Embed Size (px)
DESCRIPTION
jurnal
Citation preview

AJR:201, August 2013 W283
establishing the correct diagnosis more chal-lenging for the radiologist.
CT is the modality of choice and is the best radiologic tool currently available for reveal-ing both perforation and the underlying condi-tion when the diagnosis is unexpected. Unlike CT, sonography does not typically play a role in investigation of suspected small bowel per-foration or other acute abdominal conditions associated with overt peritonitis, pneumoperi-toneum, and bowel obstruction. However, so-nography may be the initial test chosen in pa-tients with localized abdominal symptoms when gastrointestinal perforation is not a ma-jor clinical consideration. This patient group typically includes referrals for acute appendi-citis, cholecystitis, pyelonephritis, colonic di-verticulitis, and pelvic inflammatory disease. Therefore, we believe that an understanding of the appearances of small bowel perforation seen during general abdominal sonography will aid the radiologist in identifying the true cause of abdominal pain when this condition presents with nonspecific symptoms. Further-more, there is a growing interest in recogniz-ing the role of sonography in imaging of the bowel [8], which, combined with the rising utilization of this noninvasive radiation-free modality in both the emergency department and outpatient settings [9], makes this area of abdominal imaging particularly pertinent to the radiologist.
In a recent article [10], investigators high-lighted the potential role of sonography in the diagnosis of perforated pyloroduodenal
Sonography of Small Bowel Perforation
Siarhei Kuzmich1,2
Christopher J. Burke3
Chris J. Harvey1
Tatsiana Kuzmich4
Daniel T. M. Fascia1
Kuzmich S, Burke CJ, Harvey CJ, Kuzmich T, Fas-cia DTM
1Department of Imaging, Hammersmith Hospital, London, United Kingdom.
2 Present address: Department of Radiology, Newham University Hospital, Glen Rd, London E13 8SL, United Kingdom. Address correspondence to S. Kuzmich ([email protected]).
3 Department of Radiology, Guy’s and St. Thomas’ Hospitals, London, United Kingdom.
4Department of Radiology, North Middlesex University Hospital, London, United Kingdom.
Gastrointest ina l Imaging • Cl in ica l Perspect ive
WEB This is a web exclusive article.
AJR 2013; 201:W283–W291
0361–803X/13/2012–W283
© American Roentgen Ray Society
erforation of the mesenteric small bowel, although uncommon in North America and Western Eu-rope, remains a potentially life-
threatening condition associated with high morbidity and mortality and poorer outcomes when the diagnosis is delayed [1–3]. The ra-diologist is usually the first to suggest a pre-operative diagnosis because the clinical pre-sentation of small bowel perforation may be variable and is related to a multitude of fac-tors, including the source of the perforation and its mechanism, the site and extent of the perforation, time since perforation, the degree of contamination of the peritoneal cavity, and the patient’s age and comorbidity burden.
Causes of small bowel perforation are man-ifold and include trauma and iatrogenic inju-ry, inflammatory conditions, infection, isch-emic change, diverticula, foreign bodies, and malignancy. Although some contribut-ing conditions such as traumatic or iatrogenic injury and Crohn disease are often anticipat-ed, other rare culprits such as an ingested for-eign body are commonly unexpected. Anoth-er unusual but important cause—perforated intestinal tuberculosis—is likely to continue to present a diagnostic challenge to the radi-ologist; this old disease is a growing concern, particularly in urban areas, because of com-bined effects of immigration, HIV infection, drug resistance, and rising poverty [4–7]. Whatever the cause, the rarity of small bow-el perforation combined with its propensity for nonspecific clinical presentation makes
Keywords: CT, small bowel perforation, sonography
DOI:10.2214/AJR.12.9882
Received August 28, 2012; accepted after revision October 28, 2012.
P
OBJECTIVE. This article aims to illustrate the spectrum of sonographic findings in per-foration of the small bowel due to a variety of causes and discusses the potential role of so-nography in the diagnosis.
CONCLUSION. Although sonography is not the first-line investigation of choice in sus-pected small intestinal perforation, an understanding of the characteristic appearances seen during general abdominal sonography may aid the radiologist in the early diagnosis. Recog-nition of small bowel perforation on general abdominal sonography will shorten the time to diagnosis and ultimate surgical management.
Kuzmich et al.Sonography of Small bowel Perforation
Gastrointestinal ImagingClinical Perspective
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
80.2
46.4
6.25
on
08/1
7/14
fro
m I
P ad
dres
s 18
0.24
6.46
.25.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W284 AJR:201, August 2013
Kuzmich et al.
peptic ulcer. By contrast, this article stems from our wish to share our experiences in so-nographic diagnosis of common and unusual perforations of the jejunum and ileum encoun-tered during general abdominal sonography. Correlation with CT is given when possible, and examples of surgically and histologically proven cases are discussed.
Sonographic ConsiderationsTechnique and Normal Appearances
The primary general abdominal survey is followed by focused assessment of the symp-tomatic area using 2-6–MHz curvilinear and 6-12–MHz linear multifrequency transduc-ers, depending on the achievable distance to the area of interest. Any area of potential bow-el-related disease or injury is analyzed as de-scribed later in this article. Probe compression is used judiciously to facilitate visualization by bringing the area of interest into focus and displacing loops of bowel. We did not use hy-drosonography for any of the cases presented here. This technique can potentially improve bowel conspicuity and aid evaluation but may be of limited use in practice because small bowel perforation is usually encountered when it is not expected and the patient may be in pain and experiencing nausea, making admin-istration of water unwanted. Furthermore, the finding of perforation would precipitate a nil-by-mouth status as a prerequisite to a possible operative procedure.
In most patients, much of the small bow-el, from the duodenum to the terminal ileum, can be imaged with conventional sonography
without any special preparation [11]. The small intestine usually lies in a regular manner in the abdomen with the jejunum positioned higher and more to the left and the ileum lower and more to the right, although loops can alter their position. The caliber of the normal small bowel does not usually exceed 3 cm. The nor-mal wall thickness is less than 3 mm. Small bowel loops are usually mobile; are compress-ible; and show peristalsis, which may be lively or sluggish depending on the physiologic state (Fig. 1). The circular folds are more prominent in the jejunum, diminishing toward the termi-nal ileum, which may be foldless.
Like elsewhere in the gastrointestinal tract, the bowel wall can be visualized as a five-lay-ered structure under optimal scanning con-ditions, but basic identification of thin dark muscularis and more echogenic mucosa will usually suffice in practice [12].
Abnormal Small BowelWhen diseased, the bowel wall often thick-
ens and becomes rigid with reduced or absent peristalsis. Sonographic identification of the site of abnormality therefore relies on detec-tion of tangible bowel wall thickening, which varies in extent depending on the underlying condition. Similar to a pattern approach used in CT evaluation, observing the degree of wall thickening, the length of abnormal bow-el, and associated perienteric changes on so-nography can be used to narrow the differen-tial diagnosis [13].
Sonographic Signs of PerforationLike with gastrointestinal perforation from
locations other than the small bowel, pneumo-peritoneum may be present but is often mini-mal or absent outside the setting of traumatic and iatrogenic bowel injuries. Walled-off or localized perforation is common. Free sponta-neous perforation usually results in a dramatic clinical presentation with generalized peritoni-tis and thus is optimally imaged with CT.
On sonography, small amounts of free gas are seen as strongly echogenic foci or lines on the liver surface producing ring-down or comet-tail artifacts (Fig. 2A). Free air can also be detected beneath the anterior abdom-
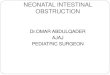
Fig. 1—Sonographic appearance of normal small bowel in healthy 25-year-old man. Oblique color Doppler image, paraumbilical view, obtained using 10-MHz transducer depicts cross sections of mid small bowel (asterisks), captured during peristaltic wave, and mesentery with vessels (m).
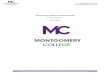
AFig. 2—Sonographic appearances of free intraperitoneal gas.A, 39-year-old man with perforated ileal tuberculosis. Right intercostal view obtained with 6-MHz transducer shows bright echogenic line of free air (arrows) overlying liver (L) surface with posterior comet-tail artifact (arrowheads). Inset shows corresponding axial CT image.B, 35-year-old woman with Crohn’s disease who presented with perforated ileum. Transverse right flank view obtained with 6-MHz transducer depicts pocket of dependent free gas (arrows) with “dirty shadowing” (arrowheads) in fluid collection (asterisks) beneath abdominal wall (aw). Inset shows corresponding axial CT image.
B
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
80.2
46.4
6.25
on
08/1
7/14
fro
m I
P ad
dres
s 18
0.24
6.46
.25.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:201, August 2013 W285
Sonography of Small bowel Perforation
inal wall where it accumulates with the pa-tient supine [10] (Fig. 2B). With judicious use, careful sonography can detect a minimal amount of free gas, equating to a single bub-ble, because of its exclusive ability to pro-duce distinctive bright echoes and artifacts [14, 15]. Nevertheless, it is worth remember-ing that although sonography has a number of strengths including its unique real-time value and excellent spatial resolution, the di-agnostic quality of a sonographic study can be compromised by obesity, extensive fecal loading in the colon, bowel obstruction, and pain. Other potential weaknesses of this mo-dality may be related to the skill of the opera-tor; the equipment used; and availability of ex-pertise for this type of evaluation, which will depend on the local radiology practice model.
Sonographic findings that suggest a per-foration site typically include unusual fluid collections related to a thickened segment of bowel associated with echogenic change in adjacent perienteric fat due to inflammation. Similar to CT, the presence of extraluminal gas on sonography provides a useful clue to the diagnosis [16, 17].
Perforated DiverticulumJejunal Diverticulum
Jejunal diverticula are usually multiple ac-quired pseudodiverticula along the mesen-teric border seen in middle-aged and elderly
patients. Most patients are asymptomatic. Je-junal diverticula can be recognized on sonog-raphy as fluid-filled pouchlike structures ad-jacent to the normal bowel [18].
Diverticulitis and perforation do occur and are thought to be caused by infection, blunt trauma, and foreign-body impaction [19–21]. Localized perforation with abscess formation is common. Sonography often shows a col-lection of fluid related to a segment of mildly thickened jejunum, echogenic perienteric fat caused by inflammatory change, and pockets of extraluminal gas [22] (Fig. 3A).
Ileal DiverticulumIleal diverticulum is usually caused by a
congenital Meckel diverticulum but can also be acquired [23–25]. The “rule of twos” is frequently quoted—that is, Meckel divertic-ulum occurs in 2% of the population 2 feet from the ileocecal valve and is usually 2 inches long. However, the size and site vary. Right lower quadrant and mid abdominal loca-tions with a tendency of the diverticulum to lie toward the midline are frequently reported [26].
Uncomplicated Meckel diverticulum is usually too subtle and is rarely seen. When diverticulitis occurs, the area of abnormality may become conspicuous and is recognized owing to the presence of echogenic inflam-matory change in the fat surrounding the di-verticulum next to a mildly thickened ileal
segment. The inflamed diverticulum is visu-alized as a blind-ending thick-walled pouch or tubular fluid-filled structure surrounded by echogenic fat. This structure is usually con-stant in position and inflexible. Visualization of a communication of the structure with the ileum provides a helpful clue to the diagno-sis (Fig. 3B). Similar to our experience, sono-graphic manifestation of an inflamed Meckel diverticulum has been consistently described, both in children and adults [27–29].
When perforation occurs, sonography shows a fluid collection next to a thickened segment of small bowel and often the pres-ence of extraluminal gas in the fluid [30] (Fig. 3C). In our experience, a perforated diverticulum may or may not be evident de-pending on its size, the degree of its col-lapse resulting from perforation, and the quality of the sonographic study, which may be restricted by guarding.
Potential pitfalls may arise, most commonly from perforated appendicitis and colonic diver-ticulitis, that can result in fluid collections and extraluminal gas lying near the small bowel. A periappendiceal abscess, for instance, can mimic perforated Meckel diverticulum when it involves the ileum. Visualization of an ab-normal appendix in such cases will confirm the correct diagnosis (Fig. 4A). Care should be taken not to confuse colonic diverticulum for a pocket of extraluminal gas when it lies close
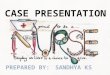
AFig. 3—Perforated versus nonperforated small bowel diverticulitis.A, 61-year-old man who presented with 5-day localized left abdominal pain and fever thought to be caused by pyelonephritis. Sonogram of left flank obtained with 6-MHz transducer shows oblique section of mildly thickened jejunum (j) and two small fluid collections (asterisks) of similar shape surrounded by echogenic fat. Small bright free gas bubbles (arrows) are difficult to see on this still image but were obvious during real-time scanning. Surgical resection revealed perforated jejunal diverticulitis and mesenteric abscess. Inset shows corresponding axial CT image.B, 32-year-old woman who presented with 3-day history of right upper quadrant pain and low-grade fever thought to be result of cholecystitis. Inset shows position of transducer (bar). Sonogram obtained with 3.5-MHz transducer depicts hypoechoic blind-ending structure (d) with thick irregular wall (arrowheads) arising from mildly thickened ileum (i). No extraluminal gas was identified. Pathology confirmed nonperforated inflamed Meckel diverticulum, which measured 3 × 2 cm.C, 72-year-old man with perforated ileal diverticulitis. Oblique pelvic view obtained using 3.5-MHz transducer shows segment of mildly thickened ileum (i) and adjacent fluid collection (asterisks) with surrounding echogenic fat. Note extraluminal gas pocket (arrows) seen as bright dependent line with “dirty shadowing” (arrowheads) in collection on left. Inset shows corresponding axial CT image.
CB
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
80.2
46.4
6.25
on
08/1
7/14
fro
m I
P ad
dres
s 18
0.24
6.46
.25.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W286 AJR:201, August 2013
Kuzmich et al.
to the small bowel (Fig. 4B). In perforated co-lonic diverticulitis, the diverticular abscess may also lie close to the small bowel. In this case, sonography can suggest the true cause by showing involvement of the mildly thick-ened colon with evidence of diverticulosis. Although sonographic differentiation may be problematic, CT will usually help (Fig. 4C). Finally, when extensive bowel thickening, a mass, or significant lymphadenopathy is pres-
ent, other causes including perforated malig-nancy should be considered.
Crohn DiseaseBecause sonography readily displays thick-
ened small bowel, this noninvasive radiation-free modality is increasingly being chosen as both the initial test and follow-up technique in Crohn disease, particularly in the younger population [31]. Sonographic manifestations
of active Crohn disease are often characteris-tic. The hallmark of the disease is circumfer-ential encasement of a thickened bowel loop with echogenic fat, which reflects transmural inflammation and is sometimes referred to as the “creeping fat” sign [32] (Fig. 5A). The mesentery is often thickened and echogenic. A predilection of this disease for the terminal ileum is well known.
Abscess formation is common and can re-sult from transmural inflammation and a deep ulcer penetrating into perienteric tissues or may be caused by localized perforation [32, 33]. A Crohn abscess is usually walled off because of preexisting fibrotic and adhesive perienteric changes and may be mesenteric, interloop, abdominal wall, or retroperitone-al in location. Sinuses and fistulas are fre-quent. Free spontaneous perforation and in-traperitoneal rupture of a Crohn abscess also occur, although much less frequently [34]. Free perforation will typically present with overt peritonitis unless the patient is receiv-ing high-dose corticosteroid therapy.
Sonography can be the first modality to de-tect an extraluminal Crohn abscess, which is usually visualized as a fluid collection with or without free gas near the diseased bowel (Fig. 5B). Focal perforation may be seen as a track of bright echogenic gas bubbles extend-ing through the irregularly thickened bowel wall beyond its outline [32]. Detection of free intraperitoneal gas will suggest free perfora-tion (Fig. 2B).
AFig. 4—Potential mimics of perforated small bowel diverticula.A, 30-year-old woman with perforated appendicitis. Inset shows position of transducer (bar). Sonogram obtained with 2.5-MHz probe shows mildly thickened ileum (i) next to small fluid collection (asterisk) that contains pocket of dependent gas (arrowhead) with shadow. Because there is also enlarged appendix (arrow) involved in collection, small periappendiceal abscess was suggested, which was confirmed at surgery.B, 69-year-old man with colonic diverticulitis. Inset shows position of transducer (bar). Sonogram obtained using 10-MHz transducer shows jejunum (j) lying close to descending colon (c) and colonic diverticulum seen as bright shadowing pocket (arrowhead) between cross sections of jejunum and colon. This finding should not be confused with pocket of extraluminal gas seen in perforation.C, 66-year-old man with sigmoid diverticulitis complicated by pericolonic abscess. Sonogram of left iliac fossa obtained with 3.5-MHz probe depicts abscess (asterisks) lying close to bowel loop that was identified to be sigmoid colon (s) with diverticulosis on careful survey. Inset shows corresponding axial CT image.
CB
A B
Fig. 5—Nonperforated versus perforated small bowel in patients with Crohn’s disease.A, 50-year-old woman with Crohn’s disease involving distal ileum. Inset shows position of transducer (bar). Color Doppler sonogram obtained with 3.5-MHz probe shows thick-walled hyperemic ileum in cross section (i) next to bladder (ub). Note thickened echogenic mesentery (m) and layer of echogenic fat (arrowheads) encasing whole bowel circumference including antimesenteric border.B, 25-year-old woman with Crohn’s disease involving terminal ileum complicated by mesenteric abscess. Inset shows position of transducer (bar). Sonogram obtained with 3.5-MHz probe shows thickened terminal ileum (i) and adjacent abscess (asterisk).
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
80.2
46.4
6.25
on
08/1
7/14
fro
m I
P ad
dres
s 18
0.24
6.46
.25.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:201, August 2013 W287
Sonography of Small bowel Perforation
The major differential diagnosis of Crohn disease is tuberculosis, which should be con-sidered in a high-risk population.
Intestinal TuberculosisThe clinical manifestations of intestinal tu-
berculosis are often nonspecific. Patients may present with diarrhea, weight loss, and abdom-inal pain [35, 36]. The ileocecal region is the most common intestinal site. Ulcerative, hy-pertrophic, and combined forms are usually described [37, 38].
The most frequent finding in cases of intes-tinal tuberculosis on sonography is moderate hypoechoic thickening of the terminal ileum and cecum, which may be quite irregular de-pending on the disease stage (Fig. 6A). When
the distal ileum becomes tightly narrowed in advanced disease, dilatation of the proximal bowel will be seen. Mesenteric lymphadenop-athy is often evident, which may show central necrosis but can be nonspecific.
A CB
Fig. 6—Nonperforated versus perforated small bowel in patients with ileal tuberculosis.A, 29-year-old man with ileocecal tuberculosis. Inset shows position of transducer (bar). Sonogram obtained using 3.5-MHz probe shows thickened terminal ileum (ti) and cecum (c). Note gas pocket (arrowhead) retained within terminal ileum wall; this finding suggests presence of ulceration.B, 34-year-old man with perforated distal ileum from tuberculosis. Inset shows position of transducer (bar). Sonogram obtained using 3.5-MHz probe shows cross section of thickened terminal ileum (ti) and large pockets of dependent extraluminal gas (arrow) in adjacent fluid collection (asterisk), which is obscured by gas shadow and thus is poorly seen.C, Same patient as in B. Coronal reformatted CT image depicts cecum (c), distal ileum (i), pockets of gas (arrow), and fluid collection (asterisk). These findings were difficult to assess with sonography. Site of perforation is not evident on CT, but subsequent surgery revealed ileal perforation was 4 cm proximal to ileocecal junction.
A B
C D
Fig. 7—Peritoneal involvement in tuberculosis versus mesothelioma and carcinomatosis.A, 52-year-old man with peritoneal tuberculosis. Transverse sonogram of right flank obtained using 6-MHz transducer shows omental cake (o) adherent to mildly thickened hypoechoic parietal peritoneum (asterisk) in ascites. Corresponding axial CT image (inset) shows findings indicating close correlation between two modalities.B, Same patient as in A. Transverse sonogram of left flank (inset) shows jejunal loops (b) clumped together and small pool of ascitic fluid, which allows visualization of small adhesion (arrow), nodule (arrowhead), and minimally thickened parietal peritoneum (asterisk). Minimal peritoneal thickening is also evident on corresponding axial CT image, but adhesion and nodule are not visible.C, 62-year-old man with malignant abdominal mesothelioma. Inset shows position of transducer (bar). Sonogram of left flank obtained using 9-MHz transducer shows small bowel (b) encased by extensively thickened visceral peritoneum (asterisk) outlined with ascites. D, 59-year-old man with peritoneal carcinomatosis from colorectal carcinoma. Inset shows position of transducer (bar). Transverse sonogram of right flank shows ascites (A) and peritoneal metastatic deposits (arrows).
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
80.2
46.4
6.25
on
08/1
7/14
fro
m I
P ad
dres
s 18
0.24
6.46
.25.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W288 AJR:201, August 2013
Kuzmich et al.
Diseased bowel can perforate spontaneous-ly during and after antituberculous treatment. Perforation is frequently solitary and walled off but can also be multifocal and free, resulting in generalized peritonitis [3, 39]. Sonography may uncover the usual features of perforation such
Fig. 8—40-year-old man with abdominal pain and known polyarteritis nodosa. Inset shows position of transducer (bar). Paraumbilical view obtained using 6-MHz transducer shows concentrically thickened ileal loops (i) and small amount of ascites (asterisk). Moderate dilatation of proximal small bowel was also present (not shown).
Fig. 9—Perforations caused by foreign bodies.A, 62-year-old man with acute left abdominal colicky pain suspected of having renal colic. Sonographic view (inset) of left flank obtained using 10-MHz transducer shows linear foreign body (arrows) embedded in thickened wall of jejunum (j) and trace of fluid (asterisks), which correlates with subsequent CT. No free gas is present. Fish bone perforating jejunum was found at surgery.B, 64-year-old man suspected of having colonic diverticulitis. Sonogram of left lower flank obtained using 6-MHz transducer shows fluid collection (asterisks) next to thickened small bowel (j) and echogenic curvilinear structure piercing bowel wall with its end (arrow) in fluid collection. A few small bubbles of gas were present in collection. Correlation of these sonographic findings is shown with unenhanced axial CT image (inset). Chicken bone fragment perforating mid small bowel was revealed at surgery.C, 40-year-old man with paraumbilical pain of 5 days’ duration with fever. Paraumbilical sonogram shows echogenic linear structure (arrows) related to fluid collection (asterisks). Patient consented to CT 2 days later after his symptoms had worsened. Multiplanar reformatted CT image (inset) shows corresponding foreign body, which is now lying deeper than on sonography 2 days earlier, surrounded by larger collection. No free gas is present. Surgery revealed toothpick in perienteric collection and perforated ileum.D, 30-year-old woman who presented with 2-month history of nonspecific pelvic pain and low-grade fever. Infraumbilical sonogram reveals bright linear structure (cursors) embedded in abdominal wall at one end and projecting toward abdomen with another end (arrows). Sonogram (inset) obtained using 10-MHz transducer shows morphology suggestive of intrauterine contraceptive device (IUCD). IUCD embedded in ileum with interloop abscess was found at surgery.
as a fluid collection, pneumoperitoneum, and extraluminal gas pockets near thickened bow-el. Sonographic evaluation, however, may be complicated by pockets of extraluminal gas obscuring views and by guarding in the area of interest (Fig. 6B). CT in these cases is more likely to be diagnostic (Fig. 6C).
Other helpful sonographic findings are re-lated to peritoneal involvement, which is of-ten associated with intestinal tuberculosis. These findings are ascites, mesenteric thick-ening, omental caking, peritoneal thickening, adhesions, and peritoneal tuberculous nod-ules [40–43]. Ascites may be diffuse or locu-lated, with fluid ranging from simple to com-plex containing movable strands and strings. The mesentery is often thickened and echo-genic with mesenteric leaves clamped togeth-er. Bowel loops are frequently fixed, which is recognized by their lack of movement and lack of separation in ascites. The great-er omentum is often thickened, echogenic, and heterogeneous. Omental cakes are recognized as bulks of thickened omentum seen beneath the abdominal wall anterior to the bowel loops. Omental caking is most easily seen in
ascites (Fig. 7A). Omental cakes may be free floating or may be adherent to the abdominal wall or visceral peritoneum. Mild hypoechoic thickening of the parietal and visceral perito-neum may be evident.
The presence of ascites greatly enhances the sonographic ability to detect subtle perito-neal changes that are otherwise occult such as minimally thickened peritoneum, adhesions, and small tuberculous nodules (Fig. 7B). De-tecting these signs on sonography, which are often too subtle to be seen on CT, will provide valuable additional clues to the diagnosis.
The appearances of peritoneal tuberculosis largely overlap with those of malignant con-ditions involving the peritoneum such as me-sothelioma and carcinomatosis. Care should be taken not to confuse thickened peritoneum and nodules caused by malignant mesotheli-oma with peritoneal tuberculosis. Unlike tu-berculosis, peritoneal thickening and nodules in mesothelioma tend to be much more ex-tensive (Fig. 7C). Peritoneal implants in car-cinomatosis are much larger, are discrete, or are congregated soft-tissue nodules of vary-ing sizes, whereas tuberculous nodules are
A
C
B
D
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
80.2
46.4
6.25
on
08/1
7/14
fro
m I
P ad
dres
s 18
0.24
6.46
.25.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:201, August 2013 W289
Sonography of Small bowel Perforation
typically small [35, 44] (Fig. 7D). Nontuber-culous peritonitis should also be considered.
In the correct clinical context, combined sonographic and CT findings may be highly suggestive but often are nonspecific. Tubercu-losis, unfortunately, remains a great mimicker.
VasculitisVasculitis is a rare cause of perforation, but
sonography may be the initial investigation in patients with vasculitis of various causes pre-senting with abdominal symptoms. The main finding is usually diffuse small bowel thicken-ing, which is thought to be caused by a combi-nation of edema and hemorrhage in the bowel wall (Fig. 8). Sonography will also show edem-atous mesentery; bowel dilatation; ascites; and, in the case of perforation, free gas. Similar to the CT appearances of vasculitis, the sonographic appearances are nonspecific and overlap con-siderably with findings of other conditions such as infection, ischemia, radiation enteritis, an-gioedema, and hemorrhage [45–47].
Polyarteritis NodosaPolyarteritis nodosa is a fibrinoid necro-
tizing vasculitis that mainly involves small and medium-sized arteries of the muscles. When it occurs in the small bowel, the con-dition causes acute abdominal pain. Perfora-tion occurs in an estimated 5% of cases [48].
Wegener GranulomatosisWegener granulomatosis is an uncommon
multisystemic disorder characterized histopath-ologically by necrotizing granulomatous vascu-litis that can affect the small bowel, although it most commonly involves the respiratory tract and kidneys. Bowel ulcerations resulting in perfora-tions have been reported [49–51].
Henoch-Schönlein PurpuraHenoch-Schönlein purpura is frequently as-
sociated with bowel involvement, but perfora-tion is very rare [52, 53].
Foreign BodiesPerforation is uncommon because ingested
foreign bodies that have passed below the di-aphragm will usually pass in the stool. When perforation occurs, localized abdominal symp-toms usually imitate various inflammatory conditions depending on the site of the per-foration and the patient’s medical history and age [54–56]. Most patients will have no recol-lection of ingesting a foreign body. Both sharp and blunt foreign bodies can cause bowel per-foration, which is thought to result from slow pressure necrosis.
A B
Fig. 10—Nonperforated versus perforated small bowel in patients with lymphoma.A, 62-year-old woman with proven non-Hodgkin B-cell lymphoma involving mid ileum. Inset shows position of transducer (bar). Paraumbilical sonogram obtained with 5-MHz probe shows abnormal segment of ileum with concentrically thickened hypoechoic wall (w) and dilated lumen (L). This sonographic finding was unexpected in this patient who was clinically suspected of having cholelithiasis.B, 56-year-old woman with follicular lymphoma involving mid small bowel loop who presented with increasing abdominal pain and rising inflammatory markers. Coronal CT image shows large mesenteric mass (M) infiltrating and causing perforation of jejunal loop (j) with adjacent pockets of free gas (arrows) and free fluid (asterisk) extending into pelvis.
In very recent or early perforation, there may be no fluid collection or extraluminal gas, but sonography may uncover the cause of abdomi-nal pain by showing a foreign body embedded in the thickened bowel wall (Fig. 9A). How-ever, more commonly, sonography will reveal a fluid collection adjacent to a short segment of mildly thickened bowel and inflammatory change in the perienteric fat [57–60]. Extralumi-nal gas next to the bowel is a helpful finding, but free gas is not always present in our experience.
Examples of ingested foreign bodies in-clude fish and chicken bones and toothpicks, which are seen as bright linear or curvilin-ear objects of peculiar geometry piercing the bowel wall or lying in a fluid collection adja-cent to the bowel [61–63] (Figs. 9B and 9C). Ingested wire bristle from a grill cleaning brush is another example of a potential per-forating foreign body that radiologists should be aware of, as Grand and colleagues [64] re-ported in a recent study. Perforating ingested plastic bread-bag clips have also been report-ed, although rarely [65, 66].
A variety of other rare perforating foreign bodies have been reported in the literature. On the very odd occasion, even an intrauterine contraceptive device may perforate the uterus and invade the small bowel [67, 68] (Fig. 9D).
MalignancyA variety of intraabdominal malignancies,
both primary and secondary, may cause small bowel perforation. Even benign desmoid tu-
mors leading to perforation have been reported [69, 70]. Nevertheless, of all small bowel ma-lignant perforations, lymphoma is the most fre-quent cause [71].
Intestinal lymphomas may be primary le-sions or part of disseminated disease and are usually non-Hodgkin type. Typical sono-graphic findings include concentric asymmet-ric or symmetric homogeneous hypoechoic bowel thickening with loss of the layered pat-tern. Wall thickening is usually more than 2 cm. The affected segment is frequently in the ileum and may be single or multiple with nar-rowing or enlargement of the lumen. Aneu-rysmal dilatation of the lumen, although not always present, is characteristic (Fig. 10A). Single or multiple ill-defined extraluminal masses and mesenteric and retroperitoneal lymphadenopathy may be evident.
Perforation can occur spontaneously and during treatment [72, 73]. Sonography may detect both an intestinal lesion and typical signs of perforation as discussed earlier, but the role of this modality is limited and CT is invariably preferred (Fig. 10B).
Other CausesSonography is of very limited use and is typ-
ically not chosen for evaluation of traumatic and iatrogenic perforations, which are usually a major clinical consideration.
Advanced segmental or focal bowel ischem-ia of various causes such as thromboembolic occlusion of the mesenteric vessels, strangu-
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
80.2
46.4
6.25
on
08/1
7/14
fro
m I
P ad
dres
s 18
0.24
6.46
.25.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

W290 AJR:201, August 2013
Kuzmich et al.
lated hernias, adhesive bands, volvulus, and vasculitis can result in transmural necrosis and perforation. At our institutions, sonography is not chosen when ischemic bowel is a consid-eration. Although a variety of suggestive fea-tures such as bowel thickening and dilatation, free fluid, portal vein gas, and mesenteric and portal vein thrombosis may be identified, so-nographic assessment is often disappointing when such patients are, on occasion, referred for sonography instead of CT.
Radiotherapy for cervical carcinoma and other intraabdominal malignancies may be as-sociated with late complications including bowel perforation [74]. AIDS-related infec-tions such as Mycobacterium avium–intracel-lulare and cytomegalovirus infections may involve the small bowel and may cause perfora-tion in severely immunocompromised patients [75, 76]. Long-standing use of nonsteroidal an-tiinflammatory drugs may lead to small bow-el ulceration and perforation, although this is rare. Various small bowel infections and infes-tations, particularly typhoid, can cause small bowel perforation, but these entities are excep-tionally rare in the western population [77].
ConclusionSmall bowel perforation is uncommon but
often produces subtle yet diagnostic sonograph-ic abnormalities of which the radiologist should be aware. Detection of localized extralumi-nal gas, a fluid collection, and inflammatory change adjacent to a thickened bowel segment should alert the radiologist to suspect a per-foration. A targeted CT study may be instigated when required depending on the initial sono-graphic study.
Familiarity with the characteristic sono-graphic appearances combined with a careful sonographic technique should allow a timely diagnosis during general abdominal sonogra-phy. Prompt diagnosis will facilitate correct management planning and a prompt opera-tive procedure.
References 1. Waisberg J, Bromberg SH, Franco MI, De Godoy
AC. Spontaneous perforations of the small intes-
tine. Int Surg 1997; 82:420–424
2. Kimchi NA, Broide E, Shapiro M, Scapa E. Non-
traumatic perforation of the small intestine: report
of 13 cases and review of the literature. Hepato-
gastroenterology 2002; 49:1017–1022
3. Lee MJ, Cresswell FV, John L, Davidson RN. Di-
agnosis and treatment strategies of tuberculous
intestinal perforations: a case series. Eur J Gas-
troenterol Hepatol 2012; 24:594–599
4. Crofts JP, Gelb D, Andrews N, Delpech V, Watson
JM, Abubakar I. Investigating tuberculosis trends
in England. Public Health 2008; 122:1302–1310
5. Hill AN, Becerra JE, Castro KG. Modelling tu-
berculosis trends in the USA. Epidemiol Infect
2012; 140:1862–1872
6. Langlois-Klassen D, Wooldrage KM, Manfreda J,
et al. Piecing the puzzle together: foreign-born
tuberculosis in an immigrant-receiving country.
Eur Respir J 2011; 38:895–902
7. Sibartie V, Kirwan WO, O’Mahony S, Stack W,
Shanahan F. Intestinal tuberculosis mimicking
Crohn’s disease: lessons relearned in a new era.
Eur J Gastroenterol Hepatol 2007; 19:347–349
8. Maturen KE, Wasnik AP, Kamaya A, et al. Ultra-
sound imaging of bowel pathology: technique and
keys to diagnosis in the acute abdomen. AJR 2011;
197:[web]W1067–W1075
9. Levin DC, Rao VM, Parker L, Franqos AJ. Non-
cardiac point-of-care ultrasound by nonradiolo-
gist physicians: how widespread is it? J Am Coll
Radiol 2011; 8:772–775
10. Kuzmich S, Harvey CJ, Fascia DTM, et al. Perfo-
rated pyloroduodenal peptic ulcer and sonogra-
phy. AJR 2012; 199:[web]W587–W594
11. Peck R. The small bowel. In: Meire H, Cosgrove
D, Dewbury K, Farrant P, eds. Abdominal and
general ultrasound, 2nd ed. London, UK:
Churchill Livingstone, 2001:823–839
12. Kuzmich S, Howlett DC, Andi A, Shah D, Kuzmich
T. Transabdominal sonography in assessment of
the bowel in adults. AJR 2009; 192:197–212
13. Macari M, Megibow AJ, Balthazar EJ. A pattern
approach to the abnormal small bowel: observa-
tions at MDCT and CT enterography. AJR 2007;
188:1344–1355
14. Wilson SR, Burns PN, Wilkinson LM, Simpson
DH, Muradali D. Gas at abdominal US: appear-
ance, relevance, and analysis of artifacts. Radiol-
ogy 1999; 210:113–123
15. Muradali D, Wilson S, Burns PN, Shapiro H,
Hope-Simpson D. A specific sign of pneumoperi-
toneum on sonography: enhancement of the peri-
toneal stripe. AJR 1999; 173:1257–1262
16. Hainaux B, Agneessens E, Bertinotti R, et al. Ac-
curacy of MDCT in predicting site of gastrointes-
tinal tract perforation. AJR 2006; 187:1179–1183
17. Ghekiere O, Lesnik A, Millet I, Hoa D, Guillon F,
Taourel P. Direct visualization of perforation sites
in patients with a non-traumatic free pneumoperito-
neum: added diagnostic value of thin transverse
slices and coronal and sagittal reformations for
multi-detector CT. Eur Radiol 2007; 17:2302–2309
18. Sinha R. Jejunal diverticulosis: sonographic diag-
nosis. J Clin Ultrasound 2006; 34:84–87
19. Gross SA, Katz S. Small bowel diverticulosis: an
overlooked entity. Curr Treat Options Gastroen-
terol 2003; 6:3–11
20. Longo WE, Vernava AM 3rd. Clinical implica-
tions of jejunoileal diverticular disease. Dis Colon
Rectum 1992; 35:381–388
21. Coulier B, Broze B. Jejunal diverticulitis: US and
CT findings with anatomical correlation. JBR-
BTR 2000; 83:153–155
22. Kelekis AD, Poletti PA. Jejunal diverticulitis with
localized perforation diagnosed by ultrasound: a
case report. Eur Radiol 2002; 12(suppl 3):S78–S81
23. Wilcox RD, Shatney CH. Surgical significance of
acquired ileal diverticulosis. Am Surg 1990;
56:222–225
24. De Raet J, Brugman T, Geukens A. Non-Meckel’s
ileal diverticulitis with perforation: a rare cause of
acute right lower quadrant pain. Acta Chir Belg
2010; 110:90–92
25. Jones D, McMillin R, Greene F. Complications of
acquired diverticula of the ileum. Am Surg 1983;
49:218–222
26. Bennett GL, Birnbaum BA, Balthazar EJ. CT of
Meckel’s diverticulitis in 11 patients. AJR 2004;
182:625–629
27. Baldisserotto M, Maffazoni DR, Dora MD. Sono-
graphic findings of Meckel’s diverticulitis in chil-
dren. AJR 2003; 180:425–428
28. Levy AD, Hobbs CM. Meckel diverticulum: ra-
diologic features with pathologic correlation. Ra-
dioGraphics 2004; 24:565–587
29. Wilhelm A, Langer C, Müller A, Becker H. Ultra-
sound diagnosis of Meckel diverticulitis in adults
[in German]. Z Gastroenterol 2001; 39:73–75
30. Coulier B, Sergeant L, Maldague P, Ramboux A,
Broze B, Hamels J. Complicated Meckel’s diver-
ticulum diagnosed preoperatively in three cases
by complementing CT with detailed US studies.
JBR-BTR 2003; 86:65–71
31. Horsthuis K, Bipat S, Bennink RJ, Stoker J. In-
flammatory bowel disease diagnosed with US,
MR, scintigraphy, and CT: meta-analysis of pro-
spective studies. Radiology 2008; 247:64–79
32. Sarrazin J, Wilson SR. Manifestations of Crohn
disease at US. RadioGraphics 1996; 16:499–520
33. Cellini C, Safar B, Fleshman J. Surgical manage-
ment of pyogenic complications of Crohn’s dis-
ease. Inflamm Bowel Dis 2010; 16:512–517
34. Freeman HJ. Spontaneous free perforation of the
small intestine in Crohn’s disease. Can J Gastro-
enterol 2002; 16:23–27
35. Jadvar H, Mindelzun RE, Olcott EW, Levitt DB.
Still the great mimicker: abdominal tuberculosis.
AJR 1997; 168:1455–1460
36. Horvath KD, Whelan RL. Intestinal tuberculosis:
return of an old disease. Am J Gastroenterol 1998;
93:692–696
37. Engin G, Acunas B, Acunas G, Tunaci M. Imaging
of extrapulmonary tuberculosis. RadioGraphics
2000; 20:471–488
38. Leder RA, Low VH. Tuberculosis of the abdo-
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
80.2
46.4
6.25
on
08/1
7/14
fro
m I
P ad
dres
s 18
0.24
6.46
.25.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved

AJR:201, August 2013 W291
Sonography of Small bowel Perforation
men. Radiol Clin North Am 1995; 33:691–705
39. Scriven JM, Berry D. Multiple small bowel perfo-
rations in a patient on treatment of tuberculosis. J
R Coll Surg Edinb 1996; 41:353
40. Vanhoenacker FM, De Backer AI, Op de Beeck B, et
al. Imaging of gastrointestinal and abdominal tuber-
culosis. Eur Radiol 2004; 14(suppl 3):E103–E115
41. Akhan O, Pringot J. Imaging of abdominal tubercu-
losis. Eur Radiol 2002; 12:312–123
42. Jain R, Sawhney S, Bhargava DK. Diagnosis of ab-
dominal tuberculosis: sonographic findings in pa-
tients with early disease. AJR 1995; 165:1391–1395
43. Hanbidge AE, Lynch D, Wilson SR. US of the
peritoneum. RadioGraphics 2003; 23:663–685
44. Burrill J, Williams CJ, Bain G, Conder G, Hine
AL, Misra RR. Tuberculosis: a radiologic review.
RadioGraphics 2007; 27:1255–1273
45. Lalani TA, Kanne JP, Hatfield GA, Chen P. Imag-
ing findings in systemic lupus erythematosus. Ra-
dioGraphics 2004; 24:1069–1086
46. De Backer AI, De Schepper AM, Vandevenne JE,
Schoeters P, Michielsen P, Stevens WJ. CT of angio-
edema of the small bowel. AJR 2001; 176:649–652
47. Ha HK, Lee SH, Rha SE, et al. Radiologic fea-
tures of vasculitis involving the gastrointestinal
tract. RadioGraphics 2000; 20:779–794
48. Jee KN, Ha HK, Lee IJ, et al. Radiologic findings
of abdominal polyarteritis nodosa. AJR 2000;
174:1675–1679
49. Deniz K, Ozseker HS, Balas S, et al. Intestinal in-
volvement in Wegener’s granulomatosis. J Gastro-
intestin Liver Dis 2007; 16:329–331
50. Geraghty J, Mackay IR, Smith DC. Intestinal perfo-
ration in Wegener’s granulomatosis. Gut 1986;
27:450–451
51. Pickhardt PJ, Curran VW. Fulminant enterocolitis
in Wegener’s granulomatosis: CT findings with
pathologic correlation. AJR 2001; 177:1335–1337
52. Chung DJ, Park YS, Huh KC, Kim JH. Radiologic
findings of gastrointestinal complications in an
adult patient with Henoch-Schönlein purpura. AJR
2006; 187:[web]W396–W398
53. Shirahama M, Umeno Y, Tomimasu R, et al. The
values of colour Doppler ultrasonography for
small bowel involvement of adult Henoch-Schön-
lein purpura. Br J Radiol 1998; 71:788–791
54. Rodríguez-Hermosa JI, Codina-Cazador A, Sir-
vent JM, Martín A, Gironès J, Garsot E. Surgi-
cally treated perforations of the gastrointestinal
tract caused by ingested foreign bodies. Colorec-
tal Dis 2008; 10:701–707
55. Pinero Madrona A, Fernández Hernández JA,
Carrasco Prats M, Riquelme Riquelme J, Parrila
Paricio P. Intestinal perforation by foreign bodies.
Eur J Surg 2000; 166:307–309
56. Goh BK, Chow PK, Quah HM, et al. Perforation
of the gastrointestinal tract secondary to ingestion
of foreign bodies. World J Surg 2006; 30:372–377
57. Rioux M, Langis P. Sonographic detection of
clinically unsuspected swallowed toothpicks and
their gastrointestinal complications. J Clin Ultra-
sound 1994; 22:483–490
58. Matricardi L, Lovati R. Intestinal perforation by a
foreign body: diagnostic usefulness of ultrasonog-
raphy. J Clin Ultrasound 1992; 20:194–196
59. Drakonaki E, Chatzioannou M, Spiridakis K, Pan-
agiotakis G. Acute abdomen caused by a small
bowel perforation due to a clinically unsuspected
fish bone. Diagn Interv Radiol 2011; 17:160–162
60. Coulier B. Diagnostic ultrasonography of perforat-
ing foreign bodies of the digestive tract [in French].
J Belge Radiol 1997; 80:1–5
61. Goh BK, Tan YM, Lin SE, et al. CT in the preop-
erative diagnosis of fish bone perforation of the
gastrointestinal tract. AJR 2006; 187:710–714
62. Zissin R, Osadchy A, Gayer G. Abdominal CT
findings in small bowel perforation. Br J Radiol
2009; 82:162–171
63. Coulier B, Tancredi MH, Ramboux A. Spiral CT
and multidetector-row CT diagnosis of perforation
of the small intestine caused by ingested foreign
bodies. Eur Radiol 2004; 14:1918–1925
64. Grand DJ, Cloutier DR, Beland MD, Mayo-Smith
WW. Inadvertent ingestion of wire bristles from a
grill cleaning brush: radiologic detection of unsus-
pected foreign bodies. AJR 2012; 198:836–839
65. Newell KJ, Taylor B, Walton JC, Tweedie EJ. Plas-
tic bread-bag clips in the gastrointestinal tract: re-
port of 5 cases and review of the literature. CMAJ
2000; 162:527–529
66. Tang AP, Kong AB, Walsh D, Verma R. Small
bowel perforation due to a plastic bread bag clip: the
case for clip redesign. ANZ J Surg 2005; 75:360–362
67. Leijonmarck CE, Fenyö G, Räf L. Nontraumatic
perforation of the small intestine. Acta Chir Scand
1984; 150:405–411
68. Rochelson BL, Mann WJ, Fromowitz F, Baim R.
Asymptomatic perforation of the small intestine
by a copper-7 intrauterine device. N Y State J Med
1985; 85:515–516
69. Buckley JA, Fishman EK. CT evaluation of small
bowel neoplasms: spectrum of disease. Radio-
Graphics 1998; 18:379–392
70. Jalini L, Hemming D, Bhattacharya V. Intraabdom-
inal desmoid tumour presenting with perforation.
Surgeon 2006; 4:114–116
71. Catena F, Ansaloni L, Gazzotti F, et al. Small bowel
tumours in emergency surgery: specificity of clinical
presentation. ANZ J Surg 2005; 75:997–999
72. Ara C, Coban S, Kayaalp C, Yilmaz S, Kirimlioglu
V. Spontaneous intestinal perforation due to non-
Hodgkin’s lymphoma: evaluation of eight cases.
Dig Dis Sci 2007; 52:1752–1756
73. Sakakura C, Hagiwara A, Nakanishi M, et al.
Bowel perforation during chemotherapy for non-
Hodgkin’s lymphoma. Hepatogastroenterology
1999; 46:3175–3177
74. Cheung CP, Chiu HS, Chung CH. Small bowel
perforation after radiotherapy for cervical carci-
noma. Hong Kong Med J 2003; 9:461–463
75. Pantongrag-Brown L, Nelson AM, Brown AE,
Buetow PC, Buck JL. Gastrointestinal manifesta-
tions of acquired immunodeficiency syndrome:
radiologic-pathologic correlation. RadioGraphics
1995; 15:1155–1178
76. Reeders JW, Yee J, Gore RM, Miller FH, Megibow
AJ. Gastrointestinal infection in the immunocompro-
mised (AIDS) patient. Eur Radiol 2004; 14:84–102
77. Stoner MC, Forsythe R, Mills AS, Ivatury RR,
Broderick TJ. Intestinal perforation secondary to
Salmonella typhi: case report and review of the
literature. Am Surg 2000; 66:219–222
Dow
nloa
ded
from
ww
w.a
jron
line.
org
by 1
80.2
46.4
6.25
on
08/1
7/14
fro
m I
P ad
dres
s 18
0.24
6.46
.25.
Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
righ
ts r
eser
ved