Embed Size (px)
Citation preview

SOS Dementia ProjectBuilding a Network for the Patient with
Cognitive Impairment Padova, 5 Ottobre 2012
What do (American) Families Need to Know?Richard W. Besdine, MD,FACP
Professor of Medicine and of Health Services Policy and PracticeGreer Professor of Geriatric Medicine
Director, Division of GeriatricsDirector, Center for Gerontology and Healthcare Research
A L P E R T
M E D I C A L
S C H O O L

Dementia Caregiver Interventions Alzheimer’s Association – a remarkable organization
providing education and support network FOR caregivers
Advance directives, LTC + financial planning Contact person identified, mobile phone # provided
for emergency situations Caregivers’ physical, mental health; consider primary
care visits coincident with those for AD patient Use of respite and adult day care Simplify and structure home environment Driving and home safety

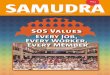
Prevalence of Dementia by Age
0
5
10
15
20
25
30
35
40
45
60–64 65–69 70–74 75–79 80–84 85–89 > 90
All types of dementia
Alzheimer's disease
Vascular dementia
Age (years)
Pre
vale
nce
(%
)

Median survival of women in the longest-lived countries has increased 3 months/year since 1840
We And Many Of Our Patients Will Live Long Enough To Develop AD
Oeppen J et al. Science. 2002;296:1029-1031
Lif
e E
xpec
tan
cy i
n Y
ears
Year

What is Dementia?
An acquired disorder producing decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
Progressive and disabling
NOT a part of pure aging
Very different from normal cognitive lapses
AD by far the most common cause

When to be Concerned Sometimes it is the psychomotor slowing of aging
+ Recall of words or names temporarily lost+ Misplacing the car keys+ Worrying about memory+ Why are you in front of the refrigerator?
Never retrieving names or words Losing the car, major financial mistakes Forgetting entire conversations or events Not recognizing that there is a memory problem Repetition not just for emphasis

Evaluation of Dementia1
Screening At annual physical >70 or earlier if red flags
Ask patient about any new problems with memory, mood, behavior and driving
Baseline MMSE and clock drawing or 3-word recall and clock (mini-cog)
Evaluation for positive screen Add reliable informant to interview Structured criteria – DSM or NINCDS-AD Search for causes Identify and manage co-morbidities Genetic testing not recommended in 2012

Chemistries (BUN, Cr, electrolytes, BS, calcium), CBC, Liver function tests
Thyroid, pituitary-adrenal axis Vitamin levels – B12, folic acid (?)
Serology for Lyme, HIV, Syphyllis Brain image (CT without contrast) IF <65,
symptoms recent (<2yrs), focal neurologic signs, suspicion of NPH, or recent trauma
Neuropsychological testing if diagnosis unclear
Evaluation of Dementia2
Small GW, et al. JAMA. 1997;278:1363-1371

Risk Factors for AD Definite Possible/Probable Age Head injury Family History Diabetes Atherosclerosis (stroke) History of depression Hypertension (stroke)HSV Apolipoprotein E4 Education (-) Down’s Syndrome Statins (-) Female Gender Exercise (-) Multiple mutations Intellectual work (-)

Physician Role in Care of Dementia Patients
Thorough evaluation to make the diagnosis Honest information - truth, but not bludgeon Continuing care - "patient" includes family unit, as well
as the victim with plaques and tangles Reality testing - timing and appropriateness of support
services and institutionalization Ethical and appropriate choices for EOL care - not at
first encounter, but not to wait for a crisis either+ Restricted Rx, advance directives beyond DNR+ Code status, tube feeding, hospitalization, Abx

Maximize General Medical Health
Decrease excess morbidity; i.e., evaluation and optimal care for co-morbidities - all worsen cognition Periodic examinations Routine lab screening, based on problem list Prevention interventions that make sense
+ Vaccines, mammograms, FOB/endoscopy, OP?+ Only if action consistent with advance directives
Comprehensive evaluation for sudden decline; delirium common, AD doesn’t worsen overnight

Non-pharmacologic Interventions Care management and psychosocial interventions Education of caregivers
+ Understanding of the disease+ Avoid antipsychotics
Performance and behavior+ Scheduled toileting, behavior modification+ Exercise+ Music, massage, pet therapy
Environmental modification+ Safe space to wander+ Remove toxins, weapons

Does AD Caregiver Support Effect Nursing Home Admission?
Randomized trial of >200 AD spouses or caregivers, follow up 3.5 yrs
6 sessions of individual, family counseling within 4 months of enrollment and join support group
What happened to the Alzheimer patients after their caregivers attended the 6 sessions?
What about nursing home admission?
Mittelman MS et al. JAMA. 1996;276:1725-1731

Mittelman MS et al. JAMA. 1996;276:1725-1731
Probability of NH Admission After Caregiver Intervention
Pro
po
rtio
n o
f A
D P
atie
nts
Rem
ain
ing
at
Ho
me
Time in Years
2/3 RR,329 days more at
home
Caregivers in intervention 1/3 less likely to place spouses in NH; greatest benefit if mild or moderate dementia

Treatment of AD Symptoms
Consider possibility of excess disability
Depression - >50% during disease course
Agitation, aggression, delusions
Wandering – behavioral, caregiver interventions
Incontinence – evaluate, treat
Malnutrition – treat, but weight loss common
Altered sleep – behavioral, modern hypnotics

Treatment of AD Pathology Proven effective therapies+ Reduce stroke risk+ Cholinesterase inhibitors (“minimally effective”)+ Memantine (not much better)+ Proven ineffective therapies+ Antioxidants+ Estrogen+ Anti-inflammatory drugs (NSAIDs)+ Drugs to improve cerebral blood flow
Statins? Probably not

Cholinesterase Inhibitor Side Effects
Common, sometimes transient, but may be long-lasting and disabling - dose-related; titrate slowly, take with food+GI – NVD, anorexia, weight loss+Vivid dreams/nightmares
Less common
+Agitation
+Hypotension

Delay in NH Placement with Donepezil
0.4
0.6
0.8
1
0 100 200 300 400 500 600 700 800
Days
Pro
bab
ilit
y o
f R
emai
nin
g a
t H
om
e Placebo
High Dose
Higher Dose

Drugs for Dementia Behavior Disorders
Antipsychotics have demonstrated superior results in most randomized trials, but off label use
Be sure symptoms justify these dangerous drugs: agitation, aggression or delusions that disrupt care and impair life quality for caregiver and patient
Data conflicting whether atypical agents are better, but easier to use – fewer daily side effects of sedation or movement disorders, but FDA black box for all antipsychotic agents (stroke, CV death)
Use should be short-term, low dose

Resources for Managing Dementia
Attorney for will, conservatorship, estate planning; can be helpful with advance directives
Community: neighbors & friends, aging & mental health networks, adult day care, respite care, home-health agency
Organizations: Alzheimer’s Association (caregiver support groups), Area Agencies on Aging, Councils on Aging
Services: Meals-on-Wheels, senior citizen centers

Principles of Dementia Care
Complicating diseases often missed Hospitals are dangerous - avoid if at all possible
Dementia brain exquisitely sensitive to drugs - avoid
Useful Rx should not be withheld for age or dementia
Painful Rx should be very carefully considered
Symptomatic Rx without evaluation is dangerous
Stop Rx whose side effects are worse than symptoms
Assess response to Rx often and stop ineffective Rx

Summary
Dementia is common, but never normal aging
AD is most common, followed by vascular dementia and dementia with Lewy bodies
Thorough evaluation is mandatory, both for diagnosis and identification of co-morbidities
Treatment directed at function and quality of life, using drugs and behavioral interventions
Social and instrumental resources supplement care for patient, caregivers and family members