Embed Size (px)
DESCRIPTION
Original ReportSonography of Tears of the Distal Biceps Tendon Theodore T. Miller & Ronald S. Adler
Citation preview
Original Report
Sonography of Tears of the Distal Biceps Tendon
Theodore T. Miller & Ronald S. Adler
Distal biceps tendon rupture : - rare, only 3% of all biceps tendon tears
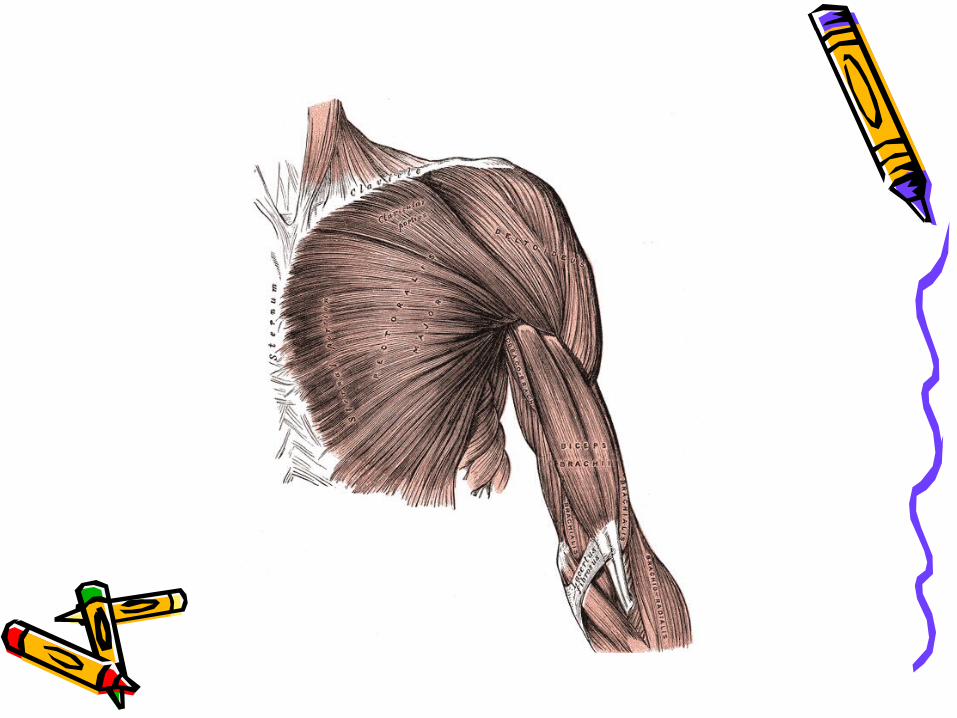
- is easily diagnosed on physical examination as a palpable defect in the antecubital fossa, a palpable mass in the anteri- or aspect of arm, and a weakness of flexion & supination
- clinical diagnose is more difficult, in cases of partial tear that are not retracted tendon because of intact aponeurosis
With MR imaging, a complete tear diagnosed by :
- absence of the tendon at its insertion
- tendon retraction
- edema or hemorrhage in the tendon sheath
MR imaging is the gold standard, but sonography is less ex-
pensive, more rapidly performed, and the contralateral elbow
is readily available for comparison
MATERIALS AND METHODESMATERIALS AND METHODES
Sonographic examination of 7 men : Sonographic examination of 7 men : * 5 recreational athletes * 5 recreational athletes * 1 competitive amateur power lifter * 1 competitive amateur power lifter * 1 manual laborer * 1 manual laborer
Mechanism of injury was eccentric contraction of the elbow Mechanism of injury was eccentric contraction of the elbow
All patients described a popping sensation at the time of injury, All patients described a popping sensation at the time of injury, pain, weakness of flexion, and swelling pain, weakness of flexion, and swelling
They were referred by orthopedist of suspected tears of the distal They were referred by orthopedist of suspected tears of the distal
biceps tendon for imaging : biceps tendon for imaging :
* 5 patients for sonography ( 1 with MRI ) * 5 patients for sonography ( 1 with MRI )
* 2 patients for MRI ( 2 with sonography ) * 2 patients for MRI ( 2 with sonography )
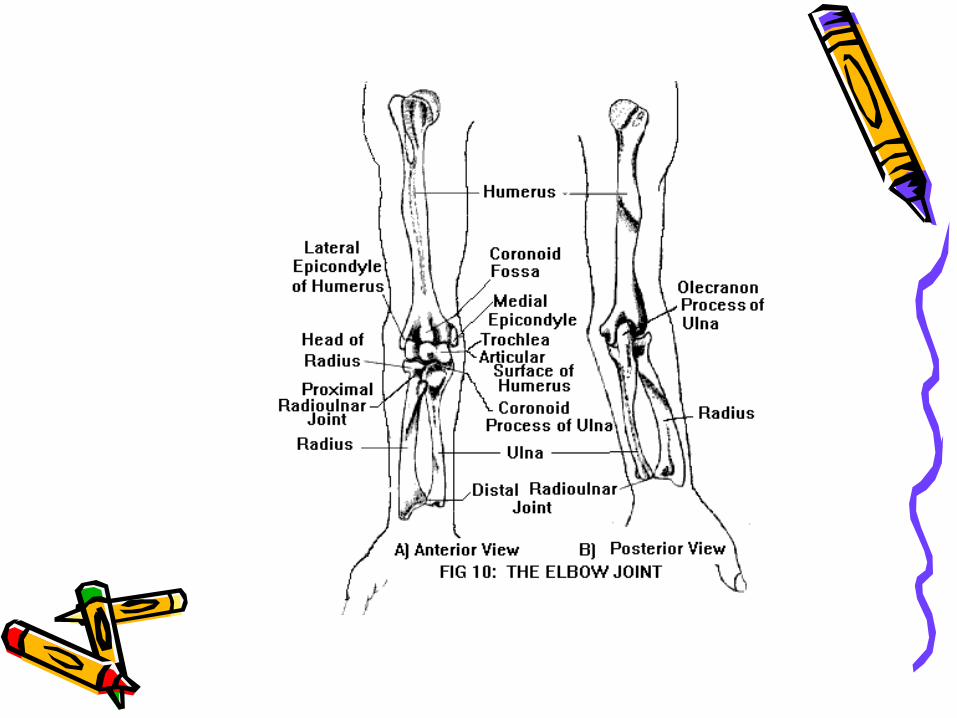
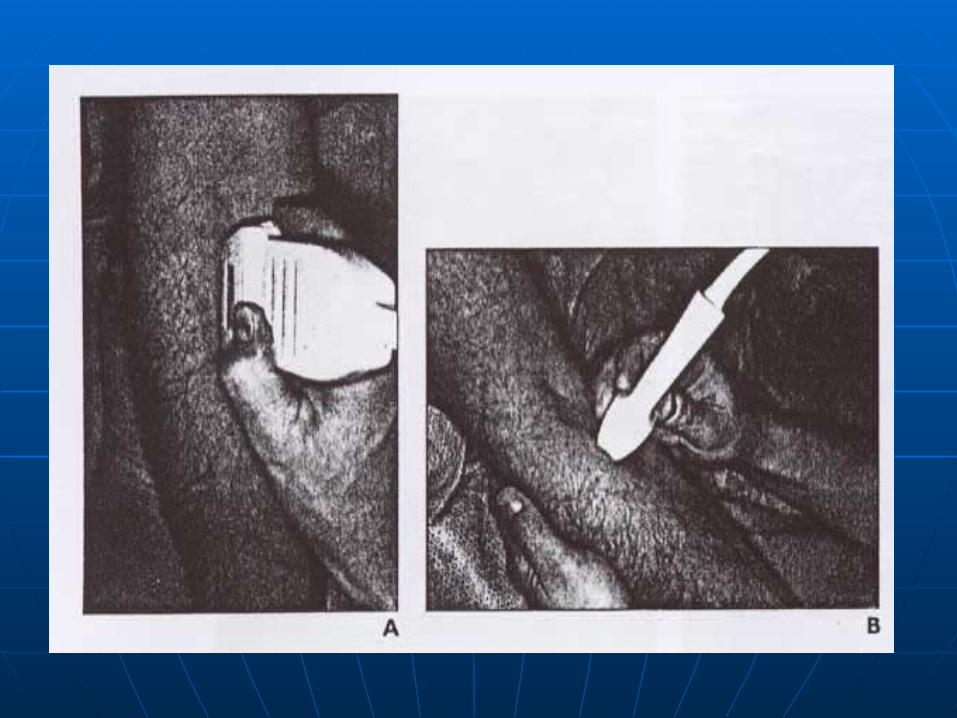
The forearm was maximally supinated to bring the tendinous in-The forearm was maximally supinated to bring the tendinous in-
sertion on the radial tuberosity into view sertion on the radial tuberosity into view
For longitudinal images, the transducer is on oblique plane slight-For longitudinal images, the transducer is on oblique plane slight-
ly inferolaterally to the long axis of forearm. For transverse i-ly inferolaterally to the long axis of forearm. For transverse i-
mages, the transducer is perpendicular to the long axis of forearmmages, the transducer is perpendicular to the long axis of forearm
The imaging criteria for rupture : The imaging criteria for rupture :
- tendinous discontinuity with or without retraction - tendinous discontinuity with or without retraction
- surrounding hypoechoic fluid on sonography - surrounding hypoechoic fluid on sonography
- high-signal-intensity fluid on T2-weighted images - high-signal-intensity fluid on T2-weighted images
The imaging criteria for partial tear : The imaging criteria for partial tear :
- thickening or thinning of the tendon - thickening or thinning of the tendon
- contour irregularity or waviness - contour irregularity or waviness
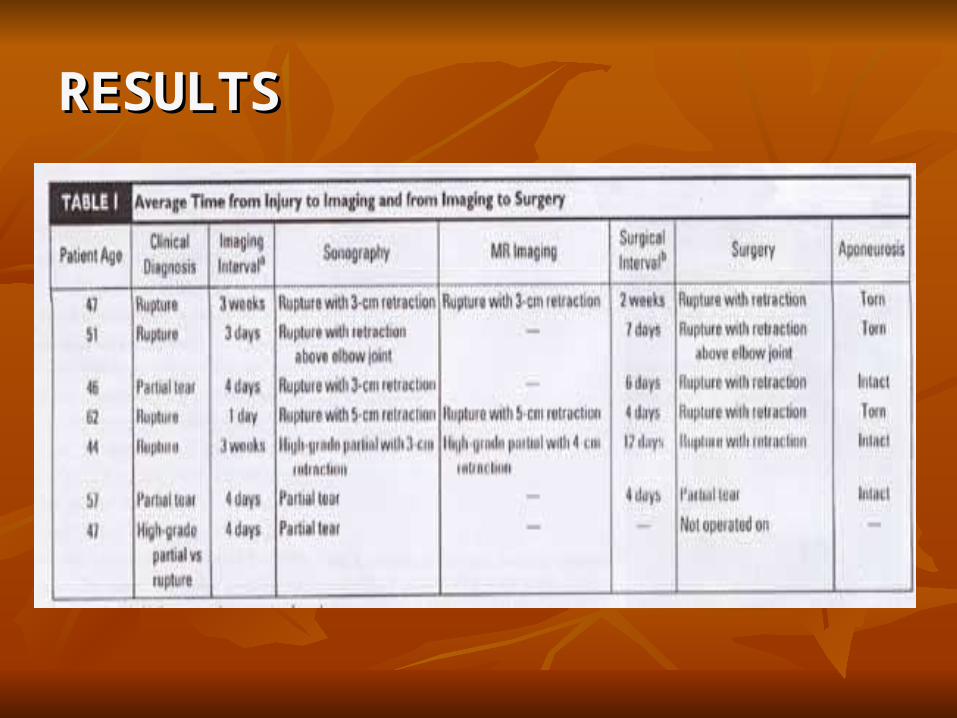
RESULTS RESULTS
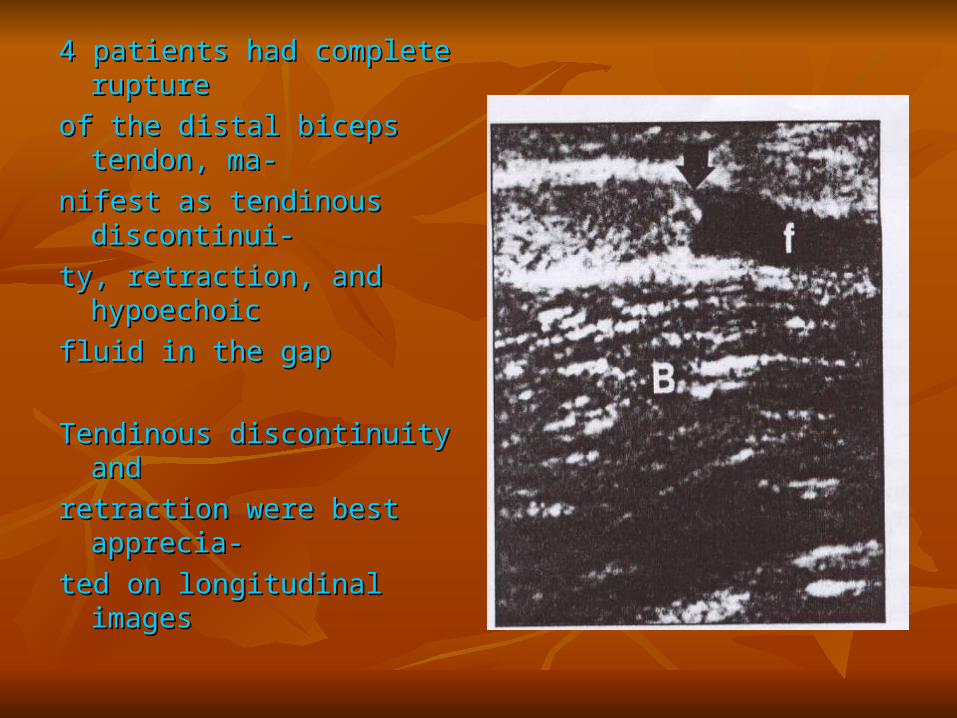
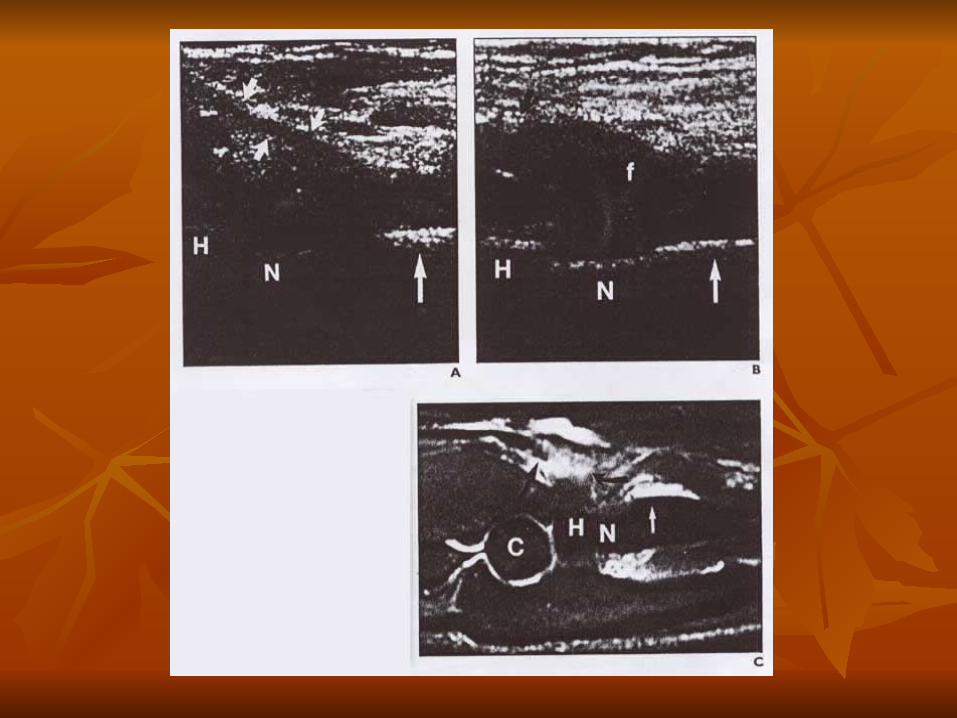
4 patients had complete 4 patients had complete rupture rupture
of the distal biceps tendon, ma-of the distal biceps tendon, ma-
nifest as tendinous discontinui-nifest as tendinous discontinui-
ty, retraction, and hypoechoic ty, retraction, and hypoechoic
fluid in the gap fluid in the gap
Tendinous discontinuity and Tendinous discontinuity and
retraction were best apprecia-retraction were best apprecia-
ted on longitudinal images ted on longitudinal images
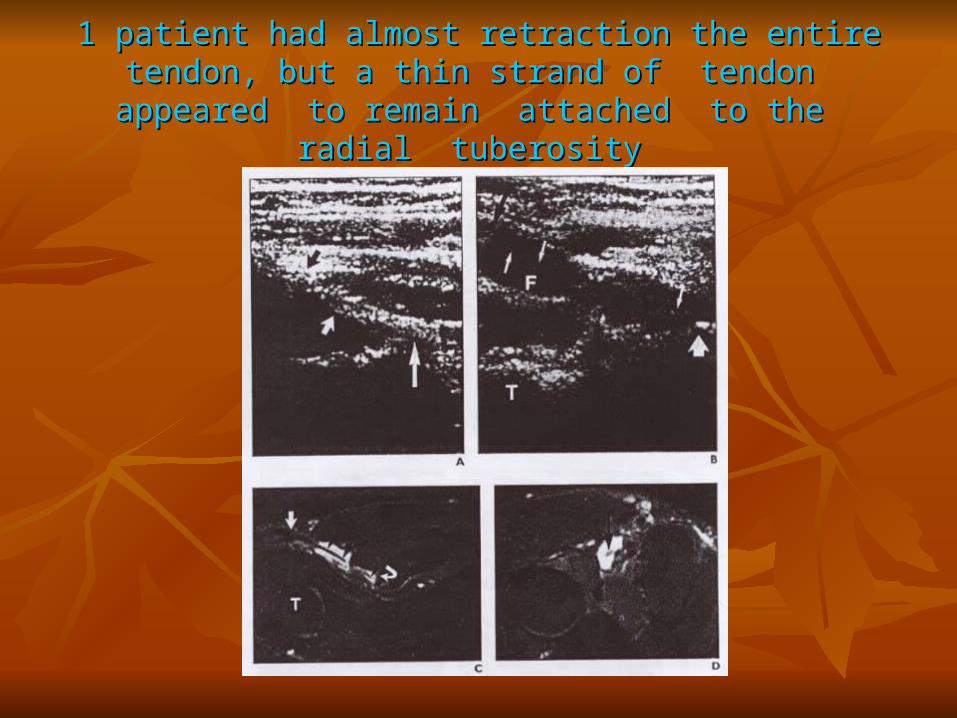
1 patient had almost retraction the entire tendon, but a thin strand 1 patient had almost retraction the entire tendon, but a thin strand of tendon appeared to remain attached to the radial tuberosityof tendon appeared to remain attached to the radial tuberosity
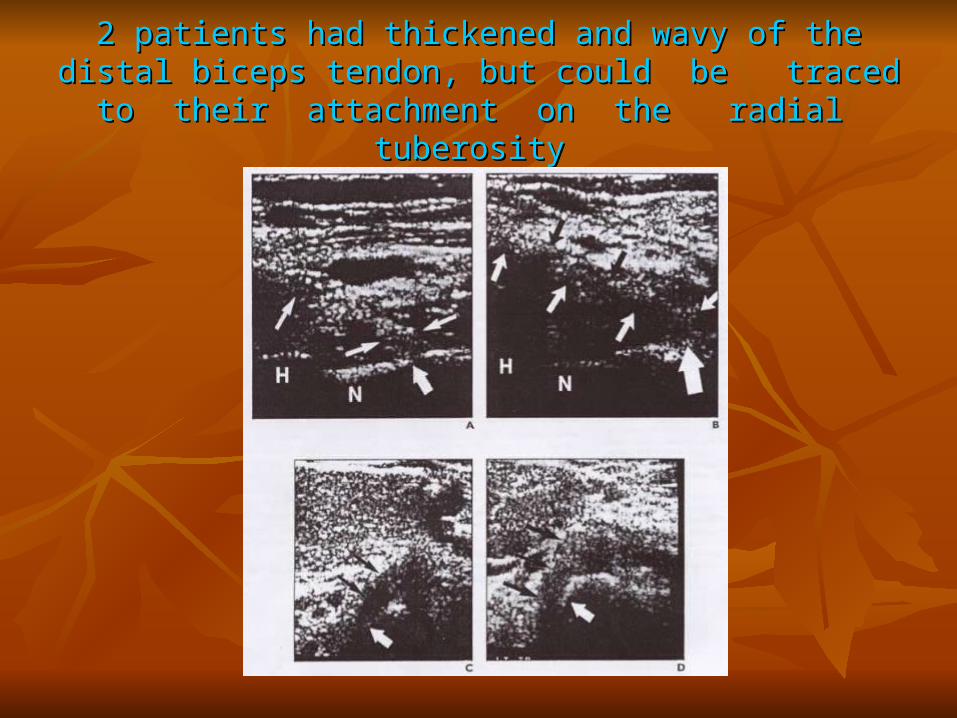
2 patients had thickened and wavy of the distal biceps tendon, but 2 patients had thickened and wavy of the distal biceps tendon, but could be traced to their attachment on the radial could be traced to their attachment on the radial
tuberositytuberosity
Sonography altered treatment of 2 patients :Sonography altered treatment of 2 patients : In one patient :In one patient :- initially clinical impression - initially clinical impression was a partial tear was a partial tear
- sonography showed complete - sonography showed complete rupture rupture
- treatment was changed from - treatment was changed from conservative to operativeconservative to operative
In another patient : In another patient : - initially clinical impression - initially clinical impression suspected high-grade partial suspected high-grade partial tear tear
- sonography showed a partial - sonography showed a partial tear with most of the tendon tear with most of the tendon intact intact
- treatment was changed from - treatment was changed from planned operative to conser-planned operative to conser- vative with NSAIDvative with NSAID
DISCUSSION
MR imaging :
-accuracy is 100% in 24 pa-
tients combined from two
series
Sonography :
-accuracy cannot be ad-
dressed because of retro-
spective nature, nonblinded
examinations in two instan-
ces, and small number of
patients
MR imaging :
-alters treatment in 8 of 21
patients (Fitzgerald)
Sonography :
-alters treatment in 2 of 7
patients
MR imaging :
-in 10 patients, tendon re-
traction <8cm correlated
with an intact aponeurosis
and >8cm correlated with a
torn aponeurosis (Le Huec)
Sonography :
-in 2 patients, tendon retrac-
tion <8cm had a torn apo-
neurosis
MR imaging :
-in partial tears, abnormal
intratendinous signal inten-
sity and thinning or thicke-
ning of the tendon are best
assessed in axial plane
Sonography :
-in partial tears, thickening
and altered echogenicity of
the tendon were apprecia-
ted in axial and longitudi-
nal planes, and irregular
contour was appreciated in
longitudinal plane only
MR imaging :
-assessment of tendon
thickness is based on the
experience of viewer with
normal biceps tendon
(Fitzgerald)
Sonography :
-assessment of tendon
thickness is based on the
comparison with the nor-
mal contralateral elbow
The advantage of sonography is its ability to optimize the
imaging plane with real-time scanning to best display ten-
don abnormality
The limitation of sonography is its dependence on the skill
and experience of the operator
Larger series investigating the accuracy of sonography of
this rare injury are necessary to determine if sonography
can be used for screening of suspected distal biceps tendon
injury and for people who cannot undergo MR imaging














![Vol [Nov 2007] 1 - Bonefix | Orthopaedicbonefix.co.nz/portals/160/files/CJOS 1.pdf · Biceps tendon decompression can relieve the symptoms of primary biceps tendonitis through a tenosynovial](https://img.pdfslide.us/doc/110x75/5f5cc85b81ddc17f426fca12/vol-nov-2007-1-bonefix-1pdf-biceps-tendon-decompression-can-relieve-the.jpg)