these specialists might further reduce this under-ascertain-ment. In a first step to test this hypothesis, we investigated to what extentPH1 had remained undetected using the current routine diagnostic pro-cedures of our own center. Therefore, we performed an automated searchon all urinary oxalate measurements that had ever been performed at thegeneral hospital laboratory. Those patients that were found to be hyper-oxaluric were reinvestigated by offering analysis of urinary oxalate, gly-colate, L-glycerate and if necessary AGXT gene analysis. Even though thesearch comprised a selected patient group, we found one new PH1patient. This demonstrates that our estimated prevalence (2.9 per million)is indeed an underestimation of the true prevalence. We conclude that thisstrategy is an easy and quick way to discover PH1 patients. Neuhaus andco-workers have studied the occurrence of hyperoxaluria in a cohort ofpediatric patients with urolithiasis or nephrocalcinosis and found hyper-oxaluria in more than 8% of the patients (2).2. As compared to children, a much higher proportion of adultpatients was diagnosed with already end-stage renal disease, despite thepresence of renal symptoms in many of them before the onset of decli-ne of renal function. In some patients, the diagnosis of PH1 was suspec-ted only after histological investigation of a kidney biopsy, after early fai-lure of a kidney transplant. These findings illustrate that the diagnosis isoften missed or delayed, especially in adults. This is supported by nume-rous case-reports that describe the diagnosis of PH1 after ‘unexplained”decline of renal function in patients (3-12). 3. The age at time of development of end-stage renal disease in ourcohort was comparable to that determined by Cochat et al. in their cohortstudy (29 vs. 25 years) (1). In both studies, data were derived frompatients in nephrology units. Therefore, the clinical spectrum of thesecohorts may be biased towards severe presentation, since nephrologistsare often consulted for the first time when renal insufficiency develops.Moreover, data from the Dutch registry RENINE have been used. Input ofpatient data in this registry is a prerequisite for reimbursement of thedialysis costs. Our search strategy ascertains that we have traced all PH1patients in end-stage renal disease, covering the severe end of the spec-trum. Because of the different methods we used, our cohort is likely torepresent the real spectrum of PH1 more accurately than other studies.However, it is very likely that, we may have missed PH1 patients, espe-cially on the mild end of the spectrum of the disease.In conclusion, we found evidence for an important underdetection ofPH1. Timely institution for adequate conservative therapy may preventrenal damage. We therefore advise extensive screening in all patientswith urolithiasis, nephrocalcinosis or renal insufficiency.
In the cohort of Dutch patients with Zellweger spectrum disordersCHAPTER 09
page 116
VAN WOERDEN 5/19/08 8:53 AM Pagina 116

(ZSDs), we found a high incidence of hyperoxaluria (83%). Althoughthree ZSD patients with hyperoxaluria had been described before, thefinding of hyperoxaluria at such a large scale was new. We were able toinvestigate these patients thoroughly due to the long period of follow-up. Pyridoxine was tried but turned out to be non- efficacious inpatients with ZSDs. Since we found marked hyperoxaluria especially inthose patients with severe psychomotor developmental delay whowere not able to express pain in case of urolithiasis, it is important toscreen the kidneys by means of ultrasound at an early age.
A considerable difference in urinary oxalate levels was observed bet-ween ZSD patients, with the highest levels found in patients with theseverest clinical form of Zellweger spectrum disorders. The variabilityof the peroxisomal defect may result in varying clinical and biochemi-cal phenotypes, as reflected by varying levels of neurological impair-ment and varying levels of urinary oxalate. These variations may arisefrom ghost peroxisomes which have some residual peroxisomal functi-on, or from peroxisome mosaics, in which livers display cells with nor-mal peroxisomes adjacent to cells that resemble Zellweger hepatocy-tes, i.e. with AGT in the cytoplasm (13). This may result in a milderphenotype. This may also explain how AGT can function to a variabledegree in patients with Zellweger spectrum disorders. To prove thishypothesis, we studied a liver biopsy specimen of a patient with mildneurodevelopmental impairment and slightly raised levels of urinaryoxalate (60 mmol/mol creatinine, upper level of normal referencerange 54 mmol/mol creatinine) (courtesy Prof. M. Espeel). After carefulelectron-microscopic analysis of the biopsy specimen, peroxisomeswere found to be present with a normal appearance in 10% of theinvestigated liver cells. Since patients with Zellweger spectrum disor-ders normally synthesize the AGT enzyme, a difference in urinary oxa-late excretion cannot be explained by differences in levels of residualAGT activity. A difference in percentage of normal AGT compartmenta-lization, however, may well explain the variation in urinary oxalateexcretion and renal involvement. The finding of peroxisomal mosaicsin a mildly affected patient is in line with this thought. Other patientsshould be studied to further explore this idea.
CLINICAL, BIOCHEMICAL AND GENETIC PREDICTORS OF OUTCOME IN PH1
Most important conclusions:1. Age at time of onset is not a good prognostic factor.2. Adults with PH1 predominantly present with renal insufficiency asfirst symptom. This implies that the so-called late onset PH1 is not abenign variant of the disease, as previously was suggested.3. There are strong indications that early conservative treatment
09.02
CHAPTER 09
page 117
VAN WOERDEN 5/19/08 8:53 AM Pagina 117

indeed may prevent the development of renal failure. 4. Neonatal PH1 has generally but not always a worse prognosis.5. Nephrocalcinosis as detected by ultrasound is a bad predictor forend-stage renal disease.6. Pyridoxine responsive patients have potentially a good prognosis,provided that adequate conservative treatment is established beforethe onset of renal failure.7. The level of residual AGT-(in)activity does not predict the outcome.8. Gly170Arg is the most predominant substitution found in Dutchpatients with PH19. Patients homozygous for Gly170Arg or Phe152Ile substitutionsare responsive to pyridoxine. 10. Patients homozygous for Gly170Arg or Phe152Ile substitutions withrenal failure should not be eligible for orthopic liver transplantation11. An additional Val336Asp substitution to a Gly170Arg substitutioninduces pyridoxine unresponsiveness.
In the epidemiologic survey, we investigated the predictive value offive clinical and biochemical outcome parameters and of the variousgenotypes. The results and clinical implications are discussed below.Since the discovery of the deficiency of the enzyme AGT in PH1 andmutations in the gene AGXT, which codes for AGT, attempts to link cli-nical prognosis to biochemical levels of AGT enzyme activity, levels ofurinary oxalate or AGXT gene mutations had not been very successful.The incompleteness of the cohort studies with respect to the clinicalfollow-up could have masked the discovery of clear relationships bet-ween biochemical and genetic parameters on the one hand and outco-me on the other hand. Therefore, in addition to a systematic approachassessing the clinical spectrum of PH1, we evaluated clinically relevantbiochemical and genetic parameters in relation to this spectrum.
Age of first symptoms Previously, it was believed that PH1 could be categorized into threegroups, namely: (1) a severe form, with infantile presentation beforethe first year of age and rapid decline of renal function; (2) a mild formwith adult onset, few symptoms and preservation of renal function,and (3) an intermediate form with childhood onset and gradual pro-gression to renal insufficiency (14). We found no prove for this categorization. In strong contrast, in ourcohort the percentage of adult patients with end-stage renal disease atthe time of diagnosis was significantly larger than of pediatric patients.We also found that patients with first manifestations of the disease ininfancy did not always develop early renal insufficiency. Infants andsmall children who did not present with end-stage renal disease butwith urolithiasis or hematuria and were treated timely could preservetheir renal function over time. Therefore, a prompt and adequate dia-
09.02.01
CHAPTER 09
page 118
VAN WOERDEN 5/19/08 8:53 AM Pagina 118

gnostic work up seems to predict the outcome and severity of renalinsufficiency rather than the age of presentation itself. Other, morerecently performed epidemiologic studies in various countries are inline with these findings (15-17).
In conclusion, our study implies that PH1 is an inherited disorder thatcan become symptomatic at any age. We suggest that all physicians,either dealing with pediatric or with adult patients, should be awarethat development of end-stage renal disease is always possible in PH1.
Pyridoxine responsivenessPyridoxine therapy had been used for more than 20 years in PH1, andMilliner et al. have assessed its benefits in an observational study (18).They demonstrated a favorable effect of pyridoxine by inhibition ofurinary crystallization. No cohort studies had addressed the efficacy ofpyridoxine since then. In our cohort, we could clearly demonstrate acorrelation between pyridoxine responsiveness and outcome. Renalinsufficiency occurred more often if urinary oxalate did not decline inresponse to pyridoxine administration. The efficacy of pyridoxine inpatients may have been underestimated in our epidemiologic studysince we censored data at renal insufficiency and we did not measureany potential effect of pyridoxine in patients diagnosed in end-stagerenal disease. As we demonstrated in our genetic study, efficacy ofpyridoxine should also be assessed after renal transplantation sincegood efficacy of pyridoxine resulted in prolonged preservation of thekidney transplant. Alternatively, pyridoxine efficacy may be assessedusing plasma oxalate and plasma glycolate (19,20), as was also demon-strated in one of our patients (21). Therefore, the addition of data on patients treated with pyridoxine inend-stage renal disease demonstrated that responsiveness to pyridoxi-ne treatment resulted in a clinically relevant decline of urinary oxalateand preservation of renal function.
NephrocalcinosisAs expected, we found an association between the appearance of neph-rocalcinosis on ultrasound and the development of renal insufficiency.However, this association was surprisingly weak. On the one hand, wefound that more patients with nephrocalcinosis than without nephro-calcinosis at the time diagnosis had an adverse outcome. On the otherhand, however, not all patients with nephrocalcinosis developed renalfailure over time. We also found patients with end-stage renal diseasedue to PH1 without apparent (cortical) nephrocalcinosis on abdominalultrasound, though oxalate crystals were demonstrated in a kidney bio-psy specimen. This phenomenon was recently confirmed by Kim et al.(22). Accordingly, it appears that the exact relationship between theresults of renal ultrasound and pathological observations is not clear
09.02.02
09.02.03
CHAPTER 09
page 119
VAN WOERDEN 5/19/08 8:53 AM Pagina 119

in humans, despite the good correlations found in animal studies bet-ween the extent of calcium oxalate depositions in kidney biopsies andnephrocalcinosis as detected by ultrasound (23). Apparently, calcifica-tions in a kidney biopsy specimen, as detected by polarized lightmicroscopy or so called von Kossa staining, may be too small to be visi-ble by renal ultrasound. Therefore, renal ultrasound is not always agood predictor of severity of renal involvement and the absence ofnephrocalcinosis does not exclude renal involvement in PH1. Moreover,nephrocalcinosis is not an independent patient characteristic, since itspresence depends on the moment at which the ultrasound is perfor-med. Since the available renal ultrasounds, as used in the epidemiolo-gic study were made at different time points during the course of thedisease in patients, they may have led to incomplete observations. Inaddition, the follow-up of nephrocalcinosis, as detected by renal ultra-sound, may be biased by the growth of the kidneys at more advancedages of patients. Although they appear less dense on the ultrasoundpicture, renal calcifications may not have vanished. Instead, the growthof the kidneys may have diluted the density of the kidney lesions. Thismay lead to an apparent decrease of the degree of nephrocalcinosis. Nostudies have addressed this problem, so its clinical implicationremains to be elucidated. More studies are necessary to assess the rela-tionship between nephrocalcinosis as detected by ultrasound, and theseverity of renal pathology, to make renal ultrasound a better predic-tor of renal involvement.
Levels of AGT activityWe found that levels of AGT activity do not predict outcome of renalfunction. This heterogeneity had been observed by others as well (24).However, AGT levels show a relationship with the presenting age ofpatients. Patients with the highest levels of AGT activity (>15%) havethe first symptoms at a more advanced age as compared with patientswith a lower level of residual AGT activity. On the other hand, asdemonstrated by the epidemiologic data of Chapter 3, all patients withrenal involvement at neonatal age have very low levels of AGT residu-al activity. This is partly presented in TABLE 04.3, of Chapter 4, and weherewith provide additional, unpublished data depicted in FIGURE 09.1.In clinical practice, this finding can be of use in patients who have beenfound by family screening: residual AGT activity of " 15% can be expec-ted to result in later development of symptoms in general. A higherresidual AGT activity could result in a better peroxisomal glyoxylate-to-glycine conversion compared with patients with a lower or undetec-table activity. This can lead to lower rates of oxalate production, and alower oxalate burden for the kidneys, with later renal involvement.This hypothesis could not be tested in our cohort, since many patientswere diagnosed in end-stage renal disease and no urine was availablefor oxalate analysis.
09.02.04
CHAPTER 09
page 120
VAN WOERDEN 5/19/08 8:53 AM Pagina 120

AGT residual activity plotted against the age of first symptoms
Even though we found this relationship between levels of AGT cataly-tical activity and age of first symptoms, from studies in families, itemerges that the outcome of the disease is quite heterogeneous inpatients from the same family (25,26). It may be difficult to comparethe clinical follow-up of the index patient with the patient who hasbeen found by screening, since screening will lead to earlier treatment,and this is likely to influence the clinical outcome. Therefore, despitethe association between age at first symptoms and AGT levels, the finaloutcome also seems to be determined by environmental factors andproper treatment.
Levels of urinary oxalateWe did not detect a relationship between levels of urinary oxalate onthe one hand, and development of renal insufficiency on the otherhand. Until the start of our project, no other studies had addressed thisrelationship. The failure to find such a relationship could be explainedin two ways: first, oxalate levels have been determined at differentlaboratories, and the use of different analysis techniques could mask aclear relationship. Secondly, many patients, especially those found atadult age, were diagnosed in end-stage renal disease. Since we couldnot measure urinary oxalate in these patients, data were incomplete.Nevertheless, urinary oxalate concentration may become a predictor ofdisease severity, if we acquire more prospective data in the future.Recently, the International Registry for primary hyperoxaluria revealedthat levels of urinary oxalate above the median level, as found in PH1patients, predispose to significantly shorter renal survival (27).
GenotypeOur genetic studies have clearly shown that a high number of DutchPH1 patients had the Gly170Arg genotype, as compared to other stu-
FIGURE 09.1
09.02.05
09.02.06CHAPTER 09
page 121
AGE OF FIRST SYMPTOMSAG
T A
CT
IVIT
Y
(%)
OF
NO
RM
AL
AC
TIV
ITY
VAN WOERDEN 5/19/08 8:53 AM Pagina 121

dies: 44% versus ~30% (16, 28-30). The German and the Dutch PH1patient cohorts were different in this respect since the homozygousGly170Arg genotype was not found in the German cohort. The closegeographic relationship between The Netherlands and Germany wouldpredict the same genotypes for PH1. This genotypic difference is pro-bably explained by a difference in patient retrieval. Our systematicsearch strategy included all nephrologists, both for children andadults, but Hoppe et al. only included patients diagnosed by pediatricnephrologists (16). We showed that the Gly170Arg mutation generallyresulted in symptoms at adult age, so these patients may not have beenfound by Hoppe et al. in their study. Other studies reported on AGXTdata of patients whose DNA had been sent in for diagnostic DNA ana-lysis from different countries. These results are also biased since theywere not obtained via a systematic search. Surprisingly, the Ile244Thrgenotype was not identified in our cohort. Instead, we observed a highallele frequency of Phe152Ile, which was detected in a homozygousform for the first time. It may therefore be a Dutch founder mutation.
Gly170Arg and Phe152Ile substitutionsWe found that patients with Gly170Arg and Phe152Ile genotypes hadrelatively high levels of AGT activity and a relatively late onset ofsymptoms. The latter finding has also been described by others (30-34). We also found they were all pyridoxine responsive and that earlypyridoxine treatment can prevent development of ESRD in thesepatients. In retrospect, the favorable outcome of patients with thismutation was also found in other patient reports, but because of thelimited number of patients in these studies, this relationship was lessclear (25,30). In addition to our findings, Monico et al. demonstrated adose dependent relationship of the Gly170Arg genotype in relationwith pyridoxine efficacy (31). Pyridoxine responsiveness was alreadypredicted in an earlier report which suggested mitochondrial mistarge-ting for the Phe152Ile mutation (32) and was demonstrated in anotherpatient in 2005 (35). We were able to demonstrate this relationshipconvincingly, because we also included patients who already receiveda kidney transplantation, showing pyridoxine responsiveness thereaf-ter. Yet, some of these patients developed end-stage renal disease des-pite the presence of the pyridoxine-responsive genotype. This occurredbefore the diagnosis of PH1 was made, and pyridoxine therapy was ini-tiated. Hence, no Gly170Arg and Phe152Ile patients with end-stage renaldisease had been on adequate treatment before the onset of end-stagerenal disease. Even after transplantation, oxalate excretion declined andkidney function was preserved as a result of pyridoxine treatment.Based on these observations, we believe that delayed diagnosis and tre-atment must have caused end-stage renal disease in these patients. Twopatients with end-stage renal disease despite having the Gly170Arggenotype received a second renal graft for reasons of increasing syste-
CHAPTER 09
page 122
VAN WOERDEN 5/19/08 8:53 AM Pagina 122

mic oxalosis and renal insufficiency. However, these patients had notbeen treated with pyridoxine previously. Probably, late diagnosis andlate initiation of pyridoxine treatment had caused widespread systemicoxalate depositions, compromising the renal graft. Alternatively, asecond, undiscovered AGXT mutation may be present in these patients,since other patients in our cohort and that of others also carried twomutations on the same allele (16). If the clinical response to pyridoxineis different contrary to what is expected based on the AGXT gene profi-le, such additional mutations should be suspected.
The mechanism of action of pyridoxine is unknown. Our studies didnot address this issue, and we can only speculate on the action of pyri-doxine. First, a chaperone role for pyridoxine, thereby inhibiting mito-chondrial import of AGT, could be envisaged, but there is no true evi-dence for this postulate (36). Secondly, we know that 10% of AGT canstill be routed to the peroxisomes, in the presence of the Gly170Arg,and possibly the Phe152Ile mutation (34). There, it may be functional,and stimulated by the addition of its cofactor pyridoxal-5-phosphate.Since pyridoxine affects both oxalate and glycolate excretion, it is like-ly that it acts on AGT activity, and not on other enzymes, such asGRHPR, that would selectively reduce oxalate production, by divertingglyoxylate to glycolate.
Although we found this relationship between these mutations and pyri-doxine responsiveness, other, yet unknown pyridoxine responsive bio-chemical phenotypes of AGT and its AGXT mutations may exist.Therefore, we advise that a trial with pyridoxine therapy should always be performed and its efficacy be measured by means of plasmaoxalate or glycolate levels.
Val336Asp substitution to the Gly170Arg and Phe152Ile substitutionInterestingly, we observed a previously unknown AGXT mutationVal336Asp, homozygous in one patient (patient 15), and heterozygousin another (patient 22). The mutation was inherited on the same alleleas the most common substitution Gly170Arg. Whether this results inelevated urinary oxalate in the parents was not investigated. Althoughthese patients were also homozygous for the favorable Gly170Arg sub-stitution, the outcome was poor. The homozygous Gly170Arg/Val336Asp patient did not respond to pyridoxine and rapidly developedend-stage renal disease. The patient who was compound heterozygousfor Phe152Ile on one allele and Gly170Arg, Val336Asp on the other alle-le, was responsive to pyridoxine. However, levels of urinary oxalateremained higher, than found in patients with only the Gly170Arg or thePhe152Ile genotype (levels about two times the upper limit of referen-ce range). This patient developed nephrocalcinosis and kidney stones,and showed development of a mild renal insufficiency (glomerular
CHAPTER 09
page 123
VAN WOERDEN 5/19/08 8:53 AM Pagina 123

filtration rate 70 ml/min/1.73 m2). Recently, Huber et al. found that aspecific region of human AGT, called PTS1A, probably contains addi-tional peroxisomal targeting information (37). This genetic informationis most likely located within the sequence coding from the amino acidregion between Val-324 and Ile-345 in the AGT protein. The Val336Aspamino acid substitution in these two Dutch patients probably interactswith this region and might prevent peroxisomal import. This couldabolish pyridoxine responsiveness and result in lower AGT activity.This implies that screening for the most common mutations can con-firm the diagnosis of PH1, but cannot predict the outcome, unless theentire AGXT gene is investigated. In this respect, it is also interestingto look at the Met340Ile mutation that is present on the minor allele insome of the patients. Since this polymorphism is also located in theregion where the PTS1A signal is proposed to exist, it may interact withthe additional peroxisomal targeting signal. Whether this is clinicallyrelevant, should be evaluated in larger patient groups.
Gly82Arg substitution, c.33_34insC insertionThe Gly82Arg substitution and c.33_34insC insertion were all associa-ted with an adverse outcome in our cohort. The c.33_34insC mutationresulted in an absent catalytic AGT activity, absent pyridoxine respon-siveness and early development of end-stage renal disease in ourcohort. These findings are in line with those found by Milosevic et al(38). For the c.33_34insC mutation, the lack of residual AGT protein isnot surprising since a frame shift occurs in the AGXT gene which leadsto a truncated protein. However, in an Italian cohort of PH1 patients,the homozygous c.33_34insC mutation was found to be associated witha less severe clinical picture. The favorable outcome may have been theresult of earlier diagnostics, but no information on this point wasgiven. In vitro studies for a Gly82Glu substitution show a failure tobind to the co-factor pyridoxal-5-phosphate, which may also occur inGly82Arg. Nevertheless, one patient found by screening because of anaffected brother with the Gly82Arg mutation, preserved her renal func-tion into adulthood, and had an uneventful pregnancy. This demon-strates that early adequate treatment may ameliorate clinical outcome.
Single heterozygous mutationsIn contrast, if only one heterozygous mutation is found in patients,AGT activity is not necessarily predicted to be normal, as we describedin Chapter 4. Mutations that exist outside the regions covered by ourprimer sets could influence gene transcription or translation, forexample if there are sequence variations in the promoter region of thegene. A transcription defect was found in three patients who werehomozygous for the minor allele by Purdue et al (34). However, com-parable studies could not be undertaken in our patients, because liversamples were not available.
CHAPTER 09
page 124
VAN WOERDEN 5/19/08 8:53 AM Pagina 124

BIOCHEMICAL STUDIES
Most important conclusions:1. 24 hours storage of 12 hours urine collection without acidification
does not influence the oxalate measurement.2. Endogenous oxalate production measurement by stable isotopes
is reliable in PH patients but not in healthy controls.
Three biochemical studies were carried out concerning diagnostic pro-cedures in PH1, which will be discussed below.
Procedure for the collection of urine for diagnostic screening in hyperoxaluriaFor diagnostic screening of PH1, acidification of urine immediatelyupon voiding has usually been performed to prevent oxalate precipita-tion, which could result in false-negative results. As we showed inChapter 2 acidification can be performed in the laboratory and can bedelayed for at least 24 hours. Collection at home is safe and reliable indry bottles, which are stored in the fridge to prevent bacterial growth.This obviates the use of hydrochloric acid and its dangers at home.
Measurement of endogenous oxalate production by stable isotopesPlasma oxalate concentration and urinary oxalate excretion have beenshown inaccurate parameters to monitor endogenous oxalate producti-on (EOP) in PH1 patients with renal insufficiency. A reliable parameter isneeded in these patients to evaluate the efficacy of any therapeuticintervention. Therefore, we devised a stable isotope oxalate tracermethod to quantify the rate of appearance of oxalate (Ra oxalate).Urinary oxalate excretion was well reflected by Ra oxalate in all threepatients. In healthy control subjects, however, Ra oxalate was higherthan expected as it exceeded urinary oxalate excretion several fold. Ourresults suggest that Ra oxalate as determined by our method results inan overestimation. Furthermore, although a large variation has beenreported in plasma oxalate concentration in healthy subjects, as sum-marized in a recent study describing a stable isotope dilution methodto quantify plasma oxalate and glycolate concentration in vitro (19),plasma oxalate concentration as determined in our control subjects wasin the higher range of the reported control values. The same dilemmawas encountered in the study of France et al who described a method ofmeasuring Ra oxalate after a single injection [1,2-13C]sodium-oxalate.They found a daily oxalate production rate of 1.89 mmol in a healthysubject (39).These authors contributed this high production rate of oxa-late to in vitro oxalogenesis from ascorbate despite acidification of theplasma samples after collection. We cannot rule out that some in vitrooxalogenesis from ascorbate occurred before analysis of the samples as
09.03
09.03.01
09.03.02
CHAPTER 09
page 125
VAN WOERDEN 5/19/08 8:53 AM Pagina 125

this has been shown to occur already in acidified frozen urine duringprolonged storage (40). If so, this will have caused an overestimation ofplasma oxalate concentration and of Ra oxalate in control subjects.Alternatively, urinary oxalate excretion could have been underestimatedin control subjects due to precipitation of oxalate with calcium in vitro.This seems less likely, however, as urinary super saturation is low incontrol subjects (41) and urinary acidification has been shown effectivein preventing calcium-oxalate precipitation (40). Since both Ra oxalateand plasma oxalate concentration are higher in patients with PH1, therelative contribution of in vitro oxalogenesis to the total oxalate con-centration in the plasma samples and Ra oxalate is smaller in patientsthan in control subjects and is probably negligible in patients with renalinsufficiency exhibiting a much higher plasma oxalate concentration. Tolimit the influence of possible in vitro oxalogenesis on the determina-tion of Ra oxalate and plasma oxalate concentration, plasma samplesshould be immediately acidified and analyzed as soon as possible aftertheir collection. In conclusion, we believe that this method is a reliabletool to establish the effect of oxalate reducing therapy in PH patientswith renal insufficiency.
Oxalate production in Agxt -/- mice hepatocytesLittle is known about the origin of glyoxylate, the direct precursor ofoxalate, in human metabolism. A clear understanding of involved meta-bolic pathways is a prerequisite for the design of alternative therapiesin PH1. Studies providing insight into the biochemistry of oxalate meta-bolism are limited especially because oxalate metabolism only occurs inhepatocytes, and immortalized hepatocyte cell lines of patients withprimary hyperoxaluria are not available for research. We performed thefirst metabolic studies in AGT deficient mice, which act as a model forprimary hyperoxaluria type 1. The experiments indicate a remarkablysmall flux through the glyoxylate pathway and none of the tested pre-cursors was significantly enhancing oxalate and glycolate production,except for glyoxylate and glycolate. Since the peroxisome is not knownas a metabolically active organelle in terms of high throughput of highamounts of metabolic products, this may reflect the true in vivo situa-tion. However, more experiments in separate compartments should bedone to observe glyoxylate fluxes through different organelles, such asthe peroxisomes or the mitochondria. At this moment, no other precur-sor is known to influence the oxalate production, which prevents pro-gress in research aiming at dietetic modifications, apart from modifica-tion of glyoxylate fluxes. In view of sustained glycine synthesis uponalanine addition and moderate oxalate excretion, our studies support apotential role for a second, potentially mitochondrial, AGT mediatedglyoxylate metabolism, at least in mice. The development of mice withdifferent knocked out enzymes, such as glycolate oxidase (GO) or gly-oxylate reductase (GR) may facilitate research in this respect.
09.03.03
CHAPTER 09
page 126
VAN WOERDEN 5/19/08 8:53 AM Pagina 126

CLINICAL IMPLICATIONS OF OUR STUDY WITH RESPECT TO DIAGNOSTIC AND THERAPEUTIC STRATEGY IN PH1
Diagnostic algorithm for primary hyperoxaluria type 1.
Therapeutic algorithm for primary hyperoxaluria type 1
09.04
FIGURE 09.2
FIGURE 09.3
VAN WOERDEN 5/19/08 8:53 AM Pagina 127

Update of diagnostic strategy Patients at any age with signs unexplained urolithiasis, nephrocalcinosisor renal insufficiency should be screened for PH1. The DNA diagnosticapproach in most patients eliminates the need for enzyme analysis bytaking a liver biopsy. The absence of nephrocalcinosis on ultrasound isnot a reliable prognostic determinant with respect to the development ofrenal damage. Family screening may detect patients at an early or evenasymptomatic stage and should always be performed. FIGURE 09.2 provi-des an algorithm for the recommended diagnostic strategy.
Update of treatment in PH1
Conservative therapyThe patients who were found by family screening, since all of themwere able to preserve renal function provide the best illustration of theprotective effects of both a timely diagnosis and initiation of treat-ment. This is remarkable, since the index patients in these familiesdeveloped renal insufficiency. Conservative treatment consisted ofhyperhydration, pyridoxine and potassium citrate in most cases, andmagnesium oxide in some. Potassium citrate was frequently prescribedas an anti-precipitating agent by pediatricians but not by adult neph-rologists, who more often used magnesium oxide. The lack of citratetherapy was seen in patients who presented with severe secondaryhyperoxaluria, as described in Chapter 5. Our observational study doesnot allow comparison between the efficacy of both drugs and we didnot collect data on urinary citrate levels or urinary pH to determine ifdosage was adequate, or if patients were compliant. All participatingphysicians prescribed hyperhydration. Since all patients, who werefound by screening, preserved renal function, even though the indexpatients had end-stage renal disease, and pyridoxine did not reduceurinary oxalate excretion, hyperhydration has proven to be very effec-tive in patients, regardless of the genotype. For pyridoxine, a clear rela-tionship between efficacy and outcome was shown, as discussed inmore detail above.
TransplantationMost patients who received a solitary kidney graft had an excellent sur-vival, contrary to what was usually expected (22,42-47). This is mostlikely due to the fact that all of these patients had a significant declineof urinary oxalate excretion under pyridoxine therapy. Most of thesepatients had developed end-stage renal disease before the diagnosis ofPH1 was established. Institution of pyridoxine therapy at the time ofdiagnosis therefore prevented oxalate induced damage in the trans-planted kidney. Mutation analysis in our cohort demonstrated pyri-doxine responsiveness in patients with the most common Gly170Arggenotype and the Phe152Ile genotype.
09.04.01
09.04.02
09.04.02.01
09.04.02.02
CHAPTER 09
page 128
VAN WOERDEN 5/19/08 8:53 AM Pagina 128

Therefore, all PH1 patients who need to have kidney transplantationshould be studied by AGXT gene analysis to predict pyridoxine res-ponsiveness. Patients with the Gly170Arg or Phe152Ile genotype willbenefit from treatment with pyridoxine, regardless of their kidneyfunction: preserved, in renal insufficiency or after kidney transplanta-tion. If results of AGXT gene analysis remain inconclusive regardingpyridoxine responsiveness, a trial with pyridoxine should be initiated.Response should be monitored by measuring urine and plasma levelsof oxalate and glycolate at baseline and after one to three months oftreatment with pyridoxine. Patient compliance can be ascertained bymeasuring plasma levels of pyridoxine.
Choice of transplantAs a liver or kidney transplantation may become necessary in patientsin end-stage renal disease, timing of the procedure is important.
We suggest the following options for transplantation in PH1:A. Kidney transplantation aloneAlthough the metabolic defect is not corrected by kidney transplanta-tion alone, our studies show that this is a reasonable option for patientsin whom pyridoxine responsiveness is established based on eitherresults of genetic studies, or after a trial of pyridoxine with assessmentof efficacy by means of studies in plasma oxalate or glycolate.B. Pre-emptive liver transplantationAlthough this is the only option to correct the enzyme defect, transplan-tation related morbidity and mortality prevents its use in all PH1 patients.Since we and others demonstrated a favorable follow-up in many patientswith conservative treatment only, especially in those with a pyridoxine-responsive genotype, liver transplantation should not be performed inthese patients. Instead, it should be reserved for patients who show noevidence of pyridoxine response, i.e. in patients with other mutations,and without any decline of plasma oxalate or glycolate levels or declineof the rate of appearance of oxalate upon treatment with pyridoxine. Sincewe also observed a favorable outcome with survival into adulthood ofnative kidneys even in patients without evidence of pyridoxine responsi-veness, we suggest that a liver transplantation should not be performeduntil renal insufficiency becomes inevitable and the glomerular filtrationrate declines below 60 ml/min/1.73m2. This level is generally regarded asthe cut-off for renal insufficiency and no morbidity from systemic oxala-te deposition is expected at this stage. Preparations for a liver transplan-tation may be taken at this stage. In patients in whom renal function decli-nes below 20-30 ml/min/1.73m2, an urgent transplantation becomesimportant in order to prevent systemic oxalate depositions, as investiga-ted previously (48).C. Combined liver-kidney transplantationIn patients with end-stage renal disease and no evidence for responsive-
CHAPTER 09
page 129
VAN WOERDEN 5/19/08 8:53 AM Pagina 129

ness to pyridoxine therapy as discussed under B, combined liver-kidneytransplantation should be performed.Unfortunately, these patients are at risk for acute kidney graft failure dueto wash out of oxalosis from body stores even after a successful comb-ined transplantation. Sequential liver kidney transplantation is thereforeproposed as a good alternative. In this procedure, renal transplantationfollows liver transplantation when pre-dialysis plasma oxalate levels havedeclined up to 25 µM during intensive hemodialysis sessions. A plasmaoxalate concentration of 25-50 µM is considered to be safe for kidneytransplantation, without early graft failure due to oxalosis in the kidney.However, it usually takes a year or more to achieve such low oxalate levelsunder these conditions (personal communication with JJ Homan van derHeide) (49,50). Dialysis may need to be continued for some time after thekidney transplantation. Immunological difficulties enhancing transplantrejection may arise as the grafts stem from different donors. However,based on a small group of patients who have undergone this procedure inThe Netherlands (n = 7), the outcome may be favorable and no increasedincidence of graft rejection was observed in this small group.Therapeutic approach to the PH1 patient: an updateBased on the current evidence we designed an algorithm that may befollowed in the choice for optimal treatment:
A. Patients with normal renal function (GFR>80 ml/min)1. conservative treatment:hyperhydration 3L/m2
potassium citrate (0.15 g/kg/day, once daily)pyridoxine (5-15 mg/kg/day, once daily)2. assess urinary oxalate or glycolate before and after treatment3. assess genotype to predict pyridoxine responsiveness
B. Patients with decreased renal function on conservative treatmentGFR 20-80: conservative treatment as under A and:GFR 60-80: preparation for liver transplantation in pyridoxineunresponsive patientsGFR 30-60: consider liver transplantation in pyridoxine unres-ponsive patientsGFR<30: absolute indication for (sequential) liver (kidney) trans-plantation in pyridoxine unresponsive patients; indication forstart hemodialysis
C. Patients with end-stage renal disease:1. assess genotype for potential pyridoxine responsiveness2. medication: start pyridoxine and evaluate responsiveness byplasma glycolate measurements or isotope dilution3. intensive (nocturnal) hemodialysis 4. consider transplantation procedure:
CHAPTER 09
page 130
VAN WOERDEN 5/19/08 8:53 AM Pagina 130

isolated kidney if pyridoxine responsiveness is expected, afterintensive dialysis sessions have declined plasma oxalate up to25-50 µM (pre-dialysis values)liver-kidney (preferably sequential, with intensive dialysis sessions declining plasma oxalate up to 25-50 µM, i.e. approxi-mately 1 year of dialysis) if pyridoxine responsiveness is notexpected.
LIMITATIONS OF THE EPIDEMIOLOGICAL AND GENETIC STUDYIN PH1 PATIENTS
In general, the strength of a cohort study depends on the completenessof patient retrieval, the availability of data, the number of patientsinvolved and the length of the follow-up period. The results of ourgenotype-phenotype study were potentially biased by a limited patientparticipation and follow-up. First, a considerable number of patientsfrom the epidemiological study have died, before their contribution tothe genetic study could be ascertained, which may have created apotential loss at the severe end of the disease spectrum. Secondly, dif-ferences in the follow-up period between recruited patients may causepotential bias to observed outcome. The conclusions of our studies canonly sustain if a careful prospective follow-up of patient data is carriedout. An extended, international registry for careful patient follow-up istherefore warranted.
Another source of potential bias is the difference in treatment strate-gies followed in our patients. We noticed a difference in conservativetreatment as prescribed by pediatric vs. adult nephrologists, as obser-ved in the cohorts of Chapter 3 and Chapter 4. Citrate was widely pre-scribed by pediatric nephrologists, but scarcely used by nephrologistsfor adults. Citrate has shown to be efficacious in the reduction of uro-lithiasis and may therefore have induced a milder phenotype in gene-ral in our cohort. The use of intravenous fluids for the prevention ofdehydration was strictly used at one of the adult centers which alsomay have contributed to a milder phenotype. These factors may con-tribute to differences within a certain genotypic sub group.
IMPLICATIONS FOR FUTURE RESEARCHFrom the work presented in this thesis, new foci for research emerge.
1. The possibility that patients may remain undetected urges a tho-rough search strategy among patients with one of the mentioned urina-ry tract symptoms that may be the initial presentation of primary hyper-oxaluria type 1. Family screening is not yet applied systematically andcould further increase the prevalence of PH1 provided it is used morewidely. Diagnostic studies in patients with unexplained recurrent uroli-
09.05
09.06
CHAPTER 09
page 131
VAN WOERDEN 5/19/08 8:53 AM Pagina 131

thiasis or other renal involvement should comprise metabolic investi-gations. Before we have implemented this, research should actively con-tribute to patient finding. Reinvestigation of patients in whom hyper-oxaluria has been detected without any further metabolic studies mayalso lead to the discovery of new patients.2. Though heterogeneity regarding genotype and phenotype hasbeen confirmed by our studies, we demonstrated for the first time arelationship between a specific genotype and phenotype. Furthermore,we stated that prognosis was strongly influenced towards favorableoutcome by early diagnosis and treatment. Since our studies were cen-sored at a certain time point, follow-up studies should be undertakento further substantiate the conclusions we extracted. These include (1)the favourable outcome of the Gly170Arg and Phe152Ile genotypes andtheir obligatory responsiveness to pyridoxine therapy, (2) the devasta-ting clinical outcome of the c.33_34insC insertion and the Gly82Argand Val336Asp substitutions.3. An unresolved genetic issue is the detection of PH1 patients withapparently only one AGXT gene mutation. The biochemical profile, inclu-ding highly elevated levels of urinary oxalate and glycolate, as well asabsent catalytical AGT activity suggests that both alleles contain muta-tions. This needs to be resolved for diagnostic purposes, since heteroge-neity of AGXT gene mutations cannot exclude PH1.If our cohort of patients is too small to reach these goals, a multi-nationaldatabase should be created to combine data for more power in research.4. The predictive value of urinary oxalate needs further considera-tion. Since elevated oxalate excretion is the key stone for renal dama-ge, and since decline of oxalate excretion upon treatment with pyri-doxine is related to decrease of symptoms and damage, urinary oxala-te levels seem to have a direct correlation with disease severity andprognosis. We were not able to demonstrate this, probably by the factthat many of the more severe patients were diagnosed with anuria andno urine was available for investigation. Collection of data from newlydiagnosed PH1 patients may demonstrate such a relationship betweenbiochemical and clinical phenotype. A relationship between genotypeand levels of urinary oxalate may also appear.5. Our studies in patients with Zellweger spectrum disorders demon-strate the importance of compartmentalization for AGT catalytic acti-vity. The levels of hyperoxaluria as observed in these patients varieswidely, but renal involvement was only observed in patients with highlevels of oxalate and this was only present in patients with a clinicallysevere form of the Zellweger spectrum disorders. Follow-up should beperformed to observe potential renal involvement in the other patients.A relationship with peroxisomal mosaics may be found if liver biopsiesare studied in more patients.6. The use of the stable isotope dilution technique in the evaluationof new potential therapies, that aim to reduce endogenous oxalate pro-
CHAPTER 09
page 132
VAN WOERDEN 5/19/08 8:53 AM Pagina 132

duction, such as scavenger molecules which bind toxic glyoxylate.7. Metabolic studies in hepatocytes are warranted to identify precur-sors of endogenous oxalate synthesis. Our first studies in Agxt -/- micewere not conclusive, probably by interference of catalytically activemitochondrial AGT. The clinical significance of alanine supplementa-tion may be investigated in vivo, since the in vitro studies showedrestored glycine synthesis in Agxt -/- hepatocytes.
REFERENCES
CHAPTER 09
page 133
1. Cochat P, Deloraine A, Rotily M,
Olive F, Liponski I, Deries N. Epidemio-
logy of primary hyperoxaluria type 1.
Société de Néphrologie and the Société
de Néphrologie Pédiatrique. Nephrol
Dial Transplant 1995;10 Suppl 8:3-7.
2. Neuhaus TJ, Belzer T, Blau N,
Hoppe B, Sidhu H, Leumann E. Urinary
oxalate excretion in urolithiasis and
nephrocalcinosis. Arch Dis Child
2000;82:322-26.
3. Verbruggen LA, Bourgain C,
Verbeelen D. Late presentation and
microcrystalline arthropathy in prima-
ry hyperoxaluria. Clin Exp Rheumatol
1989;7:631-33.
4. Lorenzo V, Alvarez A, Torres A,
Torregrosa V, Hernandez D, Salido E.
Presentation and role of transplantation
in adult patients with type 1 primary
hyperoxaluria and the I244T AGXT
mutation: Single-center experience.
Kidney Int 2006;70:1115-19.
5. David-Walek T, Niederstadt C,
Rob PM, Fricke L, Latta K, Steinhoff J,
Stange EF. Primary hyperoxaluria type 1
causing end-stage renal disease in a 45-
year-old patient. Nephron 2001;87:80-84.
6. Irish AB, Doust B. Late
presentation and development of
nephrocalcinosis in primary hyperoxa-
luria. Aust N Z J Med 1992;22:48-50.
7. Kuiper JJ. Initial manifestation
of primary hyperoxaluria type I in adults-
- recognition, diagnosis, and manage-
ment. West J Med 1996;164:42-53.
7. Farreli J, Shoemaker JD, Otti T,
Jordan W, Schoch L, Neu LT, Bastani B.
Primary hyperoxaluria in an adult
with renal failure, livedo reticularis,
retinopathy, and peripheral
neuropathy.
Am J Kidney Dis 1997;29:947-52.
9. Gluck T, Kramer BK, Zulke C,
Ruschoff J, Rogler G, Schweda F et al.
Late onset primary oxalosis type I: an un-
common presentation of a rare disease. Eur
J Gastroenterol Hepatol 1998;10: 809-12.
10. Calisir C, Yavas US. A case of late-
onset primary hyperoxaluria. Australas
Radiol 2007;51 Spec No.:B88-B91.
11. Sadeghi N, de PL, Vienne A,
Dhaene M, Struyven J, Stallenberg B.
Late diagnosis of oxalosis in an adult
patient: findings on bone radiography.
AJR Am J Roentgenol 1998;170:1248-50.
12. Doganavsargil B, Akil I, Sen S,
Mir S, Basdemir G. Autopsy findings of
a case with oxalosis. Pediatr Dev
Pathol 2007;14:1.
VAN WOERDEN 5/19/08 8:53 AM Pagina 133

13. Roels F, Saudubray JM, Giros M,
Mandel H, Eyskens F, Saracibar N et al.
Peroxisome mosaics. Adv Exp Med Biol
2003;544:97-106.
14. Cochat P, Rolland MO. Primary
hyperoxalurias. In: Fernandes J,
Saudubray JM, van den Berghe G, eds.
Inborn metabolic diseases and treat-
ment. Heidelberg: Springer Verlag,
2000:441-46.
15. Hoppe B, Langman CB. A United
States survey on diagnosis, treatment,
and outcome of primary hyperoxaluria.
Pediatr Nephrol 2003;18:986-91.
16. Hoppe B, Latta K, von
Schnakenburg C, Kemper MJ.
Primary hyperoxaluria-the German
experience. Am J Nephrol 2005;
25:276-81.
17. Takayama T, Nagata M,
Ichiyama A, Ozono S. Primary
hyperoxaluria type 1 in Japan.
Am J Nephrol 2005;25:297-302.
18. Milliner DS, Eickholt JT,
Bergstralh EJ, Wilson DM, Smith LH.
Results of long-term treatment with
orthophosphate and pyridoxine in
patients with primary hyperoxaluria.
N Engl J Med 1994;331:1553-58.
19. Inoue Y, Masuyama H,
Ikawa H, Mitsubuchi H, Kuhara T.
Monitoring method for pre- and
post-liver transplantation in patients
with primary hyperoxaluria type I. J
Chromatogr B Analyt Technol
Biomed Life Sci 2003;792:89-97.
20. Marangella M, Petrarulo M,
Bianco O, Vitale C, Finocchiaro P,
Linari F. Glycolate determination
detects type I primary hyperoxaluria
in dialysis patients. Kidney Int
1991;39:149-54.
21. Rosier JG, Baadenhuijsen H,
Koene RA. Long-term survival of a
renal allograft in a patient with
primary hyperoxaluria (type I).
Neth J Med 1981;24:179-84.
22. Kim HH, Koh HI, Ku BI, Lee HS.
Late-onset primary hyperoxaluria
diagnosed after renal transplantation
presented with early recurrence of
disease. Nephrol Dial Transplant
2005;20:1738-40.
23. Cramer B, Husa L,
Pushpanathan C. Nephrocalcinosis in
rabbits-correlation of ultrasound,
computed tomography, pathology
and renal function. Pediatr Radiol
1998;28:9-13.
24. Danpure CJ. Molecular and
clinical heterogeneity in primary
hyperoxaluria type 1. Am J Kidney
Dis 1991;17:366-69.
25. Hoppe B, Danpure CJ, Rumsby
G, Fryer P, Jennings PR, Blau N et al.
A vertical (pseudodominant) pattern of
inheritance in the autosomal recessive
disease primary hyperoxaluria type 1:
lack of relationship between genotype,
enzymic phenotype, and disease severity.
Am J Kidney Dis 1997;29:36-44.
26. Frishberg Y, Rinat C, Shalata A,
Khatib I, Feinstein S, Becker-Cohen R
et al. Intra-familial clinical heteroge-
neity: absence of genotype-phenotype
correlation in primary hyperoxaluria
type 1 in Israel. Am J Nephrol
2005;25:269-75.CHAPTER 09
page 134
VAN WOERDEN 5/19/08 8:53 AM Pagina 134

CHAPTER 09
page 135
27. Milliner D. Treatment of the
primary hyperoxalurias: a new chapter.
Kidney Int 2006;70:1198-200.
28. Rumsby G, Williams E, Coulter-
Mackie M. Evaluation of mutation
screening as a first line test for the diag-
nosis of the primary hyperoxalurias.
Kidney International Vol 66(3)()(pp
959-963), 2004 2004;959-63.
29. Tarn AC, von SC, Rumsby G.
Primary hyperoxaluria type 1: dia-
gnostic relevance of mutations and
polymorphisms in the alanine:glyoxyla-
te aminotransferase gene (AGXT).
J Inherit Metab Dis 1997;20:689-96.
30. Amoroso A, Pirulli D, Florian F,
Puzzer D, Boniotto M, Crovella S et al.
AGXT gene mutations and their influ-
ence on clinical heterogeneity of type 1
primary hyperoxaluria. J Am Soc
Nephrol 2001;12:2072-79.
31. Monico CG, Rossetti S, Olson JB,
Milliner DS. Pyridoxine effect in type I
primary hyperoxaluria is associated
with the most common mutant allele.
Kidney Int 2005;67:1704-9.
32. Danpure CJ, Purdue PE,
Fryer P, Griffiths S, Allsop J, Lumb MJ
et al. Enzymological and mutational
analysis of a complex primary hyper-
oxaluria type 1 phenotype involving
alanine:glyoxylate aminotransferase
peroxisome-to-mitochondrion mis-
targeting and intraperoxisomal
aggregation.
Am J Hum Genet 1993;53:417-32.
33. Danpure CJ, Jennings PR, Fryer
P, Purdue PE, Allsop J.
Primary hyperoxaluria type 1:
genotypic and phenotypic hetero-
geneity. J Inherit Metab Dis
1994;17:487-99.
34. Purdue PE, Takada Y, Danpure
CJ. Identification of mutations associa-
ted with peroxisome-to-mitochondrion
mistargeting of alanine/glyoxylate
aminotransferase in primary hyper-
oxaluria type 1.
J Cell Biol 1990;111:2341-51.
35. Monico CG, Olson JB, Milliner DS.
Implications of genotype and enzyme
phenotype in pyridoxine response of
patients with type I primary hyperoxa-
luria. Am J Nephrol 2005;25:183-88.
36. Lumb MJ, Birdsey GM,
Danpure CJ. Correction of an enzyme
trafficking defect in hereditary kidney
stone disease in vitro. Biochem J
2003;374:79-87.
37. Huber PA, Birdsey GM, Lumb
MJ, Prowse DT, Perkins TJ, Knight DR,
Danpure CJ. Peroxisomal import of
human alanine:glyoxylate aminotrans-
ferase requires ancillary targeting
information remote from its C terminus.
J Biol Chem 2005;280:27111-20.
38. Milosevic D, Rinat C, Batinic D,
Frishberg Y. Genetic analysis - a diag-
nostic tool for primary hyperoxaluria
type I. Pediatr Nephrol 2002;17:896-98.
39. France NC, Holland PT, Wallace
MR. Contribution of dialysis to endoge-
nous oxalate production in patients
with chronic renal failure. Clin Chem
1994;40:1544-48.
40. Mazzachi BC, Teubner JK, Ryall RL.
Factors affecting measurement of urinary
oxalate. Clin Chem 1984;30:1339-43.
VAN WOERDEN 5/19/08 8:53 AM Pagina 135

CHAPTER 09
page 136
41. van Woerden CS, Huidekoper
HH, Groothoff JW, Wijburg FA, Duran M.
Postponing urine acidification for 24 h
does not change the oxalate concentra-
tion. Clin Chim Acta 2007;384:184-85.
42. Riksen NP, Timmers HJ,
Assmann KJ, Huysmans FT. Renal graft
failure due to type 1 primary hyper-
oxaluria. Neth J Med 2002;60:407-10.
43. Cibrik DM, Kaplan B, Arndorfer
JA, Meier-Kriesche HU. Renal allograft
survival in patients with oxalosis.
Transplantation 2002;74:707-10.
44. Bilgin N, Tirnaksiz MB, Moray G,
Karakayali H, Yildirim S, Demirhan B,
Haberal M. Early recurrence of oxalate
deposition after renal transplantation
in a patient with primary hyper-
oxaluria type I.
Transplant Proc 1999;31:3219-20.
45. Calzavara P, Marangella M,
Petrarulo M, Ballanti P, Bonucci E,
Calconi G et al. Long-term survival on
renal replacement therapy for primary
hyperoxaluria type I. Nephron
1993;63:217-21.
46. Casale AJ, Leichter HE,
Sheth KJ, Segura AD, Lawson RK.
Renal transplantation in a child with
primary oxalosis.
Child Nephrol Urol 1990;10:103-6.
47. Knols G, Leunissen KM,
Spaapen LJ, Bosman FT, vd Wiel TW,
Kootstra G, van Hooff JP. Recurrence
of nephro-calcinosis after renal
transplantation in an adult patient
with primary hyperoxaluria type I.
Nephrol Dial Transplant 1989;
4:137-39.
48. Morgan SH, Purkiss P, Watts RW,
Mansell MA. Oxalate dynamics in
chronic renal failure. Comparison
with normal subjects and patients with
primary hyperoxaluria.
Nephron 1987;46:253-57.
49. Monico CG, Milliner DS.
Combined liver-kidney and kidney-
alone transplantation in primary
hyperoxaluria. Liver Transpl
2001;7:954-63.
50. Jamieson NV. A 20-year
experience of combined liver/kidney
transplantation for primary hyper-
oxaluria (PH1): the European PH1
transplant registry experience
1984-2004. Am J Nephrol
2005;25:282-89.
VAN WOERDEN 5/19/08 8:53 AM Pagina 136

CHAPTER 10 Summary
This thesis comprises clinical, genetic and biochemicalstudies on primary hyperoxaluria type 1 (PH1). In this chapter, an overview is presented of the variousstudies performed.
In CHAPTER 01, the historical developments in the field of research onprimary hyperoxaluria in the twentieth century are described, startingwith the description of the first patient with primary hyperoxaluria in1925, followed by the elucidation of the AGT enzyme deficiency in1986 and the characterization of the corresponding AGXT gene in 1990,with attempts to unravel genotype-phenotype relationships at the endof the twentieth century. An overview of the standard approach for dia-gnosis and treatment is included. A list of reference ranges for clinicalmetabolites based on extensive studies in control individuals is provi-ded in the Appendix.
CHAPTER 02 presents a study in which we assessed the need for acidi-fication of 24-hour collection of urine at home, instead of postponingacidification until arrival at the laboratory. Previously, it has been esta-blished that the oxalate concentration in a non-acidified urine sampledecreases over time as a result of precipitation with calcium.Therefore, postponement of acidification of the urine sample may leadto false negative results with respect to oxalate analysis. On the otherhand, false positive results also have been reported, caused by the invitro conversion of ascorbate to oxalate at alkaline pH. Therefore, aci-dification of urine is usually recommended in home settings. Since thisexposes patients and their caretakers to the hazards of hydrochloricacid spill or inhalation, we investigated whether acidification of urinecould be postponed for 24 hours. The study showed that urinary oxa-late levels were not different if acidification was postponed as compa-red to immediate acidification. Therefore, we suggest that acidificationshould no longer be performed at home.
In CHAPTER 03, we present the assembly of the first Dutch cohort ofpatients with primary hyperoxaluria type 1. In order to detect allpatients with primary hyperoxaluria type 1, all Dutch centers for adultand pediatric nephrology were actively approached. The epidemiologicdata present information on clinical presentation of patients, and theoutcome with special regard to kidney function. The predictive valueof five clinically relevant parameters with respect to the developmentof renal insufficiency was investigated, including levels of urinary oxa-late, levels of residual activity of AGT, responsiveness to pyridoxinetherapy, nephrocalcinosis and age at first symptoms. A total number of
CHAPTER 10
page 137
VAN WOERDEN 5/19/08 8:53 AM Pagina 137

57 patients could be included in this study, resulting in a prevalence ofnearly 3 per million. This prevalence is markedly higher than assessedby studies in other countries (France: 1 per million). Symptoms wereremarkably heterogeneous, ranging from a single stone at age 30, todevelopment of end-stage renal disease, extensive nephrocalcinosisand systemic calcium oxalate depositions before the first year of age.A high percentage of patients was diagnosed in end-stage renal disea-se (33%). Most patients diagnosed at adult age (59%) were diagnosed inend-stage renal disease, compared to 23% of those diagnosed in child-hood. It was previously assumed that the outcome in PH1 was worse inpatients with a younger presentation. Interestingly, in our cohort, ageat initial symptoms was not a predictor of outcome. Of the otherinvestigated potential prognostic parameters, absence of responsive-ness to pyridoxine therapy and presence of nephrocalcinosis were indi-cative of development of renal insufficiency.
In CHAPTER 04, we describe the genotype-phenotype analysis for theDutch PH1 cohort. Of 46 living patients, clinically described in Chapter3, 33 were available for mutation-analysis. We found a high prevalence(44%) of the most common mutation associated with the so-calledminor allele, leading to the amino acid substitution Gly170Arg. ThePhe152Ile substitution appeared to be the second most common sub-stitution in our cohort, probably being a founder mutation. All patientswho were homozygous for the Gly170Arg or the Phe152Ile mutationshowed full responsiveness to pyridoxine treatment with a significantdecrease of urinary oxalate levels and preservation of renal function.This also explained the favorable outcome of Gly170Arg or Phe152Ilepatients who received kidney transplantation without liver transplan-tation. Apparently, all patients who are responsive to pyridoxine the-rapy preserve renal function if treated timely. A rather poor outcomewas observed for the c.33_34insC mutation and a novel Gly82Arg sub-stitution. Four patients were heterozygous for one mutation only, butwere AGT deficient, confirming the diagnosis of PH1. Detection of aheterozygous AGXT mutation in the diagnostic work-up can thereforenot exclude PH1. In general, renal insufficiency was observed in allgenotypes if diagnosis and treatment were delayed, and preservationof renal function was best achieved in patients with early diagnosis andtreatment. This illustrates the importance of environmental and poten-tially other factors in the outcome of patients. It implicates early dia-gnostic screening of patients in whom primary hyperoxaluria is sus-pected in order to preserve renal function.
CHAPTER 05 shows the results of a separate cohort study. Since we sus-pected underdiagnosis of primary hyperoxaluria in patients with renalinvolvement as discussed in CHAPTER 03 and 04, we reinvestigated 32hyperoxaluric patients out of 150 in whom urinalysis for oxalate had
CHAPTER 10
page 138
VAN WOERDEN 5/19/08 8:53 AM Pagina 138

been performed. After analysis of fresh urines from 25 of the 32patients who could be reinvestigated, we detected one PH1 patient,who was responsive to pyridoxine treatment, thus confirming the needfor an active search for PH1 patients. As an additional result, four otherpatients had markedly elevated levels of urinary oxalate because ofmalabsorption syndromes due to Crohn’s disease and short bowel syn-drome. They showed considerable co-morbidity due to frequent passa-ge of renal stones and even renal insufficiency, leading to end-stagerenal disease in one patient. Conservative treatment did not comprisecitrate prescription, though its clinical benefits have been demonstra-ted in various clinical studies. We suggest that the treatment ofpatients with secondary hyperoxaluria should be optimized.
A cohort of patients with Zellweger spectrum disorders (ZSDs) wasscreened for the presence of hyperoxaluria and hyperglycolic aciduria,and the results obtained are reported in CHAPTER 06. The impairmentof peroxisome biogenesis is the biochemical hallmark in patients withgeneralized peroxisomal disorders, such as the Zellweger spectrumdisorders. These patients present with neurological impairment. At thecellular level, many peroxisomal functions are lost. However, someperoxisomal enzymes remain stable in the cytosol, including AGT. Avery high incidence of hyperoxaluria and hyperglycolic aciduria wasobserved in a group of 19 out of 23 (83%) ZSD patients. Urolithiasis andhyperoxaluria were seen in five patients, with development of end-stage renal disease in one of them. Levels of oxalate showed a widerange with apparently low levels in patients with mild neurologicaldeficits, and high levels in patients with severe neurological involve-ment. The wide range of oxalate levels may be caused by residual func-tional AGT activity outside the peroxisomes or some residual AGTimport in peroxisomes in mildly affected patients. Since absence ofhyperoxaluria is only seen in ZSD patients with a very mild neurologi-cal impairment and survival into adulthood, a potential role for peroxi-some mosaics is suggested. Follow-up of patients with ZSDs shouldinclude renal ultrasound studies to observe development of urolithia-sis. We advise prevention of renal involvement by adequate fluid inta-ke, if necessary via a nasogastric tube.
CHAPTER 07, we studied the rate of appearance of oxalate in threepatients with PH1 and three control subjects in order to develop a stra-tegy that more accurately estimates the endogenous production of oxa-late. There was a good correlation between the rate of appearance ofoxalate in plasma and the calculated daily urinary excretion of oxalate.The rate of appearance of oxalate could be used in patients with anu-ria to assess whether endogenous oxalate production declines upontreatment with novel pharmacological agents. The applicability of thismethod should be further studied in patients with renal insufficiency.
CHAPTER 10
page 139
VAN WOERDEN 5/19/08 8:53 AM Pagina 139

In CHAPTER 08, the results of metabolic investigations in hepatocytesisolated from the liver of a recently generated Agxt -/- mouse are des-cribed. This knock-out mouse serves as a model for primary hyperoxa-luria type 1. The aim was to identify precursors of oxalate synthesis byincubation of hepatocytes with different potential precursors. None ofthe tested substrates induced significant oxalate production, apartfrom glyoxylate, and to a minor extent glycolate. An apparent repair inAGT metabolism seems to take place in cells treated with alanineduring the incubation with substrates. Since wild type mice have AGTactivity in peroxisomes and mitochondria, our results suggest an alter-native, potential mitochondrial route for glyoxylate detoxification. Theapparent rescuing effect of alanine in Agxt -/- hepatocytes deserves fur-ther investigation in vivo.
Based on the conclusions from our cohort studies, we revised the dia-gnosis and treatment protocols for primary hyperoxaluria type 1, aspresented in CHAPTER 09 . The major gain in the diagnostic approachis the high diagnostic yield of DNA analysis. We recommend urine col-lection in dry containers for diagnostic purposes. For treatment, thedecision to perform kidney transplantation alone is advised if pyri-doxine responsiveness is expected by demonstration of the Gly170Argor the Phe152Ile substitution, or by a decrease in the levels of oxalateor glycolate in urine or plasma upon treatment with pharmacologicaldoses of pyridoxine. Two flow charts present these recommendations.
CHAPTER 10
page 140
VAN WOERDEN 5/19/08 8:53 AM Pagina 140

CHAPTER 11 Nederlandse samenvatting
VERKLARENDE WOORDENLIJST:
CHAPTER 11
blz. 141
enzym
een biologische katalysator, die zorgt
dat noodzakelijke chemische reacties
zich bij lichaamstemperatuur snel
genoeg kunnen afspelen
enzymdeficiëntie
het ontbreken of niet goed
functioneren van een enzym
restactiviteit
de mate waarin een enzym nog actief
is, uitgedrukt in percentage van
normaalwaarde
stofwisselingsziekte
= metabole stoornis
aandoening waarbij een van de vele
chemische reacties in het lichaam niet
goed werkt door een aangeboren fout
dialyse
hemodialyse of peritoneaaldialyse:
nierfunctievervangende therapie,
waarbij de zuiverende werking van
de nier wordt overgenomen door een
machine, die het bloed zuivert van
afvalstoffen
AGT
alanine:glyoxylaat aminotransferase,
het enzym dat de omzetting van gly-
oxylaat in glycine katalyseert
AGXT
het gen dat de code bevat voor de
aanmaak van het enzym AGT
oxaalzuur
een plantaardige stof die veel in
rabarber en spinazie voorkomt.
Oxaalzuur wordt ook in de lever
van de mens geproduceerd, in zeer
kleine hoeveelheden.
Oxaalzuur wordt overvloedig
geproduceerd in de lever van
patiënten met PH1
PH1
primaire hyperoxalurie type 1: een
stofwisselingsziekte die veroorzaakt
wordt door mutaties in het AGXT-gen,
waardoor AGT-deficiëntie ontstaat, met
verhoogde productie en uitscheiding
van oxaalzuur tot gevolg. Leidt tot
nierstenen en nierinsufficiëntie.
glycolzuur
plantaardige stof, die als neven-
product ontstaat bij de verbranding
van glyoxylzuur
glyoxylzuur
een aldehyde (bepaalde chemische
verbinding). De directe voorloper
van oxaalzuur
peroxisomen
het compartiment in de cel, waar
bepaalde vetten worden verteerd, en
een aantal specifieke biochemische
reacties zich afspeelt
precursor van oxaalzuur
stof (‘voorloper’) waaruit oxaalzuur
kan worden gevormd
incubatiestudies:
‘marineren’ van levende cellen in
een vloeistof waarin een bepaalde
precursor is verwerkt, om te zien
of de cellen deze precursor omzetten
in een andere stof
Zellweger spectrum disorders
(ZSDs):
verzamelnaam voor patiënten bij
wie de aanmaak van peroxisomen
is gestoord
Agxt -/- muis:
het muismodel van PH1, waarbij
het enzym AGT deficiënt is door
genetische modificatie van het
AGXT-gen van de muis
VAN WOERDEN 5/19/08 8:53 AM Pagina 141

INTRODUCTIE
Primaire hyperoxalurie type 1, afgekort PH1, is een stofwisselingsziektevan de lever, waarbij er een voor het lichaam nutteloze stof in overmaatwordt geproduceerd. Deze stof, oxaalzuur genaamd, verlaat het lichaamvia de nier. Bij een te hoge concentratie kan oxaalzuur met calcium neer-slaan. Dit kan leiden tot de vorming van nierstenen en nierverkalking(nefrocalcinose) met een verminderde nierfunctie (nierinsufficiëntie) alsmogelijk gevolg. Uiteindelijk kan een terminale nierinsufficiëntie ontstaanwaarbij dialyse nodig is om de nierfunctie over te nemen. In die situatievindt er stapeling van het oxaalzuur in verschillende organen van hetlichaam plaats, zoals in botweefsel, ogen en bloedvaten.
De nierstenen bij primaire hyperoxalurie type 1 bestaan dus uit de com-binatie van calcium en oxaalzuur. Oxaalzuur is een plantaardig product,dat bij de mens, voor zover bekend, nutteloos is. Normaal wordt hetslechts in kleine hoeveelheden in de lever geproduceerd. Door het etenvan producten die rijk zijn aan oxaalzuur kan deze stof via de darmenin het lichaam worden opgenomen in het bloed. De nieren zullen hetoxaalzuur dan in de urine uitscheiden.
Bij primaire hyperoxalurie type 1 produceert het lichaam veel meeroxaalzuur dan normaal. Dit oxaalzuur komt dan in het bloed terecht enwordt dan in principe door de nieren in de urine uitgescheiden.Patiënten met PH1 hebben dus een verhoogde uitscheiding van oxaal-zuur in de urine, en vandaar de term hyperoxalurie.
Oxaalzuur is in lage concentraties al in staat om met calcium een ver-binding aan te gaan, waardoor er stenen kunnen ontstaan: calciumoxa-laat nierstenen. Er kan ook een diffuse neerslag van calciumoxalaat inde niertubuli ontstaan. De niertubuli zijn de verzamelbuisjes waarinurine wordt opgevangen na filtratie. Het neerslaan van calciumoxalaatin de niertubuli wordt nefrocalcinose genoemd. Dit kan zichtbaar wor-den op een nierecho, of onder de microscoop in een nierbiopt. Door devoortdurende aanslag van calciumoxalaat in de nieren, kan de nier-functie worden aangetast. Dit leidt tot nierinsufficiëntie. De nieren zui-veren het bloed van afvalstoffen. Door nierinsufficiëntie hopen afval-stoffen zich op en zal ook de concentratie van oxaalzuur in bloed toe-nemen. Daardoor kan een vicieuze cirkel ontstaan waarbij steeds meercalciumoxalaat in de nieren neerslaat. Uiteindelijk ontstaat een termi-nale (volledige) nierinsufficiëntie. Ook kan calciumoxalaat op andereplaatsen in het lichaam neerslaan, zoals bot, zenuwweefsel, netvlies enbloedvaten. Dit beeld van systemische neerslag van calciumoxalaatheet oxalose.
De lever van mens en dier is uitgerust om de stof glyoxylzuur, waaruit
Nierschade
CHAPTER 11
blz. 142
VAN WOERDEN 5/19/08 8:53 AM Pagina 142

oxaalzuur kan ontstaan, om te zetten in een nuttig stof: het aminozuur(een bouwsteen van eiwitten) glycine. Glyoxylzuur is dus de precursorvan oxaalzuur.
glyoxylzuur -------- AGT ----------> glycineHet enzym dat deze reactie mogelijk maakt is AGT (alanine:glyoxylaataminotransferase). Bij AGT-deficiëntie, zal glyoxylzuur niet in glycineworden omgezet. Het glyoxylzuur wordt dan omgezet in oxaalzuur enin glycolzuur.
Het enzym AGT is een eiwit, dat bestaat uit 392 aminozuren. De pro-ductie van AGT geschiedt vrijwel uitsluitend in levercellen. De codevoor de opbouw van AGT ligt verankert op het gen AGXT.
Bij PH1 werkt het enzym AGT niet of onvoldoende (1). De werking vanAGT kan in een leverbiopt worden gemeten. AGT-deficiëntie kan ont-staan door mutaties (fouten) op het AGXT-gen. De genmutaties kunnenertoe leiden dat:
1. er weinig tot geen AGT wordt gevormd;2. er niet-functioneel AGT wordt gevormd;3. er wel AGT wordt gevormd, maar dat dit AGT op de verkeerde
plaats in de cel wordt afgeleverd, waar het niet werkzaam is.Deze organel ‘mistargeting’ is meestal niet absoluut, waardoor erbij patiënten met een dergelijke mutatie vaak rest-activiteit vanhet AGT aantoonbaar is.
In alle cellen spelen verschillende biochemische processen zich tege-lijkertijd af. Daartoe zijn cellen, waaronder dus ook levercellen, inge-richt met diverse compartimenten. Binnen de levercel als chemischefabriek zijn er dus deelfabrieken met elk een eigen functie. Deze com-partimenten worden organellen genoemd. Voorbeelden van organellenzijn: mitochondriën (energieproductie), lysosomen (afbraak van afval-stoffen) en peroxisomen. Peroxisomen zijn zo genoemd omdat ze instaat zijn om het schadelijke waterstofperoxide te neutraliseren.Daarnaast hebben ze een belangrijke functie bij het verteren vanbepaalde vetten, de zogenaamde langketen vetten waaruit de mito-chondriën vervolgens energie kunnen maken. Ook speelt een aantalafzonderlijke biochemische reacties zich in de peroxisomen af voorverschillende doeleinden. Eén van die reacties is de omzetting van gly-oxylzuur in glycine, gekatalyseerd door het enzym AGT. AGT verrichtdus zijn werkzaamheden in het peroxisoom. Bij de meeste mensen isAGT uitsluitend peroxisomaal gelokaliseerd (2). Bij andere dieren,meestal vleeseters, kan het echter ook mitochondriaal zijn gelokali-seerd (3,4). Sommige knaagdieren, zoals muizen, hebben AGT in zowelperoxisomen als mitochondriën.
AGT
AGT-deficiëntie
Comparti-mentalisatie
van de cel:localisatie
van AGT
CHAPTER 11
blz. 143
VAN WOERDEN 5/19/08 8:53 AM Pagina 143

De code voor het aanmaken van AGT bevindt zich op het DNA in dekern van cellen. Er is één gen, genaamd AGXT, dat hiervoor verant-woordelijk is. Dit gen is gelokaliseerd op chromosoom 2q37.3. Er zijntwee varianten van het AGXT-gen. Deze varianten worden het major enhet minor allel genoemd. Van het minor allel is sprake als er 74 extraingevoegde baseparen (bouwstenen) aan het begin van het gen voorko-men, en één specifieke puntmutatie, leidend tot de verandering vaneen proline-residu in een leucine aminozuur op positie 11. Van de alge-mene (gezonde) Westerse populatie is 20% drager voor het minor allel.In 4% komt het minor allel homozygoot voor, d.w.z. op beide ouderlijkeallelen en leidt - voor zover bekend - niet tot hyperoxalurie. Wel blijkt5% van het AGT zich in het mitochondrion te bevinden in plaats van hetperoxisoom. Inmiddels zijn meer dan 50 mutaties voor het AGXT-genontdekt bij patiënten met PH1. De helft daarvan ligt op het minor allel.Uit celstudies is gebleken dat er AGXT-gen-mutaties zijn, die alleen lei-den tot verlaging van AGT-activiteit als ze op het minor allel voorko-men. Het bekendste voorbeeld daarvan is de Gly170Arg mutatie. Dit heeft twee gevolgen voor AGT:
1. de AGT-activiteit wordt verlaagd, tot 35% van normaal;2. het enzym AGT is voor 90% in de mitochondriën en 10% in de
peroxisomen gelokaliseerd. Dit komt doordat dimerisatie nietoptreedt, het enzym minder “gevouwen” wordt, en toegankelijkerwordt voor import in het mitochondrion. Dit effect lijkt ookplaats te vinden bij de Phe152Ile mutatie in combinatie met hetminor allel.
De diagnose PH1 kan op verschillende manieren worden gesteld.Symptomen die aanleiding zijn om aan PH1 te denken, zijn nierstenen,nefrocalcinose, hematurie, recidiverende urineweginfecties (door nier-stenen, of nefrocalcinose), en tekenen van nierinsufficiëntie zoals ern-stige vermoeidheid en bloedarmoede. Gezien de sequentie van (1)mutaties op het AGXT-gen, (2) deficiëntie van AGT en (3) verhoogde uit-scheiding van oxaalzuur en glycolzuur in urine kunnen deze drie ken-merken worden gebruikt voor diagnostiek:
■ bepaling van oxaal- en glycolzuur in urine (deze zijn meestalbeiden verhoogd, hoewel glycolzuur soms normaal blijkt te zijn)
■ gendiagnostiek■ bij twijfel wordt het enzym AGT gemeten in een leverbiopt. Het
ontbreken of sterk verminderd zijn van enzymactiviteit is hetultieme bewijs voor PH1. Vaak is nog een bepaald percentage vanhet AGT-enzym actief, de zogenaamde restactiviteit.
Genetica:AGXT-gen
Diagnose
CHAPTER 11
blz. 144
VAN WOERDEN 5/19/08 8:53 AM Pagina 144

De behandeling van patiënten met primaire hyperoxalurie type 1 isonder te verdelen in:
1. conservatieve behandeling2. transplantatie
Bij conservatieve behandeling streeft men ernaar de schade van deoxaalzuur-overproductie voor de nieren te beperken. Dit kan door:
■ hyperhydratie: het drinken van voldoende vocht (3 liter per m2 lichaams-oppervlak) waardoor de oxaalzuurconcentratie in urine wordtverlaagd, en er minder snel een verbinding van oxaalzuur metcalcium ontstaat.
■ medicatie:kaliumcitraat: citraat zorgt voor het wegvangen van calcium in de urine, waardoor het zich niet aan oxaalzuur kan binden.Tevens wordt de pH van de urine verhoogd, waardoor oxaalzuurbeter blijft opgelost;pyridoxine (=vitamine B6): dit vitamine wordt in het lichaamomgezet in pyridoxal-5-fosfaat, de co-factor (hulpstof) van AGT.Bij sommige patiënten met PH1 blijkt pyridoxine in staat om deoxaalzuuruitscheiding in urine sterk te verminderen, waarbij ervermindering van nierschade en klachten wordt gezien (5);orthofosfaat: dit lijkt qua werking op citraat, hoewel er minderstudies zijn gedaan naar de dosering en het effect bij PH1 (5); magnesiumoxide:dit lijkt, vooral in combinatie met kaliumcitraat, de oplosbaar-heid van oxaalzuur te verbeteren. Nadeel is echter dat het kanleiden tot diarree, omdat het in de darm water aantrekt.Vochtverlies door diarree werkt het ontstaan van nierstenen inde hand, waartegen het gebruik van magnesiumoxide moet worden afgewogen.
Bij transplantatie kan het gaan om een niertransplantatie, levertrans-plantatie, of beide. De niertransplantatie vervangt de versteende nierenvan de patiënt met PH1. Door de levertransplantatie wordt het defecteenzym AGT vervangen en wordt de lichaamseigen lever verwijderd.Omdat niet alle patiënten, zowel volwassenen als kinderen, met pri-maire hyperoxalurie type 1 het dialysestadium bereiken, zullen nietalle patiënten direct in aanmerking hoeven komen voor een levertrans-plantatie. Alleen als nierinsufficiëntie onafwendbaar is, en met con-ventionele therapie geen verlaging van oxaalzuur-uitscheiding isbereikt, is deze vorm van transplantatie aangewezen. Daarbij wordteventueel de lever in eerste instantie getransplanteerd, en de nier pas
Behandeling
CHAPTER 11
blz. 145
VAN WOERDEN 5/19/08 8:53 AM Pagina 145

nadat de grote voorraad oxaalzuur uit het lichaam is verwijderd doorintensieve pre-, per- en postoperatieve hemodialyse. Het kan soms welmeer dan een jaar duren, voordat een dergelijke stabiele situatie isbereikt. Deze procedure wordt sequentiële lever-niertransplantatiegenoemd.
ZELLWEGER SPECTRUM DISORDERS (ZSDs)
Een aparte categorie vormen de zogenaamde patiënten met Zellwegerspectrum disorders (ZSDs). Dit zijn patiënten met een gegeneraliseer-de peroxisomale aanlegstoornis. Door mutaties in genen die zorgenvoor de synthese van peroxisomen zijn peroxisomen bij deze patiën-ten totaal afwezig. De meeste enzymen die zich normaal gesproken inde peroxisomen bevinden komen hierbij in het cytosol terecht en zul-len daar snel worden afgebroken. Enkele enzymen blijven echter aan-wezig, zoals het enzym AGT. Patiënten met ZSDs presenteren zich meteen geestelijke en lichamelijke ontwikkelingsachterstand in verschil-lende gradaties. Sommige kinderen gaan naar school en bereiken devolwassen leeftijd, anderen hebben heel ernstige beperkingen en kun-nen zich verbaal nauwelijks uiten. Algemeen werd verondersteld datAGT nog werkzaam was bij deze patiënten. Recent werd echter bij eendrietal ZSD patiënten de combinatie van nierstenen en hyperoxaluriegevonden (7).
Primaire hyperoxalurie is een aandoening, waarbij sommige patiëntenzeer ziek worden en andere (vrijwel) symptoomloos blijven. Aan hetbegin van de studie was er weinig inzicht in de factoren die bepalenhoe ernstig de ziekte verloopt. Een ander onopgelost probleem was deoorsprong van het glyoxylzuur, de voorloper van oxaalzuur. De belangrijkste vragen aan het begin van de studie waren derhalve:
1. Hoe vaak komt de ziekte voor in Nederland (prevalentie en incidentie) en wat is de verschijningsvorm?
2. In hoeverre voorspellen de ernst van de biochemische afwijkingen bij een patiënt het beloop van de ziekte?
3. In hoeverre voorspelt een bepaalde genmutatie het beloop van de ziekte?
4. Is er een model te ontwikkelen, waarbij de productie van oxaalzuur door het lichaam op betrouwbare wijze te meten is om nieuwe medicatie te testen?
5. Welke stoffen leiden tot de vorming van glyoxylzuur, de voorloper van oxaalzuur?
6. Welke gevolgen heeft de afwezigheid van peroxisomen bij patiënten met ZSDs voor het voorkomen van hyperoxalurie eneventuele nierschade?
Doel van hetonderzoek
CHAPTER 11
blz. 146
VAN WOERDEN 5/19/08 8:53 AM Pagina 146

Onderzoek naar het voorkomen van PH1 in de bevolking was slechtseenmaal verricht, namelijk in Frankrijk. In Nederland was hieroverniets bekend. Ook was geen relatie aangetoond tussen enerzijds hetgenotype (het soort van de mutaties in het AGXT-gen) en de biochemi-sche afwijkingen (hoogte van de oxaalzuuruitscheiding in de urine,AGT-restactiviteit) en anderzijds het klinisch fenotype (leeftijd waaropde klachten ontstaan, behoud of verlies van nierfunctie). Naar aanlei-ding van Zwitsers, Duits en Frans onderzoek werd verondersteld, dater drie vormen van PH1 te onderscheiden zijn (8, 9,10):
1. een ernstige vorm, met symptomen op de kinderleeftijd en ontwikkeling van nierinsufficiëntie;
2. een milde vorm die zich op volwassen leeftijd presenteert, met weinig symptomen en behoud van nierfunctie;
3. een intermediaire vorm met klachten op de kinderleeftijd en ontwikkeling van nierinsufficiëntie bij sommigen.
Het doel van het onderzoek was in de eerste plaats het in kaart bren-gen van een cohort van alle Nederlandse patiënten met PH1. De klach-ten, en het beloop van de patiënten, ook met betrekking tot de nier-functie, werd beschreven om een zo compleet mogelijk beeld te krijgenvan de het spectrum waarin PH1 zich kan openbaren. Daarbij werd eenaantal factoren gemeten die misschien het ontwikkelen van nierschadezou kunnen voorspellen. De onderzochte factoren waren: leeftijd waar-op eerste symptomen ontstaan, aanwezigheid van nefrocalcinose,hoogte van oxaalzuur in de urine, mate van AGT-restactiviteit, matevan reactie op pyridoxine-therapie. Hoewel onderzoek naar genmuta-ties had laten zien dat er een verband was tussen verschillende typenAGXT-gen-mutaties en de verlaging van AGT-activiteit, was er nog geenrelatie aangetoond tussen bepaalde AGXT-gen-mutaties en het beloopvan de ziekte PH1. Daarom werd bij zoveel mogelijk patiënten het typeAGXT-gen-mutatie bepaald om een relatie te leggen tussen enerzijds degenetische constitutie van PH1 patiënten, en anderzijds de ernst vande klachten en de mate van nierschade. Een apart onderzoek betrof eencohort van patiënten met ZSDs. Gezien het voorkomen van hyperoxa-lurie bij enkele patiënten met ZSDs, werd een groot cohort vanNederlandse patiënten met ZSDs onderzocht op de aanwezigheid vanhyperoxalurie en eventuele nierproblemen, omdat dit wellicht eenonderbelicht aspect was van patiënten met ZSDs, en consequenties kanhebben voor behandeling.
Onderzoek naar nieuwe mogelijkheden voor therapie kent een aantalbeperkingen. Twee daarvan werden aangegrepen voor verder onder-zoek, namelijk: (1) bepaling van de zogenaamde rate of appearance,dat wil zeggen de snelheid van verschijnen in het bloed, van oxalaat en(2) celbiochemisch onderzoek naar de herkomst van oxaalzuur. Met een
CHAPTER 11
blz. 147
VAN WOERDEN 5/19/08 8:53 AM Pagina 147

speciale techniek waarmee kleine concentraties stoffen kunnen wordengemeten, is het mogelijk om te berekenen hoeveel oxaalzuur per tijds-eenheid in het bloed komt. Dit is een nauwkeuriger afspiegeling van deoxaalzuurproductie in het lichaam dan het meten van de uitscheidingvan oxaalzuur in urine. Immers, dit laatste is bij veel patiënten nietmogelijk omdat ze een nierinsufficiëntie hebben ontwikkeld. Door derate of appearance te berekenen kan de werking van potentiële nieuwemedicijnen worden onderzocht. Onderzoek naar de herkomst vanoxaalzuur werd verricht door gebruik te maken van een muismodel.Door middel van genetische modificatie werd deze zogenaamde Agxt -/-
muis ontwikkeld. Deze muis mist het enzym AGT waardoor hyperoxa-lurie bij deze muis ontstaat. Onderzoek naar de herkomst van oxaal-zuur is nodig om nieuwe vormen van behandeling te kunnen ontwik-kelen die ingrijpen op de biochemische reacties waaruit het oxaalzuurontstaat.
In Hoofdstuk 1 wordt een overzicht gegeven van de kennis over pri-maire hyperoxalurie type 1, van de beschrijving tot de eerste patiënt in1925 (11), tot de ontdekking van de biochemische en genetische oor-zaak van PH1. (1, 12, 13). Aan het eind van het hoofdstuk wordtbeschreven welke vragen aanleiding waren om dit proefschrift op teschrijven.
Hoofdstuk 2 beschrijft een onderzoek naar het aantonen van hyper-oxalurie in urine. Daarvoor is een portie urine nodig, dat in een con-tainer wordt opgevangen. Het was gebruikelijk om zoutzuur tevorenaan de container toe te voegen om te voorkomen dat het oxaalzuur metcalcium kristallen vormt en neerslaat. Vanwege gevaar voor brandwon-den door spetters van zoutzuur en het gevaar op inademen van zout-zuurdamp, werd onderzocht of zoutzuur ook pas later, op het labora-torium, kan worden toegevoegd. Daartoe werd door drie patiënten metPH1, van wie één dialyse kreeg, en drie controlepersonen die geen PH1hebben, van wie één ook dialyse onderging vanwege een andere oor-zaak van nierinsufficiëntie, ochtendurine in twee bokalen opgevangen:één met en één zonder zoutzuur. Het bleek geen verschil te maken ophet gehalte aan oxaalzuur dat in het laboratorium werd gemeten.Daarom stellen wij dat het gebruik van zoutzuur voor het sparen vanurine voor oxaalzuurmeting niet nodig is.
In Hoofdstuk 3 beschrijven we de groep van Nederlandse PH1 patiën-ten: de leeftijd waarop de klachten ontstaan, het type van de klachten,de nierfunctie, de biochemische karakteristieken wat betreft urineoxaalzuur, en AGT activiteit en de behandeling. Tussen 1970 en 2000werden 57 patiënten met PH1 gediagnosticeerd, een opvallend grootaantal in vergelijking met een studie uit Frankrijk. De prevalentie komtdaarmee op bijna 3 patiënten per miljoen mensen. Deze relatief hoge
CHAPTER 11
blz. 148
VAN WOERDEN 5/19/08 8:53 AM Pagina 148

prevalentie in vergelijking met onderzoeken in andere landen komtmede doordat het mogelijk was om gedetailleerder te zoeken naar pati-ënten. Ook vonden we opvallend veel volwassenen die pas werden ont-dekt nadat ze al dialyse nodig hadden, hoewel de meeste van hen al lan-gere tijd aan nierstenen leden. Daarom denken we dat er nog veel PH1patiënten niet gediagnosticeerd zijn en dat het werkelijke aantalNederlandse patiënten met PH1 groter is. Ook bleek dat patiënten die opkinderleeftijd klachten kregen, niet altijd later dialyse nodig hadden. Destrikte indeling van patiënten met PH1 in een milde groep, ernstigegroep, en intermediaire groep, zoals was voorgesteld, lijkt daarmee nietcorrect. Als voorspellende factoren bleek dat het niet-werkzaam zijnvan pyridoxine, en de aanwezigheid van nefrocalcinose vaker voor-kwam bij patiënten die een terminale nierinsufficiëntie ontwikkelden.
Hoofdstuk 4 geeft een overzicht van de resultaten van mutatie-analy-se die werd uitgevoerd bij een grote groep patiënten met PH1. Van 33patiënten uit de groep die in Hoofdstuk 3 werd beschreven, werd eenDNA-analyse op het AGXT-gen uitgevoerd en vergeleken met de uit-komst wat betreft nierfunctie. De zogenaamde Gly170Arg-substitutiekwam bij meer dan 40% voor. Deze groep had een goede reactie op pyri-doxine (Vitamine B6) in een hoge dosering (5-15 mg/kg/dag). Dit leid-de tot behoud van nierfunctie. Bij sommigen van hen was reeds een ter-minale nierinsufficiëntie ontstaan. Dit kwam doordat de diagnose bijhen pas laat was gesteld, namelijk nadat dialyse nodig bleek. Het effectvan pyridoxine op de oxaalzuuruitscheiding kon daarom pas na eeneventuele niertransplantatie worden beoordeeld. Patiënten met deGly170Arg substitutie behielden hun transplantaatnier veel langer dantot dan toe voor mogelijk gehouden was, doordat er geen nieuwe oxa-laatstapeling optrad. De Phe152Ile- substitutie liet ook een goed effectzien op pyridoxine, en werd voor het eerst bij zoveel patiënten tegelijkgevonden. Andere mutaties, waaronder de zogenaamde ‘frameshift’mutatie c.33_34insC, en een nieuwe Gly82Arg- substitutie leidden toteen zeer ongunstig beloop. Alle patiënten met PH1 die werden ontdektdoor screening in families met PH1 bleken hun nierfunctie te kunnenbehouden door het tijdig starten van conservatieve therapie. Bij som-migen hield dit in, dat pyridoxine vroegtijdig leidde tot verlaging vande oxaalzuurconcentratie in urine. Bij anderen resulteerde het gebruikvan hyperhydratie in langdurig behoud van nierfunctie. De klinischeimplicatie van deze bevindingen is, dat vroegtijdig moet wordengescreend op primaire hyperoxalurie, om behandeling vroegtijdig tekunnen starten en nierschade te kunnen voorkomen.
In Hoofdstuk 5 wordt onderzocht of er inderdaad sprake is van‘onderdiagnostiek’ van patiënten met PH1. Daartoe werden alle patiën-ten opgespoord, bij wie ooit hyperoxalurie was ontdekt in het labora-torium voor algemene klinische chemie van het AMC. Patiënten bij wie
CHAPTER 11
blz. 149
VAN WOERDEN 5/19/08 8:53 AM Pagina 149

de concentratie oxaalzuur te hoog was werden benaderd voor het ana-lyseren van een portie 24-uurs-urine. Van de 150 patiënten bij wie ooitoxaalzuuranalyse in de urine was gedaan, was de uitslag bij 32 te hoog.Van deze 32 patiënten konden er 25 opgespoord worden voor vervol-gonderzoek. Bij zes van deze 25 patiënten bleek het oxaalzuurgehalteopnieuw te hoog. Uiteindelijk bleek één patiënt mutaties in het AGXT-gen te hebben, bewijzend voor de diagnose PH1. Vier patiënten haddeneen darmziekte waardoor hyperoxalurie ontstond door toegenomenopname van oxaalzuur uit de voeding in de darm. Dit is een vorm vanzogenaamde ‘secundaire hyperoxalurie’. Bij één patiënt met licht ver-hoogde waarden van hyperoxalurie werd geen oorzaak gevonden. Dezemethode is dus geschikt om nog niet ontdekte patiënten op te sporenen op tijd te behandelen en laat zien dat PH1 inderdaad ondergediag-nosticeerd is in Nederland.
Het onderzoek naar het voorkomen van hyperoxalurie in een cohortvan patiënten met Zellweger spectrum disorders wordt in Hoofdstuk 6beschreven. Hyperoxalurie blijkt bij 83% (19 van de 23) van de onder-zochte patiënten voor te komen. Bij vijf patiënten waren er symptomenvan nierziekte. Er blijkt sprake te zijn van een (indirect) verband tus-sen de mate van hyperoxalurie enerzijds en de ernst van de neurologi-sche verschijnselen anderzijds: de patiënten met de ernstigste vormvan de ZSDs, hadden de hoogste uitscheiding van oxaalzuur in urine.De mildste patiënten die de volwassen leeftijd hadden bereikt engeestelijk het minst waren beschadigd bleken geen hyperoxalurie tehebben. Hoewel het enzym AGT aanwezig is bij deze patiënten zorgt deafwijkende, extra-peroxisomale, localisatie voor dysfunctioneren vanhet enzym. Waarschijnlijk ontstaat de hyperoxalurie bij deze patiëntenhierdoor. De variatie in de uitscheiding van oxaalzuur zou kunnen ont-staan door een geringe restactiviteit van AGT buiten het peroxisoom ofdoor een geringe import van AGT in peroxisomen. Het voorkomen vanperoxisomale mozaïeken in ZSDs zou een additionele verklaring kun-nen zijn voor milde ZSD patiënten zonder hyperoxalurie. In verbandmet het beschermen van de nieren door voldoende vochtintake, hetgebruik van citraat, en het opsporen van nierstenen bij patiënten diegeen klachten kunnen verbaliseren, is een urinescreening van alle pati-ënten met ZSDs noodzakelijk.
In Hoofdstuk 7 beschrijven we het onderzoek dat met behulp van sta-biele isotopen werd uitgevoerd, om de rate of appearance van oxaal-zuur te berekenen. De techniek werd onderzocht bij vier patiënten envier controle-individuen. De rate of appearance van oxaalzuur bleekeen goede afspiegeling van de hoeveelheid oxaalzuur welke in de urinewerd gemeten. Daarmee kan deze techniek worden gebruikt om dewerkzaamheid van nieuwe therapieën op de endogene productie vanoxaalzuur te evalueren.
CHAPTER 11
blz. 150
VAN WOERDEN 5/19/08 8:53 AM Pagina 150

In Hoofdstuk 8 presenteren wij het onderzoek waarbij levercellen vande Agxt -/- muis werden gebruikt om de productie van oxaalzuur uitmogelijke precursors te meten. Tot onze verrassing bleek geen van dezeven onderzochte stoffen van directe invloed op de oxaalzuurpro-ductie. De productie van oxaalzuur uit twee bekende, directe, precur-sors was zeer beperkt. Dit kan een afspiegeling zijn van de kleine meta-bole flux die door het onderzochte systeem loopt of wordt veroorzaaktdoor het ‘wegvangen’ van de precursor in mitochondriën. Het toedie-nen van alanine leek de enzymatische werking van het enzym AGT,waarvoor de cellen deficiënt waren, te herstellen. Dit kan komen, door-dat een belangrijk deel van glyoxylzuur ook op een andere plaats in decel wordt verwerkt, namelijk in mitochondriën van de muis wordtomgezet in glycine.
Aanbevelingen voor vervolgonderzoek worden gedaan aan het eind vande General Summary in Hoofdstuk 9.
Deze zijn:
■ Het uitvoeren van een follow-up studie van het reeds bestaandecohort PH1 patiënten, om de genotype-fenotype-relatie verder teonderzoeken en te bevestigen;
■ Het vergroten van het nationale PH1 cohort door patiënten met(recidiverend) niersteenklachten op oxaalzuur te onderzoeken,of door het screenen van patiënten bij wie reeds hyperoxalurie is vastgesteld, zoals gedaan in Hoofdstuk 5.
■ Vervolgonderzoek naar patiënten met onbekende genmutaties,om de aard van de nieuwe mutaties te ontdekken;
■ Onderzoek naar de voorspellende waarde van de hoogte vanoxaalzuuruitscheiding op het behoud van nierfunctie door hetpoolen van meer data;
■ Een follow-up studie van de patiënten met Zellweger spectrumdisorders om eventuele nierpathologie vroegtijdig op te sporen,en verder onderzoek naar de relatie tussen peroxisoom-mosai-cisme en hyperoxalurie;
■ Het gebruik van de stabiele isotopen-verdunningstechniek bij deevaluatie van de werkzaamheid van nieuwe therapieën, zoalsscavengers van glyoxylzuur;
■ Metabole studies in hepatocyten van een Agxt -/- muis om de rolvan precursors op oxaalzuurproductie verder te onderzoeken.
CHAPTER 11
blz. 151
VAN WOERDEN 5/19/08 8:53 AM Pagina 151

1. Danpure CJ, Jennings PR.
Peroxisomal alanine:glyoxylate amino-
transferase deficiency in primary
hyperoxaluria type I.
FEBS Lett 1986;201:20-24.
2. Cooper PJ, Danpure CJ, Wise PJ,
Guttridge KM. Immunocytochemical
localization of human hepatic alanine:
glyoxylate aminotransferase in control
subjects and patients with primary
hyperoxaluria type 1. J Histochem
Cytochem 1988;36:1285-94.
3. Birdsey GM, Danpure CJ.
Evolution of alanine:glyoxylate amino-
transferase intracellular targeting:
structural and functional analysis of
the guinea pig gene. Biochem J
1998;331:49-60.
4. Holbrook JD, Birdsey GM, Yang
Z, Bruford MW, Danpure CJ. Molecular
adaptation of alanine:glyoxylate ami-
notransferase targeting in primates.
Mol Biol Evol 2000;17:387-400.
5. Milliner DS, Eickholt JT,
Bergstralh EJ, Wilson DM, Smith LH.
Results of long-term treatment with
orthophosphate and pyridoxine in
patients with primary hyperoxaluria.
N Engl J Med 1994;331:1553-8.
6. Danpure CJ, Fryer P,
Griffiths S, Guttridge KM, Jennings PR,
Allsop J et al.
Cytosolic compartmentalization of
hepatic alanine:glyoxylate amino-
transferase in patients with aberrant
peroxisomal biogenesis and its effect
on oxalate metabolism.
J Inherit Metab Dis 1994;17:27-40
7. Barth PG, Gootjes J, Bode H,
Vreken P, Majoie CB, Wanders RJ.
Late onset white matter disease in
peroxisome biogenesis disorder.
Neurology 2001;57:1949-55.
8. Kopp N, Leumann E. Changing
pattern of primary hyperoxaluria in
Switzerland. Nephrol Dial Transplant
1995;10:2224-27.
9. Latta K, Brodehl J. Primary
hyperoxaluria type I.
Eur J Pediatr 1990;149:518-22.
10. Cochat P, Deloraine A, Rotily M,
Olive F, Liponski I, Deries N.
Epidemiology of primary hyperoxaluria
type 1. Société de Néphrologie and the
Société de Néphrologie Pédiatrique.
Nephrol Dial Transplant 1995;
10 Suppl 8:3-7.
11. Lepoutre C. Calculs multiples
chez un enfant: Infiltration du paren-
chyme renal par des depots cristallins.
J Urol 1925;20:424.
12. Takada Y, Kaneko N, Esumi H,
Purdue PE, Danpure CJ. Human peroxi-
somal L-alanine: glyoxylate amino-
transferase. Evolutionary loss of a
mitochondrial targeting signal by point
mutation of the initiation codon.
Biochem J 1990;268:517-20.
13. Purdue PE, Lumb MJ, Fox M,
Griffo G, Hamon-Benais C, Povey S,
Danpure CJ. Characterization and
chromosomal mapping of a genomic
clone encoding human alanine:
glyoxylate aminotransferase.
Genomics 1991;10:34-42.
REFERENTIES
CHAPTER 11
blz. 152
VAN WOERDEN 5/19/08 8:53 AM Pagina 152

APPENDIX 01
page 153
APPENDIX 01
Oxalosis:Reports of oxalosis
VAN WOERDEN 5/19/08 8:53 AM Pagina 153

APPENDIX 01
Organs or system involved
BONE
SKIN
EYE
APPENDIX 01
page 154
OXALOSIS: Reports of oxalosis
Year of Description Number of patients Reference
report affected/ total number
--------------------------------------------------------------------------------------------------------------------1987 Diffuse sclerosis 1/1 Nemcek et al. (15) 1989 Subperiostal resorption 1/1 Brady et al. (4) 1990 Increased density, 1/1 Schneider et al. (18)
sclerotic changes 1991 Diffuse sclerosis, 20/20 Benhamou et al. (2)
bone translucency, subperiosteal phalangeal resorption
1977 Crystals in marrow Gottlieb et al. (7) 1982 Soft tissue calcifications 3/7 Martijn et al. (11)
Osseous changes 3/7 1983 Osseous changes: 1/1 Anderson et al. (1)
sclerotic bands 1990 Osteitis fibrosa cystica, 1/1 Stull et al. (22)
osteosclerosis -------------------------------------------------------------------------------------------------------------------- 1974 Macroscopic depositions 1/1 Jansen et al. (10)
at the skin Subepidermal deposits of crystals
1989 Livedo reticularis: 1/1 Bodemer et al. (3) oxalate crystals in the wall of the blood vessels of the skin
1967 Calcified elastic fibers, 1/1 Smeenk et al. (21) no oxalate at the site of the skin lesions
-------------------------------------------------------------------------------------------------------------------- 1977 Flecked retina 1/1 Gottlieb et al. (7) 1988 Oxalate deposition in 8/24 Small et al. (20)
the retina vessel wall Black subretinal ringlets, Small et al. (19) lesions, flecks
1984 Calcium Oxalate crystal 2/2 Meredith et al. (13) deposition in all vascularized ocular tissues: conjunctiva,iris, ciliary body, inner layers of the retina, choroids, episclera,sclera, ocular muscles
1991 Calcium Oxalate crystal 1/1 Sakamoto et al. (17) deposition not related to vascularized ocular tissues: outer plexiform layer, nuclear layer
VAN WOERDEN 5/19/08 8:53 AM Pagina 154

BRAIN ANDMENINGES
VASCULAR/MISCELLANEOUS
NERVES
HEART
MISCELLANEOUS
1977 Deposition in meninges, 1/1 Haqqani et al. (9) in walls of congested meningeal vessels. In the brain.
--------------------------------------------------------------------------------------------------------------------
1986 Vascular calcifications 2/7 Day et al. (6) Soft-tissue calcifications 3/7 Skeletal abnormalities 6/7osteopenicity, osteodystrophy, dense metaphyseal bands, submarginal metaphyseal lucency, a wide translucent metaphyseal zone with sclerosis of the adjacent diaphysis, metaphyseal waisting
1990 Vascular calcifications Stull et al. (22)
--------------------------------------------------------------------------------------------------------------------
1976 Axonal degeneration 1/1 Hall et al. (8) Segmental demyelination Oxalate crystals in axons
1975 calcium oxalate within 1/1 Moorhead et al. (14) the endoneurium
-------------------------------------------------------------------------------------------------------------------- 1981 Oxalate infiltration 1/1 Massie et al. (12)
of the sinoatrial node and its approaches
1991 Dilated cardiomyopathy 1/1 Rodby et al. (16) and arrhythmias
--------------------------------------------------------------------------------------------------------------------
1952 Scattered crystals 1/1 Chou et al. (5) heart, thymus, lungs, spleen, pituitary gland
1965 Depositions 2/2 van Gastel et al. (23) as described above Vascular system: oxalate between tunica mediaand lamina elastica interna Oxalate in interstitium 1/1 Hall et al. (8) of nerve cells choroids plexus, pineal gland
VAN WOERDEN 5/19/08 8:53 AM Pagina 155

1. Anderson DE, Davidson JK,
Catto ME. Case report 227: primary
hyperoxaluria (oxalosis). Skeletal
Radiol 1983;9:266-71.
2. Benhamou CL, Bardin T,
Tourliere D, Voisin L, Audran M,
Edouard C et al. Bone involvement in
primary oxalosis. Study of 20 cases.
Rev Rhum Mal Osteoartic 1991;
58:763-69.
3. Bodemer C, Flament F,
Grunfeld JP, De PY. Primary
oxalosis and livedo reticularis.
Apropos of a case.
Ann Dermatol Venereol 1989;
116:721-24.
4. Brady HR, Fay WP, Meema HE,
Rabinovich S, Rapoport A, Oreopoulos
DG. Oxalate bone disease--an emerging
form of renal osteodystrophy. Int J
Artif Organs 1989;12:715-19.
5. Chou LY, Donohue WL.
Oxalosis; possible inborn error of
metabolism with nephrolithiasis
and nephrocalcinosis due to calcium
oxalate as the predominating features.
Pediatrics 1952;10:660-66.
6. Day DL, Scheinman JI, Mahan J.
Radiological aspects of primary hyper-
oxaluria. AJR Am J Roentgenol
1986;146:395-401.
7. Gottlieb RP, Ritter JA. ‘Flecked
retina’ - an association with primary
hyperoxaluria. J Pediatr 1977;90:939-42.
8. Hall BM, Walsh JC, Horvath JS,
Lytton DG. Peripheral neuropathy com-
plicating primary hyperoxaluria.
J Neurol Sci 1976;29:343-49.
9. Haqqani MT. Crystals in brain
and meninges in primary hyperoxalu-
ria and oxalosis. J Clin Pathol
1977;30:16-18.
10. Jansen LH, Groeneveld JL, Van
Der Meer JB. Deposition of calcium oxa-
late in the skin in two patients suffe-
ring from oxalosis caused by primary
hyperoxaluria. Arch Dermatol Forsch
1974;250:323-50.
11. Martijn A, Thijn CJ. Radiologic
findings in primary hyperoxaluria.
Skeletal Radiol 1982;8:21-24.
12. Massie BM, Bharati S,
Scheinman MM, Lev M, Desai J,
Rubeson E, Schmidt W. Primary
oxalosis with pan-conduction cardiac
disease: electrophysiologic and
anatomic correlation.
Circulation 1981;64:845-52.
13. Meredith TA, Wright JD,
Gammon JA, Fellner SK, Warshaw BL,
Maio M. Ocular involvement in primary
hyperoxaluria. Arch Ophthalmol
1984;102:584-87.
14. Moorhead PJ, Cooper DJ,
Timperley WR. Progressive peripheral
neuropathy in patient with primary
hyperoxaluria. Br Med J 1975;2:312-13.
15. Nemcek AA, Jr., Ziewacz JT,
Christiansen R, Conard FU. A 30-year-
old woman with generalized skeletal
pain. Invest Radiol 1987;22:752-55.
16. Rodby RA, Tyszka TS, Williams
JW. Reversal of cardiac dysfunction
secondary to type 1 primary hyperoxa-
luria after combined liver-kidney trans-
plantation. Am J Med 1991;90:498-504.
REFERENCES
APPENDIX 01
page 156
VAN WOERDEN 5/19/08 8:53 AM Pagina 156

APPENDIX 01
page 157
17. Sakamoto T, Maeda K, Sueishi K,
Inomata H, Onoyama K. Ocular histopa-
thologic findings in a 46-year-old man
with primary hyperoxaluria. Arch
Ophthalmol 1991;109:384-87.
18. Schneider P, Rendl J, Borner W,
Heidbreder E. Primary hyperoxaluria
type 1. Bone scintigraphy, X-ray radio-
graphy, and gamma-ray quantitative
CT. Clin Nucl Med 1991;16:681-83.
19. Small KW, Letson R, Scheinman J.
Ocular findings in primary hyperoxaluria.
Arch Ophthalmol 1990;108:89-93.
20. Small KW, Pollock S, Scheinman J.
Optic atrophy in primary oxalosis.
Am J Ophthalmol 1988;106:96-97.
21. Smeenk G, Vink R. Calcinosis
cutis metastatica in a patient with
primary hyperoxaluria.
Dermatologica 1967;134:356-63.
22. Stull MA, Glass-Royal M.
Musculoskeletal case of the day.
Primary oxalosis with renal osteo-
dystrophy. AJR Am J Roentgenol
1990;154:1334-35.
23. van Gastel C, Dorhout Mees EJ,
Koten JW, de Minjer A. 2 patients with
primary oxalosis. Ned Tijdschr
Geneeskd 1965;109:832-33.
VAN WOERDEN 5/19/08 8:53 AM Pagina 157

VAN WOERDEN 5/19/08 8:53 AM Pagina 158

APPENDIX 02
Reference values for diagnostic tests in primary hyperoxaluria type 1
1. Urinary analysis of oxalate and glycolate2. Plasma analysis of oxalate and glycolate3. Peritoneal fluid analysis of oxalate and glycolate4. AGXT gene mutation analysis5. AGT enzyme analysis
APPENDIX 02
page 159
VAN WOERDEN 5/19/08 8:53 AM Pagina 159

URINE OXALATE mmol/mol creatinine a
Method (Reference) Mean Range Age
Ion-chromatography (32) 131 75-188 <1 month84 29-139 16 - 30 months70 20-121 31 - 50 months56 20-91 51 - 70 months52 22-83 71 - 100 months44 18-71 101 - 130 months42 12-73 131 - 161 months
Body
surface
area
131 75–188 0.16 - 0.24 m2
82 25-139 0.40 - 0.60 m2
73 23-123 0.61 - 0.70 m2
60 14-107 0.71 - 0.80 m2
59 23-95 0.81 - 0.90 m2
50 21-79 0.91 - 1.00 m2
45 23-67 1.01 - 1.20 m2
46 16-76 1.21 - 1.50 m2
27.5 >1.60 m2
Mean b 95% c Age
Ion-chromatography (28) 133 61 - 280 1 month125 57 - 270 1 - 6 months111 51 - 230 7 -12 months
85 40 - 180 1 - 1.5 years66 32 - 140 1.5 - 2.5 years 57 23 - 125 2.5 - 3.5 years 46 18 - 110 3.5 - 4.5 years 38 15 - 100 4.5 - 5.5 years 32 13 - 92 5.5 - 6.5 years27 10 - 80 6.5 - 7.5 years 26 8 - 76 7.5 - 8.5 years 26 8 - 79 8.5 - 9.5 years 25 8 - 79 9.5 - 10.5 years 24 6 - 82 10.5 - 11.5 years 24 7 - 76 11.5 - 12.5 years 24 8 - 72 12.5 - 13.5 years 25 6 - 73 13.5 - 14.5 years APPENDIX 02
page 160
VAN WOERDEN 5/19/08 8:53 AM Pagina 160

Percentiles
5th 95th
Ion-chromatography 141 360 < 6 monthsdried spots (2) 61 162 7 - 24 months
35 126 3-7 years19 76 8 - 16 years15 32 > 16 years
95%
Confidence
Mean Range Interval
Enzyme based 147 77 - 325 60 - 360 0 - 6 monthscolorimetry (13) 72 38 - 132 29 - 174 7 - 24 months
44 18 - 98 19 - 101 2 - 4.9 years42.1 22 - 70 22 - 82 5 years 32.4 12 - 70 15 - 69 9 years 27.5 16 - 53 15 - 50 12 years22.4 10 - 64 9 - 56 14 years 21.9 13 - 39 12 - 40 16 years
Ion- 25 10 - 40 > 18 yearschromatography(8)Enzyme based 0.238 d 0.11 - 0.46 > 20 yearscolorimetry (36)± 2SD
Oxalate excretion in newborn infants Age
Ion-chromatography (28)
99 28 - 338 1 day85 21 - 316 2 day72 18 - 362 3 day91 24 - 346 4 day
117 54 - 257 5 day76 15 - 380 6 day
117 52 - 263 7 day
Average 89 23 - 338
a. Expressed in mmol/mol, conversion factor: 1 mmol/mol = 797 mg/g
b. geometric mean calculated from log-transformed data
c. (95%) = 95% confidence limit, calculated from log-transformed data
d. mmol/24 hours
APPENDIX 02
page 161
VAN WOERDEN 5/19/08 8:53 AM Pagina 161

URINE GLYCOLATE mmol/mol creatinine
Percentiles
Method (Reference) 5th 95th Age
Ion chromatography, 11 109 < 6 monthsdried spots 22 139 7 - 24 months(2) 17 103 3-7 years
18 92 8 - 16 years 6 80 16 years
95%
Confidence
Mean Range Interval
Ion chromatography 175 63 - 363 72 - 425 0 - 6 months(13) 116 58 - 245 46 - 293 7 - 24 months
100 55 - 204 48 - 208 2 - 4.9 years95.5 58 - 229 48 - 191 5 years75.9 45 - 140 46 - 126 9 years75.3 46 - 160 40 - 140 12 years79.3 30 - 166 34 - 186 14 years46.8 22 - 125 22 - 99 16 years
Ion chromatography 38 <69 men > 18 years(8) 52 13 - 90 women > 18 years
Ion chromatography 25 ±12 adults(35) 19e 9 - 35 men
31e 18 - 54 women
Gas chromatography (6) 18 - 94 adults
e median range
APPENDIX 02
page 162
VAN WOERDEN 5/19/08 8:53 AM Pagina 162

PLASMA OXALATE µM
Method (Reference) Mean SD Range
Isotope dilution (3,9,25) 1.39 1.04 - 1.78Enzymatic (24) 1.3 - 3.1Enzymatic (36) 2.5 0.7Gas Chromatography (14) 2.8 1.1Ion-chromatography (2,8) 2.03 0.52 1.18 - 2.50Chemiluminescence (7) 1.8 1.0 adults
3.3 1.7 children
PLASMA GLYCOLATE µM
Method (Reference) Mean Range
Ion-chromatography 7.9 ± 2.4 4.51 - 12.20(16,17,21) Ion-chromatography (8) 4.7 0.4 SE
PERITONEAL FLUID OXALATE mmol/mol creatinine
Method (Reference) Mean ± SD Diagnosis
or Range
Ion chromatography (18) 162,5 ± 70,25 in oxalosis-unrelated
end-stage renal disease
643 ± 219,5 PH1, ESRD
Ion chromatography (16) 35.3 ± 15 in oxalosis-unrelated
end-stage renal disease
181 ± 36 PH1, ESRD
PERITONEAL FLUID GLYCOLATE mmol/mol creatinine
Method (Reference) Mean ± SD Diagnosis
or Range
Gas chromatography - 19.6 15.1-27.5 µmol/dayMass spectrometry (GCMS) (37)Ion chromatography (16) 20.3 ± 4.5 in oxalosis-unrelated
end-stage renal disease
1100 ±740 PH1, ESRD
APPENDIX 02
page 163
VAN WOERDEN 5/19/08 8:53 AM Pagina 163

APPENDIX 02
page 164
AGXT GENE
Overview of the most common AGXT mutations and their influence on the AGT enzyme. An update of sequence variants can be found at www.hgmd.cf.ac.uk/ac
Mutation Amino acid Co-segregation Allele
substitution with polymorphic frequency b
variant a
508 G>A Gly170Arg Minor 25%
731 T>C Ile244Thr Minor 9%
c.33_34insC Major 12%-19%245 G>A Gly82Glu Major
454 T>A Phe152Ile Minor
121 G>A Gly41Arg MajorMinor
613 T>C Ser205Pro Major Japanese population
AGT ACTIVITY
Method (Reference) Mean± SD Range Numbers
Spectrophotometry (4) 0.8 - 2.0 5Spectrophotometry (29) 17.9 - 38.5 9Micro radiochemistry (1) 0.84 - 2.4 8Spectrophotometry 106.7 ±(10-12,34) 19.6 79.8 - 133.7 NDHigh-performance liquid chromatography (22) 7.8 ± 2.9 4.8 - 11.0 9
VAN WOERDEN 5/19/08 8:53 AM Pagina 164

a Polymorphic variant: the haplotype, defined as minor allele
(in the presence of at least a Pro11Leu polymorphism in the first exon)
or major allele without polymorphismsb Allele frequency: as reported in European and North-American studiesc PLP: mutation effects pyridoxal phosphate binding site
Effects on AGT References
Aggregation leads to decreased (15,27)specific activity up to 30% of normal referenceDecreased dimerization90% mitochondrial mistargeting
Aggregation leads to decreased specific activity (33,31)Aggregation in vitroEnzyme not found in vivo
Truncated protein (19,30)PLPc (15)Abolisheshed catalytic activity (26)
Aggregation leads to Decreased specific activity (15)
Major: decreased specific activity by (5)protein destabilizationMinor: aggregation into core-like structures (23)
Decreased stability (20)Degradation
Unity Tissue sample mass
µmol/h·mg protein NDµmol/h·mg proteinµmol/h·mg protein 100 µg
nmol/min·mg protein 500 µg
µmol/h·mg protein 500 - 1000 µg
VAN WOERDEN 5/19/08 8:53 AM Pagina 165

1. Allsop J, Jennings PR, Danpure
CJ. A new micro-assay for human liver
alanine: glyoxylate aminotransferase.
Clin Chim Acta 1987;170:187-93.
2. Blau N, Matasovic A,
Lukasiewicz-Wedlechowicz A,
Heizmann CW, Leumann E.
Simultaneous determination of
oxalate, glycolate, citrate, and
sulfate from dried urine filter paper
spots in a pediatric population.
Clin Chem 1998;44:1554-56.
3. Constable AR, Joekes AM,
Kasidas GP, O'Regan P, Rose GA.
Plasma level and renal clearance of
oxalate in normal subjects and in
patients with primary hyperoxaluria
or chronic renal failure or both.
Clin Sci (Lond) 1979;56:299-304.
4. Danpure CJ, Jennings PR.
Peroxisomal alanine:glyoxylate amino-
transferase deficiency in primary
hyperoxaluria type I. FEBS Lett
1986;201:20-24.
5. Danpure CJ, Purdue PE,
Fryer P, Griffiths S, Allsop J, Lumb MJ
et al. Enzymological and mutational
analysis of a complex primary
hyperoxaluria type 1 phenotype
involving alanine:glyoxylate amino-
transferase peroxisome-to-
mitochondrion mistargeting and
intraperoxisomal aggregation.
Am J Hum Genet 1993;53:417-32.
6. Dietzen DJ, Wilhite TR, Kenagy
DN, Milliner DS, Smith CH, Landt M.
Extraction of glyceric and glycolic
acids from urine with tetrahydrofuran:
utility in detection of primary hyper-
oxaluria. Clin Chem 1997;43:1315-20.
7. Gaulier JM, Lardet G, Cochat P,
Vallon JJ. A serum oxalate assay using
chemiluminescence detection, adapted
to a paediatric population. J Nephrol
1998;11 Suppl 1:73-74.
8. Hagen L, Walker VR, Sutton RA.
Plasma and urinary oxalate and
glycolate in healthy subjects.
Clin Chem 1993;39:134-38.
9. Hodgkinson A, Wilkinson R.
Plasma oxalate concentration and
renal excretion of oxalate in man.
Clin Sci Mol Med 1974;46:61-73.
10. Horvath VA, Wanders RJ.
Rapid identification of primary
hyperoxaluria type I patients using
a novel, fully automated method for
measurement of hepatic alanine:
glyoxylate aminotransferase.
J Inherit Metab Dis 1994;17:336-38.
11. Horvath VA, Wanders RJ.
Re-evaluation of conditions required
for measurement of true alanine:
glyoxylate aminotransferase activity
in human liver: implications for the
diagnosis of hyperoxaluria type I.
Ann Clin Biochem 1994;
31 (Pt 4):361-66.
12. Horvath VAP, Wanders RJA.
Aminooxy acetic acid: A selective
inhibitor of alanine:glyoxylate
aminotransferase and its use in the
diagnosis of primary hyperoxaluria
type I. Clinica Chimica Acta Vol
243(2)(105-114), 1995 1995;105-14.
13. Leumann EP, Dietl A, Mata-sovic
A. Urinary oxalate and glycolate excre-
tion in healthy infants and children.
Pediatr Nephrol 1990;4:493-97.
REFERENCES
APPENDIX 02
page 166
VAN WOERDEN 5/19/08 8:53 AM Pagina 166

APPENDIX 02
page 167
14. Lopez M, Tuchman M,
Scheinman JI. Capillary gas chromato-
graphy measurement of oxalate in plas-
ma and urine. Kidney Int 1985;28:82-84.
15. Lumb MJ, Danpure CJ. Functional
synergism between the most common
polymorphism in human alanine:glyoxy-
late aminotransferase and four of the
most common disease-causing muta-
tions. J Biol Chem 2000;275:36415-22.
16. Marangella M, Petrarulo M,
Bianco O, Vitale C, Finocchiaro P,
Linari F. Glycolate determination
detects type I primary hyperoxaluria
in dialysis patients. Kidney Int
1991;39:149-54.
17. Marangella M, Petrarulo M,
Vitale C, Cosseddu D, Linari F. Plasma
and urine glycolate assays for differen-
tiating the hyperoxaluria syndromes.
J Urol 1992;148:986-89.
18. Mattoo TK, Katawee Y. Oxalate
creatinine ratio in the peritoneal fluid
of patients with primary hyperoxaluria.
Nephron 1992;60:496-97.
19. Monico CG, Rossetti S,
Schwanz HA, Olson JB, Lundquist PA,
Dawson DB et al. Comprehensive
Mutation Screening in 55 Probands
with Type 1 Primary Hyperoxaluria
Shows Feasibility of a Gene-Based
Diagnosis.
J Am Soc Nephrol 2007;18:1905-14.
20. Nishiyama K, Funai T, Yokota S,
Ichiyama A. ATP-dependent degrada-
tion of a mutant serine: pyruvate/ala-
nine:glyoxylate aminotransferase in a
primary hyperoxaluria type 1 case.
J Cell Biol 1993;123:1237-48.
21. Petrarulo M, Marangella M,
Linari F. High-performance liquid chro-
matographic determination of plasma
glycolic acid in healthy subjects and in
cases of hyperoxaluria syndromes.
Clin Chim Acta 1991;196:17-26.
22. Petrarulo M, Pellegrino S,
Marangella M, Cosseddu D, Linari F.
High-performance liquid chromato-
graphic microassay for L-alanine:
glyoxylate aminotransferase activity
in human liver. Clin Chim Acta
1992;208:183-92.
23. Pirulli D, Puzzer D, Ferri L,
Crovella S, Amoroso A, Ferrettini C et
al. Molecular analysis of hyperoxaluria
type 1 in Italian patients reveals eight
new mutations in the alanine:
glyoxylate aminotransferase gene.
Hum Genet 1999;104:523-25.
24. Porowski T, Galasinski W.
A semi-micromethod for determination
of oxalate in human plasma. Acta Pol
Pharm 2003;60:239-45.
25. Prenen JA, Boer P, Mees EJ,
Endeman HJ, Spoor SM, Oei HY. Renal
clearance of [14C]oxalate: comparison
of constant-infusion with single-
injection techniques. Clin Sci (Lond)
1982;63:47-51.
26. Purdue PE, Lumb MJ, Allsop J,
Minatogawa Y, Danpure CJ. A glycine-
to-glutamate substitution abolishes
alanine:glyoxylate aminotransferase
catalytic activity in a subset of patients
with primary hyperoxaluria type 1.
Genomics 1992;13:215-18.
27. Purdue PE, Takada Y, Danpure CJ.
Identification of mutations associated
with peroxisome-to-mitochondrion
VAN WOERDEN 5/19/08 8:53 AM Pagina 167

APPENDIX 02
page 168
mistargeting of alanine/glyoxylate
aminotransferase in primary
hyperoxaluria type 1.
J Cell Biol 1990;111:2341-51.
28. Reusz GS, Dobos M, Byrd D,
Sallay P, Miltenyi M, Tulassay T.
Urinary calcium and oxalate excretion in
children. Pediatr Nephrol 1995;9:39-44.
29. Rumsby G, Weir T, Samuell CT.
A semiautomated alanine:glyoxylate
aminotransferase assay for the tissue
diagnosis of primary hyperoxaluria
type 1. Ann Clin Biochem 1997;34
(Pt 4):400-04.
30. Rumsby G, Williams E, Coulter-
Mackie M. Evaluation of mutation
screening as a first line test for the
diagnosis of the primary hyper-
oxalurias. Kidney International Vol
66(3) (959-963), 2004 2004;959-63.
31. Santana A, Salido E, Torres A,
Shapiro LJ. Primary hyperoxaluria
type 1 in the Canary Islands:
A conformational disease due to
I244T mutation in the P11L-containing
alanine:glyoxylate aminotransferase.
Proceedings of the National Academy
of Sciences of the USA Vol 100(12)
7277-7282, 2003;7277-82.
32. von Schnakenburg C, Byrd DJ,
Latta K, Reusz GS, Graf D, Brodehl J.
Determination of oxalate excretion in
spot urines of healthy children by ion
chromatography. Eur J Clin Chem Clin
Biochem 1994;32:27-29.
33. von Schnakenburg C, Rumsby G.
Primary hyperoxaluria type 1: a cluster
of new mutations in exon 7 of the AGXT
gene. J Med Genet 1997;34:489-92.
34. Wanders RJ, Ruiter J, van
Roermund CW, Schutgens RB, Ofman
R, Jurriaans S, Tager JM. Human liver
L-alanine-glyoxylate aminotransferase:
characteristics and activity in controls
and hyperoxaluria type I patients using
a simple spectrophotometric method.
Clin Chim Acta 1990;189:139-44.
35. Wandzilak TR, Hagen LE,
Hughes H, Sutton RA, Smith LH,
Williams HE. Quantitation of glycolate
in urine by ion-chromatography.
Kidney Int 1991;39:765-70.
36. Wilson DM, Liedtke RR.
Modified enzyme-based colorimetric
assay of urinary and plasma oxalate
with improved sensitivity and no
ascorbate interference: reference
values and sample handling
procedures.
Clin Chem 1991;37:1229-35.
37. Wong PN, Law EL, Tong GM,
Mak SK, Lo KY, Wong AK.
Diagnosis of primary hyperoxaluria
type 1 by determination of peritoneal
dialysate glycolic acid using standard
organic-acids analysis method. Perit
Dial Int 2003;23:S210-S213.
VAN WOERDEN 5/19/08 8:53 AM Pagina 168

APPENDIX 02
page 169
VAN WOERDEN 5/19/08 8:53 AM Pagina 169

blz. 170
DANKWOORD
Dit proefschrift kwam tot stand in samenwerking met en dankzij deinspanningen van velen. Iedereen die hieraan heeft bijgedragen, dank ikdan ook hartelijk vanaf deze plaats.
De patiënten en hun ouders die belangeloos medewerking verleendenaan diverse onderzoeken vormden de basis voor het project: allen heelhartelijk bedankt. De leden van de promotiecommissie dank ik voor hunkritisch beoordelen van het manuscript.
Een aantal mensen noem ik graag bij naam:Frits Wijburg, promotor, als geen ander doorzag jij vanaf het beginwelke hoofdstukken konden worden vormgegeven. Werkoverleg gingaltijd gepaard met een humoristische kijk op het leven. Dat maakte hethele project overzichtelijk, èn afzienbaar. Jouw enthousiasme om mij alin een zeer vroeg stadium naar congressen te laten gaan heeft een stevi-ge basis gelegd, waardoor ik er al snel een steentje kon bijdragen aanvoordracht en discussie. De afgelopen jaren heb ik je bovendien als eenbijzonder betrokken clinicus leren kennen en daarvan leer ik ook zoveel!Ronald Wanders, promotor, het was een voorrecht om op jouw laborato-rium mee te mogen draaien en diverse aspecten van onderzoek doen teleren. Jouw visie stuurde mijn werk. Ik heb ontzag voor de hoge snelheidwaarmee jij kunt coachen. Het maakte het veel gemakkelijker om óóktempo te maken in denk- en schrijfwerk. Daarbij bracht jij in manuscrip-ten finesses aan die de grootmeester in je lieten zien.Jaap Groothoff, co-promotor, bij jou is het onderzoek begonnen: je toondeme direct de diepgang van de hyperoxalurie, en wist mij met je aansteke-lijke fascinatie voor deze tak van de nefrologie een grote taak over te dra-gen. Altijd kon jij feilloos de mogelijkheden en tekortkomingen van hetonderzoek onder woorden brengen, en liet je zien hoe waardevol beideaspecten kunnen zijn. Door jou niet-aflatende steun en belangstelling konik doorgaan op het ingeslagen pad en bleven we scherp. Je betrokkenheidbij patiënt en wetenschap wordt nog eens spreekwoordelijk!Ries Duran, co-promotor, met jouw komst naar het AMC werd het doenvan cel-biochemisch onderzoek concreet, en ontstond voor ons een nieuwe, verdiepende laag. Je kennis van organische chemie, je scherp-zinnigheid en creativiteit bij het zoeken naar oplossingen van problemenbij het onderzoek met de gas-chromatograaf/ massa-spectrometer warenaltijd zeer inspirerend. Hugo Heymans, mijn opleider in de kindergeneeskunde, jouw enthousi-asme zette me in 1999 in beweging om basaal onderzoek te vinden. HetEmma Kinderziekenhuis biedt kansen aan vernieuwend onderzoek. Ik
VAN WOERDEN 5/19/08 8:53 AM Pagina 170

blz. 171
ervaar het als een groot genoegen om daaraan mee te mogen werken.De manier waarop jij de vertaalslag naar kind en ouders weet te maken(en vice versa) is steeds weer verrassend. Het maakt de opleiding kinder-geneeskunde tot een bijzondere belevenis.Eduardo Salido, what a generous offer to be guest at your laboratory!Thank you very much for giving us the opportunity to investigate theAgxt -/- mice hepatocytes. It inspired us to design new focus for research.Tevens de (kinder)nefrologen en overige dokters die hun medewerkingverleenden dank ik hartelijk. Jullie hulp in speurwerk en het uitwisselenvan ideeën waren essentieel voor het slagen van twee grote pijlers vanmijn onderzoek.
Op het laboratorium Genetische Metabole Ziekten hebben zeer veel mensen meegeholpen aan verschillende projecten. Het genetische project werd verricht op de DNA-afdeling van Dr. Hans Waterham, dieervoor heeft gezorgd, dat de data uiteindelijk werden verkregen. Hans,jouw drive om de onderste steen boven te krijgen uit het AGXT genmaakte dat we als eerste in de wereld de belangrijkste genotype-fenoty-pe-relatie konden leggen bij primaire hyperoxalurie, waarvoor veel dank.Ook dank ik Wendy, die mij geduldig de beginselen van het sequencenbijbracht, bijgestaan door Janet, Evelien, Janet. Carla, bedankt dat je degrote bulk samples voltooide. Op de metabole afdeling bedank ik bijnaam: Lia, Henny, Ingrid, Maurice, Wilma en Henk voor hun baanbreken-de werk om de gecombineerde meting van oxaalzuur en glycolzuur opte kunnen zetten. Ben verrichte nauwkeurige oxaalzuurmetingen op deionchromatograaf welke in hoofdstuk 2 werden verwerkt. Excellente logistiek werd aan de balie geleid door Annlies, samen metMoniek, Sharon, Lida en anderen. Zeer goed verzorgde secretariëleondersteuning maakte de basis voor elk onderzoek compleet: veel dankaan Maddy, Suzan en Iet, Hester, Dionne en Marja. Van vele anderen hebik genoten van wetenschappelijke discussies, praktische tips, en waarde-volle adviezen. Alle analisten en onderzoekers hebben me bijzonder welkom doen voelen. Jos, een speciaal woord voor jou, omdat je in staatbent geweest om in een flits een nieuw incubatie-experiment op te zetten. De efficiëntie èn nauwkeurigheid waarmee jij weet te werken zijnverbluffend. Dankzij jou hebben we een lang-gekoesterde proef in vervulling kunnen laten gaan.
Prof. Poll-Thé en Prof. Barth, dank voor de samenwerking in het onderzoek,dat hyperoxalurie op de kaart zette bij Zellweger spectrum patiënten.Prof. Sauerwein, Mariëtte Ackermans, An Ruiter: hartelijk dank voor jullieinspanningen om de meting van de rate of appearance van oxaalzuur opte zetten. Het was fijn om altijd open van gedachten te kunnen wisselen.Jean-Claude Davin, kindernefroloog: veel dank voor je inspanningen ommij bij de kindernefrologie te betrekken. Je bood me belangrijke kansenop symposia. Een speciaal project werd geïnitieerd in samenwerking met
VAN WOERDEN 5/19/08 8:53 AM Pagina 171

dr. Carl Verkoelen vanuit het Erasmus MC. Met zijn plotselinge overlijdenhield dit op. Ik zal Carl blijven herinneren om zijn bijzonder integereaanpak, waarvoor ik hem dankbaar ben.Hidde Huidekoper, beste Hidde: door jou rasechte onderzoeksgeest kon-den we eindelijk echt gaan kwantificeren in de wereld van de hyperoxa-lurie: allereerst wist jij de sleutel te vinden voor de juiste berekening vanhet aanzuurexperiment zoals beschreven in hoofdstuk 2. Vervolgensbereikte jij een doorbraak door een doortimmerd en goedgekeurd proto-col op te stellen voor infusie van stabiele isotopen en vond jij patiëntenèn gezonde proefpersonen bereid om zich letterlijk aan onderzoek teonderwerpen. Jij hebt me geleerd hoe je kunt doorpakken in onderzoek,waardoor we in korte tijd met een uniek project zijn geslaagd. Het is eendriedubbel feest om praktisch tegelijk met jou te kunnen promoveren! Ikhoop dan ook in de toekomst nog vaak vanuit verschillende disciplinesmet elkaar samen te werken.De collega-onderzoekers in het Emma Kinderziekenhuis: dank voor jullieinhoudelijke en ludieke bijdragen aan mijn onderzoekstijd. Quirine,Florine en Leontien: dank voor jullie kamergeleerdheid. De collega arts-assistenten van het Emma Kinderziekenhuis dank ik voor hun begrip ensteun tijdens de laatste onderzoeksfase.
Thomas Reerink, en Hugo van Woerden, mijn paranimfen: wat fijn datjullie naast me staan als ridders bij de verdediging. Op cruciale momenten hebben jullie me door de afgelopen jaren heengepraat: relativerend en soms de dingen op hun kop gezet.Lies Kindt, wat heb jij het geheel prachtig vormgegeven! Het is een plezier om alles weer door te lezen, dankjewel voor je harde werken.
Zoveel vrienden hebben de vorderingen van dit boekje met belangstel-ling gevolgd. Het heeft veel weg van een beklimming op de Alpe d’Huez:vol energie begin je aan de moeilijke aanloop, en naarmate je hogerkomt, raak je steeds meer op het asfalt gericht, en schuif je als een waaslangs omstanders heen. Na de finish volgt een plezierige afdaling, waar-in er hopelijk weer tijd genoeg is om met elkaar op adem te komen. De support van jullie allen was onmisbaar en verdient groot applaus.
Mijn lieve familie, wat fijn dat jullie er zijn! Lieve grootouders Anneke enHenk, en (in gedachten) Grotie, lieve ouders Jeanet en Piet en lieveClaartje, Pien, Steven en Hugo: we mogen dan wel in een alfagezin zijngroot geworden, altijd hadden jullie oprechte belangstelling en probeer-den jullie de kwintessens van dat onderzoek met die nieren vast te houden. Het is geweldig om daarnaast van zoveel andere facetten vanhet leven te kunnen genieten.blz. 172
VAN WOERDEN 5/19/08 8:53 AM Pagina 172

blz. 173
VAN WOERDEN 5/19/08 8:53 AM Pagina 173

VAN WOERDEN 5/19/08 8:53 AM Pagina 174

STELLINGEN
1. Primaire hyperoxalurie type 1 (PH1) kan op elke leeftijd manifest worden. (dit proefschrift)
2. PH1 presenteert zich met uiteenlopende symptomen, variërend van eenenkele niersteen tot terminale nierinsufficiëntie. (dit proefschrift)
3. PH1 is ondergediagnosticeerd, vooral in volwassenen. (dit proefschrift)4. Een neonatale presentatie van PH1 hoeft niet te leiden tot de ontwikke-
ling van terminale nierinsufficiëntie, als goede conservatieve therapiewordt gewaarborgd. (dit proefschrift)
5. Afwezigheid van nefrocalcinose op nierecho-onderzoek sluit de ontwik-keling van microscopische nefrocalcinose niet uit. (dit proefschrift)
6. De Gly170Arg en de Phe152Ile substitutie op het minor allel van hetAGXT gen zijn voorspellend voor een goede respons op vitamine B6,met sterke verlaging van oxaalzuuruitscheiding en behoud van nier-functie. (dit proefschrift)
7. Uitstel van diagnostiek en behandeling bij PH1 leidt tot de ontwikkelingvan nierinsufficiëntie. (dit proefschrift)
8. Bij aanwezigheid van de Gly170Arg of de Phe152Ile substitutie inhomozygote vorm hoeft men geen levertransplantatie uit te voeren,mits vitamine B6 wordt gebruikt. (dit proefschrift)
9. Heterozygotie voor een specifieke AGXT genmutatie sluit de diagnosePH1 niet uit. (dit proefschrift)
10. Het thuis opvangen van urine voor diagnostiek van PH1 kan zondertoevoeging van zoutzuur betrouwbaar worden gedaan. (dit proefschrift)
11. Alle patiënten met Zellweger spectrum disorders moeten wordengescreend op hyperoxalurie en nierstenen teneinde nierinsufficiëntie tevoorkomen. (dit proefschrift)
12. Door infusie van stabiel gelabeld oxaalzuur kan de rate of appearancevan oxaalzuur bij patiënten met PH1 betrouwbaar worden gemeten. (dit proefschrift)
13. Primaire hyperoxalurie type 1 moet aan het neonatale screenings-programma worden toegevoegd.
14. Onderzoek doen is net als beleggen: in het verleden behaalde resultaten bieden geen garantie voor de toekomst en voorkennis kanveel vertrouwen geven om door te gaan.
15. Wetenschap is als muzak in een warenhuis: je zit er al gauw middenin.16. Het kan soms zinvol zijn om met een open-staande kraan te dweilen
(als je maar hard genoeg dweilt).17. Het bestuderen van een metabool pad is als een pianosonate van
Beethoven: je waardeert het pas echt, als je alle delen kent - en hetliefst nog de hele cyclus waarvan het deel uitmaakt.
18. Dat een moderne arts vaak in Pub Med opduikt, roept wellicht tenonrechte het beeld op van een kroegtijger.blz. 175
VAN WOERDEN 5/19/08 8:53 AM Pagina 175

CURRICULUM VITAE
Christiaan van Woerden werd op
31 maart 1976 geboren als tweede
van een tweeling in het Sint Jozef
Ziekenhuis te Gouda. Na zijn
eindexamen aan het Coornhert
Gymnasium in 1995, studeerde
hij een jaar medicijnen in Leuven,
waarna hij in 1996 opnieuw
startte met dezelfde studie aan
de Universiteit van Amsterdam.
In zijn derde studiejaar begon hij
zijn onderzoek naar primaire
hyperoxalurie type 1 in Nederland,
welk project uitgroeide tot de
huidige dissertatie. Christiaans
verpleeghulpstage vond plaats in
Wakefield, Engeland, bij de Pennine
Camphill Community for people
with special needs, en zijn oudste
co-schap in Zambia, in Kaoma en
in Luwingu. In 2004 behaalde hij
zijn artsdiploma en werd
Christiaan aangesteld als arts-
assistent kindergeneeskunde in het
Emma Kinderziekenhuis AMC
te Amsterdam, en in 2007 werd
hij toegelaten tot de opleiding
kindergeneeskunde bij
Prof.dr. Hugo Heymans.
Daarnaast speelt hij piano bij
het Trio Sine Nomine.
Christiaan woont in Amsterdam.
VAN WOERDEN 5/19/08 8:53 AM Pagina 176