Embed Size (px)
Citation preview

SOS SOS Signs of Signs of SuicideSuicide®®
An Evidence-based An Evidence-based Suicide PreventionSuicide Prevention
Program for Program for
High Schools High Schools

Youth Suicide:Youth Suicide:Overview of the ProblemOverview of the Problem

““One young person contemplating One young person contemplating suicide grips our hearts. Nine suicide grips our hearts. Nine
hundred thousand young people hundred thousand young people contemplating suicide grips our contemplating suicide grips our
collective consciousnesscollective consciousness.”.”
-Charles Curie, Administrator,-Charles Curie, Administrator,
Substance Abuse and Mental Health Services Substance Abuse and Mental Health Services AdministrationAdministration

Screening For Mental Health, Inc.Screening For Mental Health, Inc.
• 1991: Pioneered the concept of large scale mental health screening and education with National Depression Screening Day®
• SMH programs include: • SOS Signs of Suicide® for high schools and middle schools• Signs of Self-Injury™ for high schools• National Alcohol Screening Day®• National Depression Screening Day®• CollegeResponse ®• WorkplaceResponse™• Mental Health Self-Assessment Program®• HealthcareResponse ®
• Ongoing collaboration with:• government agencies• national health and mental health organizations• membership organizations representing school-based professionals• health & mental health facilities, colleges, & schools

Prevalence of Suicide Prevalence of Suicide Among Young PeopleAmong Young People
While child suicide is very uncommon, While child suicide is very uncommon, mortality from suicide increases steadily mortality from suicide increases steadily through the teensthrough the teensSuicide is the Suicide is the 3rd leading cause of death3rd leading cause of death among children ages 10-24among children ages 10-24
-Center for Disease Control and Prevention (WISQARS, 2004)
Adolescent Adolescent suicidal behaviorsuicidal behavior is deemed is deemed to be to be underreportedunderreported because many because many deaths of this type are classified as deaths of this type are classified as unintentional or accidentalunintentional or accidental
-World Medical Association, 2004-World Medical Association, 2004
Depression and YouthDepression and Youth
In 2005, 8.8% of youth (about 2.2 million youth) In 2005, 8.8% of youth (about 2.2 million youth) had experienced at least one major depressive had experienced at least one major depressive episode during the past year.episode during the past year.
-SAMHSA, 2007-SAMHSA, 2007
In children and adolescents, an untreated In children and adolescents, an untreated depressive episode may last between 7 to 9 depressive episode may last between 7 to 9 months- months- potentially, an entire academic year Depression has been linked to suicide, poor Depression has been linked to suicide, poor school performance, substance abuse, running school performance, substance abuse, running away, and feelings of worthlessness and away, and feelings of worthlessness and hopelessness hopelessness Overall, approximately 20% of youth will have one Overall, approximately 20% of youth will have one or more episodes of major depression by the time or more episodes of major depression by the time they become adultsthey become adults
-National Alliance on Mental Illness (NAMI, 2005)-National Alliance on Mental Illness (NAMI, 2005)

Prevalence of Suicide/Related Phenomena Prevalence of Suicide/Related Phenomena Among YouthAmong Youth
29% felt so sad or hopeless almost every day for two 29% felt so sad or hopeless almost every day for two weeks+ that they stopped doing some usual activitiesweeks+ that they stopped doing some usual activities14.5% seriously considered attempting suicide14.5% seriously considered attempting suicide11% made a suicide plan 11% made a suicide plan 6.9% attempted suicide6.9% attempted suicideOf those that made an attempt, more than 2% required Of those that made an attempt, more than 2% required medical attentionmedical attention
- CDC, 2007 Youth Risk Behavior Survey- CDC, 2007 Youth Risk Behavior Survey

Risk FactorsRisk Factors

What Are Risk Factors?What Are Risk Factors?
•Suicide is a complex behavior that is usually caused by a combination of risk factors in the context of negative life events
•A risk factor is anything that increases the likelihood that persons will harm themselves.
•Risk factors are not necessarily causes.
•The first step in preventing suicide is to identify and understand the risk factors.
-Adapted from the National Youth Violence Prevention Resource Center

Risk FactorsRisk Factors
The strongest risk factors for suicide in youth are The strongest risk factors for suicide in youth are depressiondepression, , substance abusesubstance abuse and and previous previous attemptsattempts
-NAMI, 2003-NAMI, 2003
Clinically depressed adolescents are nearly 5 times more likely to attempt suicide than their non-depressed peers
-Mental Health: A Report of the Surgeon General-Mental Health: A Report of the Surgeon General
Over 90 percent of children and adolescents who die by suicide have at least one major psychiatric disorder -Gould et al., 2003-Gould et al., 2003

SUICIDE: A MULTI-FACTORIAL EVENT
Neurobiology
Severe MedicalIllness
Impulsiveness
Access To Weapons
Hopelessness
Life Stressors
Family History
SuicidalBehavior
Personality Disorder/Traits
Psychiatric IllnessCo-morbidity
Psychodynamics/Psychological Vulnerability
Substance Use/Abuse
Suicide

Symptoms of Adolescent Depression-Symptoms of Adolescent Depression-Feelings/Thoughts/Behaviors/HealthFeelings/Thoughts/Behaviors/Health
Frequent sadness, tearfulness, crying Frequent sadness, tearfulness, crying Hopelessness Hopelessness Decreased interest in activities; or inability to enjoy previously favorite Decreased interest in activities; or inability to enjoy previously favorite activities activities Persistent boredom; low energy Persistent boredom; low energy Social isolation, poor communication Social isolation, poor communication Low self esteem and guilt Low self esteem and guilt Extreme sensitivity to rejection or failure Extreme sensitivity to rejection or failure Increased irritability, anger, or hostility Increased irritability, anger, or hostility Difficulty with relationships Difficulty with relationships Frequent complaints of Frequent complaints of physical illnessesphysical illnesses such as headaches and such as headaches and stomachaches stomachaches Frequent absences from school or Frequent absences from school or poor performance in schoolpoor performance in school Poor concentration Poor concentration A major change in eating and/or sleeping patterns A major change in eating and/or sleeping patterns Talk of or efforts to run away from home Talk of or efforts to run away from home Thoughts or expressions of suicide or self destructive behavior Thoughts or expressions of suicide or self destructive behavior
-AACAP, The Depressed Child -AACAP, The Depressed Child

Suicidality and Substance AbuseSuicidality and Substance Abuse
Youths aged 12 to 17 who reported past year Youths aged 12 to 17 who reported past year alcoholalcohol use use (19.6 percent) were more likely (19.6 percent) were more likely than youths who did not use alcohol (8.6 than youths who did not use alcohol (8.6 percent) to be at risk for percent) to be at risk for suicidesuicide. .
--SAMHSA. NHSDA Report: Substance Use and the Risk of SAMHSA. NHSDA Report: Substance Use and the Risk of Suicide Suicide Among Youth, 2002Among Youth, 2002
1/3-1/2 of teenagers were under the influence of drugs or alcohol shortly before they killed themselves. - National Strategy for - National Strategy for Suicide Prevention, DHHS Suicide Prevention, DHHS

Signs of Suicide*Signs of Suicide*Talking, reading, or writing about suicide or deathTalking, reading, or writing about suicide or deathTalking about feeling worthless or hopelessTalking about feeling worthless or hopelessSaying things like, “I’m going to kill myself,” “I Saying things like, “I’m going to kill myself,” “I wish I were dead,” or “I shouldn’t have been wish I were dead,” or “I shouldn’t have been born”born”Visiting or calling people to say goodbyeVisiting or calling people to say goodbyeGiving things awayGiving things awayA sudden interest in drinking alcoholA sudden interest in drinking alcoholPurposely putting oneself in dangerPurposely putting oneself in dangerObsessed with death, violence, and guns or Obsessed with death, violence, and guns or knivesknivesPrevious suicidal thoughts or suicide attemptsPrevious suicidal thoughts or suicide attempts
- - http://pbskids.org/itsmylife
*Including online communications

Self-injury in YouthSelf-injury in YouthIn the pediatric population, self-injury is defined as In the pediatric population, self-injury is defined as deliberate non-lethal harming of oneself. of oneself. Self-injury is a Self-injury is a maladaptive coping behavior employed by youth experiencing painful emotionsemployed by youth experiencing painful emotionsIs generally Is generally NOT an attempt to die by suicide. by suicide.Between Between 150,000 and 360,000 adolescents in the U.S. adolescents in the U.S. self-injury - Walsh, Lieberman, 2004 –Walsh, Lieberman, 2004 –
Relationship Between Suicide and Self-injuryRelationship Between Suicide and Self-injuryDeath can occur, even if unintentionallyDeath can occur, even if unintentionallyThose who self-injure may become suicidal in the Those who self-injure may become suicidal in the futurefutureThe student is experiencing a mental health disorder The student is experiencing a mental health disorder that should be treated professionally and stands the that should be treated professionally and stands the best chance of recovery if caught early.best chance of recovery if caught early.If handled inappropriately or not at all, there is a If handled inappropriately or not at all, there is a potential for contagion.potential for contagion.

Overview of the SOS ProgramOverview of the SOS ProgramThe SOS Strategy and Four-Pronged Safety NetThe SOS Strategy and Four-Pronged Safety Net

Developed and Supported by:Developed and Supported by:American Academy of Child and Adolescent Psychiatry American Academy of Child and Adolescent Psychiatry
American Academy of Nurse Practitioners American Academy of Nurse Practitioners American Association for Marriage and Family Therapy American Association for Marriage and Family Therapy
American Counseling Association American Counseling Association American School Counselor Association American School Counselor Association
American School Health Association American School Health Association National Association of School Nurses National Association of School Nurses
National Association of School Psychologists National Association of School Psychologists National Association of Secondary School Principals National Association of Secondary School Principals
National Association of Social Workers National Association of Social Workers National Association of Student Councils National Association of Student Councils
National Education Association Health Information Network National Education Association Health Information Network National Student Assistance Association National Student Assistance Association
National Peer Helpers Association National Peer Helpers Association School Social Work Association of America School Social Work Association of America
United Educators InsuranceUnited Educators Insurance

SOS GoalsSOS Goals
Decrease the incidence of self-injury, suicide attempts, unrecognized depression, and the number of youth who die by suicide
Increase knowledge and adaptive attitudes about depression, suicidality, and self-injury
Encourage individual help-seeking
Link suicide and self-injury to mental illness that, like physical illnesses, require treatment
Address risk factors for self-injury and suicide

SOS Goals (continued)SOS Goals (continued)
Engage parents and school staff as partners in prevention
Reduce stigma associated with mental health problems by communicating that they are treatable conditions
Increase self-efficacy and access to mental health services for at-risk youth and their families
Increase school/community-based partnerships

ACTACT
AAcknowledge that a friend or classmate has a problem, and that the symptoms are serious.
CCare: let that friend know they are there for them, and want to help.
TTell a trusted adult about their concerns

4-Pronged Strategy for Suicide Prevention4-Pronged Strategy for Suicide PreventionSCREENING for Symptoms of Depression and Suicide
BSAD: 7 item depression inventory
EDUCATION about Depression and Suicide
Video
Discussion
“Friends for Life”:
• Teaches the link between depression and suicide
• Emphasizes that depression is treatable
• Encourages help seeking
ENVIRONMENT
Parent Involvement - Parent version of screening form; letter, educational materials
Staff Involvement - Staff education and training video
BEHAVIOR
• Acknowledge (the signs)
• Care (express concern)
• Tell (a trusted adult) •

Program ComponentsProgram Components• Implementation Binder• “Friends for Life” Video and
discussion guide• Depression Screening Forms
for students and parents (English and Spanish)
• Staff Training Video• Educational Materials for
staff, parents and students• Postvention Guidelines• Self-injury resources for staff
and parents• Lecture for training staff and
parents• Customizable posters and
wallet cards

Evaluation of the SOS ProgramEvaluation of the SOS Program2001-20022001-2002

Evaluation of SOS ProgramEvaluation of SOS Program
Two approaches to evaluation (Aseltine):
Process evaluationProcess evaluation: school personnelprogram implementation, quality
Outcome evaluationOutcome evaluation: students, student attitudes & behavior

Assessing the quality of program components
Assessing the safety of program implementation within the student body
Assessing the burden on school staff after
Assessing the efficacy of the program
Evaluation of 233 Participating Schools
School-Level Process Evaluation School-Level Process Evaluation 2001-2002 Academic Year2001-2002 Academic Year
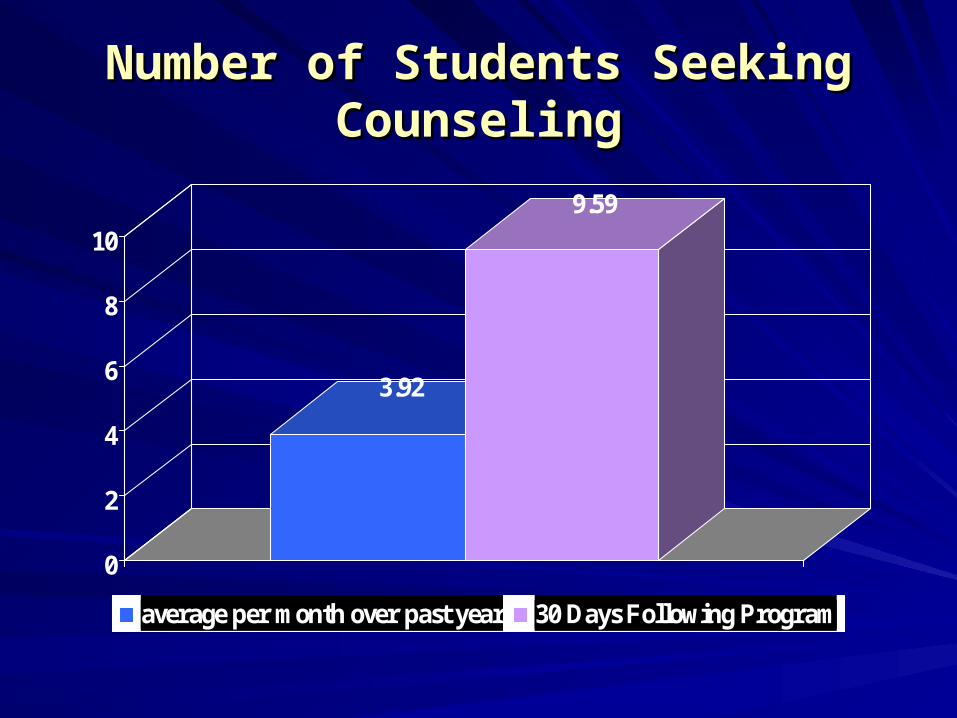
Number of Students Seeking Number of Students Seeking CounselingCounseling
3.92
9.59
0
2
4
6
8
10
average per month over past year 30 Days Following Program

Number of Students Seeking Number of Students Seeking Counseling on Behalf of FriendCounseling on Behalf of Friend
2.25
3.79
0
0.5
1
1.5
2
2.5
3
3.5
4
Average per month over past year 30 Days following Program

SOS Student-Level SOS Student-Level Research FindingsResearch Findings
“An Outcome Evaluation of the SOS Suicide Prevention Program” “An Outcome Evaluation of the SOS Suicide Prevention Program”Robert H. Aseltine, Jr, PhD and Robert DeMartino, MDRobert H. Aseltine, Jr, PhD and Robert DeMartino, MD
American Journal of Public Health, March 2004.American Journal of Public Health, March 2004.

SOS is the SOS is the only school based suicide only school based suicide prevention programprevention program to… to…
Show a reduction in suicide attempts (by 40%) in a randomized-controlled study (screening form administered in classroom setting)
American Journal of Public Health, March, 2004
Be selected by SAMHSA for its National Registry of Evidence-Based Programs and PracticesSOS has also documented dramatic increases in help-seeking
Adolescent and Family Health, 2003

• School-based program evaluation showed SOS program was effective in initiating help seeking among students.
• Safe for students.
• Received and rated positively by users.
Evaluation SummaryEvaluation Summary

Outcome EvaluationOutcome EvaluationInvolved 4133 students4133 students in 9 schools
(CT, GA, MA)
MeasuresMeasures
Attitudes/KnowledgeAttitudes/Knowledge -Attitudes: 7 item scale -Attitudes: 7 item scale -Knowledge: 10 item scale -Knowledge: 10 item scale
Help-seeking past 3 months: Help-seeking past 3 months: -Treatment Y/N -Treatment Y/N -Talked to adult Y/N -Talked to adult Y/N -Talked to adult about friend Y/N -Talked to adult about friend Y/N
Suicidal behavior past 3 months: Suicidal behavior past 3 months: -Ideation Y/N -Ideation Y/N -Attempts Y/N -Attempts Y/N

Study ParticipantsStudy Participants
GenderGenderMaleMale 48%48%FemaleFemale 52%52%
Racial/ethnic self-identificationRacial/ethnic self-identificationWhite, non HispanicWhite, non Hispanic 26%26%Black, non-HispanicBlack, non-Hispanic 24%24%HispanicHispanic 35%35%Multi-ethnicMulti-ethnic 8%8%OtherOther 7%7%

Effects of SOS Program on Knowledge Effects of SOS Program on Knowledge and Attitudes About Depression/Suicideand Attitudes About Depression/Suicide
3.83 3.994.36
5
0
1
2
3
4
5
Attitudes Knowledge
Control SOS
Treatment and controls differ at the .05 level for both outcomes.

Effects of SOS Program onEffects of SOS Program onSuicidal Ideation and Suicide AttemptsSuicidal Ideation and Suicide Attempts
0.12
0.1
0.048
0.03
0
0.02
0.04
0.06
0.08
0.1
0.12
Ideation Attempt
Control SOS
Treatment and controls differ at the .05 level for suicide attempts. 40% fewer suicide attempts among the students who completed the SOS program.

SummarySummarySOS:SOS: first program to curtail suicide attempts in randomized study first program to curtail suicide attempts in randomized study
Program well received by schoolsProgram well received by schools
Safe for students Safe for students

SOS Program ImplementationSOS Program Implementationat the school levelat the school level

• School personnel implement the program with materials provided by SMH: School Psychologists, Health Educators, School Nurses, School Counselors, Student Assistance Professionals
• Usually implemented in one classroom period:
Students view and discuss video in classroom
Students complete screening form in classroom
• Entire student body or a select portion of student body may be screened (i.e. freshmen) depending on the school’s resources
• Screenings may be taken with or without identification
• Parent version of screening forms and information provided; assists in the identification of depression and suicidality and helps initiate family discussion
• Passive or active parental permission
Implementation OverviewImplementation Overview

First StepsFirst Steps

The Team MeetingThe Team Meeting
Review program goals, assign Review program goals, assign roles/responsibilitiesroles/responsibilities
Review kit, video, and discussion guideReview kit, video, and discussion guide
Review screening form and scoringReview screening form and scoring
Designate time and date for program Designate time and date for program implementationimplementation
Review school policies for handling Review school policies for handling suicide disclosure, parental consent, suicide disclosure, parental consent, record keeping, etc.record keeping, etc.

Decide on FormatDecide on Format
Flexible model can be adapted to meet a Flexible model can be adapted to meet a school’s needsschool’s needs
Provide program school-wide or select Provide program school-wide or select target student group based on grade target student group based on grade level, class enrollment, or special needlevel, class enrollment, or special need

Screening Implementation Options
• Anonymous• Anonymous with Response Card• Non-anonymous• Anonymous with number ID • EliminateNote: Self-assessment is a critical tool in all public health
programs that address personal/social issues.

BRIEF SCREEN FOR ADOLESCENT BRIEF SCREEN FOR ADOLESCENT DEPRESSION (BSAD)DEPRESSION (BSAD)
These questions are about feelings that people sometimes have and things that may have happened to you. Most of the questions are about the LAST 4 WEEKS.Read each question carefully and answer it by circling the correct response (No/Yes).
1. In the last 4 weeks, has there been a time when nothingwas fun for you and you just weren’t interested in anything?
2. Do you have less energy than you usually do? 3. Do you feel you can’t do anything well or that you are not as
good-looking or as smart as most other people?4. Do you think seriously about killing yourself? 5. Have you tried to kill yourself in the last year? 6. Does doing even little things make you feel really tired?7. In the last 4 weeks has it seemed like you couldn’t think as
clearly or as fast as usual?

Get Teacher Buy-InGet Teacher Buy-InInvolve teachers from the startInvolve teachers from the startChange requires growthChange requires growthChange is a processChange is a processSpeak to teachers’ needsSpeak to teachers’ needsSpeak their languageSpeak their languageKeep change small and simpleKeep change small and simpleEveryone is different (process of change)Everyone is different (process of change)Change is reversibleChange is reversibleMaintain changeMaintain changeMinimize the risksMinimize the risks
– From Student Assistance Journal, Spring, 2006 and adapted from From Student Assistance Journal, Spring, 2006 and adapted from Prevention that Works! Prevention that Works! Knowles, Cynthia, 2001. Knowles, Cynthia, 2001.

Staff Training• Training faculty and staff is universally
advocated and essential to a suicide prevention program.
• Research indicates that training faculty and staff can produce positive effects on an educator’s knowledge attitudes, and referral practices.
-Doan, J., Roggenbaum, S., & Lazear, K., 2003

Staff Training• Schools must prepare all staff, as
students may disclose to any adult. • Train to increase school staff’s
knowledge about: SOS program: Why, when, where, how Warning signs School-and community based mental
health resources School protocol for providing help for
at-risk youth

Staff Training Suggestions• Show the Friends for Life video and facilitate a
discussion• Review the signs of depression and suicide• Answer questions, dispel myths • Review the school policy for handling
students who disclose suicidal intent• Review school and community mental health
resources • Review the Parent Screening form • Distribute protocol for what to do when
approached by students asking for help

Security Issues and Handling Emergencies
• Review school’s emergency procedures and parental notification
• Identify who will be handling emergencies, in advance
• Notify the nearest crisis response center/ about the program in advance to facilitate referrals

Community Partnering• If a school does not have adequate staff• Students may feel more comfortable
speaking with an outsider• As an introduction to community-based
mental health resources • Enhance referral network for the school
Allowing these agencies into the building educates and familiarizes students with their services and how to access them.

Planning for Referrals• Contact local mental health facilities
and advise them of your program dates and times
• Verify referral procedures, wait lists, insurance details, etc.
• Create a Referral Resource List to send with parent letter
• Use SAMHSA’s Find Treatment Locator to identify additional referral resources

SAMHSA’s Find Treatment Locator
http://www.mentalhealth.samhsa.gov/DATABASES/DEFAULT.ASP

Parents/Guardians as Partners in Prevention
• Studies have shown that as many as 86% of parents were unaware of their child’s suicidal behavior.
• The percentage of parents who are involved in the student’s activities is very small.
-Doan, et al, 2003• By raising parental awareness, schools can partner
with parents to watch for signs of these problems in their children and instill confidence for parents seeking help for their child, if needed.
• Involving parents may increase cooperation in prevention efforts and broaden community support

Communication withParents/Guardians
• Send parents a letter stating the goals of the program (template provided) and Parent Screening Form (reproduce Spanish materials, if needed)
• Decide between Active Consent vs. Passive Consent (templates provided)
• Hosting a Parent Night: Show the video, distribute the Parent Screening Form, answer questions, dispel myths, provide referral resources

Parent Permission IssuesParent Permission Issues
Combine permission form collection Combine permission form collection with another activity (sports, spring with another activity (sports, spring orientation with packet of all required orientation with packet of all required forms, next year’s schedule, etc.)forms, next year’s schedule, etc.)Rewards/incentives (pizza parties, raffle Rewards/incentives (pizza parties, raffle prizes)prizes)Testimonial letters of supportTestimonial letters of support““Feed them and they will come!”Feed them and they will come!”

The Day of the ProgramThe Day of the Program

Proposed Schedule
• Introduce Program• Show video• Facilitate discussion• Students complete and score
screening forms and Response Card
• Follow up with students requesting help

Ensuring Follow Up• Respond to requests for help• Set expectations about when
follow-up can be expected• Provide Referral Information • Track students seeking help using
the Student Follow-up Form provided

Reducing LiabilityReducing Liability

Common Themes in LawsuitsCommon Themes in Lawsuits
• The institution The institution ignored warning signsignored warning signs of suicide.of suicide.
• The institution The institution provided the toolsprovided the tools that that the student used for suicide.the student used for suicide.
• The institution took The institution took insufficient stepsinsufficient steps to address the warning signs.to address the warning signs.
• The institution The institution failed to notify the failed to notify the familyfamily about the student’s condition. about the student’s condition.
-United Educators, “The Suicidal Student: Issues in Prevention, -United Educators, “The Suicidal Student: Issues in Prevention, Treatment, and Institutional Liability” Roundtable Discussion, 2003Treatment, and Institutional Liability” Roundtable Discussion, 2003
LiabilityLiability
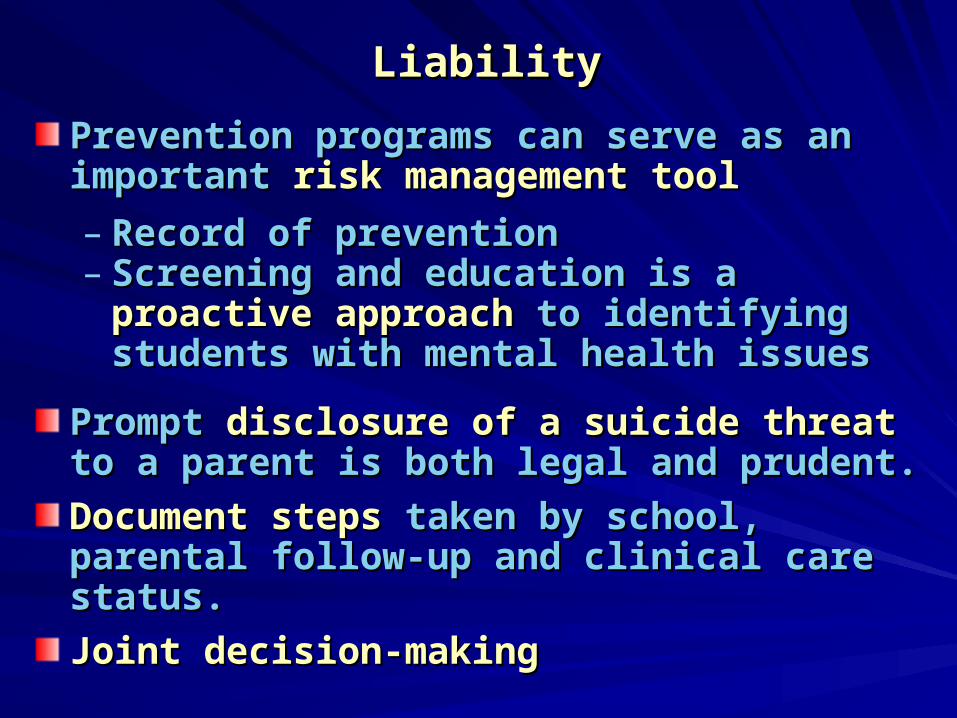
Prevention programs can serve as an important Prevention programs can serve as an important risk management toolrisk management tool
– Record of preventionRecord of prevention– Screening and education is a Screening and education is a proactive proactive
approachapproach to identifying students with mental to identifying students with mental health issueshealth issues
Prompt Prompt disclosure of a suicide threatdisclosure of a suicide threat to a to a parent is both legal and prudent.parent is both legal and prudent.
Document stepsDocument steps taken by school, parental taken by school, parental follow-up and clinical care status.follow-up and clinical care status.
Joint decision-making Joint decision-making

Common Objections & Talking PointsCommon Objections & Talking Points
Suicide is not a problem in our schoolSuicide is not a problem in our school No school is immune to adolescent suicideNo school is immune to adolescent suicide
Schools are not appropriate for suicide prevention Schools are not appropriate for suicide prevention programs programs Student problems with academics, peers, and others Student problems with academics, peers, and others
are more apt to be evident in school. The majority of are more apt to be evident in school. The majority of parents are unaware of their child’s suicidality.parents are unaware of their child’s suicidality.
The program may introduce the idea to studentsThe program may introduce the idea to students There has been no harm seen in screening teens for There has been no harm seen in screening teens for
suicide risk suicide risk Gould et al, 2005Gould et al, 2005
I don’t agree with labeling youthI don’t agree with labeling youth The screenings are not diagnosticThe screenings are not diagnostic

Common Objections & Talking PointsCommon Objections & Talking PointsI don’t have enough staff/timeI don’t have enough staff/time The program can be implemented in one class The program can be implemented in one class
period using existing resources and partnerships period using existing resources and partnerships with community providers. with community providers.
There are no referral resources in my areaThere are no referral resources in my area Identifying the need can help justify the need for Identifying the need can help justify the need for
funding. funding.
We cannot conduct mental health screeningsWe cannot conduct mental health screenings Screenings can be done confidentially or not at allScreenings can be done confidentially or not at all
We already have a suicide prevention programWe already have a suicide prevention program SOS is the only evidence-based program shown SOS is the only evidence-based program shown
to reduce suicide attemptsto reduce suicide attempts
““Graduates the ACT acronym from Graduates the ACT acronym from ““AAcknowledge, cknowledge, CCare, are, Tell an adultTell an adult” ” to “to “AAcknowledge, cknowledge, CCare, are, TreatmentTreatment--Help the person get to treatment”Help the person get to treatment”As an introduction to the mental As an introduction to the mental health communityhealth communityProvides materials for parents to Provides materials for parents to keep the lines of communication keep the lines of communication open about the problems of open about the problems of depression and suicidedepression and suicide
High School Booster ProgramHigh School Booster Program

For more information, contact:For more information, contact:
Candice Porter, MSW, LICSWCandice Porter, MSW, LICSWProgram CoordinatorProgram Coordinator781.239.0071 x122781.239.0071 x122
[email protected]@mentalhealthscreening.org
Or visit:Or visit:
www.MentalHealthScreening.org/schools/index.aspxwww.MentalHealthScreening.org/schools/index.aspx
Screening for Mental Health, Inc.One Washington Street, Suite 304 Wellesley Hills, MA 02481
Phone: 781.239.0071 Fax: 781.431.7447www.MentalHealthScreening.org
















![Survivors of Suicide A Support group Leader’s Handbook SOS[1].405... · Survivors of Suicide . A Support group Leader’s Handbook . ... RN, MSN, who has brought new insights and](https://img.pdfslide.us/doc/110x75/5b01cc8e7f8b9a65618e38b0/survivors-of-suicide-a-support-group-leaders-handbook-sos1405survivors.jpg)